disease-related and all-cause health care … 08_164-175.pdfjmcp march 2008 vol. 14, no. 2 ,...
TRANSCRIPT

164 Journal of Managed Care Pharmacy JMCP March 2008 Vol. 14, No. 2 www.amcp.org
ABSTRACT
BACKGROUND: Gout is a common cause of inflammatory arthritis in the United States, and its prevalence has increased in recent decades, espe-cially among older adults. Older adults with gout are of particular interest because they tend to experience higher rates of tophi, an advanced stage of gout, than do younger patients.
OBJECTIVE: For older adults with gout to (1) assess health care utilization and costs from a third-party payer perspective; (2) evaluate health care costs related to tophi; and (3) explore the relationship between elevated serum uric acid (UA) level, an indicator of disease control, and health care utilization.
METHODS: Data were extracted from the Integrated Healthcare Information Services (IHCIS) claims database (1999-2005), which includes approxi-mately 40 private health plans in the United States for approximately 13 million beneficiaries, about 4% of whom are aged 65 years or older. Patients were included in the study if they: (1) had 2 diagnoses of gout (International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM] code of 274.xx) on separate medical claims or 1 gout diagnosis plus at least 1 gout-related pharmacy claim (i.e., allopurinol, probenecid, colchicines, or sulfinpyrazone); (2) were at least 65 years old at the first diagnosis date (study index date); and (3) had 1 year of continuous eligibility both before and after the study index date. A comparison sample of elderly members without gout was selected using a 1:1 match to gout patients based on age, gender, and geographic region. Individuals in the comparison group also had 1 year of continuous eligibility both before and after the study index date, defined as the same index date as the respective matched gout patient. Patients with possible tophi were identified from at least 1 medical claim with an ICD-9-CM code 274.8x (274.81=gouty tophi of the ear; 274.82 = gouty tophi of other sites except ear; 274.89 = gout with other specified manifestations) during the 12-month study period following the study index date. Additionally, a subgroup of gout patients with at least 1 serum UA measure was selected. Patients were divided into 3 groups according to their serum UA level on the earliest test date (serum UA index date): low (< 6 mg per dL), moderate-high (6-8.99 mg per dL), and very high (≥ 9 mg per dL). Health care utilization was categorized into inpatient services, outpatient services, emergency room services, other medical services, and use of prescription drugs. Medical services were classified by the place of service indicated in the claim. Medical services costs and pharmacy costs were defined as the amount paid to the provider plus member cost share (e.g., deductible, copayment). Two types of costs were assessed in the analysis: total all-cause health care costs and gout-related costs, defined as costs associated with a claim with a primary or secondary diagnosis of gout (ICD-9-CM code 274.xx). Differences in total all-cause health care costs were calculated by comparing (1) gout patients and gout-free members during the 12-month period following the study index date; (2) gout patients with and without tophi during the 12-month period following the study index date; and (3) gout patients across the 3 serum UA categories during the 12-month period following the serum UA index date. Multivariate regression analyses were used to control for patients’ baseline demograph-ics, prior comorbidities indicated by the Deyo-Charlson Comorbidity Index, and number of medications used during the 12 months prior to the study index date.
RESULTS: Over the 7 years of claims data through 2005, there were 11,935 gout patients aged 65 years or older. The sample had an average age of 71.4 years and was predominantly male (73.5%). In the 12 months following the study index date, the mean unadjusted per-patient gout- related health care cost was $876 (standard deviation $3,373) in 2005 dol-lars, 5.9% of the total all-cause health care cost of $14,734 (SD $27,401) for gout patients. Unadjusted total 12-month all-cause health care cost for the gout-free members was $9,219 (SD $20,186). After statistical adjust-ment for comorbidities, the difference in total 12-month all-cause health care costs between gout patients and gout-free members was $3,038 (P < 0.001). A diagnosis suggesting possible tophi was found in 2.0% (n = 240) of gout patients in the sample. After statistical adjustment for comorbidities, the difference in total 12-month all-cause health care costs between gout patients with and without tophi was $5,501 (P < 0.001), and the difference in total adjusted 12-month gout-related costs between patients with and without tophi was $1,710 (P < 0.001). Among the 2,237 (18.7%) patients with at least 1 serum UA measure, 28.3% had a low serum UA level, 52.4% had a moderate-high serum UA level, and 19.3% had a very high serum UA level. For patients with low, moderate-high, and very high serum UA levels, regression-adjusted gout-related costs in the 12 months following the serum UA index date represented, respectively, 2.9%, 2.7%, and 3.9% of total regression-adjusted health care costs. The group with a very high serum UA level had significantly higher regression-adjusted total 12-month all-cause health care costs and gout-related costs compared with those with a low serum UA level ($3,103 and $276 higher, respectively).
CONCLUSIONS: Elderly patients with a diagnosis of gout have higher all-cause health care utilization and costs compared with matched elderly patients without a diagnosis of gout. Gout-related costs represent about 6% of total health care costs in elderly patients with gout. Very high serum UA levels (i.e., ≥ 9 mg per dL) and diagnoses suggesting possible tophi are associated with increased utilization and costs in elderly gout patients.
J Manag Care Pharm. 2008;14(2):164-75
Copyright © 2008, Academy of Managed Care Pharmacy. All rights reserved.
Disease-Related and All-Cause Health Care Costs of Elderly Patients With Gout
Eric Q. Wu, PhD; Pankaj A. Patel, PharmD, MS; Andrew P. Yu, PhD; Reema R. Mody, MBA, PhD; Kevin E. Cahill, PhD; Jackson Tang, BS; and Eswar Krishnan, MD, MPH
• The physiological pathway between hyperuricemia and prevalenceofgoutiswellunderstood.Fromanepidemiologicalperspective,however, the relationshipbetweenserumUAandcost of gout has not been well established, especially amongolderadults.
• Theexistingpharmacoeconomicsliteratureshowsthatthecostsof gout treatmentmay be substantial, although no cost study to our knowledge has focused specifically on the older adultpopulation.
What is already known about this subject
RESEARCH

www.amcp.org Vol. 14, No. 2 March 2008 JMCP Journal of Managed Care Pharmacy 165
Goutisadiseasecausedbythedepositionofmonosodiumurate crystals on the articular cartilage of joints and tissues like tendons. Gout currently affects approxi-
mately5.1millionpeopleintheUnitedStates1andisthemostcommoncauseof inflammatoryarthritis inmen.2,3 Intermsofprevalence,goutaffectsbetween0.4%and4.4%ofthepopulation, dependingonageandgender.4Theprevalenceofgouthasriseninrecentdecades.2,5-9Forexample,theincidencerateofprimarygoutintheUnitedStatesincreased2-foldbetweenthemid-1970sandthemid-1990s.5Theseincreasescanbeexplainedinpartbychangesintheprevalenceofseveralriskfactorsforgout,suchasobesity, increasing longevity,andhyperlipidemia.Other impor-tant risk factors include renal insufficiency, alcohol abuse, useofdiuretics inhypertensionandcongestivecardiac failure,andprophylacticlow-doseaspirin.2-4,10,11
Despitethehighprevalenceofgout,theeconomicburdenofthediseasehasnotbeenwellstudied.Theliteraturethatexists,however, indicates that thecostofgout treatmentmaybesub-stantial.Kimetal.estimatedthatannualgout-relatedtreatmentcostsfornewacutecasesintheUnitedStatesareapproximately$27million.2Brooketal. foundthat the totalannualemployerhealth benefit costs per person (i.e., medical and prescriptionclaims, sick and disability leave, and workers’ compensation)are$3,165higherforemployeeswithgoutcomparedwiththosewithoutgout.12
Onereasongoutcanbecostlyisthatthediseasecanevolveintoaphaseofchronictophaceousgout,characterizedbytophiformingaroundthejointsandsubcutaneoustissues.2,10Tophiarechalkydepositsof sodiumurate,whichcanproducepersistentpainandnervecompressionsyndrome,causeulcerationof theskin,andleadtojointdestructionanddeformities.2,10Thepres-ence of tophi in gout patients increaseswith the length of thediseasecourse.2,10,13Onaverage,tophidevelop11yearsaftertheinitialgoutflare-up.2
While gout tophi are prevalent among 12% to 55% ofuntreated gout patients overall, older adults with gout are ofparticular interest. Tophi ismore common amongolder adultswith gout and tends to develop relatively earlier in the courseoftheirdisease.14-16Diagnosisofgoutamongolderadultsisalsomore complicated than among other patients because of theresemblanceofgouttorheumaticarthritisandosteoarthritis.14,16 Equallychallengingistheachievementof2goalsingouttreat-ment: immediate control of symptoms during the acute phaseandmaintenanceofalowserumuricacid(UA)level(<6mgperdL),10,13 because of existing comorbidities, increased toxicity ofmedications,anddruginteractionsinolderadults.14-16Thelattergoalisespeciallycriticalingouttreatmentbecauseitmaypreventrecurrentgoutflares,inflammatoryresponsesduetodepositionofmonosodiumuratecrystals in jointsandsoft tissues.SerumUA control may even reverse urate deposition and reduce thecomplicationsintheurinarysystem.2,10,17-19,20
This study focuses on the economic costs of gout amongelderlyadultsaged65yearsandolderandhas3mainobjectives.Thefirstobjectiveistoexaminehealthcareutilizationanddirecthealthcarecostsamongelderlygoutpatientsfromathird-partypayer’s perspective. The existing literature has not provided acomprehensive picture of the economic aspects of gout amongolderadults,andthisresearchfillsthisvoid.Thesecondobjectiveofthestudyistoanalyzedirecthealthcarecostsamongelderlygout patients with tophi, an understudied group. The third objectiveistoexaminetheassociationbetweenserumUAlevelsandutilizationanddirecthealth care costs.While thepositiverelationship between serum UA and gout is well recognized,epidemiological studies have not focused on the relationshipbetweenserumUAandcost.
■■ Methods
Data SourceDatainthisstudywereobtainedfromtheIntegratedHealthcareInformation Services (IHCIS) claims database (1999-2005).IHCISincludesapproximately13millionenrollees(during2004)from40healthplansfromallcensusregionsintheUnitedStates.About4%ofenrolleesinthedatabase’scommercialormanagedcare plans are aged 65 years or older. The database containsinformationoneligibility,medicalclaims,andpharmacyclaims.Inpatient claims are summarized at the stay level. Medical servicescostsandpharmacycostsaredefinedasthetotalallowed
Disease-Related and All-Cause Health Care Costs of Elderly Patients With Gout
• Inthe12-monthperiodfollowingadiagnosisofgoutinagroupof elderly (aged 65 years or older) patients,mean unadjustedper-patientgout-relatedhealthcarecostwas$876,5.9%oftotal all-causehealthcarecostof$14,734,in2005dollars.
• Themean totaldirect12-monthall-causehealthcare cost forelderly gout patients was $14,734 compared with $9,219 forelderlymemberswithoutgout,adifferenceof$5,515(or59.8%).After controlling for comorbidities, 12-month all-cause healthcare costwas $3,038 (33.0%) higher for elderly gout patientsthanforgout-freemembers.
• Of the $876 total 12-month gout-related costs, 57.6% wasattributed to inpatient services, 23.6% to outpatient services,2.4%toemergencyservices,9.4%tootherservices,and7.1%toprescriptiondrugcosts.
• Elderly gout patients with possible tophi incurred higherregression-adjusted total 12-month all-causehealth care costsandgout-relatedcoststhanthosewithouttophi,withdifferencesof$5,501and$1,710,respectively.
• AveryhighserumUAlevel(i.e.,≥9mgperdL)wasassociatedwithanadditional$3,103inregression-adjustedtotal12-monthall-cause health care costs and $276 in regression-adjusted12-month gout-related costs, comparedwith a low serumUAlevel(i.e.,<6mgperdL).
What this study adds

166 Journal of Managed Care Pharmacy JMCP March 2008 Vol. 14, No. 2 www.amcp.org
amount,includingtheamountpaidtotheproviderplusmembercostsharing(e.g.,deductible,copayment).Laboratoryresultsareavailableforsomehealthplans.
Study Sample for Utilization and Cost Analysis of GoutEnrolleesincludedinthisstudyhadaminimumof1yearcon-tinuouseligibilityinahealthplanbothbeforeandafterthestudyindexdate,definedas thedateof the firstobservedgoutdiag-nosisduringthestudymeasurementperiodfrom1999to2005(Figure1).Studypatientswereatleast65yearsoldonthestudyindexdateandhadeither (1)2gout (International Classification of Diseases, Ninth Revision, Clinical Modification,21 ICD-9-CM, 274.xx)diagnoses thatwere identifiedondifferentdates in theprimaryorsecondarydiagnosiscodefieldsor (2)agoutdiagnosisandagout-relatedpharmacyclaim(i.e.,allopurinol,probenecid,colchicines,orsulfinpyrazone)identifiedbyNationalDrugCode(NDC)numbersduringthestudymeasurementperiod.Toesti-mate themedical and pharmacy costs associatedwith gout, agout-free comparison samplewas selected from the samedata-baseusinga1:1matchwithgoutpatients,basedonage(withamaximumof1-yeardifference),gender,andregion.Individualsin thecomparisongroupalsohad1yearcontinuouseligibilitybothbeforeandafterthestudyindexdate,definedasthesameindexdateastherespectivematchedgoutpatient.Moreover,wealso identified a subgroupof tophaceousgout
patientswithintheselectedsampleofgoutpatients.GoutpatientswithtophiweredefinedasthosewhohadanICD-9-CMcodeof274.8x (274.81=gouty tophi of the ear; 274.82=gouty tophi ofother sites except ear; 274.89=goutwithother specifiedmani-festations)duringthe12-monthperiodfollowingtheindexdate.The “other specifiedmanifestations” codewas included in ourtophidefinitionbecauseofuncertaintyabouttheaccuracyofthe5thdigitofthediagnosticcodesfortophiinourdatabase.
Study Sample for Utilization and Cost Analysis of Gout by Serum UA LevelThesubanalysisofcostby serumUA level focusedonpatientswhohadatleast1serumUAmeasureinadditiontothecriteriaabove.Theindexdateforapatientinthisstudysample(serumUAindexdate)wasdefinedastheearliestserumUAlabtestdatesinceJanuary1,2000.TobeincludedintheserumUAanalysis,patients were required to have 1 year of continuous eligibilitybothbeforeandaftertheserumUAindexdate.UtilizationandcostsforpatientsintheserumUAsubanalysiswereexaminedinthe12-monthperiodfollowingtheserumUAindexdate.
Patient CharacteristicsDemographiccharacteristics(i.e.,age,gender,geographicregion),comorbiditiesindicatedbytheDeyo-CharlsonComorbidityIndex(CCI),22andthenumberofuniquemedications(identifiedbythefirst9digitsoftheNDCnumberinthepharmacyclaim)filledduringthe12monthsbeforethestudyindexdatewereincludedin the analysis. Patients with serum UA data were classifiedinto3groupsbasedonserumUAontheserumUAindexdate: <6mgperdL,6-8.99mgperdL,and≥9mgperdL.Thecutoffpointswere chosenbasedon the relevant literature.The6mg
Disease-Related and All-Cause Health Care Costs of Elderly Patients With Gout
www.amcp.org Vol. 14, No. 2 March 2008 JMCP Journal of Managed Care Pharmacy 167
per dLmark is the recommended optimal serumUA level.17,19 The serumUAmark of 9mg per dLwas chosen because theannual incidence of gouty arthritis is much higher beyondthis level, compared with a lower serum UA level (4.9% vs.0.1-0.5%).23
Utilization and Economic OutcomesTheoutcomesinthisstudyincludedhealthcareutilizationandhealth care costs, which were obtained from the claims data-base.Healthcareutilizationwasmeasuredbythepercentageofpatientswhohadanyuseofinpatient,outpatientandemergencyservices,andanyuseofprescriptiondrugs.Eachofthemedicalclaimswasclassified into inpatient,outpatient,emergency,andotherservicesusingtheplaceofservicefieldontheclaim.Gout-related medications (i.e., allopurinol, probenecid, colchicines,probenecid/colchicines, and sulfinpyrazone) in the pharmacyclaimswereidentifiedbyNDCnumber.Health care costswere estimated from a third-party payer’s
perspectiveusingbothmedicalandpharmacyclaimsdatadur-ing the 12-month period following the study index date forthe sample of gout patients and tophaceous gout patients and duringthe12-monthperiodfollowingtheserumUAindexdatefor the sample with serum UAmeasures. Two cost categorieswere assessed in the analysis: total all-cause health care costsandgout-relatedcosts.Bothmeasuresincludedmedicalservices andpharmacycosts.Medicalservicesconsistedofinpatient,out-patient,andemergencyroom(ER)visits,andservicesprovidedinotherlocations.Totalall-causehealthcarecostsincludedcostsfrommedicalservicesandpharmacyclaimsforanyreason.Gout-relatedcostsincludedcostsfrommedicalservicesclaimswithanassociatedprimaryorsecondarydiagnosisofgoutandpharmacyclaimsforgout-relatedmedications(i.e.,allopurinol,probenecid,colchicines,orsulfinpyrazone).Allcostswereinflationadjustedto2005dollarsusingthemedicalcomponentoftheConsumerPriceIndex.
Statistical AnalysisHealth care utilization differences between gout patients andtheirmatchedgout-freemembersweremeasuredasrelativerisks.Becausethematchedsampledesignrequiredstatisticaltestsforpaired samples and the skewed utilization data required non-parametric tests,Wilcoxonsignedranksumtestswereusedtodetermine statistical significance for continuous variables, andMcNemar’stestswereusedforcategoricalvariables.Costdifferencesbetweengoutpatientsandgout-freemembers
werecalculatedusingbothdescriptiveanalysisandmultivariateregression. The descriptive analysis estimated the unadjusteddifferencesinthemeanper-member12-monthhealthcarecostsbetween gout patients and gout-free members, with statisticalsignificance determined using theWilcoxon signed rank sumtest.Theregressionwasbasedona2-stepmethodadjustingforselected baseline factors, including age at index year, gender,
indexyear,region,CCI,andthenumberofuniquemedicationsfilledduringthe1-yearperiodbeforethestudyindexdate.Thefirst step in theregressionanalysisconsistedofa2-partmodelestimatedusingthesampleofgout-freemembers.Thefirstpartof the 2-partmodelwas a logistic regressionmodel predictingwhetheranycostswereincurred,andthesecondpartwasagen-eralizedlinearmodel(GLM)withloglinkfunctionandgammadistributiontodeterminethecostamount.These2partsgener-ated the predictivemodels for total all-cause health care costsamongthegout-freecomparisonsample.Inthesecondstep,thecoefficientsfromthepredictivemodelwereusedtoestimatethecostofeachgoutpatientasifthepatienthadbeengout-free.Thedifferencebetweentheobservedcostsandtheseprojectedcostswastheestimatedadjustedcostdifferencebetweengoutpatientsandgout-freemembers.Bootstrapresamplingmethodswereusedtoestimatethe95%confidenceintervalsofthehealthcarecostdifferences.Asimilarapproachwasappliedtoestimatethetotalall-causehealthcarecostdifferencebetweengoutpatientswithandwithoutpossibletophi.ToexaminetheassociationbetweenserumUAandutilization
and costs of gout patients,we first estimatedhealth care utili-
Disease-Related and All-Cause Health Care Costs of Elderly Patients With Gout
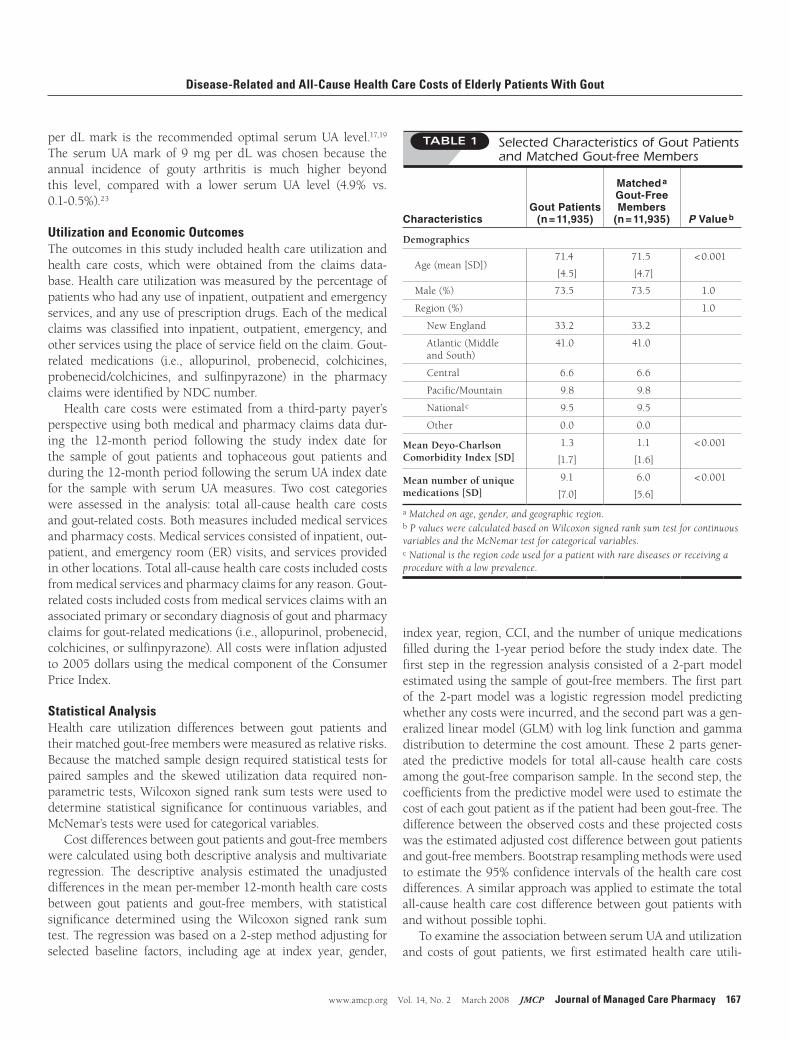
TABLE 1 Selected Characteristics of Gout Patients and Matched Gout-free Members
CharacteristicsGout Patients
(n = 11,935)
Matched a Gout-Free Members
(n = 11,935) P Value b
Demographics
Age(mean[SD])71.4
[4.5]
71.5
[4.7]
<0.001
Male(%) 73.5 73.5 1.0
Region(%) 1.0
NewEngland 33.2 33.2
Atlantic(Middle andSouth)
41.0 41.0
Central 6.6 6.6
Pacific/Mountain 9.8 9.8
National c 9.5 9.5
Other 0.0 0.0
Mean Deyo-Charlson Comorbidity Index [SD]
1.3
[1.7]
1.1
[1.6]
<0.001
Mean number of unique medications [SD]
9.1
[7.0]
6.0
[5.6]
<0.001
a Matched on age, gender, and geographic region.b P values were calculated based on Wilcoxon signed rank sum test for continuous variables and the McNemar test for categorical variables.c National is the region code used for a patient with rare diseases or receiving a procedure with a low prevalence.

168 Journal of Managed Care Pharmacy JMCP March 2008 Vol. 14, No. 2 www.amcp.org
zation and costs forpatients in each serumUAcategoryusingdescriptive statistics. Differences across serum UA categories were assessed for statistical significance using the Pearson chi-square test and the Kruskal-Wallis test, a non-parametricalternative to analysis of variance. Multivariate logistic regres-sions were then performed to assess the relationship betweenserum UA levels and risk of all-cause inpatient and ER use,controllingforotherpatientcharacteristicsincludingageatindexyear,gender,indexyear,region,CCI,andthenumberofuniquemedicationsfilledduringthe1-yearperiodbeforetheindexdate.The2-stepregressionmethoddescribedpreviouslywasusedtoassesstheassociationbetweenserumUAlevelsandhealthcarecosts.Predictive accuracy of the logistic regression models was
assessedusingthec-statistic.Goodness-of-fitfortheGLManaly-seswasassessedusingdeviance.Anapriori2-tailedα levelof0.05wasusedforallstatisticaltests.AllanalyseswereperformedusingSASsoftware,version9.1(SASInstitute,Cary,NC).
■■ ResultsSample CharacteristicsA total of 11,935 pairs ofmatched gout patients and gout-freecomparisonmemberswere included in the analysis (Figure1). The average age of gout patients was 71.4 years (standard deviation [SD]=4.5, Table 1). The sample was predominantlymale (73.5%), reflecting the fact that goutprevalence is higheramong men than women. The mean CCI score for the goutpatientgroupwas1.3(SD=1.7),whichwassignificantlyhigherthanthecomparisongroup’sscore(mean=1.1,SD=1.6,P<0.001,Table 1). The mean number of medications filled during the12-month period before the index date was 9.1 (SD=7.0) in the gout group and 6.0 (SD=5.6) in the gout-free group(P<0.001).Asubgroupof2,237goutpatients(18.7%ofthegoutsample)
withdataonlabvalueswasincludedintheserumUAanalysis.Theageandgenderdistributionsforthissub-sampleweresimilarto the distributions for the sample overall (Table 2). However,
Disease-Related and All-Cause Health Care Costs of Elderly Patients With Gout
TABLE 2 Selected Characteristics of Gout Patients With a Serum UA Value, by Serum UA Categories
Serum UA Level P Value a
[A]low
[B]moderate-
high
[C]very high
[A] vs [B] [A] vs [C] [B] vs [C]
Characteristics
< 6 mg per dL
(n = 633)
6-8.99 mg per dL
(n = 1,173)
≥ 9 mg per dL
(n = 431)
Total(n = 2,237)
Demographics
Meanage[SD] 72.3[4.5]
72.4[4.4]
72.7[4.2]
72.4[4.4]
0.925 0.276 0.288
%male 71.4 75.4 75.9 74.4 0.062 0.861 0.106
Region(%) 0.349 0.713 0.126
NewEngland 0.2 0.3 0.5 0.3
Atlantic(MiddleandSouth) 95.1 93.4 91.2 93.5
Central 0.0 0.0 0.0 0.0
Pacific/Mountain 0.2 0.1 0.2 0.1
Nationalb 4.6 6.1 7.9 6.0
Other 0.0 0.2 0.2 0.1
Prior Comorbidities (%)
Hypertension 66.8 71.2 78.0 71.3 0.055 <0.001 0.007
Renalimpairment 11.1 12.7 26.0 14.8 0.307 <0.001 <0.001
Deyo-Charlson Comorbidity Index— mean [SD]
1.0 [1.5]
1.0[1.6]
1.4[1.9]
1.1[1.6]
0.449 <0.001 0.002
Mean number of unique medications [SD]
8.5 [6.6]
7.5[6.1]
8.0[7.1]
7.9[6.5]
0.002 0.604 0.059
a P values were calculated based on the Wilcoxon signed rank sum test for continuous variables and the Pearson chi-square test for categorical variables.b National is the region code used for a patient with rare diseases or receiving a procedure with a low prevalence.UA = uric acid

www.amcp.org Vol. 14, No. 2 March 2008 JMCP Journal of Managed Care Pharmacy 169
Disease-Related and All-Cause Health Care Costs of Elderly Patients With Gout
TABLE 3 Total All-Cause Health Care Utilization and Gout-Related Utilization During the 12-Month Period Following the Index Date
Gout Patients(n = 11,935)
Matched a Gout-Free Members
(n = 11,935) Risk Ratio b
Total all-cause health care utilization
a Patients were matched by age, gender, and geographic region.b Risk ratios are unadjusted for comorbidities.c Medical service classifications were based on the place of service on the claim. Prescription drugs were indicated by the presence of a National Drug Code num-ber on the claim.d ”Gout-related” denotes medical claims with an ICD-9-CM diagnosis of gout (274.xx) in the primary or secondary position and prescription drug claims for gout-related medication (allopurinol, probenecid, colchicines, probenecid/colchicines, and sulfinpyrazone).e The minimum and maximum values for inpatient costs were $0 to $423,568 among gout patients and $0 to $339,190 among matched gout-free members; emergency room costs ranged from $0 to $79,002 among gout patients and $0 to $16,689 among matched gout-free members; outpatient costs ranged from $0 to $283,686 among gout patients and $0 to $552,940 among matched gout-free members; other costs ranged from $0 to $115,880 among gout patients and $0 to $227,406 among matched gout-free members; prescription drug costs ranged from $0 to $67,345 among gout patients and $0 to $112,403 among matched gout-free members; and total direct health care costs ranged from $4 to $470,207 among gout patients and $0 to $915,091 among matched gout-free members.f Numbers sum to $877 due to rounding.* P < 0.001 using McNemar test.ICD-9-CM = International Classification of Diseases, Ninth Revision, Clinical Modification; UA = uric acid.
Percentage with at least 1 visit (%)
Medical services c
Inpatient 27.2 17.1 1.6*
Emergencyroom(ER) 29.0 19.3 1.5*
Outpatient 99.4 93.8 1.1*
Prescription drugs 92.5 84.4 1.1*
Gout-related health care utilization d
Percentage with at least 1 visit (%)
Medical services
Inpatient 7.4 —
ER 4.8 —
Outpatient 68.8 —
Prescription drugs 68.9 —
Mean total all-cause health care cost ($), [SD] e
Medical services
Inpatient 5,674 [18,557] 3,148 [13,342]
ER 235 [11,336] 140 [508]
Outpatient 5,224 [11,336] 3,634 [9,322]
Other 1,542 [5,742] 870 [4,089]
Prescription drugs 2,059 [2,652] 1,427 [2,317]
Total direct health care costs 14,734 [27,401] 9,219 [20,186]
Median total all-cause health care cost ($)
Medical Services
Inpatient 0 0
ER 0 0
Outpatient 2,556 1,662
Other 114 24
Prescription drugs 1,419 849
Total direct health care costs 5,921 3,665
Mean gout-related health care cost ($), [SD] e
Medical services
Inpatient 505 [3,062] —
ER 21 [146] —
Outpatient 207 [557] —
Other 82 [1,016] —
Prescription drugs 62 [89] —
Total direct health care costs 876 [3,373] —
Median gout-related health care cost ($)
Medical services
Inpatient 0 —
ER 0 —
Outpatient 95 —
Other 0 —
Prescription drugs 32 —
Total direct health care costs 185 —

170 Journal of Managed Care Pharmacy JMCP March 2008 Vol. 14, No. 2 www.amcp.org
93.5%ofgoutpatientswithaserumUAvaluelivedintheAtlanticregioncomparedwith41.0%intheoverallsamplebecausemostplanswith labdataavailableare located in theAtlanticregion.AmongthosewithanavailableserumUAtest,633(28.3%)hadaserumUAvalue<6mgperdL,1,173(52.4%)hadaserumUAbetween6and8.99mgperdL,andtheremaining431(19.3%)patientshadaserumUAvalueof≥9mgperdL(Table2).Mostof thepatients’characteristicswerecomparableacrossthe3serumUA categoriesalthough thegroupwith thehighest serumUA level
(≥9mgperdL)hadasignificantlyhigherprevalenceofhyper-tensionandrenalimpairmentcomparedwiththeother2groups.The goutpatients in this group alsohad a significantlyhigherCCIscorethantheother2groups(mean=1.4vs.1.0,P=0.002,Table2).
Total All-Cause and Gout-Related Utilization and CostNearly all elderly adult gout patients in our sample (99.4%)had at least 1 outpatient visit during the 12months followingthestudyindexdate;29.0%had≥1claimwithanERplaceofservice,and27.2%had≥1claimwithaninpatientplaceofser-vice,and92.5%hadat least1pharmacyclaim(Table3).Goutpatients had consistently higher utilization in each category thangout-freemembers.Goutpatientswere59.1%more likely to have≥1 claimwith an inpatient place of service, andwere 50.3%more likely to have ≥1 claimwith an ER place of ser-vice, comparedwith gout-freemembers (bothP<0.001). Goutpatients also had a higher utilization of outpatient services andprescriptiondrugscomparedwithgout-freemembers(bothrisk ratios [RRs]=1.1; both P<0.001) although the differencesweresmallerthanthoseforinpatientandemergencycare(RR=1.6and1.5,respectively;P<0.001).Thepercentagesofpatientswithgout-relatedclaimswithinpatientplaceofserviceandERplaceofservicewere7.4%and4.8%,respectively.Gout-relatedoutpatientcareandprescriptiondruguseoccurredin68.8%and68.9%ofgoutpatients,respectively(Table3).In the 12 months following the index date, the mean
unadjusted gout-related health care cost per patient was $876 (SD$3,373),5.9%ofthetotalall-causehealthcarecostof$14,734(SD$27,401)forgoutpatients.Unadjustedmeantotal12-monthall-cause health care cost for gout-free members was $9,219 (SD$20,186,Table3).Theunadjustedall-causehealthcarecostdifference between gout patients and gout-free members was$5,515. Of the $876 total 12-month gout-related costs amonggoutpatients,57.6%wasattributedtoinpatientservices,23.6%tooutpatientservices,2.4%toemergencyservices,9.4%tootherservices,and7.1%toprescriptiondrugcosts.Afterstatisticaladjustmentforageatindexyear,gender,index
year, region,CCI, andnumber of uniquemedications at base-line,thedifferenceintotal12-monthall-causehealthcarecostsbetweengoutpatientsandmemberswithoutgoutwas$3,038(SE$371,P<0.001,Figure2).Amongtheolderadultgoutpatientsincludedinoursample,
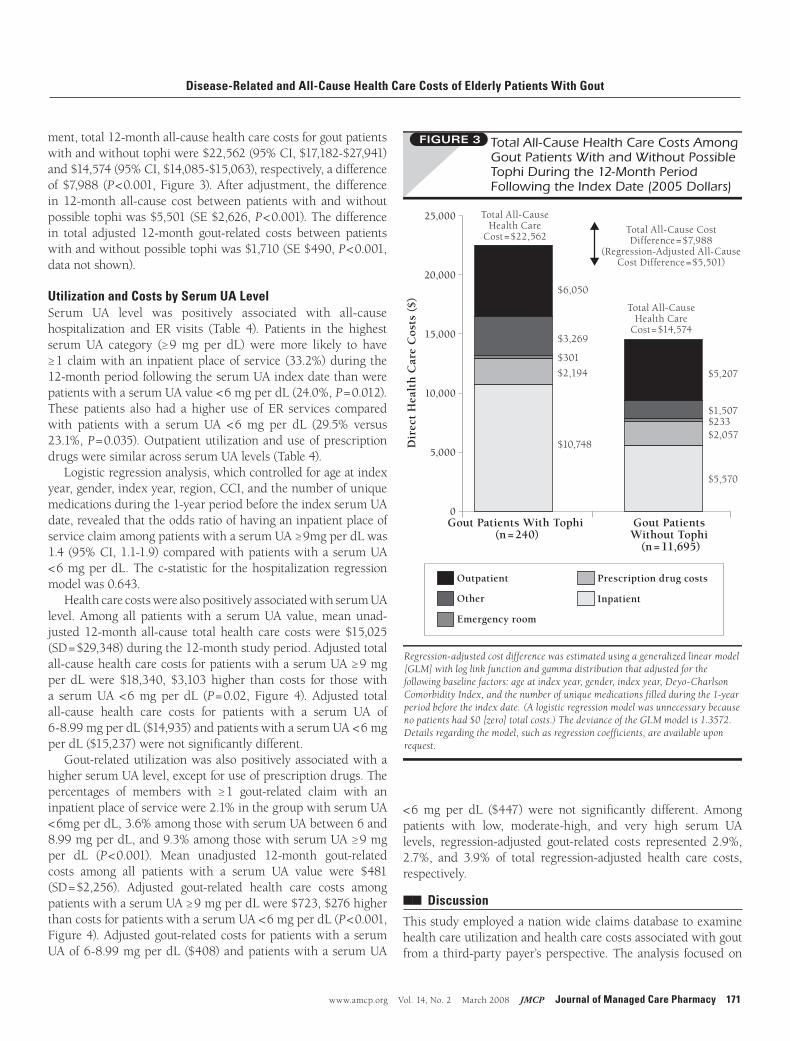
240 (2.0%) had a diagnosis suggesting possible tophi within the12-monthstudyperiod.Ofthese240patients,6.4%hadanICD-9-CMcodeof274.8(anon-specificcodeforgoutwithotherspecified manifestations), 3.9% had an ICD-9-CM of 274.81(goutytophiofear),43.8%hadanICD-9-CMof274.82(goutytophiofothersitesexceptear),and45.8%hadanICD-9-CMof274.89(goutwithotherspecifiedmanifestations).Comparedtothosewithout tophi,goutpatientswithpossible tophi incurredhighercostsineveryutilizationcategory.Priortostatisticaladjust-
Disease-Related and All-Cause Health Care Costs of Elderly Patients With Gout
www.amcp.org Vol. 14, No. 2 March 2008 JMCP Journal of Managed Care Pharmacy 171
ment,total12-monthall-causehealthcarecostsforgoutpatientswithandwithouttophiwere$22,562(95%CI,$17,182-$27,941)and$14,574(95%CI,$14,085-$15,063),respectively,adifferenceof$7,988 (P<0.001,Figure3).After adjustment, thedifferencein 12-month all-cause cost betweenpatientswith andwithoutpossibletophiwas$5,501(SE$2,626,P<0.001).Thedifferencein total adjusted 12-month gout-related costs between patientswithandwithoutpossibletophiwas$1,710(SE$490,P<0.001,datanotshown).
Utilization and Costs by Serum UA LevelSerum UA level was positively associated with all-cause hospitalization and ER visits (Table 4). Patients in the highestserumUA category (≥9mg per dL) weremore likely to have≥1claimwithan inpatientplaceofservice (33.2%)during the12-monthperiodfollowingtheserumUAindexdatethanwerepatientswithaserumUAvalue<6mgperdL(24.0%,P=0.012).These patients also had a higher use of ER services comparedwith patients with a serum UA <6 mg per dL (29.5% versus23.1%,P=0.035).OutpatientutilizationanduseofprescriptiondrugsweresimilaracrossserumUAlevels(Table4).Logisticregressionanalysis,whichcontrolledforageatindex
year,gender,indexyear,region,CCI,andthenumberofuniquemedicationsduringthe1-yearperiodbeforetheindexserumUAdate,revealedthattheoddsratioofhavinganinpatientplaceofserviceclaimamongpatientswithaserumUA≥9mgperdLwas1.4(95%CI,1.1-1.9)comparedwithpatientswithaserumUA<6mgperdL.Thec-statistic for thehospitalizationregressionmodelwas0.643.HealthcarecostswerealsopositivelyassociatedwithserumUA
level.Among all patientswith a serumUAvalue,meanunad-justed12-month all-cause totalhealth care costswere$15,025(SD=$29,348)duringthe12-monthstudyperiod.Adjustedtotalall-causehealthcarecostsforpatientswithaserumUA≥9mgper dLwere $18,340, $3,103 higher than costs for thosewitha serumUA <6mg per dL (P=0.02, Figure 4). Adjusted total all-cause health care costs for patients with a serum UA of 6-8.99mgperdL($14,935)andpatientswithaserumUA<6mgperdL($15,237)werenotsignificantlydifferent.Gout-relatedutilizationwasalsopositivelyassociatedwitha
higherserumUAlevel,exceptforuseofprescriptiondrugs.Thepercentages of members with ≥1 gout-related claim with aninpatientplaceofservicewere2.1%inthegroupwithserumUA<6mgperdL,3.6%amongthosewithserumUAbetween6and 8.99mgperdL,and9.3%amongthosewithserumUA≥9mg per dL (P <0.001). Mean unadjusted 12-month gout-relatedcosts among all patients with a serum UA value were $481(SD=$2,256). Adjusted gout-related health care costs amongpatientswithaserumUA≥9mgperdLwere$723,$276higherthancostsforpatientswithaserumUA<6mgperdL(P<0.001,Figure4).Adjustedgout-relatedcostsforpatientswithaserumUAof6-8.99mgperdL($408)andpatientswithaserumUA
<6mg per dL ($447) were not significantly different. Amongpatients with low, moderate-high, and very high serum UAlevels, regression-adjusted gout-related costs represented 2.9%,2.7%, and 3.9% of total regression-adjusted health care costs,respectively.
■■ Discussion
Thisstudyemployedanationwideclaimsdatabasetoexaminehealthcareutilizationandhealthcarecostsassociatedwithgoutfroma third-partypayer’sperspective.Theanalysis focusedon
Disease-Related and All-Cause Health Care Costs of Elderly Patients With Gout

172 Journal of Managed Care Pharmacy JMCP March 2008 Vol. 14, No. 2 www.amcp.org
Serum UA Level< 6 mg per dL
(n = 633)6-8.99 mg per dL
(n = 1,173)≥ 9 mg per dL
(n = 431) P Value a
Total all-cause health care utilization
a P values compare differences across the 3 categories using Pearson chi-square tests and Kruskal-Wallis tests.b Medical service classifications were based on the place of service on the claim. Prescription drugs were indicated by the presence of a National Drug Code number on the claim.c “Gout-related” denotes medical claims with an ICD-9-CM diagnosis of gout (274.xx) in the primary or secondary position.d “Gout-related” medications include allopurinol, probenecid, colchicines, probenecid/colchicines, and sulfinpyrazone.ICD-9-CM = International Classification of Diseases, Ninth Revision, Clinical Modification; UA = uric acid.
Percentage with at least 1 visit (%)
Medical services b
Inpatient 24.0 23.2 33.2 0.012
Emergencyroom(ER) 23.1 24.7 29.5 0.035
Outpatient 99.8 99.7 99.8 0.673
Prescription drugs 84.8 85.3 82.1 0.391
Gout-related health care utilization c
Percentage with at least 1 visit (%)
Medical services
Inpatient 2.1 3.6 9.3 <0.001
ER 0.6 2.0 2.8 0.006
Outpatient 41.1 51.6 61.9 <0.001
Prescription drugs d 56.1 45.4 55.0 0.083
Mean total all-cause health care cost ($), [SD]
Medical services
Inpatient 6,516 [22,627] 5,758 [20,757] 10,059 [24,378] <0.001
ER 150 [425] 193 [543] 233 [647] 0.055
Outpatient 5,321 [9,006] 5,361 [10,649] 5,636 [10,792] 0.228
Other 1,096 [5,079] 855 [4,156] 1,431 [4,700] 0.005
Prescription drugs 1,859 [3,150] 1,471 [2,235] 1,561 [2,225] 0.009
Total direct health care costs 14,942 [29,476] 13,638 [27,728] 18,920 [32,950] 0.009
Median total all-cause health care cost ($)
Medical services
Inpatient 0 0 0
ER 0 0 0
Outpatient 3,046 2,863 2,706
Other 0 0 0
Prescription drugs 1,167 856 875
Total direct health care costs 5,968 5,062 5,920
Mean gout-related health care cost ($), [SD]
Medical services
Inpatient 241 [2,682] 208 [1,777] 400 [2,070] <0.001
ER 3 [41] 9 [81] 12 [81] 0.022
Outpatient 125 [581] 150 [494] 233 [540] <0.001
Other 29 [422] 7 [81] 46 [700] 0.046
Prescription drugs 62 [78] 29 [63] 33 [52] <0.001
Total direct health care costs 460 [2,795] 403 [1,871] 723 [2,319] <0.001
Median gout-related health care cost ($)
Medical services
Inpatient 0 0 0
ER 0 0 0
Outpatient 0 47 69
Other 0 0 0
Prescription drugs 24 0 9
Total direct health care costs 114 80 137
TABLE 4 Health Care Utilization Among Gout Patients With a Serum UA Value During the 12-Month Period Following the Index Date (n = 2,237)
Disease-Related and All-Cause Health Care Costs of Elderly Patients With Gout

www.amcp.org Vol. 14, No. 2 March 2008 JMCP Journal of Managed Care Pharmacy 173
the older adult population, in which a higher prevalence of the disease is observed. In addition, the study also compared health costs between gout patients with and without tophi and across different serum UA categories. This study adds to a limited litera-ture on health care utilization and costs among older adult gout patients.
The findings in this study demonstrated that older adult gout patients incur substantially higher total all-cause health care costs than older adult gout-free members, $5,515 higher in a 12-month period. This number represents the total health care cost associated with gout: how much more a third-party payer has to pay for an average gout patient compared with an average gout-free member, irrespective of the associated comorbidities.24 After statistical adjustments for the comorbidities measured in our study and the number of medications, the 12-month all-cause cost difference between gout patients and gout-free members was $3,038.
The mean gout-related costs in this sample were estimated to be $876 for a 12-month period, about 5.9% of total health care costs. Of the $876, 57.6% was attributed to inpatient services, 23.6% to outpatient services, 2.4% to emergency services, 9.4% to other services, and 7.1% to prescription drug costs.
Gout patients with possible tophi incurred significantly higher regression-adjusted total all-cause health care costs and gout-related costs than those without tophi, with differences of $5,501 and $1,710 respectively. The occurrence of tophi represents a more advanced stage of gout, which generally requires more med-ical resources than the initial self-limiting stage. For example, renal complications, such as chronic urate nephropathy, occur more often in tophaceous gout.2 Previous research also found that tophi are associated with more frequent gout flares.17 Therefore, it is not surprising that gout patients with tophi have considerably higher total health care costs and gout-related costs.
Finally, the study documented a positive relationship between serum UA and health care utilization and costs among gout patients. The prevalence of use of services in an inpatient place of service was significantly higher among patients with serum UA ≥ 9 mg per dL than among patients with low serum UA (< 6 mg per dL). Moreover, serum UA ≥ 9 mg per dL was associated with higher total all-cause health care costs and gout-related health care costs. Having serum UA ≥ 9 mg per dL was associated with an additional $3,103 in 12-month all-cause health care costs and $276 in 12-month gout-related costs, compared with a serum UA < 6 mg per dL.
Although gout is a prevalent disease associated with substan-tial utilization of health care resources, the economic burden of gout has not been well documented. Kim et al.2 estimated that the annual U.S. health care cost associated with new acute gout cases is approximately $27 million. This result is likely an underesti-mation of true gout-related costs because female patients were not included in Kim et al.’s model. Brook et al. found that gout was associated with approximately $1,800 in additional medical
and prescription drug costs per person per year in an employed population.12 The cost differences between gout patients and non-gout members in our study were much higher than in previ-ous work. This is probably because our study focused on older adults. Older gout patients constitute a difficult population in gout treatment because of the high prevalence of complications and comorbidities in this group. In addition, impaired renal function, increased drug toxicity, and multiple drug interactions
Disease-Related and All-Cause Health Care Costs of Elderly Patients With Gout

174 Journal of Managed Care Pharmacy JMCP March 2008 Vol. 14, No. 2 www.amcp.org
pose further barriers to effective control of hyperuricemia inthisgroup.18,19Thesefactssuggestthatolderadultgoutpatientsmay consume more health care resources than their younger counterparts.ThegoalofmaintainingtheoptimalserumUA(≤6mgperdL)
isextremelychallengingintheolderadultpopulation.Behavioralchangesalone,suchasrestrictingdiet,reducingalcoholconsump-tion, and switching incorrect medications, generally produceunsatisfactory results.16 Insuchcases,urate-loweringdrugsareusuallyrecommendedbyphysicians.Currently,thereare2types of urate-lowering drugs: uricosuric drugs (e.g., probenecid,sulfinpyrazone) and hypouricemic drugs (e.g., allopurinol).WhileeffectiveinreducingserumUAinmostpatients,theuseof uricosuric drugs is limited in some older adults because ofdecline in renal function; according to gout treatment guide-linespublishedin1999,uricosuricdrugsshouldnotbegiventopatientswithaurineoutputof<1mLperminute,acreatinineclearance of <50 mL per minute (0.84 mL per second) or a historyofrenalcalculi.25
Allopurinolisthemostcommonlyprescribedurate-loweringdrugandisthedrugofchoiceforthispurposeinpatientswithrenal impairment.16 Allopurinol is generallywell tolerated, butapproximately 2%of patients develop a pruritic, erythematousrashthatrequiresdiscontinuationoftherapy,and0.4%ofpatientsexperience allopurionol hypersensitivity syndrome.10 However,bothoftheseadverseeffectsmaybeminimizedbykeepingtheallopurinoldoselowinagedpatientsorthosewithrenalimpair-ment,withastartingdoseof50mg-100mgonalternatedays,toamaximumdailydoseofabout100mg-300mg,baseduponthepatient’screatinineclearanceandserumuratelevel.10,16
Additional treatment options to lower serum urate wouldbewelcomed,especially thosewith improvedeffectivenessandfewersideeffects.Futurestudiesonmedicationuseanditsasso-ciationwithotherhealthcareutilizationmayshedmorelightontheeconomicaspectsofgouttreatment.
LimitationsFirst, the adjusteddifference in total all-causehealth care costsbetween goutpatients andgout-freemembers is subject tobiasbecauseofpotentialconfounders.Thegoutpatientsandgout-freemembersinoursamplehaddifferentcomorbiditiesbasedontheCCI.AlthoughwecontrolledfortheCCIinourmodel,theremayberesidualconfounding,suchasdiseaseseverity,thataffectsourestimationoftheexcesscostofgout.However,theunadjusteddif-ference,whichrepresentstheadditionalcostassociatedwithgout,isstillvalidforthepurposeofestimatinghowmuchmoreagoutpatientcostsrelativetoagout-freemember,althoughthemajorityof the cost difference could be due to comorbidities.24 Second,becausethestudywasobservational, itwasunabletoidentifyacausalrelationshipbetweengoutandexcessall-causehealthcarecosts.Third,thoughtheanalysiswasconductedtoincludeallowedamounts for costs, which includes not only third-party payer
payment but also patient cost sharing, the indirect costs thatmight be incurred by patients and their caregivers were notincluded.Fourth, as a general limitation with the use of a claims
database, costsmaynot be accurately classified as gout-relatedor tophi-relatedbecause thecalculationwasbasedonlyon thelisteddiagnoses in theclaims.Moreover,whenestimatingpre-scriptiondrugcosts,we includedonlyallopurinol,probenecid,colchicines,probenecid/colchicines,andsulfinpyrazoneasgout-related drugs. We excluded non-steroidal inflammatory drugs(NSAIDs), a commonmedicationused in acute gouty arthritis,because this class of drug is non-specific and is commonly prescribed for other non-gout related conditions. Additionally,most NSAIDs are over-the-counter drugs, the use of which is not possible to capture using claimsdata. Fifth,we based ourmedical service classifications only on place of service codesinstead ofmore specific revenue and procedure codes. To theextent that ER room and outpatient services were codedwithinpatient place of service, our inpatient cost estimates wereinflated. This may be an issue for the serum UA analysis, inparticular,ifthoseinthehighestcategoryreceivecertaintypesofoutpatienttreatment(e.g.,dialysis)thataremorelikelythanotherserumUAcategoriestobecodedwithinpatientplaceofservice.Thatsaid,thispotentialproblemaboutplaceofservicewouldnotaffectcomparisonsoftotalcostacrossthestudygroups.Sixth, the serum UA analysis measured costs for the
12monthsfollowingtheearliestserumUAtestinthedatabase.Becausewedidnotmeasurethedegreetowhichthe12-monthserumUAanalysistimeperiodcoincidedwiththe12-monthanal-ysisperiodforgout-relatedcosts,itispossiblethatthese2analyses measuredcostsincurredindifferenttimeperiods.A seventh limitation arises from theway that gout patients
with tophi were defined. The tophi-related classification wasbasedonthe4-digitICD-9-CMcodeof274.8x.The5-digitclas-sificationcodeof274.89,however,is“goutwithotherspecifiedmanifestations,”whichmayormaynotrepresent tophi.Of the240patients thatwe identified ashaving tophi, 45.8%had anICD-9-CMcode274.89.Wechosetoidentifytophiusing4-digitratherthan5-digitcodesbecauseofconcernsabouttheaccuracyof5-digitcodesinourdatabase.Somegouttophipatientsinoursamplemay,therefore,bemisclassifiedasaresultofrelyingonICD-9-CMcodesatthe4-digitlevel.Otherlimitationsarespecifictotheanalysisofasub-sample
ofgoutpatientswithaserumUAvalue.MostgoutpatientswithavalidserumUAvaluefromelectroniclaboratorydatawerecon-centratedinthemid-andsouth-Atlanticregion,whichresultedinastudysamplenotrepresentativeofallgeographiclocations.Inaddition,comparedwiththeoverallsampleofolderadultgoutpatientsinthisstudy(includingpatientsbothwithandwithouta serumUA lab test),goutpatientswitha serumUA labvalueseemtohavefewercomorbiditiesindicatedbytheCCI(meanof 1.1vs.1.3).However, thedifferencesweresmall,sotheresults
Disease-Related and All-Cause Health Care Costs of Elderly Patients With Gout

www.amcp.org Vol. 14, No. 2 March 2008 JMCP Journal of Managed Care Pharmacy 175
maynot significantly deviate from the findings thatwewouldhaveobtainedifallgoutpatientswereincluded.
■■ Conclusions
Gout-related costs represent approximately 6% of total healthcarecostsinelderlypatientswithgout.Goutisassociatedwithincreasedhealthcareutilizationandcostsamongelderlyadults.Patientswithpossibletophi,inparticular,hadincreasedhealthcarecosts.GoutpatientswithaserumUA≥9mgperdLincurhighercoststhanthosewithaserumUA<6mgperdL.
4.LeeSJ,TerkeltaubRA,KavanaughA.Recentdevelopmentsindietandgout.Curr Opin Rheumatol.2006;18:193-98.
5.ArromdeeE,MichetCJ,CrowsonCS,O’FallonWM,GabrielSE.Epidemiologyofgout:istheincidencerising?J Rheumatol.2002;29:2403-06.
6.HarrisCM,LloydDC,LewisJ.Theprevalenceandprophylaxisofgout inEngland.J Clin Epidemiol.1995;48:1153-58.
7.KlempP,StansfieldSA,CastleB,RobertsonMC.GoutisontheincreaseinNewZealand.Ann Rheum Dis.1997;56:22-26.
8.MikulsTR,SaagKG.Newinsightsintogoutepidemiology.Curr Opin Rheumatol.2006;18:199-203.
9.WortmannRL.Goutandhyperuricemia.Curr Opin Rheumatol.2002; 14:281-86.
10.FamAG.Goutintheelderly.Clinicalpresentationandtreatment. Drugs Aging.1998;13:229-43.
11.WallaceKL,RiedelAA,Joseph-RidgeN,WortmannR.Increasing prevalenceofgoutandhyperuricemiaover10yearsamongolderadultsin amanagedcarepopulation.J Rheumatol.2004;31:1582-87.
12.BrookRA,KleinmanNL,PatelPA,etal.Theeconomicburdenofgoutonanemployedpopulation.Curr Med Res Opin.2006;22:1381-89.
13.HarrisMD,SiegelLB,AllowayJA.Goutandhyperuricemia.Am Fam Physician.1999;59:925-34.
14.FamAG,ReisMD,SzalaiJP.Acutegoutysynovitisassociatedwith “uratemilk.”J Rheumatol.1997;24:2389-93.
15.GonzalezEB,MillerSB,AgudeloCA.Optimalmanagementofgoutinolderpatients.Drugs Aging.1994;4:128-34.
16.vanDornumS,RyanPF.Clinicalmanifestationsofgoutandtheir management.Med J Aust.2000;172:493-97.
17.Li-YuJ,ClayburneG,SieckM,etal.Treatmentofchronicgout.Canwedeterminewhenuratestoresaredepletedenoughtopreventattacksofgout?J Rheumatol.2001;28:577-80.
18.SarawateCA,PatelPA,SchumacherHR,YangW,BrewerKK,BakstAW.Serumuratelevelsandgoutflares:analysisfrommanagedcaredata.J Clin Rheumatol.2006;12:61-65.
19.ShojiA,YamanakaH,KamataniN.Aretrospectivestudyofthe relationshipbetweenserumuratelevelandrecurrentattacksofgouty arthritis:evidenceforreductionofrecurrentgoutyarthritiswith antihyperuricemictherapy.Arthritis Rheum.2004;51:321-25.
20.ZhangW,DohertyM,BardinT,etal.EULAREvidencebased recommendationsforgout—partIImanagement:reportofataskforce oftheEULARStandingCommitteeforInternationalClinicalStudiesIncludingTherapeutics(ESCISIT).Ann Rheum Dis.2006;65:1312-24.
21. International Classification of Diseases, Ninth Revision, Clinical Modification. 4thed.Washington,DC:TheU.S.DepartmentofHealthandHumanServices;1991.
22.DeyoRA,CherkinDC,CiolMA.AdaptingaclinicalcomorbidityindexforusewithICD-9-CMadministrativedatabases.J Clin Epidemiol.1992; 45:613-19.
23.TerkeltaubRA.Clinicalpractice.Gout.N Engl J Med.2003;349:1647-55.
24.BirnbaumHG,LeongSA,OsterEF,KinchenK,SunP.Costofstress urinaryincontinence:aclaimsdataanalysis.Pharmacoeconomics.2004; 22:95-105.
25.PittmanJR,BrossMH.Diagnosisandmanagementofgout.Am Fam Physician.1999;59(7):1799-806.Availableat:www.aafp.org/afp/990401ap/ 1799.html.
Disease-Related and All-Cause Health Care Costs of Elderly Patients With Gout
DISCLOSURES
Funding for this research was provided by TAP Pharmaceutical Products.Pankaj Patel is a former employee, and Reema R.Mody is an employee ofTAPPharmaceuticalProducts.EricWu,AndrewP.Yu,andKevinE.Cahillare employees of Analysis Group, which received funding for this study. PreliminaryresultsofthisresearchwerepresentedasaposterattheAmericanGeriatricsSocietyMeetinginSeattle,Washington,onMay4,2007. AllauthorsexceptTangcontributedtothestudyconceptanddesign.Tangwas primarily responsible for data collection,with assistance fromYu andCahill.DatainterpretationwasperformedbyWu,Yu,Mody,andKrishnan.Writing and revisionof themanuscriptwereperformedbyWu,Patel, andCahill,withinputfromtheotherauthors.
REfEREnCES
1.KramerHM,CurhanG.Theassociationbetweengoutandnephrolithiasis: theNationalHealthandNutritionExaminationSurveyIII,1988-1994.Am J Kidney Dis.2002;40:37-42.
2.KimKY,RalphSH,HunscheE,WertheimerAI,KongSX.Aliterature reviewoftheepidemiologyandtreatmentofacutegout.Clin Ther.2003; 25:1593-617.
3.RoubenoffR,KlagMJ,MeadLA,LiangKY,SeidlerAJ,HochbergMC.Incidenceandriskfactorsforgoutinwhitemen.JAMA.1991;266:3004-07.
ERIC Q. WU, PhD, is a vice president; ANDREW P. YU, PhD, is an associate; KEVIN E. CAHILL, PhD, is an associate; and JACKSON TANG, BS, is a former senior analyst, Analysis Group, Boston, Massachusetts. PANKAJ A. PATEL, PharmD, MS, is a former employee, and REEMA R. MODY, MBA, PhD, is a senior manager, TAP Pharmaceutical Products, Lake Forest, Illinois. ESWAR KRISHNAN, MD, MPH, is an assistant professor of medicine, Division of Rheumatology, University of Pittsburgh, Pennsylvania.
AUTHOR CORRESPONDENCE: Eric Q. Wu, PhD, Vice President, Analysis Group, 111 Huntington Ave, 10th Fl., Boston, MA 02199. Tel.: 617.425.8254; Fax: 617.425.8001; E-mail: [email protected]
Authors