disease of the liver & biliary system 4th year 2017 of the liver & biliary ... anatomy ,...
TRANSCRIPT
Disease of the Liver & Biliary
System 4th year 2017
Sunday 4/3/2017
Dr Monem Alshok .

Liver Lectures include :
Anatomy , Physiology & Investigations
Acute Paranchymal liver diseases
Chronic Paranchymal liver diseases
Cirrhosis & portal hypertension
Immunological LD& Intrahepatic Cholestasis
Vascular LD
Pregnancy & liver
NASH & ALD
Liver tumors & focal liver lesion
Metabolic & inherited LD
Liver Transplantation
Drugs, Toxins & liver

Structure of Liver
Liver largest internal organ.( 1 - 1.5 Kg ) Hepatocytes form hepatic plates that are 1–2 cells
thick.Arranged into functional units called lobules.
Plates separated by sinusoids.More permeable than other capillaries.
Contains phagocytic Kupffer cells. Secretes bile into bile canaliculi, which are drained
by bile ducts.

Structure of Liver (continued)
Insert fig. 18.20

Liver Cells
The majority of cells in the liver are
hepatocytes, which constitute two-thirds of the
mass of the liver. The remaining cell types are
Kupffer cells (members of the RES ), stellate
(Ito or fat-storing) cells, endothelial cells and
blood vessels, bile ductular cells, and
supporting structures
Under L\M
Viewed by light microscopy, the liver appears to
be organized in lobules, with portal areas at the
periphery and central veins in the center of each
lobule. However, from a functional point of view, the
liver is organized into acini, with both hepatic
arterial and portal venous blood entering the acinus
from the portal areas (zone 1) and then flowing
through the sinusoids to the terminal hepatic veins
(zone 3); the intervening hepatocytes constituting
zone2
Portal areas of the liver
Consist of small veins, arteries, bile ducts, and lymphatic organized in a loose Struma of supporting matrix and small amounts of collagen. Blood flowing into the portal areas is distributed through the sinusoids, passing from zone 1 to zone 3 of the acinus and draining into the terminal hepatic veins (“central veins”).
Bile : Secreted bile flows in the opposite direction, in a counter current pattern from zone 2 to zone 1. The sinusoids are lined by unique endothelial cells that have prominent fenestrate of variable size, allowing the free flow of plasma but not cellular elements. The plasma is thus in direct contact with hepatocytes in the sub endothelial space of Disse

Hepatocytes have distinct polarity
The basolateral side of the hepatocyte
lines the space of Disse and is richly lined with
microvillus; it demonstrates endocytotic and
pinocytotic activity, with passive and
active uptake of nutrients, proteins, and other
molecules

Hepatocytes
The apical pole of the hepatocyte forms the
cannicular membranes through which
bile components are secreted. The canniculi of
hepatocytes form a fine network, which fuses
into the bile ductular elements near the portal
areas.

Kupffer
Kupffer cells usually lie within the sinusoidal
vascular space and represent the largest
group of fixed macrophages in the body

The stellate cells
The stellate cells are located in the space of Disse
but are not usually prominent unless activated, when
they produce collagen and matrix. RBC stay in the
sinusoidal space as blood flows through the lobules,
but WBC can migrate through or around endothelial
cells into the space of Disse and from there to portal
areas, where they can return to the circulation through
lymphatic
Liver
Location at R. Hypochondrium &Epigastric region
4 Lobes( L lobe & R lobe by falciform ligament ). The right and left hemiliver are further subdivided into 8 segments in accordance with subdivisions of the hepatic and portal veins
Left
Quadrate
Caudate
Right
Each lobe has lobules – Contains hepatocytes –Surround sinusoids – Feed into central vein
12

Glisson’s capsule: the peritoneal lining that
surrounds the liver.
Bare area: posterior surface of the liver not covered.
Coronary ligaments: reflections of peritoneum on the
posterior surface
Triangular ligaments: lateral extensions of the
coronary ligaments.
Falciform: from umbilicus to diaphragm, contains
obliterated umbilical vein.
Ligamentum teres, extends from falciform on
undersurface of liver
Ligaments of the Liver

Anatomy
• Eight segments, based on arterial and portal venous inflow.
• Segment 1 is the caudate lobe of the liver.
• Segments 2-4 are segments of the left lobe resected during left hepatic lobectomy.
• Segments 5-8 are segments of the right lobe resected during right hepatic lobectomy.

Segments

Falciform ligament does not divide right and left lobes of
liver, the portal fissure or Cantlies line is a plane passing
from the left side of the gallbladder fossa to the left side of
the IVC. It defines the physiologic division between left
and right lobes of liver . It does separate medial and lateral
segments of left lobe
A right trisegmentectomy includes a resection of the right
lobe plus segment 4.
A left lateral segmentectomy includes resection of segments
2 and 3 to the left of the falciform.
Resection of 80% of parenchyma is compatible with life.


Liver
• Dual blood supply
– Hepatic portal vein
• Direct input from
small intestine
– Hepatic artery/vein
• Direct links to heart
19

LIVER BLOOD FLOW
HEART
LIVER
STOMACH
AND
SMALL INTESTINE
HEPATIC
PORTAL
VEIN
HEPATIC
VEIN
IVCAORTA
HEPATIC
ARTERY
ARTERIES TO
DIGESTIVE TRACT

Portal vein: drains blood from the small and large
intestines, stomach, spleen, pancreas,and gallbladder.
The portal trunk divides in to 2 lobar veins, the right drains
the cystic vein, the left receives umbilical and paraumbilical
veins that enlarge to form the caput medusae. The
coronary vein: drains the distal esophagus, which also
enlarge in PHTN.
Common hepatic artery: arises from the celiac artery and becomes the proper hepatic artery after the GD branches. Passes medial to the bile duct and anterior to portal vein. Bifurcates into right and left hepatics in liver parenchyma.Can come off SMA (right) or Left gastric (left).Pringle maneuver.(In 1908, Pringle first described a technique to minimize blood loss
during hepatic surgery by clamping the vascular pedicle. [1] The inflow of blood to the liver is via the hepatic artery and portal vein. Surgeons must be able to isolate and control these sources of blood flow to control bleeding not only in traumatic injuries to the liver but also in elective hepatic resections.)

Hepatic Portal System
• Products of digestion that are absorbed
are delivered to the liver.
• Capillaries drain into the hepatic portal
vein, which carries blood to liver.
– ¾ blood is deoxygenated.
– Hepatic vein drains liver.

Enterohepatic Circulation
• Compounds that recirculate between liver and intestine.– Many compounds can
be absorbed through small intestine and enter hepatic portal blood.
– Variety of exogenous compounds are secreted by the liver into the bile ducts.
• Can excrete these compounds into the intestine with the bile.
Insert fig. 18.22

Major Categories of Liver Function
1 .Immunological & detoxification; Phagocytosis by Kupffer cells, Chemically alteration of biologically active molecules e.g. drugs & hormones , production of less toxic compounds e.g. urea, uric acids , excretion of molecules in bile ,
Detoxifies/removes Drugs &Alcohol

Liver Function
2 .Carbohydrate metabolism
3 . Lipids metabolism
4 . Proteins ( albumin , transport proteins, clotting factors )
production (Produce blood clotting factors I, II, III, V, VII, IX,
XI.)
5 . Secretion of bile : synthesis of bile salts , conjugation & excretion
of bile pigments ,Bile is (Detergent – emulsifies fats & Release
promoted by Vagus n. , CCK , Secretin) , Bile contains : (Water
Bile salts Bile pigments Electrolytes Cholesterol Lecithin)
6 . Stores { Gycolgen , Vitamins (A, D, E, K) Fe and other minerals
,Cholesterol Activates vitamin D}
7 . Fetal RBC production
Bile Production and Secretion
• The liver produces and secretes 250–1500 ml of bile/day.
• Bile pigment (bilirubin) is produced in spleen, bone marrow, and liver.
– Derivative of the heme groups (without iron) from hemoglobin.
• Free bilirubin combines with glucuronic acid and forms conjugated bilirubin. Secreted into bile.
• Converted by bacteria in intestine to urobilinogen. , Urobilogen is absorbed by intestine and enters the hepatic vein. Recycled, or filtered by kidneys and excreted in urine.

Bile Production and Secretion (continued)
• Bile acids are derivatives
of cholesterol.
– Major pathway of
cholesterol breakdown in
the body.
• Principal bile acids are:
– Cholic acid.
– Chenodeoxycholic acid.
• Combine with glycine or
taurine to form bile salts.
– Bile salts aggregate as
micelles.
• 95% of bile acids are
absorbed by ileum.
Insert fig. 18.25

Liver Function Tests
LFT( 1/3rd have abnormal LFT , only 1%
have significant LD )
Liver function tests can be divided into 3parts :
1) Markers of acute hepatocyte injury and death.
SGPT or AST, SGOT or ALT and AP
2) Measures of hepatocyte synthesis function
Prothrombin time and Albumin
3) Indicators of hepatocyte catabolic activity
e.g. Ammonia production
Liver Function Tests
Liver Enzymes
• How does the location of liver enzymes (specifically AST, ALT,
alkaline phosphatase) affect their blood levels in certain diseases?
• The locations of these enzymes are related to their functions. AST
(the enzyme formerly known as SGOT) and ALT (the enzyme
formerly known as SGPT) allow the liver to utilize amino acids for
energy by transferring an amino group from the amino acid to
alpha-ketoglutarate to form glutamate. AST and ALT are integral
enzymes of the hepatocyte, are located in the cytosol (although
some AST is found in mitochondria), and spill into blood when there
is damage to hepatocytes.
• While ALT is highly specific to the liver, remember that AST is
found in other tissues including brain, kidney, heart, muscle,
pancreas, and red blood cells and will therefore be found in blood
when there is damage to these tissues.

Liver enzymes
Alkaline phosphatase, gamma-glutamyl transpeptidase(GGT), and 5'-nucleotidase are membrane proteins located along the canalicular surface of the hepatocyte.
In the liver, alkaline phosphatase is also synthesized by bile duct epithelial lining cells. Alkaline phosphatase actually refers to a family of enzymes that catalyze hydrolysis of phosphate esters at alkaline pH. Like AST, alkaline phosphatase is nonspecific to liver, being also located in bone, placenta, kidney, and intestine.When there is blockage of bile flow, the response of the epithelial lining cells is to increase synthesis and release of alkaline phosphatase, leading to increased levels in the serum. These enzymes are released into blood when bile flow is blocked and there is bile backing up into the liver and causing cell membrane damage. Therefore, elevation of these enzymes in blood is suggestive of cholestasis.

Liver Enzymes
It is sometimes helpful to think of liver function tests in terms of pairs of enzymes, with one member of the pair (e.g. AST) being sensitive but not specific for liver processes, and the other member of the pair (e.g. ALT) usually being specific and confirming that the dysfunction is related to the liver.
Alkaline phosphatase can be thought of as paired with GGT or 5'-nucleotidase in this way (although neither of these latter two enzymes are specific to liver, they are sometimes used as confirmatory tests for hepatobiliary origin of alkaline phosphatase
AST (20% activity is cytosolic and 80% mitochondrial , Half-life 17hrs , ALT mainly Cytosolic and Half-life 47hrs )
Stellate cell • The stellate cell (Ito cell) is the principal source of
fibrosis in cirrhosis. In normal liver, stellate cells are
perisinusoidal cells distributed throughout the liver
which are important for storing the bulk of hepatic
Vitamin A. With liver injury, these cells undergo a
characteristic "activation" (by neighboring cell
paracrine cytokines and lipid aldehydes) in which they
lose vitamin A, proliferate, and become fibrogenic



How to assess the jaundiced
patient? History & Examination : with attention to history, physical
exam and diagnostic tools.
The student shall be able to describe normal bilirubinmetabolism and physiologic consequences associated with it. The student shall be able to understand the clinical classification of jaundice as unconjugated or conjugated, and discuss the various etiologies associated with each.
The student shall be able to explain all the factors necessary in evaluating the jaundiced patient, with attention to obtaining important history from the patient, looking for specific clinical signs on exam, and ordering the appropriate diagnostic laboratory tests and imaging studies.

Signs of Liver Disease
• The student should be able to know about
20 stigmata of CLD .

Caput Medusa




Gamma-GT• Located in hepatocytes and biliary epithelial cells,
pancreas, renal tubules and intestine
• Very sensitive but Non-specific
• Raised in ANY liver discease hepatocellular or
cholestatic
• Usefulness limited
• Confirm hepatic source for a raised ALP
• Alcohol & drugs
• Isolated increase does not require any further
evaluation, suggest watch and rpt 3/12 only if other
LFT’s become abnormal then investigate
ALKALINE PHOSPHATASE
AP is 3 to 4 times raised in children .
AP level doubles in PREGNANCY.
Isolated elevation of AP without marked
hyperbilirubinemia AP:Bil ratio of 1000:1 suggests
Lymphoma, Fungal infections, Sarcoidosis , TB
involvement

PROTHROMBIN TIME
Prolongation of PT in liver diseases relects decreased synthesis of Vitamin K dependent coagulation factors
2,7,9 & 10 and as such serves as a real measure of liver function
Vit. K deficiency can be distinguished from liver synthesis dysfunction by adminstration of Vit.K (10mg IM).
A 30% reduction in PT within 24 hrs should occur in Vit K. Deficiency states.

AMMONIA
• It’s a metabolite of nitrogen containing
products.
• Its metabolised to urea in liver via Krebs
cycle.
• Very high levels are seen in fulminant liver
failure,signifying poor prognosis.

Patterns of liver enzyme alteration
• Hepatic vs cholestatic
• Magnitude of enzyme alteration (ALT >10x vs minor abnormalities)
• Rate of change
• Nature of the course of the abnormality (mild fluctuation vs progressive increase)

Patterns of liver enzyme alteration
• Acute hepatitis –transaminase > 10x ULN
• Cholestatic
• Mild rise in ALT

Acute hepatitis (ALT>10xULN)
• Viral
• Ischaemic
• Toxins & drugs
• Autoimmune
• Early phase of acute obstruction& chalangitis

Cholestasis
• Isolated ALP 3rd trimester, adolescents
• Bone – exclude by raised GGT, 5-NT or isoenzymes
• May suggest biliary obstruction, chronic liver disease or hepatic mass/tumour
• Liver USS/CT most important investigation-dilated ducts
• Ca pancreas, CBD stones, cholangioca or liver mets
Cholestasis – non-dilated ducts
Cholestatic jaundice – Drugs- Antibiotics, Nsaids, Hormones, ACEI
PBC – anti- mitochondrial Ab, M2 fraction, IgM
PSC – associated with IBD 70%, p-ANCA, MRCP and liver biopsy
Chronic liver disease
Cholangiocarcinoma – beware fluctuating levels
Primary or Metastatic cancer, lymphoma
Infiltrative – sarcoid, inflammatory-PMR, IBD
Liver biopsy often required


Investigations
Radiology:
Abdominal Ultrasound
MRCP ;ERCP PTC
CT Abdomen MRI MRA , CT – PET scan
Radionuclide Imaging
Endoscopy Upper GI endoscopy is used for the diagnosis and treatment of varices, for the detection of portal hypertensive gastropathy, and for associated lesions such as peptic ulcers. Colonoscopy may show portal hypertensive colopathy.
Endoscopic ultrasound (EUS)
Black S et al PIDJ 2002 21 810-815
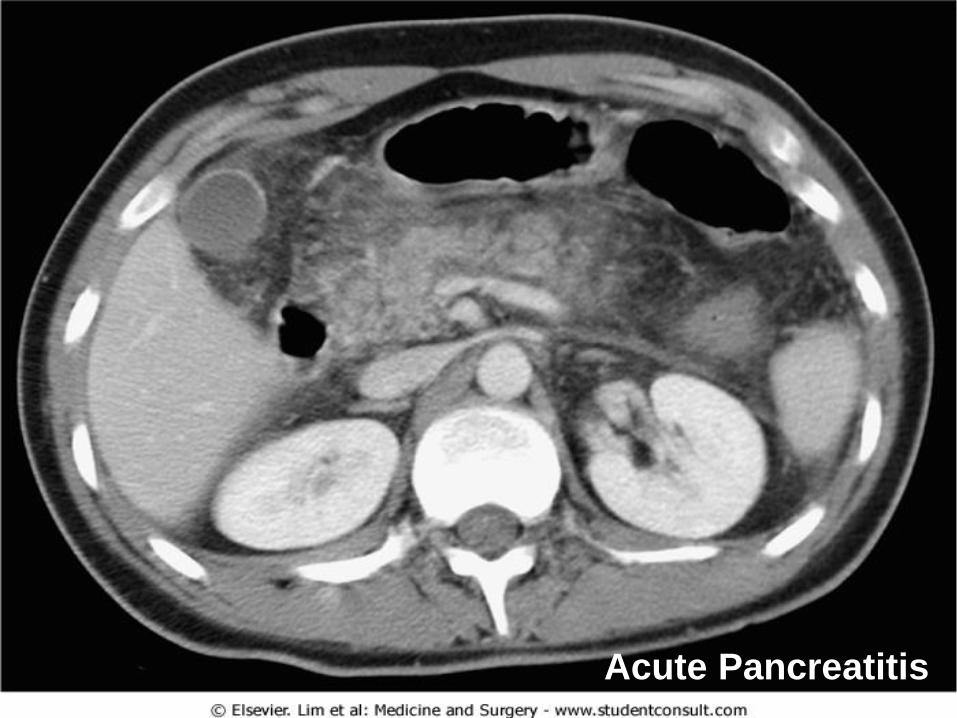
Acute Pancreatitis

Black S et al PIDJ 2002 21 810-815

CMO letter March 31st 2005

* It is important that immunisation does not delay cochlear implantation
CMO letter March 31st 2005

CMO letter March 31st 2005
PET with 18F- FDG

CMO letter March 31st 2005 Liver Adenoma with sponteneous H

MMWR 2000 49 RR-9 1-38Pancreatic Ca

Whitney CG et al NEJM 2003 348 1737-1746

Moxon R International Congress and Symposium Series No 210
London Royal Society of Medicine Press Limited 1995 31-38


Black S et al PIDJ 2000 19 187-195

Whitney CG et al NEJM 2003 348 1737-1746

Black S et al. PIDJ 2000; 19: 187-195
Choo S et al PIDJ 2000; 19: 854-862
Eskola J et al. NEJM 2001; 344: 403-409
Abscess
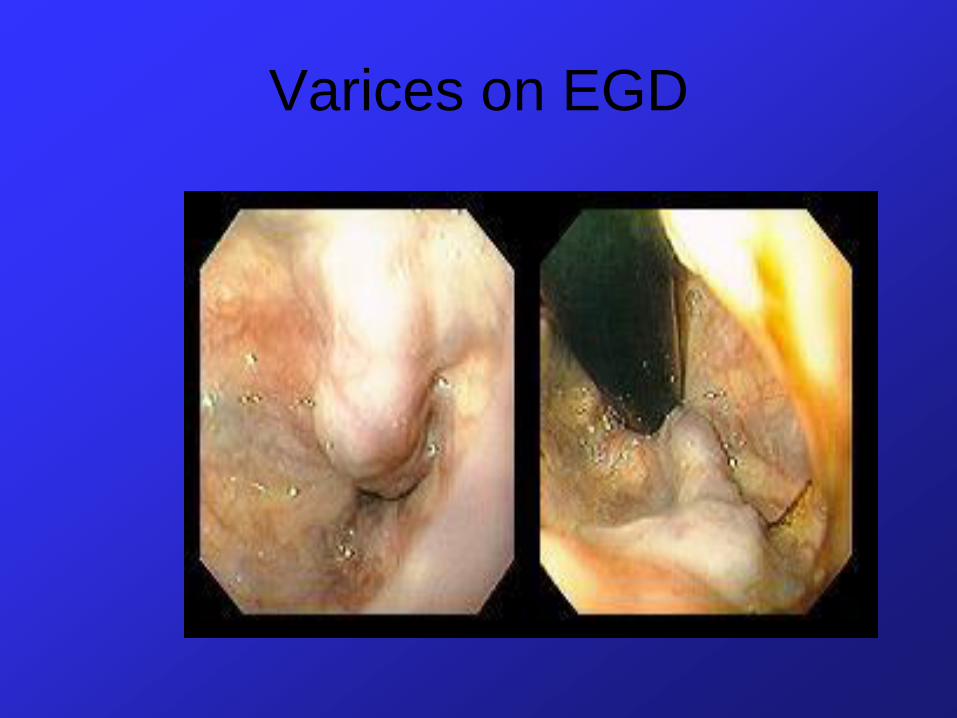
Varices on EGD

Varix Banding

Thank you