disease management programs a winning strategy in today’s competitive markets joe marlowe senior...
TRANSCRIPT

Disease Management Programs Disease Management Programs A Winning Strategy in Today’s Competitive MarketsA Winning Strategy in Today’s Competitive Markets
Joe MarloweSenior Vice PresidentAon ConsultingRadnor, [email protected]

Agenda for Today’s SessionAgenda for Today’s Session
• Setting the Stage
• Basic Principles
• Health and Productivity’s Importance
• Health Behaviors and Chronic Diseases
• Health Management
• Absence and Presenteeism
• Success Indicators

• Population identification process• Evidence-based practice guidelines• Collaborative practice models including physician• Patient self-management education (primary prevention,
behavior modification, compliance/surveillance)• Process and outcomes measurement, evaluation and
management• Routine reporting feedback loop
Source: Disease Management Association of America
““Full Service” Disease Management ComponentsFull Service” Disease Management Components

Why Disease Management?Why Disease Management?
Overall objective with disease management program is to bring
more value into the equation:
Health Care Value = Outcomes + Patient SatisfactionCost
– Coordinate patient care; health system navigation– Reduce expenditure for targeted persons– Increase worker productivity– Improve clinical outcomes– Improve functional status– Enhance patient satisfaction

• 10% individuals spend 70% dollars
• 1% individuals account for 30%
• 33% expenses for preventable conditions
• 50% to 60% hospital admissions due to chronic conditions
Why Disease Management?Why Disease Management?

Disease Management DebateDisease Management Debate
“Disease management is the only remaining strategy to deal with chronic diseases... Perhaps the greatest contribution of Disease Management lies in the fact that it has the potential to drive change in the way we approach healthcare. As a new concept in healthcare delivery, Disease Management is pushing the envelope in how we manage chronic disease.”
—Warren ToddExecutive Director, Past President, and founding
Board Member of the Disease Management Association of America (DMAA)
“There is insufficient evidence to conclude that Disease Management programs can generally reduce overall health spending…The proposition that decreased use of acute care services might offset the costs of the screening, monitoring and educational services in Disease Management programs is clearly appealing, but, unfortunately, much of the literature on those programs does not directly address health care costs.”
—Douglas Holtz-Eakin,Director of the Congressional Budget Office

Disease Management Market Overview—SummaryDisease Management Market Overview—Summary
Runaway medical costs continue to be the central issue in healthcare
Plan sponsors are highly motivated to find cost control solutions
The industry is increasingly focused on the use of integrated interventions in controlling cost
Standalone programs have limited future potential
Disease Management is seeing increased interest
Disease Management (DM) attempts to address gaps in the U.S. healthcare system
Payers are increasingly interested in managing high cost members
The DM industry is evolving to a total management focus
Disease Management is expanding beyond the leading high cost chronic conditions
The DM market is still fragmented but a few players have emerged as market leaders
Leading players are broadening their focus
There is a high level of difficulty in measuring the financial impact of Disease Management programs
The industry as a whole remains very skeptical about the results of recent studies
1
2
3
4
Industry Trend Implications
5
6
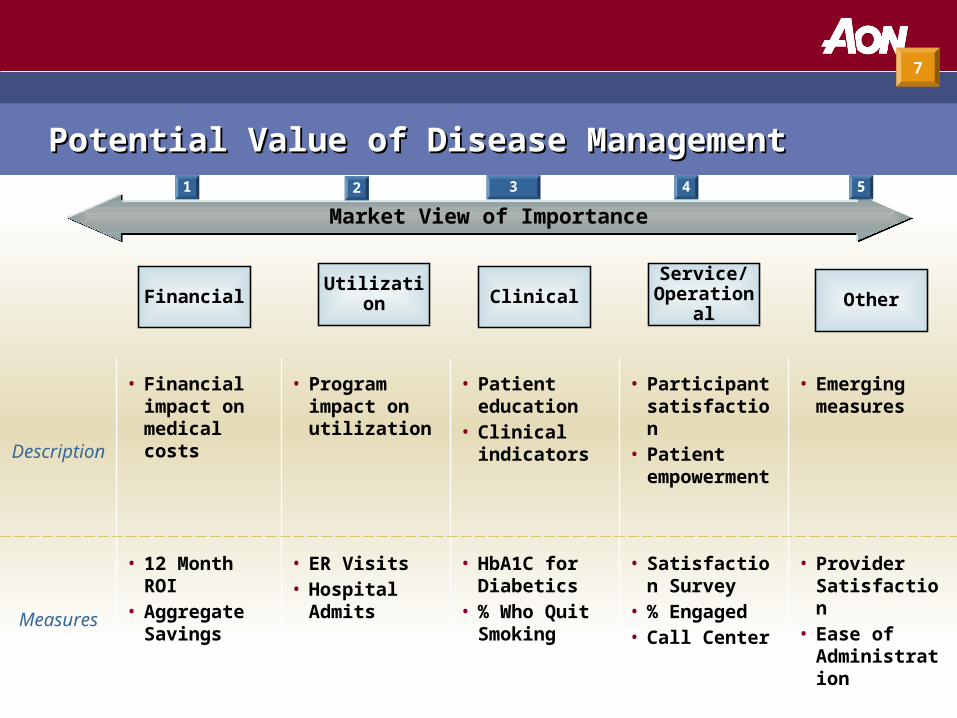
Description
• Financial impact on medical costs
• Program impact on utilization
• Patient education
• Clinical indicators
• Participant satisfaction
• Patient empowerment
• Emerging measures
Measures
• 12 Month ROI• Aggregate
Savings
• ER Visits• Hospital
Admits
• HbA1C for Diabetics
• % Who Quit Smoking
• Satisfaction Survey
• % Engaged• Call Center
• Provider Satisfaction
• Ease of Administration
Market View of ImportanceMarket View of Importance
Financial Utilization ClinicalService/
Operational Other
1 2 3 4 5
7
Potential Value of Disease ManagementPotential Value of Disease Management

Health Management ContinuumHealth Management Continuum
Complex Cases – Transplants– Cancer– Trauma cases
Chronic Care– Diabetes, asthma– CAD, CHF, COPD– Depression
Risk Factors– Alcohol/tobacco usage – Physical inactivity– Poor nutrition – Health history– Unmanaged stress– Inadequate self-care
Acute Care– Broken leg– Kidney stones– Pneumonia
Health Promotion
Care Management
Case/Disease
Management
Living w/Illness(16% population)
Staying Healthy (70% population)
15% costs 60% costs25% costs
Getting Better(14% population)
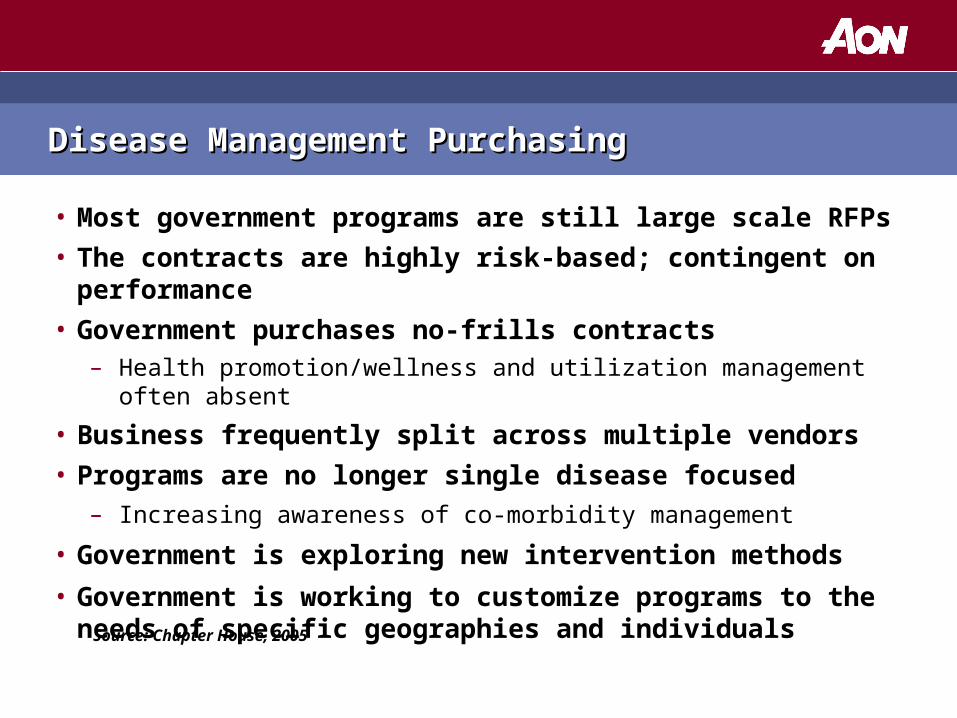
Disease Management PurchasingDisease Management Purchasing
• Most government programs are still large scale RFPs
• The contracts are highly risk-based; contingent on performance
• Government purchases no-frills contracts– Health promotion/wellness and utilization management often absent
• Business frequently split across multiple vendors
• Programs are no longer single disease focused– Increasing awareness of co-morbidity management
• Government is exploring new intervention methods
• Government is working to customize programs to the needs of specific geographies and individuals
Source: Chapter House, 2005

Managing Chronic DiseaseManaging Chronic Disease
• Identify problem diseases to target for management
• Plan your strategy
• Identify and evaluate vendors
• Develop innovative performance guarantees
• Negotiate contracts
• Communicate
• Implement the program
• Conduct ongoing performance measurement– Clinical– Financial– Satisfaction

• Prevalence of chronic disease states in population
• Prevalence of multiple co-morbid chronic disease
• Unique members with a chronic disease
• Cost implications for those with chronic disease
• Drug costs for the chronic diseases identified
• Clinical conditions driving large dollar claims
• Identify “gaps” in care delivery / availability of programs
Identifying Problem Disease States w/Dx AnalysisIdentifying Problem Disease States w/Dx Analysis

• Affects large number of population
• Expensive to treat
• Potential for serious complications
• Avoidable complications
• Measurable impact
• Reasonable return on investment
Case SelectionCase Selection

Identify and Evaluate Vendors – Key ParametersIdentify and Evaluate Vendors – Key Parameters
• Program design
• Scope of services/diseases managed
• Clinical resources
• Risk sharing/performance guarantees
• IT/Technology– Remote patient monitoring to gather clinical data coupled with “smart
system” intervention (e.g., scales, blood pressure, glucose monitors)
• Enrollment processes
• Communication
• Reporting

Essential Components for Successful ProgramEssential Components for Successful Program
• Data driven identification and risk-stratification– Predictive technology gives no insight into supportive environment for
targeted individuals
• Proven enrollment approach– Readiness to change: engage person directly
• Proactive patient outreach
• Participation incentives
• Use of evidence-based treatment guidelines
• Customized care plans to meet each patient’s unique needs
• Management of co-morbid conditions
• Clinical, financial, and satisfaction outcome reporting
• Performance guarantees

• Develop comprehensive RFP
• Incorporate your specific requirements
• Secure the necessary information from the vendors to address your particular needs and expectations
• Prepare summary evaluations of selected vendors
• Develop selection criteria
• Complete site visits with finalists
• Provide data for analysis by finalists
• Select a partner(s)
Important Evaluation StepsImportant Evaluation Steps

• Most vendors sound the same
• Have clear idea of program objectives
• Get beneath vendor’s skin
• Negotiate performance guarantees
Purchaser CautionsPurchaser Cautions

• Guide the development and selection of meaningful performance guarantees (clinical, financial, satisfaction)
• Craft risk and reward program that provides incentives to advance your financial interest
• Secure the best possible terms and contract conditions
• Financial risk sharing less popular due to:– Higher fee structure to cover reinsurance premiums– Proven results make risk sharing less important
Performance Guarantees and Contract NegotiationsPerformance Guarantees and Contract Negotiations

• Identify audiences and challenges for reaching them
• Determine appropriate strategy and media– Match messages to audience
• Not “Big Brother”
• Determine appropriate incentives for targeted groups– Financial – Non-financial
• Coordinate flow of information from the vendor and your organization
• Monitor and refine communication plan, as needed
• Reinforce message periodically
Member Communication – Critical IngredientMember Communication – Critical Ingredient

Some ConsiderationsSome Considerations
• Population-based approach to health management– Wellness services to assist those at risk of chronic condition– Coordination with case management resources– Single person, single disease state management losing appeal
• Partner with local medical providers and community resources• Behavioral health assessment and treatment
– Depression or chemical dependency as primary or secondary diagnosis
• Technology becoming increasingly important– Online program educational materials (symptom advisor)– Provider reports– Patient profiles

Realities of the High Risk PopulationRealities of the High Risk Population
• Sicker than most DM vendors anticipate• More intensive management needed (higher intervention costs)• Need to tap into social services• More costly during early patient attraction phase
– Psychosocial (not pure medical) challenges– Demands more social workers to be effective– More costly engagement strategies (lack of phone numbers)
• With effective overtures, expect solid voluntary program enrollment
– May require that >70% of targeted group enroll to give ROI– High satisfaction demonstrates pent up demand for DM services
• Premium on speed of intervention– Same day early alert for hospitalizations and discharges
• Role for face-to-face assessments– Substitute for less expensive, traditional call center approach
• Role for local pharmacists

Importance of Healthy BehaviorsImportance of Healthy Behaviors
What What
We We
Know Know
About About
Health Health
BehaviorsBehaviors


Mortality Risk Factors In The U.S.Mortality Risk Factors In The U.S.
Heredity20%
Environment19%
Health Services
10%
Lifestyle51%
Source: Centers for Disease Control and Prevention

Source: Goetzel,JOEM, Vol. 40, No. 10 Oct. 1998
Difference in Medical Costs - High vs. Low RiskDifference in Medical Costs - High vs. Low Risk
70.2
34.8
21.4 19.714.5 11.7 10.4
46.3
01020304050607080
Dep
ress
ion
Str
ess
Glu
cose
Wei
ght
Tob
acco
-Pas
t
Tob
acco
Blo
odPre
ssure
Exe
rcis
e
Per
centa
ge

Economic Case for Health Management ProgramsEconomic Case for Health Management Programs
$3,432$4,130
$6,664
$9,221$10,095
$2,025$2,741
$3,601
$5,445
$7,268
$1,247 $1,515 $1,920
$3,366
$4,319
$0
$2,000
$4,000
$6,000
$8,000
$10,000
$12,000
<35 35-44 45-54 55-64 65+
Costs Increase With Health Risk and Age
0-2 Risks
3-4 Risks
5+ Risks
Source: StayWell data analyzed by U of Michigan (N = 43,687) – HERO Study

Obesity – A National ChallengeObesity – A National Challenge
• Considered of epidemic proportion
• 31% of adults and 16% of adolescents
• Metabolic syndrome contributes to risk of serious disease
– Increased blood pressure
– Elevated insulin levels
– Excess body fat around the waist
– Abnormal cholesterol levels
• Physical inactivity and unhealthy eating primary contributors
Source: National Center for Policy Analysis, May 2003; JAMA, 1999

Medical Costs and Risks by Body Mass IndexMedical Costs and Risks by Body Mass Index
Musich, Lu, McDonald, Champagne, Edington, AJHP.18(3): 125 132, 2004. University of Michigan Health Management Research Center
Annual MedicalCosts
$0
$2,000
$4,000
$6,000
$8,000
0 risks +1 risk +2 risks +3 risks +4 risks
Risk Level
$2,667$3,201
$3,995$4,760
$6,667
$3,239$3,921
$4,500$5,079
$7,118
$3,579$4,014
$4,611$5,753
$7,758
$4,151 $4,214$5,176
$5,844
$8,075
– < 25
– 25-29.9
– 30-34.9
– > 35
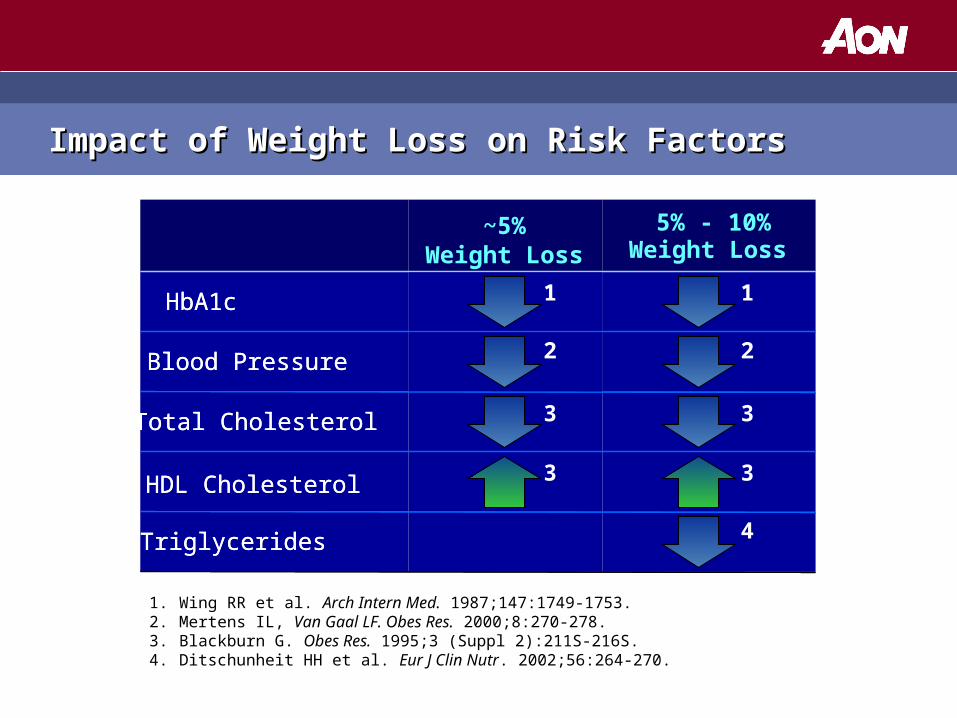
Impact of Weight Loss on Risk FactorsImpact of Weight Loss on Risk Factors
1. Wing RR et al. Arch Intern Med. 1987;147:1749-1753.2. Mertens IL, Van Gaal LF. Obes Res. 2000;8:270-278.3. Blackburn G. Obes Res. 1995;3 (Suppl 2):211S-216S.4. Ditschunheit HH et al. Eur J Clin Nutr. 2002;56:264-270.
Triglycerides
HDL Cholesterol
Total Cholesterol
Blood Pressure
HbA1c
Weight Loss~5%
Weight Loss
Triglycerides
HDL Cholesterol
Total Cholesterol
Blood Pressure
HbA1c
5% - 10%Weight Loss
~5%Weight Loss
1
2
3
3
1
2
3
3
4
Chronic Disease Linked to ObesityChronic Disease Linked to Obesity
• Cardiovascular diseases
• Diabetes
• Hyperlipidemia
• Gout
• Osteoarthritis
• Gallstones
• Cancers
Obesity accounts for 5-8% of direct medical costs Obesity accounts for 5-8% of direct medical costs and leads to premature disability and mortalityand leads to premature disability and mortality
Source: Cas Lek Cesk. 1997 Jun 12;136(12):367-72.

Depression: “The Silent Cost Driver”Depression: “The Silent Cost Driver”
• Depression can be triggered by a chronic disease
• Depression can be a marker for other conditions
• Research links depression to the later development of:
– Asthma
– Diabetes
– Heart disease
– Hypertension
– Obesity
– Stroke
Source: Centers for Disease Control and Prevention

Market TrendsMarket Trends
• Many vendors have entered this market, but only a few can offer the entire range of services:– Lots of Health Plans, TPAs, HMOs, DM vendors, HRA and other specialty
vendors operate in this space– Fair amount of purchasing, partnering, and outsourcing
• Some vendors have superficial offerings that lack design and execution capability– Participation rates– Intensity of interventions– Results
• Resist the temptation to generalize across vendors• Learn to differentiate among vendors• ROI less important than program design and execution:
– Vendors control ROI methodologies and calculations – False expectations of high ROI savings
Vendor DifferentiatorsVendor Differentiators
• Risk identification process (HRA tool, assigning risk factors)
• Healthcare coaching model (outreach, interventions, consistency)
• Track record on connecting and engaging targeted individuals• Technology (portal, personalized programs, flexibility)• Web content• Integration with employer plans and vendors• Participation incentives (ability to administer)• Metrics • Communications• Future initiatives/enhancements
Disease Management Outcomes Measurement (ROI)Disease Management Outcomes Measurement (ROI)
• New focus on utilization rather than pre-post cost analysis – Unproductive debate about statistical biases for cost-based studies
• Chronic disease-related hospital admissions and ER visits– ALOS and readmission rates– Literature does not point to reductions in outpatient visits, pharmacy, etc.
• Question: “If there a sufficient number of avoidable admissions to justify DM program fees?”
– Standard costs per avoidable hospital stay times potential reduction compared to DM program fees
• Standard financial cost methods may overstate savings• What are the savings assumptions used by your DM vendor?
– Are they specific to your unique population?– High risk group ROIs may be less than commercial population
• Confounding variable: member turnover and deaths, multiple conditions (diagnoses)
• Population risk adjustment of baseline and intervention