discrimination of patients with microsatellite...
TRANSCRIPT

Discrimination of Patients with Microsatellite Instability Colon
Cancer using 1H HR MAS MR Spectroscopy and Chemometric
Analysis
May-Britt Tessem,*,† Kirsten M. Selnæs,† Wenche Sjursen,‡,§ Gerd Tranø,|
Guro F. Giskeødegård,† Tone F. Bathen,† Ingrid S. Gribbestad,† and Eva Hofsli⊥
Department of Circulation and Medical Imaging, Norwegian University of Science and Technology (NTNU),Trondheim, Norway, Department of Laboratory Medicine Children’s and Women’s Health, NTNU, Trondheim,
Norway, Department of Pathology and Medical Genetics, St. Olavs University Hospital, Trondheim, Norway,Department of Surgery, Levanger Hospital, Sykehuset Innherred, Levanger, Norway, and Department of
Oncology, St. Olavs University Hospital, Trondheim, Norway
Received February 27, 2010
The primary aim of this study was to analyze human colon cancer and normal adjacent tissue using 1HHR MAS MR spectroscopy and chemometric analyses, evaluating possible biomarkers for colon cancer.The secondary aim was to investigate metabolic profiles of tissue samples (n ) 63, 31 patients) withmicrosatellite instability (MSI-H) compared to microsatellite stable (MSS) colon tissue. Our hypothesiswas that this method may provide an alternative to MSI genotyping. Cancer samples were clearlyseparated from normal adjacent mucosa by 100% accuracy. Several metabolites such as lactate, taurine,glycine, myo-inositol, scyllo-inositol, phosphocholine (PC), glycerophosphocholine (GPC), creatine, andglucose were identified as potential biomarkers for cancer detection. Adenomas (n ) 4) were alsoseparated from cancer and normal samples mainly based on higher GPC and PC levels. Interestingly,metabolic differences in normal colon mucosa between MSI-H and MSS patients were observed. MSIstatus was validated with 80% accuracy with a sensitivity and specificity of 79% and 82%, respectively,including both cancer and normal samples The metabolic differences between MSI-H and MSS maybe very interesting in the early detection of cancer development and of high clinical importance in thework of improving diagnosis and characterization of colon cancer.
Keywords: metabolomics • metabolites • promoter MLH1 methylation • MSI • MSS • PCA • PLSDA
Introduction
Colorectal cancer (CRC) is one of the most common malig-nancies and leading cause of cancer-related deaths. In Norway,CRC is the second most frequent cancer and the incidence ishigher compared to the U.S., where CRC is the third mostcommonly diagnosed type of cancer, accounting for 10% ofestimated new cases among leading cancer types.1 The inci-dence of CRC in Norway has been highly increasing the last50 years, and today the incidence is about the highest amongEuropean countries.2
Genetic instability can differ from whole chromosomalaberrations to small differences in a few base pairs, causingseveral changes to the phenotypical traits of the cell. In
colorectal cancer, genetic instability is usually classified intothree pathways including chromosomal instability (CIN), mi-crosatellite instability (MSI) and CpG island methylation phe-notype (CIMP).3 MSI is referred to as abnormally long or shortrepetitive DNA sequences, microsatellites, which are causedby defects in the DNA mismatch repair (MMR) system. Themajority of patients with hereditary nonpolyposis colorectalcancer (HNPCC/Lynch syndrome) have high-frequency mic-rosatellite instability (MSI-H) caused by an inherited mutationin one of the MMR-genes, and about 15% of sporadic colorectalcancers are characterized by MSI-H caused by epigeneticchanges.4 MSI status is important as a screening tool forHNPCC/Lynch syndrome, as a prognostic marker5 and as apredictor of response to therapy.3 CRC patients with MSI seemto have a better prognosis and survival compared to those whoare microsatelite stable (MSS).5 One study found that patientswith MSI-H tumors do not respond to a certain type of adjuvantchemotherapy (fluorouracil) for colon cancer,6 but the predic-tive value of chemosensitivity is controversial.7,8 Therefore, abetter understanding of tumor biology is important for opti-mizing treatment strategies and for the implementation of MSIanalyses in a clinical setting.
* To whom correspondence should be addressed. May-Britt Tessem,University of Science and Technology (NTNU), Dept. of Circulation andMedical Imaging, MTFS, MR Centre 7489 Trondheim, Norway, [email protected], Tel: +74 92406886/+47 73598836.
† Department of Circulation and Medical Imaging, NTNU.‡ Department of Laboratory Medicine Children’s and Women’s Health,
NTNU.§ Department of Pathology and Medical Genetics, St. Olavs University
Hospital.| Department of Surgery, Levanger Hospital, Sykehuset Innherred.⊥ Department of Oncology, St. Olavs University Hospital.
3664 Journal of Proteome Research 2010, 9, 3664–3670 10.1021/pr100176g 2010 American Chemical SocietyPublished on Web 05/27/2010

MSI in sporadic colorectal cancer usually arises from epi-genetic silencing of the DNA mismatch repair gene MLH1,which is caused by methylation of promoter sequences of thegene.9 Epigenetic silencing, the third pathway of geneticinstability, will not change the DNA sequence but affects thegene function by causing deficiency in protein expression. CRCpatients with MLH1 methylation causing MSI-H tumors arefound to have a better cancer-specific survival compared topatients with MSS tumors.3 The classification of MSI-H andMSS is therefore of clinical importance in the assessment ofprognosis. New methods are therefore needed to elucidatebiological mechanisms within the MSI pathway.
High resolution proton magic angle spinning (1H HR MAS)is an ex vivo method providing detailed information onmetabolic composition (metabolic profiles) of several types ofintact cancer tissue.10-13 Metabolic profiling of CRC using 1HHR MAS has recently shown promising results for understand-ing CRC and for optimizing clinical management strategies.14
A few studies have presented that metabolic profiles of col-orectal cancer and normal mucosa are clearly discriminatedanalyzed by 1H HR MAS.14-18 Altered metabolites in CRC tissuewere associated with expected metabolic perturbation such aselevated tissue glycolysis, hypoxia, nucleotide biosynthesis, lipidmetabolism, inflammation, and steroid metabolism.14 Cor-relating metabolic profiles to the pathways of genetic instabilityand clinical parameters may provide a better understandingof colon cancer development using 1H HR MAS MR spectros-copy.
MR spectra are highly multivariate data sets requiringsophisticated statistical analysis, chemometric approaches, toprovide information about the metabolic status of a tissuesample. One of the most common methods is principalcomponent analysis (PCA), by which linear combinations ofthe variables explains the variance structure in the data set.This can reveal hidden relationships, patterns or grouping ofthe multivariate MR spectral data. A supervised method suchas partial least-squares regression discriminant analysis(PLSDA) attempts to discriminate between groups, for example,cancer and normal tissue, and where the relationship betweentwo matrices x (MR spectra) and y (properties related to eachspectrum) is modeled. These chemometric analyses are im-portant tools for model building and classification of MR data.
The primary aim of this study was to characterize themetabolic profile of human colon tissue using 1H HR MAS andto evaluate possible biomarkers for colon cancer. The second-ary aim was to investigate metabolic profiles of samples withMSI-H, caused by promoter MLH1 methylation, compared toMSS. Our hypothesis was that metabolite profiling using 1HHR MAS and chemometric analyses may provide a reliablerapid alternative or additional test to MSI genotyping. Thehypothesis was validated using blind samples which had notbeen used earlier in the model building.
Material and Methods
Patients and Tissue Collection. Fresh frozen colon tissuesamples (n ) 63) from two hospitals in Norway19 were obtainedfrom 31 newly diagnosed cancer patients (mean age: 73 years(range: 48-93), 16 women and 15 men). Two samples werecollected from each patient; one from the tumor area and theother from normal mucosa. Twenty-eight samples were col-lected from patients diagnosed with colon adenocarcinoma and4 samples from patients diagnosed with adenomas. One patienthad two malignant tumors in the operation species, and both
were included in the analyses. Thirty-one samples of normalmucosa were collected. Eighteen cancer samples were MSI-Hand 14 cancer samples were MSS. Normal adjacent tissue wasalso labeled MSI-H if the patient had an adjacent tumor thatwas MSI-H. Including both cancer, adenomas and normalmucosa, a total of 35 MSI-H samples and 28 MSS samples wereanalyzed. Two of the MSI-H tumors had no MLH1 promotermethylation and was therefore most likely HNPCC/Lynchsyndrome tumors. Clinical patient data are shown in Table 1.The study was approved by the Regional Committee forMedical and Health Research Ethics, and written informedconsent was obtained from all contributing patients.
Preoperatively, broad-spectrum antibiotics and low-molec-ular-weight heparin had routinely been administrated to thepatients. In the majority of cases, the patients had been givenmechanical laxatives preoperatively. Tissue samples were col-lected immediately during surgery and frozen at -80 °C.
1H HR MAS Spectroscopy and Data Processing. A phosphate-buffered saline (PBS, 3 µL) based on deuterium oxide (D2O)containing 4.5 mM TSP (sodium-3′-trimethylsilylpropionate-2,2,3,3-d4) and 20 mM formate was added to disposable Kel-FHR MAS inserts (30 µL, Bruker, Germany). The colon tissue(weight; cancer: 14.4 ( 2.6 mg and normal: 15.1 ( 4.2 mg) wasadded to the HR MAS insert using a sterile disposable biopsypunch with plunger (2 and 1.5 mm, Miltex Gmbh, Germany),and the insert was placed into the 4 mm zirconium HR MAS-rotor. 1H HR MAS was performed on a 14.1 T Bruker AvanceDRX spectrometer equipped with a 4-mm 1H/13C MAS probe.Spectra were acquired at 4 °C with a spin rate at 5 kHz. A Carr-Purcell-Meiboom-Gill (CPMG)20 spin echo sequence [90° -(τ-180°-τ)n] with an effective echo time of 272 ms wasacquired to suppress signals from overlapping lipids andmacromolecules. One hundred and twenty-eight scans over aspectral region of 10 kHz were collected into 64k points, givingan acquisition time of 3.27 s. An exponential line broadeningof 0.30 Hz was applied to the raw data before Fouriertransformation. The spectra were chemically shift referencedto the lactate peak (left peak in the doublet) at 1.33 ppm, anda linear baseline correction was applied. MR data points were
Table 1. Clinical Data
Age Mean 73 yearsRange 48-93
Gender Males 15Females 16
Histology Cancer 28Adenoma 4Normal mucosa 31
Differentiation Low 7Medium 21
Dukes stage A 4B 14C 6D 4
T-stage T1 2T2 2T3 20T4 4
Lymph node status No (NX, N0) 18Yes (N1, N2) 10
Anatomical site Left colon 8Right colon 22
MSI MSI-H 35MSS 28
Discrimination of Patients with MSI Colon Cancer research articles
Journal of Proteome Research • Vol. 9, No. 7, 2010 3665
reduced from 64k to 16k for chemometric analysis. For assign-ment purposes, total correlation spectroscopy (TOCSY) wasperformed on some of the tissue samples.
Histopathology. After HR MAS analysis, the tissue sampleswere fixed in 10% formalin, embedded in paraffin, sectioned(3 µm) and stained with HES (hematoxylin, erythrosine andsaffron) for pathology reading. The sections were deparaffinisedin xylene for 10 min two times and subsequently rehydratedin decreasing concentrations of alcohol. An experienced pa-thologist examined the tissue slides and provided percentcancer tissue content (desmoplastic stroma not included) andinformation about necrosis and inflammatory responses.
Analyses for MSI and Promoter MLH1 Methylation. Analy-ses of MSI and MLH1 methylation were performed as describedby Tranø et al.21
Chemometric Analysis. The spectral region between 1.4 and4.8 ppm was transferred to ASCII format and used for multi-variate analysis. Contaminated areas due to ethanol andpolyethylene glycol (from preoperative bowel preparation)(3.63-3.73 ppm) and the dominating peak from acetate(1.90-1.94 ppm) were removed from the data set, resulting ina total of 3166 variables. The final data were mean normalizedand mean centered before further analysis by principal com-ponent analysis (PCA). The spectral data (n ) 63) were alsoused to build models for cancer and normal tissue, MSI-H andMSS samples and gender by using partial least-squares dis-criminant analysis (PLSDA). The relationship between age andthe spectral data was modeled using partial least-squaresregression (PLS). One cancer sample was excluded from theprediction model of cancer and normal because of a cancercontent <1%. The MR spectra from the cancer samples (n )27) were also analyzed with respect to T-stage, differentiation(medium/low), Dukes stage (A, B, C, D) and anatomical site ofcancer (right colon defined as proximal to the spleenic flexure)using PLSDA. Number of samples used for each test differeddue to availability of clinical data (see Table 1). The numberof latent variables (LVs) used for building the models wasdetermined by finding the LV where the total residual y-variance and root-mean-square error of prediction were mini-
mized. Full cross-validation was applied. All statistical analyseswere performed using PLS_Toolbox 5.2.2 for Matlab (Eigen-vector Research, Wenatchee, WA).
To investigate robustness of the models for prediction ofcancer and MSI, separate sample sets for model building andvalidation were established based on unsupervised sampleselection22 of all the spectral data (n ) 63). The Kennard Stonealgorithm selects samples that are furthest away from eachother in the data set one by one. The samples with themaximum distance (variance) were used for model construction(n ) 38), and the Kennard-Stone algorithm assured representa-tive samples for the validation (n ) 25). The training modelwas based on full cross validation. The validation samples werekept outside all model training. To further validate the PLSDAresults, additional permutation tests were performed 10 000times both for the cancer and normal model and for the MSI-Hand MSS model.
Results
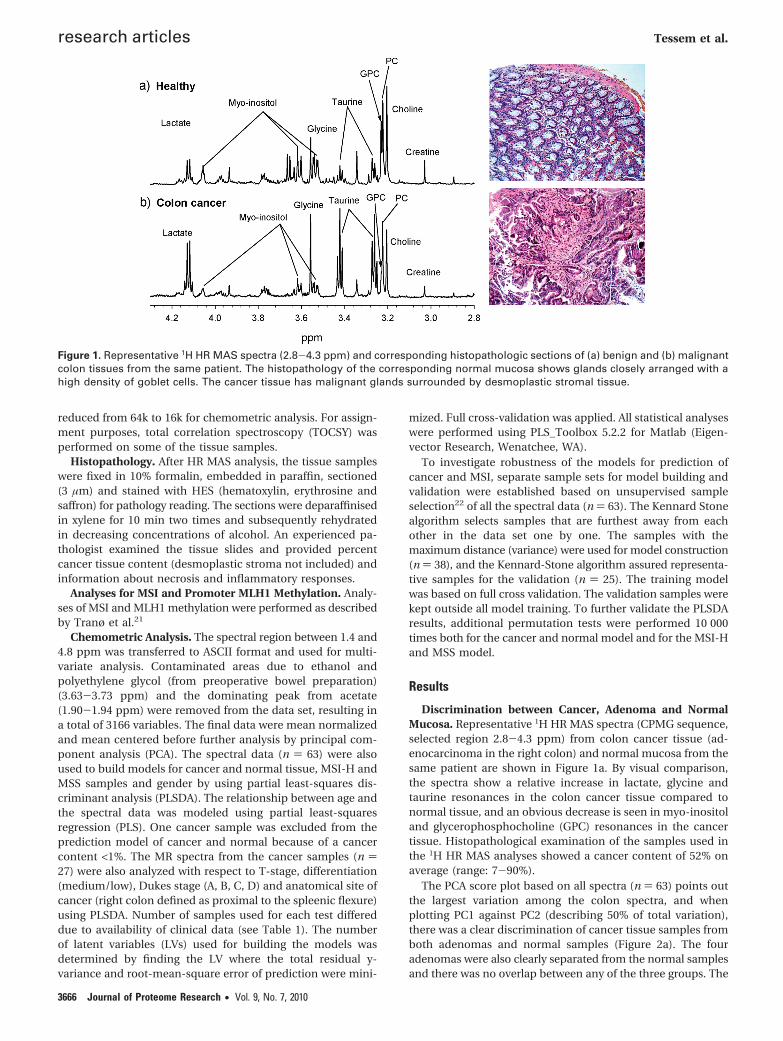
Discrimination between Cancer, Adenoma and NormalMucosa. Representative 1H HR MAS spectra (CPMG sequence,selected region 2.8-4.3 ppm) from colon cancer tissue (ad-enocarcinoma in the right colon) and normal mucosa from thesame patient are shown in Figure 1a. By visual comparison,the spectra show a relative increase in lactate, glycine andtaurine resonances in the colon cancer tissue compared tonormal tissue, and an obvious decrease is seen in myo-inositoland glycerophosphocholine (GPC) resonances in the cancertissue. Histopathological examination of the samples used inthe 1H HR MAS analyses showed a cancer content of 52% onaverage (range: 7-90%).
The PCA score plot based on all spectra (n ) 63) points outthe largest variation among the colon spectra, and whenplotting PC1 against PC2 (describing 50% of total variation),there was a clear discrimination of cancer tissue samples fromboth adenomas and normal samples (Figure 2a). The fouradenomas were also clearly separated from the normal samplesand there was no overlap between any of the three groups. The
Figure 1. Representative 1H HR MAS spectra (2.8-4.3 ppm) and corresponding histopathologic sections of (a) benign and (b) malignantcolon tissues from the same patient. The histopathology of the corresponding normal mucosa shows glands closely arranged with ahigh density of goblet cells. The cancer tissue has malignant glands surrounded by desmoplastic stromal tissue.
research articles Tessem et al.
3666 Journal of Proteome Research • Vol. 9, No. 7, 2010

four patients diagnosed with adenomas were separated fromthe normal samples by PC1 but also from the cancer samplesby PC2. The loadings for the PCA model (not shown) indicateda considerably higher relative concentration of phosphocholine(PC) in three of the adenomas (discriminated by PC1, 31% ofthe variance) compared to both cancer and normal tissue anda higher relative concentration of GPC (discriminated by PC2,19% of the variance) in 1 of the 4 adenomas. Another interestingobservation in the PCA score plot was that the two patientsmost likely having the hereditary type of MSI cancer (HNPCC/Lynch syndrome) had scores appearing close to the normalsamples (Figure 2a). Tumors from these two patients had nomethylation of the MLH1 promoter.
To demonstrate the differences between cancer and normalcolon HR MAS spectra, the adenomas were removed from thedata set and PLSDA was performed on all the cancer andnormal samples (n ) 58). The PLSDA model was based on 3LVs for describing the total residual y-variance. The score plotof LV1 against LV2 (explaining 45% x-variance and 83%y-variance) showed a clear separation of the cancer samplesfrom the normal samples. The cross-validated correlationbetween the true class and the class predicted is 0.89 (rcalibration
) 0.94, Figure 2b). The cancer samples had a more scattereddistribution than the normal samples in the PLSDA score plot(Figure 2b). This is also shown in the results listed in Figure2a. The loadings for LV1 (Figure 2c, explaining 24% x-varianceand 79% y-variance) showed the metabolites responsible forseparation between cancer and normal samples. The HR MASspectra from colon cancer tissue had a relative higher concen-tration of lactate, glycine, taurine, PC and choline than thenormal samples, but a relative lower concentration of creatine,GPC, scyllo-inositol, myo-inositol and �-glucose.
For the prediction, 24 validation samples were all classified100% correctly as cancer and normal tissue. The prediction wasbased on a training set of cross validated data from 38 sampleschosen by Kennard Stone. Permutation testing (n ) 10 000)showed that the prediction results were significantly differentfrom random (p < 0.0001).
The PLSDA results from the correlation to all the otherclinical parameters tested (Dukes stage, differentiation, age,gender, location and lymph node status) are shown in Table2. No correlations were detected except to age.
Discrimination between MSI-H and MSS. Samples frompatients with MSI-H and MSS tumors were discriminated by
Figure 2. (a) PCA score plot of PC1 and PC2 (50% of totalvariation, n ) 63) shows discrimination of cancer samples (n )27) from normal samples (n ) 31) and discrimination of ad-enomas (n ) 4) from both cancer and normal samples. Two ofthe cancer patients were most likely HNPCC/Lynch syndromepatients, in which cases the scores appear close to the normalsamples. (b) PLSDA score plot of LV1 and LV2 (explaining 45%x-variance and 83% y-variance) shows separation of metabolicprofiles from cancer (n ) 27) and normal tissue (explaining 10%x-variance and 23% y-variance, n ) 31). (c) LV2 loadings plot(explaining 24% x-variance and 79% y-variance) shows metabolicalteration in several metabolites of cancer tissue compared tonormal colon mucosa.
Table 2. Result from PLSDA of All the Tested Parametersa
correlation cofficient r (calibration/validation)
correlations
all sampleswithout
adenomas(n ) 59)
all samples withadenomas(n ) 63)
cancer(n ) 27)
normal(n ) 31)
Cancer/normal 0.92/0.82b 0.94/0.89c
MSI-H/MSS 0.81/0.50 0.86/0.58 d 0.79/0.53Age 0.68/0.43 0.67/0.45 0.85/0.56 0.83/0.59Anatomical site
(left/right)0.46/0.21
Gender d d 0.65/0.32 d
Dukes classification(A,B,C,D)
d
T-stage(T1, T2, T3, T4)
d
Lymph nodestatus (Nx, N1, N2)
d
a Correlation coefficient for both the calibration and validation (inbold) are listed. b n ) 58. c n ) 62. d Not able to build a model based onthe data, no reduction in residual variance.
Discrimination of Patients with MSI Colon Cancer research articles
Journal of Proteome Research • Vol. 9, No. 7, 2010 3667
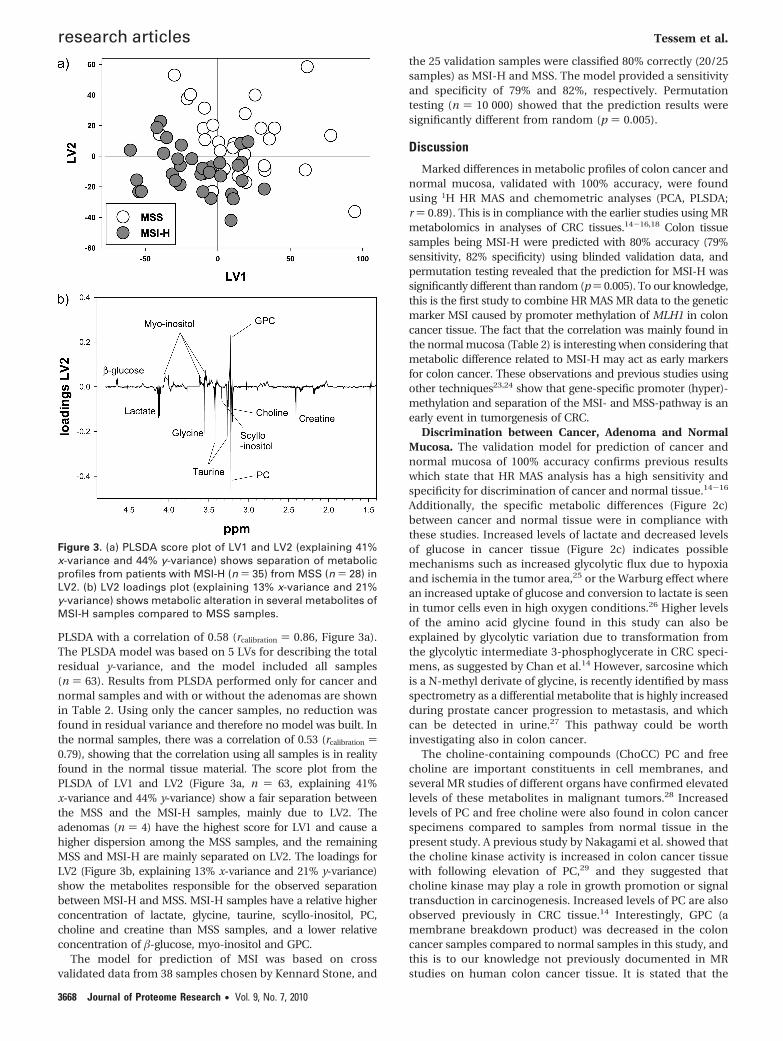
PLSDA with a correlation of 0.58 (rcalibration ) 0.86, Figure 3a).The PLSDA model was based on 5 LVs for describing the totalresidual y-variance, and the model included all samples(n ) 63). Results from PLSDA performed only for cancer andnormal samples and with or without the adenomas are shownin Table 2. Using only the cancer samples, no reduction wasfound in residual variance and therefore no model was built. Inthe normal samples, there was a correlation of 0.53 (rcalibration )0.79), showing that the correlation using all samples is in realityfound in the normal tissue material. The score plot from thePLSDA of LV1 and LV2 (Figure 3a, n ) 63, explaining 41%x-variance and 44% y-variance) show a fair separation betweenthe MSS and the MSI-H samples, mainly due to LV2. Theadenomas (n ) 4) have the highest score for LV1 and cause ahigher dispersion among the MSS samples, and the remainingMSS and MSI-H are mainly separated on LV2. The loadings forLV2 (Figure 3b, explaining 13% x-variance and 21% y-variance)show the metabolites responsible for the observed separationbetween MSI-H and MSS. MSI-H samples have a relative higherconcentration of lactate, glycine, taurine, scyllo-inositol, PC,choline and creatine than MSS samples, and a lower relativeconcentration of �-glucose, myo-inositol and GPC.
The model for prediction of MSI was based on crossvalidated data from 38 samples chosen by Kennard Stone, and
the 25 validation samples were classified 80% correctly (20/25samples) as MSI-H and MSS. The model provided a sensitivityand specificity of 79% and 82%, respectively. Permutationtesting (n ) 10 000) showed that the prediction results weresignificantly different from random (p ) 0.005).
Discussion
Marked differences in metabolic profiles of colon cancer andnormal mucosa, validated with 100% accuracy, were foundusing 1H HR MAS and chemometric analyses (PCA, PLSDA;r ) 0.89). This is in compliance with the earlier studies using MRmetabolomics in analyses of CRC tissues.14-16,18 Colon tissuesamples being MSI-H were predicted with 80% accuracy (79%sensitivity, 82% specificity) using blinded validation data, andpermutation testing revealed that the prediction for MSI-H wassignificantly different than random (p ) 0.005). To our knowledge,this is the first study to combine HR MAS MR data to the geneticmarker MSI caused by promoter methylation of MLH1 in coloncancer tissue. The fact that the correlation was mainly found inthe normal mucosa (Table 2) is interesting when considering thatmetabolic difference related to MSI-H may act as early markersfor colon cancer. These observations and previous studies usingother techniques23,24 show that gene-specific promoter (hyper)-methylation and separation of the MSI- and MSS-pathway is anearly event in tumorgenesis of CRC.
Discrimination between Cancer, Adenoma and NormalMucosa. The validation model for prediction of cancer andnormal mucosa of 100% accuracy confirms previous resultswhich state that HR MAS analysis has a high sensitivity andspecificity for discrimination of cancer and normal tissue.14-16
Additionally, the specific metabolic differences (Figure 2c)between cancer and normal tissue were in compliance withthese studies. Increased levels of lactate and decreased levelsof glucose in cancer tissue (Figure 2c) indicates possiblemechanisms such as increased glycolytic flux due to hypoxiaand ischemia in the tumor area,25 or the Warburg effect wherean increased uptake of glucose and conversion to lactate is seenin tumor cells even in high oxygen conditions.26 Higher levelsof the amino acid glycine found in this study can also beexplained by glycolytic variation due to transformation fromthe glycolytic intermediate 3-phosphoglycerate in CRC speci-mens, as suggested by Chan et al.14 However, sarcosine whichis a N-methyl derivate of glycine, is recently identified by massspectrometry as a differential metabolite that is highly increasedduring prostate cancer progression to metastasis, and whichcan be detected in urine.27 This pathway could be worthinvestigating also in colon cancer.
The choline-containing compounds (ChoCC) PC and freecholine are important constituents in cell membranes, andseveral MR studies of different organs have confirmed elevatedlevels of these metabolites in malignant tumors.28 Increasedlevels of PC and free choline were also found in colon cancerspecimens compared to samples from normal tissue in thepresent study. A previous study by Nakagami et al. showed thatthe choline kinase activity is increased in colon cancer tissuewith following elevation of PC,29 and they suggested thatcholine kinase may play a role in growth promotion or signaltransduction in carcinogenesis. Increased levels of PC are alsoobserved previously in CRC tissue.14 Interestingly, GPC (amembrane breakdown product) was decreased in the coloncancer samples compared to normal samples in this study, andthis is to our knowledge not previously documented in MRstudies on human colon cancer tissue. It is stated that the
Figure 3. (a) PLSDA score plot of LV1 and LV2 (explaining 41%x-variance and 44% y-variance) shows separation of metabolicprofiles from patients with MSI-H (n ) 35) from MSS (n ) 28) inLV2. (b) LV2 loadings plot (explaining 13% x-variance and 21%y-variance) shows metabolic alteration in several metabolites ofMSI-H samples compared to MSS samples.
research articles Tessem et al.
3668 Journal of Proteome Research • Vol. 9, No. 7, 2010

normal human gastrointestinal (GI) tract have relatively highlevels of phospholipid intermediates,30 and cancer may disturbthe highly efficient normal cell proliferation in the colonmucosa. Lower levels of GPC were however observed inbiopsies from patients with active Ulcerative Colitis comparedto normal controls,31 and Wang et al. have observed decreasedGPC levels in the human colon compared to the small bowel.30
The latter study shows that accuracy in location of the GI tractis important when considering GPC levels.30 Other metabolitessuch as lactate, myo-inositol, scyllo-inositiol and taurine arealso found to differ along the GI tract.30 However, since onlytissue from colon is included in this study, the issue on locationalong the GI tract can not be assessed.
Due to hypertonic conditions during digestion of food in theGI tract, osmotic regulation is important for balancing osmoticequilibrium between cells and the surrounding medium. Thisis achieved through maintaining a high intracellular contentof osmolytes such as myo-inositol, scyllo-inositol and taurine.30,32
Normal colon mucosa have been documented to be rich inosmolytes such as myo-inositol and scyllo-inositol,30 which areimportant for regulating long-term hypo-osmotic/hyper-osmotic stress.33 In this study, we detected a decrease in bothmyo-inositol and scyllo-inositol in colon cancer tissue com-pared to normal tissue. This phenomenon is also described bythe previous CRC MR studies;14-16 however, myo-inositol wasnot presented in the study by Chan et al.14 Taurine is anothercommonly found osmolyte, important for short-term hypo-osmotic stress.33 In the present study, taurine was increasedin the colon cancer mucosa, which is previously described inMR studies.14-16,34 The observed osmolyte changes in coloncancer tissue (decreased levels of inositols and increased levelsof taurine) may indicate imbalance in osmolyte function incancer cells.30 Taurine has many functions but has also beenimplicated in the mechanism of cell shrinkage during apoptosisand may therefore be a potential marker of apoptosis, whichis also found in human gliomas.35
Adenomas (adenomatous polyps) can be precancerous le-sions in the colon mucosa,36 and are therefore interesting forstudying precancerous conditions. This study included onlyfour adenomas, but the results show distinct differences in themetabolic profile compared to both cancer and normal mu-cosa, especially in the PC and GPC levels (plot not shown). Thefour adenomas are also observed with a large dispersion in thescore plot. The results have to be confirmed with a largeramount of samples. The metabolic difference can be associatedwith different grades of dysplasia or the presence of infiltratinggrowth of a mucosal lesion. The metabolic difference observedin adenomas may be important information for the individualpatient when accessing the risk of cancer development.
This study aimed to correlate colon HR MAS spectra toclinical parameters such as age, anatomical site, differentiation,gender, Dukes stage and lymph node status. No correlationswere detected except to age (Table 2). Due to a low number ofyounger cancer patients (6 of 31 patients were below 60 years),a study including a higher number of CRC patients of differentage groups will be necessary to assess whether metabolicdifferences are age dependent.
Discrimination between MSI-H and MSS. The validationmodel for prediction of MSI-H and MSS samples of 80%accuracy (sensitivity and specificity of 79% and 82%, respec-tively) indicates an evident difference between the MR spectraof these tissues. A difference between MSI-H and MSS ishowever not found when testing only the cancer samples, but
the correlation in this study was detected among the normalsamples (Table 2). This absence of correlation in cancer maybe caused by extreme metabolic conditions in the tumormicroenvironment due to mechanisms such as hypoxia andhigh proliferation rates. There is also evidence that hypo-methylation occurs in cancer tissue and that the epigeneticalterations, not the genetic alterations, occur in normal tissue.37
Ramirez et al. observed an increase in methylation of promoterMLH1 in normal colon mucosa.38 This supports the phenom-enom that associations found in neighboring mucosal tissuesis not found in tumor tissue. MLH1 methylation has previouslybeen classified as Type C methylation (cancer-specific), whichis in contrast to our results on metabolic profiles and to priorstudies on methylation.38,39 Metabolic alterations found innormal mucosal HR MAS spectra may describe an early stateof cancer development that may occur prior to genetic alter-ations. These metabolic differences detected in normal cellswithout cancer phenotype may serve as early biomarkers forcancer development and progression. Histopathology after HRMAS confirmed that there was no cancer invasion in thesenormal tissue samples.
Although the separation between MSI-H and MSS samplesin the score plot (Figure 3a) is not completely separated, it ispossible to point out specific metabolites responsible for theseparation (Figure 3b). The MSI-H tissue samples were char-acterized by increased relative concentrations in the majorityof the metabolites; lactate, glycine, taurine, creatine, PC andfree choline. GPC, myo-inositol and glucose were lower in theMSI-H samples compared to MSS. Comparing the loadingprofile obtained by the PLSDA of cancer and normal samples(Figure 2c), the MSI-H samples were separated from MSSsamples on the same metabolic basis as cancer is separatedfrom normal. This indicates that normal samples that have aneighboring tumor with the promoter MLH1 methylationcausing MSI-H have the same metabolic changes observed inhistopathologically confirmed cancer samples. These metabolicchanges detected in histopathologically confirmed normaltissue is very interesting regarding new biomarkers for cancerdevelopment and potentially in patient prognostics.
In conclusion, considering the fast and cost-effective HR MASanalysis on intact tissue, the metabolic picture in normal neigh-boring mucosa may be an important additional analysis inimproving clinical diagnosis and characterization of colon cancer.HR MAS analysis of normal adjacent mucosal tissue may providean indication of early development of colon cancer.
Acknowledgment. We acknowledge Elin SynnøveRøyset (St. Olav University Hospital, Trondheim) for per-forming the histopatholocial readings and Dr. Hans H.Wasmuth (St. Olav University Hospital, Trondheim) for identi-fying CRC-patients, obtaining written informed consents andcollecting tissue samples. This work was supported by theMedical Technology program at Norwegian University ofScience and Technology, the Department of GastrointestinalSurgery at St. Olavs Hospital, Trondheim, and Hamar Hospital,Innlandet Hospital Trust.
References(1) Jemal, A.; Siegel, R.; Ward, E.; Hao, Y.; Xu, J.; Thun, M. J. Cancer
statistics, 2009. CA Cancer J. Clin. 2009, 59 (4), 225–49.(2) Cancer in Norway 2008. Cancer registry of Norway; http://
www.kreftregisteret.no, 2009.(3) Soreide, K.; Janssen, E. A.; Soiland, H.; Korner, H.; Baak, J. P.
Microsatellite instability in colorectal cancer. Br. J. Surg. 2006, 93(4), 395–406.
Discrimination of Patients with MSI Colon Cancer research articles
Journal of Proteome Research • Vol. 9, No. 7, 2010 3669
(4) Boland, C. R.; Thibodeau, S. N.; Hamilton, S. R.; Sidransky, D.;Eshleman, J. R.; Burt, R. W.; Meltzer, S. J.; Rodriguez-Bigas, M. A.;Fodde, R.; Ranzani, G. N.; Srivastava, S. A National Cancer InstituteWorkshop on Microsatellite Instability for cancer detection andfamilial predisposition: development of international criteria forthe determination of microsatellite instability in colorectal cancer.Cancer Res. 1998, 58 (22), 5248–57.
(5) Popat, S.; Hubner, R.; Houlston, R. S. Systematic review ofmicrosatellite instability and colorectal cancer prognosis. J. Clin.Oncol. 2005, 23 (3), 609–18.
(6) Ribic, C. M.; Sargent, D. J.; Moore, M. J.; Thibodeau, S. N.; French,A. J.; Goldberg, R. M.; Hamilton, S. R.; Laurent-Puig, P.; Gryfe, R.;Shepherd, L. E.; Tu, D.; Redston, M.; Gallinger, S. Tumor micro-satellite-instability status as a predictor of benefit from fluorou-racil-based adjuvant chemotherapy for colon cancer. N. Engl.J. Med. 2003, 349 (3), 247–57.
(7) Des Guetz, G.; Schischmanoff, O.; Nicolas, P.; Perret, G. Y.; Morere,J. F.; Uzzan, B. Does microsatellite instability predict the efficacyof adjuvant chemotherapy in colorectal cancer? A systematicreview with meta-analysis. Eur. J. Cancer 2009, 45 (10), 1890–6.
(8) Des Guetz, G.; Uzzan, B.; Nicolas, P.; Schischmanoff, O.; Morere,J. F. Microsatellite instability: a predictive marker in metastaticcolorectal cancer. Target Oncol. 2009, 4 (1), 57–62.
(9) Kuismanen, S. A.; Holmberg, M. T.; Salovaara, R.; de la Chapelle,A.; Peltomaki, P. Genetic and epigenetic modification of MLH1accounts for a major share of microsatellite-unstable colorectalcancers. Am. J. Pathol. 2000, 156 (5), 1773–9.
(10) Tessem, M. B.; Swanson, M. G.; Keshari, K. R.; Albers, M. J.; Joun,D.; Tabatabai, Z. L.; Simko, J. P.; Shinohara, K.; Nelson, S. J.;Vigneron, D. B.; Gribbestad, I. S.; Kurhanewicz, J. Evaluation oflactate and alanine as metabolic biomarkers of prostate cancerusing 1H HR-MAS spectroscopy of biopsy tissues. Magn. Reson.Med. 2008, 60 (3), 510–6.
(11) Bathen, T. F.; Jensen, L. R.; Sitter, B.; Fjosne, H. E.; Halgunset, J.;Axelson, D. E.; Gribbestad, I. S.; Lundgren, S. MR-determinedmetabolic phenotype of breast cancer in prediction of lymphaticspread, grade, and hormone status. Breast Cancer Res. Treat. 2007,104 (2), 181–9.
(12) Sjobakk, T. E.; Johansen, R.; Bathen, T. F.; Sonnewald, U.; Juul,R.; Torp, S. H.; Lundgren, S.; Gribbestad, I. S. Characterization ofbrain metastases using high-resolution magic angle spinning MRS.NMR Biomed. 2008, 21 (2), 175–85.
(13) Giskeodegard, G. F.; Grinde, M. T.; Sitter, B.; Axelson, D. E.;Lundgren, S.; Fjosne, H. E.; Dahl, S.; Gribbestad, I. S.; Bathen,T. F. Multivariate Modeling and Prediction of Breast CancerPrognostic Factors Using MR Metabolomics. J. Proteome Res.2010, 9 (2), 972–9.
(14) Chan, E. C.; Koh, P. K.; Mal, M.; Cheah, P. Y.; Eu, K. W.; Backshall,A.; Cavill, R.; Nicholson, J. K.; Keun, H. C. Metabolic profiling ofhuman colorectal cancer using high-resolution magic angle spin-ning nuclear magnetic resonance (HR-MAS NMR) spectroscopyand gas chromatography mass spectrometry (GC/MS). J. ProteomeRes. 2009, 8 (1), 352–61.
(15) Righi, V.; Durante, C.; Cocchi, M.; Calabrese, C.; Di Febo, G.; Lecce,F.; Pisi, A.; Tugnoli, V.; Mucci, A.; Schenetti, L. Discrimination ofhealthy and neoplastic human colon tissues by ex vivo HR-MASNMR spectroscopy and chemometric analyses. J. Proteome Res.2009, 8 (4), 1859–69.
(16) Piotto, M.; Moussallieh, F. M.; Dillmann, B.; Imperiale, A.; Neuville,A.; Brigand, C.; Bellocq, J. P.; Elbayed, K.; Namer, I. Metaboliccharacterization of primary human colorectal cancers using highresolution magic angle spinning 1H magnetic resonance spec-troscopy. Metabolomics 2009, 5 (3), 292–301.
(17) Seierstad, T.; Roe, K.; Sitter, B.; Halgunset, J.; Flatmark, K.; Ree,A. H.; Olsen, D. R.; Gribbestad, I. S.; Bathen, T. F. Principalcomponent analysis for the comparison of metabolic profiles fromhuman rectal cancer biopsies and colorectal xenografts using high-resolution magic angle spinning 1H magnetic resonance spec-troscopy. Mol. Cancer 2008, 7, 33.
(18) Jordan, K. W.; Nordenstam, J.; Lauwers, G. Y.; Rothenberger, D. A.;Alavi, K.; Garwood, M.; Cheng, L. L. Metabolomic characterizationof human rectal adenocarcinoma with intact tissue magneticresonance spectroscopy. Dis. Colon Rectum 2009, 52 (3), 520–5.
(19) Trano, G.; Wasmuth, H. H.; Sjursen, W.; Hofsli, E.; Vatten, L. J.Awareness of heredity in colorectal cancer patients is insufficientamong clinicians: a Norwegian population-based study. ColorectalDis. 2009, 11 (5), 456–61.
(20) Meiboom, S.; Gill, D. Modified spin-echo method for measuringnuclear relaxation times. Rev. Sci. Instrum. 1958, 29, 688–691.
(21) Trano, G.; Sjursen, W.; Wasmuth, H. H.; Hofsli, E.; Vatten, L. J.Performance of clinical guidelines compared with moleculartumour screening methods in identifying possible Lynch syndromeamong colorectal cancer patients: a Norwegian population-basedstudy. Br. J. Cancer 2010, 102 (3), 482–8.
(22) Kennard, R. W.; Stone, L. A. Computer Aided Design of Experi-ments. Technometrics 1969, 11 (1), 137–148.
(23) Ahlquist, T.; Lind, G. E.; Costa, V. L.; Meling, G. I.; Vatn, M.; Hoff,G. S.; Rognum, T. O.; Skotheim, R. I.; Thiis-Evensen, E.; Lothe, R. A.Gene methylation profiles of normal mucosa, and benign andmalignant colorectal tumors identify early onset markers. Mol.Cancer 2008, 7, 94.
(24) Worthley, D. L.; Whitehall, V. L.; Buttenshaw, R. L.; Irahara, N.;Greco, S. A.; Ramsnes, I.; Mallitt, K. A.; Le Leu, R. K.; Winter, J.;Hu, Y.; Ogino, S.; Young, G. P.; Leggett, B. A. DNA methylationwithin the normal colorectal mucosa is associated with pathway-specific predisposition to cancer. Oncogene 2009, 29, 1653–62.
(25) Walenta, S.; Schroeder, T.; Mueller-Klieser, W. Lactate in solidmalignant tumors: potential basis of a metabolic classification inclinical oncology. Curr. Med. Chem. 2004, 11 (16), 2195–204.
(26) Warburg, O. On the origin of cancer cells. Science 1956, 123 (3191),309–14.
(27) Sreekumar, A.; Poisson, L. M.; Rajendiran, T. M.; Khan, A. P.; Cao,Q.; Yu, J.; Laxman, B.; Mehra, R.; Lonigro, R. J.; Li, Y.; Nyati, M. K.;Ahsan, A.; Kalyana-Sundaram, S.; Han, B.; Cao, X.; Byun, J.;Omenn, G. S.; Ghosh, D.; Pennathur, S.; Alexander, D. C.; Berger,A.; Shuster, J. R.; Wei, J. T.; Varambally, S.; Beecher, C.; Chinnaiyan,A. M. Metabolomic profiles delineate potential role for sarcosinein prostate cancer progression. Nature 2009, 457 (7231), 910–4.
(28) Glunde, K.; Ackerstaff, E.; Mori, N.; Jacobs, M. A.; Bhujwalla, Z. M.Choline phospholipid metabolism in cancer: consequences formolecular pharmaceutical interventions. Mol. Pharm. 2006, 3 (5),496–506.
(29) Nakagami, K.; Uchida, T.; Ohwada, S.; Koibuchi, Y.; Suda, Y.;Sekine, T.; Morishita, Y. Increased choline kinase activity andelevated phosphocholine levels in human colon cancer. Jpn. J.Cancer Res. 1999, 90 (4), 419–24.
(30) Wang, Y.; Holmes, E.; Comelli, E. M.; Fotopoulos, G.; Dorta, G.;Tang, H.; Rantalainen, M. J.; Lindon, J. C.; Corthesy-Theulaz, I. E.;Fay, L. B.; Kochhar, S.; Nicholson, J. K. Topographical variation inmetabolic signatures of human gastrointestinal biopsies revealedby high-resolution magic-angle spinning 1H NMR spectroscopy.J. Proteome Res. 2007, 6 (10), 3944–51.
(31) Bjerrum, J. T.; Nielsen, O. H.; Hao, F.; Tang, H.; Nicholson, J. K.;Wang, Y.; Olsen, J. Metabonomics in ulcerative colitis: diagnostics,biomarker identification, and insight into the pathophysiology. J.Proteome Res. 2010, 9 (2), 954–62.
(32) Yancey, P. H.; Clark, M. E.; Hand, S. C.; Bowlus, R. D.; Somero,G. N. Living with water stress: evolution of osmolyte systems.Science 1982, 217 (4566), 1214–22.
(33) Flogel, U.; Niendorf, T.; Serkowa, N.; Brand, A.; Henke, J.; Leibfritz,D. Changes in organic solutes, volume, energy state, and metabo-lism associated with osmotic stress in a glial cell line: a multi-nuclear NMR study. Neurochem. Res. 1995, 20 (7), 793–802.
(34) Moreno, A.; Rey, M.; Montane, J. M.; Alonso, J.; Arus, C. 1H NMRspectroscopy of colon tumors and normal mucosal biopsies;elevated taurine levels and reduced polyethyleneglycol absorptionin tumors may have diagnostic significance. NMR Biomed. 1993,6 (2), 111–8.
(35) Opstad, K. S.; Bell, B. A.; Griffiths, J. R.; Howe, F. A. Taurine: apotential marker of apoptosis in gliomas. Br. J. Cancer 2009, 100(5), 789–94.
(36) Tanaka, T. Colorectal carcinogenesis: Review of human andexperimental animal studies. J. Carcinog. 2009, 8, 5.
(37) Suzuki, K.; Suzuki, I.; Leodolter, A.; Alonso, S.; Horiuchi, S.;Yamashita, K.; Perucho, M. Global DNA demethylation in gas-trointestinal cancer is age dependent and precedes genomicdamage. Cancer Cell 2006, 9 (3), 199–207.
(38) Ramirez, N.; Bandres, E.; Navarro, A.; Pons, A.; Jansa, S.; Moreno,I.; Martinez-Rodenas, F.; Zarate, R.; Bitarte, N.; Monzo, M.; Garcia-Foncillas, J. Epigenetic events in normal colonic mucosa sur-rounding colorectal cancer lesions. Eur. J. Cancer 2008, 44 (17),2689–95.
(39) Kawakami, K.; Ruszkiewicz, A.; Bennett, G.; Moore, J.; Grieu, F.;Watanabe, G.; Iacopetta, B. DNA hypermethylation in the normalcolonic mucosa of patients with colorectal cancer. Br. J. Cancer2006, 94 (4), 593–8.
PR100176G
research articles Tessem et al.
3670 Journal of Proteome Research • Vol. 9, No. 7, 2010