discourse in medical settings hauptseminar: talk at work dozent: prof. dr. jürgen beneke...
TRANSCRIPT

Discourse in Medical Settings
Hauptseminar: Talk at WorkDozent: Prof. Dr. Jürgen Beneke
Referentinnen: Anna Dopatka & Antje Göldner

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
“Disease may be a medical entity, but illness is a social phenomenon.” (Suchman, 1970)

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
Part I: Doctor - Patient

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
1.1 Social skills and social competence
• doctor‘s work consists of dealing with people
• as important as technical knowledge and skills are the social skills
→ understanding of the components of the social skills is necessary in order to anticipate and understand the possible sources of success and failure

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
• how to measure the success of a doctor?
→ The average level of health of his patients?
→ The recovery rate of his patients?
→ Judging by professional colleagues?
• what are the goals of a doctor?

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
Doctor’s social skills:
• practitioner must be able to communicate, to persuade and to generally deal with the patients
• social skills have to vary with the situation and the patient
→ different age, sex, class and personality have to be handled differently
Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
1.2 Verbal and non-verbal communication:
Kinds of verbal utterance for a doctor:
• information
• talk in the doctor’s round or consultation
• patient’s medical history
• talk with relatives
• psychiatric / psychotherapeutic talk
• ......
→ all have different goals and priorities

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
Problems in a verbal communication (doctor- patient):
• technical language of medicine
→ dacryocystorhinostomy
“surgical fistulization of the lacrimal sac for external drainage of an obstructed nasolacrimal duct”
• patient’s lack of knowledge

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
Non- verbal signal accompanying speech:
three main roles:
• completing and elaborating on verbal utterance
• managing synchronising
• sending feedback signals
→ the role of reinforcement
→ the role of gaze
Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
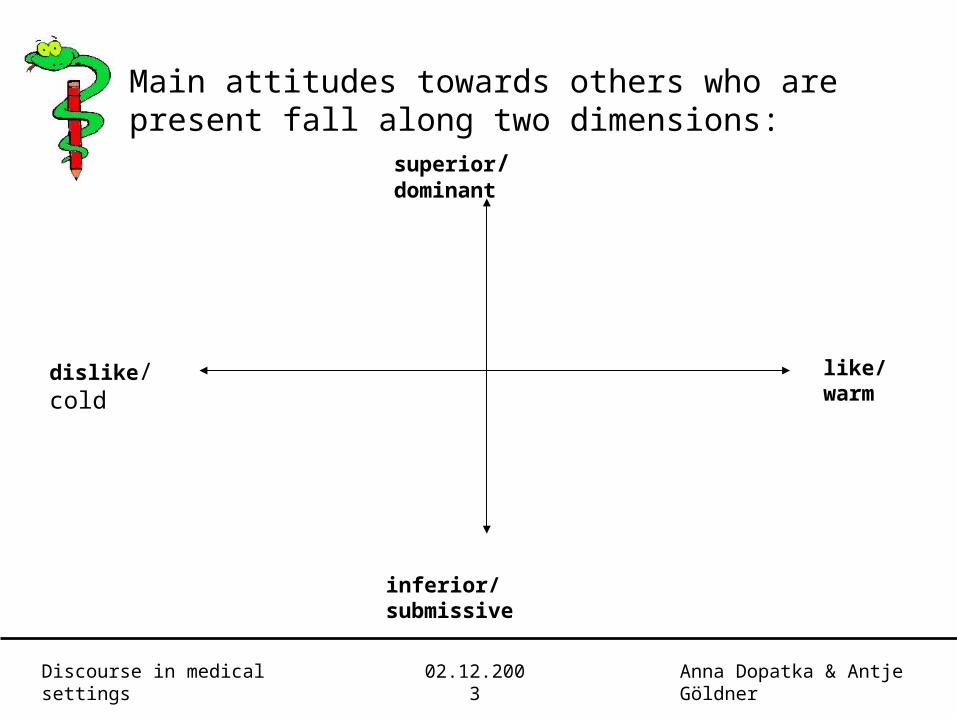
superior/ dominant
dislike/ cold
inferior/ submissive
like/ warm
Main attitudes towards others who are present fall along two dimensions:

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
1.3 Sequences of social interaction
• two- step sequences:
→ joke- laugh, complain- sympathise, request- comply or refuse
→ failure to make a pro- active move can stop a conversation:
A: Where do you come from?
B: Swindon.

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
• four- step sequences:
A (1)
B (1)
A (2)
B (2)
A: asks question
B: gives inadequate answer or does not answer
A: clarifies or repeats question
B: gives adequate answer

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
• episode sequence
→ six distinct phases of patients consultation (Byrne and Long, 1976)
1. relating to the patient
2. discussing the reason for the patients attendance
3. conducting a physical or verbal examination (or both)
4. considering of patient’s condition
5. Detailing treatment or further investigation
6. terminating

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
1.4 Main features of situations
• goals
→ social acceptance
→ food, drinks or other bodily needs
→ task goals specific to the situation
• rules
→ everyday rules
→ specific rules to situations

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
• special skills
→ many situations require special skills
• repertoire of elements
→ certain relevant moves defined by a situation
• roles
→ every situation has a limited number of roles. These roles carry a different degree of power

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
• cognitive structure
→ performers of professional social skills classify their clients in ways related to the task
• environmental setting and pieces
→ situations involve special environmental settings, although there is quite a lot of variation

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
Part II: Doctor’s Style

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
2.1 Reasons for adopting a style
• style is an amalgam of behaviours derived from personal beliefs, knowledge, experience and skilfulness
• Byrne and Long (1976) invented a scale ranging from doctor- centred to patient- centred behaviour

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
• traditional authoritarian approach based on the assumption that the doctor is responsible for his patient’s health and will go through his agenda for the patient
• opposite: doctor is seen as much less authoritarian, the responsibility for the health is shared, the patient is encouraged to go through his own agenda

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
“ Doctor’s experience is mostly based on skills, that makes it unsurprising that the pattern of behaviour tend to be disease- orientated and self- protectively authoritarian.”
(Peter Tate, 1983)

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
2.2 Flexibility of style
• studies of Byrne and Long (1976) and Bloor (1978) proved that if doctors have developed a set of behaviours, they use these stock pattern again and again
→ many of these behaviours are not significantly influenced by the patients presenting problems
• doctor- centred doctors remain in their categories for a wide variety of patients with only limited movements across the spectrum
→ patient- centred show more flexibility
Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
2.3 Style related to authority
• throughout history doctors have a “natural authority”
• Osmond (1980) divides medical authorities in three parts:
→ sapiental authority: doctor must have a greater technical knowledge
→ moral authority: the right to control - based on the doctor’s concern with the good of the patient
→ charismatic authority: medicine deals with powerful and mysterious forces (comes close to magic)

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
• the majority of doctors adopted the traditional style
→ also most expected style by patients (Fitten and Acheson, 1979)
• if patient- or doctor- centred, medical practice rests on an asymmetrical- relationship
→ doctor disposes of knowledge and technical skills
→ patient is unable to help himself, he is ignorant of the treatment of the disease

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
Two examples that influence doctor’s appearance and authority
1. seating position
the position in which the doctor sits in relation to the patient profoundly influences the mutual exchange
DA
C
B
Three seating positions at a desk (Pietroni, 1976)

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
Results:
• A - C six times more interaction than A - B
• A - C three times more interaction than A - D
• the absence of a desk reduces the perceived authority of the doctor
2. Dress
• clothes convey authority
→ casually dressed doctors are likely to be seen as a much less authoritarian figure than the one wearing a white coat

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
2.4 Information gathering and giving
• information gathering
→ normally first phase of any consultation
opening statements often dictate the path that the remainder of the consultation follows
→ different ways of opening
→ doctor has to “get” the patient to talk problem: clinical check-lists, organisation of vague symptoms into categories

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
• information giving
→ giving information includes explaining, sharing, advising, clarifying and dealing with questions and ideas
→ problems: technical language (cryptic information), patients dissatisfaction, doctor’s under- estimation of patient’s knowledge of illness, time

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
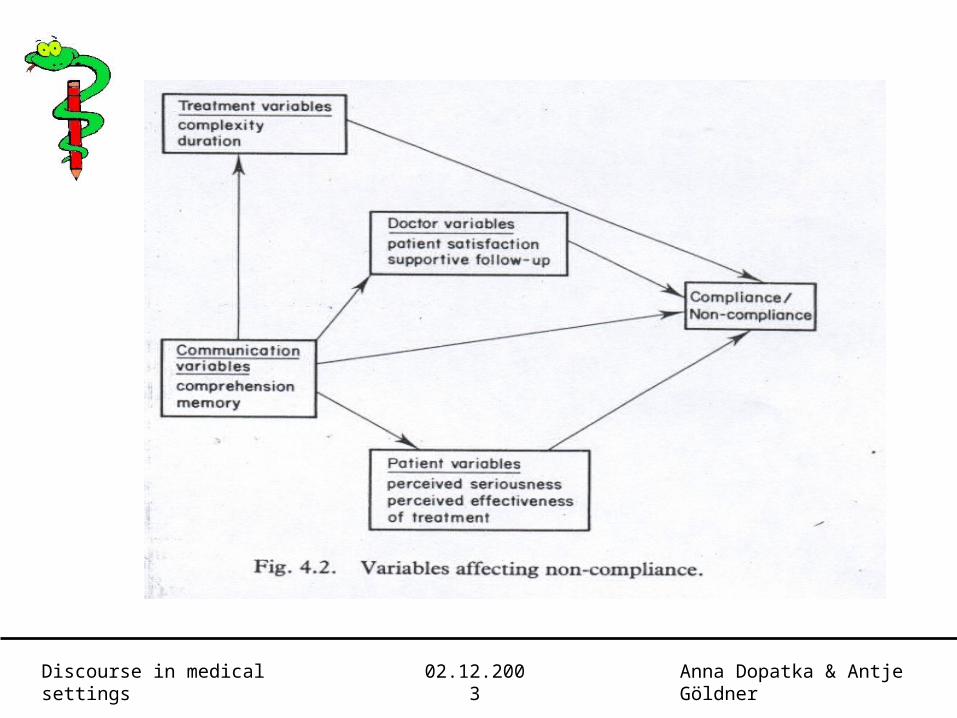
Part III: Patient’s understanding and compliance/ non- compliance with advice

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
Enduring problems in the field of health care:
• presenting information about patient’s illness in a satisfying way
• patients’ non- compliance with advice from health professionals
• dissatisfaction with doctor- patient communications is common

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
• patients wish for:
→ clear information on the effectiveness and risks of various possible treatments
→ decision by the patient to try one or none of the treatments
→ if the patient decides to pursue a given treatment, there should be regular opportunities to withdraw from the treatment
Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
Part IV: The consultation
Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
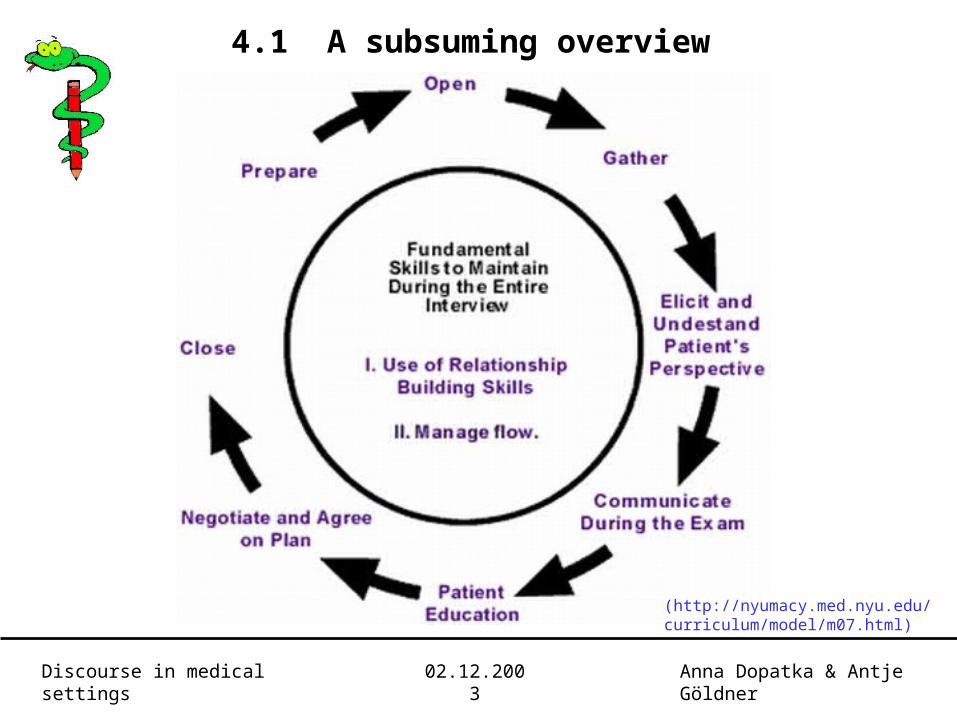
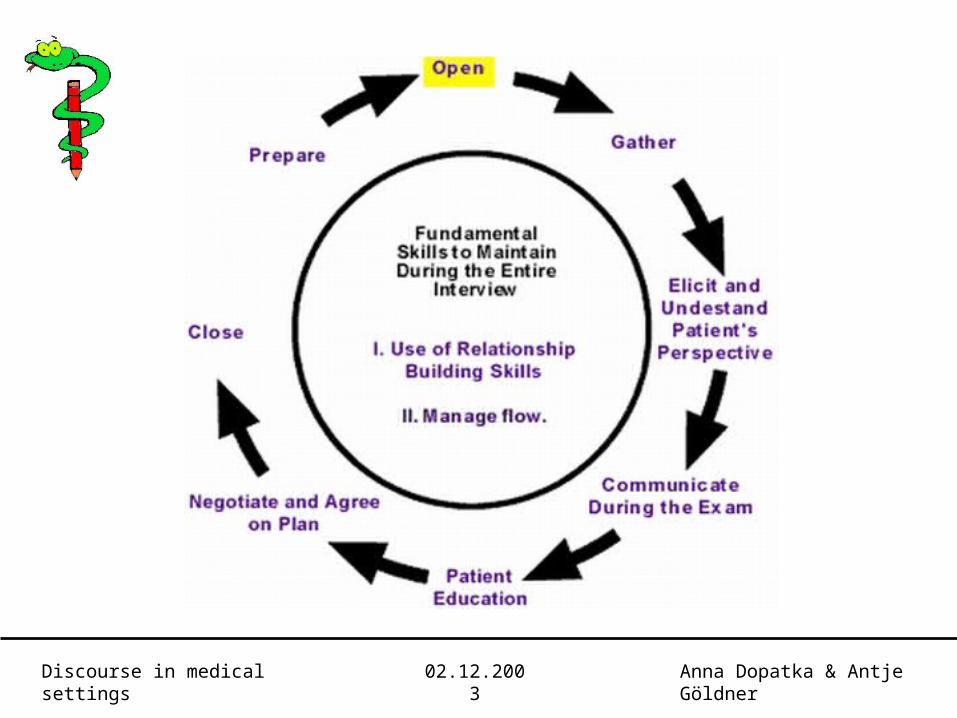
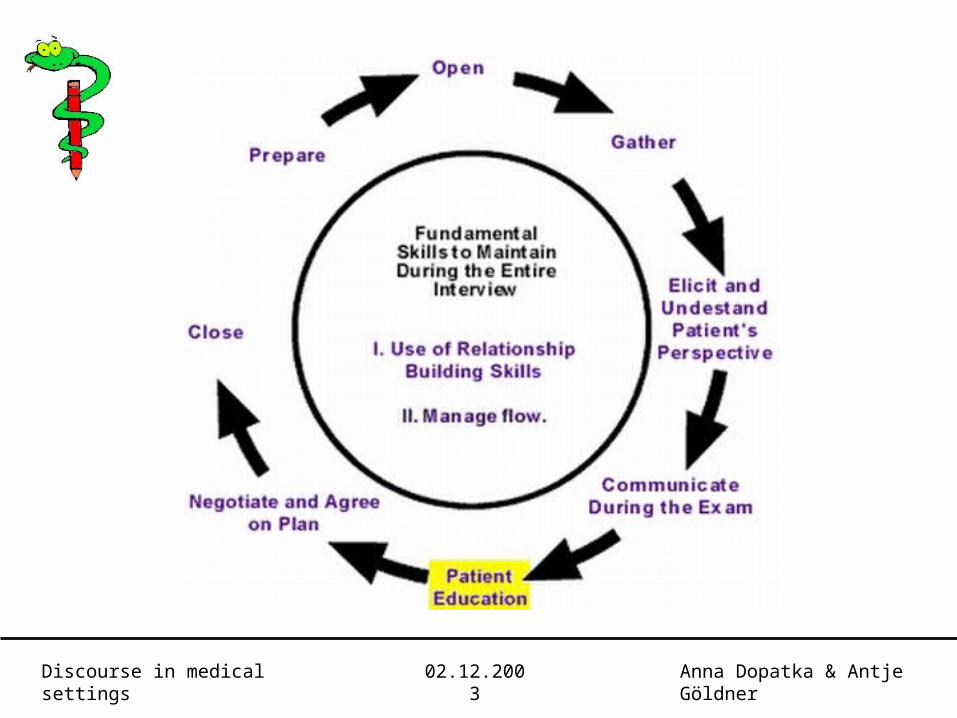
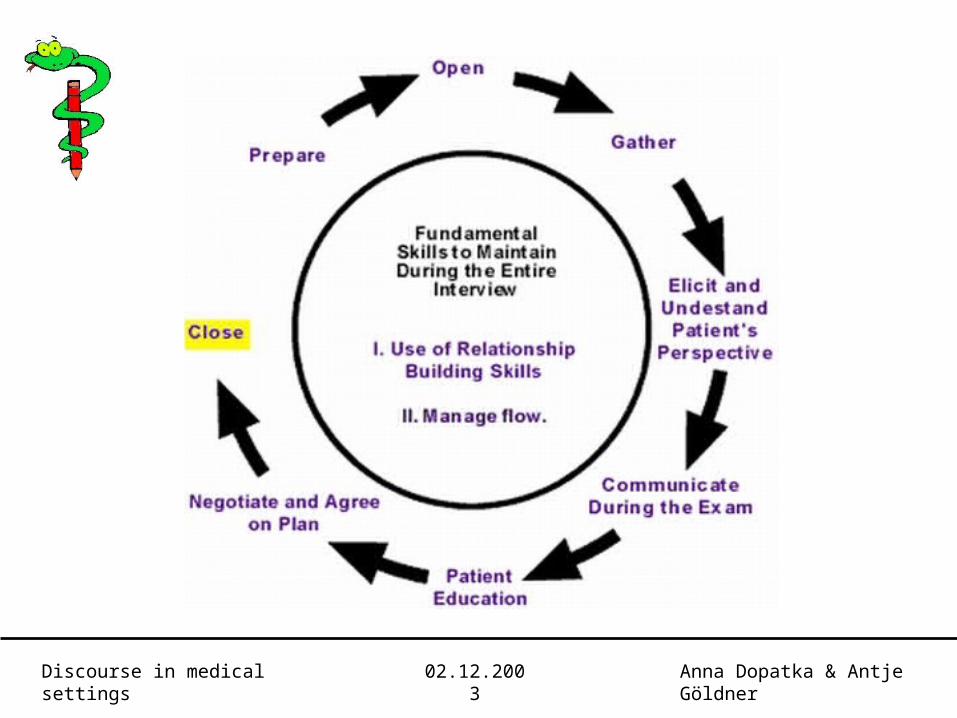
4.1 A subsuming overview
(http://nyumacy.med.nyu.edu/curriculum/model/m07.html)

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
4.2 Difficulties reported by doctors
• difficulties experienced by doctors in communicating to the patient
• difficulties in the communication from the patient→ more problems

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
• problems 1st category
→ mostly in the field of persuasive communication→ e.g. doctor is unable to influence the patient, explaining that there is (or is not) any problem
• reasons
→ patient has no confidence→ “ did not seem to understand the doctor→ “ and doctor are at cross purposes

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
• problems 2nd category
→ mostly about the “channel” and the “noise” that occurs in the information transmission
• reasons
→ patient communicates very little or not at all→ patient withholds information, sometimes deliberately→ patient uses a different “code”

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
Conclusion
• three types of basic problems
→ cognitive
→ emotional
→ social
“Emotional interference with the information transformationby the patient to the doctor and the social class of the patientdiscriminate best between consultations with and withoutcommunication problems.” (Jaspars, King, Pendleton. 1983)

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
4.3 The patients’ view on good and bad consultations
• 6 major categories
→ attention paid by the doctor
→ the doctor’s interpretation of the information
→ acceptance of the information
→ remarks about medical examination
→ observation related to the diagnosis
→ comments about medical treatment

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
• good consultation
→ treatment is effective / reassuring
→ patient is accepted as a person
→ prompt attention to the complaint
→ doctor shows understanding
→ quick and efficient examination
→ explanation of the diagnosis

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
• bad consultation
→ no attention
→ doctor did not treat patient as a person
→ prescription of wrong treatment
→ no understanding
→ wrong diagnosis
→ no explanation

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
4.4 The psychological effect of medical treatment
• psychological effect of communication from doctor
to patient
→ outcome of specific social influence process
→ doctor (“the source”) tries to affect a patient’s (“the receiver’s”) concern about his illness

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
• assessment depends on general parameters
→ attitude advocated by the doctor as
perceived by the patient
→ weight of the “source” for a particular
attitude of the “receiver”
o → weight of the “receiver’s” initial attitude
o → change in attitude of the patient
general model to predict the effectiveness of the
persuasive communication of the doctor

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
Results:
• less change in concern of the patient the more “source”
and “receiver” talk to each other
• seriousness and psychological nature of complaint
increase total amount of communication
• especially one form of behaviour has significant
influence on the effectiveness of communication
→ the more questions the doctor asks, the more
change in the patient’s concern can be remarked

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
Part V: Diagnosis and Treatment

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
5.1 The purposes of medical care
The purpose of medical care is to foster health
• “Health is a state of complete physical, mental and social
well-being, not merely the absence of disease or infirmity”
(World Health Organisation)
Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
• “Health is a satisfactory adaptation of the
individual to his total environment – physical,
psychological and socio-cultural”
(Royal College of General Practitioners)

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
• General practitioners have mostly 3 types of
opportunities to foster health
→ First contact care
→ Continuing care
→ Preventive care

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
5.2 Characteristics of general practice
• undifferentiated illness, early symptomatic diagnosis
• organisation of illness
• low-technology discipline
• person-centred approach
• awareness of compliance / non-compliance

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
• continuing care
• preventive attitude
• responsibility to community
• knowledge of different disciplines
• high skills in conducting interviews

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
5.3 Effects on communication and the doctor – patient
relationship
• 3 important purposes of communication
→ informative
→ promotive
→ evocative

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
Example
• A patient:
→ uncertainty about the extend to which he wishes to impart information
→ ability to encourage actions by the doctor
→ right to produce feelings

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
• A doctor:
→ must respect the uncertainties
→ is not obligated to accept limitation given to him
→ has the purpose to help the patient to be
rather adaptive than maladaptive

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
Conclusion:
• doctor-patient relationship is part of the communication
→ feedback during consultation
→ emotional environment is effected by doctor’s
attention and reaction to feedback
quality of relationship is part of the communication

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
5.3 The relationship as treatment for anxiety
• almost as many possible causes for anxiety as
psychological theories to describe its origins
• in this case:
→ search for source of the symptom within the
framework of stress, caused by conflicts
arising from incompatible goals

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
• types of conflict:
→ approach – approach conflict
→ avoidance – avoidance conflict
• resolution:
→ decision
• the doctor’s task:
→ construction of a suitable doctor – patient
relationship

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
• risk:
→ treatment by placebo
→ symptom – removal
• better:
→ attempt removal of cause

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner
• Important:
→ Defence mechanisms in the patient are
always involved in producing both, the
anxiety and the conflict
The doctor – patient relationship is the
environment and the instrument for
uncovering these defence mechanisms
at the same time

Discourse in medical settings 02.12.2003 Anna Dopatka & Antje Göldner

Thank you very much for your attention!