discog, università di padova istituto oncologico veneto … · primary systemic therapy in breast...
TRANSCRIPT

Valentina GuarneriDiSCOG, Università di Padova
Istituto Oncologico Veneto IRCCS

J Clin Oncol. 2014 Apr 1;32(10):1050-7.

Primary systemic therapy in breast cancer
• Tumor biology, rather than stage, is the driver of treatment selection
• Most patients with HR+/HER2- disease are offered adjuvant hormonal
therapy alone, even in case of node + disease
• In the tamoxifen era, neoadjuvant hormonal therapy has been
traditionally limited to elderly, unfit patients with large, inoperable
disease
• Aromatase inhibitors have opened new options

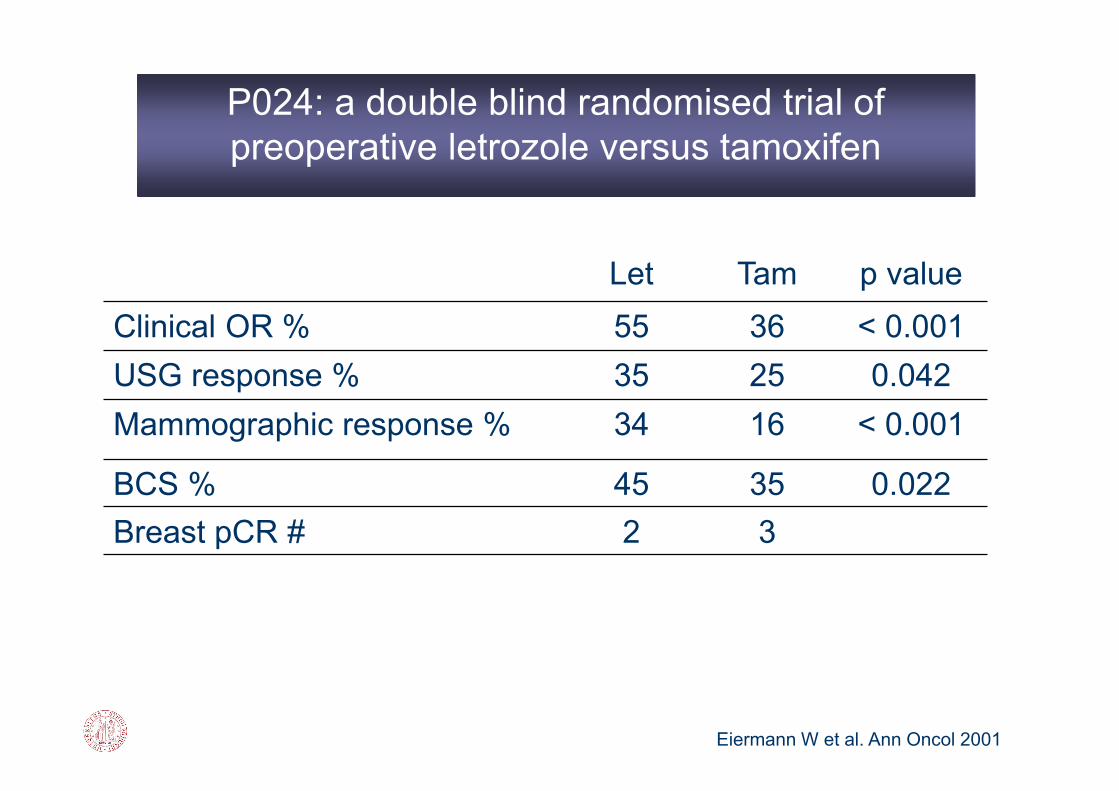
Let Tam p value
Clinical OR % 55 36 < 0.001
USG response % 35 25 0.042
Mammographic response % 34 16 < 0.001
BCS % 45 35 0.022
Breast pCR # 2 3
Eiermann W et al. Ann Oncol 2001
P024: a double blind randomised trial of
preoperative letrozole versus tamoxifen

A T A+T
Clinical OR % 37 36 39
USG response % 24 20 28
Improvement in BCS % 46* 22 26
* p 0.03
Smith IE et al , JCO 2005
IMPACT Trial: results

Neoadjuvant endocrine therapy vs CT in
postmenopausal women with HR+ BC
Doxo60+TXL200 q3w X 4 (118 pts)
ET for 3 mos (121 pts) Exemestane or Anastrozole
R Surgery
ChemoRx Endocrine Rx
Clinical OR % 63.6 64.5
USG response % 46 40
Mammography % 63 60
BCS % 24 33
pCR % 6 3
LRF at 3y % 2.3 3.3
Semiglazov VF, Cancer 2007

Alba et al, Ann Oncol 2012
CT arm HT arm p-value
ORR 66% 48% 0.075
BCS 47% 56% 0.23
pCR 2% - 0.6
pN0 36% 29% 0.47
95 ER+/ PgR +/HER2- patients randomized to:
EC x 4 → Docetaxel 100 x 4
Exemestane x 24 weeks (+ goserelin if pre-menopausal)

The Mechanism of Endocrine Resistance
De novo
ER lossER loss
CoA/CoR expressionCoA/CoR expression
Acquired
Growth factor signaling
pathway activation:
PI3K/AKT/mTOR
MAPK/ERK
Growth factor signaling
pathway activation:
PI3K/AKT/mTOR
MAPK/ERK
Tumor microenvironment
changes
Tumor microenvironment
changes
Image from Osborne CK, et al. Annu Rev Med. 2011;62:233-247.
Bianco S and Gévry N, Transcription. 2012;3(4):165-70; Zill M, et al. Biochim Biophys Acta. 2009;1795:62-81. 9
The mechanisms of Endocrine resistance

PI3K
AKT
PTEN
mTOR
RAS
RAF
MEK
MAPK
ER target gene transcription
P P
EGFRHER2
E
E
ER
E
ER
E
ER
E
TKI
Aromatase InhibitorNonsteroidal AIs
Anastrozole Letrozole
Steroidal AIsExemestane
Aromatase InhibitorNonsteroidal AIs
Anastrozole Letrozole
Steroidal AIsExemestane
Selective Estrogen Receptor ModulatorsTamoxifen Toremifene
Selective Estrogen Receptor ModulatorsTamoxifen Toremifene
ER DownregulatorFulvestrant
ER DownregulatorFulvestrant
Cell
Cycle
Combining targeted and antiestrogen therapies
in HR positive BC
Combining targeted and antiestrogen therapies
in HR positive BC
EGFR/HER2 inhibitorsEGFR/HER2 inhibitors

• Blocks signaling through
ErbB1 and ErbB2 homodimers
and heterodimers
• Might also prevent signaling
through heterodimers between
these receptors and other
ErbB family members
• Potentially blocks multiple
ErbB signaling pathways
Downstream Signaling Cascade
1 + 1 2 + 2 1 + 2
Lapatinib: HER1-2 TKI

S
U
R
G
E
R
Y
R
Letrozole 2.5 mg daily for 6 months
Sample size: 91 pts
HR+/HER2 -,
postmenopausal
operable BC
(Stage II-IIIA)Lapatinib 1500 mg daily for 6 months
Letrozole 2.5 mg daily for 6 months
Placebo daily for 6 months
♥ ♥ ♥
Study Design

Study Aims
Primary Aim
• Rate of breast clinical objective responses (cOR) (completeplus partial, measured by USG)
Secondary Aims
• Breast and axillary pCR rate
• Rate of breast conservative surgery and conversion from
mastectomy to BCS
• Safety profile
• Biomarkers analyses
• Gene expression profiling
• Time to treatment failure from start of primary therapy

Key inclusion criteria
• Previously untreated, infiltrating primary breast cancer of
more than 2.0 cm in largest clinical diameter
• Estrogen and/or progesterone receptor positivity (10% of
positive cancer cells by immunohistochemistry)
• HER2 negativity
• ECOG PS 0-1
• Normal LVEF
• Normal organ and marrow function
• Written informed consent

Enrollment
0
5
10
15
20
25
30
35
40
Cremona Modena Carpi Piacenza ReggioEmilia
Rimini

Patient and tumor characteristics
Letrozole-Lapatinib
(Arm A) n= 43
Letrozole-placebo
(Arm B) n=49
n (%) n (%)
Median age, yrs (range) 70 (49-88) 70 (47-88)
ECOG PS 0 41 (95.35) 45 (91.8)
1
NA
2 (4.65)
0
3 (6.12)
1 (2)
Clinical stage: IIA 21 (48.8) 26 (53)
IIB 17 (39.5) 21 (42.9)
IIIA 5 (11.6) 2 (4.1)
Histology: Ductal 29 (67.4) 38 (77.6)
Lobular 8 (18.6) 7 (14.3)
Other/not specified 6 (14) 4 (8.12)
Histologic Grade: 1/2 17 (39.5) 19 (38.8)
3 13 (30.2) 19 (38.8)
NA 13 (30.2) 11 (22.4)
Mean ER expression (range) 89% (40-100) 90% (30-100)
Mean PgR expression (range) 56% (0-100) 52% (0-100)ER: Estrogen Receptor; PgR: Progesterone Receptor; NA: Not Available

Adverse Events (AEs) occurring in at least 10% of
the study population and AEs Grade 3 to 4
Letrozole-Lapatinib (n=43)
N (%)
Letrozole-placebo (n=49)
N (%)
AE description overall Grade 2 Grade 3 Grade 4 overallGrade
2
Grade
3
Grade
4
Skin disorders 25 (58.1) 10 (23.2) 4 (9.3) 1 (2.3) 3 (6.1) 1 (2.0) 0 0
Nail toxicity 5 (11.6) 1 (2.3) 2 (4.6) 0 0 0 0 0
Diarrhea 26 (60.5) 4 (9.3) 6 (13.9) 0 5 (10.2) 2 (4.1) 0 0
Increased
transaminases8 (18.6) 2 (4.6) 2 (4.6) 0 2 (4.1) 0 1 (2.0) 0
Increased GGT 3 (6.9) 0 2 (4.6) 0 0 0 0 0
Mucositis 7 (16.3) 5 (11.6) 0 0 1 (2.0) 0 0 0
Fatigue 7 (16.3) 1 (2.3) 1 (2.3) 0 6 (12.2) 1 (2.0) 0 0
Muscoloskeleta
l disorders6 (13.9) 1 (2.3) 1 (2.3) 0 9 (18.4) 3 (6.1) 0 0
Dispepsia 5 (11.6) 2 (4.6) 0 0 5 (10.2) 0 0 0
Nausea 2 (4.6) 0 0 0 6 (12.2) 0 0 0
Congestive
heart failure1 (2.3) 0 1 (2.3) 0 0 0 0 0

Response rate per treatment arm

Surgical outcomes
0
10
20
30
40
50
60
70Conversion from
mastectomy
BCS
ARM A Letrozole-Lapatinib ARM B Letrozole-placebo

Treatment effect on tumor biomarkers
Guarneri V, et al. J Clin Oncol 2014

Baselga J, The Oncologist 2011

Cancer Genome Atlas Network. Nature 2012, 490:61-70
PIK3 pathway deregulation in breast cancer

• The prognostic role of PIK3CA mutation in HR-positive BC
has been controversial
• PIK3CA mutations emerge as a non-independent prognostic
factor probably because of the positive association with HR
positivity and good prognostic features.
• In the TEAM study, PIK3CA mutated patients (39.8 %)
experienced a significant better 5-yr DDFS vs wild-type
patients (91 vs 88 %; HR 0.76 95 % CI 0.63–0.91, p=0.003)
• PIK3CA mutation did not maintain an independent prognostic effect in multivariate analysis
PIK3CA mutations in HR+ BC

Responses according to PIK3CA status in
the LET-LOB study
ORR 63% in WT vs 93% in PIK3CA
mutated tumors, p=0.037ORR 66% in WT vs 63% in PIK3CA
mutated tumors, p=0.79

Mean Ki67 suppression overall, by clinical
response and by PI3KCA status

Heatmap of differentially expressed genes

Conclusions
• The combination of letrozole-lapatinib in early breast cancer
was feasible, with expected and manageable toxicities.
• In unselected ER+/HER2- patients, letrozole-lapatinib and
letrozole-placebo resulted in a similar overall clinical response
rate
• A significant decrease in Ki67 and pAKT was observed in
both treatment arms.
• A significant correlation between PIK3CA mutation and
response to letrozole-lapatinib in hormone receptor
positive/HER2 negative early breast cancer was observed
• These data warrant independent confirmation