disclosures asphyxia - ucsf medical education · 10/28/2010 2 • perinatal asphyxia occurs 1-6 /...
TRANSCRIPT

10/28/2010
1
Therapeutic Cooling after Perinatal
Asphyxia
Therapeutic Cooling after Perinatal
Asphyxia
Thomas K. Shimotake, MD
Assistant Professor of Pediatrics
Co-Director, Neurointensive Care Nursery
Benioff Children’s Hospital
University of California San Francisco
Thomas K. Shimotake, MD
Assistant Professor of Pediatrics
Co-Director, Neurointensive Care Nursery
Benioff Children’s Hospital
University of California San Francisco
UCSF OB/Gyn Update: What Does the Evidence Tell Us? October 27-29, 2010
DisclosuresDisclosures
• I have no financial investments, conflicts
of interest or other disclosure.
• Full term, presenting in active labor
• Decreased fetal movement noted earlier in day
• FHRM: Non-reassuring fetal status
• Repetitive variables and late decelerations
• Emergent C-section
• Floppy, cyanotic, no respiratory effort
• HR<60 ->compression. Intubated 2’ apnea
• APGARs 1, 4, 5
• UA 6.9/-20; low initial blood glucose
Case presentation Case: seizure and Rx cooling effects
MRI (day 4) – b/l watershed injury & deep gray nuclei

10/28/2010
2
• Perinatal asphyxia occurs 1-6 / 2-6/1000 live births.
• Moderate to severe hypoxic ischemic encephalopathy (HIE) in 0.5-1/1000 live births. (Levene MI, Lancet 1986)
• HIE has 10-20% mortality (Dixon, 2002)
• 25-60% of survivors have long-term neurodevelopmental sequelae (Robertson, 1989).
• CP, MR, LD, Epilepsy
Defining the scope of the problem
Defining the scope of the problem
• In the US, intrauterine hypoxia and birth asphyxia is 10th leading cause of neonatal death.
• Worldwide estimates:� 4-9 million newborns suffer birth asphyxia/year. � 1.2 million deaths or ~23% of all neonatal death� 1.2 million severe disability.
World Health OrganizationLawn JE, et al, Neo Survival Steering Team. 4 Mil Neo Deaths: When? Where? Why?,
Lancet, 2005
Defining the scope of the problemDefining the scope of the problem
What’s in a name?What’s in a name?• Hypoxia
• Hypoxemia
• Ischemia
• Asphyxia
• Asphyxia neonatorum
• Birth asphyxia
• Intrapartum asphyxia
• Perinatal asphyxia
• Hypoxia
• Hypoxemia
• Ischemia
• Asphyxia
• Asphyxia neonatorum
• Birth asphyxia
• Intrapartum asphyxia
• Perinatal asphyxia
What’s in a name?What’s in a name?•• Hypoxic ischemic encephalopathy Hypoxic ischemic encephalopathy (HIE)
•• Perinatal depressionPerinatal depression
•• Neonatal encephalopathy Neonatal encephalopathy
• Describes CNS dysfunction in the newborn period from all causes, including HIE and BA(ACOG Opinion, No 326, December 2005: Inappropriate Use of the Terms Fetal Distress and Birth Asphyxia)
• Use of term birth asphyxia has declined(Wu YW, et. al, Declining diagnosis of birth asphyxia in CA:1991-2000, Pediatrics 2004)
Cooling targets neonatal brain injury from Cooling targets neonatal brain injury from discrete perinatal events (within hrs of birth).discrete perinatal events (within hrs of birth).

10/28/2010
3
Modified by the ACOG Task Force on Neonatal Encephalopathy and Cerebral Palsy from the template provided by the International CP Task Force, OBGyn 2005
1.1: Essential Criteria (must meet all four)
1.Evidence of metabolic acidosis (pH<7 and BD ≥12mmol/L) in cord UA blood obtained at delivery.
2.Early onset of moderate to severe neonatal encephalopathy (in infants >34wk GA).
3.Spastic quadriplegia or dyskinetic-tyoe cerebral palsy.
4.Exclusion of other identifiable causes (eg, trauma, coagulopathy, ID, genetic)
Criteria for acute intrapartum hypoxic event sufficient to cause cerebral palsy
Criteria for acute intrapartum hypoxic event sufficient to cause cerebral palsy
Criteria for acute intrapartum hypoxic event sufficient to cause cerebral palsy
Criteria for acute intrapartum hypoxic event sufficient to cause cerebral palsy
Modified by the ACOG Task Force on Neonatal Encephalopathy and Cerebral Palsy from the template provided by the International CP Task Force, OBGyn 2005
1.2: Non-specific but suggestive criteria in close proximity to L&D (e.g., 0-48 hrs)
1.Sentinel hypoxic/ischemic event immediately before/during labor.
2.Sudden/sustained fetal bradycardia or loss of FHR variability with persistent, late, or variable decels.
3.Apgars scores of 0-3 beyond 5 min
4.Onset of multisystem involvement within 72 hours (eg, kidney, liver, etc..)
5.Early imaging study showing evidence of acute nonfocal cerebral abnormalities.
• 8-10,000 babies/yr in the U.S.
• 1 in 3 very low BW infants
• Term babies with HIE more severely impaired
• Two-thirds children with CP mentally impaired
• One-third of children with CP have seizures
• Cost of care in US ~ $30 billion per annum
• 8-10,000 babies/yr in the U.S.
• 1 in 3 very low BW infants
• Term babies with HIE more severely impaired
• Two-thirds children with CP mentally impaired
• One-third of children with CP have seizures
• Cost of care in US ~ $30 billion per annum
Background:Cerebral PalsyBackground:Cerebral Palsy
Centers for Disease Control and PreventionNational Institute of Neurologic Disease and StrokeMarch of Dimes Foundation
Cooling to the rescue?Cooling to the rescue?

10/28/2010
4
What’s going on here?What’s going on here?Latent period represents a therapeutic “window of
opportunity” between an asphyxia event and secondary
phase of impaired energy metabolism and injury.
Major variants of FT neonatal brain injuryMajor variants of FT neonatal brain injury
Primaryneuronal
death
Severeinsults
Primaryneuronal
death
Severeinsults
0 hrs hours 6 hrs …
Secondary Phase
Secondaryenergyfailure
Secondary Phase
Secondaryenergyfailure
Hyperemia Cytotoxic edema PAF in CSF Mitochondrial failureAccumulation of excitotoxins Active cell death (apoptosis)
Nitric oxide synthesis Free radical damage Activated microglia Extracell Glutamate NMDA receptor activation Intracelllular Ca++
Hyperemia Cytotoxic edema PAF in CSF Mitochondrial failureAccumulation of excitotoxins Active cell death (apoptosis)
Nitric oxide synthesis Free radical damage Activated microglia Extracell Glutamate NMDA receptor activation Intracelllular Ca++
Latent periodLatent period
“Biphasic nature of cell death”“Biphasic nature of cell death”(Gluckman PD, et al Dev Med&Child Neuro ’92)
Mechanisms of brain Mechanisms of brain injury in term neonatesinjury in term neonates
Ferriero, DM NEJM ‘04
Mechanisms of injury and Mechanisms of injury and repair unique to newborn brainrepair unique to newborn brain Animal Models Animal Models
• Animal models began to support potential benefit for mild-moderate hypothermia (33-34°C ~ 92-93°F) in neonates after birth asphyxia.
• Term and preterm animal models for hypothesis•Laptook AR, et al, Peds Research, 1994 – (Newborn piglets)
•Thoresen M, et al,, Peds Research, 1995 – (Newborn piglets)
•Thoresen M, et al., Arch Dis Children, 1996 – (Neonatal rats)
•Gunn AJ, et al, Peds Research, J Clin Invest 1997 – (Fetal sheep)

10/28/2010
5
Safety StudiesSafety Studies• Pilot studies confirmed safety of neonatal cooling.
•• Gunn AJ, et. al.Gunn AJ, et. al., Pediatrics 1998•• Azzopardi et. al Azzopardi et. al (TOBY), Pediatrics, 2000•• Thoresen M, et alThoresen M, et al., Pediatrics, 2000•• Shankaran S, et. al. Shankaran S, et. al. (NICHD), Pediatrics, 2002
• Adverse effects (in pilot trials) were transient and reversible.
• Sinus bradycardia• Increased blood pressure• Increased oxygen requirement
• Enrollment criteria for pilot studies were all similar.
Therapeutic Cooling TrialsTherapeutic Cooling Trials• Enrollment Criteria:
� >37wk GA� Need for resuscitation� Acidosis at birth (pH<7.0 or BE > -14)� Moderate-severe ncephalopathy (+/- aEEG/EEG evidence)
• Protocol:� Cooling (head vs body) to 33-34 °C � 48-72 hours� Continuous monitoring� Neuroimaging� Follow-up
• Now over 8 major RCT of neonatal cooling for BA.
Major RCT of Neonatal CoolingMajor RCT of Neonatal CoolingMajor RCT of Neonatal CoolingMajor RCT of Neonatal Cooling• 6 RCT of Cooling with 18-24 mo follow-up
– Cool Cap (Gluckman, et al, Lancet, 2005)
– NICHD (Shankaran, et al, NEJM, 2005)
– TOBY (Azzopardi, et al, NEJM, 2009)
– China Study Group (Zhou WH, et al, J Peds, 2010), n=194
– neo.nEURO.network (nnn) (Simbruner, et al, Pediatrics, 2010)
– ICE (*Jacobs, et al, ‘08) *Protocols and prelim data only
• Only two studies (NICHD & China Group#) showed significant reduction in primary outcome of death or disability at 18-24months.
Cooling Trials: Meta-analysesCooling Trials: Meta-analyses
• Schulzke, et al, BioMed Central (BMC) 2007
• Jacobs, et al, Cochrane Reviews 2007
• Edwards AD, et al, BMJ, Feb 2010
- Mortality data available from 10 RCT: n= 1320- 18 mo Follow-up data from 3 RCT: n=767
• Two pending trials w/ 18 mo f/u: n=221 (ICE) + n=129 (nnn)
10/28/2010
6
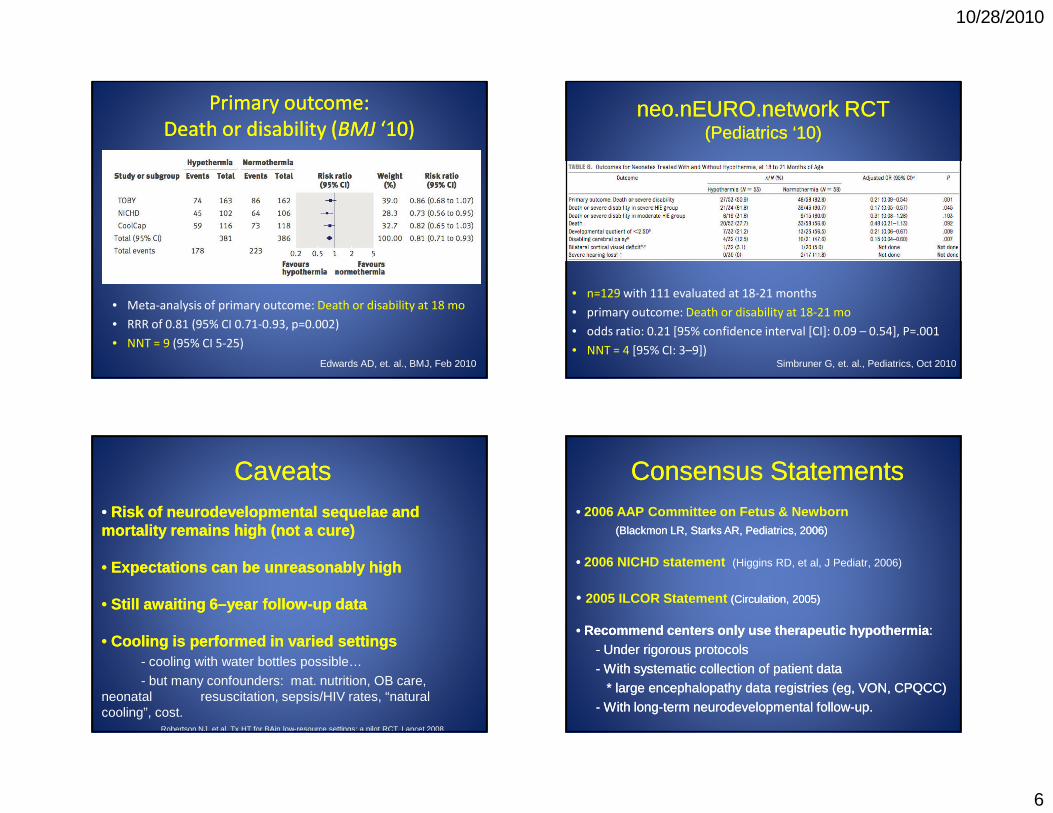
• Meta-analysis of primary outcome: Death or disability at 18 mo
• RRR of 0.81 (95% CI 0.71-0.93, p=0.002)
• NNT = 9 (95% CI 5-25)
Primary outcome:
Death or disability (BMJ ‘10)
Primary outcome:
Death or disability (BMJ ‘10)
Edwards AD, et. al., BMJ, Feb 2010
• n=129 with 111 evaluated at 18-21 months
• primary outcome: Death or disability at 18-21 mo
• odds ratio: 0.21 [95% confidence interval [CI]: 0.09 – 0.54], P=.001
• NNT = 4 [95% CI: 3–9])
neo.nEURO.network RCT(Pediatrics ‘10)
neo.nEURO.network RCT(Pediatrics ‘10)
Simbruner G, et. al., Pediatrics, Oct 2010
CaveatsCaveats•• Risk of neurodevelopmental sequelae and Risk of neurodevelopmental sequelae and mortality remains highmortality remains high (not a cure)(not a cure)
•• Expectations can be unreasonably highExpectations can be unreasonably high
•• Still awaiting 6Still awaiting 6––year followyear follow--up dataup data
•• Cooling is performed in varied settingsCooling is performed in varied settings- cooling with water bottles possible…
- but many confounders: mat. nutrition, OB care, neonatal resuscitation, sepsis/HIV rates, “natural cooling”, cost.
Robertson NJ, et al. Tx HT for BAin low-resource settings: a pilot RCT, Lancet 2008
Consensus StatementsConsensus Statements•• 2006 AAP Committee on Fetus & Newborn
(Blackmon LR, Starks AR, (Blackmon LR, Starks AR, Pediatrics,Pediatrics, 2006)2006)
•• 2006 NICHD statement (Higgins RD, et al, J Pediatr, 2006)
• 2005 ILCOR Statement ((CirculationCirculation, 2005), 2005)
•• Recommend centers only use therapeutic hypothermiaRecommend centers only use therapeutic hypothermia ::
-- Under rigorous protocols Under rigorous protocols
-- With systematic collection of patient dataWith systematic collection of patient data
* large encephalopathy data registries (eg, VON, CPQCC)* large encephalopathy data registries (eg, VON, CPQCC)
-- With longWith long--term neurodevelopmental followterm neurodevelopmental follow--up.up.

10/28/2010
7
‘08 Revised ILCOR Guidelines‘08 Revised ILCOR GuidelinesRecent review of 2005 ILCOR recommendation that cooling be used only after cardiac arrest but not after neonatal resuscitation.
With additional robust RCT data with a mean NNT between 6 and 8, now recommend therapeutic hypothermia be offered as routine clinical practice (standard of care).
Hoehn T, Hansmann G, Buhrer C, Simbruner G, Gunn AJ, Yager J, Levene M, Hamrick SE, Shankaran S, Thoresen M., Resuscitation, Jul 2008
Cooling programs in CaliforniaCooling programs in California
• 146 NICU's in California
• 14 Cooling Programs (as of October 31, 2009)– Loma Linda Univ Chlid. Hosp.(wbc) - Mattel Child. Hosp. at UCLA (CC)
– Child. Hosp. & Rsch. Ctr, Oakland (wbc) - Kaiser, Oakland (wbc)
– Child. Hosp. Orange County (CC) - UC Irvine (wbc)
– Lucille Packard CH/ Stanford (wbc) - UC Davis (wbc)
– UC San Diego (wbc) - Rady CH, San Diego (wbc)
– Sharp Mary Birch Hosp for Women (wbc) - Calif Pacific Med Ctr, SF (wbc)
– UCSF (wbc) - Santa Clara Valley MC, San Jose (wbc)
Compiled by Bhatt DR, Ramanathan R, Kahle R, and Durand D
• Contact information and protocols available on CAN website:
– http://www.canneo.org/
• 146 NICU's in California
• 14 Cooling Programs (as of October 31, 2009)– Loma Linda Univ Chlid. Hosp.(wbc) - Mattel Child. Hosp. at UCLA (CC)
– Child. Hosp. & Rsch. Ctr, Oakland (wbc) - Kaiser, Oakland (wbc)
– Child. Hosp. Orange County (CC) - UC Irvine (wbc)
– Lucille Packard CH/ Stanford (wbc) - UC Davis (wbc)
– UC San Diego (wbc) - Rady CH, San Diego (wbc)
– Sharp Mary Birch Hosp for Women (wbc) - Calif Pacific Med Ctr, SF (wbc)
– UCSF (wbc) - Santa Clara Valley MC, San Jose (wbc)
Compiled by Bhatt DR, Ramanathan R, Kahle R, and Durand D
• Contact information and protocols available on CAN website:
– http://www.canneo.org/
Newborn Brain Research Institute Newborn Brain Research Institute (NBRI)(NBRI)
Founded 2006 by Founded 2006 by David Rowitch & David Rowitch &
Donna Ferrerio underDonna Ferrerio underDean David Kessler Dean David Kessler
Newborn Brain Research Institute Newborn Brain Research Institute (NBRI)(NBRI)
Founded 2006 by Founded 2006 by David Rowitch & David Rowitch &
Donna Ferrerio underDonna Ferrerio underDean David Kessler Dean David Kessler
Neuro Intensive Care Nursery Neuro Intensive Care Nursery (NICN) Program(NICN) Program
Founded 2007Founded 2007• Nov ‘07 - First cooling patient
• Jul ’08 - Dedicated Peds Neuro• Neonatal Neurocritical Care Service (NNCS)Neonatal Neurocritical Care Service (NNCS)
Neuro Intensive Care Nursery Neuro Intensive Care Nursery (NICN) Program(NICN) Program
Founded 2007Founded 2007• Nov ‘07 - First cooling patient
• Jul ’08 - Dedicated Peds Neuro• Neonatal Neurocritical Care Service (NNCS)Neonatal Neurocritical Care Service (NNCS)
Protocols, Document Protocols, Document and Guidelinesand Guidelines
1. Cooling after birth asphyxia
• Inborn patients
• Outborn patients
• Transport protocol
2. Family Information sheet
3. Outreach/NCPeTS Tipsheet
4. Seizure management5. Neuro Exam checklist
6. Neuromonitoring guidelines

10/28/2010
8
pH<7.0 (1/1/06-1/1/08)• Cord UV = 7• Cord UA = 24
11/3,487 cord UA or UV gas
Entry CriteriaEntry Criteria(UCSF Cooling Protocol)(UCSF Cooling Protocol)
• Consider ASAP after concerning neo resuscitation
• Any staff member (MD, NNP, RN) may identify patients as candidates for cooling.
• Automatic “panic values ” may trigger evaluation. - UCSF Clinical Labs notify MD if cord/1st pt blood gas:
* pH: <7.0 <7.0 (cord gas) or <7.2 <7.2 (1st patient gas)* Base excess: < < --12 mmol/L12 mmol/L
• If any question, call a regional cooling center to discuss case (and document call).
Early Patient IdentificationEarly Patient Identification Clinical / Diagnostic grey zonesClinical / Diagnostic grey zones
• At risk babies with initial hypotonia can recover “good tone” – which exam counts?
• Encephalopathy may be evolving (“hyperalert state”).
• Severe acidosis on cord or first patient gas can recover with first/follow-up gas. – Is the 1st gas enough evidence of injury risk?– Is the rapid correction enough to reassure low risk?

10/28/2010
9
Cooling on transportCooling on transport
Fairchild K, et al., Therapeutic hypothermia on neonatal transport: 4-year experience in a single NICU., J Perinatol, 2010
Cool CapCool Cap®® SystemSystem
Whole Body Cooling SystemsWhole Body Cooling Systemse.g., CSZ Blanketrol III e.g., CSZ Blanketrol III ®®
Monitoring in the NICNMonitoring in the NICN• Vital Signs (HR, BP, RR, SaO2, TCO2, NIRS)
• Clinical lab tests, e.g.: * blood gas, glucose/electrolytes, lactate *
coag panel * liver/renal function labs
• Standard video EEG (72 hours + 24 hours)
• amplitude integrated EEG (aEEG) / CFM

10/28/2010
10
Amplitude-integrated EEG (aEEG)
Cerebral Function Monitor (CFM)
Amplitude-integrated EEG (aEEG)
Cerebral Function Monitor (CFM)
• Limited channel bedside
neuromonitor
• Easy to use
• Allows checking of:
– Background pattern
– Response to treatment
– Some seizure detection
• Full EEG still gold standard
• Limited channel bedside
neuromonitor
• Easy to use
• Allows checking of:
– Background pattern
– Response to treatment
– Some seizure detection
• Full EEG still gold standard
Toet MC and Lemmers P, Early Hum Dev, Feb 2009
Key considerationsKey considerations
• Core temperature monitoring − Turn off external heat sources ASAP − Begin passive cooling− Obtained initial blood gas and clinical details− Call regional cooling center
• Establish access− Umbilical lines (UVC/UAC) or PIV/RAL
• Provide adequate sedation (avoid shivering)− Continuous Morphine infusion or boluses
Key considerationsKey considerations• Medical management of co-morbitidies
− FEN (glucose, calcium, sodium/potassium)
− Respiratory* Hyperventilation/Hyperoxygenation* Meconium Aspiration Syndrome* Persistant Pulmonary Hypertension (PPHN)
− Cardiovascular* Bradycardia* Hypotension
− Hematologic* Coagulation disorders
− Infectious
Key considerationsKey considerations
• Neurological issues− Seizures (clinical vs. sub-clinical)
− Neuromonitoring
− Sedation
− Neuroimaging

10/28/2010
11
Neonatal seizures are common Neonatal seizures are common
• Neonatal Seizures are
common and often suggest
underlying brain injury or
dysfunction.
• Birth is most common time
of life to have seizures– 0.95/1000 term births in California
(OSWHPD database)
Glass HC, et al. Journal of Pediatrics, 2008
• Neonatal Seizures are
common and often suggest
underlying brain injury or
dysfunction.
• Birth is most common time
of life to have seizures– 0.95/1000 term births in California
(OSWHPD database)
Glass HC, et al. Journal of Pediatrics, 2008
Slide courtesy of HC Glass
Neonatal seizures are important Neonatal seizures are important
• Often indicate other brain injury or dysfunction,
only some of which may be amenable to cooling.
• Associated death or cerebral palsy – 16% death
– 39% impaired (mental retardation, cerebral palsy)
– EpilespyRonen, et al. Neurology, 2007
• Often indicate other brain injury or dysfunction,
only some of which may be amenable to cooling.
• Associated death or cerebral palsy – 16% death
– 39% impaired (mental retardation, cerebral palsy)
– EpilespyRonen, et al. Neurology, 2007
Assessing neonatal brain injury by MRI Assessing neonatal brain injury by MRI
• MRI done after 72 hr cooling
• ~ DOL #4-5
• Injury patterns can predict outcomes and severity.
Neonatal neurocritical care:
Experience and resources can matter
Neonatal neurocritical care:
Experience and resources can matter
• Transport
• Seizure detection
• Acute critical care with multi-organ failure
• Complications and side effects
• ECMO
• Palliative care support

10/28/2010
12
Complications in high-risk patientsComplications in high-risk patients
• Multi-organ failure/ischemia-reperfusion injurySarkar et al., J. Perinatol, 2009
• Other complications of cooling from clinical trials Jacobs, et al., Cochrane Database Syst Rev, 2007
– Thrombocytopenia
– Need for vasopressors (Battin et al., Pediatrics, 2009)
– Sinus bradycardia (physiologic)
– Glucose metabolism (hyper/hypo)
– Prolonged PT/PTT (physiologic) with normal fibrinogen
– Skin changes (Shankaran S, et al, NEJM, ‘05) (Hogeling, et al, Peds Derm, ’10)
Future developments in coolingFuture developments in cooling
• Late Hypothermia for HIE Trial (NICHD trial)
• 6-24 hrs after injury
• 96 hours of hypothermia
• 17 centers (Stanford Univ in CA) – Completion Mar 2014
ClinicalTrials.gov: NCT00614744
• Head cooling in Preterm infants with HIE (pilot)
• <36wk, but >32wk GA after HIE and <6hours old
• Industry sponsored, open label, safety trial
• Vanderbilt/Northwestern - Completion Feb 2010
ClinicalTrials.gov: NCT00620711
• Late Hypothermia for HIE Trial (NICHD trial)
• 6-24 hrs after injury
• 96 hours of hypothermia
• 17 centers (Stanford Univ in CA) – Completion Mar 2014
ClinicalTrials.gov: NCT00614744
• Head cooling in Preterm infants with HIE (pilot)
• <36wk, but >32wk GA after HIE and <6hours old
• Industry sponsored, open label, safety trial
• Vanderbilt/Northwestern - Completion Feb 2010
ClinicalTrials.gov: NCT00620711
SummarySummary
• Major RCT’s and meta-analyses consistently show cooling
reduces death &/or disability and outcomes to 2 years.
• Mortality for asphyxia remains high.
• Consider cooling early. Contact a regional cooling center to
discuss possible cases.
• Clinical experience and resources can matter.
• Advances in neuromonitoring, imaging and evidenced-
based care make neonatal neurointensive care possible.
• In the future, emphasis on new adjuvant therapies and
health service research.
• Major RCT’s and meta-analyses consistently show cooling
reduces death &/or disability and outcomes to 2 years.
• Mortality for asphyxia remains high.
• Consider cooling early. Contact a regional cooling center to
discuss possible cases.
• Clinical experience and resources can matter.
• Advances in neuromonitoring, imaging and evidenced-
based care make neonatal neurointensive care possible.
• In the future, emphasis on new adjuvant therapies and
health service research.

10/28/2010
13
AcknowledgmentsAcknowledgments
UCSF NICN working group
Donna FerrerioDonna Ferrerio
David RowitchDavid Rowitch
Sue Peloquin (Coordinator)Sue Peloquin (Coordinator)
Hannah GlassHannah Glass
Sonia BonifacioSonia Bonifacio
Liz RogersLiz Rogers
Sally SehringSally Sehring
Yao SunYao Sun
Jim BarkovichJim Barkovich
Joe SullivanJoe Sullivan
UCSF NICN working group
Donna FerrerioDonna Ferrerio
David RowitchDavid Rowitch
Sue Peloquin (Coordinator)Sue Peloquin (Coordinator)
Hannah GlassHannah Glass
Sonia BonifacioSonia Bonifacio
Liz RogersLiz Rogers
Sally SehringSally Sehring
Yao SunYao Sun
Jim BarkovichJim Barkovich
Joe SullivanJoe Sullivan
UCSF Pediatric NeurologyUCSF Pediatric Neurology
UCSF NICN NursesUCSF NICN Nurses
UCSF Children’s Hospital and UCSF Children’s Hospital and
Medical CenterMedical Center
Our patients and their families
UCSF Pediatric NeurologyUCSF Pediatric Neurology
UCSF NICN NursesUCSF NICN Nurses
UCSF Children’s Hospital and UCSF Children’s Hospital and
Medical CenterMedical Center
Our patients and their families