disclosure recognition and diagnosis of high-flow ... · recognition and diagnosis of high-flow...
TRANSCRIPT
Recognition and Diagnosis of High-Flow Autogenous Accesses
Dirk Hentschel, MDDirector, Interventional Nephrology
Brigham and Women’s Hospital
ASDIN 9th Annual Scientific MeetingWashington, DC, February 17, 2013
Disclosure
• Proteon Therapeutics
What is a High-Flow Autogenous Access? What is a High-Flow Autogenous Access?
• KDOQI Vascular Access (2006)★ No definition★ single mention in context of AVF aneurysm formation
What is a High-Flow Autogenous Access?
• KDOQI Vascular Access (2006)★ No definition★ single mention in context of AVF aneurysm formation
• EBPG on Vascular Access (2007) ★ “High flow access” := brachial-cubital/cephalic/basilic (upper
arm) autogenous accesses★ no blood flow range
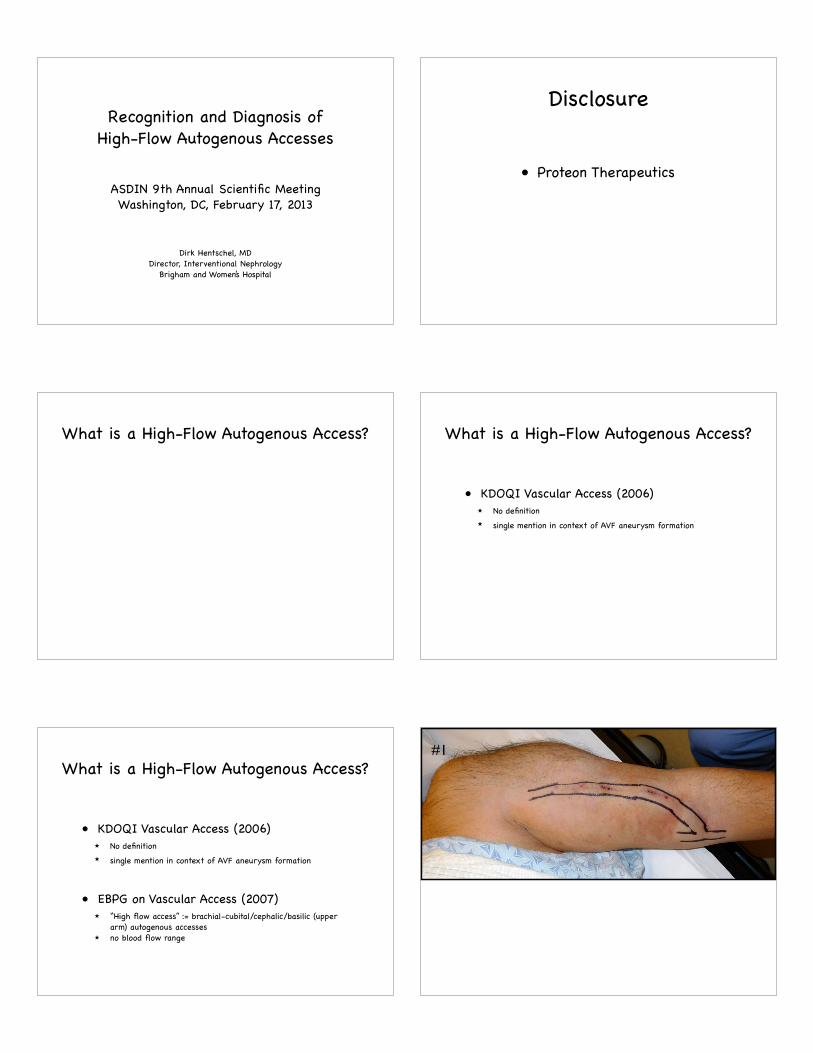
#1

flow 1400ml/min @blood pressure 146/65
#1
flow 1400ml/min @blood pressure 146/65
#1
flow 1400ml/min @blood pressure 146/65
#1
flow 1400ml/min @blood pressure 146/65
#1DMII, HTN, CAD, PVD
“STEAL”
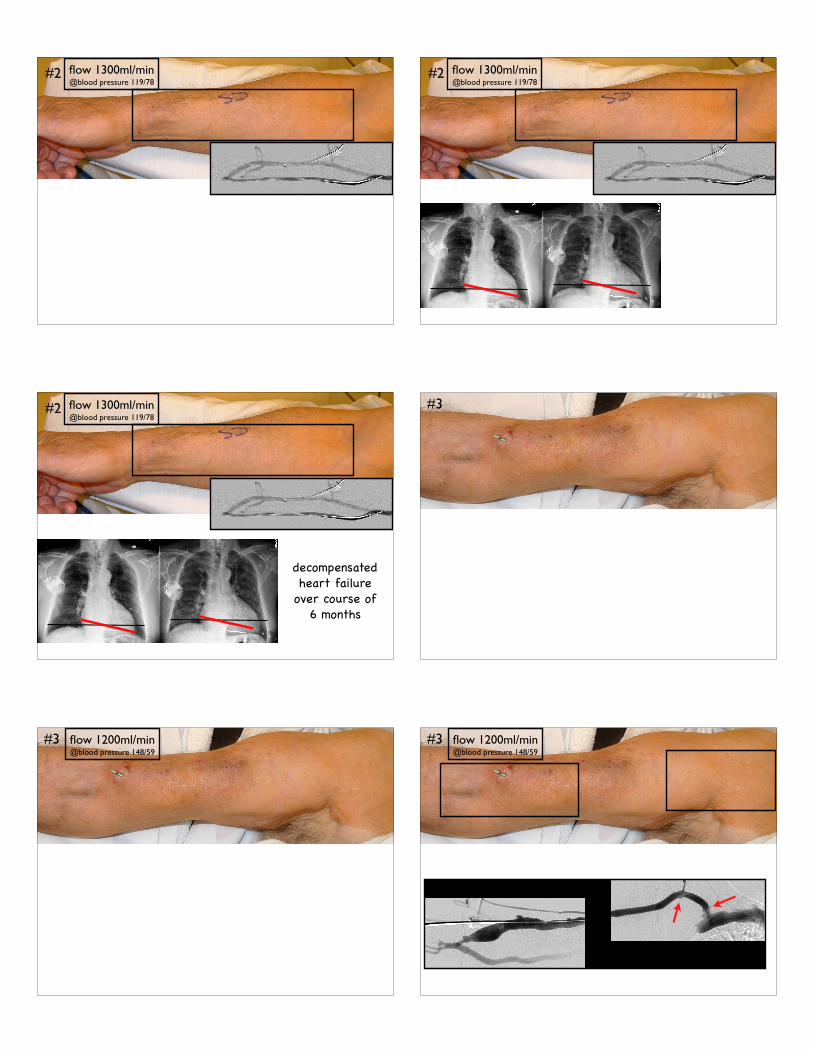
#2 flow 1300ml/min @blood pressure 119/78
#2
flow 1300ml/min @blood pressure 119/78
#2 flow 1300ml/min @blood pressure 119/78
#2
flow 1300ml/min @blood pressure 119/78
#2
decompensatedheart failure
over course of 6 months
#3
flow 1200ml/min @blood pressure 148/59
#3 flow 1200ml/min @blood pressure 148/59
#3

flow 1700ml/min @blood pressure 142/54
flow 1200ml/min @blood pressure 148/59
#3
flow 1700ml/min @blood pressure 142/54
flow 1200ml/min @blood pressure 148/59
#3
inflow-outflow mismatch
#4 flow 2500ml/min @blood pressure 129/7
#4
flow 2500ml/min @blood pressure 129/7
#4
Aug-2011 Mar-2011
flow 2500ml/min @blood pressure 129/7
#4
Aug-2011 Mar-2011
time horizon

flow 2500ml/min @blood pressure 129/7
#4
Aug-2011 Mar-2011
time horizon
#5
flow 5900ml/min @blood pressure 110/63
#5 flow 5900ml/min @blood pressure 110/63
#5
decreased URR/elevated venous pressures - cardiopulmonary
recirculation
type of high flow Steal CV strain inflow-outflow mismatch
Time Horizon(URR)
pulsatility any normal or increased
increased normal
thrill presentjuxta-anastomotic
present only systolic present
bruit continuous continuous pronounced systolic
continuous
augmentation any moderate-strong
moderate-strong
moderate
collapse with gravity
yes yes no yes
Physical exam of high-flow accesses
type of high flow Steal CV strain inflow-outflow mismatch
Time Horizon(URR)
pulsatility any normal or increased
increased normal
thrill presentjuxta-anastomotic
present only systolic present
bruit continuous continuous pronounced systolic
continuous
augmentation any moderate-strong
moderate-strong
moderate
collapse with gravity
yes yes no yes
Physical exam of high-flow accesses
type of high flow Steal CV strain inflow-outflow mismatch
Time Horizon(URR)
pulsatility any normal or increased
increased normal
thrill presentjuxta-anastomotic
present only systolic present
bruit continuous continuous pronounced systolic
continuous
augmentation any moderate-strong
moderate-strong
moderate
collapse with gravity
yes yes no yes
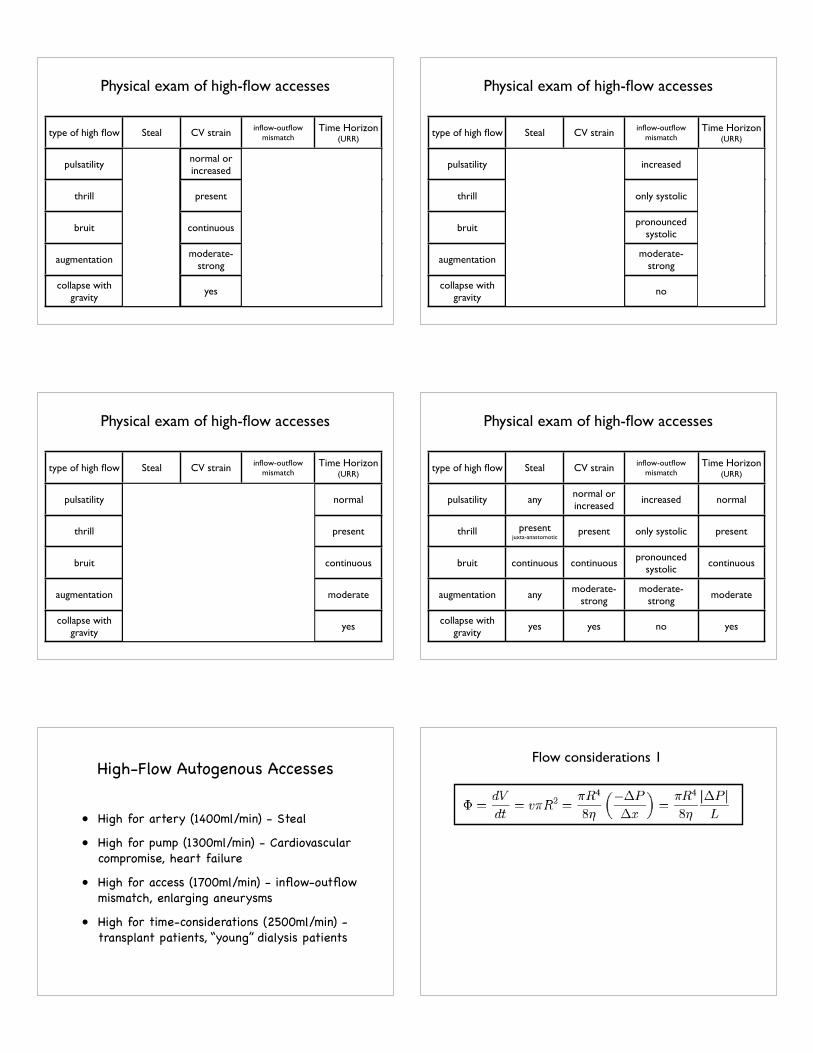
Physical exam of high-flow accesses
type of high flow Steal CV strain inflow-outflow mismatch
Time Horizon(URR)
pulsatility any normal or increased
increased normal
thrill presentjuxta-anastomotic
present only systolic present
bruit continuous continuous pronounced systolic
continuous
augmentation any moderate-strong
moderate-strong
moderate
collapse with gravity
yes yes no yes
Physical exam of high-flow accesses
type of high flow Steal CV strain inflow-outflow mismatch
Time Horizon(URR)
pulsatility any normal or increased
increased normal
thrill presentjuxta-anastomotic
present only systolic present
bruit continuous continuous pronounced systolic
continuous
augmentation any moderate-strong
moderate-strong
moderate
collapse with gravity
yes yes no yes
Physical exam of high-flow accesses
type of high flow Steal CV strain inflow-outflow mismatch
Time Horizon(URR)
pulsatility any normal or increased
increased normal
thrill presentjuxta-anastomotic
present only systolic present
bruit continuous continuous pronounced systolic
continuous
augmentation any moderate-strong
moderate-strong
moderate
collapse with gravity
yes yes no yes
Physical exam of high-flow accesses
High-Flow Autogenous Accesses
• High for artery (1400ml/min) - Steal
• High for pump (1300ml/min) - Cardiovascular compromise, heart failure
• High for access (1700ml/min) - inflow-outflow mismatch, enlarging aneurysms
• High for time-considerations (2500ml/min) - transplant patients, “young” dialysis patients
Flow considerations 1

Flow considerations 1
2xR L Δ P η Φ2 1 40 2.6 479.88
2.5 1 40 2.6 1171.5823 1 40 2.6 2429.3934 1 40 2.6 7678.084 1 20 2.6 3839.044 1 10 2.6 1919.52
diameter length pressure gradient at anastomosis
blood viscosity
FLOW ml/min
Flow considerations 1
2xR L Δ P η Φ2 1 40 2.6 479.88
2.5 1 40 2.6 1171.5823 1 40 2.6 2429.3934 1 40 2.6 7678.084 1 20 2.6 3839.044 1 10 2.6 1919.52
diameter length pressure gradient at anastomosis
blood viscosity
FLOW ml/min
arteries adjust to higher flow with increase in diameter to reach 10-25 dyn/cm2 optimum shear stress
higher flow := higher pressure if outflow stenosis
higher pressures := enlargement and calcification
Flow considerations 2
arteries adjust to higher flow with increase in diameter to reach 10-25 dyn/cm2 optimum shear stress
higher flow := higher pressure if outflow stenosis
higher pressures := enlargement and calcification
Flow considerations 2
upper arm access := anastomosis is flow limiting resistor
forearm access := calcified inflow artery may be limiting
f/u #1
Tx x 13 years10mm anastomosis @ brachial artery
f/u #1flow 4200ml/min @blood pressure 125/52
Tx x 13 years10mm anastomosis @ brachial artery

f/u #2 f/u #2
flow 700ml/min @blood pressure
124/85
f/u #2
• apparent lack of systemic vascular disease
• young age
• Access flow >2000; low URR despite large access; high venous pressures
Recognition of “high flow” High Flow Accesses
Patient Characteristics
• apparent lack of systemic vascular disease
• young age
• Access flow >2000; low URR despite large access; high venous pressures
Surgical and Angiographic Characteristics
• location/diameter of inflow artery
• diameter of anastomosis (>3-4mm?)
• velocity of contrast and/or its dilution
• MEASURE... (flow, artery, anastomosis)
Recognition of “high flow” High Flow Accesses
Patient Characteristics• steal - banding, DRIL, proximalization; inflow stenosis
• cardiovascular compromise - banding, ligation
• inflow-outflow mismatch - fix outflow +/- banding
• decreasing URR, chronically elevated venous pressures
Summary
High flow because of symptoms
• steal - banding, DRIL, proximalization; inflow stenosis
• cardiovascular compromise - banding, ligation
• inflow-outflow mismatch - fix outflow +/- banding
• decreasing URR, chronically elevated venous pressures
Summary
High flow because of symptoms
• “Normal” flows: forearm 850 ml/min (n=11); upper arm brachial-cephalic 1580ml/min (n=56) - depends on local surgeons...
• Think about high flow state if flows >1500ml/min, access pulsatile and without collapse after angioplasty
High flow because of potential complications