dimensions of personality and personality pathology
TRANSCRIPT

281
Journal of Personality Disorders, 28(2), pp. 281–318, 2014© 2014 The Guilford Press
DIMENSIONS OF PERSONALITY AND PERSONALITY PATHOLOGY: FACTOR STRUCTURE OF THE SHEDLER–WESTEN ASSESSMENT PROCEDURE-II (SWAP-II)
Drew Westen, PhD, Niels G. Waller, PhD, Jonathan Shedler, PhD, and Pavel S. Blagov, PhD
Researchers have proposed replacing the current system for diagnosing personality disorders with a dimensional trait model. Proposed trait models have been derived primarily from data provided by untrained lay informants (often via self-report questionnaires) using item sets de-rived from lay conceptions of personality. An alternative is to derive personality trait dimensions from data provided by clinically expert in-formants using an instrument that includes personality features sa-lient to clinicians who treat personality dysfunction. The authors report the factor structure of the latest edition of the Shedler–Westen Assess-ment Procedure (SWAP-II) using a normative clinical sample of 1,201 North American patients assessed by experienced psychologists and psychiatrists. Factor analysis identified 14 clinically and empirically coherent factors. The findings highlight dimensions of personality and personality pathology that have not emerged in personality item sets designed for lay personality description.
Dimensional personality diagnosis has substantial advantages over cate-gorical diagnosis, at least for research purposes (Krueger, Watson, & Bar-low, 2005; Westen, Gabbard, & Blagov, 2006; Widiger & Samuel, 2005). Some investigators equate the term “dimensional” with trait models derived via factor analysis. However, trait models represent only one of several al-ternative approaches to dimensional personality diagnosis.
One approach to dimensional diagnosis is simply to dimensionalize ex-isting DSM-IV personality disorders. This can be accomplished by sum-
This article was accepted under the editorship of Paul S. Links.
From Emory University (D. W.); University of Minnesota (N. G. W.); University of Colorado School of Medicine (J. S.); and Whitman College (P. S. B.).
This research was funded by NIMH grant R01-MH78100.
Address correspondence to Drew Westen, Department of Psychology, Emory University, 36 Eagle Row, Atlanta, GA 30322; E-mail: [email protected]; or Jonathan Shedler, Depart-ment of Psychiatry, University of Colorado School of Medicine, Mail Stop A011-04, 13001 East 17th Place, Aurora, CO 80045; E-mail: [email protected]
282 WESTEN ET AL.
ming the number of diagnostic criteria met for each disorder (instead of imposing an arbitrary cut-point; Oldham & Skodol, 2000). It can also be accomplished via a prototype matching procedure, whereby diagnosti-cians gauge the similarity or “fit” between a patient’s clinical presentation and a paragraph-length narrative description of each disorder (Rottman, Ahn, Sanislow, & Kim, 2009; Spitzer, First, Shedler, Westen, & Skodol, 2008; Westen & Shedler, 2000; Westen, Shedler, & Bradley, 2006). Else-where, we have proposed a dimensional approach to personality diagnosis based on empirically derived personality prototypes (Westen & Shedler, 1999a, 1999b; Westen, Shedler, Bradley, & DeFife, 2012). This diagnostic system preserves a syndromal approach to personality, consistent with all editions of DSM to date; however, both the diagnostic groupings and the descriptions of the diagnoses are derived empirically and reflect naturally occurring groupings in the clinical population.
The classification systems just described are person-centered and syn-dromal. That is, they focus on personality syndromes, or multifaceted constellations of interrelated personality features. A very different ap-proach to dimensional diagnosis is variable-centered, focusing on discrete trait dimensions (rather than multidimensional syndromes) derived via factor analysis (e.g., Krueger & Markon, 2011; Krueger, Watson, & Barlow, 2005; Widiger, Simonsen, Krueger, Livesley, & Verheul, 2005). For several years, trait psychologists have advocated moving away from the syndro-mal approach of DSM-IV to a diagnostic system based on the five factor model (FFM) (e.g., Widiger, Costa, & McCrae, 2002). Investigators have also proposed that both normal and pathological personality can be un-derstood in terms of a trait model comprising four superordinate factors, variously described as (1) negative affectivity or neuroticism, (2) introver-sion or low positive affectivity, (3) antagonism or low agreeableness, and (4) impulsivity or low conscientiousness (Livesley, Jang, & Vernon, 1998; Watson, Clark, & Harkness, 1994; Widiger & Simonsen, 2005).
The FFM and derivative models proposed as taxonomic alternatives to the syndromal diagnoses of DSM-IV (Widiger & Trull, 2007) have a number of advantages, perhaps most importantly that FFM factors tend to repli-cate across multiple methods and informants and reliably capture impor-tant aspects of normal personality. A potential limitation is that the re-search underlying these models (Clark, Livesley, Schroeder, & Irish, 1996; Markon, Krueger, & Watson, 2005) (including the new variant proposed by the DSM-5 Axis II Work Group; http://www.dsm5.org) has relied heavily on self-report questionnaire data. This presupposes that (a) the data nec-essary and sufficient to derive a comprehensive and clinically relevant model of personality do not require expertise in psychopathology; (b) indi-viduals with significant personality pathology have sufficient self-aware-ness and insight that their self-reports (or those of untrained peer observ-ers) are sufficient to derive a comprehensive model of personality and its pathology; and (c) that the language of lay observation (or attempts to summarize it via factor analysis) is adequate for a diagnostic manual in-

FACTOR STRUCTURE OF THE SWAP-II 283
tended to be useful to both clinical practitioners and psychopathology re-searchers.
Both meta-analytic investigations (Klonsky, Oltmanns, & Turkheimer, 2002) and data from recent large-N studies (Clifton, Turkheimer, & Olt-manns, 2005) have shown that self-reported pathological personality traits correlate only moderately (in meta-analytic research, r = .36) with the same traits assessed by lay informants and weakly with longitudinal evaluation by experts using all available data (Klein, Ouimette, Kelly, Fer-ro, & Riso, 1994; Pilkonis, Heape, Ruddy, & Serrao, 1991). By contrast, both traits and dimensional personality disorder diagnoses derived from data provided by experienced clinicians using a systematic clinical re-search interview correlate in the range of r = .50 to .70 with the same vari-ables as assessed by treating clinicians (Westen & Muderrisoglu, 2003, 2006; Westen et al., 2012). Similarly, research on “illusory mental health” (Shedler, Mayman, & Manis, 1993) demonstrates that self-report mea-sures of neuroticism (or negative affectivity) cannot distinguish psycho-logically healthy individuals from psychologically distressed individuals who lack self-awareness.
Whether superior in some respects or simply complementary to self- reports, quantified judgments made by clinically trained and experienced observers offer an alternative source of data for personality research, par-ticularly for developing dimensional personality diagnoses intended to be useful in clinical as well as research contexts (Shedler & Westen, 2007; Westen & Shedler, 2007). Although much of our research to date using expert observers has focused on personality disorder prototypes (i.e., con-stellations of interrelated characteristics that together comprise a diag-nostic syndrome), we have also developed dimensional trait models in both adult (Shedler & Westen, 2004a) and adolescent (Westen, Dutra, & Shedler, 2005) samples by factor analyzing adult and adolescent versions of the Shedler–Westen Assessment Procedure (SWAP). This article focuses on trait dimensions derived via factor analysis of the current version of the adult SWAP instrument.
The SWAP-200 (and its revised version, the SWAP-II) is a comprehensive set of 200 items capturing both personality pathology and aspects of adap-tive personality functioning. A mental health professional with a thorough knowledge of the patient based on clinical examination ranks each item from 7 (highly descriptive) to 0 (not descriptive). The assessor must have first become familiar with the patient, specifically in a professional clini-cal-evaluative context through a comprehensive research-clinical inter-view (the Clinical Diagnostic Interview; see Westen & Muderrisoglu, 2003; www.psychsystems.net/manuals) or a minimum of six clinical hours of assessment and treatment. The instrument is thus designed specifically for use by clinical professionals functioning in professional contexts. The instrument is based on the Q-sort method: To maximize reliability and as-sure comparability of scores across assessors, assessors rank-order the personality-descriptive statements using a fixed distribution (in which

284 WESTEN ET AL.
relatively few items receive the highest ranks, and progressively more items receive lower ranks, mirroring the natural distribution of psycho-pathological variables).
SWAP data can be analyzed via conventional factor analysis (a variable-centered approach) to identify underlying personality factors or trait di-mensions. They can also be analyzed via Q-factor analysis (a person-cen-tered approach) to identify groupings of patients who share a common personality syndrome (i.e., who are psychologically similar to one another and distinct from patients in other groupings). Thus, the SWAP instru-ments can be used to derive both (a) trait dimensions and (b) naturally occurring diagnostic grouping in the clinical population (i.e., diagnostic prototypes; Westen & Shedler, 1999b; Westen et al., 2012). Because the item sets for both adult and adolescent versions of the SWAP cover the domains included in DSM-III-R and DSM-IV, the instruments can addition-ally be used to derive (dimensional) DSM Axis II diagnoses.1
Factor analyses of the SWAP-200 (the prior adult version of the instru-ment) yielded 12 conceptually coherent and clinically relevant factors (Shedler & Westen, 2004a), including Psychological Health, Psychopathy, Emotional Dysregulation, Dysphoria, Obsessionality, Thought Disorder, Sexual Conflict, and Histrionic Sexualization. Factor analysis of the SWAP-200-A (the adolescent version of the instrument) yielded 11 highly similar factors, although it also included some factors distinct to this develop-mental period (e.g., Delinquent Behavior, Attentional Dysregulation, and Peer Rejection). These SWAP factors (both adult and adolescent) showed expected patterns of correlations with a wide range of criterion variables, providing support for their construct validity. Efforts to identify higher-order factors by factor analyzing the factors did not yield coherent or in-terpretable higher-order factors, suggesting that the SWAP factors mea-sured distinct constructs that were not reducible to FFM domains.
The major limitations of our prior factor-analytic studies using the SWAP-200 were sample size and representativeness. The largest sample used to derive personality traits was 530, and the sample was selected deliberately to include only patients with diagnosable DSM-IV personality disorders in relatively equal numbers. How sample selection may have influenced or biased the factors that emerged is unclear. The current study addresses these limitations.
We report on the factor structure underlying comprehensive personality descriptions of adult patients provided by experienced clinician-observers. Each clinician-observer described one randomly selected patient in his or her care who had any degree of personality impairment or dysfunction, irrespective of whether the patient did or did not meet criteria for a DSM personality disorder diagnosis. The clinician-observers described the pa-
1. Whereas the original presentations of the SWAP emphasized configural diagnosis, that is, DSM-IV diagnosis and empirical derived prototypes (Westen & Shedler, 1999a, 1999b), later research has taken the more agnostic, empirical approach we describe here, namely one that makes use of whatever data-analytic and conceptual approach or approaches prove most empirically valid and clinically useful (Shedler & Westen, 2004b; Westen & Shedler, 2007).

FACTOR STRUCTURE OF THE SWAP-II 285
tients using the most recent version the adult SWAP instrument, the SWAP-II. The study used a normative sample of 1,201 North American patients and was specifically designed to develop alternative taxonomic approaches to personality diagnosis for DSM-5.
METHODSAMPLE
We used the national membership rosters of the American Psychological Association and Psychiatric Association to invite a random sample of psy-chiatrists and psychologists with at least 5 years of experience postresi-dency (MDs) or postlicensure (PhDs) to provide assessment data. The re-sponse rate was more than 30%. There were no differences on any demographic or other variables we examined between participants who responded to our initial invitation and those who responded to a subse-quent follow-up invitation, suggesting that any sampling bias had mini-mal effects on results. The participating clinician-assessors received a consulting fee of $200 to complete all research forms and instruments, which required approximately 2 hours.
We asked the clinician-observers to describe “an adult patient you are currently treating or evaluating who has enduring patterns of thoughts, feeling, motivation or behavior—that is, personality problems—that cause distress or dysfunction.” To obtain a broad range of personality pathology, we emphasized that patients need not have a personality disorder diagno-sis. Patients had to meet the following additional inclusion criteria: ≥18 years of age, not in a current psychotic episode, and known well by the observer (using the guideline of ≥6 clinical contact hours but ≤2 years to minimize confounds imposed by personality change during treatment). To obtain a representative sample free from selection bias, we directed clini-cian-assessors to consult their calendars and select the last patient they saw during the previous week who met study criteria. In prior research, assessors reported that they followed these instructions as directed (e.g., Westen & Shedler, 1999a). To verify that this was the case in the present study, we recontacted a randomly selected group of 100 of the clinician-assessors who had provided data. Of the 46 who responded, 96% reported following the procedure as specified. Each assessor contributed data on one patient only (to minimize rater-dependent variance). Assessors had the option of providing SWAP-II data using a traditional card-sorting pro-cedure (with items printed on index cards) or providing SWAP-II data on-line using a secure Internet site.
MEASURES
The Clinical Data Form (CDF) is a set of objective clinician-report ratings of variables relevant to demographics, diagnosis, adaptive functioning, de-velopmental and family history, and etiology (Westen & Shedler, 1999a)

286 WESTEN ET AL.
with which clinically trained observers who have worked with a patient over a number of hours are usually familiar (e.g., history of foster care, family history of criminality). In prior studies, these ratings predicted the-oretically relevant criterion variables and reflected reasonable (and con-servative) decision rules (e.g., Russ, Heim, & Westen, 2003; Wilkinson & Westen, 2000) (e.g., clinicians followed our instructions to report adverse childhood events such as abuse or history of psychiatric hospitalizations to be present only if they had substantial data supporting them, such as corroboration from informants at the time of abuse or psychiatric records). In what follows, aside from demographics and treatment characteristics, we report ratings of adaptive functioning from the CDF using the Global Assessment of Functioning (GAF) scale from the DSM-IV Axis V. Recent research has shown that these clinician-rated variables correlate strongly with independent assessments of the same variables (DeFife, Drill, Na-kash, & Westen, 2010).
The SWAP-II is the latest revision of the Shedler–Westen Assessment Procedure, which has been used in numerous taxonomic studies (e.g., Shedler & Westen, 2004a, 2004b; Westen & Shedler, 1999a, 1999b, 2007). To describe a patient, a clinically experienced observer sorts 200 person-ality-descriptive statements into eight categories, from least descriptive of the patient (assigned a value of 0) to most descriptive (7). The instrument is based on the Q-sort method, which requires observers to arrange items into a fixed distribution. The psychometric advantages of the Q-sort meth-od were described by Block (1978).
The SWAP-II allows clinically trained observers to provide systematic and quantifiable in-depth psychological descriptions of patients using a standard “vocabulary” of personality-descriptive statements. The state-ments are written without jargon in a manner that stays close to the ob-servational data (e.g., “Tends to get into power struggles”; “Is capable of sustaining meaningful relationships characterized by genuine intimacy and caring”). Statements that require inference about internal psychologi-cal processes are written in clear, unambiguous language (e.g., “Tends to see own unacceptable feelings or impulses in other people instead of in him/herself”). The use of jargon-free language minimizes unreliable inter-pretive leaps and makes the item set useful to clinicians of all theoretical perspectives.
The SWAP-II item was designed to subsume Axis II criteria included in DSM-III through DSM-IV, including their appendices. Additionally, it incor-porates selected Axis I criteria relevant to personality (e.g., anxiety and depression), important personality constructs described in the clinical and research literatures over the past 50 years, and clinical observations from pilot studies. The SWAP-200 item set was the product of a 7-year it-erative item revision process that incorporated the feedback of hundreds of clinician-consultants who used earlier versions of the item set to de-scribe their patients. We asked each consultant: “Were you able to describe the things you consider psychologically important about your patient?” We added, rewrote, and revised items based on the feedback, then asked new

FACTOR STRUCTURE OF THE SWAP-II 287
consultants to describe new patients. We repeated this process over many iterations until most consultants answered “yes” most of the time.
The SWAP-II incorporates the additional feedback of over 2,000 clini-cian-consultants of all theoretical orientations. We edited items for clarity and added new item content where feedback indicated omission of rele-vant personality constructs. For example, the burgeoning literature on harm-avoidance (Pezawas et al., 2005) suggested that the SWAP-200 did not adequately cover the construct, so we added an item to address it di-rectly (“Decisions and actions are unduly influenced by efforts to avoid perceived dangers; is more concerned with avoiding harm than pursuing desires”). We also conducted item analyses of SWAP-200 items and deleted items that did not discriminate among patients in a national sample (i.e., that showed minimal variance across patients), and deleted or combined items where analyses indicated empirical redundancy. Overall, 23 items had significant content alterations from the SWAP-200 to the SWAP-II, and additional items were edited to clarify existing content. We have described the revision process and its outcome in additional detail in a prior publi-cation (Westen & Shedler, 2007).
An increasing body of research supports the validity and reliability of the adult and adolescent versions of the SWAP in predicting a wide range of criterion variables including, for example, suicide attempts, history of psychiatric hospitalizations, adaptive functioning, interview diagnoses, psychiatric disorders in first- and second-degree biological relatives, and developmental and family history variables (see reviews in Shedler & Westen, 2007; Westen & Shedler, 2007; Westen et al., 2012).
Axis II Checklist. To maximize accuracy of DSM-IV personality disorder diagnoses, we presented clinician-consultants with a randomly ordered checklist of the criteria for all Axis II personality disorders. This method produces results that mirror findings based on structured interviews (Mo-rey, 1988; Westen & Muderrisoglu, 2003). For each personality disorder, we generated DSM-IV diagnoses both categorically (by applying DSM-IV de-cision rules) and dimensionally (by counting the number of criteria met).
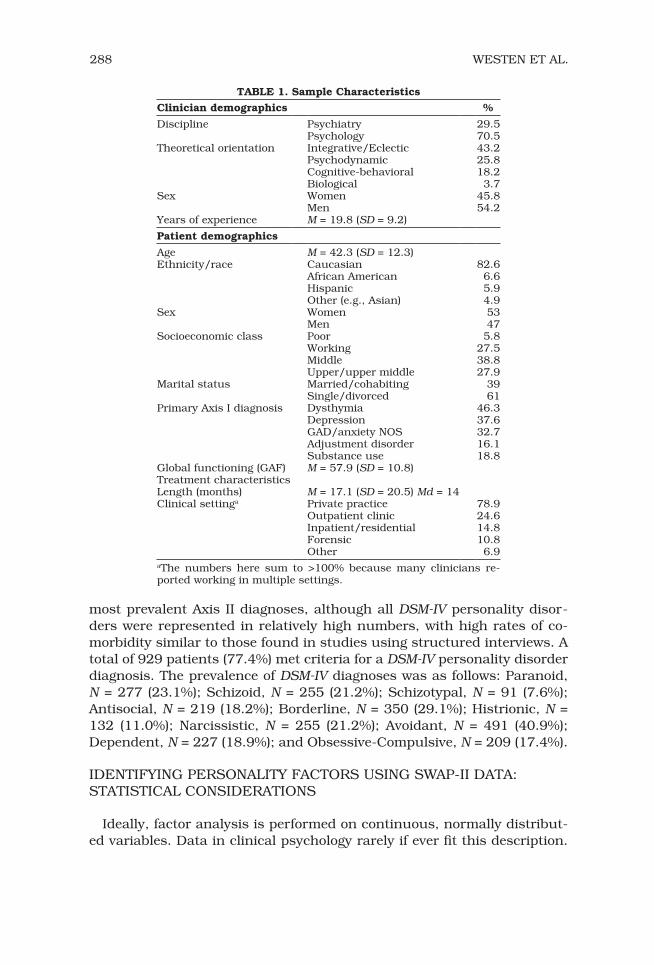
RESULTSTable 1 presents demographics of the clinician-observers and patients. The patients (N = 1,201) averaged early middle age with substantial vari-ance; were approximately equally split by gender; were roughly 80% Cau-casian, with African American (n = 79) and Hispanic (n = 71) ethnicities reasonably represented; and reflected a roughly normal distribution with respect to social class. The mean of the GAF scores indicated substantial impairment overall, whereas their high variability indicated that the ob-servers followed our instructions for random selection of patients who met study criteria (not only patients with DSM-IV Axis II diagnoses). The most common Axis I diagnoses were mood, anxiety, substance use, and adjust-ment disorders. As assessed by applying DSM-IV criteria to the Axis II Checklist, avoidant and borderline personality disorders (PDs) were the
288 WESTEN ET AL.
most prevalent Axis II diagnoses, although all DSM-IV personality disor-ders were represented in relatively high numbers, with high rates of co-morbidity similar to those found in studies using structured interviews. A total of 929 patients (77.4%) met criteria for a DSM-IV personality disorder diagnosis. The prevalence of DSM-IV diagnoses was as follows: Paranoid, N = 277 (23.1%); Schizoid, N = 255 (21.2%); Schizotypal, N = 91 (7.6%); Antisocial, N = 219 (18.2%); Borderline, N = 350 (29.1%); Histrionic, N = 132 (11.0%); Narcissistic, N = 255 (21.2%); Avoidant, N = 491 (40.9%); Dependent, N = 227 (18.9%); and Obsessive-Compulsive, N = 209 (17.4%).
IDENTIFYING PERSONALITY FACTORS USING SWAP-II DATA: STATISTICAL CONSIDERATIONS
Ideally, factor analysis is performed on continuous, normally distribut-ed variables. Data in clinical psychology rarely if ever fit this description.
TABLE 1. Sample Characteristics
Clinician demographics %
Discipline Psychiatry 29.5Psychology 70.5
Theoretical orientation Integrative/Eclectic 43.2Psychodynamic 25.8Cognitive-behavioral 18.2Biological 3.7
Sex Women 45.8Men 54.2
Years of experience M = 19.8 (SD = 9.2)
Patient demographics
Age M = 42.3 (SD = 12.3)Ethnicity/race Caucasian 82.6
African American 6.6Hispanic 5.9Other (e.g., Asian) 4.9
Sex Women 53Men 47
Socioeconomic class Poor 5.8Working 27.5Middle 38.8Upper/upper middle 27.9
Marital status Married/cohabiting 39Single/divorced 61
Primary Axis I diagnosis Dysthymia 46.3Depression 37.6GAD/anxiety NOS 32.7Adjustment disorder 16.1Substance use 18.8
Global functioning (GAF) M = 57.9 (SD = 10.8)Treatment characteristicsLength (months) M = 17.1 (SD = 20.5) Md = 14Clinical settinga Private practice 78.9
Outpatient clinic 24.6Inpatient/residential 14.8Forensic 10.8Other 6.9
aThe numbers here sum to >100% because many clinicians re-ported working in multiple settings.

FACTOR STRUCTURE OF THE SWAP-II 289
They tend to be sampled from the tails of the population distribution, re-sulting in skewed or otherwise nonnormally distributed variables (see Micceri, 1989). Furthermore, psychological rating scales tend to have rela-tively few response categories (Bernstein & Teng, 1989; Muthen & Kaplan, 1985). Factor analysis based on the commonly used maximum likelihood and generalized least squares methods can produce biased findings when applied to skewed and/or coarsely categorized data (West, Finch, & Cur-ran, 1995), yielding so-called “difficulty factors” that are psychometric ar-tifacts and substantively meaningless (McDonald, 1965; Waller, Tellegen, McDonald, & Lykken, 1996).
Many of these problems can be avoided by conducting factor analysis on tetrachoric or polychoric correlations rather than on Pearson correlations (Muthen & Speckart, 1983; Waller, 1999), or by utilizing “full-information” methods based on multidimensional item response theory (Mislevy, 1986; Wood et al., 2002). For these reasons, we factor analyzed the SWAP-II data using polychoric correlations and a least squares fit function using Micro-Fact 2.0 software designed for such applications (Waller, 2001).
Another methodological challenge concerns the treatment of sex differ-ences in the item correlation matrix (men and women may produce differ-ent item endorsement rates and/or different item correlations). When these differences go unrecognized, factor-analytic findings can be biased because correlations calculated on (sex) mixed samples reflect both with-in- and between-group sources of covariation (see Waller & Meehl, 1998, pp. 12–16). In the current sample, although men and women produced similar factor patterns, their item endorsement rates differed. For exam-ple, women scored higher than men on eating disorder items, whereas men scored higher than women on indicators of psychopathy. Had we ig-nored these differences, a factor analysis of the (uncorrected) data could produce spurious factors with items from conceptually distinct domains and spurious item cross-loadings that increase factor complexity (Sass & Schmitt, 2010).
Figure 1 presents a more thorough picture of how the men and women in our sample differed on their expected SWAP II item scores. Figure 1A shows the item endorsement rates and illustrates that, across sex, the distributions of item means are comparable. To examine these data at a higher level of resolution, we created a histogram of standardized item-difference scores (the mean differences were scaled by the standard devia-tions from the sample of women). Figure 1B elucidates numerous item-level differences. These figures convinced us of the need to partial out these sex differences before calculating a polychoric correlation matrix for the combined sample. Thus, to control group differences in item level, we computed polychoric correlation matrices separately for each sex, then averaged the matrices to form a combined matrix.
Before we discuss the factor-analytic findings, one final point concern-ing the polychoric correlations deserves mention. We collapsed several categories of the response scale to improve the precision of the estimated

290 WESTEN ET AL.
correlations. Although our sample is large relative to many psychopathol-ogy studies, the demands of our analytic procedures were extreme. When we cross-tabulated all item pairs, we noticed (using a computer program written for this task) that many cells in the 8-by-8 co-occurrence matrices had small joint frequencies. We expected this finding because many items had skewed distributions. Polychoric correlations may be poorly estimat-ed under these conditions, and the estimates can have large standard er-rors. Thus, to calculate more stable correlations, we recoded the original 8-point scales into 3-point scales.2
Following the procedures outlined above, we used MicroFACT 2.0 (Waller, 2001) to calculate a polychoric correlation matrix on the aggregate sample. Next, we extracted the eigenvalues from this matrix. Because their scree plot was not definitive, we extracted and inspected rotated factor solutions with 4 through 20 factors with numerous rotation algorithms.3
FIGURE 1. Distribution of item difficulties in male and female patients.
2. Scores of 0–3 were recoded as 0; 4–5 were recoded as 1; and 6–7 were recoded as 2. If the assumptions underlying the polychoric correlations are satisfied (latent bivariate normality), then recoding the item responses will not bias the correlations. Moreover, even when the underlying distribution departs from multivariate normality, the polychoric correlations will be estimated accurately under a wide range of latent distributions (Flora & Curran, 2004; Quiroga, 1992). However, failure to recode the data in moderate to small samples can result in highly biased correlations if the joint frequencies are small (Muthen & Speckart, 1983).
3. Each solution was rotated to optimize the Geomin, Oblimin (gamma = .00 or .25), and Promax (from an initial Varimax rotation raised to the third power) criteria using the gradient project algorithms of Robert Jennrich (Bernaads & Jennrich, 2005; Jennrich, 2002). Each
FACTOR STRUCTURE OF THE SWAP-II 291
FACTOR-ANALYTIC RESULTS
Careful inspection of the analyses led us to choose a 16-factor solution rotated using Oblimin (γ = .25; solutions based on γ = 0 were virtually in-distinguishable from those based on γ = .25). Solutions with fewer factors combined diagnostically distinct symptoms, whereas solutions with more factors produced doublets (two item factors) that reflected little more than semantic redundancy among item pairs. Consideration of the fit criteria convinced us that the 16-factor solution was optimal for these data. For instance, the average communality in the 16-factor solution was .47, with less than 5% of the items having communalities of .30 or less. This solu-tion also reproduced the data matrix (i.e., the polychoric correlations) re-markably well; fully 80% of the reproduced correlations differed from their targets by .05 or less, and the overall root mean square residual (RMSR) = .05. These findings are well summarized by McDonald’s GFI = .93. In con-trast, the findings for lower-dimensional solutions were not impressive. For instance, in the 5-factor solution, the average communality was only .29, with over 55% of the items having communalities < .30. Consider-ation of the model residuals also suggested that a 5-factor solution was a severe underfactoring, because 15% of the reproduced correlations dif-fered from their targets by .10 or greater (RMSR = .07) and McDonald’s GFI was only .84.
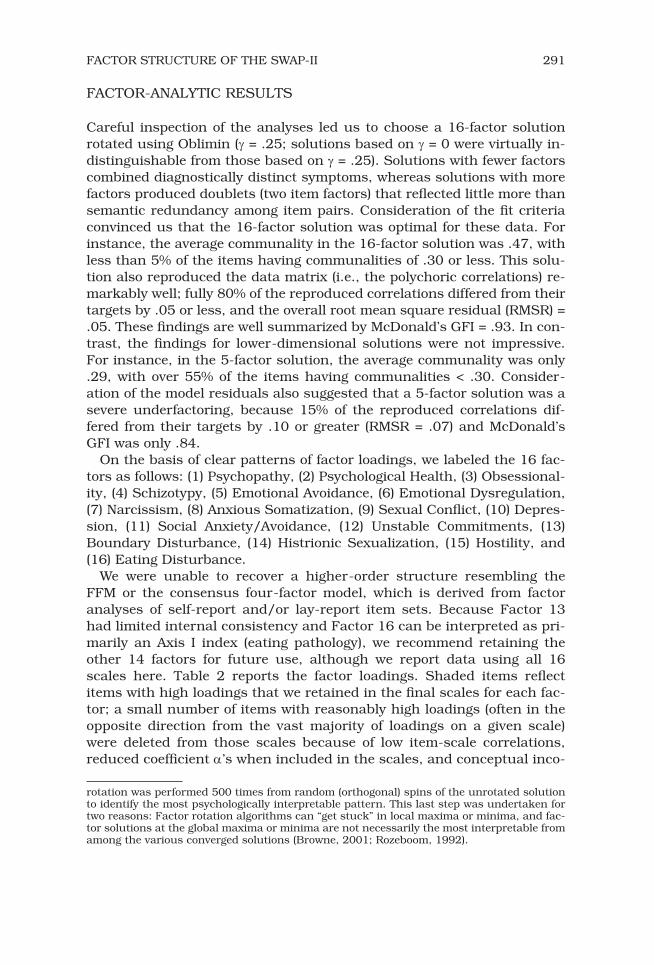
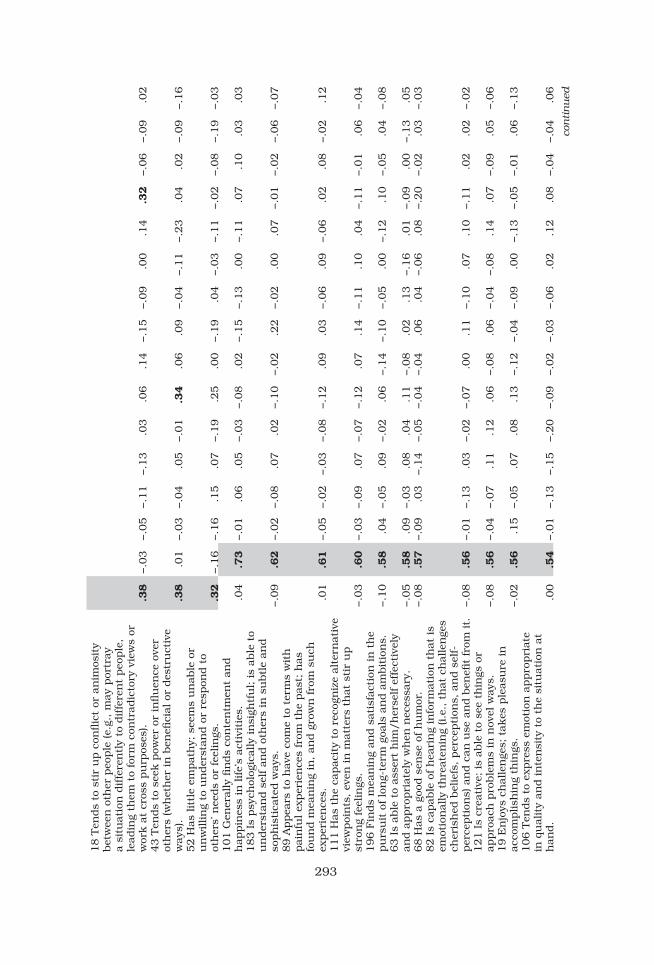
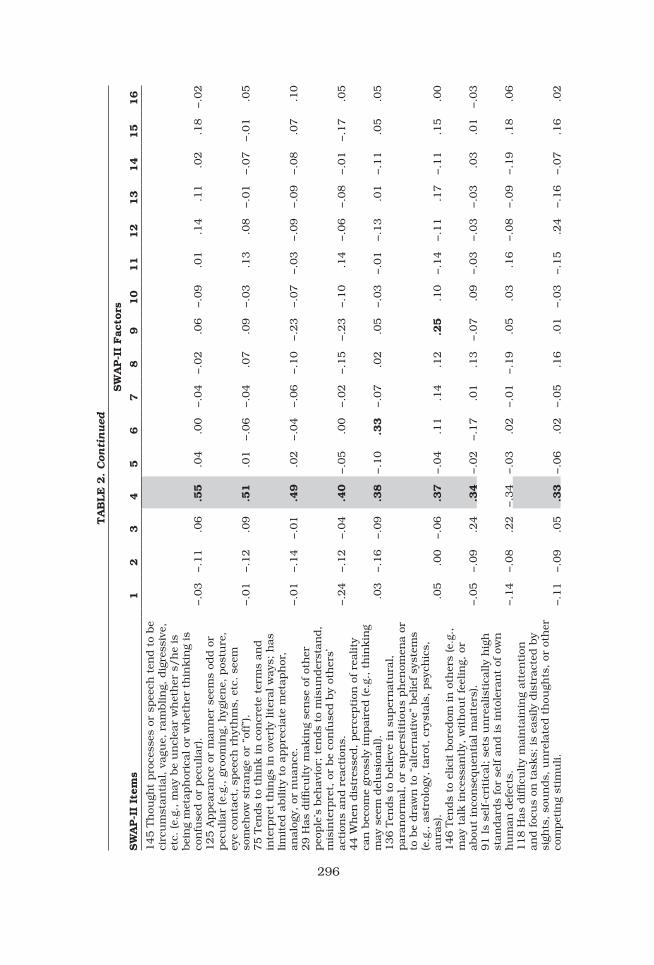
On the basis of clear patterns of factor loadings, we labeled the 16 fac-tors as follows: (1) Psychopathy, (2) Psychological Health, (3) Obsessional-ity, (4) Schizotypy, (5) Emotional Avoidance, (6) Emotional Dysregulation, (7) Narcissism, (8) Anxious Somatization, (9) Sexual Conflict, (10) Depres-sion, (11) Social Anxiety/Avoidance, (12) Unstable Commitments, (13) Boundary Disturbance, (14) Histrionic Sexualization, (15) Hostility, and (16) Eating Disturbance.
We were unable to recover a higher-order structure resembling the FFM or the consensus four-factor model, which is derived from factor analyses of self-report and/or lay-report item sets. Because Factor 13 had limited internal consistency and Factor 16 can be interpreted as pri-marily an Axis I index (eating pathology), we recommend retaining the other 14 factors for future use, although we report data using all 16 scales here. Table 2 reports the factor loadings. Shaded items reflect items with high loadings that we retained in the final scales for each fac-tor; a small number of items with reasonably high loadings (often in the opposite direction from the vast majority of loadings on a given scale) were deleted from those scales because of low item-scale correlations, reduced coefficient α’s when included in the scales, and conceptual inco-
rotation was performed 500 times from random (orthogonal) spins of the unrotated solution to identify the most psychologically interpretable pattern. This last step was undertaken for two reasons: Factor rotation algorithms can “get stuck” in local maxima or minima, and fac-tor solutions at the global maxima or minima are not necessarily the most interpretable from among the various converged solutions (Browne, 2001; Rozeboom, 1992).

292
TA
BLE
2.
Fac
tor
Pat
tern
(F
acto
r Load
ings
) fo
r 16 O
bli
min
-Rota
ted S
WA
P-I
I F
acto
rs
SW
AP-I
I F
acto
rs
SW
AP-I
I It
ems
12
34
56
78
910
11
12
13
14
15
16
40 T
ends
to e
nga
ge in
un
law
ful or
cri
min
al
beh
avio
r..7
3−.0
7−.0
2.0
2.0
0.1
0−.0
6−.0
7.0
0−.1
2.0
8.1
3.0
2−.0
4.0
6.0
43 T
akes
adva
nta
ge o
f ot
her
s; h
as lit
tle
inve
stm
ent
in m
oral
val
ues
(e.
g., pu
ts o
wn
n
eeds
firs
t, u
ses
or e
xplo
its
peo
ple
wit
h lit
tle
rega
rd for
th
eir
feel
ings
or
wel
fare
, et
c.).
.68
−.0
8−.1
0−.0
4−.0
4−.0
7.2
9.0
2−.0
4−.0
3−.0
5−.1
0−.0
4.1
0.0
1−.0
920 T
ends
to b
e dec
eitf
ul; t
ends
to lie
or
mis
lead
..6
5−.0
9−.0
2−.0
9.0
1−.1
0−.0
4−.0
1−.0
2−.0
3−.1
4.0
7−.0
5.0
8.0
3.1
131 T
ends
to s
how
rec
kle
ss d
isre
gard
for
th
e ri
ghts
, pro
per
ty, or
saf
ety
of o
ther
s..6
3−.0
6−.0
2.1
2.0
2−.1
3.2
0−.0
3.0
4−.0
3−.0
5.0
7.0
1−.0
1.0
5−.0
6113 E
xper
ien
ces
litt
le o
r n
o re
mor
se for
h
arm
or
inju
ry c
ause
d t
o ot
her
s..5
6−.0
1−.0
8.0
9.1
0.0
6.0
3−.0
6−.0
4−.1
0−.0
1.0
2.1
7−.0
7−.0
8.0
5115 I
s pro
ne
to v
iole
nce
(e.
g., m
ay b
reak
th
ings
or
bec
ome
ph
ysic
ally
ass
ault
ive)
..5
2.0
1−.0
7−.0
2−.0
2.1
8−.1
7−.0
3.0
1−.1
1.0
2−.0
3.0
3−.0
3−.2
7.2
2112 A
ppea
rs im
per
viou
s to
con
sequ
ence
s;
seem
s u
nab
le o
r u
nw
illin
g to
mod
ify
beh
avio
r in
res
pon
se t
o th
reat
s or
neg
ativ
e co
nse
quen
ces.
.49
−.1
4.0
8.0
7.0
7.0
2−.1
4−.1
1−.1
1−.0
2−.1
8.1
7.0
6.0
3.0
5.0
939 A
ppea
rs t
o ga
in p
leas
ure
or
sati
sfac
tion
by
bei
ng
sadis
tic
or a
ggre
ssiv
e to
war
d o
ther
s (w
het
her
con
scio
usl
y or
un
con
scio
usl
y).
.49
−.1
2−.1
5.0
6−.0
7−.1
2−.0
1−.0
1.2
7−.0
8−.0
7−.1
9.1
3−.1
6−.2
5.0
265 A
ttem
pts
to
dom
inat
e a
sign
ifica
nt
oth
er
(e.g
., s
pou
se, lo
ver,
fam
ily
mem
ber
) th
rou
gh
viol
ence
or
inti
mid
atio
n.
.41
−.1
0−.0
5−.0
4−.0
6−.0
4−.0
2.1
0.0
7−.1
3−.1
6−.1
6−.0
3.0
8−.2
5−.0
3194 T
ends
to b
e m
anip
ula
tive
..4
0−.1
6.0
0−.0
1.0
3.0
4.0
4.1
1−.0
2.0
1−.2
6.1
0.0
9.1
0−.1
2−.1
8134 T
ends
to a
ct im
pu
lsiv
ely
(e.g
., a
cts
wit
hou
t fo
reth
ough
t or
con
cern
for
co
nse
quen
ces)
..3
9−.1
5−.0
7.0
2−.0
6.2
9−.0
9−.1
8−.1
5−.1
0−.1
0.2
7−.1
4.1
3−.0
2−.0
1147 T
ends
to a
bu
se d
rugs
or
alco
hol
..3
9−.0
8−.1
3−.0
5.0
2.2
1−.0
8−.0
9−.0
3.0
8−.0
4.1
5−.1
5.0
3.0
3−.0
171 T
ends
to s
eek t
hri
lls,
nov
elty
, ex
cite
men
t,
etc.
; ap
pea
rs t
o re
quir
e a
hig
h lev
el o
f st
imu
lati
on.
.39
.09
.06
−.0
1−.0
2.1
3.1
8−.1
3−.0
7−.0
9−.0
9.1
9−.2
8.1
6.1
3.0
2
293
18 T
ends
to s
tir
up c
onflic
t or
an
imos
ity
bet
wee
n o
ther
peo
ple
(e.
g., m
ay p
ortr
ay
a si
tuat
ion
dif
fere
ntl
y to
dif
fere
nt
peo
ple
, le
adin
g th
em t
o fo
rm c
ontr
adic
tory
vie
ws
or
wor
k a
t cr
oss
pu
rpos
es).
.38
−.0
3−.0
5−.1
1−.1
3.0
3.0
6.1
4−.1
5−.0
9.0
0.1
4.3
2−.0
6−.0
9.0
243 T
ends
to s
eek p
ower
or
influ
ence
ove
r ot
her
s (w
het
her
in
ben
efici
al o
r des
tru
ctiv
e w
ays)
..3
8.0
1−.0
3−.0
4.0
5−.0
1.3
4.0
6.0
9−.0
4−.1
1−.2
3.0
4.0
2−.0
9−.1
652 H
as lit
tle
empat
hy;
see
ms
un
able
or
un
willin
g to
un
der
stan
d o
r re
spon
d t
o ot
her
s’ n
eeds
or fee
lin
gs.
.32
−.1
6−.1
6.1
5.0
7−.1
9.2
5.0
0−.1
9.0
4−.0
3−.1
1−.0
2−.0
8−.1
9−.0
3101 G
ener
ally
fin
ds
con
ten
tmen
t an
d
hap
pin
ess
in life’
s ac
tivi
ties
..0
4.7
3−.0
1.0
6.0
5−.0
3−.0
8.0
2−.1
5−.1
3.0
0−.1
1.0
7.1
0.0
3.0
3183 I
s psy
chol
ogic
ally
in
sigh
tfu
l; is
able
to
un
der
stan
d s
elf an
d o
ther
s in
su
btl
e an
d
soph
isti
cate
d w
ays.
−.0
9.6
2−.0
2−.0
8.0
7.0
2−.1
0−.0
2.2
2−.0
2.0
0.0
7−.0
1−.0
2−.0
6−.0
789 A
ppea
rs t
o h
ave
com
e to
ter
ms
wit
h
pai
nfu
l ex
per
ien
ces
from
th
e pas
t; h
as
fou
nd m
ean
ing
in, an
d g
row
n fro
m s
uch
ex
per
ien
ces.
.01
.61
−.0
5−.0
2−.0
3−.0
8−.1
2.0
9.0
3−.0
6.0
9−.0
6.0
2.0
8−.0
2.1
2111 H
as t
he
capac
ity
to r
ecog
niz
e al
tern
ativ
e vi
ewpoi
nts
, ev
en in
mat
ters
th
at s
tir
up
stro
ng
feel
ings
.−.0
3.6
0−.0
3−.0
9.0
7−.0
7−.1
2.0
7.1
4−.1
1.1
0.0
4−.1
1−.0
1.0
6−.0
4196 F
inds
mea
nin
g an
d s
atis
fact
ion
in
th
e pu
rsu
it o
f lo
ng-
term
goa
ls a
nd a
mbit
ion
s.−.1
0.5
8.0
4−.0
5.0
9−.0
2.0
6−.1
4−.1
0−.0
5.0
0−.1
2.1
0−.0
5.0
4−.0
863 I
s ab
le t
o as
sert
him
/h
erse
lf e
ffec
tive
ly
and a
ppro
pri
atel
y w
hen
nec
essa
ry.
−.0
5.5
8.0
9−.0
3.0
8.0
4.1
1−.0
8.0
2.1
3−.1
6.0
1−.0
9.0
0−.1
3.0
568 H
as a
goo
d s
ense
of h
um
or.
−.0
8.5
7−.0
9.0
3−.1
4−.0
5−.0
4−.0
4.0
6.0
4−.0
6.0
8−.2
0−.0
2.0
3−.0
382 I
s ca
pab
le o
f h
eari
ng
info
rmat
ion
th
at is
emot
ion
ally
th
reat
enin
g (i.e
., t
hat
ch
alle
nge
s ch
eris
hed
bel
iefs
, per
cepti
ons,
an
d s
elf-
per
cepti
ons)
an
d c
an u
se a
nd b
enefi
t fr
om it.
−.0
8.5
6−.0
1−.1
3.0
3−.0
2−.0
7.0
0.1
1−.1
0.0
7.1
0−.1
1.0
2.0
2−.0
2121 I
s cr
eati
ve; is
able
to
see
thin
gs o
r ap
pro
ach
pro
ble
ms
in n
ovel
way
s.−.0
8.5
6−.0
4−.0
7.1
1.1
2.0
6−.0
8.0
6−.0
4−.0
8.1
4.0
7−.0
9.0
5−.0
619 E
njo
ys c
hal
len
ges;
tak
es p
leas
ure
in
ac
com
plish
ing
thin
gs.
−.0
2.5
6.1
5−.0
5.0
7.0
8.1
3−.1
2−.0
4−.0
9.0
0−.1
3−.0
5−.0
1.0
6−.1
3106 T
ends
to e
xpre
ss e
mot
ion
appro
pri
ate
in q
ual
ity
and in
ten
sity
to
the
situ
atio
n a
t h
and.
.00
.54
−.0
1−.1
3−.1
5−.2
0−.0
9−.0
2−.0
3−.0
6.0
2.1
2.0
8−.0
4−.0
4.0
6
continued

294
SW
AP-I
I F
acto
rs
SW
AP-I
I It
ems
12
34
56
78
910
11
12
13
14
15
16
32 I
s ca
pab
le o
f su
stai
nin
g m
ean
ingf
ul
rela
tion
ship
s ch
arac
teri
zed b
y ge
nu
ine
inti
mac
y an
d c
arin
g.−.0
7.5
4−.0
9.0
0−.1
6−.0
1−.0
4.0
3−.0
3−.0
6−.0
9−.1
1−.0
8−.1
6.1
8−.0
82 I
s ab
le t
o u
se h
is/h
er t
alen
ts, ab
ilit
ies,
an
d e
ner
gy e
ffec
tive
ly a
nd p
rodu
ctiv
ely.
−.0
6.5
3.0
9−.0
9.1
5.0
5.0
8−.0
9−.0
8−.0
7−.0
7−.2
0−.0
4.0
5.1
2−.0
592 I
s ar
ticu
late
; ca
n e
xpre
ss s
elf w
ell in
w
ords.
−.1
4.5
3.0
5−.1
8.0
2−.0
1.0
4−.0
4.2
4.0
0−.0
4.1
2.0
2.0
0−.1
3−.1
255 F
inds
mea
nin
g an
d fu
lfillm
ent
in g
uid
ing,
m
ento
rin
g, o
r n
urt
uri
ng
oth
ers.
.00
.52
−.0
3−.0
7−.1
3−.1
2−.1
7.0
2.0
1.0
1−.1
1−.2
0.0
9−.0
9.1
0−.0
259 I
s em
pat
hic
; is
sen
siti
ve a
nd r
espon
sive
to
oth
er p
eople
s’ n
eeds
and fee
lin
gs.
−.0
4.5
1−.1
2−.0
7−.0
9−.0
6−.2
1.0
0.0
5−.0
6−.0
2−.0
7.0
4−.1
0.2
7−.1
251 T
ends
to b
e liked
by
oth
er p
eople
.−.0
7.4
9−.1
0−.1
0−.0
7−.1
3−.0
7−.0
2.0
1−.0
8−.1
3−.0
7−.1
8.0
3.2
5.0
495 A
ppea
rs c
omfo
rtab
le a
nd a
t ea
se in
soc
ial
situ
atio
ns.
.0
8.4
7−.1
2−.0
9.0
4−.0
9.1
1.0
4−.0
6−.0
3−.2
1−.0
3−.2
0.2
0.0
2.0
494 H
as a
n a
ctiv
e an
d s
atis
fyin
g se
x life
..0
0.4
5−.1
3.0
0−.0
7−.0
3.1
0.1
6−.1
0−.0
6.0
2−.1
2−.1
8.2
5−.0
1.0
4179 T
ends
to b
e en
erge
tic
and o
utg
oin
g.−.0
1.4
3.0
0.0
9−.0
3.0
3.1
5−.1
2.0
0−.1
6−.2
7.0
4−.2
7.1
4.0
6−.0
3120 H
as m
oral
an
d e
thic
al s
tan
dar
ds
and
stri
ves
to liv
e u
p t
o th
em.
−.1
9.4
1.2
0−.0
3.0
1−.1
2−.1
7−.0
9.0
1−.0
1.0
2−.1
3.0
8−.2
6.0
5−.1
0175 T
ends
to b
e co
nsc
ien
tiou
s an
d
resp
onsi
ble
.−.1
6.4
0.3
2−.1
0.1
1−.1
0−.1
7−.1
5.0
3−.0
2.0
5−.2
2.0
3−.0
6.0
2−.0
937 F
inds
mea
nin
g in
bel
ongi
ng
and
con
trib
uti
ng
to a
lar
ger
com
mu
nit
y (e
.g.,
orga
niz
atio
n, n
eigh
bor
hoo
d, ch
urc
h).
−.1
2.4
0.0
3.0
7−.1
3−.1
4−.0
4−.0
5−.1
1−.0
8−.1
3−.1
2.1
9−.2
4.1
4.0
1163 A
ppea
rs t
o w
ant
to “
pu
nis
h”
self;
crea
tes
situ
atio
ns
that
lea
d t
o u
nh
appin
ess,
or
act
ivel
y av
oids
oppor
tun
itie
s fo
r ple
asu
re
and g
rati
fica
tion
..0
1−.2
8−.0
4−.1
7.0
5−.1
1−.2
0−.1
0.2
7.1
5−.2
1−.0
1−.0
6−.1
6.1
5.0
536 T
ends
to fee
l h
elple
ss, pow
erle
ss, or
at
the
mer
cy o
f fo
rces
ou
tsid
e h
is/h
er c
ontr
ol.
−.1
4−.2
7−.0
3−.0
2−.2
5−.1
3−.2
2.1
4−.0
3.1
3.0
4−.0
7−.1
2−.1
4.0
3.0
154 T
ends
to fee
l s/
he
is in
adeq
uat
e, in
feri
or,
or a
fai
lure
.−.1
2−.2
5−.0
6−.1
8−.2
4−.1
0−.1
1−.1
9.0
8.2
2.2
3.0
1−.1
1−.0
7.2
0−.0
2167 I
s si
mu
ltan
eou
sly
nee
dy
of, an
d
reje
ctin
g to
war
d, ot
her
s (e
.g., c
rave
s in
tim
acy
and c
arin
g, b
ut
ten
ds
to r
ejec
t it
w
hen
off
ered
).−.1
7−.2
4−.0
3−.2
1.1
9.0
2−.0
4−.0
5.0
7.1
0−.0
5−.0
4.1
5.0
9−.2
0.0
7
TA
BLE
2.
Con
tin
ued

295
192 T
ends
to b
e ov
erly
con
cern
ed w
ith
ru
les,
pro
cedu
res,
ord
er, or
gan
izat
ion
, sc
hed
ule
s,
etc.
.04
−.1
1.6
7.0
3.0
3−.0
4−.0
8−.0
2.0
0−.1
3−.0
2−.0
8.0
6−.0
3−.0
3−.0
6123 T
ends
to a
dh
ere
rigi
dly
to
dai
ly r
outi
nes
an
d b
ecom
e an
xiou
s or
un
com
fort
able
wh
en
they
are
alt
ered
.−.0
2−.1
1.6
2.0
1.1
0.0
3.0
4.2
2−.0
3−.0
8.1
2−.1
3−.0
4.0
2−.0
1.0
6173 T
ends
to b
ecom
e ab
sorb
ed in
det
ails
, of
ten
to
the
poi
nt
that
s/h
e m
isse
s w
hat
is
sign
ifica
nt.
−.0
6−.0
6.6
1.1
9−.0
3−.0
6−.0
9.0
4−.1
1−.1
0−.0
6.0
9−.0
1−.0
5−.0
2−.0
3174 E
xpec
ts s
elf to
be
“per
fect
” (e
.g., in
ap
pea
ran
ce, ac
hie
vem
ents
, per
form
ance
, et
c.).
−.1
6−.0
1.4
5−.3
4.0
7.0
1.1
8−.1
3−.0
3−.1
1−.0
1−.0
9−.0
7−.0
6.1
1.1
728 T
ends
to b
e pre
occu
pie
d w
ith
con
cern
s ab
out
dir
t, c
lean
lin
ess,
con
tam
inat
ion
, et
c.
(e.g
., d
rin
kin
g fr
om a
not
her
per
son
’s g
lass
, si
ttin
g on
pu
blic
toilet
sea
ts, et
c.).
−.0
1−.0
7.4
4.0
6−.0
2−.0
4−.0
3.2
4.1
2−.0
2.0
2−.0
3.0
3.0
1−.0
6.1
8200 T
ends
to r
um
inat
e; m
ay d
wel
l on
pro
ble
ms,
rep
lay
con
vers
atio
ns
in h
is/h
er
min
d, bec
ome
pre
occu
pie
d w
ith
th
ough
ts
abou
t w
hat
cou
ld h
ave
bee
n, et
c.−.2
1−.1
2.4
0.0
7−.2
7−.0
5−.0
6−.0
2.0
1.0
9.1
3−.0
3−.0
5.0
5.0
1−.0
66 I
s tr
ouble
d b
y re
curr
ent
obse
ssio
nal
th
ough
ts t
hat
s/h
e ex
per
ien
ces
as in
tru
sive
.−.0
7−.1
1.3
8.1
3−.1
6.1
3−.0
2.1
3.1
6.1
2−.0
3−.1
6−.1
1−.0
8.1
4.0
866 I
s ex
cess
ivel
y dev
oted
to
wor
k a
nd
pro
du
ctiv
ity
to t
he
det
rim
ent
of lei
sure
an
d
rela
tion
ship
s..0
3.1
7.3
5−.2
0.1
8−.0
2−.0
1−.1
7−.1
1.0
7.0
4−.1
3.0
2.0
1.0
7.0
9164 T
ends
to b
e se
lf-r
igh
teou
s or
mor
alis
tic.
−.0
3.0
1.3
2.0
6−.0
4−.1
5.1
3−.0
6−.0
3.0
4−.1
5−.0
6.2
2−.2
0−.2
7−.0
9180 H
as t
rou
ble
mak
ing
dec
isio
ns;
ten
ds
to
be
indec
isiv
e or
to
vaci
llat
e w
hen
fac
ed w
ith
ch
oice
s.−.1
7−.2
4.2
9−.0
1−.0
5−.2
3−.1
7.1
5−.0
6−.0
9.0
9.1
6−.0
4.1
0.1
2−.0
467 T
ends
to b
e st
ingy
an
d w
ith
hol
din
g (e
.g.,
of t
ime,
mon
ey, af
fect
ion
, id
eas)
..1
4.0
1.2
7.0
0.1
4−.1
6.0
2.0
8−.0
6.0
3.0
3−.1
2.1
1.0
7−.1
4.1
7130 R
easo
nin
g pro
cess
es o
r per
ceptu
al
exper
ien
ces
seem
odd a
nd idio
syn
crat
ic (e.
g.,
may
mak
e se
emin
gly
arbit
rary
in
fere
nce
s;
may
see
hid
den
mes
sage
s or
spec
ial
mea
nin
gs in
ord
inar
y ev
ents
).−.0
2−.1
5.1
5.5
7.0
1.0
7−.0
6−.0
1.1
0−.0
8.0
2−.0
3.0
4.0
0−.0
1.0
7
continued
296
SW
AP-I
I F
acto
rs
SW
AP-I
I It
ems
12
34
56
78
910
11
12
13
14
15
16
145 T
hou
ght
pro
cess
es o
r sp
eech
ten
d t
o be
circ
um
stan
tial
, va
gue,
ram
blin
g, d
igre
ssiv
e,
etc.
(e.
g., m
ay b
e u
ncl
ear
wh
eth
er s
/h
e is
bei
ng
met
aph
oric
al o
r w
het
her
th
inkin
g is
co
nfu
sed o
r pec
uliar
).−.0
3−.1
1.0
6.5
5.0
4.0
0−.0
4−.0
2.0
6−.0
9.0
1.1
4.1
1.0
2.1
8−.0
2125 A
ppea
ran
ce o
r m
ann
er s
eem
s od
d o
r pec
uliar
(e.
g., gr
oom
ing,
hyg
ien
e, p
ostu
re,
eye
con
tact
, sp
eech
rh
yth
ms,
etc
. se
em
som
ehow
str
ange
or
“off
”).
−.0
1−.1
2.0
9.5
1.0
1−.0
6−.0
4.0
7.0
9−.0
3.1
3.0
8−.0
1−.0
7−.0
1.0
575 T
ends
to t
hin
k in
con
cret
e te
rms
and
inte
rpre
t th
ings
in
ove
rly
lite
ral w
ays;
has
lim
ited
abilit
y to
appre
ciat
e m
etap
hor
, an
alog
y, o
r n
uan
ce.
−.0
1−.1
4−.0
1.4
9.0
2−.0
4−.0
6−.1
0−.2
3−.0
7−.0
3−.0
9−.0
9−.0
8.0
7.1
029 H
as d
ifficu
lty
mak
ing
sen
se o
f ot
her
peo
ple
’s b
ehav
ior;
ten
ds
to m
isu
nder
stan
d,
mis
inte
rpre
t, o
r be
con
fuse
d b
y ot
her
s’
acti
ons
and r
eact
ion
s.−.2
4−.1
2−.0
4.4
0−.0
5.0
0−.0
2−.1
5−.2
3−.1
0.1
4−.0
6−.0
8−.0
1−.1
7.0
544 W
hen
dis
tres
sed, per
cepti
on o
f re
alit
y ca
n b
ecom
e gr
ossl
y im
pai
red (e.
g., th
inkin
g m
ay s
eem
del
usi
onal
)..0
3−.1
6−.0
9.3
8−.1
0.3
3−.0
7.0
2.0
5−.0
3−.0
1−.1
3.0
1−.1
1.0
5.0
5136 T
ends
to b
elie
ve in
su
per
nat
ura
l,
par
anor
mal
, or
su
per
stit
iou
s ph
enom
ena
or
to b
e dra
wn
to
“alt
ern
ativ
e” b
elie
f sy
stem
s (e
.g., a
stro
logy
, ta
rot,
cry
stal
s, p
sych
ics,
au
ras)
..0
5.0
0−.0
6.3
7−.0
4.1
1.1
4.1
2.2
5.1
0−.1
4−.1
1.1
7−.1
1.1
5.0
0146 T
ends
to e
lici
t bor
edom
in
oth
ers
(e.g
.,
may
tal
k in
cess
antl
y, w
ith
out
feel
ing,
or
abou
t in
con
sequ
enti
al m
atte
rs).
−.0
5−.0
9.2
4.3
4−.0
2−.1
7.0
1.1
3−.0
7.0
9−.0
3−.0
3−.0
3.0
3.0
1−.0
391 I
s se
lf-c
riti
cal; s
ets
un
real
isti
cally
hig
h
stan
dar
ds
for
self a
nd is
into
lera
nt
of o
wn
h
um
an d
efec
ts.
−.1
4−.0
8.2
2−.3
4−.0
3.0
2−.0
1−.1
9.0
5.0
3.1
6−.0
8−.0
9−.1
9.1
8.0
6118 H
as d
ifficu
lty
mai
nta
inin
g at
ten
tion
an
d foc
us
on t
asks;
is
easi
ly d
istr
acte
d b
y si
ghts
, so
un
ds,
un
rela
ted t
hou
ghts
, or
oth
er
com
pet
ing
stim
uli.
−.1
1−.0
9.0
5.3
3−.0
6.0
2−.0
5.1
6.0
1−.0
3−.1
5.2
4−.1
6−.0
7.1
6.0
2
TA
BLE
2.
Con
tin
ued

297
87 S
ense
of id
enti
ty r
evol
ves
arou
nd
a “c
ause
,” m
ovem
ent,
or
label
(e.
g.,
adu
lt c
hild o
f al
coh
olic
, ad
ult
su
rviv
or,
envi
ron
men
talist
, bor
n-a
gain
Ch
rist
ian
, et
c.); m
ay b
e dra
wn
to
extr
eme
or a
ll-
enco
mpas
sin
g bel
ief sy
stem
s.−.0
2.0
1.1
0.3
0−.1
8−.0
5.0
5−.0
8.0
5.0
6−.1
5.0
9.2
0−.2
0.0
5−.0
472 T
ends
to p
erce
ive
thin
gs in
glo
bal
an
d
impre
ssio
nis
tic
way
s (e
.g., m
isse
s det
ails
, gl
osse
s ov
er in
con
sist
enci
es, m
ispro
nou
nce
s n
ames
).−.1
5−.1
5−.1
5.2
6−.0
5.0
3.0
2−.0
5−.2
4−.1
3−.1
4−.1
3−.1
3.0
9.1
5.0
1184 V
erbal
sta
tem
ents
see
m in
con
gru
ous
wit
h a
ccom
pan
yin
g af
fect
, or
in
con
gru
ous
wit
h a
ccom
pan
yin
g n
onve
rbal
mes
sage
s.−.0
8−.1
8.0
4.2
5.2
1.0
1−.0
6−.1
1.1
6−.0
8−.1
9.0
4.1
1.0
2.0
5.0
8144 T
ends
to s
ee s
elf as
log
ical
an
d
rati
onal
, u
nin
flu
ence
d b
y em
otio
n; pre
fers
to
oper
ate
as if em
otio
ns
wer
e ir
rele
van
t or
in
con
sequ
enti
al.
−.0
9.0
0.2
0−.0
1.5
2−.0
9.0
9−.0
4−.0
8.1
0−.1
7−.1
0.0
1−.0
8−.0
4−.0
7159 T
ends
to d
eny
or d
isav
ow o
wn
nee
d
for
nu
rtu
ran
ce, ca
rin
g, c
omfo
rt, et
c. (e.
g.,
may
reg
ard s
uch
nee
ds
as w
eakn
ess,
avo
id
dep
endin
g on
oth
ers
or a
skin
g fo
r h
elp, et
c.)
−.0
2.0
1.0
2−.0
7.4
6−.0
3−.0
3−.2
0.0
0.0
8−.1
2−.0
1−.1
2−.1
6.1
0−.0
1141 I
s in
vest
ed in
see
ing
and p
ortr
ayin
g se
lf a
s em
otio
nal
ly s
tron
g, u
ntr
ouble
d, an
d
emot
ion
ally
in
con
trol
, des
pit
e cl
ear
evid
ence
of
un
der
lyin
g in
secu
rity
, an
xiet
y, o
r dis
tres
s.−.1
5−.0
9.0
9−.1
8.4
4.0
2.1
7−.0
4−.0
4−.1
8−.1
8−.0
5−.0
2−.0
6.0
2−.0
6126 A
ppea
rs t
o h
ave
a lim
ited
or
con
stri
cted
ra
nge
of em
otio
ns.
.03
−.1
6.0
2.2
1.3
9−.1
2−.1
6.0
2−.1
3.1
3.1
1−.1
6−.0
3.0
3.0
2−.0
1104 A
ppea
rs t
o h
ave
litt
le n
eed for
hu
man
co
mpan
y or
con
tact
; is
em
otio
nal
ly d
etac
hed
or
in
dif
fere
nt.
.21
.08
.03
.32
.39
−.0
9−.0
8−.0
7−.0
7.2
6.2
1−.0
5.0
3.0
1−.0
3.0
373 T
ends
to “
cata
stro
ph
ize”
; is
pro
ne
to s
ee
pro
ble
ms
as d
isas
trou
s, u
nso
lvab
le, et
c.−.1
0−.2
0.1
5−.0
7−.3
8.0
9−.0
5.1
6−.0
6.1
9.0
7−.0
8−.0
4.0
0−.0
7−.0
374 E
xpre
sses
em
otio
n in
exa
gger
ated
an
d
thea
tric
al w
ays.
−.0
5−.0
6−.0
5.1
6−.3
7.2
0.1
4.0
9−.0
9−.0
1−.1
9−.0
4.0
5.1
5−.0
8−.0
3119 T
ends
to b
e in
hib
ited
or
con
stri
cted
; h
as d
ifficu
lty
allo
win
g se
lf t
o ac
kn
owle
dge
or
expre
ss w
ish
es a
nd im
pu
lses
.−.1
3−.1
0.0
4−.0
4.3
6−.2
2−.1
7−.0
1−.0
3−.0
4.2
4−.1
4.0
0−.0
9.1
8−.0
1
continued

298
SW
AP-I
I F
acto
rs
SW
AP-I
I It
ems
12
34
56
78
910
11
12
13
14
15
16
100 T
ends
to t
hin
k in
abst
ract
an
d
inte
llec
tual
ized
ter
ms,
eve
n in
mat
ters
of
per
son
al im
por
t.−.1
2.1
5.2
1.1
3.3
1−.0
6.1
6.0
2.0
7.0
0−.0
3.0
7.1
4−.1
0.0
4−.1
8152 T
ends
to r
epre
ss o
r “f
orge
t” d
istr
essi
ng
even
ts, or
dis
tort
mem
orie
s of
dis
tres
sin
g ev
ents
bey
ond r
ecog
nit
ion
.−.2
4−.0
5−.0
8.1
3.2
9.0
0−.1
1.1
0.0
0−.1
3−.1
8.0
6.0
9−.0
5.0
7.2
377 T
ends
to b
e n
eedy
or d
epen
den
t.−.1
8−.2
4−.0
7−.0
7−.2
7−.0
8−.1
0.2
1−.2
1−.0
4−.0
4−.0
4.1
0.2
4.1
6−.1
3131 A
ppea
rs c
onflic
ted a
bou
t ex
per
ien
cin
g ple
asu
rable
em
otio
ns;
ten
ds
to in
hib
it
exci
tem
ent,
joy
, pri
de,
etc
.−.1
4−.1
6−.0
2−.1
3.2
3−.2
0−.1
3−.0
1.1
5.0
7.0
2−.0
8−.0
4−.0
9.0
9.0
95 T
ends
to b
e em
otio
nal
ly in
tru
sive
(e.
g.,
may
not
res
pec
t ot
her
peo
ple
’s n
eeds
for
auto
nom
y, p
riva
cy, et
c.).
.21
−.0
4.0
6.0
4−.2
3.0
1.0
9.0
6−.1
0−.0
9−.2
2−.0
6−.0
3.0
3−.1
6−.1
258 H
as lit
tle
or n
o in
tere
st in
sex
..0
4−.0
5.0
9.0
3.1
6−.0
7−.0
3.0
4−.0
9.1
5.1
6−.0
6.0
3−.1
6.0
4.1
6191 E
mot
ion
s te
nd t
o ch
ange
rap
idly
an
d
un
pre
dic
tably
..0
2−.1
3−.0
6−.0
4−.0
6.5
9−.0
3.0
3−.0
5.0
0−.1
5.1
1.0
6.0
7.0
5−.0
212 E
mot
ion
s te
nd t
o sp
iral
ou
t of
con
trol
, le
adin
g to
ext
rem
es o
f an
xiet
y, s
adn
ess,
ra
ge, et
c.−.1
0−.1
5−.0
8−.1
0−.2
7.5
8.0
0.0
1−.1
4.0
7−.1
1−.0
5−.0
6−.0
4−.0
5.0
6157 T
ends
to b
ecom
e ir
rati
onal
wh
en
stro
ng
emot
ion
s ar
e st
irre
d u
p; m
ay s
how
a
sign
ifica
nt
dec
lin
e fr
om c
ust
omar
y le
vel of
fu
nct
ion
ing.
−.1
5−.1
3−.0
1.2
0−.1
5.4
9−.1
8.0
2−.0
3−.0
5−.1
6−.0
4−.0
3−.0
6−.1
8.0
8138 T
ends
to e
nte
r al
tere
d, dis
soci
ated
st
ates
wh
en d
istr
esse
d (e.
g., th
e se
lf o
r w
orld
fe
els
stra
nge
, u
nre
al, or
un
fam
ilia
r).
−.0
2−.0
2−.1
5.1
6.1
4.4
5−.0
4.2
3.2
5.0
5.0
8−.0
8.1
5−.0
5.2
4.0
1185 I
s pro
ne
to in
ten
se a
nge
r, o
ut
of
pro
por
tion
to
the
situ
atio
n a
t h
and (e.
g., h
as
rage
epis
odes
)..1
8−.1
1−.1
0−.0
1.0
0.4
5−.1
3−.0
4.0
1−.0
2−.0
3−.0
9.0
4−.0
4−.4
2−.0
5109 T
ends
to e
nga
ge in
sel
f-m
uti
lati
ng
beh
avio
r (e
.g., s
elf-
cutt
ing,
sel
f-bu
rnin
g,
etc.
)..0
4−.1
2−.1
1−.0
7.0
9.4
3−.0
8.0
1.0
8.1
0−.0
3−.0
4.1
2.0
2.1
3.0
6
TA
BLE
2.
Con
tin
ued

299
64 M
ood t
ends
to c
ycle
ove
r in
terv
als
of
wee
ks
or m
onth
s bet
wee
n e
xcit
ed a
nd
dep
ress
ed s
tate
s (h
igh
pla
cem
ent
implies
bip
olar
moo
d d
isor
der
).−.0
9.0
0−.0
3.0
7−.0
5.3
9.1
3−.0
1−.0
4−.0
7−.0
9.2
0.0
1−.0
5.2
3−.0
478 T
ends
to e
xpre
ss a
nge
r in
pas
sive
an
d
indir
ect
way
s (e
.g., m
ay m
ake
mis
takes
, pro
cras
tin
ate,
for
get,
bec
ome
sulk
y, e
tc.).
−.1
5−.2
4−.1
7−.1
0.0
9−.3
5−.0
8.1
4−.0
3−.1
1−.0
9.0
7−.0
8−.0
1.0
5−.0
9199 T
ends
to b
e pas
sive
an
d u
nas
sert
ive.
−.0
4−.2
6.0
0.0
0.0
1−.3
5−.3
3.0
5−.0
8−.0
4.2
0−.0
7−.0
4.0
7.2
5−.1
8117 I
s u
nab
le t
o so
oth
e or
com
fort
him
/h
erse
lf w
ith
out
the
hel
p o
f an
oth
er p
erso
n
(i.e
., h
as d
ifficu
lty
regu
lati
ng
own
em
otio
ns)
.−.1
8−.2
7−.0
3−.0
9−.2
4.2
8−.0
9.0
5−.1
2−.0
5−.1
3−.1
1−.0
4.2
6−.0
5.0
59 W
hen
upse
t, h
as t
rou
ble
per
ceiv
ing
bot
h p
osit
ive
and n
egat
ive
qual
itie
s in
th
e sa
me
per
son
at
the
sam
e ti
me
(e.g
., m
ay
see
oth
ers
in b
lack
or
wh
ite
term
s, s
hift
sudden
ly fro
m s
eein
g so
meo
ne
as c
arin
g to
see
ing
him
/h
er a
s m
alev
olen
t an
d
inte
nti
onal
ly h
urt
ful, e
tc.).
−.2
2−.2
3−.0
7.0
3−.0
7.2
8.0
8−.0
2−.1
9−.1
0−.0
8−.0
1.0
8.0
0−.2
2.0
793 S
eem
s n
aïve
or
inn
ocen
t; a
ppea
rs t
o kn
ow les
s ab
out
the
way
s of
th
e w
orld
th
an
mig
ht
be
expec
ted g
iven
his
/h
er in
tellig
ence
or
bac
kgr
oun
d.
−.0
8.0
6.0
5.1
7−.0
3−.2
7−.0
7−.1
1−.2
4−.1
9.2
1.0
4.1
6.0
5.1
7.1
2161 T
ends
to d
eny,
dis
avow
, or
squ
elch
h
is/h
er o
wn
rea
list
ic h
opes
, dre
ams,
or
des
ires
to
pro
tect
aga
inst
an
tici
pat
ed
dis
appoi
ntm
ent
(wh
eth
er c
onsc
iou
sly
or
un
con
scio
usl
y).
−.1
6−.1
2−.0
5−.1
2.2
0−.2
6−.0
5.0
1.2
0.1
0.0
6.1
5−.0
2−.1
0−.0
1.0
4166 T
ends
to a
lter
nat
e bet
wee
n
un
der
con
trol
an
d o
verc
ontr
ol o
f n
eeds
and
impu
lses
(e.
g., so
met
imes
act
s on
des
ires
im
pu
lsiv
ely
wh
ile
at o
ther
tim
es d
enyi
ng
them
en
tire
ly).
−.0
6−.1
6.1
1−.0
5.0
3.2
3−.1
0−.1
4.0
4−.1
3−.2
1.1
1−.0
6−.0
3.0
5.1
776 M
anag
es t
o el
icit
in
oth
ers
feel
ings
si
milar
to
thos
e s/
he
is e
xper
ien
cin
g (e
.g.,
wh
en a
ngr
y, a
cts
in s
uch
a w
ay a
s to
pro
voke
ange
r in
oth
ers;
wh
en a
nxi
ous,
ac
ts in
su
ch a
way
as
to in
du
ce a
nxi
ety
in
oth
ers)
.−.0
1−.1
7−.1
0.0
0.0
7.2
3−.0
3−.0
1−.0
9.0
1−.1
7.0
2.1
0.0
1−.1
3−.0
6
continued
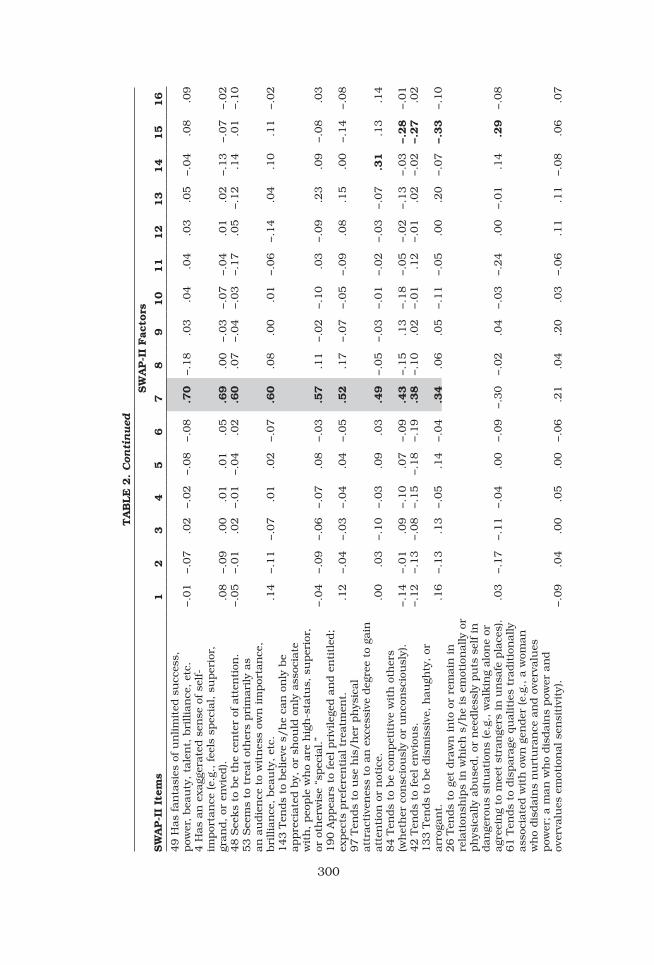
300
SW
AP-I
I F
acto
rs
SW
AP-I
I It
ems
12
34
56
78
910
11
12
13
14
15
16
49 H
as fan
tasi
es o
f u
nlim
ited
su
cces
s,
pow
er, bea
uty
, ta
len
t, b
rillia
nce
, et
c.−.0
1−.0
7.0
2−.0
2−.0
8−.0
8.7
0−.1
8.0
3.0
4.0
4.0
3.0
5−.0
4.0
8.0
94 H
as a
n e
xagg
erat
ed s
ense
of se
lf-
impor
tan
ce (e.
g., fe
els
spec
ial, s
uper
ior,
gr
and, or
en
vied
)..0
8−.0
9.0
0.0
1.0
1.0
5.6
9.0
0−.0
3−.0
7−.0
4.0
1.0
2−.1
3−.0
7−.0
248 S
eeks
to b
e th
e ce
nte
r of
att
enti
on.
−.0
5−.0
1.0
2−.0
1−.0
4.0
2.6
0.0
7−.0
4−.0
3−.1
7.0
5−.1
2.1
4.0
1−.1
053 S
eem
s to
tre
at o
ther
s pri
mar
ily
as
an a
udie
nce
to
wit
nes
s ow
n im
por
tan
ce,
bri
llia
nce
, bea
uty
, et
c..1
4−.1
1−.0
7.0
1.0
2−.0
7.6
0.0
8.0
0.0
1−.0
6−.1
4.0
4.1
0.1
1−.0
2143 T
ends
to b
elie
ve s
/h
e ca
n o
nly
be
appre
ciat
ed b
y, o
r sh
ould
on
ly a
ssoc
iate
w
ith
, peo
ple
wh
o ar
e h
igh
-sta
tus,
su
per
ior,
or
oth
erw
ise
“spec
ial.”
−.0
4−.0
9−.0
6−.0
7.0
8−.0
3.5
7.1
1−.0
2−.1
0.0
3−.0
9.2
3.0
9−.0
8.0
3190 A
ppea
rs t
o fe
el p
rivi
lege
d a
nd e
nti
tled
; ex
pec
ts p
refe
ren
tial
tre
atm
ent.
.12
−.0
4−.0
3−.0
4.0
4−.0
5.5
2.1
7−.0
7−.0
5−.0
9.0
8.1
5.0
0−.1
4−.0
897 T
ends
to u
se h
is/h
er p
hys
ical
at
trac
tive
nes
s to
an
exc
essi
ve d
egre
e to
gai
n
atte
nti
on o
r n
otic
e..0
0.0
3−.1
0−.0
3.0
9.0
3.4
9−.0
5−.0
3−.0
1−.0
2−.0
3−.0
7.3
1.1
3.1
484 T
ends
to b
e co
mpet
itiv
e w
ith
oth
ers
(wh
eth
er c
onsc
iou
sly
or u
nco
nsc
iou
sly)
.−.1
4−.0
1.0
9−.1
0.0
7−.0
9.4
3−.1
5.1
3−.1
8−.0
5−.0
2−.1
3−.0
3−.2
8−.0
142 T
ends
to fee
l en
viou
s.−.1
2−.1
3−.0
8−.1
5−.1
8−.1
9.3
8−.1
0.0
2−.0
1.1
2−.0
1.0
2−.0
2−.2
7.0
2133 T
ends
to b
e dis
mis
sive
, h
augh
ty, or
ar
roga
nt.
.16
−.1
3.1
3−.0
5.1
4−.0
4.3
4.0
6.0
5−.1
1−.0
5.0
0.2
0−.0
7−.3
3−.1
026 T
ends
to g
et d
raw
n in
to o
r re
mai
n in
re
lati
onsh
ips
in w
hic
h s
/h
e is
em
otio
nal
ly o
r ph
ysic
ally
abu
sed, or
nee
dle
ssly
pu
ts s
elf in
dan
gero
us
situ
atio
ns
(e.g
., w
alkin
g al
one
or
agre
ein
g to
mee
t st
ran
gers
in
un
safe
pla
ces)
..0
3−.1
7−.1
1−.0
4.0
0−.0
9−.3
0−.0
2.0
4−.0
3−.2
4.0
0−.0
1.1
4.2
9−.0
861 T
ends
to d
ispar
age
qual
itie
s tr
adit
ion
ally
as
soci
ated
wit
h o
wn
gen
der
(e.
g., a
wom
an
wh
o dis
dai
ns
nu
rtu
ran
ce a
nd o
verv
alu
es
pow
er; a
man
wh
o dis
dai
ns
pow
er a
nd
over
valu
es e
mot
ion
al s
ensi
tivi
ty).
−.0
9.0
4.0
0.0
5.0
0−.0
6.2
1.0
4.2
0.0
3−.0
6.1
1.1
1−.0
8.0
6.0
7
TA
BLE
2.
Con
tin
ued
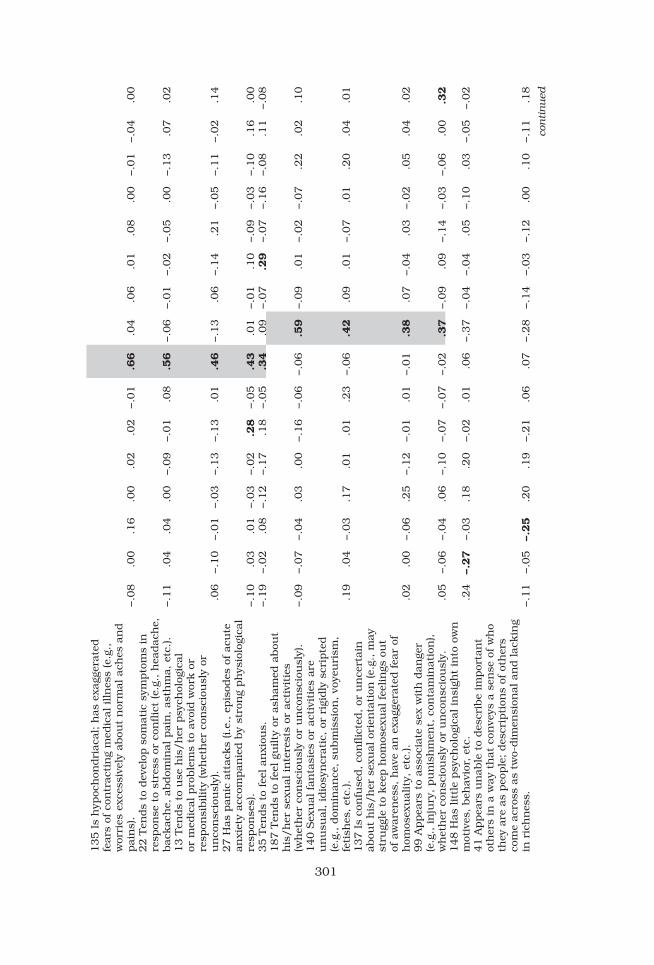
301
135 I
s h
ypoc
hon
dri
acal
; h
as e
xagg
erat
ed
fear
s of
con
trac
tin
g m
edic
al illn
ess
(e.g
.,
wor
ries
exc
essi
vely
abou
t n
orm
al a
ches
an
d
pai
ns)
.−.0
8.0
0.1
6.0
0.0
2.0
2−.0
1.6
6.0
4.0
6.0
1.0
8.0
0−.0
1−.0
4.0
022 T
ends
to d
evel
op s
omat
ic s
ympto
ms
in
resp
onse
to
stre
ss o
r co
nflic
t (e
.g., h
eadac
he,
bac
kac
he,
abdom
inal
pai
n, as
thm
a, e
tc.).
−.1
1.0
4.0
4.0
0−.0
9−.0
1.0
8.5
6−.0
6−.0
1−.0
2−.0
5.0
0−.1
3.0
7.0
213 T
ends
to u
se h
is/h
er p
sych
olog
ical
or
med
ical
pro
ble
ms
to a
void
wor
k o
r re
spon
sibilit
y (w
het
her
con
scio
usl
y or
u
nco
nsc
iou
sly)
..0
6−.1
0−.0
1−.0
3−.1
3−.1
3.0
1.4
6−.1
3.0
6−.1
4.2
1−.0
5−.1
1−.0
2.1
427 H
as p
anic
att
acks
(i.e
., e
pis
odes
of ac
ute
an
xiet
y ac
com
pan
ied b
y st
ron
g ph
ysio
logi
cal
resp
onse
s).
−.1
0.0
3.0
1−.0
3−.0
2.2
8−.0
5.4
3.0
1−.0
1.1
0−.0
9−.0
3−.1
0.1
6.0
035 T
ends
to fee
l an
xiou
s.−.1
9−.0
2.0
8−.1
2−.1
7.1
8−.0
5.3
4.0
9−.0
7.2
9−.0
7−.1
6−.0
8.1
1−.0
8187 T
ends
to fee
l gu
ilty
or
ash
amed
abou
t h
is/h
er s
exu
al in
tere
sts
or a
ctiv
itie
s (w
het
her
con
scio
usl
y or
un
con
scio
usl
y).
−.0
9−.0
7−.0
4.0
3.0
0−.1
6−.0
6−.0
6.5
9−.0
9.0
1−.0
2−.0
7.2
2.0
2.1
0140 S
exu
al fan
tasi
es o
r ac
tivi
ties
are
u
nu
sual
, id
iosy
ncr
atic
, or
rig
idly
scr
ipte
d
(e.g
., d
omin
ance
, su
bm
issi
on, vo
yeu
rism
, fe
tish
es, et
c.).
.19
.04
−.0
3.1
7.0
1.0
1.2
3−.0
6.4
2.0
9.0
1−.0
7.0
1.2
0.0
4.0
1137 I
s co
nfu
sed, co
nflic
ted, or
un
cert
ain
ab
out
his
/h
er s
exu
al o
rien
tati
on (e.
g., m
ay
stru
ggle
to
kee
p h
omos
exu
al fee
lin
gs o
ut
of a
war
enes
s, h
ave
an e
xagg
erat
ed fea
r of
h
omos
exu
alit
y, e
tc.).
.02
.00
−.0
6.2
5−.1
2−.0
1.0
1−.0
1.3
8.0
7−.0
4.0
3−.0
2.0
5.0
4.0
299 A
ppea
rs t
o as
soci
ate
sex
wit
h d
ange
r (e
.g., in
jury
, pu
nis
hm
ent,
con
tam
inat
ion
),
wh
eth
er c
onsc
iou
sly
or u
nco
nsc
iou
sly.
.05
−.0
6−.0
4.0
6−.1
0−.0
7−.0
7−.0
2.3
7−.0
9.0
9−.1
4−.0
3−.0
6.0
0.3
2148 H
as lit
tle
psy
chol
ogic
al in
sigh
t in
to o
wn
m
otiv
es, beh
avio
r, e
tc.
.24
−.2
7−.0
3.1
8.2
0−.0
2.0
1.0
6−.3
7−.0
4−.0
4.0
5−.1
0.0
3−.0
5−.0
241 A
ppea
rs u
nab
le t
o des
crib
e im
por
tan
t ot
her
s in
a w
ay t
hat
con
veys
a s
ense
of w
ho
they
are
as
peo
ple
; des
crip
tion
s of
oth
ers
com
e ac
ross
as
two-
dim
ensi
onal
an
d lac
kin
g in
ric
hn
ess.
−.1
1−.0
5−.2
5.2
0.1
9−.2
1.0
6.0
7−.2
8−.1
4−.0
3−.1
2.0
0.1
0−.1
1.1
8
continued

302
SW
AP-I
I F
acto
rs
SW
AP-I
I It
ems
12
34
56
78
910
11
12
13
14
15
16
85 H
as c
onsc
iou
s h
omos
exu
al d
esir
es
(mod
erat
e pla
cem
ent
implies
bis
exu
alit
y,
hig
h p
lace
men
t im
plies
hom
osex
ual
ity)
.−.1
0.0
8−.0
8.2
1−.1
2.1
4−.0
5−.0
8.2
7.0
7−.0
7.0
8.0
1.0
3.0
7−.0
7102 H
as a
dee
p s
ense
of in
ner
bad
nes
s; s
ees
self a
s dam
aged
, ev
il, or
rot
ten
to
the
core
(w
het
her
con
scio
usl
y or
un
con
scio
usl
y).
.03
−.1
6−.1
3−.1
6.0
2.1
6−.0
3−.1
6.2
6.1
3.1
2−.0
3.0
2−.1
5.1
9.1
481 R
epea
tedly
re-
exper
ien
ces
or r
e-live
s a
pas
t tr
aum
atic
eve
nt
(e.g
., h
as in
tru
sive
m
emor
ies
or r
ecu
rrin
g dre
ams
of t
he
even
t;
is s
tart
led o
r te
rrifi
ed b
y pre
sen
t ev
ents
th
at
rese
mble
or
sym
bol
ize
the
pas
t ev
ent)
.-.
07
.02
−.1
3.0
7.0
1.1
8−.0
7.1
6.2
4.1
1.0
4−.1
3.0
3−.1
6.0
9−.0
1158 A
ppea
rs a
frai
d o
f co
mm
itm
ent
to a
lon
g-te
rm lov
e re
lati
onsh
ip.
−.0
1−.0
5.0
4−.0
4.1
9−.1
9.0
3−.0
8.2
0−.0
3.1
5.1
6−.0
8.1
8−.0
4.0
0169 I
s af
raid
or
con
flic
ted a
bou
t bec
omin
g like
a par
ent
(or
par
ent
figu
re) ab
out
wh
om
s/h
e h
as s
tron
g n
egat
ive
feel
ings
(e.
g., m
ay
go t
o le
ngt
hs
to a
void
or
reje
ct a
ttit
udes
or
beh
avio
rs a
ssoc
iate
d w
ith
th
at p
erso
n).
−.1
7.1
7−.0
6−.1
2.0
0−.1
3.0
1−.0
2.2
0−.0
5−.0
2.0
8.0
5−.1
0−.1
1.0
750 T
ends
to fee
l life
has
no
mea
nin
g.−.1
5−.1
7−.1
0.0
3.0
3−.0
1.0
6−.0
6.0
2.6
2−.0
3.0
4−.0
7−.0
3.0
0.0
256 A
ppea
rs t
o fin
d lit
tle
or n
o ple
asu
re,
sati
sfac
tion
, or
en
joym
ent
in life’
s ac
tivi
ties
.−.1
2−.2
0−.1
2−.0
2.0
8−.1
0−.0
7.0
7−.0
6.5
7.0
6−.0
4−.1
3−.0
8−.0
3.0
3189 T
ends
to fee
l u
nh
appy,
dep
ress
ed, or
des
pon
den
t.−.2
1−.2
0−.0
6−.1
3−.0
8−.0
3−.2
0.0
7−.0
6.5
4−.0
1.0
0−.0
1.0
3−.0
5−.0
1195 T
ends
to b
e pre
occu
pie
d w
ith
dea
th a
nd
dyi
ng.
.09
−.0
2.0
0.0
5.0
4.0
6.0
5.1
0.1
4.5
1−.0
3−.0
9.0
9−.0
2.1
9−.0
4168 S
tru
ggle
s w
ith
gen
uin
e w
ish
es t
o kill
him
/h
erse
lf.
−.0
3−.0
9−.1
4−.0
2.0
6.2
6−.0
9−.0
7.0
6.4
7−.0
1−.0
4.0
5−.0
1.0
3.0
330 T
ends
to fee
l list
less
, fa
tigu
ed, or
lac
kin
g in
en
ergy
.−.1
5−.0
9−.0
3−.0
9−.0
3−.1
6−.0
2.2
9−.1
5.4
5−.0
4.0
3−.0
7−.0
7.1
5−.0
390 I
s pro
ne
to p
ain
ful fe
elin
gs o
f em
pti
nes
s (e
.g., m
ay fee
l lo
st, ber
eft,
abje
ctly
alo
ne
even
in
th
e pre
sen
ce o
f ot
her
s, e
tc.).
−.2
3−.0
8−.1
7−.0
5.0
0.1
9−.0
5−.0
2.0
5.3
9.1
4.0
7.0
9.2
0−.0
3−.0
5
TA
BLE
2.
Con
tin
ued

303
178 H
as a
per
vasi
ve s
ense
th
at s
omeo
ne
or s
omet
hin
g n
eces
sary
for
hap
pin
ess
has
bee
n los
t fo
reve
r, w
het
her
con
scio
usl
y or
u
nco
nsc
iou
sly
(e.g
., a
rel
atio
nsh
ip, yo
uth
, bea
uty
, su
cces
s).
−.2
3−.0
4−.0
2.0
0−.1
2−.1
1.0
0−.1
4.1
0.3
9−.0
9−.0
7.0
9.0
7−.1
0.0
5142 T
ends
to m
ake
repea
ted s
uic
idal
th
reat
s or
ges
ture
s, e
ith
er a
s a
“cry
for
hel
p”
or a
s an
eff
ort
to m
anip
ula
te o
ther
s..1
2−.1
5−.0
3−.2
0.0
9.2
5−.1
8.0
9−.1
8.3
0−.1
4.0
8.2
4.1
6.0
6.0
4165 T
ends
to d
isto
rt u
nac
cepta
ble
w
ish
es o
r fe
elin
gs b
y tr
ansf
orm
ing
them
in
to t
hei
r op
pos
ite
(e.g
., m
ay e
xpre
ss
exce
ssiv
e co
nce
rn w
hile
show
ing
sign
s of
u
nac
kn
owle
dge
d h
osti
lity
, dis
gust
abou
t se
xual
mat
ters
wh
ile
show
ing
sign
s of
u
nac
kn
owle
dge
d e
xcit
emen
t, e
tc.).
.00
−.1
4−.0
5.0
9.1
1.0
3−.0
4.0
7.1
8−.3
0−.1
6−.1
2.1
6.0
1.0
3.1
7162 E
xpre
sses
con
trad
icto
ry fee
lin
gs o
r bel
iefs
wit
hou
t bei
ng
dis
turb
ed b
y th
e in
con
sist
ency
; h
as lit
tle
nee
d t
o re
con
cile
or
reso
lve
con
trad
icto
ry idea
s..1
2.0
1−.0
9.1
1.0
9.1
0−.1
3.1
0−.1
8−.2
1−.0
4.1
2.2
0.0
0−.1
0.1
660 T
ends
to b
e sh
y or
sel
f-co
nsc
iou
s in
so
cial
sit
uat
ion
s.−.0
2.0
4.0
6−.0
1−.0
3−.1
1−.1
2−.0
1−.0
3−.0
1.6
5−.0
5−.0
1−.0
8.1
4−.0
3124 T
ends
to a
void
soc
ial si
tuat
ion
s bec
ause
of
fea
r of
em
bar
rass
men
t or
hu
milia
tion
.−.0
7−.1
3.0
4−.0
2−.0
3−.0
8.0
3.1
3.0
9.0
1.6
1−.0
1−.0
4−.0
3.0
7−.0
1193 L
acks
soci
al s
kills
; te
nds
to b
e so
cial
ly
awkw
ard o
r in
appro
pri
ate.
.00
−.1
6.1
1.3
5.0
5−.0
5−.0
1−.1
1−.1
0.0
6.5
3.0
5−.0
6−.0
1−.0
4−.0
586 T
ends
to fee
l as
ham
ed o
r em
bar
rass
ed.
−.1
4−.1
1−.0
7−.1
7−.1
0.0
2−.0
6−.0
9.1
4−.0
4.4
6−.0
6−.0
6−.0
8.2
1−.0
1149 T
ends
to fee
l like
an o
utc
ast
or o
uts
ider
.−.1
9−.0
3−.0
9.0
7.0
3.0
5−.0
5−.0
9.0
4.2
3.3
6.1
6−.0
3−.1
0−.1
9−.0
4160 L
acks
clos
e fr
ien
dsh
ips
and
rela
tion
ship
s..0
6−.1
5.1
0.1
5.2
6−.0
7−.0
2−.0
4−.1
6.2
1.3
3.1
0.0
0−.0
1−.1
3.0
2197 T
ends
to s
eek o
ut
or c
reat
e in
terp
erso
nal
rel
atio
nsh
ips
in w
hic
h s
/h
e is
in
th
e ro
le o
f ca
rin
g fo
r, r
escu
ing,
or
pro
tect
ing
the
oth
er.
−.0
5.1
8.0
6−.0
7.0
1−.1
6−.3
1−.1
7.0
9−.0
2−.3
2−.0
8.0
7.1
0.1
3−.1
498 T
ends
to fea
r s/
he
will be
reje
cted
or
aban
don
ed.
−.2
4−.1
1−.1
8−.2
0−.1
5.0
7−.1
1−.1
3−.1
2−.0
7.3
0−.0
1.1
3.2
1−.0
2−.0
5
continued

304
SW
AP-I
I F
acto
rs
SW
AP-I
I It
ems
12
34
56
78
910
11
12
13
14
15
16
69 D
ecis
ion
s an
d a
ctio
ns
are
un
du
ly
influ
ence
d b
y ef
fort
s to
avo
id p
erce
ived
dan
gers
; is
mor
e co
nce
rned
wit
h a
void
ing
har
m t
han
pu
rsu
ing
des
ires
.−.0
7−.1
3.0
6−.0
4.0
3−.1
5−.1
0.1
9.1
4−.0
8.2
9−.0
2−.0
5−.0
3.0
7.0
179 A
ttem
pts
to
den
y or
“ov
erri
de”
fea
r or
an
xiet
y by
rush
ing
hea
dlo
ng
into
fea
red
situ
atio
ns,
tak
ing
un
nec
essa
ry r
isks,
etc
..1
5−.1
3.1
1.0
7.1
0.1
1−.1
2−.1
8.1
1−.1
6−.2
6.0
7−.0
3.0
7.0
6.0
5172 S
eem
s u
nab
le t
o se
ttle
in
to, or
su
stai
n
com
mit
men
t to
, id
enti
ty-d
efin
ing
life
rol
es
(e.g
., c
aree
r, o
ccu
pat
ion
, life
styl
e, e
tc.).
−.0
6−.0
8−.1
4.0
4−.0
2−.1
3−.0
2.0
5.0
6.0
0.0
5.6
1.0
1.0
3−.0
5.0
2188 W
ork-l
ife
and/or
liv
ing
arra
nge
men
ts
ten
d t
o be
chao
tic
or u
nst
able
(e.
g., jo
b o
r h
ousi
ng
situ
atio
n s
eem
s al
way
s te
mpor
ary,
tr
ansi
tion
al, or
ill-d
efin
ed).
.16
−.0
9−.1
4.0
7.0
3.0
9−.1
6.0
4−.0
9.0
2−.1
3.4
9.1
0.0
7.0
8−.0
924 T
ends
to b
e u
nre
liab
le a
nd irr
espon
sible
(e
.g., m
ay fai
l to
mee
t w
ork o
bliga
tion
s or
h
onor
fin
anci
al c
omm
itm
ents
)..2
9−.0
6−.1
8−.0
4−.1
0−.1
5.1
4.0
7−.1
4−.0
3.0
4.4
8−.0
8−.1
4.0
9.0
8153 R
elat
ion
ship
s te
nd t
o be
un
stab
le,
chao
tic,
an
d r
apid
ly c
han
gin
g..1
0−.0
7−.1
1.0
0−.0
2.2
6−.1
1−.1
0−.1
1−.0
2−.0
2.3
3.1
9.2
5−.0
8.0
733 I
s co
nflic
ted o
r in
hib
ited
abou
t ac
hie
vem
ent
or s
ucc
ess
(e.g
., a
chie
vem
ents
m
ay b
e bel
ow p
oten
tial
, m
ay s
abot
age
self
just
bef
ore
atta
inin
g im
por
tan
t go
als,
etc
.).
−.2
0−.0
7−.0
9−.1
4−.0
6−.3
1−.0
5−.0
4.2
0−.0
5−.0
8.3
3−.1
0−.1
8.0
4.0
3177 R
epea
tedly
con
vin
ces
oth
ers
of h
is/
her
com
mit
men
t to
ch
ange
bu
t th
en r
ever
ts
to p
revi
ous
mal
adap
tive
beh
avio
r; t
ends
to c
onvi
nce
oth
ers
that
“th
is t
ime
is r
eally
dif
fere
nt.
”.2
1−.1
0−.0
2−.1
8−.0
1−.0
3−.0
9.0
1−.0
8−.1
0−.1
5.2
8.0
6.1
0.0
3.1
315 L
acks
a st
able
sen
se o
f w
ho
s/h
e is
(e.
g.,
atti
tudes
, va
lues
, go
als,
an
d fee
lin
gs a
bou
t se
lf s
eem
un
stab
le o
r ev
er-c
han
gin
g).
−.1
0−.1
6−.2
4.0
3−.0
4.2
4.1
3.0
3.0
5−.0
5.1
4.2
4.0
3.0
0.1
6.0
5
TA
BLE
2.
Con
tin
ued

305
150 T
ends
to iden
tify
wit
h a
dm
ired
oth
ers
to a
n e
xagg
erat
ed d
egre
e, t
akin
g on
th
eir
atti
tudes
, m
ann
eris
ms,
etc
. (e
.g., m
ay
be
dra
wn
in
to t
he
“orb
it”
of a
str
ong
or
char
ism
atic
per
son
alit
y).
−.0
3−.0
5.0
3.1
4−.0
4.0
2.1
0−.0
3.0
9−.0
7−.0
6.0
8.5
2.0
8.1
2.1
0176 T
ends
to c
onfu
se o
wn
th
ough
ts,
feel
ings
, or
per
son
alit
y tr
aits
wit
h t
hos
e of
ot
her
s (e
.g.,
may
use
th
e sa
me
wor
ds
to
des
crib
e h
im/h
erse
lf a
nd a
not
her
per
son
, bel
ieve
th
e tw
o sh
are
iden
tica
l th
ough
ts a
nd
feel
ings
, et
c.).
.05
−.0
7−.0
3−.0
4.1
0.0
7−.0
2.0
3−.0
5.0
0−.0
2.1
8.4
0.1
6−.1
5.2
1154 T
ends
to d
raw
oth
ers
into
sce
nar
ios,
or
“pu
ll”
them
in
to r
oles
, th
at fee
l al
ien
or
un
fam
ilia
r (e
.g., b
ein
g u
nch
arac
teri
stic
ally
in
sen
siti
ve o
r cr
uel
, fe
elin
g like
the
only
per
son
in
th
e w
orld
wh
o ca
n h
elp, et
c.).
−.2
0−.0
4−.1
2−.0
6−.1
5.0
7.2
7−.1
0−.0
5−.1
4−.0
8−.1
4.3
0.0
8.2
1.0
045 I
s pro
ne
to idea
lizi
ng
peo
ple
; m
ay s
ee
adm
ired
oth
ers
as p
erfe
ct, la
rger
th
an life,
al
l w
ise,
etc
..1
2−.1
5−.0
3−.2
0.0
9.2
5−.1
8.0
9−.1
8.3
0−.1
4.0
8.2
4.1
6.0
6.0
4181 T
ends
to c
hoo
se s
exu
al o
r ro
man
tic
par
tner
s w
ho
seem
in
appro
pri
ate
in t
erm
s of
age
, st
atu
s (e
.g., s
ocia
l, e
con
omic
, in
tellec
tual
), e
tc.
.09
.01
.02
.01
−.0
2−.1
0−.0
6−.0
9.0
8.0
2−.0
7.1
7.1
6.5
1.0
6−.0
6110 T
ends
to b
ecom
e at
tach
ed t
o, o
r ro
man
tica
lly
inte
rest
ed in
, peo
ple
wh
o ar
e em
otio
nal
ly u
nav
aila
ble
.−.0
9−.0
4−.0
3−.1
1−.1
2−.2
3−.0
7−.1
9.0
8.0
0.0
1.0
0.1
3.5
1.0
4−.0
523 T
ends
to b
ecom
e in
volv
ed in
rom
anti
c or
sex
ual
“tr
ian
gles
” (e
.g., is
dra
wn
to
peo
ple
wh
o ar
e al
read
y at
tach
ed, so
ugh
t by
som
eon
e el
se, et
c.).
−.0
1.0
4−.0
9.0
1−.0
2−.0
8.0
2−.0
4.1
5.0
4−.1
6−.1
2−.0
9.5
1.0
4.0
334 T
ends
to b
e se
xual
ly s
edu
ctiv
e or
pro
voca
tive
(e.
g., m
ay b
e in
appro
pri
atel
y flir
tati
ous,
pre
occu
pie
d w
ith
sex
ual
co
nqu
est,
pro
ne
to “
lead
peo
ple
on
,” e
tc.).
.17
.03
−.1
0.0
0−.0
1.0
4.2
8−.0
3.1
1−.0
6−.0
2−.0
3−.2
6.4
6.1
4.0
1171 A
ppea
rs t
o fe
ar b
ein
g al
one;
may
go
to
grea
t le
ngt
hs
to a
void
bei
ng
alon
e.−.0
5−.0
9.0
2−.0
9−.0
5.1
0−.0
8.0
9−.1
4.0
0−.0
8.0
7.0
4.4
4.1
6−.0
6128 F
anta
size
s ab
out
idea
l, p
erfe
ct lov
e.−.2
4.0
3.0
0.0
0−.1
4−.1
1.1
9−.1
9.0
6−.0
4−.0
9−.0
5.1
5.4
3.0
2.0
5
continued

306
SW
AP-I
I F
acto
rs
SW
AP-I
I It
ems
12
34
56
78
910
11
12
13
14
15
16
80 T
ends
to b
e se
xual
ly p
osse
ssiv
e or
je
alou
s; is
pre
occu
pie
d w
ith
con
cern
s ab
out
real
or
imag
ined
in
fidel
ity.
.03
.01
−.0
3.0
4−.0
8.0
2−.1
0−.0
6−.0
3−.0
6−.0
1−.1
7−.0
3.3
8−.1
6.0
8132 T
ends
to h
ave
nu
mer
ous
sexu
al
invo
lvem
ents
; is
pro
mis
cuou
s..2
5.1
5−.0
6.0
2.0
2.0
5.1
4−.0
7.0
9.0
2−.0
6.2
3−.1
1.3
8.0
7.1
211 T
ends
to b
ecom
e at
tach
ed q
uic
kly
or
inte
nse
ly; dev
elop
s fe
elin
gs, ex
pec
tati
ons,
et
c. t
hat
are
not
war
ran
ted b
y th
e h
isto
ry o
r co
nte
xt o
f th
e re
lati
onsh
ip.
−.1
4−.0
6−.1
2−.0
4−.1
8.2
1.0
4−.0
8−.1
5−.1
5−.0
9.0
2.1
5.3
8.1
2−.0
257 R
elig
iou
s or
spir
itu
al b
elie
fs a
re c
entr
al
to h
is/h
er iden
tity
an
d e
xper
ien
ce.
−.0
9.2
2.0
5.1
6−.2
2−.1
6.0
6−.0
3.0
4.1
0−.1
5−.0
9.2
1−.2
7.1
6.0
2114 T
ends
to b
e cr
itic
al o
f ot
her
s.−.0
6−.0
2.0
6−.0
5.0
1−.1
3.1
7−.0
1−.0
7.0
1−.0
3−.0
4.0
1−.0
9−.6
5−.0
6139 T
ends
to h
old g
rudge
s; m
ay d
wel
l on
in
sult
s or
sligh
ts for
lon
g per
iods.
−.0
3−.1
6.0
8.0
5−.0
8−.0
4.0
2.0
1−.0
6.1
2−.0
5.0
2−.0
8−.0
3−.5
9−.0
9122 A
ttem
pts
to
avoi
d fee
lin
g h
elple
ss o
r dep
ress
ed b
y bec
omin
g an
gry
inst
ead.
−.0
8−.0
3−.0
6−.0
3.0
8.1
5−.0
3−.0
3.0
6−.1
1−.0
5−.0
4−.1
0.0
8−.5
6−.0
416 T
ends
to b
e an
gry
or h
osti
le (w
het
her
co
nsc
iou
sly
or u
nco
nsc
iou
sly)
..1
4−.2
2−.1
8−.0
5−.0
4.1
1.0
0−.1
5−.0
2.0
5−.1
1−.1
0−.0
7−.2
4−.4
7−.0
48 T
ends
to g
et in
to p
ower
str
ugg
les.
.15
−.0
5.0
1−.0
6−.0
9.0
6.0
4−.0
2−.0
7−.1
2−.1
8.1
0−.0
1−.1
4−.4
5−.1
2116 T
ends
to s
ee o
wn
un
acce
pta
ble
fee
lin
gs
or im
pu
lses
in
oth
er p
eople
in
stea
d o
f in
h
im/h
erse
lf.
.03
−.1
5−.1
1−.0
1.1
1−.0
1.0
0.0
6−.0
9−.1
8−.0
7−.0
2.0
5−.0
4−.4
4.0
9127 T
ends
to fee
l m
isu
nder
stoo
d,
mis
trea
ted,
or v
icti
miz
ed.
−.0
1−.1
8−.0
9.1
1−.2
1−.0
6−.1
5−.0
2−.0
9.0
9−.0
9.0
7.0
8−.0
7−.4
4−.0
6170 T
ends
to b
e op
pos
itio
nal
, co
ntr
ary,
or
quic
k t
o dis
agre
e..0
1−.0
7.0
1.0
0.0
9−.0
1.0
5.0
4.0
2.0
0−.0
9.1
5.1
2−.1
5−.4
3−.1
1103 T
ends
to h
ave
extr
eme
reac
tion
s to
per
ceiv
ed s
ligh
ts o
r cr
itic
ism
(e.
g., m
ay r
eact
w
ith
rag
e, h
um
ilia
tion
, et
c.).
.01
−.2
2−.0
7−.0
2−.1
5.3
3.0
3−.0
8−.0
2−.1
0.1
6−.1
1.0
6−.0
1−.4
3−.0
6182 T
ends
to b
e co
ntr
ollin
g..1
2−.0
2.2
0−.1
1.1
5.0
6.0
9.1
2.0
1−.0
9−.2
5−.1
7−.0
3.0
1−.4
2−.1
046 T
ends
to b
e su
gges
tible
or
easi
ly
influ
ence
d.
−.0
8−.0
7−.0
2.1
2−.2
4−.1
1.0
4−.0
1−.1
6−.2
2.1
2−.0
2.0
4−.0
3.3
9−.0
4
TA
BLE
2.
Con
tin
ued

307
14 T
ends
to b
lam
e ow
n fai
lure
s or
sh
ortc
omin
gs o
n o
ther
peo
ple
or
circ
um
stan
ces;
att
ribu
tes
his
/h
er d
ifficu
ltie
s to
ext
ern
al fac
tors
rat
her
th
an a
ccep
tin
g re
spon
sibilit
y fo
r ow
n c
ondu
ct o
r ch
oice
s..1
0−.1
9−.1
7.0
7−.0
9−.1
1.1
3.1
6−.2
2−.0
6−.1
5.1
2−.0
8−.0
5−.3
9−.0
31 T
ends
to fee
l gu
ilty
(e.
g., m
ay b
lam
e se
lf o
r fe
el r
espon
sible
for
bad
th
ings
th
at h
appen
).−.1
1−.0
3.0
3−.2
0−.0
7.0
0−.1
9−.0
6.0
5.0
5.0
8−.1
4−.1
0−.1
3.3
8−.0
896 T
ends
to e
lici
t dis
like
or a
nim
osit
y in
ot
her
s..2
5−.0
3.0
2.0
4−.0
6.0
0.0
3.0
5−.1
2.1
1.0
0.1
1.0
3−.0
3−.3
7−.0
5105 I
s su
spic
iou
s; t
ends
to a
ssu
me
oth
ers
will h
arm
, dec
eive
, co
nsp
ire
agai
nst
, or
bet
ray
him
/h
er.
.11
−.0
9.0
3.3
5−.0
2.0
4−.0
6.0
1.0
4.1
2.1
2−.0
8.0
5−.0
1−.3
5−.0
425 H
as d
ifficu
lty
ackn
owle
dgi
ng
or
expre
ssin
g an
ger.
−.1
7−.1
0−.1
5−.0
9.2
4−.1
2−.1
5.0
1−.0
1−.2
0.0
0−.1
7−.0
9−.1
9.3
4−.1
417 T
ends
to b
e in
grat
iati
ng
or s
ubm
issi
ve
(e.g
., c
onse
nts
to
thin
gs s
/h
e doe
s n
ot w
ant
to d
o, in
th
e h
ope
of g
etti
ng
suppor
t or
ap
pro
val).
−.0
4−.2
5−.1
0−.1
5−.1
4−.2
9−.2
2−.0
2−.0
1−.2
8.0
3−.1
0−.0
1.0
1.3
4−.1
488 T
ends
to b
e in
suffi
cien
tly
con
cern
ed
wit
h m
eeti
ng
own
nee
ds;
appea
rs n
ot t
o fe
el e
nti
tled
to
get
or a
sk for
th
ings
s/h
e des
erve
s.−.0
7−.0
9−.0
7−.1
8.1
9−.1
6−.2
5−.0
8.0
2−.0
7.1
4−.0
8−.0
4−.1
4.3
3−.0
5129 T
ends
to b
e co
nflic
ted a
bou
t au
thor
ity
(e.g
., m
ay fee
l s/
he
mu
st s
ubm
it, re
bel
ag
ain
st, w
in o
ver,
def
eat,
etc
.).
−.0
5−.1
3−.1
1.0
2.0
2−.0
4.0
0−.1
2.1
5−.2
8−.0
3.1
7−.0
4−.1
7−.3
2−.1
038 T
ends
to fee
l s/
he
is n
ot h
is/h
er t
rue
self
wit
h o
ther
s; m
ay fee
l fa
lse
or fra
udu
len
t.−.1
2−.1
4−.0
5−.0
9.0
0.0
5.1
2−.0
5.1
9.0
0.0
6−.0
1−.0
2−.1
2.3
0.0
447 A
ttem
pts
to
avoi
d o
r flee
dep
ress
ive
feel
ings
th
rou
gh e
xces
sive
opti
mis
m,
acti
vity
, en
ergy
, et
c.−.1
5−.0
1.0
3.0
5.1
9.0
2.1
6−.1
6−.0
1−.2
6−.2
0.0
6−.1
7.0
1.2
7−.0
421 T
ends
to b
e h
osti
le t
owar
d m
ember
s of
th
e op
pos
ite
sex,
wh
eth
er c
onsc
iou
sly
or
un
con
scio
usl
y (e
.g., m
ay b
e dis
par
agin
g or
co
mpet
itiv
e).
.14
−.0
7−.1
3.0
6.0
0−.1
4.1
2−.1
1.1
9−.0
9.0
5−.1
9.0
1.0
2−.2
4.0
970 H
as u
nco
ntr
olle
d e
atin
g bin
ges
follow
ed
by
“pu
rges
” (e
.g., m
akes
sel
f vo
mit
, ab
use
s la
xati
ves,
fas
ts, et
c.); h
as b
ulim
ic e
pis
odes
..0
8−.0
1.0
6−.0
9−.0
9.0
4.0
2−.0
2.0
0.0
7−.1
0.0
1.0
6−.0
6.1
8.5
8
continued

308
SW
AP-I
I F
acto
rs
SW
AP-I
I It
ems
12
34
56
78
910
11
12
13
14
15
16
108 T
ends
to r
estr
ict
food
in
take
to t
he
poi
nt
of b
ein
g u
nder
wei
ght
and m
aln
ouri
shed
..0
5−.0
1.1
0−.0
5−.0
2.0
2.0
2.2
0.1
4.0
1.0
6−.0
4.0
7.0
5.0
2.5
3156 H
as a
dis
turb
ed o
r dis
tort
ed b
ody−
imag
e (e
.g.,
may
see
sel
f as
un
attr
acti
ve,
grot
esqu
e, d
isgu
stin
g, e
tc.).
.03
−.0
2.0
3−.0
8−.0
8.0
9.0
0−.1
3.0
7.1
9.1
6.0
5−.0
7−.0
5.0
9.4
162 T
ends
to b
e pre
occu
pie
d w
ith
foo
d, die
t,
or e
atin
g.−.0
3.0
0.2
2−.0
7−.1
6−.0
3.0
1.0
1.0
8.0
3.0
1.0
8−.0
9−.1
4.0
6.3
983 B
elie
fs a
nd e
xpec
tati
ons
seem
clich
é or
st
ereo
typic
al, as
if ta
ken
fro
m s
tory
boo
ks
or
mov
ies.
−.0
9−.0
4−.0
1.1
3.0
0−.1
5.1
4−.0
8−.2
7−.0
8−.0
2.0
3.1
2.0
3.1
4.3
7155 T
ends
to d
escr
ibe
exper
ien
ces
in
gen
eral
itie
s; is
relu
ctan
t to
pro
vide
det
ails
, ex
ample
s, o
r su
ppor
tin
g n
arra
tive
.−.1
3−.0
6−.1
8.2
0.2
4−.2
4−.0
5.0
6−.1
4−.1
3−.1
6−.0
6−.0
7−.0
3−.1
0.3
6186 H
as d
ifficu
lty
dir
ecti
ng
bot
h t
ender
fe
elin
gs a
nd s
exu
al fee
lin
gs t
owar
d t
he
sam
e per
son
(e.
g., se
es o
ther
s as
nu
rtu
rin
g an
d
virt
uou
s or
sex
y an
d e
xcit
ing,
bu
t n
ot b
oth
).−.0
4−.0
3−.0
1.0
1.1
1−.0
8.0
0−.0
2.2
6−.0
5−.1
9−.0
9.0
0.2
8−.0
5.3
1151 A
ppea
rs t
o ex
per
ien
ce t
he
pas
t as
a
seri
es o
f dis
join
ted o
r dis
con
nec
ted e
ven
ts;
has
difficu
lty
givi
ng
a co
her
ent
acco
un
t of
h
is/h
er life
stor
y.−.1
3−.1
2−.1
3.2
7.2
0.0
7−.0
4.0
1−.0
1−.1
0−.0
2.0
9.0
5−.0
6.0
9.2
910 B
elie
ves
that
som
e im
por
tan
t ot
her
has
a
spec
ial, s
eem
ingl
y m
agic
al a
bilit
y to
kn
ow
his
/h
er in
ner
mos
t th
ough
ts o
r fe
elin
gs (e.
g.,
imag
ines
rap
por
t is
so
per
fect
th
at o
rdin
ary
com
mu
nic
atio
n is
super
flu
ous)
.−.0
2−.1
3−.0
5.1
4−.1
0.0
1.0
8.0
0−.0
1−.1
1−.1
7−.1
8.1
0.0
4.1
3.2
17 A
ppea
rs c
onflic
ted a
bou
t h
is/h
er r
acia
l or
eth
nic
iden
tity
(e.
g., u
nder
valu
es a
nd
reje
cts,
or
over
valu
es a
nd is
pre
occu
pie
d
wit
h, ow
n c
ult
ura
l h
erit
age)
.−.0
4.0
2−.1
1.1
6−.0
9−.0
5.0
8−.0
5.1
0−.0
8.0
0.0
0.0
6−.0
5−.1
1.2
0107 T
ends
to e
xpre
ss q
ual
itie
s or
m
ann
eris
ms
trad
itio
nal
ly a
ssoc
iate
d
wit
h o
wn
gen
der
to
an e
xagg
erat
ed o
r st
ereo
typic
al d
egre
e (i.e
., a
hyp
er-f
emin
ine
wom
an; a
hyp
er-m
ascu
lin
e, “
mac
ho”
man
)..1
4.1
0−.0
7.1
0−.0
2−.0
6.1
1−.0
7−.1
0−.0
3−.0
5−.1
7−.1
0.1
2.0
0.1
9
Not
es.
Loa
din
gs ≥
|.2
5| i
n b
oldfa
ce.
Fac
tor
nam
es:
1:
Psy
chop
ath
y; 2
: Psy
chol
ogic
al H
ealt
h;
3:
Obse
ssio
nal
ity;
4:
Sch
izot
ypy;
5:
Em
otio
nal
Avo
id-
ance
; 6:
Em
otio
nal
Dys
regu
lati
on;
7:
Nar
ciss
ism
; 8:
An
xiou
s S
omat
izat
ion
; 9:
Sex
ual
Con
flic
t; 1
0:
Dep
ress
ion
; 11:
Soc
ial
An
xiet
y/A
void
ance
; 12:
Un
stab
le C
omm
itm
ents
; 13: B
oun
dar
y D
istu
rban
ce; 14: H
istr
ion
ic S
exu
aliz
atio
n; 15: H
osti
lity
; 16: E
atin
g D
istu
rban
ce.
TA
BLE
2.
Con
tin
ued

FACTOR STRUCTURE OF THE SWAP-II 309
herence with the scale (e.g., negatively scored suggestibility in a Hostility factor). Table 3 reports the factor correlations for the 16 obliquely rotated factors.
Two aspects of the data deserve comment. First, Table 3 illustrates a very clean simple structure solution. Second, as can be seen in Table 3, although the factors were allowed to correlate, with few exceptions most correlations were close to zero. This is a desirable quality for a multiscale inventory because it implies that each scale offers nonredundant informa-tion about the patient. Such information can be profitably summarized by factor scores because all 16 factors have high factor score validity coeffi-cients (Grice, 2001; McDonald & Mulaik, 1979), a situation uncommon among psychology scales (Guttman, 1955). Factor score validity coeffi-cients represent the correlations between the factor score estimates and the actual factor scores (see McDonald & Mulaik, 1979, for a relatively nontechnical discussion). Although the factors are clearly distinct, when we created factor-based scores from items with the highest loadings (de-scribed above), some of the seemingly anomalous findings (e.g., the ab-sence of any relationship between Depression and Anxious Somatization) disappeared. For example, Psychopathy correlated r = .43 with Narcissism and .54 with Unstable Commitments, and Depression correlated r = .23 with Anxious Somatization.
TABLE 3. Factor Correlation Matrix for 16 Oblimin-Rotated SWAP-II Factors: Factor Score Validities on Diagonal
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
1 .95 2 −.11 .95 3 −.18 .15 .89 4 .15 −.16 .00 .89 5 .09 .09 .14 .08 .88 6 .12 −.11 −.11 .03 −.12 .92 7 .22 .05 .03 .03 .03 .01 .92 8 .01 −.15 .01 .09 −.07 .01 −.05 .86 9 −.06 .15 .02 −.14 .03 .00 −.03 −.10 .8810 −.10 −.15 −.00 −.04 −.02 .07 −.14 .09 .09 .8911 −.21 −.10 .11 −.00 −.00 −.12 −.23 .01 .07 .18 .9112 .17 −.13 −.14 .04 −.05 .07 −.02 −.01 −.07 .05 −.06 .8713 .06 −.07 −.01 −.10 .00 .08 .03 .02 −.02 −.01 −.06 −.04 .8614 .10 .01 −.17 −.02 −.05 .09 .14 −.06 −.08 −.10 −.14 .09 −.01 .8815 .27 −.18 −.01 .10 .03 .14 .21 .03 −.09 .03 −.13 .03 .07 −.07 .9316 .05 −.10 −.06 .15 .06 .06 .01 −.01 .02 −.02 −.02 .07 .04 −.08 −.02 .85
Note. Factor Score validity coefficients on the diagonal. Factor Score Validities and Factor Correlations in boldface. Factor names: 1: Psychopathy; 2: Psychological Health; 3: Obses-sionality; 4: Schizotypy; 5: Emotional Avoidance; 6: Emotional Dysregulation; 7: Narcissism; 8: Anxious Somatization; 9: Sexual Conflict; 10: Depression; 11: Social Anxiety/Avoidance; 12: Unstable Commitments; 13: Boundary Disturbance; 14: Histrionic Sexualization; 15: Hostility; 16: Eating Disturbance. As with most factor analyses, the directionality of loadings (i.e., whether they are primarily positive or negative) is arbitrary and of no consequence to interpretation of the findings (e.g., the predominantly negative loadings of items associated with the Hostility factor).

310 WESTEN ET AL.
DISCUSSIONThis study provides the first normative data on the factor structure of comprehensive personality descriptions obtained using the SWAP-II in a large, representative national clinical sample. The sample included pa-tients with personality dysfunction ranging from mild to severe, drawn from a wide range of settings including private practice, outpatient clinics, residential treatment settings, and forensic facilities. Factor analysis us-ing polychoric correlations with Oblimin rotation produced a simple struc-ture that resembled the structure identified in previous research using an earlier version of the SWAP instrument and different factor-analytic meth-ods (Pearson correlations with a Promax rotation; Shedler & Westen, 2004a). Several similar factors emerged in both samples, notably Psycho-logical Health, Psychopathy, Hostility, Narcissism, Emotional Dysregula-tion, Obsessionality, Histrionic Sexualization, and Sexual Conflict. With the exception of the latter scale, the same factors emerged from factor analysis of the SWAP-200-A for adolescents.
The major differences between the factor structures uncovered using data from the SWAP-200 and the SWAP-II were: (1) the SWAP-200 data yielded a Dysphoria factor, whereas the SWAP-II data yielded more differ-entiated Depression, Anxious Somatization, and Social Anxiety/Avoid-ance scales; (2) SWAP-200 factors related to schizoid, schizotypal, and avoidant pathology were reconfigured, producing SWAP-II Schizotypy, Emotional Avoidance, and Social Anxiety factors; (3) items that loaded on the SWAP-200 Dissociation factor tended to load on the SWAP-II Emo-tional Dysregulation factor; (4) an Unstable Commitments factor emerged with the SWAP-II; and (5) a Boundary Disturbance factor emerged with the SWAP-II.
Although continuity with the factor structure observed with the earlier edition of the SWAP is greater than discontinuity, with several scales re-markably similar in item content, as noted here, differences did emerge between the previous analysis and the current analysis, and attributing these differences to one source versus another can be difficult. For exam-ple, the current findings reflect substantial improvements in sampling, including greater than double the sample size; inclusion of patients re-gardless of whether they met criteria for a DSM-IV PD; and random selec-tion of patients (rather than clinicians choosing potentially prototype pa-tients with a given PD). These are very substantial sampling improvements that were central to the design of the current study.
In addition, the SWAP-II has the advantage of making use of the feed-back of hundreds of clinicians who used the SWAP-200 and alerted us about items that were ambiguous or difficult to score as well as personal-ity constructs that were not adequately covered in the previous item set. It additionally reflects psychometric refinements based on examination of poorly performing items (e.g., those with minimal variance, extremely low base rates, or highly overlapping content leading to correlations ≥ .70). This study also employed much more sophisticated factor-analytic proce-

FACTOR STRUCTURE OF THE SWAP-II 311
dures, such as the use of polychoric correlations and the partialing out of potential biases due to gender differences. These data-analytic improve-ments no doubt helped produce some “cleaner” factors, although factor analysis of the current sample using simple Pearson’s correlations with an Oblimin rotation, extracting 16 factors from the raw data (not adjusted by gender), produced factors highly similar to those reported here (though less well defined in terms of item univocality). Thus, the factors appear robust across factor-analytic methods.
The scales generally showed good internal consistency with a mean α of .73, although two (Boundary Disturbance and Sexual Conflict) were on the low side at .44 and .55, most likely because of the relatively small number of items (4 and 6, respectively) that loaded highly on these fac-tors. Space limitations preclude reporting validity data for the SWAP-II factors here; however, convergent validity and discriminant validity be-tween two independent observers for the original SWAP-200 traits are very strong, with correlations along the diagonal (convergent validity) averaging ≥ .70 and off the diagonal (discriminant validity) averaging approximately 0.0 (Westen & Muderrisoglu, 2006). Preliminary analysis of data from a new sample of more than 200 patients for which we have independent data from multiple sources (e.g., three independent interviewers as well as treating clinicians), to be reported elsewhere, suggests that these traits have similar properties in terms of convergent and discriminant validity between two independent sources, and that they predict multiple mea-sures of adaptive functioning assessed by independent informants.
TRAIT STRUCTURE
Several aspects of the trait structure of the SWAP-II are notable. The first is the identification of a Psychopathy factor that resembles, in many re-spects, the psychopathy construct as described by Cleckley (1941) and operationalized via the Psychopathy Checklist-Revised (PCL-R; Hare, 2003). Importantly, this factor emerged empirically, and did so in both the SWAP-200 and the SWAP-II, even though neither instrument was designed with this construct or measure in mind. Furthermore, the items charac-terizing the Psychopathy factor were clearly a subset of the SWAP-II items that emerged empirically as most descriptive of 91 incarcerated men who had scores > 30 (the clinical cutoff) on the PCL-R in an independent as-sessment (Blagov et al., 2011). The factor resembles the DSM-IV Antisocial PD construct, but it also incorporates additional constructs of theoretical and etiological relevance, including failure to learn from negative conse-quences, thrill and sensation seeking, and deficits in empathy. These find-ings lend support to the psychopathy construct and suggest that a single instrument may be able to assess not only psychopathy but also other fo-rensically relevant constructs, such as emotional dysregulation and other Axis II personality disorders. Compared to Cleckley’s psychopathy con-struct, the SWAP-II’s empirically derived Psychopathy factor features more

312 WESTEN ET AL.
proneness to violence and less narcissism, with the latter comprising an independent construct.
Second, as was the case with the SWAP-200, SWAP-II Obsessionality describes something quite different from high conscientiousness (or its opposite, which emphasizes impulsivity) as described by the FFM or the consensus four-factor model. Rather, it describes a construct closer to the classic clinical concept of an obsessional personality style (Blagov, Brad-ley, & Westen, 2007; Shapiro, 1965), which includes such characteristics as excessive concern with rules, self-righteousness, stinginess, preoccu-pations with dirt and cleanliness, rumination, and excessive devotion to work to the detriment of leisure and relationships.
More broadly, the factors that emerged tend to focus on a greater range of personality processes and dimensions than most trait measures. Some overlap with DSM syndromes (e.g., narcissistic personality disorder) but nevertheless capture trait narcissism; others capture what might be called endophenotypes, such as Schizotypy; and still others describe psychologi-cal processes, focusing on the kinds of internal states, transformations, and conditional “if… then” processes increasingly emphasized by general personality theorists across theoretical orientations (Mischel & Shoda, 1995; Westen, Muderrisoglu, Fowler, Shedler, & Koren, 1997; e.g., “Tends to become irrational when strong emotions are stirred up . . .” [emphasis added]). All of these would be consistent with the broad construct of “trait” as first described by Allport (1937). These trait constructs may prove use-ful as modifiers of syndromal diagnoses, whether the traditional personal-ity disorder diagnoses of DSM or empirically derived diagnostic prototypes as we have proposed elsewhere (e.g., Schizoid Personality Disorder with high or low Schizotypy) (Westen et al., 2012).
A third aspect of the factor structure concerns the clear distinction be-tween emotional dysregulation and factors reflecting negative affectivity. This distinction between emotional dysregulation and negative affectivity has been replicated across multiple studies using both editions of the SWAP, with both adults and adolescents; the Affect Regulation and Expe-rience Q-sort (Westen et al., 1997); and a range of other measures (Brad-ley, DeFife, et al., 2011; Miller & Pilkonis, 2006). Emotional Dysregulation as identified here is conceptually very similar to an identically named su-praordinate factor uncovered empirically in both clinical and general sam-ples by Livesley et al. (1998) using the Dimensional Assessment of Person-ality Disorder–Basic Questionnaire (DAPD-BQ). The SWAP-II factor captures a number of facets that overlap with subscales of the DAPD-BQ, including emotional instability, intense negative emotions, cognitive dys-regulation (irrationality and dissociation) under stress, and identity diffu-sion. These findings, as well as recent findings linking emotional dysregu-lation to distinct genes not associated with negative affectivity (Bradley, Westen, et al., 2011), suggest that emotional dysregulation—the tendency to experience extreme feeling states and to resort to highly maladaptive strategies to try to regulate them—is distinct from the stably negative af-

FACTOR STRUCTURE OF THE SWAP-II 313
fect seen in such disorders as dysthymia and generalized anxiety disorder. Although emotional dysregulation and negative affectivity coexist in many patients (particularly those with borderline personality disorder), they ap-pear to have distinct etiologies and treatment implications.
Fourth, the emergence of an Emotional Avoidance trait was an unex-pected but conceptually and clinically meaningful finding with obvious links to such personality constructs as obsessional style (Shapiro, 1965), illusory mental health (Shedler et al., 1993), repressive coping (Weinberg-er, 1995), avoidant, dismissing, or deactivating attachment patterns (Doz-ier & Kobak, 1992), and emotional avoidance (Hayes & Melancon, 1989).
Fifth, the Schizotypy factor is consistent with prior research on the schizotypal personality disorder and the schizophrenia prodrome (e.g., Hawkins et al., 2004), capturing both positive (e.g., odd and idiosyncratic reasoning and perception) and negative (e.g., concreteness of thinking, subthreshold disorganization in thinking) symptoms. It is conceptually re-lated to the Eccentric Perceptions scale of the Schedule of Nonadaptive and Adaptive Personality (SNAP), and its content is conceptually similar to the DSM-IV diagnosis of Schizotypal PD.
Finally, it is noteworthy that the SWAP-II does not produce a higher-order structure resembling the FFM (e.g., Digman, 1990), the consensus four-factor model (Markon et al., 2005), or the five factor personality pa-thology trait model recently proposed for DSM-5. Perhaps the greater com-plexity of some of the SWAP items, designed to capitalize on expertise gained through professional training and experience, permits assessment of clinically important aspects of personality that have not been adequate-ly captured by item sets that rely primarily on personality constructs sa-lient to untrained laypersons. For example, the following SWAP-II items address personality phenomena that are readily recognizable to clinicians but would be extremely difficult to capture via self-report and do not re-semble the level of discourse commonly used by lay observers:
“Is invested in seeing and portraying self as emotionally strong, untrou-bled, and emotionally in control, despite clear evidence of underlying inse-curity, anxiety, or distress.”
“When upset, has trouble perceiving both positive and negative qualities in the same person at the same time; sees others in black or white terms (e.g., may swing from seeing someone as caring to seeing him/her as ma-levolent and intentionally hurtful).”
“Appears unable to describe important others in a way that conveys a sense of who they are as people; descriptions of others come across as two-dimensional and lacking in richness.”
LIMITATIONS
This study concerns the factor structure and content validity of the SWAP-II and does not address questions of interrater and test–retest reliability of the instrument or its construct validity. We present such evidence else-

314 WESTEN ET AL.
where (see also Westen & Shedler, 2007). Future research should evaluate the replicability of the factors presented here using confirmatory factor analysis. Furthermore, we cannot be certain that this sample is represen-tative of the population of patients treated for personality pathology in some absolute sense, although it is more representative than virtually any other sampling approach of which we are aware (in comparison, e.g., to sampling patients who meet PD criteria based on structured interviews from a single setting or small number of clinics affiliated with a university hospital).
CONCLUSIONS AND IMPLICATIONSThe findings suggest that the factor structure of an instrument designed to quantify the concepts and observations of experienced clinicians does not reproduce the FFM or any of its variants. This finding makes sense in light of the lexical hypothesis underlying the FFM, which suggests that language evolves to fit its purposes. The purposes of lay observation and clinical observation of personality are markedly different (as is the level of expertise of the observer). Just as oncologists tend to use more refined concepts than “bumps” or “growing red dots” to describe different forms of cancer, the language required by clinical observers who regularly observe and treat the more pathological end of the personality spectrum should be more differentiated than the language of lay observers (particularly when the latter is constrained for methodological reasons not to exceed a sixth-grade reading level). Factor analysis of the SWAP-II produced a coherent solution with simple structure whose factors were generally highly reli-able, clinically and empirically recognizable, and could not be reduced to a hierarchical structure with a small number of superordinate factors.
More broadly, the finding of clinically coherent factors is consistent with an increasing body of evidence, congruent with research in other medical disciplines (e.g., Arocha, Wang, & Patel, 2005), that clinically trained ob-servers can make reliable, quantifiable diagnostic inferences when these inferences are made at a level of abstraction close to that used in everyday practice (at which doctoral-level clinicians have expertise; DeFife et al., 2010; Westen & Weinberger, 2004). We have yet to observe substantial dif-ferences in the way clinically trained observers of different theoretical ori-entations use the SWAP. This suggests that, when asked to describe a particular patient (as opposed to their hypotheses or beliefs about psycho-pathology), experts in psychopathology are able to do what most people are able to do, namely to describe a person with an appropriate level of fidelity using language appropriate to their level of expertise.
With the next revision of the DSM on the horizon, that revision should be made in the light of data comparing the validity and reliability of alter-native methods of assessing and classifying personality pathology, partic-ularly dimensional diagnosis. Virtually no data exist that compare dimen-sional traits versus diagnostic prototypes (descriptions of constellations of functionally related personality characteristics that comprise clinical syn-
FACTOR STRUCTURE OF THE SWAP-II 315
dromes) on indices of validity (Westen, Gabbard, & Blagov, 2006). Like-wise, no data of which we are aware compare traits derived from self-re-port measures with those derived using item sets designed for clinically expert informants. We are currently testing the comparative validity of multiple alternative approaches to dimensional diagnosis of personality in a study using a multitrait-multimethod approach with a sample size large enough to discriminate the relative validity of these alternative approach-es. If future editions of the DSM are to reflect the best available science, then appropriate scientific comparison of alternative diagnostic systems is a prerequisite.
REFERENCES
Allport, G. (1937). Personality: A psychological interpretation. New York: Henry Holt.
Arocha, J., Wang, D., & Patel, V. (2005). Identifying reasoning strategies in medical decision making: A method-ological guide. Journal of Biomedical Informatics, 38, 154–171.
Bernaads, C., & Jennrich, R. (2005). Gradi-ent projections algorithms and soft-ware for arbitrary rotation criteria in factor analysis. Educational & Psycho-logical Measurement, 65, 676–696.
Bernstein, I., & Teng, G. (1989). Factoring items and factoring scales are differ-ent: Spurious evidence for multidimen-sionality due to item categorization. Psychological Bulletin, 105, 467–477.
Blagov, P., Bradley, R., & Westen, D. (2007). Under the Axis II radar: Clinically rel-evant personality constellations that escape DSM-IV diagnosis. Journal of Nervous & Mental Disease, 195(6), 477–483.
Blagov, P. S., Patrick, C. J., Lilienfeld, S. O., Powers, A. D., Phifer, J. E., Venables, N., et al. (2011). Personality constella-tions in incarcerated psychopathic men. Personality Disorders: Theory, Research, & Treatment, 2, 293–315.
Block, J. (1978). The Q-Sort method in per-sonality assessment and psychiatric research. Palo Alto, CA: Consulting Psychologists Press.
Bradley, B., DeFife, J.A., Guarnaccia, C., Phifer, J., Fani, N., Ressler, K.J., et al. (2011). Emotion dysregulation and negative affect: Association with psy-chiatric symptoms. Journal of Clinical Psychiatry, 72(5), 685–691.
Bradley, B., Westen, D., Mercer, K., Binder,
E., Jovanovic, T., Crain, D., et al. (2011). Association between childhood maltreatment and adult emotional dysregulation in a low income, urban, African American sample: Moderation by oxytocin receptor gene. Develop-ment & Psychopathology, 23, 439–452.
Brown, T., & Barlow, D. (1995). Long-term outcome in cognitive behavioral treat-ment of panic disorder: Clinical pre-dictors and alternative strategies for assessment. Journal of Consulting & Clinical Psychology, 63, 754–765.
Browne, M. (2001). An overview of analytic rotation in exploratory factor analysis. Multivariate Behavioral Research, 36, 111–150.
Clark, L., Livesley, W., Schroeder, M., & Irish, S. (1996). The structure of mal-adaptive personality traits: Conver-gent validity between two systems. Psychological Assessment, 8, 294–303.
Cleckley, H. (1941). The mask of sanity. St. Louis, MO: Mosby.
Clifton, A., Turkheimer, E., & Oltmanns, T. (2005). Self- and peer perspectives on pathological personality traits and in-terpersonal problems. Psychological Assessment, 17, 123–131.
DeFife, J.A., Drill, R., Nakash, O., & Westen, D. (2010). Agreement between clini-cian and patient ratings of adaptive functioning and developmental histo-ry. American Journal of Psychiatry, 167, 1472–1478.
Digman, J. (1990). Personality structure: Emergence of the Five-Factor Model. Annual Review of Psychology, 41, 417–440.
Dozier, M., & Kobak, R. (1992). Psychophysi-

316 WESTEN ET AL.
ology in attachment interviews: Con-verging evidence for deactivating strate-gies. Child Development, 63, 1473–1480.
Flora, D., & Curran, P. (2004). An empirical evaluation of alternative methods of estimation for confirmatory factor analysis with ordinal data. Psychologi-cal Methods, 9, 466–491.
Grice, J. (2001). A comparison of factor scores under conditions of factor obliquity. Psychological Methods, 6, 67–83.
Guttman, L. (1955). The determinacy of fac-tor score matrices with implications for five other basic problems of com-mon-factor theory. British Journal of Statistical Psychology, 8, 65–81.
Hare, R. (2003). Manual for the Hare Psy-chopathy Checklist-Revised (2nd ed.). Toronto, ON: Multi-Health Systems.
Hawkins, K. A., McGlashan, T. H., Quinlan, D., Miller, T. J., Perkins, D. O., Zipur-sky, R. B., et al. (2004). Factorial structure of the Scale of Prodromal Symptoms. Schizophrenia Research, 68, 339– 347.
Hayes, S., & Melancon, S. (1989). Compre-hensive distancing, paradox, and the treatment of emotional avoidance. In L. M. Ascher (Ed.), Therapeutic para-dox (pp. 184–218). New York: Guilford.
Jennrich, R. I. (2002). A simple general method for oblique rotation. Psy-chometrika, 67(1), 7–20.
Klein, D., Ouimette, P., Kelly, H., Ferro, T., & Riso, L. (1994). Test–retest reliability of team consensus best-estimate diag-noses of Axis I and II disorders in a family study. American Journal of Psy-chiatry, 151(7), 1043–1047.
Klonsky, E., Oltmanns, T., & Turkheimer, E. (2002). Informant-reports of personal-ity disorder: Relation to self-reports and future research directions. Clini-cal Psychology: Science & Practice, 9, 300–311.
Krueger, R., & Finger, M. (2001). Using item response theory to understand comor-bidity among anxiety and unipolar mood disorders. Psychological Assess-ment, 13(1), 140–151.
Krueger, R. F., & Markon, K. E. (2011). A di-mensional-spectrum model of psycho-pathology. Archives of General Psychi-atry, 68, 10–11.
Krueger, R., Markon, K., Patrick, C., & Iaco-no, W. (2005). Externalizing psycho-
pathology in adulthood: A dimension-al-spectrum conceptualization and its implications for DSM-V. Journal of Ab-normal Psychology, 114, 537–550.
Krueger, R., Watson, D., & Barlow, D. (2005). Introduction to the special section: To-ward a dimensionally based taxonomy of psychopathology. Journal of Abnor-mal Psychology, 114, 491–493.
Livesley, W., Jang, K., & Vernon, P. (1998). Phenotypic and genetic structure of traits delineating personality disorder. Archives of General Psychiatry, 55, 941–948.
Markon, K., Krueger, R., & Watson, D. (2005). Delineating the structure of normal and abnormal personality: An integrative hierarchical approach. Journal of Personality & Social Psy-chology, 88, 139–157.
McDonald, R. (1965). Difficulty factors and non-linear factor analysis. British Journal of Mathematical & Statistical Psychology, 18(1), 11–23.
McDonald, R., & Mulaik, S. (1979). Determi-nacy of common factors: A nontechni-cal review. Psychological Bulletin, 86(2), 297–306.
Micceri, T. (1989). The unicorn, the normal curve, and other improbable crea-tures. Psychological Bulletin, 105, 156–166.
Miller, J., & Pilkonis, P. (2006). Neuroticism and affective instability: The same or different? American Journal of Psychi-atry, 163, 839–845.
Mischel, W., & Shoda, Y. (1995). A cognitive-affective system theory of personality: Reconceptualizing situations, disposi-tions, dynamics, and invariance in personality structure. Psychological Review, 102(2), 246–268.
Mislevy, R. (1986). Recent developments in the factor analysis of categorical vari-ables. Journal of Educational Statis-tics, 11, 3–31.
Morey, L. (1988). Personality disorders in DSM-III and DSM-III-R: Convergence, coverage, and internal consistency. American Journal of Psychiatry, 145, 573–577.
Muthen, B., & Kaplan, D. (1985). A compari-son of some methodologies for the fac-tor analysis of non-normal Likert vari-ables. British Journal of Mathematical & Statistical Psychology, 38(2), 171–189.

FACTOR STRUCTURE OF THE SWAP-II 317
Muthen, B., & Speckart, G. (1983). Catego-rizing skewed, limited dependent vari-ables: Using multivariate probit re-gression to evaluate the California Civil Addict Program. Evaluation Re-view, 7, 257–269.
Oldham, J., & Skodol, A. (2000). Charting the future of Axis II. Journal of Person-ality Disorders, 14(1), 17–29.
Pezawas, L., Meyer-Lindenberg, A., Drabant, E. M., Verchinski, B. A., Munoz, K. E., Kolachana, B. S., et al. (2005). 5- HTTLPR polymorphism impacts hu-man cingulate-amygdala interactions: A genetic susceptibility mechanism for depression. Nature Neuroscience, 8, 828–834.
Pilkonis, P., Heape, C., Ruddy, J., & Serrao, P. (1991). Validity in the diagnosis of personality disorders: The use of the LEAD standard. Psychological Assess-ment, 31, 46–54.
Quiroga, A. (1992). Studies of the polychoric correlations and other correlation mea-sures for ordinal data. Unpublished doctoral dissertation, University of Uppsala
Rottman, B. M., Ahn, W., Sanislow, C. A., & Kim, N. S. (2009). Can clinicians rec-ognize DSM-IV personality disorders from five-factor model descriptions of patient cases? American Journal of Psychiatry, 166, 427–433.
Rozeboom, W. (1992). The glory of subopti-mal factor rotation: Why local minima in analytic optimization of simple structure are more blessing than curse. Multivariate Behavioral Research, 27(4), 585–599.
Russ, E., Heim, A., & Westen, D. (2003). Pa-rental bonding and personality patholo-gy assessed by clinician report. Journal of Personality Disorders, 17, 522–536.
Sass, D. & Schmitt, T. (2010). A comparative investigation of rotation criteria within exploratory factor analysis. Multivari-ate Behavioral Research, 45, 73–103.
Shapiro, D. (1965). Neurotic styles. New York: Basic Books.
Shedler, J., Mayman, M., & Manis, M. (1993). The illusion of mental health. American Psychology, 48, 1117–1131.
Shedler, J., & Westen, D. (2004a). Dimen-sions of personality pathology: An al-ternative to the Five Factor Model. American Journal of Psychiatry, 161, 1743–1754.
Shedler, J., & Westen, D. (2004b). Refining personality disorder diagnoses: Inte-grating science and practice. American Journal of Psychiatry, 161, 1350–1365.
Shedler, J., & Westen, D. (2007). The Shed-ler–Westen Assessment Procedure (SWAP): Making personality diagnosis clinically meaningful. Journal of Per-sonality Assessment, 89, 41–55.
Spitzer, R. L., First, M. B., Shedler, J., West-en, D., & Skodol, A. E. (2008). Clinical utility of five dimensional systems for personality diagnosis: A “consumer preference” study. Journal of Nervous & Mental Disease, 196, 356–374.
Waller, N. (1999). Searching for structure in the MMPI. In S. Embretson & S. Her-shberger (Ed.), The new rules of mea-surement: What every psychologist and educator should know (pp. 185–218). Mahwah, NJ: Lawrence Erlbaum.
Waller, N. (2001). WinMicroFACT 2.0: A mi-crocomputer factor analysis program for ordered polytomous data and main-frame sized problems. St. Paul, MN: Assessment Systems Corporation.
Waller, N., & Meehl, P. (1998). Multivariate taxometric procedures: Distinguishing types from continua (Vol. 9). Thousand Oaks, CA: Sage.
Waller, N., Tellegen, A., McDonald, R., & Lykken, D. (1996). Exploring nonlin-ear models in personality assessment: Development and preliminary valida-tion of a negative emotionality scale. Journal of Personality, 64, 545–576.
Watson, D., Clark, L., & Harkness, A. (1994). Structures of personality and their rel-evance to psychopathology. Journal of Abnormal Psychology, 103, 18–31.
Weinberger, J. (1995). Common factors aren’t so common: The common fac-tors dilemma. Clinical Psychology: Sci-ence & Practice, 2(1), 45–69.
West, S., Finch, J., & Curran, P. (1995). Structural equation models with non-normal variables: Problems and reme-dies. In R.H. Hoyle (Ed.), Structural equation modeling: Concepts, issues, and applications (pp. 56–75). Thou-sand Oaks, CA: Sage.
Westen, D., Dutra, L., & Shedler, J. (2005). Assessing adolescent personality pa-thology: Quantifying clinical judg-ment. British Journal of Psychiatry, 186, 227–238.

318 WESTEN ET AL.
Westen, D., Gabbard, G., & Blagov, P. (2006). Back to the future: Personality struc-ture as a context for psychopathology. In R. F. Krueger & J. L. Tackett (Eds.), Personality and psychopathology: Building bridges. New York: Guilford.
Westen, D., & Muderrisoglu, S. (2003). Reli-ability and validity of personality dis-order assessment using a systematic clinical interview: Evaluating an alter-native to structured interviews. Jour-nal of Personality Disorders, 17, 350–368.
Westen, D., & Muderrisoglu, S. (2003). Reli-ability and validity of personality dis-order assessment using a systematic clinical interview: Evaluating an alter-native to structured interviews. Jour-nal of Personality Disorders, 17, 350–368.
Westen, D., & Muderrisoglu, S. (2006). Clini-cal assessment of pathological person-ality traits. American Journal of Psy-chiatry, 163, 1285–1287.
Westen, D., Muderrisoglu, S., Fowler, C., Sh-edler, J., & Koren, D. (1997). Affect regulation and affective experience: Individual differences, group differ-ences, and measurement using a Q-sort procedure. Journal of Consulting & Clinical Psychology, 65, 429–439.
Westen, D., & Shedler, J. (1999a). Revising and assessing Axis II, Part 1: Develop-ing a clinically and empirically valid assessment method. American Journal of Psychiatry, 156, 258–272.
Westen, D., & Shedler, J. (1999b). Revising and assessing Axis II, Part 2: Toward an empirically based and clinically useful classification of personality dis-orders. American Journal of Psychia-try, 156, 273–285.
Westen, D., & Shedler, J. (2000). A prototype matching approach to diagnosing per-sonality disorders toward DSM-V. Journal of Personality Disorders, 14, 109–126.
Westen, D., & Shedler, J. (2007). Personality diagnosis with the Shedler–Westen Assessment Procedure (SWAP): Inte-grating clinical and statistical mea-surement and prediction. Journal of Abnormal Psychology, 116(4), 810–822.
Westen, D., Shedler, J., & Bradley R. (2006). A prototype approach to personality disorder diagnosis. American Journal of Psychiatry, 163, 846–856.
Westen, D., Shedler, J., Bradley, B., & DeFife, J. A. (2012). An empirically de-rived taxonomy for personality diagno-sis: Bridging science and practice in conceptualizing personality. American Journal of Psychiatry, 169, 273–284.
Westen, D., & Weinberger, J. (2004). When clinical description becomes statistical prediction. American Psychologist, 59, 595–613.
Widiger, T. A., Costa, P. T., & McCrae, R. R. (2002). A proposal for Axis II: Diagnos-ing personality disorders using the five factor model. In P. T. Costa & T. A. Widiger (Eds.), Personality disorders and the five factor model of personality (2nd ed., pp. 431–456). Washington, DC: American Psychological Associa-tion.
Widiger, T., & Samuel, D. (2005). Diagnostic categories or dimensions? A question for the Diagnostic and Statistical Man-ual of Mental Disorders–Fifth Edition. Journal of Abnormal Psychology, 114, 494–504.
Widiger, T., & Simonsen, E. (2005). Alterna-tive dimensional models of personality disorders: Finding a common ground. Journal of Personality Disorders, 19, 110–130.
Widiger, T., Simonsen, E., Krueger, R., Lives-ley, J., & Verheul, R. (2005). Personal-ity disorder research agenda for the DSM-V. Journal of Personality Disor-ders, 19, 315–338.
Widiger, T, & Trull, T. (2007). Plate tectonics in the classification of personality dis-order: Shifting to a dimensional mod-el. American Psychologist, 62, 71–83.
Wilkinson, R., & Westen, D. (2000). Identity disturbance in borderline personality disorder: An empirical investigation. American Journal of Psychiatry, 157, 528–541.
Wood, R., Wilson, D., Gibbons, R., Schil-lings, S., Muraki, E., & Bock R. (2002). TESTFACT. In M. D. Toit (Ed.), IRT from SSI (pp. 410–504). Lincolnwood, IL: Scientific Software International.