digest this - cleveland clinic
TRANSCRIPT

{InsIde thIs Issue}
Maximizing Minimally Invasive Colorectal Surgery p.2
Why Colorectal Surgeon and Pathologist Collaboration is Essential p.4
Case Study: Retroperitoneal Sarcoma p.12
Digestive Disease institute | winter | 2012
Digestthis
Three Genes Linked to BE/EAC Discovered p.1
Digestive Diseases 2017What lies ahead for
our subspecialties? – p.6
dear Colleagues,
I am honored to recently have been named Chair of the Department of Gastroenterology
and Hepatology in Cleveland Clinic’s Digestive Disease Institute (DDI) and to introduce
the Winter 2012 issue of Digest This.
During my nearly 20 years as a gastroenterologist here at Cleveland Clinic, our field
has evolved dramatically – and the rapid pace shows no sign of slowing down any time
soon. In this issue, we usher in the new year with a cover story (p. 6) that examines
what each of our department chairs (myself and Drs. Feza H. Remzi, R. Matthew Walsh,
Steven Wexner, Roger Charles and Raul Rosenthal) believe are the hottest innovations
of today and what likely lies ahead for the subspecialties within our institute: colorectal
surgery, gastroenterology and hepatology, and general surgery, including bariatrics. In
another forward-thinking discussion (p. 2), Drs. Meagan Costedio, David Maron and
Dana Sands share how they are using various minimally invasive approaches in their
practice and the advances they see on the horizon.
We also provide updates on other DDI key specialties. On p. 1, we discuss ground-
breaking research by Dr. Charis Eng and colleagues that has identified genetic muta-
tions specific to patients with Barrett’s esophagus and esophageal adenocarcinoma,
which may one day aid risk assessment and increase patient survival. On p. 4, we
feature two case studies that demonstrate why collaboration between pathologist and
colorectal surgeon is essential. In addition, we showcase our bariatric services (p.11)
and a case study by Dr. Sricharan Chalikonda (p. 12) that shows why the multidisci-
plinary approach used within our Surgical Oncology Clinic is key to caring for patients
with retroperitoneal sarcomas.
I hope you enjoy this issue of Digest This and we look forward to collaborating with
you to provide the best possible care for your patients.
Sincerely,
John Vargo, MD, MPHChair, Department of Gastroenterology and Hepatology | Vice-Chair, Digestive Disease Institute | [email protected]

clevelandclinic.org/digestive 855.REFER.123 {1}
Digestive Disease Institute
three genes Linked to Be/eaC Discovered
Researchers at Cleveland Clinic’s Genomic Medicine Institute have identified
genetic mutations specific to patients with Barrett’s esophagus (BE) and esophageal
adenocarcinoma (EAC). And that’s inspired continued research by a team led by
Charis eng, MD, PhD, Chair and Founding Director of the genomic Medicine institute,
which could ultimately aid risk assessment and increase patient survival.
The study by Dr. Eng, published in the July 27,
2011 issue of the Journal of the American Medical
Association, identified three genes specifically linked
to BE/EAC. It’s been Dr. Eng’s goal to find that link
after a colleague’s mother died from EAC during Dr.
Eng’s medical oncology fellowship at Dana-Farber
Cancer Institute.
“My colleague, a professor, told me the whole family
had Barrett’s, and one or two developed into esopha-
geal cancer,” Dr. Eng says. “And ever since, I thought
about this gene.”
Related to gastroesophageal reflux disease, BE is
estimated to occur in up to 10 percent of the popula-
tion and diagnoses have tripled since 1970. BE is
believed to be a precursor to EAC. But EAC is typi-
cally not diagnosed until its advanced stages, when
chances of survival are poor.
To find genetic markers for BE/EAC, Dr. Eng led
researchers at 16 U.S. institutions to identify and
evaluate 298 participants with BE, EAC, or both be-
tween 2005 and 2010. The study used the latest in
genomics approaches and state-of-the art technology,
along with functional genomic validation, to identify
MSR1, ASCC1, and CTHRC1 as three genes mutated
in 11 percent of the BE/EAC patients studied, indica-
tive of a significant genetic predisposition. Mutations
in MSR1 were the most common, affecting seven per-
cent of the patients studied – and warranting further
study, Dr. Eng says.
Dr. Eng and her team have created and are now part
of the Familial Barrett Esophagus Consortium, working
with researchers at Johns Hopkins University School
of Medicine in Baltimore and Albert Einstein College of
Medicine of Yeshiva University in New York City. They
are seeking families with at least two relatives with
BE and/or EAC to search for susceptibility genes. They
also will accrue young onset BE (under age 60) or EAC
(under age 50).
Dr. Eng hopes to find study participants in a relatively
short period of time through study referrals – and
Cleveland Clinic patients seeking care for BE and EAC.
“We see these patients in clinic, and they fly in from
around the world,” Dr. Eng says. “But that’s what
happens at Cleveland Clinic – our ability to recognize
and our ability to treat unknowns attracts patients from
around the country and the world.”
The studies could lead to a tool to estimate a person’s
risk of having BE/EAC, similar to the Genomic Medicine
Institute’s online risk calculator for estimating risk for
a PTEN mutation, often associated with Cowden syn-
drome and Bannayan-Riley-Ruvalcaba syndrome.
Ultimately, the ability to identify genetic markers for BE
and EAC could help with risk assessment, early detec-
tion, improved disease management and, eventually,
increased survival.
Dr. Eng is Chair and Founding Director of the Genomic
Medicine Institute of the Lerner Research Institute at
Cleveland Clinic. She can be reached at [email protected]
or 216.444.3440. ■
Charis eng, Md, Phd
Recommended Reading: Familial Barrett Esophagous and Esophageal Adenocarcinoma. www.lerner.ccf.org/gmi/research/fbe/
10%BE is estimated to occur
in up to 10 percent of the
population and diagnoses
have tripled since 1970.
{2} digest this Winter | 2012
Cleveland Clinic
sPeCiaL Feature
Minimally Invasive Colorectal surgery
A new era in minimally invasive colorectal surgery has begun. MIS is now routinely used to treat an
increasing number of colon and rectal conditions. With experience and technological advancements,
more and more minimally invasive procedures can match the outcomes of conventional open surgery,
with shorter hospital stays and better cosmetic results for patients.
Here, we talk to colorectal surgeons Meagan Costedio, MD, from our main campus and David Maron,
MD, and Dana Sands, MD, from Cleveland Clinic Florida to get their views on how they are utilizing
laparoscopy, single-port surgery, natural orifice surgery (NOTES), robotics and transanal endoscopic
microsurgery (TEM) today and the advances they see on the horizon.
LAPAROSCOPY
“When laparoscopy was new in the 1990s,
many colorectal surgeons thought it was
a bad idea. It was never going to apply to
colon surgery,” recalls Dr. Costedio. “It was
good for gallbladder surgery, but for colon
surgery – not worth the time or the effort.”
As surgeons’ laparoscopic skills improved
over time, they realized they could tackle
more than a gallbladder or an appendix.
Incisions got smaller. OR times dropped,
instruments got better, and surgeons started
doing right and left colectomies until it
became commonplace.
“Now, the data shows that laparoscopy means
shorter hospital stays, better outcomes for
patients, and equivalent cancer surgery,” Dr.
Costedio says. “So now, it’s widely accepted
that laparoscopy is better and whether sur-
geons do it or not is their own preference.”
As technology gets better and the instru-
ments for laparoscopy get smaller and more
advanced, surgeons will be able to complete
more advanced, difficult surgeries laparo-
scopically, expanding this technology to
other fields, she says. “The instrumentation
is becoming so advanced that we may see a
day when surgeons are able to operate inside
the colon and rectum which would mean no
incisions for patients.”
SINGLE PORT
“One of the unique facets of colon surgery,
which is not true of every specialty, is that
the surgeon must remove the colon intact,”
Dr. Costedio says. “This means that we
always need a 2- to 3-cm incision to get the
colon out.” Three centimeters is plenty of
room to put two instruments and a camera
and remove a colon with no added incisions.
So, as the tables got better, and the instru-
ments got better and the cameras got better,
single-port colorectal surgery was made
feasible. Now, Dr. Costedio says she removes
one to two colons weekly with a single-port
technique that leaves a small incision in the
umbilicus that’s either not visible or a just
barely noticeable. She also uses patients’
ileostomy sites for the incision.
“Particularly for young people, I think
there’s a real benefit to not having incisions
all over your abdomen cosmetically,” she
says. “While we still need randomized stud-
ies, surgeons who are good at it are doing
so because they believe that the results are
equal to laparoscopy. I think it’s the future
of colon and rectal surgery as we keep
moving forward.”

clevelandclinic.org/digestive 855.REFER.123 {3}
Digestive Disease Institute
ROBOTICS
Traditional laparoscopic surgery has some limi-
tations which can create obstacles in complex
and difficult operations. This is caused by the
peculiar drawbacks of laparoscopy, mainly
related to unstable video camera imaging,
which is dependent on the assistant’s skills
and is not under the surgeon’s control, the
limited motion of instruments, the related
loss of dexterity, and two dimensional imag-
ing. Robotic-assisted surgery theoretically
may overcome these pitfalls, Dr. Maron says,
because it includes three-dimensional imag-
ing under the surgeon’s direct control, and
provides instruments with seven degrees of
freedom that mimic the hand movements
and dexterity of the surgeon.
“Although data in the literature is limited,
while the use of the robot may prove to be
useful in colon surgery, its greatest benefits
are likely to be in minimally-invasive pro-
cedures involving the pelvis (rectal cancer,
rectal prolapse),” he says. Early studies have
demonstrated a decrease in the conversion
rate to open surgery in patients with rectal
cancer. DDI is now using robotics for these
deep pelvic surgery cases, but more long-
term studies are needed.
NOTES
Natural orifice transluminal endoscopic
surgery (NOTES) has encouraged industry
to catapult technology light years ahead.
However, Dr. Costedio says most general
surgeons and colorectal surgeons tend
to prefer to use the umbilicus – to avoid
disastrous holes in the stomach or colo-
vaginal fistulae.
“I think single port has been propelled from
the technology advancements from NOTES,”
she says. “And while there are people who
are good at it, NOTES is being held back
a bit because of the nervousness of these
potentially disastrous complications.”
TEM
Transanal endoscopic microsurgery (TEM) is
an older technology that served as colorectal
surgery’s gateway to NOTES. This technique
affords patients with benign and early-stage
rectal lesions an alternative to more radical
rectal resections, explains Dr. Sands.
“The technique is virtually pain free and
usually requires only an overnight hospital
stay,” Dr. Sands says. While the procedure
was first described in the early 1980s, it
did not generate significant interest due to
the complexity of the instrumentation and
surgeons difficulty learning the technique.
With the advent of laparoscopic surgery, and
the subsequent adoption of these procedures,
colorectal surgeons became for facile with
minimally invasive techniques, thereby spark-
ing a resurgence of interest in TEM in the
early part of 2000.
TEMS is an excellent alternative for a very se-
lect number of patients, including people with
large polyps in the rectum, very early rectal
cancers, and for debulking tumors in those
cancer patients who can’t withstand a big
operation. However, its application remains
limited, Dr. Costedio adds, because the TEM
instruments are straight unlike the robot’s,
which are wristed.
“As technology advances, if we’re able to get
wristed instruments thru the TEM machine,
we will be able to transect the rectum, and
take out the colon, through the anus. And
that will be the most pure form of NOTES
because we’re making a hole that needs
to be made anyway. But right now, the
instrumentation is not quite ready. There
are a few people trying it in cadavers,
but it’s quite difficult.
“Yet, TEM itself is very good. Unfortunately,
there’s a limited disease process that we can
fix with it. But it means no incisions – often
sparing somebody an abdominal operation,
going right back to work, minimal pain and
short, if any, hospital stay.”
To refer a patient for minimally invasive
colorectal surgery at DDI’s main campus,
call 1.855.REFER.123. Call 954.659.5278
for referrals to Cleveland Clinic Florida,
Weston. ■
Fascinated with forward-thinking discussions?Join us for any of the following upcoming
symposiums, which will tackle some of the
toughest issues in the diagnosis, treatment
and prevention of digestive diseases:
Feb. 14-19, 2012
23rd Annual International Colorectal
disease symposium
Combined
33rd Annual turnbull symposium
Feb. 17-18, 2012
Gastroenterology & hepatology symposium
Feb. 19-22, 2012
11th Annual surgery of the Foregut
To learn more or register for any of these
events, visit ClevelandClinicFloridaCME.org.

{4} digest this Winter | 2012
Cleveland Clinic
Behind the scenesWhy close collaboration between colorectal surgeon and pathologist is essential
At Cleveland Clinic, patients benefit from a unique partnership between colorectal surgeons
in its Digestive Disease Institute and pathologists in its Pathology and Laboratory Medicine
Institute. Very few institutions have the level of collaboration, cooperation and expertise
found between these two disciplines at both Cleveland Clinic’s main campus and Cleveland
Clinic Florida. Here we take a closer look at two cases that exemplify why the expertise of
our pathology colleagues is critical in allowing our colorectal surgeons to make key treatment
decisions to improve the care we provide to inflammatory disease and rectal cancer patients.
Case stuDy
CAse 1
Presentation: 51-year-old woman presents at an
outside institution with rectal bleeding. She had no
other significant clinical history.
diagnostics: A 1.7 cm pedunculated polypoid lesion,
7 cm from the anal verge, was colonoscopically com-
pletely removed at another hospital.
Pathological findings: A diagnosis of a “focus of well-
differentiated adenocarcinoma arising in a tubulovil-
lous adenoma” was rendered at the original institution
at which the polyp was removed. Based on the latter
diagnosis, the patient was referred to our colorectal
surgery department for radical surgery: a low anterior
resection. Our review of the outside slides revealed a
small focus of superficially invasive, well-differentiated
adenocarcinoma arising in a tubulovillous adenoma. The
invasive carcinoma involved only the head of the polyp
(Haggit level 1) without any vascular invasion or tumor
“budding.” The deepest level of the invasive carcinoma
was 6 mm from the stalk margin of resection.
Clinical Course: Based upon these histopathological
findings, a transanal excision rather than a low anterior
resection was recommended. Since no residual tumor
was identified, no additional surgery was undertaken.
Subsequent to that transanal excision, repeated endo-
scopic and imaging assessment have shown her to be
free of any disease.
discussion: The treatment of the so called “malignant
polyp” is often challenging and reaching a balance be-
tween the risks and benefits of radical resection vs. local
excision may be difficult to achieve. The pathologist
plays a critical role in the treatment decision process.
The accurate and consistent assessment of a group of
histological parameters that carry prognostic implica-
tions is essential to reach the best treatment decision
for each patient.
The level of tumor invasion within the wall of the
polyp, the presence of vascular invasion, the grade
of tumor differentiation and the distance of the
invasive carcinoma to the deep margin of resection
should routinely be assessed and documented in the
pathology report. Overall, malignant polyps could be
classified into those with “favorable histology” and
those with “unfavorable histology.” Well-differentiated
lesions with superficial invasion limited to the wall
of the polyp (head and neck of pedunculated polyps
and the superficial aspect of the submucosa in
sessile polyps), absence of vascular invasion and a
clear margin (2 mm or more) are features usually
associated with a low risk of lymph node metasta-
sis or residual carcinoma in the wall of the bowel.
Therefore, local excision seems to be a safe option
in these instances. Conversely, in cases in which one
or more unfavorable histological markers are identi-
fied, a radical surgical resection will likely be more
appropriate. In this particular case, the patient was
referred to us for a low anterior resection. However,
after critical re-evaluation of the histology slides and
based on the absence of poor prognostic markers, a
transanal excision was performed. No residual tumor
was identified. ■
Mariana Berho, Md Pathology Cleveland Clinic Florida
steven Wexner, Md Colorectal Surgery Cleveland Clinic Florida
clevelandclinic.org/digestive 855.REFER.123 {5}
Digestive Disease institute
P. Ravi Kiran, Md Colorectal Surgery Cleveland Clinic
Xiuli Liu, Md, Phd Pathology Cleveland Clinic
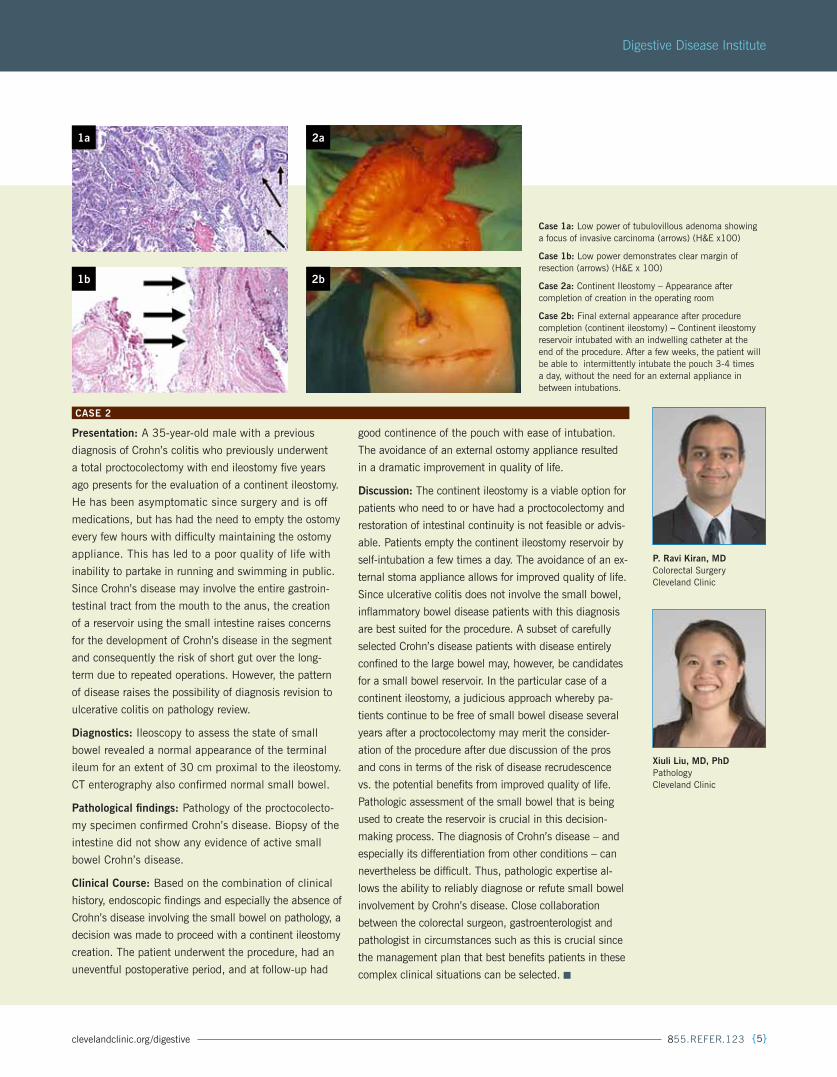
Case 1a: Low power of tubulovillous adenoma showing a focus of invasive carcinoma (arrows) (H&E x100)
Case 1b: Low power demonstrates clear margin of resection (arrows) (H&E x 100)
Case 2a: Continent Ileostomy – Appearance after completion of creation in the operating room
Case 2b: Final external appearance after procedure completion (continent ileostomy) – Continent ileostomy reservoir intubated with an indwelling catheter at the end of the procedure. After a few weeks, the patient will be able to intermittently intubate the pouch 3-4 times a day, without the need for an external appliance in between intubations.
CAse 2
Presentation: A 35-year-old male with a previous
diagnosis of Crohn’s colitis who previously underwent
a total proctocolectomy with end ileostomy five years
ago presents for the evaluation of a continent ileostomy.
He has been asymptomatic since surgery and is off
medications, but has had the need to empty the ostomy
every few hours with difficulty maintaining the ostomy
appliance. This has led to a poor quality of life with
inability to partake in running and swimming in public.
Since Crohn’s disease may involve the entire gastroin-
testinal tract from the mouth to the anus, the creation
of a reservoir using the small intestine raises concerns
for the development of Crohn’s disease in the segment
and consequently the risk of short gut over the long-
term due to repeated operations. However, the pattern
of disease raises the possibility of diagnosis revision to
ulcerative colitis on pathology review.
diagnostics: Ileoscopy to assess the state of small
bowel revealed a normal appearance of the terminal
ileum for an extent of 30 cm proximal to the ileostomy.
CT enterography also confirmed normal small bowel.
Pathological findings: Pathology of the proctocolecto-
my specimen confirmed Crohn’s disease. Biopsy of the
intestine did not show any evidence of active small
bowel Crohn’s disease.
Clinical Course: Based on the combination of clinical
history, endoscopic findings and especially the absence of
Crohn’s disease involving the small bowel on pathology, a
decision was made to proceed with a continent ileostomy
creation. The patient underwent the procedure, had an
uneventful postoperative period, and at follow-up had
good continence of the pouch with ease of intubation.
The avoidance of an external ostomy appliance resulted
in a dramatic improvement in quality of life.
discussion: The continent ileostomy is a viable option for
patients who need to or have had a proctocolectomy and
restoration of intestinal continuity is not feasible or advis-
able. Patients empty the continent ileostomy reservoir by
self-intubation a few times a day. The avoidance of an ex-
ternal stoma appliance allows for improved quality of life.
Since ulcerative colitis does not involve the small bowel,
inflammatory bowel disease patients with this diagnosis
are best suited for the procedure. A subset of carefully
selected Crohn’s disease patients with disease entirely
confined to the large bowel may, however, be candidates
for a small bowel reservoir. In the particular case of a
continent ileostomy, a judicious approach whereby pa-
tients continue to be free of small bowel disease several
years after a proctocolectomy may merit the consider-
ation of the procedure after due discussion of the pros
and cons in terms of the risk of disease recrudescence
vs. the potential benefits from improved quality of life.
Pathologic assessment of the small bowel that is being
used to create the reservoir is crucial in this decision-
making process. The diagnosis of Crohn’s disease – and
especially its differentiation from other conditions – can
nevertheless be difficult. Thus, pathologic expertise al-
lows the ability to reliably diagnose or refute small bowel
involvement by Crohn’s disease. Close collaboration
between the colorectal surgeon, gastroenterologist and
pathologist in circumstances such as this is crucial since
the management plan that best benefits patients in these
complex clinical situations can be selected. ■
1a 2a
1b 2b

{6} digest this Winter | 2012
Cleveland Clinic
COVER FEATuRE
Digestive Diseases
W H A T L I E S A H E A D F O R O u R S u B S P E C I A L T I E S ?
In our rapidly evolving subspecialties – colorectal surgery, gastroenterology and general
surgery – there are two ever-present questions: “What’s hot?” and “What’s next?”
So, Digestive Disease Institute Chairman John Fung, MD, posed these questions to his
department chairs, both at our main campus and at Cleveland Clinic Florida, Weston.
Here’s what they had to say about innovation, both today and tomorrow:

clevelandclinic.org/digestive 855.REFER.123 {7}
Digestive Disease Institute
John Vargo, Md, MPhChair, Gastroenterology & Hepatology | Cleveland Clinic Main Campus
What’s hot in gastroenterology right now is the
detection and treatment of dysplastic and precan-
cerous lesions throughout the GI tract. Now, with
advances in endoscopy – including high-definition and zoom
endoscopy, with the use of supravital staining – we are much
more efficient at detecting abnormalities in various premalig-
nant conditions, such as Barrett’s esophagus, ulcerative colitis
and Crohn’s colitis. In particular, with Barrett’s esophagus, we
follow one of the largest groups of patients in the nation and
can now treat a subset of these lesions endoscopically that
were only treatable surgically 10 years ago.
Another area where we are seeing rapid advances is in extend-
ing the endoscope’s range. We’re now able to place them in the
biliary tree, which helps us treat conditions, such as stones, and
obtain tissue for diagnosis. With balloon enteroscopy, we’re able
to achieve examination of the small bowel endoscopically, which
aids in diagnosis and treatment.
There’s also been incredible development in the treatment of
refractory Hepatitis C with the release of protease inhibitors.
Another pharmacologic advance is immunomodulator agents for
IBD, which have been hugely successful for controlling disease
activity and limiting morbidities from other medications.
Here at DDI, one of the key characteristics that sets us apart is
taking the expertise of the gastroenterology and surgical special-
ties and combining them in multidisciplinary clinics, such as
our pancreas and hepatoma clinics. I think there’s an incredible
benefit because there’s a synergistic discussion, which helps us
provide efficient and timely patient care.
With developments in proteomics and genetic research, we’re
probably going to see screening tests based biologic samples,
that are obtained during endoscopy or through a simple blood
test. We will likely see more and more gene-centered medical
therapy for Crohn’s disease, liver disease and perhaps even
for Barrett’s esophagus. Another possibility is preemptive vac-
cines for patients with a predilection for the development of
Crohn’s disease, ulcerative colitis or Barrett’s esophagus.
On the technological front, we will probably see the develop-
ment of steerable endoscopy capsules, which may use biologic
triggers. For example, it may be able to sense blood or specific
morphology and turn itself on to document what it’s see-
ing. Or, alternatively, it may use the triggering mechanism to
render therapy or maybe even to do biopsies. I also anticipate
growth in a computer-rendered virtual examination. I believe
in the future that we are going to be able to perform endo-
scopic procedures from our desktops, and we may actually be
consulted from across the world to look at a particular image
and perhaps even render therapy.
Lastly, we are utilizing The Knowledge Program to record
demographic and clinical data in the electronic medical record.
We’ve only just begun to scratch the surface of the power of
the electronic medical record in terms of data mining. I really
believe that in the future through simple questions and tests,
we will be able to stratify patients’ risk for certain disease pro-
cesses and hopefully be able to intervene in a chemopreventive
manner before the disease process even starts. ■
What innovations in your field today are improving the care your staff at the
ddI provide to patients? What emerging advances do you believe will have the
biggest impact on your subspecialty over the next five to 10 years?Q:A:
{8} digest this Winter | 2012
Cleveland Clinic
Raul Rosenthal, MdChair, Bariatric and Metabolic Institute | Cleveland Clinic Florida
In bariatric and metabolic surgery, the introduction
and standardization of sleeve gastrectomy as a new
surgical treatment option for morbidly obese patients
will become the most prevalent procedure performed in bariatric
centers for this patient population.
It is a simple technique, which results in excellent weight loss
and resolution of co-morbid conditions, including remission of
metabolic syndrome and type 2 diabetes mellitus, when com-
pared to other well-established procedures.
In addition, there are no nutritional deficiencies that have been
described in long-term follow-up series. But, most importantly,
the sleeve gastrectomy has a significantly lower morbidity when
compared to all other surgical options for weight loss. ■
Feza h. Remzi, MdChair, Colorectal Surgery | Cleveland Clinic Main Campus
In colorectal surgery, there are three areas in which
we are currently making significant leaps in the field
and where there will be tremendous advances in the
next five to 10 years: surgical technology, collaborative innova-
tion and translational research.
In surgical technology, we’ve been the leader in single-port
surgery, which has really taken MIS to an entirely different
level – with potentially less pain, early recovery times and better
cosmesis. Robotic surgery also is complementing single port-
surgery, being performed here at DDI by Drs. Meghan Costedio,
Ihya Emre Gorgun and Brooke Gurland. In addition, the combina-
tion of endoscopy and laparoscopy techniques into one picture
is very important – such as in new mucosal resections initiated
by Dr. Gorgun for precancerous or early cancerous lesions. This
marriage of technologies means that we can now minimize the
trauma in procedures for certain tumors or lesions that previously
required major surgery. While much has been recently accom-
plished, I think there is potential capability to push the envelope
even further with even newer techniques in the near future.
Innovative collaborations also are helping us improve the care
we deliver to patients today. Not only does our Institute model
of medicine make multidisciplinary approaches possible, such
as disease-specific clinics where radiologists, pathologists,
surgeons, oncologists and radiation therapists discuss cases
and arrive at uniform decisions. But, we are hoping to use this
experience and work with other centers across the nation to
help establish national center for excellence guidelines for the
treatment of rectal cancer. This year, together with Cleveland
Clinic Florida, our department brought together an alliance to
begin these discussions and we are excited at the prospect of
being able to potentially improve the care offered patients with
this extremely complex pathology.
In translational research, Dr. Matthew Kalady has been making
remarkable headway in his work on the genetics of colorectal
cancer. I think in the future, work such as his will make it pos-
sible to optimize patients’ treatments with medications that will
impact their genes and eliminate their pathology. This move to
gene therapy will impact our subspecialty in the next five to 10
years. The other area that is going to impact us is stem cell re-
search, such as that currently being done at DDI by Dr. Massarat
Zutshi for fecal incontinence, which I think will revolutionize our
field in pelvic floor. ■
A:
A:

clevelandclinic.org/digestive 855.REFER.123 {9}
Digestive Disease Institute
R. Matthew Walsh, MdChair, General Surgery | Cleveland Clinic Main Campus
Some of the most innovative procedures we are
performing today for transplant are composite tissue
transfer grafts, including abdominal wall replace-
ments. We have already performed one in our department and
look for that to be a component of future direction. This would
help meet and unmet need for patients who have had complex
prior abdominal surgery and have lost a significant portion of
their small intestine, or have had failed complex hernia repairs.
Islet cell transplants are another big area. In the future, there
is a real potential for allo-islet cell transplants for diabetes. There
are prospects for developing an islet program here as well as
performing isolated pancreatic transplants for diabetes. I also
see room for growth in our small bowel transplant program. In
addition, organ preservation is hopefully going to reach another
level. We are actively involved in research with oxygenating
organs to extend organ time and outcome.
In oncology, we are trying to build more integrated systems
between our main campus and community programs. We want
to move advanced procedures, such as robotics, out to the
community to increase accessibility. Probably the biggest ad-
vance in oncology in the future is with image-guided surgery, and
there is clearly industry interest in advancing the technology.
I think the interchange between laparoscopy, robotics and
image-guided technology is the future of surgery.
Cleveland Clinic is well-positioned to partner with industry to de-
velop these new technologies. We are currently working with a com-
pany to examine new, nonthermal ablation techniques that might be
applicable in breast cancer, giving patients a better cosmetic result.
In general surgery, there is ongoing development in the con-
cept of mesh for abdominal wall reconstructions and hernias.
New biologic-type products that will promote natural healing
are in their infancy, but will likely develop so we won’t have
to use synthetic plastics and can have a true ingrowth of
normal tissue.
Theoretically, I think minimally invasive approaches to almost
everything will continue to develop, especially in the world of
robotics, including its miniaturization. I think NOTES will con-
tinue to develop, but for very specific indications.
The future also is more integrated medicine. I think our Insti-
tute model allows us to have patients with complex diseases
evaluated by various subspecialties, have treatments specifically
designed for them, and makes neoadjuvant therapies possible,
when needed.
Also on the horizon is a better evidence-based approach to
outcomes using the electronic medical record and standardized
treatment plans. How we can use the EMR can be expanded,
including allowing for be better overall communication between
referring doctors, and facilitate web-based interactions.
In education, Cleveland Clinic has a new simulation lab and
center, which utilizes both individual and group training. The
concept is to get away from learning directly on the patient and
learn more in a simulation model. The whole world of education
is also going to be more online, independent learning. ■
A:
Abdominal wall transplants will help meet an unmet need for patients
who have had complex prior abdominal surgery and have lost a significant
portion of their small intestine, or have had failed complex hernia repairs.

{10} digest this Winter | 2012
Cleveland Clinic
steven Wexner, MdChair, Colorectal Surgery | Cleveland Clinic Florida
In colorectal surgery, what is currently having the
most impact on patient care are the continued advances
in minimally invasive surgery, including improved
platforms for transanal endoscopic surgery and laparoscopic surgery.
The ongoing refinements in both optics and instrumentation will
allow acceleration in adoption and penetration of these techniques.
The minimally invasive approaches confer significant short- and
long-term benefits, which will be appreciated by an increased num-
ber of patients as further maturation of the technology occurs.
Another significant advance has been our new methods of treat-
ing fecal incontinence. One of the most distressing conditions is
loss of bowel control. Until recently, therapeutic options in the
United States were limited to sphincter repair, nonstimulated
muscle transfer and a stoma. Within the last few months, the
U.S. FDA approved both sacral neuromodulation and injectable
therapy to treat fecal incontinence. During the next five to 10
years, more surgeons will become adept in and offer these
options and therefore, more patients will derive benefit. ■
A:
What is currently having the most impact on patient care in colorectal
surgery are the continued advances in minimally invasive surgery,
including improved platforms for transanal endoscopic surgery and
laparoscopic surgery.
Roger Charles, MdChair, Gastroenterology and Hepatology | Cleveland Clinic Florida
Advances in wireless technology have had a signifi-
cant impact on the care we deliver to GI patients.
Currently, our options include the endocapsule,
SmartPill and Bravo capsule. However, there are many techno-
logical developments on the horizon that are likely to have
a significant impact on patient care in the future.
Externally rechargeable batteries will prolong battery life, al-
lowing us to get more data – particularly in patients with slow
GI transit. Capsule endoscopies of the future will be able to
analyze GI tract secretions, biopsy abnormal tissue and deliver
drug therapy. We will gain the ability to maneuver capsule
endoscopes to have control over the rate of progress through
the GI tract and also closely inspect suspected abnormalities.
In addition, implantable wireless biosensors for the detection of
GI bleeding have been tested, which potentially can alert physi-
cians in real time of recurrent GI bleeding. These biosensors send
alerts to the physician’s cell phone so they can respond promptly,
thus improving patient outcomes.
Finally, other advances that I see in the pipeline are new gastric
pacing devices for the management of gastroparesis and using
peroral endoscopic myotomy (POEM) in patients with achalasia,
a less invasive treatment option that avoids surgery. ■
A:

clevelandclinic.org/digestive 855.REFER.123 {11}
Digestive Disease institute
DDI Spotlight: Bariatric Surgery
Cleveland Clinic surgeons perform a high percentage of full revisional operations on
patients in whom older bariatric procedures were not successful in the long term. And
a large majority of the entire scope of bariatric surgeries surgeons in our Bariatric and
Metabolic and Digestive Disease institutes perform – whether primary, revisional or
complex and high-risk – are done laparoscopically or robotically.
Laparoscopic Roux-en-Y gastric bypass continues to be
the most commonly performed bariatric procedure at
Cleveland Clinic. However, both Cleveland Clinic’s main
campus and Cleveland Clinic Florida offer the entire
gamut of bariatric procedures, giving patients a variety
of options and the ability to undergo a procedure tailored
to their individual weight-loss goals and comorbidities.
INNOVATIVE PROCEDURES ON THE HORIZON
Physicians and scientists at Cleveland Clinic and Cleve-
land Clinic Florida are investigating new techniques in
bariatric surgery, including the intragastric balloon, vagal
blocking and interventional therapies through the mouth.
“Endoluminal procedures are the next generation in
bariatric operations,” says DDI general surgeon Matthew
Kroh. “I think a lot of revisional procedures may be done
this way in the future as the tools get better.”
Cleveland Clinic also is investigating laparoscopic
gastric plication, a restrictive procedure in which the
greater curve of the stomach is folded in on itself.
“The procedure is less invasive involving no stapling,
cutting or removing stomach tissue and it is com-
pletely reversible with weight loss similar to sleeve
gastrectomy. (55 percent excess body weight loss),
says Philip Schauer, MD, Chairman of the Bariatric
and Metabolic Institute at Cleveland Clinic Ohio. The
procedure is in clinical trials to more clearly determine
the short- and long-term benefits.
BEYOND JUST WEIGHT LOSS
“Bariatric surgery as a tool to fight obesity and weight-re-
lated medical problems is really underutilized,” Dr. Kroh
says. The metabolic aspect of the operations, including
the ability of a gastric bypass procedure to put diabetes
into remission in about 80 percent of patients, is being
explored further at Cleveland Clinic. The laparoscopic
operations being done more often now do not have
the same complication rates of the open procedures,
making it possible to consider bariatric procedures in
patients with lower BMIs (30 to 35 kg/m2) in order to
treat conditions such as diabetes, hypertension, obstruc-
tive sleep apnea and abnormal cholesterol levels.
A TEAM OF ExPERIENCED ExPERTS
The surgical experience of Cleveland Clinic’s bariatric
center teams as well as the multidisciplinary approach
in supporting the patient before, during and after
surgery is what assists patients in having successful
outcomes, says Raul Rosenthal, MD, Chairman of the
Bariatric and Metabolic Institute at Cleveland Clinic
Florida. He credits the successful outcomes of Cleve-
land Clinic patients to the nurses, dietitians, program
coordinators and other allied health professionals who
work with them and handle their long-term follow-up.
Also important, he says, “We as surgeons choose who is a
candidate and which operation is best for our patients. We
customize our treatment. There is no ‘one size fits all.” ■
CENTERS OF ExCELLENCE
Both the Cleveland Clinic Bariatric and Metabolic Institute and its counterpart at Cleveland Clinic Florida
have been designated Bariatric Surgery Centers of Excellence by the American Society for Metabolic and
Bariatric Surgery. Both have been accredited as Level 1 facilities by the Bariatric Surgery Center Network
Accreditation Program of the American College of Surgeons Centers of Excellence Program.
To learn more about our programs, visit clevelandclinicweightloss.com and clevelandclinic.org/florida.
Matthew d. Kroh, Md
98%More than 98 percent of the
bariatric procedures performed
at Cleveland Clinic’s main
campus and Cleveland Clinic
Florida are minimally invasive.
8,000+Number of bariatric proce-
dures performed at Cleveland
Clinic Florida and Cleveland
Clinic main campus in the
past 11 years.

{12} digest this Winter | 2012
Cleveland Clinic
retroperitoneal sarcomaChallenging cases require multidisciplinary treatment
Case stuDy
sricharan Chalikonda, Md
MARCH 2009
A 60-year-old man presented to the Digestive Disease
Institute’s Dr. Chalikonda with symptoms of abdominal
fullness and pain. He had a CT scan performed at an
outside hospital that showed a large mass sitting in his
retroperitoneum on the right side. The mass appeared to
be involving his right kidney as well as his colon and liver
and was adjacent to his inferior vena cava. (Figure 1)
The size of the mass and location was consistent with
a soft tissue tumor known as a retroperitoneal sarcoma.
Given the size of the mass and high chance of local
recurrence if it was not completely resected, the deci-
sion was made to proceed with surgical resection and
perioperative radiation therapy.
He was then evaluated by our radiation oncologist and
it was determined that he would be a candidate for peri-
operative radiation, utilizing special catheters designed
to deliver radiation after the surgeon has packed the
bowel away from the field.
APRIL 2009
The patient underwent exploratory laparotomy and
resection of the tumor, which required a right hemi-
colectomy and right nephrectomy. He had his bowels
packed away and the catheters placed in the resection
bed. (Figure 2). He underwent radiation therapy over
the next 36 hours and was brought back to the operat-
ing room for removal of the catheters.
OCTOBER 2011
The patient’s most recent CT scan does not show any
evidence of recurrent disease and he is doing very well.
He is his back to a normal quality-of-life. (Figure 3)
DISCUSSION
Soft tissue sarcomas are very challenging to treat and
usually require multidisciplinary treatment. This case is
an excellent example of the collaboration between surgi-
cal oncology radiation therapy, and medical oncology in
our Surgical Oncology Clinic. Here at Cleveland Clinic,
we have performed nearly 30 similar procedures with
perioperative radiation over the past two years.
This type of treatment allows the radiation therapist
to administer higher doses of radiation than might
be possible with conventional external beam therapy.
In addition, the entire radiation therapy is completed
during one hospitalization without the need for subse-
quent visits.
Dr. Chalikonda is Director of Robotic Surgery in the
DDI’s Department of General Surgery. He special-
izes in surgical oncology and hepato-pancreato-biliary
surgery. He can be contacted at [email protected] or
216.445.0056. ■
Figure 1: Preop CT scan Figure 2: CT scan of catheters in resection bed Figure 3: CT scan postop

DIGESTIVE DISEASE INSTITUTE CHAIR John Fung, MD, PhD
MANAGING EDITOR Ann Bakuniene-Milanowski
ART DIRECTOR Mike Viars
SENIOR MARKETING MANAGER Matthew Chaney
MARKETING MANAGER Priya Barra
CONTRIBUTING PHOTOGRAPHERS Russell Lee
Cleveland Clinic Center for Medical Art and Photography
At the Digestive Disease Institute, one of 26 institutes at Cleveland Clinic, our colorectal surgeons and gastrointestinal specialists serve more than 66,000 patients annually. At Cleveland Clinic Florida, our gastroenterologists provide care in more than 6,200 patient visits each year. Innovative procedures and decades of experience enable our physicians to achieve success in preventing and treating the full specturm of digestive diseases. Cleveland Clinic is a nonprofit, multispecialty academic medical center consistenly ranked among the top hospitals in America by U.S.News & World Report. Founded in 1921, it is dedicated to providing qualityspecialized care and includes an outpatient clinic, a hospital with more than 1,300 staffed beds, and education institute and a research institute.
Dr. Fanning Receives Healthnetwork Foundation Service Award Alicia Fanning, MD, was awarded a Healthnetwork Foundation Service
Award for 2011. Dr. Fanning, a breast surgeon in our Department of
General Surgery, was one of 10 recipients of this annual award given
to physicians who have demonstrated an extremely high level of integ-
rity and compassionate care to Healthnetwork members. Healthnet-
work helps to fund the ground-breaking research being conducted by
these innovative national leaders in medicine. Dr. Fanning’s specialty
interests include breast cancer and breast disease, breast diagnostics,
breast diseases, breast surgical oncology, oncoplastic surgery.
Standardizing, Metric-based Protocols for rectal CancerDDI recently organized a Consortium on Rectal Cancer, which
featured surgeons and pathologists from 16 major national centers
that perform a high volume of rectal cancer surgery.
Using experience and data from their respective medical centers,
members of the consortium hope to develop a standardized, metric-
based protocol for the way rectal cancer is managed in North America
based on the current best-available evidence. They also hope to define
specific outcome measures that accurately reflect quality care for the
50,000 patients diagnosed annually with rectal cancer in the U.S.
The August 2011 event was led by colorectal surgeons from Cleve-
land Clinic and Cleveland Clinic Florida: Feza H. Remzi, MD, Steven
Wexner, MD, James Merlino, MD, and David Dietz, MD.
Dr. Vargo to Lead Gastroenterology & HepatologyFollowing a national search, John Vargo, MD, MPH, has been named
Chair of the Department of Gastroenterology and Hepatology of the
Digestive Disease Institute of Cleveland Clinic.
Dr. Vargo is Associate Professor of Medicine at the Cleveland Clinic
Lerner College of Medicine of Case Western Reserve University. He also
serves as Vice-Chair of the Digestive Disease Institute.
Dr. Vargo earned his medical degree from the University of Rochester
School of Medicine and Dentistry, completed his residency at Montefio-
re Hospital University Health Center, Pittsburgh, and his Gastroenterol-
ogy fellowship at Cleveland Clinic. Dr. Vargo was also Cleveland Clinic’s
first hepatology fellow. He holds a master of public health from Case
Western Reserve University, Cleveland, and is an honorary fellow of the
Gastroenterology Society of Ecuador. He is a councilor of the American
Society of Gastrointestinal Endoscopy and is recognized for his research
in procedural sedation, deep enteroscopy and endoscopic training.
He has earned several awards, including the American Society for
Gastrointestinal Endoscopy Career Development Award and numerous
Cleveland Clinic Innovator Awards. Dr. Vargo is currently an associate
editor for the journal Gastrointestinal Endoscopy.
A member of the Department of Gastroenterology since 1994, Dr.
Vargo’s research interests include sedation, physiologic monitoring,
outcomes and training. His endoscopic practice includes ERCP, EUS,
advanced imaging techniques, stenting, endoscopic mucosal resection
and deep enteroscopy. He holds two patents in endoscopy and
is widely published.
inBrief}
Digestive Disease InstituteThe Cleveland Clinic Foundation9500 Euclid Avenue/AC311Cleveland, OH 44195
Medical Concierge Complimentary assistance for out-of-state patients
and families 800.223.2273, ext. 55580, or email
Global Patient ServicesComplimentary assistance for national and international
patients and families 001.216.444.8184 or visit
clevelandclinic.org/gps
DDi referrals clevelandclinic.org/digestive
Colorectal Surgery | Gastroenterology & Hepatology
General Surgery | Human Nutrition
Ohio: 855.REFER.123
Florida: 954.659.5278
Clinical trialsVisit clevelandclinic.org/ddiresearch
for a complete listing of all active clinical trials.
Critical Care Transport WorldwideCleveland Clinic’s critical care transport teams and fleet of mobile ICU vehicles, helicopters and fixed-wing aircraft serves critically ill and highly complex patients across the globe. Call 216.448.7000 or 866.547.1467 or visit clevelandclinic.org/criticalcaretransport.
Track Your Patient’s Care OnlineDrConnect is a secure online service providing our physician colleagues with real-time information about the treatment their patients receive at Cleveland Clinic. To receive your next patient report electronically, establish a DrConnect account at clevelandclinic.org/drconnect.
Digestive Disease institute access guide
Same-day Visits AvailableSame-day appointments often are available for urgent cases. All same-day visits will be coordinated through the DDI patient navigator, a registered nurse who will triage all requests for same-day visits to ensure patients receive immediate attention. To arrange a same-day visit, call 216.444.7000.
SERVICES FOR PHYSICIANS
SERVICES FOR PATIENTS
90 Years Logo4 color process
Blue: 100/34/0/2Green: 100/0/85/24