difficult airway. definition the clinical situation in which a conventionally trained...
TRANSCRIPT

Difficult Airway

Definition
• The clinical situation in which a conventionally trained anesthesiologist experiences difficulty with mask ventilation, difficulty with tracheal intubation, or both.
• represents a complex interaction between patient factors, the clinical setting, and the skills of the practitioner
American Society of Anesthesiologists Task Force on Management of the Difficult Airway, 2013

• Cause serious soft tissue damage
• Hypoxaemic anaesthetic death and brain damage

Airway assessment
• Aim is to anticipate
– Difficult ventilation
– Difficult intubation
– Difficulty with patient cooperation or consent
– Difficult tracheostomy

History
• Previous history of difficult airway• Airway-related symptoms/disease
• Difficult airway bracelet/card
• Previous surgery/radiotherapy to head & neck
• Trauma to head & neck
• Head & neck infection
• Obstructive lesions/foreign body in airway

Systemic conditions
• Connective tissue diseases– RA– Scleroderma
• Endocrine– Acromegaly
• OSA• Pregnancy• Congenital syndromes

Physical Examination
• L – Look externally
• E – Evaluate 3-3-2 rules
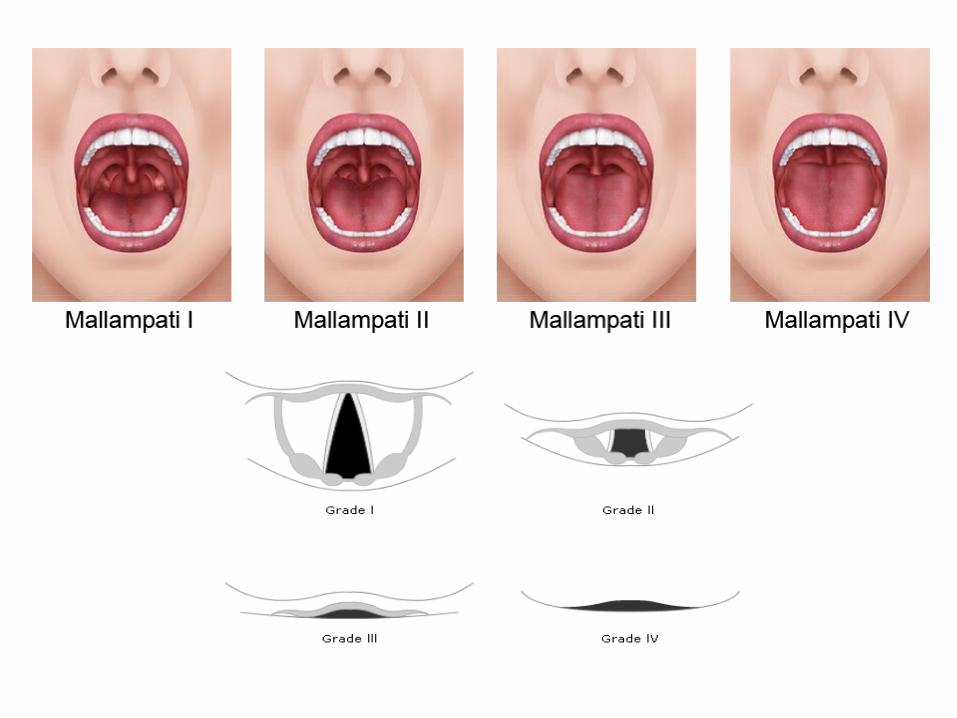
• M – Mallampati score
• O – Obstruction
• N – Neck mobility
Special Investigation
• Chest X-ray
• CT, MRI (neck, chest)

Physical Examination
• Atypical facial features or shape
• Edentulous mouth
• Morbid obesity
• Facial hair
• Protruding or “buck” teeth
• Protruding tongue
• Facial or neck trauma

Physical Examination
• Three finger mouth opening
• Three finger mentum to hyoid
• Two finger floor of mouth to thyroid cartilage

Difficult Airway Society guidelines
• Plan A: Initial tracheal intubation plan.• Plan B: Secondary tracheal intubation plan, when
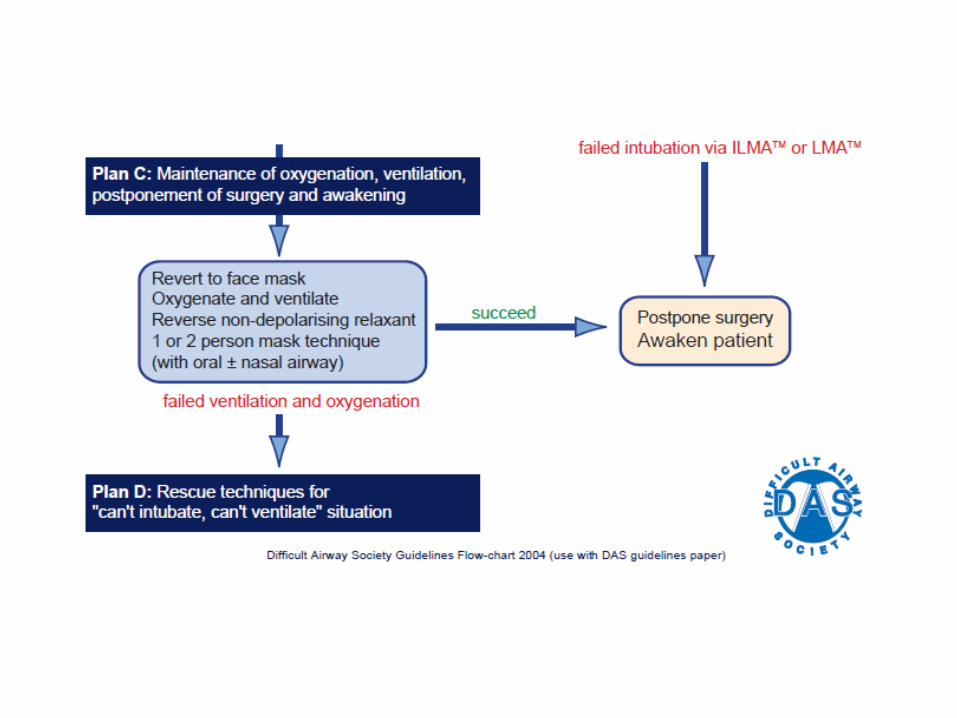
Plan A has failed.• Plan C: Maintenance of oxygenation and ventilation,
postponement of surgery, and awakening the patient, when earlier plans fail.
• Plan D: Rescue techniques for ‘can’t intubate, can’t ventilate’ (CICV) situation

• Clinical scenario of difficult intubation in an adult patient after induction of general anaesthesia and muscle paralysis, usually with a non-depolarising neuromuscular blocking drug
• Performed in optimal conditions after ensuring adequate muscle relaxation and appropriate position of the head and neck
• Use of optimum external laryngeal manipulation or Sellick maneuver
• If, despite these measures, there is still a grade 3 or 4 view, then alternative techniques will be needed. – introducer (‘gum elastic bougie’) and ⁄ or– different laryngoscope i.e McCoy and straight laryngoscope
• Oxygenation is maintained with mask ventilation between intubation attempts.
Basic preparation for difficult airway
• Inform patient
• Skilled assistance
• Suction
• Preplanned strategy/algorithm

Basic preparation for difficult airway
• Pre O2
• Supplemental O2 during the difficult airway
management

Case scenario
• Mr M, 41, comorbid HPT not on follow up. Alleged MVA at 6 am. Sustained severe crush injury of right lower limb. No other external/internal injury.
• On cervical collar.• Planned for AKA under GA• Last meal at 5 am• BP: 132/86 HR: 116• Hb: 10.6 K:3.2
Case scenario
• Preoxygenation with 100% O2• Cricoid pressure• Induction
– IV Fentanyl 100 mcg– IV Propofol 120 mg– IV Rocuronium 50 mg
• Manual in-line stabilization• 1st laryngoscopy CLIII with cricoid pressure
esophageal intubation• Mask ventilation• 2nd laryngoscopy doubtful ETT placement• 3rd laryngoscopy tracheal intubation



Greater risk of regurgitation or vomitingShort duration of succinylcholine increases the risk of laryngospasm and difficulty with laryngoscopy during recovery ofneuromuscular function



Difficult intubation cart