differences in practice and personal profiles between male and female ophthalmologists
TRANSCRIPT
Original Article
Differences in practice and personal profiles between maleand female ophthalmologistsHelen V Danesh-Meyer FRANZCO,1 Narme C Deva MBChB,1 Judy YF Ku MBChB,1 Stuart C Carroll MBChB,1
Yu Wee Tan BHB1 and Greg Gamble MSc2
Departments of 1Ophthalmology and 2Medicine, University of Auckland, Auckland, New Zealand
ABSTRACT
Purpose: To assess practice profiles and attitudes towardscareer and family among ophthalmologists in Australia andNew Zealand, with an emphasis on identifying genderdifferences.
Methods: A 43-part confidential survey addressing profes-sional and personal issues was sent to all female ophthal-mologists and to randomly selected age-matched maleophthalmologists, registered with the Royal Australian andNew Zealand College of Ophthalmologists in 2005.
Results: A total of 254 (75%) of the surveys were returned,with no significant difference in response rate betweengenders. Differences in practice profiles were identified:females preferentially practise in the city (89.6% vs. 76.1%,P < 0.001), work fewer hours (70% of males working 40hours per week, compared with 41% of females, P < 0.0001)and work part time (57.5% vs. 13.6%, P < 0.0001). Femaleophthalmologists earn less (average income beingNZ/Aus$37 913 [95% confidence interval 25 600–50 226]less, P < 0.0001); the difference remained significant (P < 0.0001) even when adjusted for hours worked. Up to 93.3%of male ophthalmologists are married or in a stable rela-tionship, compared with 75.6% of females (P = 0.0003), andmales are more likely to have children (P = 0.0007). Therewas no significant difference in overall career satisfactionbetween male and female ophthalmologists; however,females expressed greater frustration with managing pro-fessional and family commitments, and unequal careeradvancement opportunities.
Conclusion: Significant differences exist in practice profilesand personal circumstances between male and female oph-thalmologists. Females appear to balance work and personalresponsibilities by working fewer hours, and for lowerincome. Despite this, they are less likely to be in a stablerelationship, or to have children. However, there is no differ-ence between the two groups in overall career satisfaction.
Key words: career satisfaction, gender difference, ophthal-mologist, women, workforce.
INTRODUCTION
There is a trend towards an increasing number of femalesentering both medicine and specialist training programmesworldwide.1 In Australia in 2004, 50.2% of new entrants toall vocational training programmes were female2 as are 35%of vocational trainees registered with the Royal Australianand New Zealand College of Ophthalmologists (RANZCO)in 2005.
The aim of this study was to identify differences in thepersonal circumstances, practice profiles and attitudestowards career and family among female and male ophthal-mologists in Australia and New Zealand. By doing so, wehope to identify mechanisms used by ophthalmologists tobalance their personal and professional lives. An understand-ing of these mechanisms is important for future planning ofthe ophthalmology workforce and to better inform potentialentrants into ophthalmology training programmes.
METHODS
The study involved data collection through a specificallydesigned, confidential, self-administered, 43-part question-
� Correspondence: Dr Helen V Danesh-Meyer, Department of Ophthalmology, University of Auckland, Auckland, New Zealand. Email:
The preliminary results of this study were presented at the Royal Australian and New Zealand College of Ophthalmologists (RANZCO), New Zealand Branch
meeting, Auckland, May 2006 and at the annual RANZCO Scientific Congress, Sydney, Australia, November 2006.
Received 11 August 2006; accepted 1 February 2007.
Clinical and Experimental Ophthalmology 2007; 35: 318–323doi: 10.1111/j.1442-9071.2007.01480.x
© 2007 The AuthorsJournal compilation © 2007 Royal Australian and New Zealand College of Ophthalmologists

naire designed to address areas of potential gender differencein ophthalmology. The questionnaire was divided into foursections that elicited information about: (i) demographiccharacteristics; (ii) work and practice profile; (iii) personalcircumstances; and (iv) work/family balance and careersatisfaction.
In July 2005, the questionnaire was sent to all femaleophthalmologists registered with the RANZCO and twice asmany randomly selected, but age- and geographicallymatched, male ophthalmologists also registered withRANZCO. Random selection of control subjects was carriedout by the RANZCO. A database of all members belongingto the College was entered onto an Excel spreadsheet andsorted according to their geographical location. Males andfemales were then separated within each geographical groupand ranked into age groups. From these age-ranked groupsall female subjects and twice as many randomly chosen malesubjects from matching State/New Zealand age groups fromthe male population were sent a questionnaire. This resultedin a population of 108 females and 229 males.
Questions were constructed in a number of styles to elicitthe most appropriate and accurate responses. Majority ofanswers were of forced choice format; for example, respon-dents were asked to estimate their net income (afterexpenses, before tax) from the practice of ophthalmology bychecking a box next to four income ranges. Where appro-priate, respondents were also given the choice of ‘other’ aswell as space to explain reasons for their answer. Overallcareer satisfaction was assessed using adjectival-anchoredfive-point linear scale, with 1 being very happy and 5 beingvery unhappy. The respondents� opinion to statementsregarding aspects of work/family balance was explored in thesame manner with 1 being strongly agree, 5 being stronglydisagree and the midpoint being uncertain. Where appropri-ate a ‘non-applicable’ option was also available.
The questionnaire responses were anonymous. TheRANZCO office kept a list of names/tracking numbers toidentify non-responders, and remained blinded to the indi-vidual replies. The responses were in unmarked envelopesand returned to the University of Auckland unopened.
Statistics
It was anticipated that at least 75 (of 108) females wouldchoose to respond to the survey and, with 2 to 1 stratifiedsampling of age-matched males, the survey would achieve80% power to detect a difference in the proportion of malesand females choosing a given response of at least 15%. Con-fidence intervals (CI) for proportions could be reported to atleast �10%.
Dichotomous and nominal data were analysed by c2
analysis or Fisher�s exact test (for a 2 ¥ 2 table). Continuousdata were analysed by parametric (ANOVA/Student�s t-test)and non-parametric (Kruskall–Wallis/Wilcocon) tests, asappropriate. Analyses were performed using SAS v 9.1 (SASInstitute Inc, Cary, NC, USA), all tests were two-tailed andP < 0.05 was considered significant.
RESULTS
Response rate and demographic characteristics
A total of 254 responses were received, 88 from femaleophthalmologists and 166 from male ophthalmologists,giving a response rate of 81.5% for females and 72.5% formales (P = 0.079). The average age of female respondentswas 45.3 � 9.9 years and male respondents� average age was46.8 � 10.1 years (P = 0.26). The average number of yearssince completion of training was 14.2 year for males and13.8 years for females (P = 0.78). There was no significantdifference in ethnic groups between genders with predomi-nant group (76.9%) being European, followed by Asian (15.5%), Indian (5.6%) and other (2%) (P = 0.85).
Work and practice profile
Subspecialty, location and hours worked per week
The majority of the respondents (52.0%) identified them-selves as general ophthalmologist with the remainder assubspecialists. Although there was no significant differencebetween genders in subspecialization rates (P = 0.65), differ-ences were identified in relation to the type of subspecialty(Table 1), with significantly fewer females in surgical retina(2.3% vs. 20.5%, P = 0.0052) and cornea/anterior segmentsubspecialties (4.5% vs. 20.5%, P = 0.017).
Respondents reported the location of their practice (a citybeing defined as a population of greater than 100 000 and asmaller city or town as a population of less than 100 000):89.7% of females worked in a city compared with 76.1% ofmales (P < 0.01). Division of professional activity, reportedby allocation of number of half days per week spent indifferent employment settings, showed a similar number ofmales (67%) and females (61%) worked less than two ses-sions a week in a public hospital (P = 0.48). There was nodifference between genders in the number who worked in asolo private practice setting as opposed to a group privatepractice (P = 0.63).
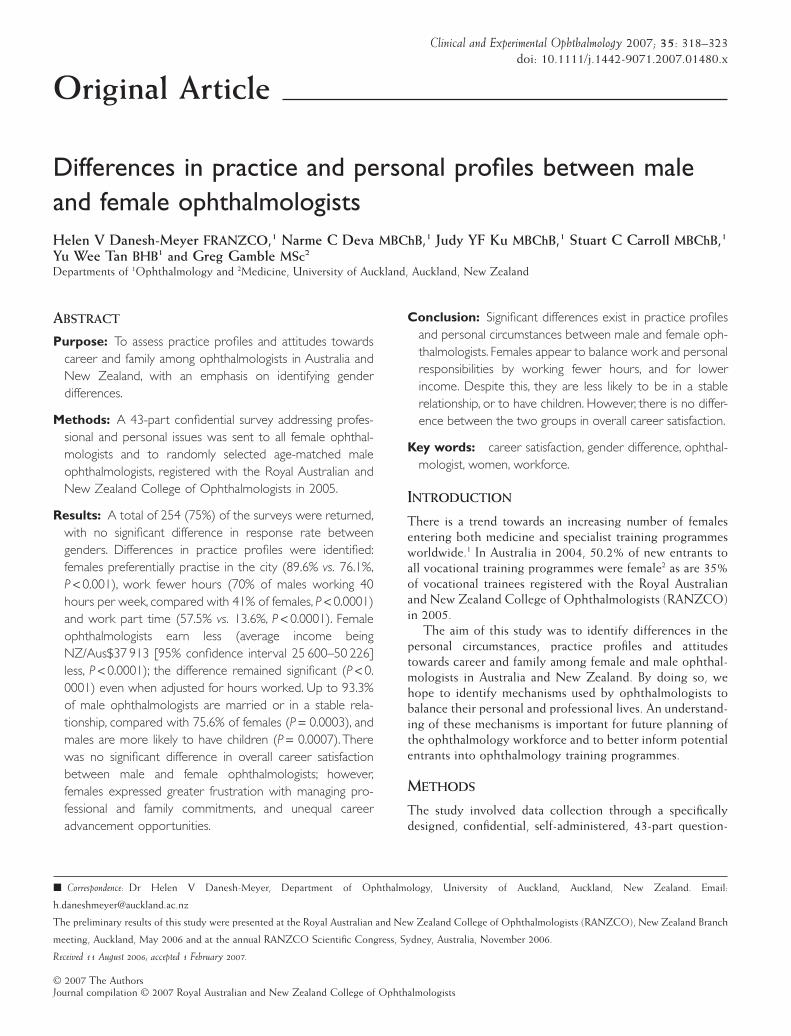
The largest proportion of males (43.3%) worked 40–49hours (h) per week, whereas the largest proportion of females
Table 1. Subspecialty choice between male and femaleophthalmologists
Specialty Male(n = 78)
n (%)
Female(n = 44)
n (%)
P-value
Surgical retina 20.5 (16) 2.3 (1) 0.0052Refractive 18.0 (14) 6.8 (3) 0.1100Cornea/anterior segment 20.5 (16) 4.5 (2) 0.0170Cataract 14.1 (11) 6.8 (3) 0.2500Medical retina 12.8 (10) 27.3 (12) 0.0540Glaucoma 12.8 (10) 20.5 (9) 0.4400Paediatrics 11.5 (9) 9.1 (4) 0.7700Oculoplastics 9.0 (7) 11.4 (5) 0.7600Other 12.8 (10) 20.5 (9) 0.3000
Ophthalmology workforce survey 319
© 2007 The AuthorsJournal compilation © 2007 Royal Australian and New Zealand College of Ophthalmologists
(28.4%) worked 30–39 h per week. Seventy per cent ofmales worked 40 h or more per week, compared with 41% offemales (P < 0.0001) (Fig. 1).
Income
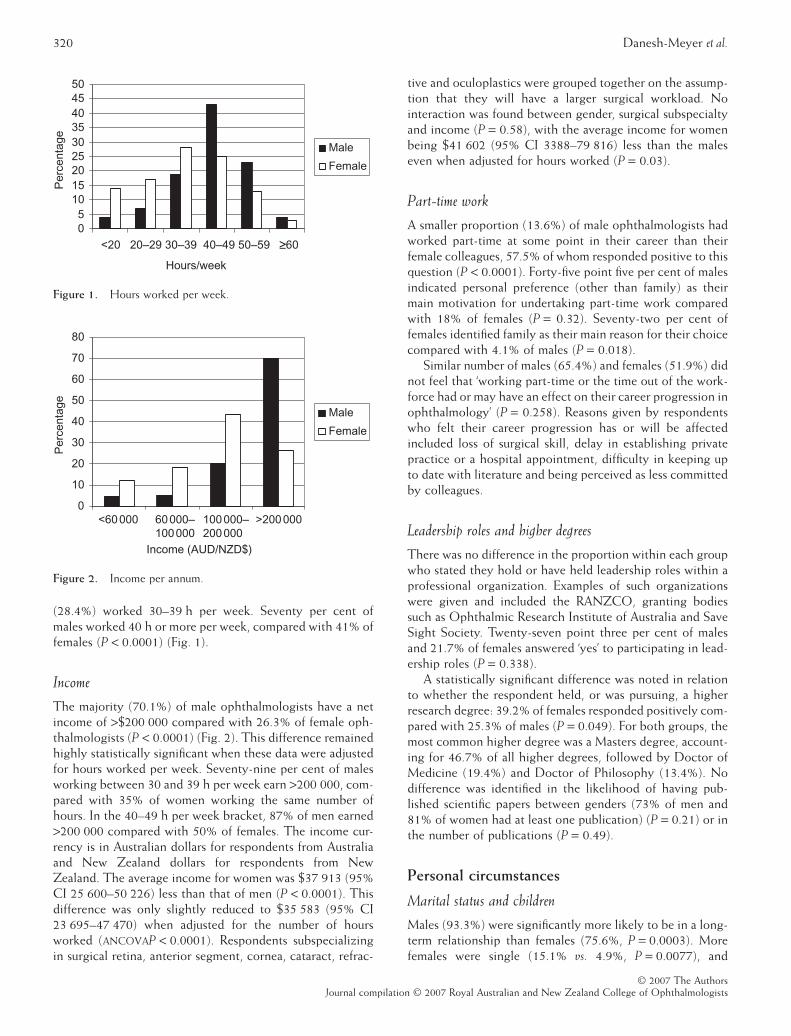
The majority (70.1%) of male ophthalmologists have a netincome of >$200 000 compared with 26.3% of female oph-thalmologists (P < 0.0001) (Fig. 2). This difference remainedhighly statistically significant when these data were adjustedfor hours worked per week. Seventy-nine per cent of malesworking between 30 and 39 h per week earn >200 000, com-pared with 35% of women working the same number ofhours. In the 40–49 h per week bracket, 87% of men earned>200 000 compared with 50% of females. The income cur-rency is in Australian dollars for respondents from Australiaand New Zealand dollars for respondents from NewZealand. The average income for women was $37 913 (95%CI 25 600–50 226) less than that of men (P < 0.0001). Thisdifference was only slightly reduced to $35 583 (95% CI23 695–47 470) when adjusted for the number of hoursworked (ANCOVAP < 0.0001). Respondents subspecializingin surgical retina, anterior segment, cornea, cataract, refrac-
tive and oculoplastics were grouped together on the assump-tion that they will have a larger surgical workload. Nointeraction was found between gender, surgical subspecialtyand income (P = 0.58), with the average income for womenbeing $41 602 (95% CI 3388–79 816) less than the maleseven when adjusted for hours worked (P = 0.03).
Part-time work
A smaller proportion (13.6%) of male ophthalmologists hadworked part-time at some point in their career than theirfemale colleagues, 57.5% of whom responded positive to thisquestion (P < 0.0001). Forty-five point five per cent of malesindicated personal preference (other than family) as theirmain motivation for undertaking part-time work comparedwith 18% of females (P = 0.32). Seventy-two per cent offemales identified family as their main reason for their choicecompared with 4.1% of males (P = 0.018).
Similar number of males (65.4%) and females (51.9%) didnot feel that ‘working part-time or the time out of the work-force had or may have an effect on their career progression inophthalmology’ (P = 0.258). Reasons given by respondentswho felt their career progression has or will be affectedincluded loss of surgical skill, delay in establishing privatepractice or a hospital appointment, difficulty in keeping upto date with literature and being perceived as less committedby colleagues.
Leadership roles and higher degrees
There was no difference in the proportion within each groupwho stated they hold or have held leadership roles within aprofessional organization. Examples of such organizationswere given and included the RANZCO, granting bodiessuch as Ophthalmic Research Institute of Australia and SaveSight Society. Twenty-seven point three per cent of malesand 21.7% of females answered ‘yes’ to participating in lead-ership roles (P = 0.338).
A statistically significant difference was noted in relationto whether the respondent held, or was pursuing, a higherresearch degree: 39.2% of females responded positively com-pared with 25.3% of males (P = 0.049). For both groups, themost common higher degree was a Masters degree, account-ing for 46.7% of all higher degrees, followed by Doctor ofMedicine (19.4%) and Doctor of Philosophy (13.4%). Nodifference was identified in the likelihood of having pub-lished scientific papers between genders (73% of men and81% of women had at least one publication) (P = 0.21) or inthe number of publications (P = 0.49).
Personal circumstances
Marital status and children
Males (93.3%) were significantly more likely to be in a long-term relationship than females (75.6%, P = 0.0003). Morefemales were single (15.1% vs. 4.9%, P = 0.0077), and
05
101520253035404550
<20 20–29 30–39 40–49 50–59 ≥60
Hours/week
Per
cent
age
Male
Female
Figure 1. Hours worked per week.
0
10
20
30
40
50
60
70
80
<60 000
Income (AUD/NZD$)
Per
cent
age
Male
Female
60 000–100 000
100 000–200 000
>200 000
Figure 2. Income per annum.
320 Danesh-Meyer et al.
© 2007 The AuthorsJournal compilation © 2007 Royal Australian and New Zealand College of Ophthalmologists
divorced (9.3% females vs. 1.8% males, P = 0.0092). Maleophthalmologists were also more likely to have children(88.3% males vs. 71.3% females, P = 0.0007). There was asignificant (P < 0.0001 Wilcoxon rank test) difference in themedian number of children between females (1.5, range 0–4)and males (2, range 0–4).
Significant differences also existed in the timing of thefirst child (Table 2). Significantly more females (55%) choseto have their first child after training, compared with theirmale colleagues (24.3%) (P < 0.05). Sixty per cent of maleophthalmologists had their first child either before orduring their ophthalmology training, compared with 30%of females (P < 0.0001). Differences in contribution tochild-care activities for children under the age of 5(assessed by asking those respondents with children toindicate the percentage contribution by themselves,partner, extended family and friends, Crèche, Nannies andothers) were identified (Table 3). Male ophthalmologistslargely depended on their partners for care of childrenunder the age of 5, contributing a median of 10% of thetotal care. In contrast, female ophthalmologists contributeda median of 45%, using Nannies and Crèche facilities assecondary sources of child care.
Paid hour worked by partners
There were significant differences in the hours worked bypartners between genders as outlined in Table 4. Partners ofmale ophthalmologists were significantly more likely to workfewer hours (P < 0.0001). Fifty-five per cent of partners ofmale ophthalmologists work less than 20 h a week comparedwith only 12.7% of partners of female ophthalmologists(P < 0.0001), with the majority of the latter (69.8%) holdingfull-time employment of 40 h or more. There was no signifi-cant difference between genders in relation to having
enough time to spend with their partners (P = 0.83) withmajority (56.0%) feeling that they did.
Work/family balance and career satisfaction
There was no significant difference in overall career satisfac-tion between genders with females scoring a mean of 1.88(95% CI 1.7–2.05) and males a mean of 1.78 (95% CI 1.67–1.91) (P = 0.39). However, notable differences were foundbetween genders in certain aspects of work/family balance.More women than men feel frustrated by the lack of time theyhad to devote to career (mean score 3.8 vs. 3.5, P = 0.0337),feel that they often had to choose between career and family(mean score of 3.1 vs. 2.7, P = 0.00085), and that if givenanother chance, they would have children at a different pointin their career (mean score of 3.9 vs. 3.3, P = 0.0003). Moremales than females felt they derived ‘personal satisfaction’from their career (mean score of 1.8 vs. 1.6, P = 0.0116). Morefemales disagreed that a woman�s opportunity for advance-ment in ophthalmology is that same as a man (mean score of3.1 vs. 2.5, P = 0.0094), and that they are treated as an equal bycolleagues (mean score of 2.4 vs. 2.1, P = 0.0001).
DISCUSSION
Clear gender differences exist in both professional and per-sonal aspects of ophthalmologists in Australia and NewZealand and several factors have been highlighted in howfemales balance personal and career commitments.
Gender differences in part-time preferences, hoursworked and income were identified by this survey. This iscomparable to several similar studies in other specialtiesincluding gastrenterology,3 general practitioners,4 physi-cians5,6 and surgical specialties.7–9 All found that women have
Table 2. Timing of first child
Before ophthalmologytraining(n = 53)
During ophthalmologytraining(n = 56)
During fellowshiptraining(n = 22)
After fellowshiptraining(n = 67)
Female (%) 19 11 15 55Male (%) 30 30 10 25P-value 0.470 0.079 0.990 0.039
Table 3. Child-care contribution to children <5 years of age
Percentage of timecontributed by:
Malemedian(range)
Femalemedian(range)
P-value
Self 10 (0–90) 45 (5–90) <0.0001Partner 80 (5–100) 10 (0–100) <0.0001Family 5 (1–70) 12.5 (5–90) <0.0001Crèche 12.5 (2–70) 35 (2.5–100) 0.0600Nanny 10 (2–70) 35 (2.5–100) 0.0080
Table 4. Distribution of hours worked by partners of ophthal-mologists
Hours workedper week
Partners of maleophthalmologists
(%)
Partners of femaleophthalmologists
(%)
<20 55.41 12.7020–29 18.92 4.7630–39 13.51 12.7040–49 9.46 33.3350–59 2.03 19.05�60 0.68 17.46
Ophthalmology workforce survey 321
© 2007 The AuthorsJournal compilation © 2007 Royal Australian and New Zealand College of Ophthalmologists

a greater preference for part-time employment, work fewerhours and earn less even when adjusted for the hours workedper week. This study also found that more women preferredto work in larger cities or urban sites. Women were alsosignificantly less represented in more surgically orientatedsubspecialties such as surgical retina and cornea/anteriorsegment. One possible explanation for these findings is thatwomen�s choices reflect the greater need for convenienceand time that will allow them to balance other commitmentssuch as family. The preference for part-time and the mainreason stipulated by women for going part-time (family com-mitments) are consistent over specialties and nations.1
However, even adjusting for the hours worked, women con-tinue to earn less, a finding that is almost universal in otherstudies.1,3–5,7,9 When adjusted for subspecialties with aheavier surgical workload the differences were maintained.
A limitation of this study is that we specifically did not askabout operating theatre time and differences here may lendto explain some of the disparity found in income measures.The reasons behind income differences between gendershave not been established, but the disparity has been shownto decrease with years of practice.3,4
Our study did not show any difference in the number ofleadership roles held by women compared with men, nor didwe identify a difference in number of scientific publications.Interestingly, our study showed female ophthalmologistswere significantly more likely to hold a higher researchdegree. These findings are not in keeping with other studiesthat reported that a larger proportion of men compared withwomen were leaders.10 Others have published that althoughmore women entered academia following training, they wereless likely to obtain higher academic ranks and publish sci-entific articles.11,12 Reasons for this difference in findings arethat our definition of leadership, both within and outsideacademic medicine, was broader than the related articles andwe did not differentiate between higher- and lower-rankedleadership roles. In addition, although we have reported nodifference in the likelihood of having a scientific publicationbetween genders, we did not explore differences in high(>20) numbers of career publications, which is where otherstudies have noted gender differences. Furthermore, becausethe increasing number of females in ophthalmology is a morerecent trend, the study population is biased towards youngerophthalmologists where the differences in higher degreesand leadership positions may not be as apparent.
Male ophthalmologists are more likely to be married, andto have children than their female counterparts. This hasbeen noted in other countries and in other specialties.3,5,9
The marital status of female ophthalmologists is comparableto those reported for female physicians and surgeons;however, female ophthalmologists have also reported to bemore likely to have children than their female surgicalcollegues.13 Of those with children, female ophthalmologistsremain the primary caregiver for very young children withthe majority of their partners holding full-time employment,whereas male ophthalmologists depend predominantly ontheir partners for the care of very young children.
Overall, in concordance with other studies, there was nodifference in career satisfaction between genders,7,9 butnotable differences were identified in opinions related tobalancing career and family commitments with womenexpressing more frustration in ‘trying to do it all’. However, ithas been established that female ophthalmologists weremore likely to be satisfied in the balance between career andpersonal commitments than their female colleagues inobstetrics and general surgery.13
This study�s limitations are that it is a cross-sectionalstudy so trends over time are not accounted for. The oph-thalmologists surveyed were in general younger than thepopulation of ophthalmologists. So although the study is anindicator of continuous trends in the future, it may not accu-rately reflect practice profiles for the entire speciality. Inaddition, the data are self-reported and captures only facetsof clinical practice and personal characteristics.
There is no doubt that women have the unique task ofbalancing greater family commitments and career and theseresponsibilities may underlie their personal and/or careerchoices. Female ophthalmologists try to find the balancebetween personal and professional commitments by workingfewer hours and for less pay. The distinct gender differences inpractice profiles may have consequences for the future plan-ning of the ophthalmology workforce in Australia and NewZealand. These consequences could be that the gender dif-ferences will persist and as a result there may be fewer full-timeequivalent ophthalmologists and a greater number needed tomaintain adequate level of health care. Alternatively the dif-ferences will become less, either by the female practice profilebecoming more similar to male by devoting less time to familyobligations or by males becoming more involved in familyobligations. The purpose of this study was to identify genderdifferences so that reasons behind such difference could beelucidated and assist in workforce planning for the future andto target areas where improvement is needed.
ACKNOWLEDGEMENTS
This research was supported through the unrestrictedresearch grant by Alcon New Zealand (Auckland, NewZealand) for the Optic Nerve Research Fellowship. Theauthors would like to acknowledge the help given by theadministrative staff at the RANZCO, in particular Mr BarryDiletti and Mrs Margaret Dunn in defining and recruiting thestudy population. The authors would also like to acknowl-edge Professor CNJ McGhee (Department of Ophthalmol-ogy, University of Auckland) for his editorial review of themanuscript.
REFERENCES
1. McMurray JE, Cohen M, Angus G et al. Women in medicine: afour-nation comparison. J Am Med Womens Assoc 2002; 57: 185–90.
2. Australian MWAC. Career Decision Making by Post Graduate Doctors– Key Findings. December 2005. Report No. 2005.3.
322 Danesh-Meyer et al.
© 2007 The AuthorsJournal compilation © 2007 Royal Australian and New Zealand College of Ophthalmologists

3. Burke CA, Sastri SV, Jacobsen G, Arlow FL, Karlstadt RG,Raymond P. Gender disparity in the practice of gastroenterol-ogy: the first 5 years of a career. Am J Gastroenterol 2005; 100:259–64.
4. Wallace AE, Weeks WB. Differences in income between maleand female primary care physicians. J Am Med Womens Assoc2002; 57: 180–4.
5. Uhlenberg P, Cooney TM. Male and female physicians: familyand career comparisons. Soc Sci Med 1990; 30: 373–8.
6. Cull WL, Mulvey HJ, O�Connor KG, Sowell DR, BerkowitzCD, Britton CV. Pediatricians working part-time: past, present,and future. Pediatrics 2002; 109: 1015–20.
7. Yutzie JD, Shellito JL, Helmer SD, Chang FC. Gender differ-ences in general surgical careers: results of a post-residencysurvey. Am J Surg 2005; 190: 955–9.
8. Bogardus AJ, Neas BR, Sullivan SM. Practice differencesbetween male and female oral and maxillofacial surgeons.
survey results and analysis. J Oral Maxillofac Surg 1999; 57:1239–47;discussion 1248.
9. Jinapriya D, Cockerill R, Trope GE. Career satisfaction andsurgical practice patterns among female ophthalmologists. CanJ Ophthalmol 2003; 38: 373–8.
10. Kvaerner KJ, Aasland OG, Botten GS. Female medical leader-ship: cross sectional study. BMJ 1999; 318: 91–4.
11. Schroen AT, Brownstein MR, Sheldon GF. Women in academicgeneral surgery. Acad Med 2004; 79: 310–18.
12. Ash AS, Carr PL, Goldstein R, Friedman RH. Compensationand advancement of women in academic medicine: is thereequity? Ann Intern Med 2004; 141: 205–12.
13. Mackinnon SE, Mizgala CL, McNeill IY, Walters BC, Ferris LE.Women surgeons: career and lifestyle comparisons among sur-gical subspecialties. Plast Reconstr Surg 1995; 95: 321–9.
Ophthalmology workforce survey 323
© 2007 The AuthorsJournal compilation © 2007 Royal Australian and New Zealand College of Ophthalmologists