did you know #1 . . . did you know #2 · did you know #1 . . . about 85% of hearing health care...
TRANSCRIPT

2/4/2014
1
HEARING AID FEATURES
ACROSS MANUFACTURERS:
WHAT REALLY WORKS AND
CLINICAL IMPLICATIONS
Todd A. Ricketts, PhD
Associate Professor and Director of Graduate Studies
Department of Hearing and Speech Sciences
Director, Dan Maddox Memorial Hearing Aid Research Laboratory
Vanderbilt University Medical Center
Nashville, TN
Financial Disclosures
• Financial support for this presentation was provided by
the MSHA
• I have the following financially relevant relationships in the
service and/or product communicated, compared,
evaluated and/or reviewed in this presentation.
• Some of the data presented was supported by investigator initiated
research grants provided by the Dan Maddox Foundation, Phonak
AG, GN Resound, Siemens, Starkey, Oticon, Widex, Persona
Medical, Frye Electronics, the Department of Veterans Affairs, and
the US National Institute of Disabilities and Rehabilitative Research
(NIDRR - DOE)
Did You Know #1 . . .
About 85% of hearing health
care providers have a “favorite”
manufacturer (Johnson &
Ricketts, 2011)
Did You Know #2 . . .
Hearing health care providers
who have a favorite
manufacturer, fit that product to
about 80% of their patients.
Did You Know #3 . . .
Regardless of what company of
the “Big Six” they picked, they
all reported they picked the
company because it had the
best technology
THEY CAN’T
ALL BE RIGHT!
How to try to ensure satisfied patients?
• Examine the Patient’s communication and
listening needs and based on the evidence
select and adjust features and processing to
best address those needs.
• Counsel regarding use and benefit from
technologies to make sure the patients
expectations are met.
• Satisfaction = Expectations Met!
6

2/4/2014
2
Why is Evidence Based Research
Particularly Important in Modern
Hearing Aids?
• 16 Participants compared two devices that were acoustically
identical, except one was described as “ new ” and the other as “
conventional ” . Participants completed a speech-in-noise test,
sound quality ratings, and rated overall personal preference for
both hearing aids.
• Significantly better mean speech-in-noise performance (70.9%
versus 66.8%), and sound quality ratings for the “new” hearing
aid
• 75% expressed an overall preference for the “ new ” hearing aid
- double-blind methodology is optimal.
Piers Dawes , Rachel Hopkins & Kevin J. Munro. Placebo effects in hearing-aid trials are
reliable. International Journal of Audiology 2013; 52: 472–477
What we’re going to do . . .
•Review X different hearing aid features. •Selected based on features for which either the manufacturer or the specific patient, or the listening environment is likely to matter significantly based on the data (or all three).
•Limit our discussion of patient benefit primarily to adults.
•Review some of our recent research and pull in some studies from the recent literature.
•Provide a few clinical tips and techniques along the way.
•What is the true patient benefit in the real
world (our best guess if limited studies
available)?
•A = Real and valid benefit, F = No benefit expected
even theoretically.
•If benefit is present, would it apply to a wide
range of patients?
•A = Nearly all patients; F = you may stumble across a
couple of patients that benefit during your career.
•Would you expect the same benefit from the
products from different manufacturers?
Finally, we’ll grade each feature in 3
different areas…
Interpreting the grades for the third category
• Small or No Difference (SD): Few patients would notice
a difference for that feature among products from
different manufacturers.
• Medium Difference (MD): Many patients would notice a
difference for that feature among products from
different manufacturers.
• Large Difference (LD): Most patients would notice a
difference for that feature among products from
different manufacturers. Or differences are so large that
the feature is aimed at different populations based on
the specific design.
The X features we’ll discuss •Sophisticated Gain Processing
•Complex amplitude compression, sliding gain windows, etc.
•Directional Technology
•Advanced Microphone Array Technologies
•Adaptive Directional, Lobe Steering, Bilateral Beamforming
•Digital Noise Reduction
•Modulation based gain reduction, Fast filtering, adaptive Weiner filtering, etc.
•Digital Feedback Suppression
•Tinnitus Masking
•Bilateral Shared Information
•Remote microphone/FM
•Extended High Frequencies
•Frequency Lowering •Frequency compression, frequency transposition, frequency duplication and lowering
•Trainable Algorithms
•Learning VC, Acclimatization Managers
•Wireless Routing Applications (not sound sharing)
•Rechargeable, advanced remote controls and other cool features?
4
Take Home Points for The 8 Features That Didn’t Make
the Cut •Sophisticated Gain Processing
•Modern versions work pretty well and generally fairly equally when looking at group data. Individual differences are present and generally complicated.
•Some emerging data in the youngest kids
•Digital Noise Reduction
•Improved comfort and preference, still hoping for more
•Tinnitus Masking •We know a lot about it when not in hearing aids, new versions are too new to know if there are other advantages other than packaged in a hearing aid.
•Bilateral Shared Information •Emerging spatialization advantages.
•Remote microphone/FM •They work, lots of questions.
•Extended High Frequencies •Slight benefit and preference in listeners with flatter high frequency loss, hard to provide enough gain.
•Frequency Lowering •On average works in kids – no average benefit in adults
•Newest outcomes less than hoped!
•Trainable Algorithms/ Acclimatization Managers
•May lead to better satisfaction, but starting from a validated and verified prescriptive gain is still critical.
2/4/2014
3
Directional Technology:
How Does It Work?
• The signal from two omnidirectional microphones (or two ports leading to a single microphone diaphragm) is altered to cause attenuation of signals from certain azimuths
• Usually signals from sides or behind are attenuated
• Signal alterations can be made to provide attenuation (polar pattern nulls) for a variety of azimuths.
Directional Technology:
How Does It Work? •The majority of directional hearing aids today are both automatic
and adaptive:
• Automatic: Based on the analysis from the signal
classification system, the hearing aid will automatically
switch to directional or omnidirectional depending on the
listening environment.
• Adaptive: Based on the analysis from the signal
classification system, the polar plot will change in an effort
to maximize the speech signal and minimize the
background noise. This is only possible in twin microphone
directional systems
• The most complex systems do not use discreet
omnidirectional and directional states, but instead slide
from lower to higher directivity depending on assumed
acoustic environment.
Directional Technology:
Potential Benefit?
•Patient must position himself correctly and the directional microphone must be functioning correctly.
•Directional microphones should improve the signal-to-noise ratio by 2-3 dB (20-35%) for many difficult listening situations.
•The actual benefit will depend on distance from the talker, room reverberation, and other factors.
The potential for benefit applies to a wide range of patients:
• Adults with mild-severe hearing loss • (e.g. Pumford et al, 2000; Ricketts, 2000; Ricketts, Lindley & Henry,
2001; Ricketts & Henry, 2002; Ricketts & Hornsby, 2003; Valente et al, 2000)
• Adults with severe-profound hearing loss • (Ricketts & Hornsby, 2006; Ricketts, Henry & Hornsby, 2005)
• Children • (Hawkins & Yacullo, 1984; Ricketts, Galster & Tharpe, 2007; Ricketts
& Picou, 2013)
Directional Technology:
Patient Population?
Other factors that might limit
Directional benefits
• Interaction between visual cues and directional benefit
• Effects of hearing aid coupling type (open versus closed)
• Directional microphone stability over time (quality control)
What About Directional/Beamformer
Benefit with Vision?
• Wu & Bentler (2012)
• Aspell, Picou & Ricketts (2013)
2/4/2014
4
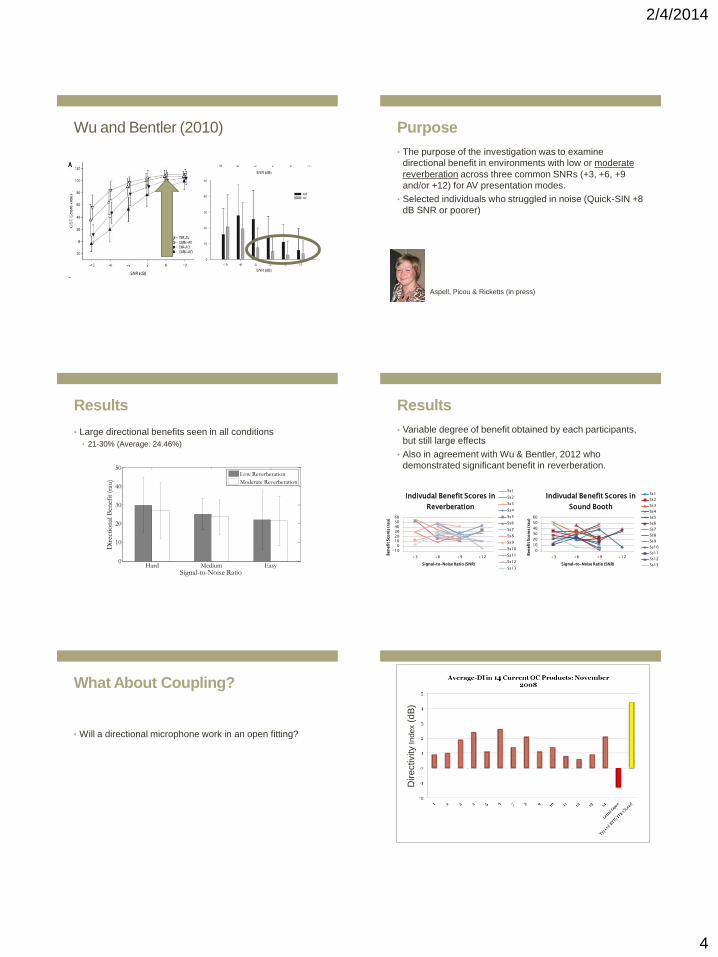
Wu and Bentler (2010) Purpose
• The purpose of the investigation was to examine
directional benefit in environments with low or moderate
reverberation across three common SNRs (+3, +6, +9
and/or +12) for AV presentation modes.
• Selected individuals who struggled in noise (Quick-SIN +8
dB SNR or poorer)
Aspell, Picou & Ricketts (in press)
Results
• Large directional benefits seen in all conditions
• 21-30% (Average: 24.46%)
Hard Medium Easy0
10
20
30
40
50
Signal-to-Noise Ratio
Dir
ecti
on
al B
enef
it (
rau)
Low Reverberation
Moderate Reverberation
Results
• Variable degree of benefit obtained by each participants,
but still large effects
• Also in agreement with Wu & Bentler, 2012 who
demonstrated significant benefit in reverberation.
0
10
20
30
40
50
60
+3 +6 +9 +12
Ben
efi
t Sco
res (ra
u)
Signal-to-Noise Ratio (SNR)
Indivudal Benefit Scores in
Sound Booth
Ss1
Ss2
Ss3
Ss4
Ss5
Ss6
Ss7
Ss8
Ss9
Ss10
Ss11
Ss12
Ss13
-10
0
10
20
30
40
50
60
+3 +6 +9 +12
Ben
efi
t Sco
res (ra
u)
Signal-to-Noise Ratio (SNR)
Indivudal Benefit Scores in
Reverberation
Ss1
Ss2
Ss3
Ss4
Ss5
Ss6
Ss7
Ss8
Ss9
Ss10
Ss11
Ss12
Ss13
What About Coupling?
• Will a directional microphone work in an open fitting?
24
Dir
ectivity I
ndex (
dB
)

2/4/2014
5
Findings from Valente and Mispagel
(2008) comparing OC omnidirectional to
OC directional
-2
-1
0
1
2
3
4
5
6
Listening Conditions
Me
an
RT
S (
dB
)
unaided
omnidirectional
directional
benefit
Unaided Omni Direct Benefit
SO IS THERE POORER PERFORMANCE
IN NOISE FOR DIRECTIONAL OC?
26
N = 280 Participants
(VA RR&D Study)
New Preliminary Data!
• The Effects of Hearing Aid Coupling and Signal
Source Location on Benefit From Different
Microphone Types
Harland, Picou, Hornsby, Tharpe,
& Ricketts (in preparation)
Purpose
• To evaluate the potential interaction between coupling
configuration (open versus closed), signal source location
(on-axis versus off-axis), and microphone type
(omnidirectional, directional, FM plus environmental
microphone) on the speech recognition in noise abilities of
pre-teens and teenagers with hearing loss (10 completed
to date).
Test Environment
• Average reverberation
time (60 dB decay)
within the moderate
range (500-800 ms)
5.1 meters
FM Transmitter
Signal
Source
180°
Signal
Source
0°
1 meter
1 meter
5.9
met
ers
Results – On Axis Listening
-10.0-9.0-8.0-7.0-6.0-5.0-4.0-3.0-2.0-1.00.01.02.03.04.0
OMNI 0° FIXED DIR 0° FM+OM 0°
BK
B-S
IN S
co
re (
dB
)
Microphone Mode
Average SNR-50 Scores Across Conditions
(Speech Front)
Open
Closed

2/4/2014
6
Clinical Implications
• The open fitting reduces speech recognition in noise
performance for all microphone types by about 1 dB (10
percentage points).
• For patients who struggle the most with speech
recognition in noise, fitting with closed coupling may be
preferred to optimize benefit.
Current Conclusions – Directional
Microphones when facing the talker
• In the hearing aids it works in - it works pretty well, even
with vision.
• Do the directional microphones used in hearing aids
general operate as expected, or are their quality control
and/or failure in the field issues we should be concerned
about?
Quality Control
• Maximum directivity (average DI or AI-DI) across instruments varies from about 1.5 dB to about 5.7 dB
• Dirt and damage will affect the average instrument over time affecting directivity and the benefit our patients
Clinical experience suggest nearly all manufacturers continue to have at least some issues with quality control.
• Perhaps as high as 5-10%!
• This happens both with new and repaired instruments.
Effect of Time –
Newer Data From a VA Study • Clinically assessed FBR on all instruments before
fittings and after every two month trial.
• For ITE instruments this was a single trial of
approximately two months.
• For BTE instruments, were refitted on more than one
patient for multiple (up to four) two month trials.
• Pilot work used to define average FBR for each type of
instrument.
• A frequency averaged FBR of 6 dB less than average was
considered a fail.
34
Directional Failure Rate for New
and Fitted Instruments
A need for verification?
36
The Bottom Line: Clinical assessment of directional
properties using a repeatable method is critical for
QUALITY CONTROL!
-15
-10
-5
0
5
10
15
20
010
2030
40
50
60
70
80
90
100
110
120
130
140
150160
170180
190200
210
220
230
240
250
260
270
280
290
300
310
320
330340
350
500
1000
2000
4000
2/4/2014
7
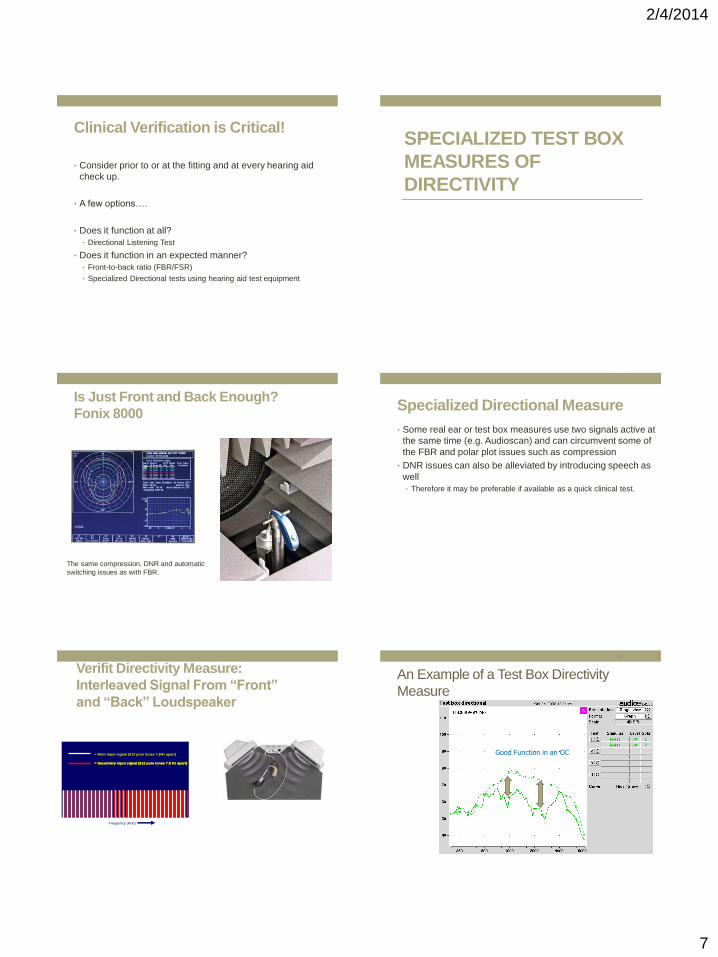
Clinical Verification is Critical!
• Consider prior to or at the fitting and at every hearing aid
check up.
• A few options….
• Does it function at all?
• Directional Listening Test
• Does it function in an expected manner?
• Front-to-back ratio (FBR/FSR)
• Specialized Directional tests using hearing aid test equipment
SPECIALIZED TEST BOX
MEASURES OF
DIRECTIVITY
Is Just Front and Back Enough?
Fonix 8000
Advanced features still must be disabled!
The same compression, DNR and automatic
switching issues as with FBR.
Specialized Directional Measure
• Some real ear or test box measures use two signals active at
the same time (e.g. Audioscan) and can circumvent some of
the FBR and polar plot issues such as compression
• DNR issues can also be alleviated by introducing speech as
well
• Therefore it may be preferable if available as a quick clinical test.
40
Verifit Directivity Measure:
Interleaved Signal From “Front”
and “Back” Loudspeaker
Frequency (KHz)
= Main input signal (512 pure tones 7.8Hz apart)
= Secondary input signal (512 pure tones 7.8 Hz apart)= Secondary input signal (512 pure tones 7.8 Hz apart)
An Example of a Test Box Directivity
Measure
42
Good Function in an OC Is Bigger Always Better? No!
2/4/2014
8
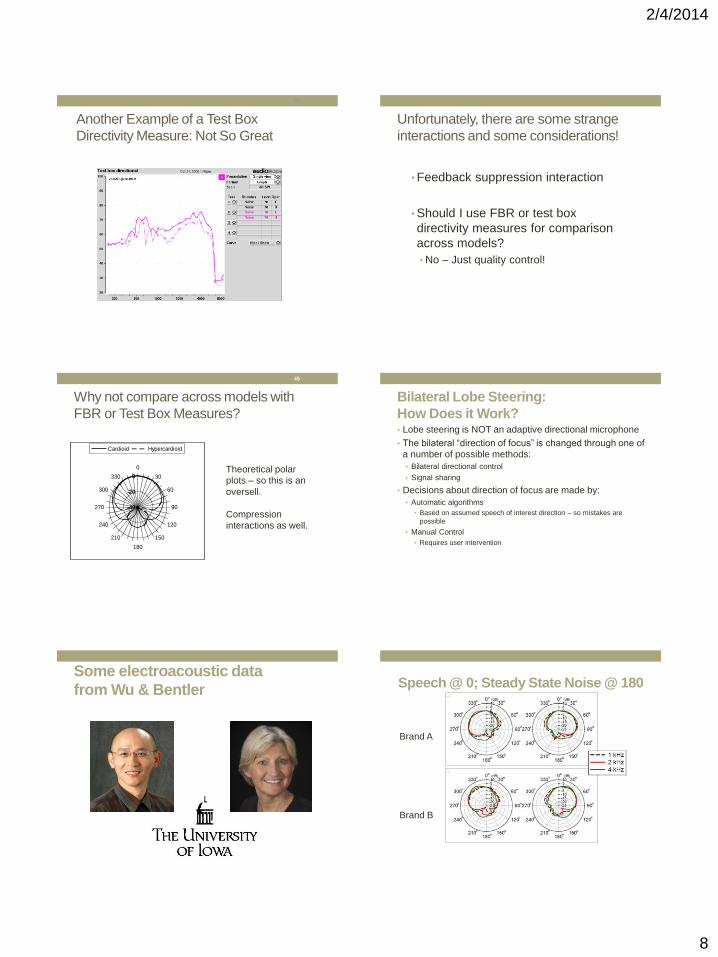
Another Example of a Test Box
Directivity Measure: Not So Great
43
Unfortunately, there are some strange
interactions and some considerations!
• Feedback suppression interaction
• Should I use FBR or test box
directivity measures for comparison
across models?
• No – Just quality control!
45
Why not compare across models with
FBR or Test Box Measures?
-40
-20
0
0
30
60
90
120
150
180
210
240
270
300
330
Cardioid Hypercardioid
Theoretical polar
plots – so this is an
oversell.
Compression
interactions as well.
Bilateral Lobe Steering:
How Does it Work? • Lobe steering is NOT an adaptive directional microphone
• The bilateral “direction of focus” is changed through one of
a number of possible methods:
• Bilateral directional control
• Signal sharing
• Decisions about direction of focus are made by:
• Automatic algorithms
• Based on assumed speech of interest direction – so mistakes are
possible
• Manual Control
• Requires user intervention
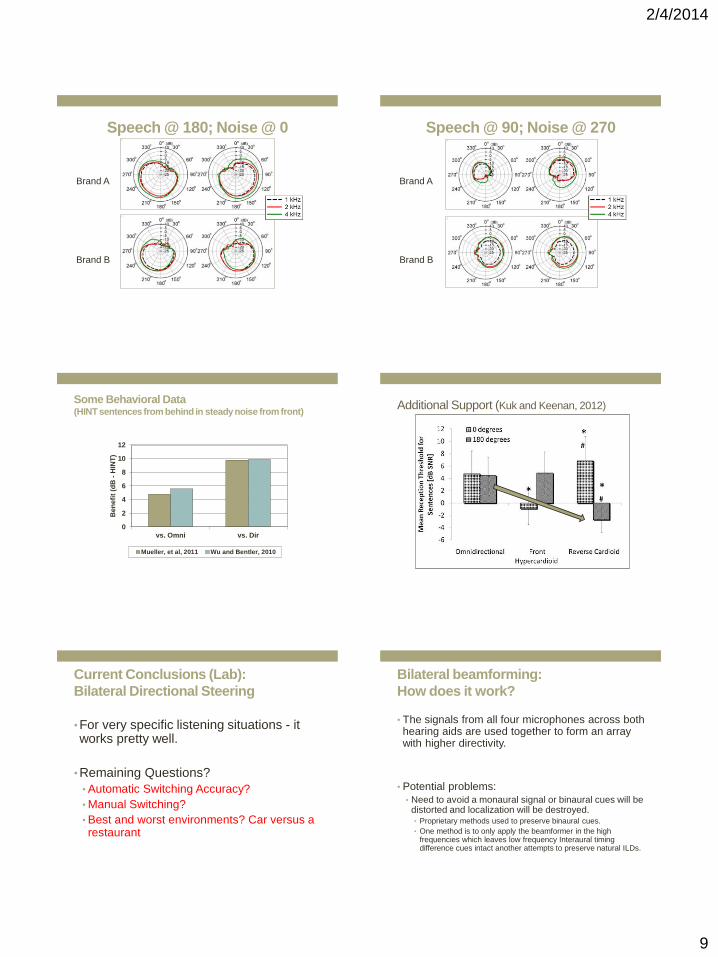
Some electroacoustic data
from Wu & Bentler
Brand A
Brand B
Speech @ 0; Steady State Noise @ 180
2/4/2014
9
Brand A
Brand B
Speech @ 180; Noise @ 0 Speech @ 90; Noise @ 270
Brand A
Brand B
Some Behavioral Data (HINT sentences from behind in steady noise from front)
0
2
4
6
8
10
12
vs. Omni vs. Dir
Ben
efi
t (d
B -
HIN
T)
Mueller, et al, 2011 Wu and Bentler, 2010
Additional Support (Kuk and Keenan, 2012)
Current Conclusions (Lab):
Bilateral Directional Steering
• For very specific listening situations - it works pretty well.
• Remaining Questions?
• Automatic Switching Accuracy?
• Manual Switching?
• Best and worst environments? Car versus a restaurant
Bilateral beamforming:
How does it work?
• The signals from all four microphones across both hearing aids are used together to form an array with higher directivity.
• Potential problems:
• Need to avoid a monaural signal or binaural cues will be distorted and localization will be destroyed. • Proprietary methods used to preserve binaural cues.
• One method is to only apply the beamformer in the high frequencies which leaves low frequency Interaural timing difference cues intact another attempts to preserve natural ILDs.

2/4/2014
10
Cue Preservation in Slightly (natural)
Directional, Directional and Beamformer?
0 10 20 30 40 50 60 70 80 900
2
4
6
8
10
Azimuth (degrees)
IL
D (
dB
)
Mild
Moderate
Strong
0 10 20 30 40 50 60 70 80 90-0.25
0
0.25
0.5
0.75
1
Azimuth (degrees)
IT
D (
ms)
Mild
Moderate
Strong
Effects of increased
venting on ITD cues
(if audible) and
expected effects.
Potential advantages to a beamformer (N = 18)
Beamformer improves speech recognition about 8-15% in reverberation (compared
to directional) – Picou, Aspell & Ricketts (in press)
(+3, +6, +9, or +12 dB SNR)
Hard Easy0
20
40
60
80
100
Sp
eech
Rec
ogn
itio
n P
erfo
rman
ce (
rau)
Low Reverberation
Hard Easy0
20
40
60
80
100
Sp
eech
Rec
ogn
itio
n P
erfo
rmac
e (r
au)
Moderate Reverberation
Omnidirectional
Directional
Beamformern.s.
n.s.
Are there significant downsides to this
cue-preserving bilateral beamformer
• Higher battery drain
• Gross Localization?
Gross Localization Test Environment
5.5 m
6.5 m
-45ᵒ
-60ᵒ
45ᵒ
60ᵒ
Moderate Reverberation (RT60= 650 ms)
Figure 4
-60 -45 45 600
20
40
60
80
100
120
Speaker Location (degrees)
Lo
caliz
atio
n A
ccura
cy (
%)
Auditory Only
-60 -45 45 600
20
40
60
80
100
120
Speaker Location (degrees)
Lo
caliz
atio
n A
ccura
cy (
%)
Auditory Visual
Moderate
Strong
Moderate
Strong
****
Subjective Preference
• 13 of 18 participants preferred the
beamformer or found it no different than
standard adaptive directional when in noisy
environments (including real “walking” trials).
• Why preferred?
• Most common reasons were “louder” or “easier to hear”

2/4/2014
11
Current Conclusions – Cue-Preserving
Bilateral Beamformer
• Bilateral beamformer has the potential to
provide additional speech recognition
benefits over adaptive directional processing
in moderate reverberation when listener is
facing signal of interest
• Some localization issues, but preference was
not significantly affected
Digital Feedback Suppression:
How Does It Work?
• First, the feedback path is acoustically
modeled in some cases for the individual
patient.
• Ongoing cancellation within the feedback
path is accomplished in a variety of ways
including cancelation and frequency shifting.
Digital Feedback Suppression:
Potential Benefit? • When feedback is minimized or eliminated,
patients are more apt to wear their hearing
aids.
• Acoustic feedback is known to be a stigma
associated with hearing aid use.
• With less feedback, there is a high probability
that more use-gain will be available without
venting alterations.
• The reduction of feedback allows for OC
fittings for greater degrees of hearing loss.
Factors related to assessing feedback
suppression effectiveness
• Magnitude of feedback reduction (e.g.
additional stable gain before feedback,
maximum REIG/REAR before feedback)
• Entrainment
• Some systems are much more susceptible
than others
• Speed in Dynamic FS systems
AGBF for 35 different hearing aid models
(20 were OC) From Ricketts, 2008 (Nov)
0
2
4
6
8
10
12
14
16
18
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35
AG
BF
(d
B)
Model
AGBF (Minimum across 2, 3, & 4 kHz)
10
15
20
25
30
35
40
2000 3000 4000
REI
G (
dB
)
Frequency (Hz)
Brand A Brand B Brand C Brand D
Brand E Brand F Brand G Average
Picking the “right” product can have a big impact
on your success with OC fittings!
Ricketts & Marcrum (2012)

2/4/2014
12
Digital Feedback Suppression
Individual Patient Differences?
• Essentially all patients could potentially
benefit from digital feedback suppression
• Data suggest considerable variability in
effectiveness across individual listeners
Feedback Suppression in Dynamic and
Static Conditions for 14 Participants
Maximum REIG Before Feedback
0
5
10
15
20
25
30
35
40
2000 3000 4000
RE
IG (
dB
)
Frequency (Hz)
Brand A-1 Brand A-2 Brand B Brand C
Distance (phone to ear): Initial point of feedback
and distance for sustained feedback (or touching
ear)
0
5
10
15
20
25
30
35
40
Initial Distance Final Distance
Dis
tan
ce
(m
m)
Distance From Ear For Feedback
Brand A-1 Brand A-2 Brand B Brand C
Note: 7 mm distance is touching the ear. Gain at 75% of AGBF
Duration of Feedback
(Past Initial FB Distance)
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
Brand A-1 Brand A-2 Brand B Brand C
Du
rati
on
of
Fe
ed
ba
ck
in
Se
co
nd
s
Note: Half Way between Initial and Final Distance. Gain at 75% of AGBF
QUANTIFYING DIGITAL
FEEDBACK SUPPRESSION
IN THE CLINIC
72
2/4/2014
13
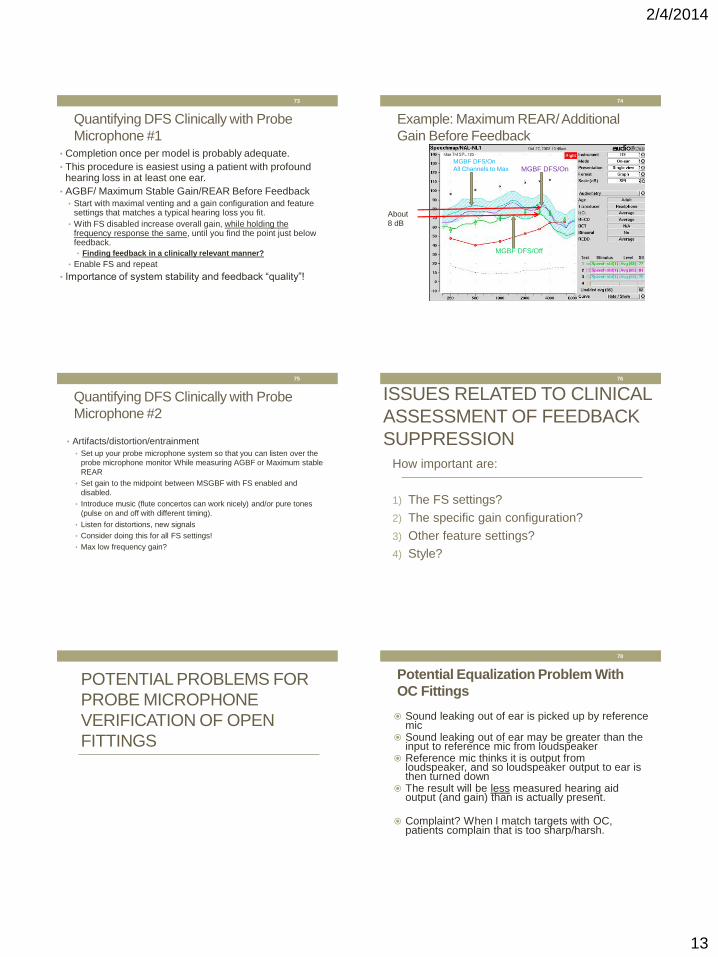
Quantifying DFS Clinically with Probe
Microphone #1 • Completion once per model is probably adequate.
• This procedure is easiest using a patient with profound hearing loss in at least one ear.
• AGBF/ Maximum Stable Gain/REAR Before Feedback • Start with maximal venting and a gain configuration and feature
settings that matches a typical hearing loss you fit.
• With FS disabled increase overall gain, while holding the frequency response the same, until you find the point just below feedback.
• Finding feedback in a clinically relevant manner?
• Enable FS and repeat
• Importance of system stability and feedback “quality”!
73
Example: Maximum REAR/ Additional
Gain Before Feedback
74
MGBF DFS/Off
MGBF DFS/On MGBF DFS/On
All Channels to Max
About
8 dB
Quantifying DFS Clinically with Probe
Microphone #2
• Artifacts/distortion/entrainment
• Set up your probe microphone system so that you can listen over the
probe microphone monitor While measuring AGBF or Maximum stable
REAR
• Set gain to the midpoint between MSGBF with FS enabled and
disabled.
• Introduce music (flute concertos can work nicely) and/or pure tones
(pulse on and off with different timing).
• Listen for distortions, new signals
• Consider doing this for all FS settings!
• Max low frequency gain?
75
ISSUES RELATED TO CLINICAL
ASSESSMENT OF FEEDBACK
SUPPRESSION
76
How important are:
1) The FS settings?
2) The specific gain configuration?
3) Other feature settings?
4) Style?
POTENTIAL PROBLEMS FOR
PROBE MICROPHONE
VERIFICATION OF OPEN
FITTINGS
Potential Equalization Problem With
OC Fittings
Sound leaking out of ear is picked up by reference mic
Sound leaking out of ear may be greater than the input to reference mic from loudspeaker
Reference mic thinks it is output from loudspeaker, and so loudspeaker output to ear is then turned down
The result will be less measured hearing aid output (and gain) than is actually present.
Complaint? When I match targets with OC, patients complain that is too sharp/harsh.
78
2/4/2014
14
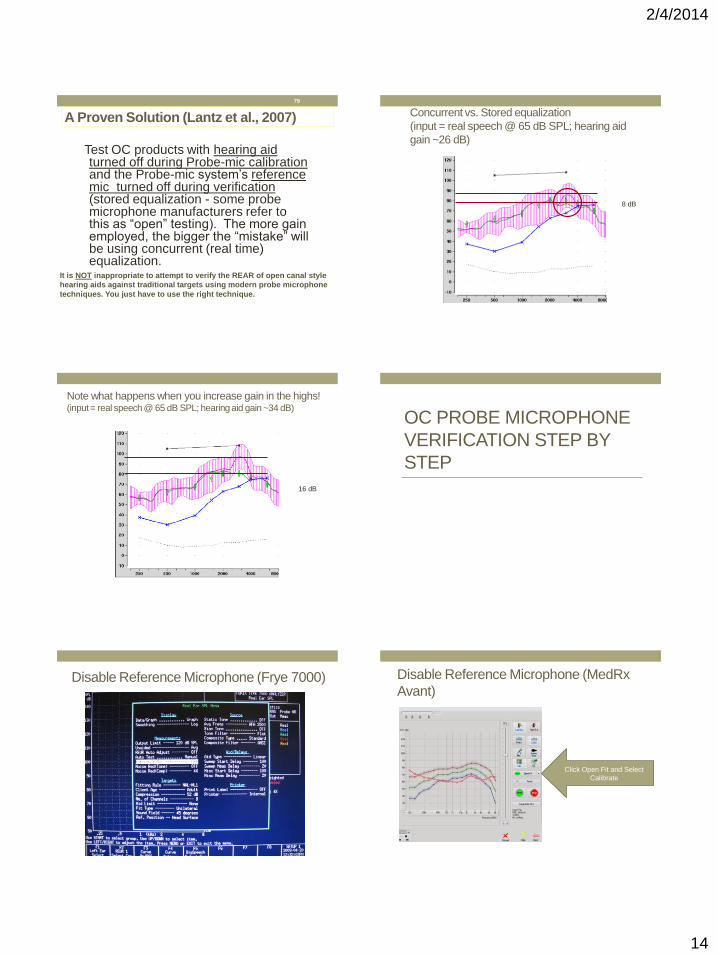
Test OC products with hearing aid turned off during Probe-mic calibration and the Probe-mic system’s reference mic turned off during verification (stored equalization - some probe microphone manufacturers refer to this as “open” testing). The more gain employed, the bigger the “mistake” will be using concurrent (real time) equalization.
79
A Proven Solution (Lantz et al., 2007)
It is NOT inappropriate to attempt to verify the REAR of open canal style
hearing aids against traditional targets using modern probe microphone
techniques. You just have to use the right technique.
Concurrent vs. Stored equalization
(input = real speech @ 65 dB SPL; hearing aid
gain ~26 dB)
8 dB
Note what happens when you increase gain in the highs! (input = real speech @ 65 dB SPL; hearing aid gain ~34 dB)
16 dB
OC PROBE MICROPHONE
VERIFICATION STEP BY
STEP
Disable Reference Microphone (Frye 7000) Disable Reference Microphone (MedRx
Avant)
Click Open Fit and Select
Calibrate
2/4/2014
15
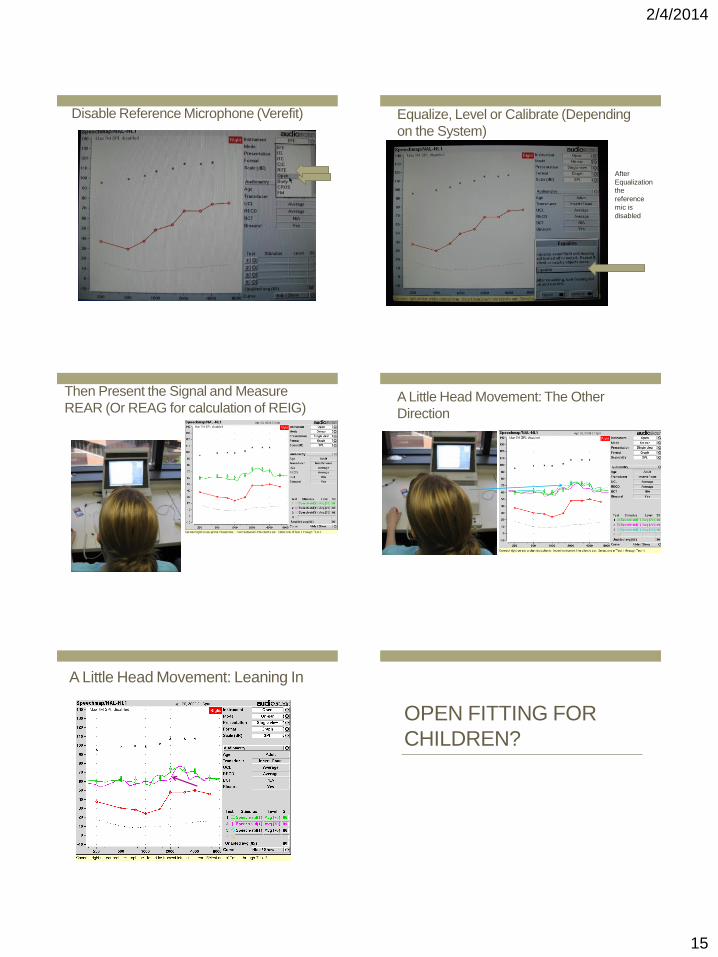
Disable Reference Microphone (Verefit) Equalize, Level or Calibrate (Depending
on the System)
After
Equalization
the
reference
mic is
disabled
Then Present the Signal and Measure
REAR (Or REAG for calculation of REIG) A Little Head Movement: The Other
Direction
A Little Head Movement: Leaning In
OPEN FITTING FOR
CHILDREN?
2/4/2014
16
Problems with RECD: Is REAR Possible?
• Kim and Ricketts (2013)
• REAR in 22 children aged 4 to 13
• Fitted Both Open (stored equalization) and
Closed (concurrent equalization) using the
Verifit.
• Examined Test – Re-Test Reliability
REAR Test Re-test Standard Deviation
0
0.5
1
1.5
2
2.5
3
3.5
100 1000
Te
st
Re
-te
st
Sta
nd
ard
De
via
tio
n
Frequency (Hz)
OPEN Closed
Conclusions
• No correlation between child’s age and
magnitude of test re-test error.
• Only three children were 4 or 5 yo; however,
REAR appears approximately as reliable in
children 4-13 as in adults, even when fitting OC.
A related issue which applies to all mini-
BTEs including Open: Custom versus
non-custom eartips
• Efficiency issues
• Retention issues
• Durability issues
• Feedback issues
• Is it really still open – subjective versus objective
“open”
• Consistent placement for feedback suppression
94
Wireless Routing:
How Does It Work?
• Signals from external devices (telephone, stereo, TV)
are routed to a single or multiple “middle men”
devices or in some of the newest hearing aids,
directly from smartphone to hearing aid.
Wireless Routing:
How Does It Work?
One large across company
difference is the distance this
signal can be sent; from a few
feet to a few hundred feet. This
affects where the middle
man/men can be placed or if one
is needed at all.
2/4/2014
17
Wireless Routing:
Potential Benefit? • Improve the SNR for several common listening
situation such as the telephone, television, etc.
• Bilateral signal for devices such as the
telephone
• Convenience for linking to or switching
between multiple external devices
• Smartphone control of the hearing aid
Wireless Routing:
Target Population?
• Applies to a wide range of hearing loss
groups, but best suited for patients who place
a high priority on using external devices.
• Patient also needs to be somewhat “gadget
savvy”
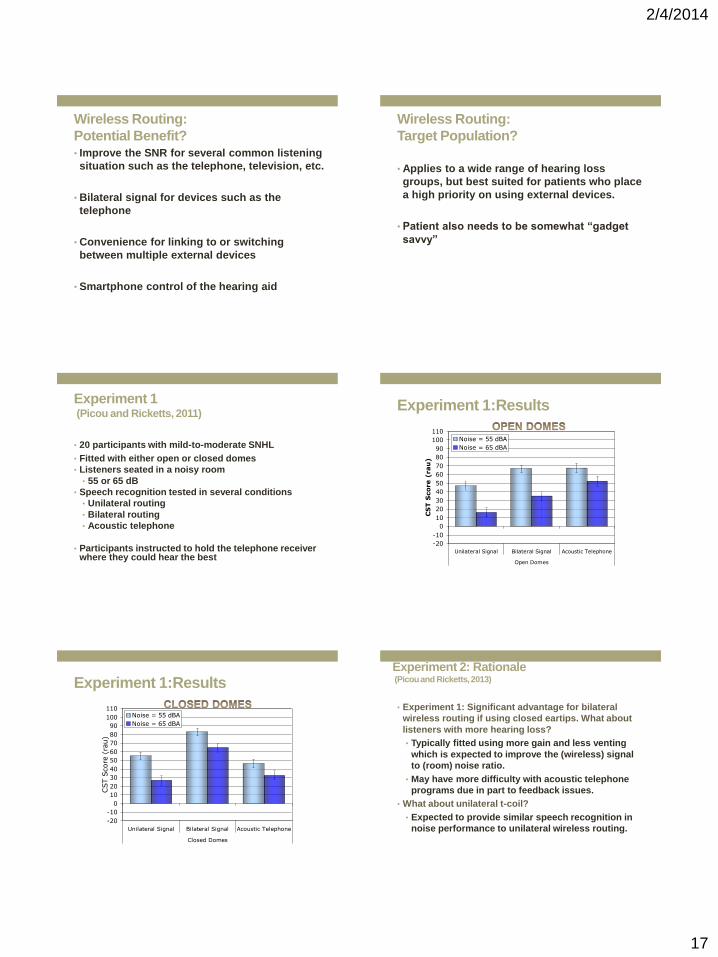
Experiment 1 (Picou and Ricketts, 2011)
• 20 participants with mild-to-moderate SNHL
• Fitted with either open or closed domes
• Listeners seated in a noisy room
• 55 or 65 dB
• Speech recognition tested in several conditions
• Unilateral routing
• Bilateral routing
• Acoustic telephone
• Participants instructed to hold the telephone receiver where they could hear the best
Experiment 1:Results
-20
-10
0
10
20
30
40
50
60
70
80
90
100
110
Unilateral Signal Bilateral Signal Acoustic Telephone
Open Domes
CS
T S
core (
rau
)
Noise = 55 dBA
Noise = 65 dBA
Experiment 1:Results
-20
-10
0
10
20
30
40
50
60
70
80
90
100
110
Unilateral Signal Bilateral Signal Acoustic Telephone
Closed Domes
CST S
core
(ra
u)
Noise = 55 dBA
Noise = 65 dBA
Experiment 2: Rationale (Picou and Ricketts, 2013)
• Experiment 1: Significant advantage for bilateral
wireless routing if using closed eartips. What about
listeners with more hearing loss?
• Typically fitted using more gain and less venting
which is expected to improve the (wireless) signal
to (room) noise ratio.
• May have more difficulty with acoustic telephone
programs due in part to feedback issues.
• What about unilateral t-coil?
• Expected to provide similar speech recognition in
noise performance to unilateral wireless routing.
2/4/2014
18
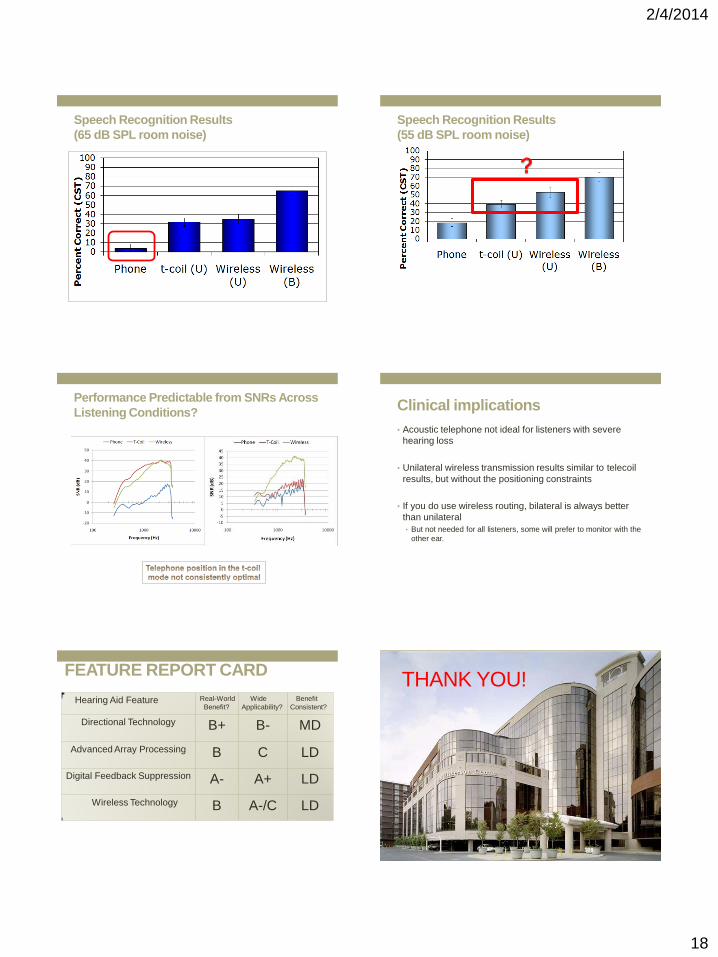
Speech Recognition Results
(65 dB SPL room noise)
Speech Recognition Results
(55 dB SPL room noise)
Performance Predictable from SNRs Across
Listening Conditions? Clinical implications
• Acoustic telephone not ideal for listeners with severe
hearing loss
• Unilateral wireless transmission results similar to telecoil
results, but without the positioning constraints
• If you do use wireless routing, bilateral is always better
than unilateral
• But not needed for all listeners, some will prefer to monitor with the
other ear.
FEATURE REPORT CARD
Hearing Aid Feature Real-World
Benefit?
Wide
Applicability?
Benefit
Consistent?
Directional Technology B+ B- MD
Advanced Array Processing
B C LD
Digital Feedback Suppression A- A+ LD
Wireless Technology B A-/C LD
THANK YOU!
108