diagnóstico y manejo de infecciones recurrentes en...
TRANSCRIPT

Diagnóstico Diagnóstico y y manejo manejo de de infecciones recurrentes infecciones recurrentes en en
pediatríapediatría
Ricardo Sorensen,MD
Chairman,Department of Pediatrics
LSUHSC••
Department of Pediatrics
LSUHSC

AFEBRILE



RECURRENT “PATHOLOGIC” INFECTIONS
Abnormality of infections defined by:• Age. Infections continuing after 3-5
years • Recurrence after antibiotic treatment• Severity and complications
• Lack of local or systemic predisposing factors

Distribution of Primary ImmunodeficienciesDiagnosed in 1,259 Patients
in 8 Latin American Countries in 1997
Defects of phagocytosis
7%Granulocyte
dysfunction with associated
abnormalities8%
Combined cellular & antibody IDs
5% Complement deficiencies
1%
Cellular & antibody IDs with
other abnormalities19%
Predominantly antibody IDs
60%


CLASSIFICATION OF PREDOMINANTLY ANTIBODY-DEFICIENCY SYNDROMES
Immunoglobulin deficiencies:• X-linked agammaglobulinemia• X-linked hyper IgM syndrome• Common variable immunodeficiency• Transient hypogammaglobulinemia of
infancy• IgM deficiency• IgA deficiencySorensen R, Moore C. Peds Clin NA 47:1225-1252, 2000
CLASSIFICATION OF PREDOMINANTLY ANTIBODY-DEFICIENCY SYNDROMES
IgG subclass deficiencies:• IgG 1 deficiency• IgG 2 deficiency
– selective deficiency– with IgA deficiency– with IgG4 deficiency
• IgG 3 deficiency• IgG 4 deficiency

ANTIBODY DEFICIENCIES
Clinical presentation (after 6 mo of age): • Recurrent upper and/or lower respiratory
infections• Severe or recurrent invasive infections
• Bronchiectasis• Chronic diarrhea

ANTIBODY DEFICIENCIES
Pathogens common to all deficiencies: • Streptococcus pneumoniae• Branhamella catarrhalis• Haemophilus influenzae (type b and
non typable)• Staphylococcus aureus

NEED FOR EVALUATION OF ANTIBODY MEDIATED
IMMUNITY
• Clinical manifestations common to many conditions
• Possible treatment of deficient specific immunity included in
evaluation

EVALUATION OF ANTIBODY-MEDIATED IMMUNITY
• IgM, IgG, IgA and IgE concentrations• IgG subclass concentrations
• Specific antibodies– Anti-protein antibodies– Anti-conjugate polysaccharide antibodies– Anti-polysaccharide antibodies

Patient 1Recurrent antibiotic use is abnormal
Importance of physical examination
Neutropenia may be part of some antibody deficiencies
Relationship between immunological phenotypes and molecular and gene abnormalities

CASE REPORT
Well-developed, well-nourished 14 month-old male at the 75th percentile for height and weight
Unremarkable family history
Recurrent URI and otitis media starting at age 3 months requiring 12 antibiotic treatments in the last 12 months
One severe febrile episode requiring hospitalization
Ear tubes were not placed

CASE REPORT (Continued)
Physical examination:
•Allergic shiners
•Purulent nasal secretion
•Cervical lymph nodes: not palpable
•Tonsils: absent

CASE REPORT (Continued)
WBC: 4.77 cells/ml
ANC 0.24 cells/ml

CASE REPORT (Continued)
Immunoglobulin concentrations: IgG mg/dl <7.9IgA mg/dl <6.0IgM mg/dl <5.0IgE IU/ml <7.0
Lymphocyte subpopulations: CD3/CD4 NormalCD19 <1CD 20 <1


CASE REPORT(Continued)
B cell tyrosine kinase (Btk):
Absent


Antibody DeficiencyPhenotypes-Genotypes
C V I DB cells IgM IgG IgA
H I G M
Agammaglobulinemia
IgM IgG IgA
B cells IgG IgA
SAP
CD40L
NEMO
B tk
, X linked& , AR
ICOS
CD40AIDUNG
Cµ IGHMIgα CD79Aλ Light chain
CD179BBLNK
IgM
B cells
Deficient Normal Elevated


CLASSIFICATION OF PREDOMINANTLY ANTIBODY-DEFICIENCY SYNDROMES
Continued
Specific antibody deficiencies with normal immunglobulin concentrations (SAD)

Patient 2
Normal immunoglobulinconcentrations do not rule out an
antibody deficiency

CASE REPORTWell developed 5-year-old boy.
Chronic rhinitis, treated with antihistamines and nasalsteroids.
Recurrent wheezing treated with anti-leukotrienes andinhaled steroids.
History of recurrent upper respiratory infectionsincluding purulent otitis media and chronicsinusitis that improve transiently on antibiotics.
These infections persist despite ear tube placementand sinus surgery.

CASE REPORT continued
INITIAL EVALUATIONNo evidence of atopy,
low normal IgE concentration,
negative skin prick test withcommon inhalant and foodallergens.

CASE REPORT continued
Immunoglobulin Concentrations
ImmunoglobulinsIgG mg/dl 750IgA mg/dl 66IgM mg/dl 75IgE IU/ml 10
IgG Subclasses:IgG1 mg/dl 510IgG2 mg/dl 175IgG3 mg/dl 67IgG4 mg/dl 25

PNEUMOCOCCAL INFECTIONS
Importance in evaluation of antibody-mediated immunity
• Frequency of infections
• Multi-valent vaccines



PNEUMOCOCCAL CAPSULAR VACCINES
• POLYSACCHARIDE VACCINES
– 23 VALENT, PPV
• CONJUGATED VACCINES
– HEPTAVALENT, PCV-7

Number of Vaccines Neededfor Protection
Vaccines
4
1
1 2 >2Age in YearsIM
MU
NO
LOG
AIC
AL
MA
TUR
ATI
ON
3
2

Pneumococcal immunization depending on age of initiation
1 dose> 5 years
1 dose1 dose2-5 years
2 doses13-24 months
3 doses7-12 months
2,4,6,12-15 months
Normal infants
Polysaccharide (PPV)
Conjugate (PCV-7)
Vaccine

CASE REPORT continuedAntibody response to pneumococcal polysaccharide vaccine
Serotypes Vaccine Antibody response (IgG mg/ml)
Danish # US # PV Baseline Post- PV
1 1 X3 3 X4 4 X
6B 26 X9V 68 X14 14 X
18C 56 X19F 19 X23F 23 X
0.08 0.120.10 0.100.16 0.240.10 0.160.20 0.300.16 0.200.30 0.240.12 0.200.22 0.24
PV = Polysaccharide VaccineCV = heptavalent conjugate vaccine (Prevnar)

CASE REPORT continued
Specific tetanus, diphtheria and H. Influenzae antibodies:
Anti-proteinantibodies
Post-Immunization
Reference
Diphtheriatoxoid
2.69 >0.01 AU/ml
Tetanus toxoid 1.34 >0.1 IU/ml
H. Influenzae prp 2.400 >100 ng/ml

PATIENT DIAGNOSIS
Specific antibody deficiency to polysaccharide antigens with normal immunglobulins and normal specific antibodies to protein and conjugate polysaccharides

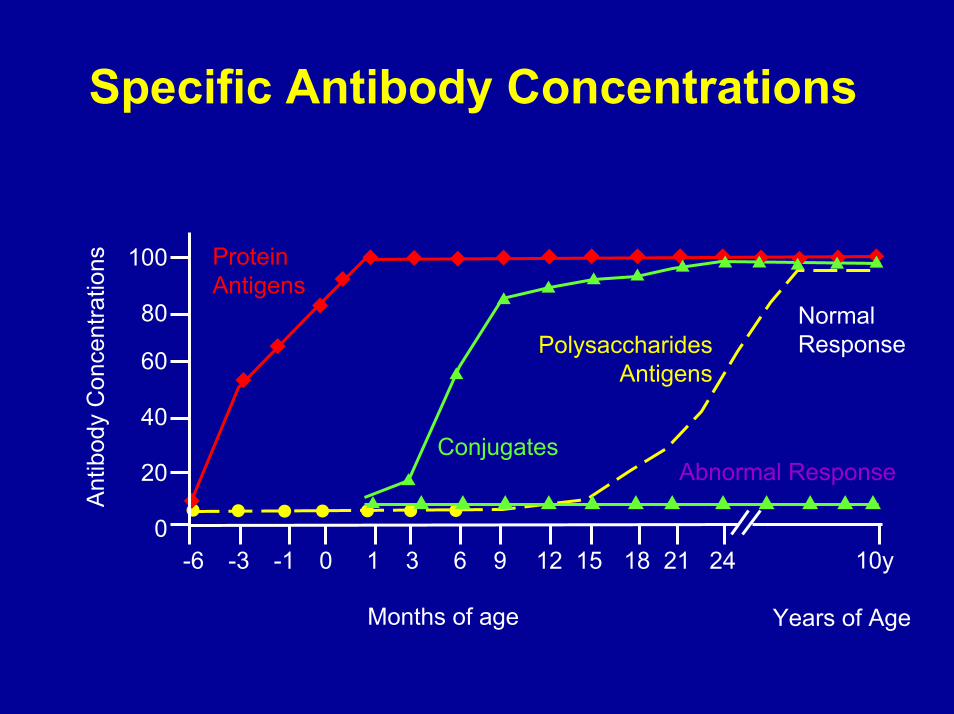
Specific Antibody Concentrations
0
20
40
60
80
100
-6 -3 -1 0 1 3 6 9 12 15 18 21 24
Ant
ibod
y C
once
ntra
tions
Months of age
ProteinAntigens
Conjugates
Normal Response
Years of Age
10y
PolysaccharidesAntigens
Abnormal Response
Specific Antibody Concentrations
0
20
40
60
80
100
-6 -3 -1 0 1 3 6 9 12 15 18 21 24
Ant
ibod
y C
once
ntra
tions
Months of age
ProteinAntigens
Conjugates
Normal Response
Years of Age
10y
PolysaccharidesAntigens
Abnormal Response
SPECIFIC ANTIBODY DEFICIENCIES
Associations• Atopic diseases
– Asthma– Atopic dermatitis
• Chromosomal abnormalities– Down syndrome– Pierre Robin– Ring chromosome 18– Other
• Any condition with recurrent infections
ANTIBODY DEFICIENCIESSUMMARY
• Variable immunological phenotypes• Recurrent or severe respiratory
infections• Frequent antibiotic use• May have mild clinical phenotypes with
late onset of infections• Patients usually do not appear ill

Recurrent Mucosal Infections
• Immunological evaluation after:
• Proper antibiotic treatment
• Reduction of inflammation
• Placement of ventilation tubes

Recurrent/Severe InfectionImmunization & EvaluationFully
ImmunizedIncomplete
Immunization
PathologicalRecurrent Infections
SevereInfection• Male• Absenttonsils
Mild InfectionNormal
Lymphoid Tissue
Evaluate* ImmunizeEvaluate if
infections continue
Evaluate*
* Immunuglobulin & specific antibodies

Visit our Website:www.medschool.lsuhsc.edu/pediatrics
About Us Faculty & Staff Clinics Subspecialties CME Education ResearchAffiliated Hospitals Board Review Contact Us LSU School of Medicine
Web graphics byLSU Learning Resources