diagnostic imaging of pleural lesions
TRANSCRIPT

ChestPleural Lesions

Mohamed Zaitoun
Assistant Lecturer-Diagnostic Radiology Department , Zagazig University Hospitals
EgyptFINR (Fellowship of Interventional
Neuroradiology)[email protected]



Knowing as much as possible about your enemy precedes successful battle
and learning about the disease process precedes successful management

Pleural Lesions1-Pleural Fluid Collections2-Pleural Tumors


1-Pleural Fluid Collections :a) Pleural Effusionb) Hemothoraxc) Empyemad) Chylothorax

a) Pleural Effusion :1-Types2-Causes3-Radiographic Features4-Differential Diagnosis

1-Types :a) Transudateb) Exudate

Transudate Exudate
1-Protein < 3gm/dl > 3gm/dl
2-Protein (plasma/fluid)
< 0.5 > 0.5
3-LDH < 200 IU< 70% of serum level
> 200 IU> 70% of serum level
4-Causes CHF,RF,Cirrhosis Infection,Tumor, Embolism

2-Causes :a) Tumorb) Inflammationc) Cardiovasculard) Congenitale) Metabolicf) Trauma
a) Tumor :1-Bronchogenic carcinoma2-Pleural metastases3-Malignant mesothelioma4-Lymphoma

b) Inflammation :1-Pneumonia , TB , Empyema2-Collagen vascular disease3-Abdominal Disease :a) Pancreatitisb) Subphrenic abscessc) Boerhaave's syndromed) Meigs' syndrome

c) Cardiovascular :1-Congestive heart failure2-Pulmonary embolism3-Renal failured) Congenital :-Hydrops (neonate)e) Metabolic :-Hypoproteinemiaf) Trauma

-N.B. Pleural effusion due to extrathoracic causes :
1-Pancreatitis2-Subphrenic abscess3-Following abdominal surgery4-Meig’s syndrome5-Neoplastic syndrome6-Fluid overload7-Cirrhosis

3-Radiographic Features :a) Plain Radiographyb) CT
a) Plain Radiography :1-Lateral Decubitus2-PA & Lateral 3-Large Effusions4-Subpulmonic Effusions

1-Lateral Decubitus :-Most sensitive, may detect as little as 25
mL

Lateral Decubitus


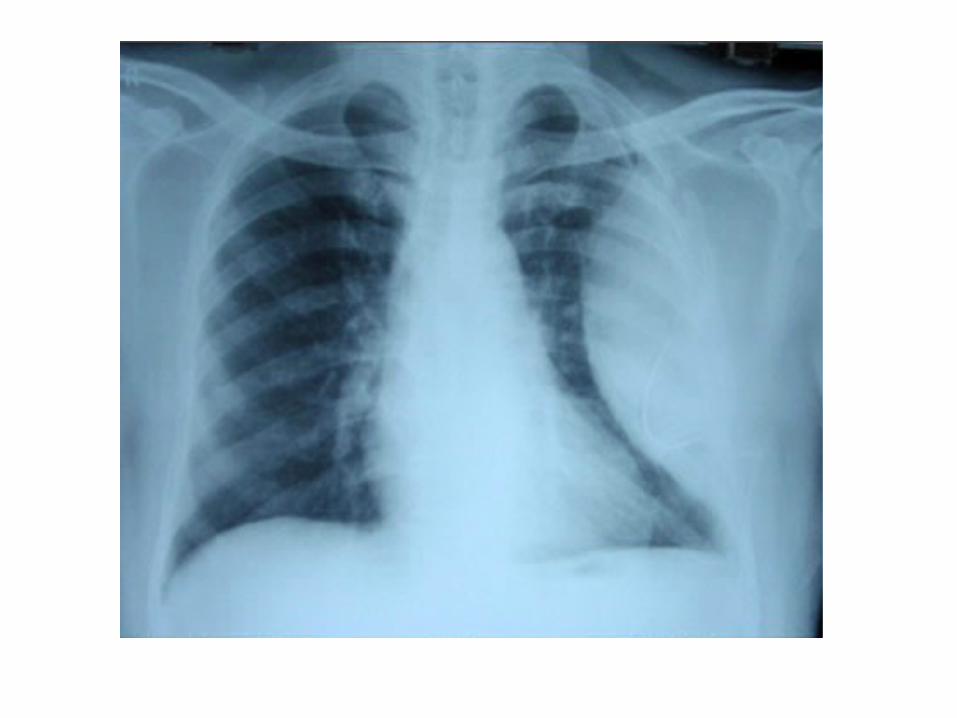
2-PA & Lateral : -Blunting of costophrenic angles

Normal CPA Blunted CPA
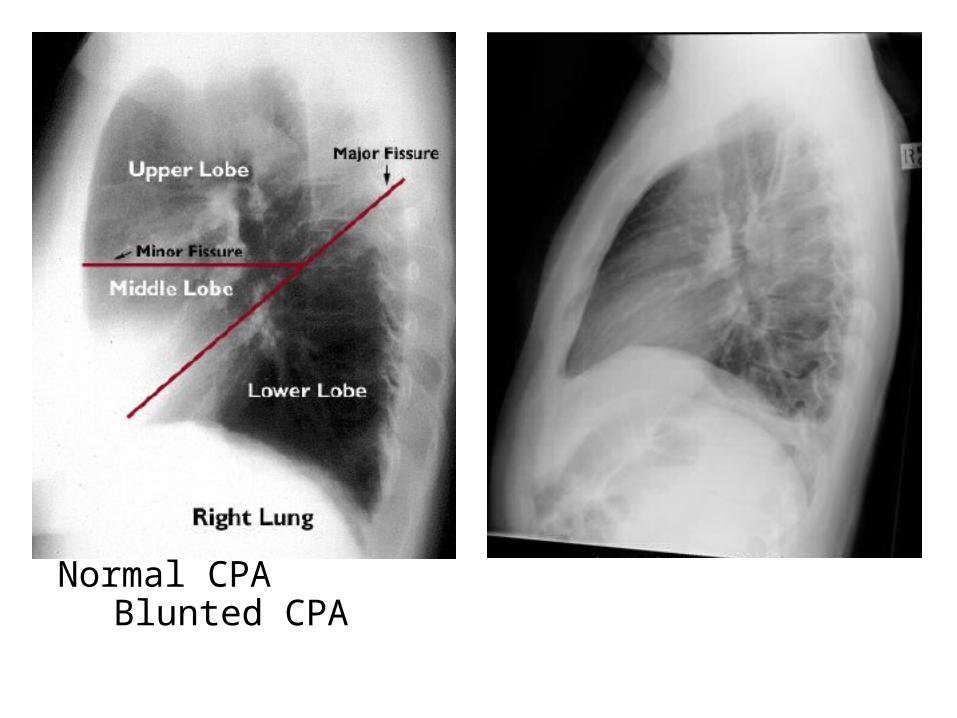
Normal CPA Blunted CPA


Loculated effusion in the minor fissure (arrow) ,the opacity is smoothly marginated and biconvex

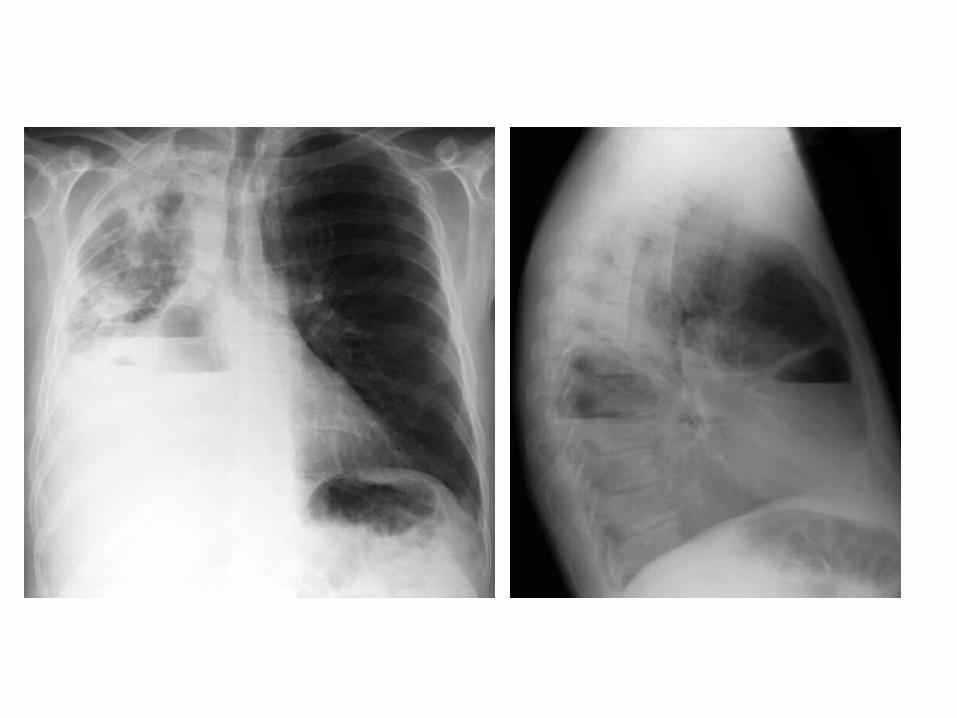
3-Large Effusions :-All cardiophrenic angles obliterated-Mediastinal shift-Elevated diaphragm

-Opacity (E) in the lower left hemithorax with obliteration of the left hemidiaphragm and a curvilinear upper margin (arrow) and a mediastinal shift to the right , these findings are typical of a pleural effusion , in addition , minimal blunting of the right costophrenic angle is seen



4-Subpulmonic Effusions :a) Definitionb) Diagnosis

a) Definition :-Accumulation of pleural fluid in isolation between
the lung base and diaphragmb) Diagnosis :1-Abnormally large distance between fundus of
stomach and lung base2-Abrupt termination of vascular shadows at the
level of the diaphragm3-Blunting of affected costophrenic angle (PA)

4-A blunted posterior costophrenic sulcus may be seen on the lateral film
5-Pseudodiaphragm can appear to peak more laterally
6-Pseudodiaphragm can appear more horizontal medially than would typically be seen with a normal diaphragm
7-Crowding of lung parenchyma on affected side

Increased distance between the air-filled fundus of the stomach and the left "hemidiaphragm" (arrowed) , the left lateral decubitus chest image demonstrates fluid in the pleural space (arrow)

The left dome of diaphragm is higher than right with increased distance of diaphramatic outline to the fundal air bubble of stomach , suggestive of a subpulmonic pleural effusion , confirmed by CT


b) CT :-Excellent at detecting small amounts of fluid
and is also often able to identify the underlying intrathroacic causes (e.g. malignant pleural deposits or primary lung neoplasms) as well as subdiaphragmatic diseases (e.g. subdiaphragmatic abscess)
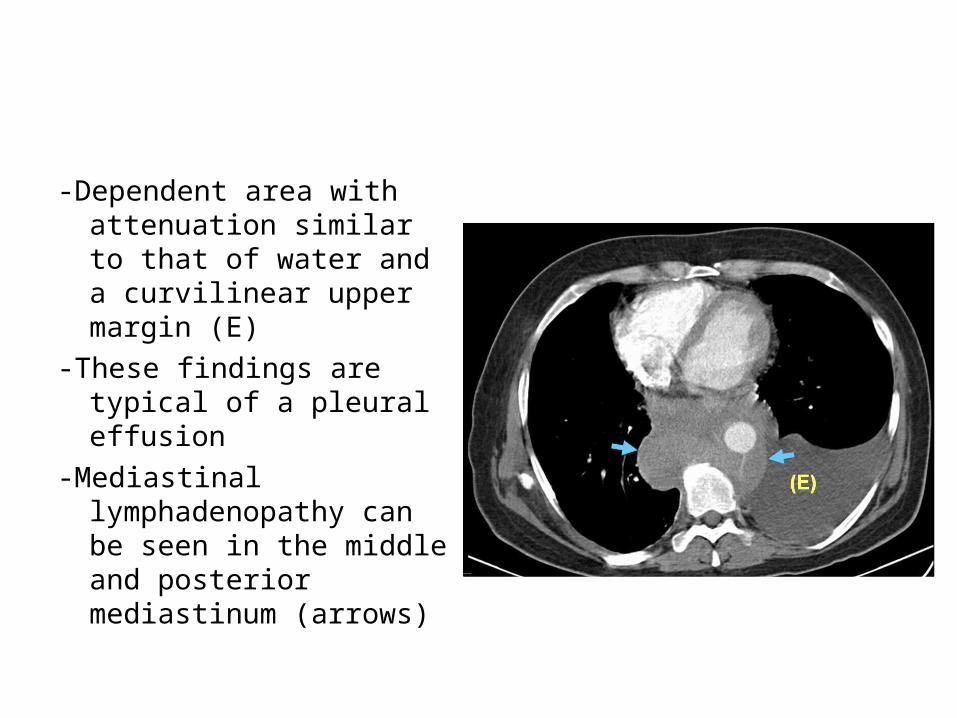
-Dependent area with attenuation similar to that of water and a curvilinear upper margin (E)
-These findings are typical of a pleural effusion
-Mediastinal lymphadenopathy can be seen in the middle and posterior mediastinum (arrows)

-Mass in the right upper lobe abutting the pleura (*)
-Irregular soft tissue thickening of the pleural surface (arrow) and pleural effusion (E) are present
-The findings are most consistent with primary lung neoplasm with pleural metastasis and malignant pleural effusion


4-Differential Diagnosis :a) Raised hemidiaphragm , e.g.
hepatomegaly , phrenic nerve palsy b) Collapse or consolidationc) Pleural thickening, e.g. old T.B. or
empyemad) Inferior pulmonary ligament

b) Hemothorax :-See Lung Trauma

Hemothorax, there is complete opacification of the right hemithorax with slight shift of the trachea towards the left , fluid is seen tracking up the lateral margin of the thorax (red arrow) , the clue to the diagnosis is the bullet (blue circle)

c) Empyema :1-Definition2-Stages3-Causes4-Radiographic Features5-Differential Diagnosis

1-Definition :-Infected purulent and often loculated
pleural effusion and is a cause of a large unilateral pleural collection

2-Stages :-Stage 1 : Exudative-Stage 2 : Fibrinopurulent -Stage 3 : Fibrinous

3-Causes :a) Postinfection (parapneumonic) , 60%b) Postsurgical , 20%c) Posttraumatic , 20%
4-Radiographic Features :a) Plain Radiographyb) CT

a) Plain Radiography :-Can resemble a pleural effusion and can mimic a
peripheral pulmonary abscess -Pleural fluid is typically unilateral or markedly
asymmetric-Form an obtuse angle with the chest wall -The lenticular shape (bi-convex) is also
suggestive of the diagnosis, as transudative / sterile pleural effusions tend to be cresentic in shape (i.e. concave towards the lung)






-Thick and irregular rind of calcified pleura (yellow arrows) in the right hemithorax with slight shift of the heart and mediastinal structures towards the right due to volume loss , calcified tuberculous empyema

(A) CXR shows pleural-based opacity (arrow) with tapering obtuse margins in left hemithorax
(B) CT+C shows loculated collection (arrowhead) with peripherally enhancing thick walls

(A) CXR shows volume loss right hemithorax with veil-like calcified (arrow) pleural opacity
(B) CT+C shows evidence of calcified chronic empyema (arrow) with proliferation of extrapleural fat and crowding of ribs suggestive of volume loss in right hemithorax

b) CT :-Typically appears as a fluid density collection in the pleural
space , sometimes with locules of gas (due to BPF or gas forming organisms)
-They form obtuse angles with the adjacent lung which is displaced and compressed
-The pleura is thickened due to fibrin deposition and in-growth of vessels
-Pleural enhancement-At the margins of the empyema , the pleura can be seen
dividing into parietal and visceral layers , the so-called split pleura sign which is the most sensitive and specific sign on CT









Thick and irregular calcification of both visceral and parietal pleura encasing a small amount of hypodense loculated pleural collection , Tberculous empyema

Organized liquid collection was found with trabeculations and calcifications , T.B.

5-Differential Diagnosis :-From pleural effusion-From Peripherally Located Abscess-Pleural Calcification

-From pleural effusion :1-Shape & Location : Empyema usually-Form an obtuse angle with the chest wall-Unilateral or markedly asymmetric whereas
pleural effusions are (if of any significant size) usually bilateral and similar in size
-Lenticular in shape (bi-convex) whereas pleural effusions are crescentic in shape (i.e. concave towards the lung)

2-CT Findings : Features suggestive of empyema :-Enhancing thickened pleura (split pleura sign)
whereas pleural effusion have thin imperceptable pleural surfaces
-Locules of gas-Obvious septations-Associated consolidation-Associated adjacent infection (e.g. sub-
diaphragmatic abscess)

-From Peripherally Located Abscess :1-Shape :-Abscess is usually round in all projections-Abscess may form a acute angle with the
costal surface / chest wall-Empyema is usually lentiform

2-CT Findings :a) Relationship to adjacent bronchi / vessels-Abscesses will abruptly interrupt
bronchovascular structures-Empyema will usually distort and compress
adjacent lungb) Split pleura sign (thickening and
separation of visceral and parietal pleura is a sign of empyema)

c) Wall :-Abscesses have thick irregular wall-Empyema are usually smootherd) Angle with pleura :-Abscesses usually have an acute angle
(claw sign)-Empyema have obtuse angles


Empyema Abscess

-Pleural Calcification :1-Old Empyema2-Old Hemothorax3-Asbestosis Inhalation4-Silicosis5-Talc Exposure6-Malignant pleural methoselioma (5 %)

d) Chylothorax :1-Definition2-Causes3-Radiographic Features

1-Definition :-Presence of chylous fluid in pleural space
often as a result of obstruction or disruption to thoracic duct
-It may be congenital or acquired

2-Causes :a) Tumor , 55% (especially lymphoma)b) Trauma , 25%-Iatrogenic duct laceration-Sharp , blunt traumac) Idiopathic , 15%d) Rare causes -Lymphangioleiomyomatosis-Filariasis
3-Radiographic Features :a) Plain Radiographyb) CT

a) Plain Radiography :-Increased density of hemithorax with
ipsilateral pleural effusion (most common on the left)
-Less frequently bilateral


b) CT :Most of the time , it appears as a simple fluid
collection of near water density


2-Pleural Tumors :a) Primary Pleural Tumorsb) Secondary Pleural Tumors

a) Primary Pleural Tumors :1-Malignant Pleural Mesothelioma2-Pleural Fibroma3-Pleural Fibrosarcoma4-Pleural Liposarcoma

1-Malignant Pleural Mesothelioma :a) Incidenceb) Pathologyc) Radiographic Featuresd) Differential Diagnosis

a) Incidence :-Uncommon entity and accounts for 5-28 %
of all malignancies that involve the pleura-Risk is 300 times larger in asbestos
workers than in general population

b) Pathology :1-Epithelial : 60%2-Mixed : 25%3-Sarcomatoid : 15%


c) Radiographic Features :1-General Appearance2-Plain Radiography3-CT

1-General Appearance :a) Pleural thickening together with effusion ,
60%b) Isolated pleural thickening , 25%c) Isolated pleural effusion , 15%d) Hemithoracic contraction , 25%e) Pleural calcification , 5%

Pleural thickening together with effusion

Thickening of the pleura in the left upper zone (white arrow) and bilateral calcified pleural plaques (black arrow)

Isolated Pleural Effusion

Diffuse left-sided pleural thickening , a pleural effusion and ipsilateral volume loss

Unilateral circumferential pleural thickening and calcification and contracted hemi thorax

2-Plain Radiography :-Is of limited value and non-specific-Pleural opacity which may extend around and encase the
lung-Reduction in volume of the affected hemithorax is common
resulting in shift of the mediastinum towards the lesion-Rib destruction or extension beyond the lateral and
anterior margins of the chest wall may be evident-Mediastinal lymph node enlargement and pleural effusion
may also be seen







3-CT :-Soft tissue attenuation nodular mass which spreads along
pleural surfaces -Calcification is seen which usually represents engulfed
calcified pleural plaques rather than true tumor calcification , sarcomatoid variants may demonstrate osteosarcoma or chondrosarcomatous components which may also be calcified
-Mesotheliomas have a predilection for direct invasion of adjacent structures (chest wall , diaphragm and mediastinal content) but also frequently metastasize to the contralateral lung and local nodes

-To confidently predict chest wall invasion the extrapleural fat plane should be seen to be infiltrated and / or direct extension in bone or muscle identified
-Presence of a pericardial effusion suggests transpericardial extension

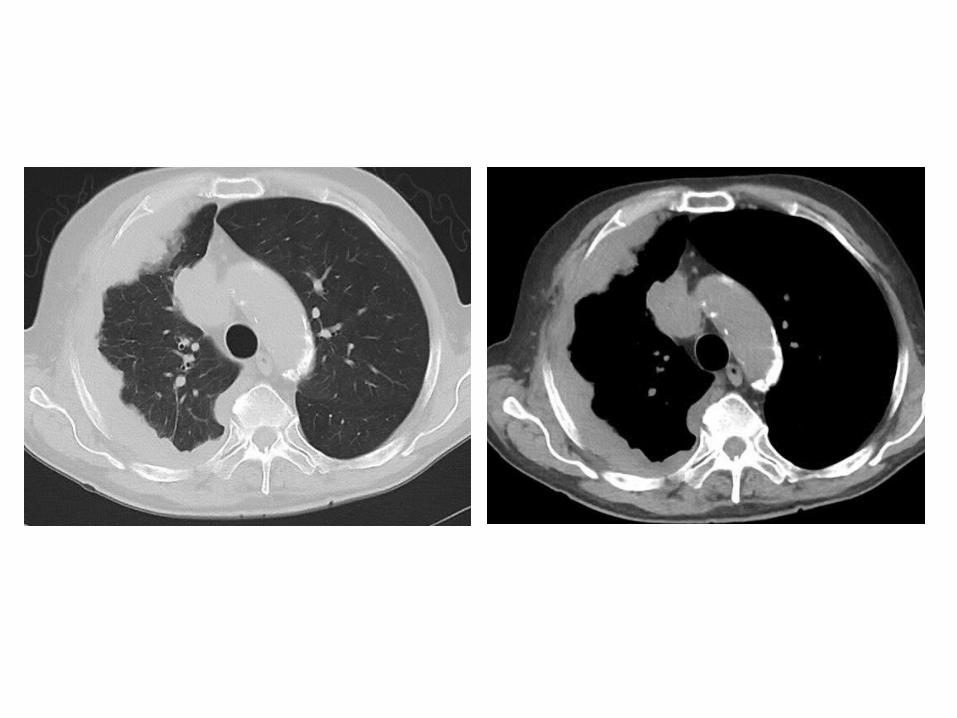
CT+C shows enhancing nodular pleural thickening (arrows) involving the costal and mediastinal pleura extending into the major fissure (arrowhead) with crowding of ribs suggestive of volume loss changes in left hemithorax

CT+C shows homogeneously enhancing nodular pleural thickening (arrows) involving the mediastinal and costal pleura with volume loss changes in left hemithorax
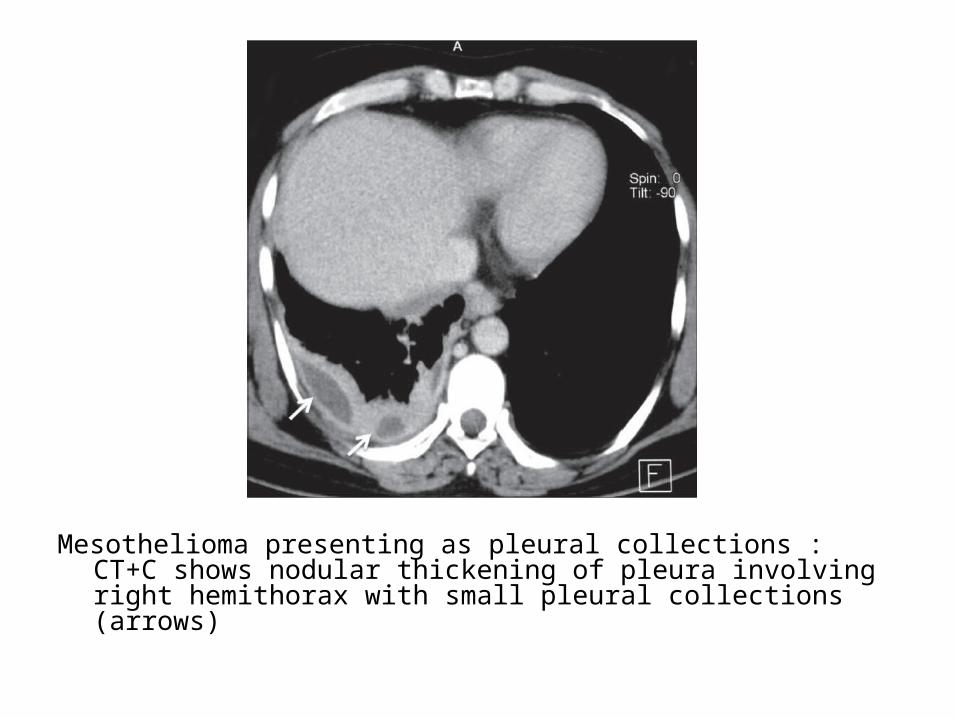
Mesothelioma presenting as pleural collections : CT+C shows nodular thickening of pleura involving right hemithorax with small pleural collections (arrows)

Mesothelioma presenting as a pleural effusion : CT+C shows moderate left pleural effusion as loculated collection with thickening of pleura (arrows) in a case of mesothelioma



d) Differential Diagnosis : Single pleural massa) Tumors :1-Pleural Tumors :-Mesothelioma-Pleural Fibroma-Pleural Fibrosarcoma & Liposarcoma2-Pleural Metastases3-Peripheral Bronchogenic Carcinoma
b) Loculated Fluid (on plain film) :1-Pleural Effusion (pseudotumor)2-Empyema3-Hemothoraxc) Mass related to ribs or chest wall : e.g. Ewing
sarcoma of chest wall , Askin tumord) Splenosise) Infection including tuberculosisf) Benign Asbestos Related Pleural Disease

2-Pleural Fibroma :a) Incidenceb) Locationc) Pathologyd) Radiographic Featurese) Differential Diagnosis

a) Incidence :-Also known as a Solitary Fibrous Tumor of
the Pleura (SFTP) -Rare benign pleural based tumor which
accounts for < 5 % of all tumors involving the pleura
-Usually presents in the 6th to 7th decades
b) Location :-More in the mid to lower zones of the chest-In 75% of cases they arise from visceral
pleura with the remainder arising from the parietal pleura

c) Pathology :1-Benign , 80% (previously classified as
benign mesothelioma)2-Invasive , 20% (unlike malignant
mesothelioma , this tumor grows only locally)

d) Radiographic Features :1-Plain Radiography2-CT
1-Plain Radiography :-Presents as a pleural based mass-Tends to be relatively circumscribed and
can sometimes be lobulated-It often forms an obtuse angle with the
chest wall -Calcification , rib destruction and pleural
effusions are typically not associated feature

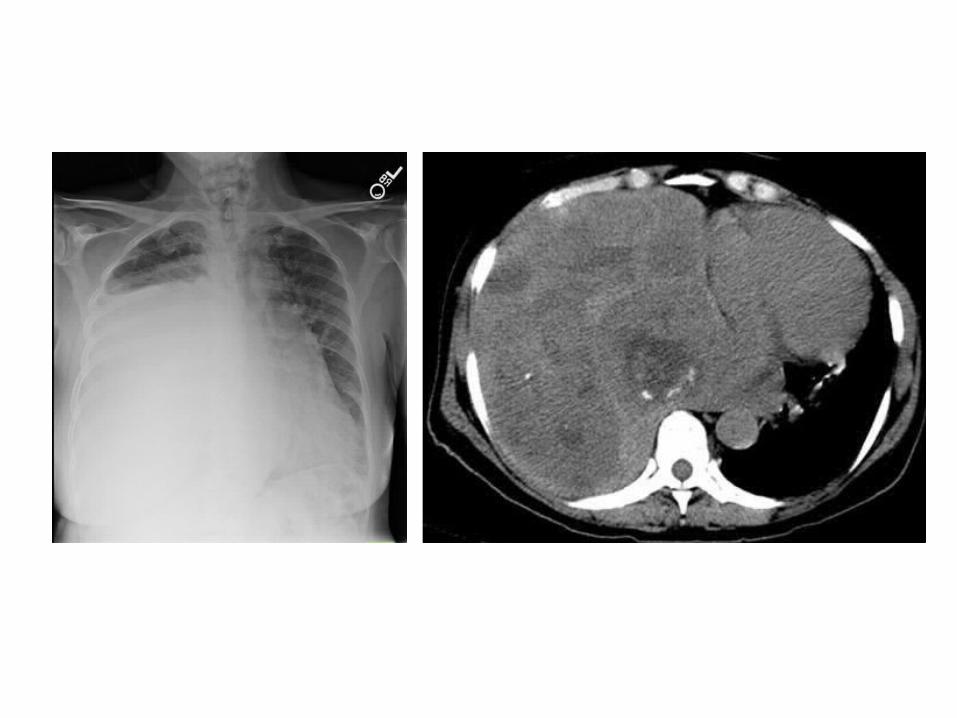
A well-circumscribed pleural-based mass is seen in the upper left hemithorax , the angle between the mass and the chest wall is obtuse



(A) CXR shows pleural-based opacity (arrow) in right hemithorax with peripheral obtuse margins
(B) CT+C shows heterogeneously enhancing pleural-based mass (arrowhead) proved to be benign fibrous pleural tumor

(A) CXR shows lobulated pleural-based opacity (arrow) in right apical region
(B) CT+C shows heterogeneously enhancing peripheral mass lesion (arrow)


2-CT :-Well delineated solitary pleural based mass ,
often lobulated-Tends to have soft tissue attenuation on
unenhanced scans-Homogenous intense background enhancement
on contrast enhanced scans (from rich vascularization)
-Chest wall invasion may be seen in the invasive form , absent in benign form




-CT+C shows a huge mass in the left hemithorax-X-ray chest PA view providing an impression of a loculated
pleural effusion

Malignant fibrous tumor of pleura : CT shows heterogeneously enhancing mass lesion left hemithorax (arrowhead) causing mediastinal displacement to the right


e) Differential Diagnosis :-Single pleural mass :See before

b) Secondary Pleural Tumors :1-Pleural Metastases2-Invasive Tumors to the Pleura :-Thymoma with pleural invasion-Pericardial tumors with pleural invasion3-Invasive Chest Wall Tumors :-Ewing sarcoma of chest wall with pleural
invasion

-Pleural Metastases :a) Causesb) Radiographic Features

a) Causes :-The adenocarcinoma histological type is the most likely to produce
metastasis in the pleura 1-Lung Cancer :-May account for up to 40% of pleural metastases2-Breast Carcinoma :-May account for 20% of pleural metastases-Commonly gives a pleural effusion3-Ovarian Cancer4-Lymphoma :-May account for 10% of metastases5-Gastric Carcinoma6-Invasive Thymoma

b) Radiographic Features :1-Plain Radiography2-CT

1-Plain Radiography :-Pleural metastases itself does not usually
give radiological image so that the chest radiograph usually shows only the images of pleural effusion



2-CT :- CT may show nodules hidden by pleural effusion-The pleural metastases usually manifest as
nodular or lenticular masses-The soft tissue component is enhanced frequently
after administration of intravenous contrast-Other findings seen on CT are enlarged
mediastinal lymph nodes , lung nodules , rib lesions or subcutaneous mass

CT+C shows heterogeneously enhancing pleural-based soft tissue (white arrow) with rib destruction (black arrow) in a case of pleural metastases from renal cell carcinoma

CT+C shows heterogeneously enhancing pleural-based mass lesion (arrow) in left hemithorax with extrathoracic extension in a case of metastatic adenocarcinoma

CT+C shows nodular pleural thickening (arrows) involving the costal and mediastinal pleura with malignant pleural effusion in a case of metastatic ovarian adenocarcinoma

Pleural drop metastases in invasive Thymoma: CT+C shows heterogeneously enhancing anterior mediastinal mass (black arrow) with mild left pleural effusion and ipsilateral pleural implants (arrows)
