diagnostic evaluation of suspected drug-induced liver injury · paracetamol; ~50% of dili)...
TRANSCRIPT

Diagnostic evaluation of suspected
Drug-Induced Liver Injury
Ynto de Boer, MD
Department of Gastroenterology and Hepatology

Disclosure
No disclosures
Drug-induced liver injury
?
Outline
What is DILI?
What, other than the drug, causes DILI?
How to diagnose DILI?
Resources

Drug-induced liver injury
Hepatotoxicity:
Hepatocytes ALT/AST elevation
Cholangiocytes Alk Phos elevation
Direct toxicity, dose dependent (eg. Paracetamol; ~50%
of DILI)
Idiosyncratic injury

Drug-induced liver injury
Kleiner et al. Hepatology 2014
Ciprofloxacin -
Acute hepatitic
injury
Isoniazid -
chronic
hepatitic injury
Anabolic steroid
- Acute
cholestatic injury
Amox-clav -
Chronic
cholestatic injury
Duloxetine -
Cholestatic
hepatitis injury

Mechanisms
Cell death: apoptosis and necrosis
Reactive metabolite formation/bioactivation
Drug transporter–mediated drug-induced
hepatotoxicity
Immune-mediated response
Mitochondrial dysfunction
Activation of stress signaling pathways
Shesu et al. Clin Liv Dis 2017
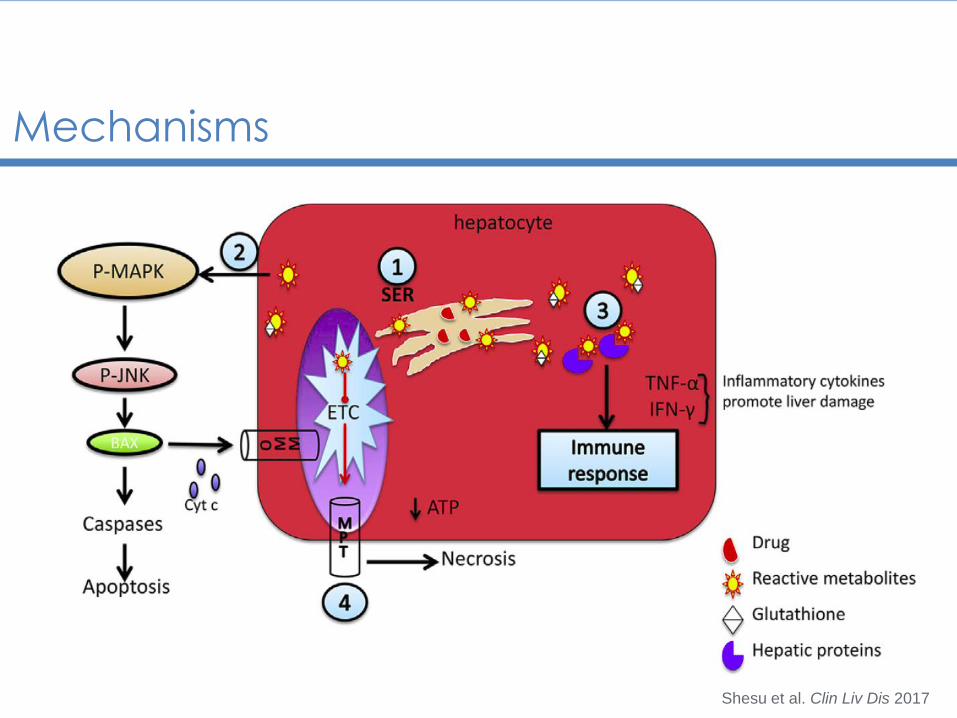
Mechanisms
Shesu et al. Clin Liv Dis 2017

Genetics - Flucloxacillin
HLA-B*57:01
Daly et al. Nat Genet 2009
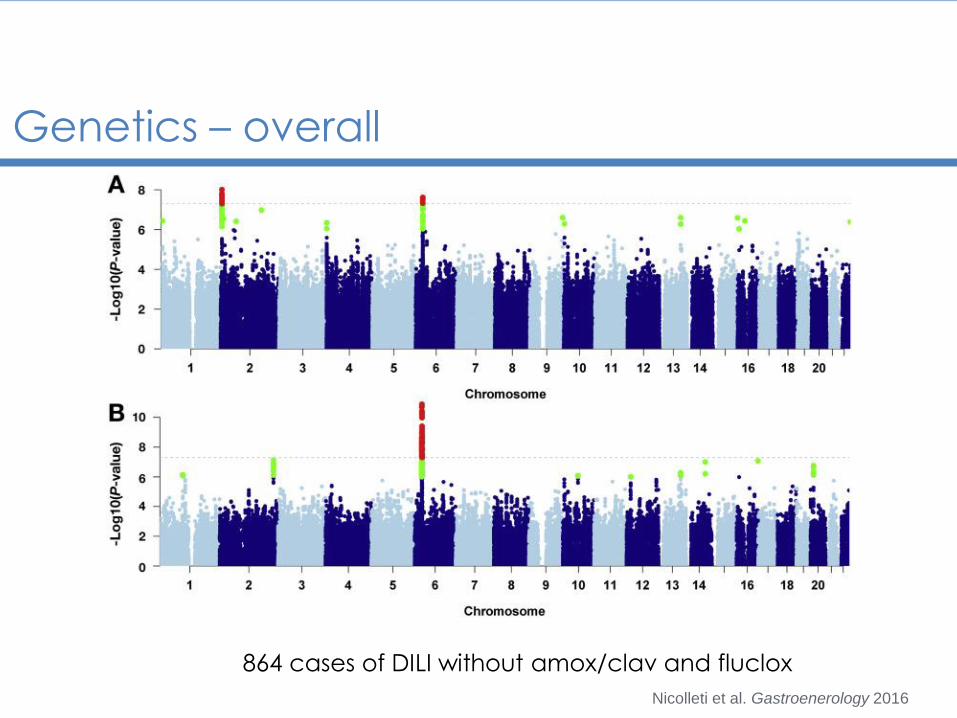
Genetics – overall
864 cases of DILI without amox/clav and fluclox
Nicolleti et al. Gastroenerology 2016

Genetics
Association Effect Size of rs72631567, A*33:01, and rs28521457 Across Different Liver Injury Patterns
CohortAssociatedvariant OR 95% CI P value
AF cases AF controls
Entire DILI cohort rs72631567 2.0 1.6−2.5 9.7 × 10−9 0.05 0.03
A*33:01 2.6 1.8−3.7 7.0 × 10−8 0.02 0.01
rs28521457 1.5 1.3−1.9 7.0 × 10−8 0.06 0.04
Cholestatic and mixed DILI cohort rs72631567 2.4 1.7−3.4 9.5 × 10−7 0.06 0.03
A*33:01 5.0 3.3−7.9 4.2 × 10−13 0.04 0.01
rs28521457 1.0 0.7−1.5 .9 0.04 0.04
Hepatocellular DILI cohort rs72631567 1.6 1.2−2.3 2.5 × 10−3 0.04 0.03
A*33:01 1.5 0.8−2.6 .19 0.01 0.011
rs28521457 2.1 1.6−2.7 4.8 × 10−9 0.08 0.040
Nicolleti et al. Gastroenerology 2016
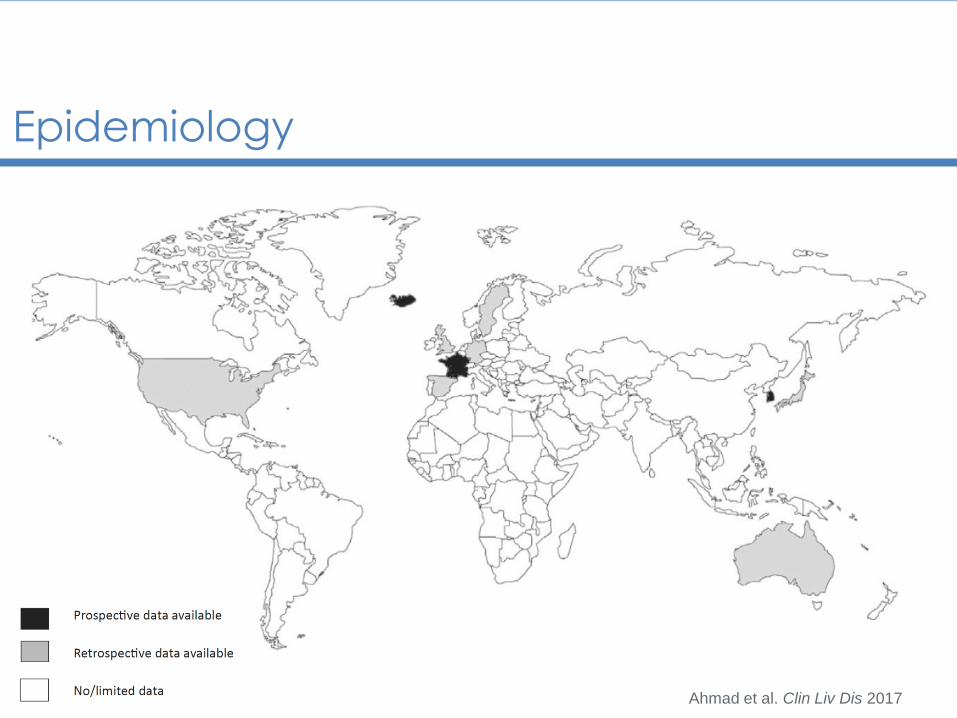
Epidemiology
Ahmad et al. Clin Liv Dis 2017

Idiosyncratic DILI
National studies of drug-induced liver injury incidence
Country Iceland France Korea United Kingdom Spain Sweden
Years of study 2010–2011 1997–2000 2005–2007 1994–1999 2004–2009 1995–2005
Study type Prospective Prospective Prospective Retrospective Retrospective Retrospective
Number of DILI cases 96 34 371 128 57 77
Crude DILI incidencerate/100,000 per year 19.1 13.9 12 2.4 3.01 2.3
Ahmad et al. Clin Liv Dis 2017

Idiosyncratic DILI
Drug-induced liver injury registries across the world
Country United States Spain Korea
Years of study 2004–2013 1994–2004 2005–2007
Study type Prospective Prospective Prospective
Number of DILI cases 899 461 371
Antimicrobials (% of total) 45.3% 32% —
HDS (% of total) 16.1% — 73%
Ahmad et al. Clin Liv Dis 2017
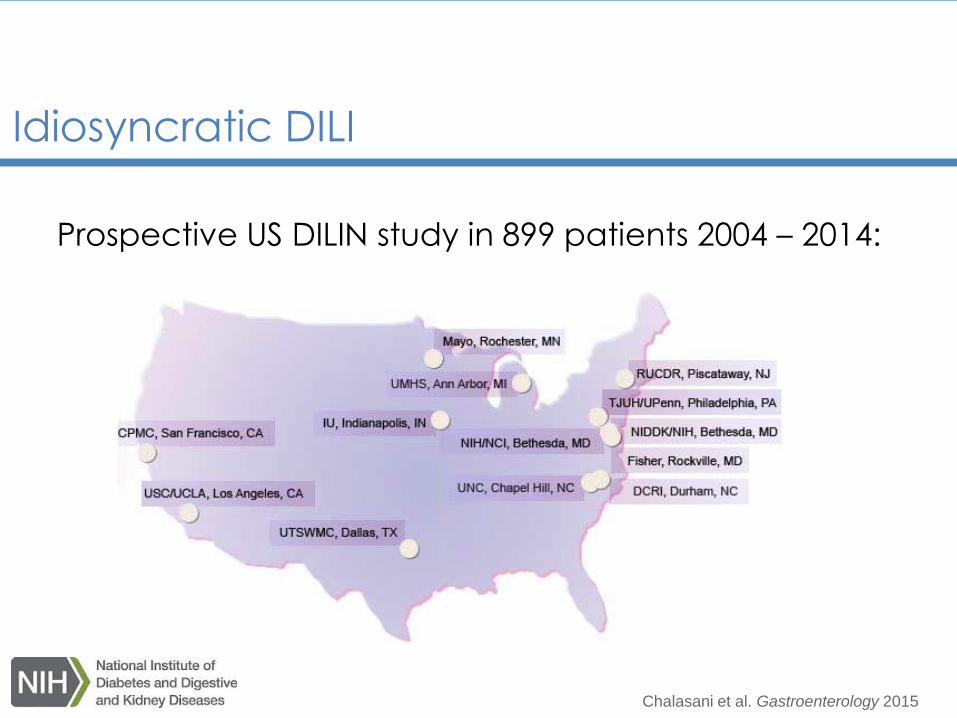
Idiosyncratic DILI
Chalasani et al. Gastroenterology 2015
Prospective US DILIN study in 899 patients 2004 – 2014:

Idiosyncratic DILI
Chalasani et al. Gastroenterology 2015
Therapeutic classes n Individual agents n
1 Antimicrobials 408 1 Amoxicillin-clavulanate 91
2 Herbal and dietary supplements 145 2 Isoniazid 48
3 Cardiovascular agents 88 3 Nitrofurantoin 42
4 Central nervous system agents 82 4 Sulfamethoxazole/trimethoprim 31
5 Anti-neoplastic agents 49 5 Minocycline 28
6 Analgesics 33 6 Cefazolin 20
7 Immunomodulatory 27 7 Azithromycin 18
8 Endocrine 20 8 Ciprofloxacin 16
9 Rheumatologic 13 9 Levofloxacin 13
10 Gastrointestinal 12 10 Diclofenac 12
Prospective US DILIN study in 899 patients 2004 – 2014:
Clinical presentation
Mild transaminase elevation Acute liver failure
Bilirubinemia
Up to 51% of transplantation for acute liver failure is due
to DILI
Ostapowicz et al. Ann Intern Med 2002

Augmentin
Mild transaminase elevation Acute liver failure
Bilirubinemia
Up to 51% of transplantation for acute liver failure is due
to DILI
livertox.nih.gov
64 year old man

Minocycline
Mild transaminase elevation Acute liver failure
Bilirubinemia
Up to 51% of transplantation for acute liver failure is due
to DILI
livertox.nih.gov
64 year old man55 year old woman
Unexplained liver test abnormalities
Ascertain the type of injury
Exclusion of other etiologies:
obstruction, (acute) viral hepatitis, (non-)alcoholic
hepatitis, shock liver, autoimmune liver disease
History of exposure to drugs, herbals and dietary
supplements?
Look for typical/distinguishing features:
immunoallergic or autoimmune features
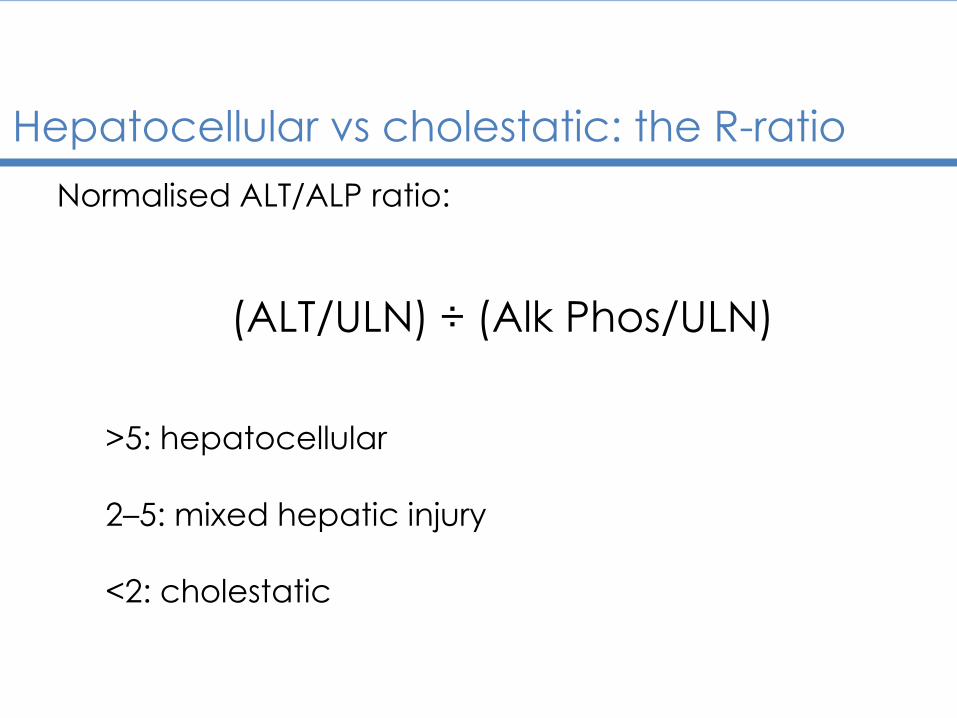
Hepatocellular vs cholestatic: the R-ratio
Normalised ALT/ALP ratio:
(ALT/ULN) ÷ (Alk Phos/ULN)
>5: hepatocellular
2–5: mixed hepatic injury
<2: cholestatic

Characteristics for causality assessment
Time to onset/latency
Course
Risk factors
Concomitant drugs
Nondrug causes of liver injury
Previous information on the hepatotoxicity of the drug
Response to rechallengeDanan et al. Clin Epidemiol 1993

Risk factors
Age:
exposure, multiple drugs
Gender:
metabolism, exposure
Alcohol
Other liver disease
Ethnicity/Genetics:
Asian ethnicity
HLA genotypesDanan et al. Clin Epidemiol 1993

Phenotypes
Autoimmune (ANA, SMA, IgG):
nitrofurantoin, minocycline, hydralazine, methyldopa
Immunoallergic (rash, fever, eosinophilia):
aromatic anticonvulsants, allopurinol, sulfonamides
and fluoroquinolones
Drug specific phenomena:
icterus in anabolic steroids

Diagnostic scores: RUCAM
Roussel-Uclaf Causality Assessment Method:
The individual points range from -3 to +3
The total possible score ranges from -9 to +14.
0 or less “excluded”
1 to 2 “unlikely”
3 to 5 “possible”
6 to 8 “probable”
>8, “highly probable”
Danan et al. Clin Epidemiol 1993
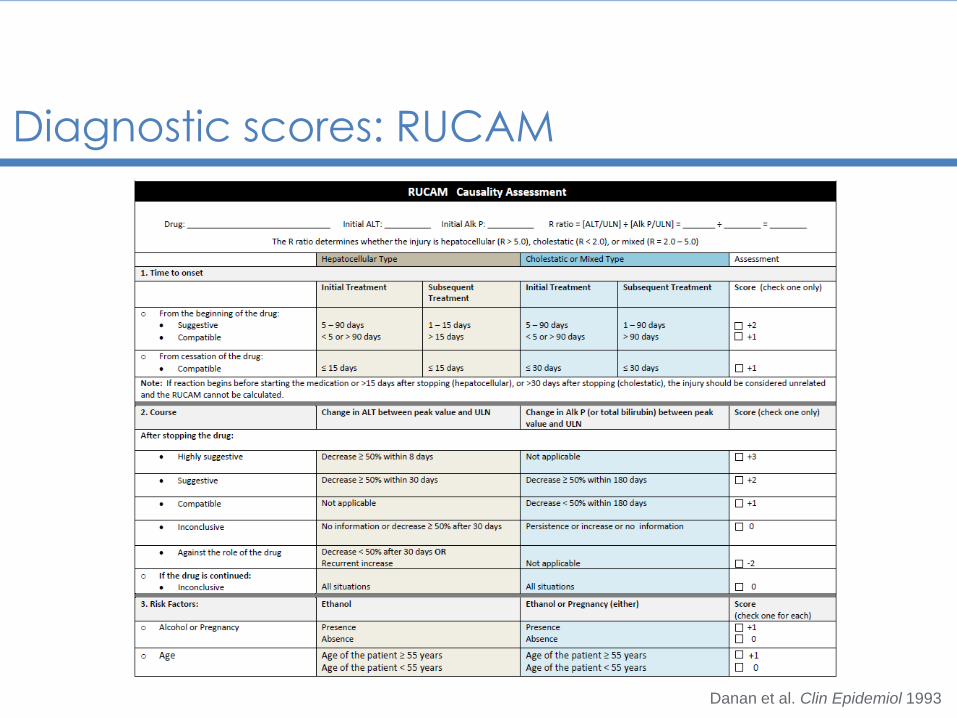
Diagnostic scores: RUCAM
Danan et al. Clin Epidemiol 1993

Liver biopsy
Can be helpful, but
is usually not necessary
Exclusion of
other etiologies
Distinctive patterns
can be recognised
Kleiner et al. Hepatology 2014
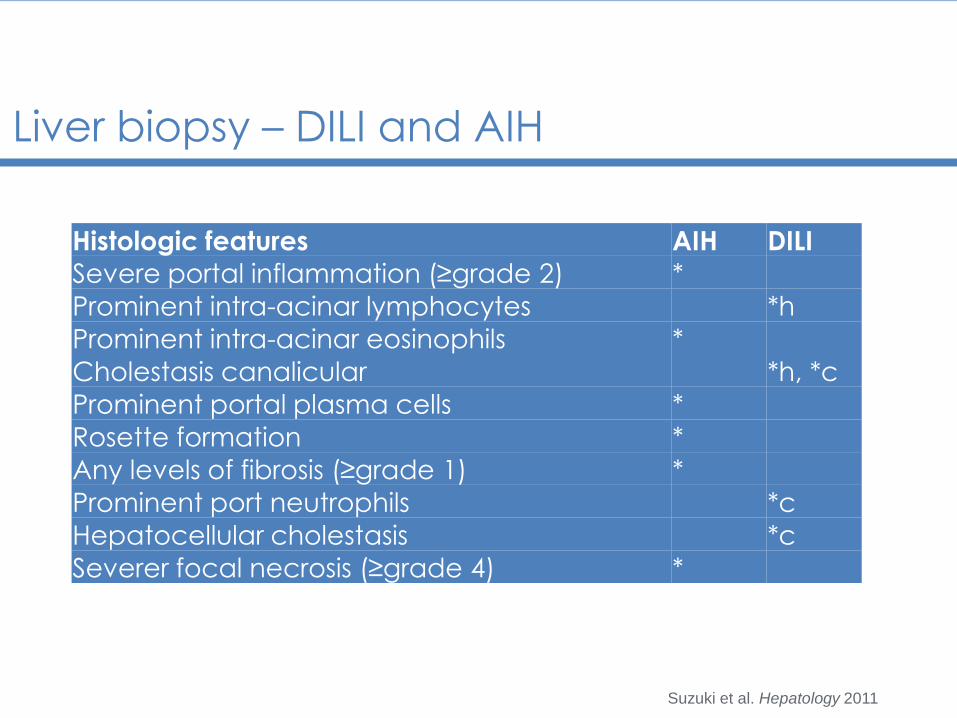
Liver biopsy – DILI and AIH
Suzuki et al. Hepatology 2011
Histologic features AIH DILI
Severe portal inflammation (≥grade 2) *
Prominent intra-acinar lymphocytes *h
Prominent intra-acinar eosinophils *
Cholestasis canalicular *h, *c
Prominent portal plasma cells *
Rosette formation *
Any levels of fibrosis (≥grade 1) *
Prominent port neutrophils *c
Hepatocellular cholestasis *c
Severer focal necrosis (≥grade 4) *

Autoimmune features in DILI
adslkf
De Boer et al. Clin Gastroenterol Hepatol 2017
nitrofurantoin, minocycline, methyldopa and hydralazine

Hy’s Law
Hyman Zimmerman: “drug-induced hepatocellar
jaundice is a serious lesion, with mortality from 10 to 50%”
Bob Temple:
Hepatocellular-type injury (ALT > 3 upper limit of
normal: ULN)
Bilirubin >2x ULN, no evidence of obstruction (> Alk
Phos) or Gilbert’s syndrome
Exclude other causesTemple Pharmacoepidemiol Drug Saf 2006

Outcome
US DILIN outcome data
Characteristics Antimicrobials
(n = 408)
Cardiovascular
(n = 88)
CNS agents
(n = 82)
Antineoplastics
(n = 49)
Analgesics
(n = 33)
Fatal, (%) 6.9 5.7 6 10 3
Death, at any time (%) 5.1 5.7 6.1 29 3
Liver transplantation (%) 3.9 2.3 3.7 0 0
Chalasani et al. Gastroenterology 2015

Outcome
Iceland
Björnsson et al. Gastroenterology 2013

Herbal and dietary supplements
De Boer et al. Clin Liv Dis 2017
The incidence of HDS-ILI is rising
Ask, and ask again
Herbal and dietary supplements
De Boer et al. Clin Liv Dis 2017

Livertox
adslkf
livertox.nih.gov
Conclusion
DILI can mimic any other liver disease and diagnosis is
based on careful history and pattern of injury
Liver biopsy may be helpful but generally not necessary
HDS product are often not perceived as drugs or
potentially dangerous: Ask and ask again
A helpful resource: livertox.nih.gov

Thank you for your attention!