diagnosis and management of fatty liver
TRANSCRIPT
Diagnosis and Management of Fatty LiverHemant Shah MD MScCH HPTE
University Health Network, University of Toronto

Hemant Shah Financial Disclosures (over past 24 months)
Speaker Advisory Research Consultant
Abbvie √ √ √
Boehringer-
Ingelheim
√
Gilead √ √ √
Intercept √ √
Lupin √ √ √
Merck √ √ √
• Affiliation with a not-for-profit organization:• Freeport Physicians’ Education Fund Honorarium
Mitigating Potential Bias
• Recommendations for Drug Therapy will be based on peer reviewed journal articles and published guidelines

Learning Objectives
At the conclusion of this activity, participants will be able to:
1. Identify current guidelines for screening for fatty liver disease
2. Determine a management plan for incidental findings of fatty liver disease
3. Identify and determine a management plan for low-risk patients
4. Define lifestyle changes for low-risk patients
5. Identify patients who should be referred for further investigation
6. Formulate the options for treatment for fatty liver disease
Case of Patient ND
• 56F new to your practice
• PMH: Severe obesity (BMI 47), PCOS, OSA, Depression
• Meds: Cymbalta
• SocHx: No significant alcohol, Non-smoker, Desk job (taxi dispatch)
• Labs: Hb 117, WBC 7.1, Plt 180, ALT 128, AST 96, ALP 75, INR 0.9, Bilirubin 12, Albumin 39
• Abdo U/S: Liver 23.1cm, Spleen 17.1cm, Fatty liver
• Initial workup: Hep B, Hep C, Iron all normal

Case of Patient ND
• 56F new to your practice
• PMH: Severe obesity (BMI 47), PCOS, OSA, Depression
• Meds: Cymbalta
• SocHx: No significant alcohol, Non-smoker, Desk job (taxi dispatch)
• Labs: Hb 117, WBC 7.1, Plt 180, ALT 128, AST 96, ALP 75, INR 0.9, Bilirubin 12, Albumin 39
• Abdo U/S: Liver 23.1cm, Spleen 17.1cm, Fatty liver
• Initial workup: Hep B, Hep C, Iron all normal
What’s the Diagnosis?What’s the Severity of the Liver Disease?What’s the Prognosis?What treatments should I recommend?

Definition of NAFLD
Non-alcoholic fatty liver disease (NAFLD) is defined as the presence of fat in the liver (hepatic steatosis) either on imaging or on liver histology after the exclusion of secondary causes of fat accumulation in the liver (e.g., significant alcohol consumption, certain medications, and other medical conditions).
Puri and Sanyal. Clinical Liver Disease. Aug 2012
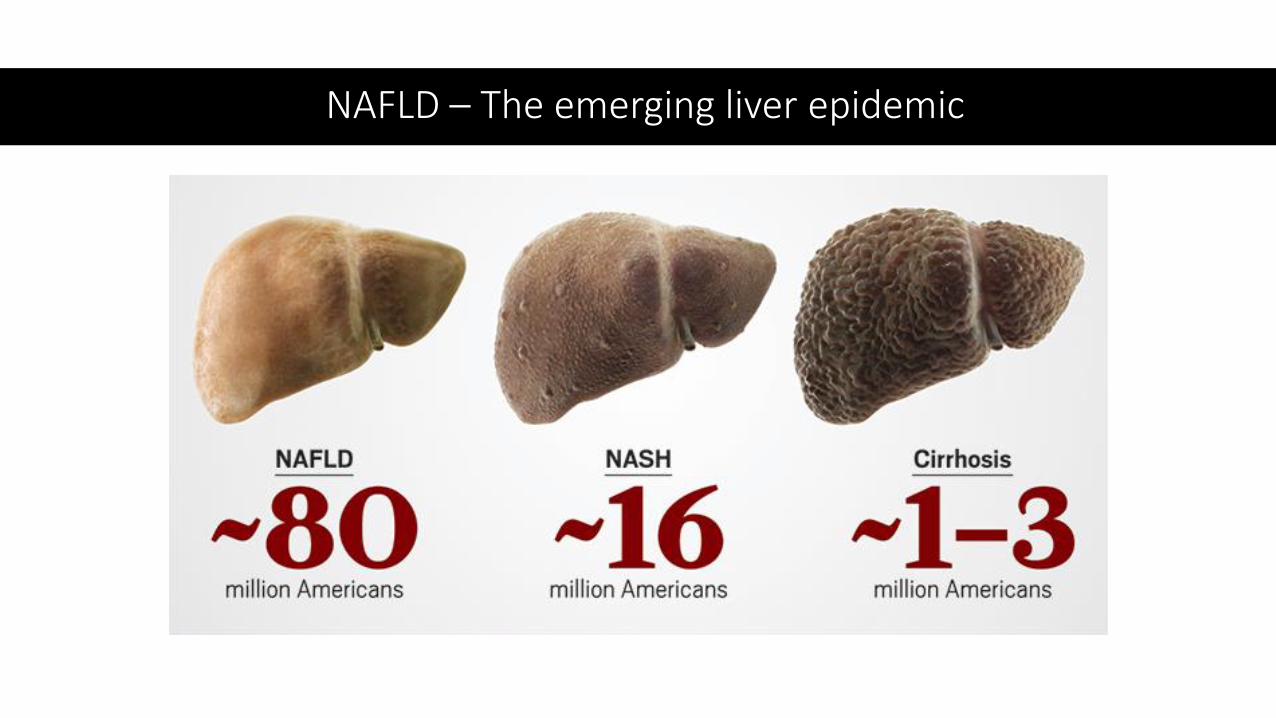
NAFLD – The emerging liver epidemic

Steatosis
(NAFL)
Normal Steatohepatitis
(NASH)
Cirrhosis
NAFLD is a spectrum
Banini & Sanyal Am J Gastroenterol 2017
10-15% normal70-80% obese
2-3% normal15-20% in severely obese(BMI > 35)
<1% normal3-5% obese
**Emerging Terminology
MAFLD: Metabolic-Associated Fatty Liver Disease
BAFLD: Both Alcoholic and Nonalcoholic Fatty Liver Disease

NAFLD – A Diagnosis of Exclusion
• Labs• ALT>AST (usually AST:ALT<1 unless cirrhotic, never>2)• May have GGT elevation, ALP elevation (1/3)• Ferritin often high – (50-62%)
• Exclude ALWAYS: • Viral hepatitis (HBV/HCV)• Hemochromatosis• Drug• Alcohol (<2/day)
• Exclude if relevant:• Autoimmune hepatitis (IgG, ANA, SMA)• Wilsons - (ceruloplasmin, Urine Copper)• Others

Clinical Features
General Features
• Mainly asymptomatic (48-100%)
• Uncommonly:• RUQ discomfort
• Fatigue
• Malaise
Liver Specific
• Hepatomegaly (75%)
• Splenomegaly
(if cirrhosis)
• Uncommonly:• Palmar erythema
• Spider naevi
• Ascites

Epidemiology – General Population Studies
• Ultrasound ~22%• Lean 16%
• Obese 76%
• Liver tests• NHANES III 3-23%
• 11% liver tests >1.5 x ULN
• NAFLD 46% in pop’n study in US!
Farrell, Hepatology 2006, Williams Gastroenterology 2011
NAFLD is the commonest cause of elevated
ALT in N. America

Bril. Endocrinol Metab Clin N Am. 2016;45:765
Simple Fatty Liver vs NASH - It Matters!
Liver relatedCardiovascularOther
40
30
20
10
0
Mo
rtal
ity
(%)
No NAFLD(14.5-yr follow-up)
Nonalcoholic Fatty Liver(13.3-yr follow-up)
NASH(13.0-yr follow-up)
Patients with NASH have a significantly higher liver-related mortality than patients with simple steatosis
Major cause of death in NAFLD is cardiovascular disease

NAFLD stage correlates with hard outcomes
As stage of liver disease (fibrosis from NAFLD) increases, so does all-cause mortality and liver-related events risk
Taylor et al. Gastroenterology. May 2020

But the Challenge:
ALL THE PATIENTS
Patients with NASH
-Demographics-Labs-Special Testing

Separating Simple Steatosis from NASH
Detect Fat
• Fatty Liver Index
• Ultrasound
• CAP
• MRI-PDFF
Detect Inflammation
• Clinical Factors
• Biomarkers
Detect Fibrosis
• Clinical scores
• Elastography
• MultiparametricMRI

Separating Simple Steatosis from NASH
Detect Fat
• Fatty Liver Index
• Ultrasound
• CAP
• MRI-PDFF
Detect Inflammation
• Clinical Factors
• Biomarkers
Detect Fibrosis
• Clinical scores
• Elastography
• MultiparametricMRI
➕

Separating Simple Steatosis from NASH
Detect Fat
• Fatty Liver Index
• Ultrasound
• CAP
• MRI-PDFF
Detect Inflammation
• Clinical Factors
• Biomarkers
Detect Fibrosis
• Clinical scores
• Elastography
• MultiparametricMRI

FIB-4
• Age important factor• Well-validated in NAFLD• >3.25 – likely cirrhosis• <1.45 – very unlikely
advanced fibrosis• 1.45-3.25 – a bit less helpful
Sterling Hepatology 2006
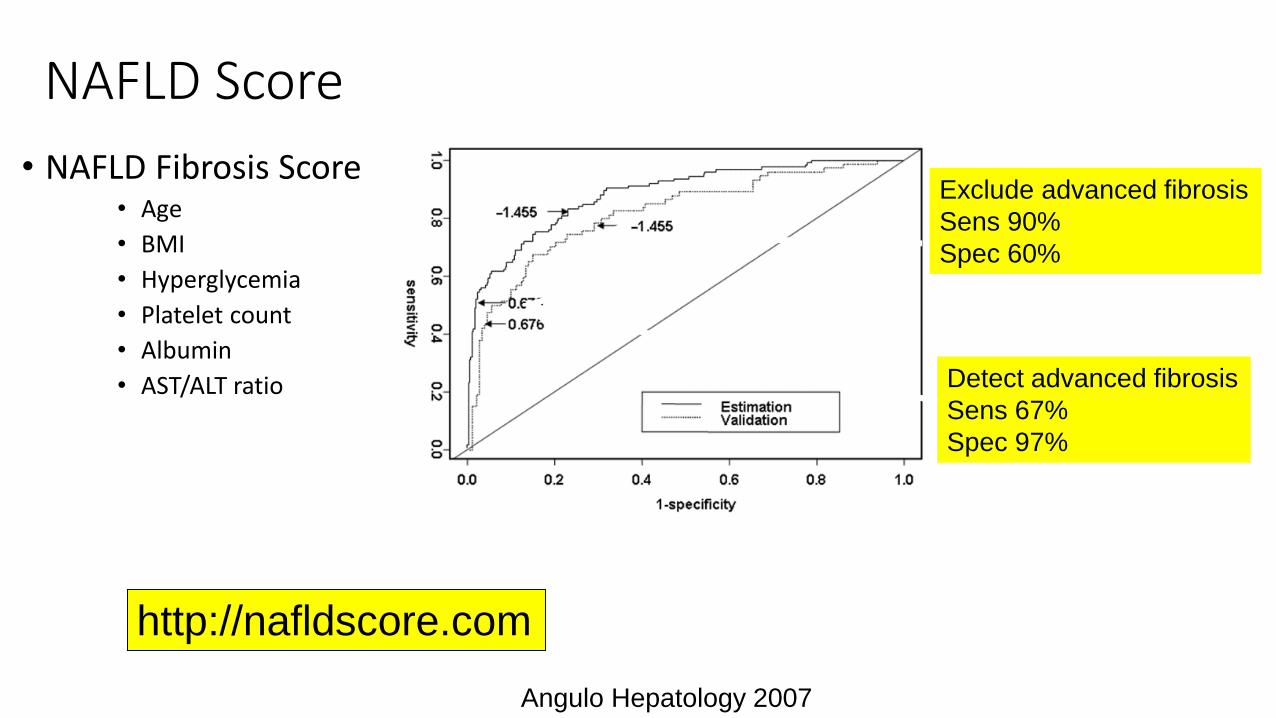
NAFLD Score
• NAFLD Fibrosis Score• Age
• BMI
• Hyperglycemia
• Platelet count
• Albumin
• AST/ALT ratio
http://nafldscore.com
Angulo Hepatology 2007
Exclude advanced fibrosis
Sens 90%
Spec 60%
Detect advanced fibrosis
Sens 67%
Spec 97%

Before Treatment - A Diagnostic Pathway for NAFL
Identify Fatty Liver (imaging, etc)
Rule Out Advanced Fibrosis
FIB-4 <1.3NFS <-1.455
Low-Risk: Monitor Annually
FIB-4 >1.3NFS >-1.455
Intermediate to High-Risk
Rule In/Out High Risk (Advanced Fibrosis)
Fibroscan MRE
Low Score: Low Risk (Annual Monitoring)Intermediate Score: BiopsyHigh Score: Liver-focused Treatment/Trials/Biopsy
PRIMARY CARE REFERRAL CENTRE

The Management of NASH

Treatment Targets in NAFLD
Treatments targeted at the Liver- ⬇ Hepatic fat
accumulation- ⬇ Oxidative stress- Anti-fibrotics
Treatments targeted at Metabolic Syndrome

NASH and SDOH
• Even when controlling for co-morbidities…
• NASH is more common in those living below the poverty line
• NASH is more common in those living in high-density areas
• NASH is more common in blacks and hispanics (US data)
Aboubergi et al. Am J Gastro. Oct 2017
Cannot ignore the complex socioeconomic factors and system
structural inequities that contribute to NASH and make it difficult to treat

Treatment of NAFLD
Possible➢Vitamin E➢Anti-Diabetes Meds➢Anti-Cholesterol Meds➢Newer weight loss drugs➢Coffee
Proven➢ Lifestyle, diet and exercise➢Weight loss surgery (if BMI >35)
Unlikely to help➢Older weight loss drugs➢Anti-inflammatories➢Milk thistle, Other herbals
Investigational➢Antifibrotics➢Bile acid pathways

Comprehensivelifestyle approach
Energy restriction• Calorie restriction (500−1,000/day)• 7−10% weight loss target• Long-term maintenance approach
Macronutrient composition• Low-to-moderate fat• Moderate-to-high
carbohydrate• Low-carbohydrate ketogenic
diets or high protein
Fructose intake• Avoid fructose-containing
food and drink
Daily alcohol intake• Strictly below 30 g men
and 20 g women
Coffee consumption• No liver-related limitations
Physical activity• 150−200 min/week moderate intensity
in 3−5 sessions• Resistance training to promote
musculoskeletal fitness and improvemetabolic factors
EASL Guidelines

Which diet is effective?
Romero-Gomez et al. J Hepatol 2017.

Ontario Bariatric Network
Vitamin E – Potential Early Treatment
Consider use of Vitamin E 400IU/d for patients with earlier disease, minimal or controlled cardiac risk factors

• Glucagon-like peptide 1 reduces liver fat, ALT and insulin resistance in mice models
• RCT liraglutide vs. placebo x 48 weeks (LEAN trial)
• Resolution of NASH in 9/23 (39%) liraglutide vs. 2/22 (9%) placebo p=0.019• Secondary outcomes showed improvements in weight
and ALT
• Liraglutide well tolerated
• Being studied in Phase 3 (Semaglutide)
• Recent large GLP-1 trial showed improvements for DM and weight loss
Liraglutide – Opportunity to Synergize DM Therapy
Armstrong et al Lancet 2016

New Treatments of NASH – Many Targets
Konerman MA, et al. J Hepatol 2018

Examples of NASH Treatments in Phase II or III Investigations (as of January 2020)
Steatohepatitis (NASH) CirrhosisNormal Liver Steatosis (NAFL)
Insulin resistance and/or lipid metabolism
Lipotoxicity and oxidative stress
Inflammation and immune activation
Cell death (apoptosis and
necrosis)
Fibrogenesis and collagen turnover
PPARγ: PioglitazoneGLP-1: Liraglutide,
semaglutideSGLT: Empagliflozin,
licogliflozin, canagliflozin
DPP-4 SitagliptinACC: GS-0976, PF-05221304SCD1: AramcholASBT: Volixibat
Some agents have multiple targets
PPARα/∂: ElafibranorPPARα/γ: SaroglitazarPan-PPAR: LanifibranorFGF19: NGM282
FGF21: Pegbelferim
FXR: OCA, cilofexor,tropifexor, nidufexor
MPC: MSDC-0602KTGR-5: INT-767/777THR-β: MGL-3196, VK2809
Slide credit: clinicaloptions.com
CCR2/5: Cenicriviroc (inflammatory target but affects fibrosis)
ASK1: Selonsertib (cell death target but affects fibrosis)Caspase: Emricasan
AOC3: BI-1467335P2X7R: SGM-1019TLR-4: JKB-121/122
Galectin: GR-MD-02LOXL2: Simtuzumab
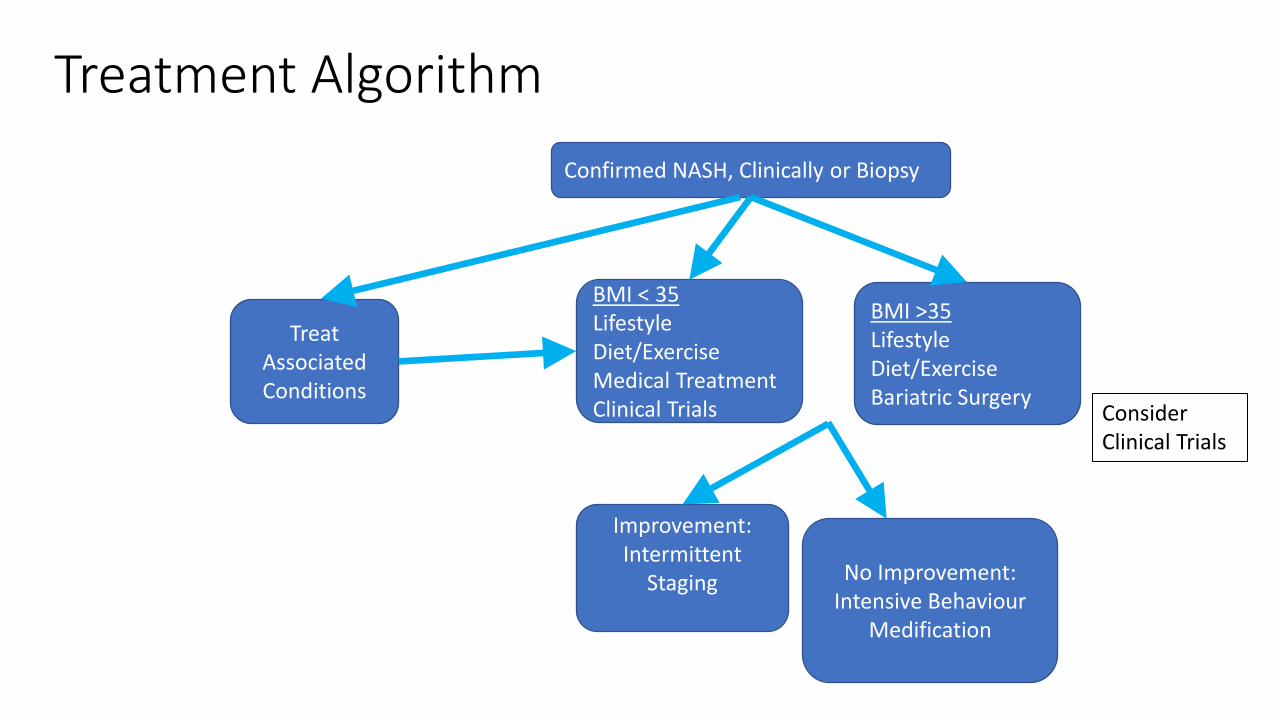
Treatment Algorithm
Confirmed NASH, Clinically or Biopsy
BMI < 35LifestyleDiet/ExerciseMedical TreatmentClinical Trials
Treat Associated Conditions
Improvement:Intermittent
Staging No Improvement: Intensive Behaviour
Medification
BMI >35LifestyleDiet/ExerciseBariatric Surgery
Consider Clinical Trials

Summary
• NAFLD is highly prevalent and intertwined with social factors
• Identifying high-risk patients important
• Look for ways to optimize therapy within the context of patient’s existing health and social situation
• Lots more therapies being studied for NASH. So far, no home runs but there never are for metabolic diseases
• Thank you for your attention!