“diagnosis & treatment planning in paediatric dentistry”
TRANSCRIPT

Lecture 3 Paediatric Dentistry Dr. Israa Ali
1/11/2018 1
“Diagnosis & Treatment Planning
In PaeDiatric Dentistry”
In any clinical dental practice, Provision of dental care for a child patient
represents a challenge. This is initially attributed to the need to take into account
many factors during history taking and clinical examination of these young
patients, in addition to the need to design a realistic treatment plan that could
suit each patient individually.
Ethics and consent:
The fundamental ethical responsibility of any dentist treating a child patient is
to do no harm, to act in the child’s best interest, and to respect the child’s right
to reject treatment. However, the dentist may sometimes need to proceed with a
procedure that the child is not completely satisfied with. This is only viable
when the procedure is in the best interest of the child, when there are no other
alternatives, when delaying the procedure will complicate the treatment, when
failure to provide the procedure will cause pain and distress to the child, and
only when a valid consent is being taken from the parents.
Consent is the permission given by a person or parents (in cases of children
aged less than 16) before receiving any type of medical examination, test or
treatment. It must be done on the basis of an explanation by a clinician and it
could be verbal or written.
Although having a valid consent for examination, investigation and treatment is
important, it is substantial to ensure that the patient and parents understand the
nature and purpose of the proposed procedure, any alternatives available, and
the potential risks and benefits.
It is also important to ensure the relativeness of the adult accompanying the
child and make sure that at least one of the parents knows the proposed
treatment as the childminders, grandparents and teachers may not have the total
authority to consent. However, the dentist could proceed without the parental
presence, only when the child’s life is in danger, or when the condition would
deteriorate irreversibly.

1/11/2018
2
The diagnostic method:
Accurate diagnosis cannot be achieved without gathering and carefully
assessing the information related to the patient’s or parents’ chief concern and
any other dental or oral problems. Therefore, following a systematic approach is
essential in order to reach into a precise diagnosis for all of the patient’s
problems and potential problems. However, there is an exception for this rule. It
is when the patient attends with an emergency problem that needs urgent
intervention, i.e. newly fractured crown or facial swelling of dental origin.
The forthcoming steps are the key points required to reach into as accurate
diagnosis as possible:
History:
With any dental consultation, the first thing that the dentist will do is to take a
history from the patient. This history will include:
1- Personal details:
The dentist should register the patient’s name, age, address, and telephone
number. Knowing the chronological age of the child is very important when
evaluating the child’s dental age, sequence of teeth eruption, eligibility of
primary molars for pulp therapy and other considerations.
2- Presenting complaint(s):
This should include a question about why the child has come to the dental office
or what they are seeking from the dental treatment. It is a good practice to ask
the child this question prior to asking his parents, although the dentist should be
prepared to receive different answers from these two sources.
If the child chief complaint is pain, the history of pain should be recorded
(onset, nature, duration, frequency, exacerbating and relieving factors).
3- Dental history:
For any paediatric dentist, obtaining information regarding the child’s previous
dental treatment is essential in order to design a particular treatment plan that
would fit the patient based on the manner of his/her reaction to the previous
treatments.
Other information could be of particular importance because they may be the

1/11/2018
3
causative factors for the existing oral and dental problems. These involve
information regarding oral hygiene (frequency of brushing and type of
toothpaste used), dietary habits (including between meal snacks and bottle
feeding at bedtime for the younger patients), as well as dummy/digit sucking.
A question about the regularity of previous dental attendance may give the
dentist an indicator for a plan that could fit the parental attitude of their child’s
dental treatment.
4- Social (family) history:
This is an important section in history taking, as the dentist can use it to engage
the child in the conversation. In this section, the dentist can record information
regarding the child’s parents, siblings, and favourite subjects at school to use
them later as ‘ice-breakers’ in the future appointments.
5- Medical history:
Taking a comprehensive medical history should precede any dental treatment.
This is fundamental because general health problems could not only cause oral
problems, but they may also affect the delivery of oral or dental care. Health
problems of most significant impact on oral health involve: allergies, severe
asthma, diabetes, cerebral palsy, cardiac diseases, haematological disorders, and
oncology.
From the medical history, the dentist should obtain information regarding any
previous hospitalisation or operations, allergies, current medications, any
previous or current problems associated with each of the major systems (CVS,
CNS, haematological, respiratory, immunological, endocrine, gastrointestinal,
and skeletal). At the end of medical history taking, it is a good practice to ask
the parents if there is anything else they think the dentist should know about
their child. This is a useful approach in relation to children who have
behavioural or learning problems, such as autism.
Clinical examination:
The first impression:
As soon as the child enters the dental office, his general health and development
could be assessed by noting the overall health, physical and mental
development, in addition to weight and muscle coordination.

1/11/2018
4
Informal evaluation of the child’s probable cooperation is also possible during
history taking. According to Frankl behavioural rating scale, child’s
behaviour at the dental office could be one of the following:
Definitely negative (- -): Refusal of treatment, forceful crying, fearfulness
or any other overt evidence of extreme negativism.
Negative (-): Reluctant to accept treatment, uncooperative, some evidence
of negative attitude but not pronounced (sullen, withdrawn)
Positive (+): Acceptance of treatment; cautious behaviour at times;
willingness to comply with the dentist, at times with reservations; but
patient follows the dentist’s directions cooperatively.
Definitely positive (+ +): Good rapport with the dentist, interest in the
dental procedures, laughter and enjoyment.
Extra-oral examination:
It usually involves assessment of the child’s general physical health by
noticing the following:
Height: Is the child very tall or very short for his/her age? If so; the child
should be referred for a paediatrician for further investigations.
Weight: Is the child over or underweight for their age? If so; there might
be a need to assess the underlying cause by referring to the specialist.
Skin: Record any prominent bruising or injuries on exposed parts of the
child’s body.
Hands: Is there any signs of digit-sucking, nail-biting or abnormal nail or
finger morphology.
The extra-oral examination should also involve a brief evaluation for the
child’s head and neck; including the following:
Head: Record if there is any abnormal size, morphology, or facial
asymmetry.
Hair: Write down if the hair is significantly sparse or if there is an
obvious hair lice.
Eyes: Note if there is any visual impairment or abnormality of the sclera.
Ears: Write if there is any abnormal shape or if the child is wearing
hearing aids.

1/11/2018
5
Skin: Register any scars, bruising, lacerations, or pallor. A special
attention should also be paid for any prominent contagious infections
such as impetigo.
Temporomandibular joint: Document any pain, crepitus, deviation or
restricted opening.
Lymph nodes: Palpate any enlarged submandibular or cervical lymph
nodes. Lymphadenopathy in children may not be caused only by infection
of dental origin, but it may also be a result of viral infection.
Lips: Notice if there is any cold sore, swelling, or abnormal colour.
Any positive finding for the above mentioned points should be recorded.
Clinical photography or annotated sketch could be used as an aid for future
reference. Particularly in cases of suspected child physical abuse and with
respect to medico-legal purposes.
Intra-oral examination:
In order to avoid overlooking important anomalies or pathologies intra-orally,
inspecting intra-oral structures should be performed systematically; rather than
focusing only on the clearly prominent carious lesions. Therefore, intra-oral
examination should be started with the soft tissues, then the gingival and
periodontal tissues, followed by charting the teeth and ending with the occlusion
Soft tissues:
It is substantial to carefully examine the tongue, palate, frenum, and cheeks in
order to note any colour changes, ulceration, swelling, or any other pathology.
A chronic dental sinus tract (fistula) can also be noticed on the attached gingiva
mostly buccal to a grossly decayed tooth.
Gingival and periodontal tissues:
In young children, chronic periodontal disease is uncommon. However, plaque-
induced gingival disease may exist in a child with poor oral hygiene. Any
colour changes (redness), swelling, ulceration, spontaneous bleeding, or
gingival recession should be recorded. Furthermore, level of oral cleanliness
should be assessed and registered.

1/11/2018
6
Teeth:
Recording the presence or absence of a tooth only is not sufficient; the dentist
must have a thorough knowledge of the eruption dates of the primary and
permanent teeth as any significant change in the eruption time may alert the
dentist to a potential problem.
A comprehensive dental charting should be carried out. The charting should
include the following features:
Caries: Is it active/arrested, restorable/unrestorable.
Restorations: Are they intact/deficient?
Fissure sealants: Are they intact/deficient?
Tooth surface loss: Record site and extent of erosion/attrition
Trauma: Report site and extent as well as any signs of loss of vitality
Tooth structure: Any localised or generalised enamel
opacities/hypoplasia
Tooth shape/size: Double teeth, conical teeth, micro/macrodontia, talon
cusp, deep cingulum pits.
Tooth number: Any missing/extra-teeth.
Tooth mobility: Is it physiological or pathological?
Tooth eruption: Are there any impaction, infra-occluded primary
molars, or ectopically erupting first permanent molars?
Occlusion:
A comprehensive orthodontic assessment is not needed in each routine
examination of a paediatric patient. However, Tooth alignment and occlusion
should be evaluated briefly in order to intervene when required. It is a good
practice to write down notes for the following:
Severe skeletal abnormalities.
Overjet and overbite.
First molar relationships.
Presence of crowding/spacing.
Deviations/displacements.
1/11/2018
7
Further investigations:
After finishing with history taking and clinical examination; there might be a
need to perform other investigations to assist in the diagnosis. The forthcoming
intra-oral investigations are the ones most commonly used with paediatric
patients:
Sensibility testing: Using ethyl chloride and electric pulp tester. They are
usually used to aid in assessing pulpal status after a trauma.
Trans-illumination: Usually used to visualise interproximal caries,
enamel infractions, or pulpal haemorrhage following a trauma.
Mobility: Used with gentle finger pressure to assess grade of mobility.
Percussion: To detect a tooth with periapical lesion or an ankylosed
tooth (that sounds like a cracked tea-cup).
Periodontal probing: Can be used with specific periodontal diseases.
Saliva tests: If the patient has a xerostomia, there might be a need to
assess salivary flow rate and buffering capacity.
Oral microbial tests: To aid in selecting the antibiotic following
culturing and performing sensitivity for the intra-oral pus sample.
Tooth measurement: It may sometimes be useful for space analysis in
orthodontic assessment.
Oral histology/pathology: Examination of soft and hard tissue
specimens are usually beneficial to reach into a definite diagnosis.
Study models: They are helpful in providing a record for erosion, infra-
occlusion, and orthodontic status.
Photographs: They could be used as a reference for the presenting
problem(s) pre-operatively and to show the final outcome of the treatment
post-operatively.
Radiographs:
Radiographic screening of children’s teeth should not be carried out routinely.
However, there are specific situations in which radiographs could be used to aid
in:
1/11/2018
8
- Caries diagnosis: By using bitewing radiograph to detect interproximal
caries.
- Trauma assessment: Intra-oral and/or extra-oral radiographs could be
used with patients who have had facial or dental trauma.
- Orthodontic treatment planning: Panoramic radiographs are usually
mandatory before starting orthodontic treatment. Other radiographs, e.g.
cephalometric, could also be used.
- Identification of any abnormalities in dental development:
Radiographs are usually needed when there is delayed dental
development, suspected missing/extra-teeth, potential ectopic tooth
position, or first permanent molar of poor prognosis.
- Detection of any bony or dental pathology: periapical radiographs are
usually used to detect localised pathology while panoramic view is useful
in cases where the pathology involves more than one quadrant.
Risk assessment:
Prior to designing a treatment plan, risk assessment of the child patient is an
important task that is needed to be performed. Risk assessment is the evaluation
of the probability of a disease or condition to develop in an individual patient.
This will basically help in directing the required treatment for each patient and
will also aid in determining the optimum recall interval. For the paediatric
patient, risk assessment may involve an assessment for periodontal disease,
erosion, orofacial trauma and most commonly dental caries.
Caries risk assessment:
Caries risk assessment is a fundamental step in the diagnosis process of any
paediatric patient. It will help to predict when the caries will likely to develop in
the caries-free child, to determine the rate of disease progression in patient who
had caries, to propose the most appropriate preventive strategy, and to
determine the frequency of radiographic investigation for caries diagnosis and
recall visits. However, it is important to remember that caries risk status is not
static and may change due to any change in personal circumstances, and
therefore, will need to reassess it at subsequent visits.
1/11/2018
9
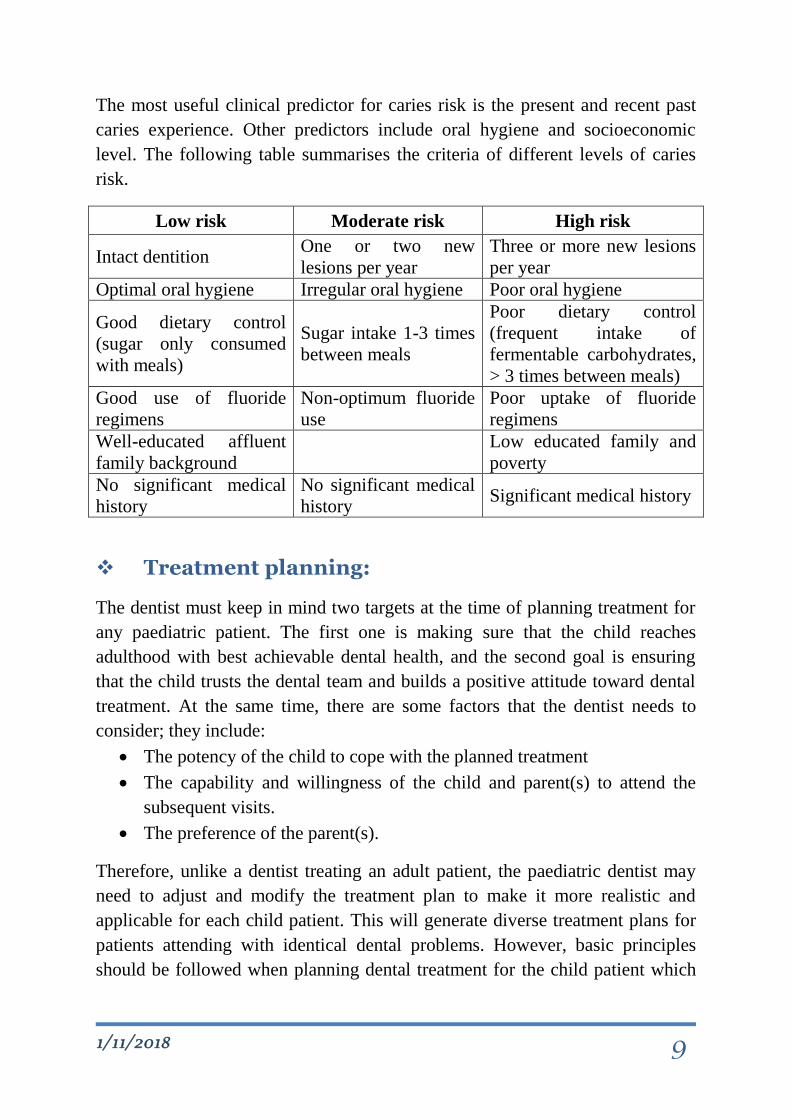
The most useful clinical predictor for caries risk is the present and recent past
caries experience. Other predictors include oral hygiene and socioeconomic
level. The following table summarises the criteria of different levels of caries
risk.
Low risk Moderate risk High risk
Intact dentition One or two new
lesions per year
Three or more new lesions
per year
Optimal oral hygiene Irregular oral hygiene Poor oral hygiene
Good dietary control
(sugar only consumed
with meals)
Sugar intake 1-3 times
between meals
Poor dietary control
(frequent intake of
fermentable carbohydrates,
> 3 times between meals)
Good use of fluoride
regimens
Non-optimum fluoride
use
Poor uptake of fluoride
regimens
Well-educated affluent
family background
Low educated family and
poverty
No significant medical
history
No significant medical
history Significant medical history
Treatment planning:
The dentist must keep in mind two targets at the time of planning treatment for
any paediatric patient. The first one is making sure that the child reaches
adulthood with best achievable dental health, and the second goal is ensuring
that the child trusts the dental team and builds a positive attitude toward dental
treatment. At the same time, there are some factors that the dentist needs to
consider; they include:
The potency of the child to cope with the planned treatment
The capability and willingness of the child and parent(s) to attend the
subsequent visits.
The preference of the parent(s).
Therefore, unlike a dentist treating an adult patient, the paediatric dentist may
need to adjust and modify the treatment plan to make it more realistic and
applicable for each child patient. This will generate diverse treatment plans for
patients attending with identical dental problems. However, basic principles
should be followed when planning dental treatment for the child patient which

1/11/2018
10
are summarized in the following figure:
Recall according to risk assessment
DiscussionParent Patient
Definitive treatmentRestoration/ extraction Prevention Aesthetic consideration
DiscussionParent Patient
Assessment of patient cooperation
Initial treatmentAcclimitazation Preventive advice Stabilizaztion
Assessment of patient cooperation
Management of acute dental problems
DiscussionParent Patient Medical/ dental specialist
History and examinationAssessment of treatment needs Vs Likely patient/ parent cooperation

1/11/2018
11
The essential aspects that are usually present in the treatment plan include:
Management of acute dental problems:
If the child attends his first dental visit with acute dental pain, relieving this pain
should be a primacy. However, any treatment provided should not endanger the
accomplishment of the future planned treatment. This may demand avoidance
of extraction in most of such cases.
Prevention:
Providing preventive measures (involving dietary advice, oral hygiene
instructions and fluoride application) for the child patient at the beginning and
during dental treatment will aid in:
- Acclimatizing the child for future treatment.
- Building confidence of the child.
- Avoiding failure of restorations as a result of continuously active caries
process. Repeated restorations will have deleterious effects on the child’s
ability to cooperate and on the dentist-parent relationship.
- Avoiding multiple extractions in the future
- Ensuring that the child maintain dental health in the future.
Stabilization:
This phase is sometimes offered prior to the provision of definitive treatment
where the child has open cavities. Stabilization may involve restoration with or
without extraction of the grossly decayed teeth. The advantages of
implementing this phase are to:
- Help the child to acclimatize for treatment.
- Allow provision of preventive advice.
- Aid in assessing the child’s potency for the more complicated subsequent
treatment.
- Minimize the overall bacterial load.
- Slow down caries progression.
- Reduce the possibility of the child attending with pain and sepsis.
The restorations performed at this stage will not involve complete removal of
1/11/2018
12
caries and will not need the use of local anaesthetic. Caries could be removed
only to allow placement of temporary dressing. Therefore, it is substantial to
explain to the parents that what is provided is not permanent
Operative treatment:
When planning operative dental care for the paediatric patient, the following
should be considered:
- Small simple restorations should be performed first.
- Upper teeth should be restored prior to the lower ones as it is easier to
give local anaesthesia for the maxillary teeth.
- Posterior teeth should be treated before the anterior ones in order to
ensure that the patient returns for treatment.
- Except for very young children, it is preferable to perform quadrant
dentistry wherever possible.
- Perform endodontic treatment after finishing the simple restorations.
- Unless the patient attends with acute dental problem at earlier stage,
extraction should be carried out as the last item of operative care
Recall (follow-up):
Accomplishing the treatment plan for the child patient does not finish by the
end of the treatment journey. A scheduled recall is essential for the child patient
because caries progression can be faster in children and primary teeth than in
adults and permanent teeth. The recall interval may be scheduled on 3, 6, 9, or
12 months basis depending on the disease risk assessment of the child.
On the recall visits, the dentist will be able to reassess child’s needs and caries
risk, deliver and reinforce preventive advice. It would be beneficial to arrange
the recall visits with the periodic evaluation of orofacial growth and developing
occlusion (usually around the age of 6, 9 and 12 years).
References: 1. Cameron, A. C & Widmer, R. P. 2013. Handbook of Paediatric Dentistry. 4th
edition. Edinburgh: Mosby Elsevier.
2- Welbury, R. et al. 2012. Paediatric Dentistry. 4th edition. Oxford: Oxford
University Press.
3. Dean, JA. et al. 2015. McDonals and Avery’s Dentistry for the child and
adolescent. 10th edition. Missouri: Elsevier.