diabetic neuropathy: new developments in early diagnosis ... · pdf fileprevalence of...
TRANSCRIPT

Institute for Clinical Diabetology
German Diabetes Center at the Heinrich Heine University
Leibniz Center for Diabetes Research
Department of Endocrinology and Diabetology
University Hospital, Düsseldorf, Germany
Diabetic Neuropathy: New Developments
in Early Diagnosis and Treatment
Dan Ziegler, MD, FRCPE

painful painless
?
Prevalence: ≈30%
Diabetic sensorimotorpolyneuropathy (DSPN)

PROTECT Study: Percentages of previously undiagnosed neuropathyin participants with distal sensory polyneuropathy (DSPN)
D S P N S ch m erz h af t e D S P N * S ch m erz lo se D S P N *
0
1 0
2 0
3 0
4 0
5 0
6 0
7 0
8 0
9 0
1 0 0
% (
95
%C
I)
Painful
DSPN
Painless
DSPN
Total
DSPN
■ No DM (n=167)
■ Type 1 DM (n=24)
■ Type 2 DM (n=242)
■ All (n=433)
Educational initiative “Diabetes! Do you listen to your feet?”
Shopping centers and diabetes/health care fairs in Germany (n=1,589)
Ziegler et al., EASD, 2016

Curr Diab Rep 2012;12: 376-383

Prevalence of polyneuropathy, neuropathic pain, and cardiacautonomic dysfunction in prediabetes and diabetes
Ziegler et al., Diabetes Care 2008; 31: 556-561
Ziegler et al., Pain Med 2009; 10: 393-400
Ziegler et al., Eur J Pain 2009; 13: 582-587
Bongaerts et al., Diabetes Care 2012; 35: 1891-1893
Ziegler et al., Diabetologia 2015; 58: 1118-1128
Survey Measure NGT
(%)
IFG
(%)
IGT
(%)
IFG+IGT
(%)
New DM
(%)
Known DM
(%)
S2+S3 MNSI>2 7.4 11.3 13.0 28.0
F4 VPT/MF bilat. 11.1 5.5 14.8 23.9 16.1 22.0
S2+S3 MNSI>2+pain 1.2 4.2 8.7 13.3
AMIR MNSI>2+pain 3.7 5.7 14.8 21.0
S4 Reduced HRV 4.5 8.1 5.9 11.4 11.7 17.5
NGT = normal glucose tolerance
IFG = isolated impaired fasting glucose
IGT = isolated impaired glucose tolerance
New DM = newly detected diabetes mellitus
Known DM = known diabetes mellitus
MNSI = Michigan Neuropathy Screening Instrument
VPT = vibration perception threshold
MF = monofilament
HRV = heart rate variability
AMIR = Augsburg Myocardial Infarction Registry
5 min

How to diagnose diabetic neuropathy?
Motor Sensory Autonomic
Myelinated Myelinated Thinlymyelinated
Un-myelinated
Thinlymyelinated
Un-myelinated
A A/ A C A C
Large
Motor,sensory
NCV
Touch,Vibration, Position
perception
Warm perc. Pain
IENFDCCM
HRV, AFTs, BRSSudomotor,
GIT, GUT function
Small
Modified after Vinik
Coldperception
Pain

Ziegler et al., Diabetes 2014; Diabetologia 2015
Control Type 2 DM
German Diabetes Study: Reduced epidermal nerve fiber density
and enhanced antioxidative defense in recent-onset type 2 DM
Intraepidermal nerve fiber density
PGP9.5
Control
Mean diabetes
duration: 1 year
0.16
Type 2 DM (n=69)
0.26
Increase in superoxide dismutase (SOD)2 area
Control (n=51)
Green: SOD2
Blue: nucleus
Control Type 2 DM

In vivo laser scanning
corneal confocal
microscopy (CCM)

Corneal Confocal Microscopy (CCM)
Diabetic neuropathyHealthy subject
Ziegler et al., Diabetes, 2014; 63: 2454-2463

CCM in recently diagnosed Type 2 diabetic patients
Ziegler et al., Diabetes, 2014; 63: 2454-2463

Key Messages I
Prevalence of neuropathy is increasedin prediabetes, particularly in combinedIFG-IGT.
An array of abnormalities in nerve functionand morphology are detected in conjunctionwith oxidative stress and inflammation asearly as in recent-onset DM.

Glycemiccontrol
Lifestyle/multi-factorial riskintervention
Analgesics
Pathogenetic
treatment
Treatment
of Diabetic
Neuropathy

DCCT/EDIC: Reduced incidence of DPN following previousintensive vs standard insulin therapy in type 1 diabetic
patients at year 13-14 („metabolic memory“)
Albers et al., Diabetes Care, 2010
0
5
10
15
20
25
30
35
40Intensive
Standard
DCCTBaseline
DCCTEnd
EDICYear 13-14
% w
ith
DP
N **p<0.05
*

+ = benefit; = no effect; #higher mortality on IT.
ST = standard therapy; IT = intensive therapy
NCV = nerve conduction velocity; VPT = vibration perception threshold
Trial
n Duration
(years)
HbA1c(%)
ST vs IT
DSPN endpoints
Clinical NCV VPT
UKPDS 3,867 up to 15 7.9 vs 7.0 ? ? ?
Kumamoto 110 up to 10 9.4 vs 7.1 ? ? ?
VADT 1,791 5.6 8.4 vs 6.9 ? ? ?
ADVANCE 11,140 5 7.3 vs 6.5 ? ? ?
ACCORD 10,251 3.7 / 1.3 7.6 vs 6.3#/7.2 ? ? ?
HOME 390 4.3 7.9 vs 7.5 ? ? ?
BARI 2D 2,159 4 7.6 vs 7.1 (IP/IS) ? ? ?
ADDITION 1,161 6 6.4 vs 6.3 ? ? ?
Steno Type 2 160 8 / 5 9.0 vs 7.7 ? ? ?
Effects of intensive diabetes therapy on
development/progression of DSPN in type 2 DM

+ = benefit; = no effect; #higher mortality on IT.
ST = standard therapy; IT = intensive therapy
NCV = nerve conduction velocity; VPT = vibration perception threshold
Trial
n Duration
(years)
HbA1c(%)
ST vs IT
DSPN endpoints
Clinical NCV VPT
UKPDS 3,867 up to 15 7.9 vs 7.0 +
Kumamoto 110 up to 10 9.4 vs 7.1 +
VADT 1,791 5.6 8.4 vs 6.9
ADVANCE 11,140 5 7.3 vs 6.5
ACCORD 10,251 3.7 / 1.3 7.6 vs 6.3#/7.2 +
HOME 390 4.3 7.9 vs 7.5
BARI 2D 2,159 4 7.6 vs 7.1 (IP/IS) +
ADDITION 1,161 6 6.4 vs 6.3
Steno Type 2 160 8 / 5 9.0 vs 7.7
Effects of intensive diabetes therapy on
development/progression of DSPN in type 2 DM

Gibbons & Freeman, Brain, 2015; 138: 43-52
HbA1c ↓ 4–7% (n=52)HbA1c ↓ 2–3.9% (n=27) HbA1c ↓ >7% (n=25)
Treatment-induced neuropathy of diabetes (TIND)
All patients with pain
Many patients with pain

Treatment-induced neuropathy of diabetes (TIND)
HbA1c ↓ 2–3% points over 3 months: 20% risk of TIND
HbA1c ↓ >4% points over 3 months: >80% risk of TIND
Risk of developing TIND
TIND was present in 10.9% of all individuals seen in a
tertiary referral diabetic neuropathy clinic over a 5-year period
Gibbons & Freeman, Brain, 2015; 138: 43-52

X
Hyperglycemia-induced micro- and macrovascular
endothelial cell damage
Glucose
ROS
Insulin resistance
Insulin
Ox-FFA-k
PARP
FFA-k
Polyol pathway
AGE pathway
PKC activation
Hexosamine pathway
Mitochondrium
Adipocyte
Endothelial cell
Brownlee M. Diabetes 2005;54:1615–1625.
GAPDH
1
2
3
4
5
Glucose toxicity(oxidative stress)
FFA = free fatty acids
PKC = proteinkinase C
PARP = Poly(ADP-Ribose)
polymerase
GAPDH = Glyceraldehyde 3-phosphate
dehydrogenase
α-Lipoic acid
Actovegin
Benfotiamine
Courtesy P. Kempler (modified)

-Lipoic Acid in Diabetic Neuropathy:
Randomized Placebo-Controlled Trials
ALADINALADIN 2ALADIN 3ORPILDEKANSYDNEYSYDNEY 2NATHAN 1NATHAN 2
R(+) S(-)
• Intravenous• Oral

Meta-Analysis of Individual Neuropathic SymptomsRelative Differences between -Lipoic Acid (600 mg/day i.v.) and Placebo after 3 Weeks
Numbness
Paresthesias
Burning
Pain
TSS
GM with 95% CI
n=1258
Favors -lipoic acid; p<0.05
% -10 0 10 20 30 40 50Ziegler et al., Diabetic Med, 2004;21:114-21
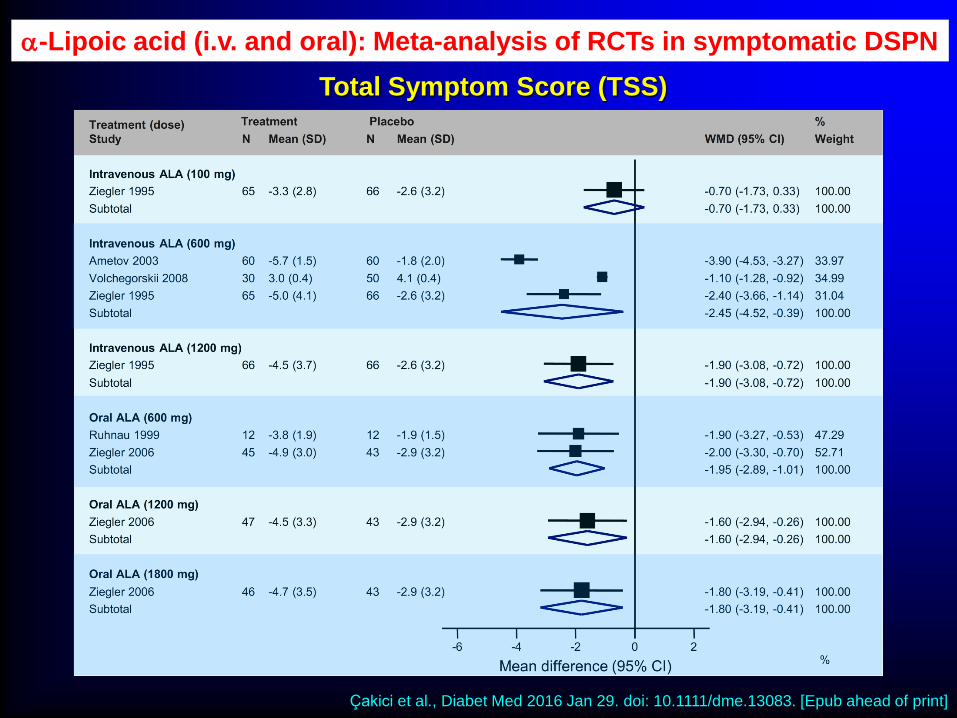
-Lipoic acid (i.v. and oral): Meta-analysis of RCTs in symptomatic DSPN
Çakici et al., Diabet Med 2016 Jan 29. doi: 10.1111/dme.13083. [Epub ahead of print]
Total Symptom Score (TSS)

20
25
30
35
40
45
%
-Lipoic acid (n=219)
Placebo (n=210)
NATHAN 1 Study: NIS-LL Responders vs NIS-LL Progressors
RespondersNIS-LL -2 pts
UnchangedNIS-LL > -2 to < +2
Progressors NIS-LL +2 pts
P=0.025
35.6
29.0
36.2 34.8
40.2
24.2
After4 years:
Ziegler et al., Diabetes Care, 2011; 34: 2054-60
NIS-LL = Neuropathy Impaiment Score- Lower Limbs

NATHAN 1 Trial: Predictors of NIS-LL Improvement
Baseline variables: diabetes-related, DSPN, and analgesic treatment
ATC codes: N02: analgesics, N03: antiepileptics, N06: psychoanaleptics
F Favors placebo Favors α-lipoic acid
Ziegler et al., J Diabetes Complications 2016; 30: 350-6

Measures of treatment effect in
neuropathic pain
Pain relief Mood Functionality
Chronic pain treatementrequires assessment of
Pain intensity Sleep
0 321 4 5 6 7 108 9No pain Intolerable pain
Numeric Analog Scale (NAS = Likert Scale)

Finnerup et al., Lancet Neurol 2015; 14: 162-73
GRADE = Grading of Recommendations Assessment, Development, and Evaluation
Pharmacotherapy of neuropathic pain
GRADE Recommendations (I)

Finnerup et al., Lancet Neurol 2015; 14: 162-73
Pharmacotherapy of neuropathic pain
GRADE Recommendations (II)

Treatment of Painful Diabetic Neuropathy
under Consideration of Comorbidities
Duloxetine(SNRI)
Amitriptyline(TCA)
Pregabalin/Gabapentin
Opioids α-Lipoicacid
Depression + + ↔ ↔ ↔Obesity ↔ ↔ ↔Coronary heart
disease↔ ↔ ↔ ↔
Autonomic
neuropathy? (+) +
Pathogenetic
treatmentNo No No No Yes
+ favorable, unfavorable, ↔ neutral

Holbech et al., Pain. 2015; 156: 958-966
Analgesic combination therapy
in painful neuropathy
●Placebo
▲Pregabalin
300 mg/Tag
Imipramine
75 mg/Tag
Combination
*P<0,05 vs Placebo†P<0,05 vs either
monotherapy
n=50, 22% DM
Cross-over
NRS: Numerical
Rating Scale

Non-pharmacological pain treatment
AcupunctureNerve
stimulationMuscle
stimulation
Psychologicalsupport
TENS

Protective effects of near-normoglycemiaon nerve function are proven in type 1 but not in type 2 diabetes.
Key Messages II
Antioxidant treatment with -lipoic acid for up to 4 years is safe and improves neuropathic symptoms and signs.
Since analgesic monotherapy of neuropathicpain is effective in 50% of the patients,drug combinations are often required.

German Diabetes Center (DDZ)
Leibniz Center for Diabetes Research
Eυχαριστώ πολύ!