diabetes mellitus overview. definition disease of abnormal carbohydrate metabolism characterized by...
TRANSCRIPT
Diabetes Mellitus OverviewDiabetes Mellitus Overview
DefinitionDefinition
Disease of abnormal carbohydrate Disease of abnormal carbohydrate metabolism characterized by metabolism characterized by hyperglycemia hyperglycemia
Caused by:Caused by:– Impairment in insulin secretion and/orImpairment in insulin secretion and/or– Peripheral resistance to insulinPeripheral resistance to insulin
??????
True or FalseTrue or False
Diabetes insipidus is the opposite of Diabetes insipidus is the opposite of diabetes mellitus, in other words, a diabetes mellitus, in other words, a problem of low blood sugar. problem of low blood sugar.
FalseFalse
Diabetes insipidusDiabetes insipidus– Disorder involving the secretion or response Disorder involving the secretion or response
to ADH (antidiuretic hormone)to ADH (antidiuretic hormone)– Causes high-volume urine output and Causes high-volume urine output and
hypernatremiahypernatremia– Not a glucose problemNot a glucose problem
Diabetes MellitusDiabetes Mellitus
Over 7% of U.S. populationOver 7% of U.S. population
14% of health care expenditures14% of health care expenditures
132 billion dollars (2002)132 billion dollars (2002)
Associated with:Associated with:– Higher psychiatric illnessHigher psychiatric illness– Decreased work productivityDecreased work productivity– Increased absenteeismIncreased absenteeism
Diabetes MellitusDiabetes Mellitus
Type 1: destruction of pancreatic beta Type 1: destruction of pancreatic beta cells leading to insulin deficiency (10%)cells leading to insulin deficiency (10%)
Type 2: insulin resistance with varying Type 2: insulin resistance with varying degrees of insulin deficiency (80%)degrees of insulin deficiency (80%)
Gestational: insulin resistance created by Gestational: insulin resistance created by anti-insulin hormones secreted by anti-insulin hormones secreted by placenta during pregnancyplacenta during pregnancy
Other causes: drugs, infectionsOther causes: drugs, infections
Type 1 DMType 1 DM
Autoimmune destruction of insulin-Autoimmune destruction of insulin-producing cells in pancreasproducing cells in pancreas– Islet cell autoantibodiesIslet cell autoantibodies– Glutamic acid decarboxylase antibodiesGlutamic acid decarboxylase antibodies– Anti-insulin antibodiesAnti-insulin antibodies– Associated with other autoimmune diseasesAssociated with other autoimmune diseases
Genetically susceptibleGenetically susceptible
Triggered by environmental agentTriggered by environmental agent
??????
Diabetes mellitus damages:Diabetes mellitus damages:
A.A. EyesEyes
B.B. KidneyKidney
C.C. NervesNerves
D.D. HeartHeart
E.E. BrainBrain
ComplicationsComplications
MicrovascularMicrovascular– NephropathyNephropathy– NeuropathyNeuropathy– RetinopathyRetinopathy
MacrovascularMacrovascular– Coronary artery diseaseCoronary artery disease– Peripheral vascular diseasePeripheral vascular disease– StrokeStroke
Diabetic nephropathyDiabetic nephropathy
Microalbuminuria > Macroalbuminuria > Microalbuminuria > Macroalbuminuria > Elevated creatinine > End stage renal Elevated creatinine > End stage renal disease > Dialysisdisease > Dialysis
AsymptomaticAsymptomatic
Diabetic neuropathyDiabetic neuropathy
18% have evidence of nerve damage at 18% have evidence of nerve damage at diagnosisdiagnosis
Usually symmetrical, affecting lower Usually symmetrical, affecting lower extremities firstextremities first
Stocking-glove syndromeStocking-glove syndrome
Impaired sensation (pain, light touch, Impaired sensation (pain, light touch, temperature, vibration, proprioception)temperature, vibration, proprioception)
Can feel numb or painfulCan feel numb or painful
Diabetic neuropathyDiabetic neuropathy
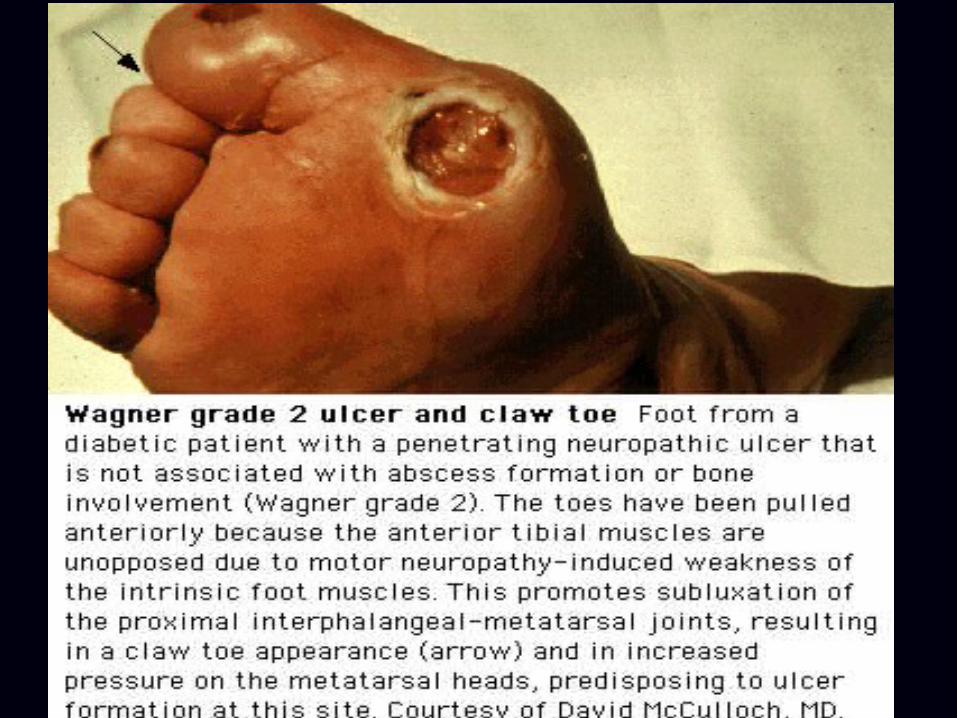
Major risk factor for foot ulcersMajor risk factor for foot ulcers
Autonomic neuropathyAutonomic neuropathy– Postural hypotensionPostural hypotension– GastroparesisGastroparesis– Enteropathy (constipation/diarrhea)Enteropathy (constipation/diarrhea)
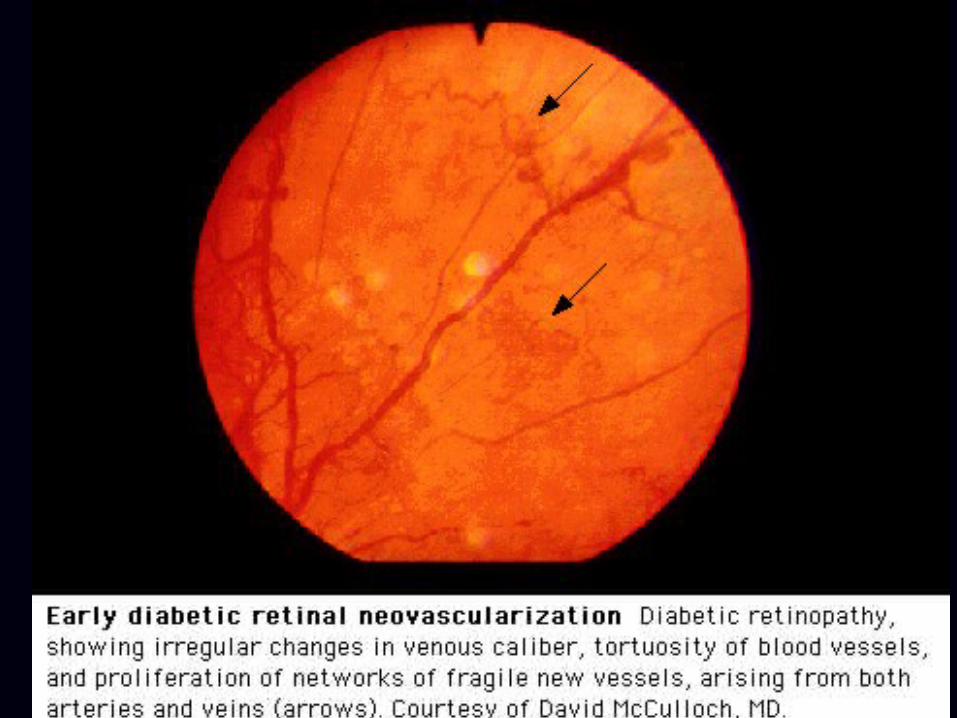
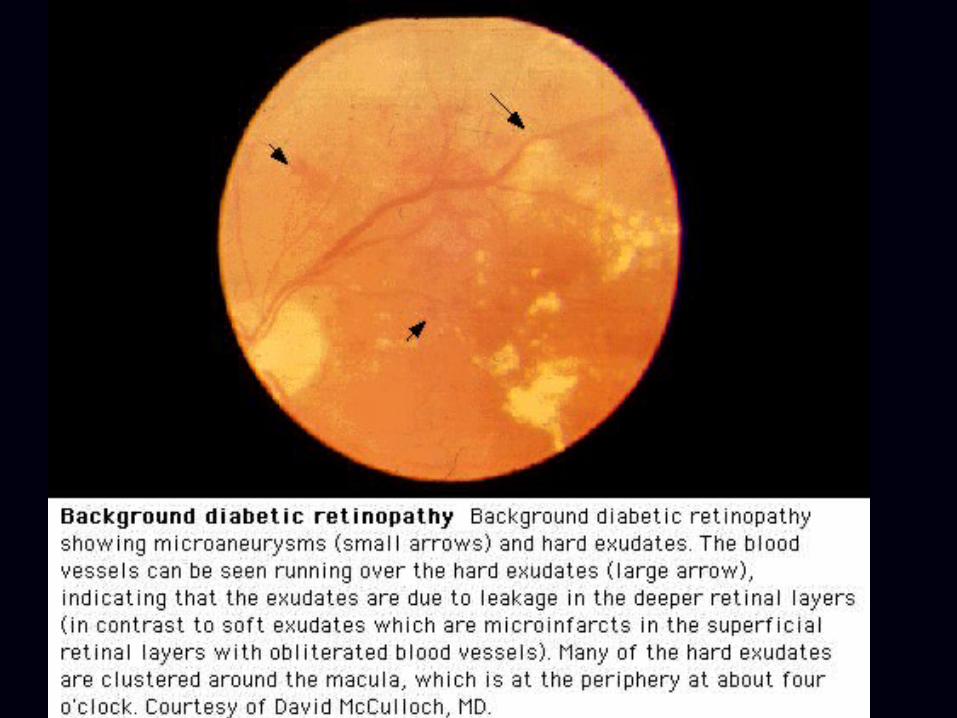
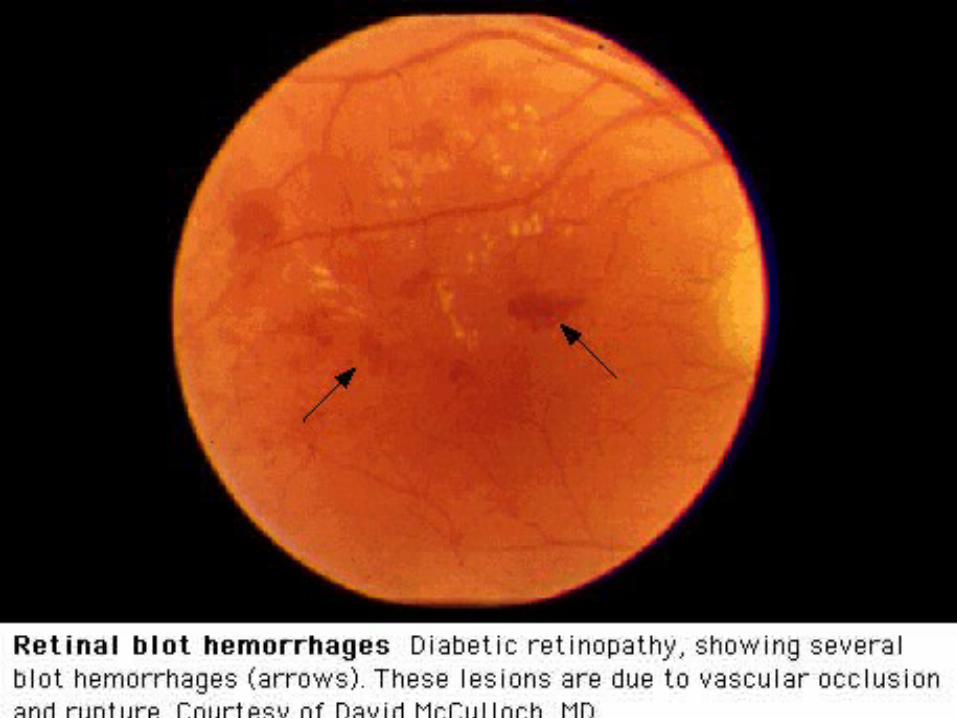
Diabetic retinopathyDiabetic retinopathy
Most common cause of blindness in Most common cause of blindness in middle-aged peoplemiddle-aged people
Blindness 25x higher in diabeticsBlindness 25x higher in diabetics
Asymptomatic until late stagesAsymptomatic until late stages
80% of type 2’s have retinopathy at 20y80% of type 2’s have retinopathy at 20y
MechanismsMechanisms– Impaired blood flowImpaired blood flow– Accumulation of sorbitol in retinaAccumulation of sorbitol in retina
Diabetes and the HeartDiabetes and the Heart
Diabetics have:Diabetics have:– Higher rate of heart diseaseHigher rate of heart disease– Greater coronary ischemiaGreater coronary ischemia– Higher chance of MI and silent MIHigher chance of MI and silent MI
CHD risk equivalentCHD risk equivalent– Aggressive LDL goalAggressive LDL goal
??????
Per ADA, DM (type 2) screening should Per ADA, DM (type 2) screening should begin at what age?begin at what age?
A.A. 2525
B.B. 3535
C.C. 4545
ScreeningScreening
Start at age 45; if normal repeat every 3 Start at age 45; if normal repeat every 3 yearsyearsScreen earlier or more frequently if Screen earlier or more frequently if overweight with additional risk factor overweight with additional risk factor – InactiveInactive– Family history (1Family history (1stst degree relative) degree relative)– HTNHTN– IFG or IGTIFG or IGT– Vascular diseaseVascular disease
DiagnosisDiagnosisAmerican Diabetes AssociationAmerican Diabetes Association
Fasting plasma glucoseFasting plasma glucose
Random glucose with symptomsRandom glucose with symptoms
Oral glucose tolerance testOral glucose tolerance test
Should be confirmed with repeat testing on Should be confirmed with repeat testing on different daydifferent day
DiagnosisDiagnosis
Fasting plasma glucoseFasting plasma glucose
Fasting = no caloric intake for 8 hoursFasting = no caloric intake for 8 hours
Greater than or equal to Greater than or equal to 126126 mg/dl mg/dl
DiagnosisDiagnosis
Random glucose with symptomsRandom glucose with symptoms
Glucose greater than or equal to Glucose greater than or equal to 200200 mg/dl at any timemg/dl at any time
Classic symptoms: polydipsia, polyuria, Classic symptoms: polydipsia, polyuria, weight lossweight loss
DiagnosisDiagnosis
Oral glucose tolerance testOral glucose tolerance test
Glucose greater than or equal to Glucose greater than or equal to 200200 mg/dl two hours after 75g glucose loadmg/dl two hours after 75g glucose load
TreatmentTreatment
Nonpharmacologic (lifestyle)Nonpharmacologic (lifestyle)– Proper dietProper diet– ExerciseExercise– Weight lossWeight loss
Benefits greater to type 2’sBenefits greater to type 2’s
Drug treatmentDrug treatment
InsulinInsulin
- Initial treatment in type 1’s- Initial treatment in type 1’s
- In type 2’s, more commonly used after oral - In type 2’s, more commonly used after oral agents failagents fail
Multiple daily injectionsMultiple daily injections– Lantus + HumalogLantus + Humalog
Continuous infusionContinuous infusion
Adjustments based on HgbA1c and daily Adjustments based on HgbA1c and daily glucose checksglucose checks
Drug treatmentDrug treatment
MetforminMetformin
SulfonylureasSulfonylureas
MeglitinidesMeglitinides
ThiazolidinedionesThiazolidinediones
Alpha-glucosidase inhibitorsAlpha-glucosidase inhibitors
MetforminMetformin
Decreases liver glucose productionDecreases liver glucose production
Improves insulin sensitivityImproves insulin sensitivity
Modest weight reductionModest weight reduction
Avoid in renal insufficiencyAvoid in renal insufficiency
Avoid before IV contrast load or surgical Avoid before IV contrast load or surgical procedure (lactic acidosis)procedure (lactic acidosis)
Start 500mg once daily with dinnerStart 500mg once daily with dinner
??????
Metformin should be held ___ hours Metformin should be held ___ hours before IV contrast studies.before IV contrast studies.
A.A. 88
B.B. 2424
C.C. 4848
D.D. 9696
SulfonylureasSulfonylureas
Increase insulin releaseIncrease insulin release
Oldest class of oral agentOldest class of oral agent
Higher rate of hypoglycemic complicationsHigher rate of hypoglycemic complications
Starting dosesStarting doses– Glipizide 5mg dailyGlipizide 5mg daily– Glyburide 2.5 to 5mg dailyGlyburide 2.5 to 5mg daily– Glimeperide 1 to 2 mg dailyGlimeperide 1 to 2 mg daily
MeglitinidesMeglitinides
Increase insulin releaseIncrease insulin release
Short-acting, expensiveShort-acting, expensive
Taken with mealsTaken with meals
Starlix, PrandinStarlix, Prandin
ThiazolidinedionesThiazolidinediones
Increases insulin sensitivityIncreases insulin sensitivity
Less effective than metformin and Less effective than metformin and sulfonylureas as monotherapysulfonylureas as monotherapy
Causes weight gain, fluid retentionCauses weight gain, fluid retention
Avoid in heart failureAvoid in heart failure
Alpha-glucosidase inhibitorsAlpha-glucosidase inhibitors
Modifies intestinal absorption of Modifies intestinal absorption of carbohydratecarbohydrate
Less potent than oral agents (0.5-1% A1c Less potent than oral agents (0.5-1% A1c reduction)reduction)
Main side effects: gas, diarrheaMain side effects: gas, diarrhea
Take with mealsTake with meals
Persistent hyperglycemiaPersistent hyperglycemia
Combination therapy (type 2’s)Combination therapy (type 2’s)– 2 or 3 drugs together2 or 3 drugs together– 2 orals then add insulin if needed2 orals then add insulin if needed– No need for sulfonylurea and insulin togetherNo need for sulfonylurea and insulin together
Exenatide (Byetta)Exenatide (Byetta)– Twice daily subcutaneous injectionTwice daily subcutaneous injection– Promotes weight lossPromotes weight loss– GI side effectsGI side effects– Overweight patient gaining weight on oralsOverweight patient gaining weight on orals
??????
True or FalseTrue or False
Insulin can be inhaled.Insulin can be inhaled.

Persistent hyperglycemiaPersistent hyperglycemia
Inhaled insulinInhaled insulin– Rapid, similar to lispro insulinRapid, similar to lispro insulin– Taken with mealsTaken with meals– Excludes patients with respiratory disordersExcludes patients with respiratory disorders– Long-term effects on lungs not definedLong-term effects on lungs not defined
Long-term careLong-term care
HgbA1c (goal < 7%)HgbA1c (goal < 7%)
7% = 150 (1% change = 30)7% = 150 (1% change = 30)
Glucose targets (frequency 2-4x day)Glucose targets (frequency 2-4x day)– Preprandial (90 to 130)Preprandial (90 to 130)– Postprandial (<180)Postprandial (<180)
Long-term careLong-term care
Routine eye examsRoutine eye exams– Dilated and comprehensive exam shortly after Dilated and comprehensive exam shortly after
diagnosisdiagnosis– Annual exams thereafterAnnual exams thereafter– Ophthalmologist or optometrist recommendedOphthalmologist or optometrist recommended
Long-term careLong-term care
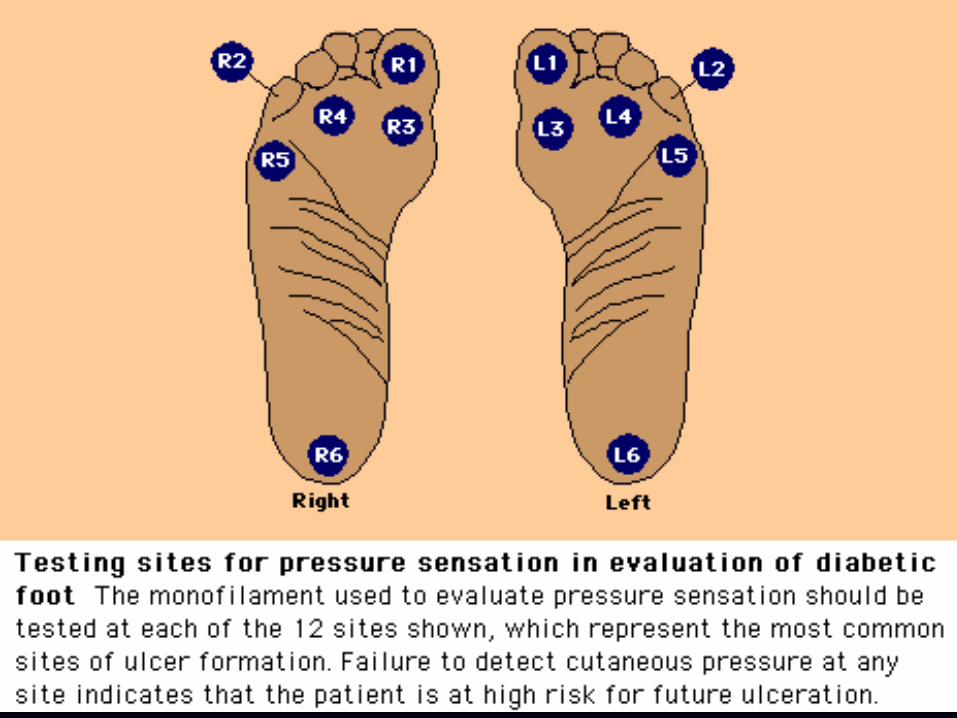
Routine foot examsRoutine foot exams– Detect or monitor vascular/neurologic Detect or monitor vascular/neurologic
complicationscomplications– Visual inspection of feet at each routine visitVisual inspection of feet at each routine visit– Comprehensive exam yearlyComprehensive exam yearly
PulsesPulses
Monofilament testMonofilament test
Long-term careLong-term care
Screen or treat microalbuminuriaScreen or treat microalbuminuria– Dipstick is insensitiveDipstick is insensitive– Spot urine collection measuring albumin to Spot urine collection measuring albumin to
creatinine ratiocreatinine ratio > 30mg/g abnormal> 30mg/g abnormal
ACE-inhibitor or ARB prevents ACE-inhibitor or ARB prevents progression of nephropathyprogression of nephropathy
Long-term careLong-term care
Aggressively treat cardiac risk factorsAggressively treat cardiac risk factors– SmokingSmoking– Hypertension (< 130/80)Hypertension (< 130/80)– Dyslipidemia (LDL < 100)Dyslipidemia (LDL < 100)
Aspirin (81mg) for 1Aspirin (81mg) for 1° CHD prevention for ° CHD prevention for anyone with one risk factoranyone with one risk factor
Acute complicationsAcute complications
Diabetic ketoacidosisDiabetic ketoacidosis– Metabolic acidosis is main concernMetabolic acidosis is main concern
Nonketotic hyperglycemiaNonketotic hyperglycemia– Glucose often > 1000Glucose often > 1000– Neurologic abnormalities frequentNeurologic abnormalities frequent
Precipitating factors: MI, pancreatitis, trauma, Precipitating factors: MI, pancreatitis, trauma, any stress to bodyany stress to bodyTreatment requires IV insulin, hydration, Treatment requires IV insulin, hydration, electrolyte replacementelectrolyte replacement
Questions?