diabetes mellitus james w. mold, m.d., m.p.h. ou-hsc department of family and preventive medicine
TRANSCRIPT

Diabetes Mellitus
James W. Mold, M.D., M.P.H.OU-HSCDepartment of Family and Preventive Medicine
Objective
Attendees should be able to: Construct a rational management
plan for an older patient with type 2 DM, taking into account life expectancy, risks for adverse events, and patient goals, preferences, and resources

Format
Lecture (30 minutes) Small group case-discussions (30
minutes) Presentations of case discussions in
large group (30 minutes)

Type 2 Diabetes Mellitus
Insulin resistance plus beta cell failure Insulin resistance (metabolic syndrome)
usually precedes beta cell failure by 10-20 years
Connection between the two is still unclearBeta cell fatigue? Genetically linked?
Inflammation? DM diagnosed when beta cell function
insufficient to control blood glucose levelsFirst manifestation is postprandial hyperglycemia

Insulin Resistance/Metabolic Syndrome
Insulin resistance Hypertension Lipid abnormalities Endovascular inflammation Hypercoagulability
Doubles the risk of:Macrovascular events (MI, CVA)

Metabolic SyndromeNCEP ATP III Criteria (3 or more criteria)
NCEP ATP III. JAMA. 2001;285:2486–2497.
Criteria Defining LevelWaist circumference
Men >40 inchesWomen >35 inches
Triglycerides >150 mg/dL
HDL CholesterolMen <40 mg/dLWomen <50 mg/dL
Blood Pressure >130/>85 mm Hg
Fasting Glucose >110 mg/dL

Metabolic Syndrome: Prevalence by ATP III Criteria — NHANES III Population
Overall 22% for age 20 and older
0
5
10
15
20
25
30
35
40
45
30-39 40-49 50-59 60-69 70
Men
Women
Age (yr)
Pre
vale
nce
(%
)
Adapted from: Ford ES et al. JAMA. 2002;287:356–359.

Why Worry About Insulin Resistance
Twice the risk of MI, CVA, PAD Eight times the risk of development of
type 2 DM Substantially reduced life expectancy
(by approximately 8 years)*
*Franco et al. Arch Intern Med 2007;167:1145-1151

Beta Cell Failure
Hyperglycemia increases risk for: Microvascular disease (retinopathy,
nephropathy) Neuropathy Infection
Some small additional risk for: Macro-vascular disease/events
Hypercoagulability Endothelial cell dysfunction

UKDPS: Benefits of Glycemic Control vs BP Control With ACEIs or -Blockers
UKPDS Group. BMJ. 1998;317:703–713. Lancet. 1998;352:837–853.
-9
+7
-12-8
-56
-44
-21
-32
0
20
-20
-40
-60
Rel
ativ
e R
isk
Red
uct
ion
%
Heart Failure Stroke MI Diabetic Death
Glycemic ControlACEI or BB

Early Detection/Screening
USPSTF: Screen all adults with hypertension or hyperlipidemia for type 2 diabetes mellitus.
Prevention
In at risk patients: The onset of beta cell failure (diabetes) can
be delayed or prevented with exercise, diet, metformin, glitazones, acarbose, an ACEI or an ARB. Exercise and diet are much more efficacious
than medications.
However, The cost effectiveness of delaying the onset
of diabetes has not yet been established.

American Geriatrics Society Offer individualized therapy that
considers Life expectancy Cognitive impairment Patient preferences Functional status Social support
Keep therapy as simple and inexpensive as possible

Goals
Things you would want to make happen for which it makes very little sense to ask, “so that….?”
Examples:A longer life, the ability to communicate
through writing, the ability to make decisions for myself.

Goals of Health Care
Prevent premature death and disability (QALE) Increase life expectancy (LOL) Reduce the risk of disabling complications
(future QOL)
Improve or maintain current quality of life (QOL) Maximize ability to function in ways that
make life worth living

Clinical Decision-making
Strategies in individual cases should depend upon:
1. Outcomes of importance to the patient Desire to continue to try to stay alive Ability to participate in valued life activities
2. Estimated impact of interventions on those outcomes
3. Ability and willingness of the patient to adhere to the interventions

DM and Length of Life
75% of Type 2 diabetics die of cardiovascular events (MI, CVA)
2-4 times more likely to have cardiovascular events
Risk of MI is as high for type 2 diabetics with no prior MI as for non-diabetics with a prior MI
When they have an MI, diabetics are significantly more likely to die or to develop CHF
Lifestyle Modifications
Exercise*** Aerobic: Substantial benefits for both LOL and
QOL Strengthening: Substantial benefits for future
QOL, ??LOL Balance: Reduced falls
Diet Weight reduction: Difficult.** Associated with
better QOL. Be more careful in the elderly. Mediterranean diet: Associated with reduced
macrovascular events. Be careful in the elderly.

Low-Dose Aspirin
Reduced risk of MI; greater in men Reduced risk of CVA; greater in
women
USPSTF recommends low dose aspirin for men 45 to 79 and women 55 to 79

DM and LOL
ACE inhibitor (ramipril): 24% reduction in overall mortality over 4.5 years (16% after controlling for effects of BP reduction)
Overall mortality reduced in patients with HTN and LVH with ARBs. 42% reduced risk of CVA even if little change in BP. ARBs reduce cardiovascular events more than atenolol.
HOPE Study Investigators. Lancet 2000; 355 (9200): 253-259 LIFE Study Investigators. Lancet 2002; 359: 1004-1010

DM and LOL
Possible reasons for benefits of ACEIs: Anti-ischemic
Stimulate endothelial nitric oxide Decrease myocardial O2 consumption
Anti-atherogenic Reduce systemic vascular resistance and
BP ?Reduce cardiac remodeling

RRR and ARR
Base Risk X RRR = Absolute Risk Reduction
If base risk = 10%, and RRR = 50%, then ARR = 5%
If base risk = 50%, and RRR = 50%, then ARR = 25%
Therefore, the actual benefit of risk reduction is often greater in the elderly assuming equal RRR (because base risk is higher).

Effects of DM on QOL
RCT of glipizide XL vs. placebo for 12 weeks
594 patients; mean age 58.5 (range: 30-85) Glipizide XL titrated upward as needed Home glucose monitoring Final mean A1c’s: 7.5% (glipizide) vs. 9.3%
(placebo) Final average fasting BS’s: 126mg/dl
(glipizide) vs. 168 mg/dl (placebo)

Effects of DM on QOL
Global QOL directly related to A1c level
Glipizide group had significantly (p<0.001) less: Weakness; fatigue Urinary frequency; nocturia Thirst; polydipsia Dryness of mouth, eyes, or nose Sweet taste in mouth

Effects of DM on QOL (cont.)
Glipizide group also had significantly (p<0.01) less: Foot cramps; foot pain Sweating Numbness of lips or mouth Blurred or double vision Crabbiness; short-temperedness

Effects of DM on QOL (cont.)
Glipizide group also had (p<0.05) less: Headaches Tiredness, drowsiness Muscle cramps Vertigo (spinning sensation) Lightheadedness when standing up Chest pain with exertion Confusion

Effects of DM on QOL (cont.)
Glipizide group also had fewer: Days absent from work Days spent in bed Days of restricted activity
Testa MA, et al. JAMA 1998; 280 (17): 1490-1496

Micro-vascular Disease
Greater benefit from reduction of A1c from 9 to 8 than from 8 to 7
It takes 8-10 yrs of glycemic control to realize the benefits for micro-vascular disease

ESRD
End Stage Renal Disease (ESRD) by age at diagnosis of DM:
Age at Dx A1c Lifetime Risk_ 55 7.0 0.9% 55 9.0 1.6%
65 7.0 0.3% 65 9.0 0.6%

Blindness
Blindness from DM Retinopathy by age at diagnosis of DM:
Age at Dx A1c Lifetime Risk 55 7.0 0.1% 55 9.0 1.2%
65 7.0 <0.1% 65 9.0 0.5%

Diabetic Peripheral and Autonomic Neuropathies Proposed mechanisms: sorbitol,
myoinosital, ischemia, glycosylation, osmotic
Improved glucose control probably slows progression, but size of effect is unknown
Some evidence of minor benefits from: C-peptide, Vitamin E, other antioxidants, nerve growth factors

Why Not Control Everything? Law of diminishing returns
Less benefit from successive interventions Diminishing ability to correctly adhere to
more complicated regimens Increased side effects and drug
interactions from more meds (exponential increase above 4-5)
Impact of testing and interventions on lifestyle

Math
ARR = RRR (baseline risk)
Most interventions that can reduce risk of heart attack have RRR of about 25%.
If 10-yr base = 20%, then the first intervention results in an ARR of 5%, the second in an ARR of 3.75% (25% of 15%), and so on (diminishing returns)
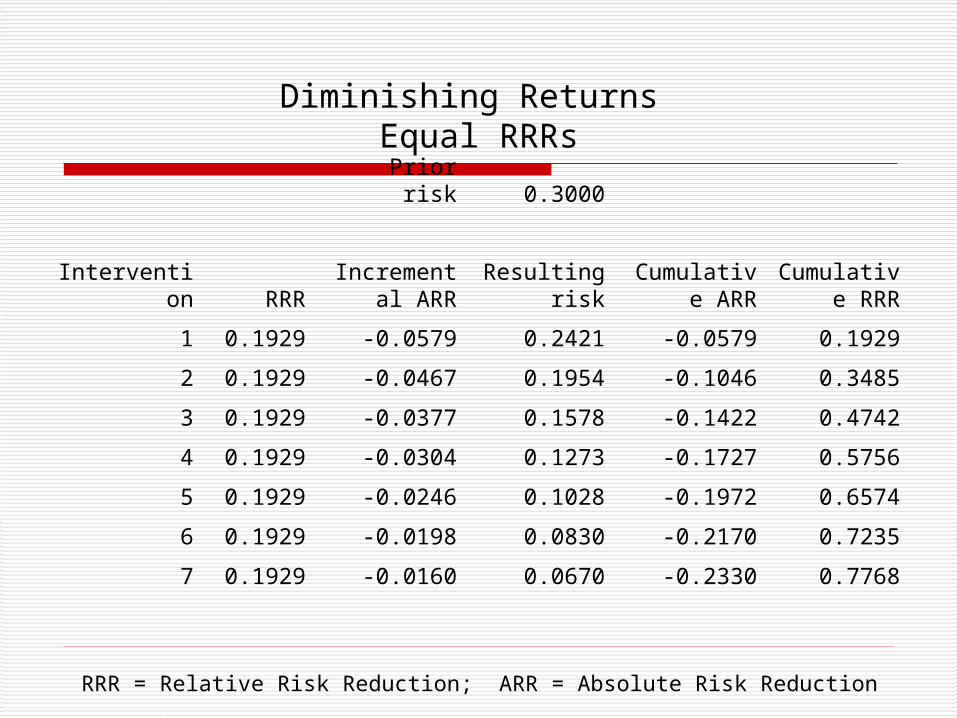
Diminishing Returns Equal RRRs
Prior risk 0.3000
Intervention RRR
Incremental ARR
Resulting risk
Cumulative ARR
Cumulative RRR
1 0.1929 -0.0579 0.2421 -0.0579 0.1929
2 0.1929 -0.0467 0.1954 -0.1046 0.3485
3 0.1929 -0.0377 0.1578 -0.1422 0.4742
4 0.1929 -0.0304 0.1273 -0.1727 0.5756
5 0.1929 -0.0246 0.1028 -0.1972 0.6574
6 0.1929 -0.0198 0.0830 -0.2170 0.7235
7 0.1929 -0.0160 0.0670 -0.2330 0.7768
RRR = Relative Risk Reduction; ARR = Absolute Risk Reduction
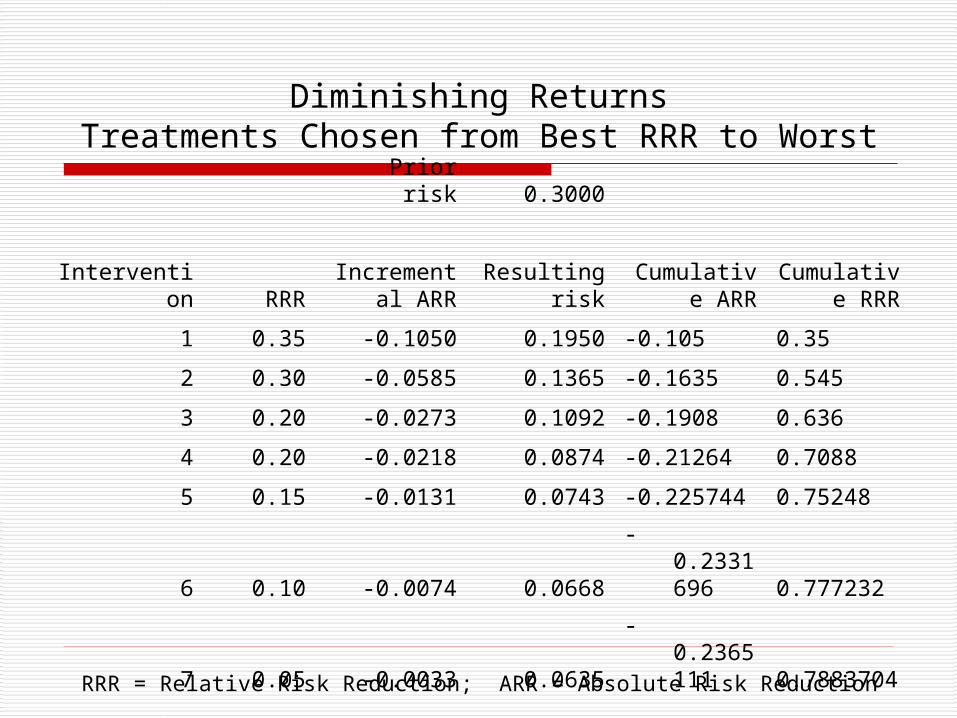
Diminishing ReturnsTreatments Chosen from Best RRR to Worst
Prior risk 0.3000
Intervention RRR
Incremental ARR
Resulting risk
Cumulative ARR
Cumulative RRR
1 0.35 -0.1050 0.1950 -0.105 0.35
2 0.30 -0.0585 0.1365 -0.1635 0.545
3 0.20 -0.0273 0.1092 -0.1908 0.636
4 0.20 -0.0218 0.0874 -0.21264 0.7088
5 0.15 -0.0131 0.0743 -0.225744 0.75248
6 0.10 -0.0074 0.0668 -0.2331696 0.777232
7 0.05 -0.0033 0.0635 -0.2365111 0.7883704
RRR = Relative Risk Reduction; ARR = Absolute Risk Reduction

Problems with Hypoglycemia
Case-control study involving 111 community-dwelling adults >75 years of age Strong correlation between A1c<7 and
increased risk of falls NHLBI-funded ACCORD study, a RCT
with 10,251 participants Intensive treatment group had an excess
number of deaths
SimulationFictitious 79 year-old woman with DM, COPD, HTN,
OA, and osteoporosis.Researchers applied relevant clinical practice
guidelines using a conservative approach and generics.
Required 12 medications $406 per month (pre-Medicare D) Taken at 5 different times per day Multiple potential interactions
Boyd CM, et al. JAMA 2005; 294(6): 716-724.
CaseMr. M is a 65 yo man with type 2 diabetes mellitus
diagnosed a yr. ago. Sedentary lifestyle; no cigarettes or alcohol. Recent onset of fatigue, decreased libido, polyuria and polydipsia, and increasing pain in his joints. He currently takes no medications. Past and family history are unremarkable. His primary care physician finds: body mass index (BMI) of 30.5, BP 200/100 mmHg, osteoarthritis involving fingers and knees, hemoglobin A1c 10%, LDL cholesterol 140 mg/dl, HDL cholesterol 40 mg/dl, total cholesterol 260 mg/dl, ALT and AST slightly elevated, and serum testosterone low.

Diabetes Personal Health Decisions (PHD) Engine
Archimedes program• Attempts to model diabetes by including
>100 biological variables, symptoms, signs, tests, treatments, and outcomes
• Uses differential equations and object-oriented programming to model the links between variables
• Keeps all continuous variables continuous

Diabetes Personal Health Decisions (PHD) Engine
• Addresses co-morbidities and treatments with multiple effects
• Includes not only individual patients, but also aspects of the helath care delivery system (facilities, equipment, policies and procedures, costs, and utilities)
• Data based upon knowledge of pathophysiology, clinical trials, and data from Kaiser Permanente

PHD Validation• Subjected to a series of 74 validation
exercises involving 18 clinical trials, 10 of which were not used in the construction of the engine
• Correlation between results of PHD simulations and clinical trials overall was astounding (r=0.99)
• Correlation between absolute differences in outcomes also amazing (r=0.97)

Mr. Waldman (Diabetes PHD Risk Engine)Life expectancy is about 7 years.7-yr. Risk MI CVA
40% 17%
ARR Sum ARR Sum
Aspirin 11% 2% Moderate Exercise 10% 20% 5% 6%BP to 130 with ACEI 7% 24% 3% 9%Lower LDL to 100 5% 27% 0% 9%Lower A1c to 6.5% 1% 28% 0% 9%Reduce BMI to 26 9% 31% 3%
11%www.diabetes.org

Objective
Attendees should be able to: Construct a rational management
plan for an older patient with DM, taking into account goals and preferences, life expectancy, abilities, and resources