diabetes medical care 2010
TRANSCRIPT

Standards of Medical Care in Diabetes—2010AMERICAN DIABETES ASSOCIATION
D iabetes is a chronic illness that re-quires continuing medical care andongoing patient self-management
education and support to prevent acutecomplications and to reduce the risk oflong-term complications. Diabetes care iscomplex and requires that many issues,beyond glycemic control, be addressed. Alarge body of evidence exists that sup-ports a range of interventions to improvediabetes outcomes.
These standards of care are intendedto provide clinicians, patients, research-ers, payors, and other interested individ-uals with the components of diabetescare, general treatment goals, and tools toevaluate the quality of care. While indi-vidual preferences, comorbidities, andother patient factors may require modifi-cation of goals, targets that are desirablefor most patients with diabetes are pro-vided. These standards are not intendedto preclude clinical judgment or more ex-tensive evaluation and management of thepatient by other specialists as needed. For
more detailed information about manage-ment of diabetes, refer to references 1–3.
The recommendations included arescreening, diagnostic, and therapeutic ac-tions that are known or believed to favor-ably affect health outcomes of patientswith diabetes. A grading system (Table 1),developed by the American Diabetes As-sociation (ADA) and modeled after exist-ing methods, was used to clarify andcodify the evidence that forms the basisfor the recommendations. The level of ev-idence that supports each recommenda-tion is listed after each recommendationusing the letters A, B, C, or E.
These standards of care are revisedannually by the ADA multidisciplinaryProfessional Practice Committee, andnew evidence is incorporated. Membersof the Professional Practice Committeeand their disclosed conflicts of interest arelisted in the Introduction. Subsequently,as with all position statements, the stan-dards of care are reviewed and approved
by the Executive Committee of ADA’sBoard of Directors.
I. CLASSIFICATION ANDDIAGNOSIS
A. ClassificationThe classification of diabetes includesfour clinical classes:
● type 1 diabetes (results from �-cell de-struction, usually leading to absoluteinsulin deficiency)
● type 2 diabetes (results from a progres-sive insulin secretory defect on thebackground of insulin resistance)
● other specific types of diabetes due toother causes, e.g., genetic defects in�-cell function, genetic defects in insu-lin action, diseases of the exocrine pan-creas (such as cystic fibrosis), and drug-or chemical-induced diabetes (such asin the treatment of AIDS or after organtransplantation)
● gestational diabetes mellitus (GDM)(diabetes diagnosed during pregnancy)
Some patients cannot be clearly classifiedas having type 1 or type 2 diabetes. Clin-ical presentation and disease progressionvary considerably in both types of diabe-tes. Occasionally, patients who otherwisehave type 2 diabetes may present with ke-toacidosis. Similarly, patients with type 1diabetes may have a late onset and slow(but relentless) progression despite hav-ing features of autoimmune disease. Suchdifficulties in diagnosis may occur in chil-dren, adolescents, and adults. The truediagnosis may become more obvious overtime.
B. Diagnosis of diabetes
RecommendationsFor decades, the diagnosis of diabetes hasbeen based on plasma glucose (PG) crite-ria, either fasting PG (FPG) or 2-h 75-goral glucose tolerance test (OGTT) values.In 1997, the first Expert Committee onthe Diagnosis and Classification of Diabe-tes Mellitus revised the diagnostic criteriausing the observed association between
● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ●
Originally approved 1988. Most recent review/revision October 2009.DOI: 10.2337/dc10-S011Abbreviations: ABI, ankle-brachial index; ACCORD, Action to Control Cardiovascular Risk in Diabetes;
ADAG, A1C-Derived Average Glucose Trial; ADVANCE, Action in Diabetes and Vascular Disease: Pre-terax and Diamicron Modified Release Controlled Evaluation; ACE, angiotensin converting enzyme; ARB,angiotensin receptor blocker; ACT-NOW, ACTos Now Study for the Prevention of Diabetes; BMI, bodymass index; CBG, capillary blood glucose; CFRD, cystic fibrosis–related diabetes; CGM, continuousglucose monitoring; CHD, coronary heart disease; CHF, congestive heart failure; CCM, chronic caremodel; CKD, chronic kidney disease; CMS, Centers for Medicare and Medicaid Services; CSII, continuoussubcutaneous insulin infusion; CVD, cardiovascular disease; DASH, Dietary Approaches to Stop Hyper-tension; DCCT, Diabetes Control and Complications Trial; DKA, diabetic ketoacidosis; DMMP, diabetesmedical management plan; DPN, distal symmetric polyneuropathy; DPP, Diabetes Prevention Program;DPS, Diabetes Prevention Study; DREAM, Diabetes Reduction Assessment with Ramipril and Rosiglita-zone Medication; DRS, Diabetic Retinopathy Study; DSME, diabetes self-management education; DSMT,diabetes self-management training; eAG, estimated average glucose; eGFR, estimated glomerular filtrationrate; ECG, electrocardiogram; EDIC, Epidemiology of Diabetes Interventions and Complications; ERP,education recognition program; ESRD, end-stage renal disease; ETDRS, Early Treatment Diabetic Reti-nopathy Study; FDA, Food and Drug Administration; FPG, fasting plasma glucose; GDM, gestationaldiabetes mellitus; GFR, glomerular filtration rate; HAPO, Hyperglycemia and Adverse Pregnancy Out-comes; ICU, intensive care unit; IFG, impaired fasting glucose; IGT, impaired glucose tolerance; LookAHEAD, Action for Health in Diabetes; MDRD, Modification of Diet in Renal Disease; MNT, medicalnutrition therapy; NDEP, National Diabetes Education Program; NGSP, National Glycohemoglobin Stan-dardization Program; NPDR, nonproliferative diabetic retinopathy; OGTT, oral glucose tolerance test;PAD, peripheral arterial disease; PCOS, polycystic ovarian syndrome; PDR, proliferative diabetic retinop-athy; PPG, postprandial plasma glucose; RAS, renin-angiotensin system; SMBG, self-monitoring of bloodglucose; STOP-NIDDM, Study to Prevent Non-Insulin Dependent Diabetes; SSI, sliding scale insulin;TZD, thiazolidinedione; UKPDS, U.K. Prospective Diabetes Study; VADT, Veterans Affairs Diabetes Trial;XENDOS, XENical in the prevention of Diabetes in Obese Subjects.
© 2010 by the American Diabetes Association. Readers may use this article as long as the work is properlycited, the use is educational and not for profit, and the work is not altered. See http://creativecommons.org/licenses/by-nc-nd/3.0/ for details.
P O S I T I O N S T A T E M E N T
care.diabetesjournals.org DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 S11

glucose levels and presence of retinopa-thy as the key factor with which to iden-tify threshold FPG and 2-h PG levels. Thecommittee examined data from threecross-sectional epidemiologic studies thatassessed retinopathy with fundus photog-raphy or direct ophthalmoscopy andmeasured glycemia as FPG, 2-h PG, andHbA1c (A1C). The studies demonstratedglycemic levels below which there was lit-tle prevalent retinopathy and abovewhich the prevalence of retinopathy in-creased in an apparently linear fashion.The deciles of FPG, 2-h PG, and A1C atwhich retinopathy began to increase werethe same for each measure within eachpopulation. The analyses helped to in-form a then-new diagnostic cut point of�126 mg/dl (7.0 mmol/l) for FPG andconfirmed the long-standing diagnostic2-h PG value of �200 mg/dl (11.1mmol/l) (4).
ADA has not previously recom-mended the use of A1C for diagnosingdiabetes, in part due to lack of standard-ization of the assay. However, A1C assaysare now highly standardized, and their re-sults can be uniformly applied both tem-porally and across populations. In arecent report (5), after an extensive reviewof both established and emerging epide-miological evidence, an international ex-pert committee recommended the use of
the A1C test to diagnose diabetes with athreshold of �6.5%, and ADA affirms thisdecision (6). The diagnostic test shouldbe performed using a method certified bythe National Glycohemoglobin Standard-ization Program (NGSP) and standard-ized or traceable to the Diabetes Controland Complications Trial (DCCT) refer-ence assay. Point-of-care A1C assays arenot sufficiently accurate at this time to usefor diagnostic purposes.
Epidemiologic datasets show a rela-tionship between A1C and the risk of ret-inopathy similar to that which has beenshown for corresponding FPG and 2-h PGthresholds. The A1C has several advan-tages to the FPG, including greater conve-nience, since fasting is not required;evidence to suggest greater preanalyticalstability; and less day-to-day perturba-tions during periods of stress and illness.These advantages must be balanced bygreater cost, limited availability of A1Ctesting in certain regions of the develop-ing world, and incomplete correlation be-tween A1C and average glucose in certainindividuals. In addition, the A1C can bemisleading in patients with certain formsof anemia and hemoglobinopathies. Forpatients with a hemoglobinopathy butnormal red cell turnover, such as sicklecell trait, an A1C assay without interfer-ence from abnormal hemoglobins should
be used (an updated list of A1C assays andwhether abnormal hemoglobins impactthem is available at www.ngsp.org/prog/index3.html). For conditions with abnor-mal red cell turnover, such as pregnancy oranemias from hemolysis and iron defi-ciency, the diagnosis of diabetes must useglucose criteria exclusively.
The established glucose criteria forthe diagnosis of diabetes (FPG and 2-hPG) remain valid. Patients with severe hy-perglycemia such as those who presentwith severe classic hyperglycemic symp-toms or hyperglycemic crisis can continueto be diagnosed when a random (or ca-sual) PG of �200 mg/dl (11.1 mmol/l) isfound. It is likely that in such cases thehealth care professional would also con-duct an A1C test as part of the initial as-sessment of the severity of the diabetesand that it would be above the diagnosticcut point. However, in rapidly evolvingdiabetes such as the development of type1 in some children, the A1C may not besignificantly elevated despite frankdiabetes.
Just as there is �100% concordancebetween the FPG and 2-h PG tests, thereis not perfect concordance between A1Cand either glucose-based test. Analyses ofNational Health and Nutrition Examina-tion Survey (NHANES) data indicate that,assuming universal screening of the undi-agnosed, the A1C cut point of �6.5%identifies one-third fewer cases of undiag-nosed diabetes than a fasting glucose cutpoint of �126 mg/dl (7.0 mmol/l) (E.Gregg, personal communication). How-ever, in practice, a large portion of thediabetic population remains unaware oftheir condition. Thus, the lower sensitiv-ity of A1C at the designated cut point maywell be offset by the test’s greater practi-cality, and wider application of a moreconvenient test (A1C) may actually in-crease the number of diagnoses made.
As with most diagnostic tests, a testresult diagnostic of diabetes should be re-peated to rule out laboratory error, unlessthe diagnosis is clear on clinical grounds,such as a patient with classic symptoms ofhyperglycemia or hyperglycemic crisis. Itis preferable that the same test be repeatedfor confirmation, since there will be agreater likelihood of concurrence in thiscase. For example, if the A1C is 7.0% anda repeat result is 6.8%, the diagnosis ofdiabetes is confirmed. However, there arescenarios in which results of two differenttests (e.g., FPG and A1C) are available forthe same patient. In this situation, if thetwo different tests are both above the di-
Table 1 —ADA evidence grading system for clinical practice recommendations
Level ofevidence Description
A Clear evidence from well-conducted, generalizable, randomized controlled trials thatare adequately powered, including:● Evidence from a well-conducted multicenter trial● Evidence from a meta-analysis that incorporated quality ratings in the analysis
Compelling nonexperimental evidence, i.e., �all or none� rule developed by Centerfor Evidence Based Medicine at Oxford
Supportive evidence from well-conducted randomized controlled trials that areadequately powered, including:● Evidence from a well-conducted trial at one or more institutions● Evidence from a meta-analysis that incorporated quality ratings in the analysis
B Supportive evidence from well-conducted cohort studies:● Evidence from a well-conducted prospective cohort study or registry● Evidence from a well-conducted meta-analysis of cohort studies
Supportive evidence from a well-conducted case-control studyC Supportive evidence from poorly controlled or uncontrolled studies
● Evidence from randomized clinical trials with one or more major or three ormore minor methodological flaws that could invalidate the results
● Evidence from observational studies with high potential for bias (such as caseseries with comparison to historical controls)
● Evidence from case series or case reportsConflicting evidence with the weight of evidence supporting the recommendation
E Expert consensus or clinical experience
Standards of Medical Care
S12 DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 care.diabetesjournals.org

agnostic threshold, the diagnosis of dia-betes is confirmed.
On the other hand, if two differenttests are available in an individual and theresults are discordant, the test whose re-sult is above the diagnostic cut pointshould be repeated, and the diagnosis ismade on the basis of the confirmed test.That is, if a patient meets the diabetes cri-terion of the A1C (two results �6.5%) butnot the FPG (�126 mg/dl or 7.0 mmol/l),or vice versa, that person should be con-sidered to have diabetes. Admittedly, inmost circumstance the “nondiabetic” testis likely to be in a range very close to thethreshold that defines diabetes.
Since there is preanalytic and analyticvariability of all the tests, it is also possiblethat when a test whose result was abovethe diagnostic threshold is repeated, thesecond value will be below the diagnosticcut point. This is least likely for A1C,somewhat more likely for FPG, and mostlikely for the 2-h PG. Barring a laboratoryerror, such patients are likely to have testresults near the margins of the thresholdfor a diagnosis. The healthcare profes-sional might opt to follow the patientclosely and repeat the testing in 3– 6months.
The current diagnostic criteria for di-abetes are summarized in Table 2.
C. Categories of increased risk fordiabetesIn 1997 and 2003, The Expert Committeeon the Diagnosis and Classification of Di-abetes Mellitus (4,7) recognized an inter-mediate group of individuals whoseglucose levels, although not meeting cri-teria for diabetes, are nevertheless toohigh to be considered normal. This groupwas defined as having impaired fastingglucose (IFG) (FPG levels of 100 mg/dl[5.6 mmol/l] to 125 mg/dl [6.9 mmol/l])
or impaired glucose tolerance (IGT) (2-hOGTT values of 140 mg/dl [7.8 mmol/l]to 199 mg/dl [11.0 mmol/l]).
Individuals with IFG and/or IGT havebeen referred to as having pre-diabetes,indicating the relatively high risk for thefuture development of diabetes. IFG andIGT should not be viewed as clinical en-tities in their own right but rather riskfactors for diabetes as well as cardiovas-cular disease (CVD). IFG and IGT areassociated with obesity (especiallyabdominal or visceral obesity), dyslipide-mia with high triglycerides and/or lowHDL cholesterol, and hypertension.Structured lifestyle intervention, aimed atincreasing physical activity and produc-ing 5–10% loss of body weight, and cer-tain pharmacological agents have beendemonstrated to prevent or delay the de-velopment of diabetes in people with IGT(see Table 7). It should be noted that the2003 ADA Expert Committee report re-duced the lower FPG cut point to defineIFG from 110 mg/dl (6.1 mmol/l) to 100mg/dl (5.6 mmol/l), in part to make theprevalence of IFG more similar to that ofIGT. However, the World Health Organi-zation (WHO) and many other diabetesorganizations did not adopt this change.
As the A1C becomes increasinglyused to diagnose diabetes in individualswith risk factors, it will also identify thoseat high risk for developing diabetes in thefuture. As was the case with the glucosemeasures, defining a lower limit of an in-termediate category of A1C is somewhatarbitrary, since risk of diabetes with anymeasure or surrogate of glycemia is a con-tinuum extending well into the normalranges. To maximize equity and efficiencyof preventive interventions, such an A1Ccut point, should balance the costs of falsenegatives (failing to identify those who aregoing to develop diabetes) against the
costs of false positives (falsely identifyingand then spending intervention resourceson those who were not going to developdiabetes anyway).
Linear regression analyses of nation-ally representative U.S. data (NHANES2005–2006) indicate that among thenondiabetic adult population, an FPG of110 mg/dl corresponds to an A1C of5.6%, while an FPG of 100 mg/dl corre-sponds to an A1C of 5.4%. Receiver op-erating curve analyses of these dataindicate that an A1C value of 5.7%, com-pared with other cut points, has the bestcombination of sensitivity (39%) andspecificity (91%) to identify cases of IFG(FPG �100 mg/dl [5.6 mmol/l]) (R.T.Ackerman, Personal Communication).Other analyses suggest that an A1C of5.7% is associated with diabetes risk sim-ilar to that of the high-risk participants inthe Diabetes Prevention Program (DPP)(R.T. Ackerman, personal communica-tion). Hence, it is reasonable to consideran A1C range of 5.7–6.4% as identifyingindividuals with high risk for future dia-betes and to whom the term pre-diabetesmay be applied (6).
As is the case for individuals found tohave IFG and IGT, individuals with anA1C of 5.7–6.4% should be informed oftheir increased risk for diabetes as wellas CVD and counseled about effectivestrategies to lower their risks (see IV. PRE-VENTION/DELAY OF TYPE 2 DIABETES).As with glucose measurements, the contin-uum of risk is curvilinear, so that as A1Crises, the risk of diabetes rises dispropor-tionately. Accordingly, interventionsshould be most intensive and follow-upshould be particularly vigilant for thosewith an A1C �6.0%, who should be con-sidered to be at very high risk. However,just as an individual with a fasting glucose of98 mg/dl (5.4 mmol/l) may not be at negli-gible risk for diabetes, individuals with anA1C �5.7% may still be at risk, dependingon the level of A1C and presence of otherrisk factors, such as obesity and familyhistory.
Table 2—Criteria for the diagnosis of diabetes
1. A1C �6.5%. The test should be performed in a laboratory using a methodthat is NGSP certified and standardized to the DCCT assay.*
OR2. FPG �126 mg/dl (7.0 mmol/l). Fasting is defined as no caloric intake for at
least 8 h.*OR
3. Two-hour plasma glucose �200 mg/dl (11.1 mmol/l) during an OGTT.The test should be performed as described by the World HealthOrganization, using a glucose load containing the equivalent of 75 ganhydrous glucose dissolved in water.*
OR4. In a patient with classic symptoms of hyperglycemia or hyperglycemic
crisis, a random plasma glucose �200 mg/dl (11.1 mmol/l).
*In the absence of unequivocal hyperglycemia, criteria 1–3 should be confirmed by repeat testing.
Table 3—Categories of increased risk fordiabetes*
FPG 100–125 mg/dl (5.6–6.9 mmol/l)�IFG�
2-h PG on the 75-g OGTT 140–199 mg/dl(7.8–11.0 mmol/l) �IGT�
A1C 5.7–6.4%
*For all three tests, risk is continuous, extendingbelow the lower limit of the range and becomingdisproportionately greater at higher ends of therange.
Position Statement
care.diabetesjournals.org DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 S13

Table 3 summarizes the categories ofincreased risk for diabetes.
II. TESTING FOR DIABETESIN ASYMPTOMATICPATIENTS
Recommendations● Testing to detect type 2 diabetes and
assess risk for future diabetes in asymp-tomatic people should be considered inadults of any age who are overweight orobese (BMI �25 kg/m2) and who haveone or more additional risk factors fordiabetes (Table 4). In those withoutthese risk factors, testing should beginat age 45 years. (B)
● If tests are normal, repeat testing shouldbe carried out at least at 3-year inter-vals. (E)
● To test for diabetes or to assess risk offuture diabetes, either A1C, FPG , or2-h 75-g OGTT are appropriate. (B)
● In those identified with increased riskfor future diabetes, identify and, if ap-propriate, treat other CVD risk factors.(B)
For many illnesses there is a major dis-tinction between screening and diagnos-tic testing. However, for diabetes the sametests would be used for “screening” as fordiagnosis. Type 2 diabetes has a longasymptomatic phase and significant clin-ical risk markers. Diabetes may be identi-fied anywhere along a spectrum of clinicalscenarios ranging from a seemingly low-risk individual who happens to have glu-cose testing, to a higher-risk individual
who the provider tests because of highsuspicion of diabetes, to the symptomaticpatient. The discussion herein is primar-ily framed as testing for diabetes in indi-viduals without symptoms. Testing fordiabetes will also detect individuals at in-creased future risk for diabetes, herein re-ferred to as pre-diabetic.
A. Testing for type 2 diabetes andrisk of future diabetes in adultsType 2 diabetes is frequently not diag-nosed until complications appear, andapproximately one-fourth of all peoplewith diabetes in the U.S. may be undiag-nosed. Although the effectiveness of earlyidentification of pre-diabetes and diabetesthrough mass testing of asymptomatic in-dividuals has not been proven definitively(and rigorous trials to provide such proofare unlikely to occur), pre-diabetes anddiabetes meet established criteria for con-ditions in which early detection is appro-priate. Both conditions are common, areincreasing in prevalence, and impose sig-nificant public health burdens. There is along presymptomatic phase before the di-agnosis of type 2 diabetes is usually made.Relatively simple tests are available to de-tect preclinical disease (9). Additionally,the duration of glycemic burden is astrong predictor of adverse outcomes,and effective interventions exist to pre-vent progression of pre-diabetes to diabe-tes (see IV. PREVENTION/DELAY OFTYPE 2 DIABETES) and to reduce risk ofcomplications of diabetes (see VI. PRE-VENTION AND MANAGEMENT OF DI-ABETES COMPLICATIONS).
Recommendations for testing for dia-betes in asymptomatic undiagnosedadults are listed in Table 4. Testing shouldbe considered in adults of any age withBMI �25 kg/m2 and one or more risk fac-tors for diabetes. Because age is a majorrisk factor for diabetes, testing of thosewithout other risk factors should begin nolater than at age 45 years.
Either A1C, FPG, or 2-h OGTT is ap-propriate for testing. The 2-h OGTT identi-fies people with either IFG or IGT and thusmore people at increased risk for the devel-opment of diabetes and CVD. It should benoted that the two tests do not necessarilydetect the same individuals (10). The effi-cacy of interventions for primary preven-tion of type 2 diabetes (11–17) hasprimarily been demonstrated among indi-viduals with IGT, but not for individualswith IFG (who do not also have IGT) orthose with specific A1C levels.
The appropriate interval betweentests is not known (18). The rationale forthe 3-year interval is that false negativeswill be repeated before substantial timeelapses, and there is little likelihood thatan individual will develop significantcomplications of diabetes within 3 yearsof a negative test result.
Because of the need for follow-up anddiscussion of abnormal results, testingshould be carried out within the healthcare setting. Community screening out-side a health care setting is not recom-mended because people with positivetests may not seek, or have access to, ap-propriate follow-up testing and care.Conversely, there may be failure to ensureappropriate repeat testing for individualswho test negative. Community screeningmay also be poorly targeted, i.e., it mayfail to reach the groups most at risk andinappropriately test those at low risk (theworried well) or even those already diag-nosed (19,20).
B. Testing for type 2 diabetes inchildrenThe incidence of type 2 diabetes in ado-lescents has increased dramatically in thelast decade, especially in minority popu-lations (21), although the disease remainsrare in the general pediatric population(22). Consistent with recommendationsfor adults, children and youth at in-creased risk for the presence or the devel-opment of type 2 diabetes should betested within the health care setting (23).The recommendations of the ADA con-sensus statement on type 2 diabetes in
Table 4—Criteria for testing for diabetes in asymptomatic adult individuals
1. Testing should be considered in all adults who are overweight (BMI �25 kg/m2*) andhave additional risk factors:
● physical inactivity● first-degree relative with diabetes● members of a high-risk ethnic population (e.g., African American, Latino, Native
American, Asian American, Pacific Islander)● women who delivered a baby weighing �9 lb or were diagnosed with GDM● hypertension (�140/90 mmHg or on therapy for hypertension)● HDL cholesterol level �35 mg/dl (0.90 mmol/l) and/or a triglyceride level �250
mg/dl (2.82 mmol/l)● women with polycystic ovary syndrome● A1C �5.7%, IGT, or IFG on previous testing● other clinical conditions associated with insulin resistance (e.g., severe obesity,
acanthosis nigricans)● history of CVD
2. In the absence of the above criteria, testing diabetes should begin at age 45 years3. If results are normal, testing should be repeated at least at 3-year intervals, with
consideration of more frequent testing depending on initial results and riskstatus.
*At-risk BMI may be lower in some ethnic groups.
Standards of Medical Care
S14 DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 care.diabetesjournals.org

children and youth, with some modifica-tions, are summarized in Table 5.
C. Screening for type 1 diabetesGenerally, people with type 1 diabetespresent with acute symptoms of diabetesand markedly elevated blood glucose lev-els, and most cases are diagnosed soonafter the onset of hyperglycemia. How-ever, evidence from type 1 diabetes pre-vention studies suggests that measurementof islet autoantibodies identifies individ-uals who are at risk for developing type 1diabetes. Such testing may be appropriatein high-risk individuals, such as thosewith prior transient hyperglycemia orthose who have relatives with type 1 dia-betes, in the context of clinical researchstudies (see, for example, http://www2.diabetestrialnet.org). Widespread clini-cal testing of asymptomatic low-riskindividuals cannot currently be recom-mended, as it would identify very few in-dividuals in the general population whoare at risk. Individuals who screen posi-tive should be counseled about their riskof developing diabetes. Clinical studiesare being conducted to test various meth-ods of preventing type 1 diabetes or re-versing early type 1 diabetes in those withevidence of autoimmunity.
III. DETECTION ANDDIAGNOSIS OF GDM
Recommendations● Screen for GDM using risk factor anal-
ysis and, if appropriate, an OGTT. (C)● Women with GDM should be screened
for diabetes 6–12 weeks postpartumand should be followed up with subse-quent screening for the development ofdiabetes or pre-diabetes. (E)
For many years, GDM has been defined asany degree of glucose intolerance with on-
set or first recognition during pregnancy(4). Although most cases resolve with de-livery, the definition applied whether thecondition persisted after pregnancy anddid not exclude the possibility that unrec-ognized glucose intolerance may have an-tedated or begun concomitantly with thepregnancy. This definition facilitated auniform strategy for detection and classi-fication of GDM, but its limitations wererecognized for many years. As the ongo-ing epidemic of obesity and diabetes hasled to more type 2 diabetes in women ofchildbearing age, the number of pregnantwomen with undiagnosed type 2 diabeteshas increased (24). After deliberations in2008 –2009, the International Associa-tion of Diabetes and Pregnancy StudyGroups (IADPSG), an international con-sensus group with representatives frommultiple obstetrical and diabetes organi-zations, including ADA, recommendedthat high-risk women found to have dia-betes at their initial prenatal visit usingstandard criteria (Table 2) receive a diag-nosis of overt, not gestational, diabetes.
Approximately 7% of all pregnancies(ranging from 1 to 14% depending on thepopulation studied and the diagnostictests used) are complicated by GDM, re-sulting in more than 200,000 casesannually.
Because of the risks of GDM to themother and neonate, screening and diag-nosis are warranted. Current screeningand diagnostic strategies, based on the2004 ADA position statement on GDM(25), are outlined in Table 6.
Results of the Hyperglycemia and Ad-verse Pregnancy Outcomes (HAPO) study(26), a large-scale (�25,000 pregnantwomen) multinational epidemiologicstudy, demonstrated that risk of adversematernal, fetal, and neonatal outcomescontinuously increased as a function ofmaternal glycemia at 24–28 weeks, even
within ranges previously considered nor-mal for pregnancy. For most complica-tions there was no threshold for risk.These results have led to careful reconsid-eration of the diagnostic criteria for GDM.The IADPSG recommended that allwomen not known to have prior diabetesundergo a 75-g OGTT at 24–28 weeks ofgestation. The group developed diagnos-tic cut points for the fasting, 1-h, and 2-hPG measurements that conveyed an oddsratio for adverse outcomes of at least 1.75compared with women with the meanglucose levels in the HAPO study.
At the time of this update to the Stan-dards of Medical Care in Diabetes, ADA isplanning to work with U.S. obstetrical or-ganizations to consider adoption of theIADPSG diagnostic criteria and to discussthe implications of this change. While thischange will significantly increase theprevalence of GDM, there is mounting ev-idence that treating even mild GDM re-duces morbidity for both mother andbaby (27).
Because women with a history ofGDM have a greatly increased subsequentrisk for diabetes (28), they should bescreened for diabetes 6–12 weeks post-partum, using nonpregnant OGTT crite-ria, and should be followed up withsubsequent screening for the develop-ment of diabetes or pre-diabetes, as out-lined in II. TESTING FOR DIABETES INASYMPTOMATIC PATIENTS. Informa-tion on the National Diabetes EducationProgram (NDEP) campaign to preventtype 2 diabetes in women with GDM canbe found at http://ndep.nih.gov/media/NeverTooEarly_Tipsheet.pdf.
IV. PREVENTION/DELAYOF TYPE 2 DIABETES
Recommendations● Patients with IGT (A), IFG (E), or an
A1C of 5.7– 6.4% (E) should be re-ferred to an effective ongoing supportprogram for weight loss of 5–10% ofbody weight and an increase in physicalactivity of at least 150 min/week ofmoderate activity such as walking.
● Follow-up counseling appears to be im-portant for success. (B)
● Based on potential cost savings of dia-betes prevention, such counselingshould be covered by third-party pay-ors. (E)
● In addition to lifestyle counseling, met-formin may be considered in those whoare at very high risk for developing di-abetes (combined IFG and IGT plus
Table 5—Testing for type 2 diabetes in asymptomatic children
Criteria: Overweight (BMI �85th percentile for age and sex, weight for height�85th percentile, or weight �120% of ideal for height)
Plus any two ofthe followingrisk factors:
● Family history of type 2 diabetes in first- or second-degree relative● Race/ethnicity (Native American, African American, Latino, Asian
American, Pacific Islander)● Signs of insulin resistance or conditions associated with insulin
resistance (acanthosis nigricans, hypertension, dyslipidemia,polycystic ovary syndrome, or small for gestational agebirthweight)
● Maternal history of diabetes or GDM during the child’s gestationAge of
initiation:Age 10 years or at onset of puberty, if puberty occurs at a younger
ageFrequency: Every 3 years
Position Statement
care.diabetesjournals.org DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 S15

other risk factors such as A1C �6%,hypertension, low HDL cholesterol, el-evated triglycerides, or family history ofdiabetes in a first-degree relative) andwho are obese and under 60 years ofage. (E)
● Monitoring for the development of di-abetes in those with pre-diabetesshould be performed every year. (E)
Randomized controlled trials have shownthat individuals at high risk for develop-ing diabetes (those with IFG, IGT, orboth) can be given interventions that sig-nificantly decrease the rate of onset of di-abetes (11–17). These interventionsinclude intensive lifestyle modificationprograms that have been shown to be veryeffective (58% reduction after 3 years)and use of the pharmacologic agents met-formin, �-glucosidase inhibitors, orlistat,and thiazolidinediones, each of which has
been shown to decrease incident diabetesto various degrees. A summary of majordiabetes prevention trials is shown in Ta-ble 7.
Two studies of lifestyle interventionhave shown persistent reduction in therole of conversion to type 2 diabetes with3 years (29) to 14 years (30) of postinter-vention follow-up.
Based on the results of clinical trialsand the known risks of progression ofpre-diabetes to diabetes, an ADA Consen-sus Development Panel (36) concludedthat people with IGT and/or IFG shouldbe counseled on lifestyle changes withgoals similar to those of the DPP (5–10%weight loss and moderate physical activ-ity of �30 min/day). Regarding the moredifficult issue of drug therapy for diabetesprevention, the consensus panel felt thatmetformin should be the only drug con-sidered for use in diabetes prevention. For
other drugs, the issues of cost, side effects,and lack of persistence of effect in somestudies led the panel to not recommenduse for diabetes prevention. Metforminuse was recommended only for very-high-risk individuals (those with com-bined IGT and IFG who are obese andhave at least one other risk factor for dia-betes) who are under 60 years of age. Inaddition, the panel highlighted the evi-dence that in the DPP, metformin wasmost effective compared with lifestyle inindividuals with BMI �35 kg/m2 andthose under age 60 years.
V. DIABETES CARE
A. Initial evaluationA complete medical evaluation should beperformed to classify the diabetes, detectthe presence of diabetes complications,review previous treatment and glycemiccontrol in patients with established diabe-tes, assist in formulating a managementplan, and provide a basis for continuingcare. Laboratory tests appropriate to theevaluation of each patient’s medical con-dition should be performed. A focus onthe components of comprehensive care(Table 8) will assist the health care team toensure optimal management of the pa-tient with diabetes.
B. ManagementPeople with diabetes should receive med-ical care from a physician-coordinatedteam. Such teams may include, but arenot limited to, physicians, nurse practitio-ners, physician’s assistants, nurses, dieti-tians, pharmacists, and mental healthprofessionals with expertise and a specialinterest in diabetes. It is essential in thiscollaborative and integrated team ap-proach that individuals with diabetes as-sume an active role in their care.
The management plan should be for-mulated as a collaborative therapeutic al-liance among the patient and family, thephysician, and other members of thehealth care team. A variety of strategiesand techniques should be used to provideadequate education and development ofproblem-solving skills in the various as-pects of diabetes management. Imple-mentation of the management planrequires that each aspect is understoodand agreed to by the patient and the careproviders and that the goals and treat-ment plan are reasonable. Any planshould recognize diabetes self-manage-ment education (DSME) and on-going di-abetes support as an integral component
Table 6—Screening for and diagnosis of GDM
Carry out diabetes risk assessment at the first prenatal visit.Women at very high risk should be screened for diabetes as soon as possible after the
confirmation of pregnancy. Criteria for very high risk are:● Severe obesity● Prior history of GDM or delivery of large-for-gestational-age infant● Presence of glycosuria● Diagnosis of PCOS● Strong family history of type 2 diabetes
Screening/diagnosis at this stage of pregnancy should use standard diagnostic testing (Table2).
All women of greater than low risk of GDM, including those above not found to have diabetesearly in pregnancy, should undergo GDM testing at 24–28 weeks of gestation. Low-risk status, which does not require GDM screening, is defined as women with ALL ofthe following characteristics:
● Age �25 years● Weight normal before pregnancy● Member of an ethnic group with a low prevalence of diabetes● No known diabetes in first-degree relatives● No history of abnormal glucose tolerance● No history of poor obstetrical outcome
Two approaches may be followed for GDM screening at 24–28 weeks:1. Two-step approach:
A. Perform initial screening by measuring plasma or serum glucose 1 h after a 50-g loadof �140 mg/dl identifies �80% of women with GDM, while the sensitivity is furtherincreased to �90% by a threshold of �130 mg/dl.
B. Perform a diagnostic 100-g OGTT on a separate day in women who exceed the chosenthreshold on 50-g screening.
2. One-step approach (may be preferred in clinics with high prevalence of GDM): Performa diagnostic 100-g OGTT in all women to be tested at 24–28 weeks.
The 100-g OGTT should be performed in the morning after an overnight fast of at least 8h.
To make a diagnosis of GDM, at least two of the following plasma glucose values must befound:
● Fasting �95 mg/dl● 1-h �180 mg/dl● 2-h �155 mg/dl● 3-h �140 mg/dl
Standards of Medical Care
S16 DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 care.diabetesjournals.org

of care. In developing the plan, consider-ation should be given to the patient’s age,school or work schedule and conditions,physical activity, eating patterns, socialsituation and cultural factors, and pres-ence of complications of diabetes or othermedical conditions.
C. Glycemic control
1. Assessment of glycemic controlTwo primary techniques are available forhealth providers and patients to assess theeffectiveness of the management plan onglycemic control: patient self-monitoringof blood glucose (SMBG) or interstitialglucose and A1C.
a. Glucose monitoring
Recommendations● SMBG should be carried out three or
more times daily for patients using mul-
tiple insulin injections or insulin pumptherapy. (A)
● For patients using less frequent insulininjections, noninsulin therapies, ormedical nutrition therapy (MNT)alone, SMBG may be useful as a guide tothe success of therapy. (E)
● To achieve postprandial glucose tar-gets, postprandial SMBG may be appro-priate. (E)
● When prescribing SMBG, ensure thatpatients receive initial instruction in,and routine follow-up evaluation of,SMBG technique and using data to ad-just therapy. (E)
● Continuous glucose monitoring (CGM)in conjunction with intensive insulinregimens can be a useful tool to lowerA1C in selected adults (age �25 years)with type 1 diabetes (A).
● Although the evidence for A1C lower-ing is less strong in children, teens, andyounger adults, CGM may be helpful inthese groups. Success correlates with
adherence to ongoing use of the device.(C)
● CGM may be a supplemental tool toSMBG in those with hypoglycemia un-awareness and/or frequent hypoglyce-mic episodes. (E)
The ADA consensus and position state-ments on SMBG provide a comprehensivereview of the subject (37,38). Major clin-ical trials of insulin-treated patients thatdemonstrated the benefits of intensiveglycemic control on diabetes complica-tions have included SMBG as part ofmultifactorial interventions, suggestingthat SMBG is a component of effectivetherapy. SMBG allows patients to eval-uate their individual response to ther-apy and assess whether glycemic targetsare being achieved. Results of SMBG canbe useful in preventing hypoglycemiaand adjusting medications (particularlyprandial insulin doses), MNT, andphysical activity.
Table 7—Therapies proven effective in diabetes prevention trials
Study (ref.) n Population
Meanage
(years)Duration(years)
Intervention(daily dose)
Incidence incontrolsubjects(%/year)
Relative riskreduction (%)
(95% CI)
3-Yearnumber
needed totreat*
LifestyleFinnish DPS (12) 522 IGT, BMI �25 kg/m2 55 3.2 I-D&E 6 58 (30–70) 8.5DPP (11) 2,161† IGT, BMI �24 kg/m2,
FPG �5.3 mmol/l51 3 I-D&E 10.4 58 (48–66) 6.9
Da Qing (13) 259† IGT (randomizedgroups)
45 6 G-D&E 14.5 38 (14–56) 7.9
Toranomon Study (31) 458 IGT (men), BMI 24kg/m2
�55 4 I-D&E 2.4 67 (P � 0.043)‡ 20.6
Indian DPP (17) 269† IGT 46 2.5 I-D&E 23 29 (21–37) 6.4Medications
DPP (11) 2,155† IGT, BMI �24 kg/m2,FPG �5.3 mmol/l
51 2.8 Metformin(1,700mg)
10.4 31 (17–43) 13.9
Indian DPP (17) 269† IGT 46 2.5 Metformin(500 mg)
23 26 (19–35) 6.9
STOP NIDDM (15) 1,419 IGT, FPG �5.6mmol/l
54 3.2 Acarbose(300 mg)
12.4 25 (10–37) 9.6
XENDOS (32) 3,277 BMI �30 kg/m2 43 4 Orlistat (360mg)
2.4 37 (14–54) 45.5
DREAM (16) 5,269 IGT or IFG 55 3.0 Rosiglitazone(8 mg)
9.1 60 (54–65) 6.9
Voglibose Ph-3 (33) 1,780 IGT 56 3.0 (1-year Rx) Vogliobose(0.2 mg)
12.0 40 (18–57) 21 (1-yearRx)
ACT-NOW (34) 602 IGT or IFG 52 2.6 Pioglitizone(45 mg)
6.8 81 (61–91) 6.3
Modified and reprinted with permission (35). Percentage points: *Number needed to treat to prevent 1 case of diabetes, standardized for a 3-year period to improvecomparisons across studies. †Number of participants in the indicated comparisons, not necessarily in entire study. ‡Calculated from information in the article.ACT-NOW, ACTos Now Study for the Prevention of Diabetes; DPP, Diabetes Prevention Program; DPS, Diabetes Prevention Study; DREAM, Diabetes ReductionAssessment with Ramipril and Rosiglitazone Medication; STOP NIDDM, Study to Prevent Non-Insulin Dependent Diabetes; XENDOS, Xenical in the prevention ofDiabetes in Obese Subjects. I, individual; G, group; D&E, diet and exercise.
Position Statement
care.diabetesjournals.org DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 S17

The frequency and timing of SMBGshould be dictated by the particular needsand goals of the patient. SMBG is espe-cially important for patients treated withinsulin in order to monitor for and pre-vent asymptomatic hypoglycemia and hy-perglycemia. For most patients with type1 diabetes and pregnant women takinginsulin, SMBG is recommended three ormore times daily. For these populations,significantly more frequent testing may berequired to reach A1C targets safely with-out hypoglycemia. The optimal frequencyand timing of SMBG for patients with type2 diabetes on noninsulin therapy is un-
clear. A meta-analysis of SMBG in non–insulin-treated patients with type 2diabetes concluded that some regimen ofSMBG was associated with a reduction inA1C of 0.4%. However, many of the stud-ies in this analysis also included patienteducation with diet and exercise counsel-ing and, in some cases, pharmacologic in-tervention, making it difficult to assess thecontribution of SMBG alone to improvedcontrol (39). Several recent trials havecalled into question the clinical utilityand cost-effectiveness of routine SMBG innon–insulin-treated patients (40–42).
Because the accuracy of SMBG is in-
strument and user dependent (43), it isimportant to evaluate each patient’s mon-itoring technique, both initially and atregular intervals thereafter. In addition,optimal use of SMBG requires proper in-terpretation of the data. Patients shouldbe taught how to use the data to adjustfood intake, exercise, or pharmacologicaltherapy to achieve specific glycemic goals,and these skills should be reevaluatedperiodically.
CGM through the measurement of in-terstitial glucose (which correlates wellwith PG) is available. These sensors re-quire calibration with SMBG, and the lat-ter are still recommended for makingacute treatment decisions. CGM devicesalso have alarms for hypo- and hypergly-cemic excursions. Small studies in se-lected patients with type 1 diabetes havesuggested that CGM use reduces the timespent in hypo- and hyperglycemic rangesand may modestly improve glycemic con-trol. A larger 26-week randomized trial of322 type 1 diabetic patients showed thatadults age 25 years and older using inten-sive insulin therapy and CGM experi-enced a 0.5% reduction in A1C (from�7.6 to 7.1%) compared with usual in-tensive insulin therapy with SMBG (44).Sensor use in children, teens, and adultsto age 24 years did not result in significantA1C lowering, and there was no signifi-cant difference in hypoglycemia in anygroup. Importantly, the greatest predictorof A1C lowering in this study for all age-groups was frequency of sensor use,which was lower in younger age-groups.In a smaller randomized controlled trial of129 adults and children with baselineA1C �7.0%, outcomes combining A1Cand hypoglycemia favored the group us-ing CGM, suggesting that CGM is alsobeneficial for individuals with type 1 dia-betes who have already achieved excellentcontrol with A1C �7.0% (45). AlthoughCGM is an evolving technology, emergingdata suggest that it may offer benefit inappropriately selected patients who aremotivated to wear it most of the time.CGM may be particularly useful in thosewith hypoglycemia unawareness and/orfrequent episodes of hypoglycemia, andstudies in this area are ongoing.
b. A1C
Recommendations● Perform the A1C test at least two times
a year in patients who are meeting treat-ment goals (and who have stable glyce-mic control). (E)
Table 8—Components of the comprehensive diabetes evaluation
Medical history● Age and characteristics of onset of diabetes (e.g., DKA, asymptomatic laboratory finding)● Eating patterns, physical activity habits, nutritional status, and weight history; growth
and development in children and adolescents● Diabetes education history● Review of previous treatment regimens and response to therapy (A1C records)
Current treatment of diabetes, including medications, meal plan, physical activity patterns,and results of glucose monitoring and patient’s use of data
● DKA frequency, severity, and cause● Hypoglycemic episodes
● Hypoglycemia awareness● Any severe hypoglycemia: frequency and cause
● History of diabetes-related complications● Microvascular: retinopathy, nephropathy, neuropathy (sensory, including history of
foot lesions; autonomic, including sexual dysfunction and gastroparesis)● Macrovascular: CHD, cerebrovascular disease, PAD● Other: psychosocial problems*, dental disease*
Physical examination● Height, weight, BMI● Blood pressure determination, including orthostatic measurements when indicated● Fundoscopic examination*● Thyroid palpation● Skin examination (for acanthosis nigricans and insulin injection sites)● Comprehensive foot examination:
● Inspection● Palpation of dorsalis pedis and posterior tibial pulses● Presence/absence of patellar and Achilles reflexes● Determination of proprioception, vibration, and monofilament sensation
Laboratory evaluation● A1C, if results not available within past 2–3 months● If not performed/available within past year:
● Fasting lipid profile, including total, LDL- and HDL cholesterol and triglycerides● Liver function tests● Test for urine albumin excretion with spot urine albumin/creatinine ratio● Serum creatinine and calculated GFR● TSH in type 1 diabetes, dyslipidemia, or women over age 50 years
Referrals● Annual dilated eye exam● Family planning for women of reproductive age● Registered dietitian for MNT● DSME● Dental examination● Mental health professional, if needed
* See appropriate referrals for these categories.
Standards of Medical Care
S18 DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 care.diabetesjournals.org

● Perform the A1C test quarterly in pa-tients whose therapy has changed orwho are not meeting glycemic goals. (E)
● Use of point-of-care testing for A1C al-lows for timely decisions on therapychanges, when needed. (E)
Because A1C is thought to reflect averageglycemia over several months (43) andhas strong predictive value for diabetescomplications (11,46), A1C testingshould be performed routinely in all pa-tients with diabetes, at initial assessmentand then as part of continuing care. Mea-surement approximately every 3 monthsdetermines whether a patient’s glycemictargets have been reached and main-tained. For any individual patient, the fre-quency of A1C testing should bedependent on the clinical situation, thetreatment regimen used, and the judg-ment of the clinician. Some patients withstable glycemia well within target may dowell with testing only twice per year,while unstable or highly intensively man-aged patients (e.g., pregnant type 1 dia-betic women) may be tested morefrequently than every 3 months. Theavailability of the A1C result at the timethat the patient is seen (point-of-care test-ing) has been reported to result in in-creased intensification of therapy andimprovement in glycemic control(47,48).
The A1C test is subject to certain lim-itations. Conditions that affect erythro-cyte turnover (hemolysis, blood loss) andhemoglobin variants must be considered,particularly when the A1C result does notcorrelate with the patient’s clinical situa-tion (43). In addition, A1C does not pro-vide a measure of glycemic variability orhypoglycemia. For patients prone to gly-cemic variability (especially type 1 dia-betic patients, or type 2 diabetic patientswith severe insulin deficiency), glycemiccontrol is best judged by the combinationof results of SMBG testing and the A1C.The A1C may also serve as a check on theaccuracy of the patient’s meter (or the pa-tient’s reported SMBG results) and the ad-equacy of the SMBG testing schedule.
Table 9 contains the correlation be-tween A1C levels and mean PG levelsbased on data from the international A1C-Derived Average Glucose (ADAG) trialusing frequent SMBG and CGM in 507adults (83% Caucasian) with type 1, type2, and no diabetes (49). ADA and theAmerican Association of Clinical Chem-ists have determined that the correlation(r 0.92) is strong enough to justify re-
porting both an A1C result and an esti-mated average glucose (eAG) result whena clinician orders the A1C test. In previ-ous versions of the Standards of MedicalCare in Diabetes, the table describing thecorrelation between A1C and mean glu-cose was derived from relatively sparsedata (one seven-point profile over 1 dayper A1C reading) in the primarily Cauca-sian type 1 participants in the DCCT (50).Clinicians should note that the numbersin the table are now different, as they arebased on �2,800 readings per A1C in theADAG trial.
In the ADAG trial, there were no sig-nificant differences among racial and eth-nic groups in the regression lines betweenA1C and mean glucose, although therewas a trend toward a difference betweenAfricans/African Americans participantsand Caucasians that might have been sig-nificant had more Africans/African Amer-icans been studied. A recent studycomparing A1C to CGM data in 48 type 1diabetic children found a highly statisti-cally significant correlation between A1Cand mean blood glucose, although thecorrelation (r 0.7) was significantlylower than in the ADAG trial (51).Whether there are significant differencesin how A1C relates to average glucose inchildren or in African American patientsis an area for further study. For the timebeing, the question has not led to differentrecommendations about testing A1C ordifferent interpretations of the clinicalmeaning of given levels of A1C in thosepopulations.
For patients in whom A1C/eAG andmeasured blood glucose appear discrep-
ant, clinicians should consider the possi-bilities of hemoglobinopathy or alteredred cell turnover and the options of morefrequent and/or different timing of SMBGor use of CGM. Other measures of chronicglycemia such as fructosamine are avail-able, but their linkage to average glucoseand their prognostic significance are notas clear as is the case for A1C.
2. Glycemic goals in adults● Lowering A1C to below or around 7%
has been shown to reduce microvascu-lar and neuropathic complications oftype 1 and type 2 diabetes. Therefore,for microvascular disease prevention,the A1C goal for nonpregnant adults ingeneral is �7%. (A)
● In type 1 and type 2 diabetes, random-ized controlled trials of intensive versusstandard glycemic control have notshown a significant reduction in CVDoutcomes during the randomized por-tion of the trials. Long-term follow-upof the DCCT and UK Prospective Dia-betes Study (UKPDS) cohorts suggeststhat treatment to A1C targets below oraround 7% in the years soon after thediagnosis of diabetes is associated withlong-term reduction in risk of macro-vascular disease. Until more evidencebecomes available, the general goal of�7% appears reasonable for manyadults for macrovascular risk reduc-tion. (B)
● Subgroup analyses of clinical trials suchas the DCCT and UKPDS, and evidencefor reduced proteinuria in the Action inDiabetes and Vascular Disease: Preteraxand Diamicron Modified Release Con-trolled Evaluation (ADVANCE) trialsuggest a small but incremental benefitin microvascular outcomes with A1Cvalues closer to normal. Therefore, forselected individual patients, providersmight reasonably suggest even lowerA1C goals than the general goal of�7%, if this can be achieved withoutsignificant hypoglycemia or other ad-verse effects of treatment. Such patientsmight include those with short dura-tion of diabetes, long life expectancy,and no significant CVD. (B)
● Conversely, less-stringent A1C goalsthan the general goal of �7% may beappropriate for patients with a historyof severe hypoglycemia, limited life ex-pectancy, advanced microvascular ormacrovascular complications, and ex-tensive comorbid conditions and thosewith longstanding diabetes in whomthe general goal is difficult to attain de-
Table 9—Correlation of A1C with averageglucose
A1C (%)
Mean plasma glucose
mg/dl mmol/l
6 126 7.07 154 8.68 183 10.29 212 11.810 240 13.411 269 14.912 298 16.5
These estimates are based on ADAG data of �2,700glucose measurements over 3 months per A1C mea-surement in 507 adults with type 1, type 2, and nodiabetes. The correlation between A1C and averageglucose was 0.92 (49). A calculator for convertingA1C results into estimated average glucose (eAG),in either mg/dl or mmol/l, is available athttp://professional.diabetes.org/eAG.
Position Statement
care.diabetesjournals.org DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 S19

spite diabetes self-management educa-tion, appropriate glucose monitoring,and effective doses of multiple glucose-lowering agents including insulin. (C)
Glycemic control is fundamental to themanagement of diabetes. The DCCT, aprospective, randomized, controlled trialof intensive versus standard glycemiccontrol in patients with relatively recentlydiagnosed type 1 diabetes, showed defin-itively that improved glycemic control isassociated with significantly decreasedrates of microvascular (retinopathy andnephropathy) as well as neuropathiccomplications (53). Follow-up of theDCCT cohorts in the Epidemiology of Di-abetes Interventions and Complications(EDIC) study has shown persistence ofthis effect in previously intensivelytreated subjects, even though their glyce-mic control has been equivalent to that ofprevious standard arm subjects duringfollow-up (54,55).
In type 2 diabetes, the Kumamotostudy (56) and the UKPDS (57,58) dem-onstrated significant reductions in micro-vascular and neuropathic complicationswith intensive therapy. Similar to theDCCT-EDIC findings, long-term fol-low-up of the UKPDS cohort has recentlydemonstrated a “legacy effect” of early in-tensive glycemic control on long-termrates of microvascular complications,even with loss of glycemic separation be-tween the intensive and standard cohortsafter the end of the randomized con-trolled trial (59). The more recent Veter-ans Affairs Diabetes Trial (VADT) in type2 diabetes also showed significant reduc-tions in albuminuria with intensive(achieved median A1C 6.9%) comparedwith standard glycemic control but nodifference in retinopathy and neuropathy(60,61).
In each of these large randomizedprospective clinical trials, treatment regi-mens that reduced average A1C to 7%(1% above the upper limits of normal)were associated with fewer markers oflong-term microvascular complications;however, intensive control was found toincrease the risk of severe hypoglycemiaand led to weight gain (46,60,62).
Epidemiological analyses of theDCCT and UKPDS (46,53) demonstrate acurvilinear relationship between A1C andmicrovascular complications. Such anal-yses suggest that, on a population level,the greatest number of complications willbe averted by taking patients from verypoor control to fair or good control. These
analyses also suggest that further loweringof A1C from 7 to 6% is associated withfurther reduction in the risk of microvas-cular complications, albeit the absoluterisk reductions become much smaller.The ADVANCE study of intensive versusstandard glycemic control in type 2 dia-betes found a statistically significant re-duction in albuminuria with an A1Ctarget of �6.5% (achieved median A1C6.3%) compared with standard therapyachieving a median A1C of 7.0% (63).Given the substantially increased risk ofhypoglycemia (particularly in those withtype 1 diabetes, but also in the recent type2 diabetes trials described below), theconcerning mortality findings in the Ac-tion to Control Cardiovascular Risk in Di-abetes (ACCORD) trial described belowand the relatively much greater effort re-quired to achieve near-normoglycemia,the risks of lower targets may outweighthe potential benefits on microvascularcomplications on a population level.However, selected individual patients, es-pecially those with little comorbidity andlong life expectancy (who may reap thebenefits of further lowering glycemia be-low 7%) may, at patient and providerjudgment, adopt glycemic targets as closeto normal as possible as long as significanthypoglycemia does not become a barrier.
Whereas many epidemiologic studiesand meta-analyses (64,65) have clearlyshown a direct relationship between A1Cand CVD, the potential of intensive glyce-mic control to reduce CVD has been lessclearly defined. In the DCCT, there was atrend toward lower risk of CVD eventswith intensive control (risk reduction41%, 95% CI 10–68%), but the numberof events was small. However, 9-yearpost-DCCT follow-up of the cohort hasshown that participants previously ran-domized to the intensive arm had a 42%reduction (P 0.02) in CVD outcomesand a 57% reduction (P 0.02) in therisk of nonfatal myocardial infarction(MI), stroke, or CVD death comparedwith participants previously in the stan-dard arm (66). The benefit of intensiveglycemic control in this type 1 diabeticcohort has recently been shown to persistfor up to 30 years (67).
The UKPDS trial of type 2 diabetesobserved a 16% reduction in cardiovascu-lar complications (combined fatal or non-fatal MI and sudden death) in theintensive glycemic control arm, althoughthis difference was not statistically signif-icant (P 0.052), and there was no sug-gestion of benefit on other CVD outcomes
such as stroke. In an epidemiologic anal-ysis of the study cohort, a continuous as-sociation was observed such that for everypercentage point lower median on-studyA1C (e.g., 8–7%), there was a statisticallysignificant 18% reduction in CVD events,again with no glycemic threshold. A re-cent report of 10 years of follow-up of theUKPDS cohort described, for the partici-pants originally randomized to intensiveglycemic control compared with thoserandomized to conventional glycemiccontrol, long-term reductions in MI (15%with sulfonylurea or insulin as initialpharmacotherapy, 33% with metforminas initial pharmacotherapy, both statisti-cally significant) and in all-cause mortal-ity (13 and 27%, respectively, bothstatistically significant) (59).
Because of ongoing uncertainty re-garding whether intensive glycemic con-trol can reduce the increased risk of CVDevents in people with type 2 diabetes, sev-eral large long-term trials were launchedin the past decade to compare the effectsof intensive versus standard glycemiccontrol on CVD outcomes in relativelyhigh-risk participants with establishedtype 2 diabetes. In 2008, results of threelarge trials (ACCORD, ADVANCE, andVADT) suggested no significant reductionin CVD outcomes with intensive glycemiccontrol in these populations. Details ofthese three studies are shown in Table 10,and their results and implications are re-viewed more extensively in a recent ADAposition statement (52).
The ACCORD study randomized10,251 participants with either history ofa CVD event or significant CVD risk to astrategy of intensive glycemic control (tar-get A1C �6.0%) or standard glycemiccontrol (A1C target 7.0–7.9%). Investiga-tors used multiple glycemic medicationsin both arms. From a baseline medianA1C of 8.1%, the intensive arm reached amedian A1C of 6.4% within 12 months ofrandomization, while the standard groupreached a median A1C of 7.5%. Otherrisk factors were treated aggressively andequally in both groups. The intensive gly-cemic control group had more use of in-sulin in combination with multiple oralagents, significantly more weight gain,and more episodes of severe hypoglyce-mia than the standard group.
In early 2008, the glycemic controlarm of ACCORD was halted on the rec-ommendation of the study’s data safetymonitoring board due to the finding of anincreased rate of mortality in the intensivearm compared with the standard arm
Standards of Medical Care
S20 DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 care.diabetesjournals.org

(1.41 vs. 1.14%/year, hazard ratio 1.22,95% CI 1.01–1.46), with a similar in-crease in cardiovascular deaths. The pri-mary outcome of ACCORD (MI, stroke,or cardiovascular death) was lower in theintensive glycemic control group due to areduction in nonfatal MI, although thisfinding was not statistically significantwhen the study was terminated (68). Ofnote, prespecified subset analyses showedthat participants with no previous CVDevent and those who had a baseline A1C�8% had a statistically significant reduc-tion in the primary CVD outcome, al-though overall mortality was not reducedin these groups.
The cause of excess deaths in the in-tensive group of the ACCORD has beendifficult to pinpoint (and is discussed insome detail in a 2009 ADA position state-ment [52]). However, exploratory analy-ses of the mortality findings of ACCORD(evaluating variables including weightgain, use of any specific drug or drugcombination, and hypoglycemia) were re-portedly unable to identify a clear expla-nation for the excess mortality in theintensive arm. At the 69th Scientific Ses-sions of the American Diabetes Associa-t ion, the ACCORD inves t iga torspresented additional analyses showing noincrease in mortality in participants who
achieved A1C levels �7% or in those wholowered their A1C quickly after trial en-rollment. In fact, the converse was ob-served: those at highest risk for mortalitywere participants in the intensive armwith the highest A1C levels.
The ADVANCE study randomizedparticipants to a strategy of intensive gly-cemic control (with primary therapy be-ing the sulfonylurea gliclizide andadditional medications as needed toachieve a target A1C of �6.5%) or to stan-dard therapy (in which any medicationbut gliclizide could be used and the gly-cemic target was according to “localguidelines”). ADVANCE participants
Table 10—Comparison of the three trials of intensive glycemic control and CVD outcomes
ACCORD ADVANCE VADT
Participant characteristicsn 10,251 11,140 1,791Mean age (years) 62 66 60Duration of diabetes (years) 10 8 11.5History of CVD (%) 35 32 40Median baseline A1C (%) 8.1 7.2 9.4On insulin at baseline (%) 35 1.5 52
Protocol characteristicsA1C goals (%) (I vs. S)* �6.0 vs. 7.0–7.9 �6.5 vs. “based on local guidelines” �6.0 (action if �6.5) vs.
planned separation of 1.5Protocol for glycemic control
(I vs. S)* Multiple drugs in botharms
Multiple drugs added to gliclizide vs.multiple drugs with no gliclizide
Multiple drugs in both arms
Management of other riskfactors Embedded blood pressure
and lipid trialsEmbedded blood pressure trial Protocol for intensive
treatment in both armsOn-study characteristics
Achieved median A1C (%)(I vs. S) 6.4 vs. 7.5 6.3 vs. 7.0 6.9 vs. 8.5
On insulin at study end (%)(I vs. S)* 77 vs. 55* 40 vs. 24 89 vs. 0.74
Weight changes (kg)Intensive glycemic control arm 3.5 �0.1 7.8Standard glycemic control arm 0.4 �1.0 3.4Severe hypoglycemia
(participants with one or moreepisodes during study) (%)
Intensive glycemic control arm 16.2 2.7 21.2Standard glycemic control arm 5.1 1.5 9.9
OutcomesDefinition of primary outcome Nonfatal MI, nonfatal
stroke, CVD deathMicrovascular plus macrovascular
(nonfatal MI, nonfatal stroke, CVDdeath) outcomes
Nonfatal MI, nonfatal stroke,CVD death,hospitalization for heartfailure, revascularization
HR for primary outcome(95% CI) 0.90 (0.78–1.04) 0.9 (0.82–0.98);
macrovascular 0.94 (0.84–1.06)0.88 (0.74–1.05)
HR for mortality findings(95% CI) 1.22 (1.01–1.46) 0.93 (0.83–1.06) 1.07 (0.81–1.42)
*Insulin rates for ACCORD are for any use during the study. I, intensive glycemic control; S, standard glycemic control. Abridged from ref. 52.
Position Statement
care.diabetesjournals.org DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 S21

were slightly older than those in AC-CORD and VADT and had similar highCVD risk. However, they had an averageduration of diabetes that was 2 yearsshorter, lower baseline A1C (median7.2%), and almost no use of insulin atenrollment. The median A1C levelsachieved in the intensive and standardarms were 6.3 and 7.0%, respectively,and maximal separation between thearms took several years to achieve. Use ofother drugs that favorably impact CVDrisk (aspirin, statins, and angiotensin en-zyme inhibitors) was lower in ADVANCEthan in ACCORD or VADT.
The primary outcome of ADVANCEwas a combination of microvascularevents (nephropathy and retinopathy)and major adverse cardiovascular events(MI, stroke, and cardiovascular death).Intensive glycemic control significantlyreduced the primary end point, althoughthis was due to a significant reduction inthe microvascular outcome, primarily de-velopment of macroalbuminuria, with nosignificant reduction in the macrovascu-lar outcome. There was no difference inoverall or cardiovascular mortality be-tween the intensive compared with thestandard glycemic control arms (63).
VADT randomized participants withtype 2 diabetes uncontrolled on insulin ormaximal dose oral agents (median entryA1C 9.4%) to a strategy of intensive gly-cemic control (goal A1C �6.0%) or stan-dard glycemic control, with a plannedA1C separation of at least 1.5%. Medica-tion treatment algorithms were used toachieve the specified glycemic goals, witha goal of using similar medications in bothgroups. Median A1C levels of 6.9 and8.4% were achieved in the intensive andstandard arms, respectively, within the1st year of the study. Other CVD risk fac-tors were treated aggressively and equallyin both groups.
The primary outcome of VADT was acomposite of CVD events. The cumulativeprimary outcome was nonsignificantlylower in the intensive arm. There weremore CVD deaths in the intensive armthan in the standard arm, but the differ-ence was not statistically significant (60).Post hoc subgroup analyses suggestedthat duration of diabetes interacted withrandomization such that participantswith duration of diabetes less than about12 years appeared to have a CVD benefitof intensive glycemic control while thosewith longer duration of disease prior tostudy entry had a neutral or even adverseeffect of intensive glycemic control. Other
exploratory analyses suggested that se-vere hypoglycemia within the past 90days was a strong predictor of the primaryoutcome and of CVD mortality (69).
All three of these trials were carriedout in participants with established diabe-tes (mean duration 8–11 years) and eitherknown CVD or multiple risk factors sug-gesting the presence of established ath-erosclerosis. Subset analyses of the threetrials suggested a significant benefit of in-tensive glycemic control on CVD in par-ticipants with shorter duration ofdiabetes, lower A1C at entry, and/or ab-sence of known CVD. The DCCT-EDICstudy and the long-term follow-up of theUKPDS cohort both suggest that intensiveglycemic control initiated soon after diag-nosis of diabetes in patients with a lowerlevel of CVD risk may impart long-termprotection from CVD events. As is thecase with microvascular complications, itmay be that glycemic control plays agreater role before macrovascular diseaseis well developed and minimal or no rolewhen it is advanced. Consistent with thisconcept, data from an ancillary study ofVADT demonstrated that intensive glyce-mic control was quite effective in reduc-ing CVD events in individuals with lessatherosclerosis at baseline (assessed bycoronary calcium) but not in people withmore extensive baseline atherosclerosis(70).
The benefits of intensive glycemiccontrol on microvascular and neuro-pathic complications are well establishedfor both type 1 and type 2 diabetes. AD-VANCE and VADT have added to that ev-idence base by demonstra t ing asignificant reduction in the risk of new orworsening albuminuria with intensiveglycemic control. The lack of significantreduction in CVD events with intensiveglycemic control in ACCORD, AD-VANCE, and VADT should not lead clini-cians to abandon the general target of anA1C �7.0% and thereby discount thebenefit of good control on serious and de-bilitating microvascular complications.
The evidence for a cardiovascularbenefit of intensive glycemic control pri-marily rests on long-term follow-up ofstudy cohorts treated early in the courseof type 1 and type 2 diabetes as well assubset analyses of ACCORD, ADVANCE,and VADT. A recent group-level meta-analysis of the three trials suggests thatglucose lowering has a modest (9%) butstatistically significant reduction in majorCVD outcomes, primarily nonfatal MI,with no significant increase in mortality.
A prespecified subgroup analysis sug-gested that major CVD outcome reduc-tion occurred in patients without knownCVD at baseline (HR 0.84 [95% CI 0.74–0.94]) (71). Conversely, the mortalityfindings in ACCORD and subgroup anal-yses of VADT suggest that the potentialrisks of very intensive glycemic controlmay outweigh its benefits in some pa-tients, such as those with very long dura-tion of diabetes, known history of severehypoglycemia, advanced atherosclerosis,and advanced age/frailty. Certainly, pro-viders should be vigilant in preventing se-vere hypoglycemia in patients withadvanced disease and should not aggres-sively attempt to achieve near-normalA1C levels in patients in whom such atarget cannot be reasonably easily andsafely achieved.
Recommended glycemic goals fornonpregnant adults are shown in Table11. The recommendations are based onthose for A1C values, with listed bloodglucose levels that appear to correlatewith achievement of an A1C of �7%. Theissue of pre- versus postprandial SMBGtargets is complex (72). Elevated post-challenge (2-h OGTT) glucose valueshave been associated with increased car-diovascular risk independent of FPG insome epidemiological studies. In diabeticsubjects, some surrogate measures of vas-cular pathology, such as endothelial dys-function, are negatively affected bypostprandial hyperglycemia (73). It isclear that postprandial hyperglycemia,like preprandial hyperglycemia, contrib-utes to elevated A1C levels, with its rela-tive contribution being higher at A1Clevels that are closer to 7%. However, out-come studies have clearly shown A1C tobe the primary predictor of complica-tions, and landmark glycemic control tri-als such as the DCCT and UKPDS reliedoverwhelmingly on preprandial SMBG.Additionally, a randomized controlledtrial in patients with known CVD foundno CVD benefit of insulin regimens tar-geting postprandial glucose comparedwith those targeting preprandial glucose(74). For individuals who have premealglucose values within target but A1C val-ues above target, a reasonable recommen-dation for postprandial testing and targetsis monitoring postprandial plasma glu-cose (PPG) 1–2 h after the start of the mealand treatment aimed at reducing PPG val-ues to �180 mg/dl to help lower A1C.
As noted above, less stringent treat-ment goals may be appropriate for adultswith limited life expectancies or advanced
Standards of Medical Care
S22 DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 care.diabetesjournals.org

vascular disease. Glycemic goals for chil-dren are provided in VII.A.1.a. Glycemiccontrol. Severe or frequent hypoglycemiais an absolute indication for the modifica-tion of treatment regimens, including set-ting higher glycemic goals.
Regarding goals for glycemic controlfor women with GDM, recommendationsfrom the Fifth International Workshop-Conference on Gestational Diabetes (75)are to target maternal capillary glucoseconcentrations of:
● Preprandial �95 mg/dl (5.3 mmol/l)and either● 1-h postmeal �140 mg/dl (7.8
mmol/l)or● 2-h postmeal �120 mg/dl (6.7
mmol/l)
For women with preexisting type 1 ortype 2 diabetes who become pregnant, arecent consensus statement (76) recom-mends the following as optimal glycemicgoals, if they can be achieved without ex-cessive hypoglycemia:
● premeal, bedtime, and overnight glu-cose 60–99 mg/dl (3.3–5.4 mmol/l)
● peak postprandial glucose 100 –129mg/dl (5.4–7.1 mmol/l)
● A1C �6.0%
3. Approach to treatment
a. Therapy for type 1 diabetes. TheDCCT clearly showed that intensive insu-lin therapy (three or more injections perday of insulin or continuous subcutane-
ous insulin infusion [CSII] or insulinpump therapy) was a key part of im-proved glycemia and better outcomes(53,66). At the time of the study, therapywas carried out with short- and interme-diate-acting human insulins. Despite bet-ter microvascular outcomes, intensiveinsulin therapy was associated with a highrate in severe hypoglycemia (62 episodesper 100 patient-years of therapy). Sincethe time of the DCCT, a number of rapid-acting and long-acting insulin analogshave been developed. These analogs areassociated with less hypoglycemia withequal A1C lowering in type 1 diabetes(77,78).
Recommended therapy for type 1 di-abetes therefore consists of the followingcomponents: 1) use of multiple dose in-sulin injections (3–4 injections per day ofbasal and prandial insulin) or CSII ther-apy; 2) matching of prandial insulin tocarbohydrate intake, premeal blood glu-cose, and anticipated activity; and 3) formany patients (especially if hypoglycemiais a problem), use of insulin analogs.There are excellent reviews available thatguide the initiation and management ofinsulin therapy to achieve desired glyce-mic goals (3,77,79).
Because of the increased frequency ofother autoimmune diseases in type 1 dia-betes, screening for thyroid dysfunction,vitamin B12 deficiency, or celiac diseaseshould be considered based on signs andsymptoms. Periodic screening in the ab-sence of symptoms has been recom-mended, but the effectiveness andoptimal frequency are unclear.
b. Therapy for type 2 diabetes. The ADAand the European Association for theStudy of Diabetes (EASD) published aconsensus statement on the approach tomanagement of hyperglycemia in individ-uals with type 2 diabetes (80) and a sub-sequent update (81). Highlights of thisapproach include: intervention at thetime of diagnosis with metformin in com-bination with lifestyle changes (MNT andexercise) and continuing timely augmen-tation of therapy with additional agents(including early initiation of insulin ther-apy) as a means of achieving and main-taining recommended levels of glycemiccontrol (i.e., A1C �7% for most patients).The overall objective is to achieve andmaintain glycemic control and to changeinterventions when therapeutic goals arenot being met.
The algorithm took into account theevidence for A1C lowering of the individ-ual interventions, their additive effects,and their expense. The precise drugs usedand their exact sequence may not be asimportant as achieving and maintainingglycemic targets safely. Medications notincluded in the consensus algorithm, ow-ing to less glucose-lowering effectiveness,limited clinical data, and/or relative ex-pense, still may be appropriate choices forindividual patients to achieve glycemicgoals. Initiation of insulin at the time ofdiagnosis is recommended for individualspresenting with weight loss or other se-vere hyperglycemic symptoms or signs.
D. Medical nutrition therapy
General recommendations● Individuals who have pre-diabetes or
diabetes should receive individualizedMNT as needed to achieve treatmentgoals, preferably provided by a regis-tered dietitian familiar with the compo-nents of diabetes MNT. (A)
● Because it can result in cost savings andimproved outcomes (B), MNT shouldbe covered by insurance and other pay-ors (E).
Energy balance, overweight, andobesity● In overweight and obese insulin-
resistant individuals, modest weightloss has been shown to reduce insulinresistance. Thus, weight loss is recom-mended for all overweight or obese in-dividuals who have or are at risk fordiabetes. (A)
● For weight loss, either low-carbohy-drate or low-fat calorie-restricted diets
Table 11 —Summary of glycemic recommendations for non-pregnant adults with diabetes
A1C �7.0%*Preprandial capillary plasma glucose 70–130 mg/dl (3.9–7.2 mmol/l)Peak postprandial capillary plasma glucose† �180 mg/dl (�10.0 mmol/l)Key concepts in setting glycemic goals:
● A1C is the primary target for glycemic control● Goals should be individualized based on:
● duration of diabetes● age/life expectancy● comorbid conditions● known CVD or advanced microvascular
complications● hypoglycemia unawareness● individual patient considerations
● More or less stringent glycemic goals may beappropriate for individual patients
Postprandial glucose may be targeted if A1C goals are notmet despite reaching preprandial glucose goals
*Referenced to a nondiabetic range of 4.0–6.0% using a DCCT-based assay. †Postprandial glucose mea-surements should be made 1–2 h after the beginning of the meal, generally peak levels in patients withdiabetes.
Position Statement
care.diabetesjournals.org DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 S23

may be effective in the short-term (upto 1 year). (A)
● For patients on low-carbohydrate diets,monitor lipid profiles, renal function,and protein intake (in those with ne-phropathy) and adjust hypoglycemictherapy as needed. (E)
● Physical activity and behavior modifi-cation are important components ofweight loss programs and are mosthelpful in maintenance of weight loss.(B)
Primary prevention of diabetes● Among individuals at high risk for de-
veloping type 2 diabetes, structuredprograms emphasizing l i festylechanges that include moderate weightloss (7% body weight) and regularphysical activity (150 min/week) withdietary strategies including reducedcalories and reduced intake of dietaryfat can reduce the risk for developingdiabetes and are therefore recom-mended. (A)
● Individuals at high risk for type 2 dia-betes should be encouraged to achievethe U.S. Department of Agriculture(USDA) recommendation for dietary fi-ber (14 g fiber/1,000 kcal) and foodscontaining whole grains (one-half ofgrain intake). (B)
Dietary fat intake in diabetesmanagement● Saturated fat intake should be �7% of
total calories. (A)● Reducing intake of trans fat lowers LDL
cholesterol and increases HDL choles-terol (A); therefore intake of trans fatshould be minimized (E).
Carbohydrate intake in diabetesmanagement● Monitoring carbohydrate intake,
whether by carbohydrate counting, ex-changes, or experience-based estima-tion, remains a key strategy in achievingglycemic control. (A)
● For individuals with diabetes, use of theglycemic index and glycemic load mayprovide a modest additional benefit forglycemic control over that observedwhen total carbohydrate is consideredalone. (B)
Other nutrition recommendations● Sugar alcohols and nonnutritive sweet-
eners are safe when consumed withinthe acceptable daily intake levels estab-lished by the Food and Drug Adminis-tration (FDA). (A)
● If adults with diabetes choose to usealcohol, daily intake should be limitedto a moderate amount (one drink perday or less for adult women and twodrinks per day or less for adult men).(E)
● Routine supplementation with antioxi-dants, such as vitamins E and C andcarotene, is not advised because of lackof evidence of efficacy and concern re-lated to long-term safety. (A)
● Benefit from chromium supplementa-tion in people with diabetes or obesityhas not been conclusively demon-strated and therefore cannot be recom-mended. (C)
● Individualized meal planning shouldinclude optimization of food choices tomeet recommended dietary allowances(RDAs)/dietary reference intakes(DRIs) for all micronutrients. (E)
MNT is an integral component of diabetesprevention, management, and self-management education. In addition to itsrole in preventing and controlling diabe-tes, ADA recognizes the importance ofnutrition as an essential component of anoverall healthy lifestyle. A full review ofthe evidence regarding nutrition in pre-venting and controlling diabetes and itscomplications and additional nutrition-related recommendations can be found inthe ADA position statement, NutritionRecommendations and Interventions forDiabetes, published in 2006 and updatedfor 2008 (82). Achieving nutrition-related goals requires a coordinated teameffort that includes the active involvementof the person with pre-diabetes or diabe-tes. Because of the complexity of nutritionissues, it is recommended that a registereddietitian who is knowledgeable andskilled in implementing nutrition therapyinto diabetes management and educationbe the team member who provides MNT.
Clinical trials/outcome studies ofMNT have reported decreases in A1C at3–6 months ranging from 0.25 to 2.9%with higher reductions seen in type 2 di-abetes of shorter duration. Multiple stud-ies have demonstrated susta inedimprovements in A1C at 12 months andlonger when a registered dietitian pro-vided follow-up visits ranging frommonthly to three sessions per year (83–90). Meta-analyses of studies in nondia-betic, free-living subjects report that MNTreduces LDL cholesterol by 15–25 mg/dl(91) or by up to 16% (92), while clinicaltrials support a role for lifestyle modifica-tion in treating hypertension (92,93).
Because of the effects of obesity oninsulin resistance, weight loss is an im-portant therapeutic objective for over-weight or obese individuals with pre-diabetes or diabetes (94). Short-termstudies have demonstrated that moderateweight loss (5% of body weight) in sub-jects with type 2 diabetes is associatedwith decreased insulin resistance, im-proved measures of glycemia and lipemia,and reduced blood pressure (95); longer-term studies (�52 weeks) showed mixedeffects on A1C in adults with type 2 dia-betes (96 –99), and results were con-founded by pharmacologic weight losstherapy. A systematic review of 80 weightloss studies of �1 year duration demon-strated that moderate weight lossachieved through diet alone, diet and ex-ercise, and meal replacements can beachieved and maintained over the longterm (4.8–8% weight loss at 12 months[100]). The multifactorial intensive life-style intervention used in the DPP, whichincluded reduced intake of fat and calo-ries, led to weight loss averaging 7% at 6months and maintenance of 5% weightloss at 3 years, associated with a 58% re-duction in incidence of type 2 diabetes(11). Look AHEAD (Action for Health inDiabetes) is a large clinical trial designedto determine whether long-term weightloss will improve glycemia and preventcardiovascular events in subjects withtype 2 diabetes. One-year results of theintensive lifestyle intervention in this trialshow an average of 8.6% weight loss, sig-nificant reduction of A1C, and reductionin several CVD risk factors (101). Whencompleted, the Look AHEAD studyshould provide insight into the effects oflong-term weight loss on important clin-ical outcomes.
The optimal macronutrient distribu-tion of weight loss diets has not been es-tablished. Although low-fat diets havetraditionally been promoted for weightloss, several randomized controlled trialsfound that subjects on low-carbohydratediets (�130 g/day of carbohydrate) lostmore weight at 6 months than subjects onlow-fat diets (102,103); however, at 1year, the difference in weight loss be-tween the low-carbohydrate and low-fatdiets was not significant and weight losswas modest with both diets. Anotherstudy of overweight women randomizedto one of four diets showed significantlymore weight loss at 12 months with theAtkins low-carbohydrate diet than withhigher-carbohydrate diets (104).Changes in serum triglyceride and HDL
Standards of Medical Care
S24 DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 care.diabetesjournals.org

cholesterol were more favorable with thelow-carbohydrate diets. In one study,those subjects with type 2 diabetes dem-onstrated a greater decrease in A1C with alow-carbohydrate diet than with a low-fatdiet (103). A recent meta-analysis showedthat at 6 months, low-carbohydrate dietswere associated with greater improve-ments in triglyceride and HDL cholesterolconcentrations than low-fat diets; how-ever, LDL cholesterol was significantlyhigher with the low-carbohydrate diets(105). In a 2-year dietary interventionstudy, Mediterranean and low-carbohy-drate diets were found to be effective andsafe alternatives to a low-fat diet forweight reduction in moderately obeseparticipants (99).
The RDA for digestible carbohydrateis 130 g/day and is based on providingadequate glucose as the required fuel forthe central nervous system without reli-ance on glucose production from ingestedprotein or fat. Although brain fuel needscan be met on lower-carbohydrate diets,long-term metabolic effects of very-low-carbohydrate diets are unclear, and suchdiets eliminate many foods that are im-portant sources of energy, fiber, vitamins,and minerals that are important in dietarypalatability (106).
Although numerous studies have at-tempted to identify the optimal mix ofmacronutrients for meal plans of peoplewith diabetes, it is unlikely that one suchcombination of macronutrients exists.The best mix of carbohydrate, protein,and fat appears to vary depending onindividual circumstances. For thoseindividuals seeking guidance as to macro-nutrient distribution in healthy adults,DRIs may be helpful (106). It must beclearly recognized that regardless of themacronutrient mix, the total caloric in-take must be appropriate to the weightmanagement goal. Further, individualiza-tion of the macronutrient compositionwill depend on the metabolic status of thepatient (e.g., lipid profile and renal func-tion) and/or food preferences. Plant-based diets (vegan or vegetarian) that arewell planned and nutritionally adequatehave also been shown to improve meta-bolic control (107,108).
The primary goal with respect to di-etary fat in individuals with diabetes is tolimit saturated fatty acids, trans fatty ac-ids, and cholesterol intake so as to reducerisk for CVD. Saturated and trans fatty ac-ids are the principal dietary determinantsof plasma LDL cholesterol. There is a lackof evidence on the effects of specific fatty
acids on people with diabetes; therefore,the recommended goals are consistentwith those for individuals with CVD(92,109).
The FDA has approved five nonnutri-tive sweeteners for use in the U.S.: acesul-fame potassium, aspartame, neotame,saccharin, and sucralose. Before being al-lowed on the market, all underwent rig-orous scrutiny and were shown to be safewhen consumed by the public, includingpeople with diabetes and women duringpregnancy. Reduced calorie sweetenersapproved by the FDA include sugar alco-hols (polyols) such as erythritol, isomalt,lactitol, maltitol, mannitol, sorbitol, xyli-tol, tagatose, and hydrogenated starch hy-drolysates. The use of sugar alcoholsappears to be safe; however, they maycause diarrhea, especially in children. Ste-via (Rebaudioside A) has been designatedby the FDA as being generally recognizedas safe (GRAS).
Reimbursement for MNTMNT, when delivered by a registered dieti-tian according to nutrition practice guide-lines, is reimbursed as part of the Medicareprogram as overseen by the Centers forMedicare and Medicaid Services (www.cms.hhs.gov/ medicalnutritiontherapy).
E. Bariatric surgery
Recommendations● Bariatric surgery should be considered
for adults with BMI �35 kg/m2 andtype 2 diabetes, especially if the diabe-tes or associated comorbidities are dif-ficult to control with lifestyle andpharmacologic therapy. (B)
● Patients with type 2 diabetes who haveundergone bariatric surgery need life-long lifestyle support and medical moni-toring. (E)
● Although small trials have shown glyce-mic benefit of bariatric surgery in patientswith type 2 diabetes and BMI of 30–35kg/m2, there is currently insufficient evi-dence to generally recommend surgery inpatients with BMI�35 kg/m2 outside of aresearch protocol. (E)
● The long-term benefits, cost-effectiveness,and risks of bariatric surgery in individ-uals with type 2 diabetes should bestudied in well-designed, randomizedcontrolled trials with optimal medicaland lifestyle therapy as the comparator.(E)
Gastric reduction surgery, either gastricbanding or procedures that involve by-
passing or transposing sections of thesmall intestine, when part of a compre-hensive team approach, can be an effec-tive weight loss treatment for severeobesity, and national guidelines supportits consideration for people with type 2diabetes who have BMI �35 kg/m2. Bari-atric surgery has been shown to lead tonear or complete normalization of glyce-mia in �55–95% of patients with type 2diabetes, depending on the surgical pro-cedure. A meta-analysis of studies of bari-atric surgery reported that 78% ofindividuals with type 2 diabetes had com-plete “resolution” of diabetes (normaliza-tion of blood glucose levels in the absenceof medications) and that the resolutionrates were sustained in studies that hadfollow-up exceeding 2 years (110). Reso-lution rates are lower with proceduresthat only constrict the stomach andhigher with those that bypass portions ofthe small intestine. Additionally, there is asuggestion that intestinal bypass proce-dures may have glycemic effects that areindependent of their effects on weight.
A recent randomized controlled trialcompared adjustable gastric banding tothe “best available” medical and lifestyletherapy in subjects with type 2 diabetesdiagnosed �2 years before randomiza-tion and with BMI 30–40 kg/m2 (111). Inthis trial, 73% of surgically treated pa-tients achieved “remission” of their diabe-tes, compared with 13% of those treatedmedically. The latter group lost only 1.7%of body weight, suggesting that their ther-apy was not optimal. Overall the trial had60 subjects, and only 13 had a BMI �35kg/m2, making it difficult to generalizethese results to diabetic patients who areless severely obese or with longer dura-tion of diabetes.
Bariatric surgery is costly in the shortterm and has some risks. Rates of morbidityand mortality directly related to the surgeryhave been reduced considerably in recentyears, with 30-day mortality rates now0.28%, similar to those of laparoscopic cho-lecystectomy (112). Longer-term concernsinclude vitamin and mineral deficiencies,osteoporosis, and rare but often severe hy-poglycemia from insulin hypersecretion.Cohort studies attempting to match sub-jects suggest that the procedure may reducelonger-term mortality rates (113), and it isreasonable to postulate that there may berecouping of costs over the long term. How-ever, studies of the mechanisms of glycemicimprovement, long-term benefits and risks,and cost-effectiveness of bariatric surgery inindividuals with type 2 diabetes will require
Position Statement
care.diabetesjournals.org DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 S25

well-designed, randomized clinical trialswith optimal medical and lifestyle therapyof diabetes and cardiovascular risk factors asthe comparators.
F. Diabetes self-managementeducation
Recommendations● People with diabetes should receive
DSME according to national standardswhen their diabetes is diagnosed and asneeded thereafter. (B)
● Effective self-management and qualityof life are the key outcomes of DSMEand should be measured and moni-tored as part of care. (C)
● DSME should address psychosocial is-sues, since emotional well-being is as-sociated with posit ive diabetesoutcomes. (C)
● Because DSME can result in cost-savings and improved outcomes (B),DSME should be reimbursed by third-party payors. (E)
DSME is an essential element of dia-betes care (114–120), and national stan-dards for DSME (121) are based onevidence for its benefits. Education helpspeople with diabetes initiate effective self-management and cope with diabeteswhen they are first diagnosed. OngoingDSME and support also help people withdiabetes mainta in ef fec t ive se l f -management throughout a lifetime of di-abetes as they face new challenges and astreatment advances become available.DSME helps patients optimize metaboliccontrol, prevent and manage complica-tions, and maximize quality of life in acost-effective manner (122).
DSME is the on-going process of fa-cilitating the knowledge, skill, and abilitynecessary for diabetes self-care (121).This process incorporates the needs,goals, and life experiences of the personwith diabetes. The overall objectives ofDSME are to support informed decision-making, self-care behaviors, problem-solving, and active collaboration with thehealth care team and to improve clinicaloutcomes, health status, and quality of lifein a cost-effective manner (121).
Current best practice of DSME is askills-based approach that focuses onhelping those with diabetes make in-formed self-management choices. DSMEhas changed from a didactic approach fo-cusing on providing information, to amore theoretically based empowermentmodel that focuses on helping those with
diabetes make informed self-managementdecisions. Care of diabetes has shifted toan approach that is more patient centeredand places the person with diabetes at thecenter of the care model working in col-laboration with health care professionals.Patient-centered care is respectful of andresponsive to individual patient prefer-ences, needs, and values and ensures thatpatient values guide all decision making(123).
1. Evidence for the benefits of DSMEMultiple studies have found that DSME isassociated with improved diabetesknowledge and self-care behavior (115);improved clinical outcomes such as lowerA1C (116,117,119,120,124), lower self-reported weight (115), improved qualityof life (118,125), and healthy coping(126); and lower costs (127). Better out-comes were reported for DSME interven-tions that were longer and includedfollow-up support (115,128–131), thatwere culturally (132) and age appropriate(133,134) and tailored to individualneeds and preferences (114), and that ad-dressed psychosocial issues (114,115,119,135). Both individual and group ap-proaches have been found effective (136–138). There is growing evidence for therole of community health workers andpeer (139) and lay leaders (140) in deliv-ering DSME and support in addition tothe core team (141).
Diabetes education is associated withincreased use of primary and preventiveservices and lower use of acute, inpatienthospital services (127). Patients who par-ticipate in diabetes education are morelikely to follow best practice treatmentrecommendations, particularly amongthe medicare population, and to havelower Medicare and commercial claimcosts (142).
2. National Standards for DSMEThe National Standards for DSME are de-signed to define quality diabetes self-management education and to assistdiabetes educators in a variety of settingsto provide evidence-based education(121). The standards, most recently re-vised in 2007, are reviewed and updatedevery 5 years by a task force representingkey organizations involved in the field ofdiabetes education and care.
3. Reimbursement for DSMEDSME, when provided by a program thatmeets ADA recognition standards, is re-imbursed as part of the Medicare program
overseen by the Centers for Medicare andMedicaid Services (www.cms.hhs.gov/DiabetesSelfManagement).
G. Physical activity
Recommendations● People with diabetes should be advised
to perform at least 150 min/week ofmoderate-intensity aerobic physical ac-tivity (50 –70% of maximum heartrate). (A)
● In the absence of contraindications,people with type 2 diabetes should beencouraged to perform resistance train-ing three times per week. (A)
ADA technical reviews on exercise in pa-tients with diabetes, currently being up-dated, have summarized the value ofexercise in the diabetes management plan(143,144). Regular exercise has beenshown to improve blood glucose control,reduce cardiovascular risk factors, con-tribute to weight loss, and improve wellbeing. Furthermore, regular exercise mayprevent type 2 diabetes in high-risk indi-viduals (11–13). Structured exercise in-terventions of at least 8 weeks’ durationhave been shown to lower A1C by an av-erage of 0.66% in people with type 2 di-abetes, even with no significant change inBMI (145). Higher levels of exercise in-tensity are associated with greater im-provements in A1C and fitness (146).
1. Frequency and type of exerciseThe U.S. Department of Health and Hu-man Services’ Physical Activity Guide-lines for Americans (147) suggest thatadults over age 18 years perform 150 min/week of moderate-intensity or 75 min/week of vigorous aerobic physical activityor an equivalent combination of the two.In addition, the guidelines suggest thatadults also do muscle-strengthening ac-tivities that involve all major musclegroups two or more days per week. Theguidelines suggest that adults over age 65years, or those with disabilities, follow theadult guidelines if possible or (if this is notpossible) be as physically active as theyare able. Studies included in the meta-analysis of effects of exercise interventionson glycemic control (145) had a meannumber of sessions per week of 3.4, witha mean of 49 min/session. The DPP life-style intervention, which included 150min/week of moderate intensity exercise,had a beneficial effect on glycemia inthose with pre-diabetes. Therefore, itseems reasonable to recommend that peo-
Standards of Medical Care
S26 DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 care.diabetesjournals.org

ple with diabetes try to follow the physicalactivity guidelines for the generalpopulation.
Progressive resistance exercise im-proves insulin sensitivity in older menwith type 2 diabetes to the same or even toa greater extent as aerobic exercise (148).Clinical trials have provided strong evi-dence for the A1C-lowering value of re-sistance training in older adults with type2 diabetes (149,150) and for an additivebenefit of combined aerobic and resis-tance exercise in adults with type 2 diabe-tes (151).
2. Evaluation of the diabetic patientbefore recommending an exerciseprogramPrior guidelines have suggested that be-fore recommending a program of physicalactivity, the provider should assess pa-tients with multiple cardiovascular riskfactors for coronary artery disease (CAD).As further discussed in VI.A.5. Coronaryheart disease screening and treatment, thearea of screening asymptomatic diabeticpatients for CAD remains unclear, and arecent ADA consensus statement on thisissue concluded that routine screening isnot recommended (152). Providersshould use clinical judgment in this area.Certainly, high-risk patients should beencouraged to start with short periods oflow-intensity exercise and to increase theintensity and duration slowly.
Providers should assess patients forconditions that might contraindicate cer-tain types of exercise or predispose to in-jury, such as uncontrolled hypertension,severe autonomic neuropathy, severe pe-ripheral neuropathy or history of foot le-s ions, and unstable prol i ferat iveretinopathy. The patient’s age and previ-ous physical activity level should beconsidered.
3. Exercise in the presence ofnonoptimal glycemic controla. Hyperglycemia. When people withtype 1 diabetes are deprived of insulin for12–48 h and are ketotic, exercise canworsen hyperglycemia and ketosis (153);therefore, vigorous activity should beavoided in the presence of ketosis. How-ever, it is not necessary to postpone exer-cise simply based on hyperglycemia,provided the patient feels well and urineand/or blood ketones are negative.b. Hypoglycemia. In individuals takinginsulin and/or insulin secretagogues,physical activity can cause hypoglycemiaif medication dose or carbohydrate con-
sumption is not altered. For individualson these therapies, added carbohydrateshould be ingested if pre-exercise glucoselevels are �100 mg/dl (5.6 mmol/l)(154,155). Hypoglycemia is rare in dia-betic individuals who are not treated withinsulin or insulin secretagogues, and nopreventive measures for hypoglycemiaare usually advised in these cases.
4. Exercise in the presence of specificlong-term complications of diabetesa. Retinopathy. In the presence of pro-liferative diabetic retinopathy (PDR) orsevere non-proliferative diabetic retinop-athy (NPDR), vigorous aerobic or resis-tance exercise may be contraindicatedbecause of the risk of triggering vitreoushemorrhage or retinal detachment (156).b. Peripheral neuropathy. Decreasedpain sensation in the extremities results inincreased risk of skin breakdown and in-fection and of Charcot joint destruction.Prior recommendations have advisednon–weight-bearing exercise for patientswith severe peripheral neuropathy. Stud-ies have shown that moderate-intensitywalking may not lead to increased risk offoot ulcers or reulceration in those withperipheral neuropathy (157). All individ-uals with peripheral neuropathy shouldwear proper footwear and examine theirfeet daily for early detection of lesions.Anyone with a foot injury or open soreshould be restricted to non–weight-bearing activities.c. Autonomic neuropathy. Autonomicneuropathy can increase the risk of exer-cise-induced injury or adverse eventsthrough decreased cardiac responsive-ness to exercise, postural hypotension,impaired thermoregulation, impairednight vision due to impaired papillary re-action, and unpredictable carbohydratedelivery from gastroparesis predisposingto hypoglycemia (158). Autonomic neu-ropathy is also strongly associated withCVD in people with diabetes (159,160).People with diabetic autonomic neuropa-thy should undergo cardiac investigationbefore beginning physical activity moreintense than that to which they areaccustomed.d. Albuminuria and nephropathy. Phys-ical activity can acutely increase urinaryprotein excretion. However, there is noevidence that vigorous exercise increasesthe rate of progression of diabetic kidneydisease and likely no need for any specificexercise restrictions for people with dia-betic kidney disease (161).
H. Psychosocial assessment and care
Recommendations● Assessment of psychological and social
situation should be included as an on-going part of the medical managementof diabetes. (E)
● Psychosocial screening and follow-upshould include, but is not limited to,attitudes about the illness, expectationsfor medical management and out-comes, affect/mood, general and diabe-tes-related quality of life, resources(financial, social, and emotional), andpsychiatric history. (E)
● Screen for psychosocial problems suchas depression and diabetes-related dis-tress, anxiety, eating disorders, andcognitive impairment when self-management is poor. (C)
Psychological and social problems canimpair the ability of the individual (162–164) or the family to carry out diabetescare tasks and therefore compromisehealth status. There are opportunities forthe clinician to assess psychosocial statusin a timely and efficient manner so thatreferral for appropriate services can beaccomplished.
Key opportunities for screening ofpsychosocial status occur at diagnosis,during regularly scheduled managementvisits, during hospitalizations, at discov-ery of complications, or when problemswith glucose control, quality of life, or ad-herence are identified. Patients are likelyto exhibit psychological vulnerability atdiagnosis and when their medical statuschanges, i.e., the end of the honeymoonperiod, when the need for intensifiedtreatment is evident, and when complica-tions are discovered (164).
Issues known to impact se l f -management and health outcomes in-clude but are not limited to: attitudesabout the illness, expectations for medicalmanagement and outcomes, affect/mood,general and diabetes-related quality oflife, diabetes-related distress (165), re-sources (financial, social, and emotional)(166), and psychiatric history (167,168).Screening tools are available for a numberof these areas (135). Indications for refer-ral to a mental health specialist familiarwith diabetes management may includegross noncompliance with medical regi-men (by self or others) (168), depressionwith the possibi l i ty of sel f-harm(169,170), debilitating anxiety (alone orwith depression), indications of an eatingdisorder, or cognitive functioning that
Position Statement
care.diabetesjournals.org DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 S27

significantly impairs judgment. It is pref-erable to incorporate psychological as-sessment and treatment into routine carerather than waiting for identification of aspecific problem or deterioration in psy-chological status (135). Although the cli-nician may not feel qualified to treatpsychological problems, using the pa-tient-provider relationship as a founda-tion for further treatment can increase thelikelihood that the patient will accept re-ferral for other services. It is important toestablish that emotional well-being is partof diabetes management.
I. When treatment goals are not metFor a variety of reasons, some people withdiabetes and their health care providersdo not achieve the desired goals of treat-ment (Table 11). Rethinking the treat-ment regimen may require assessment ofbarriers including income, health literacy,diabetes distress, depression, and com-peting demands, including those relatedto family responsibilities and dynamics.Other strategies may include culturallyappropriate and enhanced DSME, co-management with a diabetes team, refer-ral to a medical social worker forassistance with insurance coverage, orchange in pharmacological therapy. Initi-ation of or increase in SMBG, utilizationof CGM, frequent contact with the pa-tient, or referral to a mental health profes-sional or physician with special expertisein diabetes may be useful. Providing pa-tients with an algorithm for self-titrationof insulin doses based on SMBG resultsmay be helpful for type 2 patients whotake insulin (171).
J. Intercurrent illnessThe stress of illness, trauma, and/or sur-gery frequently aggravates glycemic con-trol and may precipitate diabeticketoacidosis (DKA) or nonketotic hyper-osmolar state, life-threatening conditionsthat require immediate medical care toprevent complications and death (172).Any condition leading to deterioration inglycemic control necessitates more fre-quent monitoring of blood glucose and(in ketosis-prone patients) urine or bloodketones. Marked hyperglycemia requirestemporary adjustment of the treatmentprogram and, if accompanied by ketosis,vomiting, or alteration in level of con-sciousness, immediate interaction withthe diabetes care team. The patient treatedwith noninsulin therapies or MNT alonemay temporarily require insulin. Ade-quate fluid and caloric intake must be as-
sured. Infection or dehydration are morelikely to necessitate hospitalization of theperson with diabetes than the personwithout diabetes.
The hospitalized patient should betreated by a physician with expertise inthe management of diabetes. For furtherinformation on management of patientswith hyperglycemia in the hospital, seeVIII.A. Diabetes care in the hospital. Forfurther information on management ofDKA or nonketotic hyperosmolar state,refer to the ADA consensus statement onhyperglycemic crises (173).
K. Hypoglycemia
Recommendations● Glucose (15–20 g) is the preferred
treatment for the conscious individualwith hypoglycemia, although any formof carbohydrate that contains glucosemay be used. If SMBG 15 min aftertreatment shows continued hypoglyce-mia, the treatment should be repeated.Once SMBG glucose returns to normal,the individual should consume a mealor snack to prevent recurrence of hypo-glycemia. (E)
● Glucagon should be prescribed for allindividuals at significant risk of severehypoglycemia, and caregivers or familymembers of these individuals should beinstructed in its administration. Gluca-gon administration is not limited tohealth care professionals. (E)
● Individuals with hypoglycemia un-awareness or one or more episodes ofsevere hypoglycemia should be advisedto raise their glycemic targets to strictlyavoid further hypoglycemia for at leastseveral weeks to partially reverse hypo-glycemia unawareness and reduce riskof future episodes. (B)
Hypoglycemia is the leading limiting fac-tor in the glycemic management of type 1and insulin-treated type 2 diabetes (174).Treatment of hypoglycemia (PG �70 mg/dl) requires ingestion of glucose- or car-bohydrate-containing foods. The acuteglycemic response correlates better withthe glucose content than with the carbo-hydrate content of the food. Althoughpure glucose is the preferred treatment,any form of carbohydrate that containsglucose will raise blood glucose. Addedfat may retard and then prolong the acuteglycemic response (175). Ongoing activ-ity of insulin or insulin secretagogues maylead to recurrence of hypoglycemia unlessfurther food is ingested after recovery.
Severe hypoglycemia (where the indi-vidual requires the assistance of anotherperson and cannot be treated with oralcarbohydrate due to confusion or uncon-sciousness) should be treated using emer-gency glucagon kits, which require aprescription. Those in close contact withor who have custodial care of people withhypoglycemia-prone diabetes (familymembers, roommates, school personnel,child care providers, correctional institu-tion staff, or coworkers) should be in-structed in use of such kits. An individualdoes not need to be a health care profes-sional to safely administer glucagon. Careshould be taken to ensure that unexpiredglucagon kits are available.
Prevention of hypoglycemia is a crit-ical component of diabetes management.Teaching people with diabetes to balanceinsulin use, carbohydrate intake, and ex-ercise is a necessary but not always suffi-cient strategy. In type 1 diabetes andseverely insulin-deficient type 2 diabetes,the syndrome of hypoglycemia unaware-ness, or hypoglycemia-associated auto-nomic failure, can severely compromisestringent diabetes control and quality oflife. The deficient counter-regulatory hor-mone release and autonomic responses inthis syndrome are both risk factors forand are caused by hypoglycemia. A corol-lary to this “vicious cycle” is that severalweeks of avoidance of hypoglycemia hasbeen demonstrated to improve counter-regulation and awareness to some extentin many patients (174,176,177). Hence,patients with one or more episodes of se-vere hypoglycemia may benefit from atleast short-term relaxation of glycemictargets.
L. Immunization
Recommendations● Annually provide an influenza vaccine
to all diabetic patients �6 months ofage. (C)
● Administer pneumococcal polysaccha-ride vaccine to all diabetic patients �2years of age. A one-time revaccination isrecommended for individuals �64years of age previously immunizedwhen they were �65 years of age if thevaccine was administered �5 yearsago. Other indications for repeat vacci-nation include nephrotic syndrome,chronic renal disease, and other immu-nocompromised states, such as aftertransplantation. (C)
Standards of Medical Care
S28 DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 care.diabetesjournals.org

Influenza and pneumonia are common,preventable infectious diseases associatedwith high mortality and morbidity in theelderly and in people with chronic dis-eases. Though there are limited studiesreporting the morbidity and mortality ofinfluenza and pneumococcal pneumoniaspecifically in people with diabetes, ob-servational studies of patients with a vari-ety of chronic illnesses, includingdiabetes, show that these conditions areassociated with an increase in hospitaliza-tions for influenza and its complications.People with diabetes may be at increasedrisk of the bacteremic form of pneumo-coccal infection and have been reportedto have a high risk of nosocomial bactere-mia, which has a mortality rate as high as50% (178).
Safe and effective vaccines are avail-able that can greatly reduce the risk ofserious complications from these diseases(179,180). In a case-control series, influ-enza vaccine was shown to reduce diabe-tes-related hospital admission by as muchas 79% during flu epidemics (179). Thereis sufficient evidence to support that peo-ple with diabetes have appropriate sero-logic and clinical responses to thesevaccinations. The Centers for DiseaseControl and Prevention’s Advisory Com-mittee on Immunization Practices recom-mends influenza and pneumococcalvaccines for all individuals with diabetes(http://www.cdc.gov/vaccines/recs/). Fora complete discussion on the preventionof influenza and pneumococcal disease inpeople with diabetes, consult the techni-cal review and position statement on thissubject (178,181).
VI. PREVENTION ANDMANAGEMENT OFDIABETES COMPLICATIONS
A. Cardiovascular diseaseCVD is the major cause of morbidity andmortality for individuals with diabetes andthe largest contributor to the direct and in-direct costs of diabetes. The common con-ditions coexisting with type 2 diabetes (e.g.,hypertension and dyslipidemia) are clearrisk factors for CVD, and diabetes itself con-fers independent risk. Numerous studieshave shown the efficacy of controlling indi-vidual cardiovascular risk factors in pre-venting or slowing CVD in people withdiabetes. Large benefits are seen when mul-tiple risk factors are addressed globally(182,183). Risk for coronary heart diseaseand CVD in general can be estimated usingmultivariable risk factor approaches, and
such a strategy may be desirable to under-take in adult patients prior to institutingpreventive therapy.
1. Hypertension/blood pressurecontrol
Recommendations
Screening and diagnosis● Blood pressure should be measured at
every routine diabetes visit. Patientsfound to have systolic blood pressure�130 mmHg or diastolic blood pres-sure �80 mmHg should have bloodpressure confirmed on a separate day.Repeat systolic blood pressure �130mmHg or diastolic blood pressure �80mmHg confirms a diagnosis of hyper-tension. (C)
Goals● Patients with diabetes should be treated
to a systolic blood pressure �130mmHg. (C)
● Patients with diabetes should be treatedto a diastolic blood pressure �80mmHg. (B)
Treatment● Patients with a systolic blood pressure
130–139 mmHg or a diastolic bloodpressure 80–89 mmHg may be givenlifestyle therapy alone for a maximumof 3 months, and then if targets are notachieved, patients should be treatedwith the addition of pharmacologicalagents. (E)
● Patients with more severe hypertension(systolic blood pressure �140 mmHgor diastolic blood pressure �90mmHg) at diagnosis or follow-upshould receive pharmacologic therapyin addition to lifestyle therapy. (A)
● Lifestyle therapy for hypertension con-sists of weight loss if overweight,DASH-style dietary pattern includingreducing sodium and increasing potas-sium intake, moderation of alcohol in-take, and increased physical activity.(B)
● Pharmacologic therapy for patientswith diabetes and hypertension shouldbe paired with a regimen that includeseither an ACE inhibitor or an angioten-sin II receptor blocker (ARB). If oneclass is not tolerated, the other shouldbe substituted. If needed to achieveblood pressure targets, a thiazide di-uretic should be added to those with anestimated glomerular filtration rate(GFR) (see below) �30 ml � min/1.73
m2 and a loop diuretic for those with anestimated GFR �30 ml � min/1.73 m2.(C)
● Multiple drug therapy (two or moreagents at maximal doses) is generallyrequired to achieve blood pressure tar-gets. (B)
● If ACE inhibitors, ARBs, or diuretics areused, kidney function and serum potas-sium levels should be closely moni-tored. (E)
● In pregnant patients with diabetes andchronic hypertension, blood pressuretarget goals of 110–129/65–79 mmHgare suggested in the interest of long-term maternal health and minimizingimpaired fetal growth. ACE inhibitorsand ARBs are contraindicated duringpregnancy. (E)
Hypertension is a common comorbidityof diabetes that affects the majority of pa-tients, with prevalence depending on typeof diabetes, age, obesity, and ethnicity.Hypertension is a major risk factor forboth CVD and microvascular complica-tions. In type 1 diabetes, hypertension isoften the result of underlying nephropa-thy, while in type 2 diabetes it usuallycoexists with other cardiometabolic riskfactors.a. Screening and diagnosis. Measure-ment of blood pressure in the officeshould be done by a trained individualand should follow the guidelines estab-lished for nondiabetic individuals: mea-surement in the seated position, with feeton the floor and arm supported at heartlevel, after 5 min of rest. Cuff size shouldbe appropriate for the upper arm circum-ference. Elevated values should be con-firmed on a separate day. Because of theclear synergistic risks of hypertension anddiabetes, the diagnostic cutoff for a diag-nosis of hypertension is lower in peoplewith diabetes (blood pressure �130/80mmHg) than in those without diabetes(blood pressure �140/90 mmHg) (184).
Home blood pressure self-monitoringand 24-h ambulatory blood pressuremonitoring may provide additional evi-dence of “white coat” and masked hyper-tension and other discrepancies betweenoffice and “true” blood pressure, andstudies in nondiabetic populations showthat home measurements may correlatebetter with CVD risk than office measure-ments (185,186). However, the prepon-derance of the clear evidence of benefits oftreatment of hypertension in people withdiabetes is based on office measurements.
Position Statement
care.diabetesjournals.org DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 S29

b. Treatment goals. Randomized clinicaltrials have demonstrated the benefit (re-duction of coronary heart disease [CHD]events, stroke, and nephropathy) of low-ering blood pressure to �140 mmHg sys-tolic and �80 mmHg diastolic inindividuals with diabetes (184,187–189).Epidemiologic analyses show that bloodpressure �115/75 mmHg is associatedwith increased cardiovascular event ratesand mortality in individuals with diabetes(184,190,191). Therefore, a target bloodpressure goal of �130/80 mmHg is rea-sonable if it can be achieved safely. Theongoing ACCORD trial is designed to de-termine whether blood pressure loweringto systolic blood pressure �120 mmHgprovides greater cardiovascular protec-tion than a systolic blood pressure level of�140 mmHg in patients with type 2 dia-betes (192).c. Treatment strategies. Although thereare no well-controlled studies of diet andexercise in the treatment of hypertensionin individuals with diabetes, the DietaryApproaches to Stop Hypertension(DASH) study in nondiabetic individualshas shown antihypertensive effects simi-lar to those of pharmacologic mono-therapy. Lifestyle therapy consists ofreducing sodium intake (to �1,500 mg/day) and excess body weight; increasingconsumption of fruits, vegetables (8–10servings/day), and low-fat dairy products(2–3 servings/day); avoiding excessive al-cohol consumption (no more than twoservings per day in men and no more thanone serving per day in women); and in-creasing activity levels (184,193). Thesenonpharmacological strategies may alsopositively affect glycemia and lipid con-trol. Their effects on cardiovascularevents have not been established. An ini-tial trial of nonpharmacologic therapymay be reasonable in diabetic individu-als with mild hypertension (systolic130 –139 mmHg or diastolic 80 – 89mmHg). If the blood pressure is �140mmHg systolic and/or �90 mmHg dia-stolic at the time of diagnosis, pharma-cologic therapy should be initiatedalong with nonpharmacologic therapy(184).
Lowering of blood pressure with reg-imens based on a variety of antihyperten-sive drugs, including ACE inhibitors,ARBs, �-blockers, diuretics, and calciumchannel blockers, has been shown to beeffective in reducing cardiovascularevents. Several studies suggested thatACE inhibitors may be superior to dihy-dropyridine calcium channel blockers in
reducing cardiovascular events (194 –196). However, a variety of other studieshave shown no specific advantage to ACEinhibitors as initial treatment of hyperten-sion in the general hypertensive popula-tion, but rather an advantage oncardiovascular outcomes of initial therapywith low-dose thiazide diuret ics(184,197,198).
In people with diabetes, inhibitors ofthe renin-angiotensin system (RAS) mayhave unique advantages for initial or earlytherapy of hypertension. In a nonhyper-tension trial of high-risk individuals in-cluding a large subset with diabetes, anACE inhibitor reduced CVD outcomes(199). In patients with congestive heartfailure (CHF), including diabetic sub-groups, ARBs have been shown to reducemajor CVD outcomes (200–203), and intype 2 patients with significant nephrop-athy, ARBs were superior to calciumchannel blockers for reducing heart fail-ure (204–206). Though evidence for dis-tinct advantages of RAS inhibitors onCVD outcomes in diabetes remains con-flicting (187,207), the high CVD risks as-sociated with diabetes, and the highprevalence of undiagnosed CVD, may stillfavor recommendations for their use asfirst-line hypertension therapy in peoplewith diabetes (184). Recently, the bloodpressure arm of the ADVANCE trial dem-onstrated that routine administration of afixed combination of the ACE inhibitorperindopril and the diuretic indapamidesignificantly reduced combined micro-vascular and macrovascular outcomes, aswell as CVD and total mortality. The im-proved outcomes also could have beendue to lower achieved blood pressure inthe perindopril-indapamide arm (208).In addition, the ACCOMPLISH (AvoidingCardiovascular Events in CombinationTherapy in Patients Living with SystolicHypertension) trial showed a decrease inmorbidity and mortality in those receiv-ing benazapril and amlodipine versusbenazapril and hydrochlorothiazide. Thecompelling benefits of RAS inhibitors indiabetic patients with albuminuria or re-nal insufficiency provide additional ratio-nale for use of these agents (see below,VI.B. Nephropathy screening andtreatment).
An important caveat is that most pa-tients with hypertension require multi-drug therapy to reach treatment goals,especially diabetic patients whose targetsare lower. Many patients will requirethree or more drugs to reach target goals(184). If blood pressure is refractory to
optimal doses of at least three antihyper-tensive agents of different classifications,one of which should be a diuretic, clini-cians should consider an evaluation forsecondary forms of hypertension.
During pregnancy in diabetic womenwith chronic hypertension, target bloodpressure goals of 110–129 mmHg sys-tolic and 65–79 mmHg diastolic are rea-sonable, as they contribute to long-termmaternal health. Lower blood pressurelevels may be associated with impairedfetal growth. During pregnancy, treat-ment with ACE inhibitors and ARBs iscontraindicated, since they can cause fetaldamage. Antihypertensive drugs knownto be effective and safe in pregnancy in-clude methyldopa, labetalol, diltiazem,clonidine, and prazosin. Chronic diureticuse during pregnancy has been associatedwith restricted maternal plasma volume,which might reduce uteroplacental perfu-sion (209).
2. Dyslipidemia/lipid management
Recommendations
Screening● In most adult patients, measure fasting
lipid profile at least annually. In adultswith low-risk lipid values (LDL choles-terol �100 mg/dl, HDL cholesterol�50 mg/dl, and triglycerides �150mg/dl), lipid assessments may be re-peated every 2 years. (E)
Treatment recommendations and goals● Lifestyle modification focusing on the
reduction of saturated fat, trans fat,and cholesterol intake; increase of n-3fatty acids, viscous fiber, and plantstanols/sterols; weight loss (if indi-cated); and increased physical activityshould be recommended to improvethe lipid profile in patients with dia-betes. (A)
● Statin therapy should be added to life-style therapy, regardless of baselinelipid levels, for diabetic patients:● with overt CVD. (A)● without CVD who are over the age of
40 years and have one or more otherCVD risk factors. (A)
● For patients at lower risk than de-scribed above (e.g., without overt CVDand under the age of 40 years), statintherapy should be considered in addi-tion to lifestyle therapy if LDL choles-terol remains �100 mg/dl or in thosewith multiple CVD risk factors. (E)
● In individuals without overt CVD, the
Standards of Medical Care
S30 DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 care.diabetesjournals.org

primary goal is an LDL cholesterol�100 mg/dl (2.6 mmol/l). (A)
● In individuals with overt CVD, a lowerLDL cholesterol goal of �70 mg/dl (1.8mmol/l), using a high dose of a statin, isan option. (B)
● If drug-treated patients do not reach theabove targets on maximal tolerated sta-tin therapy, a reduction in LDL choles-terol of �30–40% from baseline is analternative therapeutic goal. (A)
● Triglycerides levels �150 mg/dl (1.7mmol/l) and HDL cholesterol �40mg/dl (1.0 mmol/l) in men and �50mg/dl (1.3 mmol/l) in women, are de-sirable. However, LDL cholesterol–targeted statin therapy remains thepreferred strategy. (C)
● If targets are not reached on maximallytolerated doses of statins, combinationtherapy using statins and other lipid-lowering agents may be considered toachieve lipid targets but has not beenevaluated in outcome studies for eitherCVD outcomes or safety. (E)
● Statin therapy is contraindicated inpregnancy. (E)
a. Evidence for benefits of lipid-loweringtherapy. Patients with type 2 diabeteshave an increased prevalence of lipid ab-normalities, contributing to their highrisk of CVD. Over the past decade ormore, multiple clinical trials have demon-strated significant effects of pharmaco-logic (primarily statin) therapy on CVDoutcomes in subjects with CHD and forprimary CVD prevention (210). Analysesof diabetic subgroups of larger trials(211–215) and trials specifically in sub-jects with diabetes (216,217) showed sig-
n ifican t pr imary and secondaryprevention of CVD events with and with-out CHD deaths in diabetic populations.As shown in Table 12, and similar to find-ings in nondiabetic subjects, reduction in“hard” CVD outcomes (CHD death andnonfatal MI) can be more clearly seen indiabetic subjects with high baseline CVDrisk (known CVD and/or very high LDLcholesterol levels), but overall the benefitsof statin therapy in people with diabetes atmoderate or high risk for CVD areconvincing.
Low levels of HDL cholesterol, oftenassociated with elevated triglyceride lev-els, are the most prevalent pattern of dys-lipidemia in people with type 2 diabetes.However, the evidence base for drugs thattarget these lipid fractions is significantlyless robust than that for statin therapy(217). Nicotinic acid has been shown toreduce CVD outcomes (218), althoughthe study was done in a nondiabetic co-hort. Gemfibrozil has been shown to de-crease rates of CVD events in subjectswithout diabetes (219,220) and in a di-
abetic subgroup of a larger trial (219).However, in a large trial specific to dia-betic patients, fenofibrate failed to re-duce overall cardiovascular outcomes(221).b. Dyslipidemia treatment and targetlipid levels. For most patients with dia-betes, the first priority of dyslipidemiatherapy (unless severe hypertriglyceride-mia is the immediate issue) is to lowerLDL cholesterol to a target goal of �100mg/dl (2.60 mmol/l) (222). Lifestyle in-tervention, including MNT, increasedphysical activity, weight loss, and smok-ing cessation, may allow some patients toreach lipid goals. Nutrition interventionshould be tailored according to each pa-tient’s age, type of diabetes, pharmacolog-ical treatment, lipid levels, and othermedical conditions and should focus onthe reduction of saturated fat, cholesterol,and trans unsaturated fat intake and in-creases in n-3 fatty acids, viscous fiber(such as in oats, legumes, citrus), andplant stanols/sterols. Glycemic controlcan also beneficially modify plasma lipidlevels, particularly in patients with veryhigh triglycerides and poor glycemiccontrol.
In those with clinical CVD or who areover age 40 years and have CVD risk fac-tors, pharmacological treatment shouldbe added to lifestyle therapy regardless ofbaseline lipid levels. Statins are the drugsof choice for lowering LDL cholesterol.
In patients other than those describedabove, statin treatment should be consid-ered if there is an inadequate LDL choles-terol response to lifestyle modificationsand improved glucose control or if thepatient has increased cardiovascular risk
Table 12—Reduction in 10-year risk of major CVD endpoints (CHD death/non-fatal MI) in major statin trials, or sub-studies of major trials,in diabetic subjects (N � 16,032)
Study (ref.)CVD
prevention Statin dose and comparator Risk reductionRelative riskreduction
Absolute riskreduction
LDLcholesterol
reduction (%)
4S-DM (211) 2° Simvastatin 20–40 mg vs. placebo 85.7 to 43.2% 50% 42.5% 186 to 119 mg/dl (36%)ASPEN 2° (216) 2° Atorvastatin 10 mg vs. placebo 39.5 to 24.5% 34% 12.7% 112 to 79 mg/dl (29%)HPS-DM (212) 2° Simvastatin 40 mg vs. placebo 43.8 to 36.3% 17% 7.5% 123 to 84 mg/dl (31%)CARE-DM (213) 2° Pravastatin 40 mg vs. placebo 40.8 to 35.4% 13% 5.4% 136 to 99 mg/dl (27%)TNT-DM (214) 2° Atorvastatin 80 mg vs. 10 mg 26.3 to 21.6% 18% 4.7% 99 to 77 mg/dl (22%)HPS-DM (212) 1° Simvastatin 40 mg vs. placebo 17.5 to 11.5% 34% 6.0% 124 to 86 mg/dl (31%)CARDS (234) 1° Atorvastatin 10 mg vs. placebo 11.5 to 7.5% 35% 4.0% 118 to 71 mg/dl (40%)ASPEN 1° (216) 1° Atorvastatin 10 mg vs. placebo 9.8 to 7.9% 19% 1.9% 114 to 80 mg/dl (30%)ASCOT-DM (215) 1° Atorvastatin 10 mg vs. placebo 11.1 to 10.2% 8% 0.9% 125 to 82 mg/dl (34%)
Studies were of differing lengths (3.3–5.4 years) and used somewhat different outcomes, but all reported rates of CVD death and non-fatal MI. In this tabulation,results of the statin on 10-year risk of major CVD endpoints (CHD death/non-fatal MI) are listed for comparison between studies. Correlation between 10-year CVDrisk of the control group and the absolute risk reduction with statin therapy is highly significant (P 0.0007). Analyses provided by Craig Williams, PharmD, OregonHealth & Science University, 2007.
Table 13—Summary of recommendationsfor glycemic, blood pressure, and lipid controlfor adults with diabetes
A1C �7.0%*Blood pressure �130/80 mmHgLipids
LDL cholesterol �100 mg/dl (�2.6mmol/l)†
*Referenced to a nondiabetic range of 4.0–6.0%using a DCCT-based assay. †In individuals withovert CVD, a lower LDL cholesterol goal of �70mg/dl (1.8 mmol/l), using a high dose of a statin, isan option.
Position Statement
care.diabetesjournals.org DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 S31

(e.g., multiple cardiovascular risk factorsor long duration of diabetes). Very littleclinical trial evidence exists for type 2 di-abetic patients under the age of 40 yearsand for type 1 diabetic patients of any age.In the Heart Protection Study (lower agelimit 40 years), the subgroup of 600 pa-tients with type 1 diabetes had a propor-tionately similar reduction in risk aspatients with type 2 diabetes although notstatistically significant (212). Althoughthe data are not definitive, considerationshould be given to lipid-lowering goalsfor type 1 diabetic patients similar tothose for type 2 diabetic patients, partic-ularly if other cardiovascular risk factorsare present.c. Alternative LDL cholesterol goals.Virtually all trials of statins and CVD out-come have tested specific doses of statinsagainst placebo, other doses of statin, orother statins, rather than aiming for spe-cific LDL cholesterol goals (223). As canbe seen in Table 10, placebo-controlledtrials generally achieved LDL cholesterolreductions of 30 – 40% from baseline.Hence, LDL cholesterol lowering of thismagnitude is an acceptable outcome forpatients who cannot reach LDL choles-terol goals due to severe baseline eleva-t ions in LDL choles tero l and/orintolerance of maximal, or any, statindoses. Additionally, for those with base-line LDL cholesterol minimally �100 mg/dl, prescribing statin therapy to lowerLDL cholesterol to �30–40% from base-line is probably more effective than pre-scr ibing just enough to get LDLcholesterol slightly �100 mg/dl.
Recent clinical trials in high-risk pa-tients, such as those with acute coronarysyndromes or previous cardiovascularevents (224 –226), have demonstratedthat more aggressive therapy with highdoses of statins to achieve an LDL choles-terol of �70 mg/dl led to a significant re-duction in further events. Therefore, areduction in LDL cholesterol to a goal of�70 mg/dl is an option in very-high-riskdiabetic patients with overt CVD (227).
In individual patients, LDL choles-terol lowering with statins is highly vari-able, and this variable response is poorlyunderstood (228). Reduction of CVDevents with statins correlates very closelywith LDL cholesterol lowering (229).When maximally tolerated doses of st-atins fail to significantly lower LDL cho-lesterol (�30% reduction from patientsbaseline), the primary aim of combinationtherapy should be to achieve additionalLDL cholesterol lowering. Niacin, fenofi-
brate, ezetimibe, and bile acid seques-trants all offer additional LDL cholesterollowering. The evidence that combinationtherapy provides a significant incrementin CVD risk reduction over statin therapyalone is still elusive.d. Treatment of other lipoprotein frac-tions or targets. Severe hypertriglyceri-demia may warrant immediate therapy ofthis abnormality with lifestyle and usuallypharmacologic therapy (fibric acid deriv-ative or niacin) to reduce the risk of acutepancreatitis. In the absence of severe hy-pertriglyceridemia, therapy targetingHDL cholesterol or triglycerides has intu-itive appeal but lacks the evidence base ofstatin therapy (186). If the HDL choles-terol is �40 mg/dl and the LDL choles-terol is 100–129 mg/dl, gemfibrozil orniacin might be used, especially if a pa-tient is intolerant to statins. Niacin is themost effective drug for raising HDL cho-lesterol. It can significantly increase bloodglucose at high doses, but recent studiesdemonstrate that at modest doses (750–2,000 mg/day), significant improvementsin LDL cholesterol, HDL cholesterol, andtriglyceride levels are accompanied byonly modest changes in glucose that aregenerally amenable to adjustment of dia-betes therapy (230,231).
Combination therapy with a statinand a fibrate or a statin and niacin may beefficacious for treatment of all three lipidfractions, but this combination is associ-ated with an increased risk for abnormaltransaminase levels, myositis, or rhabdo-myolysis. The risk of rhabdomyolysis ishigher with higher doses of statins andwith renal insufficiency and seems to belower when statins are combined with fe-nofibrate than gemfibrozil (232). Severalongoing trials may provide much-neededevidence for the effects of combinationtherapy on cardiovascular outcomes.
In 2008, a consensus panel convenedby ADA and the American College of Car-diology (ACC) recommended a greaterfocus on non-HDL cholesterol and apolipoprotein B (apo B) in patients who arelikely to have small LDL particles, such aspeople with diabetes (233). The consen-sus panel suggested that for statin-treatedpatients in whom the LDL cholesterolgoal would be �70 mg/dl (non-HDL cho-lesterol �100 mg/dl), apo B should bemeasured and treated to �80 mg/dl. Forpatients on statins with an LDL choles-terol goal of �100 mg/dl (non-HDL cho-lesterol �130 mg/dl), apo B should bemeasured and treated to �90 mg/dl.
For a summary of recommendations
for glycemic, blood pressure, and lipidcontrol for adults with diabetes, see Table13.
3. Antiplatelet agents
Recommendations● Consider aspirin therapy (75–162 mg/
day) as a primary prevention strategy inthose with type 1 or type 2 diabetes atincreased cardiovascular risk (10-yearrisk �10%). This includes most men�50 years of age or women �60 yearsof age who have at least one additionalmajor risk factor (family history ofCVD, hypertension, smoking, dyslipi-demia, or albuminuria). (C)
● There is not sufficient evidence to rec-ommend aspirin for primary preven-tion in lower risk individuals, such asmen �50 years of age or women �60years of age without other major riskfactors. For patients in these age-groupswith multiple other risk factors, clinicaljudgment is required. (C)
● Use aspirin therapy (75–162 mg/day)as a secondary prevention strategy inthose with diabetes with a history ofCVD. (A)
● For patients with CVD and docu-mented aspirin allergy, clopidogrel (75mg/day) should be used. (B)
● Combination therapy with ASA (75–162 mg/day) and clopidogrel (75 mg/day) is reasonable for up to a year afteran acute coronary syndrome. (B)
ADA and the American Heart Association(AHA) have, in the past, jointly recom-mended that low-dose aspirin therapy beused as a primary prevention strategy inthose with diabetes at increased cardio-vascular risk, including those who areover 40 years of age or those with addi-tional risk factors (family history of CVD,hypertension, smoking, dyslipidemia, oralbuminuria) (235). These recommenda-tions were derived from several older tri-als that included small numbers ofpatients with diabetes.
Aspirin has been shown to be effec-tive in reducing cardiovascular morbidityand mortality in high-risk patients withprevious MI or stroke (secondary preven-tion). Its net benefit in primary preven-tion among patients with no previouscardiovascular events is more controver-sial, both for patients with and withouta history of diabetes (236). The U.S.Preventive Services Task Force recentlyupdated its evidence base and recommen-dations about aspirin use for primary pre-
Standards of Medical Care
S32 DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 care.diabetesjournals.org

vention (237,238). The Task Forcerecommended encouraging aspirin use inmen 45–79 and women 55–79 years ofage and not encouraging aspirin use inyounger adults and did not differentiatebased on the presence or absence ofdiabetes.
Two recent randomized controlledtrials of aspirin specifically in patientswith diabetes failed to show a significantreduction in CVD end points, raising fur-ther questions about the efficacy of aspi-rin for primary prevention in people withdiabetes (239,240). In 2009, ADA AHA,and ACC convened a group of experts toreview and synthesize the available evi-dence and use this information to createan updated recommendation. Their re-port, including analyses in addition tothose described below, will be publishedin early 2010.
The ATT (Anti-Thrombotic Trialists’)collaborators recently published an indi-vidual patient-level meta-analysis of thesix large trials of aspirin for primary pre-vention in the general population (236).These trials collectively enrolled over95,000 participants, including almost4,000 with diabetes. Overall, they foundthat aspirin reduced the risk of vascularevents by 12% (RR 0.88 [95% CI 0.82–0.94]). The largest reduction was for non-fatal MI (0.77 [0.67–0.89]). Aspirin hadlittle effect on CHD death (0.95 [0.78–1.15]) or total stroke (0.95 [0.85–1.06]).The net effect on total stroke reflected arelative reduction in risk of ischemicstroke (�14%) and a relative increasedrisk of hemorrhagic stroke (32%).There was some evidence of a differencein aspirin effect by sex. Aspirin reducedCHD events in men (0.77 [0.67–0.89])but not in women (0.95 [0.77–1.17]).Conversely, aspirin had no effect onstroke in men (1.01 [0.74–1.39]) but re-duced stroke in women (0.77 [0.59 –0.99]). These potential differences ineffect by sex were of borderline statisticalsignificance, were affected strongly by theresults of one trial, and cannot be consid-ered definitive. Notably, sex differences inaspirin’s effects have not been observed instudies of secondary prevention (236). Inthe six trials examined by the ATT collab-orators, the effect of aspirin on major vas-cular events was similar for patients withand without diabetes (0.88 [0.67–1.15]and 0.87 [0.79–0.96], respectively). TheCI was wider for those with diabetes be-cause of their smaller number.
Based on the currently available evi-dence, aspirin appears to have a modesteffect on ischemic vascular events withthe absolute decrease in events dependingon the underlying CVD risk. The mainadverse effects appear to be an increasedrisk of gastrointestinal bleeding. The ex-cess risk may be as high as 1–5 per 1,000per year in real-world settings. In adultswith CVD risk greater than 1% per year,the number of CVD events prevented willbe similar to or greater than the number ofepisodes of bleeding induced, althoughthese complications do not have equal ef-fects on long-term health (241).
Average daily dosages used in mostclinical trials involving patients with dia-betes ranged from 50–650 mg but weremostly in the range of 100–325 mg/day.There is little evidence to support any spe-cific dose, but using the lowest possibledosage may help reduce side effects(242). Although platelets from patientswith diabetes have altered function, it isunclear what, if any, impact that findinghas on the required dose of aspirin forcardioprotective effects in the patientwith diabetes. Many alternate pathwaysfor platelet activation exist that are inde-pendent of thromboxane A2 and thus notsensitive to the effects of aspirin (243).Therefore, while “aspirin resistance” ap-pears higher in diabetic patients whenmeasured by a variety of ex vivo and invitro methods (platelet aggrenometry,measurement of thromboxane B2), theseobservations alone are insufficient to em-pirically recommend at this time thathigher doses of aspirin be used in the di-abetic patient (244–246).
Aspirin use for secondary preventioncontinues to have a strong evidence baseand is recommended. Until further evi-dence is available, low-dose (75–162 mg/day) aspirin use for primary prevention isreasonable for adults with diabetes and noprevious history of vascular disease whoare at increased CVD risk (10-year risk ofCVD events �10%) and who are not atincreased risk for bleeding. This generallyincludes most men over age 50 years andwomen over age 60 years who also haveone or more of the following major riskfactors: smoking, hypertension, dyslipi-demia, family history of premature CVD,and albuminuria.
Aspirin should not be recommendedfor those at low CVD risk (women underage 60 years and men under age 50 yearswith no major CVD risk factors; 10-yearCVD risk �5%), as the low benefit is off-
set by the incidence of significant bleed-ing. Clinical judgment should be used forthose at intermediate risk (younger pa-tients with one or risk factors or older pa-tients with no risk factors; those with 10-year CVD risk 5–10%) until furtherresearch is available. Use of aspirin in pa-tients under the age of 21 years is contra-indicated due to the associated risk ofReye’s syndrome.
Clopidogrel has been demonstratedto reduce CVD events in diabetic individ-uals (247). It is recommended as adjunc-tive therapy in the 1st year after an acutecoronary syndrome or as alternative ther-apy in aspirin-intolerant patients.
4. Smoking cessation
Recommendations● Advise all patients not to smoke. (A)● Include smoking cessation counseling
and other forms of treatment as a rou-tine component of diabetes care. (B)
Issues of smoking and diabetes are reviewedin detail in the ADA technical review (248)and position statement (249) on this topic.A large body of evidence from epidemiolog-ical, case-control, and cohort studies pro-vides convincing documentation of thecausal link between cigarette smoking andhealth risks. Cigarette smoking contributesto one of every five deaths in the U.S. and isthe most important modifiable cause of pre-mature death. Much of the prior work doc-umenting the impact of smoking on healthdid not separately discuss results on subsetsof individuals with diabetes, suggesting thatthe identified risks are at least equivalent tothose found in the general population.Other studies of individuals with diabetesconsistently found a heightened risk ofCVD and premature death among smokers.Smoking is also related to the premature de-velopment of microvascular complicationsof diabetes and may have a role in the de-velopment of type 2 diabetes.
A number of large randomized clini-cal trials have demonstrated the efficacyand cost-effectiveness of smoking cessa-tion counseling in changing smoking be-havior and reducing tobacco use. Theroutine and thorough assessment of to-bacco use is important as a means of pre-vent ing smoking or encouragingcessation. Special considerations shouldinclude assessment of level of nicotine de-pendence, which is associated with diffi-culty in quitting and relapse (250,251).
Position Statement
care.diabetesjournals.org DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 S33
5. Coronary heart disease screeningand treatment
Recommendations
Screening● In asymptomatic patients, evaluate risk
factors to stratify patients by 10-yearrisk, and treat risk factors accordingly.(B)
Treatment● In patients with known CVD, ACE in-
hibitor (C), aspirin (A), and statin ther-apy (A) (if not contraindicated) shouldbe used to reduce the risk of cardiovas-cular events.
● In patients with a prior MI, �-blockersshould be continued for at least 2 yearsafter the event. (B)
● Longer-term use of �-blockers in theabsence of hypertension is reasonable ifwell tolerated, but data are lacking. (E)
● Avoid thiazolidinedione (TZD) treat-ment in patients with symptomaticheart failure. (C)
● Metformin may be used in patients withstable CHF if renal function is normal.It should be avoided in unstable or hos-pitalized patients with CHF. (C)
Screening for CAD is reviewed in a re-cently updated consensus statement (93).To identify the presence of CAD in dia-betic patients without clear or suggestivesymptoms, a risk factor–based approachto the initial diagnostic evaluation andsubsequent follow-up has intuitive ap-peal. However, recent studies concludedthat using this approach fails to identifywhich patients will have silent ischemiaon screening tests (159,252).
Candidates for cardiac testing includethose with 1) typical or atypical cardiacsymptoms and 2) an abnormal restingelectrocardiogram (ECG). The screeningof asymptomatic patients remains contro-versial, especially since intensive medicaltherapy, indicated in diabetic patients athigh risk for CVD, has an increasing evi-dence base for providing equal outcomesto invasive revascularization, including indiabetic patients (253,254). There is alsorecent preliminary evidence that silentmyocardial ischemia may reverse overtime, adding to the controversy concern-ing aggressive screening strategies (255).Finally, a recent randomized observa-tional trial demonstrated no clinical ben-efit to routine screening of asymptomaticpatients with type 2 diabetes and normalECGs (256). Despite abnormal myocar-
dial perfusion imaging in more than onein five patients, cardiac outcomes were es-sentially equal (and very low) in screenedversus unscreened patients. Accordingly,the overall effectiveness, especially thecost-effectiveness, of such an indiscrimi-nate screening strategy is in question.
In all patients with diabetes, cardio-vascular risk factors should be assessed atleast annually. These risk factors includedyslipidemia, hypertension, smoking, apositive family history of premature cor-onary disease, and the presence of micro-or macroalbuminuria. Abnormal riskfactors should be treated as describedelsewhere in these guidelines. Patients atincreased CHD risk should receive aspirinand a statin, and ACE inhibitor, or ARBtherapy if hypertensive, unless there arecontraindications to a particular drugclass. While clear benefit exists for ACEinhibitor and ARB therapy in patientswith nephropathy or hypertension, thebenefits in patients with CVD in the ab-sence of these conditions is less clear,especially when LDL cholesterol is con-comitantly controlled (257,258).
B. Nephropathy screening andtreatment
Recommendations
General recommendations● To reduce the risk or slow the progres-
sion of nephropathy, optimize glucosecontrol. (A)
● To reduce the risk or slow the progres-sion of nephropathy, optimize bloodpressure control. (A)
Screening● Perform an annual test to assess urine
albumin excretion in type 1 diabetic pa-tients with diabetes duration of 5 yearsand in all type 2 diabetic patients, start-ing at diagnosis. (E)
● Measure serum creatinine at least annu-ally in all adults with diabetes regard-less of the degree of urine albuminexcretion. The serum creatinine shouldbe used to estimate GFR and stage thelevel of chronic kidney disease (CKD),if present. (E)
Treatment● In the treatment of the nonpregnant pa-
tient with micro- or macroalbuminuria,either ACE inhibitors or ARBs shouldbe used. (A)
● While there are no adequate head-to-head comparisons of ACE inhibitors
and ARBs, there is clinical trial supportfor each of the following statements:● In patients with type 1 diabetes, hy-
pertension, and any degree of albu-minuria, ACE inhibitors have beenshown to delay the progression of ne-phropathy. (A)
● In patients with type 2 diabetes, hy-pertension, and microalbuminuria,both ACE inhibitors and ARBs havebeen shown to delay the progressionto macroalbuminuria. (A)
● In patients with type 2 diabetes, hy-pertension, macroalbuminuria, andrenal insufficiency (serum creatinine�1.5 mg/dl), ARBs have been shownto delay the progression of nephrop-athy. (A)
● If one class is not tolerated, the othershould be substituted. (E)
● Reduction of protein intake to 0.8–1.0g � kg body wt–1 � day–1 in individualswith diabetes and the earlier stages ofCKD and to 0.8 g � kg body wt–1 � day–1
in the later stages of CKD may improvemeasures of renal function (urine albu-min excretion rate and GFR) and is rec-ommended. (B)
● When ACE inhibitors, ARBs, or diuret-ics are used, monitor serum creatinineand potassium levels for the develop-ment of acute kidney disease and hy-perkalemia. (E)
● Continued monitoring of urine albu-min excretion to assess both responseto therapy and progression of disease isrecommended. (E)
● Consider referral to a physician experi-enced in the care of kidney diseasewhen there is uncertainty about the eti-ology of kidney disease (active urinesediment, absence of retinopathy, orrapid decline in GFR), difficult manage-ment issues, or advanced kidney dis-ease. (B)
Diabetic nephropathy occurs in 20–40%of patients with diabetes and is the singleleading cause of end-stage renal disease(ESRD). Persistent albuminuria in therange of 30–299 mg/24 h (microalbu-minuria) has been shown to be the earlieststage of diabetic nephropathy in type 1diabetes and a marker for development ofnephropathy in type 2 diabetes. Mi-croalbuminuria is also a well-establishedmarker of increased CVD risk (259,260).Patients with microalbuminuria whoprogress to macroalbuminuria (�300mg/24 h) are likely to progress to ESRD(261,262). However, a number of inter-ventions have been demonstrated to re-
Standards of Medical Care
S34 DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 care.diabetesjournals.org

duce the risk and slow the progression ofrenal disease.
Intensive diabetes managementwith the goal of achieving near-normoglycemia has been shown in largeprospective randomized studies to de-lay the onset of microalbuminuria andthe progression of micro- to macroalbu-minuria in pat ients with type 1(263,264) and type 2 (57,58) diabetes.The UKPDS provided strong evidencethat control of blood pressure can re-duce the development of nephropathy(187). In addition, large prospectiverandomized studies in patients withtype 1 diabetes have demonstrated thatachievement of lower levels of systolicblood pressure (�140 mmHg) resultingfrom treatment using ACE inhibitorsprovides a selective benefit over otherantihypertensive drug classes in delay-ing the progression from micro- to mac-roalbuminuria and can slow the declinein GFR in patients with macroalbumin-uria (205,206,265). In type 2 diabeteswith hypertension and normoalbuminuria,RAS inhibition has been demonstrated todelay onset of microalbuminuria (266).
In addition, ACE inhibitors have beenshown to reduce major CVD outcomes(i.e., MI, stroke, and death) in patientswith diabetes (199), thus further support-ing the use of these agents in patients withmicroalbuminuria, a CVD risk factor.ARBs do not prevent microalbuminuria innormotensive patients with type 1 or type2 diabetes (267,268); however, ARBshave been shown to reduce the rate ofprogression from micro- to macroalbu-minuria as well as ESRD in patients withtype 2 diabetes (269 –271). Some evi-dence suggests that ARBs have a smallermagnitude of rise in potassium comparedwith ACE inhibitors in people with ne-phropathy (272,273). It is important tonote that both ACE inhibitors and ARBsreduce loss of kidney function in peoplewith diabetic nephropathy, above and be-yond any such effect attributable to a re-duction in systemic blood pressure.Combinations of drugs that block the ren-nin-angiotensin-aldosterone system (e.g.,an ACE inhibitor plus an ARB, a miner-alocorticoid antagonist, or a direct renininhibitor) have been shown to provide ad-ditional lowering of albuminuria (274–277). However, the long-term effects ofsuch combinations on renal or cardiovas-cular outcomes have not yet been evalu-ated in clinical trials.
Other drugs, such as diuretics, cal-cium channel blockers, and �-blockers,
should be used as additional therapy tofurther lower blood pressure in patientsalready treated with ACE inhibitors orARBs (204) or as alternate therapy in therare individual unable to tolerate ACE in-hibitors or ARBs.
Studies in patients with varying stagesof nephropathy have shown that proteinrestriction helps slow the progression ofalbuminuria, GFR decline, and occur-rence of ESRD (278 –281). Protein re-s t r i c t i on shou ld be cons ide redparticularly in patients whose nephropa-thy seems to be progressing despite opti-mal glucose and blood pressure controland use of ACE inhibitor and/or ARBs(281).
Assessment of albuminuria statusand renal functionScreening for microalbuminuria can beperformed by measurement of the albu-min-to-creatinine ratio in a random spotcollection (preferred method); 24-h ortimed collections are more burdensomeand add little to prediction or accuracy(282,283). Measurement of a spot urinefor albumin only, whether by immunoas-say or by using a dipstick test specific formicroalbumin, without simultaneouslymeasuring urine creatinine, is somewhatless expensive but susceptible to false-negative and -positive determinations as aresult of variation in urine concentrationdue to hydration and other factors.
Abnormalities of albumin excretionare defined in Table 14. Because of vari-ability in urinary albumin excretion, twoof three specimens collected within a 3- to6-month period should be abnormal be-fore considering a patient to have crossedone of these diagnostic thresholds. Exer-cise within 24 h, infection, fever, CHF,marked hyperglycemia, and marked hy-pertension may elevate urinary albuminexcretion over baseline values.
Information on presence of abnormalurine albumin excretion in addition tolevel of GFR may be used to stage CKD.The National Kidney Foundation classifi-
cation (Table 15) is primarily based onGFR levels and therefore differs fromother systems, in which staging is basedprimarily on urinary albumin excretion(284). Studies have found decreased GFRin the absence of increased urine albuminexcretion in a substantial percentage ofadults with diabetes (285,286). Epidemi-ologic evidence suggests that a substantialfraction of those with CKD in the settingof diabetes have little or no detectable al-buminuria (285). Serum creatinineshould therefore be measured at least an-nually in all adults with diabetes, regard-less of the degree of urine albuminexcretion.
Serum creatinine should be used toestimate GFR and to stage the level ofCKD, if present. Estimated GFR (eGFR) iscommonly co-reported by laboratories orcan be estimated using formulae such asthe Modification of Diet in Renal Disease(MDRD) study equation (287). Recent re-ports have indicated that the MDRD ismore accurate for the diagnosis and strat-ification of CKD in patients with diabetesthan the Cockcroft-Gault formula (288).GFR calculators are available at http://www.nkdep.nih.gov.
The role of continued annual quanti-tative assessment of albumin excretion af-ter diagnosis of microalbuminuria andinstitution of ACE inhibitor or ARB ther-apy and blood pressure control is unclear.Continued surveillance can assess bothresponse to therapy and progression ofdisease. Some suggest that reducing ab-normal albuminuria (�30 mg/g) to thenormal or near-normal range may im-prove renal and cardiovascular prognosis,but this approach has not been formallyevaluated in prospective trials.
Complications of kidney disease cor-relate with level of kidney function. Whenthe eGFR is less than 60 ml � min/1.73 m2,screening for anemia, malnutrition, andmetabolic bone disease is indicated. Earlyvaccination against Hepatitis B is indi-cated in patients likely to progress to end-stage kidney disease.
Consider referral to a physician expe-rienced in the care of kidney disease whenthere is uncertainty about the etiology ofkidney disease (active urine sediment, ab-sence of retinopathy, or rapid decline inGFR), difficult management issues, or ad-vanced kidney disease. The threshold forreferral may vary depending on the fre-quency with which a provider encountersdiabetic patients with significant kidneydisease. Consultation with a nephrologistwhen stage 4 CKD develops has been
Table 14—Definitions of abnormalities in al-bumin excretion
Category
Spot collection(�g/mg
creatinine)
Normal �30Microalbuminuria 30–299Macroalbuminuria (clinical) �300
Position Statement
care.diabetesjournals.org DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 S35

found to reduce cost, improve quality ofcare, and keep people off dialysis longer(289,290). However, nonrenal specialistsshould not delay educating their patientsabout the progressive nature of diabetickidney disease, the renal preservationbenefits of aggressive treatment of bloodpressure, blood glucose, and hyperlipid-emia, and the potential need for renal re-placement therapy.
C. Retinopathy screening andtreatment
Recommendations
General recommendations● To reduce the risk or slow the progres-
sion of retinopathy, optimize glycemiccontrol. (A)
● To reduce the risk or slow the progres-sion of retinopathy, optimize bloodpressure control. (A)
Screening● Adults and children aged 10 years or
older with type 1 diabetes should havean initial dilated and comprehensiveeye examination by an ophthalmologistor optometrist within 5 years after theonset of diabetes. (B)
● Patients with type 2 diabetes shouldhave an initial dilated and comprehen-sive eye examination by an ophthalmol-ogist or optometrist shortly after thediagnosis of diabetes. (B)
● Subsequent examinations for type 1and type 2 diabetic patients should berepeated annually by an ophthalmolo-gist or optometrist. Less frequent exams(every 2–3 years) may be consideredfollowing one or more normal eye ex-ams. Examinations will be requiredmore frequently if retinopathy is pro-gressing. (B)
● High-quality fundus photographs candetect most clinically significant dia-
betic retinopathy. Interpretation of theimages should be performed by atrained eye care provider. While retinalphotography may serve as a screeningtool for retinopathy, it is not a substi-tute for a comprehensive eye exam,which should be performed at least ini-tially and at intervals thereafter as rec-ommended by an eye care professional.(E)
● Women with preexisting diabetes whoare planning pregnancy or who havebecome pregnant should have a com-prehensive eye examination and becounseled on the risk of developmentand/or progression of diabetic retinop-athy. Eye examination should occur inthe first trimester with close follow-upthroughout pregnancy and for 1 yearpostpartum. (B)
Treatment● Promptly refer patients with any level of
macular edema, severe NPDR, or anyPDR to an ophthalmologist who isknowledgeable and experienced in themanagement and treatment of diabeticretinopathy. (A)
● Laser photocoagulation therapy is indi-cated to reduce the risk of vision loss inpatients with high-risk PDR, clinicallysignificant macular edema, and in somecases of severe NPDR. (A)
● The presence of retinopathy is not acontraindication to aspirin therapy forcardioprotection, as this therapy doesnot increase the risk of retinal hemor-rhage. (A)
Diabetic retinopathy is a highly specificvascular complication of both type 1 andtype 2 diabetes, with prevalence stronglyrelated to duration of diabetes. Diabeticretinopathy is the most frequent cause ofnew cases of blindness among adults aged20–74 years. Glaucoma, cataracts, and
other disorders of the eye occur earlierand more frequently in people withdiabetes.
In addition to duration of diabetes,other factors that increase the risk of, orare associated with, retinopathy includechronic hyperglycemia (291), the pres-ence of nephropathy (292), and hyper-tension (293). Intensive diabetesmanagement with the goal of achievingnear normoglycemia has been shown inlarge prospective randomized studies toprevent and/or delay the onset and pro-gress ion of diabet ic re t inopathy(53,57,58). Lowering blood pressure hasbeen shown to decrease the progressionof retinopathy (187). Several case seriesand a controlled prospective study sug-gest that pregnancy in type 1 diabetic pa-t ients may aggravate ret inopathy(294,295); laser photocoagulation sur-gery can minimize this risk (295).
One of the main motivations forscreening for diabetic retinopathy is theestablished efficacy of laser photocoagu-lation surgery in preventing vision loss.Two large trials, the Diabetic RetinopathyStudy (DRS) and the Early Treatment Di-abetic Retinopathy Study (ETDRS), pro-vide the strongest support for thetherapeutic benefits of photocoagulationsurgery.
The DRS (296) showed that panreti-nal photocoagulation surgery reduced therisk of severe vision loss from PDR from15.9% in untreated eyes to 6.4% intreated eyes. The benefit was greatestamong patients whose baseline evalua-tion revealed high-risk characteristics(chiefly disc neovascularization or vitre-ous hemorrhage). Given the risks of mod-est loss of visual acuity and contraction ofthe visual field from panretinal laser sur-gery, such therapy is primarily recom-mended for eyes with PDR approachingor having high-risk characteristics.
The ETDRS (297) established thebenefit of focal laser photocoagulationsurgery in eyes with macular edema,particularly those with clinically signif-icant macular edema, with reduction ofdoubling of the visual angle (e.g., 20/50 –20/100) from 20% in untreatedeyes to 8% in treated eyes. The ETDRSalso verified the benefits of panretinalphotocoagulation for high-risk PDR,but not for mild or moderate NPDR. Inolder-onset patients with severe NPDRor less-than-high-risk PDR, the risk ofsevere vision loss or vitrectomy was re-duced 50% by early laser photocoagu-lation surgery at these stages.
Table 15—Stages of CKD
Stage Description
GFR (ml/min per1.73 m2 bodysurface area)
1 Kidney damage* with normal or increased GFR �902 Kidney damage* with mildly decreased GFR 60–893 Moderately decreased GFR 30–594 Severely decreased GFR 15–295 Kidney failure �15 or dialysis
*Kidney damage defined as abnormalities on pathologic, urine, blood, or imaging tests. Adapted from ref.283.
Standards of Medical Care
S36 DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 care.diabetesjournals.org

Laser photocoagulation surgery inboth trials was beneficial in reducing therisk of further vision loss, but generallynot beneficial in reversing already dimin-ished acuity. This preventive effect andthe fact that patients with PDR or macularedema may be asymptomatic providestrong support for a screening program todetect diabetic retinopathy.
As retinopathy is estimated to take atleast 5 years to develop after the onset ofhyperglycemia (298), patients with type 1diabetes should have an initial dilated andcomprehensive eye examination within 5years after the onset of diabetes. Patientswith type 2 diabetes who generally havehad years of undiagnosed diabetes (299)and who have a significant risk of preva-lent diabetic retinopathy at the time ofdiabetes diagnosis should have an initialdilated and comprehensive eye examina-tion soon after diagnosis. Examinationsshould be performed by an ophthalmolo-gist or optometrist who is knowledgeableand experienced in diagnosing the pres-ence of diabetic retinopathy and is awareof its management. Subsequent examina-tions for type 1 and type 2 diabetic pa-tients are generally repeated annually.Less frequent exams (every 2–3 years)may be cost effective after one or morenormal eye exams (300–302), while ex-aminations will be required more fre-quently if retinopathy is progressing.
Examinations can also be done withretinal photographs (with or without di-lation of the pupil) read by experiencedexperts. In-person exams are still nec-essary when the photos are unaccept-able and for follow-up of abnormalitiesdetected. Photos are not a substitute fora comprehensive eye exam, whichshould be performed at least initiallyand at intervals thereafter as recom-mended by an eye care professional.This technology has great potential inareas where qualified eye care profes-sionals are not available and may alsoenhance efficiency and reduce costswhen the expertise of ophthalmologistscan be used for more complex examina-tions and for therapy (303).
Results of eye examinations shouldbe documented and transmitted to thereferring health care professional. For adetailed review of the evidence and fur-ther discussion of diabetic retinopathy,see the ADA technical review andposition statement on this subject(304,305).
D. Neuropathy screening andtreatment (306)
Recommendations● All patients should be screened for dis-
tal symmetric polyneuropathy (DPN) atdiagnosis and at least annually thereaf-ter using simple clinical tests. (B)
● Electrophysiological testing is rarelyneeded, except in situations where theclinical features are atypical. (E)
● Screening for signs and symptoms ofcardiovascular autonomic neuropathyshould be instituted at diagnosis of type2 diabetes and 5 years after the diagno-sis of type 1 diabetes. Special testing israrely needed and may not affect man-agement or outcomes. (E)
● Medications for the relief of specificsymptoms related to DPN and auto-nomic neuropathy are recommended,as they improve the quality of life of thepatient. (E)
The diabetic neuropathies are heteroge-neous with diverse clinical manifesta-tions. They may be focal or diffuse. Mostcommon among the neuropathies arechronic sensorimotor DPN and auto-nomic neuropathy. Although DPN is adiagnosis of exclusion, complex investi-gations to exclude other conditions arerarely needed.
The early recognition and appropri-ate management of neuropathy in the pa-tient with diabetes is important for anumber of reasons: 1) nondiabetic neu-ropathies may be present in patients withdiabetes and may be treatable; 2) a num-ber of treatment options exist for symp-tomatic diabetic neuropathy; 3) up to50% of DPN may be asymptomatic, andpatients are at risk of insensate injury totheir feet; 4) autonomic neuropathy mayinvolve every system in the body; and 5)cardiovascular autonomic neuropathycauses substantial morbidity and mortal-ity. Specific treatment for the underlyingnerve damage is not currently available,other than improved glycemic control,which may slow progression but not re-verse neuronal loss. Effective symptom-atic treatments are available for somemanifestations of DPN and autonomicneuropathy.
1. Diagnosis of neuropathy
a. Distal symmetric polyneuropathy.Patients with diabetes should be screenedannually for DPN using tests such as pin-prick sensation, vibration perception (us-ing a 128-Hz tuning fork), 10-g
monofilament pressure sensation at thedistal plantar aspect of both great toes andmetatarsal joints, and assessment of anklereflexes. Combinations of more than onetest have �87% sensitivity in detectingDPN. Loss of 10-g monofilament percep-tion and reduced vibration perceptionpredict foot ulcers (306).b. Diabetic autonomic neuropathy (307).The symptoms and signs of autonomicdysfunction should be elicited carefullyduring the history and physical examina-tion. Major clinical manifestations of dia-betic autonomic neuropathy includeresting tachycardia, exercise intolerance,orthostatic hypotension, constipation,gastroparesis, erectile dysfunction, sudo-motor dysfunction, impaired neurovas-cular function, “brittle diabetes,” andhypoglycemic autonomic failure.
Cardiovascular autonomic neuropa-thy, a CVD risk factor (93), is the moststudied and clinically important form ofdiabetic autonomic neuropathy. Cardio-vascular autonomic neuropathy may beindicated by resting tachycardia (�100bpm), orthostasis (a fall in systolic bloodpressure �20 mmHg upon standingwithout an appropriate heart rate re-sponse), or other disturbances in auto-nomic nervous system function involvingthe skin, pupils, or gastrointestinal andgenitourinary systems.
Gastrointestinal neuropathies (e.g.,esophageal enteropathy, gastroparesis,constipation, diarrhea, and fecal incon-tinence) are common, and any sectionof the gastrointestinal tract may be af-fected. Gastroparesis should be sus-pected in individuals with erraticglucose control or with upper gastroin-testinal symptoms without other identi-fied cause. Evaluation of solid-phasegastric emptying using double-isotopescintigraphy may be done if symptomsare suggestive, but test results often cor-relate poorly with symptoms. Constipa-t ion is the most common lower-gastrointestinal symptom but canalternate with episodes of diarrhea.
Diabetic autonomic neuropathy isalso associated with genitourinary tractdisturbances. In men, diabetic autonomicneuropathy may cause erectile dysfunc-tion and/or retrograde ejaculation. Evalu-ation of bladder dysfunction should beperformed for individuals with diabeteswho have recurrent urinary tract infec-tions, pyelonephritis, incontinence, or apalpable bladder.
Position Statement
care.diabetesjournals.org DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 S37

2. Symptomatic treatments
a. Distal symmetric polyneuropathy.The first step in management of patientswith DPN should be to aim for stable andoptimal glycemic control. Although con-trolled trial evidence is lacking, severalobservational studies suggest that neuro-pathic symptoms improve not only withoptimization of control, but also with theavoidance of extreme blood glucose fluc-tuations. Patients with painful DPN maybenefit from pharmacological treatmentof their symptoms: many agents have ef-ficacy confirmed in published random-ized controlled trials, with several FDA-approved for the management of painfulDPN. See Table 16 for examples of agentsto treat DPN pain.b. Diabetic autonomic neuropathy. Gas-troparesis symptoms may improve withdietary changes and prokinetic agentssuch as metoclopramide or erythromycin.Treatments for erectile dysfunction mayinclude phosphodiesterase type 5 inhibi-tors, intracorporeal or intraurethral pros-taglandins, vacuum devices, or penileprostheses. Interventions for other mani-festations of autonomic neuropathy aredescribed in the ADA statement on neu-ropathy (306). As with DPN treatments,these interventions do not change the un-derlying pathology and natural history ofthe disease process but may have a posi-tive impact on the quality of life of thepatient.
E. Foot care
Recommendations● For all patients with diabetes, perform
an annual comprehensive foot exami-nation to identify risk factors predictiveof ulcers and amputations. The foot ex-amination should include inspection,assessment of foot pulses, and testing
for loss of protective sensation (LOPS)(10-g monofilament plus testing anyone of: vibration using 128-Hz tuningfork, pinprick sensation, ankle reflexes,or vibration perception threshold). (B)
● Provide general foot self-care educationto all patients with diabetes. (B)
● A multidisciplinary approach is recom-mended for individuals with foot ulcersand high-risk feet, especially those witha history of prior ulcer or amputation.(B)
● Refer patients who smoke, have LOPSand structural abnormalities, or havehistory of prior lower-extremity com-plications to foot care specialists for on-going preventive care and life-longsurveillance. (C)
● Initial screening for peripheral arterialdisease (PAD) should include a historyfor claudication and an assessment ofthe pedal pulses. Consider obtaining anankle-brachial index (ABI), as many pa-tients with PAD are asymptomatic. (C)
● Refer patients with significant claudica-tion or a positive ABI for further vascu-lar assessment and consider exercise,medications, and surgical options. (C)
Amputation and foot ulceration, conse-quences of diabetic neuropathy and/orPAD, are common and major causes ofmorbidity and disability in people withdiabetes. Early recognition and manage-ment of risk factors can prevent or delayadverse outcomes.
The risk of ulcers or amputations isincreased in people who have the follow-ing risk factors:
● previous amputation● past foot ulcer history● peripheral neuropathy● foot deformity● peripheral vascular disease
● visual impairment● diabetic nephropathy (especially pa-
tients on dialysis)● poor glycemic control● cigarette smoking
Many studies have been published pro-posing a range of tests that might usefullyidentify patients at risk of foot ulceration,creating confusion among practitioners asto which screening tests should beadopted in clinical practice. An ADA taskforce was therefore assembled in 2008 toconcisely summarize recent literature inthis area and recommend what should beincluded in the comprehensive foot examfor adult patients with diabetes. Their rec-ommendations are summarized below,but clinicians should refer to the taskforce report (308) for further details andpractical descriptions of how to performcomponents of the comprehensive footexamination.
At least annually, all adults with dia-betes should undergo a comprehensivefoot examination to identify high-riskconditions. Clinicians should ask abouthistory of previous foot ulceration or am-putation, neuropathic or peripheral vas-cular symptoms, impaired vision, tobaccouse, and foot care practices. A general in-spection of skin integrity and musculo-skeletal deformities should be done in awell-lit room. Vascular assessment wouldinclude inspection and assessment ofpedal pulses.
The neurologic exam recommendedis designed to identify LOPS rather thanearly neuropathy. The clinical examina-tion to identify LOPS is simple and re-quires no expensive equipment. Fivesimple clinical tests (use of a 10-g mono-filament, vibration testing using a 128-Hztuning fork, tests of pinprick sensation,ankle reflex assessment, and testing vibra-tion perception threshold with a biothesi-ometer), each with evidence from well-conducted prospective clinical cohortstudies, are considered useful in the diag-nosis of LOPS in the diabetic foot. Thetask force agrees that any of the five testslisted could be used by clinicians to iden-tify LOPS, although ideally two of theseshould be regularly performed during thescreening exam—normally the 10-gmonofilament and one other test. One ormore abnormal tests would suggestLOPS, while at least two normal tests (andno abnormal test) would rule out LOPS.The last test listed, vibration assessmentusing a biothesiometer or similar instru-ment, is widely used in the U.S.; however,
Table 16—Table of drugs to treat symptomatic DPN
Class Examples Typical doses*
Tricyclic drugs Amitriptyline 10–75 mg at bedtimeNortriptyline 25–75 mg at bedtimeImipramine 25–75 mg at bedtime
Anticonvulsants Gabapentin 300–1,200 mg t.i.d.Carbamazepine 200–400 mg t.i.d.Pregabalin† 100 mg t.i.d.
5-Hydroxytryptamine andnorepinephrine uptakeinhibitor
Duloxetine† 60–120 mg daily fs
Substance P inhibitor Capsaicin cream 0.025–0.075% applied t.i.d.-q.i.d.
*Dose response may vary; initial doses need to be low and titrated up. †Has FDA indication for treatment ofpainful diabetic neuropathy.
Standards of Medical Care
S38 DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 care.diabetesjournals.org

identification of the patient with LOPScan easily be carried out without this orother expensive equipment.
Initial screening for PAD should in-clude a history for claudication and anassessment of the pedal pulses. A diagnos-tic ABI should be performed in any pa-tient with symptoms of PAD. Due to thehigh estimated prevalence of PAD in pa-tients with diabetes and the fact thatmany patients with PAD are asymptom-atic, an ADA consensus statement onPAD (309) suggested that a screeningof ABI be performed in patients over50 years of age and considered in patientsunder 50 years of age who have otherPAD risk factors (e.g., smoking, hyperten-sion, hyperlipidemia, or duration of dia-betes �10 years). Refer patients withsignificant symptoms or a positive ABIfor further vascular assessment and con-sider exercise, medications, and surgicaloptions (309).
Patients with diabetes and high-riskfoot conditions should be educated re-garding their risk factors and appropriatemanagement. Patients at risk should un-derstand the implications of the LOPS,the importance of foot monitoring on adaily basis, the proper care of the foot in-cluding nail and skin care, and the selec-tion of appropriate footwear. Patientswith LOPS should be educated on ways tosubstitute other sensory modalities (handpalpation, visual inspection) for surveil-lance of early foot problems. Patients’ un-derstanding of these issues and theirphysical ability to conduct proper footsurveillance and care should be assessed.Patients with visual difficulties, physicalconstraints preventing movement, or cog-nitive problems that impair their ability toassess the condition of the foot and to in-stitute appropriate responses will needother people, such as family members, toassist in their care.
People with neuropathy or evidenceof increased plantar pressure (e.g., ery-thema, warmth, callus, or measured pres-sure) may be adequately managed withwell-fitted walking shoes or athleticshoes that cushion the feet and redis-tribute pressure. Callus can be debridedwith a scalpel by a foot care specialist orother health professional with experienceand training in foot care. People withbony deformities (e.g., hammertoes,prominent metatarsal heads, or bunions)may need extra-wide or -depth shoes.People with extreme bony deformities(e.g., Charcot foot) who cannot be accom-
modated with commercial therapeuticfootwear may need custom-moldedshoes.
Foot ulcers and wound care may re-quire care by a podiatrist, orthopedicor vascular surgeon, or rehabilitationspecialist experienced in the manage-ment of individuals with diabetes. For acomplete discussion, see the ADA con-sensus statement on diabetic foot woundcare (310).
VII. DIABETES CARE INSPECIFIC POPULATIONS
A. Children and adolescents
1. Type 1 diabetesThree-quarters of all cases of type 1 dia-betes are diagnosed in individuals �18years of age. Because children are not sim-ply “small adults,” it is appropriate to con-sider the unique aspects of care andmanagement of children and adolescentswith type 1 diabetes. Children with dia-betes differ from adults in many respects,including changes in insulin sensitivityrelated to sexual maturity and physicalgrowth, ability to provide self-care, super-vision in child care and school, andunique neurologic vulnerability to hypo-glycemia and DKA. Attention to such is-sues as family dynamics, developmentalstages, and physiologic differences relatedto sexual maturity are all essential in de-veloping and implementing an optimaldiabetes regimen. Although recommen-dations for children and adolescents areless likely to be based on clinical trial ev-idence, because of current and historicalrestraints placed on conducting researchin children, expert opinion and a reviewof available and relevant experimentaldata are summarized in the ADA state-ment on care of children and adolescentswith type 1 diabetes (311).
Ideally, the care of a child or adoles-cent with type 1 diabetes should be pro-vided by a multidisciplinary team ofspecialists trained in the care of childrenwith pediatric diabetes. At the very least,education of the child and family shouldbe provided by health care providerstrained and experienced in childhood di-abetes and sensitive to the challengesposed by diabetes in this age-group. Atthe time of initial diagnosis, it is essentialthat diabetes education be provided in atimely fashion, with the expectation thatthe balance between adult supervisionand self-care should be defined by, and
will evolve according to, physical, psy-chological, and emotional maturity. MNTshould be provided at diagnosis, and atleast annually thereafter, by an individualexperienced with the nutritional needs ofthe growing child and the behavioral is-sues that have an impact on adolescentdiets, including risk for disordered eating.
a. Glycemic control
Recommendations● Consider age when setting glycemic
goals in children and adolescents withtype 1 diabetes, with less stringent goalsfor younger children. (E)
While current standards for diabetesmanagement reflect the need to maintainglucose control as near to normal as safelypossible, special consideration must begiven to the unique risks of hypoglycemiain young children. Glycemic goals need tobe modified to take into account the factthat most children �6 or 7 years of agehave a form of “hypoglycemic unaware-ness.” Their counterregulatory mecha-nisms are immature and they may lack thecognitive capacity to recognize and re-spond to hypoglycemic symptoms, plac-ing them at greater risk for severehypoglycemia and its sequelae. In addi-tion, and unlike the case in adults, youngchildren under the age of 5 years are atrisk for permanent cognitive impairmentafter episodes of severe hypoglycemia(312–314). Extensive evidence indicatesthat near normalization of blood glucoselevels is seldom attainable in children andadolescents after the honeymoon (remis-sion) period. The A1C level achieved inthe “intensive” adolescent cohort of theDCCT group was �1% higher than thatachieved by adult DCCT subjects andabove current ADA recommendations forpatients in general. However, the in-creased frequency of use of basal bolusregimens (including insulin pumps) inyouth from infancy through adolescencehas been associated with more childrenreaching ADA blood glucose targets(315,316) in those families in which bothparents and the child with diabetes aremotivated to perform the required diabe-tes-related tasks.
In selecting glycemic goals, the bene-fits on long-term health outcomes ofachieving a lower A1C must be weighedagainst the unique risks of hypoglycemiaand the difficulties achieving near-normoglycemia in children and youth.Age-specific glycemic and A1C goals arepresented in Table 17.
Position Statement
care.diabetesjournals.org DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 S39
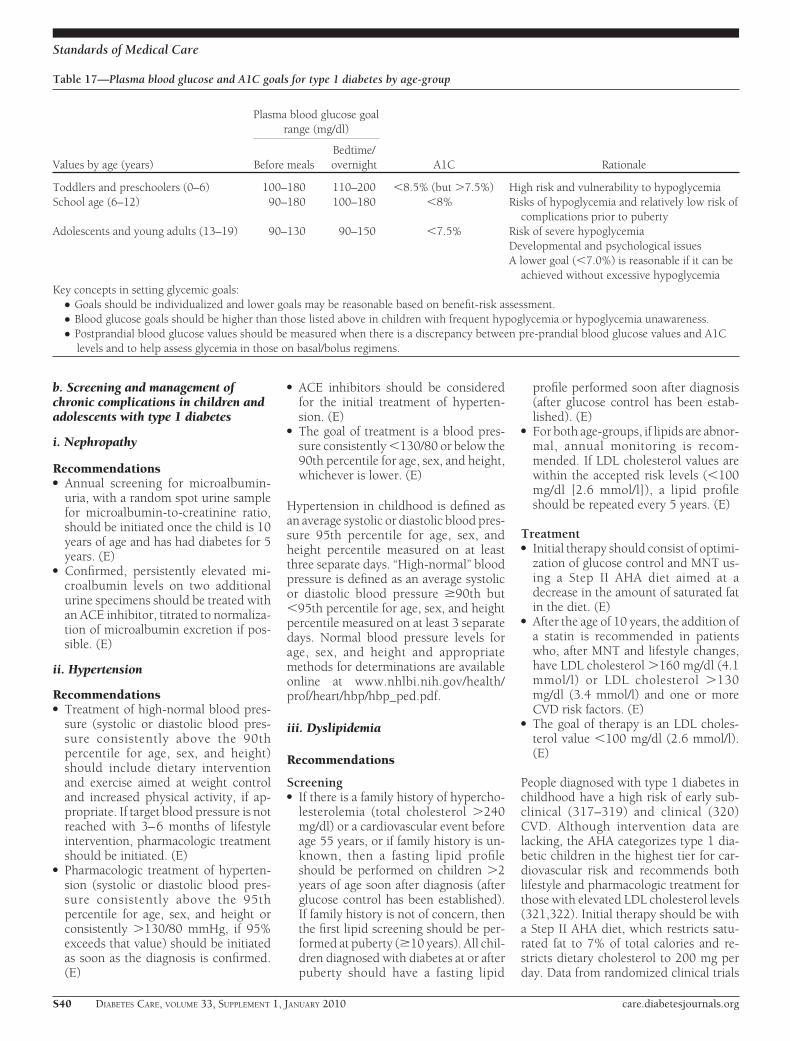
b. Screening and management ofchronic complications in children andadolescents with type 1 diabetes
i. Nephropathy
Recommendations● Annual screening for microalbumin-
uria, with a random spot urine samplefor microalbumin-to-creatinine ratio,should be initiated once the child is 10years of age and has had diabetes for 5years. (E)
● Confirmed, persistently elevated mi-croalbumin levels on two additionalurine specimens should be treated withan ACE inhibitor, titrated to normaliza-tion of microalbumin excretion if pos-sible. (E)
ii. Hypertension
Recommendations● Treatment of high-normal blood pres-
sure (systolic or diastolic blood pres-sure consistently above the 90thpercentile for age, sex, and height)should include dietary interventionand exercise aimed at weight controland increased physical activity, if ap-propriate. If target blood pressure is notreached with 3–6 months of lifestyleintervention, pharmacologic treatmentshould be initiated. (E)
● Pharmacologic treatment of hyperten-sion (systolic or diastolic blood pres-sure consistently above the 95thpercentile for age, sex, and height orconsistently �130/80 mmHg, if 95%exceeds that value) should be initiatedas soon as the diagnosis is confirmed.(E)
● ACE inhibitors should be consideredfor the initial treatment of hyperten-sion. (E)
● The goal of treatment is a blood pres-sure consistently �130/80 or below the90th percentile for age, sex, and height,whichever is lower. (E)
Hypertension in childhood is defined asan average systolic or diastolic blood pres-sure 95th percentile for age, sex, andheight percentile measured on at leastthree separate days. “High-normal” bloodpressure is defined as an average systolicor diastolic blood pressure �90th but�95th percentile for age, sex, and heightpercentile measured on at least 3 separatedays. Normal blood pressure levels forage, sex, and height and appropriatemethods for determinations are availableonline at www.nhlbi.nih.gov/health/prof/heart/hbp/hbp_ped.pdf.
iii. Dyslipidemia
Recommendations
Screening● If there is a family history of hypercho-
lesterolemia (total cholesterol �240mg/dl) or a cardiovascular event beforeage 55 years, or if family history is un-known, then a fasting lipid profileshould be performed on children �2years of age soon after diagnosis (afterglucose control has been established).If family history is not of concern, thenthe first lipid screening should be per-formed at puberty (�10 years). All chil-dren diagnosed with diabetes at or afterpuberty should have a fasting lipid
profile performed soon after diagnosis(after glucose control has been estab-lished). (E)
● For both age-groups, if lipids are abnor-mal, annual monitoring is recom-mended. If LDL cholesterol values arewithin the accepted risk levels (�100mg/dl [2.6 mmol/l]), a lipid profileshould be repeated every 5 years. (E)
Treatment● Initial therapy should consist of optimi-
zation of glucose control and MNT us-ing a Step II AHA diet aimed at adecrease in the amount of saturated fatin the diet. (E)
● After the age of 10 years, the addition ofa statin is recommended in patientswho, after MNT and lifestyle changes,have LDL cholesterol �160 mg/dl (4.1mmol/l) or LDL cholesterol �130mg/dl (3.4 mmol/l) and one or moreCVD risk factors. (E)
● The goal of therapy is an LDL choles-terol value �100 mg/dl (2.6 mmol/l).(E)
People diagnosed with type 1 diabetes inchildhood have a high risk of early sub-clinical (317–319) and clinical (320)CVD. Although intervention data arelacking, the AHA categorizes type 1 dia-betic children in the highest tier for car-diovascular risk and recommends bothlifestyle and pharmacologic treatment forthose with elevated LDL cholesterol levels(321,322). Initial therapy should be witha Step II AHA diet, which restricts satu-rated fat to 7% of total calories and re-stricts dietary cholesterol to 200 mg perday. Data from randomized clinical trials
Table 17—Plasma blood glucose and A1C goals for type 1 diabetes by age-group
Values by age (years)
Plasma blood glucose goalrange (mg/dl)
A1C RationaleBefore mealsBedtime/overnight
Toddlers and preschoolers (0–6) 100–180 110–200 �8.5% (but �7.5%) High risk and vulnerability to hypoglycemiaSchool age (6–12) 90–180 100–180 �8% Risks of hypoglycemia and relatively low risk of
complications prior to pubertyAdolescents and young adults (13–19) 90–130 90–150 �7.5% Risk of severe hypoglycemia
Developmental and psychological issuesA lower goal (�7.0%) is reasonable if it can be
achieved without excessive hypoglycemiaKey concepts in setting glycemic goals:
● Goals should be individualized and lower goals may be reasonable based on benefit-risk assessment.● Blood glucose goals should be higher than those listed above in children with frequent hypoglycemia or hypoglycemia unawareness.● Postprandial blood glucose values should be measured when there is a discrepancy between pre-prandial blood glucose values and A1C
levels and to help assess glycemia in those on basal/bolus regimens.
Standards of Medical Care
S40 DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 care.diabetesjournals.org

in children as young as 7 months of ageindicate that this diet is safe and does notinterfere with normal growth and devel-opment (323,324).
For children over the age of 10 yearswith persistent elevation of LDL choles-terol despite lifestyle therapy, statinsshould be considered. Neither long-termsafety nor cardiovascular outcome effi-cacy has been established for children.However, recent studies have shownshort-term safety equivalent to that seenin adults and efficacy in lowering LDLcholesterol levels, improving endothelialfunction, and causing regression of ca-rotid intimal thickening (325–327). Nostatin is approved for use under the age of10 years, and statin treatment should gen-erally not be used in type 1 diabetic chil-dren prior to this age.
iv. Retinopathy
Recommendations● The first ophthalmologic examination
should be obtained once the child is 10years of age and has had diabetes for3–5 years. (E)
● After the initial examination, annualroutine follow-up is generally recom-mended. Less frequent examinationsmay be acceptable on the advice of aneye care professional. (E)
Although retinopathy most commonlyoccurs after the onset of puberty and after5–10 years of diabetes duration, it hasbeen reported in prepubertal childrenand with diabetes duration of only 1–2years. Referrals should be made to eyecare professionals with expertise in dia-betic retinopathy, an understanding ofthe risk for retinopathy in the pediatricpopulation, and experience in counselingthe pediatric patient and family on theimportance of early prevention/inter-vention.
v. Celiac disease
Recommendations● Children with type 1 diabetes should be
screened for celiac disease by measuringtissue transglutaminase or anti-endomysial antibodies, with documenta-tion of normal serum IgA levels, soonafter the diagnosis of diabetes. (E)
● Testing should be repeated if growthfailure, failure to gain weight, weightloss, or gastroenterologic symptoms oc-cur. (E)
● Consideration should be given to peri-
odic rescreening of asymptomatic indi-viduals. (E)
● Children with positive antibodiesshould be referred to a gastroenterolo-gist for evaluation. (E)
● Children with confirmed celiac diseaseshould have consultation with a dieti-tian and be placed on a gluten-free diet.(E)
Celiac disease is an immune-mediateddisorder that occurs with increased fre-quency in patients with type 1 diabetes(1–16% of individuals compared with0.3–1% in the general population)(328,329). Symptoms of celiac disease in-clude diarrhea, weight loss or poor weightgain, growth failure, abdominal pain,chronic fatigue, malnutrition due to mal-absorption, other gastrointestinal prob-lems, and unexplained hypoglycemia orerratic blood glucose concentrations.
vi. Hypothyroidism
Recommendations● Children with type 1 diabetes should be
screened for thyroid peroxidase andthyroglobulin antibodies at diagnosis.(E)
● Thyroid-stimulating hormone (TSH)concentrations should be measured af-ter metabolic control has been estab-lished. If normal, they should berechecked every 1–2 years or if the pa-tient develops symptoms of thyroiddysfunction, thyromegaly, or an abnor-mal growth rate. Free T4 should bemeasured if TSH is abnormal. (E)
Autoimmune thyroid disease is the mostcommon autoimmune disorder associ-ated with diabetes, occurring in 17–30%of patients with type 1 diabetes (330). Thepresence of thyroid auto-antibodies ispredictive of thyroid dysfunction, gener-ally hypothyroidism and less commonlyhyperthyroidism (331). Subclinical hy-pothyroidism may be associated with in-c rea sed r i sk o f symptomat i chypoglycemia (332) and with reducedlinear growth (333). Hyperthyroidism al-ters glucose metabolism, potentially re-sulting in deterioration of metaboliccontrol.c. Self-management. No matter howsound the medical regimen, it can only beas good as the ability of the family and/orindividual to implement it. Family in-volvement in diabetes remains an impor-tant component of optimal diabetesmanagement throughout childhood and
into adolescence. Health care providerswho care for children and adolescentstherefore must be capable of evaluatingthe behavioral, emotional, and psychoso-cial factors that interfere with implemen-tation and then must work with theindividual and family to resolve problemsthat occur and/or to modify goals asappropriate.d. School and day care. Since a sizableportion of a child’s day is spent in school,close communication with school or daycare personnel is essential for optimal di-abetes management, safety, and maximalacademic opportunities. See VIII.B. Dia-betes Care in the School and Day CareSetting, for further discussion.
2. Type 2 diabetesThe incidence of type 2 diabetes in ado-lescents is increasing, especially in ethnicminority populations (21). Distinctionbetween type 1 and type 2 diabetes inchildren can be difficult, since the preva-lence of overweight in children continuesto rise and since autoantigens and ketosismay be present in a substantial number ofpatients with features of type 2 diabetes(including obesity and acanthosis nigri-cans). Such a distinction at the time ofdiagnosis is critical because treatmentregimens, educational approaches, anddietary counsel will differ markedly be-tween the two diagnoses.
Type 2 diabetes has a significant in-cidence of comorbidit ies alreadypresent at the time of diagnosis (334). Itis recommended that blood pressuremeasurement, a fasting lipid profile,microalbuminuria assessment, and di-lated eye examination be performed atthe time of diagnosis. Thereafter,screening guidelines and treatment rec-ommendations for hypertension, dys-lipidemia, microalbuminuria, andretinopathy in youth with type 2 diabe-tes are similar to those for youth withtype 1 diabetes. Additional problemsthat may need to be addressed includepolycystic ovary disease and the variouscomorbidities associated with pediatricobesity such as sleep apnea, hepatic ste-atosis, orthopedic complications, andpsychosocial concerns. The ADA con-sensus statement on this subject (23)provides guidance on the prevention,screening, and treatment of type 2 dia-betes and its comorbidities in youngpeople.
Position Statement
care.diabetesjournals.org DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 S41

B. Preconception care
Recommendations● A1C levels should be as close to normal
as possible (�7%) in an individual pa-tient before conception is attempted.(B)
● Starting at puberty, preconceptioncounseling should be incorporated inthe routine diabetes clinic visit for allwomen of child-bearing potential. (C)
● Women with diabetes who are contem-plating pregnancy should be evaluatedand, if indicated, treated for diabeticretinopathy, nephropathy, neuropathy,and CVD. (E)
● Medications used by such womenshould be evaluated prior to concep-tion because drugs commonly used totreat diabetes and its complicationsmay be contraindicated or not recom-mended in pregnancy, including st-atins, ACE inhibitors, ARBs, and mostnoninsulin therapies. (E)
Major congenital malformations remainthe leading cause of mortality and seriousmorbidity in infants of mothers with type1 or type 2 diabetes. Observational stud-ies indicate that the risk of malformationsincreases continuously with increasingmaternal glycemia during the first 6–8weeks of gestation, as defined by first-trimester A1C concentrations. There is nothreshold for A1C values below whichrisk disappears entirely. However, mal-formation rates above the 1–2% back-ground rate of nondiabetic pregnanciesappear to be limited to pregnancies inwhich first-trimester A1C concentrationsare �1% above the normal range for anondiabetic pregnant woman.
Preconception care of diabetes ap-pears to reduce the risk of congenital mal-formations. Five nonrandomized studiescompared rates of major malformations ininfants between women who participatedin preconception diabetes care programsand women who initiated intensive diabe-tes management after they were alreadypregnant. The preconception care pro-grams were multidisciplinary and de-signed to train patients in diabetes self-management with diet, intensified insulintherapy, and SMBG. Goals were set toachieve normal blood glucose concentra-tions, and �80% of subjects achievednormal A1C concentrations before theybecame pregnant (335–339). In all fivestudies, the incidence of major congenitalmalformations in women who partici-pated in preconception care (range 1.0–
1.7% of infants) was much lower than theincidence in women who did not partici-pate (range 1.4–10.9% of infants). Onelimitation of these studies is that partici-pation in preconception care was self-selected rather than randomized. Thus, itis impossible to be certain that the lowermalformation rates resulted fully fromimproved diabetes care. Nonetheless, theevidence supports the concept that mal-formations can be reduced or preventedby careful management of diabetes beforepregnancy.
Planned pregnancies greatly facilitatepreconception diabetes care. Unfortu-nately, nearly two-thirds of pregnanciesin women with diabetes are unplanned,leading to a persistent excess of malfor-mations in infants of diabetic mothers. Tominimize the occurrence of these devas-tating malformations, standard care for allwomen with diabetes who have child-bearing potential, beginning at the onsetof puberty or at diagnosis, should include1) education about the risk of malforma-tions associated with unplanned pregnan-cies and poor metabolic control; and 2)use of effective contraception at all times,unless the patient has good metaboliccontrol and is actively trying to conceive.
Women contemplating pregnancyneed to be seen frequently by a multidis-ciplinary team experienced in the man-agement of diabetes before and duringpregnancy. The goals of preconceptioncare are to 1) involve and empower thepatient in the management of her diabe-tes, 2) achieve the lowest A1C test resultspossible without excessive hypoglycemia,3) assure effective contraception until sta-ble and acceptable glycemia is achieved,and 4) identify, evaluate, and treat long-term diabetes complications such as reti-nopathy, nephropathy, neuropathy,hypertension, and CHD (76).
Among the drugs commonly used inthe treatment of patients with diabetes, anumber may be relatively or absolutelycontraindicated during pregnancy. St-atins are category X (contraindicated foruse in pregnancy) and should be discon-tinued before conception, as should ACEinhibitors (340). ARBs are category C(risk cannot be ruled out) in the first tri-mester but category D (positive evidenceof risk) in later pregnancy and shouldgenerally be discontinued before preg-nancy. Among the oral antidiabeticagents, metformin and acarbose are clas-sified as category B (no evidence of risk inhumans) and all others as category C. Po-tential risks and benefits of oral antidia-
betic agents in the preconception periodmust be carefully weighed, recognizingthat data are insufficient to establish thesafety of these agents in pregnancy.
For further discussion of preconcep-tion care, see the related ADA consensusstatement (76) and position statement(341) on preexisting diabetes andpregnancy.
C. Older adults
Recommendations● Older adults who are functional, are
cognitively intact, and have significantlife expectancy should receive diabetescare using goals developed for youngeradults. (E)
● Glycemic goals for older adults notmeeting the above criteria may be re-laxed using individual criteria, but hy-perglycemia leading to symptoms orrisk of acute hyperglycemic complica-tions should be avoided in all patients.(E)
● Other cardiovascular risk factorsshould be treated in older adults withconsideration of the time frame of ben-efit and the individual patient. Treat-ment of hypertension is indicated invirtually all older adults, and lipid andaspirin therapy may benefit those withlife expectancy at least equal to the timeframe of primary or secondary preven-tion trials. (E)
● Screening for diabetes complicationsshould be individualized in olderadults, but particular attention shouldbe paid to complications that wouldlead to functional impairment. (E)
Diabetes is an important health conditionfor the aging population; at least 20% ofpatients over the age of 65 years have di-abetes, and this number can be expectedto grow rapidly in the coming decades.Older individuals with diabetes havehigher rates of premature death, func-tional disability, and coexisting illnessessuch as hypertension, CHD, and strokethan those without diabetes. Older adultswith diabetes are also at greater risk thanother older adults for several common ge-riatric syndromes, such as polypharmacy,depression, cognitive impairment, uri-nary incontinence, injurious falls, andpersistent pain.
The American Geriatric Society’sguidelines for improving the care of theolder person with diabetes (342) have in-fluenced the following discussion andrecommendations. The care of older
Standards of Medical Care
S42 DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 care.diabetesjournals.org

adults with diabetes is complicated bytheir clinical and functional heterogene-ity. Some older individuals developed di-abetes years earlier and may havesignificant complications; others who arenewly diagnosed may have had years ofundiagnosed diabetes with resultant com-plications or may have few complicationsfrom the disease. Some older adults withdiabetes are frail and have other underly-ing chronic conditions, substantial diabe-tes-related comorbidity, or limitedphysical or cognitive functioning. Otherolder individuals with diabetes have littlecomorbidity and are active. Life expectan-cies are highly variable for this populationbut often longer than clinicians realize.Providers caring for older adults with di-abetes must take this heterogeneity intoconsideration when setting and prioritiz-ing treatment goals.
There are few long-term studies inolder adults that demonstrate the benefitsof intensive glycemic, blood pressure, andlipid control. Patients who can be ex-pected to live long enough to reap thebenefits of long-term intensive diabetesmanagement and who are active, havegood cognitive function, and are willingshould be provided with the needed edu-cation and skills to do so and be treatedusing the goals for younger adults withdiabetes.
For patients with advanced diabetescomplications, life-limiting comorbid ill-ness, or substantial cognitive or func-tional impairment, it is reasonable to setless-intensive glycemic target goals. Thesepatients are less likely to benefit from re-ducing the risk of microvascular compli-cations and more likely to suffer seriousadverse effects from hypoglycemia. How-ever, patients with poorly controlleddiabetes may be subject to acute compli-cations of diabetes, including dehydra-t ion , poor wound hea l ing , andhyperglycemic hyperosmolar coma. Gly-cemic goals at a minimum should avoidthese consequences.
Although control of hyperglycemiamay be important in older individualswith diabetes, greater reductions in mor-bidity and mortality may result from con-trol of other cardiovascular risk factorsrather than from tight glycemic controlalone. There is strong evidence from clin-ical trials of the value of treating hyper-tension in the elderly (343,344). There isless evidence for lipid-lowering and aspi-rin therapy, although the benefits of theseinterventions for primary and secondaryprevention are likely to apply to older
adults whose life expectancies equal orexceed the time frames seen in clinicaltrials.
Special care is required in prescribingand monitoring pharmacologic therapy inolder adults. Metformin is often contrain-dicated because of renal insufficiency orsignificant heart failure. TZDs can causefluid retention, which may exacerbate orlead to heart failure. They are contraindi-cated in patients with CHF (New YorkHeart Association class III and IV), and ifused at all should be used very cautiouslyin those with, or at risk for, milder degreesof CHF. Sulfonylureas, other insulinsecretagogues, and insulin can cause hy-poglycemia. Insulin use requires that pa-tients or caregivers have good visual andmotor skills and cognitive ability. Drugsshould be started at the lowest dose andtitrated up gradually until targets arereached or side effects develop.
Screening for diabetes complicationsin older adults also should be individual-ized. Particular attention should be paidto complications that can develop overshort periods of time and/or that wouldsignificantly impair functional status,such as vision and lower-extremitycomplications.
D. Cystic fibrosis–related diabetesCystic fibrosis-related diabetes (CFRD) isthe most common comorbidity in peoplewith cystic fibrosis, occurring in �20% ofadolescents and 40–50% of adults. Theadditional diagnosis of diabetes in thispopulation is associated with worse nutri-tional status, more severe inflammatorylung disease, and greater mortality fromrespiratory failure. For reasons that arenot well understood, women with CFRDare particularly vulnerable to excess mor-bidity and mortality. Insulin insufficiencyrelated to partial fibrotic destruction ofthe islet mass is the primary defect inCFRD. Genetically determined functionof the remaining �-cells and insulin resis-tance associated with infection and in-flammation may also play a role.Encouraging new data suggest that earlydetection and aggressive insulin therapyhave narrowed the gap in mortality be-tween cystic fibrosis patients with andwithout diabetes and have eliminated thesex difference in mortality.
A consensus conference on CFRDwas cosponsored in 2009 by ADA, theCystic Fibrosis Foundation, and the Law-son Wilkins Pediatric Endocrine Society.Recommendations for the clinical man-
agement of CFRD will be found in theconsensus report to be published in 2010.
VIII. DIABETES CARE INSPECIFIC SETTINGS
Diabetes care in the hospital
Recommendations● All patients with diabetes admitted to
the hospital should have their diabetesclearly identified in the medical record.(E)
● All patients with diabetes should havean order for blood glucose monitoring,with results available to all members ofthe health care team. (E)
● Goals for blood glucose levels● Critically ill patients: Insulin therapy
should be initiated for treatment ofpersistent hyperglycemia starting at athreshold of �180 mg/dl (10 mmol/l). Once insulin therapy is started, aglucose range of 140 –180 mg/dl(7.8 –10 mmol/l) is recommendedfor the majority of critically ill pa-tients. (A) These patients require anintravenous insulin protocol that hasdemonstrated efficacy and safety inachieving the desired glucose rangewithout increasing risk for severe hy-poglycemia. (E)
● Non–critically ill patients: There isno clear evidence for specific bloodglucose goals. If treated with insulin,the premeal blood glucose targetshould generally be �140 mg/dl (7.8mmol/l) with random blood glucose�180 mg/dl (10.0 mmol/l), providedthese targets can be safely achieved.More stringent targets may be appro-priate in stable patients with previoustight glycemic control. Less stringenttargets may be appropriate in thosewith severe comorbidites. (E)
● Scheduled subcutaneous insulin withbasal, nutritional, and correction com-ponents is the preferred method forachieving and maintaining glucosecontrol in noncritically ill patients. (C)Using correction dose or “supplemen-tal” insulin to correct premeal hyper-glycemia in addition to scheduledprandial and basal insulin is recom-mended. (E)
● Glucose monitoring should be initiatedin any patient not known to be diabeticwho receives therapy associated withhigh risk for hyperglycemia, includinghigh-dose glucocorticoid therapy, initi-ation of enteral or parenteral nutrition,or other medications such as octreotide
Position Statement
care.diabetesjournals.org DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 S43

or immunosuppressive medications.(B) If hyperglycemia is documentedand persistent, treatment is necessary.Such patients should be treated to thesame glycemic goals as patients withknown diabetes. (E)
● A plan for treating hypoglycemiashould be established for each patient.Episodes of hypoglycemia in the hospi-tal should be tracked. (E)
● All patients with diabetes admitted tothe hospital should have an A1C ob-tained if the result of testing in the pre-vious 2–3 months is not available. (E)
● Patients with hyperglycemia in the hos-pital who do not have a diagnosis ofdiabetes should have appropriate plansfor follow-up testing and care docu-mented at discharge. (E)
The subject of diabetes in the hospital isextensively reviewed in an ADA technicalreview (345). A recent updated consensusstatement by the American Association ofClinical Endocrinologists (AACE) and theADA (346) form the basis for the discus-sion and guidelines in this section.
The literature on hospitalized pa-tients with hyperglycemia typically de-scribes three categories:
● Medical history of diabetes: diabetes pre-viously diagnosed and acknowledged bythe patient’s treating physician.
● Unrecognized diabetes: hyperglycemia(fasting blood glucose �126 mg/dl orrandom blood glucose �200 mg/dl)occurring during hospitalization andconfirmed as diabetes after hospitaliza-tion by standard diagnostic criteria butunrecognized as diabetes by the treat-ing physician during hospitalization.
● Hospital-related hyperglycemia: hyper-glycemia (fasting blood glucose �126mg/dl or random blood glucose �200mg/dl) occurring during the hospital-ization that reverts to normal after hos-pital discharge.
The management of hyperglycemia in thehospital has logically been consideredsecondary in importance to the conditionthat prompted admission (345). How-ever, a body of literature now supportstargeted glucose control in the hospitalsetting for potential improved clinicaloutcomes. Hyperglycemia in the hospitalmay result from stress; decompensationof type 1, type 2, or other forms of dia-betes; and/or may be iatrogenic due towithholding of antihyperglycemicmedications or administration of hyper-
glycemia-provoking agents such as glu-cocorticoids or vasopressors.
People with diabetes are more likelyto be hospitalized and to have longerlengths of stay than those without diabe-tes. A recent survey estimated that 22% ofall hospital inpatient days were incurredby people with diabetes and that hospitalinpatient care accounted for one-half ofthe $174 billion total U.S. medical expen-ditures for this disease (347). This is due,in part, to the continued expansion of theworldwide epidemic of type 2 diabetes. Inthe U.S. alone, there are �1.6 million newcases of diabetes each year with an overallprevalence of 23.6 million people (7.8%of the population, with one-quarter ofcases remaining undiagnosed). An addi-tional 57 million American adults are athigh risk for type 2 diabetes (348). Whilethe costs of illness-related stress hypergly-cemia are not known, they are likely to besignificant given the poor prognosis ofsuch patients (349–352).
There is substantial observational ev-idence linking hyperglycemia in hospital-ized patients (with or without diabetes) topoor outcomes. Cohort studies as well asa few early randomized controlled trials(RCTs) suggested that intensive treatmentof hyperglycemia improved hospital out-comes (345,351,352). Interventions tonormalize glycemia, however, have hadinconsistent results. Indeed, recent trialsin critically ill patients have failed to showa significant improvement in mortalitywi th in tens ive g lycemic contro l(353,354) or have even shown increasedmortality risk (355). Moreover, these re-cent RCTs have highlighted the risk of se-vere hypoglycemia resulting from suchefforts (353–358).
The largest study to date, NICE-SUGAR, a multicenter, multinationalRCT, tested the effect of tight glycemiccontrol (target 81–108 mg/dl) on out-comes among 6,104 critically ill partici-pants, the majority of whom (�95%)required mechanical ventilation (355).Ninety-day mortality was significantlyhigher in the intensive versus the conven-tional group (target 144–180 mg/dl) (78more deaths; 27.5 vs. 24.9%, P 0.02) inboth surgical and medical patients. Mor-tality from cardiovascular causes wasmore common in the intensive group (76more deaths; 41.6 vs. 35.8%; P 0.02).Severe hypoglycemia was also more com-mon in the intensively treated group (6.8vs. 0.5%; P � 0.001). The precise reasonfor the increased mortality in the tightlycontrolled group is unknown. The results
of this study lie in stark contrast to a fa-mous 2001 single-center study that re-ported a 42% relative reduction inintensive care unit (ICU) mortality in crit-ically ill surgical patients treated to a tar-get blood glucose of 80 –110 mg/dl.Importantly, the control group in NICE-SUGAR had reasonably good blood glu-cose management, maintained at a meanglucose of 144 mg/dl, only 29 mg/dlabove the intensively managed patients.Accordingly, this study’s findings do notdisprove the notion that glycemic controlin the ICU is important. However, they dostrongly suggest that it is not necessary totarget blood glucose values �140 mg/dland that a highly stringent target of �110mg/dl actually may be dangerous.
In a recent meta-analysis of 26 trials(N 13,567), which included the NICE-SUGAR data, the pooled relative risk (RR)of death with intensive insulin therapywas 0.93 as compared with conventionaltherapy (95% CI 0.83–1.04) (358). Ap-proximately half of these trials reportedhypoglycemia, with a pooled RR of inten-sive therapy of 6.0 (95% CI 4.5–8.0). Thespecific ICU setting influenced the find-ings, with patients in surgical ICUs ap-pearing to benefit from intensive insulintherapy (RR 0.63 [95% CI 0.44–0.91]),while those in other critical care settingsdid not (medical ICU: 1.0 [0.78–1.28];“mixed” ICU: 0.99 [0.86–1.12]). It wasconcluded that overall, intensive insulintherapy increased the risk of hypoglyce-mia but provided no overall benefit onmortality in the critically ill, although abenefit to patients admitted to the surgicalICU was suggested.
It is very clear that the management ofhyperglycemia in the hospital presentsunique challenges that stem from varia-tions in a patient’s nutritional status andlevel of consciousness, the practical limi-tations of intermittent glycemic monitor-ing, and the ultimate importance ofpatient safety. Accordingly, reasonableglucose targets in the hospital setting aremodestly higher than may be routinelyadvised in patients with diabetes in theoutpatient setting. The following recom-mendations represent a synthesis of theevidence base over the past decade andare somewhat less stringent than priorrecommendations of the ADA Standardsof Medical Care in Diabetes. For a com-prehensive review of these data, thereader is referred to the latest consensusstatement from AACE and ADA on inpa-tient management of hyperglycemia(346).
Standards of Medical Care
S44 DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 care.diabetesjournals.org

1. Glycemic targets in hospitalizedpatientsa. Definition of glucose abnormalities inthe hospital setting. Hyperglycemia hasbeen defined as any blood glucose �140mg/dl (7.8 mmol/l). Levels that are signif-icantly and persistently above this may re-quire treatment in hospitalized patients.In patients without a previous diagnosisof diabetes, elevated blood glucose maybe due to “stress hyperglycemia,” a condi-tion that can be established by a review ofprior records or measurement of an A1C.A1C values �6.5% suggest that diabetespreceded hospitalization (359). Hypogly-cemia has been defined as any blood glu-cose �70 mg/dl (3.9 mmol/l). This is thestandard definition in outpatients andcorrelates with the initial threshold for therelease of counterregulatory hormones(177). Severe hypoglycemia in hospital-ized patients has been defined by manyas �40 mg/dl (2.2 mmol/l), althoughthis is lower than the �50 mg/dl (2.8mmol/l) level at which cognitive impair-ment begins in normal individuals(177,360,361). As with hyperglycemia,hypoglycemia among inpatients is also as-sociated with adverse short- and long-term outcomes. Early recognition andtreatment of mild to moderate hypoglyce-mia (40 and 69 mg/dl [2.2 and 3.8 mmol/l]) can prevent deterioration to a moresevere episode with potential adverse se-quelae (361,362).i. Critically ill patients. Based on theweight of the available evidence, for themajority of critically ill patients in the ICUsetting, insulin infusion should be used tocontrol hyperglycemia, with a startingthreshold of �180 mg/dl (10.0 mmol/l).Once intravenous insulin is started, theglucose level should be maintained be-tween 140 and 180 mg/dl (7.8 and 10.0mmol/l). Greater benefit may be realizedat the lower end of this range. Althoughstrong evidence is lacking, somewhatlower glucose targets may be appropriatein selected patients. However, targets�110 mg/dl (6.1 mmol/l) are not recom-mended. Use of insulin infusion protocolswith demonstrated safety and efficacy, re-sulting in low rates of hypoglycemia, arehighly recommended.ii. Noncritically ill patients. With no pro-spective, RCT data to inform specific gly-cemic targets in noncritically ill patients,recommendations are based on clinicalexperience and judgment. For the major-ity of noncritically ill patients treated withinsulin, premeal glucose targets shouldgenerally be �140 mg/dl (7.8 mmol/l)
with random blood glucose �180 mg/dl(10.0 mmol/l), as long as these targets canbe safely achieved. To avoid hypoglyce-mia, consideration should be given to re-assessing the insulin regimen if bloodglucose levels fall below 100 mg/dl (5.6mmol/l). Modification of the regimen isrequired when blood glucose values are�70 mg/dl (3.9 mmol/l), unless the eventis easily explained by other factors (suchas a missed meal, etc.).
Occasional patients with a prior his-tory of successful tight glycemic control inthe outpatient setting who are clinicallystable may be maintained with a glucoserange below the above cut points. Con-versely, higher glucose ranges may be ac-ceptable in terminally ill patients or inpatients with severe comorbidities, aswell as in those in patient-care settingswhere frequent glucose monitoring orclose nursing supervision is not feasible.
Clinical judgment, combined withongoing assessment of the patient’s clini-cal status, including changes in the trajec-tory of glucose measures, severity ofillness, nutritional status, or concurrentuse of medications that might affect glu-cose levels (e.g., steroids, octreotide)must be incorporated into the day-to-daydecisions regarding insulin dosing (363).
2. Treatment options in hospitalizedpatientsIn the hospital setting, insulin therapy isthe preferred method of glycemic controlin majority of clinical situations (346). Inthe ICU, intravenous infusion is the pre-ferred route of insulin administration.Outside of critical care units, subcutane-ous insulin is used much more frequently.Oral agents have a limited role in the in-patient setting.a. Intravenous insulin infusions. In thecritical care setting, continuous intrave-nous insulin infusion has been shown tobe the most effective method for achiev-ing specific glycemic targets (346). Be-cause of the very short half-life ofcirculating insulin, intravenous deliveryallows rapid dosing adjustments to ad-dress alterations in patients’ status.
Intravenous insulin is ideally admin-istered via validated written or computer-ized protocols that allow for predefinedadjustments to the insulin infusion rateaccording to glycemic fluctuations and in-sulin dose. An extensive review of themerits and deficiencies of published pro-tocols is beyond the intent of this state-ment, and the reader is referred to severalavailable reports and reviews (364–366).
Continued education of staff with peri-odic ongoing review of patient data arecritical for successful implementation ofany insulin protocol (364–366).
Patients who receive intravenous in-sulin infusion will usually require transi-tion to subcutaneous insulin when theybegin eating regular meals or are trans-ferred to lower intensity care. Typically, apercentage (usually 75–80%) of the totaldaily intravenous infusion dose is propor-tionately divided into basal and prandialcomponents (see below). Importantly,subcutaneous insulin must be given 1–4h prior to discontinuation of intravenousinsulin to prevent hyperglycemia (367).b. Subcutaneous insulin. Scheduledsubcutaneous insulin is the preferredmethod for achieving and maintainingglucose control in non-ICU patients withdiabetes or stress hyperglycemia. The rec-ommended components of inpatient sub-cutaneous insulin regimens include abasal, nutritional, and supplemental (cor-rection) component (345,346,368). Eachcomponent can be met by one of severalavailable insulin products, depending onthe particular hospital situation. Thereader is referred to several recent publi-cations and reviews that describe cur-rently available insulin preparations andprotocols (366–370).
A topic that deserves particular atten-tion is the persistent overuse of what hasbeen branded as sliding scale insulin (SSI)for management of hyperglycemia. Theterm “correction insulin,” which refers tothe use of additional short or rapid-actinginsulin with scheduled insulin doses totreat blood glucose above desired targets,is preferred (345). Prolonged therapywith SSI as the sole regimen is ineffectivein the majority of patients (and potentiallydangerous in type 1 diabetes) (370–375).c. Noninsulin agents. These agents areinappropriate in the majority of hospital-ized patients because they are less titrat-able than insulin in the short tem and aremeant to be used in patients eating on aregular meal schedule. Continuation ofthese agents may be appropriate in se-lected stable patients who are expected toconsume meals at regular intervals. Spe-cific caution is required with metformin,due to the possibility that a contraindica-tion may develop during the hospitaliza-tion, such as renal insufficiency, unstablehemodynamic status, or need for an im-aging study that requires a radio-contrastdye (345,376). Injectable noninsulintherapies such as exenatide and pramlint-
Position Statement
care.diabetesjournals.org DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 S45

ide have limitations similar to those oforal agents in the hospital setting.d. Specific clinical situationsi. Insulin pumps. Patients who use CSIIpump therapy in the outpatient settingcan be candidates for diabetes self-management in the hospital, providedthat they have the mental and physicalcapacity to do so (346,368). It is impor-tant that nursing personnel documentbasal rates and bolus doses on a regularbasis (at least daily). The availability ofhospital personnel with expertise in CSIItherapy is essential.ii. Enteral nutrition. Hyperglycemia is acommon side effect of inpatient enteralnutrition therapy (377). A recent reportusing a combination of basal insulin withcorrection insulin achieved a mean glu-cose value of 160 mg/dl (8.9 mmol/l).Similar results were achieved in the grouprandomized to receive SSI alone; how-ever, 48% of patients required the addi-tion of intermediate-acting insulin toachieve glycemic targets (373).iii. Parenteral nutrition. The high glu-cose load in standard parenteral nutritionfrequently results in hyperglycemia,which is associated with a higher inci-dence of complications and mortality incritically ill ICU patients (378). Insulintherapy is highly recommended, with glu-cose targets as defined previously by se-verity of illness.iv. Glucocorticoid therapy. Hyperglyce-mia is a common complication of cortico-steroid therapy (363). Several approacheshave been proposed for treatment of thiscondition, but there are no publishedprotocols or studies that investigate theefficacy of these approaches. A reasonableapproach is to institute glucose monitor-ing for at least 48 h in all patients receiv-ing high dose glucocorticoid therapy andinitiate insulin as appropriate. In patientswho are already being treated for hyper-glycemia, early adjustment of insulindoses is recommended. Importantly, dur-ing steroid tapers, insulin dosing shouldbe proact ively adjusted to avoidhypoglycemia.v. Hypoglycemia prevention. Hypogly-cemia, especially in insulin-treated pa-tients, is the leading limiting factor in theglycemic management of type 1 and type2 diabetes (174). In the hospital, multipleadditional risk factors for hypoglycemiaare present, even among patients who areneither “brittle” nor tightly controlled. Pa-tients with or without diabetes may expe-rience hypoglycemia in the hospital inassociation with altered nutritional state,
heart failure, renal or liver disease, malig-nancy, infection, or sepsis (379,379,380).Additional triggering events leading toiatrogenic hypoglycemia include suddenreduction of corticosteroid dose, alteredability of the patient to self-report symp-toms, reduction of oral intake, emesis,new NPO status, inappropriate timing ofshort- or rapid-acting insulin in relationto meals, reduction of rate of administra-tion of intravenous dextrose, and unex-pected interruption of enteral feedings orparenteral nutrition.
Despite the preventable nature ofmany inpatient episodes of hypoglyce-mia, institutions are more likely to havenursing protocols for the treatment of hy-poglycemia than for its prevention.Tracking such episodes and analyzingtheir causes are important quality im-provement activities.
3. Diabetes care providers in thehospitalInpatient diabetes management may beeffectively provided by primary care phy-sicians, endocrinologists, or hospitalists.Involvement of appropriately trained spe-cialists or specialty teams may reducelength of stay, improve glycemic control,and improve outcomes (381–384). In thecare of diabetes, implementation of stan-dardized order sets for scheduled and cor-rection-dose insulin may reduce relianceon sliding-scale management. A team ap-proach is needed to establish hospitalpathways. To achieve glycemic targetsassociated with improved hospital out-comes, hospitals will need multidisci-plinary support to develop protocols forsubcutaneous insulin therapy that effec-tively and safely achieve glycemic targets(385).
4. Self-management in the hospitalSelf-management of diabetes in the hos-pital may be appropriate for competentadult patients who have a stable level ofconsciousness, have reasonably stabledaily insulin requirements, successfullyconduct self-management of diabetes athome, have physical skills needed to suc-cessfully self-administer insulin and per-form SMBG, have adequate oral intake,and are proficient in carbohydrate count-ing, use of multiple daily insulin injec-tions, or insulin pump therapy and sick-day management. The patient andphysician, in consultation with nursingstaff, must agree that patient self-management is appropriate under theconditions of hospitalization. For patients
conducting self-management in the hos-pital, it is imperative that basal, prandial,and correction doses of insulin and resultsof bedside glucose monitoring be re-corded as part of the patient’s hospitalmedical record. While many institutionsallow patients on insulin pumps to con-tinue these devices in the hospital, othersexpress concern regarding use of a deviceunfamiliar to staff, particularly in patientswho are not able to manage their ownpump therapy. If a patient is too ill toself-manage either multiple daily injec-tions or CSII, then appropriate subcuta-neous doses can be calculated on the basisof their basal and bolus insulin needs dur-ing hospitalization, with adjustments forchanges in nutritional or metabolic status.
5. DSME in the hospitalTeaching diabetes self-management topatients in hospitals is a challenging task.Patients are ill, under increased stress re-lated to their hospitalization and diagno-sis, and in an environment not conduciveto learning. Ideally, people with diabetesshould be taught at a time and place con-ducive to learning—as an outpatient ina recognized program of diabeteseducation.
For the hospitalized patient, diabetes“survival skills” education is generally afeasible approach. Patients and/or familymembers receive sufficient informationand training to enable safe care at home.Those newly diagnosed with diabetes orwho are new to insulin and/or blood glu-cose monitoring need to be instructedbefore discharge. Those patients hospital-ized because of a crisis related to diabetesmanagement or poor care at home neededucation to prevent subsequent episodesof hospitalization. An assessment of theneed for a home health referral or referralto an outpatient diabetes education pro-gram should be part of discharge plan-ning for all patients.
6. MNT in the hospitalHospital diets continue to be ordered bycalorie levels based on the “ADA diet.”However, since 1994 the ADA has not en-dorsed any single meal plan or specifiedpercentages of macronutrients, and theterm “ADA diet” should no longer beused. Current nutrition recommenda-tions advise individualization based ontreatment goals, physiologic parameters,and medication usage. Because of thecomplexity of nutrition issues in the hos-pital, a registered dietitian, knowledge-able and skilled in MNT, should serve as
Standards of Medical Care
S46 DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 care.diabetesjournals.org

an inpatient team member. The dietitianis responsible for integrating informationabout the patient’s clinical condition, eat-ing, and lifestyle habits and for establish-ing treatment goals in order to determinea realistic plan for nutrition therapy(386,387).
7. Bedside blood glucose monitoringBedside blood glucose monitoring usingpoint-of-care glucose meters is performedbefore meals and bedtime in the majorityof inpatients who are eating usual meals.In patients who are receiving continuousenteral or parenteral nutrition, glucosemonitoring is optimally performed every4–6 h. In patients who are receiving cy-cled enteral or parenteral nutrition, theschedule for glucose monitoring can beindividualized but should be frequentenough to detect hyperglycemia duringfeedings and risk of hypoglycemia whenfeedings are interrupted (374,376). Morefrequent blood glucose testing ranging fromevery 30 min to every 2 h is required forpatients on intravenous insulin infusions.
Safe and rational glycemic manage-ment relies on the accuracy of blood glu-cose measurements using point-of-careblood glucose meters, which have severalimportant limitations. Although the FDAallows a 20% error for glucose meters,questions about the appropriateness ofthis criterion have been raised (388). Glu-cose measures differ significantly betweenplasma and whole blood, terms which areoften used interchangeably and can leadto misinterpretation. Most commerciallyavailable capillary glucose meters intro-duce a correction factor of �1.12 to re-port a “plasma-adjusted” value (389).
Significant discrepancies betweencapillary, venous, and arterial plasmasamples have been observed in patientswith low or high hemoglobin concentra-tions, hypoperfusion, and the presence ofinterfering substances (389,390). Analyt-ical variability has been described withseveral point-of-care meters (391). Anyglucose result that does not correlate withthe patient’s status should be confirmedthrough conventional laboratory sam-pling of PG.
While laboratory measurement of PGhas less variability and interference, mul-tiple daily phlebotomies are not practical.The use of indwelling lines as the sam-pling source also poses risks for infection.Studies performed using continuous in-terstitial glucose monitoring systems inthe critical care setting (392) currently are
limited by the lack of reliability in the hy-poglycemic range as well as by cost.
8. Discharge planningIt is important to anticipate the postdis-charge antihyperglycemic regimen in allpatients with diabetes or newly discov-ered hyperglycemia. The optimal pro-gram will need to consider the type andseverity of diabetes, the effects of thepatient’s illness on blood glucose levels,and the capacities and desires of the pa-tient. Smooth transition to outpatientcare should be ensured, especially inthose new to insulin therapy or inwhom the diabetes regimen has beensubstantially altered during the hospi-talization. All patients in whom the di-agnosis of diabetes is new should have,at minimum, “survival skills” trainingprior to discharge.
It is recommended that the followingareas be reviewed and addressed prior tohospital discharge:
● level of understanding related to the di-agnosis of diabetes
● SMBG and explanation of home bloodglucose goals
● definition, recognition, treatment, andprevention of hyperglycemia andhypoglycemia
● identification of health care providerwho will provide diabetes care afterdischarge
● information on consistent eatingpatterns
● when and how to take blood glucose–lowering medications including insulinadministration (if going home oninsulin)
● sick-day management● proper use and disposal of needles and
syringes
More expanded diabetes education canbe arranged in the community. An out-patient follow-up visit with the primarycare provider, endocrinologist, or diabe-tes educator within 1 month of dischargeis advised for all patients having hypergly-cemia in the hospital. Clear communica-tion with outpatient providers eitherdirectly or via hospital discharge summa-ries facilitates safe transitions to outpa-tient care. Providing informationregarding the cause or the plan for deter-mining the cause of hyperglycemia, re-lated complications and comorbidities,and recommended treatments can assistoutpatient providers as they assume on-going care.
IX. STRATEGIES FORIMPROVING DIABETESCARE — The implementation of thestandards of care for diabetes has beensuboptimal in most clinical settings. A re-cent report (393) indicated that only57.1% of adults with diagnosed diabetesachieved an A1C of �7%, only 45.5%had a blood pressure �130/80 mmHg,and just 46.5% had a total cholesterol�200 mg/dl. Most distressing was thatonly 12.2% of people with diabetesachieved all three treatment goals.
While numerous interventions to im-prove adherence to the recommendedstandards have been implemented, thechallenge of providing uniformly effectivediabetes care has thus far defied a simplesolution. A major contributor to subopti-mal care is a delivery system that too oftenis fragmented, lacks clinical informationcapabilities, often duplicates services, andis poorly designed for the delivery ofchronic care. The chronic care model(CCM) includes five core elements for theprovision of optimal care of patients withchronic disease: delivery system design,self-management support, decision sup-port, clinical information systems, andcommunity resources and policies. Redef-inition of the roles of the clinic staff andpromoting self-management on the partof the patient are fundamental to the suc-cessful implementation of the CCM(394). Collaborative, multidisciplinaryteams are best suited to provide such carefor people with chronic conditions likediabetes and to empower patients’ perfor-mance of appropriate self-management.Alterations in reimbursement that rewardthe provision of quality care, as defined bythe attainment of quality measures devel-oped by such programs as the ADA/Nat iona l Commit tee for Qual i tyAssurance Diabetes Provider RecognitionProgram, will also be required to achievedesired outcome goals.
In recent years, numerous health careorganizations, ranging from large healthcare systems such as the U.S. Veteran’sAdministration to small private practices,have implemented strategies to improvediabetes care. Successful programs havepublished results showing improvementin process measures such as measurementof A1C, lipids, and blood pressure. Effectson in important intermediate outcomes,such as mean A1C for populations, havebeen more difficult to demonstrate (395–397), although examples do exist (398–402), often taking more than 1 year tomanifest (394). Features of successful
Position Statement
care.diabetesjournals.org DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 S47

programs reported in the literatureinclude
● Delivery of DSME: increases adherenceto standard of care and educating pa-tients on glycemic targets and improvesthe percentage of patients who reachgoal A1C (142,403)
● Adoption of practice guidelines, withparticipation of health care profession-als in the process of development:Guidelines should be readily accessibleat the point of service, preferably ascomputerized reminders at the point ofcare. Guidelines should begin with asummary of their major recommenda-tions instructing health care profes-sionals what to do and how to do it.
● Use of checklists that mirror guidelines:successful at improving adherence tostandards of care
● Systems changes: such as provision ofautomated reminders to health careprofessionals and patients and auditand feedback of process and outcomedata to providers
● Quality improvement programs com-bining continuous quality improve-ment or other cycles of analysis andintervention with provider perfor-mance data
● Practice changes: such as availability ofpoint of care testing of A1C, schedulingplanned diabetes visits, clustering ofdedicated diabetes visits into specifictimes within a primary care practiceschedule, or group visits and/or visitswith multiple health care professionalson a single day
● Tracking systems with either an elec-tronic medical record or patient regis-try: helpful at increasing adherence tostandards of care by prospectively iden-tifying those requiring assessmentsand/or treatment modifications. Theylikely could have greater efficacy if theysuggested specific therapeutic interven-tions to be considered for a particularpatient at a particular point in time(404).
● Availability of case or (preferably) caremanagement services (405): Nurses,pharmacists, and other nonphysicianhealth care professionals using detailedalgorithms working under the supervi-sion of physicians have demonstratedthe greatest reduction in A1C andblood pressure (406,407).
Evidence suggests that these individualinitiatives work best when provided ascomponents of a multifactorial interven-
tion. When practices are compared, thosethat address more of the CCM elementsdemonstrate lower A1C levels and lowercardiovascular risk scores (408). Themost successful practices have an institu-tional priority for quality of care, involveall of the staff in their initiatives, redesigntheir delivery system, activate and edu-cate their patients, and use electronichealth record tools (409,410).
NDEP maintains an online resource(www.betterdiabetescare.nih.gov) to helphealth care professionals design and im-plement more effective health care deliv-ery systems for those with diabetes.
It is clear that optimal diabetes man-agement requires an organized, system-atic approach and involvement of acoordinated team of dedicated health careprofessionals working in an environmentwhere quality care is a priority.
References1. American Diabetes Asociation. Medical
Management of Type 1 Diabetes. Alexan-dria, VA, American Diabetes Associa-tion, 2008
2. American Diabetes Asociation. MedicalManagement of Type 2 Diabetes. Alexan-dria, VA, American Diabetes Associa-tion, 2008
3. American Diabetes Association. IntensiveDiabetes Management. Alexandria, VA,American Diabetes Association, 2009
4. Expert Committee on the Diagnosis andClassification of Diabetes Mellitus. Re-port of the Expert Committee on the Di-agnosis and Classification of DiabetesMellitus. Diabetes Care 1997;20:1183–1197
5. International Expert Committee. Inter-national Expert Committee report on therole of the A1C assay in the diagnosis ofdiabetes. Diabetes Care 2009;32:1327–1334
6. American Diabetes Association. Diagno-sis and classification of diabetes mellitus.Diabetes Care 2010;33(Suppl. 1):S62–S69
7. Genuth S, Alberti KG, Bennett P, Buse J,Defronzo R, Kahn R, Kitzmiller J,Knowler WC, Lebovitz H, Lernmark A,Nathan D, Palmer J, Rizza R, Saudek C,Shaw J, Steffes M, Stern M, Tuomilehto J,Zimmet P, Expert Committee on the Di-agnosis and Classification of DiabetesMellitus. Follow-up report on the diag-nosis of diabetes mellitus. Diabetes Care2003;26:3160–3167
9. Engelgau MM, Narayan KM, HermanWH. Screening for type 2 diabetes. Dia-betes Care 2000;23:1563–1580
10. Gabir MM, Hanson RL, Dabelea D, Im-peratore G, Roumain J, Bennett PH,Knowler WC. The 1997 American Dia-
betes Association and 1999 WorldHealth Organization criteria for hyper-glycemia in the diagnosis and predictionof diabetes. Diabetes Care 2000;23:1108–1112
11. Knowler WC, Barrett-Connor E, FowlerSE, Hamman RF, Lachin JM, Walker EA,Nathan DM, Diabetes Prevention Pro-gram Research Group. Reduction in theincidence of type 2 diabetes with lifestyleintervention or metformin. N Engl J Med2002;346:393–403
12. Tuomilehto J, Lindstrom J, Eriksson JG,Valle TT, Hamalainen H, Ilanne-ParikkaP, Keinanen-Kiukaanniemi S, Laakso M,Louheranta A, Rastas M, Salminen V,Uusitupa M, Finnish Diabetes Preven-tion Study Group. Prevention of type 2diabetes mellitus by changes in lifestyleamong subjects with impaired glucosetolerance. N Engl J Med 2001;344:1343–1350
13. Pan XR, Li GW, Hu YH, Wang JX, YangWY, An ZX, Hu ZX, Lin J, Xiao JZ, CaoHB, Liu PA, Jiang XG, Jiang YY, Wang JP,Zheng H, Zhang H, Bennett PH, HowardBV. Effects of diet and exercise in pre-venting NIDDM in people with impairedglucose tolerance. The Da Qing IGT andDiabetes Study. Diabetes Care 1997;20:537–544
14. Buchanan TA, Xiang AH, Peters RK, KjosSL, Marroquin A, Goico J, Ochoa C, TanS, Berkowitz K, Hodis HN, Azen SP.Preservation of pancreatic beta-cellfunction and prevention of type 2 diabe-tes by pharmacological treatment of in-sulin resistance in high-risk hispanicwomen. Diabetes 2002;51:2796–2803
15. Chiasson JL, Josse RG, Gomis R,Hanefeld M, Karasik A, Laakso M,STOP-NIDDM Trail Research Group.Acarbose for prevention of type 2 diabe-tes mellitus: the STOP-NIDDM random-ised trial. Lancet 2002;359:2072–2077
16. DREAM (Diabetes REduction Assess-ment with ramipril and rosiglitazoneMedication) Trial Investigators, GersteinHC, Yusuf S, Bosch J, Pogue J, SheridanP, Dinccag N, Hanefeld M, Hoogwerf B,Laakso M, Mohan V, Shaw J, Zinman B,Holman RR. Effect of rosiglitazone onthe frequency of diabetes in patientswith impaired glucose tolerance or im-paired fasting glucose: a randomisedcontrolled trial. Lancet 2006;368:1096–1105
17. Ramachandran A, Snehalatha C, Mary S,Mukesh B, Bhaskar AD, Vijay V, IndianDiabetes Prevention Programme (IDPP).The Indian Diabetes Prevention Pro-gramme shows that lifestyle modifica-tion and metformin prevent type 2diabetes in Asian Indian subjects withimpaired glucose tolerance (IDPP-1).Diabetologia 2006;49:289–297
18. Johnson SL, Tabaei BP, Herman WH.The efficacy and cost of alternative strat-
Standards of Medical Care
S48 DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 care.diabetesjournals.org
egies for systematic screening for type 2diabetes in the U.S. population 45–74years of age. Diabetes Care 2005;28:307–311
19. Harris R, Donahue K, Rathore SS, FrameP, Woolf SH, Lohr KN. Screening adultsfor type 2 diabetes: a review of the evi-dence for the U.S. Preventive ServicesTask Force. Ann Intern Med 2003;138:215–229
20. U.S. Preventive Services Task Force. S.Preventive Services Task Force. S. Pre-ventive Services Task Force: Screeningfor type 2 diabetes mellitus in adults:recommendations and rationale. AnnIntern Med 2003;138:212–214
21. Writing Group for the SEARCH for Dia-betes in Youth Study Group, Dabelea D,Bell RA, D’Agostino RB Jr, Imperatore G,Johansen JM, Linder B, Liu LL, Loots B,Marcovina S, Mayer-Davis EJ, Pettitt DJ,Waitzfelder B. Incidence of diabetes inyouth in the United States. JAMA 2007;297:2716–2724
22. SEARCH for Diabetes in Youth StudyGroup, Liese AD, D’Agostino RB Jr,Hamman RF, Kilgo PD, Lawrence JM,Liu LL, Loots B, Linder B, Marcovina S,Rodriguez B, Standiford D, Williams DE.The burden of diabetes mellitus amongUS youth: prevalence estimates from theSEARCH for Diabetes in Youth Study.Pediatrics 2006;118:1510–1518
23. American Diabetes Association: Type 2diabetes in children and adolescents(Consensus Statement). Diabetes Care2000;23:381–389
24. Lawrence JM, Contreras R, Chen W,Sacks DA. Trends in the prevalence ofpreexisting diabetes and gestational dia-betes mellitus among a racially/ethni-cally diverse population of pregnantwomen, 1999–2005. Diabetes Care2008;31:899–904
25. American Diabetes Association: Gesta-tional diabetes mellitus (Position State-ment). Diabetes Care 2004;27(Suppl.1):S88–S90
26. HAPO Study Cooperative ResearchGroup, Metzger BE, Lowe LP, Dyer AR,Trimble ER, Chaovarindr U, CoustanDR, Hadden DR, McCance DR, Hod M,McIntyre HD, Oats JJ, Persson B, RogersMS, Sacks DA. Hyperglycemia and ad-verse pregnancy outcomes. N Engl J Med2008;358:1991–2002
27. Landon MB, Spong CY, Thom E, Car-penter MW, Ramin SM, Casey B, Wap-ner RJ, Varner MW, Rouse DJ, Thorp JMJr, Sciscione A, Catalano P, Harper M,Saade G, Lain KY, Sorokin Y, PeacemanAM, Tolosa JE, Anderson GB, EuniceKennedy Shriver National Institute ofChild Health and Human DevelopmentMaternal-Fetal Medicine Units Network.A multicenter, randomized trial of treat-ment for mild gestational diabetes.N Engl J Med 2009;361:1339–1348
28. Kim C, Newton KM, Knopp RH. Gesta-tional diabetes and the incidence of type2 diabetes: a systematic review. DiabetesCare 2002;25:1862–1868
29. Lindstrom J, Ilanne-Parikka P, PeltonenM, Aunola S, Eriksson JG, Hemio K, Ha-malainen H, Harkonen P, Keinanen-Kiukaanniemi S, Laakso M, LouherantaA, Mannelin M, Paturi M, Sundvall J,Valle TT, Uusitupa M, Tuomilehto J,Finnish Diabetes Prevention StudyGroup. Sustained reduction in the inci-dence of type 2 diabetes by lifestyle in-tervention: follow-up of the FinnishDiabetes Prevention Study. Lancet 2006;368:1673–1679
30. Li G, Zhang P, Wang J, Gregg EW, YangW, Gong Q, Li H, Li H, Jiang Y, An Y,Shuai Y, Zhang B, Zhang J, ThompsonTJ, Gerzoff RB, Roglic G, Hu Y, BennettPH. The long-term effect of lifestyle in-terventions to prevent diabetes in theChina Da Qing Diabetes PreventionStudy: a 20-year follow-up study. Lancet2008;371:1783–1789
31. Kosaka K, Noda M, Kuzuya T. Preven-tion of type 2 diabetes by lifestyle inter-vention: a Japanese trial in IGT males.Diabetes Res Clin Pract 2005;67:152–162
32. Torgerson JS, Hauptman J, Boldrin MN,Sjostrom L. XENical in the prevention ofdiabetes in obese subjects (XENDOS)study: a randomized study of orlistat asan adjunct to lifestyle changes for theprevention of type 2 diabetes in obesepatients. Diabetes Care 2004;27:155–161
33. Kawamori R, Tajima N, Iwamoto Y,Kashiwagi A, Shimamoto K, Kaku K,Voglibose Ph-3 Study Group. Voglib-ose for prevention of type 2 diabetesmellitus: a randomised, double-blindtrial in Japanese individuals with im-paired glucose tolerance. Lancet 2009;373:1607–1614
34. DeFronzo RA, for ACT NOW StudyGroup. ACTos NOW Study for the Pre-vention of Diabetes (ACT NOW) Study.Late-breaking abstract presented at 68thAnnual Scientific Sessions of the Ameri-can Diabetes Association, 6 June 2008,San Francisco, CA
35. Gerstein HC. Point: If it is important toprevent type 2 diabetes, it is important toconsider all proven therapies within acomprehensive approach. Diabetes Care2007;30:432–434
36. Nathan DM, Davidson MB, DeFronzoRA, Heine RJ, Henry RR, Pratley R, Zin-man B, American Diabetes Association.Impaired fasting glucose and impairedglucose tolerance: implications for care.Diabetes Care 2007;30:753–759
37. American Diabetes Association: Consen-sus statement on self-monitoring ofblood glucose. Diabetes Care 1987;10:95–99
38. American Diabetes Association: Self-monitoring of blood glucose. DiabetesCare 1994;17:81–86
39. Welschen LM, Bloemendal E, Nijpels G,Dekker JM, Heine RJ, Stalman WA,Bouter LM. Self-monitoring of bloodglucose in patients with type 2 diabeteswho are not using insulin: a systematicreview. Diabetes Care 2005;28:1510–1517
40. Farmer A, Wade A, Goyder E, YudkinP, French D, Craven A, Holman R,Kinmonth AL, Neil A. Impact of selfmonitoring of blood glucose in the man-agement of patients with non-insulintreated diabetes: open parallel grouprandomised trial. BMJ 2007;335:132
41. O’Kane MJ, Bunting B, Copeland M,Coates VE, ESMON study group. Effi-cacy of self monitoring of blood glucosein patients with newly diagnosed type 2diabetes (ESMON study): randomisedcontrolled trial. BMJ 2008;336:1174–1177
42. Simon J, Gray A, Clarke P, Wade A, NeilA, Farmer A, Diabetes Glycaemic Educa-tion and Monitoring Trial Group. Costeffectiveness of self monitoring of bloodglucose in patients with non-insulintreated type 2 diabetes: economic evalu-ation of data from the DiGEM trial. BMJ2008;336:1177–1180
43. Sacks DB, Bruns DE, Goldstein DE, Ma-claren NK, McDonald JM, Parrott M.Guidelines and recommendations forlaboratory analysis in the diagnosis andmanagement of diabetes mellitus. ClinChem 2002;48:436–472
44. Juvenile Diabetes Research FoundationContinuous Glucose Monitoring StudyGroup, Tamborlane WV, Beck RW,Bode BW, Buckingham B, Chase HP,Clemons R, Fiallo-Scharer R, Fox LA,Gilliam LK, Hirsch IB, Huang ES, Koll-man C, Kowalski AJ, Laffel L, LawrenceJM, Lee J, Mauras N, O’Grady M, RuedyKJ, Tansey M, Tsalikian E, Weinzimer S,Wilson DM, Wolpert H, Wysocki T,Xing D: Continuous glucose monitoringand intensive treatment of type 1 diabe-tes. N Engl J Med 2008; 359:1464–1476
45. Juvenile Diabetes Research FoundationContinuous Glucose Monitoring StudyGroup: The effect of continuous glucosemonitoring in well-controlled type 1 di-abetes. Diabetes Care 2009;32:1378–1383
46. Stratton IM, Adler AI, Neil HA, Mat-thews DR, Manley SE, Cull CA, HaddenD, Turner RC, Holman RR. Associationof glycaemia with macrovascular andmicrovascular complications of type 2diabetes (UKPDS 35): prospective ob-servational study. BMJ 2000;321:405–412
47. Cagliero E, Levina EV, Nathan DM. Im-mediate feedback of HbA1c levels im-proves glycemic control in type 1 and
Position Statement
care.diabetesjournals.org DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 S49

insulin-treated type 2 diabetic patients.Diabetes Care 1999;22:1785–1789
48. Miller CD, Barnes CS, Phillips LS, Zi-emer DC, Gallina DL, Cook CB, Mary-man SD, El-Kebbi IM. Rapid A1cavailability improves clinical decision-making in an urban primary care clinic.Diabetes Care 2003;26:1158–1163
49. Nathan DM, Kuenen J, Borg R, Zheng H,Schoenfeld D, Heine RJ, A1c-DerivedAverage Glucose Study Group. Translat-ing the A1C assay into estimated averageglucose values. Diabetes Care 2008;31:1473–1478
50. Rohlfing CL, Wiedmeyer HM, Little RR,England JD, Tennill A, Goldstein DE.Defining the relationship betweenplasma glucose and HbA(1c): analysis ofglucose profiles and HbA(1c) in the Di-abetes Control and Complications Trial.Diabetes Care 2002;25:275–278
51. Diabetes Research in Children Network(DirecNet) Study Group, Wilson DM,Kollman. Relationship of A1C to glucoseconcentrations in children with type 1diabetes: assessments by high-frequencyglucose determinations by sensors. Dia-betes Care 2008;31:381–385
52. Skyler JS, Bergenstal R, Bonow RO, BuseJ, Deedwania P, Gale EA, Howard BV,Kirkman MS, Kosiborod M, Reaven P,Sherwin RS, American Diabetes Associ-ation, American College of CardiologyFoundation, American Heart Associa-tion. Intensive glycemic control and theprevention of cardiovascular events: im-plications of the ACCORD, ADVANCE,and VA diabetes trials: a position state-ment of the American Diabetes Associa-tion and a scientific statement of theAmerican College of Cardiology Foun-dation and the American Heart Associa-tion. Diabetes Care 2009;32:187–192
53. The effect of intensive treatment of dia-betes on the development and progres-sion of long-term complications ininsulin-dependent diabetes mellitus.The Diabetes Control and Complica-tions Trial Research Group. N EnglJ Med 1993;329:977–986
54. Retinopathy and nephropathy in pa-tients with type 1 diabetes four years af-ter a trial of intensive therapy. TheDiabetes Control and ComplicationsTrial/Epidemiology of Diabetes Interven-tions and Complications Research Group.N Engl J Med 2000;342:381–389
55. Martin CL, Albers J, Herman WH,Cleary P, Waberski B, Greene DA,Stevens MJ, Feldman EL, DCCT/EDICResearch Group. Neuropathy among thediabetes control and complications trialcohort 8 years after trial completion. Di-abetes Care 2006;29:340–344
56. Ohkubo Y, Kishikawa H, Araki E, MiyataT, Isami S, Motoyoshi S, Kojima Y, Fu-ruyoshi N, Shichiri M. Intensive insulintherapy prevents the progression of dia-
betic microvascular complications inJapanese patients with non-insulin-de-pendent diabetes mellitus: a randomizedprospective 6-year study. Diabetes ResClin Pract 1995;28:103–117
57. Effect of intensive blood-glucose controlwith metformin on complications inoverweight patients with type 2 diabetes(UKPDS 34): UK Prospective DiabetesStudy (UKPDS) Group. Lancet 1998;352:854–865
58. Intensive blood-glucose control withsulphonylureas or insulin comparedwith conventional treatment and risk ofcomplications in patients with type 2 di-abetes (UKPDS 33): UK Prospective Di-abetes Study (UKPDS) Group. Lancet1998;352:837–853
59. Holman RR, Paul SK, Bethel MA, Mat-thews DR, Neil HA: 10-Year follow-up ofintensive glucose control in type 2 dia-betes. N Engl J Med 2008;359:1577–1589
60. Duckworth W, Abraira C, Moritz T,Reda D, Emanuele N, Reaven PD, ZieveFJ, Marks J, Davis SN, Hayward R, War-ren SR, Goldman S, McCarren M, VitekME, Henderson WG, Huang GD, VADTInvestigators. Glucose control and vas-cular complications in veterans withtype 2 diabetes. N Engl J Med 2009;360:129–139
61. Moritz T, Duckworth W, Abraira C. Vet-erans Affairs diabetes trial–corrections.N Engl J Med 2009;361:1024–1025
62. Lawson ML, Gerstein HC, Tsui E, Zin-man B. Effect of intensive therapy onearly macrovascular disease in young in-dividuals with type 1 diabetes: A system-atic review and meta-analysis. DiabetesCare 1999;22(Suppl. 2):B35–B39
63. ADVANCE Collaborative Group, PatelA, MacMahon S, Chalmers J, Neal B, Bil-lot L, Woodward M, Marre M, CooperM, Glasziou P, Grobbee D, Hamet P,Harrap S, Heller S, Liu L, Mancia G, Mo-gensen CE, Pan C, Poulter N, Rodgers A,Williams B, Bompoint S, de Galan BE,Joshi R, Travert F. Intensive blood glu-cose control and vascular outcomes inpatients with type 2 diabetes. N EnglJ Med 2008;358:2560–2572
64. Selvin E, Marinopoulos S, Berkenblit G,Rami T, Brancati FL, Powe NR, GoldenSH. Meta-analysis: glycosylated hemo-globin and cardiovascular disease in di-abetes mellitus. Ann Intern Med 2004;141:421–431
65. Stettler C, Allemann S, Juni P, Cull CA,Holman RR, Egger M, Krahenbuhl S,Diem P. Glycemic control and macro-vascular disease in types 1 and 2 diabetesmellitus: Meta-analysis of randomizedtrials. Am Heart J 2006;152:27–38
66. Nathan DM, Cleary PA, Backlund JY,Genuth SM, Lachin JM, Orchard TJ,Raskin P, Zinman B, Diabetes Controland Complications Trial/Epidemiology
of Diabetes Interventions and Complica-tions (DCCT/EDIC) Study ResearchGroup. Intensive diabetes treatment andcardiovascular disease in patients withtype 1 diabetes. N Engl J Med 2005;353:2643–2653
67. Diabetes Control and ComplicationsTrial/Epidemiology of Diabetes Inter-ventions and Complications (DCCT/EDIC) Research Group, Nathan DM,Zinman B, Cleary PA, Backlund JY, Ge-nuth S, Miller R, Orchard TJ. Modern-day clinical course of type 1 diabetesmellitus after 30 years’ duration: the di-abetes control and complications trial/epidemiology of diabetes interventionsand complications and Pittsburgh epide-miology of diabetes complications expe-rience (1983–2005). Arch Intern Med2009;169:1307–1316
68. Action to Control Cardiovascular Risk inDiabetes Study Group, Gerstein HC,Miller ME, Byington RP, Goff DC Jr, Big-ger JT, Buse JB, Cushman WC, GenuthS, Ismail-Beigi F, Grimm RH Jr, Probst-field JL, Simons-Morton DG, FriedewaldWT. Effects of intensive glucose lower-ing in type 2 diabetes. N Engl J Med2008;358:2545–2559
69. Duckworth W. VADT Results. Late-breaking abstract presented at 68th An-nual Scientific Sessions of the AmericanDiabetes Association, 6 June 2008, SanFrancisco, CA
70. Reaven PD, Moritz TE, Schwenke DC,Anderson RJ, Criqui M, Detrano R,Emanuele N, Kayshap M, Marks J, Mu-daliar S, Rao RH, Shah JH, Goldman S,Reda DJ, McCarren M, Abraira C, Duck-worth W: Intensive glucose loweringtherapy reduces cardiovascular diseaseevents in VADT participants with lowercalcified coronary atherosclerosis. Dia-betes 2009;59:2642–2648
71. Turnbull FM, Abraira C, Anderson RJ,Byington RP, Chalmers JP, DuckworthWC, Evans GW, Gerstein HC, HolmanRR, Moritz TE, Neal BC, Ninomiya T,Patel AA, Paul SK, Travert F, WoodwardM: Intensive glucose control and macro-vascular outcomes in type 2 diabetes.Diabetologia 2009;52:2288–2298
72. American Diabetes Association: Post-prandial blood glucose (ConsensusStatement). Diabetes Care 2001;24:775–778
73. Ceriello A, Taboga C, Tonutti L, Quagli-aro L, Piconi L, Bais B, Da Ros R, Motz E.Evidence for an independent and cu-mulative effect of postprandial hyper-triglyceridemia and hyperglycemia onendothelial dysfunction and oxidativestress generation: effects of short- andlong-term simvastatin treatment. Circu-lation 2002;106:1211–1218
74. Raz I, Wilson PW, Strojek K, Kowalska I,Bozikov V, Gitt AK, Jermendy G, Cam-paigne BN, Kerr L, Milicevic Z, Jacober
Standards of Medical Care
S50 DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 care.diabetesjournals.org

SJ. Effects of prandial versus fasting gly-cemia on cardiovascular outcomes intype 2 diabetes: the HEART2D trial. Di-abetes Care 2009;32:381–386
75. Metzger BE, Buchanan TA, Coustan DR,de Leiva A, Dunger DB, Hadden DR,Hod M, Kitzmiller JL, Kjos SL, Oats JN,Pettitt DJ, Sacks DA, Zoupas C. Sum-mary and recommendations of the FifthInternational Workshop-Conference onGestational Diabetes Mellitus. DiabetesCare 2007;30(Suppl. 2):S251–S260
76. Kitzmiller JL, Block JM, Brown FM,Catalano PM, Conway DL, Coustan DR,Gunderson EP, Herman WH, HoffmanLD, Inturrisi M, Jovanovic LB, Kjos SI,Knopp RH, Montoro MN, Ogata ES,Paramsothy P, Reader DM, Rosenn BM,Thomas AM, Kirkman MS. Managingpreexisting diabetes for pregnancy: sum-mary of evidence and consensus recom-mendations for care. Diabetes Care2008;31:1060–1079
77. DeWitt DE, Hirsch IB. Outpatient insu-lin therapy in type 1 and type 2 diabetesmellitus: scientific review. JAMA 2003;289:2254–2264
78. Rosenstock J, Dailey G, Massi-BenedettiM, Fritsche A, Lin Z, Salzman A. Re-duced hypoglycemia risk with insulinglargine: a meta-analysis comparing in-sulin glargine with human NPH insulinin type 2 diabetes. Diabetes Care 2005;28:950–955
79. Mooradian AD, Bernbaum M, Albert SG.Narrative review: a rational approach tostarting insulin therapy. Ann Intern Med2006;145:125–134
80. Nathan DM, Buse JB, Davidson MB,Heine RJ, Holman RR, Sherwin R, Zin-man B. Management of hyperglycemia intype 2 diabetes: a consensus algorithmfor the initiation and adjustment of ther-apy: a consensus statement from theAmerican Diabetes Association and theEuropean Association for the Study ofDiabetes. Diabetes Care 2006;29:1963–1972
81. Nathan DM, Buse JB, Davidson MB, Fer-rannini E, Holman RR, Sherwin R, Zin-man B, American Diabetes Association,European Association for Study of Dia-betes. Medical management of hypergly-cemia in type 2 diabetes: a consensusalgorithm for the initiation and adjust-ment of therapy: a consensus statementof the American Diabetes Associationand the European Association for theStudy of Diabetes. Diabetes Care 2009;32:193–203
82. Bantle JP, Wylie-Rosett J, Albright AL,Apovian CM, Clark NG, Franz MJ,Hoogwerf BJ, Lichtenstein AH, Mayer-Davis E, Mooradian AD, Wheeler ML.Nutrition recommendations and inter-ventions for diabetes—2006. DiabetesCare 2006;29:2140–2157
83. DAFNE Study Group. Training in flexi-
ble, intensive insulin management to en-able dietary freedom in people with type1 diabetes: dose adjustment for normaleating (DAFNE) randomised controlledtrial. BMJ 2002;325:746
84. Franz MJ, Monk A, Barry B, McClain K,Weaver T, Cooper N, Upham P, Bergen-stal R, Mazze RS. Effectiveness of medi-cal nutrition therapy provided bydietitians in the management of non-in-sulin-dependent diabetes mellitus: arandomized, controlled clinical trial.J Am Diet Assoc 1995;95:1009–1017
85. Goldhaber-Fiebert JD, Goldhaber-FiebertSN, Tristan ML, Nathan DM. Randomizedcontrolled community-based nutritionand exercise intervention improves glyce-mia and cardiovascular risk factors in type2 diabetic patients in rural Costa Rica. Di-abetes Care 2003;26:24–29
86. Lemon CC, Lacey K, Lohse B, HubacherDO, Klawitter B, Palta M. Outcomesmonitoring of health, behavior, andquality of life after nutrition interventionin adults with type 2 diabetes. J Am DietAssoc 2004;104:1805–1815
87. Miller CK, Edwards L, Kissling G, San-ville L. Nutrition education improvesmetabolic outcomes among older adultswith diabetes mellitus: results from arandomized controlled trial. Prev Med2002;34:252–259
88. Wilson C, Brown T, Acton K, Gilliland S.Effects of clinical nutrition educationand educator discipline on glycemiccontrol outcomes in the Indian healthservice. Diabetes Care 2003;26:2500–2504
89. Graber AL, Elasy TA, Quinn D, Wolff K,Brown A. Improving glycemic control inadults with diabetes mellitus: shared re-sponsibility in primary care practices.South Med J 2002;95:684–690
90. Gaetke LM, Stuart MA, Truszczynska H.A single nutrition counseling sessionwith a registered dietitian improvesshort-term clinical outcomes for ruralKentucky patients with chronic diseases.J Am Diet Assoc 2006;106:109–112
91. Yu-Poth S, Zhao G, Etherton T, NaglakM, Jonnalagadda S, Kris-Etherton PM.Effects of the National Cholesterol Ed-ucation Program’s Step I and Step IIdietary intervention programs on car-diovascular disease risk factors: a meta-analysis. Am J Clin Nutr 1999;69:632–646
92. Van Horn L, McCoin M, Kris-EthertonPM, Burke F, Carson JA, ChampagneCM, Karmally W, Sikand G. The evi-dence for dietary prevention and treat-ment of cardiovascular disease. J AmDiet Assoc 2008;108:287–331
93. Appel LJ, Moore TJ, Obarzanek E,Vollmer WM, Svetkey LP, Sacks FM,Bray GA, Vogt TM, Cutler JA,Windhauser MM, Lin PH, Karanja N. Aclinical trial of the effects of dietary pat-
terns on blood pressure. DASH Collab-orative Research Group. N Engl J Med1997;336:1117–1124
94. Norris SL, Zhang X, Avenell A, Gregg E,Bowman B, Schmid CH, Lau J. Long-term effectiveness of weight-loss inter-ventions in adults with pre-diabetes: areview. Am J Prev Med 2005;28:126–139
95. Klein S, Sheard NF, Pi-Sunyer X, Daly A,Wylie-Rosett J, Kulkarni K, Clark NG,American Diabetes Association, NorthAmerican Association for the Study ofObesity, American Society for ClinicalNutrition. Weight management throughlifestyle modification for the preventionand management of type 2 diabetes: ra-tionale and strategies: a statement ofthe American Diabetes Association, theNorth American Association for theStudy of Obesity, and the American So-ciety for Clinical Nutrition. DiabetesCare 2004;27:2067–2073
96. Norris SL, Zhang X, Avenell A, Gregg E,Schmid CH, Kim C, Lau J. Efficacy ofpharmacotherapy for weight loss inadults with type 2 diabetes mellitus: ameta-analysis. Arch Intern Med 2004;164:1395–1404
97. Wolf AM, Conaway MR, Crowther JQ,Hazen KY, L Nadler J, Oneida B, Bovb-jerg VE, Improving Control with Activityand Nutrition (ICAN) Study. Translat-ing lifestyle intervention to practice inobese patients with type 2 diabetes: Im-proving Control with Activity and Nutri-tion (ICAN) study. Diabetes Care 2004;27:1570–1576
98. Manning RM, Jung RT, Leese GP, New-ton RW. The comparison of four weightreduction strategies aimed at overweightpatients with diabetes mellitus: four-yearfollow-up.DiabetMed1998;15:497–502
99. Shai I, Schwarzfuchs D, Henkin Y, Sha-har DR, Witkow S, Greenberg I, GolanR, Fraser D, Bolotin A, Vardi H, Tangi-Rozental O, Zuk-Ramot R, Sarusi B,Brickner D, Schwartz Z, Sheiner E,Marko R, Katorza E, Thiery J, FiedlerGM, Bluher M, Stumvoll M, StampferMJ, Dietary Intervention RandomizedControlled Trial (DIRECT) Group.Weight loss with a low-carbohydrate,Mediterranean, or low-fat diet. N EnglJ Med 2008;359:229–241
100. Franz MJ, VanWormer JJ, Crain AL,Boucher JL, Histon T, Caplan W, Bow-man JD, Pronk NP. Weight-loss out-comes: a systematic review and meta-analysis of weight-loss clinical trials witha minimum 1-year follow-up. J Am DietAssoc 2007;107:1755–1767
101. Look AHEAD Research Group, Pi-Su-nyer X, Blackburn G, Brancati FL, BrayGA, Bright R, Clark JM, Curtis JM, Es-peland MA, Foreyt JP, Graves K, HaffnerSM, Harrison B, Hill JO, Horton ES, Ja-
Position Statement
care.diabetesjournals.org DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 S51
kicic J, Jeffery RW, Johnson KC, Kahn S,Kelley DE, Kitabchi AE, Knowler WC,Lewis CE, Maschak-Carey BJ, Montgom-ery B, Nathan DM, Patricio J, Peters A,Redmon JB, Reeves RS, Ryan DH, SaffordM, Van Dorsten B, Wadden TA, Wagen-knecht L, Wesche-Thobaben J, Wing RR,Yanovski SZ. Reduction in weight and car-diovascular disease risk factors in individ-uals with type 2 diabetes: one-year resultsof the look AHEAD trial. Diabetes Care2007;30:1374–1383
102. Foster GD, Wyatt HR, Hill JO,McGuckin BG, Brill C, Mohammed BS,Szapary PO, Rader DJ, Edman JS, KleinS. A randomized trial of a low-carbohy-drate diet for obesity. N Engl J Med2003;348:2082–2090
103. Stern L, Iqbal N, Seshadri P, ChicanoKL, Daily DA, McGrory J, Williams M,Gracely EJ, Samaha FF. The effects oflow-carbohydrate versus conventionalweight loss diets in severely obeseadults: one-year follow-up of a random-ized trial. Ann Intern Med 2004;140:778–785
104. Gardner CD, Kiazand A, Alhassan S,Kim S, Stafford RS, Balise RR, KraemerHC, King AC. Comparison of the At-kins, Zone, Ornish, and LEARN dietsfor change in weight and related riskfactors among overweight premeno-pausal women. JAMA 2007;297:969 –977
105. Nordmann AJ, Nordmann A, Briel M,Keller U, Yancy WS, Jr, Brehm BJ,Bucher HC. Effects of low-carbohydratevs low-fat diets on weight loss and car-diovascular risk factors: a meta-analysisof randomized controlled trials. Arch In-tern Med 2006;166:285–293
106. Institute of Medicine: DIetary ReferenceIntakes: Energy, Carbohydrate, Fiber, Fat,Fatty Acids, Cholesterol, Protein, andAmino Acids. Washington, DC, NationalAcademies Press, 2002
107. Barnard ND, Cohen J, Jenkins DJ, Turner-McGrievy G, Gloede L, Jaster B, Seidl K,Green AA, Talpers S. A low-fat vegandiet improves glycemic control and car-diovascular risk factors in a randomizedclinical trial in individuals with type 2diabetes. Diabetes Care 2006;29:1777–1783
108. Turner-McGrievy GM, Barnard ND, Co-hen J, Jenkins DJ, Gloede L, Green AA.Changes in nutrient intake and dietaryquality among participants with type 2diabetes following a low-fat vegan diet ora conventional diabetes diet for 22weeks. J Am Diet Assoc 2008;108:1636–1645
109. Franz MJ, Bantle JP, Beebe CA, BrunzellJD, Chiasson JL, Garg A, HolzmeisterLA, Hoogwerf B, Mayer-Davis E, Moora-dian AD, Purnell JQ, Wheeler M. Evi-dence-based nutrition principles andrecommendations for the treatment and
prevention of diabetes and related com-plications. Diabetes Care 2002;25:148–198
110. Buchwald H, Estok R, Fahrbach K, BanelD, Jensen MD, Pories WJ, Bantle JP,Sledge I. Weight and type 2 diabetes af-ter bariatric surgery: systematic reviewand meta-analysis. Am J Med 2009;122:248–256
111. Dixon JB, O’Brien PE, Playfair J, Chap-man L, Schachter LM, Skinner S, Proi-etto J, Bailey M, Anderson M. Adjustablegastric banding and conventional ther-apy for type 2 diabetes: a randomizedcontrolled trial. JAMA 2008;299:316–323
112. Buchwald H, Estok R, Fahrbach K, BanelD, Sledge I. Trends in mortality in bari-atric surgery: a systematic review andmeta-analysis. Surgery 2007;142:621–632
113. Sjostrom L, Narbro K, Sjostrom CD,Karason K, Larsson B, Wedel H, LystigT, Sullivan M, Bouchard C, Carlsson B,Bengtsson C, Dahlgren S, GummessonA, Jacobson P, Karlsson J, Lindroos AK,Lonroth H, Naslund I, Olbers T, StenlofK, Torgerson J, Agren G, Carlsson LM,Swedish Obese Subjects Study. Effects ofbariatric surgery on mortality in Swedishobese subjects. N Engl J Med 2007;357:741–752
114. Piette JD, Glasgow RE: Sttategies for im-proving behavioral and health outcomesamong people with diabetes: self man-agement education. In Evidence-BasedDiabetes Care. Gerstein HC, Hayes RB,Eds. Ontario, Canada, BC Decker, 2000
115. Norris SL, Engelgau MM, Narayan KM.Effectiveness of self-management train-ing in type 2 diabetes: a systematic re-view of randomized controlled trials.Diabetes Care 2001;24:561–587
116. Norris SL, Lau J, Smith SJ, Schmid CH,Engelgau MM. Self-management educa-tion for adults with type 2 diabetes: ameta-analysis of the effect on glycemiccontrol. Diabetes Care 2002;25:1159–1171
117. Gary TL, Genkinger JM, Guallar E, Pey-rot M, Brancati FL. Meta-analysis of ran-domized educational and behavioralinterventions in type 2 diabetes. Diabe-tes Educ 2003;29:488–501
118. Steed L, Cooke D, Newman S. A system-atic review of psychosocial outcomesfollowing education, self-managementand psychological interventions in dia-betes mellitus. Patient Educ Couns2003;51:5–15
119. Ellis SE, Speroff T, Dittus RS, Brown A,Pichert JW, Elasy TA. Diabetes patienteducation: a meta-analysis and meta-re-gression. Patient Educ Couns 2004;52:97–105
120. Warsi A, Wang PS, LaValley MP, AvornJ, Solomon DH. Self-management edu-cation programs in chronic disease: a
systematic review and methodologicalcritique of the literature. Arch InternMed 2004;164:1641–1649
121. Funnell MM, Brown TL, Childs BP, HaasLB, Hosey GM, Jensen B, Maryniuk M,Peyrot M, Piette JD, Reader D, SiminerioLM, Weinger K, Weiss MA. Nationalstandards for diabetes self-managementeducation. Diabetes Care 2007;30:1630–1637
122. Mulcahy K, Maryniuk M, Peeples M, Pey-rot M, Tomky D, Weaver T, Yarborough P.Diabetes self-management education coreoutcomes measures. Diabetes Educ29:768- 2003;84:787
123. Glasgow RE, Peeples M, Skovlund SE.Where is the patient in diabetes perfor-mance measures? The case for includingpatient-centered and self-managementmeasures. Diabetes Care 2008;31:1046–1050
124. Barker JM, Goehrig SH, Barriga K, Hoff-man M, Slover R, Eisenbarth GS, NorrisJM, Klingensmith GJ, Rewers M, DAISYstudy. Clinical characteristics of chil-dren diagnosed with type 1 diabetesthrough intensive screening and follow-up. Diabetes Care 2004;27:1399–1404
125. Cochran J, Conn VS. Meta-analysis ofquality of life outcomes following diabe-tes self-management training. DiabetesEduc 2008;34:815–823
126. Fisher EB, Thorpe CT, Devellis BM, De-vellis RF. Healthy coping, negative emo-tions, and diabetes management: asystematic review and appraisal. Diabe-tes Educ 2007;33:1080–1103
127. Robbins JM, Thatcher GE, Webb DA,Valdmanis VG. Nutritionist visits, diabe-tes classes, and hospitalization rates andcharges: the Urban Diabetes Study. Dia-betes Care 2008;31:655–660
128. Renders CM, Valk GD, Griffin SJ, Wag-ner EH, Eijk Van JT, Assendelft WJ. In-terventions to improve the managementof diabetes in primary care, outpatient,and community settings: a systematic re-view. Diabetes Care 2001;24:1821–1833
129. Polonsky WH, Earles J, Smith S, PeaseDJ, Macmillan M, Christensen R, TaylorT, Dickert J, Jackson RA. Integratingmedical management with diabetes self-management training: a randomizedcontrol trial of the Diabetes OutpatientIntensive Treatment program. DiabetesCare 2003;26:3048–3053
130. Anderson RM, Funnell MM, NwankwoR, Gillard ML, Oh M, Fitzgerald JT.Evaluating a problem-based empower-ment program for African Americanswith diabetes: results of a randomizedcontrolled trial. Ethn Dis 2005;15:671– 678
131. Brown SA, Blozis SA, Kouzekanani K,Garcia AA, Winchell M, Hanis CL. Dos-age effects of diabetes self-managementeducation for Mexican Americans: the
Standards of Medical Care
S52 DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 care.diabetesjournals.org
Starr County Border Health Initiative.Diabetes Care 2005;28:527–532
132. Glazier RH, Bajcar J, Kennie NR, WillsonK. A systematic review of interventionsto improve diabetes care in socially dis-advantaged populations. Diabetes Care2006;29:1675–1688
133. Sarkisian CA, Brown AF, Norris KC,Wintz RL, Mangione CM. A systematicreview of diabetes self-care interventionsfor older, African American, or Latinoadults. Diabetes Educ 2003;29:467–479
134. Chodosh J, Morton SC, Mojica W, Ma-glione M, Suttorp MJ, Hilton L, RhodesS, Shekelle P. Meta-analysis: chronic dis-ease self-management programs forolder adults. Ann Intern Med 2005;143:427–438
135. Peyrot M, Rubin RR. Behavioral and psy-chosocial interventions in diabetes: aconceptual review. Diabetes Care 2007;30:2433–2440
136. Rickheim PL, Weaver TW, Flader JL,Kendall DM. Assessment of group versusindividual diabetes education: a ran-domized study. Diabetes Care 2002;25:269–274
137. Trento M, Passera P, Borgo E, TomalinoM, Bajardi M, Cavallo F, Porta M. A5-year randomized controlled study oflearning, problem solving ability, andquality of life modifications in peoplewith type 2 diabetes managed by groupcare. Diabetes Care 2004;27:670–675
138. Deakin T, McShane CE, Cade JE, Wil-liams RD: Group based training for self-management strategies in people withtype 2 diabetes mellitus. Cochrane Da-tabase Syst Rev CD003417, 2005
139. Heisler, M. Building Peer Support Pro-grams to Manage Chronic Disease: SevenModels for Success. Oakland, CA, Califor-nia Health Care Foundation, 2006
140. Foster G, Taylor SJ, Eldridge SE, RamsayJ, Griffiths CJ: Self-management educa-tion programmes by lay leaders for peo-ple with chronic conditions. CochraneDatabase Syst Rev CD005108, 2007
141. Norris SL, Chowdhury FM, Van Le K,Horsley T, Brownstein JN, Zhang X, JackL Jr, Satterfield DW. Effectiveness ofcommunity health workers in the care ofpersons with diabetes. Diabet Med2006;23:544–556
142. Duncan I, Birkmeyer C, Coughlin S, LiQE, Sherr D, Boren S. Assessing thevalue of diabetes education. DiabetesEduc 2009;35:752–760
143. Sigal RJ, Kenny GP, Wasserman DH,Castaneda-Sceppa C. Physical activity/exercise and type 2 diabetes. DiabetesCare 2004;27:2518–2539
144. Wasserman DH, Zinman B. Exercise inindividuals with IDDM. Diabetes Care1994;17:924–937
145. Boule NG, Haddad E, Kenny GP, WellsGA, Sigal RJ. Effects of exercise on gly-cemic control and body mass in type 2
diabetes mellitus: a meta-analysis ofcontrolledclinicaltrials.JAMA2001;286:1218–1227
146. Boule NG, Kenny GP, Haddad E, WellsGA, Sigal RJ. Meta-analysis of the effectof structured exercise training on cardio-respiratory fitness in Type 2 diabetesmellitus. Diabetologia 2003;46:1071–1081
147. U.S. Department of Health and HumanServices. 2008 Physical Activity Guide-lines for Americans. Atlanta, GA,Centers for Disease Control and Pre-vention, 2008
148. Cauza E, Hanusch-Enserer U, Strasser B,Ludvik B, Metz-Schimmerl S, Pacini G,Wagner O, Georg P, Prager R, Kostner K,Dunky A, Haber P. The relative benefitsof endurance and strength training onthe metabolic factors and muscle func-tion of people with type 2 diabetes mel-litus. Arch Phys Med Rehabil 2005;86:1527–1533
149. Dunstan DW, Daly RM, Owen N, JolleyD, De Courten M, Shaw J, Zimmet P.High-intensity resistance training im-proves glycemic control in older patientswith type 2 diabetes. Diabetes Care2002;25:1729–1736
150. Castaneda C, Layne JE, Munoz-OriansL, Gordon PL, Walsmith J, Foldvari M,Roubenoff R, Tucker KL, Nelson ME. Arandomized controlled trial of resistanceexercise training to improve glycemiccontrol in older adults with type 2 dia-betes. Diabetes Care 2002;25:2335–2341
151. Sigal RJ, Kenny GP, Boule NG, WellsGA, Prud’homme D, Fortier M, Reid RD,Tulloch H, Coyle D, Phillips P, JenningsA, Jaffey J. Effects of aerobic training, re-sistance training, or both on glycemiccontrol in type 2 diabetes: a randomizedtrial. Ann Intern Med 2007;147:357–369
152. Bax JJ, Young LH, Frye RL, Bonow RO,Steinberg HO, Barrett EJ, ADA. Screen-ing for coronary artery disease in pa-tients with diabetes. Diabetes Care 2007;30:2729–2736
153. Berger M, Berchtold P, Cuppers HJ,Drost H, Kley HK, Muller WA,Wiegelmann W, Zimmerman-TelschowH, Gries FA, Kruskemper HL, Zimmer-mann H. Metabolic and hormonal ef-fects of muscular exercise in juveniletype diabetics. Diabetologia 1977;13:355–365
154. American Diabetes Association: Physicalactivity/exercise and diabetes (PositionStatement). Diabetes Care 2004;27(Suppl. 1):S58–S62
155. Berger M: Adjustment of insulin and oralagent therapy. In Handbook of Exercise inDiabetes. 2nd ed. Ruderman N, DevlinJTSSH, Krisska A, Eds. Alexandria, VA,American Diabetes Association, 2002, p.365–376
156. Aiello LP, Wong J, Cavallerano J, BursellSE, Aiello LM: Retinopathy. In Handbookof Exercise in Diabetes. 2nd ed. Ru-derman N, Devlin JT, Kriska A, Eds.Alexandria, VA, American Diabetes As-sociation, 2002, p. 401–413
157. Lemaster JW, Reiber GE, Smith DG,Heagerty PJ, Wallace C. Daily weight-bearing activity does not increase therisk of diabetic foot ulcers. Med SciSports Exerc 2003;35:1093–1099
158. Vinik A, Erbas T: Neuropathy. In Hand-book of Exercise in Diabetes. 2nd ed. Ru-derman N, Devlin JT, Kriska A, Eds.Alexandria, VA, American Diabetes As-sociation, 2002, p. 463–496
159. Wackers FJ, Young LH, Inzucchi SE,Chyun DA, Davey JA, Barrett EJ,Taillefer R, Wittlin SD, Heller GV, Filip-chuk N, Engel S, Ratner RE, IskandrianAE, Detection of Ischemia in Asymp-tomatic Diabetics Investigators. Detec-tion of silent myocardial ischemia inasymptomatic diabetic subjects: theDIAD study. Diabetes Care 2004;27:1954–1961
160. Valensi P, Sachs RN, Harfouche B,Lormeau B, Paries J, Cosson E, Paycha F,Leutenegger M, Attali JR. Predictivevalue of cardiac autonomic neuropathyin diabetic patients with or without si-lent myocardial ischemia. Diabetes Care2001;24:339–343
161. Mogensen CE: Nephropathy. In Hand-book of Exercise in Diabetes. 2nd ed. Ru-derman N, Devlin JT, Kriska A, Eds.Alexandria, VA, American Diabetes As-sociation, 2002, p. 433–449
162. Anderson RJ, Grigsby AB, Freedland KE,de Groot M, McGill JB, Clouse RE, Lust-man PJ. Anxiety and poor glycemic con-trol: a meta-analytic review of theliterature. Int J Psychiatry Med 2002;32:235–247
163. Delahanty LM, Grant RW, Wittenberg E,Bosch JL, Wexler DJ, Cagliero E, MeigsJB. Association of diabetes-related emo-tional distress with diabetes treatment inprimary care patients with Type 2 diabe-tes. Diabet Med 2007;24:48–54
164. American Diabetes Association: Psycho-social factors affecting adherence, qual-ity of life, and well-being: HelpingPatients cope. In Medical Management ofType 1 Diabetes. 5 ed. Francine R. Kauf-man, Ed. Alexandria, VA, American Di-abetes Association, 2008, p. 173–193
165. Fisher L, Skaff MM, Mullan JT, Arean P,Mohr D, Masharani U, Glasgow R, Lau-rencin G. Clinical depression versus dis-tress among patients with type 2diabetes: not just a question of seman-tics. Diabetes Care 2007;30:542–548
166. Surwit RS, Schneider MS, Feinglos MN.Stress and diabetes mellitus. DiabetesCare 1992;15:1413–1422
167. McCulloch DK, Glasgow RE, HampsonSE, Wagner E. A systematic approach to
Position Statement
care.diabetesjournals.org DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 S53

diabetes management in the post-DCCTera. Diabetes Care 1994;17:765–769
168. Rubin RR, Peyrot M. Psychological is-sues and treatments for people with di-abetes. J Clin Psychol 2001;57:457–478
169. Jacobson AM. Depression and diabetes.Diabetes Care 1993;16:1621–1623
170. Lustman PJ, Griffith LS, Clouse RE,Cryer PE. Psychiatric illness in diabetesmellitus. Relationship to symptoms andglucose control. J Nerv Ment Dis 1986;174:736–742
171. Blonde L, Merilainen M, Karwe V,Raskin P, TITRATE Study Group. Pa-tient-directed titration for achieving gly-caemic goals using a once-daily basalinsulin analogue: an assessment of twodifferent fasting plasma glucose targets-the TITRATE study. Diabetes ObesMetab 2009;11:623–631
172. American Diabetes Association: Hyper-glycemic crises in diabetes. DiabetesCare 2004;27 (Suppl. 1):S94–S102
173. Kitabchi AE, Umpierrez GE, Miles JM,Fisher JN. Hyperglycemic crises in adultpatients with diabetes. Diabetes Care2009;32:1335–1343
174. Cryer PE. Hypoglycaemia: the limitingfactor in the glycaemic management ofType I and Type II diabetes. Diabetolo-gia 2002;45:937–948
175. Gannon MC, Nuttall FQ: Protein andDiabetes. In American Diabetes Associa-tion Guide to Medical Nutrition Therapyfor Diabetes. Franz MJ, Bantle JP, Eds.Alexandria, VA, American Diabetes As-sociation, 1999, p. 107–125
176. Cryer PE. Diverse causes of hypoglyce-mia-associated autonomic failure in dia-betes. N Engl J Med 2004;350:2272–2279
177. Cryer PE, Davis SN, Shamoon H. Hypo-glycemia in diabetes. Diabetes Care2003;26:1902–1912
178. Smith SA, Poland GA. Use of influenzaand pneumococcal vaccines in peoplewith diabetes. Diabetes Care 2000;23:95–108
179. Colquhoun AJ, Nicholson KG, Botha JL,Raymond NT. Effectiveness of influenzavaccine in reducing hospital admissionsin people with diabetes. Epidemiol In-fect 1997;119:335–341
180. Bridges CB, Fukuda K, Uyeki TM, CoxNJ, Singleton JA. Prevention and controlof influenza. Recommendations of theAdvisory Committee on ImmunizationPractices (ACIP). MMWR Recomm Rep2002;51:1–31
181. American Diabetes Association: Influ-enza and pneumococcal immunizationin diabetes (Position Statement). Diabe-tes Care 2004;27(Suppl. 1):S111–S113
182. Gaede P, Lund-Andersen H, ParvingHH, Pedersen O. Effect of a multifacto-rial intervention on mortality in type 2diabetes. N Engl J Med 2008;358:580–591
183. Buse JB, Ginsberg HN, Bakris GL, ClarkNG, Costa F, Eckel R, Fonseca V, Ger-stein HC, Grundy S, Nesto RW, PignoneMP, Plutzky J, Porte D, Redberg R, Stit-zel KF, Stone NJ, American Heart Asso-ciation, American Diabetes Association.Primary prevention of cardiovasculardiseases in people with diabetes melli-tus: a scientific statement from theAmerican Heart Association and theAmerican Diabetes Association. Diabe-tes Care 2007;30:162–172
184. Chobanian AV, Bakris GL, Black HR,Cushman WC, Green LA, Izzo JL Jr,Jones DW, Materson BJ, Oparil S,Wright JT Jr, Roccella EJ, NationalHeart, Lung, and Blood Institute JointNational Committee on Prevention, De-tection, Evaluation, and Treatment ofHigh Blood Pressure, National High BloodPressure Education Program Coordinat-ing Committee. The Seventh Report of theJoint National Committee on Prevention,Detection, Evaluation, and Treatment ofHigh Blood Pressure: the JNC 7 report.JAMA 2003;289:2560–2572
185. Bobrie G, Chatellier G, Genes N, ClersonP, Vaur L, Vaisse B, Menard J, MallionJM. Cardiovascular prognosis of“masked hypertension” detected byblood pressure self-measurement in el-derly treated hypertensive patients.JAMA 2004;291:1342–1349
186. Sega R, Facchetti R, Bombelli M, CesanaG, Corrao G, Grassi G, Mancia G. Prog-nostic value of ambulatory and homeblood pressures compared with officeblood pressure in the general popula-tion: follow-up results from the Pres-sioni Arteriose Monitorate e LoroAssociazioni (PAMELA) study. Circula-tion 2005;111:1777–1783
187. UKPDS: Tight blood pressure controland risk of macrovascular and microvas-cular complications in type 2 diabetes:UKPDS 38. UK Prospective DiabetesStudy Group. BMJ 1998;317:703–713
188. Hansson L, Zanchetti A, Carruthers SG,Dahlof B, Elmfeldt D, Julius S, Menard J,Rahn KH, Wedel H, Westerling S. Ef-fects of intensive blood-pressure lower-ing and low-dose aspirin in patientswith hypertension: principal results ofthe Hypertension Optimal Treatment(HOT) randomised trial. HOT StudyGroup. Lancet 1998;351:1755–1762
189. Adler AI, Stratton IM, Neil HA, YudkinJS, Matthews DR, Cull CA, Wright AD,Turner RC, Holman RR. Association ofsystolic blood pressure with macrovas-cular and microvascular complicationsof type 2 diabetes (UKPDS 36): prospec-tive observational study. BMJ 2000;321:412–419
190. Lewington S, Clarke R, Qizilbash N,Peto R, Collins R, Prospective StudiesCollaboration. Age-specific relevance ofusual blood pressure to vascular mortal-
ity: a meta-analysis of individual data forone million adults in 61 prospectivestudies. Lancet 2002;360:1903–1913
191. Stamler J, Vaccaro O, Neaton JD, Went-worth D. Diabetes, other risk factors,and 12-yr cardiovascular mortality formen screened in the Multiple Risk Fac-tor Intervention Trial. Diabetes Care1993;16:434–444
192. Cushman WC, Grimm RH Jr, Cutler JA,Evans GW, Capes S, Corson MA, SadlerLS, Alderman MH, Peterson K, BertoniA, Basile JN, ACCORD Study Group: Ra-tionale and design for the blood pressureintervention of the Action to ControlCardiovascular Risk in Diabetes (AC-CORD) trial. Am J Cardiol 2007;99:44i–55i
193. Sacks FM, Svetkey LP, Vollmer WM, Ap-pel LJ, Bray GA, Harsha D, Obarzanek E,Conlin PR, Miller ER 3rd, Simons-Mor-ton DG, Karanja N, Lin PH, DASH-So-dium Collaborative Research Group.Effects on blood pressure of reduced di-etary sodium and the Dietary Ap-proaches to Stop Hypertension (DASH)diet. DASH-Sodium Collaborative Re-search Group. N Engl J Med 2001;344:3–10
194. Tatti P, Pahor M, Byington RP, Di MauroP, Guarisco R, Strollo G, Strollo F. Out-come results of the Fosinopril VersusAmlodipine Cardiovascular Events Ran-domized Trial (FACET) in patients withhypertension and NIDDM. DiabetesCare 1998;21:597–603
195. Estacio RO, Jeffers BW, Hiatt WR, Big-gerstaff SL, Gifford N, Schrier RW. Theeffect of nisoldipine as compared withenalapril on cardiovascular outcomes inpatients with non-insulin-dependent di-abetes and hypertension. N Engl J Med1998;338:645–652
196. Schrier RW, Estacio RO, Mehler PS, Hi-att WR. Appropriate blood pressurecontrol in hypertensive and normoten-sive type 2 diabetes mellitus: a summaryof the ABCD trial. Nat Clin Pract Neph-rol 2007;3:428–438
197. ALLHAT Officers and Coordinators forthe ALLHAT Collaborative ResearchGroup. The Antihypertensive and Lipid-Lowering Treatment to Prevent HeartAttack Trial: the Antihypertensive andLipid-Lowering Treatment to PreventHeart Attack Trial (ALLHAT). JAMA2002;288:2981–2997
198. Psaty BM, Lumley T, Furberg CD, Schel-lenbaum G, Pahor M, Alderman MH,Weiss NS. Health outcomes associatedwith various antihypertensive therapiesused as first-line agents: a network meta-analysis. JAMA 2003;289:2534–2544
199. Effects of ramipril on cardiovascular andmicrovascular outcomes in people withdiabetes mellitus: results of the HOPEstudy and MICRO-HOPE substudy:Heart Outcomes Prevention Evaluation
Standards of Medical Care
S54 DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 care.diabetesjournals.org

Study Investigators. Lancet 2000;355:253–259
200. Pfeffer MA, Swedberg K, Granger CB,Held P, McMurray JJ, Michelson EL,Olofsson B, Ostergren J, Yusuf S, PocockS, CHARM Investigators and Commit-tees. Effects of candesartan on mortalityand morbidity in patients with chronicheart failure: the CHARM-Overall pro-gramme. Lancet 2003;362:759–766
201. Granger CB, McMurray JJ, Yusuf S, HeldP, Michelson EL, Olofsson B, OstergrenJ, Pfeffer MA, Swedberg K, CHARM In-vestigators and Committees. Effects ofcandesartan in patients with chronicheart failure and reduced left-ventricularsystolic function intolerant to angioten-sin-converting-enzyme inhibitors: theCHARM-Alternative trial. Lancet 2003;362:772–776
202. McMurray JJ, Ostergren J, Swedberg K,Granger CB, Held P, Michelson EL,Olofsson B, Yusuf S, Pfeffer MA,CHARM Investigators and Committees.Effects of candesartan in patients withchronic heart failure and reduced left-ventricular systolic function taking an-giotensin-converting-enzymeinhibitors: the CHARM-Added trial.Lancet 2003;362:767–771
203. Lindholm LH, Ibsen H, Dahlof B, De-vereux RB, Beevers G, de Faire U, Fyhr-quist F, Julius S, Kjeldsen SE,Kristiansson K, Lederballe-Pedersen O,Nieminen MS, Omvik P, Oparil S,Wedel H, Aurup P, Edelman J, SnapinnS, LIFE Study Group. Cardiovascularmorbidity and mortality in patients withdiabetes in the Losartan Intervention ForEndpoint reduction in hypertensionstudy (LIFE): a randomised trial againstatenolol. Lancet 2002;359:1004–1010
204. Berl T, Hunsicker LG, Lewis JB, PfefferMA, Porush JG, Rouleau JL, Drury PL,Esmatjes E, Hricik D, Parikh CR, Raz I,Vanhille P, Wiegmann TB, Wolfe BM,Locatelli F, Goldhaber SZ, Lewis EJ,Irbesartan Diabetic Nephropathy Trial.Collaborative Study Group. Collabora-tive Study Group. Cardiovascular out-comes in the Irbesartan DiabeticNephropathy Trial of patients with type2 diabetes and overt nephropathy. AnnIntern Med 2003;138:542–549
205. Laffel LM, McGill JB, Gans DJ. The ben-eficial effect of angiotensin-convertingenzyme inhibition with captopril on di-abetic nephropathy in normotensiveIDDM patients with microalbuminuria.North American MicroalbuminuriaStudy Group. Am J Med 1995;99:497–504
206. Bakris GL, Williams M, Dworkin L, El-liott WJ, Epstein M, Toto R, Tuttle K,Douglas J, Hsueh W, Sowers J. Preserv-ing renal function in adults with hyper-tension and diabetes: a consensusapproach: National Kidney Foundation
Hypertension and Diabetes ExecutiveCommittees Working Group. Am J Kid-ney Dis 2000;36:646–661
207. Psaty BM, Smith NL, Siscovick DS, Ko-epsell TD, Weiss NS, Heckbert SR, Le-maitre RN, Wagner EH, Furberg CD.Health outcomes associated with antihy-pertensive therapies used as first-lineagents: a systematic review and meta-analysis. JAMA 1997;277:739–745
208. Patel A, ADVANCE CollaborativeGroup, MacMahon S, Chalmers J, NealB, Woodward M, Billot L, Harrap S,Poulter N, Marre M, Cooper M, GlasziouP, Grobbee DE, Hamet P, Heller S, LiuLS, Mancia G, Mogensen CE, Pan CY,Rodgers A, Williams B. Effects of a fixedcombination of perindopril and indap-amide on macrovascular and microvas-cular outcomes in patients with type 2diabetes mellitus (the ADVANCE trial):a randomised controlled trial. Lancet2007;370:829–840
209. Sibai BM. Treatment of hypertension inpregnant women. N Engl J Med 1996;335:257–265
210. Baigent C, Keech A, Kearney PM, Black-well L, Buck G, Pollicino C, Kirby A,Sourjina T, Peto R, Collins R, Simes R,Cholesterol Treatment Trialists’ (CTT)Collaborators. Efficacy and safety ofcholesterol-lowering treatment: pro-spective meta-analysis of data from90,056 participants in 14 randomisedtrials of statins. Lancet 2005;366:1267–1278
211. Pyorala K, Pedersen TR, Kjekshus J,Faergeman O, Olsson AG, ThorgeirssonG. Cholesterol lowering with simvasta-tin improves prognosis of diabetic pa-tients with coronary heart disease: asubgroup analysis of the ScandinavianSimvastatin Survival Study (4S). Diabe-tes Care 1997;20:614–620
212. Collins R, Armitage J, Parish S, Sleigh P,Peto R, Heart Protection Study Collabo-rative Group: MRC/BHF Heart Protec-tion Study of cholesterol-lowering withsimvastatin in 5963 people with diabe-tes: a randomised placebo-controlledtrial. Lancet 2003;361:2005–2016
213. Goldberg RB, Mellies MJ, Sacks FM,Moye LA, Howard BV, Howard WJ,Davis BR, Cole TG, Pfeffer MA, Braun-wald E. Cardiovascular events and theirreduction with pravastatin in diabeticand glucose-intolerant myocardial in-farction survivors with average choles-terol levels: subgroup analyses in thecholesterol and recurrent events (CARE)trial. The Care Investigators. Circulation1998;98:2513–2519
214. Shepherd J, Barter P, Carmena R, Deed-wania P, Fruchart JC, Haffner S, Hsia J,Breazna A, LaRosa J, Grundy S, WatersD. Effect of lowering LDL cholesterolsubstantially below currently recom-mended levels in patients with coronary
heart disease and diabetes: the Treatingto New Targets (TNT) study. DiabetesCare 2006;29:1220–1226
215. Sever PS, Poulter NR, Dahlof B, WedelH, Collins R, Beevers G, Caulfield M,Kjeldsen SE, Kristinsson A, McInnes GT,Mehlsen J, Nieminen M, O’Brien E, Os-tergren J. Reduction in cardiovascularevents with atorvastatin in 2,532 pa-tients with type 2 diabetes: Anglo-Scan-dinavian Cardiac Outcomes Trial–lipid-lowering arm (ASCOT-LLA). DiabetesCare 2005;28:1151–1157
216. Knopp RH, d’Emden M, Smilde JG, Po-cock SJ. Efficacy and safety of atorvasta-tin in the prevention of cardiovascularend points in subjects with type 2 di-abetes: the Atorvastatin Study for Pre-vention of Coronary Heart DiseaseEndpoints in non-insulin-dependent di-abetes mellitus (ASPEN). Diabetes Care2006;29:1478–1485
217. Singh IM, Shishehbor MH, Ansell BJ.High-density lipoprotein as a therapeu-tic target: a systematic review. JAMA2007;298:786–798
218. Canner PL, Berge KG, Wenger NK,Stamler J, Friedman L, Prineas RJ,Friedewald W. Fifteen year mortality inCoronary Drug Project patients: long-term benefit with niacin. J Am Coll Car-diol 1986;8:1245–1255
219. Rubins HB, Robins SJ, Collins D, Fye CL,Anderson JW, Elam MB, Faas FH, Lin-ares E, Schaefer EJ, Schectman G, WiltTJ, Wittes J. Gemfibrozil for the second-ary prevention of coronary heart diseasein men with low levels of high-densitylipoprotein cholesterol. Veterans AffairsHigh-Density Lipoprotein CholesterolIntervention Trial Study Group. N EnglJ Med 1999;341:410–418
220. Frick MH, Elo O, Haapa K, HeinonenOP, Heinsalmi P, Helo P, Huttunen JK,Kaitaniemi P, Koskinen P, Manninen V:Helsinki Heart Study: primary-preven-tion trial with gemfibrozil in middle-aged men with dyslipidemia: safety oftreatment, changes in risk factors, andincidence of coronary heart disease.N Engl J Med 1987;317:1237–1245
221. Keech A, Simes RJ, Barter P, Best J, ScottR, Taskinen MR, Forder P, Pillai A, DavisT, Glasziou P, Drury P, Kesaniemi YA,Sullivan D, Hunt D, Colman P, d’EmdenM, Whiting M, Ehnholm C, Laakso M,FIELD study investigators. Effects oflong-term fenofibrate therapy on cardio-vascular events in 9795 people with type2 diabetes mellitus (the FIELD study):randomised controlled trial. Lancet2005;366:1849–1861
222. Expert Panel on Detection, Evaluation,and Treatment of High Blood Choles-terol in Adults: Executive Summary ofThe Third Report of The National Cho-lesterol Education Program (NCEP) Ex-pert Panel on Detection, Evaluation,
Position Statement
care.diabetesjournals.org DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 S55

And Treatment of High Blood Choles-terol In Adults (Adult Treatment PanelIII). JAMA 2001;285:2486–2497
223. Hayward RA, Hofer TP, Vijan S. Nar-rative review: lack of evidence for rec-ommended low-density lipoproteintreatment targets: a solvable problem.Ann Intern Med 2006;145:520–530
224. Cannon CP, Braunwald E, McCabe CH,Rader DJ, Rouleau JL, Belder R, Joyal SV,Hill KA, Pfeffer MA, Skene AM, Prava-statin or Atorvastatin Evaluation andInfection Therapy-Thrombolysis inMyocardial Infarction 22 Investigators.Intensive versus moderate lipid loweringwith statins after acute coronary syn-dromes. N Engl J Med 2004;350:1495–1504
225. de Lemos JA, Blazing MA, Wiviott SD,Lewis EF, Fox KA, White HD, RouleauJL, Pedersen TR, Gardner LH, Mukher-jee R, Ramsey KE, Palmisano J, Bilhei-mer DW, Pfeffer MA, Califf RM,Braunwald E, A to Z Investigators. Earlyintensive vs a delayed conservative sim-vastatin strategy in patients with acutecoronary syndromes: phase Z of the A toZ trial. JAMA 2004;292:1307–1316
226. Nissen SE, Tuzcu EM, Schoenhagen P,Brown BG, Ganz P, Vogel RA, Crowe T,Howard G, Cooper CJ, Brodie B, GrinesCL, DeMaria AN, REVERSAL Investiga-tors. Effect of intensive compared withmoderate lipid-lowering therapy on pro-gression of coronary atherosclerosis: arandomized controlled trial. JAMA2004;291:1071–1080
227. Grundy SM, Cleeman JI, Merz CN,Brewer HB Jr, Clark LT, HunninghakeDB, Pasternak RC, Smith SC Jr, Stone NJ,National Heart, Lung, and Blood Institute,American College of Cardiology Founda-tion, American Heart Association. Impli-cations of recent clinical trials for theNational Cholesterol Education ProgramAdult Treatment Panel III guidelines. Cir-culation 2004;110:227–239
228. Chasman DI, Posada D, SubrahmanyanL, Cook NR, Stanton VP, Jr, Ridker PM.Pharmacogenetic study of statin therapyand cholesterol reduction. JAMA 2004;291:2821–2827
229. Baigent C, Keech A, Kearney PM, Black-well L, Buck G, Pollicino C, Kirby A,Sourjina T, Peto R, Collins R, Simes R,Cholesterol Treatment Trialists’ (CTT)Collaborators. Efficacy and safety ofcholesterol-lowering treatment: pro-spective meta-analysis of data from90,056 participants in 14 randomisedtrials of statins. Lancet 2005;366:1267–1278
230. Elam MB, Hunninghake DB, Davis KB,Garg R, Johnson C, Egan D, Kostis JB,Sheps DS, Brinton EA. Effect of niacin onlipid and lipoprotein levels and glycemiccontrol in patients with diabetes and pe-ripheral arterial disease: the ADMIT
study: A randomized trial. Arterial Dis-ease Multiple Intervention Trial. JAMA2000;284:1263–1270
231. Grundy SM, Vega GL, McGovern ME,Tulloch BR, Kendall DM, Fitz-Patrick D,Ganda OP, Rosenson RS, Buse JB, Rob-ertson DD, Sheehan JP, Diabetes Multi-center Research Group. Efficacy, safety,and tolerability of once-daily niacin forthe treatment of dyslipidemia associatedwith type 2 diabetes: results of the as-sessment of diabetes control and evalu-ation of the efficacy of niaspan trial. ArchIntern Med 2002;162:1568–1576
232. Jones PH, Davidson MH. Reporting rateof rhabdomyolysis with fenofibrate statin versus gemfibrozil any statin.Am J Cardiol 2005;95:120–122
233. Brunzell JD, Davidson M, Furberg CD,Goldberg RB, Howard BV, Stein JH, Wit-ztum JL, American Diabetes Association,American College of Cardiology Foun-dation. Lipoprotein management inpatients with cardiometabolic risk: con-sensus statement from the American Di-abetes Association and the AmericanCollege of Cardiology Foundation. Dia-betes Care 2008;31:811–822
234. Colhoun HM, Betteridge DJ, DurringtonPN, Hitman GA, Neil HA, Livingstone SJ,Thomason MJ, Mackness MI, Charlton-Menys V, Fuller JH, CARDS investigators.Primary prevention of cardiovascular dis-ease with atorvastatin in type 2 diabetes inthe Collaborative Atorvastatin DiabetesStudy (CARDS): multicentre randomisedplacebo-controlled trial. Lancet 2004;364:685–696
235. Buse JB, Ginsberg HN, Bakris GL, ClarkNG, Costa F, Eckel R, Fonseca V, Ger-stein HC, Grundy S, Nesto RW, PignoneMP, Plutzky J, Porte D, Redberg R, Stit-zel KF, Stone NJ, American Heart Asso-ciation, American Diabetes Association.Primary prevention of cardiovasculardiseases in people with diabetes melli-tus: a scientific statement from theAmerican Heart Association and theAmerican Diabetes Association. Diabe-tes Care 2007;30:162–172
236. Antithrombotic Trialists’ (ATT) Collab-oration, Baigent C, Blackwell L, CollinsR, Emberson J, Godwin J, Peto R, BuringJ, Hennekens C, Kearney P, Meade T,Patrono C, Roncaglioni MC, ZanchettiA. Aspirin in the primary and secondaryprevention of vascular disease: collabo-rative meta-analysis of individual partic-ipant data from randomised trials.Lancet 2009;373:1849–1860
237. Wolff T, Miller T, Ko S. Aspirin for theprimary prevention of cardiovascularevents: an update of the evidence for theU.S. Preventive Services Task Force.Ann Intern Med 2009;150:405–410
238. US Preventive Services Task Force: As-pirin for the prevention of cardiovascu-lar disease: U.S. Preventive Services Task
Force recommendation statement. AnnIntern Med 2009;150:396–404
239. Ogawa H, Nakayama M, Morimoto T,Uemura S, Kanauchi M, Doi N, Jinnou-chi H, Sugiyama S, Saito Y, Japanese Pri-mary Prevention of Atherosclerosis WithAspirin for Diabetes (JPAD) Trial Inves-tigators. Low-dose aspirin for primaryprevention of atherosclerotic events inpatients with type 2 diabetes: a random-ized controlled trial. JAMA 2008;300:2134–2141
240. Belch J, MacCuish A, Campbell I, CobbeS, Taylor R, Prescott R, Lee R, Bancroft J,MacEwan S, Shepherd J, Macfarlane P,Morris A, Jung R, Kelly C, Connacher A,Peden N, Jamieson A, Matthews D, LeeseG, McKnight J, O’Brien I, Semple C, Pet-rie J, Gordon D, Pringle S, MacWalter R.The prevention of progression of arterialdisease and diabetes (POPADAD) trial:factorial randomised placebo controlledtrial of aspirin and antioxidants in pa-tients with diabetes and asymptomaticperipheral arterial disease. BMJ 2008;337:a1840
241. Pignone M, Earnshaw S, Tice JA,Pletcher MJ. Aspirin, statins, or bothdrugs for the primary prevention of cor-onary heart disease events in men: acost-utility analysis. Ann Intern Med2006;144:326–336
242. Campbell CL, Smyth S, Montalescot G,Steinhubl SR. Aspirin dose for the pre-vention of cardiovascular disease: a sys-tematic review. JAMA 2007;297:2018–2024
243. Davì G, Patrono C. Platelet activationand atherothrombosis. N Engl J Med2007;357:2482–2494
244. Watala C, Golanski J, Pluta J, Boncler M,Rozalski M, Luzak B, Kropiwnicka A,Drzewoski J. Reduced sensitivity ofplatelets from type 2 diabetic patients toacetylsalicylic acid (aspirin)-its relationto metabolic control. Thromb Res 2004;113:101–113
245. Lev EI. Aspirin resistance transient lab-oratory finding or important clinical en-tity? J Am Coll Cardiol 2009;53:678–680
246. Santilli F, Rocca B, De Cristofaro R, Lat-tanzio S, Pietrangelo L, Habib A, Petti-nella C, Recchiuti A, Ferrante E,Ciabattoni G, Davì G, Patrono C. Plateletcyclooxygenase inhibition by low-doseaspirin is not reflected consistently byplatelet function assays: implications foraspirin “resistance”. J Am Coll Cardiol2009;53:667–677
247. Bhatt DL, Marso SP, Hirsch AT, RinglebPA, Hacke W, Topol EJ. Amplified ben-efit of clopidogrel versus aspirin in pa-tients with diabetes mellitus. Am JCardiol 2002;90:625–628
248. Haire-Joshu D, Glasgow RE, Tibbs TL.Smoking and diabetes. Diabetes Care1999;22:1887–1898
Standards of Medical Care
S56 DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 care.diabetesjournals.org

249. American Diabetes Asociation: Smokingand diabetes (Position Statement). Dia-betes Care 2004;27(Suppl. 1):S74–S75
250. US Preventive Services Task Force.Counseling to Prevent Tobacco Use and To-bacco-Related Diseases: RecommendationStatement. Rockville, MD, Agency forHealthcare Research and Quality, 2003
251. Ranney L, Melvin C, Lux L, McClain E,Lohr KN. Systematic review: smokingcessation intervention strategies foradults and adults in special populations.Ann Intern Med 2006;145:845–856
252. Scognamiglio R, Negut C, Ramondo A,Tiengo A, Avogaro A. Detection of coro-nary artery disease in asymptomatic pa-tients with type 2 diabetes mellitus. J AmColl Cardiol 2006;47:65–71
253. Boden WE, O’Rourke RA, Teo KK, Har-tigan PM, Maron DJ, Kostuk WJ, Knudt-son M, Dada M, Casperson P, Harris CL,Chaitman BR, Shaw L, Gosselin G,Nawaz S, Title LM, Gau G, Blaustein AS,Booth DC, Bates ER, Spertus JA, BermanDS, Mancini GB, Weintraub WS,COURAGE Trial Research Group. Opti-mal medical therapy with or without PCIfor stable coronary disease. N Engl J Med2007;356:1503–1516
254. BARI 2D Study Group, Frye RL, AugustP, Brooks MM, Hardison RM, Kelsey SF,MacGregor JM, Orchard TJ, ChaitmanBR, Genuth SM, Goldberg SH, HlatkyMA, Jones TL, Molitch ME, Nesto RW,Sako EY, Sobel BE. A randomized trial oftherapies for type 2 diabetes and coro-nary artery disease. N Engl J Med 2009;360:2503–2515
255. Wackers FJ, Chyun DA, Young LH,Heller GV, Iskandrian AE, Davey JA,Barrett EJ, Taillefer R, Wittlin SD, Filip-chuk N, Ratner RE, Inzucchi SE: Reso-lution of asymptomatic myocardialischemia in patients with type 2 diabetesmellitus in the DIAD Study. DiabetesCare 2007;30:2892–2898
256. Young LH, Wackers FJ, Chyun DA,Davey JA, Barrett EJ, Taillefer R, HellerGV, Iskandrian AE, Wittlin SD, Filip-chuk N, Ratner RE, Inzucchi SE, DIADInvestigators. Cardiac outcomes afterscreening for asymptomatic coronary ar-tery disease in patients with type 2 dia-betes: the DIAD study: a randomizedcontrolled trial. JAMA 2009;301:1547–1555
257. Braunwald E, Domanski MJ, Fowler SE,Geller NL, Gersh BJ, Hsia J, Pfeffer MA,Rice MM, Rosenberg YD, Rouleau JL,PEACE Trial Investigators. Angiotensin-converting-enzyme inhibition in stablecoronary artery disease. N Engl J Med2004;351:2058–2068
258. Effects of the angiotensin-receptorblocker telmisartan on cardiovascularevents in high-risk patients intolerant toangiotensin-converting enzyme inhibi-tors: a randomised controlled trial. Lan-
cet 2008;372:1174–1183259. Garg JP, Bakris GL. Microalbuminuria:
marker of vascular dysfunction, risk fac-tor for cardiovascular disease. Vasc Med2002;7:35–43
260. Klausen K, Borch-Johnsen K, Feldt-Ras-mussen B, Jensen G, Clausen P,Scharling H, Appleyard M, Jensen JS.Very low levels of microalbuminuria areassociated with increased risk of coro-nary heart disease and death indepen-dently of renal function, hypertension,and diabetes. Circulation 2004;110:32–35
261. Gall MA, Hougaard P, Borch-Johnsen K,Parving HH. Risk factors for develop-ment of incipient and overt diabetic ne-phropathy in patients with non-insulindependent diabetes mellitus: prospec-tive, observational study. BMJ 1997;314:783–788
262. Ravid M, Lang R, Rachmani R, LishnerM. Long-term renoprotective effect ofangiotensin-converting enzyme inhibi-tion in non-insulin-dependent diabetesmellitus. A 7-year follow-up study. ArchIntern Med 1996;156:286–289
263. Reichard P, Nilsson BY, Rosenqvist U. Theeffect of long-term intensified insulintreatment on the development of micro-vascular complications of diabetes melli-tus. N Engl J Med 1993;329:304–309
264. Effect of intensive therapy on the devel-opment and progression of diabetic ne-phropathy in the Diabetes Control andComplications Trial. The Diabetes Con-trol and Complications (DCCT) Re-search Group. Kidney Int 1995;47:1703–1720
265. Lewis EJ, Hunsicker LG, Bain RP, RohdeRD. The effect of angiotensin-convert-ing-enzyme inhibition on diabetic ne-phropathy. The Collaborative StudyGroup. N Engl J Med 1993;329:1456–1462
266. Remuzzi G, Macia M, Ruggenenti P. Pre-vention and treatment of diabetic renaldisease in type 2 diabetes: the BENE-DICT study. JAmSocNephrol 2006;17:S90–S97
267. Bilous R, Chaturvedi N, Sjølie AK, FullerJ, Klein R, Orchard T, Porta M, ParvingHH. Effect of candesartan on microalbu-minuria and albumin excretion rate indiabetes: three randomized trials. AnnIntern Med 2009;151:11–14
268. Mauer M, Zinman B, Gardiner R, SuissaS, Sinaiko A, Strand T, Drummond K,Donnelly S, Goodyer P, Gubler MC,Klein R. Renal and retinal effects of ena-lapril and losartan in type 1 diabetes.N Engl J Med 2009;361:40–51
269. Lewis EJ, Hunsicker LG, Clarke WR,Berl T, Pohl MA, Lewis JB, Ritz E, AtkinsRC, Rohde R, Raz I, Collaborative StudyGroup. Renoprotective effect of the an-giotensin-receptor antagonist irbesartanin patients with nephropathy due to type
2 diabetes. N Engl J Med 2001;345:851–860
270. Brenner BM, Cooper ME, de Zeeuw D,Keane WF, Mitch WE, Parving HH, Re-muzzi G, Snapinn SM, Zhang Z, Shahin-far S, RENAAL Study Investigators.Effects of losartan on renal and cardio-vascular outcomes in patients with type2 diabetes and nephropathy. N EnglJ Med 2001;345:861–869
271. Parving HH, Lehnert H, Brochner-Mortensen J, Gomis R, Andersen S,Arner P, Irbesartan in Patients with Type2 Diabetes and Microalbuminuria StudyGroup. The effect of irbesartan on thedevelopment of diabetic nephropathy inpatients with type 2 diabetes. N EnglJ Med 2001;345:870–878
272. Pepine CJ, Handberg EM, Cooper-De-Hoff RM, Marks RG, Kowey P, MesserliFH, Mancia G, Cangiano JL, Garcia-Bar-reto D, Keltai M, Erdine S, Bristol HA,Kolb HR, Bakris GL, Cohen JD, ParmleyWW, INVEST Investigators. A calciumantagonist vs a non-calcium antagonisthypertension treatment strategy for pa-tients with coronary artery disease: theInternational Verapamil-Trandolaprilstudy (INVEST): a randomized con-trolled trial. JAMA 2003;290:2805–2816
273. Bakris GL, Siomos M, Richardson D,Janssen I, Bolton WK, Hebert L, AgarwalR, Catanzaro D. ACE inhibition or an-giotensin receptor blockade: impact onpotassium in renal failure. VAL-K StudyGroup. Kidney Int 2000;58:2084–2092
274. Mogensen CE, Neldam S, Tikkanen I,Oren S, Viskoper R, Watts RW, CooperME. Randomised controlled trial of dualblockade of renin-angiotensin system inpatients with hypertension, microalbu-minuria, and non-insulin dependent di-abetes: the candesartan and lisinoprilmicroalbuminuria (CALM) study. BMJ2000;321:1440–1444
275. Schjoedt KJ, Jacobsen P, Rossing K,Boomsma F, Parving HH. Dual blockadeof the renin-angiotensin-aldosteronesystem in diabetic nephropathy: the roleof aldosterone. Horm Metab Res 2005;37(Suppl. 1):4–8
276. Schjoedt KJ, Rossing K, Juhl TR,Boomsma F, Rossing P, Tarnow L, Parv-ing HH. Beneficial impact of spironolac-tone in diabetic nephropathy. KidneyInt 2005;68:2829–2836
277. Parving HH, Persson F, Lewis JB, LewisEJ, Hollenberg NK, AVOID Study Inves-tigators. Aliskiren combined with losar-tan in type 2 diabetes and nephropathy.N Engl J Med 2008;358:2433–2446
278. Pijls LT, de Vries H, Donker AJ, van EijkJT. The effect of protein restriction onalbuminuria in patients with type 2 dia-betes mellitus: a randomized trial.Nephrol Dial Transplant 1999;14:1445–1453
Position Statement
care.diabetesjournals.org DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 S57

279. Pedrini MT, Levey AS, Lau J, ChalmersTC, Wang PH. The effect of dietary pro-tein restriction on the progression of di-abetic and nondiabetic renal diseases: ameta-analysis. Ann Intern Med 1996;124:627–632
280. Hansen HP, Tauber-Lassen E, JensenBR, Parving HH. Effect of dietary proteinrestriction on prognosis in patients withdiabetic nephropathy. Kidney Int 2002;62:220–228
281. Kasiske BL, Lakatua JD, Ma JZ, Louis TA.A meta-analysis of the effects of dietaryprotein restriction on the rate of declinein renal function. Am J Kidney Dis 1998;31:954–961
282. Eknoyan G, Hostetter T, Bakris GL, He-bert L, Levey AS, Parving HH, SteffesMW, Toto R. Proteinuria and othermarkers of chronic kidney disease: a po-sition statement of the national kidneyfoundation (NKF) and the national insti-tute of diabetes and digestive and kidneydiseases (NIDDK). Am J Kidney Dis2003;42:617–622
283. Levey AS, Coresh J, Balk E, Kausz AT,Levin A, Steffes MW, Hogg RJ, PerroneRD, Lau J, Eknoyan G, National KidneyFoundation. National Kidney Founda-tion practice guidelines for chronic kid-ney disease: evaluation, classification,and stratification. Ann Intern Med 2003;139:137–147
284. Kramer H, Molitch ME. Screening forkidney disease in adults with diabetes.Diabetes Care 2005;28:1813–1816
285. Kramer HJ, Nguyen QD, Curhan G, HsuCY. Renal insufficiency in the absence ofalbuminuria and retinopathy amongadults with type 2 diabetes mellitus.JAMA 2003;289:3273–3277
286. Tsalamandris C, Allen TJ, Gilbert RE,Sinha A, Panagiotopoulos S, Cooper ME,Jerums G. Progressive decline in renalfunction in diabetic patients with andwithout albuminuria. Diabetes 1994;43:649–655
287. Levey AS, Bosch JP, Lewis JB, Greene T,Rogers N, Roth D. A more accuratemethod to estimate glomerular filtrationrate from serum creatinine: a new pre-diction equation. Modification of Diet inRenal Disease Study Group. Ann InternMed 1999;130:461–470
288. Rigalleau V, Lasseur C, Perlemoine C,Barthe N, Raffaitin C, Liu C, ChauveauP, Baillet-Blanco L, Beauvieux MC,Combe C, Gin H. Estimation of glomer-ular filtration rate in diabetic subjects:Cockcroft formula or modification ofDiet in Renal Disease study equation?Diabetes Care 2005;28:838–843
289. Levinsky NG. Specialist evaluation inchronic kidney disease: too little, toolate. Ann Intern Med 2002;137:542–543
290. American Diabetes Association: Ne-phropathy in diabetes (Position State-
ment). Diabetes Care 2004;27(Suppl.1):S79–S83
291. Klein R. Hyperglycemia and microvas-cular and macrovascular disease in dia-betes. Diabetes Care 1995;18:258–268
292. Estacio RO, McFarling E, Biggerstaff S,Jeffers BW, Johnson D, Schrier RW.Overt albuminuria predicts diabetic ret-inopathy in Hispanics with NIDDM.Am J Kidney Dis 1998;31:947–953
293. Leske MC, Wu SY, Hennis A, Hyman L,Nemesure B, Yang L, Schachat AP, Bar-bados Eye Study Group. Hyperglycemia,blood pressure, and the 9-year incidenceof diabetic retinopathy: the BarbadosEye Studies. Ophthalmology 2005;112:799–805
294. Fong DS, Aiello LP, Ferris FL 3rd, KleinR. Diabetic retinopathy. Diabetes Care2004;27:2540–2553
295. Diabetes Control and ComplicationsTrial Research Group: Effect of preg-nancy on microvascular complicationsin the diabetes control and complica-tions trial. The Diabetes Control andComplications Trial Research Group.Diabetes Care 2000;23:1084–1091
296. The Diabetic Retinopathy Study (DRS)Research Group. Preliminary report onthe effects of photocoagulation therapy:DRS Report #1. Am J Ophthalmol 1976;81:383–396.
297. Photocoagulation for diabetic macularedema. Early Treatment Diabetic Reti-nopathy Study report number 1. EarlyTreatment Diabetic Retinopathy Studyresearch group. Arch Ophthalmol 1985;103:1796–1806
298. Klein R, Klein BE, Moss SE, Davis MD,DeMets DL. The Wisconsin epidemiologicstudy of diabetic retinopathy. II. Preva-lence and risk of diabetic retinopathywhen age at diagnosis is less than 30 years.Arch Ophthalmol 1984;102:520–526
299. Harris MI, Klein R, Welborn TA,Knuiman MW. Onset of NIDDM occursat least 4–7 yr before clinical diagnosis.Diabetes Care 1992;15:815–819
300. Vijan S, Hofer TP, Hayward RA. Cost-utility analysis of screening intervals fordiabetic retinopathy in patients withtype 2 diabetes mellitus. JAMA 2000;283:889–896
301. Klein R. Screening interval for retinopa-thy in type 2 diabetes. Lancet 2003;361:190–191
302. Younis N, Broadbent DM, Vora JP, Har-ding SP, Liverpool Diabetic Eye Study.Incidence of sight-threatening retinopa-thy in patients with type 2 diabetes in theLiverpool Diabetic Eye Study: a cohortstudy. Lancet 2003;361:195–200
303. Ahmed J, Ward TP, Bursell SE, AielloLM, Cavallerano JD, Vigersky RA. Thesensitivity and specificity of nonmydri-atic digital stereoscopic retinal imagingin detecting diabetic retinopathy. Diabe-tes Care 2006;29:2205–2209
304. American Diabetes Association: Reti-nopathy in diabetes. Diabetes Care2004;27 Suppl. 1:S84–S87
305. Ciulla TA, Amador AG, Zinman B. Dia-betic retinopathy and diabetic macularedema: pathophysiology, screening, andnovel therapies. Diabetes Care 2003;26:2653–2664
306. Boulton AJ, Vinik AI, Arezzo JC, Bril V,Feldman EL, Freeman R, Malik RA, Ma-ser RE, Sosenko JM, Ziegler D, AmericanDiabetes Association. Diabetic neuropa-thies: a statement by the American Dia-betes Association. Diabetes Care 2005;28:956–962
307. Vinik AI, Maser RE, Mitchell BD, Free-man R. Diabetic autonomic neuropathy.Diabetes Care 2003;26:1553–1579
308. Boulton AJ, Armstrong DG, Albert SF,Frykberg RG, Hellman R, Kirkman MS,Lavery LA, Lemaster JW, Mills JL Sr,Mueller MJ, Sheehan P, Wukich DK,American Diabetes Association, Ameri-can Association of Clinical Endocrinolo-gists. Comprehensive foot examinationand risk assessment: a report of the taskforce of the foot care interest group ofthe American Diabetes Association, withendorsement by the American Associa-tion of Clinical Endocrinologists. Diabe-tes Care 2008;31:1679–1685
309. American Diabetes Association: Periph-eral arterial disease in people with dia-betes (Consensus Statement). DiabetesCare 2003;26:3333–3341
310. American Diabetes Association: Consen-sus Development Conference on Dia-betic Foot Wound Care, 7–8 April1999, Boston, Massachusetts. DiabetesCare 1999;22:1354–1360
311. Silverstein J, Klingensmith G, CopelandKC, Plotnick L, Kaufman F, Laffel L,Deeb LC, Grey M, Anderson BJ, Hol-zmeister LA, and Clark NG Care of chil-dren and adolescents with type 1diabetes mellitus: A statement of theAmerican Diabetes Association. Diabe-tes Care 2005; 28:186–212.
312. Northam EA, Anderson PJ, Werther GA,Warne GL, Adler RG, Andrewes D. Neu-ropsychological complications of IDDMin children 2 years after disease onset.Diabetes Care 1998;21:379–384
313. Rovet J, Alvarez M. Attentional function-ing in children and adolescents withIDDM. Diabetes Care 1997;20:803–810
314. Bjørgaas M, Gimse R, Vik T, Sand T.Cognitive function in type 1 diabeticchildren with and without episodes ofsevere hypoglycaemia. Acta Paediatr1997;86:148–153
315. Doyle EA, Weinzimer SA, Steffen AT,Ahern JA, Vincent M, Tamborlane WV.A randomized, prospective trial compar-ing the efficacy of continuous subcuta-neous insulin infusion with multipledaily injections using insulin glargine.Diabetes Care 2004;27:1554–1558
Standards of Medical Care
S58 DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 care.diabetesjournals.org
316. Nimri R, Weintrob N, Benzaquen H,Ofan R, Fayman G, Phillip M. Insulinpump therapy in youth with type 1 dia-betes: a retrospective paired study. Pedi-atrics 2006;117:2126–2131
317. Krantz JS, Mack WJ, Hodis HN, Liu CR,Liu CH, Kaufman FR. Early onset of sub-clinical atherosclerosis in young personswith type 1 diabetes. J Pediatr 2004;145:452–457
318. Jarvisalo MJ, Putto-Laurila A, Jartti L,Lehtimaki T, Solakivi T, Ronnemaa T,Raitakari OT. Carotid artery intima-me-dia thickness in children with type 1 di-abetes. Diabetes 2002;51:493–498
319. Haller MJ, Samyn M, Nichols WW,Brusko T, Wasserfall C, Schwartz RF, At-kinson M, Shuster JJ, Pierce GL, Silver-stein JH. Radial artery tonometrydemonstrates arterial stiffness in chil-dren with type 1 diabetes. Diabetes Care2004;27:2911–2917
320. Orchard TJ, Forrest KY, Kuller LH,Becker DJ, Pittsburgh Epidemiology ofDiabetes Complications Study. Lipidand blood pressure treatment goals fortype 1 diabetes: 10-year incidence datafrom the Pittsburgh Epidemiology of Di-abetes Complications Study. DiabetesCare 2001;24:1053–1059
321. Kavey RE, Allada V, Daniels SR, HaymanLL, McCrindle BW, Newburger JW,Parekh RS, Steinberger J, AmericanHeart Association Expert Panel on Pop-ulation and Prevention Science, Ameri-can Heart Association Council onCardiovascular Disease in the Young,American Heart Association Council onEpidemiology and Prevention, Ameri-can Heart Association Council on Nutri-tion, Physical Activity and Metabolism,American Heart Association Council onHigh Blood Pressure Research, Ameri-can Heart Association Council on Car-diovascular Nursing, American HeartAssociation Council on the Kidney inHeart Disease, Interdisciplinary Work-ing Group on Quality of Care and Out-comes Research. Cardiovascular riskreduction in high-risk pediatric patients:a scientific statement from the AmericanHeart Association Expert Panel on Pop-ulation and Prevention Science; theCouncils on Cardiovascular Disease inthe Young, Epidemiology and Preven-tion, Nutrition, Physical Activity andMetabolism, High Blood Pressure Re-search, Cardiovascular Nursing, and theKidney in Heart Disease; and the Inter-disciplinary Working Group on Qualityof Care and Outcomes Research: en-dorsed by the American Academy of Pe-diatrics. Circulation 2006;114:2710–2738
322. McCrindle BW, Urbina EM, DennisonBA, Jacobson MS, Steinberger J, Roc-chini AP, Hayman LL, Daniels SR, Amer-ican Heart Association Atherosclerosis,
Hypertension, and Obesity in YouthCommittee, American Heart AssociationCouncil of Cardiovascular Disease in theYoung, American Heart AssociationCouncil on Cardiovascular Nursing.Drug therapy of high-risk lipid abnor-malities in children and adolescents: ascientific statement from the AmericanHeart Association Atherosclerosis, Hy-pertension, and Obesity in Youth Com-mittee, Council of CardiovascularDisease in the Young, with the Councilon Cardiovascular Nursing. Circulation2007;115:1948–1967
323. Salo P, Viikari J, Hamalainen M, Lapin-leimu H, Routi T, Ronnemaa T, Sep-panen R, Jokinen E, Valimaki I, SimellO. Serum cholesterol ester fatty acids in7- and 13-month-old children in a pro-spective randomized trial of a low-satu-rated fat, low-cholesterol diet: the STRIPbaby project. Special Turku coronaryRisk factor Intervention Project for chil-dren. Acta Paediatr 1999;88:505–512
324. Efficacy and safety of lowering dietaryintake of fat and cholesterol in childrenwith elevated low-density lipoproteincholesterol. The Dietary InterventionStudy in Children (DISC). The WritingGroup for the DISC Collaborative Re-search Group. JAMA 1995;273:1429–1435
325. McCrindle BW, Ose L, Marais AD. Effi-cacy and safety of atorvastatin in chil-dren and adolescents with familialhypercholesterolemia or severe hyper-lipidemia: a multicenter, randomized,placebo-controlled trial. J Pediatr 2003;143:74–80
326. de Jongh S, Lilien MR, op’t RJ, Stroes ES,Bakker HD, Kastelein JJ. Early statintherapy restores endothelial function inchildren with familial hypercholesterol-emia. J Am Coll Cardiol 2002;40:2117–2121
327. Wiegman A, Hutten BA, de Groot E, Ro-denburg J, Bakker HD, Buller HR, Si-jbrands EJ, Kastelein JJ. Efficacy andsafety of statin therapy in children withfamilial hypercholesterolemia: a ran-domized controlled trial. JAMA 2004;292:331–337
328. Holmes GK. Screening for coeliac dis-ease in type 1 diabetes. Arch Dis Child2002;87:495–498
329. Rewers M, Liu E, Simmons J, RedondoMJ, Hoffenberg EJ: Celiac disease asso-ciated with type 1 diabetes mellitus. En-docrinol Metab Clin North Am 2004;33:197–214, xi
330. Roldan MB, Alonso M, Barrio R. Thyroidautoimmunity in children and adoles-cents with Type 1 diabetes mellitus. Di-abetes Nutr Metab 1999;12:27–31
331. Kordonouri O, Deiss D, Danne T,Dorow A, Bassir C, Gruters-Kieslich A.Predictivity of thyroid autoantibodiesfor the development of thyroid disorders
in children and adolescents with Type 1diabetes. Diabet Med 2002;19:518–521
332. Mohn A, Di Michele S, Di Luzio R,Tumini S, Chiarelli F. The effect of sub-clinical hypothyroidism on metaboliccontrol in children and adolescents withType 1 diabetes mellitus. Diabet Med2002;19:70–73
333. Chase HP, Garg SK, Cockerham RS,Wilcox WD, Walravens PA. Thyroidhormone replacement and growth ofchildren with subclinical hypothyroid-ism and diabetes. Diabet Med 1990;7:299–303
334. Eppens MC, Craig ME, Cusumano J,Hing S, Chan AK, Howard NJ, Silink M,Donaghue KC. Prevalence of diabetescomplications in adolescents with type 2compared with type 1 diabetes. DiabetesCare 2006;29:1300–1306
335. Kitzmiller JL, Gavin LA, Gin GD, Jo-vanovic-Peterson L, Main EK, ZigrangWD. Preconception care of diabetes.Glycemic control prevents congenitalanomalies. JAMA 1991;265:731–736
336. Goldman JA, Dicker D, Feldberg D, Ye-shaya A, Samuel N, Karp M. Pregnancyoutcome in patients with insulin-depen-dent diabetes mellitus with preconcep-tional diabetic control: a comparativestudy. AmJ Obstet Gynecol 1986;155:293–297
337. Rosenn B, Miodovnik M, Combs CA,Khoury J, Siddiqi TA. Pre-conceptionmanagement of insulin-dependent dia-betes: improvement of pregnancy out-come. Obstet Gynecol 1991;77:846–849
338. Tchobroutsky C, Vray MM, Altman JJ.Risk/benefit ratio of changing late ob-stetrical strategies in the management ofinsulin-dependent diabetic pregnancies.A comparison between 1971–1977 and1978–1985 periods in 389 pregnancies.Diabete Metab 1991;17:287–294
339. Willhoite MB, Bennert HW, Jr, PalomakiGE, Zaremba MM, Herman WH, Wil-liams JR, Spear NH. The impact of pre-conception counseling on pregnancyoutcomes. The experience of the MaineDiabetes in Pregnancy Program. Diabe-tes Care 1993;16:450–455
340. Cooper WO, Hernandez-Diaz S, Arbo-gast PG, Dudley JA, Dyer S, Gideon PS,Hall K, Ray WA. Major congenital mal-formations after first-trimester exposureto ACE inhibitors. N Engl J Med 2006;354:2443–2451
341. American Diabetes Association: Precon-ception care of women with diabetes(Position Statement). Diabetes Care2004;27(Suppl. 1):S76–S78
342. Brown AF, Mangione CM, Saliba D,Sarkisian CA, California HealthcareFoundation/American Geriatrics SocietyPanel on Improving Care for Elders withDiabetes. Guidelines for improving thecare of the older person with diabetes
Position Statement
care.diabetesjournals.org DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 S59
mellitus. J Am Geriatr Soc 2003;51:S265–S280
343. Curb JD, Pressel SL, Cutler JA, SavagePJ, Applegate WB, Black H, Camel G,Davis BR, Frost PH, Gonzalez N, GuthrieG, Oberman A, Rutan GH, Stamler J. Ef-fect of diuretic-based antihypertensivetreatment on cardiovascular disease riskin older diabetic patients with isolatedsystolic hypertension. Systolic Hyper-tension in the Elderly Program Cooper-ative Research Group. JAMA 1996;276:1886–1892
344. Beckett NS, Peters R, Fletcher AE, Staes-sen JA, Liu L, Dumitrascu D, StoyanovskyV, Antikainen RL, Nikitin Y, Anderson C,Belhani A, Forette F, Rajkumar C, Thijs L,Banya W, Bulpitt CJ, HYVET StudyGroup. Treatment of hypertension in pa-tients 80 years of age or older. N EnglJ Med 2008;358:1887–1898
345. Clement S, Braithwaite SS, Magee MF,Ahmann A, Smith EP, Schafer RG, Hir-sch IB, Hirsh IB, American Diabetes As-sociation Diabetes in Hospitals WritingCommittee. Management of diabetesand hyperglycemia in hospitals. Diabe-tes Care 2004;27:553–591
346. Moghissi ES, Korytkowski MT, DiNardoM, Einhorn D, Hellman R, Hirsch IB, In-zucchi SE, Ismail-Beigi F, Kirkman MS,Umpierrez GE, American Association ofClinical Endocrinologists, AmericanDiabetes Association. American Asso-ciation of Clinical Endocrinologistsand American Diabetes Associationconsensus statement on inpatient gly-cemic control. Diabetes Care 2009;32:1119 –1131
347. American Diabetes Association: Eco-nomic costs of diabetes in the U.S. In2007. Diabetes Care 2008;31:596–615
348. Centers for Disease Control and Preven-tion. National Diabetes Fact Sheet: Gen-eral Information and National Estimates onDiabetes in the United States, 2007. At-lanta, GA, US Department of Health andHuman Services, 2008
349. Levetan CS, Passaro M, Jablonski K, KassM, Ratner RE. Unrecognized diabetesamong hospitalized patients. DiabetesCare 1998;21:246–249
350. Umpierrez GE, Isaacs SD, Bazargan N,You X, Thaler LM, Kitabchi AE. Hyper-glycemia: an independent marker of in-hospital mortality in patients withundiagnosed diabetes. J Clin EndocrinolMetab 2002;87:978–982
351. van den Berghe G, Wouters P, WeekersF, Verwaest C, Bruyninckx F, Schetz M,Vlasselaers D, Ferdinande P, Lauwers P,Bouillon R. Intensive insulin therapy inthe critically ill patients. N Engl J Med2001;345:1359–1367
352. Malmberg K, Norhammar A, Wedel H,Ryden L. Glycometabolic state at admis-sion: important risk marker of mortality inconventionally treated patients with dia-
betes mellitus and acute myocardial in-farction: long-term results from theDiabetes and Insulin-Glucose Infusion inAcute Myocardial Infarction (DIGAMI)study. Circulation 1999;99:2626–2632
353. Wiener RS, Wiener DC, Larson RJ. Ben-efits and risks of tight glucose control incritically ill adults: a meta-analysis.JAMA 2008;300:933–944
354. Brunkhorst FM, Engel C, Bloos F, Meier-Hellmann A, Ragaller M, Weiler N, Mo-erer O, Gruendling M, Oppert M, GrondS, Olthoff D, Jaschinski U, John S, Ros-saint R, Welte T, Schaefer M, Kern P,Kuhnt E, Kiehntopf M, Hartog C, Natan-son C, Loeffler M, Reinhart K, GermanCompetence Network Sepsis (SepNet).Intensive insulin therapy and pen-tastarch resuscitation in severe sepsis.N Engl J Med 2008;358:125–139
355. NICE-SUGAR Study Investigators, Fin-fer S, Chittock DR, Su SY, Blair D, FosterD, Dhingra V, Bellomo R, Cook D,Dodek P, Henderson WR, Hebert PC,Heritier S, Heyland DK, McArthur C,McDonald E, Mitchell I, Myburgh JA,Norton R, Potter J, Robinson BG, RoncoJJ. Intensive versus conventional glucosecontrol in critically ill patients. N EnglJ Med 2009;360:1283–1297
356. Krinsley JS, Grover A. Severe hypoglyce-mia in critically ill patients: risk factorsand outcomes. Crit Care Med 2007;35:2262–2267
357. Van den Berghe G, Wilmer A, HermansG, Meersseman W, Wouters PJ, MilantsI, Van Wijngaerden E, Bobbaers H,Bouillon R. Intensive insulin therapy inthe medical ICU. N Engl J Med 2006;354:449–461
358. Griesdale DE, de Souza RJ, van Dam RM,Heyland DK, Cook DJ, Malhotra A,Dhaliwal R, Henderson WR, ChittockDR, Finfer S, Talmor D. Intensive insulintherapy and mortality among criticallyill patients: a meta-analysis includingNICE-SUGAR study data. CMAJ 2009;180:821–827
359. Saudek CD, Herman WH, Sacks DB,Bergenstal RM, Edelman D, DavidsonMB. A new look at screening and diag-nosing diabetes mellitus. J Clin Endocri-nol Metab 2008;93:2447–2453
360. Mitrakou A, Ryan C, Veneman T, MokanM, Jenssen T, Kiss I, Durrant J, Cryer P,Gerich J. Hierarchy of glycemic thresholdsfor counterregulatory hormone secretion,symptoms, and cerebral dysfunction. Am JPhysiol 1991;260:E67–E74
361. Korytkowski M, DiNardo M, Donihi AC,Bigi L, Devita M. Evolution of a diabetesinpatient safety committee. Endocr Pract2006;12(Suppl. 3):91–99
362. DiNardo M, Noschese M, KorytkowskiM, Freeman S. The medical emergencyteam and rapid response system: find-ing, treating, and preventing hypoglyce-mia. Jt Comm J Qual Patient Saf 2006;
32:591–595363. Donihi AC, Raval D, Saul M, Koryt-
kowski MT, DeVita MA. Prevalence andpredictors of corticosteroid-related hy-perglycemia in hospitalized patients.Endocr Pract 2006;12:358–362
364. Goldberg PA, Siegel MD, Sherwin RS,Halickman JI, Lee M, Bailey VA, Lee SL,Dziura JD, Inzucchi SE. Implementationof a safe and effective insulin infusionprotocol in a medical intensive care unit.Diabetes Care 2004;27:461–467
365. Rea RS, Donihi AC, Bobeck M, Herout P,McKaveney TP, Kane-Gill SL, Koryt-kowski MT. Implementing an intrave-nous insulin infusion protocol in theintensive care unit. Am J Health SystPharm 2007;64:385–395
366. Nazer LH, Chow SL, Moghissi ES. Insu-lin infusion protocols for critically ill pa-tients: a highlight of differences andsimilarities. Endocr Pract 2007;13:137–146
367. DeSantis AJ, Schmeltz LR, Schmidt K,O’Shea-Mahler E, Rhee C, Wells A,Brandt S, Peterson S, Molitch ME. Inpa-tient management of hyperglycemia: theNorthwestern experience. Endocr Pract2006;12:491–505
368. Noschese M, Donihi AC, Koerbel G,Karslioglu E, DiNardo M, Curll M, Ko-rytkowski MT. Effect of a diabetes orderset on glycaemic management and con-trol in the hospital. Qual Saf Health Care2008;17:464–468
369. Umpierrez GE, Hor T, Smiley D, Tem-poni A, Umpierrez D, Ceron M, MunozC, Newton C, Peng L, Baldwin D. Com-parison of inpatient insulin regimenswith detemir plus aspart versus neutralprotamine hagedorn plus regular inmedical patients with type 2 diabetes.J Clin Endocrinol Metab 2009;94:564–569
370. Moghissi ES, Hirsch IB. Hospital man-agement of diabetes. Endocrinol MetabClin North Am 2005;34:99–116
371. Umpierrez GE, Smiley D, Zisman A, Pri-eto LM, Palacio A, Ceron M, Puig A, Me-jia R. Randomized study of basal-bolusinsulin therapy in the inpatient manage-ment of patients with type 2 diabetes(RABBIT 2 trial). Diabetes Care 2007;30:2181–2186
372. Umpierrez GE, Palacio A, Smiley D.Sliding scale insulin use: myth or insan-ity? Am J Med 2007;120:563–567
373. Queale WS, Seidler AJ, Brancati FL. Gly-cemic control and sliding scale insulinuse in medical inpatients with diabetesmellitus. Arch Intern Med 1997;157:545–552
374. Korytkowski MT, Salata RJ, Koerbel GL,Selzer F, Karslioglu E, Idriss AM, LeeKK, Moser AJ, Toledo FG. Insulin ther-apy and glycemic control in hospitalizedpatients with diabetes during enteral nu-trition therapy: a randomized controlled
Standards of Medical Care
S60 DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 care.diabetesjournals.org

clinical trial. Diabetes Care 2009;32:594–596
375. Hirsch IB. Sliding scale insulin–time tostop sliding. JAMA 2009;301:213–214
376. Umpierrez GE. Basal versus sliding-scaleregular insulin in hospitalized patientswith hyperglycemia during enteral nu-trition therapy. Diabetes Care 2009;32:751–753
377. Pancorbo-Hidalgo PL, García-Fernan-dez FP, Ramírez-Perez C. Complicationsassociated with enteral nutrition by na-sogastric tube in an internal medicineunit. J Clin Nurs 2001;10:482–490
378. Nylen ES, Muller B. Endocrine changesin critical illness. J Intensive Care Med2004;19:67–82
379. Shilo S, Berezovsky S, Friedlander Y,Sonnenblick M. Hypoglycemia in hospi-talized nondiabetic older patients. J AmGeriatr Soc 1998;46:978–982
380. Fischer KF, Lees JA, Newman JH. Hypo-glycemia in hospitalized patients.Causes and outcomes. N Engl J Med1986;315:1245–1250
381. Markovitz LJ, Wiechmann RJ, Harris N,Hayden V, Cooper J, Johnson G, Harel-stad R, Calkins L, Braithwaite SS. De-scription and evaluation of a glycemicmanagement protocol for patients withdiabetes undergoing heart surgery. En-docr Pract 2002;8:10–18
382. Levetan CS, Salas JR, Wilets IF, ZumoffB. Impact of endocrine and diabetesteam consultation on hospital length ofstay for patients with diabetes. Am J Med1995;99:22–28
383. Levetan CS, Passaro MD, Jablonski KA,Ratner RE. Effect of physician specialtyon outcomes in diabetic ketoacidosis.Diabetes Care 1999;22:1790–1795
384. Koproski J, Pretto Z, Poretsky L. Effectsof an intervention by a diabetes team inhospitalized patients with diabetes. Dia-betes Care 1997;20:1553–1555
385. Furnary AP, Braithwaite SS. Effects ofoutcome on in-hospital transition fromintravenous insulin infusion to subcuta-neous therapy. Am J Cardiol 2006;98:557–564
386. American Diabetes Association: Diabe-tes nutrition recommendations forhealth care institutions (Position State-ment). Diabetes Care 2004;27(Suppl.1):S55–S57
387. Boucher JL, Swift CS, Franz MJ,Kulkarni K, Schafer RG, Pritchett E,Clark NG. Inpatient management of di-abetes and hyperglycemia: implicationsfor nutrition practice and the food andnutrition professional. J Am Diet Assoc2007;107:105–111
388. Scott MG, Bruns DE, Boyd JC, Sacks DB.Tight glucose control in the intensivecare unit: are glucose meters up to thetask? Clin Chem 2009;55:18–20
389. D’Orazio P, Burnett RW, Fogh-Andersen N, Jacobs E, Kuwa K, Kulp-mann WR, Larsson L, Lewenstam A,Maas AH, Mager G, Naskalski JW,Okorodudu AO, International Federa-tion of Clinical Chemistry Scientific Di-vision Working Group on SelectiveElectrodes and Point of Care Testing.Approved IFCC recommendation on re-porting results for blood glucose (abbre-viated). Clin Chem 2005;51:1573–1576
390. Dungan K, Chapman J, Braithwaite SS,Buse J. Glucose measurement: con-founding issues in setting targets for in-patient management. Diabetes Care2007;30:403–409
391. Boyd JC, Bruns DE. Quality specifica-tions for glucose meters: assessment bysimulation modeling of errors in insulindose. Clin Chem 2001;47:209–214
392. Goldberg PA, Siegel MD, Russell RR, Sh-erwin RS, Halickman JI, Cooper DA,Dziura JD, Inzucchi SE. Experience withthe continuous glucose monitoring sys-tem in a medical intensive care unit. Di-abetes Technol Ther 2004;6:339–347
393. Cheung BM, Ong KL, Cherny SS, ShamPC, Tso AW, Lam KS. Diabetes preva-lence and therapeutic target achieve-ment in the United States, 1999 to 2006.Am J Med 2009;122:443–453
394. Coleman K, Austin BT, Brach C, WagnerEH. Evidence on the Chronic CareModel in the new millennium. HealthAff (Millwood) 2009;28:75–85
395. Clark CM, Jr, Snyder JW, Meek RL, StutzLM, Parkin CG. A systematic approachto risk stratification and interventionwithin a managed care environment im-proves diabetes outcomes and patientsatisfaction.DiabetesCare2001;24:1079–1086
396. Meigs JB, Cagliero E, Dubey A, Murphy-Sheehy P, Gildesgame C, Chueh H,Barry MJ, Singer DE, Nathan DM. A con-trolled trial of web-based diabetes dis-ease management: the MGH diabetesprimary care improvement project. Dia-betes Care 2003;26:750–757
397. O’Connor PJ, Desai J, Solberg LI, RegerLA, Crain AL, Asche SE, Pearson TL,Clark CK, Rush WA, Cherney LM,Sperl-Hillen JM, Bishop DB. Random-ized trial of quality improvement inter-vention to improve diabetes care inprimary care settings. Diabetes Care2005;28:1890–1897
398. Sperl-Hillen JM, O’Connor PJ. Factorsdriving diabetes care improvement in alarge medical group: ten years ofprogress. Am J Manag Care 2005;11:S177–S185
399. Siminerio LM. Implementing diabetesself-management training programs:breaking through the barriers in pri-mary care. EndocrPract 2006;12(Suppl.
1):124–130400. Mahoney JJ. Reducing patient drug ac-
quisition costs can lower diabetes healthclaims. Am J Manag Care 2005;11:S170–S176
401. Maney M, Tseng CL, Safford MM, MillerDR, Pogach LM. Impact of self-reportedpatient characteristics upon assessmentof glycemic control in the VeteransHealth Administration. Diabetes Care2007;30:245–251
402. Bergenstal RM. Treatment models fromthe International Diabetes Center: ad-vancing from oral agents to insulin ther-apy in type 2 diabetes. Endocr Pract2006;12(Suppl. 1):98–104
403. Berikai P, Meyer PM, Kazlauskaite R,Savoy B, Kozik K, Fogelfeld L. Gain inpatients’ knowledge of diabetes manage-ment targets is associated with betterglycemic control. Diabetes Care 2007;30:1587–1589
404. O’Connor PJ. Electronic medical recordsand diabetes care improvement: are wewaiting for Godot? Diabetes Care 2003;26:942–943
405. Shojania KG, Ranji SR, McDonald KM,Grimshaw JM, Sundaram V, RushakoffRJ, Owens DK. Effects of quality im-provement strategies for type 2 diabeteson glycemic control: a meta-regressionanalysis. JAMA 2006;296:427–440
406. Davidson MB. How our current medicalcare system fails people with diabetes:lack of timely, appropriate clinical deci-sions. Diabetes Care 2009;32:370–372
407. McLean DL, McAlister FA, Johnson JA,King KM, Makowsky MJ, Jones CA,Tsuyuki RT, SCRIP-HTN Investigators. Arandomized trial of the effect of commu-nity pharmacist and nurse care on improv-ing blood pressure management inpatients with diabetes mellitus: study ofcardiovascular risk intervention by phar-macists-hypertension (SCRIP-HTN). ArchIntern Med 2008;168:2355–2361
408. Parchman ML, Zeber JE, Romero RR,Pugh JA. Risk of coronary artery diseasein type 2 diabetes and the delivery ofcare consistent with the chronic caremodel in primary care settings: a STAR-Net study. Med Care 2007;45:1129–1134
409. Feifer C, Nemeth L, Nietert PJ, WessellAM, Jenkins RG, Roylance L, OrnsteinSM. Different paths to high-quality care:three archetypes of top-performingpractice sites. Ann Fam Med 2007;5:233–241
410. Ornstein S, Nietert PJ, Jenkins RG, Wes-sell AM, Nemeth LS, Feifer C, CorleyST. Improving diabetes care through amulticomponent quality improvementmodel in a practice-based research net-work. Am J Med Qual 2007;22:34–41
Position Statement
care.diabetesjournals.org DIABETES CARE, VOLUME 33, SUPPLEMENT 1, JANUARY 2010 S61