diabetes management of patients with covid -19 …
TRANSCRIPT
DIABETES MANAGEMENT OF PATIENTS WITH COVID-19 INFECTION
Prof DR Dr Agung Pranoto, Mkes, SpPD, K-EMD, FINASIMDr Deasy Ardiany, SpPD, K-EMD, FINASIM
Diabetes & Nutrition CenterDivision of Endocrinology Metabolism
Department of Internal MedicineRSUD Dr.Soetomo General Hospital-Medical Faculty of Airlangga University

About COVID-19
Link between COVID-19
and Diabetes
Preventionand
Treatment
Summary
OUTLINE
PowerPoint Presentation Date 2

WORLDWIDE COVID-19 OUTBREAK SITUATION
74,327,556102,628,183 2,216,279 221
Recovered/Discharged
Confirmedcases
Confirmed Deaths
Countries, areas or
territories with cases
Ref:WorldHealthOrganization(updateon30th January,2021),worldometers.info/coronavirus/coronavirus-cases/

INDONESIA COVID-19 OUTBREAK SITUATION
852,2601,051,795 29,518 9,124,005
Recovered/Discharged
Confirmed cases
Confirmed deaths
Total COVID-19 tests
conducted
Ref:WorldHealthOrganization(updateon30th January,2021),worldometers.info/coronavirus/coronavirus-cases/

PREVALENCE OF COMORBIDITIES IN COVID 19 INFECTION
Yang J et al. Int J Infect Dis. S1201-9712(20)30136-3. doi: 10.1016/j.ijid.2020.03.017.
Meta analysis of 8 studies with 46,248 COVID-19 patients showed the most prevalent comorbidity:
Hypertension 17±7
(95% CI 14-22%)
Diabetes 8±6
(95% CI 6-11%)
Cardiovascular diseases
5±4(95% CI 4-7%)
Respiratory system disease
2±0(95% CI 1-3%)

About COVID-19
Link between COVID-19
and Diabetes
Preventionand
Treatment
Summary
OUTLINE
PowerPoint Presentation Date 6

• People with diabetes are NOT MORE likely to get COVID-19 than the general population
• Diabetes is one of the high risk groups for developing severe illness from COVID-19
• The risk of having worse outcomes is similar for people with T1D and T2D
DIABETES AND COVID-19
T1D, type 1 diabetes; T2D, type 2 diabetesADA: https://www.diabetes.org/coronavirus-covid-19; CDC: https://www.cdc.gov/coronavirus/2019-ncov/specific-groups/people-at-higher-risk.html

SURVIVAL RATE IN COVID-19 PATIENT WITH DIABETES
• Survival rate of COVID-19 patient with Diabetes is worse than patient without diabetes
Shi Q,. Diabetes Care. 2020 May 14.

DIABETES MAY ACCENTUATE COVID-19: POTENTIAL MECHANISM
Diabetes
SARS-CoV
Activate
Promotes
• High levels of IL-6, TNF-α and other
inflammatory cytokines in people with
diabetes1
• Coronavirus likely to activate TLR3 and
TLR4, leading to IL-6-dominated cytokine
storms2,3
• IL-6 associated with death of COVID-19
patients4
Overactivation of TLR4 signaling in diabetesmay lead to severe disease and death
1. Reza F, et al. Cytokine ,2019, 125 (2020) 154832
2. Travis B. ,et al. mBio, 2017 8:e00818-17.3. Allison L. T, et al. mBio, 2015 , 3:e00638-15
4. Zhou F , et al. The Lancet 2020 March 9 online
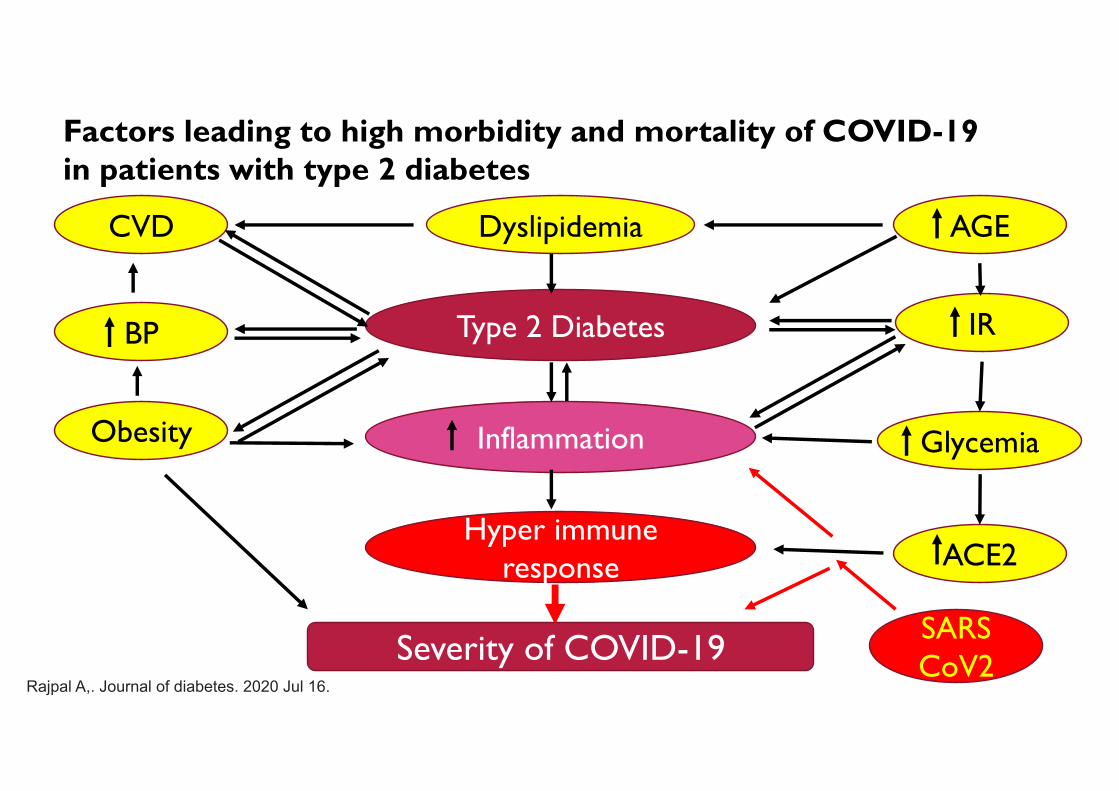
Type 2 Diabetes
Inflammation
Hyper immune response
Severity of COVID-19
ACE2
Glycemia
IR
AGEDyslipidemiaCVD
BP
Obesity
SARS CoV2
Factors leading to high morbidity and mortality of COVID-19 in patients with type 2 diabetes
Rajpal A,. Journal of diabetes. 2020 Jul 16.
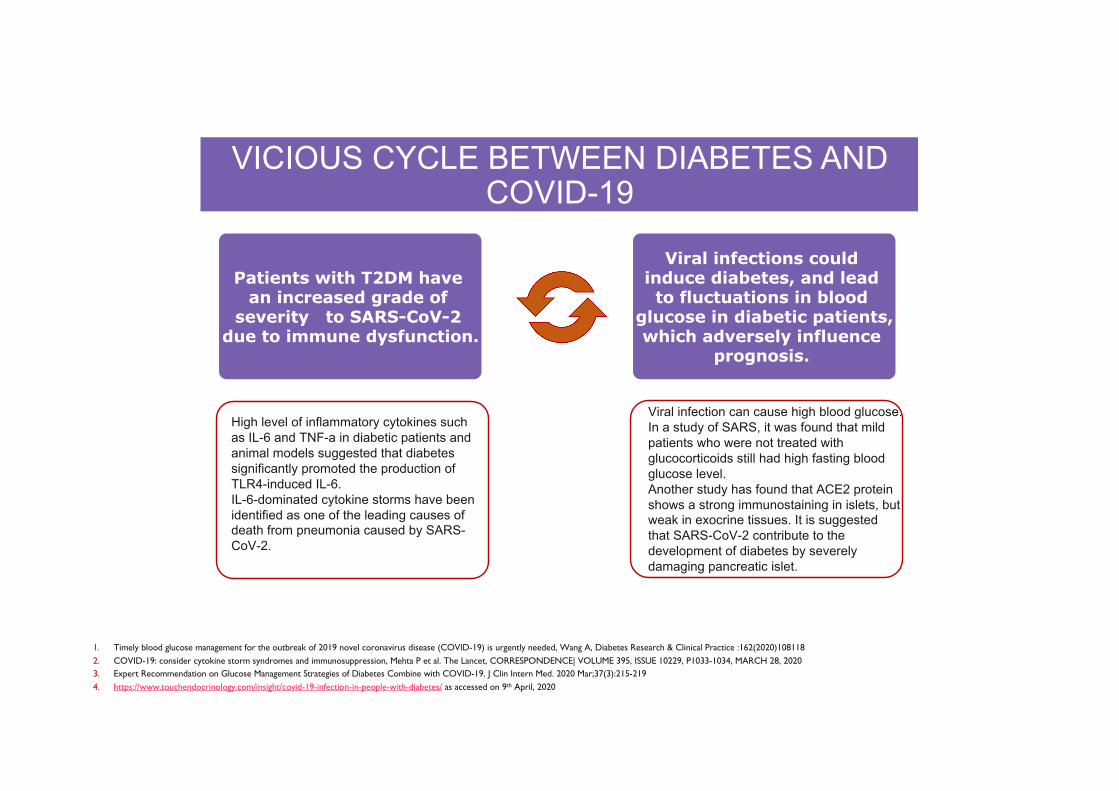
VICIOUS CYCLE BETWEEN DIABETES AND COVID-19
Patients with T2DM have an increased grade of
severity to SARS-CoV-2 due to immune dysfunction.
Viral infections could induce diabetes, and lead to fluctuations in blood
glucose in diabetic patients, which adversely influence
prognosis.
High level of inflammatory cytokines such as IL-6 and TNF-a in diabetic patients and animal models suggested that diabetes significantly promoted the production of TLR4-induced IL-6.IL-6-dominated cytokine storms have been identified as one of the leading causes of death from pneumonia caused by SARS-CoV-2.
Viral infection can cause high blood glucose. In a study of SARS, it was found that mild patients who were not treated with glucocorticoids still had high fasting blood glucose level.Another study has found that ACE2 protein shows a strong immunostaining in islets, but weak in exocrine tissues. It is suggested that SARS-CoV-2 contribute to the development of diabetes by severely damaging pancreatic islet.
1. Timely blood glucose management for the outbreak of 2019 novel coronavirus disease (COVID-19) is urgently needed, Wang A, Diabetes Research & Clinical Practice :162(2020)1081182. COVID-19: consider cytokine storm syndromes and immunosuppression, Mehta P et al. The Lancet, CORRESPONDENCE| VOLUME 395, ISSUE 10229, P1033-1034, MARCH 28, 20203. Expert Recommendation on Glucose Management Strategies of Diabetes Combine with COVID-19. J Clin Intern Med. 2020 Mar;37(3):215-2194. https://www.touchendocrinology.com/insight/covid-19-infection-in-people-with-diabetes/ as accessed on 9th April, 2020

COVID-19 MAY ACCENTUATE DIABETES: POTENTIAL MECHANISM
1. YangJ-K, et al Acta Diabetol. 2010;47(3):193-199
2. WuF, et al. Nature. February 2020.
ACE2 - Angiotensin converting enzyme 2
• ACE2 is the functional receptor of SARS-CoV (SARS
epidemic)
• ACE2 expression in the pancreatic tissue
suggests SARS-CoV may damage pancreatic
islets1
• SARS-CoV-2 (COVID-19 pandemic) is able to
efficiently use human ACE2 as a receptor for cellular
entry2
SARS mortality was higher inpatients with hyperglycemia1
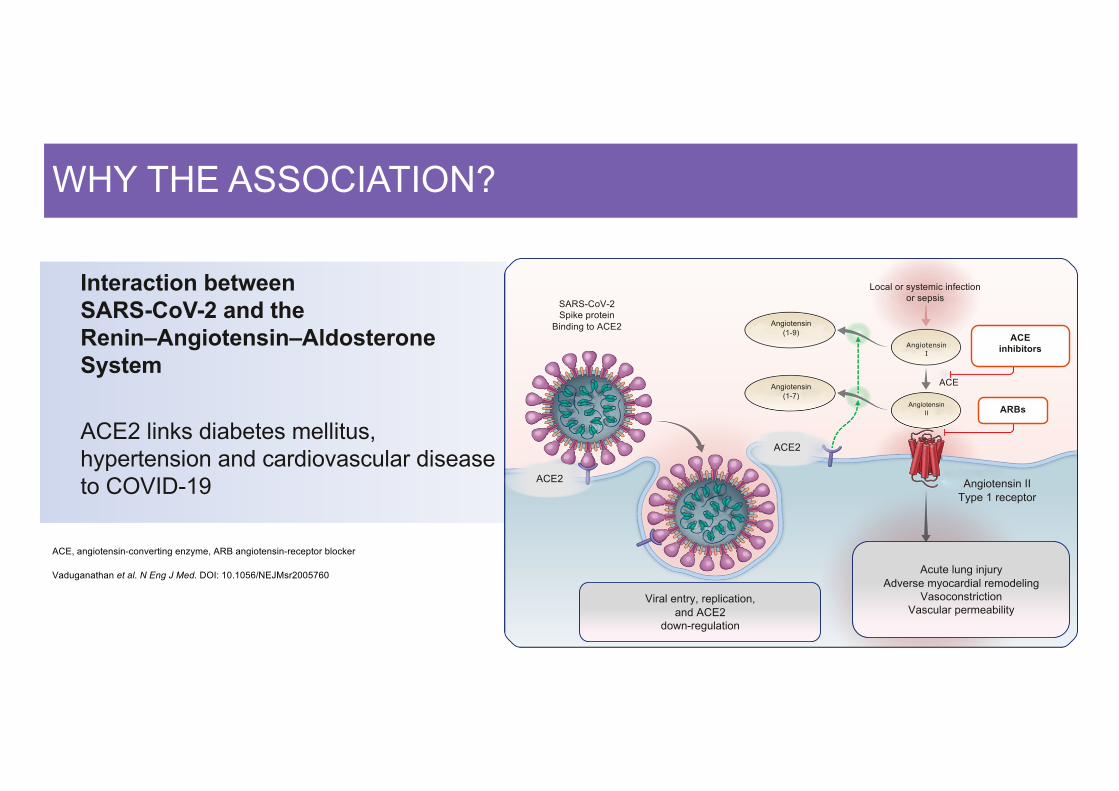
WHY THE ASSOCIATION?
ACE, angiotensin-converting enzyme, ARB angiotensin-receptor blocker
Vaduganathan et al. N Eng J Med. DOI: 10.1056/NEJMsr2005760
Interaction between SARS-CoV-2 and the Renin–Angiotensin–Aldosterone System
ACE2 links diabetes mellitus, hypertension and cardiovascular disease to COVID-19
SARS-CoV-2Spike protein
Binding to ACE2
ACE2
Angiotensin (1-9)
Angiotensin (1-7)
Angiotensin I
Angiotensin II
ACEinhibitors
ARBs
Local or systemic infection or sepsis
ACE
Angiotensin IIType 1 receptor
Viral entry, replication, and ACE2
down-regulation
Acute lung injuryAdverse myocardial remodeling
VasoconstrictionVascular permeability
ACE2
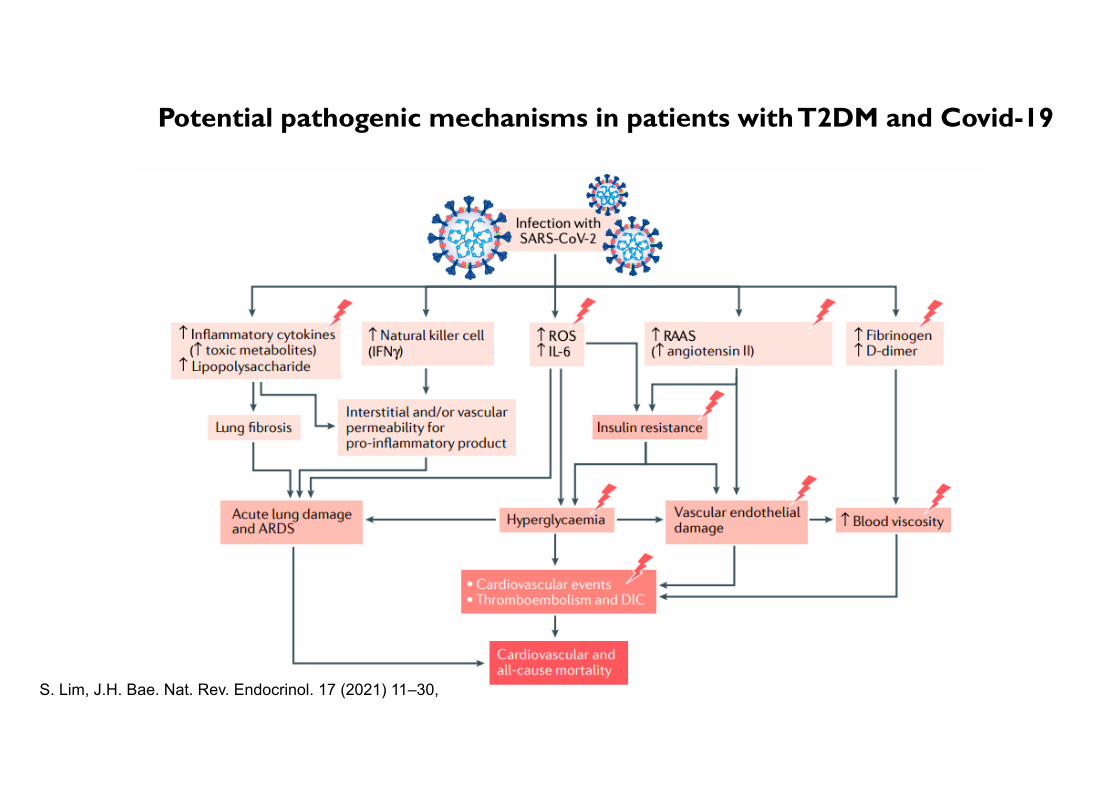
Potential pathogenic mechanisms in patients with T2DM and Covid-19
S. Lim, J.H. Bae. Nat. Rev. Endocrinol. 17 (2021) 11–30,
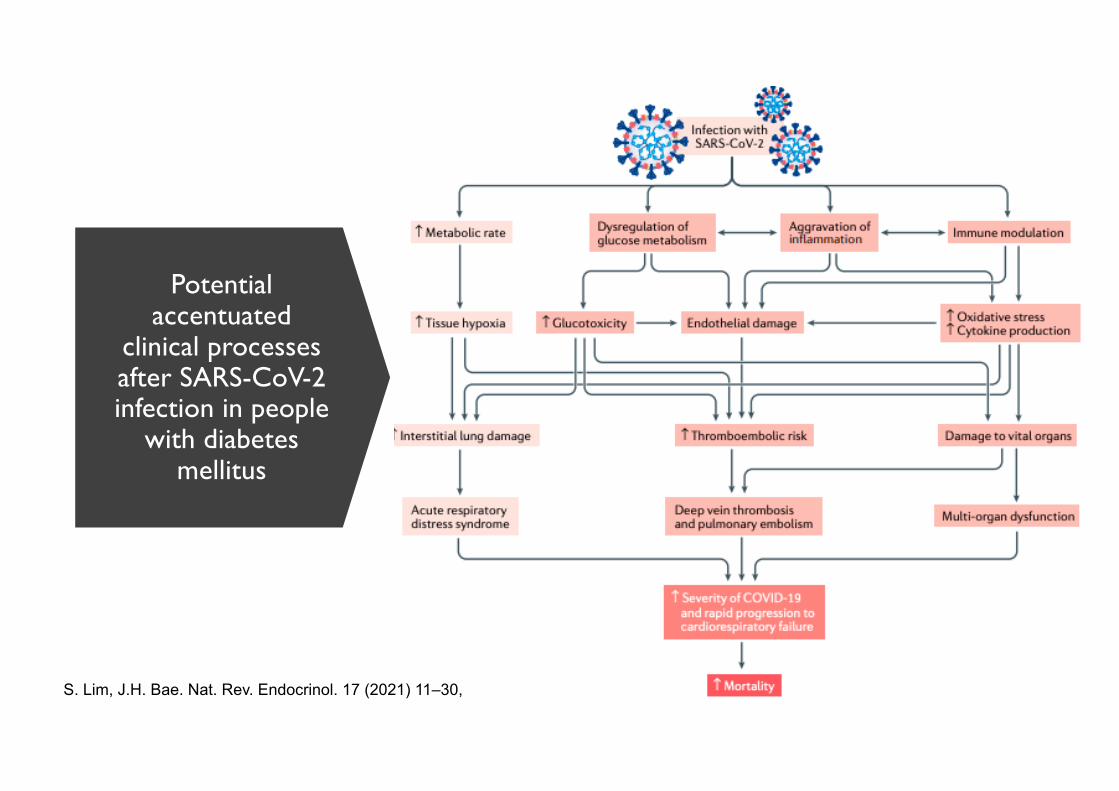
Potential accentuated
clinical processes after SARS-CoV-2 infection in people
with diabetes mellitus
S. Lim, J.H. Bae. Nat. Rev. Endocrinol. 17 (2021) 11–30,

DatePowerPoint Presentation
16
Umpierrez & Pasquel, 2017

Clinical characteristics and outcomes in patients with diabetes mellitus and COVID-19
S. Lim, J.H. Bae. Nat. Rev. Endocrinol. 17 (2021) 11–30,
Well Controlled Glycemic Good
Prognostic
HbA1c > 7.5% Bad Prognostic

CLINICAL SCENARIOS OF DIABETES MANAGEMENT DURING THE COVID-19 PANDEMIC
Stressful, anxious,depressed
Increased consumption of alcohol
Insomnia/hypersomnia/change in diurnal
rhythms
Change in regimen (withdraw or change
medications )
No exercise/over-exercise
Change in compliance to
medications (dosing time and frequency)
Miss routine visit
Eat too much/miss meals
Delayed visit to emergency
care
Change in diet composition
Recommendations for COVID-19 Prevention in Diabetes Patients Endorsed by Chinese Diabetes Society (CDS). CDS website: www.diab.net.cn CDS WeChat: CDS-TNB

DIABETES PROMOTES SEVERE PROGRESSION IN COVID-19 PATIENTS
*Data was extracted regarding 1099 patients with laboratory-confirmed Covid-19 from 552 hospitals in 30 provinces, autonomous regions, and municipalities in China through January 29th, 2020.
1.Guan WJ , et al. NEJM , 2020 Feb 28, DOI: 10.1056/NEJMoa2002032
2.Guan WJ,medRxiv preprint ,2020 online
The risk of reaching to the composite endpoints*and disease severity among patients with COVID-192
• The presence of coexisting diabetes was more common among COVID-19 patients with severe disease than among those with non-severe disease (16.2% vs.5.7%).*1
• Another nationwide analysis of comorbidity and its impact on 1,590 patients with COVID-19 in China also revealed that,(22.9% vs 6.8%)2
COVID-19 patients with comorbidities1
*Composite endpoint: admission to an intensive care unit (ICU),the use of mechanical ventilation, or death. 。
With chronic medical illness
With diabetes
23,7%
38,7%
21,0%
7,4%
16,2%
5,7%
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
All patients Severe Non-severe
Prop
ortio
n of
pat
ient
s(%)
N=1099 N=173 N=926
8,2%
22,9%
6,8%
16,0%
34,6%
14,3%
0%
5%
10%
15%
20%
25%
30%
35%
40%
All patients Diabetic Non-diabetic
Prop
ortio
n of
pat
ient
s (
%)
P<0.001
N=1590 N=130 N=1460
P<0.001 Composite endpoint %*
Severe%

DIABETES IS A RISK FACTOR FOR MORTALITY OF COVID-19
1. Zhang BC, et al. medRxiv preprint , 2020 online
2. Guan WJ,et al. medRxiv preprint , 2020 online
3.China CDC Weekly,2020, 2(8): 113-122
4.《Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19),2020
• A large national sample study showed that the mortality of patients with diabetes was significantly higher than that of non-diabetic patients(10% vs 2.5% P<0.0012) (Figure 1)
• Chinese CDC declared that patients who reported no comorbid conditions had a case fatality rate(CFR**) of 0.9%, while patients with comorbid conditions had much higher rates--7.3% for diabetes.3(Figure 2)
3,1%
10,0%
2,5%
0%
4%
8%
12%
All patients Diabetic Non- diabetic
P<0.001
Figure 1:The mortality of 1590COVID-19 patients
N=1590 N=130 N=1460
Cas
e fa
talit
y ra
te (
%)
2,3%
7,3%
0,9%
0%
2%
4%
6%
8%
All patients Diabetic No comorbid conditions*
Figure 2:The mortality of COVID-19 patients reported by China CDC
N=20,982 N=1,102 N=15,536
Cas
e fa
talit
y ra
te (
%)
* The comorbid condition variable, only includes a total of 20,812 patients and 504 deaths and these values were used to calculate percentages in the confirmed cases anddeaths columns.
**The Joint Mission acknowledges the known challenges and biases of reporting crude CFR early in an epidemic.

ASSOCIATIONS OF DIABETES AND FBG WITH FATALITY OF COVID-19
FBG, fasting blood glucose
Zhang Y et al. https://www.medrxiv.org/content/10.1101/2020.03.24.20042358v1
Model Ia Model IIb Model IIIc
Variable AHR(95% CI)
P AHR(95% CI)
P AHR(95% CI)
P
DM 2.80 (1.01,7.80) 0.048 2.840(1.01, 8.01)
0.048 3.64 (1.09, 12.21)
0.036
FBG (mmol/L) 1.14 (1.06,1.22) <0.001 1.142 (1.07, 1.23)
<0.001 1.19 (1.08, 1.31)
<0.001
AHR, adjusted hazard ratio; CI: confidence interval. DM: diabetes mellitus; FBG: fasting blood glucose. a Adjusted for age. b Additionally adjusted for preexisting cardiovascular disease and chronic kidney disease. c Additionally adjusted for inflammatory biomarkers (leucocytes, neutrophils, lymphocyte, eosinophil, NLR, neutrophil-to-lymphocyte ratio; C-reactive protein, procalcitonin).
RSUD Dr Soetomo:OR 2,66 (95%CI 1.99– 3.57)
(n= 883, 1 Jan – 27 Sept, tanpa RIK 1 & 3), unpublished data

PowerPoint Presentation Date 22
Zhu, L., She, Z.G., Cheng, X., Qin, J.J., Zhang, X.J., Cai, J., Lei, F., Wang, H., Xie, J., Wang, W. and Li, H., 2020. Association of blood glucose control and outcomes in patients with COVID-19 and pre-existing type 2 diabetes. Cell metabolism.

About COVID-19
Link between COVID-19
and Diabetes
Preventionand
Treatment
Summary
OUTLINE
PowerPoint Presentation Date 23
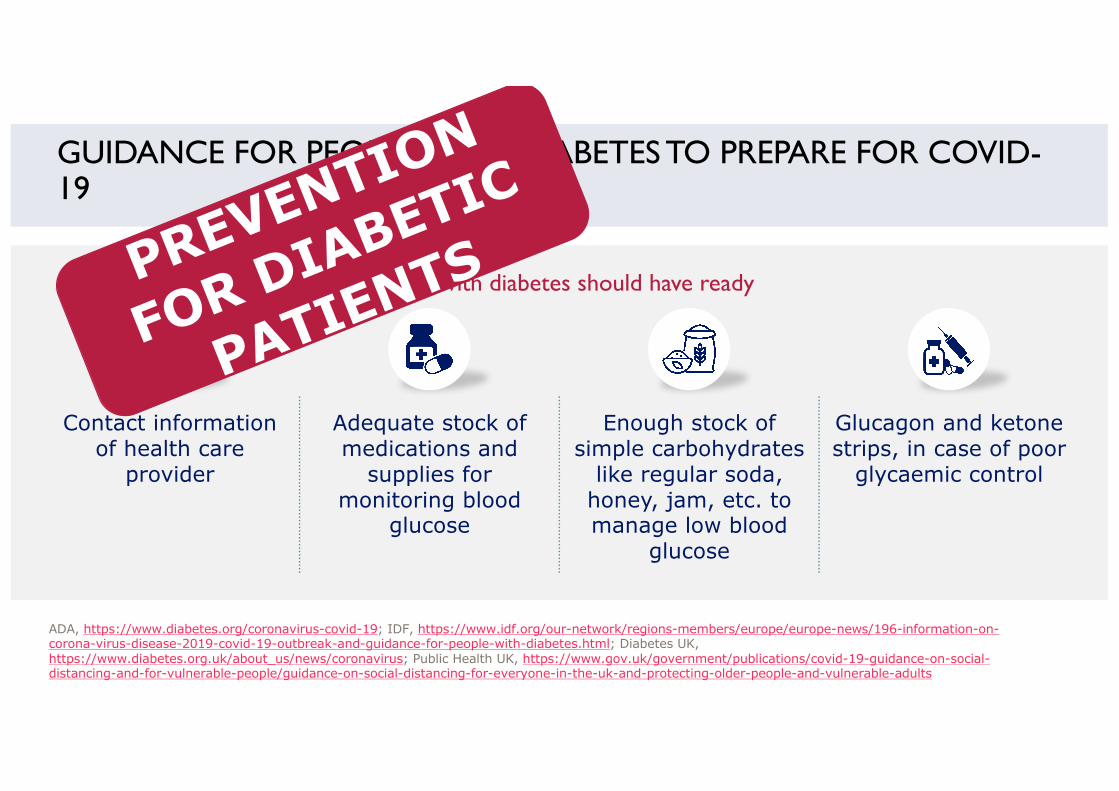
People with diabetes should have ready
GUIDANCE FOR PEOPLE WITH DIABETES TO PREPARE FOR COVID-19
ADA, https://www.diabetes.org/coronavirus-covid-19; IDF, https://www.idf.org/our-network/regions-members/europe/europe-news/196-information-on-corona-virus-disease-2019-covid-19-outbreak-and-guidance-for-people-with-diabetes.html; Diabetes UK, https://www.diabetes.org.uk/about_us/news/coronavirus; Public Health UK, https://www.gov.uk/government/publications/covid-19-guidance-on-social-distancing-and-for-vulnerable-people/guidance-on-social-distancing-for-everyone-in-the-uk-and-protecting-older-people-and-vulnerable-adults
Contact information of health care
provider
Adequate stock of medications and
supplies for monitoring blood
glucose
Enough stock of simple carbohydrates
like regular soda, honey, jam, etc. to manage low blood
glucose
Glucagon and ketone strips, in case of poor
glycaemic control

PERKENI RECOMMENDATION
PowerPoint Presentation Date 25
https://pbperkeni.or.id/pernyataan-resmi-dan-rekomendasi-penanganan-diabetes-mellitus-di-era-pandemi-covid-19/

PERKENI RECOMMENDATION
PowerPoint Presentation Date 26
https://pbperkeni.or.id/pernyataan-resmi-dan-rekomendasi-penanganan-diabetes-mellitus-di-era-pandemi-covid-19/

MANAGEMENT OF PEOPLE WITH DIABETES INFECTED WITH COVID-19 RECOMMENDATIONS
General:1) Patients are advised to drink lots of fluids to stay hydrated. To avoid dehydration, patients should have small sips every 15 minutes or so
throughout the day if they are having trouble keeping water down.2) Hands should be washed, and injection/infusion and finger-stick sites should be cleaned with soap and water or rubbing alcohol. 3) Recommendations of local authority should be followed if suspected of COVID-19 symptoms.
ADA, https://www.diabetes.org/coronavirus-covid-19; Diabetes UK, https://www.diabetes.org.uk/about_us/news/coronavirus; IDF, https://www.idf.org/our-network/regions-members/europe/europe-news/196-information-on-corona-virus-disease-2019-covid-19-outbreak-and-guidance-for-people-with-diabetes.html; ISPAD, https://www.ispad.org/news/494473/COVID-19-and-Children-with-Diabetes.htm
• Patients should follow the advice of the physician (diabetes care team) on adjustments to their anti-diabetic medication(s)
• Blood glucose levels should be frequently checked (generally, every 2-3 hours)
• Management of COVID-19 infection by patient and HCPs should follow sick day rules appropriate to any other infection
• Patients should be aware of signs and symptoms of hyperglycaemia
Anti-diabetic medication Monitoring Maintain
glycaemic control

For the COVID-19 patients with diabetes, tailored therapeutic strategy and optimal goal of glucose control should be formulated based on clinical classification, coexisting comorbidities, age and other risk factors.
TIMELY BLOOD GLUCOSE MANAGEMENT FOR THE OUTBREAK OF 2019 NOVELCORONAVIRUS DISEASE (COVID-19) IS URGENTLY NEEDED
PowerPoint Presentation Date 28
Hospitalized Critical Case
• During the 4-week follow-up period after discharge, blood
glucose homeostasis should be maintained continuously and
patients need to avoid infectious diseases due to a lower immune response. Long-term follow-up is still essential for diabetic patients
to reduce diabetes-related complications and mortality
Afterdischarge
Blood glucose should be controlled for all
patients during hospitalization to
monitor the progress of illness and avoid
aggravation.
For critical cases, early identification and timely reduction adverse drug reaction (for instance, glucocorticoid-induced hyperglycemia) could
prevent worse symptoms.
https://www.diabetesresearchclinicalpractice.com/article/S0168-8227(20)30368-5/pdf

• Expert Recommendation on Glucose Management Strategies of Diabetes Combine with COVID-19. J Clin Intern Med. 2020 Mar;37(3):215-219
Target stratification of glucose management:ü For mild and moderate non-elderly COVID-19 patients, stick to strict high control
targetü For mild and moderate elderly patients, or patients who have been using
glucocorticoid, set up a low or medium control target ü For severe and critical patients, elderly patients, hypoglycemia intolerable patients,
or patients who have organ dysfunction or serious cardiovascular and cerebrovascular diseases, set up a low control target
Target stratification of glucose management in hospitalized patients
Hypoglycemia occurrence should be minimized during glucose management in diabetes patients with COVID-19. Medical care should be performed in time if hypoglycemia occurs.
High (mmol/L) (mg/dL)
Medium (mmol/L) (mg/dL)
Low (mmol/L) (mg/dL)
FPG/PPG 4.4-6.1 (79.2-109.8) 6.1-7.8 (109.8-140.4) 7.8-10.0 (140.4-180)
2h PPG/GLU 6.1-7.8 (109.8-140.4) 7.8-10.0 (140.4-180) 7.8-13.9 (140.4-250.2)

CATEGORIZED GUIDANCE TO MANAGE DIABETES IN CRITICAL INFECTIONS
1. International Diabetes Federation, sick day rules Accessed 8 March 2020.2. Sichuan Da Xue Xue Bao Yi Xue Ban. 2020 Mar;51(2):146-150.© 2020 Eli Lilly and Company.
• Take diabetes medication as usual. Insulin treatment should never be stopped
• Test blood glucose every four hours, and keep track of the results
• Drink extra (calorie-free) fluid*, and try to eat as normal • Weigh yourself every day. Losing weight while eating normally
is a sign of high blood glucose • Check temperature every morning and evening. A fever may be
a sign of infection
General guidelines to manage Diabetes during COVID-191
Individualized target based treatment strategies2
Patient Category
BG Targets Management FPG 2h PG
Mildly ill Patients
4.4-6.1 mmol/L79.2-109.8 mg/dL
6.1-7.8 mmol/L109.8-140.4 mg/dL
Maintain Strict Glycemic Control
Moderately ill 6.1-7.8 mmol/L109.8-140.4 mg/dL
7.8-10.0 mmol/L140.4-180 mg/dL
Subcutaneous Insulin Delivery system
Critically Ill patients
7.8-10.0 mmol/L140.4-180 mg/dL
7.8-13.9 mmol/L140.4-250.2 mg/dL
IV Insulin Infusion

CORTICOSTEROID-INDUCED HYPERGLYCEMIA• Steroids are the main cause of drug-induced hyperglycemia.
• Patients with known diabetes à exacerbate hyperglycemia
• Patients without documented hyperglycemia before the initiation of glucocorticoids (GC) therapy à cause DM , with an incidence that can reach up to 46% of patients, and increases in glucose levels up to 68% compared to baseline.
• Precipitate acute complications à nonketotic hyperosmolar state, and diabetic ketoacidosis.
• Patophysiology: Increase in insulin resistance with increased glucose production and inhibition of the production and secretion of insulin by pancreatic β-cells
04/02/2021
Tamez-Pérez HE et al . Steroid hyperglycemia: A narrative review. World J Diabetes 2015 July 25; 6(8): 1073-1081

CONSENSUS RECOMMENDATIONS FOR COVID-19 AND METABOLIC DISEASE
DatePowerPoint Presentation
Bornstein, S.R., Rubino, F., Khunti, K., Mingrone, G., Hopkins, D., Birkenfeld, A.L., Boehm, B., Amiel, S., Holt, R.I., Skyler, J.S. and DeVries, J.H., 2020. Practical recommendations for the management of diabetes in patients with COVID-19. The lancet Diabetes & endocrinology.
Hypoglycemia (< 70 mg/dl)• Less than 4%• < 1% in frail and older people

Use of antidiabetic medications in patients with T2DM and COVID-19
S. Lim, J.H. Bae. Nat. Rev. Endocrinol. 17 (2021) 11–30,
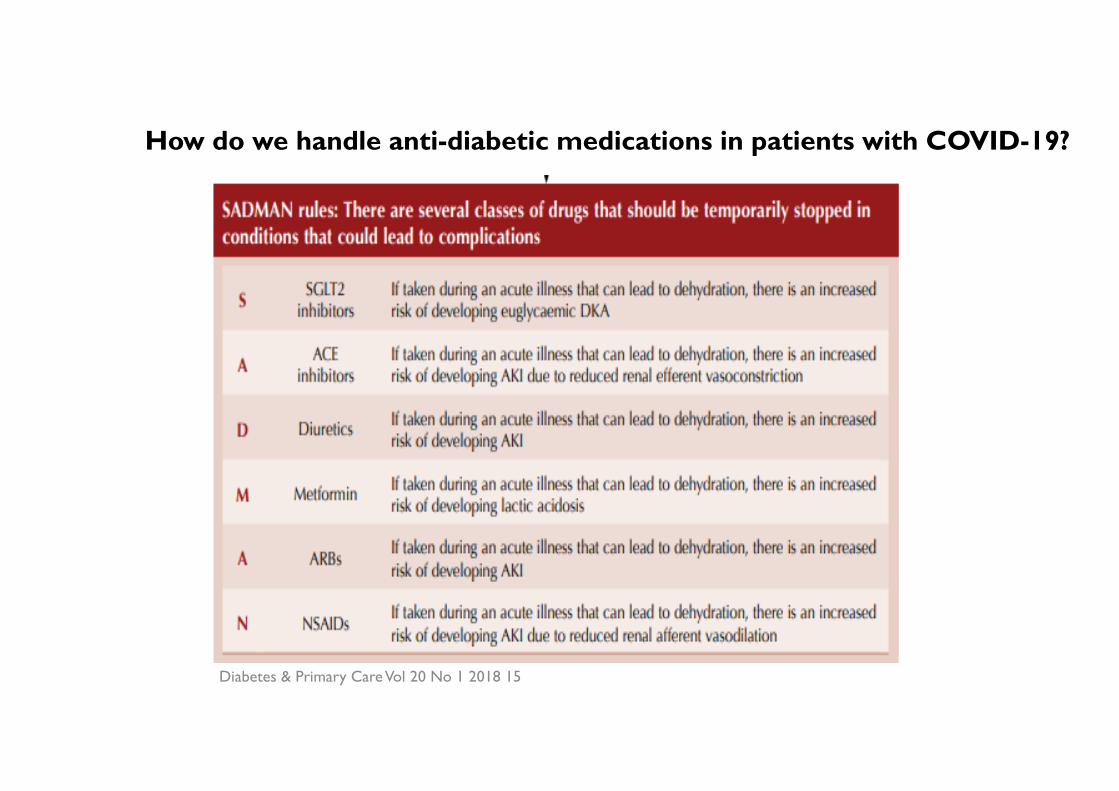
Diabetes & Primary Care Vol 20 No 1 2018 15
How do we handle anti-diabetic medications in patients with COVID-19?
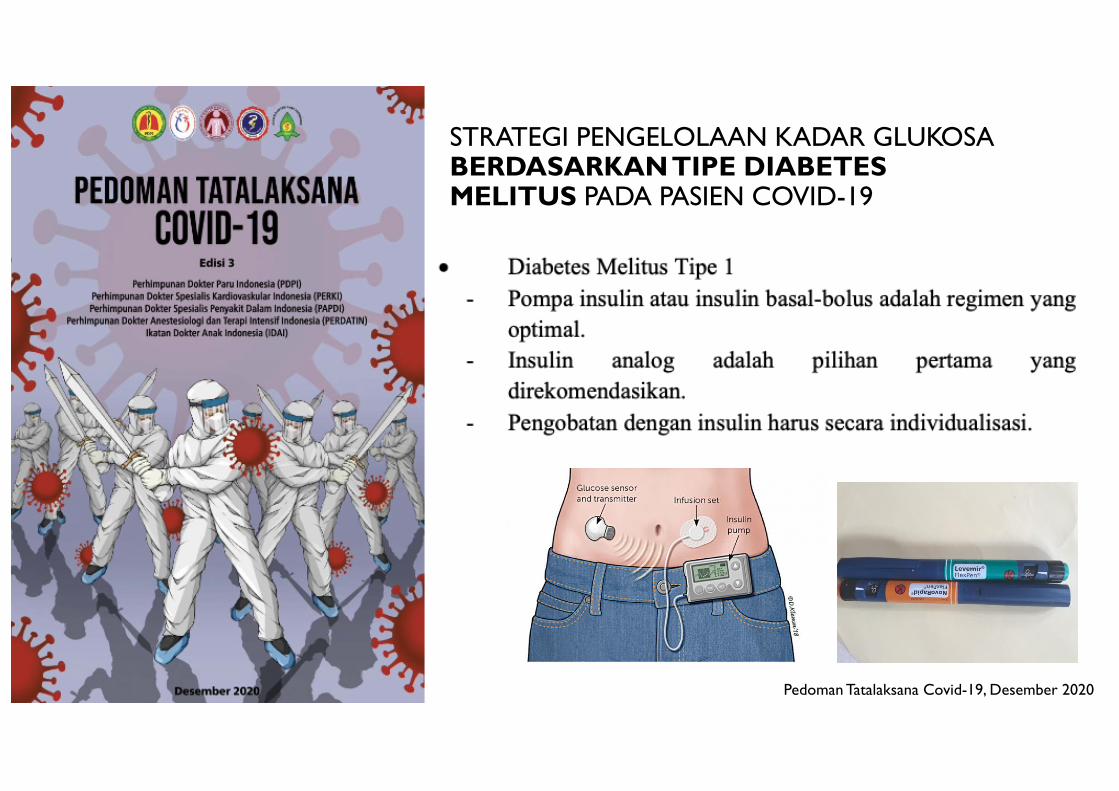
STRATEGI PENGELOLAAN KADAR GLUKOSABERDASARKANTIPE DIABETES MELITUS PADA PASIEN COVID-19
Pedoman Tatalaksana Covid-19, Desember 2020

STRATEGI PENGELOLAAN KADAR GLUKOSA BERDASARKAN TIPE DIABETES MELITUS PADA PASIEN COVID-19
Pedoman Tatalaksana Covid-19, Desember 2020
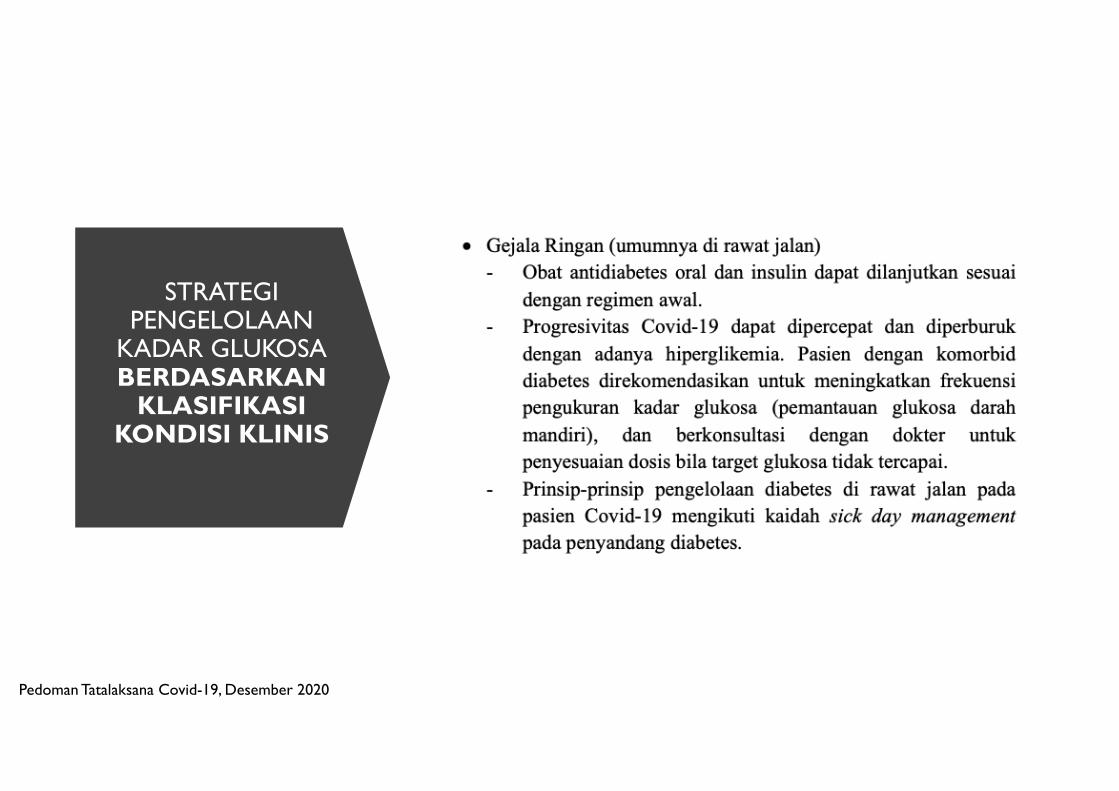
STRATEGI PENGELOLAAN
KADAR GLUKOSABERDASARKAN
KLASIFIKASIKONDISI KLINIS
Pedoman Tatalaksana Covid-19, Desember 2020
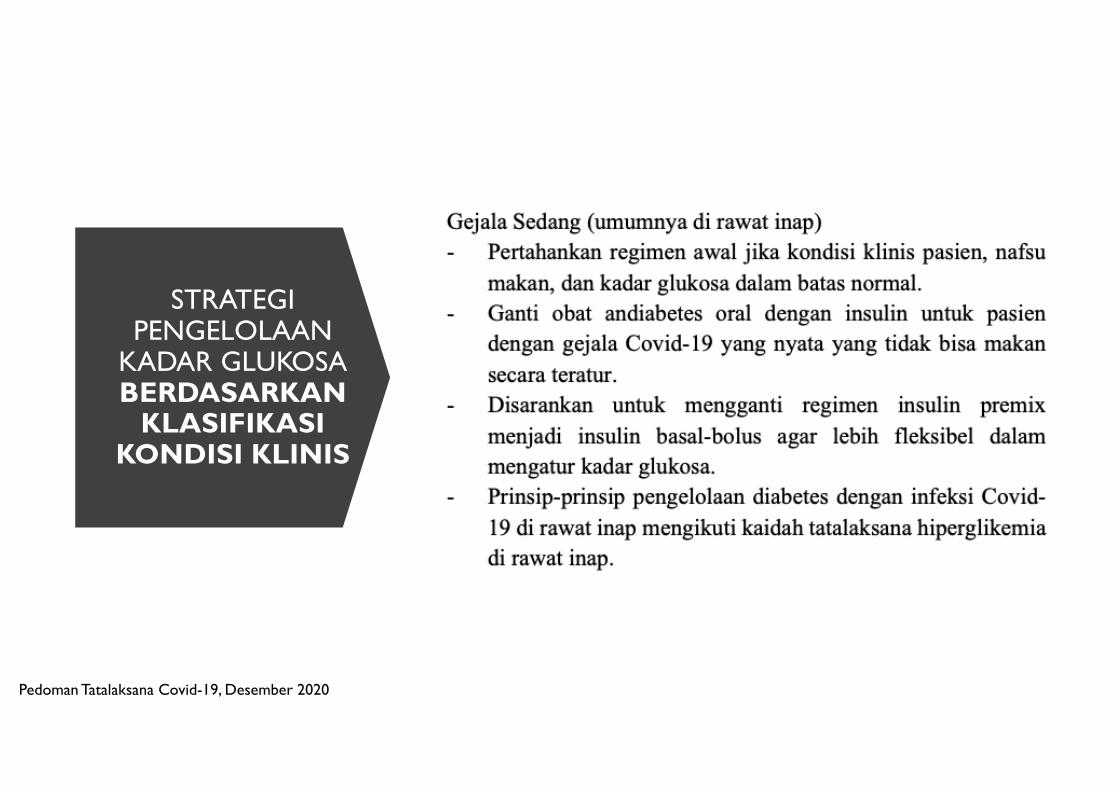
STRATEGI PENGELOLAAN
KADAR GLUKOSABERDASARKAN
KLASIFIKASIKONDISI KLINIS
Pedoman Tatalaksana Covid-19, Desember 2020
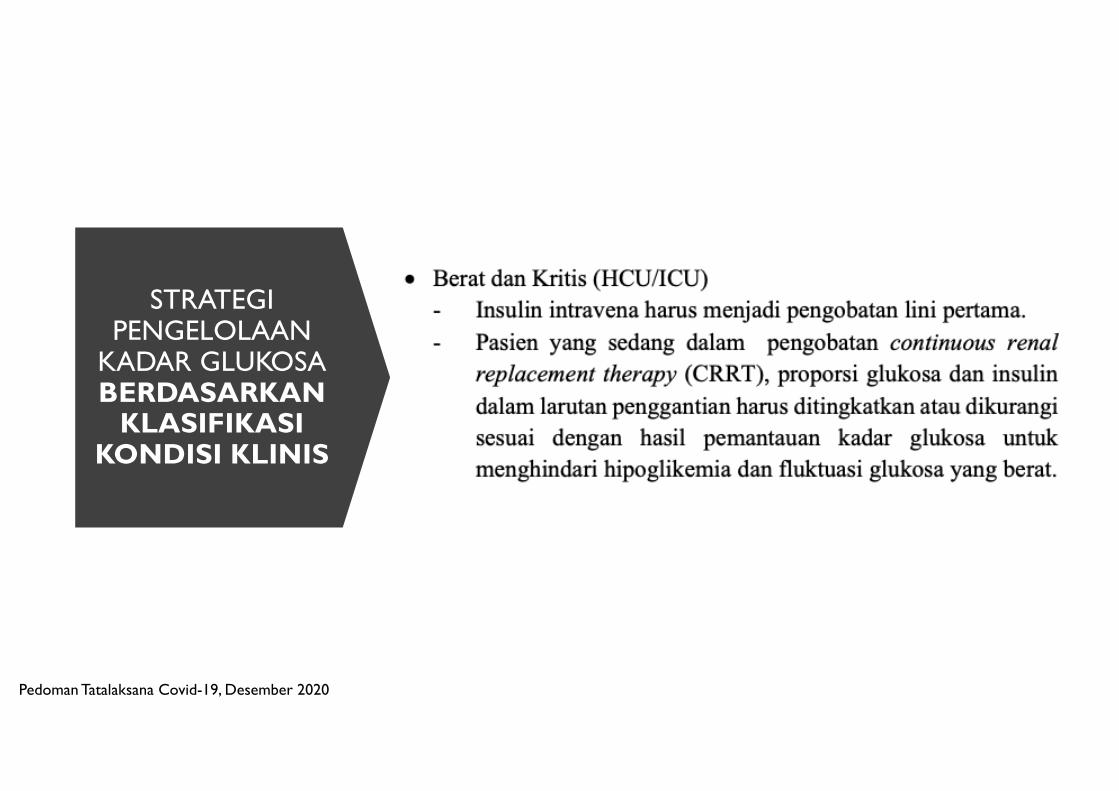
STRATEGI PENGELOLAAN
KADAR GLUKOSABERDASARKAN
KLASIFIKASIKONDISI KLINIS
Pedoman Tatalaksana Covid-19, Desember 2020

PRINSIPPENGELOLAANKADARGLUKOSA
Pedoman Tatalaksana Covid-19, Desember 2020

04/02/2021
41
JBDS-IP, 2014

DatePowerPoint Presentation
42

TREATMENT OF HYPERGLYCEMIA IN CRITICALLY ILL PATIENTS
• Continuous IV insulin infusion à the most effective method for achieving specific glycemic targets. Because of the very short half-life of circulating insulin, IV delivery allows rapid dosing adjustments to address alterations in the status of patients.
• IV insulin therapy à the glucose level should be maintained between 140 and 180 mg/dl (7.8 and 10.0 mmol/l).
• Transition to subcutaneously administered insulin à begin eating regular meals or are transferred to lower-intensity care.
• A percentage (usually 75– 80%) of the total daily IV infusion dose is proportionately divided into basal and prandial components & must be given 1– 4 h before discontinuation of IV insulin therapy in order to prevent hyperglycemia
AACE/ADA consensus on inpatient glycemic control. Diabetes Care 2009 Jun; 32(6): 1119-1131.
• In hospitalized patients, monitoring should start with capillary glucose determination from the start of steroid treatment.
• Since almost 94% of cases of hyperglycemia develop within 1-2 d of initiation of steroid therapy in the hospital setting, in nondiabetic patients who maintain glucose levels < 140 mg/dL without insulin requirements for 24-48 h, glycemic monitoring can be discontinued.
• in patients with glucose levels > 140 mg/dL with persistent insulin requirements, a basal/ bolus subcutaneous insulin scheme must be established.
• in patients with severe and/or persistent hyperglycemia despite the subcutaneous scheme, insulin by infusion pump should be started.
04/02/2021
MANAGEMENT OF CORTICOSTEROID-INDUCED HYPERGLYCEMIA
Tamez-Pérez HE et al . Steroid hyperglycemia: A narrative review. World J Diabetes 2015 July 25; 6(8): 1073-1081

CLINICAL SITUATIONS THAT INCREASE THE RISK FOR HYPOGLYCEMIA AND HYPERGLYCEMIA IN THE HOSPITAL INCLUDE THE FOLLOWING:
1. Changes in caloric or carbohydrate intake (“nothing by mouth” status, enteral nutrition, or parenteral nutrition)
2. Change in clinical status or medications (for example, corticosteroids or vasopressors)
3. Failure of the clinician to make adjustments to glycemic therapy based on daily BG patterns
4. Prolonged use of SSI (Sliding Scale Insulin) as monotherapy
5. Poor coordination of BG testing and administration of insulin with meals
6. Poor communication during times of patient transfer to different care teams
7. Use of long-acting sulfonylureas in elderly patients and those with kidney or liver insufficiency
8. Errors in order writing and transcription
AACE/ADA consensus on inpatient glycemic control. Diabetes Care 2009 Jun; 32(6): 1119-1131.

BG MONITORING
• Bedside BG monitoring with use of pointof-care (POC) glucose meters is performed before meals and at bedtime in most inpatients who are eating usual meals.
• In patients who are receiving continuous enteral or parenteral nutrition, glucose monitoring is optimally performed every 4 – 6 h.
• In patients who are receiving cycled enteral nutrition or parenteral nutrition, the schedule for glucose monitoring can be individualized but should be frequent enough to detect hyperglycemia during feedings and the risk of hypoglycemia when feedings are interrupted
• More frequent BG testing, ranging from every 30 min to every 2 h, is required for patients receiving IV insulin infusions.
AACE/ADA consensus on inpatient glycemic control. Diabetes Care 2009 Jun; 32(6): 1119-1131.

About COVID-19
Link between COVID-19
and Diabetes
Preventionand
Treatment
Summary
OUTLINE
PowerPoint Presentation Date 47

CONCLUSIONS
üUnderlying diabetes mellitus risk factors for increased coronavirus disease 2019(COVID-19) disease severity and worse outcomes, including higher mortality.
üPotential pathogenetic links between COVID-19 and diabetes mellitus includeeffects on glucose homeostasis, inflammation, altered immune status andactivation of the renin–angiotensin–aldosterone system (RAAS).
üDuring the COVID-19 pandemic, tight control of glucose levels and prevention ofdiabetes complications might be crucial in patients with diabetes mellitus to keepsusceptibility low and to prevent severe courses of COVID-19.
üTarget stratification of glucose management depends the disease severity& improvement

LESSON LEARNED
• DM is the bad prognostic outcome
• Diabetes is one of the high risk groups for developing severe illness from COVID-19
• Intensive Insulin glucose regulation
• Strictly glucose monitoring (CGM/FGM)
• Needs continuously of management improvement
04/02/2021
49

DatePowerPoint Presentation
50
THANK YOU