developmental aspects of kangaroo care
TRANSCRIPT

c I, I N I c A I, I s s u E: s
Developmental Aspects of Kangaroo Care
Susan M. Ludington-Hoe, CNM, PhD, FAAN Joan Y. Swinth, RNC, BSN
Kangaroo care (skin-to-skin holding) is an intervention that meets development care criteria by fostering neurobehavioral development. The five dimensions of neurobehavioral development are autonomic, motor, state, attention/interaction, and self-regulation. Kangaroo care promotes stability of heart and respiratory function, minimizes purposeless movements, improves behavioral state profiles, offers maternal proximity for attention/interaction episodes, and permits self-regulatory behavior expression. Kangaroo care satisfies in part the handling, self-consoling/soothing, nonnutritive sucking, and parenting interventions recommended by the National Association of Neonatal Nurses’ Infant and FamilyCentered Developmental Care Gutdelines. JOGNN, 25,691-703; 1996.
angaroo care (KC) is a synonym for skin-to-skin K ontact in which the preterm infant, wearing only a diaper, is placed upright, chest-to-chest with hidher parent. The emergence of KC (Martinez, Rey, & Marquette, 1992; Whitelaw & Sleath, 1985) and its use in developed and developing countries (Davanzo, 1993; Levin, 1994; Charpak, Ruiz-Pelaez, & Charpak, 1994) have prompted the use of a classification system that is based on how soon after birth KC is begun (Anderson, Marks, & Wahlberg, 1986). The classification system is as follows: birth, very early, early, intermediate, or late. Extensive testing with mothers (Anderson, 1991) and fathers (Ludington-Hoe, Hashemi, Argote, Medellin, & Rey, 1992) and each classification has been reported (Anderson, 1991, 1995, in press); the results of this testing provide empirical data of KC’s contribution
ronmental events, known as neurobehavioral organiza- tion. The five dimensions of neurobehavioral organiza- tion are: autonomic, motor, state, attention/interaction, and self-regulatory (Als, 1986). For each dimension the goal is an “organized” infant, one who responds to envi- ronmental demands without disruption in physiologic and behavioral responses. “When developmentally sup- portive care is administered, the infant’s growth develop- ment can be facilitated. This care allows for stabilization of physiologic and behavioral functioning” (National As- sociation of Neonatal Nurses, 1995, p. 2).
Kangaroo care studies and findings relating to each dimension of neurobehavioral organization are dis- cussed.
Autonomic Dimension of Neurobehavioral Organization
The autonomic dimension is the first in which the infant must gain control. Preterm infants respond to environ- mental stressors with a wide variation in physiologic pa- rameters. For example, if an alarm sounds, the infant’s heart and respiratory rates change, oxygen saturation lev- els drop, and color goes from pink to gray. This response reflects physiologic instability, with parameters slowly re- turning to baseline. Older, healthier infants demonstrate greater autonomic stability with less vacillation in basic physiologic functions. An autonomically organized in- fant is one who maintains autonomic stability in the pres- ence of environmental disturbances.
as a developmental care intervention.
tween KC and developmental care using Als’ (1986) neu- robehavioral framework. The article concludes with ex- amples of how KC is an intervention for modifying the environment, individualizing care to the infant, and pro- moting closeness and confidence in the parents.
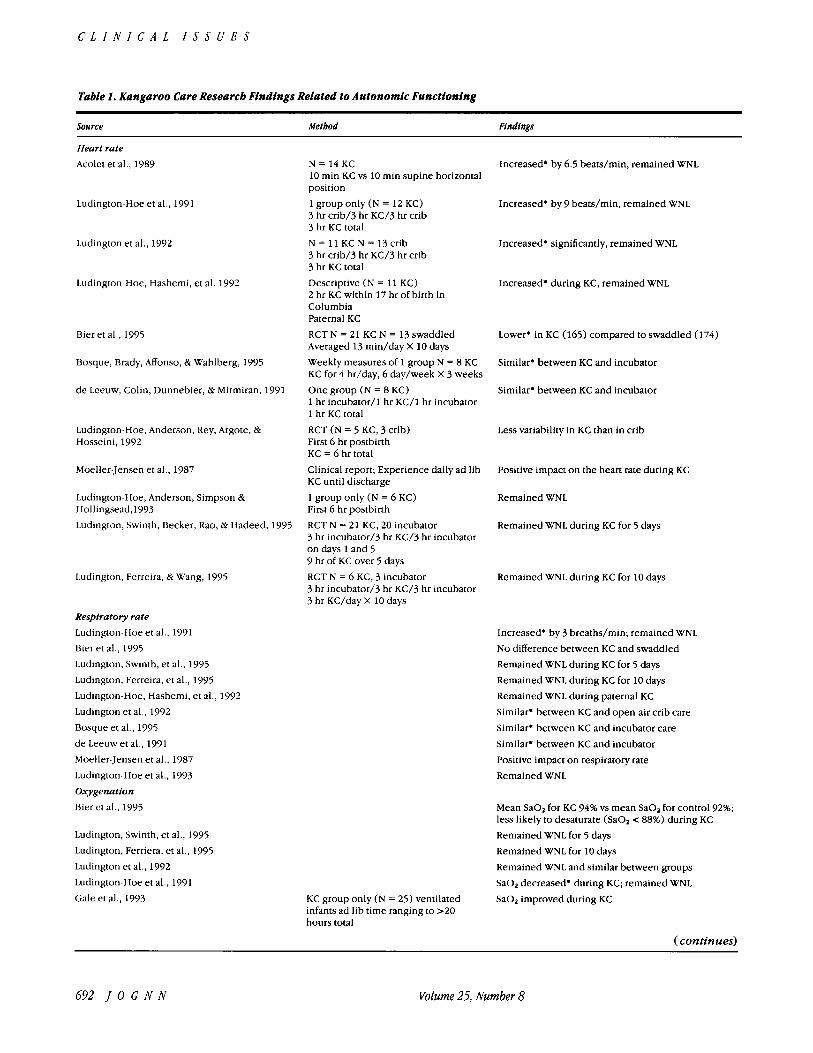
This article discusses the research-based linkages be- Relationsb@ Between Kc and Autonomic Kangaroo care has been found to provide a milieu that supports autonomic stability and fosters improvement in basic physiologic functions (Table 1). Clearly, when im- plemented in the selected populations tested to date, KC promotes cardiorespiratory stabilization, as shown by de- creased variation in heart and respiratory rates (Fig. l),
Neurobehavioral Organization improved oxygenation, less bradycardia, fewer and shorter apneic episodes, and fewer episodes of periodic
The goal of developmental care is to support and pro- mote the premature infant’s adaptability to external envi-
breathing. “Events such as apnea and bradycardia can trigger or involve associated changes in cerebral autoreg-
October 1996 J O G N N 631
C L I N I C A L I S S U E S
Table 1. Kangaroo Care Research Findings Related to Autonomic Functioning
Source Metbod Findings
Heart rate Acolet et al., 1989
Ludington-Hoe et al., 1991
Ludington et al., 1992
Ludington-Hoe, Hashemi, et al. 1992
Bieret al., 1995
Bosque, Brady, Atfonso, L Wahlberg, 1995
d e Leeuw, Colin, Dunnebier, L Mirmiran, 1991
Ludington-Hoe. Anderson, Rey, Argote, L Hosseini. 1992
Moeller-Jensen et al., 1987
Ludington-Hoe, Anderson, Simpson Lk Hollingsead,1993 Ludington, Swinth, Becker, Rao, L Hadeed, 1995
Ludington, Ferreira. L Wang, 1995
Respiratoty rate Ludington-Hoe et al., 1991 Bier et al., 1995 Ludington, Swinth, et al., 1995 Ludington, Ferreira. et al., 1995 Ludington-Hoe, Hashemi, et al., 1992 Ludington et al., 1992 Bosque et al., 1995 de Leeuw et al., 1991 Moeller-Jensen et al., 1987 Ludington-Hoe et al.. 1993 Oxygenation Bier et al., 1995
Ludington, Swinth, et al., 1995 Ludington, Ferriera, et al., 1995 Ludington et al., 1992 Ludington-Hoe et al., 1991 Gale et al., 1993
N = 1 4 K C 10 min KC vs 10 min supine horizontal position
1 group only (N = 12 KC) 3 hr crib/3 hr KC/3 hr crib 3 hr KC total N = 11 KC N = 13 crib 3 hr crib/3 hr KC/3 hr crib 3 hr KC total Descriptive (N = 11 KC) 2 hr KC within 17 hr of birth in Columbia Paternal KC RCT N = 21 KC N = 13 swaddled Averaged 13 m i d d a y X 10 days Weekly measures of 1 group N = 8 KC KC for 4 hr/day, 6 day/week X 3 weeks One group (N = 8 KC) 1 hr incubator/l hr KC/l hr incubator 1 hr KC total
RCT (N = 5 KC, 3 crib) First 6 hr postbirth KC = 6 hr total Clinical report; Experience daily ad lib KC until discharge 1 group only (N = 6 KC) First 6 hr postbirth RCT N = 21 KC, 20 incubator 3 hr incubator/3 hr KC/3 hr incubator on days 1 and 5 9 hr of KC over 5 days RCT N = 6 KC, 3 incubator 3 hr incubator/3 hr KC/3 hr incubator 3 hr KC/day X 10 days
Increased' by 6.5 beats/min, remained WNL
Increased. by 9 beats/min, remained WNL
Increased. significantly, remained WNL
Increased* during KC, remained WNL
Lower. in KC (165) compared to swaddled (174)
Similar. between KC and incubator
Similar. between KC and incubator
Less variability in KC than in crib
Positive impact on the heart rate during KC
Remained WNL
Remained WNL during KC for 5 days
Remained WNL during KC for 10 days
Increased. by 3 breaths/min; remained WNL N o difference between KC and swaddled Remained WNL during KC for 5 days Remained WNL during KC for 10 days Remained WNL during paternal KC
Similar. between KC and open-air crib care Similar' between KC and incubator care Similar' between KC and incubator Positive impact on respiratory rate Remained WNL
Mean Sa02 for KC 94% vs mean SaO, for control 92%; less likely to desaturate (SaO, < 88%) during KC Remained WNL for 5 days Remained WNL for 10 days Remained WNL and similar between groups SaO, decreased. during KC; remained WNL Sa02 improved during KC KC group only (N = 25) ventilated
infants ad lib time ranging to >20 hours total
(continues)
692 J O G N N Volume 25, Number 8

Developmentally Based Care
Table 1 (continued). Kangaroo Care Researcb Findings Related to Autonomic Functioning
Source Metbod Findings
Acolet et al., 1989 Ludington-Hoe, Hashemi, et al., 1992 de Leeuw et al., 1991 Bosque et al., 1995 Ilamelin & Ramachandran, 1993 Lutlington-Hoe et al., 1993
Luclington-Hoe et al., 1993 Ludington-Hoe et al., 1993; Ludington-Hoe, Anderson, et al., 1992
Apnea Whitelaw, 1986
Acolet et al., 1989 de Leeuw et al., 1991
Ludington, Swinth, et al., 1995
Ludington, Swinth, et al., 1995 Hadeed, Ludington, Ilr Siege], 1995
Bosque et al., 1995 Hamelin Ilr Ramachandran, 1993 Ludington, Irwin, Swinth, Becker, Rao, & Hadeed, 1994 Ludington, Ferreira, et al., 1995
Bradycardia Acolet et al., 1989 Bosque et al., 1995 de Leeuw et al., 1991 Hamelin & Ramachandran, 1993 Periodic breathing Ludington, Ferreira, et al., 1995 Ludington, Irwin, et al., 1994 Temperature Moeller-Jensen et al., 1987 Mondlane, de Graca, & Ebrahim, 1989
Ludington-Hoe et al., 1991
Ludington et al., 1992 Ludington, Swinth, et al., 1995; Ludington-Hoe, Anderson, et al., 1992 Ludington, Ferreira, et al., 1995
Clinical report of experience with KC
Descriptive study, N = 20 KC Maternal/paternal KC to 3 hr/ day beginning as early as 3 days of age
RCT; N = 20 KC, 21 incubator 3 hr incubator/3 hr KC/3 hr incubator 9 hr KC for 5 days
RCT; N = 15 KC, 13 incubator 3 hr incubator/3 hr KC/3 hr incubator
Descriptive (N = 132 KC) Two KC groups divided by start data ad lib KC until discharge
TcPO2 rose by 1.0 kPa during KC; no hypoxia Fluctuated little WNL during KC
Similar. TcPO2 between KC and incubator Similar. between KC and incubator O2 requirements stabilized or decreased. during KC
No hypoxia in KC even with audible expiratory grunting Stabilized in high 90s Resolution of mild respiratory distress with KC and hood O2 within 6 hrs of birth
No apnea during KC
No serious apnea during KC
Similar' number of apneic episodes > 10 secs plus similar total apnea time between the KC and control groups Sevenfold reduction in central apnea during KC on day 1 and day 5 @< 0.01); no change in central pattern for control infants Obstructive apnea rare occurrence Frequency and duration of apnea reduced during KC
Similar' between KC and incubator care Less frequent episodes during KC
Fewer central apneic spells and no obstructive apnea during KC
N o prolonged apnea during KC for 10 days
No serious bradycardia during KC Similar. between KC and incubator care Increased' insignificantly in 2 of 8 infants during KC
Less frequent episodes in KC
Present in both groups in all periods Fewer episodes during KC
Positive impact on temperature Warmed infants more than equipment after bath; KC at other than bath time maintained body temperature at higher level Increased. abdominal (abd) and rectal temperature
Temperature increased. significantly during KC
Increased. abdominal and toe temperature during KC
(36.6'-37.2' C)
Increased. abdominal and axillary temperature during KC plus abdominal and axillary temperatures the same Body temperature "well maintained"
(continues)
Whitelaw, 1986
October 199G J O G N N 693

C L I N I C A L I S S U E S
Table 1 (continued). Kangaroo Care Researcb Findings Related to Autonomic Functioning
Source Method Findings
Whitelaw, Heisterkamp, Sleath, Acolet, & Richards, 1988
RCT; N = 35 KC, 36 control Questionnaire at discharge and at 6 months of age W t < 1 , 5 0 0 g Avg. 36 min/day of KC
Maintain stable temperature WNL
Gale et al.. 1993 Acolet et al . . 1989 d e Leeuwet al. , 1991
U i e r e t al.. 1995
Hosque et al., 1988, 1995
kauer, [Jhrig, Sperling, & Versmold, 1995
Whitelaw & Sleath, 1985
Ludington-Hoe, Hashemi et al., 1992
I.udington-Hoe et al.. 1993
Johanson, Spencer, Rolfe.Jones. & Malla, 1992
M e t a b o l i c Kozin et al., 1995
O n e group only (N = 8 KC) 1 hr incubator/l hr KC/I hr incubator Clinical report of KC program in Bogota
KCT, 3 groups N = 98 KC N = 100 oil massage N = 99 plastic swaddle Data collected over 48 hr 22% LBW < 2,500 g
RCT (N = 144 KC, 133 incubator) Measures taken at randomization, 14 days later, and calculated term
Commonly increased' during KC Skin temperature stable, rising slightly Similar' and stable rectal temperature between KC and incubator periods Similar. body temperature between KC and swaddling Abdominal axilhry temperatures decreased' (36.8-C incubator; 36.5"C); remained WNI. N o cold stress (1 ' KC) as measured by abdominal/toe temperature gradient Temperature maintence excellent in very low-birth- weight infants Abdominal. toe, and tympanic temperature increased' during paternal KC; remained WNI. Abdominal and toe temperature increased to thermal neutral range by 56 mins of age Similar' rectal temperatures for each group
Hormonal maturation of thyroxine, TSH and 17-OHP not compromised by KC
*Similar/increase/decrease refers t o statistically significant group means. RCT: randomized control led trial; 17-OHP: 17-alpha-hydroxy-progesterone; TSH: thyroid stimulating hormone; WNL: within normal,
clinically acceptable limits.
ulation of blood flow, intracranial pressure, cerebral oxy- genation, and carbon dioxide tension, putting infants with these events at risk for postnatal intraventricular hemorrhage or infarctions" (Gorski, Huntington, & Lew- kowitz, 1990, p. 11 1). Metabolic enhancement and stabi- lization also have been noted in infants receiving KC.
Results of KC research provide confirmation that KC also prevents body heat loss and is associated with main- tained or increased body warmth throughout the duration of KC. These findings are not surprising because the mother's and father's skin temperatures are not only ade- quate to conduct body heat to the infant (Ludington,
Thompson, & Swinth, 1992; Ludington-Hoe, Hadeed, 62 Anderson, 1991; Ludington-Hoe, Thompson, Swinth, Hadeed, & Anderson, 1994) but also become warmer to conduct heat. With infants weighing less than 1,000 g, one may want to monitor the infant's temperature. The warming that is seen with KC induces sleep, thus assist- ing with state stability.
Motor Dimension of Neurobehavioral Organization
The motor system includes behaviors associated with muscle tone, posture, and generalized body movements
Figure I . PCG strip illuslrating cardiorespiratory slabilicy during KC.
694 J O C N N
Kangaroo care has been found to provide a milieu that supports autonomic stability
and fosters improvement in basic physiologic functions.
Volume 25, Number 8

Developmentally Based Care
(Als, 1986). The younger an infant’s gestational age, the less control over purposeless movements she or he has. When somatic or environmental changes are perceived by the infant, over-reaction of gross motor movements may occur. Arms flail, legs extend, the chest heaves, and the head turns from side-to-side. These purposeless movements consume precious oxygen and caloric sup- plies, limiting the nutrients available for recovery, repair, growth, and maturation. With increasing maturation, the motor response becomes less general and more specific, such as a simple grimace or flexion of the fingers. Ran- dom, disorganized body movements (twitches, tremors, extensor movements, jerks, and startles) are signs of mo- tor disorganization. Purposeful, focused, and flexor body movements characterize a motor organized infant (Als, 1986; Becker, Grunwald, Morrman, & Stuhr, 1993).
Motor activity is predominantly observed when the infant is awake. A sleeping preterm infant also will ex- hibit a large number of motor movements in any consec- utive 5 minutes, consuming as much as 40% more energy and additional oxygen to support this activity (Brooke, Alvear, & Arnold, 1979). The goal of developmental care is to minimize purposeless and energy-depleting move- ments and reduce the infant’s over-reaction to changes in the environment.
Relationskip Between KC and Motor Regulation The KC position has particular importance in motor reg- ulation because it involves the upright and contained posture of the infant and presents opportunities for relax- ation. Posture, a generic component of the motor dimen- sion, is altered by KC in such a way that respiratory and activity functions are improved. The outward recoil of an infant’s chest is inhibited when the infant lies supine. Once the infant is upright (60 degrees or more), the contents of the abdominal cavity shift away from the up- per abdomen, creating an increased negative subdi- aphragmatic pressure. This change in pressure favors out- ward recoil of the chest wall (Nichols & Rogers, 1987), which increases the efficiency of the diaphragm and pul- monary function. A change in position from supine to prone is associated with improvements in lung mechan- ics because this activates proprioceptors that respond to changes in rib position and tension applied across the joint space (Davis & Bureau, 1987). Oxygenation is im- proved because prone positioning supports the chest wall and allows gravitational forces to improve the venti- lation/perfusion ratio (Fox & Molesky, 1990).
In KC, the infant’s head is kept at a 60-degree upright angle, which allows for better pulmonary functional re- sidual capacity and easier breathing (Acolet, Sleath, & Whitelaw, 1989). Easier breathing reduces agitation and its accompanying jerky movements, two goals of devel- opmental care (Becker et al., 1993).
Extrauterine containment similar to in utero contain- ment effectively reduces random motor activity. In ma- ternal KC, containment is provided by enclosure be- tween maternal breasts, by being held in a flexed posi- tion, and by being covered by parents’ clothing or a blanket. Lipton, Steinschneider, and Richmond (1965)
concluded in their extensive review of more than 10 con- tainment experiments, each using a similar methodol- ogy, that containment evoked quiescence and decreased arousal.
Kangaroo care provides containment similar to in utero containment, thus
evoking quiescence, decreased arousal, and a significant increase in the amount
of quiet sleep.
Relaxation is a condition in which muscles become less tonic, and visible signs of tension disappear. During relaxation, respiratory muscles become less rigid, allow- ing the air to be more fully distributed throughout the lung and the chest wall to become more compliant. The respiratory system also exerts pressure that is the sum of the elastic, surface, and gravitational forces operating on the lung and chest wall, thus decreasing vital capacity (Agustoni & Hyatt, 1986). In addition, as a component of vital capacity, tidal volume can increase, with a resultant decrease in the inspiratory reserve volume (Hodgkin, 1984). Opportunities for infant relaxation should be en- couraged for optimizing physiologic organization.
Many evaluations of motor movements are subsumed in behavioral state assessments. For example, an active awake state is one in which the infant’s eyes are open and there is slow or moderately paced movement of one or more extremities. When activity is a component of the definition of a behavioral state, the effect of KC has been presented in this section, rather than in the section on the state dimension. Infants receiving KC usually are calm and relaxed-terms that imply quiescence of motor ac- tivity (Table 2).
State Dimension of Neurobebavioral Organization
“The state organization system involves the infant’s abil- ity to display, and to do so with clarity, the different ranges of state from sleep to the aroused state. This sys- tem is also associated with the infant’s ability to transition between states”(Nationa1 Association of Neonatal Nurses “ANN], 1995, p. 4). A state organized infant can make smooth transitions between appropriate states and bring into phase all of the physiologic and behavioral condi- tions to attain, sustain and withdraw from any given state. For the infant who is bombarded by ill-timed and inap- propriate stimulation in the neonatal intensive care unit (NICU), the most developmentally appropriate state is one that enables him or her to shut out the noxious stim- uli. This respite comes with the quiet sleep state. How- ever, 60-70% of sleep time is active sleep in preterm in-
October 1996 J O G ” 695

C L I I V I L A L I J J U C J
Table 2. Kangaroo Care Researcb Findings Related to Motor Functioning
Source Method Findings
Activity level Syfrett, Anderson;Behnke, & Neu, 1993 “Outstanding neurobehavioral organization”
seen soon after birth Ludington-Hoe, et al., 1994
Ludington-Hoe, Hashemi, et al., 1992 Ludington, 1990
Ludington et al., 1992
de Leeuw et al., 1991 Gale et al., 1993 Hamelin & Ramachandran, 1993 Tuomikoski-Koiranen, 1988
Ludington, Ferreira, et al., 1995 Anderson, 1995 Wahlberg, Person, & Monso, 1990
Relaxation Whitelaw & Sleath 1985 Anderson, 1989b
Ludington-Hoe, Hashemi, et al., 1992 Anderson, 1995, (in press) Whitelaw, 1986 Colonna, Uxa, de Graca, & de Vonderweld, 1990
RCT (N = 8 KC) 3 hr crib/3 hr KC/3 hr crib 3 hr KC total
Descriptive (N = 8 KC) 3 hr pretest/3 hr test/3 hr post- test 3 hr KC total
50% decrease. in all activity states
Infant inactive during paternal KC Significantly lower activity level
Significant increase* in % time in quiet regular sleep No difference in % time in active sleep during KC Infants < 1.2 kg “wriggly” after 15-20 mins of KC Infants rest peacefully during KC More calm, less active during KC 2 group on ad hoc basis
N = 8 KC, 8 control KC for 20-60 min/day or every other day X 18-20 days
Clinical and research review 2 group design N = 33 KC, 33 incubator Unlimited KC
Report of KC practices in Western Europe
Review of KC research
KC group only (N = 100) Ad lib KC until discharge
Slept more during KC Some restless infants become quieter in KC Significantly less active during KC
Occurred during KC Look of total relaxtion is seen
*Similar/increase/decrease refers to statistically significant group means. RCT: randomized controlled trial; WNL: within normal, clinically acceptable limits.
Appear comfortable and contented Stress-free expression during KC Relaxed against the mother “Astonishing maturation, tone, reactivity and spontaneous motor movements with KC”
fants (High & Gorski, 1985; Holditch-Davis, 1990). Inter- ventions that decrease active sleep and maximize quiet sleep are needed to protect the infant from environmen- tal stimulants and foster motor control (Yecco, 1993).
When noxious stimuli are present, arousal and dis- tress cues, such as crying, are developmentally appropri- ate for short periods only. Crying, the highest behavior state, is a detrimental state for any infant because it im- pairs lung functioning, jeopardizes closure of the fora- men ovale, increases intracranial pressures, and initiates a cascade of stress reactions within the infant (Anderson, 1989a). Throughout the infant’s hospital stay, all distress cues should be minimized by vigilant observation and timely intervention to remove the source of discomfort and stress.
Alertness is the state from which attention and in- teraction capacities emerge. Alertness is fleeting in pre- term infants because of visual cortical and central ner- vous system immaturity. Alertness increases with matura- tion; at 38 weeks’ postconceptional age, the infant can maintain alertness for several minutes, but attentiveness lasts only 2.5-4.0 seconds (Miranda, 1970).
Many diagnostic tools exist for determining the in- fant’s state. These tools are electrophysiologic (such as electroencephalographic, electro-oculographic, and electromyographic) , parental report, or behavioral state scales. Behavioral state scales and scoring systems are widely used because of their relative ease in administra- tion, but the scales differ in the number of states they are able to discriminate. Several enumerate only six states
696 J O G N N Volume 25, Number 8

Developmentally Based Care
Table 3. Kangaroo Care Research Findings Related to State Functioning
Source Method Findings
Sleep Ludington-Hoe et al., 1994 Ludington-Hoe, Anderson, et al., 1992 Ludington, 1990 Ludington-Hoe, Hashemi, et al., 1992 de Leeuw et al., 1991 Bosque et al., 1995 Tuomikoski-Koiranen, 1990
Crying Ludington, 1990; Whitelaw, 1986 Whitelaw et al., 1988 Ludington-Hoe, Hashemi, et al., 1992 de Leeuw et al., 1991
2.5-fold increase; in quiet regular sleep Increase in frequency of quiet sleep Duration of sleep bouts 2 times longer 65% time in quiet regular sleep No difference in % sleep time between KC and pre and post-test periods Lower % total sleep (47% vs 64%) during KC than incubator Less alert than control infants because KC infants were 29 weeks gestational age and control infants were 32 weeks gestatinoal age
Virtually nonexistent in KC Less at 6 months after discharge (p = 0.0422) Occurred infrequently None observed during KC
* Similar/increase/decrease refers to statistically significant group means. RCT: randomized controlled trial; WNL: within normal, clinically acceptable limits.
(deep sleep, light sleep, drowsy, awake, active, crying) (Wolff, 1959); others include an “indiscriminate” state to accommodate infant behaviors that do not fit the qualifi- ers of other states (Thoman, 1990). Anderson’s scoring system (Gill, Behnke, Conlon, & Anderson, 1992) is sufficiently detailed to be comprehensive and sensitive enough to discriminate all possible states.
Relationsbip Between KC and State Regulation The relationship of KC to infant state has been studied by many researchers using many different scientific methods (Table 3), including the stringent randomized controlled trial approach. The Anderson Behavioral State Score re- sults show that KC reduces the amount of time the infant spends in active sleep with a concomitant increase in the amount of time spent in quiet, regular sleep (Ludington, 1990). The predominant sleep state during KC, as deter- mined by the observational method, is deep, quiet, regu- lar respiration sleep. The preeminence of quiet regular sleep during KC has been documented in infants younger than 32 weeks postconceptional age, the age at which quiet regular sleep is purported to appear (Yecco, 1993). Alertness, although brief in most infants, has been seen during KC, especially after many sessions conducted dur- inga week or more (Anderson, 1989b) (Fig. 2). Kangaroo care also is accomparlied by a clinically and statistically significant reduction in crying (Moeller-Jensen, Hjort- Gregersen, Mattiessen, Vestergaard, & Jepsen, 1991).
Attention/lnteraction Dimension of Neurobehavioral Organization
Once alertness has been achieved, the infant may be able to focus his or her cognitive skills on attentive-
Figure 2. Alertnessduring KCin a 745-g, 26-weekgestationalageinfantat 17days ofage. The infant is receiving KC while on ventilation.
October 1996 J O G N N 697
C L I N I C A L I S S U E S
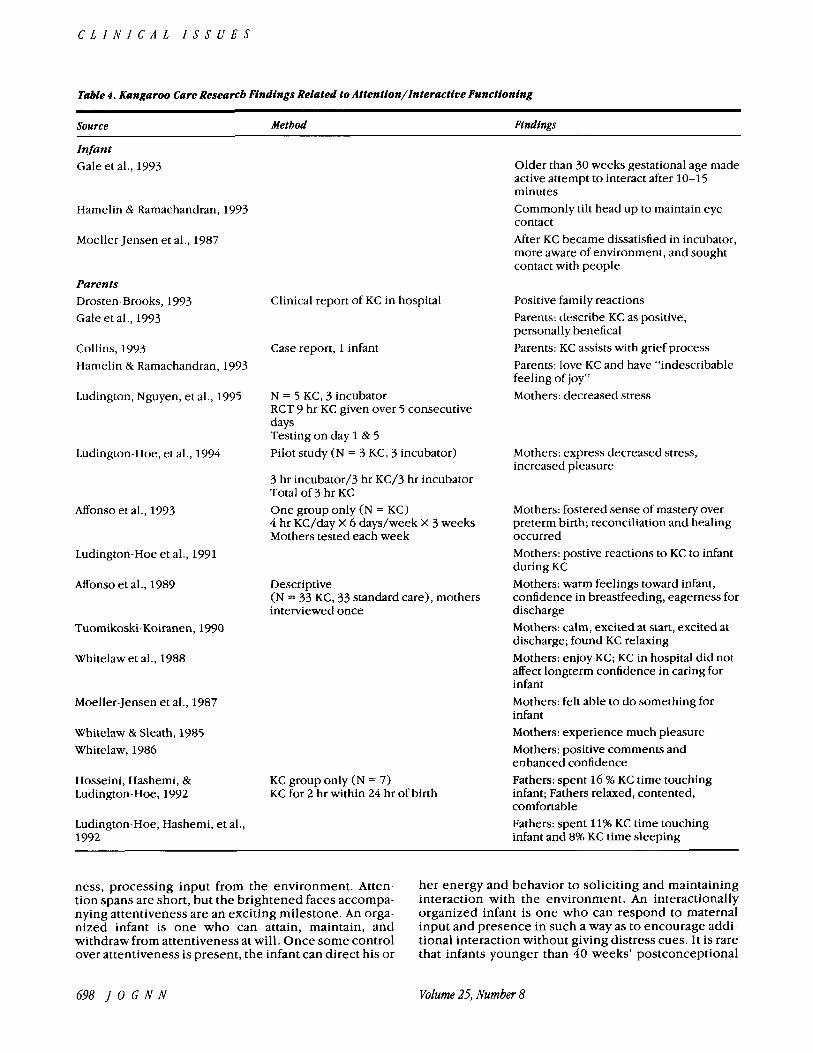
Table 4. Kangaroo Care Research Findings Related to Attention/lnteractive Functioning
Source Method Findtngs
Infant Gale et al., 1993
Hamelin & Ramachandran, 1993
Moeller-Jensen et al., 1987
Parents Drosten-Brooks, 1993 Gale et al., 1993
Collins, 1993 Hamelin & Ramachandran, 1993
Ludington, Nguyen, et al., 1995
Ludington-Hoe, et al., 1994
Monso et al., 1993
Ludington-Hoe et al., 1991
Monso et al., 1989
Tuomikoski-Koiranen, 1990
Whitelaw et al., 1988
Moeller-Jensen et al., 1987
Whitelaw & Sleath, 1985 Whitelaw, 1986
Hosseini, Hashemi, & Ludington-Hoe, 1992
Ludington-Hoe, Hashemi, et al., 1992
Clinical report of KC in hospital
Case report, 1 infant
N = 5 KC, 3 incubator RCT 9 hr KC given over 5 consecutive days Testing on day 1 & 5 Pilot study (N = 3 KC, 3 incubator)
3 hr incubator/3 hr KC/3 hr incubator Total of 3 hr KC One group only (N = KC) 4 hr KC/day X 6 days/week X 3 weeks Mothers tested each week
Descriptive (N = 33 KC, 33 standard care), mothers interviewed once
KC group only (N = 7) KC for 2 hr within 24 hr of birth
Older than 30 weeks gestational age made active attempt to interact after 10-15 minutes Commonly tilt head up to maintain eye contact After KC became dissatisfied in incubator, more aware of environment, and sought contact with people
Positive family reactions Parents: describe KC as positive, personally benefical Parents: KC assists with grief process Parents: love KC and have “indescribable feeling of joy” Mothers: decreased stress
Mothers: express decreased stress, increased pleasure
Mothers: fostered sense of mastery over preterm birth; reconciliation and healing occurred Mothers: postive reactions to KC to infant during KC Mothers: warm feelings toward infant, confidence in breastfeeding, eagerness for discharge Mothers: calm, excited at start, excited at discharge; found KC relaxing Mothers: enjoy KC; KC in hospital did not affect longterm confidence in caring for infant Mothers: felt able to do something for infant Mothers: experience much pleasure Mothers: positive comments and enhanced confidence Fathers: spent 16 % KC time touching infant; Fathers relaxed, contented, comfortable Fathers: spent 11% KC time touching infant and 8% KC time sleeping
ness, processing input from the environment. Atten- tion spans are short, but the brightened faces accompa- nying attentiveness are an exciting milestone. An orga- nized infant is one who can attain, maintain, and withdraw from attentiveness at will. Once some control over attentiveness is present, the infant can direct his or
her energy and behavior to soliciting and maintaining interaction with the environment. An interactionally organized infant is one who can respond to maternal input and presence in such a way as to encourage addi- tional interaction without giving distress cues. It is rare that infants younger than 40 weeks’ postconceptional
698 J O G N N Volume 25, Number 8

Developmentally Based Care
age can demonstrate attentive and interactional organi- zation (Gorski, Davidson, & Brazelton, 1979). Relationship Between KC and Attention/lnteraction Functioning No studies have examined the effect of KC on infants’ at- tention and interactional capacities, but several reports of clinical observations made while KC was being imple- mented provide some indication of expected results (Ta- ble 4). Some infants have been observed extending their heads to get into the en-face position with the parent pro- viding KC, gazing intently at the parent, and maintaining the gaze for exceptional lengths of time (Gale, Franck, & Lund, 1993). Additional empirical investigations are needed but will be limited by the maturation and slow developmental progress of preterm infants.
Parental confidence in caregiving and sensitivity to the infant’s cues are enhanced
by kangaroo care.
True developmental care should encompass strate- gies to enhance the parent’s attention and interaction contributions. Parents are partners in the NICU, and nurs- ing’s task is to encourage the development of parenting skills, including caring for the infant (Baker, 1995). Hav- ing opportunities to hold their infant in the NICU gives parents a chance to learn about their infant’s state, behav- ioral cues, positioning, and how to provide developmen- tally appropriate care and feel more confident in the care they give. All of these areas have been identified as edu- cational needs of parents before the infant is discharged from the hospital (Robinson, 1995). Several studies of KC have examined these effects (Table 4). Maternal confi- dence and closeness to the infant are enhanced, as is res- olution of the grief process related to premature birth (Affonso, Bosque, Wahlberg, & Brady, 1993). Mothers commonly express relief and intense pleasure in being able to hold their infant close. Maternal comments reflect an awareness of infant behavior (“This is the first time I have heard him burp” and “My baby loves lying on my chest”) and signs of claiming (“Now I know that he is mine”) (Ludington-Hoe & Golant, 1993). Fathers have responded to KC with pleasure and willingness and dem- onstrated fathering behaviors similar to those manifested with swaddled infants (Ludington-Hoe et al., 1992). Fa- thers have not been tested for increased awareness of and sensitivity to the infant and his cues. Still, the data indi- cate that KC can facilitate maternal and paternal attentive- ness and offer opportunities for interaction with the pre- term infant.
SeVRegulatory Dimension of Neurobehavioral Organization The self-regulatory dimension is associated with the in- fant’s ability to achieve and maintain a balance of all neu-
robehavioral dimensions through use of self-consoling behaviors, such as sucking or hand-to-mouth maneuvers (Als, 1986). Investigations report that infants are relaxed and contented and usually fall asleep with KC, eliminat- ing the need for self-consoling behaviors (Table 2) . However, KC does have a role in promoting self-regula- tory abilities.
Relationskip Between KC and Self-Regulatory Functioning One self-regulatory behavior that is constantly available to the infant during maternal KC is on-demand suckling or breastfeeding. The impact of KC on breastfeeding has been well documented (Table 5). Whitelaw (1990, p. 605) summarized KC’s impact in his statement: “the maintenance of lactation by kangaroo care may be life saving for preterm infants with only a cot (or incubator) and milk formula as alternatives.”
Other Contributions of KC
Kangaroo care has been shown to decrease maternal stress levels. Ludington, Nguyen, and Swinth (1995) studied 14 mothers (10 using KC and 4 control subjects) to determine if 5 days of KC modified maternal stress re- lated to hospital stays of the premature infant. Stress was measured by the “Parental Stress Scale: Neonatal Inten- sive Care Unit” of Miles, Funk, and Carlson (1993). Re- sults showed significant reduction in stress related to “in- fant behavior and appearance” and “parental role alter- ation” in the mothers using KC. The “overall stress level” was significantly lower in the mothers using KC than in the control mothers on the fifth day of KC.
The effect of KC on painful routine nursing proce- dures has been studied (Ludington-Hoe, 1996). In a cross-over design, 12 healthy, preterm infants were ran- domly assigned to receive either 3 hours of incubator care, followed by 3 hours of KC, or the opposite. A heel- stick was performed during the last minute of both the incubator and KC periods. Voice-activated recordings and pain signs were monitored. Crying was significantly shorter (5-12 seconds) during KC than when the infants were in the incubator (22-45 seconds), and far fewer of the usual pain responses (usually only a change in facial expression accompanied by a slight cry) were observed in infants receiving KC (Ludington-Hoe, 1996) (Fig. 3). Four common signs of pain are facial expression compo- nents accompanying a slight cry; increased cry; grimac- ing; and leg/knee flexion (Evans & Vogelpohl, 1995). In Evans and Vogelpohl’s study, one-third of neonates dem- onstrated all four pain signs with skin puncture for heel- stick or the start of an intravenous line, and all neonates responded to painful procedures with grimacing and leg/knee flexion (Evans & Vogelpohl, 1995).
summary and implications
The NANN (1995) has published guidelines for develop- mental care. The review of the literature presented here indicates that KC is a strategy that will satisfactorily fulfill the role of many of these interventions, particularly (a)
October 1YYG J O G N N 699

C L I N I C A L I S S U E S
Table 5. Kangaroo Care Research Findings Related to Self-Regulatory Functioning
Source Method Findings
Gale et al., 1993
Wahlberg, Monso,bi Persson, 1992
Colonna et a]., 1990
Tuomikoski-Koiranen, 1990 Whitelaw et al., 1986
Syfrett et al . , 1993
Ludington-Hoe et al., 1993 Anderson (in press) Bier et al., 1995
Bier et al., 1995 Schmidt & Wittreich, 1986
Moeller-Jensen et a]., 1987
Hamelin & Ramachandran, 1993 Whitelaw, 1986
Increased’ breastfeeding at discharge but no increased milk production 82% KC vs 45% control mothers breastfeeding at discharge ( p = 0.005)
Successful lactation, no gavage feeds, limited use of formula supplements Increase; milk production and more infants breastfed only
Retrospective, comparative (N = 33 KC, 33 standard care): mdthers interviewed once
Mean duration lactation; KC = 9.2 weeks, control = 5.1 weeks (p = 0.0167) Breastfeeding after discharge; KC = average of 4.6 months, control = average of 2 months KC infants competent breastfeeders by 24 ’ after birth
7 of 13 control mothers stopped breastfeeding before discharge, compared with 1 of 21 KC mothers N o difference in milk production between the groups
RCT (12 KC, 11 incubator): KC ad Milk production: KC moms = 640 cc; incubator moms = lib every day until discharge; 400 cc testing throughout hospital stay
During breastfeeding, KC infants more awake, seeking and eager to suck than other infants Mothers experience milk letdown during KC
Mothers stated lactation better after KC
*Similar/increase/decrease refers to statistically significant group means. RCT: randomized controlled trial; WNL: within normal, clinically acceptable limits
handling, through containment, prone positioning, and gentle touch; (b) self-consoling/soothing, by nesting; (c) non-nutritive sucking opportunities, by providing ac- cess to the breast; (d) parenting, by involving parents in caregiving and having parents provide containment and
holding. The NANN guidelines suggest consideration of “skin-to-skin contact between the infant and parent” (1995, p. 11) when the infant is in medically stable con- dition. Gloppestad (1995) and others (Anderson, 1995; Davanzo, 1993; Drosten-Brooks, 1993; Gale et al., 1993; Wallace & Ridpath-Parker, 1993) recommend that KC be- gin even when the infant is not in medically stable condi- tion, such as during the use of a ventilator, although em- pirical validation of KC’s safety with infants receiving ventilation is unavailable (Ludington, Anderson, Swinth, Thompson, & Hadeed, 1994). Beginning KC while the infant is receiving ventilation can reduce the separation time (time from birth to first parent contact) by 66.8% (Gloppestad, 1995). The potential for KC to make contri- butions to neurobehavioral development is enhanced if the practice begins early.
The spreading acceptance and use of kangaroo care in- dicate that it is no longer a strategy to consider for tomorrow but one that can be applied today. Some units may sense future shock when urged to implement KC. Future shock, first defined by Alvin Toffler (1970), is the dizzying disori- entation brought on by the premature arrival of the future. However, there should be no future shock with KC; its roots are in the forces of naturalism and the foundations of devel- Figure 3. Performing beelstick blood draw during KC.
700 J O C N N Volume 25, Number 8

Developmentally Based Care
opmental care. Kangaroo care’s acceptance is attributable t o the positive clinical ou tcomes presented here.
Acknowledgments
This s tudy was s u p p o r t e d in part by National Inst i tute of Nursing Research (NINR) R01-02251-4 t o Susan M. Lud- ing ton-Hoe and a gift f rom Infant Care Specialists i n Ir- vine, California, and a grant i n loving memory of Anna by Black Marlin Product ions.
References
Acolet, D., Sleath, K., & Whitelaw, A. (1989). Oxygenation, heart rate, and temperature in very low birthweight infants during skin-to-skin contact with their mothers. Acta Pedi- atrica Scandinauica, 78, 189-193.
Affonso, D., Bosque, E. , Wahlberg, V., & Brady, J . (1993). Rec- onciliation and healing for mothers through skin-to-skin contact provided in an American tertiary level intensive care nursery. Neonatal Network, 12(3), 25-32.
Affonso, D., Wahlberg, V., & Persson, B. (1989). Exploration of mothers’ reactions to the kangaroo method of prematurity care. Neonatal Network, 7,43-51.
Agustoni, E. , & Hyatt, R. (1986). Infant respiratory physiology. In S. Geiger (Ed.), Handbook ofphysiology (pp. 113-130). Bethesda, MD: American Physiological Society.
Als, H. (1986). A synactive model of neonatal behavioral orga- nization: Framework for the assessment of neurobehavioral development in the premature infant and for support of in- fants and parents in the neonatal intensive care environ- ment. Physical C Occupational Therapy in Pediatrics, 6, 3-53.
Anderson, G. C. (1989a). Risk in mother-infant separation post- birth. Image: Journal ofNursing Scholarsbzp, 21(4), 196- 199.
Anderson, G. C. (1989b). Skin-to-skin: Kangaroo care in western Europe. American Journal of Nursing, 89,662-666.
Anderson, G . C. (1991). Current knowledge about skin-to-skin (kangaroo) care for preterm infants. Journal of Perinatol- ogy, 11(3), 216-226.
Anderson, G. C. (1995). Touch and the kangaroo care method. In T. Field (Ed.), Touch in early development (pp. 35-51). Mahwah, NJ: Earlbaum.
Anderson, G. C. (in press). Kangaroo care of the premature in- fant. In E. Goldson (Ed.), Nurturing thepremature infant: Developmental interventions in the neonatal intensive care nursery. New York: Oxford University Press.
Anderson, G. C., Marks, E. , & Wahlberg, V. (1986). Kangaroo care for premature infants. American Journal of Nursing,
Baker, J . G. (1995). Parents as partners in the NICU. Neonatal Network, 14(1), 9-10.
Bauer, K., Uhrig, C., Sperling, P., &Versmold, H. T. (1995). One hour of skin-to-skin care was no cold stress for VLBW in- fants, as oxygen consumption and central/peripheral tem- perature gradient did not increase. Pediatric Research, 37(4) Pt. 2 , 196A.
Becker, P. T., Grunwald, P. C., Morrman, J., & Stuhr, S. (1993). Effects of developmental care on behavioral organization in very-low-birth-weight infants. Nursing Research, 42,
Bier, J . A. B., Ferguson, A. E., Liebling, J . A., Morales, Y., Archer, D., Oh, W., 62 Bohr, B. (1995). Skin-to-skin contact im-
86,807-809.
214-220.
proves physiologic states of breast-fed low birthweight in- fants. Pediatric Research, 37(4) Pt. 2, 103A.
Bosque, E., Brady, J., Atfonso, D., & Wahlberg, V. (1988). Con- tinuous physiological measurements of kangaroo versus in- cubator care in a tertiary level nursery. Pediatric Research, 23,402A.
Bosque, E., Brady, J., Affonso, D., & Wahlberg, V. (1995). Physi- ologic measures of kangaroo versus incubator care in a ter- tiary level nursery. JOGNN, 24,219-228.
Brooke, 0. G.,Alvear, J., &Arnold, M. (1979). Energyretention, energy expenditure and growth in healthy immature in- fants. Pediatric Research, 13, 215-220.
Charpak, N., Ruiz-Pelaez, J. G . , & Charpak, Y. (1994). Rey-Mar- tinez kangaroo mother program: An alternative way of car- ing for low birth weight infants? One year mortality in a two-cohort study. Pediatrics, 94, 804-810.
Collins, S. (1993). Baby Stephanie: A case study in compassion- ate care. Neonatallntensiue Care, March/April, 47-49.
Colonna, F., Uxa, F., de Graca, A. M., & d e Vonderweld, U. (1990). The ‘kangaroo-mother’ method: Evaluation of an alternative model for the care of low birth weight newborns in developing countries. InternationalJournal of Gynecol- ogy and Obstetrics, 31, 335-339.
Davanzo, R. (1993). Care of the low birth weight infants with the kangaroo mother method in deueloping countries. Guide- lines for health workers. Trieste, Italy: Bureau for Interna- tional Cooperation in Maternal and Child Health, WHO Collaborating Centre for Maternal and Child Health, Insti- tuto per L’Infanzia.
Davis, G., & Bureau, M. (1987). Pulmonaryand chest wall me- chanics in the control of respiration in the newborn. Clinics in Perinatology, 14, 551-579.
de Leeuw, R., Colin, E. M., Dunnebier, E. A., & Mirmiran, M. (1991). Physiologic effects of kangaroo care in very small preterm infants. Biology of the Neonate, 59, 149-155.
Drosten-Brooks, F. (1993). Kangaroo care: Skin-to-skin contact in the NICU. MCN 18(5), 250-253.
Evans, J. C., & Vogelpohl, D. G. (1995). Behavioral manifesta- tions of ‘pain’ associated with routine caregiving [abstract]. In Proceedings of the Seattle InternationalCIinical Update and Research Symposium of the National Association of Neonatal Nurses (p. 34). Petaluma, CA: National Associa- tion of Neonatal Nurses.
Fox, M., & Molesky, M. 1990 Effects of prone and supine posi- tion on arterial oxygen pressure. Neonatal Network, 8(4),
Gale, G., Franck, L., & Lund, C. (1993). Skin-to-skin (kangaroo) holding of the intubated premature infant. Neonatal Net- work, 12(6), 49-57.
Gill, N. E., Behnke, M., Conlon, M., &Anderson, G. C. (1992). Nonnutritive sucking modulates behavioral state for pre- term infants before feeding. Scandinavian Journal of Car- ing Science, 6( l ) , 3-7.
Gloppestad, K. (1995). Initial separation time between fathers and their premature infants: Comparison between two pe- riods of time. VardINorden, 15(2), 10-17.
Gorski, P., Huntington, L., & Lewkowitz, D. (1990). Handling preterm infants in hospitals. Clinics in Perinatology, 17,
Gorski, P., Davidson, M. S., & Brazelton, T. B. (1979). Stages of behavioral organization in the high risk neonate: Theoreti- cal and clinical considerations. Seminars in Perinatology, 3(1), 61-72.
Hadeed, A, , Ludington, S., & Siegel, S. (1995). Skin-to-skin con- tact (SSC) between mother and infant reduces idiopathic
25-29.
103-112.
October 1PPG J O C N N 701

C L I N I C A L I S S U E S
apnea of prematurity. Pediatric Research, .37(4) Pt. 2, 208A.
Hamelin, K., & Ramachandran, C. (1993). Kangaroo care. Cana- dian Nurse, 8(6), 15-17.
High, P., & Gorski, P. (1985). Recording environmental influ- ences on infmt development in the intensive care nursery: Womb for improvement. In A. W. Gottfried & J . L. Gaiter (Eds.), Infant stress under intensive care: Environmental neonatology (pp. 131-155). Baltimore: University Park Press.
Hodgkin, J . E. (1984). Routine pulmonary function tests. In G. C. Burton & J . E. Hodgkin (Eds.), Respiratorycare: Aguide to clinicalpractice, 2nd ed. (pp. 231-239). Philadelphia: J . B. Lippincott.
Ilolditch-Davis, D. (1990). The development of sleeping and waking states in high-risk preterm infants. Infant Behavior I; Development, 1.3, 513-531.
Hosseini, R., Hashemi, M., & Ludington-Hoe, S. M . (1992). Pre- term infants and fathers: Physiologic and behavioral effects o f skin-to-skin contact. Ursus Medicus, 2, 47-55.
Johanson, R. B., Spencer, S. A,, Rolfe, P., Jones, P., & Malla, D. S. (1992). Effect of post-delivery care on neonatal body tem- perature. Acta Pediatrica, 81, 859-863.
Levin, A. (1994). The mother-infant unit at Talinn Children’s Hospital, Estonia: A truly baby-friendly unit. Birth, 21(1), 39-44.
Lipton, E. , Steinschneider, A., & Richmond, J . (1965). Swad- dling, a child care practice: Historical and experimental ob- servations. Pediatrics, 35, 521-567.
Ludington, S. M. (1990). Energy conservation during skin-to- skin contact between preterm infants and their mothers. HeartandLung 1 9 ( 5 ) Pt. 1,445-451.
I.udington, S. M . , Anderson, G. C., Swinth, J., Thompson, C., 62 Hadeed, A. J . (1994). Kangaroo care. Neonatal Network, 13(4), 61-62.
Ludington, S. M., Ferreira, C., & Wang, J. I . J . (1995). Prelimi- nary cardiorespiratory, thermal, and behavioral outcomes for 10 days of skin-to-skin contact for incubator care prema- ture infants. In Proceedings of the International Clinical Update and Research Symposium of the National Associa- tion ofNeonatalNurses (p. 93). Petaluma, CA: NANN.
Ludington, S. M., Irwin, S., Swinth, J . , Becker, J., Rao, S., & Hadeed, A. J . (1994). Skin contact and breathing in pre- terms. Respiratory Care, 39, 1060.
Ludington, S. M., Nguyen, N., & Swinth, J . (1995). Kangaroo care minimizes maternal stress. In Proceedings of the In- ternational Clinical Update and Research Symposium of the National Association of Neonatal Nurses (p. 35). Peta- luma: NANN.
Ludington, S. M., Swinth, J . , Becker, J., Rao, S., & Hadeed, A. (1995). The effects of kangaroo care o n apnea of prematu- rity. In Proceedings of the International Clinical Update and Research Symposium of the National Association of NeonatalNurses (p. 93). Petaluma: NANN.
Ludington, S. M., Thompson, C., & Swinth, J. (1992). Efficacyof kangaroo care with preterm infants in open air cribs. Neo- natalNetwork, 11(6), 101.
Ludington-Hoe, S. M. (1996). Decreased pain response follow- ing kangaroo care. Manuscript in preparation.
Ludington-Hoe, S. M., Anderson, G. C., Rey, H., Argote, L. A., & Hosseini, B. (1992). Transitional physiology and state be- havior of Colombian preterm infants in skin-to-skin (kan- garoo) care and open-air cribs beginning in the delivery room. Infant Behavior and Development (Special Issue), 15,537.
Ludington-Hoe, S. M., Anderson, G. C., Simpson, S., & Holling-
sead, A. (1993). Skin-to-skin contact beginning in the de- livery room for Colombian mothers and their preterm in- fants. Journal ofHuman Lactation, 9(4), 241-242.
Ludington-Hoe, S . M., 62 Golant, S. K. (1993). Kangaroo care; The bestyou can do foryourpremature infant. New York: Bantam Books.
Ludington-Hoe, S. M., Hadeed, A. J., 62 Anderson G. C. (1991). Physiologic responses to skin-to-skin contact in hospital- ized premature infants. JournalofPerinatology, 11(1), 19- 24.
Ludington-Hoe, S. M., Hashemi, M. S., Argote, L. A., Medellin, G . , & Rey, H. (1992). Selected physiologic measures and behavior during paternal skin contact with Colombian pre- term infants. Journal of Developmental Physiology, 18,
Ludington-Hoe, S. M., Thompson, C., Swinth, J., Hadeed, A. J . , &Anderson, G. C. (1994). Kangaroo care: Research results, and practice implications and guidelines. Neonatal Net- work, 13(l) , 19-27.
Martinez, H. G., Rey, E. S., & Marquette, C. M. (1992). The Mother Kangaroo Programme. International Child Health, 3(1), 55-67.
Miles, M . S., Funk, S. G., 6; Carlson, J . (1993). Parental stressor scale: Neonatal intensive care unit. Nursing Research, 42, 148-152.
Miranda, S. B. (1970). Visual abilities and pattern preferences of premature infants and fullterm neonates. Journal Experi- mental Child Psychology, 10, 189-205.
Moeller-Jensen, H., Hjort-Gregersen, K . , Mattiessen, M., Vester- gaard, H. F., & Jepsen, B. H. (1987). The kangaroo method used in practice at the hospital of Soenderborg, Denmark. Sygeplejersken, 19(87), 12-16. (English version available from UNICEF.)
Mondlane, R. P., de Graca, A. M. P., & Ebrahim, G. J. (1989). Skin-to-skin contact as a method of body warmth for infants of low birth weight. Journal Tropical Pediatrics, 35, 321- 326.
National Association of Neonatal Nurses (NANN). (1995). In- fant and family-centered developmental care guidelines. Petaluma, CA: NANN.
Nichols, D., 6; Rogers, M. (1987). Developmental physiologyof the respiratory system. In M. C. Rogers (Ed.), Textbook of pediatric intensive care (Vol. 1, pp. 83-1 11). Baltimore: Williams and Wilkins.
Robinson, T. M. S. (1995). Educating secondarycaregivers. Neo- natal Network, 14(4), 69-70.
Rozin, A., Weller, A,, Charpak, N., Ruiz, J . G., de Calume, Z., Charpak, Y., & Sack, J . (1995). Maturation of the pituitary- thyroid axis and the adrenal in low birth weight infants raised by the ‘kangaroo’ method. PediatricResearch, 37(4) Pt. 2, 235A.
Schmidt, E., & Wittreich, G. (1986). Care of the abnormal new- born: A random controlled trial study of the ‘kangaroo method’ of care of low birth weight newborns. In World Health Organization Interregional Conference on Appro- priate Technology Following Birth. Trieste: World Health Organization.
Syfrett, E. B., Anderson, G. C . , Behnke, M., & Neu, J . (1993). Early and virtually continuous kangaroo care for lower-risk preterm infants: Effect on temperature, breastfeeding, sup- plementation, and weight. Proceedings of the Biennial Conference of the Council of Nurse Researchers, American Nurses Association, Washington, D.C., November 1993.
Thoman, E. B. (1990). Sleeping and waking states in infancy: A functional perspective. Neuroscience and Biobehavioral Reviews, 14,93- 107.
223-232.
702 J O C N N Volume 25, Number 8

Developmentally Based Care
Toffler, A. (1970). Future shock. New York: Random House. Tuomikoski-Koiranen, P. (1990, June). Kangaroo careasapart
of nursing premature infants and some results from a study on kangaroo care in the neonatal unit of Turku Uni- versity Hospital, 1986. Paper presented at the Third Bien- nial International Conference for Maternity Nurse Re- searchers, Nordic School for Public Health, Gothenberg, Sweden.
Wahlberg, V., Persson, B., & Atfonso, D. (1990). Kangurumeto- den: den manskliga kuvosen (The kangaroo method: Moth- er’s memories). Lakartidningen, 87(5), 288-289.
Wahlberg, V., Monso , D., & Persson, B. (1992). A retrospective, comparative study using the kangaroo method as a comple- ment to the standard incubator care. European Journal of Public Health, 2, 34-37.
Wallace, J., 8r Ridpath-Parker, J . (1993). Kangaroo care. Quality Management in Healthcare, 2(1), 1-5.
Whitelaw, A. (1986). Skin-to-skin contact in the care of very low birth weight babies. Maternal Child Health, 7,242-246.
Whitelaw, A. (1990). Kangaroo baby care: Just a nice experience or an important advance for preterm infants? Pediatrics, 85(4), 604-605.
Whitelaw, A,, Heisterkamp, G., Sleath, K., Acolet, D., & Rich- ards, M. (1988). Skin-to-skin contact for very low birth-
weight infants and their mothers. Archives of Disease in Childhood, 63, 1377-1381.
Whitelaw, A., 8r Sleath, K . (1985). Myth of marsupial mother: Home care of very low birth weight babies in Bogota, Co- lombia. Lancet, I, 1206-1208.
Wolff, P. H. (1959). Observations o n newborn infants. Psychoso- matic Medicine, 21, 110-1 18.
Yecco, G. J . (1993). Neurobehavioral development and devel- opmental support of premature infants. Journal ofPerina- tal andNeonatalNursing, 7(1), 56-65.
Address for correspondence: Susan M. Ludtngton-Hoe, CNM, PhD, FAAN, Untverstty of Maryland at Balttmore, School of Nurstng, 655 West Lombard Street, Baltimore, MD 21201.
Susan M. LudingtonHoe is aprofessor in the School ofNurstng at the University ofMaryland tn Baltimore.
Joan Y. Swtnth ts a staffnurse tn the Neonatal Intenstve Care Unit at Kadlec Medtcal Center tn Rtchland, WA.
October 199G J O C N N 703