development of inf venacava and pulmonary veins
TRANSCRIPT
Development of Inf. venacavaand Pulmonary vein
Anup Pandey
Dept. of Human Anatomy
B.P. Koirala Institute of Health Sciences
Dharan Nepal
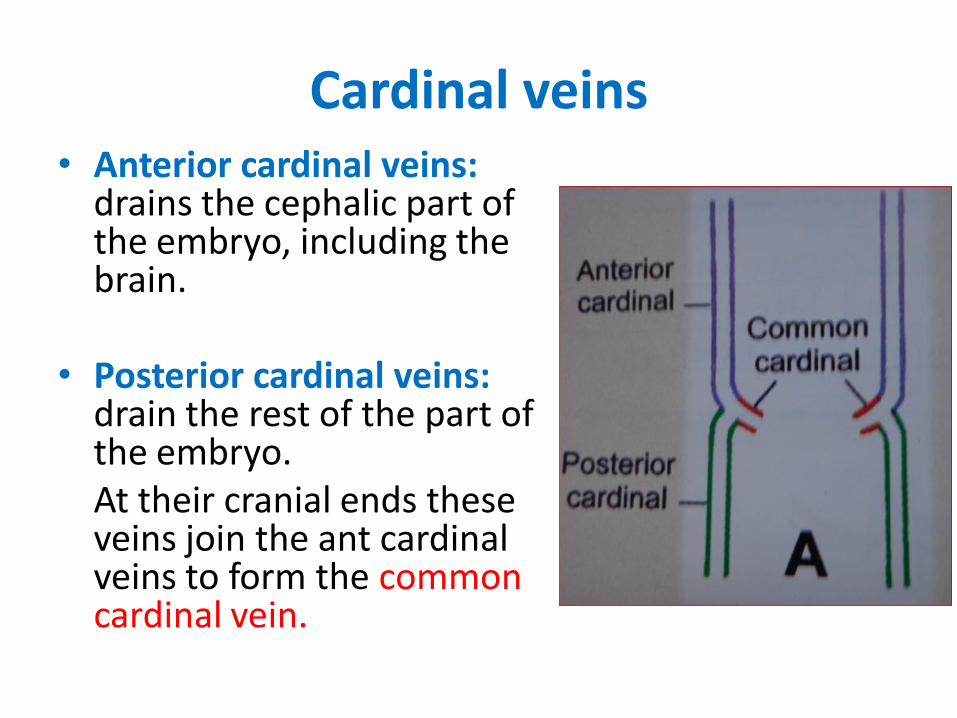
Cardinal veins• Anterior cardinal veins:
drains the cephalic part of the embryo, including the brain.
• Posterior cardinal veins: drain the rest of the part of the embryo. At their cranial ends these veins join the ant cardinal veins to form the common cardinal vein.
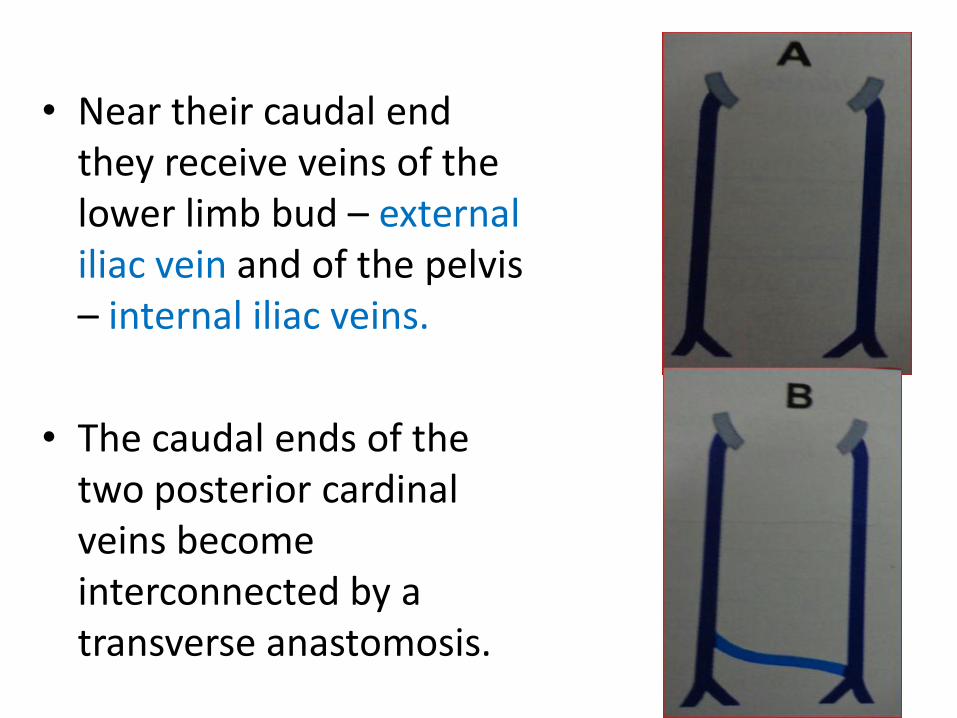
• Near their caudal end they receive veins of the lower limb bud – external iliac vein and of the pelvis – internal iliac veins.
• The caudal ends of the two posterior cardinal veins become interconnected by a transverse anastomosis.
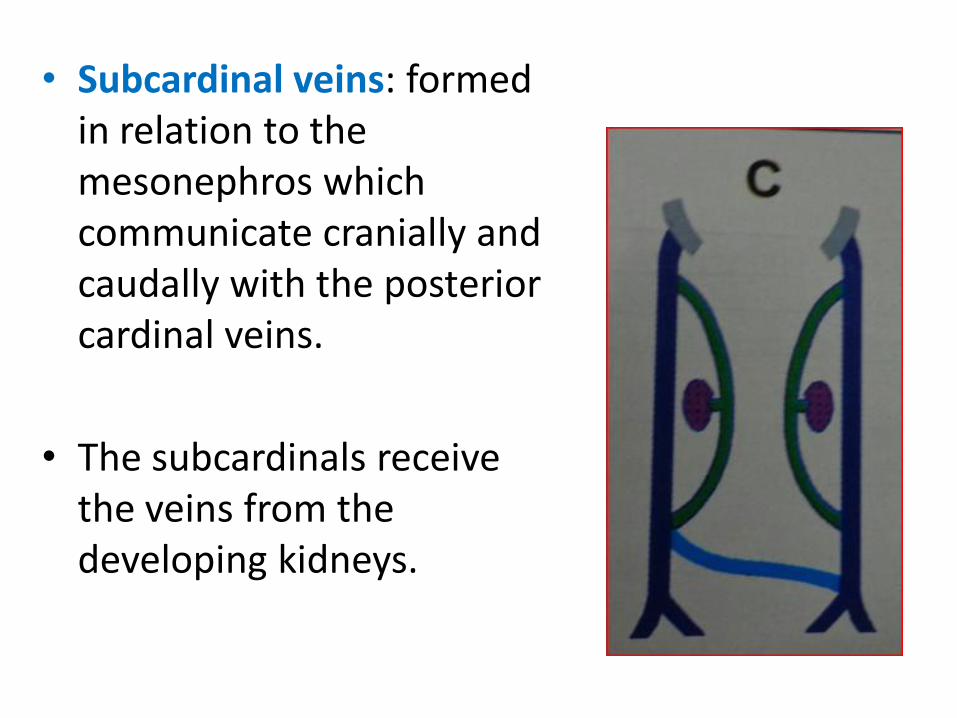
• Subcardinal veins: formed in relation to the mesonephros which communicate cranially and caudally with the posterior cardinal veins.
• The subcardinals receive the veins from the developing kidneys.
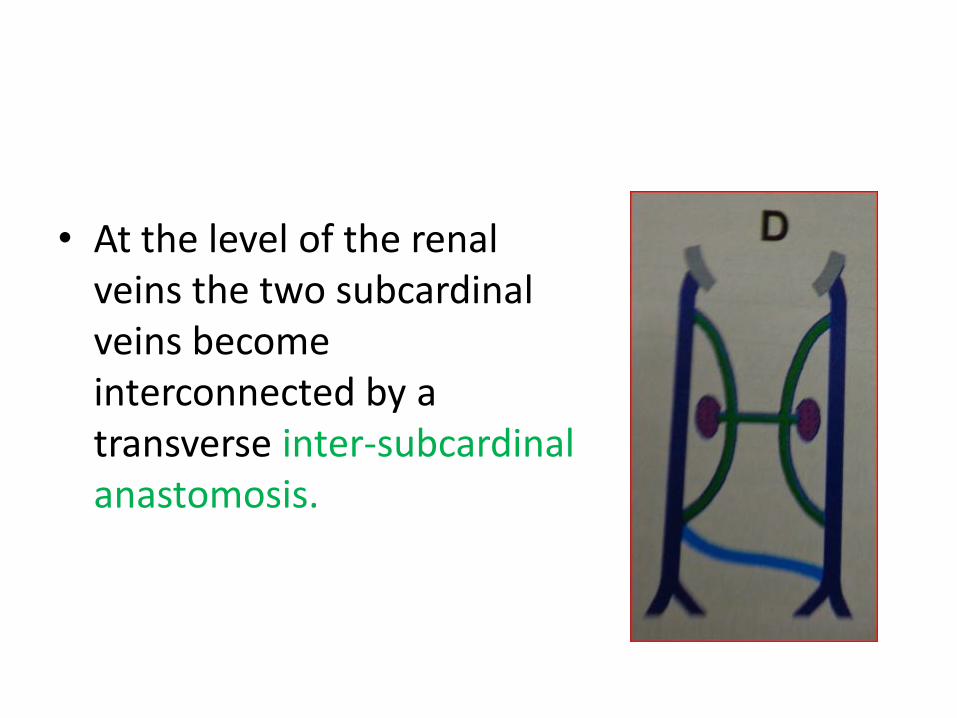
• At the level of the renal veins the two subcardinalveins become interconnected by a transverse inter-subcardinalanastomosis.
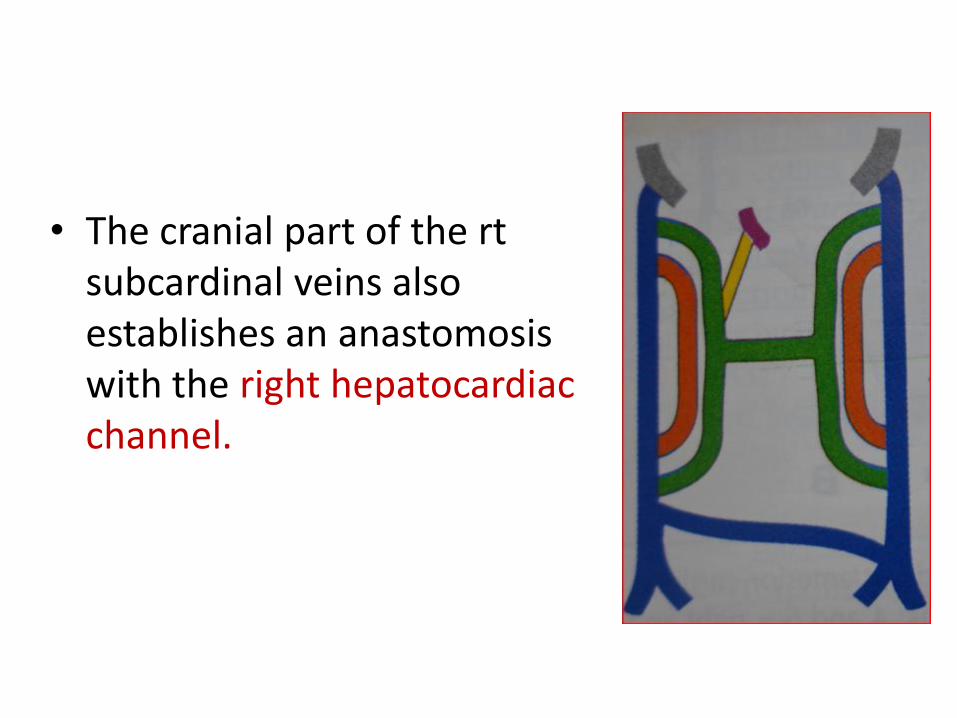
• The cranial part of the rtsubcardinal veins also establishes an anastomosiswith the right hepatocardiacchannel.
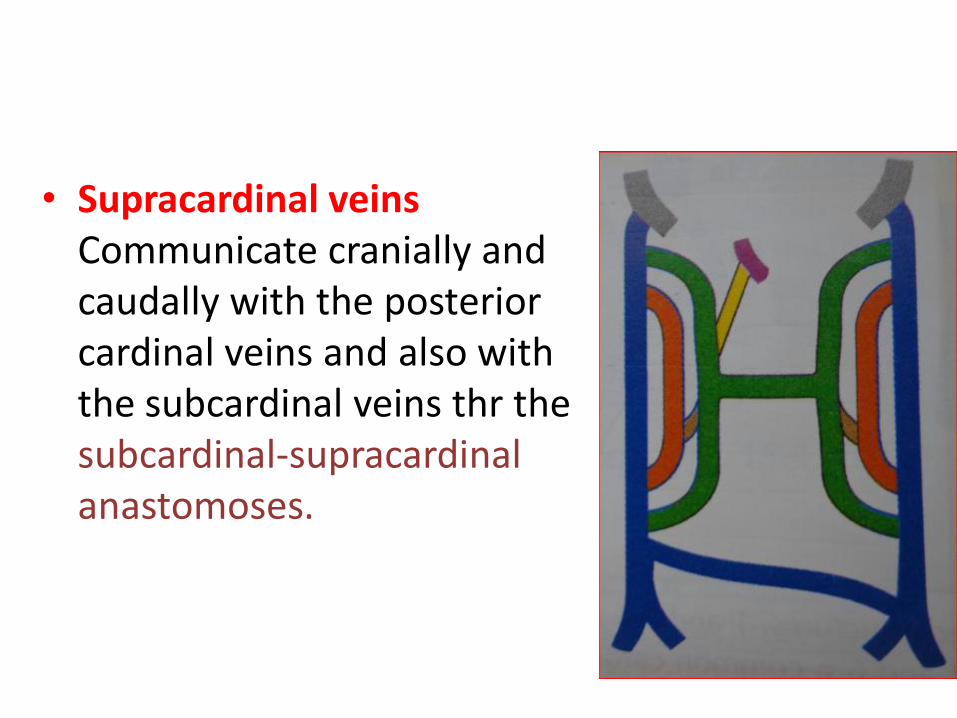
• Supracardinal veins Communicate cranially and caudally with the posterior cardinal veins and also with the subcardinal veins thr the subcardinal-supracardinalanastomoses.
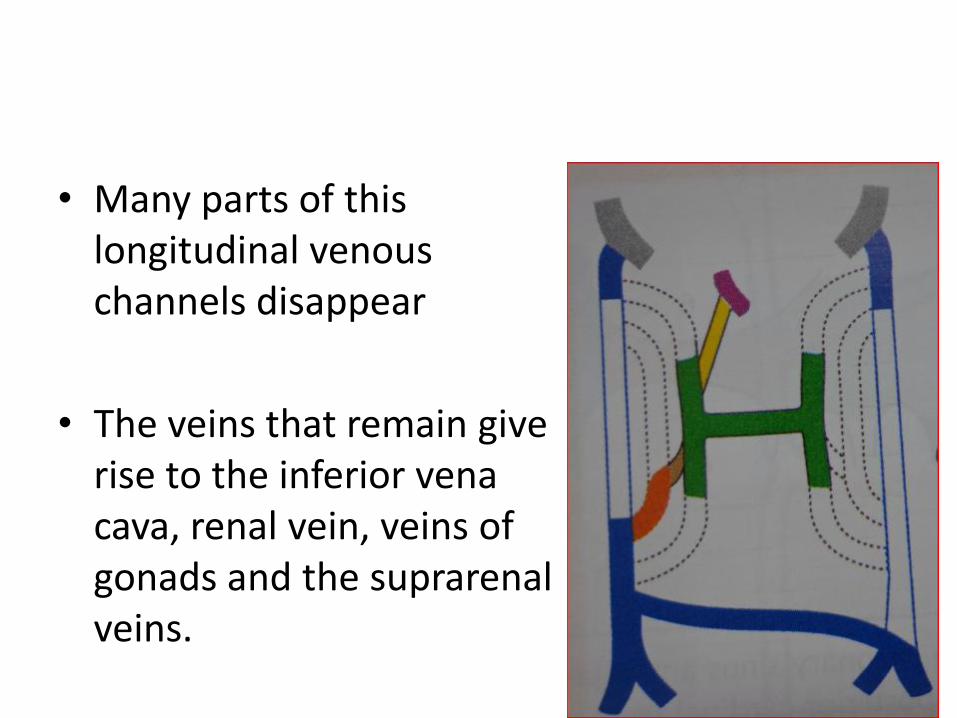
• Many parts of this longitudinal venous channels disappear
• The veins that remain give rise to the inferior vena cava, renal vein, veins of gonads and the suprarenal veins.
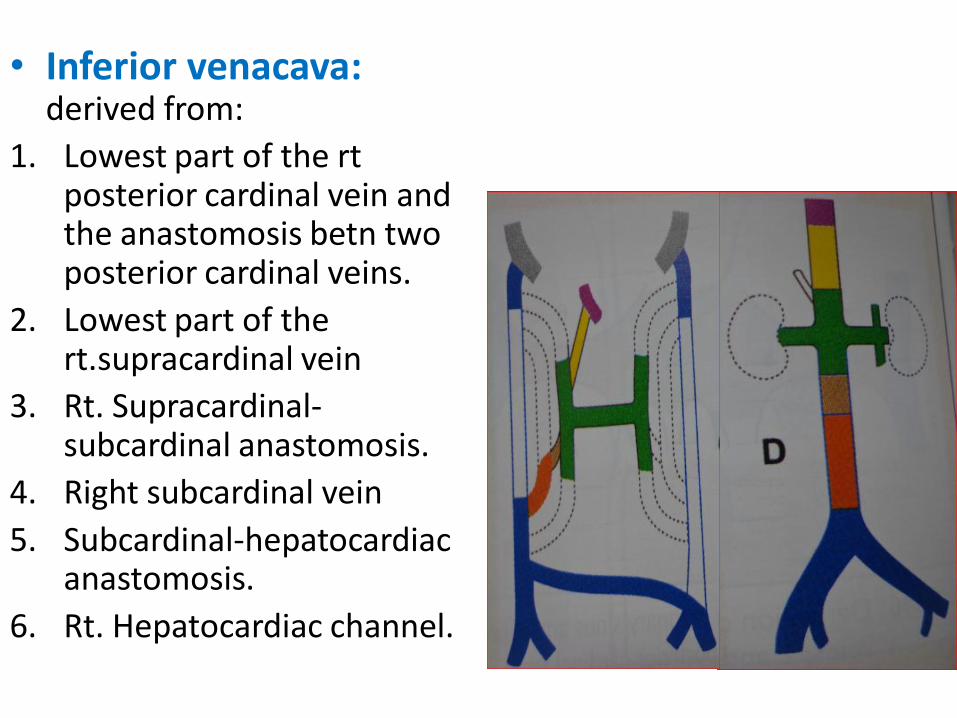
• Inferior venacava: derived from:
1. Lowest part of the rtposterior cardinal vein and the anastomosis betn two posterior cardinal veins.
2. Lowest part of the rt.supracardinal vein
3. Rt. Supracardinal-subcardinal anastomosis.
4. Right subcardinal vein
5. Subcardinal-hepatocardiacanastomosis.
6. Rt. Hepatocardiac channel.
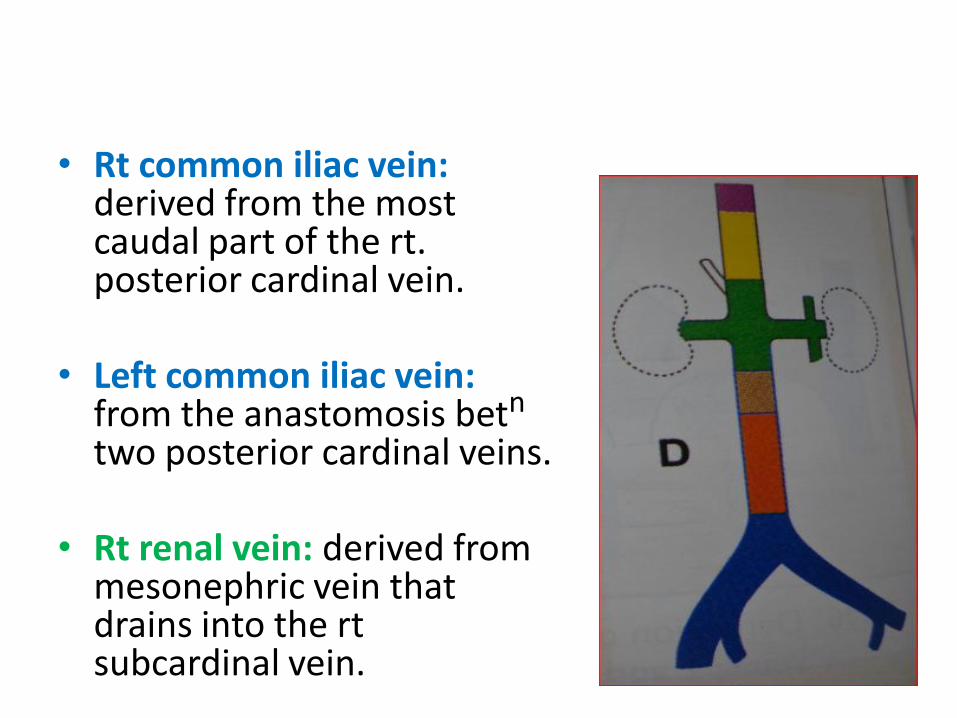
• Rt common iliac vein: derived from the most caudal part of the rt. posterior cardinal vein.
• Left common iliac vein: from the anastomosis betn
two posterior cardinal veins.
• Rt renal vein: derived from mesonephric vein that drains into the rtsubcardinal vein.
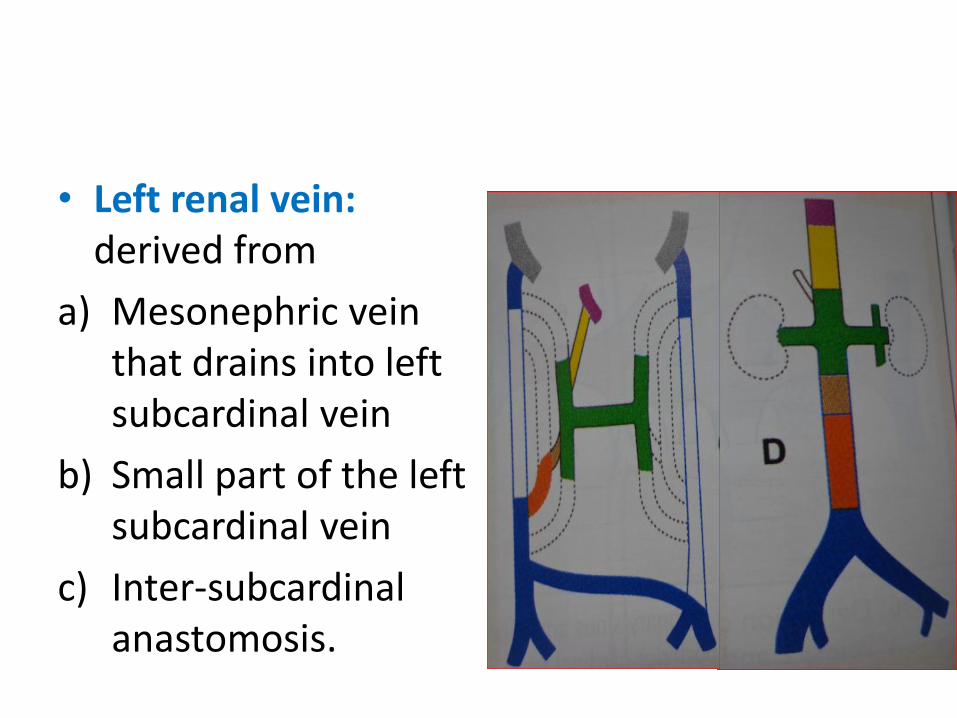
• Left renal vein: derived from
a) Mesonephric vein that drains into left subcardinal vein
b) Small part of the left subcardinal vein
c) Inter-subcardinalanastomosis.
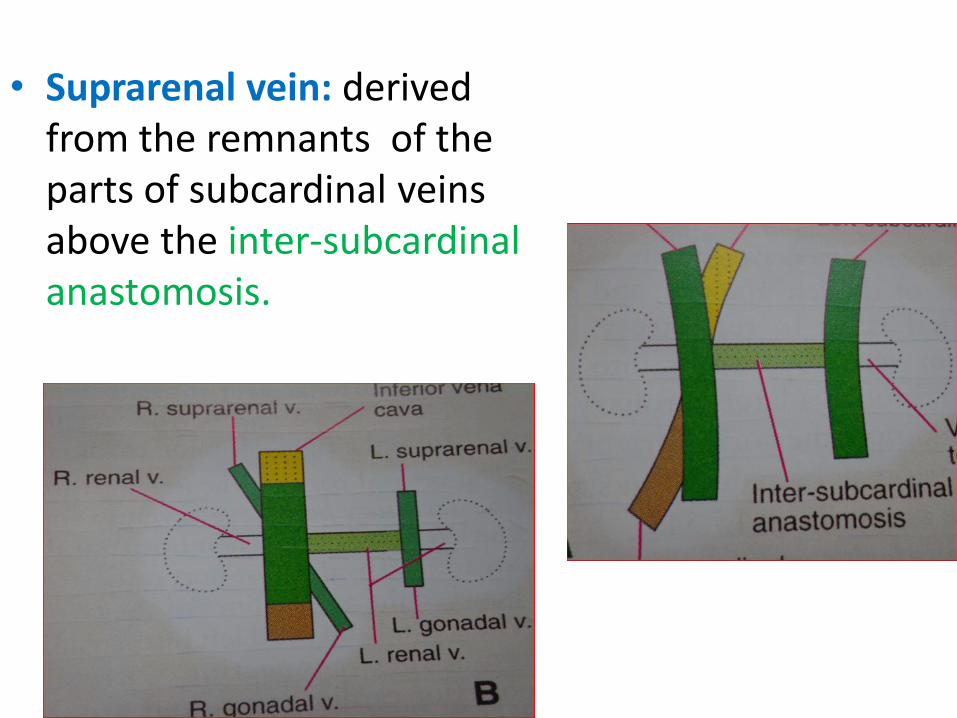
• Suprarenal vein: derived from the remnants of the parts of subcardinal veins above the inter-subcardinalanastomosis.
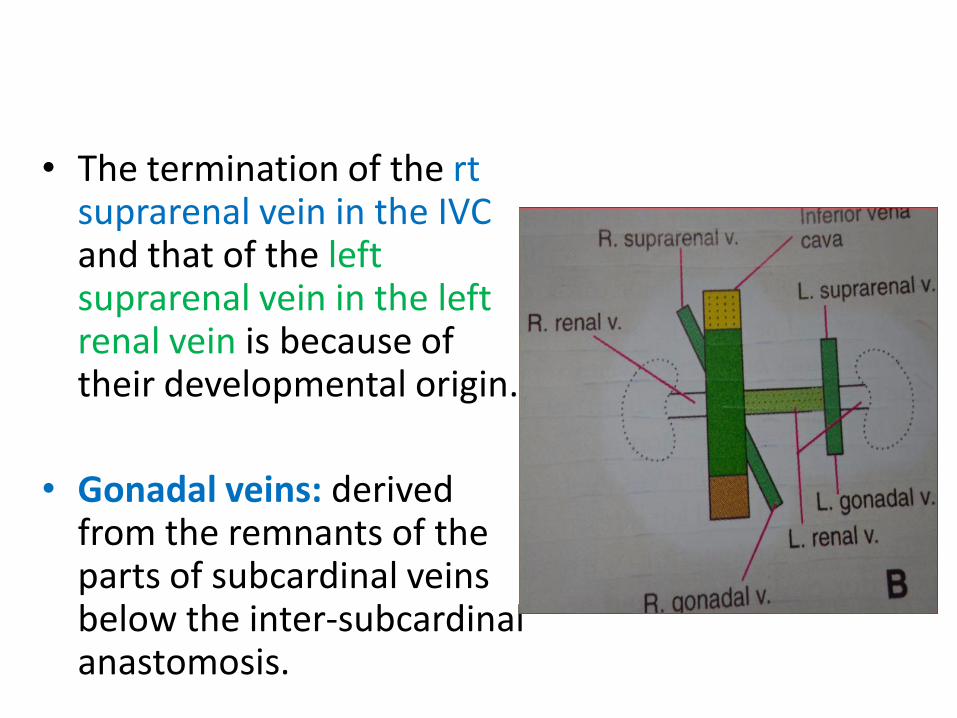
• The termination of the rtsuprarenal vein in the IVC and that of the left suprarenal vein in the left renal vein is because of their developmental origin.
• Gonadal veins: derived from the remnants of the parts of subcardinal veins below the inter-subcardinalanastomosis.
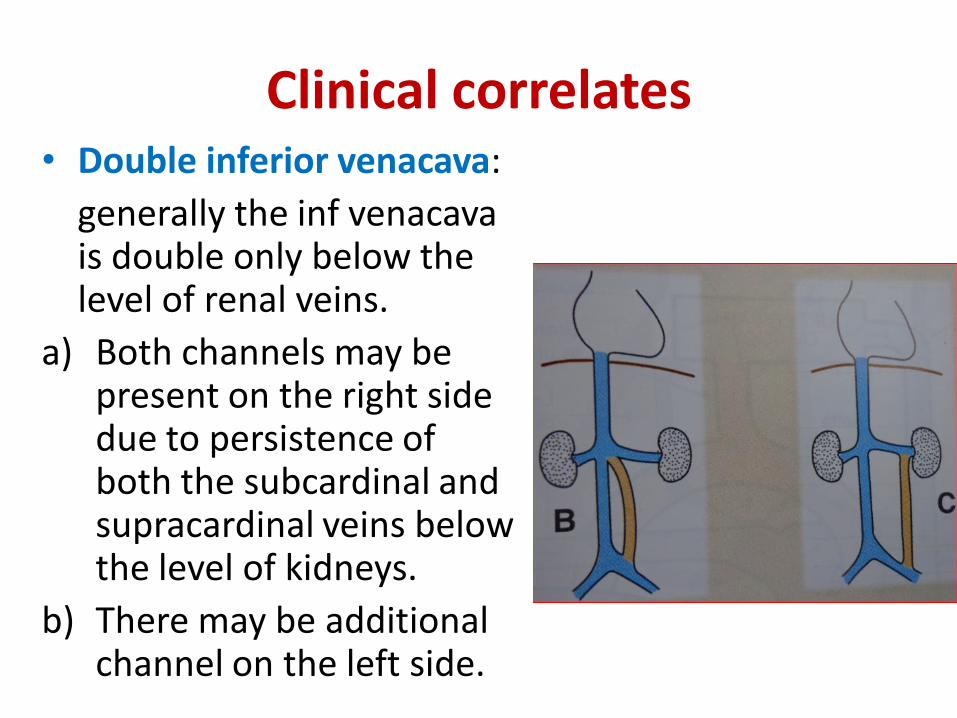
Clinical correlates• Double inferior venacava:
generally the inf venacavais double only below the level of renal veins.
a) Both channels may be present on the right side due to persistence of both the subcardinal and supracardinal veins below the level of kidneys.
b) There may be additional channel on the left side.
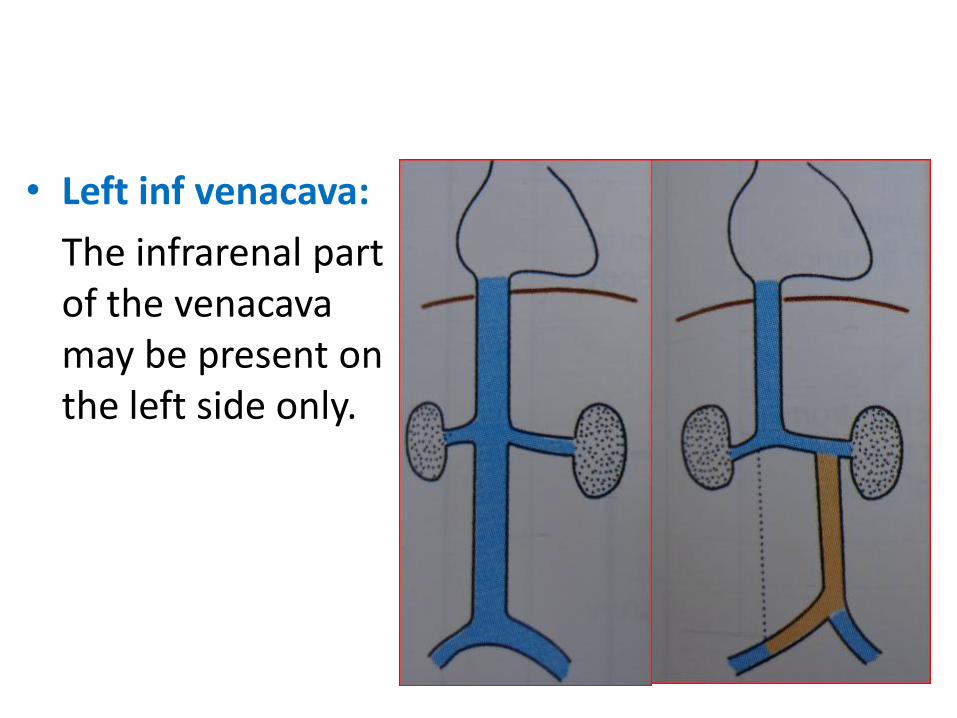
• Left inf venacava:
The infrarenal part of the venacavamay be present on the left side only.
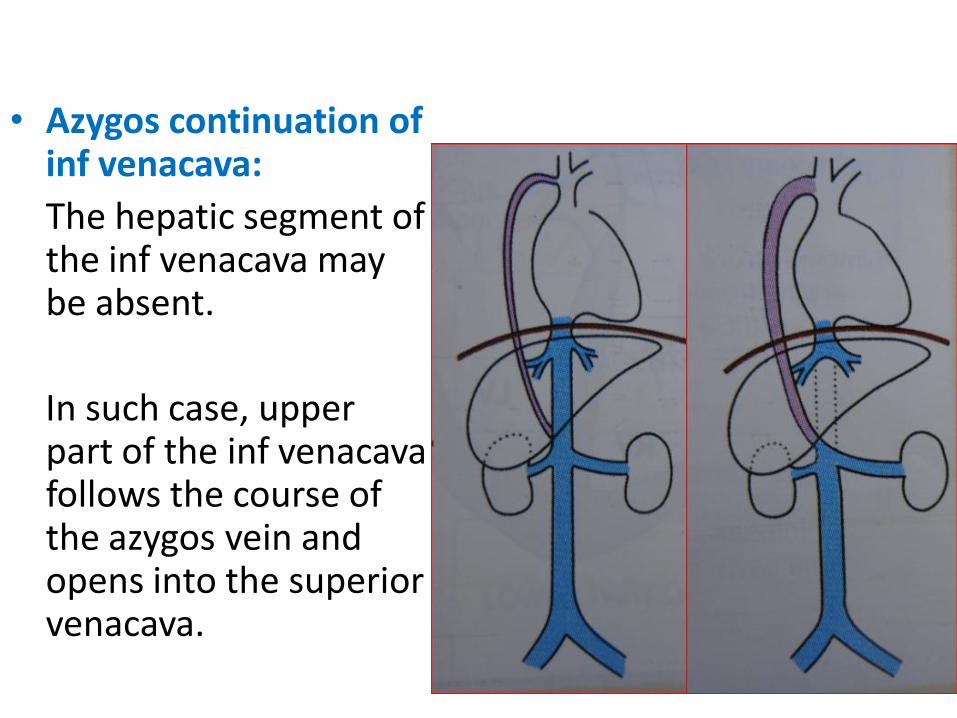
• Azygos continuation of inf venacava:
The hepatic segment of the inf venacava may be absent.
In such case, upper part of the inf venacavafollows the course of the azygos vein and opens into the superior venacava.
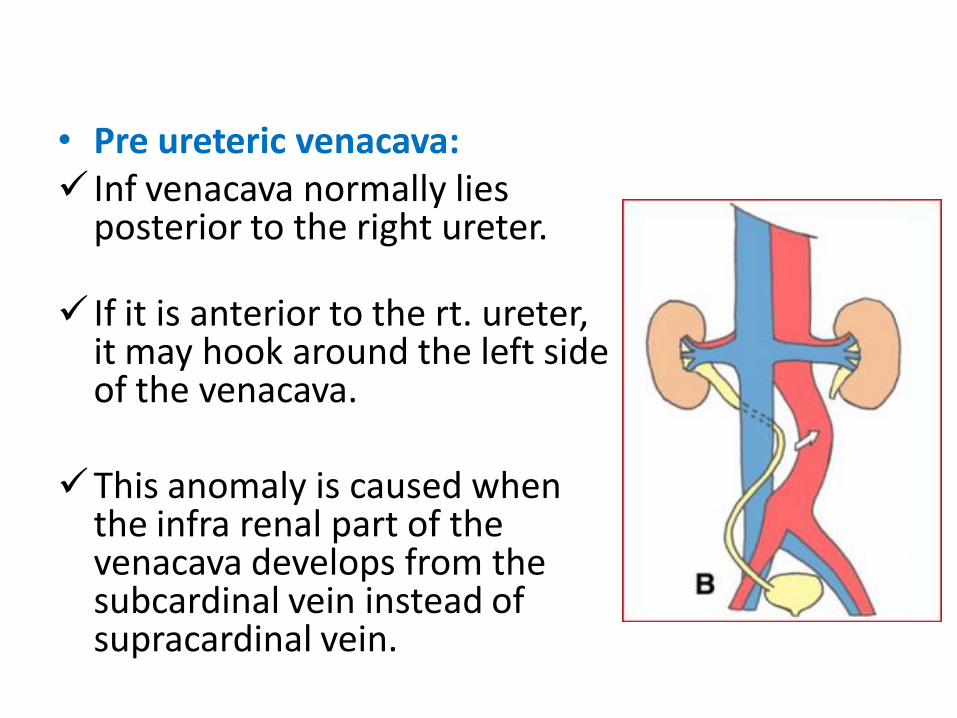
• Pre ureteric venacava: Inf venacava normally lies
posterior to the right ureter.
If it is anterior to the rt. ureter, it may hook around the left side of the venacava.
This anomaly is caused when the infra renal part of the venacava develops from the subcardinal vein instead of supracardinal vein.
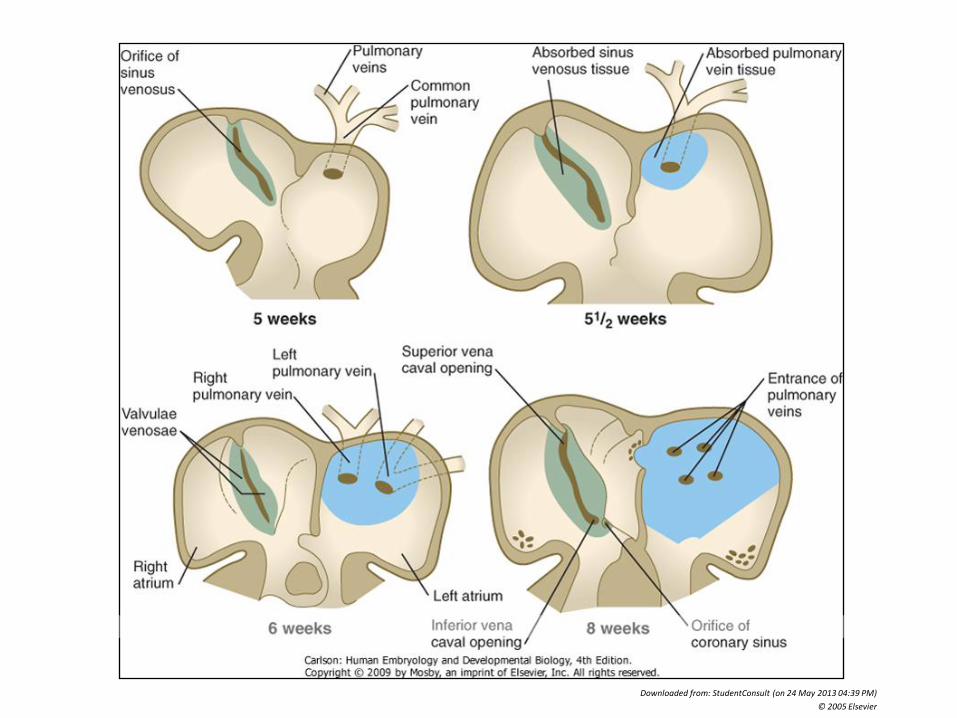
Pulmonary veins
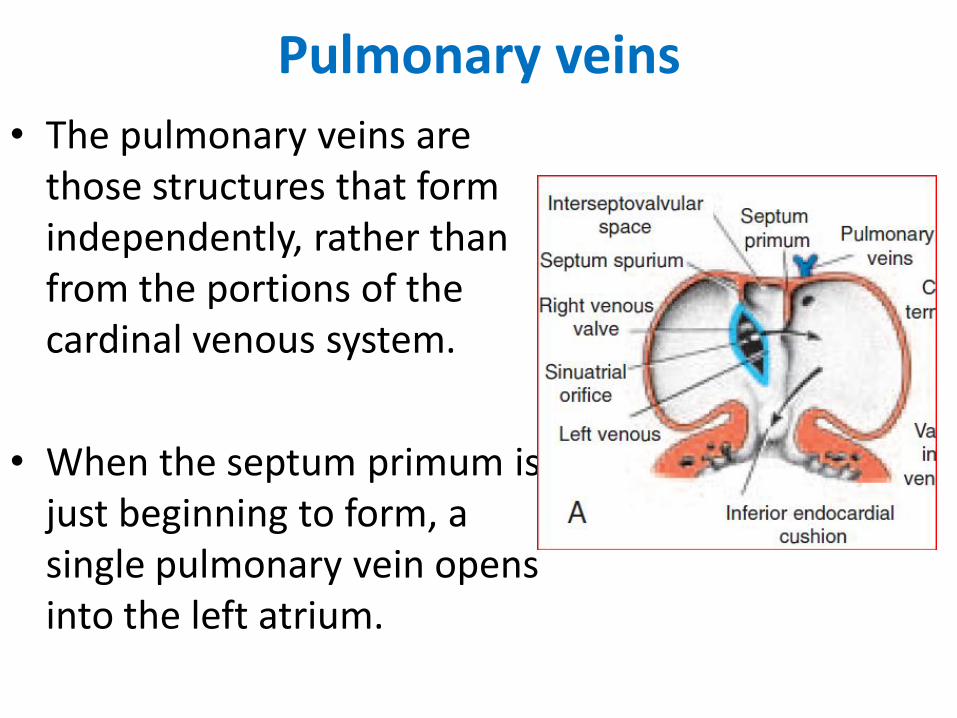
• The pulmonary veins are those structures that form independently, rather than from the portions of the cardinal venous system.
• When the septum primum is just beginning to form, a single pulmonary vein opens into the left atrium.
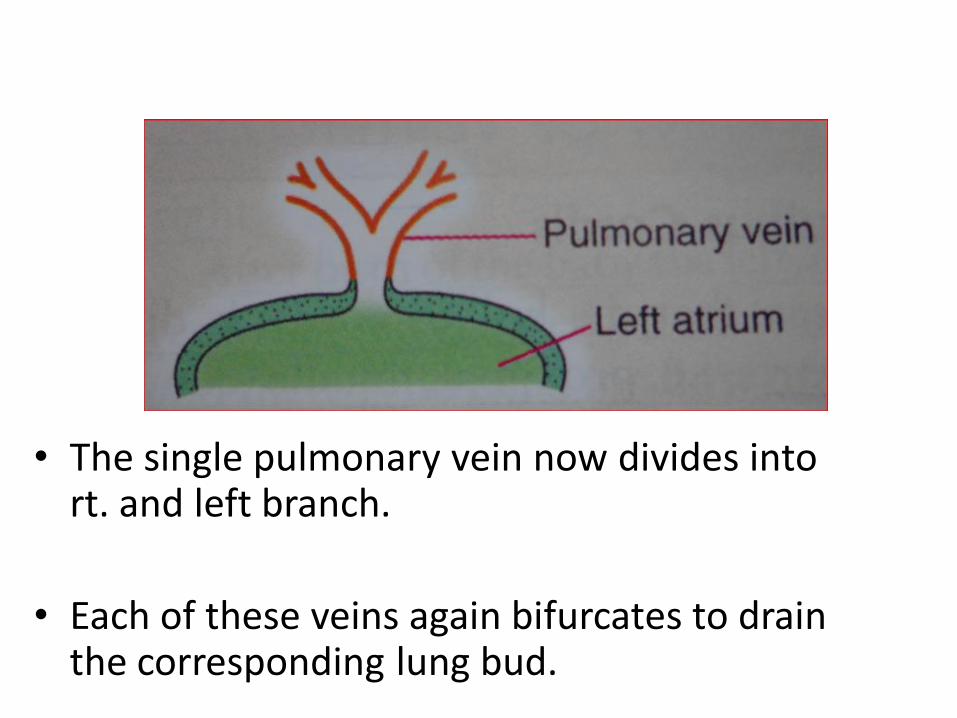
• The single pulmonary vein now divides into rt. and left branch.
• Each of these veins again bifurcates to drain the corresponding lung bud.
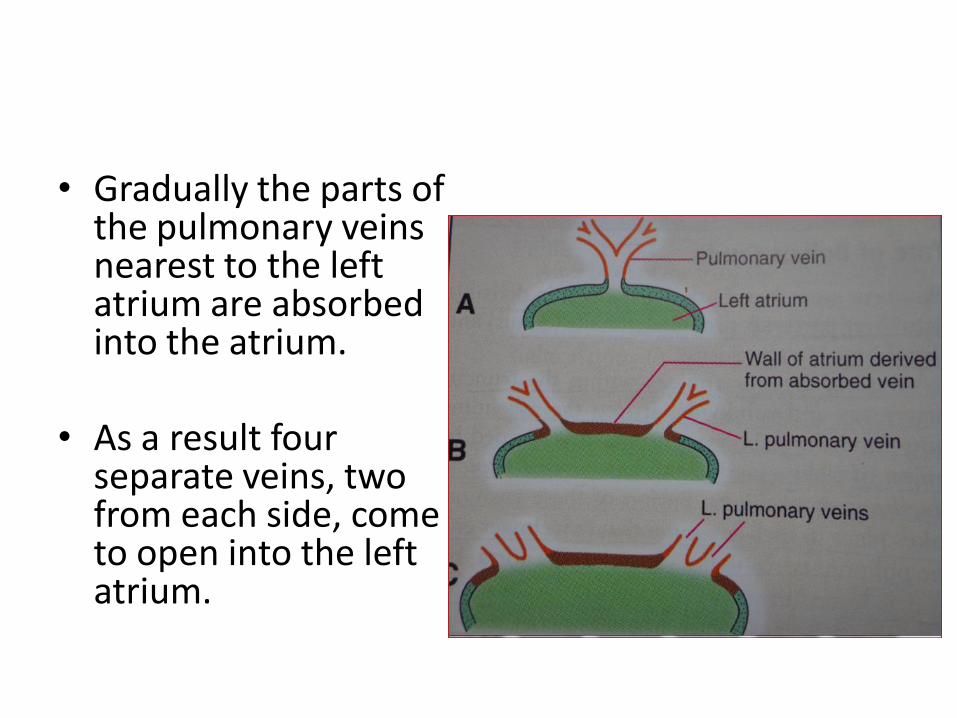
• Gradually the parts of the pulmonary veins nearest to the left atrium are absorbed into the atrium.
• As a result four separate veins, two from each side, come to open into the left atrium.
Downloaded from: StudentConsult (on 24 May 2013 04:39 PM)
© 2005 Elsevier
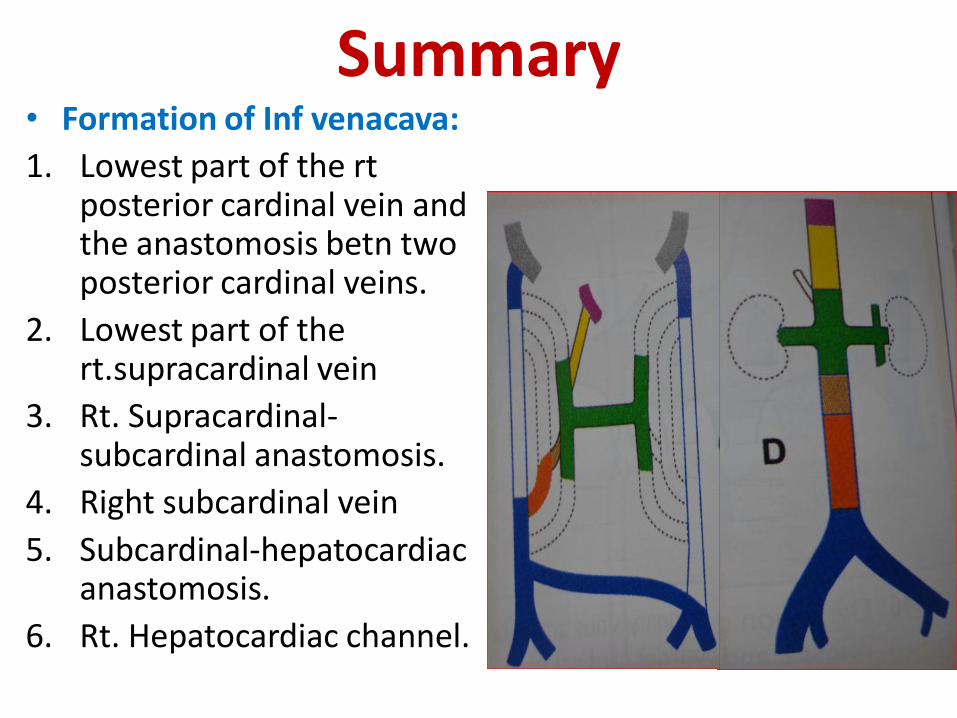
Summary• Formation of Inf venacava:
1. Lowest part of the rtposterior cardinal vein and the anastomosis betn two posterior cardinal veins.
2. Lowest part of the rt.supracardinal vein
3. Rt. Supracardinal-subcardinal anastomosis.
4. Right subcardinal vein
5. Subcardinal-hepatocardiacanastomosis.
6. Rt. Hepatocardiac channel.
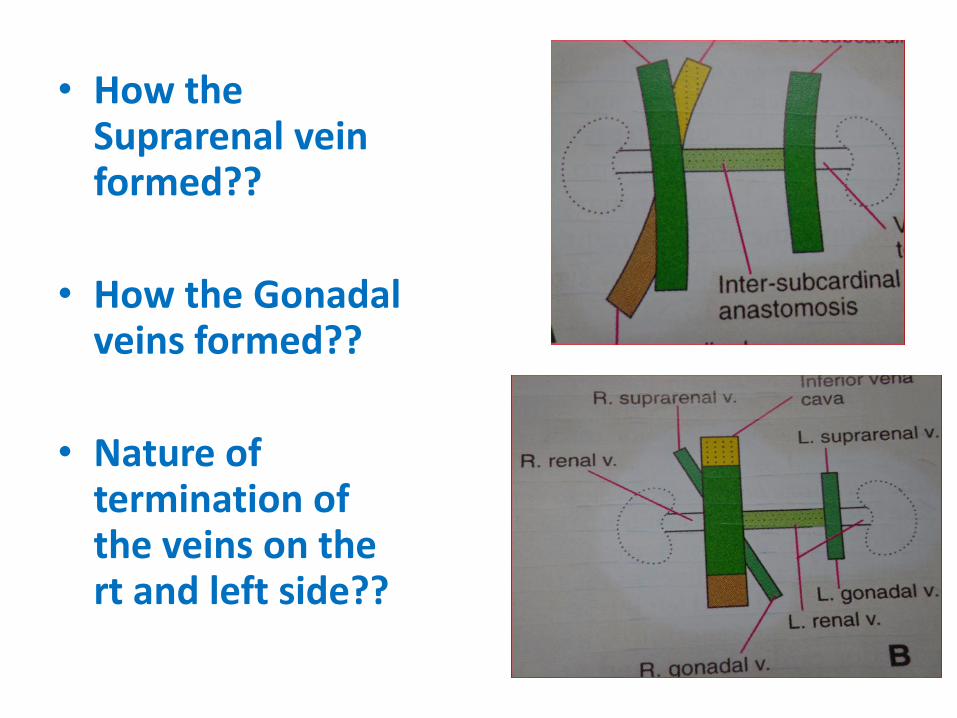
• How the Suprarenal vein formed??
• How the Gonadalveins formed??
• Nature of termination of the veins on the rt and left side??
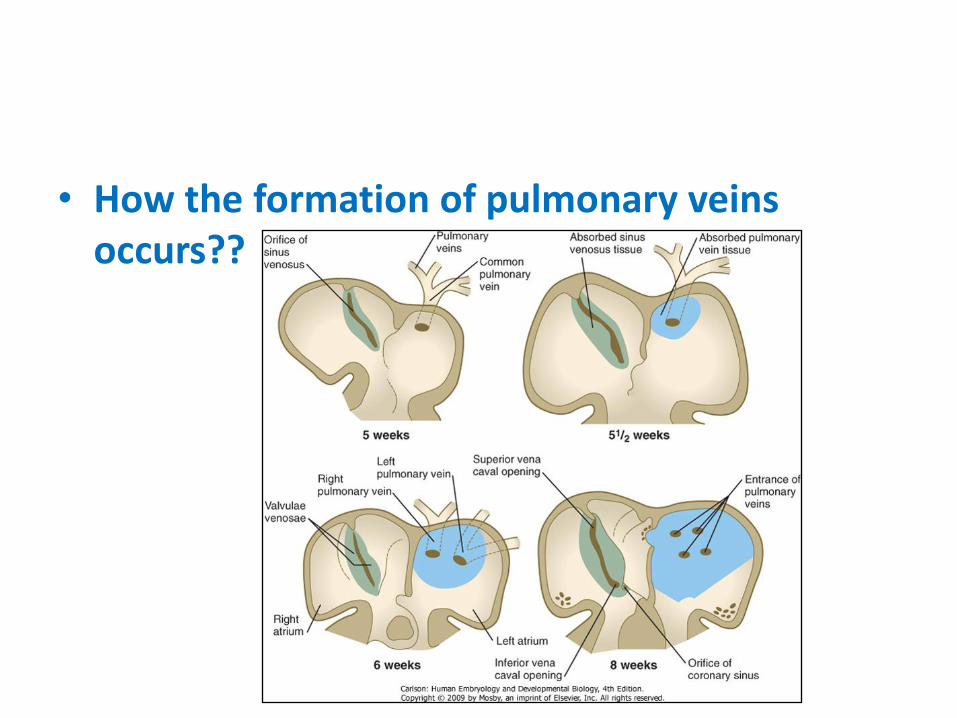
• How the formation of pulmonary veins occurs??

THANK YOU