developing an algorithmic mode of self harm management in enhanced medium secure services for women...
TRANSCRIPT

Developing an algorithmic mode of self harm management in enhanced medium secure services for womenDr. Chris Beeley [email protected]
Co- author Dr. Jay Sarkar

Summary
• Aspects of self harm risk• Model description
– Types of self harm– Managing self harm
• Model fidelity on ward (and vice versa)
• Staff satisfaction and effectiveness

Context
• Medium secure women’s ward•High levels of self harm•Index offence typically arson/ harm to children or vulnerable adults•Disorders of attachment due to developmental trauma, abuse and neglect•Primary diagnosis of severe PD, co-morbid psychosis, substance abuse and PTSD

Self harm
• High levels of aggression to self and others
•In 18 month period 546 acts of self-harm and 536 acts of other-harm
•Severe self harm including:•Open wounds in subcutaneous tissue•Insertion of foreign objects into wounds•Ligation and suffocation•Poisoning and contamination of wounds

Aspects of risk
• Lethality is the probability that the patient’s act of self-harm is likely to end in death. It is also referred to as the ‘how quickly to death’ question.•Intentionality- intensity of the patient’s desire or wish to die.
•‘How likely to die’ question•Self reports can be unreliable and so inferred objectively from the nature and severity of self harm
•Inimicality- making the circumstances unfavourable or unduly complicated in order to avoid detection by others, and thus increase the likelihood of serious harm or death
•‘How to avoid detection’ question

Lethality
Lethality of the self-injury Types of self-injury (‘Act’)Traditional methods of suicide Hanging, strangulation, shooting, jumping
gas, drugs, pesticides), stabbing, electrocution, drowning from a high place, poisoning
Highly lethal Overdose, recreational drug-OD as self-harm, cutting, burning
Self-injury with tissue damage Self-biting, scratching, gouging, carving words of symbols on skin, sticking needles or pins into skin, interfering with wound healing
Less lethal Self-hitting, head-banging, fist against hard objects, pinching, pulling hair
Self-injury with no tissue damage Over-exercising, denying a necessity to hurt oneself, stopping medications, starving with intent to cause harm, tattoos, multiple body piercing
Non-lethal Deliberate recklessness with cars, drugs, trains, etc.

Inimicality
Inimicality of the self-injury
Monitoring
Three staff observing, two staff observing, line of sight observations, observations every 5/ 15 minutes
Level of observations
Graded access to objects based upon observation levels
Access to objects to self-harm with
Graded access to various parts of the ward, unit, hospital based upon observation and access to objects level
Access to spaces on/ off ward
Manage personnel deployed on high risk shifts (nights, weekends, bank shifts)
Access to certain staff profiles and shifts

Level 1 Level 2 Level 3 Level 4 Level 5 Cutting Superficial,
little blood loss
Subcutaneous, moderate blood loss
Puncture, stab wounds, deep wounds into muscle, deep biting, significant blood loss
Headbanging Gentle and brief
Gentle or brief Moderate Repetitive, forceful
Severe, intense, repetitive and staggering, altered consciousness
Self hitting Gentle, brief Firm brief Moderately hard causing tissue damage
Causes fracture Severe, intense, repetitive
Insertion/ stabbing
Causes tissue damage
Into old wounds
Into new wounds
Burning/ scalding
Scratching, rubbing
Clothes, carpet burns
Scalding Cigarette burn, embers
Ingestion Low lethality- convex, non-sharp, nontoxic
High lethality- any hooks, sharpness or toxicity
Ligation Low lethality- no fixed ligation point
High lethality- fixed ligation point
Suffocation Partial occlusion of airway
Full occlusion of airway

Level 1 Level 2 Level 3 Level 4 Level 5 Internal response
Staff HCSW under supervision
Senior staff on duty
Junior doctor/ PHC
Extra staff required to observe patient
Senior on-call nurse, consultant, manager
Blicks No On NICs judgement
Yes Yes Yes
PHC No On NICs judgement
Yes Post incident PHC management
Yes, also Toxbase
Level 1 Level 2 Level 3 Level 4 Level 5 Observation/ support
Observation From a distance
Level 1 Close obs, no formal physical obs
Vitals- pulse, BP
Mobility, gait, level of consciousness, coherent speech
Support Offer support- de-escalation
Dialogue, distraction and diversion
Intervention/ wound care
Intervention No hands on
Safely remove implements
Staff in close proximity
Immediately cut ligation
Wound care/ other medical intervention
Offer cleaning materials to patients (not steri-strips)
Wound cleaned and steri-strips applied by staff
Wash and remove objects if visible and/ or splint limb to prevent penetrating wounds
Tie ligatures and compress freely bleeding wounds
O2 cylinder available- cyanosis in fingertips only O2 cylinder used- cyanosis in face or lips

Introducing the model
• Manualised programme of self-harm training devised•Delivered over 3 days•Clinical vignettes and scenario planning•Policies and procedures updated•Particularly, senior clinical and managerial staff were to be involved

Method
•Iterative model testing and development•Model tested for fidelity to practice and vice versa
•Changes were made to the model following initial examination of the data
•External response removed•“Low risk” ligation added
•Testing particularly for:•Reducing level of intervention to lowest safe level•Clinical and resource implications
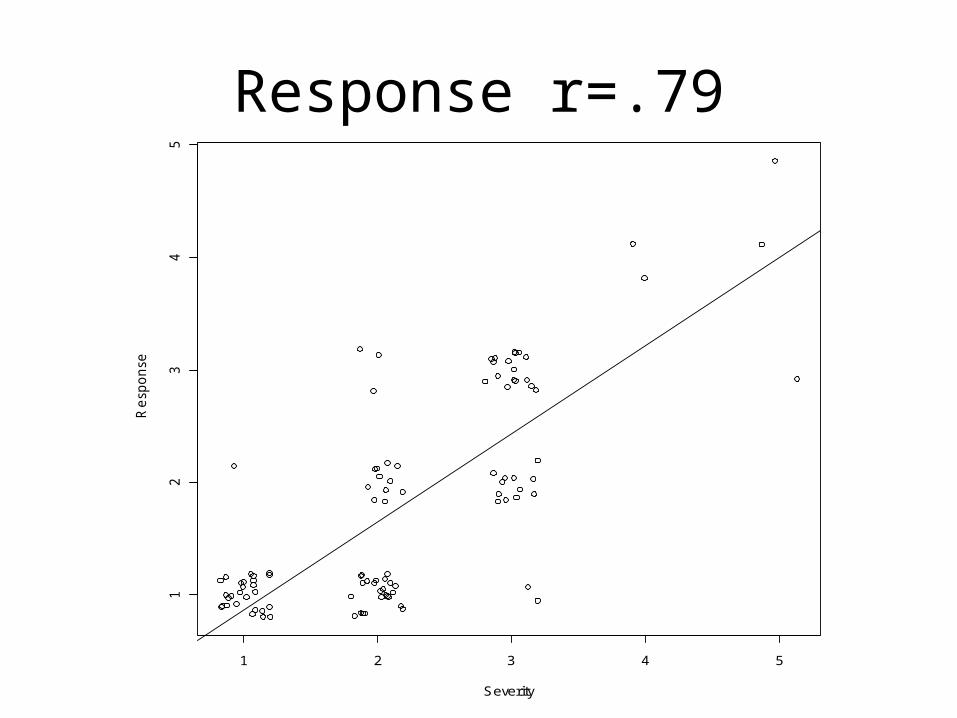
Response r=.79
1 2 3 4 5
12
34
5
Severity
Re
spo
nse

Observation/ support (inimicality) r=.75
1 2 3 4 5
12
34
5
Severity
Ob
serv
atio
n/ s
up
po
rt

Intervention/ wound care r=.69
1 2 3 4 5
12
34
5
Severity
Inte
rve
ntio
n/ w
ou
nd
ca
re

Overall effectiveness
Week
Ave
rag
e in
cid
en
ts p
er
we
ek
0 50 100 150
0.0
0.5
1.0
1.5
2.0
2.5
Cutting• Assess
– Location and depth of wound– Risk to others– Blood loss
• Levels– Low
•Remove patient from area and encourage to stop•Help to dress and clean
– Medium•Intervene if no risk to staff•Medic/ PHC
– High•Intervene if safe (or if risk to patient outweighs risk to staff)•Blicks/ Medic/ PHC•A and E, 999 on medics’ judgement
Swallowing
• Assess– Physical obs, pain, breathing, vomiting
– Type of battery
• Levels– Low
•Observation only
– Medium•A and E (medics’ judgement)
– High•999

Ligature
• Assess– Consciousness, colour, respiratory
function/ damage, breathing, respiration, pulse
• Levels– Low
•Remove ligature and monitor– High
•Remove ligature•Summon medics•Consider use of oxygen/ 999

Headbanging
• Assess– Severity of banging and type of surface– Consciousness– Swelling/ bleeding– Physical obs, breathing, pulse, BP– Neuro obs
• Levels– Low
•Encourage to stop, obs
– Medium•Encourage to stop, increase obs
– High•Intervene where safe
Seclusion
• From interviews:– When secluded if there is blood loss or headbanging only verbal
intervention will be used- only where risk to patient outweighs risk to staff will they intervene
– In seclusion if there are sharp objects then important to assess as a weapon. Where serious weapons are involved seclusion will not be entered.
– Entering seclusion entered purely on basis of weighing risk to staff versus risk to patient
Enter seclusion where risk to patients clearly outweighs risk to staff, i.e. low risk to staff (unconsciousness, extreme
blood loss) or very high risk to patient (e.g. occluded airways)

General
• Outline – Patients feel unsafe when staff are unused to dealing with self
harm– When self harm is in seclusion need to ask who is most at risk,
staff or patient• Process developed
– Practice has “just developed”. Confidence has developed with practice
– The ward has become more comfortable with self harm over time• How
– Knowing the patient and risk factors is important– Blicks can be useful to summon other experienced staff– Environment makes it easier to manage risk– Response to self harm is fairly individualised according to care
plan

General
• Why– Works very well, and incidents of self harm
have reduced– Method is effective, especially considering
history of patients– Always going to be challenging with such
serious self harm– Nursing team are very aware of what to do.
Staff from other wards can find it hard

Developing an algorithmic mode of self harm management in enhanced medium secure services for womenDr. Chris Beeley [email protected]
Co- author Dr. Jay Sarkar