deterioration in the eeg in children with cerebral palsy
TRANSCRIPT

Develop. Med. Child Neurol. 1968, 10, 287-301
Deterioration in the EEG in Children with Cerebral Palsy
John Foley
Introduction Studies of the EEG in cerebral palsy are
inevitably vitiated by three facts : firstly, cerebral palsy is not a disease but a group of disorders in which it is seldom possible to make a precise neuro-anatomical (neuro-pathological) diagnosis during life ; secondly, the significance of an abnormal focus in relation to the underlying disease process has rarely been determined; and thirdly, in many cases of cerebral palsy the principal lesions are in deep structures in- accessible to current clinical techniques. Furthermore, the interpretation of EEG records is highly subjective and it is virtu- ally impossible for different observers to agree on a method of classifying the abnormalities seen. This study was promp- ted by the impression gained over a num- ber of years that progressive deterioration in serial records was a reliable indicator of coming epilepsy. Closer examination showed that this impression, like so many clinical impressions, was incorrect. The present paper has therefore two main aims -to examine the EEG in relation to clinical findings, and to investigate its predictive value.
Gordon (1966) found that in cere- bral palsy the EEG is of limited value in that it shows some correlation with the severity of physical handicap but little with the
level of intelligence, and concluded that this test should not be carried out as a routine in children with cerebral palsy, but only after clinical selection or as part of a research programme. The position is made more difficult by the fact that different authorities inevitably employ slightly differ- ent clinical criteria: while the diagnosis of hemiplegia is clear enough, many cases of infantile hemiplegia will, on closer exami- nation, prove to have minimal abnormali- ties on the supposedly normal side, and it is a matter of choice whether these are accepted as hemiplegics or as grossly asymmetrical quadriplegics or triplegics. Similarly, some authors restrict the term athetosis to the relatively uncommon syndrome of choreoathetoid movements with hypotonia, while others use it with less discretion for cases of quadriplegia with more or less in the way of involuntary movements or fluctuations of tone. In general, however, there are some accepted broad correlations--e.g,. that between the extent of cortical as opposed to basal damage and the incidence of epilepsy and of mental retardation-and there is a largely assumed correlation between the extent of cortical damage and the degree of abnormality of the EEG, though there are certain notable exceptions where the lesion involves subcortical white matter,
_ _ _ ~ ~ Centre for Spastic Children, 61 Cheyne Walk, Chelsea, London S.W.3.
287

DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1968, 10
for in such cases there may be no correla- tion between the EEG and the mental state and the prognosis. Thus Perlstein el a/. (1917) found an incidence of epilepsy of 86 per cent in their spastic cases, but only 12 per cent in the athetoids, whereas Aird and Cohen (1950) found that 66 per cent of their spastic group had fits, as opposed to 34 per cent of the athetoid group; a further breakdown of the spastic group seems to have little to offer. Crothers and Paine (1959) found that the EEG was abnormal in 75 per cent of hemiplegics, of whom over half had fits; it was abnormal in 5 7 . 5 per cent of cases of ‘spastic cerebral palsy’: but also in no less than 48.5 per cent of cases of ‘extrapyramidal syndromes and mixed cerebral palsy’. Skatved (1956) found that 60.6 per cent of 370 cases had abnormal EEGS; the reported incidence of epilepsy was very low (22 per cent), perhaps because of incomplete clinical information. She found no definite relationship between the incidence of epilepsy and the clinical severity of the physical state. Gordon (1962) thought that the correlation was poor between the type of cerebral palsy, the incidence of epilepsy and the degree of abnormality seen in the EEG, though his figures for all his clinical groups (hemi- plegia, quadriplegia, diplegia, athetosis and ataxia) showed quite clearly that when fits have occurred the EEG is much more often abnormal than when fits have not occurred. In other words the EEG is a fairly sensitive indicator of epilepsy. Nevertheless, 33 per cent of his epileptic cases had normal EEGS, though it is not clear whether the criterion of normality of the EEG was based on one or on several records. He con- cluded that the presence or absence of epileptic activity in a single EEG may be of no particular significance in relation to the occurrence of epilepsy.
Gibbs et nl. (1963) attempted to establish the predictive value of the EEG in cerebral palsy. They studied 324 patients usually
seen first before the age of three years, and who had not had fits. They found that a normal EEG under the age of two years is of less predictive value than a normal EEG over this age, whereas a normal EEG after five years is virtually a guarantee that fits will not occur. (‘Among our cases seizures did not develop in any children with normal EEGS after the age of five’). Thus, if the EEG was normal up to two years, the ultimate incidence of epilepsy was 18 per cent and if it was normal beyond two years, the incidence was only 2 per cent; if nega- tive spikes occurred under the age of two the incidence of epilepsy was 56 per cent, whereas if negative spikes occurred over the age of two, the incidence was 40 per cent. Some may disagree with their inter- pretation of the EEG, though from their studies it would appear that the predictive value of the EEG in cerebral palsy, so far as epilepsy is concerned, is greater than in any other clinical condition. One difficulty perhaps arises from the fact that Gibbs et al. confined their attention to positive EEC abnormalities--spikes, etc.-and paid little attention to negative findings-low voltage records, or the suppression of normal rhythms over areas of supposed atrophy. Woods (1965) studied 206 cases with 382 records. noting again the higher percentage of abnormalities in the hemi- plegic and diplegic groups than in cases with principal involvement of the basal ganglia. Though observing the close corre- lation between the abnormality of the EEG and the development of epilepsy, she warned that a poor prognosis should never be based on the EEG alone, since the EEG may be abnormal in the absence of epilepsy or of any evidence of clinical deterioration. She drew particular attention to low volt- age or electrically silent EEGS in cases of athetosis. This finding had not been com- mented on by other authors and is difficult to evaluate without further information about the state of apprehensiveness of the
288

JOHN FOLEY
subjects concerned. Woods commented that the records did not tend to change to any significant degree over the years, a fact which supported the supposedly static nature of the underlying lesion. She found that deterioration in the EEG occurred in only 7 cases out of 206, and that in 6 of these there was no evidence of any physical deterioration in the patients.
All are agreed that a single record is of little diagnostic or prognostic significance. This paper is concerned with the nature and significance of the changes seen in serial records of cases of cerebral palsy studied in a single clinic over a number of years, and the study was prompted by the impression that not only did the EEG seem to predict epilepsy in these cases, but it also seemed in some cases to exhibit a progres- sive deterioration which has not often received comment before.
Classification In order to assess deterioration in the
EEG it is necessary to classify records. Lundervold (1960), who observed the in- creasing incidence of abnormal EEGS in his cases with age, 61 per cent of the older cases having abnormal records as opposed to only 14 per cent of the young cases, classified his records into three groups-( 1) focal and bifocal dysrhythmias, including spikes, sharp waves, delta and theta activity and reduction of activity; (2) generalised dysrhythmias, slight or moder- ate in degree; and (3) bilateral synchronous spikes or sharp-slow waves. Gordon (1962) classified his records into five groups-(1) normal, (2) generalised dysrhythmia, (3) focal slow activity, (4) focal spikes-sharp activity, and (5) generalised ‘epileptic’ activity, though the distinction between generalised ‘epileptic’ activity and general- ised dysrhythmia is not clear, and is pre- sumably quantitative rather than qualita- tive. So insecure is the neurophysiological basis of the EEG that it is extremely difficult
to devise a classification which will prove scientifically acceptable, but it is practical and quite logical to classify EEGS as in- different, bad in parts, or thoroughly bad, while making certain provisos-namely that the EEG must be interpreted in relation to the age and the expected maturation of the child, and that it may be wholly un- informative if cortical atrophy is complete or if the damage is purely subcortical. We have, therefore, classified our records into the following six groups :
(1) Normal. (2) Slightly or non-specifically abnormal. (3) Focal (positive or negative) with one
(4) Focal, with two or more foci. (5) Paroxysmal dysrhythmia with or
without several foci. (6) Paroxysmal dysrhythmia but show-
ing certain ominous features such as periodic repetition of stereotyped discharges and so-called hypsarrhy- thmia.
focus.
Epilepsy and Serial Records This study is concerned with changes
seen in the serial records of children who have attended the Centre for Spastic Children, Chelsea. Though these cases total over 500, not all cases were acceptable as examples of cerebral palsy, not all attended regularly over a number of years, and only those from whom satisfactory serial records are available have been included. Acceptance of these criteria reduced the number to 165 cases, with 498 records. Since this study is retrospective there is considerable variation in the intervals between records, and also in the length of time over which the cases were observed (Fig. 1).
In 62 cases there were two sets of com- parable records, 58 had three, 23 had four, and 22 had five or more records ; 67 cases were under the age of 3 years at the first recording (Fig. 2). The final prevalence of
289

DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1968, 10
hlOZIh3
7 3 - a4
61 - 7 2
4 9 - 60
25-36-
0 Cases without f i t s
Cases w i t h f i t s
Months
6 - 7
13 - 24
0 - 12
Number 5 10 15 20 25
Fig. 1. Period of observation.
epilepsy in the main clinical groups is shown in Table 1.
i n brief, about half the cases in these groups, with the exception of the athetoid, have epilepsy.
Table I1 shows the number of cases with initially normal or abnormal EEGS and the number of cases showing deterioration in the records, deterioration in this sense being independent of whether the first record was normal or abnormal, and
TABLE I Cases According to Diagnosis and Incidence of
Epilepsy
Spastic diplegta . . 31 18 13 48
Spastic quadriplegia 71 31 40 56 and triplegia
Athetoid . 25 22 3 12
Herniplegla 24 9 15 63
Ataxia . , 14 7 7 50
165 87 78 -
4-5E== 3 - 4
2 - 3
0 - 1
l - r N u m b e r Fig. 2. Age 10 at first 15 EEG. 20 ’ 25 I
depending only on whether the later records were classified lower on the scale than the earlier ones. (In Tables I and I1 records in both Category I and Category 11 were accepted as ‘normal’. Deterioration could thus involve a change from the two top categories downwards, or an initially abnormal record might become more abnormal). From this it can be seen that initially normal records outnumbered initi- ally abnormal ones by nearly two to one; but in 61 of 165 cases (37 per cent) the serial EEGS showed deterioration. If the cases of athetosis are removed, since they have the least abnormal records, the lowest incidence of epilepsy and the least evidence of deterioration in the records, it is found that in the remainder, 37.5 per cent of the cases have initially abnormal records, and 39 per cent show deterioration in the EEGS,
bringing the proportion of finally abnormal records in these groups to 60.5 per cent. If one takes the same groups (spastic and ataxic, as opposed to athetoid), it is found that those with epilepsy outnumber those without it by 75 to 65, suggesting that deterioration in the EEG is not always indicative of epilepsy. The trend towards
290

JOHN FOLEY
normal abnormal abnormal
TABLE I1 Cases with Initially Normal or Abnormal EEGs, and Cases Showing Deterioration
11 I 3
107 I 58
Diplegia . . . . Quadriplegia, triplegia
Athetoid . . ..
Hemiplegia . . .. Ataxic . . . . 7
92
Total
With epilepsy (78) 1 19 59 16
Without epilepsy (87) 55 32 36.5 -
91 , 74
31
71
25
24
14
165
I I
41 1 30 I 42
21 4 7
1 1 ~ 13 1 19
deterioration in the EEG is definite in all but the athetoid groups.
Deterioration in serial records is in fact not confined to children with ‘brain damage’, for in a separate series of 78 epileptic children without any abnormal physical signs, and whose records were classified in the same manner, deterioration in the serial EEG occurred in 36.5 per cent. Tables I and I1 show that the incidence of a finally abnormal EEG is higher than the incidence of epilepsy itself. It may well be, of course, that with a more prolonged period of observation the incidence of epilepsy might approach the incidence of abnormality in the EEG, but we are here concerned with the prognostic value of the EEG within a reasonable period of months. Actual improvement in the EEG occurred in only 17 cases-once a record had become abnormal it tended to remain so.
abnormal EEG
55
59
28
79
50
57
No. of cases showing deterioration
in records
12
26
6
12
5
61
The proportion of cases, epileptic and non-epileptic, with norma1 and abnormal EEGS is set out in Tables 111 and IV, in which an attempt has been made to find out whether a ‘mildly abnormal’ record has anything other than a subjective meaning. In Table 111 the ‘normal’ records include those in both Category I and Category 11 --i.e., undoubtedly normal records and also records thought to be mildly or non- specifically abnormal, whereas in Table 1V these records of Category I1 have been treated as abnormal. The relationship between the abnormal EEG and epilepsy is significant, x2 being 23.55 for Table I11 and 29.125 for Table IV. The EEG is abnormal in over three-quarters of the cases with fits; but if a child does not develop fits there is a very considerable chance of his having an abnormal EEG. The EEG thus tends to confirm the occurrence
B

DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1968, 10
TABLE 1V EEG in Relation to Epilepsy
, h'ornial EEG Abtiortnal EEG
Category I including Abnormal , only Category I1 _____ ______ _______
With epilepsy (78) 8 70 90
Without epilepsy (87) 44 43 49 5 ________ __-- ~
52 1 I3
o f epilepsy rather than to diagnose it. The inclusion of Category I1 records in the abnormal group does not make a signifi- cant difference to the final figures (z2 = 0 I 14), for it increases the proportion of abnormal EEGS in both the epileptic and non-epileptic groups about equally.
In other words subtle phenomena in the F i x ; are not of great importance: the EEG
i n these children is either normal or ob\iously abnormal and little is to be gained by verbosity or equivocation in the report. This at least is a useful conclusion. Anticonv~ilsants in these cases did not appear to alter the nature of the records to a significant degree. There can be little doubt from the present study that deteriora- tion in serial records can occur in a child \ tho is not epileptic and is not going to have fits within the foreseeable future. though it is also true that an abnormal record and deterioration in serial traces are commoner amongst the epileptic. Table V shows that 37 per cent of all the cases show deterioration in their EEGS; of those who do not have fits, 32 per cent show deterioration in their EECS: amongst those who have fits or eventually develop them, the incidence of deterioration in the serial records is admittedly higher, namely 43.5 per cent but this difference is not statistically significant (z* -= 1 .82. not significant at p =: 0.05). The fact emerges that deterioration in the EEG can occur in non-epileptic cases, or cases not known to %e epileptic so far as our limited period of
observation goes. There is also no differ- ence in the age at which the EEG deteriora- tion occurs between cases with and without eventual epilepsy, the age of maximum change seeming to be the third and fourth years in both groups. The significant relationship is that between epilepsy and the abnormal EEG: a change for the worse in the records does not seem to mean much. Thus 76 per cent of the cases with fits had finally abnormal EEGS, while of the cases who did not develop fits 36.5 per cent nevertheless had abnormal EECS.
Taking all the cases with finally normal EEGS (Category I and Il), 25 per cent had fits, while of those with finally abnormal EEGS 65 per cent had fits.
We cannot agree with Gibbs el al. (1963) that a normal EEG after the age of 5 years is virtually a guarantee against epilepsy. If we take Category I and I1 records as being normal, there are 55 cases with normal
TABLE V Deterioration in the EEGs in Cases with and without
Epilepsy
With Without deterioration deterioration
in EEG in EEG
Cases without fits . . . . 28 59
Cases with fit5 34 I 44 ~
I fits . . . . 28 i 59 I Cases without
I Cases with fit5 ~ 34 I 44 I
With Without deterioration deterioration
in EEG in EEG
y.? = 1.82, no t significant at p = 0.05.
292

JOHN FOLEY
records over the age of 5 years and 33 per cent of these developed fits. Restricting the designation ‘normal’ to Category I records only, there are 37 of these over the age of 5 years and 19 per cent had or developed fits-in other words a normal EEG after 5 years is little more of a safeguard against epilepsy than a normal record before this age.
Clinical Deterioration Deterioration in the serial records has
not been a spectacular feature in the 24 cases which have shown physical or mental deterioration; 14.6 per cent of cases with deteriorating records showed actual physical or mental deterioration; in cases without deterioration in the records the incidence of physical or mental deteriora- tion was 15.2 per cent, the important fact bzing that 1 in 7 of these children showed physical or mental deterioration. The numbers are too small to be of statistical value, but half of the cases showing physical deterioration died, and only 6 showed a downward trend in the serial records. Cases with both physical and mental deterioration showed a slightly higher incidence of abnormal EEGS. Of the 8 children who died, 4 had normal records. Deterioration in the EEG cannot therefore be relied upon to forecast physical deterio- ration or even a fatal outcome, though there are of course examples of very striking physical and mental deterioration in some children who have fits, as the following case illustrates:
T.S., Case 318, born 28.4.57: a girl with spastic diplegia; there was no family history of epilepsy, though her father had a small facial naevus. Born at 34 weeks she weighed 34 Ib. (1.58 Kg.), was cared for in an incubator for a week, and had four cyanotic attacks. At 2$ she showed minimal involvement of the hands and moderate spastic weakness of the legs, and could sit without support, though she could not crawl. She had plenty of words, but did not yet use sentences. Her intelli- gence seemed to be within normal limits. The EEG was abnormal with excessive fast activity and spike-slow activity in the occipital areas. Three
months later she had her first fit. Another followed six months later. The EEG became more abnormal, with bilateral parietal spikes. At 4 years 3 months she was a bright happy child with an IQ of 86, imaginative in her play, with normal speech and a good ear for sound and rhythm. Her hands were almost normal, her legs moderately spastic, though she was still not crawling, partly because of a sub- luxated hip. She then had a number of fits, and on emerging from hospital she was a completely different child, shrieking and biting; in desperation her mother, previously solicitous, demanded institutional care. There was virtually complete loss of speech, she could no longer sing, and was intractable and negativistic; the right arm was weak and there was a peculiar rigidity of the arms, particularly the left, which were now in a position of slight flexion while the spasticity of the legs had increased. The EEG had, if anything improved. Her IQ fell to 57; by the age of 44 years it was 60; her speech was largely automatic, often meaningless. By 5 years there had been no further physical or mental progress though her fits had remained controlled.
In contrast there may occur a striking physical deterioration leading even to death, without any mental change, epilepsy or alteration in the EEG, and cases of this kind suggest that the underlying process is a slowly progressive subcortical disease.
One cannot deny that epilepsy (or its treatment) may have a deleterious effect on a child’s mental and physical development, for we have had experience of several such cases at the Centre. But it so happens that in the limited series of cases included in the present study it has not been possible to forecast such deterioration or to link it with any specific change in the EEG.
EEG, Intelligence and Physical Disability It is somewhat surprising to find that in
this series an abnormal EEG is only slightly more common in the lower IQ groups than in the higher ones (Table VIa), and that deterioration in the records occurs most commonly in the groups with an IQ above 80-perhaps because these have furthest to fall. It would thus appear that in the fairly short period of observation available in our cases, the EEG, whether it shows deterioration or not, bears practically no relationship to the intelligence of the child -a finding which seems contrary to all
293

DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1968, 10
I . Q . 0-20 20-40 40-60 60-80 1 80-100 100- _ _ _ _ _ _ _ _ _ _ _ _ ~ _ _ _ _ _ _. - ___ __.__
", u i t h ,ibnornidl EEG . . 69 62 59 48.5 53.5 57
" , Mith fits . . . . . . 64 67 1 62 41 42 I 23
previous series (Table Vll), except that of is the greatest disparity between the Gordon (1962). On the other hand the incidence of epilepsy and of abnormalities incidence of epilepsy (sooner or later) is in the final EEG. This can be seen most lowest in the group with the highest intelli- clearly by comparing the group of dull gence (Table Vlb) and comparison of the children with IQ 60-80 with the group of percentages in Table VIc shows that it is bright children with IQ 100-+. Of the dull in this group of bright children that there children, 17 had abnormal records and 18
I I . Q . Range
TABLE VI a. I.Q. and the EEG
I I.Q. Range -~ ~-
0-20 ~ 20-40 40-60 60-80 80-100 100+ - ___ _ _ ~ _ _ ____ _ ~ _ _ _ _ _ _ _ _ _ _ _
EEG finally abnormal . . 9 13 13 17 1 23 17 , EEG finally nornial . . 5 8 9 18 20 13
(' , abnormal EEGs . . . . 69 62 59 48.5 I 53.5 57
(Category I and 11)
b. I.Q. and Epilepsy
I . Q. 0-20 20-40 4C60 60-80 80-100 100+ __ - _ _ _ _ ~ _ _ _ _ ~ _ _ _ _ _ _ _ _ _ _ _ _ _ ~ -____- Total cnses . 14 21 21 36 1 43 30
With fits 9 14 13 17 18 7
" , v, ith fits 64 67 62 47 42 23
c. I.Q., Epilepsy and abnormal EEG
TABLE V11 Final I.Q. and the Deteriorating EEG
___ - __ ~~ ___- _____ 0-20 2040 40-60 60-80 80-100 100 .-
- ~ - _ _ ~ - - _ _ - - - - _ _ _ _ - ~ - _ ~ ~ _ ________ Deteriorating EEG . 4 7 5 I2 16 18
Non-deteriorating EEG I
" ~, deteriorating . . .. 28 5 3 3 . 3 22 7 34 2 37 60
\\hether normal or abnormal 10 14 17 23 ~ 27 12
I I
294

JOHN FOLEY
had normal ones. Five of the children with normal records (27 per cent) had or developed fits, while 11 of the 17 cases with abnormal records (65 per cent) had fits. Amongst the bright children, 17 had abnormal final records and 13 had normal ones. Of the 17 cases with abnormal records 7 (or 41 per cent) had fits; but of the cases with normal records none had fits. The age at which the fits developed did not differ materially in the two groups, but there was a slight difference in the degree of abnormality seen in the records of the two groups. In each group there were 17 cases with abnormal final records, but among the dull children 12 of these 17 fell into the lowest three EEG categories- i.e., IV-VI-while among the bright children only 5 of the 17 final records fell into these lowest categories : the abnormal- ity seen in the dull children tended to be more severe than that encountered in the bright children. The important fact which emerges is that, although a bright child with an abnormal EEG may have fits, one can be confident that a bright child with a normal series of records will not have fits (Fig. 3).
0 8 ,\* 0-20 20-40 40-60 60-80 80-100 >lo0
10 range
Fig. 3. Epilepsy, Intelligence and the EEC.
It is difficult to explain why in cases with normal EEGS the relationship is not linear in the lowest IQ group, but above the IQ of 40 the incidence of epilepsy seems to be
directly related to low intelligence, whether the EEG is normal or abnormal.
The triangular relationship between intelligence, the degree of physical dis- ability and abnormality in the EEG is worthy of further consideration. One would expect the degree of abnormality in the EEG to depend on the extent of the cerebral lesion and therefore to be related to the degree of physical disability, except in cases where the damage has fallen most heavily on the basal ganglia--i.e., cases of pure athetosis. The diagnostic categories so far used-diplegia, quadriplegia, etc.-do not bear a precise relationship to the actual severity of the disability: a quadri- paresis can be minimal, a diplegia severe. For this reason the cases were all re- classified with the help of the therapists on the staff according to the physical disability (the functional diagnosis) instead of accord- ing to diagnoses by the motor disorder (the physiological diagnosis), using a 6-point scale ranging from I (minimal disability) down to VI (totally dependent). In Table VlIl physical disability is related to the six grades of intellectual attainment. In general the greatest physical incapacity is associated with the lowest intelligence, though exceptions occur in the IQ 100-1- group, in which fairly severe incapacity can be associated with high intelligence- reassuring evidence, admittedly hardly necessary these days, that special facilities are required for a proportion of children with cerebra1 palsy. The relation between the EEG and the severity of the physical disability is shown in Table IX. Abnormal EEGS are distributed fairly evenly amongst the six grades, though the highest propor- tion of finally abnormal records is, rather unexpectedly, found in the cases with the slightest physical handicap. These are in fact, cases where one assumes that the amount of cortical damage is least (though it might be argued that cases with the most severe physical disability may
295

IXVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1968, 10
TABLE VlII Intelligence and Physical Disability
loo - 6 12 4 1 5 3 80-100 I 6 8 10 13 4
40- 60 2 4 4 3 7 .. 20 40 6 9 5 0- 20 10 2 1 .. . .
ho- 80 2 2 1 2 1 7 l 9 I
I
TABLE 1X Physical Grade and EEG
~ Physical Grade
I-?--- 1 VI 1 v 1 I V \ 111 , I
N o finally abnormal ’ 13 1 13 27 1 10 22 ~ 7
___~___ EEG I
- -~~ __ ___ ~ _ _ _ ~ _ _ _ _
N o . finally normal . . 9 17 16 ‘ 15 14 - 7
abnormal. . . 59 43 5 63 ~ 40 61 78
-_ - __ _________ I-- ___-- I
N o deteriorating . . 5 9 19 6 * 16 6
44 60 ‘Ig, deteriorating . , . . 22.5 30 44 1 24 1
TABLE X Epilepsy and Physical Disability
I Phjsical Grade
1 VI _ _ ~ _ _ _ _
v I I V I 111 I If 1
No with fits . 1 16 1 10 15 1 12 1 19 5 _ _ ~ _ _ ~ _-__ - -_ __-I__ - -___
1
N o uithout fits . . I 6 20 28 13 17 4
u o with fits . 73 33 3 1 5 3 . 5 1 48 I 53 55 .6 I 1
I I
have mainly subcortical damage, and that In view of this unexpected finding it is damage to the basal ganglia perhaps exerts necessary to examine the relationship a ‘protective’ egect on the cortex so far as between the degree of physical disability the development of an abnormal EEG is and the occurrence of epilepsy. Table X concerned). The incidence of deterioration shows that the cases with maximal physical in serial records is also highest in the cases disability do in fact have the highest with the least physical disability. incidence of epilepsy, but even in the top
296

JOHN FOLEY
Non-epileptic cases .. I 43
! Epileptic I cases . . 1 32
I
three grades--i.e., including cases with slight or minimal disability-the incidence is round about 50 per cent.
Hitherto we have considered only striking abnormalities in the EEG, and only definite deterioration in the nature of the record--i.e., a change from category 111 downwards-and the results have been so equivocal as to cast serious doubts on the value of the EEG as a prognostic investiga- tion. Further consideration of slighter changes in the EEG therefore seems justifi- able and in the following section all records in and below category J1 are con- sidered abnormal, and any change even from category I to category I1 is regarded as a deterioration in the EEG. Category I is normal and category 11 is diffusely but mildly or non-specifically abnormal--i.e., without spikes or striking patterns. The change is subtle. Even if these slight changes are included, the difference be- tween the epileptic and non-epileptic cases remains insignificant, deterioration in the EEG occurring in 55 cases without fits as opposed to 42 cases with fits, while a static EEG occurred in 34 epileptic cases and 34 non-epileptic cases. In general, however, subtle abnormalities in the EEG did not occur in the epileptic cases-these had either normal or frankly abnormal records.
Another way of looking at the problem is to consider the number of EEGS that actually show improvement with the years in the epileptic and non-epileptic cases : and once again there is no difference be-
38
4 4 . 5
12 34
34 10
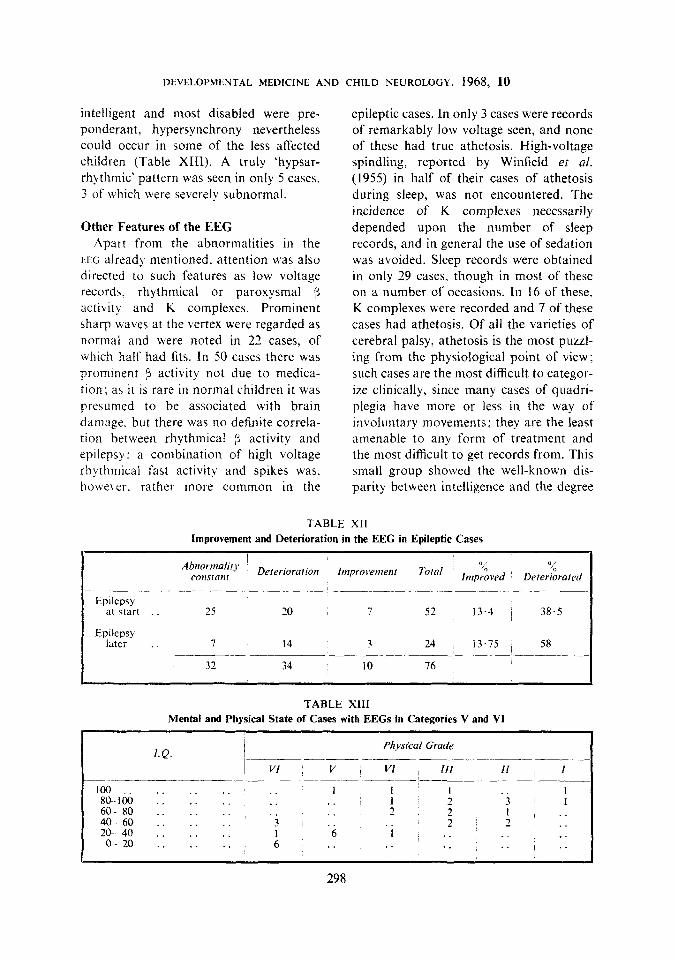
tween them (Table Xt). If, however, one considers the epileptic group alone, divid- ing it into cases that had fits before the first EEG and cases who developed fits during the period of observation, it is apparent that, although improvement in the EEG is equally uncommon in the two groups, deterioration in the EEG is con- siderably more common in the cases which developed fits during the period of observa- tion than in the cases who had fits at the start (Table XII).
Within the epileptic group--i.e., the group that has or ultimately develops fits-there appears to be some evidence that deterioration in serial records indicates that fits will occur, for deterioration is more common in the cases which are going to have fits than in those which have a fit before the first recording, but this informa- tion is of no value if one is merely pre- sented with a set of serial records showing EEG deterioration, because the difference between the non-epileptic and the ultim- ately epileptic cases is not statistically significant.
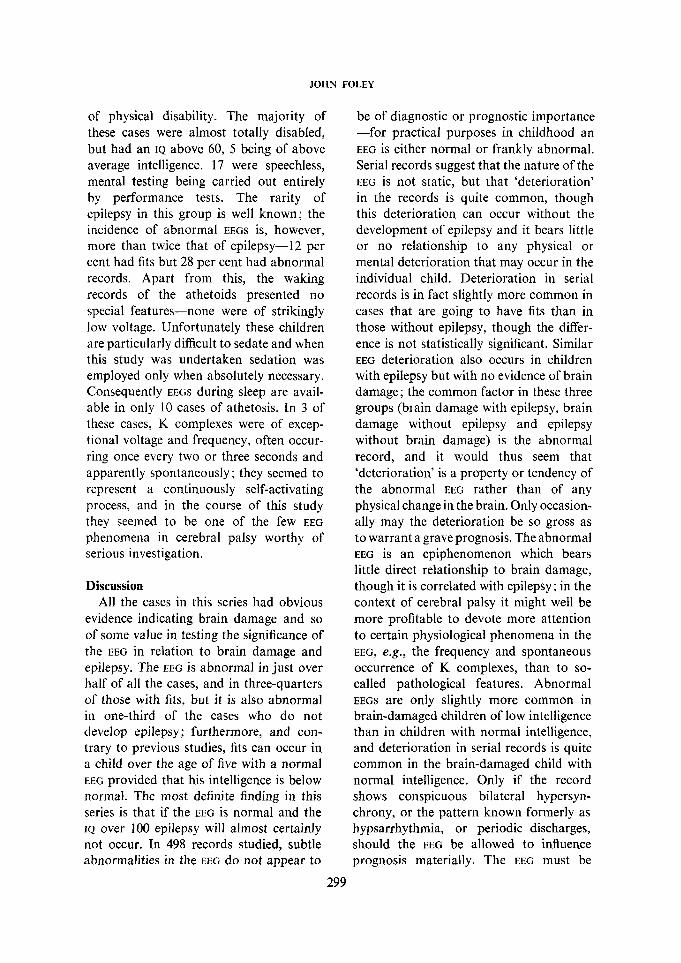
EEGs of Category V and VI There were 37 cases in which one or
more of the records were extremely abnormal and fell into the bottom two categories; in 7 of these there was sub- sequent improvement, but the remainder suggest that if bilateral hypersynchrony is achieved it tends to be permanent. Of the 37 cases, 28 had fits. Although the least
TABLE XI Improvement and Deterioration in the EEG of Epileptic and Non-Epileptic Cases
297
DEVELOPMENTAL MEDICINE AND CHILD NEUROLOGY. 1968, 10
intelligent and most disabled were pre- ponderant, hypersynchrony nevertheless could occur in some of the less affected children (Table XIII). A truly 'hypsar- rhythmic' pattern was seen in only 5 cases. 3 of which were severely subnormal.
Other Features of the EEG Apart from the abnormalities in the
LEG already mentioned, attention was also directed to such features as low voltage records, rhythmical or paroxysmal 3 activity and K complexes. Prominent sharp waves at the vertex were regarded as normal and were noted in 22 cases, of which half had fits. In 50 cases there was prominent 9 activity not due to medica- tion: as i t is rare i n normal children i t was presumed to be associated with brain damage. but there was no definite correla- tion between rhythmical 7 activity and epilepsy: a combination of high voltage rhythmical fast activity and spikes was, howr\,er. rather more common in the
epileptic cases. In only 3 cases were records of remarkably low voltage seen, and none of these had true athetosis. High-voltage spindling, reported by Winfield et al. (1955) in half of their cases of athetosis during sleep, was not encountered. The incidence of K complexes necessarily depended upon the number of sleep records, and in general the use of sedation was avoided. Sleep records were obtained in only 29 cases, though in most of these on a number of occasions. L n 16 of these, K complexes were recorded and 7 of these cases had athetosis. Of all the varieties of cerebral palsy, athetosis is the most puzzl- ing from the physiological point of view ; such cases are the most difficult to categor- ize clinically, since many cases of quadri- plegia have more or less in the way of involuntary movements; they are the least amenable to any form of treatment and the most difficult to get records from. This small group showed the well-known dis- parity between intelligence and the degree
TABLE XII Improvement and Deterioration in the EEG in Epileptic Cases
Abnorr'laiits Deterioration Improvement Total Inlp~oved '0 "', consfnnf
tp1lepsy at start . . 25 10 7 52 13.4 ~ 38.5
I Epilepsy later . . 7 14 3 24 13.75 58
32 34 10 I 76
TABLE XI11 Mental and Physical State of Cases with EEGs in Categories V and VI
Physical Grade ____________ __-_-_ ~ _ _ _ I.Q. I
I- VI , V 1 VI Ill I1 ~ I -__I_ ____-~~____________I_ .- -~.
100 . . . . . . . . 1 I I . . 1 80-100 . . .. . . . . . . 1 3 1
40- 60 . . . . . . 3 , . . 2 2 . . 20 40 . . . . . . 1 6 1 .. .. .. 0 20 . . . . . . 6 . . . . . . . . . .
60- 80 .. . . . . . . . . 2 2 l 2 I , . .
,
298
JOHN FOLEY
of physical disability. The majority of these cases were almost totally disabled, but had an IQ above 60, 5 being of above average intelligence. 17 were speechless, mental testing being carried out entirely by performance tests. The rarity of epilepsy in this group is well known; the incidence of abnormal EEGS is, however, more than twice that of epilepsy-I2 per cent had fits but 28 per cent had abnormal records. Apart from this, the waking records of the athetoids presented no special features-none were of strikingly low voltage. Unfortunately these children are particularly difficult to sedate and when this study was undertaken sedation was employed only when absolutely necessary. Consequently EEGS during sleep are avail- able in only 10 cases of athetosis. In 3 of these cases, K complexes were of excep- tional voltage and frequency, often occur- ring once every two or three seconds and apparently spontaneously ; they seemed to represent a continuously self-activating process, and in the course of this study they seemed to be one of the few EEG
phenomena in cerebral palsy worthy of serious investigation.
Discussion All the cases in this series had obvious
evidence indicating brain damage and so of some value in testing the significance of the EEG in relation to brain damage and epilepsy. The EEG is abnormal in just over half of all the cases, and in three-quarters of those with fits, but it is also abnormal in one-third of the cases who do not develop epilepsy; furthermore, and con- trary to previous studies, fits can occur in a child over the age of five with a normal EEG provided that his intelligence is below normal. The most definite finding in this series is that if the EEG is normal and the IQ over 100 epilepsy will almost certainly not occur. In 498 records studied, subtle abnormalities in the EEG do not appear to
be of diagnostic or prognostic importance -for practical purposes in childhood an EEG is either normal or frankly abnormal. Serial records suggest that the nature of the EEG is not static, but that ‘deterioration’ in the records is quite common, though this deterioration can occur without the development of epilepsy and it bears little or no relationship to any physical or mental deterioration that may occur in the individual child. Deterioration in serial records is in fact slightly more common in cases that are going to have fits than in those without epilepsy, though the differ- ence is not statistically significant. Similar EEG deterioration also occurs in children with epilepsy but with no evidence of brain damage; the common factor in these three groups (bIain damage with epilepsy, brain damage without epilepsy and epilepsy without brain damage) is the abnormal record, and it would thus seem that ‘deterioration’ is a property or tendency of the abnormal EEG rather than of any physical change in the brain. Only occasion- ally may the deterioration be so gross as to warrant a grave prognosis. The abnormal EEG is an epiphenomenon which bears little direct relationship to brain damage, though it is correlated with epilepsy; in the context of cerebral palsy it might well be more profitable to devote more attention to certain physiological phenomena in the EEG, e.g., the frequency and spontaneous occurrence of K complexes, than to so- called pathological features. Abnormal EEGS are only slightly more common in brain-damaged children of low intelligence than in children with normal intelligence, and deterioration in serial records is quite common in the brain-damaged child with normal intelligence. Only if the record shows conspicuous bilateral hypersyn- chrony, or the pattern known formerly as hypsarrhythmia, or periodic discharges, should the EEG be allowed to influence prognosis materially. The EEG must be
299

DEVELOPMENTAL MEDICINE A N D
looked at critically and, as has often been said before, must not be regarded as a machine for making a diagnosis. This of course is not the same as saying that it has no diagnostic value. for there is no doubt that there is a high correlation between very abnormal EEGS and a poor prognosis in terms of mental and physical develop- ment. Indeed there are occasional cases in which a very abnormal EEC can alter a diegnosis; it sometimes happens that in infancy or early childhood a syndrome of in\oluntary movements is thought to be atlletoid, though the nature of the record may suggest that the movements are in fact due to multiple myoclonus. There is a further conclusion that can be tentatively draun. While there is no denying that the abnormal EEG indicates extensive cortical damage. the lack of correlation between the EEG and the physical and intellectual state of the child in so many cases suggests that in the context of diffuse pathology the .xig!pllifiwiii lesion may not be the one that is electrophysiologically obvious ; and it follows that many of the motor phenomena of cerebral palsy are due to extrapyramidal rather than to cortical lesions, although the pathological process involves both.
This investigation was started on the nssuniption that deterioration in serial records heralded epilepsy and that fits necessarily resulted in physical or mental deterioration. On closer examination these assumptions have not been proved entirely correct, though it is not denied that very frequent fits may cause further serious brain damage. The prognostic import of an abnormal EEG or of a change for the worse in a series of records is not definite enough to justify the use of anticonvul- sants, except where fits are known to have occurred, though a deteriorating series may sometimes serve as a warning of coming epilepsy. Only if a child’s IQ is high can a normal record be accepted as a virtual guarantee that epilepsy will not
CHILD NEUROLOGY. 1968, 10
develop; but it is also in this group that the EEG may be persistently abnormal without fits occurring, and the present investigation fully supports Grace Woods’ (1965) warn- ing that the prognosis in a case of cerebral palsy should rarely be influenced by an abnormal FEG.
Disappointing though it may have been, this study is of some interest in relation to the child without cerebral palsy who is found to have an abnormal EEG. It must surely be agreed that if the prognostic significance of a series of abnormal records in a child with ecident brain damage is so indefinite, then there can be little justifica- tion for the prophylactic exhibition of anti- convulsants on the evidence of the EEC
alone in a child without neurological abnormalities, unless fits have actually occurred : in other words it is the child who must be treated and not his EEG.
This critical appraisal of the EEG in relation to chronic brain damage is not intended to invalidate this method of investigation in paediatric neurology in general. All diagnostic tests can on occasion be misleading and so it is important to study their correlations closely. There are of course many conditions in childhood in which the EEG may be of decisive value-in cerebral abscess, after cardiac arrest, in the diagnosis of infantile spasms, obscure minor attacks, petit ma1 status masquerad- ing as a confusional state or autism, niyoclonic status presenting as ataxia, and in subacute sclerosing leucoencephalitis and the lipidoses, to mention only a few. l n connection with chronic and non- progressive brain damage, however, it is clear that the EEG must be interpreted with caution, and that it is only of value if correlated with a detailed knowledge of the clinical state.
Acknowfedgements. I would like to acknowledge the valuable help given by Miss Annabelle Newton and Mrs D. Vince, recordists at the Centre for Spastic Children, and members of the M.R.C. Unri at Graylingwell Hospital for their criticism and advice.
300
JOHN FOLEY
SUMMARY 498 serial EEGS in 165 cases of cerebral palsy have been studied. The EEG in cerebral
palsy is not static but shows a tendency to deterioration. While there is a positive correlation between the abnormal EEG and epilepsy, the relationship between deterioration in the EEG
and the development of epilepsy is not statistically significant. The degree of abnormality of the EEG bears little relationship either to the intelligence of the child or to the presumed degree of brain damage as judged by physical disability, though there appears to be a relationship between the intelligence of the child and resistance to fits despite an abnormal record.
RESUME De‘tkrioration de ~ ’ E E G chez les enfants atteints d’injirmite‘ motrice chrkbrale
498 EEG en sCrie longitudinale dans 165 cas d’infirmitC motrice cCrCbrale out CtC ttudiC Dans I’infirmitC motrice drtbrale, ~’EEG n’est pas stable mais tend h se dCtCriorer. Tandis qu’il y a une corrClation positive entre I’EEG anormal et l’tpilepsie, la relation entre la dCtCrioration de ~’EEG et le dtveloppement de 1’Cpilepsie n’est pas significative au point de vue statistique. Le degrd d’anormalitt de I’EEG a peu de rapport avec l’intelligence de l’enfant ou avec le degrC prCsumC de dommage ctrtbral jug& par l’infirmiti physique, mais il semble y avoir une relation entre l’intelligence de l’enfant et sa rtsistance aux crises malgrC un enregistrement anormal.
ZUSAMMENFASSUNG Verschlechterung der Elektroencephalogramme von Kindern mit Cerebralparese
Es wurden 498 Elektroencephalogramme von 165 Fallen mit Cerebralparese untersucht. Das EEG bei Cerebralparese ist nicht statisch, sondern neigt zur Verschlechterung. Wahrend zwischen dem abnormen EEG und der Epilepsie eine positive Korrelation besteht, ist die Beziehung zwischen Verschlechterung des Elektroencephalograms und der Entstehung einer Epilepsie statistisch nicht signifikant. Der Grad der EEG-Abnormitat hat weder zur Intelligenz des Kindes noch zu dem nach der physischen Behinderung ermittelten Grad der Cerebralparese eine signifikante Beziehung. Es scheint aber eine Beziehung zu bestehen zwischen der Intelligenz des Kindes und seiner Resistenz gegen Anfalle trotz eines abnormen EEG-Befundes.
REFERENCES Aird, R. B., Cohen, P. (1950) ‘Electroencephalography in cerebral palsy.’ J. Pediat., 37,448. Crothers, B., Paine, R. S. (1959) The Natural History of Cerebral Palsy. Cambridge, Mass.: Harvard
University Press. Gibbs, F. A , Gibbs, E. L., Perlstein, M A., Rich, C. L. (1963) ‘Electroencephalographic prediction of
epilepsy as a complication of cerebral palsy.’ Neurology (Minneap.), 13, 143. Gordon, N. S. (1962) ‘The investigation of epilepsy.’ Develop. Med. Child Neurol., 4, 170. - (1966) ‘The E.E.G. in cerebral palsy.’ Develop. Med. Child NeuroI., 8,216. Kiloh, L. G., Osselton, J. W. (1961) Clinical Electroencephalography. London: Butterworth. Lundervoold, A. (1960) ‘The E.E.G. in cerebral palsy.’ Cerebr. Palsy BUN., 2, 82. Perlstein, M. A., Gibbs, E. L., Gibbs, F. A. (1947) ‘The electroencephalogram in infantile cerebral palsy.’
Skatved, M. (1956) ‘Cerebral palsy: A clinical study of 370 cases.’ Actapaediat. Uppsala, Suppl. 101. Winfield, D. L., Hughes, J. G., Sayle, W. E. (1955) ‘Electroencephalography: sleep findings in cerebral
Woods, G. F. (1965) ‘Some clinical notes and E.E.G. findings in cerebral palsy.’ Arch. Dis. Childh., 40,394.
Ass. Res. nerv. Dis. Proc., 26, 377.
palsy.’ Pediatrics, 16, 88.
301