department of clinical haematology -...
TRANSCRIPT

Department of Clinical Haematology
H.82 Page 1 of 11 January 2015 V2.3 Management of TTP Authorised by: Dr Andy Peniket, Dr Sylvie Benjamin
This is a controlled document and therefore must not be changed
Diagnosis and management of thrombotic thrombocytopenic purpura (TTP): Summary
Suspect TTP if MAHA and thrombocytopenia in absence of other identifiable cause Start treatment immediately if TTP is suspected and refer urgently for specialist advice and Plasma Exchange (PEX) Suspected
TTP Take blood before starting PEX: FBC, blood film, reticulocytes, clotting, fibrinogen, U+E, Trop I/T, LFTs, TFTs, calcium, Amylase, LDH, Haptoglobins, pregnancy test, DAT, blood group with antibody screen, ADAMTS13 assay, Hep A/B/C, HIV serology and autoantibody screen
Investigations
Other investigations should be performed promptly but can be delayed until after starting PEX: urinalysis, stool culture (if diarrhoea), echocardiogram, CT brain (if neurological signs), and CT chest/abdomen/pelvis to check for underlying malignancy (if indicated) Further
Investigations Request S/D FFP. If any delay in starting PEX then give FFP (watch for fluid overload) Use standard FFP if S/D unavailable. Transfuse packed red cells when necessary to correct anaemia. PLATELET TRANFUSIONS CONTRAINDICATED unless life threatening bleeding
Blood Products
Start PEX with S/D FFP ASAP 1.5 plasma volumes per day then 1 plasma volume per day with stabilisation of condition URGENT
treatment
Give steroids - IV Methylprednisolone 1 g/day for 3 days with an oral proton pump inhibitor. Give oral folic acid 5 mg OD
Start immediately
after PEX If HIV positive, start HAART immediately. If neurological or cardiac involvement, start Rituximab
Special cases
When platelet count >50 x 109/L, start low molecular weight heparin thromboprophylaxis and aspirin 75 mg OD
Prevent thrombosis
Continue daily plasma exchange for a minimum of 2 days after platelet count has been >150 x 109/L then stop. If progressive symptoms, refractory disease or early relapse, consider additional therapy Treatment
success?

Department of Clinical Haematology
H.82 Page 2 of 11 January 2015 V2.3 Management of TTP Authorised by: Dr Andy Peniket, Dr Sylvie Benjamin
This is a controlled document and therefore must not be changed
Diagnosis and management of thrombotic thrombocytopenic purpura (TTP) Diagnosis: Thrombocytopenia and red cell fragmentation with no other known cause. Patients may deteriorate rapidly and need ITU treatment. Urgent spun apheresis plasma exchange (PEX) should be instituted ASAP, preferably
within 4-8 hours regardless of time of presentation. PLATELET TRANSFUSIONS ARE CONTRAINDICATED – they often exacerbate
microthrombi and end organ hypoperfusion and must not be given, however low the platelet count, unless there is life-threatening bleeding.
Urgent liaison with blood bank needed to order suitable products. All diagnostic blood tests MUST be taken before first PEX. Cardiac TTP is an early cause of death so monitor with echocardiogram and troponin
levels Liaise with National Health Service Blood and Transplant Specialist Therapeutic Services
(NHSBT STS) Oxford for PEX. Patients need daily monitoring of clinical and laboratory parameters. Disease modifying treatment is often also needed. Introduction Thrombotic thrombocytopenic purpura (TTP) is a rare but serious and often life-threatening disease characterised by microangiopathic haemolytic anaemia and thrombocytopenia with no other identifiable cause. Idiopathic TTP is an acquired immune disorder leading to presence of unusually large multimers of von Willebrand factor (VWF) due to the decreased activity of ADAMTS13, the enzyme that cleaves von Willebrand multimers. These large multimers cause platelet aggregation and platelet microthrombi which lead to hypoperfusion of vital organs. Patients may present with fever, purpura, microangiopathic haemolytic anaemia, and neurological or renal dysfunction. Untreated, the mortality approaches 100%. With intensive treatment up to 90% of patients survive, often with complete recovery. Treatment is based on daily PEX to relieve acute symptoms and with immunosuppression to affect the underlying disease process. Close co-operation is needed between clinicians looking after the patient, the apheresis unit staff and the blood bank. Intensive care treatment may be needed. This guideline outlines the plan for diagnosis, investigation, treatment and monitoring of patients with TTP at Oxford University Hospitals NHS Trust (OUH) Trust and NHSBT Oxford STS. Referrals Referrals should be directed to the haematology Specialist Registrar (transfusion SpR based at NHSBT during working hours and the on-call SpR out-of-hours). The patient is admitted under the named consultant on-call for clinical haematology, who should be immediately informed. Day to day medical care is co-ordinated by this consultant’s SpR. Where bed capacity does not exist to take a patient, the referrer should be asked to contact another unit. E.g. UCH. Blood bank must be informed as soon as the patient is accepted, so suitable products can be ordered. No patient should be accepted for medical care until it is ascertained that there is: i. an appropriate bed where close observation by experienced staff can be undertaken

Department of Clinical Haematology
H.82 Page 3 of 11 January 2015 V2.3 Management of TTP Authorised by: Dr Andy Peniket, Dr Sylvie Benjamin
This is a controlled document and therefore must not be changed
ii. capacity in the apheresis unit to undertake ongoing daily PEX iii. an ITU bed if patient transferred from another ITU Patients with this condition may deteriorate rapidly after presentation, so must never be accepted for treatment as an out-patient. Where the TTP patient has another underlying disease e.g. SLE, specific advice should be sought from appropriate specialist physicians. This document provides guidance on the diagnosis and management of patients with TTP, including up-to-date management guidelines from the 2012 BCSH guidelines. Clinical Haematology has experience in managing patients with TTP in collaboration with the NHSBT STS team; contact the on-call Haematology SpR or one of the Consultants for advice. NHSBT Oxford STS provides 8am-4pm, 7 days/week service. PEX may be possible at other times depending on operational constraints. (See Appendix 1 for contact details). Diagnosis The diagnosis is clinical and based on: a) - Thrombocytopenia - Red cell fragments on blood film (Microangiopathic haemolysis) - High LDH
- Normal coagulation screen (PT, APTT, Fibrinogen) - For which no other cause is found
b) Associated features result from microvascular insufficiency and include:
− neurological impairment e.g. (confusion, headache, seizures, coma) − cardiac ischaemia e.g. (chest pain, ECG changes, raised troponin, LV
dysfunction) − renal impairment e.g. (raised creatinine, microscopic haematuria, proteinuria)
c) A low metalloprotease (ADAMTS13) is supportive of TTP, but the result will only be
available later and cannot be used at time of initial diagnosis. See p7.
d) TTP associated with underlying malignancy or post bone marrow transplant is unresponsive to PEX, which is not recommended. Treat the underlying malignancy if possible. Change the calcineurin inhibitor and consider defibrotide if post HSCT.
e) TTP is life-threatening and early treatment more effective, so any patient with a low
platelet count and neurological symptoms (assuming no other clear identified cause) should be treated as presumptive TTP and urgent PEX instituted.
Underlying Cause of TTP Idiopathic, Autoimmune disorder 33% Bacterial or viral infection including HIV or hepatitis Pregnancy Drug induced Other autoimmune disorders Pancreatitis Disseminated malignancy Post haematopoietic stem cell transplant

Department of Clinical Haematology
H.82 Page 4 of 11 January 2015 V2.3 Management of TTP Authorised by: Dr Andy Peniket, Dr Sylvie Benjamin
This is a controlled document and therefore must not be changed
Differential Diagnosis of MAHA and low Platelets: Disseminated intravascular coagulation (DIC) Severe infection e.g. Meningococcus, pneumococcus Pregnancy associated e.g. Haemolysis with elevated liver enzymes and low platelets
(HELLP), Pre-eclampsia Autoimmune: Cerebral systemic lupus erythematosus (SLE), Lupus Nephritis, Acute
Scleroderma Renal Crisis Malignant Hypertension Haemolytic uraemic syndrome Catastrophic Antiphospholipid Syndrome Autoimmune haemolysis and Immune Thrombocytopenia (Evans Syndrome)
Diagnostic Investigations (repeat all tests at acute relapse) All blood tests must be carried out before 1st PEX as this is the only ‘neat’ sample of patient’s blood. Investigations required and results in keeping with TTP: FBC & blood film Reticulocyte count LDH Haptoglobins ESR DAT
Anaemia, fragments and thrombocytopenia Raised Raised Reduced If raised consider occult malignancy Usually negative
Clotting screen U&E LFT Calcium
Amylase Blood group & Antibody screen
Usually normal Renal Impairment (often mild) Usually normal Raised in malignancy, may be reduced with
PEX TTP is rarely associated with pancreatitis For blood product provision
Anticardiolipin antibody Lupus anticoagulant Autoimmune profile Rheumatoid factor ANA
Thyroid Function Tests
Consider an underlying autoimmune precipitant
Blood cultures Hepatitis serology (Hep A, B,C) HIV Stool for E.Coli
Consider an underlying infectious precipitant. Also important prior to PEX and Rituximab treatment.
Consider HUS if E coli in stool MC+S Urinalysis (Pregnancy / Protein) Rule out Pregnancy, HELLP, and Pre-
Eclampsia ADAMTS13 assay: protease
activity+ Inhibitor - 4 x citrate tubes - double spin & freeze - label as urgent for the
attention of the OHC
Confirmation of diagnosis with low ADAMTS 13 assay (activity and antibody profile). Do not wait for result before starting treatment in suspected TTP
Liaise with coagulation laboratory – phone Peter Baker or James Beaver at Oxford Haemophilia Centre (OHC) to give notice of urgent protease samples coming.
Continued on next page
Department of Clinical Haematology
H.82 Page 5 of 11 January 2015 V2.3 Management of TTP Authorised by: Dr Andy Peniket, Dr Sylvie Benjamin
This is a controlled document and therefore must not be changed
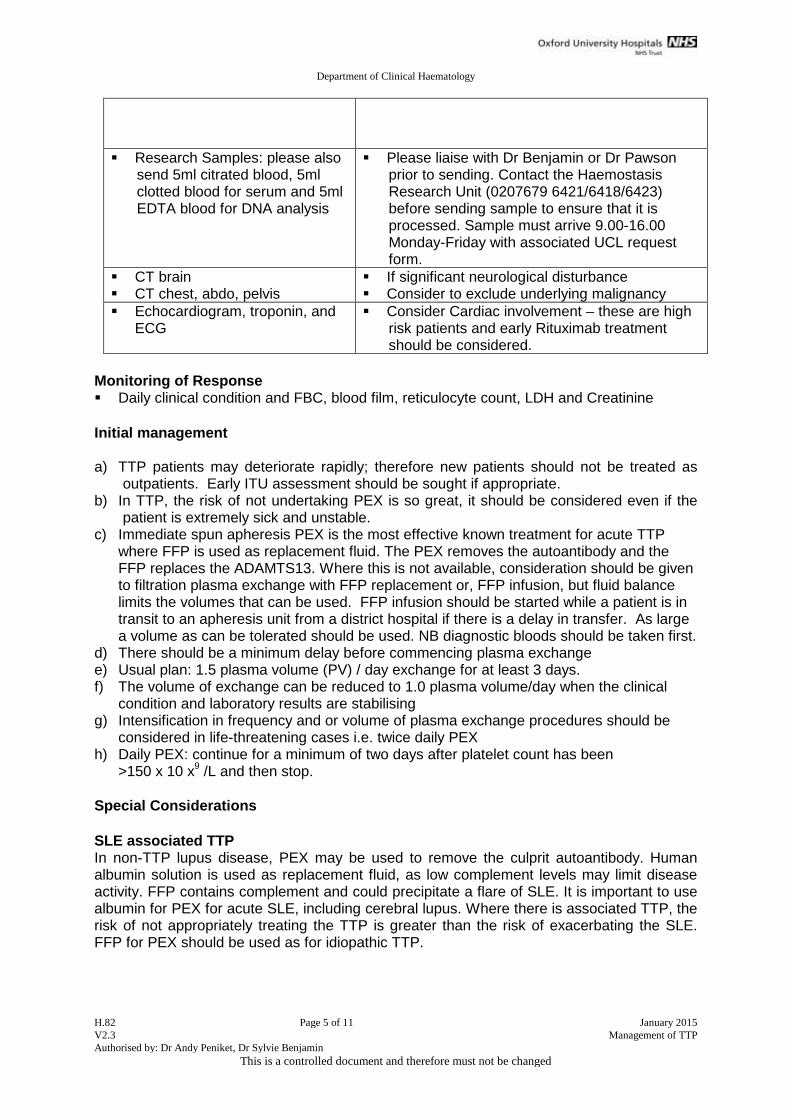
Research Samples: please also send 5ml citrated blood, 5ml clotted blood for serum and 5ml EDTA blood for DNA analysis
Please liaise with Dr Benjamin or Dr Pawson prior to sending. Contact the Haemostasis Research Unit (0207679 6421/6418/6423) before sending sample to ensure that it is processed. Sample must arrive 9.00-16.00 Monday-Friday with associated UCL request form.
CT brain CT chest, abdo, pelvis
If significant neurological disturbance Consider to exclude underlying malignancy
Echocardiogram, troponin, and ECG
Consider Cardiac involvement – these are high risk patients and early Rituximab treatment should be considered.
Monitoring of Response Daily clinical condition and FBC, blood film, reticulocyte count, LDH and Creatinine Initial management a) TTP patients may deteriorate rapidly; therefore new patients should not be treated as
outpatients. Early ITU assessment should be sought if appropriate. b) In TTP, the risk of not undertaking PEX is so great, it should be considered even if the
patient is extremely sick and unstable. c) Immediate spun apheresis PEX is the most effective known treatment for acute TTP
where FFP is used as replacement fluid. The PEX removes the autoantibody and the FFP replaces the ADAMTS13. Where this is not available, consideration should be given to filtration plasma exchange with FFP replacement or, FFP infusion, but fluid balance limits the volumes that can be used. FFP infusion should be started while a patient is in transit to an apheresis unit from a district hospital if there is a delay in transfer. As large a volume as can be tolerated should be used. NB diagnostic bloods should be taken first.
d) There should be a minimum delay before commencing plasma exchange e) Usual plan: 1.5 plasma volume (PV) / day exchange for at least 3 days. f) The volume of exchange can be reduced to 1.0 plasma volume/day when the clinical
condition and laboratory results are stabilising g) Intensification in frequency and or volume of plasma exchange procedures should be
considered in life-threatening cases i.e. twice daily PEX h) Daily PEX: continue for a minimum of two days after platelet count has been
>150 x 10 x9 /L and then stop. Special Considerations SLE associated TTP In non-TTP lupus disease, PEX may be used to remove the culprit autoantibody. Human albumin solution is used as replacement fluid, as low complement levels may limit disease activity. FFP contains complement and could precipitate a flare of SLE. It is important to use albumin for PEX for acute SLE, including cerebral lupus. Where there is associated TTP, the risk of not appropriately treating the TTP is greater than the risk of exacerbating the SLE. FFP for PEX should be used as for idiopathic TTP.

Department of Clinical Haematology
H.82 Page 6 of 11 January 2015 V2.3 Management of TTP Authorised by: Dr Andy Peniket, Dr Sylvie Benjamin
This is a controlled document and therefore must not be changed
HIV associated TTP TTP may be the initial presenting feature of HIV or following non- compliance with antiviral treatment (HAART). PEX should be used as an adjunct to HAART. Remission is dependent on improving the immune status of the patient. Stopping HAART can result in acute TTP relapse and continued use of HAART usually prevents further relapses. Pregnancy associated TTP
Differentiating TTP from the more common pregnancy related thrombotic microangiopathies, such as pre-eclampsia (PET), haemolysis, elevated liver enzymes, low platelets (HELLP syndrome) and haemolytic-uraemic syndrome (HUS) is difficult, especially if TTP presents post partum. (See table in 2012 BCSH guidelines).There is a continued risk of relapse during subsequent pregnancies. Women with normal levels of ADAMTS13 pre-pregnancy have a lower risk of relapse. Treatment involves delivery as a definitive treatment, PEX as a holding measure and close liaison with obstetrics and the fetal medicine department. Pregnant patients should be discussed with Dr Lucy Mackillop, Consultant in Obstetric Medicine. Drug associated TTP Fewer than 15% of cases. Thienopyridine–associated TTP is well recognised in association with ticlodipine with an incidence of 1 per 1600 to 5000. The described association with clopidogrel remains a matter of debate. TTP is also described with quinine, trimethoprim, peglyated interferon, combined OCP and HRT. Gemcitabine, bleomycin and mitomycin–C can cause HUS or TTP-like illness. There is no clear consensus on treatment but some patients have recovered with PEX. Preparing patient for Apheresis procedure Venous Access a) The patient must have adequate venous access for the procedure. Veins should be
large enough to easily site a 16G Kimal needle in the antecubital fossa. If veins are inadequate a suitable apheresis line must be inserted and functioning before the procedure. Initially a femoral line can be placed, when there is severe thrombocytopenia. For ongoing treatment a long-term line must be inserted.
b) The risk of placing a line with low platelet count must be balanced against the known high risk of the patient’s clinical condition deteriorating because venous access is lost and plasma exchange cannot be continued.
c) Platelet transfusions are contraindicated in TTP and must not be given routinely before line insertion even in the presence of severe thrombocytopenia. This is true however low the platelet count is and PLATELET TRANSFUSION SHOULD BE AVOIDED EXCEPT WHERE THERE IS MAJOR LIFE-THREATENING BLEEDING.
d) Although initial PEX may be performed using peripheral access, the need for continued treatment makes a long-term apheresis line a necessity.
Replacement fluid: Fresh Frozen Plasma (FFP) (Liaise with blood bank daily to arrange to order and defrost products) Use group compatible: a) Solvent detergent treated (S/D) FFP. (To reduce the risk of transfusion transmitted
infection as per the Department of Health guidance) b) If S/D is not available, use standard FFP

Department of Clinical Haematology
H.82 Page 7 of 11 January 2015 V2.3 Management of TTP Authorised by: Dr Andy Peniket, Dr Sylvie Benjamin
This is a controlled document and therefore must not be changed
c) There is evidence that Methylene-Blue treated FFP is less effective than S/D FFP and should not be used.
Red cell transfusion Transfusion of red blood cells should be given to keep Hb > 90g/L (higher if cardiovascular disease). Drug treatment a) Treatment with drugs is aimed at immunosuppression to affect the underlying disease
process. b) Given the thrombotic nature of the disease, and the fact that Protein S levels are
decreased in S/D FFP, the incidence of venous thromboembolism is high, so routine prophylaxis with low molecular weight heparin (LMWH) is recommended when the platelet count is greater than > 50 x 109/L and patients should wear TED stockings.
At diagnosis:
Methylprednisolone (IV 1g/d)
x 3 doses (daily) give immediately after PEX.
Rituximab 375mg/m2 weekly for a total of 4 doses
Consider upfront use in neurological or cardiac involvement: these complications have a high mortality. This may be increased to twice per week in selected cases. Give immediately after PEX and allow 4 hours before next PEX.
Folic Acid 5 mg po od during active haemolysis Aspirin 75 mg po od when platelet > 50 x 109/L LMWH as thrombo-prophylaxis when platelet > 50 x
109/L Hepatitis B vaccination when platelet > 50 x 109/L. High plasma
exposure. Omeprazole 20mg po od whilst on steroids
No response by day 7:
Rituximab if not already given
IV 375mg/m2 weekly x 4 doses
Previous second line treatments prior to the introduction of Rituximab, such as vincristine, cyclophosphamide, and polychemotherapy are not recommended. Splenectomy may rarely be considered in the non-acute period of immune-mediated TTP but has limited proven benefit. Monitoring the response to treatment a) The clinical response should be monitored with daily record of the patient’s clinical
condition, including neurological examination. b) Tests to monitor the response to treatment (e.g. Hb, reticulocytes, platelet count,
fragments on the film, LDH, and renal function) should be taken prior to each PEX (and more often if clinically indicated).

Department of Clinical Haematology
H.82 Page 8 of 11 January 2015 V2.3 Management of TTP Authorised by: Dr Andy Peniket, Dr Sylvie Benjamin
This is a controlled document and therefore must not be changed
Discontinuation of Heparin Heparin should be continued until the patient is in full clinical and haematological remission, is fully ambulant and off PEX for >10d.
ADAMTS13 Assay Results
Severely reduced ADAMTS13 activity (<5%) +/- the presence of an inhibitor or IgG antibodies, confirms the diagnosis. A decreased ADAMTS13 activity (<40% but >5%) has been reported in a variety of non-TTP conditions such as uraemia, inflammatory states, post operatively and during pregnancy. The specificity of severe ADAMTS13 deficiency (<5%) in distinguishing acute TTP from HUS is 90%. It is important to note that the ADAMTS13 level measured will be higher (falsely raised) if the sample has been taken after the initial infusion of plasma. An inhibitor is considered positive if >15 units/ml.
Information for patients
Please see the Transfusion section of the NSSG site for a patient information leaflet on TTP.
Discharge and Follow up
Patients should be counselled about symptoms, signs and risk of relapse before discharge with verbal and written information. (See Appendix 2). Please liaise with Dr Benjamin for outpatient follow up. Relapse Increased PEX and/or Rituximab are the modalities of choice in relapsing disease. In patients with a documented reduction of ADAMTS 13 activity to <5%, elective therapy with Rituximab can be considered if an inhibitor has reappeared. References BCSH – Guideline on the Diagnosis and Management of Thrombotic Thrombocytopenic Purpura and the other Thrombotic Microangiopathies. British Journal of Haematology, 2012, 158, 323–335 BCSH – Guidelines for the administration of blood and blood components and the management of transfused patients. BCSH Guidelines website, published in 2010. http://www.bcshguidelines.com/documents/Admin_blood_components_bcsh_05012010.pdf Department of Health – D H letter January 2006 Gateway Reference: 5999 Annex A (ii) A Systematic Review of randomised controlled trial for plasma exchange in the treatment of TTP Brunskill, SL, Transfusion Medicine 2007 17(1), 17-35. Appendix 1 Useful phone numbers, page 10 Appendix 2 Patient discharge information, page 11
Department of Clinical Haematology
H.82 Page 9 of 11 January 2015 V2.3 Management of TTP Authorised by: Dr Andy Peniket, Dr Sylvie Benjamin
This is a controlled document and therefore must not be changed
Version Control Authors: Dr Mike Murphy, Sylvia Benjamin Version 1.0: February 2001 Version 1.2: Revision October 2001 Version 1.3: Revision May 2003 Version 1.4: Revision July 2003 Version 1.5: Revision June 2007 Version 1.6 Revision July 2010 Review Name Revision Date Version Review date Dr Sylvia Benjamin, Dr Toby Eyre, Dr Michael Desborough, Dr Henna Wong, Dr Dalia Khan.
Pathway review May 2014 2.1 May 2016
Sandy Hayes, QM Formatting July 2014 2.2 May 2016
Sandy Hayes, Quality manager Misprint page 7, Rituximab: allow 4 hours before next PEX
January 2015
2.3 May 2016

Department of Clinical Haematology
H.82 Page 10 of 11 May 2014 V2.2 Management of TTP Authorised by: Dr Andy Peniket, Dr Sylvie Benjamin
This is a controlled document and therefore must not be changed
Appendix 1
Useful phone numbers Name / Department Contact Number
ITU(JR) ITU(CH)
01865 220625 01865235077
JR Blood Bank CH Haematology lab
01865 220339 01865 572136
JR Coagulation Laboratory 01865 220360
Line Team 01865 221653 (bleep 1749)
NHSBT Hospital Services Department (Oxford)
01865 387963 (to contact Apheresis Staff out of hours)
NHSBT Oxford STS (Apheresis) Unit
01865 220303
Peter Baker, James Beavis, Haemophilia Centre
01865 225305
Clinical Haematology Ward 01865 235048/9
Dr S Benjamin 01865 387710
Transfusion SpR Bleep 6888 (08.30-17.00 Monday – Friday)
PA to Dr S Benjamin and Dr Pawson
01865 387710
On-call Haematology SpR Via switchboard from 5pm until 9am 01865 741166
Dr Lucy Mackillop
Silver Star Unit 01865 221710 (Monday - Friday 09.00 - 17.30)
UCL Haemostasis Research Unit 020 7679 6421/6418/6423
On-call Apheresis 01865 387963
NHSBT SMART divert for on-call transfusion consultant (24/7) – non-apheresis
01179 594666
JR Blood Bank (out of hours) Bleep 1719

Department of Clinical Haematology
H.82 Page 11 of 11 May 2014 V2.2 Management of TTP Authorised by: Dr Andy Peniket, Dr Sylvie Benjamin
This is a controlled document and therefore must not be changed
Appendix 2 Patient Discharge Information Sheet What happens now? Plasma exchange is a very effective treatment for TTP, and often results in the condition never recurring. We would however normally like to follow patients up in our clinic following the episode to check there are no signs of recurrence and to check on their general health. What should I look out for? The symptoms that might suggest that TTP is reoccurring are often symptoms that patients have initially experienced when the TTP was first diagnosed, but this is not always the case. We would like to know if you notice any of the following symptoms, as they could represent a recurrence of the TTP: • Bruising, severe fatigue, abdominal pain • Slurring of speech • Arm, Face or Leg weakness or loss of sensation • Visual disturbance • Problems with Balance • Poor co-ordination • Seizure (someone might witness it occur) • Chest pain or shortness of breath, particularly on exertion This is not a totally inclusive list, but covers the main potential symptoms. If you are concerned about any other symptoms that you think might be relevant, do get in touch. When TTP recurs the symptoms can evolve rapidly, so please do not hesitate to contact us. Who do I contact and when?
Best wishes. The Transfusion Team, Oxford University Hospitals NHS Trust
Monday-Friday • 9am - 4pm, please contact the Specialist Therapeutic
Services Unit at the NHS Blood and Transplant Unit at the John Radcliffe Hospital on 01865 720303.
Out-of-hours • If you are worried please contact Haematology Ward at the
Churchill Hospital: 01865 235048/235049
11