department of child health - prsharma.com.npprsharma.com.np/professionals/jobresidents.pdf · -...
TRANSCRIPT

1

2
Department of Child Health
Maharajgunj Campus
Guidelines for MD Paediatric residents
I. Responsibilities
1. A MD residents must carry out the following clinical responsibilities in the Unit where they are posted :
a. Must know the working diagnosis of all in- patients. b. Should write follow-up notes timely, completely, accurately directed towards the patient problem,
properly, sequentially eliciting salient positive and negative points to support the diagnosis on the continuation sheet.
c. Should be able to present history, clinical examination findings when asked and justify logically by
applying knowledge of disease and its pathophysiology in clear, organized, complete, accurate and polished manner. It should include psychosocial and preventive aspect also.
d. Should suggest investigations based on the working diagnosis with limitations incorporating considerations of costs, risks and benefits.
e. Should make available the investigations for the round. f. Should guide juniors in history writing, examination and supervise them. g. Should be responsible for the drugs written in the cardex. h. Should write clear nursing instructions. i. Should counsel parents in clear, appropriate, jargon-free and empathetic way. j. Should be responsible for the planning of the nutrition needs for the child and instruct for its
implementation to the dietician, nurses and counsel the parents on ways to fulfil it. k. Should perform bedside procedures when needed. l. Should perform the daily ward round being enthusiastic responsive, reliable, committed,
cooperative and respectful way before the consultants round. m. Should write the discharge summaries completely, with salient informations, write own full name
and sign. n. Should write referral notes as advised by the consultant and follow-up the referrals.
o. A third year MD residents will work as a second on call. They will carry out the following
responsibilities:
- Review all cases admitted in the ward and observation room in the evening of the admission day.
- Be available to solve the problem if any as shown by the first on call. - Inform the consultants about the problem and types of patients admitted. - Review the treatment provided by the emergency or first on call doctor.

3
- Present the cases in the post admission morning round - Be responsible for the presentation of the admitted cases in the seminar.
p. Take evening tutorial bedside clinical classes for the MBBS students.
2. They are responsible for the duties that are allotted to them. 3. They are responsible for the topic, journal club, cases, and a bedside clinical presentation of that is
allotted to them and show the presentations outline three days ahead to the faculty member.
4. They should hand over the patients to each other during or after their duties.
5. They are responsible for the patient’s care in OPD.
6. They should carry out the functions that are allotted to them by their consultants. 7. They should teach juniors about the cases admitted in the ward.
8. Must inform the consultant if unable to attend the duties and should make alternative arrangements for
their duties.
9. Should collect the evaluation form from the department and submit it to the respective unit heads for their own evaluation. Finally they should submit the evaluated form to the co-ordinator within one week after the end of respective posting.
10. They must maintain a log book as mentioned in the format and submit it duly signed by the unit head
and to the co-ordinator within one week after the end of posting. II. Thesis works: Department will allot preceptor to each candidate at the end of first six month Residents should try to identify their own topic for the thesis within first year of their enrollment. The prepared protocol must be submitted to the department at the end of first year. They will be asked to present litterateur review, hypothesis, justification for the study, methods and materials and statistical methods to be used for the analysis for the result of their topics for the study. It is compulsory that the thesis should be submitted to the Department before six months of the final examination. List of topics for thesis work is available in the department They will start collecting data from the second year and data collections should be completed by the Ashwin of the second year. By Magh they should complete analysis and midterm presentation of the thesis work will be in Phalgun of the second year. Please read the document “How to write a MD thesis” by DR. Pushpa Raj Sharma, available in Health Net Nepal under the topic Health resources "Thesis". Final presentation, which includes results, discussions, limitations of the study and final recommendations will be done in Shrawan of the third year. By Ashwin of the third year they should present six printed copies of their thesis work to the department, failure of this will lead to inability to appear in the final examination.

4
III. Presentations Residents will be asked to take part in the following teaching learning activities of the department: topic presentation
a. journal club presentation b. case presentation c. bedside clinical presentation.
A faculty member will be available for their guidance. Residents are responsible to inform the faculty member well ahead of their presentation and take suggestions. See attached list of topics for the presentations. a. Journal club meeting Residents should choose the journal article from the recent journals as far as possible for the presentation. Journals are available in the TUTH and departmental library. It is mandatory that they should use the facility of Internet, which is available free of cost in the department to find out the recent articles. Residents should present the paper in the IMRaD format (Introduction, Methods, Results and Discussions). Suggested structures for the discussion of the journal article: The following questions should be answered: 1. What were the study objectives?
• What were the study purpose and the scientific hypothesis to be tested? • Is the objective clearly formulated?
2. What was the study about? • How were the subject recruited? • Describe the study site and study population: hospital or community • What were the inclusion and exclusion criteria?
3. What was the design of the study? • Describe the study design: randomised controlled trials; case control, prospective, retrospective
etc. • What specific interventions were considered, what was it compared with? • What was measured and how?
4. How were the preliminary questions dealt with? • Was the sample size or power calculation described? • What is the duration of the follow-up? • Completeness of the follow-up? • Was the method of randomisation adequately described?
5. How did the author measure the outcome? • Are primary and other outcomes clearly defined? • Is a gold standard for outcome assessment described?
6. Quality control issues? • How were the quality control and validation procedures for the intervention and outcome assessment described? • Was assessment blind?

5
7. Data analysis:
• What sort of data authors examining? • Which statistical tests were done? • Were the statistical tests were appropriate? • Are the data analysed according to the original protocol?
8. Was systemic bias avoided or minimised? 9. Ethical issues:
• Are the ethical issues adequately described? 10. Conclusion and their use?
• Which were the generalizable conclusions: statistical significance or clinical . • Are there new questions arising from the paper? • Does this research as to the literature in any way?
For further guidance residents are asked to read the following articles available from Medline and library at TUTH:
1. Ad Hoc Working Group for Critical Appraisal of the Medical Literature. A proposal for more informative abstracts for clinical studies. Ann Intern Med 1987; 106: 598-604.
2. Reading the medical literature. In Princples and Practice of Pediatrics. Ed: Frank A. Oski. Second edition (1994). Page 24-29.
b. Topic presentation A specific topic will be allotted to each resident depending upon his/her residency year as listed. The resident should present the topic within 45 minutes. Faculty member will guide the discussion after the presentation. At the beginning of topic presentation there well be MCQ test in important topics. The resident should inform the faculty about the topic to be presented one week ahead of the presentation date. This presentation is not just delivering what is present in textbooks. The topic presentation should include the following:
a. review of the subject b. report on research c. provide practical instruction d. provide supporting facts with adequate information and illustration. e. Make reasonable conclusion from an interpretation of, his/her work, which is warranted by the
information provided C. Case presentation The residents should ask the respective unit head for the type of cases to present. It should be informed to all the residents one/two day ahead of the presentations so that other will be able to review the cases before the day of presentation. During the presentation they should be able to show the transparency having following points:
- Age, address and presenting complaints.

6
- History - Examination findings. - Working diagnosis. - Differential diagnosis - Suggested investigations. - Results of carried investigations. - Final diagnosis. - Summary of the disease.
Following reference is available at the departmental library:
James Calhan, Andras Barabas. Speaking at medical meetings: a practical guide. (Second edition).
D. Case of the month This presentation consists of case presentation and definition, aetiology, epidemiology, pathophysiology, clinical features, differential diagnosis, treatment and prognosis of the case presented. D. Problem solving Each month one problem solving seminar will be held. Residents, house officers and interns are divided in different groups and each group will be led by the senior most resident. All groups will receive a simulated case history. Students will work in group and finally present the most likely diagnosis and plan of management.
IV. Bhaktapur community paediatrics posting: Residents will be posted once a week to Siddhi Memorial Mother and Child Hospital during their second year residency. They will visit different schools and the community satellite clinic of the Institute of Medicine. They should report to the Field Director and take active part in the following programs:
a. School health programs. b. Adolescent health programs. c. Community research
V. Ward work-up Admission day:
1. Do quick ward round and attend OPD at 9.00 AM 2. Attend OPD cases. 3. Admit cases. Do not write history in the OPD but only necessary treatment and investigations. All admitted cases
should be seen by senior resident of the unit. 4. Allot cases to interns to write history and supervise them 5. Attend the observation ward and sort out the cases. 6. Prepare the cases for the presentation to the consultant.
Post admission day: 1. Must know the working diagnosis of each patient. 2. Should give the evidence for their working diagnosis. 3. Should scientifically justify the treatment that has been provided. 4. Should give the plan for further investigations and treatment. Third day: 1. All investigations as planned must be available. If it is not available he/should justify for the non-availability. 2. Case notes must be completed including detailed history, examination and plan of investigations. 3. Guardian of the patient must know the provisional/confirmatory diagnosis.

7
4. Guardian of the patient must know the home care of the disease the child is suffering from. All days: 1. Should check the daily follow-up notes Under the SOAP format if not complete should complete it. 2. Is responsible for the care provided under the unit head 3. Should be available in the hospital during the duty hours, except during the classes. 4. Should check the written discharge notes, sign and write own name in capitals. 5. Should supervise juniors on assigned activities.
VI. Internal assessments:
Internal assessments will be based on the observation of the work performances based on the evaluation form, this will be done by the head of the unit at the end of unit posting and two clinical bedside practical examinations. These practical examinations will be held at the end of first and second year. The formats of these examinations are very similar to the final examination.
VII. Log Book Residents should maintain a log book in the following format and it must be signed by the consultant every month. This log book must be submitted to the department at the end of each posting. Month…………Year………..Resident Name………………… …….. Consultant…………….. Date Procedures/activities performed Signature of the consultant VII. Evaluation Residents should present the evaluation form to the unit head of the unit where they are working for the evaluation and submit the evaluated form to the Department .
VII. Core Topics for the presentation by MD Residents
MD 1st year MD 2nd year MD 3rd year
1. Seminar Acute watery diarrhoea Principle of fluid therapy
Development of in diarrhoea and vomiting. GI system and its anamolies
2. Seminar Persistent diarrhoea Metabolic acidosis and alkalosis. Approach to a child With vomiting
3. Seminar Dysentery Acute Renal
failure

8
Approach to a child With diarrhoea
4. Seminar Common surgical problems Immunological
An approach to a child of GI tract disease of GI with abdominal pain tract
5. Seminar Approach to a child with Portal hypertension Hepatic failure Hematemesisi and malena
6. Seminar
Approach to a child with Jaundice in neonate Immunological Jaundice basis of the hepatobiliary disease
7. Seminar Development of respiratory Pulmonary function tests Blood gas abnormalities System and its anamolies
8. Seminar
Approach to a child with Management of asthma Common ENT problem Cough or difficulty breathing
9. Seminar
Pathophysiology of Nutritional requirements Management of PEM in children PEM
11. Seminar
Rheumatic heart disease Mycotic infections Immunological diseases
11. . Hypertension in children Protozoal infections Child abuse
12. Seminar Congestive cardiac failure Intracranial tumours Disabled child
13. Seminar Development of urogenital Nocturnal enuresis Common surgical System and its anamolies problems of gentio-urinary System. 14. Seminar Approach to a child with Renal function tests Immunological Haematuria basis for renal disease.
15. Seminar Approach to a child with Myopathies Approach to a child with chromosomal disorders oedema
9
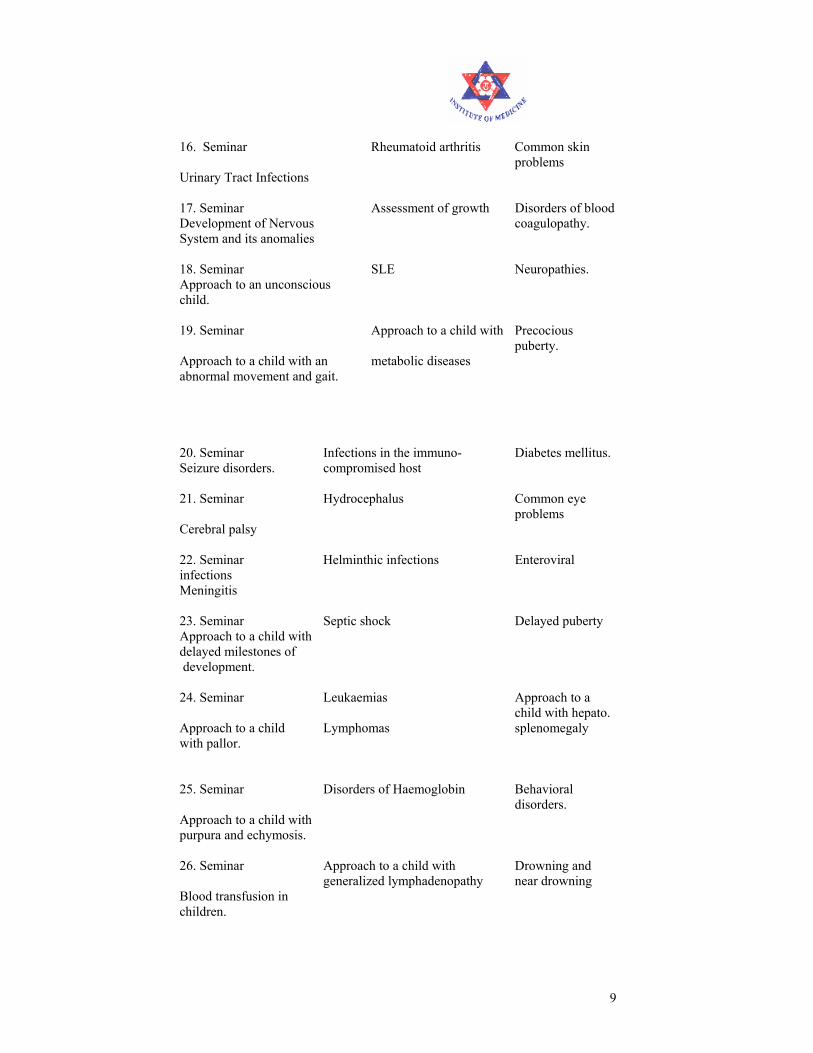
16. Seminar Rheumatoid arthritis Common skin problems Urinary Tract Infections
17. Seminar Assessment of growth Disorders of blood Development of Nervous coagulopathy. System and its anomalies
18. Seminar SLE Neuropathies. Approach to an unconscious child.
19. Seminar Approach to a child with Precocious puberty. Approach to a child with an metabolic diseases abnormal movement and gait.
20. Seminar Infections in the immuno- Diabetes mellitus. Seizure disorders. compromised host
21. Seminar Hydrocephalus Common eye problems Cerebral palsy
22. Seminar Helminthic infections Enteroviral infections Meningitis
23. Seminar Septic shock Delayed puberty Approach to a child with delayed milestones of development. 24. Seminar Leukaemias Approach to a
child with hepato. Approach to a child Lymphomas splenomegaly with pallor.
25. Seminar Disorders of Haemoglobin Behavioral disorders. Approach to a child with purpura and echymosis.
26. Seminar Approach to a child with Drowning and generalized lymphadenopathy near drowning Blood transfusion in children.

10
27. Seminar AIDS Immunological reactions in disease An approach to a child limp
28. Seminar Immunization principle Laboratory diagnosis of An approach to a child with and vaccine use immunological
disease rash.
29. Seminar Vasculitis syndrome Common orthopaedic problems An approach to a child with PUO.
30. Seminar Essential newborn care Common
childhood poisioning. Approach to a child with hematemesis
31. Seminar Developmental assessments SIDS Pallor in a newborn.
32. Seminar Fluid therapy in children Adolescent health Septicaemia in newborn.
33. Seminar Approach to a child with Paediatric emergencies LBW babies. Abnormal movement
34. Seminar
Approach to a child with Thyroid Attention deficit and hyperactivity Obesity disorders
35. Seminar Tuberculosis in children Adrenal hyperplasis Anxiety, habit and mood Disorders.
36. Seminar Development of heart Failure to thrive Psychiatric treatment in children And its congenital anamolies
37. Seminar Approach to a child with Immunological reaction Childhood malignancy heart disease
IX. Schedule of teaching/learning activities Sunday:
Morning 9-10 First and third : Radiodiagnosis Second: Topic presentation(1st Year RS) Fourth: Topic presentation(2nd Year RS)

11
9-12 MBBS problem solving cases Afternoon 1-2 Admitted cases discussion (unit Two)
Monday Morning 9-10 First Monday: Topic presentation( 3rd t year RS)
Second Monday: Last month's morbidity seminar Third Monday: Journal club meeting (2nd year RS)
Fourth Monday: Problem solving Afternoon 1-2 First Monday: Topic presentation (1st year RS) Second Monday: Case of the month (RS) Third Monday: Topic presentation (2nd year RS) Fourth Monday: Topic presentation ( 3rd RS) Tuesday
Ward round, OPD Wednesday Morning 9-10 Computer training, thesis discussions.
Faculty presentation. Afternoon 1-2 Second Wednesday: Perinatal meeting Thursday
Morning 9-10 First Thursday: Bedside(2nd r RS) Second Thursday: Bedside (3rd year RS) Third Thursday: Bedside (3rd year RS) Fourth Thursday: Bedside (3rd year RS) Afternoon 1-2 Admitted cases discussion (Unit One)
Friday Ward round, OPD
• Ward rounds every day 10-12
X. Schedule for the MD residents Schedule for the MD residents Residents 2060 2061 206
Jestha -- Kartik Man-Bais Jes-Kartik
Man-Bais
1st Year K P Badal Unit 2 Patan TUTH PICU
A Garg Patan Unit 2 PICU TUTH
M Shrestha Patan Unit 1 TUTH PICU
KM Poudel Patan Unit 1 Patan PICU TUTH
2nd Year Abhisek TUTH Unit 1 PICU Onc:MangSpecialP
Arun TUTH PICU Unit 1 Onc:Jest Special
12
P
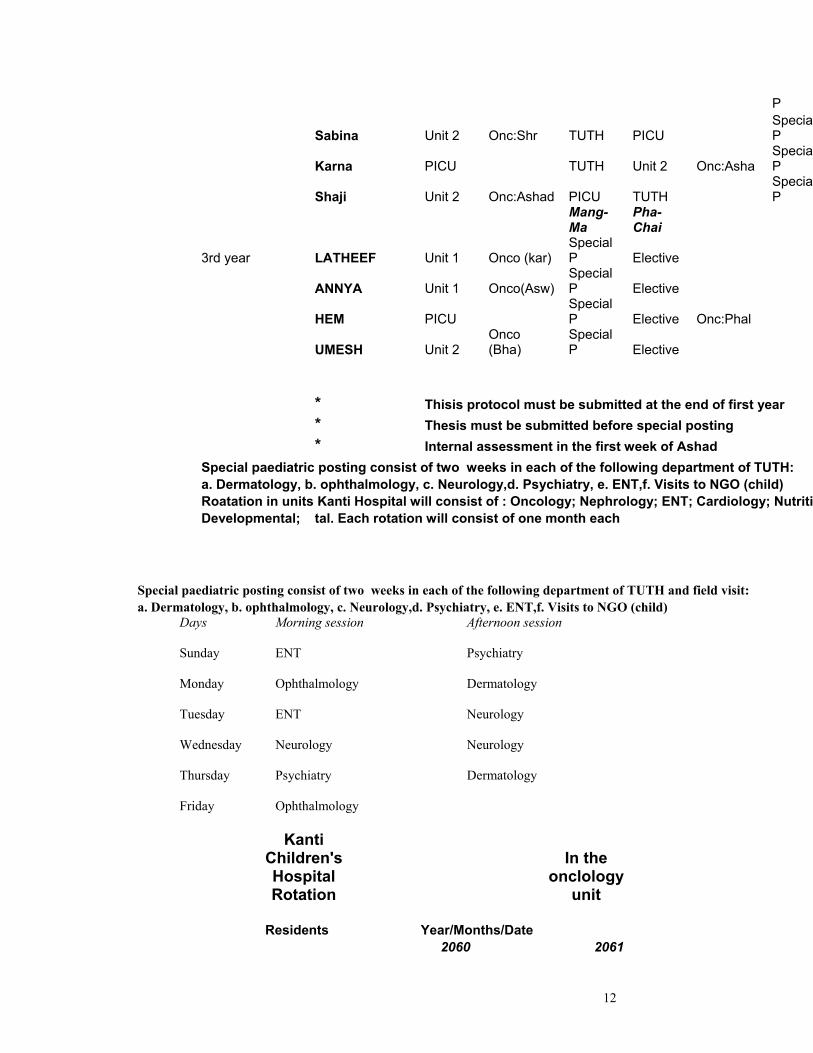
Sabina Unit 2 Onc:Shr TUTH PICU SpecialP
Karna PICU TUTH Unit 2 Onc:Asha SpecialP
Shaji Unit 2 Onc:Ashad PICU TUTH SpecialP
Mang-Ma
Pha-Chai
3rd year LATHEEF Unit 1 Onco (kar) Special P Elective
ANNYA Unit 1 Onco(Asw)Special P Elective
HEM PICU Special P Elective Onc:Phal
UMESH Unit 2 Onco (Bha)
Special P Elective
* Thisis protocol must be submitted at the end of first year * Thesis must be submitted before special posting * Internal assessment in the first week of Ashad Special paediatric posting consist of two weeks in each of the following department of TUTH: a. Dermatology, b. ophthalmology, c. Neurology,d. Psychiatry, e. ENT,f. Visits to NGO (child) Roatation in units Kanti Hospital will consist of : Oncology; Nephrology; ENT; Cardiology; Nutritio Developmental; tal. Each rotation will consist of one month each Special paediatric posting consist of two weeks in each of the following department of TUTH and field visit: a. Dermatology, b. ophthalmology, c. Neurology,d. Psychiatry, e. ENT,f. Visits to NGO (child)
Days Morning session Afternoon session Sunday ENT Psychiatry Monday Ophthalmology Dermatology Tuesday ENT Neurology Wednesday Neurology Neurology Thursday Psychiatry Dermatology Friday Ophthalmology
Kanti Children's Hospital Rotation
In the onclology
unit Residents Year/Months/Date 2060 2061

13
Umesh Bhadra 1-15 Annya Bhadra 16-30 Latheef Ashwin 1-15 Shazi Ashwin 15-30 Kiran Kartik 1-15 Krishna Kartik 16-30 Abhisek Mangsir 1-15 Garg Mangsir 16-30 Merina Magh 1-15 Hem Sagar Phalgun 1-15 Arun Jestha 1-15 Karna Jestha 16-30
XI Final examination
Components of the Final Examination: The knowledge and psychomotor skills of the students are assessed through two systems: internal assessment and final examination. Examination has two components: through theory and practical examinations. Examination in theory is done through two papers: general paediatrics and recent advances. General paediatrics consists of MCQ and recent advances consist of short answer questions. Practical examination is conducted under the four headings: Long case, short case, OSCE and Viva voce. Practical examination Components Time allowed Max. Marks Min. Pass Marks A. CLINICAL LONG CASE 60 minutes 50 25 (One) 30 minutes for history taking and 30 minutes for discussion SHORT CASE 60 minutes 50 25 (Four) (includes both examination and discussion) B. OSCE AND VIVA VOCE OSCE 75 minutes 50 25 (2 minutes per station. It consists

14
of slides, heart sounds, dummy, X-rays, pictures, ECG, Lab. reports, patients, parents) VIVA VOCE 30 minutes 50 25 (15 minutes in each table. Each table will ask 5 questions relating to the areas as mentioned
in the assessment form) Candidates have to pass clinical examinations (long case , short case, OSCE and Viva Voce separately). Assessments methodology: A pair of examiners ( one external and one internal) duly appointed by the examination section will assess the candidates in each subcomponent. Each examiner will be provided with separate assessment sheets for each candidate. Areas on which the candidate has to be assessed are listed on these forms. Examiner examining the long case will not examine the short cases and vice versa. Each examiner has to rate the candidate on all the areas identified in the assessment form even though he/she will ask questions from on section only. Hence, at the end of assessment each examiner would have given ratings for all the areas identified in the assessment form for each subcomponent. Assessment forms have to be filled with ink and will be collected immediately. The examiner shall not communicate the marks given to the candidate or to the co-examiner. If the disparity of marks given by the two examiners in each subcomponent is more than 50% it should be decided by the meeting of all the examiners for that subcomponent. Objectives of the clinical examination: Long case: The objectives of the long case examination is to assess: -history taking and clinical examination skills in identifying relevant information and presenting them effectively and efficiently. -Critical thinking and problem solving skills including investigations and management. -Knowledge of the latest advances relevant to a particular health problem. What do the examiners do during the "long" case examination? During history and clinical examination part: The candidates will be given 30 minutes for the history taking and clinical examination. During this period examiners will stay two feet apart (minimum) at the foot end of the bed and observe the candidates performance without any discussion. The examiner should not interrupt the candidate nor comment on his/her performance while the candidate is taking the history or performing the clinical examination.

15
When the candidate finishes this part in 30 minutes each examiner will give the marks with ink in the respective column of the long case form. During case presentation and discussion: After completion of 30 minutes the examiners will ask the candidate to present the findings and history and examination and discuss the case with him/her. The total time for this section is 30 minutes (15 minutes per examiner). The areas to be assessed are listed in the assessment form. The two examiners should mutually divide the areas amongst themselves before examining the candidate and may interchange the areas while examining the second candidate In case the candidate asks for the results of investigations, these should be provided, if available. Short cases Objectives: The objectives of the short case examination are to assess: - performance on a particular component of the systemic examination or regional examination. -detection and interpretation of clinical findings. -developing a management plan. What do the examiners do during the "short case" examination? During this period the pair of examiner should stand at a reasonable distance and at a position from where they can observe the candidate's performance. The examiner should ask the candidate to present the findings on examination and discuss the case. Total time for one patient is 15 minutes (8 minutes for examination and 7 minutes for discussion). The two examiner should mutually decide who will take lead in questioning a candidate and may interchange the next candidate. The areas to be assessed are listed in the assessment form. Viva voce examination Objective: The objectives of the viva voce examination is to: -Determine whether the candidate possesses a sound knowledge of the key features of the issue under discussion i.e. definitions, explanations etc. -Determine whether the candidate is able to apply the possessed knowledge in interpreting related information and formulating a management plan. -Determine whether the candidate is able to justify an action related to the key feature in curative, preventive and promotive paediatrics. -Determine whether the candidate is able to comprehend the questions correctly, organize his/her thought and respond correctly. What do the examiners do during the viva voce examination? It is important that the viva voce examination is structured. Examiners will meet one day ahead and will identify the topics, which should be covered in the examination. Each examiner should prepare a five set of questions and answers for this part of examination. These prepared questions and answers should be discussed on the morning of examination date. 10 questions should be selected in the morning of the examination date and it will be divided in two tables.
16
The areas to be questioned are grouped in two sections. One examiner should ask questions from one section and the other from the second. These sections may be interchanged while interviewing the next candidate. All the candidates should receive the same questions. The two examiners should mutually decide who will take lead in questioning a candidate and may interchange the next candidate. OSCE examination Objective The objective of OSCE are to assess the skills in -clinical decision making. -Detection and interpretation of clinical findings and laboratory data. -Performance of a particular component of the clinical examination and counseling. -Identification of a management plan. What do the examiners do for the "OSCE" examination? Examiners will select the slides, x-rays, laboratory reports, ECG reports, heart sounds and other items to be kept in the OSCE stations one day prior to the date of examination. These stations will consist of unobserved/static and observed/interactive stations. On unobserved/static stations the candidate will be presented with a clinical case, laboratory data, x-ray, ultra sound, CT scan, instrument, heart sounds etc and will be asked to give written responses to questions asked. In the observed/interactive stations the candidate will have to perform a procedure for example counseling, assembling the instrument etc. One examiner will be present in these stations who will rate candidates performance based on the check lists.
XII. Faculty members: 1. Dr. Ramesh K Adhikari Professor 2. Dr. Prakash S Shrestha Professor, HOD 3. Dr. Pushpa R Sharma Professor, MD co-ordinator 4. Dr. Fakir C Gami Assoc. Professor 5. Dr. Laxman Shrestha Assist. Professor 6. Dr. Siva Shrestha Assist. Professor 7. Dr. Ranendra PB Shrestha Visiting Professor 8. Dr. Neelam Adhikari Visiting Professor
XII. Teaching/ Working Places:
1. Tribhuvan University Teaching Hospital, Kathmandu. 2. Kanti Children’s Hospital, Kathmandu. 3. Patan Hospital, Patan. 4. Siddhi Memmorial Mother and Child Hospital, Bhaktapur. 5. Seminar and presentations at Meeting Hall of Health learning Material Center,
IOM, Maharajgunj..

17