dental sealants: proven to prevent decay - s3.amazonaws.comsealant+report+2014.pdf · dental...
TRANSCRIPT
DentalSealants:ProventoPreventToothDecay
ALookatIssuesImpactingtheDeliveryofStateandLocalSchool‐BasedSealantPrograms
May2014

TheChildren’sDentalHealthProject(CDHP)extendsdeepthankstoallwhoprovidedinformation,dataandtechnicalreviewofthisreport,includingstatepublichealthdentalleaders,theCentersforDiseaseControlandPrevention,CentersforMedicareandMedicaidServices,AssociationofStateandTerritorialDentalDirectorsandtheHealthResourcesandServicesAdministration.CDHPisanindependentnonprofitbasedinWashington,D.C.CDHPworkstoimproveoralhealthforchildrenandfamiliesbyidentifyingandadvancingsolutionsthatareinnovativeandcost‐effective.CDHPpromotesstrategiesthataregroundedinthebestavailableresearchandwhereevidenceislacking,leadseffortstoexplorenewapproaches.Tolearnmore,visitwww.cdhp.org.
Note:MaterialsforthisprojectwerepreparedbytheChildren’sDentalHealthProjectandconsultants.ThereportwassupportedbyCentersforDiseaseControlandPreventionCooperativeAgreementNo.5U58DP002285‐04totheChildren’sDentalHealthProject.ItscontentsaresolelytheresponsibilityoftheauthorsanddonotnecessarilyrepresentofficialCDCviews.

TableofContents
Methods……………………………………………………………………………………………….1
Findings……………………………………………………………...........................................4
Featuresof5StateswithSustainableandSubstantialSchoolSealantPrograms(SSPs)…………………………..……………………………..11KeystoSuccessforSustainableandSubstantialSSPs……..………………….14
TranslatingLessonsLearnedintoPractice…..…………………………………….17
Conclusion……………………..…………………………………………………………………..20
1
chool‐baseddentalsealantdeliveryprogramsareanevidence‐
basedpublichealthstrategyforpreventingtoothdecayamong
school‐agedchildren,particularlythoseathighestrisk.1Dental
sealantsareprotectivecoatings,generallyappliedtochildren’spermanent
teeth,whichhavebeenshowntoreducetoothdecayby60percent.2The
CommunityPreventiveServicesTaskForcerecommendsschool‐based
sealantdeliveryprograms,reflectingevidencethattheseprograms
“increasethenumberofchildrenwhoreceivesealants…andthatdental
sealantsresultinalargereductionintoothdecayamongschool‐aged
children(5to16yearsofage).”3
Thisreportprovidesanoverviewoftheprogramdesignandkeyissuesin
school‐baseddentalsealantprogramsintheU.S.Itoffersexamplesoffactorsthat
mayfacilitateorcomplicateprogramfinancing,reach,andsustainability.It
considersfeaturesoffivestates—IL,NY,OH,SC,andWI—thathavehad
longstandingschoolsealantprogramsandexplorescurrentandpotentialchallenges
forimplementingsuchprograms.Finally,thereportprovidesrecommendationsfor
allwhoareengagedinpromotingchildren’soralhealththroughschoolsealant
programs(SSPs).
Informationforthisreportwasobtainedbetween2011and2013andincluded
surveysofstateoralhealthofficialsandselectSSPprogramofficials,qualitative
structuredinterviews,andin‐depthcasestudies,allconductedunderacooperative
agreementbetweentheChildren’sDentalHealthProjectandtheCentersforDisease
ControlandPrevention.
METHODS
Thisprojectdefinedstateswith“sustained”school‐basedsealantprogramsas
havingoneormoreSSPoperatingeachyearfor10years(2003—2012),asself‐
reportedbystatesintheannualAssociationofStateandTerritorialDentalDirectors
(ASTDD)StateSynopsisReports(“SynopsisReports”)4.Toassesswhetherastate’s
2
SSPsreacheda“substantial”numberofchildren(approx.10,000eachyear),the
state’smostrecentSynopsisReportsdataonchildrenserved(2011or2012)was
dividedbythenumberofschool‐agedchildrenasreportedbytheUSCensus.*Based
onthesedata,wecontacted13StateOralHealthProgramsformoredetailed
information.Sevenstateofficialsagreedtocompleteapre‐tested34‐question
questionnaire(AppendixA)anda90‐minutetelephoneinterviewwithfollow
up.Fromthesemoredetailedassessments,fivestates(IL,NY,OH,SC,andWI)were
selectedforcasestudies.
Tocapturesealantactivitiesinthe37states(andtheDistrictofColumbia)that
didnotmeetthedefinitionofhaving“substantialandsustainedSSPs,”thoseState
OralHealthProgramDirectorswerequeriedthroughane‐mailed15‐question
survey(AppendixB).Fourlistservs†werealsoqueriedfortheidentitiesoflocal
SSPsthathadeitheroperatedfor10consecutiveyearsorprovidedsealantstoat
least10,000childreninoneprogramyear.Tofurtherbuildunderstandingofhighly
regardedSSPsatthelocallevel,respondentswereaskedtoidentifyonelocal
programthat“mightbethebestinthecountry.”Theseprocessesidentified36local
SSPswhowerethenemailedan8‐questionsurvey(AppendixC),towhich27local
programsin22statesresponded.Theirresponsesinformedthefindingsinthis
report.
Thisreportreflectsthebestavailableinformationasprovidedbykey
informants.However,sealantprogramsareinconstantfluxandreported
informationmaynotcaptureallfactorsthataffectSSPs’reachandsustainability.
Thereportalsobuildsonandcomplementssignificantreportsandresources,
including:a2013reviewbythePewChildren’sDentalCampaignofstates’
* *Penetration was grossly estimated by dividing the number of children the respective SOHPs were able to document as having received sealants via SSPs for the most recent year for which they had complete data (2011‐12 or 2010‐11) by the number of school‐aged children in the state according to the 2010 U.S. Census. † 1. *University of Pittsburgh. Pitt Dental Public Health Mailing List. Referenced at: https://list.pitt.edu/mailman/listinfo/dental‐public‐health; 2. Association of State and Territorial Dental Directors (ASTDD) ListServ. Referenced at: http://www.astdd.org/membership‐benefits/; 3. National Network for Oral Health Access (NNOHA) Listserv. Referenced at: http://www.nnoha.org/join/nnoha‐listserv/ ; 4. Community Oral Health Programs E‐mail Discussion List. Referenced at: http://lists.mchgroup.org/listinfo.cgi/cohp‐mchgroup.org.
3
performanceonfoursealantmeasures;‡earlierrecommendationsmadebythe
collaborativeWorkshoponGuidelinesforSealantUsein1994;5theCommunity
TaskForceonPreventiveServicesin2013;6theAmericanDentalAssociation’s
CouncilonScientificAffairsin2008;7andtheCDC‐sponsoredexpertworkgroupin
2009;8aswellasmaterialsprovidedbySealAmerica©9andtheNationalMaternal
andChildOralHealthResourceCenter.10Itseekstocomplementinformationfrom
ASTDD’s“BestPracticeApproachReportonSchool‐basedDentalSealantPrograms”
(availableatwww.astdd.org/school‐based‐dental‐sealant‐programs‐introduction/)
byprovidingacomprehensiveassessmentofSSPsandhighlightingcharacteristics
thatsupportefficiencyandeffectiveness.
‡ 1. The prevalence of programs in “high‐need schools”; 2. Allowance of sealant placement by hygienists without a prior dentist examination of the child; 3. Compliance with data collection and reporting; and 4. Attainment of national sealant oral health objectives.
4
FINDINGS
DiversityofModels
Takentogether,studyinformantsidentifiedmorethan640SSPs;most
reportedlydeliversealantsaspartofabroaderschool‐affiliatedcariesprevention
programwhichmayincludedentalscreening,dentalprophylaxis,topicalapplication
offluorides,andoralhealtheducation.InformationonSSPdesignwasprovidedby
39statesandtheDistrictofColumbia.Ofthose,27statesreportthat“allormost”
SSPswerepartofbroadercariespreventionprogramsand13reportthat“atleast
some”SSPswerepartofsuchprograms.
RolesofStateOralHealthPrograms(SOHPs)
Nearlyallofthe40SOHPsrespondingreportinvolvementwithSSPs,though
theyhavevariedrolesinprogramdesign,operation,funding,oversight,and
regulation.Ingeneral,SOHPshavegreaterinputandcloserpartnershipswhenthey
providedirectfundingtolocalSSPs.
Almosthalf(n=23)§ofreportingstatesindicatedthattheirSOHPprovides
fundingtolocalentitiestooperateschoolsealantprograms.Threestates(MA,ND,
NM)reportedthatSOHPsprovidegrantsforSSPsinadditiontooperatingtheirown
SSPs.FourSOHPs(AR,CT,SC,UT)reportedprovidingnodirectfundingforSSPsbut
supporttheseprogramsthroughfacilitation,coordination,regulatoryaction,and/or
reporting.
SOHPsin13statesweredirectlyinvolvedintheoperationofSSPs:five(DC,DE,
NC,OR,TX)byprovidingorcontractingforSSPstaff;five(GA,LA,MS,TN,VA)by
fundingandcollaborativelyoperatinglocalSSPs;andthree(MA,ND,NM)byfunding
localSSPsandalsooperatingtheirownSSPs.
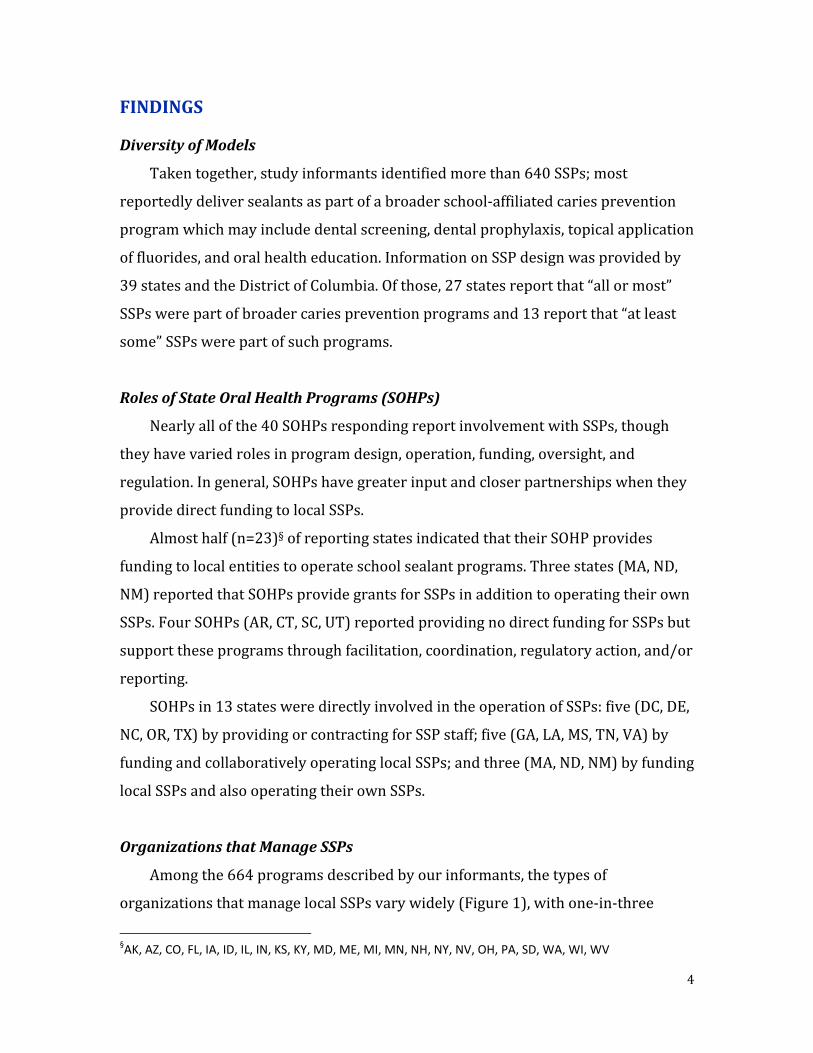
OrganizationsthatManageSSPs
Amongthe664programsdescribedbyourinformants,thetypesof
organizationsthatmanagelocalSSPsvarywidely(Figure1),withone‐in‐three
§AK, AZ, CO, FL, IA, ID, IL, IN, KS, KY, MD, ME, MI, MN, NH, NY, NV, OH, PA, SD, WA, WI, WV
5
programsdeliveredbylocalhealthdepartments;one‐in‐sixdeliveredbyeither
federallyqualifiedhealthcenters(FQHCs),non‐profitorfor‐profitagencies;and
smallerproportionsbycolleges/universities,schooldistricts,andhospitals.While
SOHPsareoftenengagedwithSSPs,only1%ofprogramsweredelivereddirectlyby
stateoralhealthprograms.
Figure 1 (N=664 programs)
RegionalPatterns
Differenttypesoforganizationsclusterregionally.
Midwesternstates(IA,IL,OH,WI)arehometo75%ofSSPsmanagedbylocal
orcountyhealthdepartments;Southernstates(FL,GA,NC,TN,VA)arealso
characterizedbyhavingstrongaffiliationswithhealthdepartments.
FQHC‐affiliatedSSPsarestronglyrepresentedintheNortheast(CT,MA,NH,
NY,RI)andafewMidwesternstates(IL,KS,MI,WI)andinWV.NineSOHPs
reportedfiveormoreFQHCsoperatingSSPsintheirstates.
For‐profitSSPprovidersarereportedtooperatein20states;12states
reporthavingmorethanonefor‐profitSSP.Ofthefor‐profitSSPsreported,60%are
foundinthreestates:IL,MA,andWA.For‐profitcompaniesalmostexclusivelyserve
childMedicaidbeneficiariesandsomeextendsomeservicetouninsuredchildren
throughaffiliatedfoundations.
6
FinancingSources
FederalsourcesoffinancingthatcanbeusedtosupportSSPsinclude:
StateOralHealthGrants:competitive5yearcooperativeagreementswith
statesfromtheCentersforDiseaseControlandPreventionDivisionofOral
HealththroughitsState‐BasedOralDiseasePreventionProgram;
FundingtostatesfromtheTitleVMaternalandChildHealthServicesBlock
GrantProgramthatstatesmayallocatetooralhealthprograms;
GrantstostatesundertheHealthResourcesandServicesAdministration
(HRSA)BureauofHealthProfession’sStateOralHealthWorkforceGrants;
and
ReimbursementsfromMedicaidthroughthestate‐administeredEarlyand
PeriodicScreeningDiagnosticandTreatment(EPSDT)pediatricdentalbenefit
andthestate’sChildren’sHealthInsuranceProgram(CHIP)(instatesthat
maintainCHIPplansseparatelyfromMedicaidEPSDT).
Inaddition,statesandlocalesmayprovidedirectfundingforSSPsthrough
generalrevenuesbywayofgrants,contracts,andcooperativeagreements;also,
foundations,professionalassociations,andothernon‐profitsmayprovidecharitable
financing.Industrymayprovidediscountsfordentalmaterialsandsuppliesto
safety‐netprogramsincludingSSPs.Whilenotcommon,SSPsmayalsocollectfees
fromcommercialinsurerswhenchildrenservedhaveprivatedentalcoverage.
Amongfederalprograms,CDC’sState‐BasedOralDiseasePrevention
ProgramprovidesthemostfocusedfundingforSSPs.Twenty‐onestatesreceive
thissupport**to“strengthentheiroralhealthprogramsandimprovetheoralhealth
oftheirresidents.”11Amongtargetedexpendituresare:
supportforastate‐widesealantcoordinator,
** CO, CT, GA, HI, ID, IA, KS, LA, MD, MI, MN, MS, NH, NY, ND, RI, SC, VT, VA, WV, WI. In 2010, Congress authorized the expansion of CDC program funding to all states through The Patient Protection and Affordable Care Act. Authorized expansions will require future Congressional appropriations.
7
Twenty‐one states receive CDC support for school‐based sealant programs. This funding covers various needs, including state‐wide sealant coordinators and data collection.
translatinganddisseminatingthescience
supportingschool‐basedsealantprogramsas
aneffectivepreventiveintervention,
monitoringdataforprogramefficiencyand
reach,
carryingoutBasicScreeningSurveysfor3rd
graders,and
fundingforportablesealantequipment.
TheTitleVMaternalandChildHealthServicesBlockGrantProgramisa
federalpartnershipwithstatesthatsupportsawiderangeofpublichealth,
infrastructure,andclinicalservicestargetingwomenandchildrenwithafocuson
specialneedspopulations.12FundscancomplementMedicaidandCHIPfee‐for‐
servicepaymentsby“providinggap‐fillingservicestoenrollees;assistinginthe
identificationofpotentiallyeligiblebeneficiaries;andcreatinganinfrastructurein
communitiestoensurethatthecapacityexiststosupportthedeliveryofquality
healthcareservicesforwomenandchildren.”13TheMaternalandChildHealth
Bureau(MCHB)alsonotesthat“successfulcoordinationofTitleVwith
Medicaid/CHIPprogramsassistsinmaximizingFederal,Stateandlocalfundsto
meetthehealthcareneedsoflow‐incomewomenandchildren.”14Manystates
utilizeTitleVfundingtosupportSOHPfunctionsincludingthedesign,
implementation,andmonitoringoftheirSSPs.ExamplesincludeIllinois’useofTitle
Vfundstoprovidesealantstohigh‐caries‐riskchildrennoteligiblefor
Medicaid/CHIPandNewYork’ssignificantexpansionofitsSSPwithTitleVsupport
in1995.
TitleV,withabreadthofmaternalandchildhealthinterestsandcollaborations,
alsoprovidesaplatformforSOHPstopromoteoralhealthwithpartnergroupsand
tohighlighttheimportanceoforalhealthanddentalcarewithmaternalandchild
communitiesofinterest.Forexample,WI’s2010MCHBNeedsAssessmenttoIdentify
Prioritiesfor2011‐2015identifiedtheSOHPasa“PrimaryPartner”inreachingthe
8
MCHBNationalPerformanceMeasure(#9)onthe“percentofthird‐gradechildren
whohavereceivedprotectivesealantsonatleastonepermanentmolartooth.”
Acrossstates,SSPscontributevariablytothefulfillmentofthismeasure’sstate‐
specificannualgoal.15Forthelatestyearavailable††,therangeofperformancefor
thismeasurewas13.8%inFloridato73.6%inDelaware,withanaverageacrossall
statesof42.3%.
MCHBintermittentlyreformulatesitssetofrequiredTitleVPerformance
Measuresandisexpectedtoissuethenextsetin2015.Whilethesealantmeasure
hasservedSSPswellinhighlightingtheimportanceofdentalsealantstochildren’s
oralhealthandintrackingprogressinreachingHealthyPeopleoralhealth
objectives,it—likeallsuchmeasures—issubjecttorevisionorelimination.
StateOralHealthWorkforceGrantsadministeredbyHRSAcompetitivelyfund
10statestoimplementoneormoreof13designatedactivitiesthathelpstates
expandtheiroralhealthworkforceindentalhealthprofessionalshortageareas.
Amongallowableactivitiesare“community‐basedpreventionservicessuchas…
dentalsealantprograms”andotheractivitiesthatcansupportSSPs,including
teledentistry,mobiledentalprogramsinunderservedareas,supportofdental
trainees,and“thedevelopmentofaStatedentalofficerpositionortheaugmentation
ofaStatedentalofficetocoordinateoralhealthandaccessissuesintheState.”16
Inearlierfundingcycles,29stateshaveutilizedgrantfundstosupport
community‐basedpreventiveservices‡‡includingOhiowhichusedfundingto
expanditssealantnetwork.
MedicaidandCHIPreimbursementsareacriticalrevenuesourceforSSPs:21
of23localprogramsrespondingtooursurveyreportbillingMedicaid.Although
Medicaidisasustainablefundingsourceforchildren’sdentalcarethatmaybe
utilizedbySSPs,statesvaryconsiderablyinpaymentratesandinadministrative
rules,policies,andpracticesthatimpactSSPs’accesstothissourceoffunding.
†† 2012 reports from all states except FL which reported 2011 data ‡‡ Analysis by Tener Huang and Burton Edelstein reported in a 2014 NOHC abstract
9
Billing:Aswithallproviders,SSPsthatbillMedicaidareimpactedbyclaims
processingrules,numbersandtimingofsimultaneousclaimsbyprovideror
location,claimsreview
procedures,claimsformatsand
submissionprocesses,and
timelinessofpayment.
Allowableprovidersandservice
locations:Whilemoststatesallow
hygieniststoprovidesealantsin
SSPs,programsareimpactedby
Medicaidinterpretationofstate
licensurepoliciesonlevelsofsupervisionofhygienistsandscopeofpractice,
provisionofuniquebillingcodesforhygienists,anddisallowanceofsealant
billingintheabsenceofadditionaldentalservices,suchasdental
examinationsandradiographs.
Services:StateMedicaidpoliciesoftenproscribetheageofchildreneligible
forsealantbenefitsorregulatetheparticularteeththatcanbesealedaswell
asthefrequencywithwhichpaymentwillbemadeforre‐sealingteeth.
Programtypes:Statepoliciesvaryonthetypesofprogramsthatcanbill
Medicaid,forexampleprohibitingclaimsfrommobiledentalprogram
operatorsorschooldistricts.AsstateMedicaidprogramsshiftintomanaged
carecontractingfordentalservices,SSPsmaybefurtherimpactedasnon‐
networkproviders.
“FreeCareRule”:Federalhealthinsuranceprograms,includingMedicaidand
CHIP,prohibithealthcareprovidersfromchargingmoreforservices
deliveredtopublicbeneficiariesthanarechargedotherpayers,including
commercialinsurersandtheuninsured.SinceSSPsaretypicallydesignedto
deliversealantservicestostudentswithoutcharge(i.e.,“freecare”),anSSP’s
abilitytobillforsealantsdeliveredtoMedicaid‐eligiblechildrenisimpacted
10
Medicaid and CHIP reimbursements are a critical revenue source for SSPs. Yet states vary widely in payment rates and in the rules, policies, and practices that impact SSPs’ access to this funding.
bytheirstate’sinterpretationofthispolicy.Significantly,onOctober8,2013
theU.S.DepartmentofHealthandHumanServicesOfficeofInspector
General(OIG)addresseditsMedicaidenforcementpolicybystatingthatfree
careprovidedtoneedychildrenwhoareuninsuredorunderinsureddoesnot
affectdeterminationofcustomarycharges
andallowablebillableamountsfor
servicesprovidedtoMedicaidbene‐
ficiaries.17Whilewritteninresponsetoa
specificappeal,thisOIGOpinionmayhelp
statesimplementtheMedicaidfreecare
policymoregenerallybyclarifyingthat
federalMedicaidenforcementpolicyis
liberalwithregardstofreecarefor
financiallyvulnerablechildren—allowingbothMedicaidbillingandfreecare
fortargeteduninsuredorunderinsuredchildren.Theopinion,however,is
limitedwithregardtorequirementstobillnon‐governmentalinsurers.
ClearlyneededisauniversalrulingbyMedicaidthataddressesthe
appropriatenessofbillingMedicaid,butnotothers,throughSSPs.
Inadditiontoservice‐specificfeespayablebyMedicaid,thefederal
governmentsupportsstatestoadministerMedicaidthroughan
“AdministrativeMatch”forwhichthefederalgovernmentpaysstatesone
dollarforeverystatedollarcommittedtoprogrammanagement.Illinoishas
utilizedthisAdministrativeMatchforitssealantprogrambyhavingthe
SOHPprovidequalityassuranceservicestoMedicaid.TheSOHPreviews
operationsofallSSPsthatbillMedicaid,conductsannualstructuredsite
visitsoftheseprograms,providesadministrativeservicesrelatedto
providingsealantstoMedicaidbeneficiaries,andprovidesinformationto
Medicaidonevidence‐basedoralhealthservices.
11
FEATURESOF5STATESWITHSUSTAINABLEANDSUBSTANTIALSSPs
Thelessonlearnedfromcomparingandcontrastingfivestatesthatmeetcriteriafor
bothsustainabilityandsubstantialreachisthatthereisno“one‐size‐fits‐all”
approachtoSSPsuccess.Acrossthesestates,variationsexistinSOHProles,funding
sources,Medicaidpolicyonbillingbynon‐dentistproviders,andattendantstate
policiessuchasMedicaidmanagedcarecontracting,requirementsforschool‐entry
dentalexaminations,andpresenceofschool‐basedhealthcenters.
Illinois(SSPsince1986):PaymentstoSSPsarereceivedforthree‐quartersof
treatedchildreneitherfromMedicaid/CHIPorfromstatefundsallocatedto
childrenwhoareeligibleforsubsidizedschoollunchprogramsbutnotenrolledin
Medicaid/CHIP.Thestateallowsgranteesflexibilityinprogramdesignanddelivery
toaddresslocalconditionsandrequiresgranteestoprovidedentalexaminations
consistentwithastatemandatoryschooldentalexaminationlawpassedin2006.
TheSOHPconductsannualsitevisitsofbothgranteeandnon‐granteeSSPs.Sealant
programspredominateinChicagowheretwo‐thirdsofthestate’sSSPsprovide
moresealantstochildrenthananyotherlocalityorstateinthenation.An

12
To enhance efficiency, Ohio contracts with a small number of SSPs that each serves multiple schools.
interagencyagreementbetweentheChicagoDepartmentofPublicHealthandthe
ChicagoPublicSchoolsgovernstheprogramwhichisdeliveredbyfor‐profit
vendorsthatpayanadministrativefeetoparticipate.
NewYork(SSPsince1972):Thestate’sSOHPhaslegalauthoritytosetstandards
for,approve,andmonitoralloralhealthservicesprovidedinpublicschools.The
staterequiresalloralhealthprogramsinschoolstobeaffiliatedwithschool‐based
healthcentersthatprovideprimarydentalcareservices.Itprovidesfunding
throughitsTitleVBlockGrant.Asthestatewiththelongest‐runningSSP,NewYork
hasextensiveexperienceinadaptingtochangingdeliveryandfinancingconditions.
RespondentsreportthatNewYorkiscurrentlychallengedbythreetrendsthatexist
tovaryingdegreesinotherstates:(1)Medicaid’sincreasingdependenceon
managedcarethathasrequiredthestatetoseek“carveouts”allowingcontinued
paymentstoSSPsforchildrenreceivingsealantsinschools;(2)theintegrationof
schoolsealantprogramsintodentalpreventionandtreatmentprogramsthatbegan
in2006‐7;and(3)changingconceptsoftherolesoflocalitiesinpublichealth
reflectedindecreasedprovisionofdirectcarecomplementedwithincreased
provisionoforalhealthpromotionandpubliceducation.
Ohio(SSPsince1984):OhioutilizedTitleV
fundingtooperate18of22localhealth
departmentSSPswhichexclusivelyprovide
sealantservices.SSPsbillMedicaidforsealant
placementsbutnotfordentalexamination,thus
allowingtheexaminationtobeperformedandbilledbyproviderswhomayseethe
childlatertoprovideotherdentalservices.Toenhanceefficiency,Ohiocontracts
withasmallnumberofSSPsthateachservesmultipleschools.Ithasuseda2010
HRSAStateOralHealthWorkforcegranttodevelopastrategicplansupportingSSP
expansionsandrefinementsandhasdevelopedawidely‐usedstateSealantProgram
Manual(availableat
http://www.odh.ohio.gov/~/media/ODH/ASSETS/Files/ohs/oral%20health/Dent
al%20Sealant%20Manual%202012.ashx)andDistanceLearningCurriculum
13
(availableathttp://www.ohiodentalclinics.com/distancelearning.html).TheSOHP
collectsandutilizesdatatomanageandreportontheprogram.
SouthCarolina(SSPsince2003):Thestate’sSOHPprovidesnofundingforSSPs
whichrelyinsteadonMedicaidbillingfor96%ofchildrenserved.Thestatehas
regulatoryauthoritytoapprovedentalhygienistsasprovidersinschoolsunderan
arrangementcalled“publichealthsupervision”governedbyamemorandumof
agreement(MOA).TheSOHPmaintainsan“internalsealantmanagementteam”that
providessupportforandevaluation
ofSSPs.SixSSPsoperateinthestate,
fourunderSOHP‐hygienistMOAs,
withoneprovidingsealantstoover
80%ofSouthCarolinachildren
served.TheSOHPcreditssupport
andcollaborationoftheSouth
CarolinaOralHealthCoalitionwith
itssuccessinbuildingschoolsealantprogramcapacity.
Wisconsin(SSPsince1996):Since2001,thestate’sSOHPhaspartneredwiththe
non‐profitChildren’sHealthAllianceofWisconsintoobtainandleveragemultiple
publicandprivatefundingsourcesandsteadilyexpandSSPs’reachtovulnerable
children.Respondentsreportthatstateleveladministrationprovidescentralized
structurewithroomforlocalimplementation,providingsomeflexibilitytotailorthe
programtocommunitycircumstances.Partnersreportcommitmenttorigorous
datacollectionanduseofthedataforprogrammanagementandreporting.State
policiesallowhygieniststopracticeinpublichealthsettings,includingschools,
underadentist’sgeneralsupervisionandtoplacesealantswithoutarequirement
thatadentistfirstexaminethechild.Medicaidcanbebilleddirectlyforboth
sealantsandanoralhealthassessmentprovidedinschools.
14
KEYSTOSUCCESSFORSUSTAINABLE&SUBSTANTIALSSPs
1. Financing:Whilefinancingiscentraltoallprograms’success,thesurveysand
casestudiesrevealthatavarietyoffinancingapproachescansupporteffective
SSPs.Examplesrangefrompublic‐privatefinancingpartnerships,tomarket‐
drivenmodels,toexclusivelyMedicaid‐financed.
SeenascriticallyimportantisthecapacityofSSPstobillMedicaid/CHIPwhen
providingservicestoenrolledchildren.SOHPsmustworkcollaborativelywith
stateMedicaidprogramstofacilitateSSPoperationsbyreducingcited
administrativebarriersandbyaddressingimpedimentscreatedbysomestates’
interpretationsofthefederal“freecare”rule.Featuredstateswerealsonotably
effectiveinsecuringstatesupportfortheirsealantprogramsthroughallocation
offederalTitleVblockgrantfundsandinsecuringcompetitivefundingthrough
CDC‐sponsoredcooperativeagreementstosupportStateOralHealthPrograms
andinHRSA‐sponsoredOralHealthWorkforceGrants.
2. Partnershipsandcollaborations:Inadditiontohavingpartnershipswithstate
Medicaidauthorities,successfulSOHPswereleadersandfacilitatorsthat
15
Successful states like Wisconsin used data to create persuasive arguments for state and private financing of SSPs.
arrangedpartnershipagreementsandformalizedcontractsforqualitycontrol
andadministrativesupportoflocalSSPs.Statesalsoleverageddataasin
Wisconsin,whichcreatedpersuasiveargumentsforstateandprivatefinancing.
FeaturedSOHPsaresubstantiallyinvolvedinsupportingadministrative
structuresandaccountability.
3. Efficiencies:Supportingthecostefficiencyand
reachofSSPs,threeofthefivestatesprofiled
havepracticeactsthatpermitdentalhygienists
topracticeinpublichealthsettingsunder
generalsupervision.Efficientprogramsalso
maintainedeffectiveadministrativestructuresandtrackedaccountability.One
state(WI)refineditsdatacollectionanddataanalysestodemonstrate
efficienciesandprogramcost‐effectiveness,therebyattractingsignificant
fundingfromtheprivatesector.§§
4. Adaptability:Featuredprogramsrecognizeandrespondcreativelytotheever‐
changingpolitical,policy,andadministrativecontextswithinwhichtheydeliver
sealantservices.Amongthesearechangingstatepracticeactsthatgovernthe
availabilityandconditionsunderwhichallieddentalprofessionalscan
participateinSSPsandtheevolutionofMedicaidmanagedcarethroughwhich
contractedvendorsbecomesignificantplayersindeterminingthecomposition
ofprovidernetworks.TheAffordableCareActwilllikelyimpactSSPsby
authorizingexpansionsofschool‐basedhealthcenters,bypeggingdental
benefitsforchildrento“benchmarkdentalplans”thatalmostuniversallyinclude
coveragefordentalsealantstoage16,andbydeterminingthattheonly
preventiveservicesthatmustbeprovidedatnocosttothebeneficiaryarethose
receivinganAorBrecommendationfromtheUnitedStatesPreventiveServices
§§ Wisconsin’s model for collecting and reporting data is being adapted by three states in 2014 through the CDC’s Cooperative Agreement with the Children’s Dental Health Project.
16
TaskForce(USPSTF).TheUSPSTFdoesnotmakerecommendationsforservices
deliveredbydentalpersonnel.***
ClearlyevidentfromthesefourkeystosuccessisthatSOHPleadershipis
essentialinleveragingopportunitiesandcreativelyrespondingtolocal
circumstancesindesigning,implementing,monitoring,andsustainingSSPs.
Effectiveleadershipinvolves:
workingcloselywithotherstomutuallybuildcapacitybasedonshared
goals;
measurementbasedonrelevantmetrics;
mutuallyreinforcingandcomplementaryactivities;and
ongoingcommunicationthatbuildsstakeholderinvestment.
SubstantialreachandsustainabilityofstateSSPsalsorequiresthatSOHPs
leveragemultiplefundingapproachestomaximizefinancialsupportfortheir
programsfrombothgovernmentalandnon‐governmentalsources.
17
The nearly 20‐year‐old guidelines for sealant use in community programs need to be updated. Then these revised guidelines must be promoted by federal, state and local officials who oversee sealant programs.
TRANSLATINGLESSONSLEARNEDTOPRACTICE
Translatinglessonsgleanedfromthisreportandfromadditionalsourcesinto
greateravailabilityofsealantstohigh‐riskUSchildreninschoolswillrequireactive
collaborationandcommitmenttoSSPsamongmultipleplayersincludingsealant
experts,publichealthleaders,thedentalprofessionalcommunity,schoolofficials,
Medicaidofficials,andstateandfederalpolicymakers.
First,thenearly20‐year‐oldguidelinesfor
sealantuseincommunityprogramsneedtobe
updated.Fromthere,strongandpersistent
promotionofrevisedguidelinesbyfederal,stateand
localauthoritieswithinfluenceoversealant
programswillbeessential.
Suggestedstepsinclude:
1. ConveneanexpertSSPSustainabilityWork
Grouptocollaborativelyreviewavailable
informationandrecommendordevelopnewstrategiesforinclusioninASTDD
BestPracticeApproachesandnewresources,asappropriate,inexisting
authoritativeProgramGuidance(e.g.,throughtheAmericanAssociationof
CommunityDentalPrograms’[AACDP]SealAmericamanual).ThisWorkGroup
maybeginbyconsideringthefollowingneedsthathaveemergedfromSSPs:
businessplanningtemplate(addressingfundingsources,staffing,etc.);
protocolforanalyzingandimprovingsealant‐relatedprogrampolicies;
resourcestoassistinassessingandaddressingbarrierstoparticipation(e.g.,
parentalconsent,cooperationofolderchildrenandmiddleschool
personnel);
systemsforeasilyacquiringpatientidentificationnumbersneededfor
Medicaidreimbursement;
protocolsforcollecting,presentingandusingdatatogainnewresourcesand
maintaincurrentfunding;and
18
samplepartnershipagreements.
2.ConveneanexpertSSPDesignandOperationsWorkGroup,primarilyto
updateprogramplanningguidelinesfromthe1994WorkshoponGuidelinesfor
SealantUsethatwerenotaddressedintheCDC’s2009“Updated
RecommendationsandReviewsofEvidence”andhavenotbeenrevisitedsince.
UsingtheWorksheetforDeterminingtheNeedforCommunitySealantPrograms
andDesigningaDirectServiceCommunitySealantProgram
(http://www.dentalcare.com/media/en‐
US/education/ce128/WorkshopGuidelinesSealantUse.pdf),sections1through6,
thisworkgroupcouldbeginbyconsideringthefollowingitemsthathave
emergedfromthisstudyandfromdiscussionswiththosewhooperateSSPs:
strategiesforidentifyingandreachingappropriatehigh‐riskorvulnerable
populations;
strategiesforprovidingappropriateservicesundertheconditionsofschool‐
based/linkedprograms(e.g.,relyingonevidencetodeterminewhich—if
any—servicesaddvalueforparticularchildrenreceivingsealants,andtooth
selectionguidancethattargetshard‐to‐reachpopulationssuchasmiddle‐
schoolchildrenwith2ndmolardevelopment);
strategiesforconnectingchildrenwithsourcesofdentalcarewhile
maintainingadequatepersonneltimetomaximizetheprimaryprogram
objectiveofsealantplacement;
protocolsforshort‐andlong‐termsealantretentionratechecksandother
clinicalqualityassessments;and
protocolstomonitorprogramoperationsforqualityimprovementpurposes
(e.g.,dataonrateofconsentreturn,numberofchildrenreceivingvarious
levelsofservice).
3. ConveneanexpertSSPFacilitatorsandBarriersWorkGrouptoreviewand
analyzefederalandstatepoliciesthatmayfacilitateoractasbarrierstoSSPs,
withinputfromoralhealth,publichealth,andpublicfinancepolicyexperts.This
19
thirdWorkGroupshouldmakespecificrecommendations,includingmodel
policies,topromoteexpansionofcost‐effectiveandefficientSSPs.
OncetheseWorkGroupshavecompletedtheirreports,thecombinedinfluence
ofpublichealthagenciesatalllevelsandoftheirorganizationalpartnerswillbe
criticalbothfordisseminatingnewguidanceandensuringsuccessinincorporating
theupdatedrecommendationsintopractice.Determinativeorganizationalactors
include:
Federalagencies—withcapacitytodrawoninter‐agencycollaborationand
partnerorganizationsupport—toinfluenceimplementation;
StateOralHealthProgramstoinfluenceand/orimplement;and
Localandstate‐operatedSSPstoinfluenceandimplement.
Federalandstateoralhealthofficialshavesignificantoptionsandresourcesto
exercisesuchleadership.TheAssociationofStateandTerritorialDentalDirectors’
BestPracticeApproachreportondentalsealantsisarichresourcethatisregularly
updated.Findingsofthisreport
pointstatestoavarietyof
financinganddeliveryoptions,
partnershipsandcollaborations,
andefficienciesforsustainable
andsubstantialprograms.
Further,thesurveyinstruments
developedforthisreport(see
AppendicesA,B,C)canbe
readilyadaptedbystatesto
closelyexaminetheirsealant
activities.
TechnicalassistanceisavailablethroughCDCandHRSAresourcesandtheir
grantees.ConsultationwithSOHPDirectorswhohavesuccessfullyprioritizedSSPs
20
intheirstatescanfurtherassistallwhoarecommittedtoimprovingchildren’soral
healthandequitythroughSSPs.
CONCLUSION
ThecostofpreventingtoothdecaybyplacingdentalsealantsthroughSSPsis
muchlessthanthecostoftreatingtoothdecaythatwasnotprevented.By
expandingthereachandeffectivenessofSSPs,stateagenciesandtheirpartnerscan
preventthemostcommoncavitiesinthepermanentteethofschool‐agechildren.
Preventionisapowerfultoolforpotentialcostsavingsandformeasurable
improvementsinthehealthandwellbeingofchildrenwhoareatgreatestriskfor
thesignificantconsequencesofunaddressedtoothdecay.Thelessonshighlightedin
thisreportareofferedtohelpprovidefocusandtoassistinmeetingthosegoals.
21
NOTES 1 The Guide to Community Preventive Services. Preventing Dental Caries: School‐Based Dental Sealant Delivery Programs. Accessed at: http://www.thecommunityguide.org/oral/schoolsealants.html 2 Truman BI, Gooch BF, Sulemana I, et al. Reviews of Evidence on Interventions to Prevent Dental Caries, Oral and Pharyngeal Cancers, and Sports‐Related Craniofacial Injuries. Am J Prev Med 2002;23(1S)21‐54. 3 The Guide to Community Preventive Services. Preventing Dental Caries: School‐Based Dental Sealant Delivery Programs. Accessed at: http://www.thecommunityguide.org/oral/schoolsealants.html 4 U.S. Department of Health & Human Services, Centers for Disease Control and Prevention (CDC). Synopses of State and Territorial Dental Public Health Programs. Accessed at: http://apps.nccd.cdc.gov/synopses/ 5 Siegal MD, Kumar JV. Workshop on Guidelines for Sealant Use: Preface. Journal of Public Health Dentistry 1995;55 (5 Spec. Iss.) 261‐262. Accessed at: http://www.mchoralhealth.org/seal/PDFs/Step1_WorkshopGuidelinesSealantUse.pdf 6 Task Force on Community Preventive Services. Recommendations on Selected Interventions to Prevent Dental Caries, Oral and Pharyngeal Cancers, and Sports‐Related Craniofacial Injuries. Am J Prev Med 2002;23 (1S) 16‐20. 7 Jean Beauchamp, DDS; Page W. Caufield, DDS, PhD; James J. Crall, DDS, ScD; Kevin Donly, DDS, MS; Robert Feigal, DDS, PhD; Barbara Gooch, DMD, MPH; Amid Ismail, BDS, MPH, MBA, DrPH; William Kohn, DDS; Mark Siegal, DDS, MPH; Richard Simonsen, DDS, MS. Evidence‐based clinical recommendations for the use of pit‐and‐fissure sealantsA report of the American Dental Association Council on Scientific Affairs. JADA 2008;139 (3):257‐267. 8 Gooch BF, Griffin SO, Gray SK, et al. Preventing dental caries through school‐based sealant programs: Updated recommendations and reviews of evidence, Journal of the American Dental Association 2009 Nov;140(11);1356‐1365. 9 Carter NL, with the American Association for Community Dental Programs and the National Maternal and Child Oral Health Resource Center. 2011. Seal America: The Prevention Invention (2nd ed., rev.). Washington, DC: National Maternal and Child Oral Health Resource Center. 10 Bertness J, Holt K, eds. 2010. Dental Sealants: A Resource Guide (3rd ed.). Washington, DC: National Maternal and Child Oral Health Resource Center. 11 http://www.cdc.gov/oralHealth/state_programs/cooperative_agreements/index.htm) 12 http://www.hrsa.gov/about/pdf/mchb.PDF 13 http://www.mchb.hrsa.gov/programs/collaboration/ 14 http://www.mchb.hrsa.gov/programs/collaboration/ 15https://mchdata.hrsa.gov/tvisreports/MeasurementData/NationalMeasures/NationalMeasuresMenu.aspx 16 http://www.hrsa.gov/about/news/pressreleases/131030oralhealth.html 17 Office of the Inspector General Advisory Opinion OIG #13‐13 available at http://oig.hhs.gov/fraud/docs/advisoryopinions/2013/AdvOpn13‐13.pdf