dental management of a kidney transplant patient · decrease the incidence of acute allograft...
TRANSCRIPT
Continuing Education
Dental Management of aKidney Transplant Patient
Authored by Ronald S. Brown, DDS, MS; Crystal L. McIntosh, DDS, MS;Claudia C. Cotca, DDS, MPH; and Alison L. Glascoe, DDS, MS
Course Number: 151
Upon successful completion of this CE activity 2 CE credit hours may be awarded
A Peer-Reviewed CE Activity by
Opinions expressed by CE authors are their own and may not reflect those of Dentistry Today. Mention of
specific product names does not infer endorsement by Dentistry Today. Information contained in CE articles and
courses is not a substitute for sound clinical judgment and accepted standards of care. Participants are urged to
contact their state dental boards for continuing education requirements.
Dentistry Today, Inc, is an ADA CERP Recognized Provider. ADA CERP isa service of the American Dental Association to assist dental professionalsin indentifying quality providers of continuing dental education. ADA CERPdoes not approve or endorse individual courses or instructors, nor does itimply acceptance of credit hours by boards of dentistry. Concerns orcomplaints about a CE provider may be directed to the provider or to ADA CERP at ada.org/goto/cerp.
Approved PACE Program ProviderFAGD/MAGD Credit Approval doesnot imply acceptance by a state orprovincial board of dentistry orAGD endorsement. June 1, 2012 toMay 31, 2015 AGD PACE approvalnumber: 309062
LEARNING OBJECTIVESAfter participating in this CE activity, the individual will learn: • The reasons and the process regarding dentistsperforming a pretreatment dental/oral evaluation ofpatients scheduled for kidney transplant.
• The etiology and management issues related to drug-induced gingival overgrowth (DIGO).
ABOUT THE AUTHORSDr. Brown is an associate professor in thedepartments of Oral and Maxillofacial Path -ology and Oral Diagnosis and Radiology atHoward University College of Dentistry,and a clinical associate professor in theDepartment of Otolaryngology at
Georgetown University Med ical Center. He is past president ofthe American Academy of Oral Medicine. He can be reachedat [email protected].
Disclosure: Dr. Brown reports no disclosures.
Dr. McIntosh is an assistant professor in the department ofPeriodontics at Howard Uni versity College of Dentistry. Shecan be reached at [email protected].
Disclosure: Dr. McIntosh reports no disclosures.
Dr. Cotca is in private practice in Washington, DC. She can bereached at the e-mail ad dress [email protected].
Disclosure: Dr. Cotca reports no disclosures.
Dr. Glascoe is an assistant professor in the department ofPreventive Services at How ard University College ofDentistry in Wash ington, DC. She is a Diplomate of theAmerican Board of Periodontology, and practices
periodontics in private practice in Baltimore, Md. She canbe reached via e-mail at [email protected].
Disclosure: Dr. Glascoe reports no disclosures.
INTRODUCTIONDe Rossi and Glick1 reported in 1996 that the number ofAmericans living with end stage renal disease (ESRD) isincreasing. ESRD patients are typically placed on dialysistherapy. There have been steady yearly increases in thenumber of ESRD patients requiring dialysis. Therefore,more and more dentists will need to acquire the knowledgeand training in order to treat these patients. These pa tientstend to have advanced dental disease and a number ofcomorbid conditions such as hypertension and diabetes(which also happen to be the most common causes ofESRD).2 The function of the kidneys is to filter out andremove wastes and poisons from the circulatory system.The destruction of the nephrons results in the loss offiltering capacity, and such damage can happen quickly,although most kidney diseases tend to be slowlyprogressive. Slowly progressive kidney disease tends to besilent in that symptoms may not be evident until 80% or90% of the nephrons in both kidneys are destroyed.Previous to the utilization of dialysis therapy, ESRD tendedto result in death, as kidney function is essential. Dialysistherapy allows mechanical kidney functions to be performedin patients without viable kidney function. The dialysisprocedures are usually performed 3 times a week and eachsession takes several hours. Further more, the patient istethered to the dialysis equipment and is heparinized duringthe procedure.1-5
Fortunately, kidney organ transplant procedures haveproven relatively successful in allowing patients to reattainrenal function, discontinue renal dialysis, and attain a betterquality of life.3 However, transplant patients have anincreased risk of death compared to age-matched controlsand a prognosis similar to patients with a cancer diagnosis.Graft rejections occur secondary to allograft nephropathy,and such conditions as cardiac disease, malignancy, andinfection are often lethal in this patient population.Immunosuppressive drug regimens are designed to
Continuing Education
1
Dental Management of aKidney Transplant PatientEffective Date: 07/1/2012 Expiration Date: 07/1/2015
decrease the incidence of acute allograft rejection withaggressive induction therapy, and afterwards, maintenancerequires powerful but somewhat toxic drug regimens.Further more, maintenance therapies include ex pensiveprophylactic protocols against bacterial, fungal, and viralinfections. Despite emerging discoveries, the 20-yearsurvival rate of kidney transplant patients has not improvedvery much during the past 30 years.6,7
Before performing renal transplantation, it is important tocontrol ongoing infections. As dental infections are relativelycommon, and particularly so with regard to renal dialysispatients, a pretransplant dental evaluation is helpful inproviding information to the transplant team regarding oraland dental infections so that necessary dental therapies canbe accomplished previous to the transplantationprocedure.2,8,9 Thus, the importance of a prekidneytransplant dental evaluation is emphasized.
Drug-induced gingival overgrowth/en largement (DIGO)is a relatively common condition secondary mainly toanticonvulsant drugs such as phenytoin, calcium channelblocking agents (CCBA), antihypertensive drugs such asnifedipine and amlodipine, and the immunosuppressive drugcyc losporine. Other antiseizure inducing drugs includesodium valproate, valproic acid, phenobarbital, andprimidone, and other CCBA-inducing drugs includediltiazem, verapamil, and nitren dipine. DIGO was previouslyknown as drug-induced gingival hy perplasia al though thecondition is neither hyperplastic nor hypertrophic, but ratherdue to an in creased deposition of connective tissue(glycosaminoglycans/interstitial ground substance).Therefore, the descriptive terms of overgrowth orenlargement ra ther than hyperplasia are more accurate. Thehis to pathology of DIGO is noted for acanthosis andelongated rete pegs.10-12
This article reports a case in which an ESRD patientscheduled for a kidney transplant presented with DIGO, anddiscusses how dentists can evaluate and manage thesepatients.
CASE REPORTA 25-year-old male presented to an oral medicine clinicianreferred by a hospital-based kidney transplant team for apretransplant oral/dental evaluation. The chief complaint
was, “Work-up for a kidney transplant.” The medicaldiagnosis was kidney failure secondary to hypertension.Current treatment for hypertension consisted of nifedipineand clonidine. The patient was presently being treated withdialysis therapy 3 times a week and was scheduled for akidney transplant procedure with a donation from a relativewith matching human leukocyte antigens compatibility. Thepatient reported no known drug allergies. The family medicalhistory was not significant. The patient’s physicians hadprescribed amoxicillin for the patient’s dental infection. Thepatient reported pain of the left mandibular area which wasparticularly painful when eating and chewing. The patientreported that his gums bled when flossing. There was nolymph adenopathy noted on palpation.
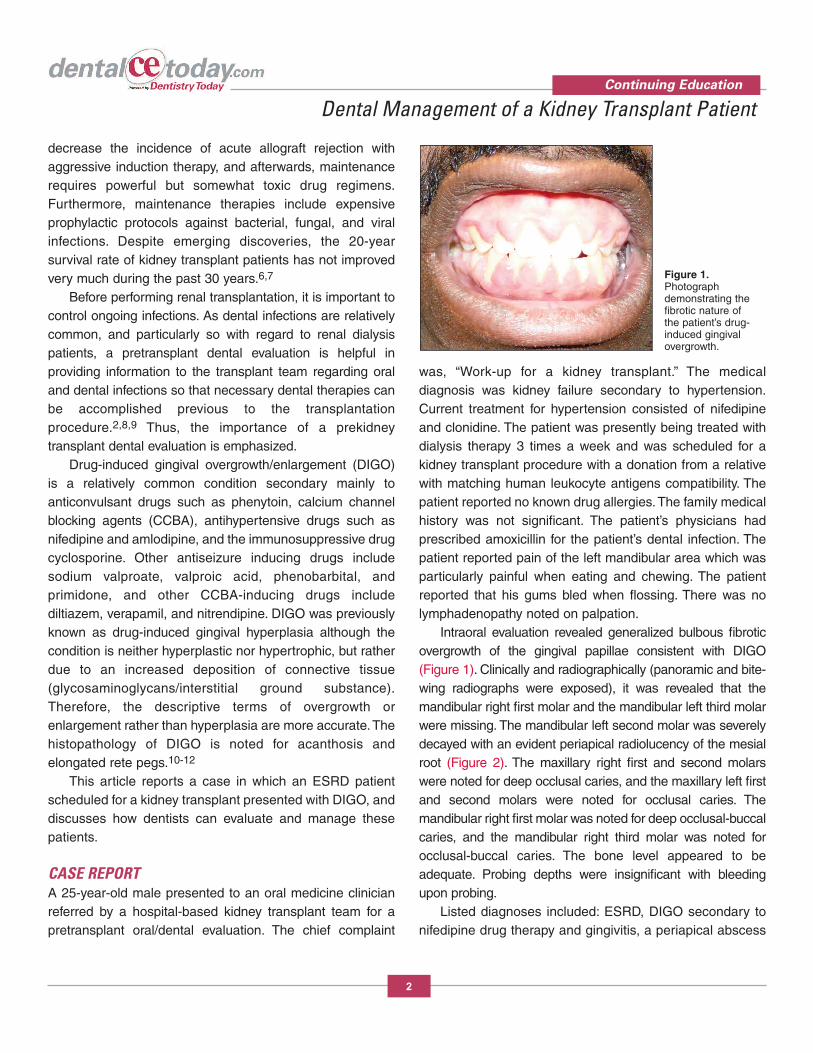
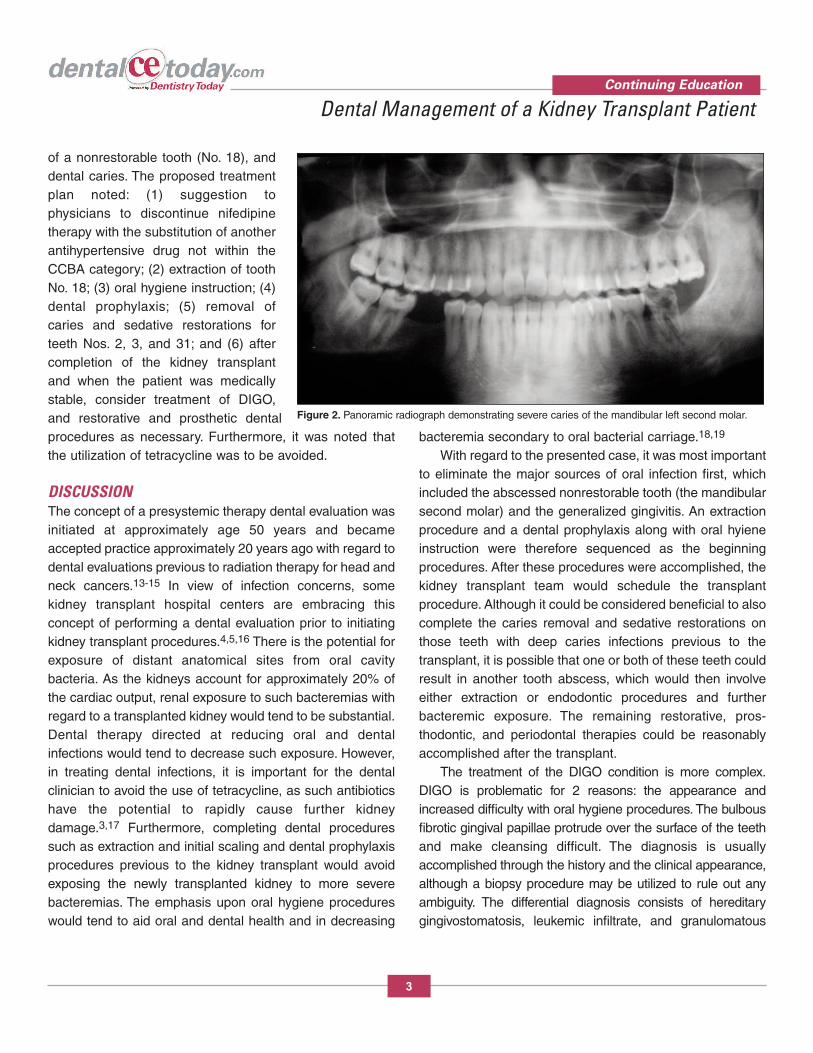
Intraoral evaluation revealed generalized bulbous fibroticovergrowth of the gingival papillae consistent with DIGO(Figure 1). Clinically and radiographically (panoramic and bite-wing radiographs were exposed), it was revealed that themandibular right first molar and the mandibular left third molarwere missing. The mandibular left second molar was severelydecayed with an evident periapical radiolucency of the mesialroot (Figure 2). The maxillary right first and second molarswere noted for deep occlusal caries, and the maxillary left firstand second molars were noted for occlusal caries. Themandibular right first molar was noted for deep occlusal-buccalcaries, and the man dibular right third molar was noted forocclusal-buccal caries. The bone level ap peared to beadequate. Probing depths were insignificant with bleedingupon probing.
Listed diagnoses included: ESRD, DIGO secondary tonifedipine drug therapy and gingivitis, a periapical abscess
Continuing Education
2
Dental Management of a Kidney Transplant Patient
Figure 1.Photographdemonstrating thefibrotic nature ofthe patient’s drug-induced gingival overgrowth.
of a nonrestorable tooth (No. 18), anddental caries. The proposed treatmentplan noted: (1) suggestion tophysicians to discontinue nifedipinetherapy with the substitution of anotherantihypertensive drug not within theCCBA category; (2) extraction of toothNo. 18; (3) oral hygiene instruction; (4)dental prophylaxis; (5) removal ofcaries and sedative restorations forteeth Nos. 2, 3, and 31; and (6) aftercompletion of the kidney transplantand when the patient was medicallystable, consider treatment of DIGO,and restorative and prosthetic dentalprocedures as necessary. Furthermore, it was noted thatthe utilization of tetracycline was to be avoided.
DISCUSSIONThe concept of a presystemic therapy dental evaluation wasinitiated at ap prox imately age 50 years and becameaccepted practice approximately 20 years ago with regard todental evaluations previous to radiation therapy for head andneck cancers.13-15 In view of infection concerns, somekidney transplant hospital centers are embracing thisconcept of performing a dental evaluation prior to initiatingkidney transplant procedures.4,5,16 There is the potential forexposure of distant anatomical sites from oral cavitybacteria. As the kidneys account for approximately 20% ofthe cardiac output, renal exposure to such bacteremias withregard to a transplanted kidney would tend to be substantial.Dental therapy directed at reducing oral and dentalinfections would tend to decrease such exposure. However,in treating dental infections, it is important for the dentalclinician to avoid the use of tetracycline, as such antibioticshave the potential to rapidly cause further kidneydamage.3,17 Furthermore, completing dental proceduressuch as extraction and initial scaling and dental prophylaxisprocedures previous to the kidney transplant would avoidexposing the newly transplanted kidney to more severebacteremias. The emphasis upon oral hygiene procedureswould tend to aid oral and dental health and in decreasing
bacteremia secondary to oral bacterial carriage.18,19
With regard to the presented case, it was most importantto eliminate the major sources of oral infection first, whichincluded the abscessed nonrestorable tooth (the mandibularsecond molar) and the generalized gingivitis. An extractionprocedure and a dental prophylaxis along with oral hy ieneinstruction were therefore sequenced as the beginningprocedures. After these procedures were accomplished, thekidney transplant team would schedule the transplantprocedure. Although it could be considered beneficial to alsocomplete the caries re moval and sedative restorations onthose teeth with deep caries infections previous to thetransplant, it is possible that one or both of these teeth couldresult in another tooth abscess, which would then involveeither extraction or endodontic procedures and furtherbacteremic exposure. The remaining restorative, pros -thodontic, and perio dontal therapies could be reasonablyac complished after the transplant.
The treatment of the DIGO condition is more complex.DIGO is problematic for 2 reasons: the appearance andincreased difficulty with oral hygiene procedures. The bulbousfibrotic gingival papillae protrude over the surface of the teethand make cleansing difficult. The diagnosis is usuallyaccomplished through the history and the clinical appearance,al though a biopsy procedure may be utilized to rule out anyambiguity. The differential diagnosis consists of hereditarygingivo stomatosis, leukemic infiltrate, and granulomatous
Continuing Education
3
Dental Management of a Kidney Transplant Patient
Figure 2. Panoramic radiograph demonstrating severe caries of the mandibular left second molar.

conditions such as tuberculosis, sarcoidosis, Crohn’s disease,and orofacial granulomatosis. However, DIGO is much morecommonplace compared to other conditions noted within thedifferential diagnosis. Fur thermore, the medical histories andclinical presentations would tend to rule out a definitivenecessity for biopsy in most in stances.10 Current therapies forDIGO include discontinuation and decreasing the dosage ofthe inducing drug, attention to oral hygiene includingantiplaque rinses, surgical treatment (both scalpel and laser),topical folate therapy, and azithromycin therapy.20-22
Partially based upon a successful folate efficacy studyreported by Drew et al,23 Brown et al11 presented amultifactorial hypothetical mechanism model in 1992. Thishypothesis is based upon several issues: (1) bacterial plaquetends to cause inflammation of the gingiva which initiates anincrease in connective tissue growth, (2) DIGO is due toincreased connective tissue buildup and not due tohyperplasia, (3) all of the inducing drugs affect cationfunction, (4) folate transport is de pendent upon both energydependent ion channel transport and passive diffusionpathways, (5) collagenase activation is a multistep processaffected by matrix metalloproteins (MMPs), and (6) DIGOappears to be secondary to the failure of catabolism to breakdown the buildup of increased connective tissue within thegingiva. The following cascade of events was hypothesized:the inducing drug decreases gingival cellular uptake of folicacid (folic acid is necessary for the addition of carbonmolecules necessary for the conversion of purines topyrimidines base-pairs), the synthesis of a particular MMP(MMP 1, 2, 8, 9, or 13) is decreased, which results in theinability to activate sufficient collagenase, resulting indecreased efficiency in catabolism, resulting in overgrowth.
Seymour et al24 also favored a similar multifactorialhypothetic model which included many of the same concerns(although excluding folic acid concerns) but tended to focusmore upon genetic issues. Gómez et al,25 Tokgöz et al,26 Nashand Zaltzman,27 and Ramalho et al28 all reported the efficacyof azith romycin therapy in the treatment of DIGO. Kim et al21
proposed that azathioprine improves DIGO symptoms byinterfering with collagen accumulation by activating MMP 2.
With the above in mind, the treatment of a patient withDIGO undergoing a kidney transplant is a complicatedmatter. As the patient in this case presented with DIGO
secondary to nifedipine, it would seem reasonable that this patient would have a pre dilection toward DIGOsecondary to cyclosporin. Possibly, kidney transplanta-tion with tacrolimus immunosuppression is another possible consideration. Tacrolimus is a relatively newimmunosuppresive drug, which although implicated as aDIGO inducing drug, may be less of a problem compared tocyclosporin.29,30 How ever, it would be reasonable to treatthe patient’s DIGO condition sometime after the transplant,and then determine the treatment strategy. Availabletreatment strategies consist of topical folate therapy,systemic azithromycin therapy, chlorhexidine therapy, andperiodontal surgery either with laser or scapel.20,21 Kara etal31 compared oral improvement of gingival overgrowth in60 adolescent subjects. The subjects received oral hygieneinstructions, scaling, surgical therapy, and periodontalmaintenance therapy. Although they noted statisticallysignificant improvement with regard to all therapies,treatment of DIGO surgical (scalpel) therapy was the mostsuccessful and was the treatment of choice. Mavrogianniset al32 reported that DIGO is a common clinical problemthat usually requires surgical intervention. They agree thatnonsurgical therapies are helpful and may reduce the rateof recurrence, and should be the first-line therapies.However, they reported that surgical therapy is usually themost reliable option and scalpel gingivectomy remains thetreatment of choice.
However, laser-assisted surgical treatment is preferred bymany be cause of improved hemostasis during surgery,optimal final gingival tissue positioning and tissuearchitecture, and a possible sterilization effect of laser ongranulomatous tissue and bacterial colonization within perio -dontal pockets and gingival sulci. Various soft-tissue laserssuch as diodes and Nd:YAG may be accommodated forfibrotic tissue noted for some DIGO cases, and generally,choices of wavelength can be adjusted depen dent uponindividual tissue characteristics. Mavrogiannis et al33
reported that after 6 months’ follow-up, there was significantlyless recurrence of DIGO. They33 concluded that al thoughDIGO can be managed by a variety of techniques, laserexcision resulted in a reduced rate of recurrence.
According the 2002 American Acad emy of PeriodontologyAcademy Re port, laser therapy is considered su perior to
Continuing Education
4
Dental Management of a Kidney Transplant Patient

scalpel use in conventional soft-tissue removal for severalreasons. Laser therapy has less bleeding, less discomfort(possibly due to cauterizing soft tissue, forming a proteincoagulum that acts as a dressing, and closing off the sensorynerve endings), and may req uire less local anesthesia, lesshealing time, and less scar tissue.34 How ever, Cobb35
concluded that scal pel surgery requires less time and ef fortwhen compared to laser surgery. Furthermore, the tissues inconventional surgery are not subjected to irradiation.
The consensus regarding the 2 surgical therapies is thatwhen there is an excess of gingival enlargement, it maybe more advantageous to remove the bulk of gingivalexcess with a scalpel. Scalpel therapy allows greater tactilesensitivity necessary to correct the gingival discrepancyand reduces the operating time significantly. Be cause of thedifficulty in recontouring fibrotic tissues, the laser takessignificantly more time. However, the laser has theadvantage of greater recontouring control. Therefore, thescalpel is advocated for the initial tissue re duction and thelaser has an advantage in obtaining tissue hemostasis,decreased patient discomfort, and fi nal tissuerecontouring.20,34,35
CONCLUSIONPatients scheduled for a kidney transplant may benefit froma pretherapy dental evaluation. The side effect of DIGOpresents challenges with regard to various dentaltherapeutic strategies in patients scheduled for kidneytransplantation.
REFERENCES1. De Rossi SS, Glick M. Dental considerations for the
patient with renal disease receiving hemodialysis. J Am Dent Assoc. 1996;127:211-219.
2. Klassen JT, Krasko BM. The dental health status ofdialysis patients. J Can Dent Assoc. 2002;68:34-38.
3. Brockmann W, Badr M. Chronic kidney disease:pharmacological considerations for the dentist. J Am Dent Assoc. 2010;141:1330-1339.
4. Saif I, Adkins A, Kewley V, et al. Routine andemergency management guidelines for the dentalpatient with renal disease and kidney transplant. Part 1. Dent Update. 2011;38:179-182, 185-186.
5. Saif I, Adkins A, Kewley V, et al. Routine andemergency management guidelines for the dentalpatient with renal disease and kidney transplant. Part2. Dent Update. 2011;38:245-248, 250-251.
6. Chapman JR. Clinical renal transplantation: where arewe now, what are our key challenges? TransplantProc. 2010;42(9 suppl):S3-S6.
7. Veroux M, Corona D, Veroux P. Kidney transplantation:future challenges. Minerva Chir. 2009;64:75-100.
8. Schander K, Jontell M, Johansson P, et al. Oralinfections and their influence on medical rehabilitationin kidney transplant patients. Swed Dent J.2009;33:97-103.
9. Nishide N, Nishikawa T, Kanamura N. Extensivebleeding during surgical treatment for gingivalovergrowth in a patient on haemodialysis—a casereport and review of the literature. Aust Dent J.2005;50:276-281.
10. Pette GA, Siegel MA, Parker WB. Gingivalenlargement. J Am Dent Assoc. 2011;142:1265-1268.
11. Brown RS, Beaver WT, Bottomley WK. On themechanism of drug-induced gingival hyperplasia. J Oral Pathol Med. 1991;20:201-209.
12. Brown RS, Sein P, Corio R, et al. Nitrendipine-inducedgingival hyperplasia. First case report. Oral Surg OralMed Oral Pathol. 1990;70:593-596.
13. Brown RS, Miller JH Jr, Bottomley WK. A retrospectiveoral/dental evaluation of 92 head and neck oncologypatients, before, during and after irradiation therapy.Gerodontology. 1990;9:35-39.
14. Dreizen S, Brown LR, Daly TE, et al. Prevention ofxerostomia-related dental caries in irradiated cancerpatients. J Dent Res. 1977;56:99-104.
15. Silverman S Jr, Chierici G. Radiation therapy of oralcarcinoma. I. Effects on oral tissues and managementof the periodontium. J Periodontol. 1965;36:478-484.
16. Wilczy�ska-Borawska M, Bagi�ska J, Malyszko J.Dental problems in a potential kidney transplantrecipient: case report and literature review. Ann Acad Med Stetin. 2010;56:51-54.
17. Miller CS, McGarity GJ. Tetracycline-induced renalfailure after dental treatment. J Am Dent Assoc.2009;140:56-60.
18. Lockhart PB, Brennan MT, Sasser HC, et al.Bacteremia associated with toothbrushing and dentalextraction. Circulation. 2008;117:3118-3125.
Continuing Education
5
Dental Management of a Kidney Transplant Patient
19. Lockhart PB, Brennan MT, Thornhill M, et al. Poor oralhygiene as a risk factor for infective endocarditis-relatedbacteremia. J Am Dent Assoc. 2009;140:1238-1244.
20. Rossmann JA, Ingles E, Brown RS. Multimodal treatmentof drug-induced gingival hyperplasia in a kidney transplantpatient. Compendium. 1994;15:1266-1274.
21. Kim JY, Park SH, Cho KS, et al. Mechanism ofazithromycin treatment on gingival overgrowth. J DentRes. 2008;87:1075-1079.
22. Clementini M, Vittorini G, Crea A, et al. Efficacy ofAZM therapy in patients with gingival overgrowthinduced by cyclosporine A: a systematic review. BMCOral Health. 2008;8:34.
23. Drew HJ, Vogel RI, Molofsky W, et al. Effect of folateon phenytoin hyperplasia. J Clin Perio dontol.1987;14:350-356.
24. Seymour RA, Thomason JM, Ellis JS. Thepathogenesis of drug-induced gingival overgrowth. JClin Periodontol. 1996;23(3 pt 1):165-175.
25. Gómez E, Sánchez-Nuñez M, Sánchez JE, et al.Treatment of cyclosporin-induced gingival hyperplasiawith azithromycin. Nephrol Dial Transplant.1997;12:2694-2697.
26. Tokgöz B, Sari HI, Yildiz O, et al. Effects ofazithromycin on cyclosporine-induced gingivalhyperplasia in renal transplant patients. TransplantProc. 2004;36:2699-2702.
27. Nash MM, Zaltzman JS. Efficacy of azithromycin inthe treatment of cyclosporine-induced gingivalhyperplasia in renal transplant recipients.Transplantation. 1998;65:1611-1615.
28. Ramalho VL, Ramalho HJ, Cipullo JP, et al.Comparison of azithromycin and oral hygiene programin the treatment of cyclosporine-induced gingivalhyperplasia. Ren Fail. 2007;29:265-270.
29. Paixão CG, Sekiguchi RT, Saraiva L, et al. Gingivalovergrowth among patients medicated withcyclosporin A and tacrolimus undergoing renaltransplantation: a prospective study. J Periodontol.2011;82:251-258.
30. Cota LO, Aquino DR, Franco GC, et al. Gingivalovergrowth in subjects under immunosuppressiveregimens based on cyclosporine, tacrolimus, orsirolimus. J Clin Periodontol. 2010;37:894-902.
31. Kara C, Demir T, Tezel A. Effectiveness of periodontaltherapies on the treatment of different aetiologicalfactors induced gingival overgrowth in puberty. Int J Dent Hyg. 2007;5:211-217.
32. Mavrogiannis M, Ellis JS, Thomason JM, et al. Themanagement of drug-induced gingival overgrowth. J Clin Periodontol. 2006;33:434-439.
33. Mavrogiannis M, Ellis JS, Seymour RA, et al. Theefficacy of three different surgical techniques in themanagement of drug-induced gingival overgrowth. J Clin Periodontol. 2006;33:677-682.
34. Research, Science and Therapy Committee of theAmerican Academy of Periodontology. Lasers inperiodontics. J Periodontol. 2002;73:1231-1239.
35. Cobb CM. Lasers in periodontics: a review of theliterature. J Periodontol. 2006;77:545-564.
Continuing Education
6
Dental Management of a Kidney Transplant Patient
POST EXAMINATION INFORMATION
To receive continuing education credit for participation inthis educational activity you must complete the programpost examination and receive a score of 70% or better.
Traditional Completion Option:You may fax or mail your answers with payment to DentistryToday (see Traditional Completion Information on followingpage). All information requested must be provided in orderto process the program for credit. Be sure to complete your“Payment,” “Personal Certification Information,” “Answers,”and “Evaluation” forms. Your exam will be graded within 72hours of receipt. Upon successful completion of the post-exam (70% or higher), a letter of completion will be mailedto the address provided.
Online Completion Option:Use this page to review the questions and mark youranswers. Return to dentalcetoday.com and sign in. If youhave not previously purchased the program, select it fromthe “Online Courses” listing and complete the onlinepurchase process. Once purchased the program will beadded to your User History page where a Take Exam linkwill be provided directly across from the program title.Select the Take Exam link, complete all the programquestions and Submit your answers. An immediate gradereport will be provided. Upon receiving a passing grade,complete the online evaluation form. Upon submitting the form, your Letter Of Completion will be providedimmediately for printing.
General Program Information:Online users may log in to dentalcetoday.com any time inthe future to access previously purchased programs andview or print letters of completion and results.
POST EXAMINATION QUESTIONS
1. Which of the following drugs should be avoided forpatients with end stage renal disease (ESRD)?
a. Penicillin.
b. Erythromycin.
c. Tetracycline.
d. Metronidiazole.
2. The main function of the kidneys is ____________.
a. To monitor water and salt balance.
b. To filter out and remove wastes and poisons fromthe circulatory system.
c. To provide red blood cells for distribution of oxygen.
d. To buffer the circulatory pH.
3. Slowly progressive kidney disease tends to besilent and symptoms do not tend to occur until_____________ of the nephrons in both kidneysare destroyed.
a. 20% to 30%.
b. 40% to 50%.
c. 50% to 60%.
d. 80% to 90%.
4. In describing the prognosis of kidney transplantpatients, which of the below statements is themost accurate?
a. Kidney transplant patients have similar life spanscompared to other patients.
b. Maintenance therapies such a prophylaxis areentirely unnecessary for kidney transplant patients.
c. Graft rejection is unheard of with regard to kidneytransplantation.
d. Despite emerging discoveries, the 20-year survivalrate of kidney transplant patients has not improvedmuch during the past 30 years.
5. Which of the drug categories below is NOTsubstantially involved with DIGO?
a. Calcium channel blocking agents.
b. Antibiotics.
c. Cylclosporin (and other calcineurin inhibitors).
d. Phenytoin (and other anticonvulsants).
6. DIGO is due to _________.
a. Increased accumulation of connective tissue.
b. Hypertrophy.
c. Hyperplasia.
d. Edema.
Continuing Education
7
Dental Management of a Kidney Transplant Patient
7. Studies have confirmed that such drug therapy/therapies as _________ have been helpful in thetreatment of DIGO.
a. Folic acid therapy only.
b. Tetracycline therapy only.
c. Azithromycin therapy only.
d. Both folic acid and azithromycin therapies.
8. The histopathologic appearance of drug-inducedgingival enlargement is noted for ______.
a. Lymphocytic infiltration.
b. Fibrosis.
c. Acanthosis and elongated rete pegs.
d. Necrosis.
9. Renal transplant medical centers are beginning to utilize ________.
a. Pretreatment/surgical dental evaluations.
b. Post-treatment/surgical dental evaluations.
c. Full-mouth dental extractions.
d. Antibiotic prophylaxis protocols for ESRD patients.
10. Pretreatment dental evaluation was first utilizedregarding _________ patients.
a. Chronic obstructive pulmonary disease.
b. Head and neck radiology oncology.
c. Crohn’s disease.
d. Sjögren’s syndrome.
11.Which of the following is NOT a first-line dentaltherapy for patients scheduled for a kidneytransplant surgical procedure?
a. Periodontal services.
b. Homecare instruction.
c. Prosthodontic therapy.
d. Emergency dental therapy.
12. The main issue(s) with regard to gingivalovergrowth is/are _________.
a. Pain.
b. Appearance and difficulty of oral hygiene.
c. Increased incidence of periodontal disease.
d. Increased caries incidence.
13. The diagnosis of DIGO/enlargement is usuallyattained through __________.
a. Histopathology.
b. DNA evaluation.
c. History and clinical appearance.
d. Plaque analysis.
14. The differential diagnosis of DIGO does NOTinclude which of the below?
a. Hereditary gingival fibromatosis.
b. Orofacial granulomatosis.
c. Leukemic infiltrate.
d. Ludwig’s angina.
15.With regard to collagenase activation, whichchemical or drug appears to be involved?
a. Folic acid.
b. Azithromycin.
c. Purines.
d. Matrix metalloproteins.
16.With regard to immunosuppression drugs forkidney transplantation, which immunosuppressantmay be substituted for cyclosporine in the future?
a. Tacrolimus.
b. Azithromycin.
c. Azathioprine.
d. Amphotericin B.
Continuing Education
8
Dental Management of a Kidney Transplant Patient
PROGRAM COMPLETION INFORMATION
If you wish to purchase and complete this activitytraditionally (mail or fax) rather than online, you mustprovide the information requested below. Please be sure toselect your answers carefully and complete the evaluationinformation. To receive credit you must answer at least 12 ofthe 16 questions correctly.
Complete online at: dentalcetoday.com
TRADITIONAL COMPLETION INFORMATION:Mail or fax this completed form with payment to:
Dentistry TodayDepartment of Continuing Education100 Passaic AvenueFairfield, NJ 07004
Fax: 973-882-3622
PAYMENT & CREDIT INFORMATION:
Examination Fee: $40.00 Credit Hours: 2.0
Note: There is a $10 surcharge to process a check drawn on any bank other than a US bank. Should you have additionalquestions, please contact us at (973) 882-4700.
� I have enclosed a check or money order.
� I am using a credit card.
My Credit Card information is provided below.
� American Express � Visa � MC � Discover
Please provide the following (please print clearly):
Exact Name on Credit Card
Credit Card # Expiration Date
Signature
PROGRAM EVAUATION FORMPlease complete the following activity evaluation questions.
Rating Scale: Excellent = 5 and Poor = 0
Course objectives were achieved. Content was useful and benefited your clinical practice. Review questions were clear and relevant to the editorial. Illustrations and photographs were clear and relevant.Written presentation was informative and concise.How much time did you spend reading the activity and completing the test?
Continuing Education
Dental Management of a Kidney Transplant Patient
ANSWER FORM: COURSE #: 151Please check the correct box for each question below.
1. � a � b � c � d 9. � a � b � c � d
2. � a � b � c � d 10. � a � b � c � d
3. � a � b � c � d 11. � a � b � c � d
4. � a � b � c � d 12. � a � b � c � d
5. � a � b � c � d 13. � a � b � c � d
6. � a � b � c � d 14. � a � b � c � d
7. � a � b � c � d 15. � a � b � c � d
8. � a � b � c � d 16. � a � b � c � d
PERSONAL CERTIFICATION INFORMATION:
Last Name (PLEASE PRINT CLEARLY OR TYPE)
First Name
Profession / Credentials License Number
Street Address
Suite or Apartment Number
City State Zip Code
Daytime Telephone Number With Area Code
Fax Number With Area Code
E-mail Address
/
Dentistry Today, Inc, is an ADA CERP RecognizedProvider. ADA CERP is a service of the AmericanDental Association to assist dental professionals inindentifying quality providers of continuing dentaleducation. ADA CERP does not approve or endorseindividual courses or instructors, nor does it implyacceptance of credit hours by boards of dentistry.Concerns or complaints about a CE provider may bedirected to the provider or to ADA CERP atada.org/goto/cerp.
Approved PACE Program ProviderFAGD/MAGD Credit Approval doesnot imply acceptance by a state orprovincial board of dentistry or AGDendorsement. June 1, 2012 to May 31, 2015 AGD PACE approvalnumber: 309062
9