defining asthma: clinical criteria - columbia university€¦ · defining asthma: clinical criteria...
TRANSCRIPT

1
Defining Asthma: Clinical Criteria
Asthma11%
n = 807
Recent wheeze20%
Atopy 34%
AHR 19%
From: Woolcock, AJ. “Asthma” in Textbook of Respiratory Medicine, 2nd ed.Murray, Nadel, eds.(Saunders:Philadelphia) pp. 1288-1330, 1994
Defining Asthma:Bronchial Hyperresponsiveness

2
Impaired Ventilation in Asthma
Normal Asthmatic
From: Klarreich, Nature 424:873, 2003
Dynamic Imaging of Asthma
Pre-treatment Post-treatment

3
Mucus Plugging is a Prominent Feature of Moderate to Severe Asthma
From: Bousquet et al., Am. J. Respir. Crit. Care Med., 161:1720, 2000
Some Landmarks in the History of the Immunology of Asthma*
*Highly biased view; therefore, commit to memory
1989: Early genetic mapping assigns chromosome 5q to the“cytokine gene cluster.”
Early 1990s: Asthma is an inflammatory disease.1990: Upregulation of ICAM-1 and LFA-1, adhesion
molecules, in a primate model of asthma1992: TH2 bias of lymphocytes in asthma1997: Experimental support grows for the “Hygiene hypothesis,”
first proposed in 1989.2000: Role of Tregs in regulation of asthma

4
Nature of Inflammatory Cells inBiopsies From Airways of Asthmatics
From: Ollerenshaw and Woolcock., Am. Rev. Resp. Dis. 145:922, 1992
Defining Asthma: Pathological Features
Normal AsthmaticSmooth muscle
hypertrophy
Epithelialsloughing
Goblet cellhyperplasia
Subepithelialfibrosis
From: Bousquet et al., Am. J. Respir. Crit. Care Med., 161:1720, 2000
Inflammation

5
Pro-survival and Metaplatic Pathwaysto Goblet Cell Production
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
From: Cohn, Am. J. Clin. Invest, 116:306, 2006
Tissue “Compartments” in Asthma
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

6
Adhesion Molecules ICAM-1 and LFA-1 in Experimental Asthma
ICAM-1 LFA-1 Control
From: Wegner et al., Science 247:456, 1990
Asthma and the Immune Response

7
Early- and Late-phase Allergic Reactions
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Presence of Degranulated Eosinophils in Asthmatic Airways
From: Bousquet et al., N. Engl. J. Med. 323:1033, 1990

8
Eosinophils and Asthma
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
From: Wills-Karp and Karp, Science 305:1726-1729, 2004
Asthma as a TH2-dominated Disease

9
First Recognition of a TH2 Bias in Lymphocytes Obtained by BAL in Asthmatics
From: Robinson et al., New Engl. J. Med. 326:298,1992
Emergence of TH1 and TH2 Cellsfrom Naïve Precursors
From: Elias et al., J. Clin. Invest. 111:291, 2003

10
STAT-6 Signaling PathwaysLeading to the Asthmatic Phenotype
From: Elias et al., J. Clin. Invest. 111:291, 2003
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
From: Wark and Gibson, Thorax 61:909, 2006
Defective Innate Immunity toRhinovirus Infection in Asthmatics

11
Potential Drug Targets in Asthma
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
From: Barnes, Nature Reviews Drug Discovery 3:831,2004
Understanding the Immunology of AsthmaLeads to Insights Into Novel Therapeutics
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
From: Barnes, Nature Reviews Drug Discovery 3:831,2004
12
Who Gets Asthma?
13
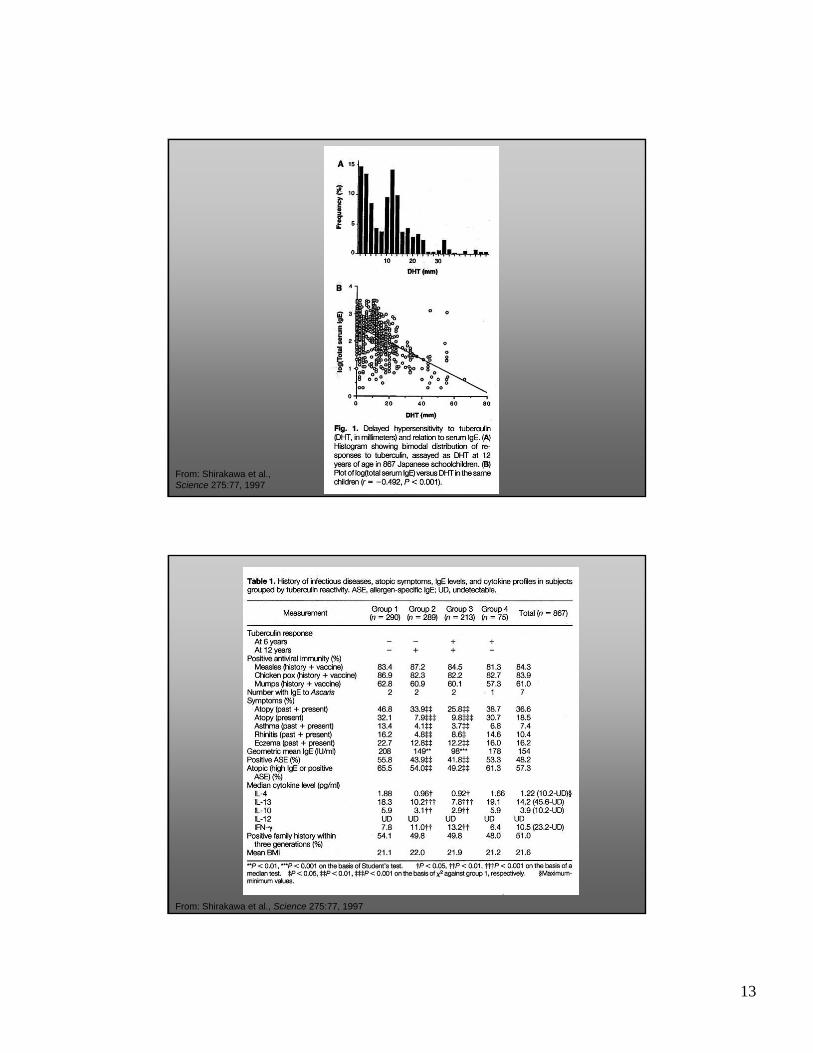
From: Shirakawa et al.,Science 275:77, 1997
From: Shirakawa et al., Science 275:77, 1997

14
From: Shirakawa et al., Science 275:77, 1997
Environmental Influences and Asthma:The Hygiene Hypothesis

15
Paradox: Why Does Chronic Infection with Helminths
Not Predispose to Allergy?
From: Yazdanbakhsh et al., Science 296:490, 2002

16
An Alternative to the Hygiene Hypothesis: Regulatory T-cells
The Role of Regulatory T-cellsin Modifying TH2 Immunity
Modified from: Maizels & Yazdanbakhsh,Nature Rev. Immunol. 3:733, 2003

17
Immunotherapy of Atopic Diseases: a Role for Tregs?
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Following 2-year grass pollen immunotherapy (closed circles), there were significant increases in (A) allergen-stimulated PBMC production of IL-10; (B) serum concentrations of grass pollen allergen-specific IgG4; and (C) serum inhibitory activity for allergen-IgE binding to B cells compared with controls (open circles). These changes were accompanied by a reduction in symptoms and inhibition allergen-induced late cutaneous response.
From: Robinson et al., J. Clin. Invest 114:1389, 2004
Regulatory T-cells (Tregs) in Asthma
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
From: Robinson et al., J. Clin. Invest 114:1389, 2004

18
Chemokines: the Gatekeepers ofInflammation
Chemokines Direct Traffic
From: Luster, Curr. Opin. Immunol. 14:129, 2002

19
Chemokine Receptor Specificityin Th2 Cells and Eosinophils
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Potential Drug Targets in Asthma:Chemokines and their Receptors
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
From: Barnes, Nature Reviews Drug Discovery 3:831,2004

20
Inflammatory Mediators asNovel Drug Targets
Lipid Mediators in Asthma:LTB4, PGD2, LTC4
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
From: Luster and Tager Nature Reviews Immunol. 4:711, 2004
LTC4S
PGD2LTB4
LTC4, LTD4
21
Biological Activities of LTB4 and PGD2
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
From: Tilley and Boucher J. Clin. Invest. 115:13-16 (2005)
Adenosine Receptors as Drug Targets in Asthma

22
Pro- and Anti-inflammatoryActivities of Adenosine in Asthma
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
From: Tilley and BoucherJ. Clin. Invest. 115:13-16 (2005)
Pharmacogenetics:The Future of Asthma Therapeutics?

23
Summary of Genes Associated With Atopy
From: Halapi and Hakonarson,Curr. Opin. Pulm. Med. 10:22, 2003
Summary
1. Asthma is a chronic disease of the airways characterized by reversible airway obstruction, bronchial hyperreactivity, chronic inflammation, and mucus hypersecretion.
2. The allergic response is characterized by an early phase, dominated by degranulation of mast cells, followed by a late phase, involving T cells and eosinophils.
3. Asthma is accompanied by up-regulation of leukocyte adhesion molecules and the presence of multiple pro-inflammatory mediators, including chemokines, prostaglandins, leukotrienes, adenosine, and toxic products released from eosinophil granules.
4. Asthma is a prototypical Th2 disease, with increased production if IL-4 and IL-13, and STAT6 activation. The immunobiology of asthma is highly complex, but includes defects in the anti-viral response in airway epithelia.
5. The hygiene hypothesis states that asthma may arise from an imbalance in the Th1 and Th2 lymphocyte populations, possibly from differences in exposure to Th1-polarizing stimuli early in life.
6. An alternative view is that asthma arises from a defect in immune regulation. Insufficient production of Tregs may predispose to airway sensitization and atopy.
7. Future insights into the cellular immunology and genetics underlying asthma offer hope for future therapeutics.