decision making in geriatric oncology · between overtreatment and undertreatment and must be...
TRANSCRIPT

Decision m
aking in geriatric oncology
M
arije Emilie H
amaker
Decision making in geriatric oncology
Marije Emilie Hamaker

Decision making in geriatric oncology

Decision making in geriatric oncology
PhD thesis, University of Amsterdam, The Netherlands
© M.E. Hamaker, Amsterdam, The Netherlands 2012
All rights reserved. No part of this thesis may be reproduced or transmitted in any form or
by any means without prior permission of the author. A digital version of this thesis can be
found at www.dare.uva.nl
Lay‐out: J.W. Broek
Printed by: Buijten & Schipperheijn
ISBN 978‐90‐9027018‐0
The printing of this thesis is financially supported by: Stichting Oncocare Alkmaar, Servier Nederland Farma B.V., Amgen B.V., Vifor Pharma Nederland B.V., Janssen‐Cilag B.V., Celgene B.V., Nutricia Advanced Medical Nutrition and Diakonessenhuis.

Decision making in geriatric oncology
ACADEMISCH PROEFSCHRIFT
ter verkrijging van de graad van doctor
aan de Universiteit van Amsterdam
op gezag van de Rector Magnificus
Prof. dr. D.C. van den Boom
ten overstaan van een door het college voor promoties ingestelde
commissie, in het openbaar te verdedigen in de Agnietenkapel
op vrijdag 30 november 2012, te 14.00 uur
door Marije Emilie Hamaker
geboren te Assen

Promotiecommissie Promotor: Prof. dr. M.M. Levi
Prof. dr. S.E.J.A. de Rooij Co‐promotores: Dr. B.C. van Munster
Dr. C.H. Smorenburg Overige leden: Prof. dr. A.H. Zwinderman
Prof. dr. C. Koning
Prof. dr. D.J. Richel
Prof. dr. J.W.R. Nortier
Prof. dr. M.G.M. Olde‐Rikkert
Dr. H.A.A.M. Maas
Faculteit der Geneeskunde

Table of contents
Introduction 7
Part I. Breast cancer treatment in the elderly
Chapter 1 Breast cancer in the elderly: a retrospective study on diagnosis and
treatment according to national guidelines 13
Chapter 2 Trends in breast cancer treatment in the elderly at a breast cancer out‐
patient clinic (translated from Dutch) 29
Chapter 3 Omission of surgery in elderly patient with early stage breast cancer 39
Chapter 4 Non‐referral of nursing home patients with suspected breast cancer 53
Chapter 5
Slow accrual of elderly patients with metastatic breast cancer in the
OMEGA study of the Dutch Breast cancer Trialists’ Group (BOOG) 65
Part II. Treatment of elderly patients with other cancer types
Chapter 6 Colon cancer in the elderly: does age still matter? 79
Chapter 7 Diagnostic choices and clinical outcome in octogenarians with iron‐
deficiency anaemia 93
Chapter 8 Age‐related differences in guideline adherence for head and neck
cancer 107
Part III. Decision making in geriatric oncology
Chapter 9 The value of a comprehensive geriatric assessment in patient care and
prognostication for elderly cancer patients acutely admitted to hospital 125
Chapter 10 Baseline comprehensive geriatric assessments predicts toxicity and
survival in elderly patients with metastatic breast cancer receiving
palliative chemotherapy
141
Chapter 11 The value of geriatric assessments in predicting treatment tolerance
and prognosis in older cancer patients – a systematic review 157
Chapter 12 Frailty screening tools for predicting outcome of a comprehensive
geriatric assessment in older cancer patients – a systematic review 183
Part IV. General discussion, summary and acknowledgements
Chapter 13 General discussion 205
Chapter 14 Summary / Samenvatting 213
Author Affiliations 227
Curriculum Vitae 231
Acknowledgements (Dankwoord) 235


Introduction

Introduction
Demographic changes In Western societies, the population is ageing. In the Netherlands, the proportion of
inhabitants aged 75 years and older has increased from 5% in 1990 to 7% in 2012, and will
continue to increase rapidly to 14% by 2030 before plateauing at around 15% by 2040.1
These changes are caused by two separate demographic developments. First, the post‐
war baby boom generation ‐ clearly visible as a wave passing through the demographic
pyramid (Figure 1) ‐ is soon reaching their seventies. Second, due to medical advances and
increased prosperity, the elderly are becoming older. In the course of the past 50 years,
life‐expectancy has risen by 10 years for women and by 8.5 years for men.1 Another 5
years will be added in the coming thirty years, meaning that by 2040, the average life‐
expectancy will be 87.4 years for women and 84.5 years for men.1
Ageing is very much an individual process, in the course of which differences in genetic
predisposition and life‐style will become apparent, intercurrent and chronic diseases will
leave their mark and the speed with which physiologic reserves decline will vary from
person to person. Essentially, in the course of a life‐time an individual will become more
and more unique and as a result, the elderly form a highly heterogeneous population.
Figure 1: Age structure of the Dutch population in 2012, 2025 and 2040
age age age
-----------------------------------------------------------------------------------------
2012 2025 2040
men x 1000 women x 1000 men x 1000 women x 1000 men x 1000 women x 1000
Source: Statistics Netherlands (cbs.nl)
8

Introduction
Ageing and cancer As the population ages, many diseases that predominantly affect the elderly will become
more prevalent. This also holds true for cancer: in the past 20 years, the number of newly
diagnosed cancer patients rose by 67% in the Netherlands, from 57,000 to over 95,000.2
Although malignant disease can occur at all ages, it disproportionally strikes those aged 75
years and older. While only 7% of Dutch inhabitants currently falls into this age group,
30% of malignancies occur in individuals aged 75 years and older as well as 46% of cancer‐
related deaths,2 and these percentages are expected to rise even further over the coming
decades. Optimal cancer care for the older patient ideally strikes the golden mean
between overtreatment and undertreatment and must be tailored to the individual
patient as well as the customary disease‐related factors incorporated in treatment
guidelines. Cancer specialists are now collaborating with geriatricians to optimize the
decision‐making process. However, such initiatives are complicated by the lack of elderly‐
specific data from clinical trials or even observational cohort studies on which to base such
ecisions. d
Aim and outline of this thesis The aim of this thesis is two‐fold: first, to study current treatment practice and decision
making in older cancer patients and second, to investigate the potential value of a
comprehensive geriatric assessment in this decision‐making process.
Part I consists of four cohort studies, focusing on current patterns of care for breast
cancer in elderly patients. Chapter 1 is a retrospective analysis of the diagnostic process
and treatment in a single centre breast cancer outpatient clinic and compares these to
national guidelines. In Chapter 2 the trends in these treatment practices over a six‐year
period is studied, as well as the impact of the introduction of a multidisciplinary breast
cancer team. Chapter 3 examines survival and cause of death in a historical cohort of 187
patients with resectable breast cancer for whom surgery was omitted. Chapter 4
addresses decision making and referral practices for elderly patients residing in nursing
homes who are suspected of breast cancer. As Chapter 5 demonstrates, accrual of elderly
patients in clinical trials is not straight‐forward, emphasizing the value of observational
studies in understanding and optimizing cancer treatment for these patients.
In Part II, current treatment practices for older patients with two other cancer types are
studied. Chapter 6 compares treatment choices and outcome for older colon cancer
patients with their younger counterparts. Iron‐deficiency anaemia can be a first sign of
colon cancer, and in Chapter 7, we assessed diagnostic decision making and clinical
outcome for a cohort of 112 patients with this condition. Chapter 8 addresses age‐related
differences in the treatment of head and neck cancer, and the consequences of guideline
discordance for cancer‐specific survival.
9

Introduction
10
Part III focuses on the potential value of the comprehensive geriatric assessment (CGA) in
decision making for older cancer patients. In Chapter 9, the value of CGA for patient care
and prognostication is studied in a cohort of elderly cancer patients acutely admitted to
hospital. Chapter 10 addresses the ability of a CGA to predict toxicity and survival in
patients undergoing chemotherapy for metastatic breast cancer. This issue is addressed
further in a systematic review in Chapter 11, focusing on the value of geriatric
assessments in predicting treatment tolerance and prognosis in older cancer patients. As a
CGA is a time‐consuming process, Chapter 12 addresses the value of frailty screening tools
for selecting patients likely to benefit from further geriatric assessment.
Finally, Part IV contains a summary of the main findings of this thesis, and a discussion of
e potential consequences of these finding for clinical practice and future research. th
References 1. www.cbs.nl 2. www.cijfersoverkanker.nl

Part I
Breast cancer treatment in the elderly


Chapter 1
Breast cancer in the elderly: retrospective study on diagnosis and treatment according
to national guidelines
M.E. Hamaker, W.H. Schreurs, H.J. van Slooten, J.M. Uppelschoten, C.H. Smorenburg
The Breast Journal 2009;15:26‐33

Chapter 1
Abstract Introduction: We set out to investigate the level of accordance of diagnosis and treatment
of elderly breast cancer patients with national guidelines and to study predictors of
deviation.
Methods: Data on patient and tumour variables were collected from the charts of 166
patients aged 70 years and older, diagnosed at our hospital in 2002‐2004. Diagnostic
work‐up and treatment were compared to guidelines and reasons for deviation were
recorded.
Results: In all, 122 (74%) patients were diagnosed and treated in accordance with
guidelines. Diagnosis was incomplete in 19 patients (11%). Surgery, radiotherapy and
hormonal therapy were withheld in 19 (11%), 11 (7%) and 9 (5%) patients, respectively.
Guideline deviation was motivated in 18 patients (11%) (comorbidity n=11, patients’
preferences n=5, age n=2), unmotivated in 18 (11%), and undeliberate in 8 (5%).
Conclusion: Our study demonstrates that deviation from guidelines in elderly breast
cancer patients mainly occurs due to a deliberate adjustment to patient’s comorbidity and
preference.
14

Breast cancer in the elderly
Introduction In the Netherlands, breast cancer is diagnosed in over 11,500 women each year, of which
30% is aged 70 or older. It is the most frequently diagnosed cancer in women and its
incidence increases with age. In western societies, due to increasing life expectancy and
ageing of the population, the number of elderly patients with breast cancer will increase
substantially over the next decades. It is expected that by the year 2035, 60% of all new
breast cancer patients are 70 years or older.1
Unfortunately, insufficient data are available on the optimal treatment of elderly patients
with breast cancer. Various studies have demonstrated that treatment for women with
breast cancer differs substantially with age.2‐13 If patients are older, they are treated less
extensively, and treatment guidelines are less likely to be followed.6,14
However, this does not automatically imply that elderly patients are undertreated.
Treatment guidelines are based on clinical trials in which patients 65 years of age or older
are greatly underrepresented or even excluded.15‐17 Increasing comorbidity with age
results in an increasingly heterogeneous patient population.5,6,10 Both the physiological
process of ageing as well as comorbidity result in a decreased physical reserve, and the
question whether or not older patients are able to tolerate treatment as well as younger
patients has not been answered conclusively.18 Comorbidity in elderly patients may also
increase the risk of dying of other causes, thereby decreasing the relative impact of breast
cancer on overall survival.19‐23 In addition, studies have demonstrated that elderly women
are often diagnosed at a later stage of the disease,4,19 and that the biology of breast
cancer changes with age.19 Furthermore, patient’s preferences in treatment modalities
need to be taken into account, as older patients may be less willing to trade current
quality of life for survival.24
These differences suggest that guidelines based on studies examining mainly non‐elderly
patients without comorbidity cannot automatically be extended to elderly patients. It may
be possible that observed differences in treatment between older and younger patients
are not a reflection of age but are adequate adjustments to altered biology, physiology,
comorbidity and preferences of older patients.
We set out to investigate the level of adherence to Dutch guidelines in newly diagnosed
breast cancer patients aged 70 years or older and to study various predictors of deviation
t our hospital. a
Methods This study is a retrospective cohort study of women aged 70 years and older diagnosed
with breast cancer at the Medical Centre Alkmaar in the Netherlands between January
2002 and December 2004. Patients with non‐invasive breast cancer or a second primary
breast tumour were excluded from this study.
15

Chapter 1
Using patient’s charts, surgical records, and pathology reports, we collected data on the
following variables: patient’s age, comorbidities, date of diagnosis, tumour histology,
tumour grade, mitotic activity index (MAI), stage of disease (TNM), oestrogen receptor
status, progesterone receptor status, as well as the initial treatment with surgery,
chemotherapy, radiotherapy and/or hormonal therapy. Breast cancer histology was
classified as ductal carcinoma, lobular carcinoma, other, or “not determined” if no
histological or cytological examination was performed. Steroid receptors were determined
by immunohistochemistry and classified as positive (10% or more cells stained positive),
negative (<10%) or unknown. Stage of disease was classified in five groups: stage I (T1 N0
M0), stage II (T0‐2 N1 M0, or T2 N0‐1 M0, T3 N0 M0), stage III (T3 N1 M0,Tany N2‐3 M0), stage
IV (Tany Nany M1) and unknown. Information on functional status was lacking in most
patient charts and subsequently was not collected.
Patients were followed until March 1st 2007. Data on survival was collected from the
charts; if this was insufficient, the patient’s general practitioner was contacted for
additional information.
In addition, diagnostic work‐up and treatment modalities were compared with work‐up
and treatment advised by national guidelines. In the Netherlands, guidelines on diagnosis
and treatment of breast cancer are frequently updated by the Dutch National Breast
Cancer Platform (NABON) and the Dutch Society for Medical Oncology (NVMO). Table 1
summarizes these guidelines for patients aged 70 and older, as used in the period 2002‐
2004.25 This guideline is similar to that of younger post‐menopausal women for diagnostic
work‐up, surgery, hormonal therapy and radiotherapy. The guideline provides no strict
indication for adjuvant chemotherapy, stating that this can be considered in patients with
high‐risk hormone receptor negative disease.
For patients not receiving the standard treatment, reasons for deviating from guidelines
were collected from the charts. These reasons were classified in three categories:
“motivated” if the reason for deviation was documented, “deliberate, reason not
documented” if the treating physician had noted that the guideline was not followed,
without motivating this decision in the patient’s chart; and “undeliberate” if the chart
owed no remark on any deviation from guidelines. sh
Statistical analysis To compare different groups in terms of comorbidity, disease stage, and different
treatment modalities, a chi‐square test was used. A p‐value of lower than 0.05 was
considered to be statistically significant. Statistical analyses were performed using the
tatistical program SPSS for Windows version 14.0. s
16

Breast cancer in the elderly
Table 1: Diagnosis and treatment guidelines for patients aged 70 and older in accordance with the Dutch multidisciplinary guidelines for treatment of breast cancer 2002
25
I. Diagnosis Histology In all patients, histological confirmation of breast cancer should be sought. Lymph node status In all patients with invasive tumours receiving surgery, a diagnostic procedure to determine axillary node status is required. Distant metastases In all patients with T3‐4 and/or N2‐3 tumours, imaging studies for distant metastases is recommended. II. Treatment Surgery In all tumours except T4 and/or M1, surgery is required. Radiotherapy 1. After breast conserving therapy a. radiation of the breast is always required b. regional lymph nodes: in case of pN2‐N3 tumours 2. After modified radical mastectomy, locoregional radiation is required if: a. mastectomy was irradical b. pN2‐N3 c. positive top axillary node d. cT4 e. to be considered in T3 tumours Hormonal therapy 1. If tumour is hormone receptor negative, no hormonal treatment is necessary. 2. In case of lymph node N0 and receptor positive tumour, hormonal therapy is required if : a. tumour size is > 3 cm b. tumour size is 1‐3 cm and mitotic activity index > 10 3. Lymph nodes N1‐2 and receptor positive tumour always require treatment. 4. M1 disease if hormone receptor positive Chemotherapy For patients over age 70, there is no strict guideline with indications for (neo)adjuvant chemotherapy.
17

Chapter 1
Results
Patient and tumour characteristics Between January 2002 and December 2004, 791 patients were diagnosed with breast
cancer in our hospital, of which 205 patients (26%) were aged 70 years or older. Thirty‐
nine patients were excluded from our analysis because of a second primary breast tumour
(n=23), non‐invasive breast cancer (n=14) and treatment elsewhere (n=2). As a result, 166
patients were included in this study (165 females and one male). Patient characteristics
are listed in Table 2. The median age at diagnosis was 78 years (range 70‐96 years).
In our series, 51 patients presented with stage I disease (31%), 57 with stage II (34%,
node‐negative n=29, node‐positive n=28), 29 with stage III (17%) and 17 with metastatic
disease (stage IV, 10%). Overall, older patients presented with more advanced disease
(p=0.003). Tumour stage was unknown in 12 patients (7%) because of insufficient data on
lymph node involvement or tumour size. The percentage of patients with unknown stage
correlated with increase in age.
Table 2: Patient characteristics per age group
70 ‐ 79 yrs 80 ‐ 89 yrs 90+ yrs p‐value*
Number of patients 100 56 10
Chronic and/or current disease 0 1 2 3+
42 (42%) 29 (29%) 16 (16)% 13 (13)%
10 (19%) 14 (26%) 17 (31%) 13 (24%)
1 (11%) 2 (22%) 3 (33%) 3 (33%)
0.04
Stage of disease I II III IV unknown
40 (40%) 34 (34%) 14 (14%) 8 (8%) 3 (3%)
10 (19%) 22 (39%) 10 (19%) 7 (12%) 7 (12%)
1 (10%) 1 (10%) 5 (50%) 1 (10%) 2 (20%)
0.002
0.003
Tumour morphology Not determined Ductal Lobular Other
1 (1%)
77 (77%) 15 (15%) 7 (7%)
3 (5%)
32 (57%) 14 (25%) 7 (12%)
2 (20%) 4 (40%) 1 (10%) 3 (30%)
Hormone receptors Oestrogen receptor positive Progesterone receptor positive
81 (84%) 67 (69%)
40 (82%) 34 (72%)
4 (80%) 4 (80%)
0.95 0.82
Tumour grade Grade I Grade II Grade III Not determined
12 (12%) 35 (35%) 14 (14%) 39 (39%)
3 (5%)
13 (23%) 10 (18%) 30 (54%)
1 (10%) 0 (0%) 2 (20%) 7 (70%)
ns ns ns 0.02
* p‐value in bold signifies a significant differences between age groups (p<0.05); ns = not significant
18

Breast cancer in the elderly
In the majority of patients (n=160; 96%), a histological examination of tumour was
performed. Tumour morphology and grade were less frequently determined in older age
groups (p=0.023). Hormone receptor (HR) status was determined in 90% of tumours.
There were no significant differences in HR status between age groups.
Data on comorbidity were available for 159 patients (96%). Only 53 patients (32%) had no
current or chronic disease. Twenty‐nine patients (18%) had three or more current diseases
at the time of diagnosis. Both presence and number of comorbidities increased with age
(p=0.044, Table 2). Cardiovascular disease was most frequently observed (53%), including
hypertension (29%), coronary artery disease (16%), and TIA or stroke (7%). Other
comorbidities were diabetes mellitus (13%), COPD (5%), thyroid disease (5%), dementia
(3%), and depression (3%). Apart from a prior diagnosis of breast cancer (excluded),
nother 10 patients (6%) had a prior or concurrent malignancy. a
Treatment Early breast cancer (Stage I‐II) In accordance with guidelines, 99 out of 108 patients (92%) with early breast cancer (stage
I and II disease) had surgery; 66 patients had a modified radical mastectomy (MRM), and
33 patients had breast conserving therapy (BCT). A sentinel lymph node procedure (SNP)
was done in a majority of 62 patients (63%), of whom 14 were tumour positive and
followed by an axillary lymph node dissection (ALND). A primary ALND was performed in
34 patients (34%). In three out of 99 patients (3%), no axillary lymph node surgery was
done. Nine patients did not have any surgery.
Twenty‐nine out of 33 patients (88%) with BCT received radiotherapy as indicated by
guidelines. According to the guidelines, radiotherapy was indicated in eight patients after
MRM, and seven patients (88%) were treated accordingly.
Adjuvant hormonal therapy was indicated in 47 patients and 40 patients (85%) were
treated accordingly. Four patients with stage II disease received adjuvant chemotherapy
due to irradical surgery or lymph node metastases.
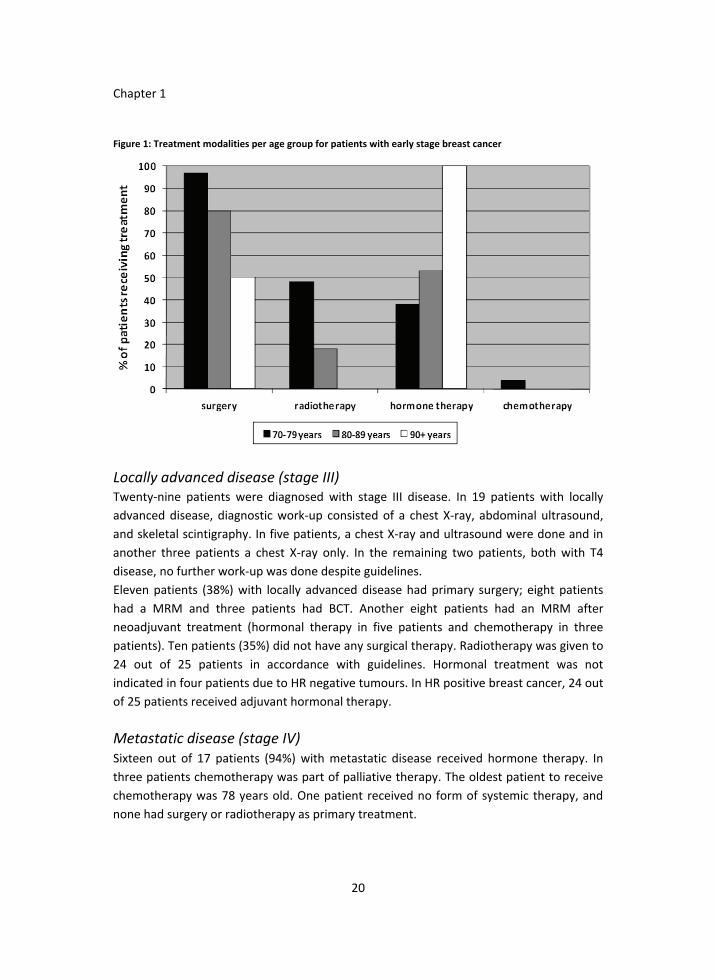
Figure 1 lists treatment modalities per age group for patients with early stage breast
cancer. Older patients were less likely to receive surgery (97% in patients aged 70‐79 years
vs. 50% in the patients aged 90 and over, p=0.002). If surgery was performed, older
patients more often had a MRM than BCT (84% in patients aged 80‐89 years vs. 52 % in
patients aged 70‐79 years, p<0.05 after correction for stage of disease). Differences in the
type of lymph node staging procedure were not significant after correction for stage of
disease. Older patients were less likely to receive radiotherapy as compared to younger
patients (0% vs. 49%, p<0.001). The use of hormonal therapy increased with age: 38% in
atients aged 70‐79 compared to 100% of patients aged >90 (p=0.024). p
19
Chapter 1
Figure 1: Treatment modalities per age group for patients with early stage breast cancer
Locally advanced disease (stage III) Twenty‐nine patients were diagnosed with stage III disease. In 19 patients with locally
advanced disease, diagnostic work‐up consisted of a chest X‐ray, abdominal ultrasound,
and skeletal scintigraphy. In five patients, a chest X‐ray and ultrasound were done and in
another three patients a chest X‐ray only. In the remaining two patients, both with T4
disease, no further work‐up was done despite guidelines.
Eleven patients (38%) with locally advanced disease had primary surgery; eight patients
had a MRM and three patients had BCT. Another eight patients had an MRM after
neoadjuvant treatment (hormonal therapy in five patients and chemotherapy in three
patients). Ten patients (35%) did not have any surgical therapy. Radiotherapy was given to
24 out of 25 patients in accordance with guidelines. Hormonal treatment was not
indicated in four patients due to HR negative tumours. In HR positive breast cancer, 24 out
f 25 patients received adjuvant hormonal therapy. o
Metastatic disease (stage IV) Sixteen out of 17 patients (94%) with metastatic disease received hormone therapy. In
three patients chemotherapy was part of palliative therapy. The oldest patient to receive
chemotherapy was 78 years old. One patient received no form of systemic therapy, and
none had surgery or radiotherapy as primary treatment.
20

Breast cancer in the elderly
Unknown stage of disease Two out of 12 patients (17%) with unknown stage of disease had surgery; one BCT and
one MRM. No axillary lymph node surgery was performed. One patient, with HR negative
disease, received no adjuvant treatment. Eleven patients, with either HR positive disease
r in which receptor status was unknown, received primary or adjuvant hormonal therapy. o
Adherence to guidelines The accordance with guidelines and reasons for deviation are listed in Table 3. Overall,
122 out of 166 patients (74%) were adequately staged and given surgical and adjuvant
treatment in accordance with guidelines.
Diagnosis and staging were incomplete in 19 patients (11%). In six patients (4%), diagnosis
was made on clinical data only, without cytological or histological confirmation;
furthermore, for three of these patients, stage was not determined. In six patients (4%),
no lymph node staging procedure was performed during surgery, and in another seven
patients (4%), the diagnostic strategy supplied insufficient information for staging.
In older patients, treatment guidelines were followed less frequently than in younger
patients (88% of patients aged 70‐79 was treated in accordance to guidelines vs. 40% in
patients aged 90+, p<0.001).
Surgery was withheld in nineteen patients (11%), of whom nine with stage I‐II disease and
ten with stage III disease. The reason stated most frequently was the presence of
comorbidity (n=10), varying from moderate chronic obstructive pulmonary disease to
severe cardiovascular disease, dementia or other metastatic malignancy. Other reasons
stated were patient’s request (n=4), age (n=2) and in two patients the reason was not
clear. One patient died of myocardial infarction before any treatment could be started.
Eleven patients (7%) did not receive radiotherapy despite guidelines. One patient refused
radiotherapy, and for the other patient, the reason stated was her age and comorbidity. In
the remaining patients, it remains unclear why the guidelines were not followed.
Nine patients (5%) did not receive hormonal therapy according to guidelines; reasons for
this were not stated in patients’ charts.
Overall, deviation from diagnostic and treatment guidelines was deliberate in 36 patients
(22%); in 18 of them the decision was motivated in patient’s charts. In only eight patients
(5%), the treating physician seemed unaware of the fact that guidelines were not
followed. In the majority of these patients, this consisted of omitting adjuvant hormonal
or radiotherapy. All eight had early stage breast cancer.
Patients not treated according to guidelines were significantly older (83.0 vs. 76.9 years,
p<0.001), and had more comorbidity (1.7 vs. 1.2 comorbid conditions, p=0.024). There
were no differences in hormone receptor status or stage of disease. In a multivariate
analysis, no single factor was an independent predictor of adherence to guidelines, with
21

Chapter 1
the exception of patients with stage II disease, in which case both advanced age (p=0.028)
and increasing comorbidity (p=0.016) were significantly correlated with deviation from
guidelines.
Table 3: Adherence to national guidelines
70‐79
yrs
n=100
80‐89
yrs
n=56
90+
yrs
n=10
Total
n=166
Treatment and diagnosis in accordance with
guidelines***
86
(86%)
34
(61%)
4
(40%)
122
(74%)
Incomplete diagnosis
No histological/cytological confirmation
No axillary lymph node procedure during surgery
Insufficient information for staging
1
2
2
3
4
6
2
0
2
6
6
10
A.*
Insufficient treatment
No surgery
No radiotherapy
No hormonal therapy
4
4
5
12
3
4
3
4
0
19
11
9
B. ** Motivated deviation***
Comorbidity
Malignancy of another origin
Dementia
Moderate to severe cardiovascular disease
Multiple sclerosis
Parkinson’s disease
Moderately severe COPD
Age
At patient’s request
Deliberate deviation, reason not documented
Undeliberate deviation
3
0
1
4
4
4
2
4
9
4
4
0
0
3
0
11
2
2
4
1
1
1
2
5
18
8
* Panel A lists the number of patients in which guidelines were followed and the ways in which treatment or staging deviated from guidelines. ** Panel B lists the reasons for deviating from guidelines as stated in the patients’ chart. *** In some patients, both staging and treatment was not according to guidelines, or more than one treatment modality was withheld. Similarly, in some patients, multiple reasons for deviating from guidelines were given Therefore, patients may be listed more than once.
22

Breast cancer in the elderly
Figure 2: Kaplan Meier survival plots, stratified per stage of disease
Survival After a median follow‐up of 38 months, 70.5% of patients were still alive. Figure 2 shows
Kaplan Meier plots, stratified per stage of disease.
Patients who died were significantly older (p<0.001), had more comorbidity (p=0.001), had
more advanced disease (p=0.034) and were less likely to have been treated in accordance
with guidelines (p=0.003). In a multivariate analysis, only comorbidity and stage of disease
mained independent predictors of mortality. re
Discussion In this study, we examined the diagnosis and treatment patterns of women with newly
diagnosed breast cancer, aged 70 and older, in relation to age, disease stage and
comorbid conditions. Using Dutch national guidelines, which are stage‐specific and
modified for age, we found that in 74% of patients guidelines were followed, and that
adherence to guidelines decreased with advancing age.
Several other studies have examined adherence to treatment guidelines in elderly breast
cancer patients. Giordano et al noticed that in patients aged >75 years, accordance with a
stage‐specific guideline decreased with age, varying from 80% for surgical therapy to 29%
23

Chapter 1
for adjuvant chemotherapy.14 Yancik et al found that only 7% of 448 patients with stage I
and II breast cancer aged >70 were given less than minimally expected treatment, but this
study only examined surgical treatment.6 Bouchardy et al observed that nearly 50% of
patients aged >80 had sub‐optimal treatment strategies;7 however, optimal treatment
was not clearly defined and was not stage‐specific. As breast cancer treatment guidelines
depend on age and stage of disease, both factors need to be taken into account to
examine accordance to these guidelines. One of the strengths of our study is that national
guidelines we used are stage‐specific and have been modified for age.
Several studies have shown that patients with comorbidity are less likely to be treated
according to guidelines than patients without comorbidity.5‐7,9,20,24 Similarly, we found that
comorbidity was the most frequently stated reason for deviating from guidelines (11 out
of 18 motivated deviations, Table 3), also being an independent predictor of mortality.
Other studies have demonstrated that the impact of breast cancer on prognosis decreases
as the risk of dying from comorbid disease increases.20‐23 For example, Coebergh et al
found that, although overall 10‐year survival is much lower in women aged >70 as
compared to younger patients (16% vs. 41%, respectively), the cancer‐specific survival is
quite similar (49% vs. 53%).27 Therefore, serious comorbidity can be a legitimate reason
for deviating from treatment guidelines if the life‐expectancy of a patient is significantly
reduced by it. In our study, the adjustment of treatment in ten patients because of
comorbidity seems adequate, considering the severity of these comorbid conditions
(Table 3).
Age was not a major factor in determining whether guidelines were followed, being a
reason for deviating from treatment guidelines in only two patients in our study. Although
older women were less likely to be treated according to guidelines, age was not an
independent predictor of guideline deviation after correcting for comorbidity and stage of
disease. Bickell et al recently published a study on reasons for omitting adjuvant therapy
in both elderly and non‐elderly breast cancer patients.26 Physicians did not recommend
therapy because of older age, comorbidity or unawareness of treatment benefit in 14%,
11% and 3% of treatment omissions, respectively, while 31% of treatment omissions was
due to patient preference. In our study, deviation from guidelines was undeliberate in
eight out of 44 patients with any guideline deviation; this occurred primarily in patients
with early stage breast cancer and frequently involved hormonal therapy. Given the
relatively low treatment burden for the patient, this possibly implies undertreatment. Of
notice, other studies have observed that older women with a relatively low risk of
recurrence (i.e. early stage disease) are less likely to receive treatment according to
guidelines. For example, Giardano et al found that in post‐menopausal women, deviations
from guidelines were found primarily in early stage breast cancer, while advanced disease
24

Breast cancer in the elderly
was highly predictive of accordant therapy.14 This suggests that in early stage disease the
need for adjuvant therapy is not as obvious as it is in advanced disease.
At present, diagnostic and therapeutic decisions for patients with breast cancer in the
Netherlands are made in multidisciplinary meetings with dedicated breast surgeons,
radiographers, pathologists, oncologists, radiation oncologists and breast care nurses. In
our hospital, these meetings were initiated in 2006, thus after the time period of this
study. We intend to evaluate the effect of these multidisciplinary meetings on the
adherence to national guidelines in the elderly.
Most studies on the effect of age and comorbidity in elderly breast cancer patients have
used national databases, with central data collection by national cancer institutes.6
However, patient’s medical records are generally regarded as the most complete source of
information on the patient’s past and current health status.20 Thus, one of the strengths of
this study is that the data we accumulated using patients’ charts may be more clinically
precise than those obtained from self‐reports or administrative databases using discharge
data.
However, in a retrospective analysis, it is impossible to determine whether discordance
with guidelines is justifiable based on patient’s health status or should be considered as
undertreatment. Furthermore, it is still not certain how to measure health status or
functional reserves in elderly cancer patients.7,9,19,28‐29 Therefore, prospective studies are
needed to validate comprehensive geriatric assessments as a decision‐making tool in
geriatric oncology.28 Until such a tool is developed and incorporated into guidelines,
treating physicians will have to determine for each individual patient whether or not
uidelines provide adequate treatment. g
In conclusion, this study provides new insight into the accordance with diagnosis and
treatment guidelines in elderly breast cancer patients. Our study demonstrates that
deviation from treatment guidelines occurs in a fourth of patients, mainly due to
deliberate deviation from guidelines as an adjustment to the patient’s comorbidity and
preference.
25

Chapter 1
References 1. Hillen HF, Hupperets PS. [Breast cancer in patients 70 years and older]. Ned Tijdschr Geneesk
2000;144:1099‐104. 2. Vulto AJ, Lemmens VE, Louwman MW et al. The influence of age and comorbidity on receiving
radiotherapy as part of primary treatment for cancer in South Netherlands, 1995‐2002. Cancer 2006;106:2734‐42.
3. Wanebo HJ, Cole B, Chung M et al. Is surgical management compromised in elderly patients with breast cancer? Ann Surg 1997;225:579‐89.
4. Bergman L, Kluck HM, Leeuwen FE van et al. The influence of age on treatment choice and survival of elderly breast cancer patients in South‐Eastern Netherlands: a population‐based study. Eur J Cancer 1992;28A:1475‐80.
5. Janssen‐Heijnen ML, Maas HA, Lemmens VE et al. Samenhang van leeftijd en comorbiditeit met therapie en overleving bij patiënten met kanker in Noord‐Brabant en Noord‐Limburg 1955‐2001. Ned Tijschr Geneeskd 2005;149:1686‐90.
6. Yancik R, Wesley MN, Ries LAG et al.. Effect of age and comorbidity in postmenopausal breast cancer patients aged 55 years and older. JAMA 2001;285:885‐892.
7. Bouchardy C, Raptiti E, Rioretta G et al. Undertreatment strongly decreases prognosis of breast cancer in elderly women. J Clin Oncol 2003;21:3580‐7.
8. Livi L, Paiar F, Saieva C et al. Breast cancer in the elderly: treatment of 1500 patients. The Breast Journal 2006;4:353‐9.
9. Louwman WJ, Janssen‐Heijnen ML, Houterman S et al. Less extensive treatment and inferior prognosis for breast cancer patients with comorbidity: a population‐based study. Eur J Cancer 2005;41:779‐85.
10. Hurria A, Leung D, Trainor K et al. Factors influencing treatment patterns of breast cancer patients age 75 and older. Crit Rev Oncol Hematol 2003;46:121‐6.
11. Gajdos C, Tartter PI, Bleiweiss IJ et al. The consequence of undertreating breast cancer in the elderly. J Am Coll Surg 2001;192:598‐707.
12. Enger SM, Thwin SS, Buist DS et al. Breast cancer treatment of older women in integrated health care settings. J Clin Oncol 2006;24:4377‐83.
13. Ballard‐Barbash R, Potosky AL, Harlan LC et al. Factors associated with surgical and radiation therapy for early stage breast cancer in older women. J Natl Cancer Inst 1996;88:716‐26.
14. Giordano SH, Horobagyi GN, Kau SW et al. Breast cancer treatment guidelines in older women. J Clin Oncol 2005;23:783‐91.
15. Townsley CA, Selby R, Siu LL. Systematic review of barriers to the recruitment of older patients with cancer onto clinical trials. J Clin Oncol 2005;23:3112‐24.
16. Hutchins LF, Unger JM, Crowley JJ et al. Underrepresentation of patients 65 years of age or older in cancer‐treatment trials. N Engl J Med 1999:341:2061‐7.
17. Early Breast Cancer Trialist Collaborative Group (EBCTCG). Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15‐year survival: and overview of the randomised trials. Lancet 2005;365:1687‐717.
18. Silliman RA. What constitutes optimal care for older women with breast cancer? J Clin Oncol 2003;21:3554‐6
19. Diab SG, Elledge RM, Clark GM. Tumour characteristics and clinical outcome of elderly women with breast cancer. J Natl Cancer Inst 2000;92:550‐6.
20. Houterman S, Janssen‐Heijnen ML, Verheij CD et al. Comorbidity has negligible impact on treatment and complications but influences survival in breast cancer patients. Br J Cancer 2004;90:2332‐7.
21. Rijke JM de, Schouten LJ, Hillen HF et al. Cancer in the very elderly Dutch population. Cancer 2000;89:1121‐33
22. Extermann M, Balducci L, Lyman GH. What threshold for adjuvant therapy in older breast cancer patients. J Clin Oncol 2000;18:1709‐17.
23. Read WL, Tierney RM, Page NC et al. Differential prognostic impact of comorbidity. J Clin Oncol 2004;22:3099‐103.
24. Yellen SB, Cella DF, Leslie WT. Age and clinical decision making in oncology patients. J Natl Cancer Inst 1994;86:1766–1770.
26

Breast cancer in the elderly
27
25. Multidisciplinaire richtlijn voor de behandeling van borstkanker. Kwaliteitsinstituut voor gezondheidszorg CBO 2002. Revised 2004.
26. Bickell NA, LePar F, Wang JJ, Leventhal H. Lost opportunities: physician’s reasons and disparities in breast cancer treatment. J Clin Oncol 2007;23:2516‐21.
27. Coebergh JW, Heyden LH van der, Jansen‐Heijnen ML. Cancer incidence and survival in the South‐east of the Netherlands. Eindhoven: integraal kankercentrum Zuid 1995.
28. Terret C, Zulian G, Droz JP. Statements on the interdependence between the oncologist and the geriatrician in geriatric oncology. Crit Rev Oncol Hematol 2004;52:127‐22.
29. Extermann M, Aarpo M, Barnabei R et al. Use of comprehensive geriatric assessment in older cancer patients. Crit Rev Oncol Hematol 2005;55:241‐52.


Chapter 2
Trends in breast cancer treatment in the elderly at a breast cancer outpatient clinic
M.E. Hamaker,
W. H. Schreurs, H.J. van Slooten, J.M. Uppelschoten, C.H. Smorenburg
Nederlands Tijdschrift voor Geneeskunde 2009;153:A562
A translation of: “Trends in de behandeling van borstkanker bij ouderen op een mammapolikliniek: minder vaak operatieve behandeling”

Chapter 2
Abstract Aim: To assess the treatment of elderly patients with resectable breast cancer treated at
the Medical Centre Alkmaar before and after the implementation of a multidisciplinary
breast cancer team in February 2006.
Methods: Retrospective chart review of all patients aged 70 years and older with a newly
diagnosed resectable breast tumour (stage I and II) treated between 2002 and 2007.
Results: Of 232 patients, 84% received surgical treatment. Adjuvant treatment with
radiotherapy, endocrine therapy and chemotherapy was given to 88, 91 and 5 patients
respectively. Over time, there was a significant decrease in the percentage of patients that
were treated surgically, particularly for patients aged 80 years and older. The number of
patients receiving radiotherapy in accordance with guidelines improved over time, while
the guideline adherence for endocrine treatment remained more or less stable. The
reporting of decisions regarding treatment and guideline discordance improved.
Conclusion: Between 2002 and 2007, treating physicians seemed more aware of guidelines
and guideline discordance was more clearly motivated in the patient’s chart. Guideline
adherence for radiotherapy improved but there was a significant decrease in surgical
treatment over time, particularly in patients aged 80 years and older.
30

Trends in breast cancer treatment for the elderly
Introduction In the coming decades, increasing life expectancy and ageing of the population will result
in a substantial increase in the number of older cancer patients;1‐4 it is expected that by
2035, 60% of all new breast cancer patients will be over 70 years of age.2 Although
attempts have been made to actively include older patients in oncologic trials, most
treatment guidelines are still based on research done in relatively fit patients.3 In addition,
changes in tumour characteristics with increasing age have important prognostic and
therapeutic implications.5‐7 Furthermore, comorbidity, polypharmacy, decreased
functional capacity and decreased physiological reserve result in increasing heterogeneity
in the elderly population;8,9 these factors must be taken into account in the decision‐
making process.10,11
Previous studies have shown that case review by a multidisciplinary breast cancer team at
a breast cancer clinic resulted in an alteration of the treatment for over 50% of patients.12
Furthermore, pre‐operative consultation with an oncologist has been shown to result in
better guideline adherence for breast cancer patients.13
In the Netherlands, decision making for breast cancer treatment is increasingly done in a
multidisciplinary breast cancer team (MBCT),14 which includes treating physicians
(surgeons, oncologists, radiotherapists), supporting specialists (pathologists, radiologists)
and specialised nurses. These MBCTs have been developed by the Integral Cancer Centres
(IKC) and their procedures have been recorded in the “Organization of Breast Cancer
Care” written by the National Breast Cancer Council Netherlands (NABON).
In February 2006, a weekly MBCT meeting was initiated at the Medical Centre Alkmaar in
the Netherlands. In this study, we examined if the implementation of this MBCT
influenced treatment decisions and guideline adherence for older patients with a
sectable breast cancer treated at the breast cancer out‐patient clinic of this hospital. re
Methods We performed a retrospective cohort study of patients aged 70 years and older, treated at
the Medical Centre Alkmaar, in the Netherlands, for a newly diagnosed, primary
resectable breast cancer (stage I or II) between January 2002 and December 2007.
Patients with a second primary breast cancer, involvement of a fixed parasternal (N2),
subclavicular or supraclavicular lymph node (N3) or distant metastases (M1) were
excluded.
The following variables were collected from the patient’s medical and surgical charts, and
pathology reports: age, date of diagnosis, histological data, tumour grade, mitotic activity,
stage (TNM), oestrogen and progesterone receptor status, expression of human epidermal
growth factor type 2 (Her2Neu), as well as data on the initial treatment. The stage of
31

Chapter 2
disease was subdivided into two categories: stage I (T1N0M0) and stage II (T0‐2N1M0 or
T3N0M0).
The presence of the following comorbid diseases was recorded: valvular disease, angina
pectoris, myocardial infarction, heart failure, arrhythmias, left ventricular hypertrophy,
hypertension, diabetes, stroke, Parkinson’s disease, pulmonary embolism, chronic
obstructive lung disease, rheumatoid arthritis, renal insufficiency, prior malignancies,
osteoporosis, thyroid disease, dementia, mood disorders, psychotic disorders and
personality disorders.
The actual diagnostic process and initial treatment were compared to the national
guidelines, as developed by the NABON.15,16 Table 1 lists an overview of the
recommendations for diagnosis and treatment for patients aged 70 years and over during
the study period.
In case of discordance with guidelines, the patient’s chart was consulted to find the
motivation behind these treatment choices. Table 1: Diagnostic and treatment guidelines for stage I and II breast cancer in patients aged 70 years and older
15,16
Indication
Histology Breast cancer should be histologically confirmed in all patients. Diagnostic procedures Lymph node
status In case of surgical treatment, a diagnostic procedure for assessing lymph node status is required.
Surgery Surgery is indicated in all patients with stage I and II disease.
Radiotherapy 1. Radiotherapy is always required after breast conserving treatment. 2. Locoregional radiotherapy is also required in case of irradical mastectomy.
Endocrine therapy Jan 2002 to Sept 2005
1. In case of hormone receptor negative breast cancer, endocrine treatment is not required. 2. In the absence of lymph node metastases and in case of hormone receptor positive disease, endocrine treatment is recommended if: a. tumour is larger than 3 cm b. tumour size is between 1 and 3 cm and mitotic activity is greater than 10 3. In case of lymph node metastases and hormone receptor positive disease, endocrine treatment is always required.
Endocrine therapy Oct 2005 to Dec 2007
1. As in Jan 2002 to Sept 2005 2. In the absence of lymph node metastases and in case of hormone receptor positive disease, endocrine treatment is recommended if: a. tumour is larger than 1 cm and grade III disease b. tumour is larger than 2 cm and grade II‐III c. tumour is larger than 3 cm 3. As in Jan 2002 to Sept 2005
Treatment
Chemotherapy
There are no strict recommendations for chemotherapy in patients aged 70 years or older. Chemotherapy should be considered for patients with hormone receptor negative disease and a high risk of recurrence.
32

Trends in breast cancer treatment for the elderly
Statistical analysis To assess differences between age groups and differences in guideline adherence
between various subgroups, the SPSS (Statistical Package for the Social Sciences) version
14.0 was used. The chi‐square test was used for nominal and ordinal variables. For
continuous variables with a normal distribution, the Student t‐test was used, and for
ontinuous variables with a non‐normal distribution the Mann‐Whitney test. c
Results
Patient and tumour characteristics Between January 2002 and December 2007, 285 patients aged 70 years and older
presented with a resectable breast cancer at our clinic. After exclusion of 53 patients with
a second primary breast cancer, 232 patients (229 women, 3 men) remained for further
analysis. Median age of these patients was 77.9 years (range 70‐94 years; Table 2). For 102
patients, disease was at stage I (44%), and for 120 at stage II (56%).
For the great majority of patients, the presence of breast cancer was histologically
confirmed (n=227, 98%). Hormone receptor status was assessed in 220 patients (95%);
86% (189/220) was oestrogen receptor positive and 74% (163/220) was progesterone
receptor positive. Her2Neu status was assessed in 84 patients, and an overexpression of
these receptors was found in seven patients (8.3%).
Over time, no significant changes were seen in the stage of disease at presentation or the
tumour characteristics.
Data on comorbidity was available for 230 patients; 68 had no concurrent disease (30%).
The most frequent comorbid conditions were cardiac arrhythmias (n=33), angina pectoris
or myocardial infarction (n=40), hypertension (n=81), diabetes (n=32), heart failure (n=11),
stroke (n=22), pulmonary disease (n=13), psychiatric disorders and dementia (n=19) and a
prior malignancy (n=18). Comorbidity increased over time; in 2002, 19% of patients had
three or more comorbid conditions, which increased to 33% by 2007 (p=0.059).
Table 2: Patient characteristics
Total 2002‐3 2004‐5 2006‐7 p‐value*
Number of patients 232 71 75 86
Median age 75.9 years 76.8 years 78.4 years 78.3 years 0.178
Stage I Stage II
102 (44%) 130 (56%)
33 (46%) 38 (54%)
31 (41%) 44 (59%)
38 (44%) 48 (56%)
ns
Oestrogen receptor positive Progesterone receptor positive Her2neu overexpression
189/220 (86%)163/220 (74%)
7/84 (8%)
55/67 (82%)48/67 (71%)
0/0 (‐)
65/74 (88%)55/73 (75%)4/25 (16%)
76/86 (88%) 65/86 (75%) 3/59 (5%)
ns ns ns
Number of comorbid disease 1.5 1.3 1.4 1.8 0.059 *ns = not significant
33

Chapter 2
Treatment Overall, 195 patients received surgical treatment (84%); 109 had a modified radical
mastectomy and 86 patients had breast conserving surgery. In 192 of the 195 patients
treated surgically, an additional procedure for staging of the axillary nodes was
performed; for 128 of these, a sentinel node procedure was used.
Of the 86 patients with breast conserving surgery, 80 received adjuvant radiotherapy
(93%) in accordance with guidelines. Radiation after a modified radical mastectomy was
recommended by guidelines for nine patients, and eight were treated accordingly (88%).
Adjuvant hormonal treatment was recommended for 103 patients, and was given to 91 of
these (88%). In addition, five patients received adjuvant chemotherapy due to irradical
surgery, high risk disease or lymph node metastases.
Despite resectable disease, surgery was withheld in 37 patients (13 with stage I disease, 24
with stage II). These patients were significantly older (median age 86.1 years vs. 76.3 years
in patients treated surgically, p<0.001) and had significantly more comorbidity (median
number of disease 2.43 vs. 1.33 in patients treated surgically, p<0.001). For one patient,
no treatment was given and for two patients, treatment was unclear. The remaining 34
patients received primary endocrine treatment (tamoxifen n=21, anastrozole n=13). Two
patients eventually did receive a modified radical mastectomy, one due to disease
progression after 10 months of endocrine treatment, and one due to an alteration in the
patient’s wishes 11 months after diagnosis. At the end of the study period, after a median
follow‐up of 1.9 years, 14 of these 37 patients had stable disease, three had progressive or
metastatic disease and 13 patients had died. Cause of death was generally not available. A
further seven patients were lost to follow‐up.
Figure 1 shows the changes in guideline adherence over time. The use of endocrine
treatment and chemotherapy remained more or less the same, while the use of
radiotherapy increased (2002‐2003 85%, 2004‐2005 97%, 2006‐2007 100%, p=0.03). There
was a significant decrease in guideline adherence for surgical treatment: in the first two
years 94% of patients with stage I and II were treated surgically, but this decreased to 84%
in 2004‐2005 and was as low as 76% in 2006‐2007 (p=0.002). This decrease was
particularly evident in patients aged 80 years and over, for whom guideline adherence
decreased from 80% in 2002‐2003 to 33% in 2006‐2007 (p=0.01); in the same time period,
the percentage of patients aged 70‐80 years that received surgical treatment, as
commended by guidelines, remained over 95%. re
Guideline adherence and the MBCT Overall, 170 of the 232 patients were diagnosed and treated in accordance with national
guidelines (77%). Over time, a non‐significant decrease in guideline adherence was seen:
83% of patients (59/71) in 2002‐2003, 77% (58/75) in 2004‐2005, and 74% (62/85) in
34

Trends in breast cancer treatment for the elderly
2006‐2007 (p=0.23). As demonstrated by Figure 1, this decrease was primarily due to the
decrease in the percentage of patients treated surgically.
Reporting of reasons behind guideline discordance improved over time: in 2002‐2003 this
decision was motivated in 22% of patients (2/9), in 2004‐2005 in 93% (12/13) and in 2006‐
2007 in 100% (21/21, p<0.001). Of the 35 documented decisions not to follow guidelines,
19 were due to comorbidity (42%) including previous malignancy (n=3), cardiac disease
(n=5), dementia (n=1), depression (n=3) and stroke (n=4). Other documented reasons for
guideline discordance were the patient’s overall condition (n=4, 9%), age (n=5, 13%) or the
patient’s preference (n=14, 35%).
The weekly MBCT conference at the Medical Centre Alkmaar was initiated in February
2006. In the first year, 82% of newly diagnosed patients were discussed at this conference;
this percentage increased to 98% in 2007. Although a direct comparison of treatment
before and after the start of the MBCT conference does show significant differences in
guideline adherence, Figure 1 shows that these are due to trends that were already visible
in the years before the MBCT meetings were initiated. This makes causal relationship
between the start of the MBCT conferences and these developments unlikely.
Figure 1: Treatment patterns per two year interval
Surg=surgery, Ax=surgical procedure for axillary lymph node staging, RT=radiotherapy, ET=endocrine therapy, CT=chemotherapy Percentages represent the amount of patients for whom a specific treatment was recommended that actually receiving this treatment. For chemotherapy, this percentage represents the number of patients for whom chemotherapy should have been considered that actually received chemotherapy. The multidisciplinary breast cancer team meetings started in February 2006.
35

Chapter 2
Discussion In this study, we assessed changes in the treatment of resectable breast cancer in patients
aged 70 years and older in a large peripheral Dutch hospital between 2002 and 2007. Over
time, the use of endocrine treatment and chemotherapy remained stable, and an increase
was seen in the use of adjuvant radiotherapy. However, we found a significant decrease in
the number of patients treated surgically, particularly in patients aged 80 years and older,
for whom adherence to surgical guidelines decreased from 80 to 33% over time. These
patients were older and had more comorbidity than surgically treated patients, and often
received primary endocrine therapy instead. Interestingly, we also found an increase in
the number of comorbid conditions for the entire patient group. This trend has been seen
in other studies.17,18
Breast cancer surgery in itself has a low mortality risk (0.0‐0.3%).1,10 However, previous
studies have demonstrated that comorbid conditions are the primary cause of post‐
operative complications and mortality.19 Furthermore, 10% of older patients experience a
post‐operative decrease in cognitive function.20 In addition, multiple studies have shown
that comorbidity plays a greater role in overall survival than cancer‐specific mortality,
particularly in case of early stage disease.1,10,11,21 This is also demonstrated by a recent
Cochrane review, on breast cancer in women aged 70 years and older,22 which found no
difference in overall survival between patients receiving surgical treatment only when
compared to endocrine monotherapy. Limited life‐expectancy due to comorbidity could
therefore be a legitimate reason to withhold surgery. However, progressive disease can
have a significant impact on quality of life; the same Cochrane review demonstrated that
primary endocrine treatment results in a significant decrease in progression‐free
survival.22
We found that between 2002 and 2007 treating physicians seemed to be more aware of
guidelines as guideline discordance was more frequently motivated in the patient’s chart:
in 2002‐2003 only 22% of these decisions were motivated in the chart compared to 100%
in 2006‐2007 (p<0.001). Comorbidity (in 42%) and patient’s preference (in 35%) were the
primary reasons to adjust treatment.
Although assessing for differences between treatment before and after the
implementation of the weekly MBCT conference reveals some differences, these are
based on trends already visible before the start of the MBCT meetings (Figure 1). The
implementation of these conferences thus seems to be a part of a greater awareness of
the importance of adequate treatment for older patient with breast cancer, and a
recognition of the complexity of treatment decisions, requiring a multidisciplinary
approach. This fact has also been stressed in a recent report by the Dutch Health Care
Inspection (IGZ) on coordinated care trajectories for cancer patients, addressing the
36

Trends in breast cancer treatment for the elderly
importance of multidisciplinary treatment and collaboration of the different specialists
volved in the treatment process.23 in
In conclusion, between 2002 and 2007, we found an increased awareness of treatment
guidelines among the treating physicians involved in the treatment of breast cancer;
treatment decisions were better motivated. For older patients, guidelines on adjuvant
radiotherapy were followed more frequently, but we found a significant decrease in the
use of surgical treatment, particularly in patients aged 80 years and older. Comorbidity
and patient’s preference were of primary importance for guideline discordance. Well‐
coordinated multidisciplinary treatment remains of the utmost importance, particularly in
older cancer patients.
37

Chapter 2
38
References 1. Wildiers H, Kunkler I, Biganzoli L et al. Management of breast cancer in elderly individuals:
recommendations of the International Society of Geriatric Oncology. Lancet Oncol 2007; 8:1101‐1115. 2. Hillen HF, Hupperets PS. [Breast cancer in patients, 70 years or older]. Ned Tijdschr Geneeskd
2000;144:1099‐1104. 3. Smorenburg CH, Sijp JR. [Breast cancer in the elderly]. Ned Tijdschr Oncol 2006;3:247‐252. 4. Janssen‐Heijnen ML, Maas HA, Lemmens VE et al. [The correlation of age and comorbidity with therapy and
survival in cancer patients in North‐Brabant and North‐Limburg, 1995‐2001]. Ned Tijdschr Geneeskd 2005;149:1686‐1690.
5. Molino A, Giovannini M, Auriemma A et al. Pathological, biological and clinical characteristics, and surgical management, of elderly women with breast cancer. Crit Rev Oncol Hematol 2006;59:226‐233.
6. Gennari R, Curigliano G, Rotmensz N et al. Breast carcinoma in elderly women: features of disease presentation, choice of local and systemic treatments compared with younger postmenopasual patients. Cancer 2004;101:1302‐1310.
7. Diab SG, Elledge RM, Clark GM. Tumor characteristics and clinical outcome of elderly women with breast cancer. J Natl Cancer Inst 2000;92:550‐556.
8. Extermann M, Overcash J, Lyman GH et al. Comorbidity and functional status are independent in older cancer patients. J Clin Oncol 1998;16:1582‐1587.
9. Louwman WJ, Vulto JC, Verhoeven RH et al. Clinical epidemiology of breast cancer in the elderly. Eur J Cancer 2007;43:2242‐2252.
10. Wyld L, Reed M. The role of surgery in the management of older women with breast cancer. Eur J Cancer 2007; 43:2253‐2263.
11. Janssen‐Heijnen ML, Maas HA, Houterman S et al. Comorbidity in older surgical cancer patients: influence on patient care and outcome. Eur J Cancer 2007;43:2179‐2193.
12. Newman EA, Guest AB, Helvie MA et al. Changes in surgical management resulting from case review at a breast cancer multidisciplinary tumor board. Cancer 2006;107:2346‐2351.
13. Keating NL, Landrum MB, Ayanian JZ et al. Consultation with a medical oncologist before surgery and type of surgery among elderly women with early‐stage breast cancer. J Clin Oncol 2003;21:4532‐4539.
14. van Nes JG, van de Velde CJ. [The multidisciplinary breast cancer care team: promoting better care]. Ned Tijdschr Geneeskd 2005;149:1929‐1931.
15. Multidisciplinaire richtlijn voor de behandeling van borstkanker. Kwaliteitsinstituut voor gezondheidszorg CBO 2002. Revisie 2004.
16. Multidiciplinaire richtlijn voor de behandeling van borstkanker. Kwaliteitsinstituut voor gezondheidszorg CBO 2005.
17. Jagger C, Matthews RJ, Matthews FE et al. Cohort differences in disease and disability in the young‐old: findings from the MRC Cognitive Function and Ageing Study (MRC‐CFAS). BMC Public Health 2007;7:156.
18. Deeg D. Gezond ouder worden. Geriatrie dagen; 2008. 19. Tiret L, Desmonts JM, Hatton F, Vourc'h G. Complications associated with anaesthesia‐‐a prospective survey
in France. Can Anaesth Soc J 1986;33:336‐344. 20. Samain E, Schauvliege F, Deval B, Marty J. Anesthesia for breast cancer surgery in the elderly. Crit Rev Oncol
Hematol 2003;46:115‐120. 21. Satariano WA, Ragland DR. The effect of comorbidity on 3‐year survival of women with primary breast
cancer. Ann Intern Med 1994;120:104‐110. 22. Hind D, Wyld L, Beverley CB, Reed MW. Surgery versus primary endocrine therapy for operable primary
breast cancer in elderly women (70 years plus). Cochrane Database Syst Rev 2006;(1):CD004272. .

Chapter 3
Omission of surgery in elderly patients with early stage breast cancer
M.E. Hamaker, E. Bastiaannet, D. Evers, W. van de Water, C.H. Smorenburg, E. Maartense,
A.M. Zeilemaker, G.J. Liefers, L. van der Geest, S.E. de Rooij, B.C. van Munster, J.E.A. Portielje
European Journal of Cancer 2012 Sept 6 [Epub ahead of print]

Chapter 3
Abstract Aim: To assess national trends over time in surgery for elderly patients with resectable
breast cancer and to evaluate clinical outcome and cause of death after omission of
surgery in a regional cohort of elderly patients.
Methods: National trends in 1995‐2005 were calculated using cancer registry data. In
addition, a chart review was performed in a cohort of patients aged ≥75 years, with early
stage breast cancer but no primary surgery, diagnosed at five Dutch hospitals in 1990‐
2005. Patient characteristics, comorbidity and reason for omission of surgery were
collected from the chart. Cause of death was retrieved from death certificate data
registered at Statistics Netherlands.
Results: Omission of surgery increased significantly over time for patients aged 80 years
and older (p<0.05). Of the 187 patients in the regional cohort (median age 85.9 years
(range75.0‐97.7), 174 (92%) received hormonal therapy. Omission of surgery was at the
patient's request in 59 patients (32%). Of the 178 patients that died during follow‐up, 60
patients (34%) died of breast cancer. For 81 patients (45%), breast cancer was not
clinically relevant at the time of death. Median overall survival was 2.3 years (range 0.2‐
10.7) and did not differ between breast cancer and other causes of death (p=0.9).
Conclusion: Omission of surgery for elderly patients with resectable breast cancer has
increased significantly over the past decade; instead patients often received primary
endocrine treatment. Although this may appear an effective alternative to surgery, the
potential for a longer term negative impact on disease control and quality of life deserves
further investigation.
40

Omission of breast cancer surgery in the elderly
Introduction Western societies are ageing; for example, in the Netherlands, the proportion of
inhabitants aged 75 years and over will rise from its current 7% to as much as 15% by
2045.1 As breast cancer incidence increases with age,2 these demographic changes mean
that the number of elderly breast cancer patients will also increase considerably over the
coming decades.3
Cancer specialists are faced with the challenge of determining the appropriate treatment
for these elderly patients. National guidelines are based on trials from which older
patients and those with comorbidity were often excluded.4,5 It is uncertain if the results of
these trials can be extrapolated to the elderly population, with their somatic and
psychogeriatric comorbidity and decreased physiological reserves.6 These conditions can
alter the ability of a patient to tolerate treatment and represent competing causes of
death.7,8 Limited life‐expectancy of frail elderly patients may indicate that they do not live
long enough to benefit from treatment aimed at decreasing the risk of cancer recurrence,8
while they may suffer the side‐effects and complications of this treatment.
As a result, elderly cancer patients do not always receive standard treatment. For
example, surgery may be replaced by primary endocrine therapy and adjuvant treatment
may be omitted.6,9 In a recently published study on treatment patterns for older breast
cancer patients in a single cancer clinic, we concluded that the number of patients aged 80
years and older that received surgery for resectable breast cancer decreased greatly over
the last decade, from 80% to 33%.10 However, the number of patients and duration of
follow‐up was insufficient to ascertain the clinical outcome for these patients.
Therefore, the aim of this study was two‐fold: first, to determine whether this local trend
towards less surgery for elderly patients with resectable breast cancer could also be found
on a national level and second, to evaluate the effect of omission of surgery by examining
clinical outcome and cause of death for a multicentre cohort of elderly patients (aged 75
ears and older) with resectable breast cancer that did not undergo surgery. y
Methods In the Netherlands, all new cancer diagnoses are collected in the National Cancer Registry,
based on data from the central pathology database and the ICD‐9 (international
classification of disease‐9) codes as registered by the hospital. Along with the cancer
diagnosis, patient and tumour characteristics are recorded, as well as the primary cancer
treatment. Using this national database, we examined treatment choices for all patients
newly diagnosed with resectable breast cancer over a period of 10 years (1995‐2005).
Resectable breast cancer was defined as stage T1‐3N0‐2M0. Primary cancer treatment was
dichotomized as surgery vs. no surgery, irrespective of (neo)adjuvant or alternative cancer
41

Chapter 3
treatment. For each incidence year and per five‐year age group, the percentage of
patients receiving surgery was calculated.
To ascertain clinical outcome after omission of surgery for elderly patients with resectable
breast cancer, we examined a regional cohort of such patients in greater detail. All
patients over the age of 75 years, who were diagnosed with a resectable primary breast
cancer and not receiving primary surgery at five different centres in the Netherlands
(Leiden University Medical Centre, Leiden; Haga Hospital, The Hague; Medical Centre
Alkmaar, Alkmaar; Rijnland Hospital, Leiderdorp; and Reinier de Graaf Hospital, Delft)
between 1990 and 2005 were included. For these patients, the following data were
collected from their medical charts: date of birth, date of diagnosis, prior medical history,
tumour stage, and the oestrogen and progesterone receptor status. The human epidermal
growth factor receptor 2 (Her2) was not available in the Netherlands until 2003 and was
therefore not included. Comorbidity burden was assessed using the Charlson comorbidity
index.11 In addition, data on the primary treatment and the reason for omission of surgery
were also collected. Date and cause of death were obtained from the national database at Statistics
Netherlands, based on death certificate data. In the Netherlands, when a patient has died,
it is mandatory that a physician fills out a death certificate including date of death and the
primary cause of death, as well as a maximum of three underlying diseases or secondary
causes of death. Based on primary cause of death as registered on the death certificate,
deceased patients were classified as death due to breast cancer or due to other causes.
Statistical analysis Stata version 11.0 was used for all analyses. For the assessment of national time‐trends,
three‐year moving means were calculated; changes over time were assessed using a
logistic regression analysis. To examine differences in clinical parameters between those
patients that died of breast cancer and those that died of other causes, we used the chi‐
square test. For cancer‐specific survival, breast cancer as primary cause of death was
counted as an event. A univariate and multivariable Cox regression analysis was
performed to assess which of the following baseline characteristics were associated with
breast cancer specific survival: time period (1990‐1999 vs. 2000‐2005), age, T‐stage, lymph
node status, comorbidity using the Charlson score, hormone receptor status and
prescription of endocrine treatment. For each multivariable model, the Cox proportional
hazards assumption was tested. Factors with a p‐value <0.10 in the univariate analysis
were included in the multivariable analysis, as were clinically relevant factors. Kaplan
Meier survival plots, with a log‐rank analysis, were used to determine differences in
survival stratified by cause of death. Relative mortality was calculated as the number of
observed deaths divided by the number of expected deaths based on the corresponding
42

Omission of breast cancer surgery in the elderly
(sex, age, year) general population, based on data from Statistics Netherlands.1 For all
nalyses, a p‐value p <0.05 was considered statistically significant. a
Results Trends over time Between 1995 and 2005, 108,651 patients were newly diagnosed with a resectable breast
cancer in the Netherlands. Of these, 95.6% received primary surgical treatment: the
proportion of patients was 98.7% for those aged 75 years and under, but decreased in
older patients, reaching only 48.9% for those aged 90 years and older (p<0.001). Figure 1
shows the trends over time per age group. For patients aged 75 years or less, the
proportion of patients undergoing surgery remained stable at around 99%. For patients
aged 75 to 79 years, these was a trend towards decrease (98.4% in 1995 to 95.6% in 2005,
p=0.08) while for patients aged 80 years and older this decrease was significant,
particularly in the last five years (p=0.001, Figure 1).
Figure 1: National time‐trends in surgical treatment for resectable breast cancer per age‐group
*For age groups marked with an asterisk, p‐value for change of time was <0.05.
43

Chapter 3
Table 1: Baseline characteristics
Characteristic n %
Period 1990‐1995 1996‐2000 2001‐2005
38 55 94
20 29 50
Age (median + range) 85.9 (75‐97.7)
Charlson 0 1 2 3 4+ Missing
39 43 28 19 16 42
21 23 15 10 9 23
Stage
T1 T2 T3 Unknown
19 44 8 29
19 44 8 29
Lymph node status Negative Positive Unknown
91 24 72
49 13 39
Oestrogen receptor status
Positive Negative Unknown
87 7 93
29 4 50
Progesterone receptor status Positive* Negative Unknown
50 16 121
27 9 65
*All progesterone receptor positive tumours were also oestrogen receptor positive.
Clinical characteristics of older patients not receiving surgery Between 1990 and 2005, 187 patients with resectable breast cancer and not receiving
surgery were identified at the five participating centres; baseline characteristics of these
patients can be found in Table 1. Median age was 85.9 years (range75.0‐97.7). The median
Charlson comorbidity index score was 1 (range 0‐7) and 18 patients had a score of 3 or
more (12%); data on comorbidity were not available for 33 patients. Tumour stage was T1
in 35 patients (16%), T2 in 83 (44%), T3 in 15 (8%) and unknown in 54 (29%). Lymph node
status was negative in 91 patients (49%), positive in 24 patients (13%) and not determined
in 72 patients (39%). All patients were registered as having no metastases. Oestrogen
receptor (ER) status was known in 94 patients (50%) while progesterone receptor (PR)
status was available for 66 patients (35%). The number of patients with unknown receptor
status was approximately 70% until 2000 (1990‐1995 71%, 1996‐2000 73%) but decreased
to 28% between 2001 and 2005. Of patients with a known receptor status, 93% had a
positive ER and/or PR status.
Over half of included patients were diagnosed between 2001 and 2005. Median age
increased in the course of the study period (1990‐1995 83.6 years, 1996‐2000 85.9 years,
2001‐2005 86.4 years, p=0.02) as did the mean Charlson comorbidity index (1990‐1995 0,
1996‐2000 0.5, 2001‐2005 0.9, p=0.02).
44

Omission of breast cancer surgery in the elderly
Figure 2: Kaplan Meier survival curve for (A) observed all‐cause survival compared to expected survival and (B) breast‐cancer related mortality compared to all other causes of death
A.
B.
45

Chapter 3
Treatment For 59 patients (32%), the reason for omitting surgery was stated to be patient's choice.
Other reasons mentioned were age (8 patients, 4%), comorbidity (11 patients, 6%) and
overall health status (10 patients, 5%). For the remaining patients (68%), the reason for
omission of surgery could not be retrieved. The proportion of patients for which omission
of surgery was done at patient’s request did not change over time (p=0.72).
Of the 169 patients for which data on treatment were available, 156 (92%) received
endocrine therapy and 13 (8%) did not receive any treatment. All patients with hormone
receptor positive disease received endocrine treatment, as did 43% of patients with
receptor negative disease and 89% of those with unknown receptor status. The use of
endocrine treatment did not change in the course of the study period (p=0.87). No
patients received radiotherapy or chemotherapy as primary treatment. Seven patients
(4%) required secondary surgical intervention due to disease progression (median time to
surgery 1 year); two of these patients had hormone‐receptor negative disease. Of note,
ne patient died during surgery due to a cardiac arrest. o
Outcome Patients were followed until December 31st 2010. At the end of follow‐up, 178 patients
had died (95.2%); for three patients, survival status was unknown. Median time to death
was 2.3 years (range 0.2‐10.7 years, Figure 2a). Observed survival was significantly lower
than the expected survival based on the matched general population, with a relative
mortality ratio of 2.3 (p<0.001, Figure 2a).
Breast cancer was the primary cause of death for 60 of the 178 patients that died (34%,
Table 2); for 32 of these, breast cancer was the only registered cause of death without
additional contributing diseases. Cardiac disease was the most frequent non‐malignant
cause of death (36 patients, 20%), followed by dementia (17 patients, 10%), pulmonary
disease (13 patients, 7%) and cerebrovascular disease (10 patients, 6%). Ten patients died
of another type of cancer (6%). In addition, breast cancer was stated to be an underlying
cause of death for 37 patients (21%) whose primary cause of death was not breast cancer
(Table 2). For the remaining 81 patients (45%), breast cancer was not mentioned on the
death certificate. Survival did not differ between patients dying of breast cancer vs. those
dying of all other causes (p=0.9, Figure 2b).
Table 3 shows the multivariable analysis for the breast cancer‐specific mortality. Positive
and unknown lymph node status were both significantly associated with mortality (hazard
ratio 3.1 (95% confidence interval (CI) 1.3‐7.1,) and 2.0 (95%CI 1.0‐4.0) respectively,
p=0.02). Increasing comorbidity demonstrated a trend towards a significant association
(p=0.1), as did the time period (p=0.1), with increased hazard of dying of breast cancer in
later years.
46

Omission of breast cancer surgery in the elderly
Table 2. Primary causes of death and underlying diseases in breast cancer patients not receiving surgery
Primary cause of death Relevant underlying disease
Breast cancer
60 (34%) None Cardiovascular disease Dementia Other
32 (53%) 8 (13%) 9 (15%) 11 (18%)
Non‐breast cancer cause of death Cardiac disease (Cerebro)vascular Dementia Pulmonary disease Second malignancy Other
118 (66%) 36 (20%) 10 (6%) 17 (10%) 13 (7%) 10 (6%) 32 (18%)
Breast cancer 37 (31%)
Table 3: Multivariable model for breast cancer‐specific survival
Variable Univariate Hazard ratio p‐value
Multivariable Hazard ratio p‐value
Age Continuous 1.0 (0.9‐1.0) 0.8 1.0 (0.9‐1.0) 0.6
Stage T1 T2 T3 Unknown
Reference 0.7 (0.3‐1.4) 1.3 (0.5‐3.4) 0.8 (0.4‐1.7)
0.5 Reference 0.8 (0.3‐1.7) 0.9 (0.3‐2.4) 1.1 (0.5‐2.8)
0.7
Lymph nodes Negative Positive Unknown
Reference 3.1 (1.5‐6.6) 1.6 (0.9‐2.9)
0.01 Reference 3.1 (1.3‐7.1) 2.0 (1.0‐4.0)
0.02
Charlson 0 1 2 3+
Reference 1.9 (1.0‐3.7) 1.0 (0.4‐2.2) 0.7 (0.3‐1.6)
0.08 Reference 1.7 (0.9‐3.3) 1.1 (0.4‐2.4) 0.6 (0.2‐1.3)
0.1
Period 1990‐1999 2000‐2008
Reference 1.8 (1.0‐3.1)
0.03 Reference 1.6 (0.9‐2.8)
0.1
Oestrogen receptor Positive Negative Unknown
Reference 1.0 (0.3‐3.4) 0.9 (0.5‐1.5)
0.8
Endocrine treatment Yes No Unknown
Reference 1.0 (0.3‐2.7) 1.7 (0.7‐4.3)
0.5
Factors with p<0.1 and clinically relevant factors (age and stage) were entered in the multivariable model.
47

Chapter 3
Discussion This study addresses the incidence and effects of omission of surgery in patients aged 75
years and older with resectable breast cancer. We found that the proportion of these
patients for whom surgery is omitted has increased significantly in the past decade,
particularly in those aged 80 years and older. Data from the regional cohort of 187
patients show that omission of surgery was frequently at patient’s request (32%). When
surgery is omitted, primary endocrine therapy (PET) is generally the alternative of choice
(92% of patients). Median survival was 2.3 years, significantly worse than expected when
compared to an age‐ and gender‐matched cohort of the general population (relative
mortality ratio 2.3). One‐third of patients died of breast cancer, while breast cancer was
not clinically relevant at the time of death in 45%.
This study confirms the findings of our prior single‐centre study that surgery is increasingly
omitted for elderly breast cancer patients.10 Several factors could explain this finding. On
the one hand, therapeutic choices of breast cancer specialists may have changed, based
on clinical trials on primary endocrine treatment for resectable breast cancer in patients
unfit or unwilling to undergo surgery.12 Another explanation could be an alteration in
referral patterns. Not all patients with suspected breast cancer are referred to a breast
cancer clinic, for instance due to significant comorbidity or because the patient and/or
family prefer an expectative approach.13 However, in the past decade, public awareness
on the relevance of breast cancer has increased, as has the general practitioners’
awareness of alternatives to surgical treatment. This could mean that the decrease in the
number of patients undergoing surgery is due to an increased referral of frail patients who
are unsuitable or unwilling to receive surgery for diagnosis and possible hormone therapy.
A third option is a change in patient preferences over time; however, although omission of
surgery was at patient’s request for one‐third of patients in our cohort, this proportion did
not increase during the study period.
The question rises whether omission of surgery for an elderly patient with breast cancer is
justified. Prior studies have demonstrated that concurrent diseases will have a greater
impact on the overall survival and quality of life of older breast cancer patients than the
cancer itself.14‐18 Therefore, withholding treatment in the presence of serious comorbidity
that significantly limits the remaining life‐expectancy seems legitimate, provided that
adequate follow‐up is in place to allow timely intervention if complications do occur. It
must be kept in mind, however, that estimation of life‐expectancy is notoriously difficult,19
particularly in the very elderly who can experience a persistent level of disability and
frailty over an extended period of time, before succumbing to a minor illness due to a lack
of physical reserves.20
In our cohort, it appears that the availability of primary endocrine treatment (PET) may
have facilitated the decision to omit surgery, as 92% of patients received this alternative.
48

Omission of breast cancer surgery in the elderly
However, although studies in unselected elderly patients with resectable breast cancer
have demonstrated that the survival benefit of surgery compared to PET does not become
clinically relevant until three years after diagnosis,21 PET has been proven to result in a
significantly decreased locoregional control compared to primary surgery.12 This could
seriously affect a patient’s quality of life and for many older patients, quality of life and
functional independence are considered to be of greater importance than survival.22,23 In
addition, although increasing age, poor general health and comorbidity – which are
frequently stated as reasons for choosing PET – do affect the ability of a patient to tolerate
surgery,14,15,24 these factors will also increase the risk of side‐effects of endocrine
treatment.25‐27 These include constitutional symptoms such as fatigue, dizziness, nausea,
headaches, muscle weakness and pains, as well as an increased risk of thrombo‐embolic
events.25‐27 Furthermore, exposure to these adverse effects will be much longer in case of
PET. These factors suggest that although endocrine treatment may appear an easy, safe
and effective alternative to surgery, the potential for a negative impact on the quality of
the patient’s remaining lifetime should not be underestimated.
Patient’s refusal of treatment was another important reason for omission of surgery in our
cohort. Older patients tend to rely much more on their physician’s opinion than younger
patients and generally prefer a more passive role when it comes to treatment
decisions.28,29 As a result, part of what is stated to be the patient’s preference could in fact
be a reflection of the physician’s preference. In addition, the decision that a patient makes
will be greatly influenced by the information that he or she has been offered by the cancer
specialist,30 particularly in case of older patients who are less likely to access alternative
sources of information,29 such as the internet.
The relatively poor survival of the patients in our regional cohort is most likely due to the
fact that this represents a selected cohort of unfit patients, with a poor a priori prognosis
irrespective of the breast cancer. However, the patient charts generally did not provide an
extensive description of the patient’s health status and rarely included data on functional
limitations or the presence of geriatric syndromes that can significantly diminish overall
prognosis.31 Therefore, we were unable to quantify the fitness of the patients in our
cohort. Another factor contributing to the poor survival rate could be a possible
underestimated or incomplete staging of disease. This is suggested by the fact that 17 of
the 60 patients (28%) that died of breast cancer died within the first year (Figure 2b),
which is very unlikely in genuine early stage disease. Finally, it is possible that breast‐
cancer related therapeutic decision affected survival, but in an observational cohort study
with limited clinical data, it is not possible to provide an accurate estimate of this effect.
This study has several weaknesses. Due to the retrospective nature of this study, we could
only draw on what was recorded in the patient’s charts, resulting in missing data. In
addition, we were not always able to retrieve the medical records, particularly for patients
49

Chapter 3
diagnosed in the earliest years of this study. Furthermore, patients were frequently
referred back to their primary care physician for follow‐up and thus, we had to rely on the
death certificate to ascertain the clinical relevance of the breast cancer at the time of
death. In addition, establishing the cause of death in elderly patients with multiple
interacting comorbidities can be susceptible to errors.32,33 Despite these issues, we believe
that this real‐life patient cohort provides an interesting and relevant supplement to
linical trial data. c
In conclusion, omission of surgery for elderly patients with resectable breast cancer and
the use of primary endocrine therapy have increased significantly over the past decade.
Breast cancer was not considered clinically relevant at the time of death for a significant
number of patients, suggesting that PET was successful in suppressing the cancer for the
patient’s remaining lifetime. However, although PET may appear an easy, safe and
effective alternative to surgery, the longer term negative impact on disease control and
quality of life should not be underestimated. For the very frail, it may be preferable and
legitimate to withhold treatment altogether. As clinical trials addressing this issue in such
a vulnerable patient population are unfeasible, prospective observational cohort studies
incorporating a broad scope of patient characteristics including frailty data and geriatric
syndromes, may aid in identifying which baseline factors could guide decision making
garding the initiation or withholding of the available treatment options. re
Acknowledgements: the authors would like to thank the Netherlands Cancer Registry, as
well as the Zoleon foundation and Statistics Netherlands.
50

Omission of breast cancer surgery in the elderly
References 1. www.cbs.nl. 3‐2‐2012. 2. www.cijfersoverkanker.nl. 2‐3‐2012. 3. Alberg AJ, Singh S. Epidemiology of breast cancer in older women: implications for future healthcare.
Drugs Aging 2001;18:761‐772. 4. Hutchins LF, Unger JM, Crowley JJ et al. Underrepresentation of patients 65 years of age or older in
cancer‐treatment trials. N Engl J Med 1999;341:2061‐2067. 5. Peto R, Davies C, Godwin J et al. Comparisons between different polychemotherapy regimens for early
breast cancer: meta‐analyses of long‐term outcome among 100,000 women in 123 randomised trials. Lancet 2012;379:432‐444.
6. Hamaker ME, Schreurs WH, Uppelschoten JM, Smorenburg CH. Breast cancer in the elderly: retrospective study on diagnosis and treatment according to national guidelines. Breast J 2009;15:26‐33.
7. Bastiaannet E, Liefers GJ, de Craen AJ et al. Breast cancer in elderly compared to younger patients in the Netherlands: stage at diagnosis, treatment and survival in 127,805 unselected patients. Breast Cancer Res Treat 2010;124:801‐807.
8. Ring A, Sestak I, Baum M et al. Influence of comorbidities and age on risk of death without recurrence: a retrospective analysis of the Arimidex, Tamoxifen Alone or in Combination trial. J Clin Oncol 2011;29:4266‐4272.
9. Lavelle K, Moran A, Howell A et al. Older women with operable breast cancer are less likely to have surgery. Br J Surg 2007;94:1209‐1215.
10. Hamaker ME, Schreurs WH, van Slooten HJ et al. [Trends in breast cancer treatment in the elderly at a breast cancer outpatient clinic: guidelines followed better]. Ned Tijdschr Geneeskd 2009;153:A562.
11. Charlson ME, Pompei P, Ales KL, Mackenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987;40:373‐383.
12. Hind D, Wyld L, Beverley CB, Reed MW. Surgery versus primary endocrine therapy for operable primary breast cancer in elderly women (70 years plus). Cochrane Database Syst Rev 2006;(1):CD004272.
13. Hamaker ME, Hamelinck VC, van Munster BC et al. Nonreferral of Nursing Home Patients With Suspected Breast Cancer. J Am Med Dir Assoc 2012;13:464‐9.
14. Wildiers H, Kunkler I, Biganzoli L et al. Management of breast cancer in elderly individuals: recommendations of the International Society of Geriatric Oncology. Lancet Oncol 2007; 8:1101‐1115.
15. Wyld L, Reed M. The role of surgery in the management of older women with breast cancer. Eur J Cancer 2007; 43:2253‐2263.
16. Janssen‐Heijnen ML, Maas HA, Houterman S et al. Comorbidity in older surgical cancer patients: influence on patient care and outcome. Eur J Cancer 2007;43:2179‐2193.
17. Satariano WA, Ragland DR. The effect of comorbidity on 3‐year survival of women with primary breast cancer. Ann Intern Med 1994;120:104‐110.
18. Patnaik JL, Byers T, Diguiseppi C et al. The influence of comorbidities on overall survival among older women diagnosed with breast cancer. J Natl Cancer Inst 2011;103:1101‐1111.
19. Christakis NA, Lamont EB. Extent and determinants of error in physicians' prognoses in terminally ill patients: prospective cohort study. West J Med 2000;172:310‐313.
20. Gill TM, Gahbauer EA, Han L, Allore HG. Trajectories of disability in the last year of life. N Engl J Med 2010; 362:1173‐1180.
21. Fennessy M, Bates T, MacRae K et al. Late follow‐up of a randomized trial of surgery plus tamoxifen versus tamoxifen alone in women aged over 70 years with operable breast cancer. Br J Surg 2004;91:699‐704.
22. Yellen SB, Cella DF, Leslie WT. Age and clinical decision making in oncology patients. J Natl Cancer Inst 1994; 86:1766‐1770.
23. Steinhauser KE, Christakis NA, Clipp EC et al. Factors considered important at the end of life by patients, family, physicians, and other care providers. JAMA 2000;284:2476‐2482.
24. Tiret L, Desmonts JM, Hatton F, Vourc'h G. Complications associated with anaesthesia‐‐a prospective survey in France. Can Anaesth Soc J 1986;33:336‐344.
25. Hernandez RK, Sorensen HT, Pedersen L et al. Tamoxifen treatment and risk of deep venous thrombosis and pulmonary embolism: a Danish population‐based cohort study. Cancer 2009;115:4442‐4449.
51

Chapter 3
52
26. Biganzoli L, Wildiers H, Oakman C et al. Management of elderly patients with breast cancer: updated recommendations of the International Society of Geriatric Oncology (SIOG) and European Society of Breast Cancer Specialists (EUSOMA). Lancet Oncol 2012;13:e148‐e160.
27. Aapro M, Monfardini S, Jirillo A, Basso U. Management of primary and advanced breast cancer in older unfit patients (medical treatment). Cancer Treat Rev 2009;35:503‐508.
28. Fallowfield L. Participation of patients in decisions about treatment for cancer. BMJ 2001;323:1144. 29. Pinquart M, Duberstein PR. Information needs and decision‐making processes in older cancer patients. Crit
Rev Oncol Hematol 2004;51:69‐80. 30. Pierce PF. Deciding on breast cancer treatment: a description of decision behavior. Nurs Res 1993;42:22‐
28. 31. Ferrucci L, Guralnik JM, Studenski S et al. Designing randomized, controlled trials aimed at preventing or
delaying functional decline and disability in frail, older persons: a consensus report. J Am Geriatr Soc 2004;52:625‐634.
32. Ederer F, Geisser MS, Mongin SJ et al. Colorectal cancer deaths as determined by expert committee and from death certificate: a comparison. The Minnesota Study. J Clin Epidemiol 1999;52:447‐452.
33. Lu TH, Shih TP, Lee MC et al. Diversity in death certification: a case vignette approach. J Clin Epidemiol 2001;54:1086‐1093.

Chapter 4
Non‐referral of nursing home patients with suspected breast cancer
M.E. Hamaker, V.C. Hamelinck, B.C. van Munster, E. Bastiaannet, C.H. Smorenburg,
W.P. Achterberg, G.J. Liefers, S.E. de Rooij
Journal of the American Medical Directors Association 2012;13:464‐9

Chapter 4
Abstract Introduction: People with suspected breast cancer who are not referred for diagnostic
testing remain unregistered and are not included in cancer statistics. Little is known about
the extent of and motivation for non‐referral of these patients.
Methods: A web‐based survey was sent to all elderly care physicians (ECPs) registered at
the National Association of Elderly Care Physicians and Social Geriatricians in the
Netherlands, inquiring about the number of patients with suspected breast cancer they
encountered and subsequent choices regarding referral.
Results: Surveys were completed by 419 out of 1239 ECPs (34%); 249 of these had
encountered one or more patients with suspected breast cancer in the past year (60%).
Seventy‐four ECPS reported not referring the last patient (33%). Reasons for non‐referral
were end‐stage dementia (57%), patient/family preference (29%) and limited life‐
expectancy (23%). Referral was frequently thought to be too burdensome (13%). For 16%
of non‐referred patients, hormonal treatment was started by the ECP without diagnostic
confirmation of cancer.
Conclusion: In this survey, over 33% of nursing home patients with suspected breast
cancer were not referred for further testing, in particular those with advanced dementia,
limited life‐expectancy and poor functional status. As the combination of dementia and
suspected breast cancer is expected to double in the coming decades, now is the time to
optimize cancer care for these vulnerable patients.
54

Non‐referral of nursing home patients with suspected breast cancer
Introduction Cancer statistics show that in 2009, a total of 13,177 women were diagnosed with breast
cancer in the Netherlands.1 These data are based on the Netherlands Cancer Registry
(NCR),1 a nationwide network which collects histo‐ and cytopathology data from all Dutch
hospitals, supplemented by data from the national hospital discharge databank. After
cancer cases are identified, trained personnel from regional cancer registries gather
additional data on diagnosis, staging and treatment.
As all oncologic treatment in the Netherlands is provided by hospital‐based specialists, the
registry can provide a comprehensive overview of current cancer treatment. It also allows
for a comparison of actual treatment with treatment as recommended by guidelines. For
example, using registry data, studies have demonstrated that older breast cancer patients
are often treated less extensively than their younger counterparts and that they are at risk
for being undertreated.2‐5
In the Netherlands, primary care physicians form an important first link in the cancer
treatment pathway (Figure 1), as they are generally responsible for referral to hospital
specialists – although some alternative routes are possible. For patients residing in nursing
homes, either permanently or temporarily in case of rehabilitation, this tasks falls on
specially trained physicians, called elderly care physicians (ECPs), for whom nursing homes
are the primary place of work.6 This differentiation between primary medical care and
hospital‐based care in the Netherlands, results in an important limitation of the cancer
registry: patients with a clinical suspicion of cancer that are not referred to hospital for
further diagnostic testing will remain unregistered and will not be included in Dutch
cancer statistics.
Surprisingly, little is known about the issue of non‐referral. Studies using Medicare‐data
Figure 1: Global overview of breast cancer care pathway in the Netherlands
55

Chapter 4
in the United States show that little cancer care is claimed for patients living in a nursing
home setting,7 and that Alzheimer patients receive less treatment for breast cancer than
comparable female Medicare beneficiaries,8 but the authors could not determine whether
this was due to less cancer vigilance resulting in missed cancer diagnoses or to omission of
referral for specialised cancer care. Even less is known about the motivation behind non‐
referral or the consequences for the patient.
For this study, we sent a survey to all members of the National Association of Elderly Care
Physicians and Socials Geriatricians, to determine a) the extent of and reasons for non‐
referral of patients suspected of breast cancer by ECP, and b) the motivations behind this
hoice. c
Method We developed a web‐based survey using the SurveyMethods, Inc. software.9 The survey
contained questions relating to the incidence of suspected breast cancer in nursing
homes, whether or not these patients were referred and the motivation behind referral
choices. The content of the survey is depicted in Figure 2. After a concept of this survey
was successfully tested in 19 ECPs, it was subsequently sent to all ECPs registered at
Verenso, the National Association of Elderly Care Physicians and Social Geriatricians in
August 2011. Of the 1525 ECPs active in the Netherlands, 1238 are registered at Verenso;
onsequently 81% of all Dutch ECPs were invited to participate in the survey. c
Statistical analysis To compare differences between referred and non‐referred patients, the SPSS (Statistical
Package for the Social Sciences) version 19.0 was used. The chi‐square test was used for
nominal and ordinal variables. For continuous variables with a normal distribution, the
Student t‐test was used, and for continuous variables with a non‐Gaussian distribution the
ann‐Whitney test. M
Results
Response rate Surveys were completed by 419 of the 1239 ECPs (response rate was 34%, Figure 2).
Characteristics of respondents are listed in Table 1. The median age of respondents was
47 years (range 25‐66 years) and 66% were female. Responses came from all over the
country, covering over 90% of the 90 primary zip code‐areas in the Netherlands. Almost
60% of respondents stated they had encountered at least one patient with suspected
breast cancer in the past year; of these patients, 33% were not referred for further
diagnostic testing (Figure 3).
56

Non‐referral of nursing home patients with suspected breast cancer
Figure 2: Content of survey
Question 1: How old are you?
Question 2: What sex are you? Question 3: What are the four numbers of the zip code where your practice is located? Question 4: How many patients did you care for in the past year?
Question 5: What percentage of these patients is female?
Do you have any additional comments relating to this survey?
IF YES IF NO
IF NONE IF ONE IF MORE THAN ONE
Question 6: In the past year, did you suspect one or more of your patients of having breast cancer?
Question 7: how many of these patients did you refer for further testing and/or treatment?
The following questions concern the last patient you suspected of having breast cancer
Question 8: What was this patient’s age? Question 9: Did you refer this patient for further testing and/or treatment?
Question 10: With whom did you discuss this decision?
Question 10: With whom did you discuss this decision?
Question 11: What were your reasons for referring this patient?
Question 11: What were your reasons for not referring this patient?
Question 12: What treatment did the patient receive?
Question 12: Did you yourself start any anti‐cancer treatment?
Question 13: How is the patient doing now?
Question 13: How is the patient doing now?
Question 14: Have you recently had any patients who you did
Question 14: Have you recently had any patient who you not choose to refer,
and if so, what were your reasons for this?did choose to refer, and if
so, what were your reasons for this?
END OF SURVEY
57

Chapter 4
Referral vs. non‐referral Table 2 lists a comparison of patients that were or were not referred. Patients not referred
were older (median age 86 vs. 82 years, p<0.001), although some non‐referred patients
were as young as 60 years. Over 99% of physicians discussed their decision on referral
with at least one other party: in 54% of cases, it was discussed with the patient, while in
87% a family member was consulted; in 9% it was only discussed with another physician.
Of note, of the patients that were not referred, less than half were personally involved in
making this decision.
The motivations for choosing to refer patients to hospital (Table 3) were primarily the
desire to confirm the diagnosis (28%), the fear of future ulceration or metastases (21%),
good general health and life‐expectancy (19%), and patient’s or family’s preference for
referral (18%). Current or imminent ulceration was stated in 9% of cases, while
maintaining quality of life or optimizing palliative care were stated in 7% and 4%
respectively. For 11%, the main reason for referral was to assess the suitability of primary
hormonal treatment, as the ECP felt that due to cognitive or functional status, the patient
was not a candidate for more invasive treatment.
The primary reason stated for not referring was end‐stage dementia (57%, Table 4). Other
reasons were the preferences of patient and/or family (29%), limited life‐expectancy
(23%), poor functional status or somatic comorbidity (18% and 16%, respectively) and
advanced age in 8%. The expected burden of the hospital visits and subsequent diagnostic
process and treatment for the patient was stated in 13%, particularly for patients with
dvanced dementia. a
Treatment and outcome Of the patients that were referred to hospital, seven were found to have a benign tumour
(5%); 16% received no treatment and 24% received hormonal treatment only. Surgery was
performed in 28% of patients, radiotherapy given to 8% and chemotherapy to one patient.
For 18%, the diagnostic process was still on‐going. In addition, twelve non‐referred
patients (16%) were prescribed primary hormonal treatment by the ECP without
confirmation of breast cancer.
The current health status of referred and non‐referred patients is listed in Table 5. Thirty‐
four patients were lost to follow‐up. Three referred patients died of breast cancer or
breast cancer treatment, and three patients suffered from locally advanced or metastatic
disease (two referred and one non‐referred patient). Forty‐four patients had died of
causes other than breast cancer (17%).
58

Non‐referral of nursing home patients with suspected breast cancer
Figure 3: Flow chart of response rate and referrals
Number of survey returned: n=419/1238 (34%)
One or more patient with suspected breast cancer No patients with suspected breast cancer n=249 (59.4%) n=170 (40.6%)
Table 1: Characteristics of respondents
Elderly care physicians
Response rate 419/1238 (34%) Median age of respondents (range) 47 years (25‐66) % female of respondents 66.1% % with ≥1 patients suspected of breast cancer 59.4% Number of patients suspected of breast cancer in past year 0 1 2 3 4 5 more than 5
170 140 81 20 4 3 1
% of patients referred to hospital 67.1%
Table 2: Comparison of patients that were and were not referred
Patients referred (n=151) Patients not referred (n=74) p=
Median age of patients (range) 82 (45‐99) years 86 (60‐102) years <0.001
(non‐) Referral discussed with* No one
Patient Family member Colleague Clinical geriatrician Oncologist Surgeon Radiotherapist Others Nursing staff
0%*61%85%14%4%
13%29%3%7%6%
1%* 41% 91% 23% 1% 5% 5% 0%
12% 7%
ns <0.001 <0.001 <0.001 0.02
<0.001 <0.001 0.01
0.002
* n=146 of these responses originated from question 9 and n=17 from question 14
Last patient referredn=151 (67.1%)
Last patient not referred Missingn=74 (32.9%) n=24
59

Chapter 4
Table 3: Reasons for referral
Reason Frequency
(out of 121 responses)* %
Dementia/cognitive function 69 57 Preference of patient and/or family 35 29 Limited life expectancy 28 23 Functional status 22 18 Somatic comorbidity 19 16 Burden of referral too high for specific patient 16 13 Tumour characteristics 10 9 Advanced age 10 8 Lack of subjective burden of tumour 6 5 No expected benefit of referral for patient’s quality of life 3 2 * n=146 of these responses originated from question 9 and n=17 from question 14
Table 4: Reasons for non‐referral
Reason
Frequency (out of 121 responses)*
%
Dementia/cognitive function 69 57 Preference of patient and/or family 35 29 Limited life expectancy 28 23 Functional status 22 18 Somatic comorbidity 19 16 Burden of referral too high for specific patient 16 13 Tumour characteristics 10 9 Advanced age 10 8 Lack of subjective burden of tumour 6 5 No expected benefit of referral for patient’s quality of life 3 2 * n=80 of these responses originated from question 9 and n=41 from question 14
Table 5: Current status of patients
Referred patients n=151
Non‐referred patients n=74
Lost to follow‐up 32 21% 2 3% Stable/asymptomatic disease or disease‐free
97 64% 46 62%
Locally advanced/metastatic disease 2 1% 1 1% Died of other causes 19 13% 25 34% Died of breast cancer or breast cancer treatment
3 2% 0 0%
60

Non‐referral of nursing home patients with suspected breast cancer
Discussion We found that 60% of the responding ECPs had encountered one or more patients whom
they suspected of having breast cancer in the past year, and 33% of these patients were
not referred. The primary reasons for non‐referral were dementia, poor functional status,
comorbid diseases and limited life‐expectancy, as well as the expected burden of a visit to
a clinic or the subsequent treatment. Of referred patients, only 28% received surgical
treatment, while 40% received no oncologic treatment or primary hormonal therapy only.
To our knowledge, this is the first study to address the issue of non‐referral of nursing
home residents with suspected breast cancer. We believe it provides valuable information
on a vulnerable population that has thus far remained outside the scope of cancer
research and national cancer statistics.
This study has some weaknesses. First of all, the response rate was 34%. This is an issue
frequently encountered in survey‐based studies.10 For this survey, it is not unlikely that
those ECPs who had recently dealt with the issue of suspected breast cancer were more
prone to respond to the survey than those who had not. This makes it difficult to know to
what extent the incidence of suspected breast cancer in nursing home patients can be
extrapolated from these results. Furthermore, as this survey requires ECPs to recollect
their last patient, data may be somewhat influenced by recall bias. Another limitation is
that this study was done in a single country only; as the organisation of care and of cancer
registries will differ from country to country, it remains unclear whether our findings can
be extrapolated to other countries.
This study highlights an important limitation of the current cancer registration in the
Netherlands and consequently of cancer statistics, particularly for the very elderly where
non‐referral is likely to be more prevalent. Although there is a mandatory registration of
confirmed cancer cases, there is no obligation to report suspected but unconfirmed cases;
what is more, a procedure for reporting such cases is currently lacking. As the prevalence
of dementia is expected to double in the coming decades,11 and the proportion of newly
diagnosed patients with breast cancer aged 85 years and over will rise from 9% to 17% by
2030,12 the combination of patients with advanced dementia and suspected breast cancer
will also increase greatly. If no procedure is developed for their registration, the number
of very elderly or frail cancer patients that remain unregistered is likely to increase,
making the cancer statistics for these patients increasingly unreliable. Addressing this
issue in the registry will be challenging, however, as suspected cancer is not confirmed
cancer, and these additional patients cannot automatically be added to what is currently
recorded.
The increasing number of patients suffering from both dementia and suspected breast
cancer asks for a careful evaluation of the current care process. Although the diagnostic
process for breast cancer is not very invasive, and breast cancer surgery has a low risk of
61

Chapter 4
perioperative complications,13 for a patient with advanced dementia, even the process of
going to an out‐patient clinic or undergoing physical examination can be of great burden.
However, this needs to be weighed against the risks of leaving a suspected malignancy
unaddressed. Uncontrolled breast cancer, particularly when ulceration occurs, may have
serious impact on a patient’s comfort and quality of life.
Of course, as this study demonstrates, many patients who were thought to be too frail to
refer for further testing have a life‐expectancy that is limited, leaving little time to suffer
the potential consequences of untreated breast cancer or the potential benefits of
treatment. Watchful waiting with regular physical examination to determine rate of local
progression and symptomatic treatment of cancer‐related complaints such as pain, can be
a useful strategy in such patients. However, estimating life expectancy is not always
easy,14 particularly in those with advanced dementia who can experience a persistent level
of severe disability and frailty over an extended period of time, before succumbing to a
minor illness due to lack of physical reserves.15 Therefore, if the extend of remaining life‐
years is not clear, and there is a desire to start oncologic treatment, but burden of a visit
to clinic is considered too great, what options are left?
One possibility is to start treatment with endocrine therapy without actual confirmation of
breast cancer diagnosis or assessing hormone receptor status. In our study, this option
was chosen for 16% of patients that were not referred. As over 75% of patients aged 80
years or older have oestrogen receptor positive disease,16 and partial remission and loco‐
regional control can often be attained17 – albeit temporarily – this is not an unreasonable
option. However, there will be a proportion of patients who either have hormone
receptor negative disease, or who have no breast cancer at all, and therefore will not
profit from treatment but will be exposed to side‐ effects of treatment. These side‐effects
are limited, but even in fit subjects have been shown to affect their feeling of well‐being,
particularly in the first months of treatment.18,19 For example, all types of hormonal
treatment can cause hot flushes, dizziness, gastro‐intestinal complaints such as nausea
and anorexia, as well as psychological effects such as depression or agitation.20
Furthermore, the very frail are more likely to experience adverse effects,21 and what is
seen as a minor side‐effect for a fit subject can have great impact on the quality of life,
functional status and behaviour of the very frail.
Another option is to alter the diagnostic testing process in a way that minimizes the
burden for these vulnerable patients. For example, one ECP explained that the pathologist
came to their nursing home, to take biopsies of palpable tumours, offering the possibility
of confirming the diagnosis and assessing receptor status. Although for some patients
even this may be too burdensome, for many, a consultation in their own care setting – by
a pathologist, surgeon or oncologist – may be a solution.
62

Non‐referral of nursing home patients with suspected breast cancer
The results of this study can form a starting point for a range of future clinical studies. First
of all, as this is the first study on non‐referral of nursing home patients, from a single
country, similar studies should be done in other countries to confirm our findings. In
addition, a more in‐depth case review of non‐referred patients may provide additional
information to supplement the survey data. Second, studies could look at non‐referral of
other patient groups, such as frail elderly patients living at home, or nursing home
residents suspected of having other types of cancer. Third, studies on guideline adherence
– particularly in older patients – should take the possibility of non‐referral of patients into
account and address in what way this could influence the outcome of their results.
However, more importantly, studies should focus on the potential of non‐oncologic non‐
pharmacologic interventions to optimize quality of life and minimize cancer‐related
symptom burden, and on developing new treatment pathways, such as a specialist
consultation in the patient’s place of residence, suitable for these vulnerable patients.
Possibly, the option of initiating endocrine treatment without histological confirmation of
breast cancer – as is sometimes chosen already – could be evaluated in a placebo‐
controlled study weighing the benefit in disease control against the potential harmfulness
f side‐effects. o
In conclusion, our survey shows that suspicion of breast cancer is not uncommon in a
nursing home setting. Over 33% of patients were not referred for further testing, in
particular those with advanced dementia and poor functional status, because the burden
of referral is expected to be greater than the benefit for the patient. With the expected
increase in the occurrence of both dementia and breast cancer, now is the time to start
thinking about how best to provide them with the care they need in a way that is suitable
their overall condition. to
Acknowledgements: the authors would like to thank all participating elderly care
physicians, and in particular the chair of the Dutch organisation of the Elderly Care
Physicians, Mieke Draaijer and the director, Franz Roos, for their willingness to collaborate
with us.
63

Chapter 4
64
References 1. www.cijfersoverkanker.nl 2. Hamaker ME, Schreurs WH, Slooten HJ van et al. Trends in breast cancer treatment in the elderly at a
breast cancer outpatient clinic: guidelines followed better. Ned Tijdsch Geneeskd 2009;153:A562. 3. Hamaker ME, Schreurs WH, Uppelschoten JM, Smorenburg CH. Breast cancer in the elderly: retrospective
study on diagnosis and treatment according to national guidelines. Breast J 2009;15:26‐33. 4. Bastiaannet E, Liefers GJ, Craen AJM de et al. Breast cancer in elderly compared to younger patients in the
Netherlands: stage at diagnosis, treatment and survival in 127,805 unselected patients. Breast Cancer Res Treat 2010;124:801–807.
5. Bastiaannet E, Portielje JEA, Velde JH van de et al. Lack of survival gain for elderly women with breast cancer. Oncologist 2011;16:415‐23.
6. Koopmans RT, Lavrijsen JC, Hoek JF et al. Dutch elderly care physician: a new generation of nursing home physician specialists. J Am Geriatr Soc 2010;58:1807‐9.
7. Bradley CJ, Clement JP, Lin C. Absence of cancer diagnosis and treatment in elderly Medicaid‐insured nursing home residents. J Natl Cancer Inst 2008;100:21‐31.
8. Sheinfeld Gorin S, Heck JE, Albert S, Hershman D. Treatment for breast cancer in patients with Alzheimer’s disease. J Am Geriatr Soc 2005;53:1897‐1904.
9. www.surveymethods.com 10. Dillman DA. Internet, mail, and mixed‐mode surveys: the tailored design method. Mail and internet
surveys. Hoboken, N.J.: Wiley & Sons; 2009. 1941. 11. www.alzheimer‐nederland.nl 12. Hayat MJ, Howlader N, Reichman ME, Edwards BK. Cancer statistics, trends and multiple primary cancer
analysis from the surveillance, epidemiology and end results (SEER) program. Oncologist 2007;12:20‐37. 13. Audisio RA, Bozzetti F, Gennari F et al. The surgical management of elderly cancer patients:
recommendations of the SIOG surgical task force. Eur J Cancer 2004;40:926‐38. 14. Christakis NA, Lamont EB. Extent and determinants of error in doctors’ prognoses in terminally ill patients:
prospective cohort study. BMJ 2000;320:469‐73. 15. Gill TM, Gahbauer EA, Han L, Allore HG. Trajectories of disability in the last year of life. N Engl J Med 2010;
362:1173‐80. 16. Diab SG, Elledge RM, Clark GM. Tumor characteristics and clinical outcome of elderly women with breast
cancer. J Natl Cancer Inst 2000;92:550‐617. 17. Hind D, Wyld L, Beverley C, Reed MW. Surgery versus primary endocrine therapy for operable primary
breast cancer in elderly women (70 years plus). The Cochrane Library: DOI: 10.1002/14651858.CD004272.pub2.
18. Cella D, Fallowfield L, Baker P et al on behalf of the ATAC trialists’ group. Quality of life of postmenopausal women in the ATAC trial after completion of 5 years’ adjuvant treatment for early breast cancer. Breast Cancer Res Treat 2006;100:273‐84.
19. Fallowfield L, Cella D, Cuzick J et al. Quality of life of postmenopausal women in the arimidex, tamoxifen, alone or in combination adjuvant breast cancer trial. J Clin Oncol 2004;22:4261‐71.
20. www.fk.cvz.nl 21. Routledge PA, O’Mahoney MS, Woodhouse KW. Adverse drug reactions in elderly patient. Br J Clin
Pharmacol 2004;52:121‐6.

Chapter 5
Slow accrual of elderly patients with metastatic breast cancer in the Dutch
multicentre OMEGA study
M.E. Hamaker, C. Seynaeve, J.W.R. Nortier, M. Wymenga, E. Maartense, E. Boven, A.E. van Leeuwen‐Stok, S.E. de Rooij, B.C. van Munster, C.H. Smorenburg
[Submitted]

Chapter 5
Abstract Background: In a Dutch multicentre study, elderly (65+ year) metastatic breast cancer
patients, eligible for first‐line chemotherapy, were randomised between two types of
single‐agent chemotherapy. As accrual was slow, with 78 randomised patients between
April 2007 and September 2011, we explored potential barriers in the accrual process and
their consequences for characteristics of included patients.
Methods: We sent surveys on the reasons for non‐inclusion to all coordinating
investigators. We also examined inclusion in a concurrent, non‐elderly breast cancer study
of the trialists’ group and analysed baseline geriatric characteristics of included patients.
Results: Investigators from fifteen participating centres returned the survey. Most
commonly reported barriers to inclusion were: patient’s refusal of chemotherapy (n=8) or
of randomisation (n=9), impaired cognition (n=3) and insufficient cardiac function (n=2).
Oncologists’ preference for combination regimens over single‐agent chemotherapy was
reported twice. Twenty‐eight potentially eligible patients, aged 65 to 71 years, were
included in a concurrent, study investigating combination chemotherapy in fit non‐elderly
patients with metastatic breast cancer. However, baseline characteristics of the included
patients showed that the OMEGA study succeeded in including frail and older patients,
with a performance status of 2 in 22% of patients and 54% of patients aged 75 years or
older.
Conclusion: Accrual in this study was mainly hampered by patient’s refusal or preference
for a particular type of treatment, and an overall condition considered as too fit or too
frail for inclusion. Future trials in elderly metastatic breast cancer patients should focus on
non‐restrictive inclusion criteria as well as on education of physicians and elderly patients
on the advantages of trial participation.
66

Slow accrual in the OMEGA study
Introduction In the Netherlands, breast cancer is diagnosed in over 13,000 women each year, of which
53% is aged 65 or older. It is the most frequently diagnosed cancer in women and its
incidence increases with age. Due to increasing life expectancy and ageing of the
population, the number of elderly patients with breast cancer will increase substantially
over the next decades. It is expected that by the year 2035, 60% of all new breast cancer
patients will be 70 years or older.1
Breast cancer treatment in older patients is complicated by the lack of elderly‐specific
evidence on which to base treatment decisions, especially for chemotherapy. Older
patients and those with comorbidity have historically been excluded from clinical trials; for
example, in a study published in 1999, only 9% of patients in breast cancer trials was aged
65 years and over, while at that time 49% of breast cancer patients in the United States
fell into this age group.1 Although these findings have led researchers to develop trials
without upper age limits, more recent publications still report an underrepresentation of
elderly patients and underline the need for trials focusing on this patient population.2
The Dutch Breast Cancer Trialists Group (BOOG) has performed a multicentre, randomised
clinical trial regarding the tolerance and efficacy of first‐line, single‐agent palliative
chemotherapy for metastatic breast cancer patients aged 65 years or older, with
incorporation of a comprehensive geriatric assessment, the OMEGA trial (trial number
NTR897, BOOG 2006‐02). This study was specifically designed to allow inclusion of frail,
elderly patients and those with comorbidity: selection criteria were limited to acceptable
bone marrow, kidney and liver function, an European Cooperative Oncology Group (ECOG)
performance status ≤ 2 (or ≤ 3 if limitations are caused by pain or a pre‐existent disabling
disease), a left ventricular ejection fraction above the lower limit of normal, and the
absence of clinically relevant cardiac disease or a previous malignancy in the past five
years. Patients were randomised between pegylated liposomal doxorubicin (Caelyx®)
administered intravenously once every four weeks for a maximum of six cycles, or
capecitabine, given orally on days 1 to 4, every three weeks for a maximum of eight cycles.
In addition to standard analyses of toxicity and efficacy, this study performed an
evaluation of quality of life and a comprehensive geriatric assessment3‐7 at baseline,
twelve weeks, end‐of‐treatment (24 weeks if all cycles were completed) and after twelve
months.
Despite a total of 25 participating Dutch institutions, accrual for the OMEGA study was
slow with only 78 patients randomised between April 2007 and September 2011 (end of
study); this is just over half of the intended 154 patients based on power calculations and
a pre‐study audit on potentially eligible patients (Figure 1). To determine the implications
of this difficult accrual process for future clinical studies in frail elderly cancer patients, we
explored potentials barriers in the accrual process.
67

Chapter 5
Figure 1: Expected versus actual accrual
Methods In the summer of 2008, a survey was sent to all coordinating investigators of the
participating centres (19 at that time, six centres joined this study after 2008) to assess
potential barriers to accrual (Appendix 1), focusing on study‐related barriers such as in‐
and exclusion criteria of the study protocol, patient‐related factors such as patient’s
refusal to participate or preference for a specific type of treatment, and physician‐related
factors like the preference for a particular study arm and their attitude towards treatment
with chemotherapy in older patients.
To assess if any of these factors ultimately influenced the characteristics of enrolled
patients or only affected the number of patients, we analysed the baseline data of the 78
randomised patients. These data were collected by the research nurses, and included:
social status and living situation, comorbidity as assessed by the Charlson comorbidity
68

Slow accrual in the OMEGA study
index (CCI),3 Eastern Cooperative Oncology Group performance status (PS), functional
status assessed by the Lawton & Brody scale for instrumental activities of daily living
(IADL),4 polypharmacy (defined as 5 or more types of medication), undernutrition (defined
by a BMI <20 kg/m2), cognitive dysfunction assessed by the mini‐mental state examination
(MMSE),5,6 depressive symptoms assessed by the geriatric depression scale (GDS)6 and
frailty assessed by the Groningen Frailty Index (GFI).7
In addition, data were obtained on the accrual of patients aged 65 years and older in the
ATX study, a concurrent BOOG study for metastatic breast cancer patients, in which
patients were randomised to first‐line combination chemotherapy with either
bevacizumab and paclitaxel or bevacizumab, paclitaxel and capecitabine. This study
cruited fit patients aged ≤ 75 years with an ECOG performance status of 0 or 1. re
Statistical analysis O
nly descriptive data were used.
Results
Potential barriers to accrual Surveys regarding barriers to accrual were sent to the coordinating investigators of the 19
centres that were participating in the OMEGA study in 2008; surveys were returned from
15 centres. Regarding potential patient‐related barriers, eight respondents stated that
potentially eligible patients had refused chemotherapy (53%), and nine respondents
mentioned that potential patients had refused randomisation (60%). The most important
physician‐related factors were their preference for a particular type of chemotherapy
(7%), their hesitance in offering chemotherapy to older patients (13%) and a lack of man‐
power (7%). In response to questions on study‐related barriers to accrual, three
investigators stated that cognitive impairment in patients limited their ability to
participate in the trial (20%) and two mentioned that the exclusion of patients with an
impaired left ventricular ejection fraction posed a barrier (13%), while one respondent
mentioned that many of the patients were too frail to receive any form of chemotherapy
(7%) and another found the patient information form as too complicated (7%). The
comprehensive geriatric assessment was considered to be too time‐consuming by the
patient (one respondent, 7%) or the investigators (two respondents, 13%). The use of
single‐agent chemotherapy as opposed to combination treatment was stated by one
respondent (7%), while three respondents reported that concurrent trials in this particular
patient group limited accrual (20%).
69

Chapter 5
Table 1: Baseline characteristics of patients included in the OMEGA study
Number of patients 78
Median age (range) 75.5 years (65.8–86.8)
Marital status Married Widowed Single Missing
43 23 8 4
Current living situation Independent Residential care Missing
71 2 5
Additional persons in household 0 32 1 37 2 5 Missing 4
Offspring Yes 60 No 14 Missing 4
Education level College/university 6 High school/vocational education 51 Primary school 15 None 1 Missing 5
Performance status 0 23 1 37 2 16 3 1 Missing 1
Body Mass index Undernutrition (BMI <20 kg/m2)
Normal (BMI 20‐30 kg/m2)
Overweight (BMI >30 kg/m2)
5 50 23
IADL4 Fully independent (28‐30 points) 8
Partially dependent (14‐27 points) 65 Fully dependent (≤13 points) 0 Missing 5
Polypharmacy 0‐4 types of medication 39 5+ types of medication 37 Missing 2
Charlson comorbidity index3 0 45
1‐2 22 3‐4 2 5+ 1 Missing 8
MMSE5 No cognitive dysfunction (24 points or more) 69
Cognitive dysfunction (≤23 points) 5 Missing 4
GDS6 No depressive symptoms (0‐4 points) 49
Mild depressive symptoms (5‐9 points) 21 Moderate/severe depressive symptoms (10 points or more) 3 Missing 5
GFI7 Not frail (0‐3 points) 32
Frail (4 or more points) 40 Missing 6
70

Slow accrual in the OMEGA study
Inclusion in a concurrent non‐elderly study A total of 28 potentially eligible patients for the OMEGA study, aged 65 to 71 years, were
included in the concurrent ATX‐study with combination chemotherapy in metastatic
breast cancer by centres participating in the OMEGA trial during the time period that the
tter trial was open to inclusion. la
Baseline characteristics of patients included in the OMEGA study Baseline characteristics of included patients are shown in Table 1. Median age was 75.5
years (range 65.8 – 86.8 years) and 32 patients (54%) were aged 75 years or older.
Patients primarily lived independently (n=71, 91%) and 54% of patients (n=42) lived with
at least one other person. Although most patients had an ECOG performance status (PS) of
0 or 1, seventeen patients (22%) had a PS of 2 or 3. Five patients had a BMI below 20
kg/m2 (6%). Over 80% of patients (n=65) were partially dependent in their instrumental
activities of daily living (IADL), but no patients were fully IADL dependent. The median
number of different medications being taken at baseline was five (range 0‐14). For 45
patients (58%), no significant comorbidity was present (Charlson comorbidity index score
0). Twenty‐two patients had a Charlson score of 1 or 2 (28%), while only three patients
scored 3 or higher (4%). Few patients had cognitive dysfunction (n=5, 6%) but mild to
moderate depressive symptoms were present in 24 patients (31%). According to the
roningen frailty index, more than half of patients were considered frail (n=40, 51%). G
Discussion In the current report on accrual problems in the OMEGA study, a first‐line chemotherapy
study in frail older patients with metastatic breast cancer, we identified three major
barriers: 1) the patient’s refusal of chemotherapy, or their preference for a particular
treatment arm, 2) patient’s being considered too frail for chemotherapy, and therefore
more suitable for supportive care only, or alternatively, fit enough to be suitable for more
aggressive (combination) treatment such as in the ATX study, and 3) study characteristics
such as the time investment required for the geriatric assessments resulting in patient’s
refusal to participate or physician’s reticence to discuss this study with their patients.
However, despite these barriers and the subsequent lower than intended number of
patients included in this study, the baseline characteristics suggest that we did succeed in
including frail, elderly patients with geriatric syndromes.
This analysis of barriers to accrual may be hampered by the fact that the survey
retrospectively inquired about the barriers as experienced by the investigators which may
not necessarily reflect the actual process of accrual. Unfortunately, screening and
enrolment logs were not available for most participating centres, and no data were
71

Chapter 5
available on the number of potentially eligible patients who were not even considered for
enrolment.
The results of our survey demonstrate the dilemmas in designing a chemotherapy study
that allows for inclusion of sufficient numbers of older patients, while at the same time
ensuring sufficient homogeneity in the baseline characteristics to permit drawing
conclusions on the treatment outcome. Due to the great heterogeneity in the elderly
patient population, cancer treatment for these patients typically requires tailored care,2
while cancer trials by definition offer predefined and standardized care. Still, the baseline
characteristics of the included patients show that it is possible to enrol an older, frail
population, and future studies should maintain non‐restrictive inclusion criteria regarding
comorbidity and performance status.8 In addition, trials could use a form of stratification
to allow for inclusion of greater number of patients, or allow for dose‐adjustment (for
example, a primary dose reduction with the option of dose escalation if treatment is well
tolerated); Although this strategy was successfully implemented in previous studies,9 the
resultant heterogeneity in dosing schedules could affect the generalizability of study
outcomes. In addition, there is no consensus on what kind of instruments should be used
to guide stratification.10
The OMEGA trial is not the first study in older breast cancer patients to encounter accrual
issues. Recently, the CASA and ACTION trial, both focusing on adjuvant chemotherapy in
older women with breast cancer, were closed prematurely due to poor patient
recruitment.11 In the ACTION trial, patients were randomised between four cycles of
anthracycline/cyclophosphamide or alternatively observation only.12 In their analysis of
potential causes, the ACTION trial investigators stated that in contrast to their pre‐trial
audits, many patients were not eligible, and eligible ones often refused participation
because they did not want to be randomised to the chemotherapy arm. The investigators
stated that this is a particularly important issue in trials that use a no‐treatment arm.
Although the OMEGA study did not have a no‐treatment arm, patients were randomised
between two distinct types of chemotherapy, one given orally and one intravenously.
Previous studies have demonstrated that cancer patients receiving chemotherapy often
have a preference for a particular administration method,13 and in our survey, preference
for a particular treatment arm was indeed an important reason for patient’s refusal of
participation. It is likely that studies with more comparable treatment arms will be able to
circumvent this issue, at least partially.
A final issue is the time component: our survey showed that the time‐consuming nature of
the geriatric assessments, considered necessary for a meaningful characterisation of the
overall health status of elderly patients in clinical trials,14 was an issue for some patients
(and/or their family members) and time restraints can also cause reticence in treating
physicians to discuss the possibility of trial participation with the patient. Explaining a
72

Slow accrual in the OMEGA study
clinical trial to an older patient often requires a greater time investment than to younger
patients. However, a study on the attitudes of older patients towards enrolment in clinical
trials demonstrated that, despite initial hesitation due to randomisation, over 75% of
patients were willing to participate after additional explanation of the trial process.15 In
another study, the amount of time spent with the patient (by the treating physician or a
clinical research assistant) was identified as an important factor associated with the
likelihood of participation of older patients in clinical trials.16 Another prime factor was the
ndorsement of the clinical trial by the treating physician.15,16 e
In conclusion, our analysis of the accrual process in the OMEGA study demonstrates that
accrual of older breast cancer patients in this randomised clinical trial on chemotherapy
was mainly hampered by either patient’s refusal of chemotherapy or randomisation or a
medical condition considered as being too fit or too frail for inclusion. In line with previous
randomised studies on adjuvant chemotherapy in elderly patients, preference for a
specific treatment was an important reason for patient’s refusal of trial participation.
Ultimately, we did manage to include frail, elderly patients, and the results on toxicity,
efficacy and the impact of comprehensive geriatric assessments are expected this year.
Future trials in elderly breast cancer patients should focus on non‐restrictive inclusion
criteria regarding co‐morbidity and performance status, avoid concurrent trials with
overlapping eligibility criteria, as well as on education of physicians and elderly patients on
e advantages of trial participation. th
Financial support: The OMEGA study received unrestricted financial support from Amgen
BV the Netherlands, Janssen‐Cilag BV the Netherlands, MSD the Netherlands and the
Dutch Cancer Society.
73
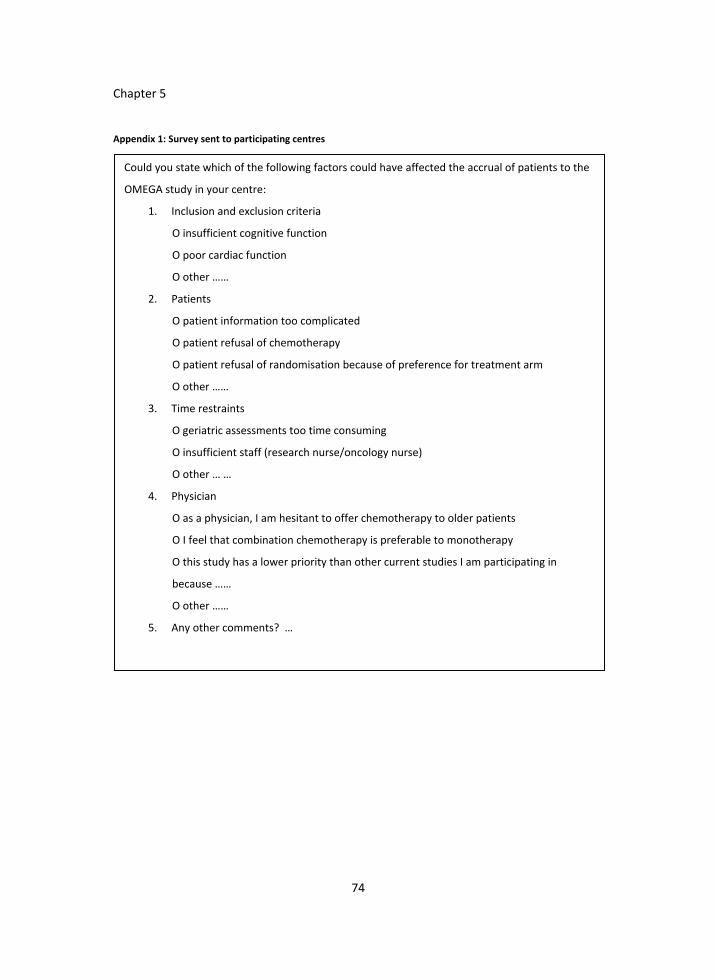
Chapter 5
Appendix 1: Survey sent to participating centres
Could you state which of the following factors could have affected the accrual of patients to the
OMEGA study in your centre:
1. Inclusion and exclusion criteria
O insufficient cognitive function
O poor cardiac function
O other ……
2. Patients
O patient information too complicated
O patient refusal of chemotherapy
O patient refusal of randomisation because of preference for treatment arm
O other ……
3. Time restraints
O geriatric assessments too time consuming
O insufficient staff (research nurse/oncology nurse)
O other … …
4. Physician
O as a physician, I am hesitant to offer chemotherapy to older patients
O I feel that combination chemotherapy is preferable to monotherapy
O this study has a lower priority than other current studies I am participating in
because ……
O other ……
5. Any other comments? …
74

Slow accrual in the OMEGA study
75
References 1. Hutchins LF, Unger JM, Crowley JJ et al. Underrepresentation of patients 65 years of age or older in
cancer‐treatment trials. N Engl J Med 1999;341:2061‐2067. 2. Wildiers H, Kunkler I, Biganzoli L et al. Management of breast cancer in elderly individuals:
recommendations of the International Society of Geriatric Oncology. Lancet Oncol 2007;8:1101‐1115. 3. Charlson ME, Pompei P, Ales KL, Mackenzie CR. A new method of classifying prognostic comorbidity in
longitudinal studies: development and validation. J Chronic Dis 1987;40:373‐383. 4. Lawton MP, Brody EM. Assessment of older people: self‐maintaining and instrumental activities of daily
living. Gerontologist 1969;9:179‐186. 5. Folstein MF, Folstein SE, McHugh PR. "Mini‐mental state". A practical method for grading the cognitive
state of patients for the clinician. J Psychiatr Res 1975;12:189‐198. 6. Sheikh JI, Yesavage JA, Brooks JO et al. Proposed factor structure of the Geriatric Depression Scale. Int
Psychogeriatr 1991;3:23‐28. 7. Slaets JP. Vulnerability in the elderly: frailty. Med Clin North Am 2006;90:593‐601. 8. Ferrucci L, Guralnik JM, Studenski S et al. Designing randomised, controlled trials aimed at preventing or
delaying functional decline and disability in frail, older persons: a consensus report. J Am Geriatr Soc 2004; 52:625‐634.
9. ten Tije AJ, Smorenburg CH, Seynaeve C et al. Weekly paclitaxel as first‐line chemotherapy for elderly patients with metastatic breast cancer. A multicentre phase II trial. Eur J Cancer 2004;40:352‐357.
10. Maas HA, Janssen‐Heijnen ML, Olde Rikkert MG, Machteld Wymenga AN. Comprehensive geriatric assessment and its clinical impact in oncology. Eur J Cancer 2007;43:2161‐2169.
11. Reed MW, Wyld L, Ellis P et al. Breast cancer in older women: trials and tribulations. Clin Oncol (R Coll Radiol ) 2009;21:99‐102.
12. Leonard R, Ballinger R, Cameron D et al. Adjuvant chemotherapy in older women (ACTION) study ‐ what did we learn from the pilot phase? Br J Cancer 2011;105:1260‐1266.
13. Liu G, Franssen E, Fitch MI, Warner E. Patient preferences for oral versus intravenous palliative chemotherapy. J Clin Oncol 1997;15:110‐115.
14. Audisio RA, Van LB. When reporting on older patients with cancer, frailty information is needed. Annals of Surgical Oncology 2011;18: 4‐5.
15. Townsley CA, Chan KK, Pond GR et al. Understanding the attitudes of the elderly towards enrolment into cancer clinical trials. BMC Cancer 2006;6:34.
16. Wright JR, Whelan TJ, Schiff S et al. Why cancer patients enter randomised clinical trials: exploring the factors that influence their decision. J Clin Oncol 2004;22:4312‐4318
.


Part II
Treatment in elderly patients with other cancer types


Chapter 6
Colon cancer treatment and adherence to national guidelines: does age still matter?
J.M. Jonker, M.E. Hamaker, M. Soesan, C.R. Tulner, I.M.J.A. Kuper
Journal of Geriatric Oncology 2012;3:131‐137

Chapter 6
Abstract Introduction: In the past decades, much attention has been given to the risks of
undertreatment of cancer in older patients. We set out to determine whether current
treatment of colon cancer in older patients still differs from younger patients and to
identify risk factors and physician’s reasons for deviation from Dutch treatment guidelines.
Patients and methods: Retrospective cohort study of all consecutive patients newly
diagnosed with colon cancer at the Slotervaart Hospital in Amsterdam between January
2002 and December 2007. Data were collected using clinical charts.
Results: Of 286 newly diagnosed colon cancer patients, 183 were 70 years or older.
Ninety‐one percent of older patients received curative surgery and 32% received adjuvant
chemotherapy in accordance with guidelines compared to 100% and 85% in the younger
group (p=0.002 and p<0.001 respectively). The primary reasons stated by the treating
physician for withholding surgery were comorbidity and poor general health. For adjuvant
chemotherapy, the main reason stated was age. For both surgery and chemotherapy,
multivariate analysis revealed that deviation from guidelines was most strongly associated
with age (surgery OR 1.18 (CI 1.06‐1.30); p=0.002 and chemotherapy OR 1.19 (CI 1.08‐
1.31); p<0.001 respectively). Despite this selection, older patients experienced more
postoperative morbidity and mortality than younger patients. Chemotherapy toxicity was
equal in both groups, despite less aggressive regimens for older patients.
Conclusion: At our centre, guideline adherence for surgery in older patients was high, and
deviations were well motivated. Age still seems to be the most important factor for
withholding chemotherapy, despite evidence suggesting benefit in selected older patients.
80

Colon cancer in the elderly
Introduction Colon cancer is one of the most common cancers worldwide, particularly in developed
countries.1 In the Netherlands, it ranks third in the incidence of all cancers, with 37.8 new
cases per 100.000 inhabitants in 2008. In 2008 the mortality rate of colon cancer in the
Netherlands was 16.8/100.000. The occurrence increases with age, with 58% being 70
years or older.2 As a result of increasing life expectancy, the incidence of colon cancer in
the older population is expected to increase even further in the coming decades.
Much is yet unknown about how to treat these older cancer patients. Ageing is an
individual process, making this group heterogeneous in terms of comorbidity, general
health, functional status and social network. In view of this heterogeneity, it is incorrect to
automatically assume that older patients not receiving standard oncologic treatment are
being undertreated, as good reasons may exist for deviation from treatment guidelines.
Recent studies have demonstrated that surgery and chemotherapy are safe and
efficacious in selected older patients with colon cancer,3‐7 but as clinical trials have often
excluded older patients and those with severe comorbidity, it is unclear how these results
are to be interpreted when treating this older, heterogeneous population.8
Many experts agree that chronological age itself should not be the reason for withholding
cancer treatment. However, several studies on colon cancer treatment in older patients,
based primarily on patient cohorts diagnosed between 1990 and 2000, have
demonstrated that age alone was the prime risk factor for deviation from standard
treatment.9‐15 Several of these studies did not address the motivation behind discordance
with recommended cancer treatment.
In this study, we set out to determine whether current treatment of colon cancer in older
patients still differs from that in younger patients in terms of adherence to national
treatment guidelines, to describe physician’s reasons for withholding treatment in the
older patients group and to identify risk factors for deviations from recommended
eatment. tr
Methods This is a retrospective cohort study of all consecutive patients newly diagnosed with colon
cancer in a middle‐sized teaching hospital in Amsterdam, the Netherlands, between
January 2002 and December 2007.
Patients were identified from the regional cancer registry, the IKA (Integraal Kanker
Centrum Amsterdam). To ensure that no patients were omitted, the registry data were
compared with the hospital’s pathology database. This study was reviewed by the Medical
Research Ethics Committee at Slotervaart Hospital and found it exempt from IRB review.
For all patients, the following data were collected from their charts: age, sex, Charlson
Comorbidity Index16, polypharmacy (the use of 4 or more types of medication), TNM
81

Chapter 6
stage, histological grade, initial treatment regimens (surgery and/or chemotherapy), and if
applicable, post‐operative complications and toxicity of chemotherapy.
Initial treatment was compared to treatment as recommended by national treatment
guidelines.17 For stage I and II colon cancer, the recommended treatment is surgery only.
Chemotherapy for patients with stage II disease is not recommended as standard care, but
might be offered to patients with high risk disease, for example T4 or imminent blow‐out.
For stage III colon cancer, standard treatment consists of surgery and subsequent adjuvant
chemotherapy. In patients with metastatic disease, palliative chemotherapy is advised,
with surgical intervention when appropriate. The latter is not considered standard care.
For patients not receiving standard treatment, the physician’s correspondence to the
general physician of the patient was consulted to collect the reasons for deviation from
the guidelines. When the reason was not found, the patient’s medical chart was
consulted. Duration of follow‐up was 2 years. Data on mortality was collected from the
Municipal Data Registry. Post‐operative mortality was defined as death within 30 days of
rgery. su
Statistical analysis To compare baseline characteristics and guideline adherence, patients were categorized
into two age groups, younger than 70 years and 70 years and older. For these
comparisons, the chi‐square test was used.
To determine which factors were associated with guideline discordance a univariable
logistic‐regression analysis was performed. For surgical treatment, five factors were
included in the analysis: age, sex, comorbidity scored by the Charlson index, the presence
of polypharmacy and anaemia. For chemotherapy, the occurrence of post‐operative
complications was added to these five factors. All factors with a p‐value <0.2 and possible
confounders (sex, age and comorbid disease) were subsequently analysed in a
multivariable logistic‐regression analysis. A backward selection procedure, accepting a p‐
value of p<0.05, was used. Kaplan Meier survival plots, with a log‐rank analysis, were used
to determine survival.
The SPSS (Statistical Package for the Social Sciences) version 16.0 was used for the
nalyses. a
Results
Patient characteristics From January 2002 to December 2007, 286 new cases of colon cancer patients were
identified, of which 183 were 70 years or older (64%). Patient characteristics are listed in
Table 1. Mean Charlson comorbidity score was 1.2 (SD 1.4) in the older adults compared
82

Colon cancer in the elderly
to 0.6 (SD 1.0) in the younger group (p=0.001). Tumour stage did not differ between age
groups. However, 9% of the older patients could not be staged due to omission of surgery
the absence of clinically evident metastases. in
Guideline adherence Six patients died before treatment could be initiated. These patients were not included in
further analyses. Guideline adherence per age group is presented in Figure 1. All patients
under 70 years of age with stage I to III disease received surgery in accordance with
national guidelines. Of the 147 patients aged 70 and over, 133 received surgical treatment
(91%, p=0.002), and this percentage remained over 80% even in patients aged 85 years
and older. Resection margins were tumour free in 99% of younger patients and 98% in
older patients. Only 12 of 38 patients older than 70 years with stage III colon cancer
received adjuvant chemotherapy in accordance with guidelines (32%), compared to 29 of
34 younger patients (85%, p<0.001). Treatment with chemotherapy decreased steadily
Table 1: Patient characteristics per age group
Total < 70 years ≥ 70 years p‐value
No. of patients 286 103 (36.0%) 183 (64.0%)
Median age (range) 75 (21‐97) 62 (21‐69) 80 (70‐97)
Female, n (%) 165 (57.7) 50 (48.5) 115 (62.8) 0.013
Charlson comorbidity score, n (%)
0
1
2
≥ 3
134 (46.9)
76 (26.6)
50 (17.5)
26 (9.1)
65 (63.1)
21 (20.4)
12 (11.7)
5 (4.9)
69 (37.7)
55 (30.1)
38 (20.8)
21 (11.5)
<0.001
0.045
Tumour stage, n (%)
I
II
III
IV
Unknown
41 (14.3)
99 (34.6)
72 (25.2)
58 (20.3)
16 (5.6)
18 (17.5)
29 (28.2)
34 (33.0)
22 (21.4)
0 (0.0)
23 (12.6)
70 (38.3)
38 (20.8)
36 (19.7)
16 (8.7)
0.001
Histology grade n (%)
Well differentiated
Mildly differentiated
Poorly differentiated
Not determined
4 (1.4)
213 (74.5)
45 (15.7)
24 (8.4)
2 (1.9)
71 (68.9)
24 (23.3)
6 (5.8)
2 (1.1)
142 (77.6)
21 (11.5)
18 (9.8)
0.007
83
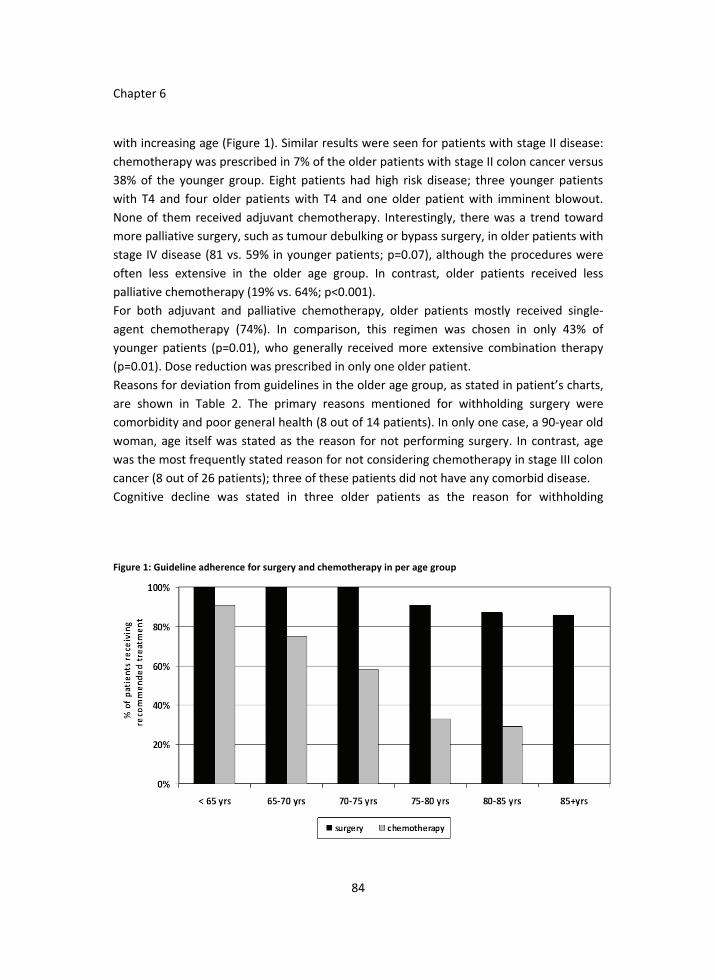
Chapter 6
with increasing age (Figure 1). Similar results were seen for patients with stage II disease:
chemotherapy was prescribed in 7% of the older patients with stage II colon cancer versus
38% of the younger group. Eight patients had high risk disease; three younger patients
with T4 and four older patients with T4 and one older patient with imminent blowout.
None of them received adjuvant chemotherapy. Interestingly, there was a trend toward
more palliative surgery, such as tumour debulking or bypass surgery, in older patients with
stage IV disease (81 vs. 59% in younger patients; p=0.07), although the procedures were
often less extensive in the older age group. In contrast, older patients received less
palliative chemotherapy (19% vs. 64%; p<0.001).
For both adjuvant and palliative chemotherapy, older patients mostly received single‐
agent chemotherapy (74%). In comparison, this regimen was chosen in only 43% of
younger patients (p=0.01), who generally received more extensive combination therapy
(p=0.01). Dose reduction was prescribed in only one older patient.
Reasons for deviation from guidelines in the older age group, as stated in patient’s charts,
are shown in Table 2. The primary reasons mentioned for withholding surgery were
comorbidity and poor general health (8 out of 14 patients). In only one case, a 90‐year old
woman, age itself was stated as the reason for not performing surgery. In contrast, age
was the most frequently stated reason for not considering chemotherapy in stage III colon
cancer (8 out of 26 patients); three of these patients did not have any comorbid disease.
Cognitive decline was stated in three older patients as the reason for withholding
Figure 1: Guideline adherence for surgery and chemotherapy in per age group
84

Colon cancer in the elderly
chemotherapy, while for seven patients the reason was not stated. In the younger group
reasons for withholding chemotherapy were prolonged post‐operative course (n=2),
comorbidity (n=1) and poor general health (n=1). One patient declined chemotherapy.
Univariate and multivariate analysis, performed to determine baseline factors associated
with guidelines discordance are shown in Table 3. Advancing age was shown to be the
most important factor for both surgery (odds ratio (OR) 1.18 (95% confidence interval (CI)
1.06‐1.30); p=0.002) and chemotherapy (OR 1.19 (95%CI 1.08‐1.31); p<0.001).
Comorbidity was borderline significant for surgery (OR 1.39 (95%CI 0.99‐1.95); p=0.06) but
was not associated with chemotherapy use (p=0.44). However, withholding of
chemotherapy was associated with post‐operative complications (OR 8.81 (95%CI 1.74‐
44.50); p=0.01) while polypharmacy showed a borderline significant association (OR 4.62
5%CI 0.98‐21.85); p=0.05). (9
Complications of surgery and chemotherapy Complications of treatment are shown in Table 4. Nearly 50% of the older patients (75 out
of 157) experienced some kind of complication after surgery; in 30 patients (19%), these
complications were life threatening (requiring intensive care treatment and/or resulting in
death). This is significantly higher than in the younger group, for which these percentages
were 30% (p=0.003) and 9% (p=0.02) respectively. The two groups did not differ in the
occurrence of wound infection (9 versus 12% in younger and older patients respectively)
or anastomotic leak (7 versus 10% respectively) but older patients experienced
significantly more cardiopulmonary complications (13% versus 27%; p= 0.01). Post‐
operative mortality was 12% for older patients, compared to 3% in the younger age group
(p= 0.03).
Table 2: Reason stated in clinical charts for deviation of guidelines older age group
Surgery Chemotherapy
Number of patients not treated in accordance with guidelines
14 26
Reason stated Death during treatment Age Comorbidity Patient refusal Cognitive decline Poor general health Prolonged post‐operative course Unknown
3 1 5 2 0 3 ‐ 0
3 8 2 1 3 0 2 7
85

Chapter 6
Table 3: Univariate and multivariate analysis
Univariate analysis Multivariate analysis *
Odds ratio
95% confidence interval
p= * Odds ratio
95% confidence interval
p= *
Surgery Age 1.16 1.05‐1.29 0.005 1.18 1.06‐1.30 0.002 Sex 0.74 0.18‐3.12 0.68 0.75 0.18‐3.17 0.70 Comorbidity 1.42 0.96‐2.10 0.08 1.42 1.00‐1.95 0.06 Polypharmacy 0.69 0.16‐3.02 0.62 Anaemia 0.35 0.036‐3.37 0.36
Chemotherapy Age 1.17 1.06‐1.29 0.002 1.19 1.08‐1.31 <0.001 Sex 1.10 0.22‐5.48 0.91 1.14 0.23‐5.63 0.87 Comorbidity 1.37 0.61‐3.07 0.44 1.37 0.62‐3.05 0.44 Polypharmacy 3.74 0.76‐18.47 0.11 4.62 0.98‐21.85 0.05 Anaemia 0.58 0.13‐2.64 0.48 Postoperative complications
7.97 1.54‐41.25 0.013 8.81 1.74‐44.5 0.008
*Variables with a p‐value <0.20 in the univariate analysis were included in the multivariate analysis. Age, sex and
comorbidity were also included as potential confounders. A backward selection procedure was applied; a
forward analysis selected the same variables.
Table 4: Treatment complications
< 70 years ≥ 70 years p‐value
Surgery*
All complications Wound infection Anastomotic leak Cardiopulmonary complications Life‐threatening complications Postoperative mortality (30‐days)
26/88 (30%)8/88( 9%)6/88 ( 7%)
11/88 (13%)8/88 ( 9%)3/88 ( 3%)
75/157 (48%)18/157(12%)15/157(10%)42/157(27%)30/157 (19%)18/157 (12%)
0.004 0.36 0.32
0.006 0.03 0.02
Chemotherapy**
Toxicity all grades
Toxicity grade III‐IV
Hospital admission due to toxicity Termination therapy due to toxicity
44/50 (88%)16/50 (32%)9/50 (18%)
10/50 (20%)
18/22 (82%)6/22 (27%)4/22 (18%)5/22 (23%)
* Polipectomie not included ** 6 patients lost to follow up (4 young, 2 old)
86

Colon cancer in the elderly
Of the 78 patients receiving chemotherapy, four younger patients and two older patients
no information on toxicity was available, as they were treated elsewhere. No statistically
significant differences in toxicity or toxicity‐related sequalae were seen between age
groups, but numbers are small and treatment regimens were diverse. In both age groups,
18% required admission to hospital due to toxicity of chemotherapy and around 20%
rminated their initial chemotherapy regimens before receiving all planned cycles. te
Survival Figure 2 shows two‐year survival plots. Patients not receiving standard treatment had a
significantly poorer prognosis: one‐year survival was 84% for those patients receiving
standard treatment, and 68% in case of a deviation from treatment guidelines while two‐
year survival was 74% and 56% respectively (p=0.04).
Figure 2: Kaplan Meier survival plots
87

Chapter 6
Discussion In the past decades, much attention has been paid to the risks of undertreatment of
cancer in older patients. In this study, we set out to determine whether current treatment
of colon cancer in older patients still differs from standard treatment and to explore
treating physicians’ reasons for deviating from guidelines. We found that 91% of patients
aged 70 years and older received surgery in accordance with guidelines, compared to
100% of younger patients. Only 32% of older patients receiving adjuvant chemotherapy,
compared to 85% of younger patients. With advancing age, use of adjuvant chemotherapy
declines drastically. Age was the factor most strongly associated with withholding
chemotherapy, followed by the occurrence of post‐operative complications, while for
surgery, age and comorbidity were the most important factors.
Although various prior studies have addressed guideline adherence in older patients with
colon cancer,3‐7 most did not address the reasons behind discordance with treatment
recommendations. We believe that these data are necessary to differentiate between
undertreatment and adequate adjustment of treatment to the individual patient. Our
study is unique in that we have collected these reasons, in combination with information
on surgical complications and toxicity of chemotherapy. Another strength of this study is
that it represents every day practice rather than a selected population. An important
limitation of this study, however, is its retrospective character, as not all parameters were
systematically documented and some data could not be retrieved from patient’s charts.
For example, we were not able to include relevant factors such as functional and
nutritional status, cognitive function and social support. The data we collected were from
a single‐centre, and therefore, it is unclear if our findings can be extrapolated to
treatment patterns at other centres.
The rate of guideline adherence for surgical treatment in our study is higher than those
found in previous studies,9,10,18 which state rates of 67 to 88% for older patients. As these
studies addressed patients diagnosed between 1990 and 2000, perhaps the higher rate
found at our centre is a reflection of an increased awareness of the risks of
undertreatment.
Post‐operative morbidity and mortality were high for our older patients (all complications
48% and postoperative mortality 12%). This finding is confirmed by various previous
studies, which, despite substantial differences in complication rates and mortality, all
found these to be significantly higher in older patients.3 In our study, comorbidity and
poor general health were the primary reasons stated by the treating physician for
withholding surgery. In light of the higher surgical risk for older patients, these may be
good reasons for deviating from guidelines.
We found that older patients received chemotherapy less often than younger patients,
and when administered, less extensive treatment regimens were chosen. Earlier European
88

Colon cancer in the elderly
studies showed similar results, with 13‐24% of patients aged 75 years and older receiving
chemotherapy; in the United States treatment rates are considerable higher (≥75 years
range 35% to 52%).18 In our study, chronological age was the most important reason
mentioned by the treating physician for not following chemotherapy guidelines. Despite
selection of older patients and less extensive treatment regimes in our cohort, one‐third
of patients experienced grade III‐IV toxicity.
Prior studies addressing the reasons for not offering adjuvant chemotherapy in older
patients found that patient’s refusal was the primary reason in the patients aged 71 to 80
years and age alone or age in combination with comorbidity for those aged 80 years and
older.11,14,19 Thus, age is still an important factor in treatment decisions regarding
chemotherapy.
Treating physicians may consider the benefit of adjuvant chemotherapy in preventing
cancer recurrence to be too small or toxicity too great. Eighty percent of recurrences of
colon cancer occur within 3 years and 90% of patients with recurrence die within 24
months.20 In 1990 the first study with levamisole and fluorouracil in stage III colon cancer
showed a 15% absolute risk reduction for recurrence and 16% absolute risk reduction of
mortality compared to patients without this adjuvant chemotherapy.21 Later studies,
replacing levamisole with leucovorin, have shown similar benefit of adjuvant
chemotherapy in selected older patients.22 Furthermore, various studies have
demonstrated that fit older patients with no significant comorbidity are able to tolerate
standard colon cancer treatment as well as younger patients.3‐7,23,24 In summary, any
patient with a life expectancy of 3 to 5 years, in reasonable general health, and a high risk
of recurring disease, could benefit from the addition of chemotherapy. The average life‐
expectancy for an 80 year old woman is another 9.3 years and for a man 7.5 years so
curative treatment should be considered in this age group.
Therefore, the challenge surgeons and oncologists are facing is how to differentiate the fit
from the vulnerable, and how to predict life expectancy. Although chronological age
obviously influences life expectancy and a recent study showed that older patients may
experience more chemotherapy toxicity, ageing is a heterogeneous process and age alone
should not be the reason for withholding a potentially curative treatment.25
Elements of a comprehensive geriatric assessment (CGA) can predict morbidity and
mortality in older patients with cancer, which are both important factors in determining if
cancer treatment is appropriate.26 A CGA provides information on the functional ability,
comorbid medical conditions, cognition, nutritional status, psychological state and social
support of older cancer patients.27‐29 Screening instruments such as American Society of
Anaesthesiologists (ASA)‐score and Karnofsky performance status (PS) score were not
developed to detect these geriatric conditions.27,30‐31 However, it may well be that these
additional factors determine if an older patient is vulnerable or has a good chance to
89

Chapter 6
undergo cancer treatment without serious adverse effects.32 For example, a recent study
showed that the results of a CGA were predictive of complications after surgery for
colorectal cancer in 171 older patients (median age 80 years), while age, ASA class, and
stage of disease were not.33 In addition, preoperative assessment in elderly cancer
patients (PACE) showed that IADL, fatigue and performance status were associated with
50% increase in relative risk of post‐operative complications.34 Two recent studies focused
on predicting chemotherapy toxicity in older adults with cancer. One study found that
hearing impairment, one or more falls in the last 6 months, limitations in walking one
block, the need for assistance in taking medications, and decreased social activities were
risk factors for toxicity.25 In the other study IADL was a risk factor of hematologic toxicity,
while self‐rated health, mini‐mental status scores and mini‐nutritional assessment score
were predictors for non‐hematologic toxicity.35 Further research into the optimal form of
CGA and its role in cancer treatment decision making is much needed and is slowly
ecoming available.36‐38 b
In conclusion, colon cancer treatment in the older patients still differs greatly from their
younger counterparts in our centre. Curative surgery in the older patient is not withheld
based on chronological age alone but mostly because of comorbidity and physical fitness.
As chronological age alone is the most important reason mentioned for omitting adjuvant
chemotherapy, it is possible that a potentially curative treatment was withheld in these
patients. Further research is needed on the role of CGA in differentiating frail older
patients from those that will benefit from standard treatment despite advanced age.
90

Colon cancer in the elderly
References 1. Jemal A, Bray F, Centre MM et al. Global cancer statistics. CA Cancer J Clin 2011;61:134 . 2. IKCnet (Integraal kankerregistratie: Dutch cancer registry); Available from URL: http//www.ikcnet.nl 3. Colorectal Cancer Collaborative Group. Surgery for colorectal cancer in elderly patients: a systemic review.
Lancet 2000;356:968‐74. 4. Sargent DJ, Goldberg RM, Jacobson SD et al. A pooled analysis of adjuvant chemotherapy for resected
colon cancer in elderly patients. N Engl J Med 2001;345:1091‐7. 5. Sundararajan V, Mitra N, Jacobson JS et al. Survival associated with 5‐fluorouracil‐based adjuvant
chemotherapy among elderly patients with node‐positive colon cancer. Ann Intern Med 2002;136:349‐57 6. Jessup, JM, Steward A, Green FL, Minsky BD. Adjuvant chemotherapy for stage III colon cancer: implication
of race/ethnicity, age, and differentiation. JAMA 2005;294:2703‐11. 7. Goldberg RM, Tabah‐Fisch I, Bleiberg H et al. Pooled analysis of safety and efficacy of oxaliplatin plus
fluorouracil/leucovorin administered bimonthly in elderly patients with colorectal cancer. J Clin Oncol 2006;24;4085‐91.
8. Hutchins LF, Unger JM, Crowley JJ et al. Underrepresentation of patients 65 years of age or older in cancer‐treatment trials. N Engl J Med 1999;341:2061‐7.
9. Damhuis RAM, Wereldsma JCJ, Wiggers T. The influence of age on resection rates and postoperative mortality in 6457 patients with colorectal cancer. Int Colorect Dis 1996;11:45‐48.
10. Aparicio T, Navazesh A, Boutron et al. Half of elderly patients routinely treated for colorectal cancer receive a sub‐standard treatment. Crit Rev Oncol Hematol 2009;71:249‐57.
11. Mahoney T, Kuo YH, Topilow A, Davis JM. Stage III colon cancers; why adjuvant chemotherapy is not offered to elderly patients. Arch Surg 2000;135:182‐5.
12. Schrag D, Cramer LD, Bach PB, Begg CB. Age and adjuvant chemotherapy use after surgery for stage III colon cancer. J Natl Cancer Inst 2001;93:850‐7.
13. Potosky AL, Harlan LC, Kaplan RS et al. Age, sex, and racial differences in the use of standard adjuvant therapy for colorectal cancer. J Clin Oncol 2002;20:1192–202.
14. Ayanian, JZ, Zaslavsky, AM, Fuchs CS et al. Use of adjuvant chemotherapy and radiation therapy for colorectal cancer in a population‐based cohort. J Clin Oncol 2003;21:1293‐300.
15. Lemmers VE, van Halteren AH, Janssen‐Heijnen ML et al. Adjuvant treatment for elderly patients with stage III colon cancer in the southern Netherlands is affected by socioeconomic status, gender, and comorbidity. Ann Oncol 2005;16:767‐72.
16. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987;40:373–83.
17. Dutch national guidelines: Coloncarcinoom versie 1.2;www.oncoline.nl 18. Faivre J, Lemmens VE, Quipourt V, Bouvier AM. Management and survival of colorectal cancer in the
elderly in population‐based studies. Eur J Cancer 2007;43:2279‐84. 19. Ananda S, Field KM, Kosmider S et al. Patient age and comorbidity are major determinants of adjuvant
chemotherapy use for stage III colon cancer in routine clinical practice. J Clin Oncol 2008;26:2532‐7. 20. Sargent DJ, Wieand HS, Haller DG et al. Disease‐free survival versus overall survival as a primary end point
for adjuvant colon cancer studies: individual patient data from 20,898 patients on 18 randomized trials. J Clin Oncol 2007;25:4569‐74.
21. Moertel CG, Fleming TR, Macdonald JS et al. Levamisole and fluorouracil for adjuvant therapy of resected colon carcinoma. N Engl J Med 1990;322:352‐8
22. Haller DG, Catalano PJ, Macdonald JS et al. Phase III study of fluorouracil, leucovorin, and levamisole in high‐risk stage II and III colon cancer: final report of Intergroup 0089. J Clin Oncol 2005;23:8671‐8.
23. Scheithauer W, McKendrick J, Begbie S et al on behalf of the X‐ACT Study Group. Oral capecitabine as an alternative to i.v. 5‐fluorouracil‐based adjuvant therapy for colon cancer: safety results of a randomized, phase III trial. Ann Oncol 2003;14:1735‐43.
24. Popescu RA, Norman A, Ross PJ et al. Adjuvant or palliative chemotherapy for colorectal cancer in patients 70 years or older. J Clin Oncol 1999;17:2412‐8.
25. Hurria A, Togawa K, Mohile SG et al. Predicting Chemotherapy Toxicity in Older Adults With Cancer: A Prospective Multicentre Study. J Clin Oncol 2011;25:3457‐65.
26. Extermann M, Hurria, A. Comprehensive Geriatric Assessment for older patients with cancer. J Clin Oncol 2007;25:1824‐1831.
91

Chapter 6
92
27. Repetto L, Fratino L, Audisio RA et al. Comprehensive geriatric assessment adds information to Eastern Cooperative Oncology Group performance status in elderly cancer patients: an Italian Group for Geriatric Oncology Study. J Clin Oncol 2002;20:494‐502.
28. Monfardini S. Balducci L. A comprehensive geriatric assessment (CGA) is necessary for the study and the management of cancer in the elderly. Eur J Cancer 1999;35:1771‐72.
29. Extermann M, Aapro M, Bernabei R et al. Use of comprehensive geriatric assessment in older cancer patients: recommendations from the task force on CGA of the International Society of Geriatric Oncology (SIOG). Crit Rev Oncol Hematol 2005;55:241‐52.
30. Extermann M, Meyer J, McGinnis M et al. A comprehensive geriatric intervention detects multiple problems in older breast cancer patients. Crit Rev Oncol Hematol 2004;49:69‐75.
31. Gosney MA. Clinical assessment of elderly people with cancer. Lancet Oncol 2005;6:790‐797. 32. Aaldriks AA, Maartense E, le Cessie S et al. Predictive value of geriatric assessment for patients older than
70 years, treated with chemotherapy. Crit Rev Oncol Hematol 2011;79:205‐12. 33. Kristjansson SR, Nesbakken A, Jordhøy MS et al. Comprehensive geriatric assessment can predict
complications in elderly patients after elective surgery for colorectal cancer: a prospective observational cohort study. Crit Rev Oncol Hematol 2010;76:208‐17.
34. Audisio RA, Pope D, Ramesh HS et al. Shall we operate? Preoperative assessment in elderly cancer patients (PACE) can help: A SIOG surgical task force prospective study. Crit Rev Oncol Hematol 2008;65:156‐63.
35. Extermann, M, Boler I, Reich RR et al. Predicting the risk of chemotherapy toxicity in older: the chemotherapy risk assesment scale for high‐age patients (CRASH) score. Cancer 2012;118:3377‐86.
36. Hurria A, Gupta S, Zauderer M et al. Developing a cancer‐specific geriatric assessment. Cancer 2005;9:1998‐2005.
37. Hurria A, Cirrincione CT, Muss HB et al. Implementing a geriatric assessment in cooperative group clinical cancer trials: CALGB 360401. J Clin Oncol 2011;29:1290‐6.
38. Brunello A, Sandri R, Extermann M. Multidimentional geriatric evalution for cancer patients as a clinical and research tool. Canc Treat Rev 2009;35:487‐92.

Chapter 7
Diagnostic choices and clinical outcome in octogenarians with iron‐deficiency anaemia
M.E. Hamaker, T. Acampo, J.A. Remijn, S.A.C. van Tuyl, A. Pronk, H.A. Paling,
C.H. Smorenburg, S.E. de Rooij, B.C. van Munster
[submitted]

Chapter 7
Abstract Aim: To evaluate current clinical practice for octogenarians with iron‐deficiency anaemia
(IDA) by assessing referral patters and diagnostic choices, the clinical consequences of
omission of endoscopy, and the risks and benefits of IDA‐related surgery.
Methods: Chart review of all patients aged 80 years and older diagnosed with IDA (Hb ≤6.9
mmol/l and ferritin ≤25 ug/l) at a regional hospital‐based laboratory between January
2008 and December 2010.
Results: During the study period, 471 patients were newly diagnosed with IDA (median age
85.4 years). Of these, 276 (59%) did not undergo any diagnostic procedures for IDA. A
cause of anaemia was identified in 50% of patients undergoing initial work‐up. Of the 61
gastrointestinal malignancies that were identified, sixteen were found during follow‐up,
primarily in patients for whom initial diagnostic work‐up was limited or omitted. In case of
colon cancer, perioperative mortality was 15%, and survival benefit of surgery compared
to supportive care was not apparent until 1.3 years after ascertainment of iron‐deficiency
anaemia.
Conclusion: Omission of endoscopy for iron‐deficiency anaemia and omission of surgery
for colon cancer occur frequently in octogenarians, and appears legitimate in the presence
of relevant comorbidity and in case of limited remaining life‐expectancy. Further research
is needed to determine which baseline factors should guide decision making to optimize
outcome and quality of life.
94

Octogenarians with iron‐deficiency anaemia
Introduction Iron‐deficiency anaemia (IDA) occurs in 2‐5 % of men and post‐menopausal women in the
western world.1 Many benign causes are possible, such as insufficient iron intake or
absorption, arteriovenous malformations and erosive lesions, but 2‐15% of IDA patients
are diagnosed with colorectal cancer and 2‐6% with cancer of the upper gastro‐intestinal
tract.2‐5
In the care for an elderly patient with IDA, physicians are faced with a number of
dilemmas on how to proceed with diagnosis and treatment. First, although endoscopic
procedures are frequently performed in older patients, both the procedure itself – and in
case of colonoscopy the required bowel preparation – are burdensome and not entirely
without risk,6‐10 particularly in frail older patients or in case of significant comorbidity.
Second, omission of endoscopy will mean that the cause of IDA remains unclear. A lack of
diagnosis is most relevant in case of a potentially curable disease, such as colon cancer,
provided that a patient is fit enough and willing to undergo treatment. However, many
causes of IDA cannot be easily eliminated even when identified, in which case treatment
will focus on alleviation of symptoms with blood transfusions and/or iron suppletion; for
these patients, the clinical consequences of not identifying an exact cause of IDA due to
omission of endoscopy will be very limited.
In this study, we performed a population‐based cohort study of octogenarian patients
with iron‐deficiency anaemia to determine: a) current diagnostic practice in case of IDA,
by assessing the proportions of elderly patients receiving a full, partial or no endoscopic
work‐up; b) the clinical consequences of omission of endoscopy by assessing how
frequently a potentially curable cause of iron‐deficiency was diagnosed during follow‐up in
case of an incomplete initial work‐up; and c) to assess risks and benefit of cancer
treatment in case a colon malignancy is identified, by comparing survival in patients
ceiving surgical treatment with those for whom such treatment was omitted. re
Methods This is a cohort study of all patients aged 80 years and older for whom haemoglobin level
(Hb) and ferritin was determined at the Laboratory for Clinical Chemistry and
Haematology of the Gelre hospitals in Apeldoorn, the Netherlands, between January 2008
and December 2010. The Gelre hospital is the only laboratory in the Apeldoorn region and
serves as a regional laboratory for both hospital specialists and primary care physicians.
Patients were included in this study if they had a newly ascertained Hb‐level ≤ 6.9 mmol/l,
with a ferritin level below 25 ug/l. Patients were excluded if they had a previous diagnosis
of iron‐deficiency in the past five years.
For included patients, the following data were collected from the hospital database, which
contains all correspondence, data on diagnostic procedures and laboratory results: age at
95

Chapter 7
diagnosis, sex, medical history, medication use at diagnosis, laboratory findings
(haemoglobin, MCV, ferritin), the reason for blood sampling, symptoms or complaints
suggestive of anaemia or malignancy, the initial diagnostic procedures for anaemia
(imaging studies, endoscopic studies) and the underlying cause of anaemia. Comorbidity
was scored using the Charlson comorbidity index.11 All diagnostic procedures that were
part of the initial work‐up were classified as “initial diagnostic procedures”. In addition,
subsequent treatment was recorded, including the initiation or cessation of medication as
well as invasive treatment such as surgery.
Patients were followed until May 15th, 2012. All blood transfusions, secondary anaemia‐
related diagnoses, complications related to gastrointestinal disease and all‐cause deaths
ere recorded. w
Statistical analysis Descriptive statistics were used for most outcome data. For comparisons between patient
groups, the chi‐square test was used for nominal and ordinal variables. For continuous
variables with a normal distribution, the Student t‐test was used, and for continuous
variables with a non‐normal distribution the Mann‐Whitney test. All analysis was
performed using the SPSS (Statistical Package for the Social Sciences) version 19.0.
To determine which factors were associated with diagnostic choices, a univariate logistic
regression analysis was performed. Factors with a p‐value ≤0.20 were subsequently
entered into a multivariable model. To compare survival, Kaplan Meier survival plots with
log‐rank analysis were used. a
Results
Baseline characteristics Between 2008 and 2010, iron‐deficiency anaemia was ascertained in 471 patients aged 80
years and older living in the Apeldoorn region. Baseline characteristics can be found in
Table 1. Median age was 85.4 years (range 80‐101 years); 345 were women (73%).
Median haemoglobin level at diagnosis was 6.0 mmol/l (range 2.4‐6.9 mmol/l) and median
ferritin was 13 ug/l (range 2.0‐25.0 ug/l; for reference values, see Table 1). MCV was
below 80 fl in 289 patients (61%). Median Charlson comorbidity index was 1 (range 0‐7).
Laboratory testing was initiated by a hospital‐based specialist in 128 patients (27%) and by
the primary care physician in 343 (73%). Of the latter group, 138 were not referred to
hospital for analysis and therefore no further anaemia‐related information was available
(29% of all patients). For the remaining 333 patients, reason for testing haemoglobin
levels was suspected anaemia in 157 (47%), routine laboratory testing in 97 patients (29%)
and not retrievable in 79 (26%). Only 39 patients (12%) did not have any anaemia‐related
96

Octogenarians with iron‐deficiency anaemia
symptoms or complaints (Table 1); 51% of patients had constitutional symptoms, while
symptoms suggestive of upper and lower digestive tract pathology were present in 12%
nd 17% of patients respectively. a
Diagnostic procedures and diagnostic yield In addition to the 138 patients that were not referred to hospital, another 138 referred
patients did not have any diagnostic testing of the gastrointestinal tract (276 patients in
total, 59%). Ninety‐two patients had both a colonoscopy and a gastroduodenoscopy
(20%), 41 (9%) had a gastroduodenoscopy only, 43 (9%) a colonoscopy only and for 19
patients (4%), the diagnostic procedures were limited to imaging studies (ultrasound
and/or CT‐scan). Two of the 135 patients undergoing colonoscopy suffered from a colon
perforation (1.5%), one of which had a fatal outcome.
Table 2 shows factors associated with the likelihood of endoscopic procedures during the
initial diagnostic work‐up. In the multivariable analysis, female sex (odds ratio (OR) 0.57,
95% confidence interval (CI) 0.32‐0.91, p=0.02) and being 90 years of age or older (OR
0.34, 95%CI 0.17‐0.69, p=0.003) were independently associated with a decreased
likelihood that endoscopic procedures were performed while the odds of endoscopy
increased in the presence of gastrointestinal symptoms (OR 2.34, 95%CI 1.38‐3.96,
p=0.002).
The yield of the initial diagnostic procedures is listed in Table 3. A benign cause of anaemia
was identified in 46 of the 133 patients undergoing gastroduodenoscopy (34%) and a
malignancy in nine patients (7%). Colonoscopy identified a benign cause in 31 of 135
patients under this procedure (23%) and a malignancy in 31 patients (23%), of which five
were located in the rectum and 26 in the colon. When diagnostic procedures were limited
to imaging studies, a malignancy was identified in six out of 19 patients (32%), of which
four were located in the gastrointestinal tract. Two additional colon cancers were
identified on imaging studies performed in patients for whom colonoscopy could not be
completed. Overall, a cause of anaemia was identified in 97 of the 195 patients (50%)
during the initial IDA work‐up.
In addition to these nine upper and 37 lower gastrointestinal tract cancers identified in the
initial work‐up, another 24 malignancies were identified during follow‐up, of which six
were found outside the digestive tract, two in the pancreas, 15 in the colon and one in the
rectum. Of these latter 16 patients, three had received a complete initial work‐up; three
had received only imaging studies while for the remaining ten, no initial diagnostic
procedures were performed.
97
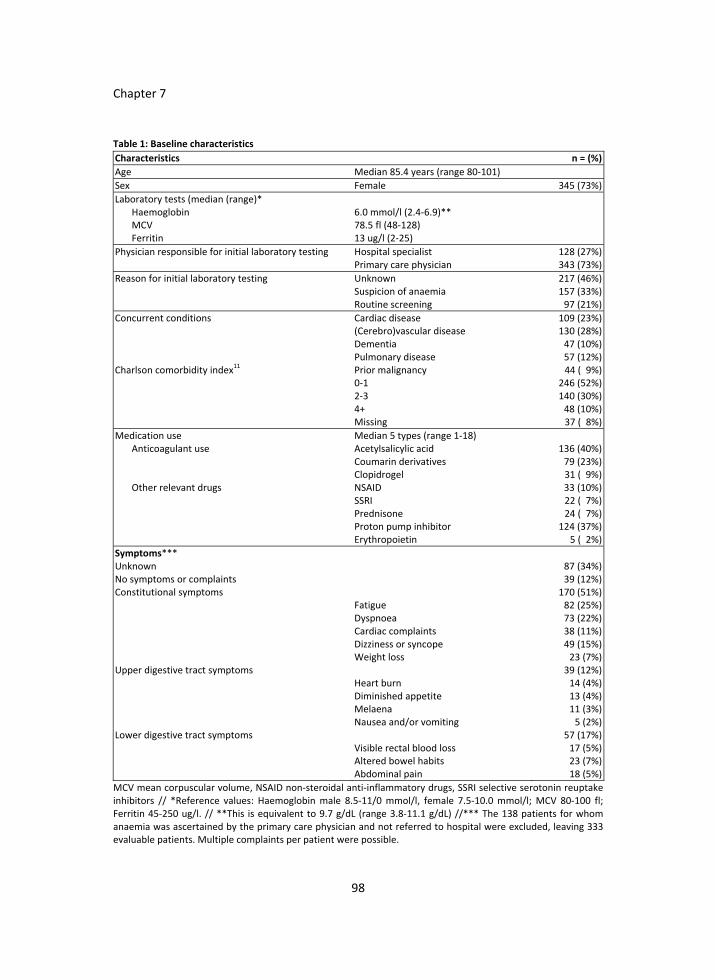
Chapter 7
Table 1: Baseline characteristics
Characteristics n = (%)
Age Median 85.4 years (range 80‐101)
Sex Female 345 (73%)
Laboratory tests (median (range)* Haemoglobin MCV Ferritin
6.0 mmol/l (2.4‐6.9)** 78.5 fl (48‐128) 13 ug/l (2‐25)
Physician responsible for initial laboratory testing Hospital specialist Primary care physician
128 (27%) 343 (73%)
Reason for initial laboratory testing Unknown Suspicion of anaemia Routine screening
217 (46%) 157 (33%) 97 (21%)
Concurrent conditions Charlson comorbidity index
11
Cardiac disease (Cerebro)vascular disease Dementia Pulmonary disease Prior malignancy 0‐1 2‐3 4+ Missing
109 (23%) 130 (28%) 47 (10%) 57 (12%) 44 ( 9%)
246 (52%) 140 (30%) 48 (10%) 37 ( 8%)
Medication use Median 5 types (range 1‐18) Anticoagulant use Acetylsalicylic acid
Coumarin derivatives Clopidrogel
136 (40%) 79 (23%) 31 ( 9%)
Other relevant drugs NSAID SSRI Prednisone Proton pump inhibitor Erythropoietin
33 (10%) 22 ( 7%) 24 ( 7%) 124 (37%) 5 ( 2%)
Symptoms*** Unknown 87 (34%) No symptoms or complaints 39 (12%) Constitutional symptoms
Fatigue Dyspnoea Cardiac complaints Dizziness or syncope Weight loss
170 (51%) 82 (25%) 73 (22%) 38 (11%) 49 (15%) 23 (7%)
Upper digestive tract symptoms
Heart burn Diminished appetite Melaena Nausea and/or vomiting
39 (12%) 14 (4%) 13 (4%) 11 (3%) 5 (2%)
Lower digestive tract symptoms
Visible rectal blood loss Altered bowel habits Abdominal pain
57 (17%) 17 (5%) 23 (7%) 18 (5%)
MCV mean corpuscular volume, NSAID non‐steroidal anti‐inflammatory drugs, SSRI selective serotonin reuptake inhibitors // *Reference values: Haemoglobin male 8.5‐11/0 mmol/l, female 7.5‐10.0 mmol/l; MCV 80‐100 fl; Ferritin 45‐250 ug/l. // **This is equivalent to 9.7 g/dL (range 3.8‐11.1 g/dL) //*** The 138 patients for whom anaemia was ascertained by the primary care physician and not referred to hospital were excluded, leaving 333 evaluable patients. Multiple complaints per patient were possible.
98

Octogenarians with iron‐deficiency anaemia
Table 2: Multivariable analysis of factors associated with performing of endoscopic procedures
Univariate Multivariable
Factor OR 95% CI p= OR 95% CI p=
Female sex 0.41 0.27‐0.62 <0.001 0.57 0.32‐0.91 0.02 Age >90 years 0.25 0.14‐0.46 <0.001 0.34 0.17‐0.69 0.003 Charlson 1.06 0.89‐1.27 0.5 Polypharmacy 1.30 0.84‐2.02 0.2 Use of anticoagulants 0.94 0.60‐1.48 0.8 Gastro‐intestinal symptoms 2.28 1.39‐3.74 0.001 2.34 1.38‐3.96 0.002 Haemoglobin level <6.0 mmol/l 1.63 1.12‐2.37 0.01 ‐ Ferritin level ≤12 mmol/l 1.36 0.94‐1.98 0.11 ‐ Median Corpuscular Volume <80 fl 1.35 0.92‐2.00 0.13 ‐
Table 3. Initial diagnostic procedures for anaemia and their outcomes
Procedure Outcome n= (%)
Gastroduodenoscopy Performed in 133 patients (28%)
No abnormalities Benign cause of anaemia Malignancy
78 (59%) 46 (34%) 9 ( 7%)
Colonoscopy/Sigmoidoscopy Performed in 135 patients (29%)
No abnormalities Benign cause of anaemia Malignancy*
83 (61%) 31 (23%) 31 (23%)
Imaging studies only Performed in 19 patients (4%)
No abnormalities Gastrointestinal malignancy Other malignancy
13 (68%) 4 (21%) 2 (11%)
Overall n= 471
No referral No initial work‐up No cause identified Benign cause of anaemia Gastrointestinal malignancy
138 (29%) 138 (29%) 95 (20%) 55 (12%) 45 (10%)
*
An additional 2 malignancies were identified with CT‐scan after incomplete colonoscopy
Treatment and outcome Pharmaceutical treatment of anaemia was initiated in 160 patients (34%), including iron
supplements in 146 patients (31%), Helicobacter eradication treatment in six patients (1%)
and proton pump inhibitors (PPIs) in 44 patients (9%). Of these 44, only eight had been
diagnosed with ulcerative lesions in the upper digestive tract; 31 had had no diagnostic
work‐up and five received PPI despite an unremarkable gastroduodenoscopy. Blood
transfusion was required for 219 patients (46%), of which 101 required repeated
transfusions (21%). Surgery was performed in 25 of the 32 patients initially diagnosed with
colon cancer (78%) and for nine of the 15 patients diagnosed during follow‐up (60%). Four
of the six patients with rectal cancer received radiotherapy (66%) and three of the nine
patients with upper gastro‐intestinal tract cancer were treated with chemotherapy (33%).
The remaining 20 patients diagnosed with gastro‐intestinal cancer and all patients
diagnosed with cancer outside the digestive tract received supportive care only.
99

Chapter 7
Table 4: Outcome per diagnosis
Diagnosis % recovery of anaemia
% requiring blood transfusion
Median survival
No diagnosis 49% 40% 3.2 years Benign cause upper gastrointestinal tract 70% 53% not reached
Benign cause lower gastrointestinal tract 38% 80% 3.3 years Malignancy lower gastrointestinal tract 47% 75% 3.0 years Malignancy upper gastrointestinal tract 22% 67% 1.1 years Malignancy outside of gastrointestinal tract 50% 70% 1.3 years
p‐value <0.001 0.10 <0.001
Figure 1a: Kaplan Meier survival plots per initial diagnosis
Log rank p<0.001
1. Benign cause upper gastrointestinal tract 2. Benign cause lower gastrointestinal tract 3. No diagnosis 4. Malignancy lower gastrointestinal tract 5. Malignancy upper gastrointestinal tract 6. Malignancy outside of gastrointestinal tract
100

Octogenarians with iron‐deficiency anaemia
Figure 1b: Kaplan Meier survival plots comparing patients with colon cancer who undergo surgery with those who do not
Median survival Surgery: 2.2 years No surgery: 1.5 years Log rank p=0.05
Prognosis varied greatly depending on the initial diagnosis (p<0.001, Table 4).
Haemoglobin levels normalized for 232 patients (49%); this was most likely in patients
with a benign upper digestive tract cause of anaemia (recovery rate 70%), and least likely
in case of a malignancy of the upper digestive tract (22%, Table 4).
During a median follow‐up of 3.0 years (range 1.4‐4.4 years), 220 patients died (47%).
Survival per diagnosis is shown in Figure 1a. Patients with a benign upper gastrointestinal
tract cause of the iron‐deficiency anaemia demonstrated the best survival (median not
reached, Table 4); patients with a benign cause located in the colon, a colon malignancy or
those without a diagnosis demonstrated an intermediate prognosis (median survival 3.0‐
3.3 years); and patients with an upper gastrointestinal tract malignancy or a malignancy
outside the gastrointestinal tract that caused iron‐deficiency anaemia had a poor
prognosis (median survival 1.1‐1.3 years, p<0.001).
101

Chapter 7
For the 34 patients receiving surgery for colon cancer, thirty‐day mortality was 15% (5 out
of 34) and one‐year mortality was 26% (9 of 34). One‐year mortality for patients with
colon cancer who did not undergo surgery was 17%. However, after 1.3 years the survival
benefit of patients undergoing surgery became apparent (Figure 1b), and median survival
for these patients was 1.0 years longer than for colon cancer patients those who did not
ceive surgery (p=0.05). re
Discussion The aim of this study was to evaluate current clinical practice for octogenarians with iron‐
deficiency anaemia by assessing referral patterns and diagnostic choices, the clinical
consequences of omission of endoscopy, and the risks and benefits of IDA‐related surgery.
We found that in 59% of patients no initial diagnostic procedures were performed. A
cause of anaemia was identified in 50% of patients undergoing an initial work‐up. Of the
61 gastrointestinal malignancies that were identified in this cohort, sixteen were found
during follow‐up, often in patients for whom initial diagnostic work‐up was limited or
omitted. In case of colon cancer, perioperative mortality was 15%, and benefit of surgery
compared to supportive care was not apparent until 1.3 years after ascertainment of iron‐
deficiency anaemia.
Few prior studies have assessed diagnostic choices in IDA in a population‐based cohort of
elderly patients. One study addressed adult patients of all ages diagnosed with iron‐
deficiency by the general practitioner and found that 69% of those patients did not
undergo any anaemia‐related work‐up,12 while another study found that of patients aged
40 years and older with IDA, also diagnosed by the general practitioner, only 35% received
a relevant referral for further analysis.13 These percentages are comparable to what we
found, suggesting that the lack of diagnostic procedures and referral in our patient cohort
is not entirely an age‐related issue. However, we did find that for patients aged 90 years
and older, the likelihood of endoscopic assessment in case of iron‐deficiency decreased
greatly.
In geriatric medicine, making a diagnosis is not a goal in itself, but rather a means towards
optimizing quality of life and survival; therefore, an undiagnosed cause of IDA is
acceptable if its ascertainment has no therapeutic consequences. In this study, the main
diagnosis‐related treatment choices were surgery for colon cancer and proton pump
inhibitors (PPIs). However, many patients were given PPIs even if no such erosive lesions
were found or no work‐up was done, and therefore the question remains whether these
patients would not also have received this treatment if no gastroduodenoscopy was
performed. For this reason, it seems that the primary benefit of a work‐up for IDA in
octogenarian patients would be to identify colon cancer as early as possible, so that
surgery can be performed before disease progression limits the resectability of the
102

Octogenarians with iron‐deficiency anaemia
tumour, potentially resulting in a poorer prognosis.14 However, one could question
whether the risks of delayed diagnosis of colon cancer would have justified performing a
colonoscopy in the 336 patients in our cohort that did not undergo this procedure during
the initial work‐up. Colonoscopy does not exclude a delayed diagnosis and is not without
risk: in addition to the 1.5% of patients that suffered an iatrogenic bowel perforation
during endoscopy in our cohort, 2% of patients that did have a colonoscopy were
nonetheless diagnosed with colon cancer during follow‐up.
In addition, if the patient is considered not fit enough or unwilling to undergo surgery
should a colon cancer be found, the benefit of making an early diagnosis is nullified.
Perioperative mortality for elderly patients undergoing colon surgery is high (10‐15%),15‐17
and these patients remain at an excess risk for mortality during the first year after
surgery.16 In our cohort, surgical benefit compared to best supportive care did not become
apparent until approximately 1.3 years after initial ascertainment of iron‐deficiency
anaemia. As omission of surgery is frequently related to comorbidity and poor general
health,15 the remaining life expectancy of these patients was likely to be shorter
irrespective of cancer and cancer treatment, and the surgical risks would generally have
been higher. Therefore, omission of surgery in case of poor general health and in the
presence of comorbidity that limits the remaining life‐expectancy seems legitimate.
Similarly, if the outcome of endoscopy will have no clinical consequences, the risks and
burden of endoscopy mean that withholding such diagnostic procedures is acceptable. On
the other hand, it is important to realize that estimation of life‐expectancy is notoriously
difficult,18 particularly in the very elderly who can experience a persistent level of disability
and frailty over an extended period of time, before succumbing to a minor illness due to
lack of physical reserves.19
Future research should focus on developing predictive models that will aid in estimating
potential benefits and risks of further examination of IDA and/or surgery for colon cancer
in elderly patients. Recently published data on the predictive value of the presence of
geriatric syndromes, such as functional limitations, polypharmacy, cognitive impairment,
and depressive symptoms for predicting prognosis and treatment‐related risks for older
cancer patients seem promising,22‐27 but more research is needed to clarify the exact role
of these geriatric conditions in the decision‐making process. Studies should also include
patient‐centred outcome measures, such as quality of life and functional independence, as
these are often considered of greater importance by elderly patients than survival
itself.20,21 Development of such models will allow for more precise tailoring of care to
prevent unnecessary or non‐beneficial procedures as well avoidable delays in diagnosis.
This study has several limitations. First, we have assumed that all diagnostic procedures in
these patients were performed at the Gelre hospitals. Over 95% of the patients in this
cohort had had at least one or more appointments with medical specialists based in this
103

Chapter 7
hospital, but this does not exclude the possibility that some patients were referred to
other centres for the diagnostic work‐up. A second limitation is that many different
definitions of iron‐deficiency anaemia exist, with different cut‐off values and laboratory
measurements.28,29 The composition of the patient cohort will change depending on the
definition that is used, which could alter the prevalence of the various causes of iron‐
deficiency anaemia and thus clinical outcome. This could limit the possibility to generalise
our results to other patient cohorts. A third limitation is that cause of death was
frequently unknown and we were therefore unable to calculate a cause‐specific mortality.
Finally, as this was a retrospective study, available data were limited to what was recorded
the patient’s charts. in
In conclusion, omission of endoscopy for iron‐deficiency anaemia and omission of surgery
for colon cancer occur frequently in octogenarians, and appears legitimate in the presence
of relevant comorbidity and in case of limited remaining life‐expectancy. Further research
is needed to determine which baseline factors should guide decision making to optimize
outcome and quality of life.
104

Octogenarians with iron‐deficiency anaemia
References 1. Joosten E, Pelemans W, Hiele M et al. Prevalence and causes of anaemia in a geriatric hospitalized
population. Gerontology 1992;38:111‐117. 2. Luman W, Ng KL. Audit of investigations in patients with iron deficiency anaemia. Singapore Med J
2003;44:504‐510. 3. Lindsay JO, Robinson SD, Jackson JE, Walters JR. The investigation of iron deficiency anaemia‐‐a hospital
based audit. Hepatogastroenterology 1999;46:2887‐2890. 4. Stephens MR, Hopper AN, White SR et al. Colonoscopy first for iron‐deficiency anaemia: a Numbers Needed
to Investigate approach. QJM 2006;99:389‐395. 5. Majid S, Salih M, Wasaya R, Jafri W. Predictors of gastrointestinal lesions on endoscopy in iron deficiency
anaemia without gastrointestinal symptoms. BMC Gastroenterol 2008;8:52. 6. Chatrenet P, Friocourt P, Ramain JP et al. Colonoscopy in the elderly: a study of 200 cases. Eur J Med
1993;2:411‐413. 7. Lukens FJ, Loeb DS, Machicao VI et al. Colonoscopy in octogenarians: a prospective outpatient study. Am J
Gastroenterol 2002;97:1722‐1725. 8. Avgerinos DV, Llaguna OH, Lo AY, Leitman IM. Evolving management of colonoscopic perforations. J
Gastrointest Surg 2008;12:1783‐1789. 9. Jafri SM, Arora A. Silent perforation: an iatrogenic complication of colonoscopy. Surg Laparosc Endosc
Percutan Tech 2007;17:452‐454. 10. Jafri SM, Monkemuller K, Lukens FJ. Endoscopy in the elderly: a review of the efficacy and safety of
colonoscopy, esophagogastroduodenoscopy, and endoscopic retrograde cholangiopancreatography. J Clin Gastroenterol 2010;44:161‐166.
11. Charlson ME, Pompei P, Ales KL, Mackenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987;40:373‐383.
12. Droogendijk J, Beukers R, Berendes PB et al. Screening for gastrointestinal malignancy in patients with iron deficiency anaemia by general practitioners: an observational study. Scand J Gastroenterol 2011;46:1105‐1110.
13. Damery S, Ryan R, Wilson S et al. Iron deficiency anaemia and delayed diagnosis of colorectal cancer: a retrospective cohort study. Colorectal Dis 2011;13:e53‐e60.
14. Weiser MR, Landmann RG, Kattan MW et al. Individualized prediction of colon cancer recurrence using a nomogram. J Clin Oncol 2008;26:380‐385.
15. Jonker JM, Hamaker ME, Soesan M et al. Colon cancer treatment and adherence to national guidelines: does age still matter? J Geriatr Oncol 2012;3:131‐137.
16. Gooiker GA, Dekker JW, Bastiaannet E et al. Risk Factors for Excess Mortality in the First Year After Curative Surgery for Colorectal Cancer. Ann Surg Oncol 2012.
17. Cull JD, Kukreja S, Hieken TJ. Surgical treatment of colorectal cancer in the advanced elderly: does outcome justify treatment? J.Clin.Oncol. ASCO meeting abstracts 2012:3629.
18. Christakis NA, Lamont EB. Extent and determinants of error in physicians' prognoses in terminally ill patients: prospective cohort study. West J Med 2000;172:310‐313.
19. Gill TM, Gahbauer EA, Han L, Allore HG. Trajectories of disability in the last year of life. N Engl J Med 2010;362:1173‐1180.
20. Yellen SB, Cella DF, Leslie WT. Age and clinical decision making in oncology patients. J Natl Cancer Inst 1994;86:1766‐1770.
21. Steinhauser KE, Christakis NA, Clipp EC et al. Factors considered important at the end of life by patients, family, physicians, and other care providers. JAMA 2000;284:2476‐2482.
22. Arnoldi E, Dieli M, Mangia M et al. Comprehensive geriatric assessment in elderly cancer patients: an experience in an outpatient population. Tumori 2007;93:23‐25.
23. Bamias A, Lainakis G, Kastritis E et al. Biweekly carboplatin/gemcitabine in patients with advanced urothelial cancer who are unfit for cisplatin‐based chemotherapy: report of efficacy, quality of life and geriatric assessment. Oncology 2007;73:290‐297.
24. Basso U, Tonti S, Bassi C et al. Management of Frail and Not‐Frail elderly cancer patients in a hospital‐based geriatric oncology program. Crit Rev Oncol Hematol 2008;66:163‐170.
105

Chapter 7
106
25. Tucci A, Ferrari S, Bottelli C et al. A comprehensive geriatric assessment is more effective than clinical judgment to identify elderly diffuse large cell lymphoma patients who benefit from aggressive therapy. Cancer 2009;115:4547‐4553.
26. Kristjansson SR, Nesbakken A, Jordhoy MS et al. Comprehensive geriatric assessment can predict complications in elderly patients after elective surgery for colorectal cancer: a prospective observational cohort study. Crit Rev Oncol Hematol 2010;76:208‐217.
27. Cheema FN, Abraham NS, Berger DH et al. Novel approaches to perioperative assessment and intervention may improve long‐term outcomes after colorectal cancer resection in older adults. Ann Surg 2011;253:867‐874.
28. Choi CW, Cho WR, Park KH et al. The cutoff value of serum ferritin for the diagnosis of iron deficiency in community‐residing older persons. Ann Hematol 2005;84:358‐361.
29. Beutler E, Waalen J. The definition of anaemia: what is the lower limit of normal of the blood hemoglobin concentration? Blood 2006;107:1747‐1750.

Chapter 8
Age‐related differences in guideline adherence for head and neck cancer
M.E. Hamaker, C.H. Smorenburg, R.J. Bun, G.T. de Kuyper, B.C. van Munster, S.E. de Rooij,
B.M. Wiarda, N.G. Breeuwsma, J.M. Uppelschoten
In print: Journal of Geriatric Oncology

Chapter 8
Abstract Background: The aim of this study was to examine which factors influence guideline
adherence and to determine the impact of non‐adherence on survival.
Patients and methods: Cohort of 606 patients (median age 65.3 years) newly diagnosed
with head and neck cancer at Medical Centre Alkmaar between 1997 and 2009. Treatment
was compared to guideline recommendations. Multivariable analyses were performed to
determine factors associated with non‐adherence and associated outcome.
Results: Ninety‐one percent of patients were treated in accordance with guidelines for
head and neck cancer. Reasons for discordant treatment were comorbidity, lack of
cooperation in patients aged <70 years, and patients’ refusal to undergo recommended
treatment. Age (OR 1.40 95%CI 1.04‐1.87), comorbidity (OR 1.68, 95%CI 1.32‐2.13) and
advanced disease (OR 1.83, 95%CI 1.46‐2.28) were independently associated with non‐
adherence. Five‐year overall survival was 64% for accordant treatment and 16% for
discordant treatment (p<0.001). Higher age (HR 1.03, 95%CI 1.01‐1.04), advanced stage
(HR 1.36, 95%CI 1.21‐1.53), recurrent disease (HR 3.29, 95%CI 1.97‐5.52) and treatment
discordant with guidelines (HR 3.22, 95%CI 2.15‐4.85) were independently associated with
cancer‐specific mortality.
Conclusion: Discordance with guidelines occurred in less than 10% of patients at our
centre and was associated with age, tumour stage, comorbidity and a significantly poorer
cancer‐specific survival.
108

Age‐related differences in head and neck cancer treatment
Introduction Head and neck cancers are the sixth most common malignancy and account for 6% of
cancer deaths.1 Worldwide, over 650,000 new cases of head and neck cancer are
diagnosed and 350,000 patients die of these types of malignancies every year.1 In the
Netherlands, over 3,000 new patients are diagnosed every year.2 The majority of new
cases occur in patients aged 50 years and older, primarily because of its relationship with
chronic tobacco and alcohol exposure.3,4 Approximately 25% of these patients are aged 70
and over.3,5 However, in the coming decades, the number of older patients with cancer
will increase substantially, as a result of increasing life expectancy and ageing of the
population.6
Due to the anatomical complexity of the head and neck region, and the high impact of
head and neck cancer and its treatment on quality of life, treatment decisions are
complex. Radical surgical treatment is often mutilating, while the effect of uncontrolled
disease on the patient’s speech, swallowing and breathing is devastating and often fatal.5
Although more aggressive treatment provides gains in terms of locoregional control and
disease recurrence,7 it can also have a negative impact on vital organ functions and quality
of life.8‐10 Moreover, patients with head and neck cancer often suffer from other alcohol‐
and tobacco related diseases, such as cardiac and respiratory illnesses, second primary
tumours, hepatic or metabolic diseases, as well as cognitive disorders,3,5,11 that may
decrease their resilience, quality of life and treatment tolerance.4,11‐15
As a result, older patients and those with comorbidity are often given a modified
treatment in an attempt to avoid treatment‐related complications and mortality.16‐19
Although this increases the risk of recurrent or metastatic disease in time,20 limited life
expectancy and competing causes of death could also mean that a patient does not live
long enough to suffer from this increased risk. In this case, more radical treatment would
be unnecessarily aggressive. On the other hand, there are concerns that elderly patients
are undertreated purely because of their age.21 Finding the right balance between
undertreatment and overtreatment for this vulnerable patient group presents a major
challenge and requires thorough knowledge of the potential benefit and risks of the
available treatment options.
The aim of this study was to examine which factors influence guideline adherence in
patients with head and neck cancer and to determine the impact of non‐adherence on
verall and cancer‐specific survival. o
Methods At the Medical Centre Alkmaar, a large teaching hospital, all medical charts of patients
treated for newly diagnosed head and neck cancer between 1997 and 2009 were
reviewed. Patients with a first presentation of a primary squamous cell carcinoma (SCC) of
109

Chapter 8
the oral cavity, lip, larynx, hypopharynx or oropharynx were included. Rare types of head
and neck cancer, such as salivary gland tumours, lymphomas and sarcomas were excluded
from our analysis.
The following data were collected: age at diagnosis, tumour localisation, stage of disease
(TNM), as well as the initial treatment with radiotherapy surgery and/or chemotherapy.
Comorbidity was scored using the Charlson comorbidity index;22 the current tumour was
not included in the score. Stage of disease was classified in seven groups: in situ, stage I
(T1 N0 M0), stage II (T2 N0 M0), stage III (T3 N0‐1 M0 or T1‐2 N1 M0), stage IVab (T4Nany M0,
TanyN2‐3 M0), stage IVc (TanyNany M1), and unknown. Staging was standardized for all
try. Cause of death was extracted from the data of the Central Bureau of
atistics.
for
the Cox regression
nalysis, adherence to guidelines and disease recurrence were added.
patients.
Delivered treatment modalities were compared with treatment advised by national
guidelines. In the Netherlands, treatment guidelines have been developed by the Dutch
Head and Neck Cancer Cooperative Working Group (NWHHT). A summary of these
guidelines per tumour localisation can be found in Appendix 1. Evaluation of guideline
adherence was done without knowledge of the patient’s survival status. For patients not
receiving the standard treatment, reasons stated by the treating physician for non‐
adherence to guidelines were subsequently collected from the charts; these were
subsequently classified as comorbidity, poor general condition, tumour characteristics,
patient’s refusal (if the patient chose not to have recommended treatment), and lack of
cooperation (if planned treatment could not be carried out due to patient factors, such as
failure to show up for treatment). Follow‐up data were retrieved after 1, 2 and 5 years
from the patient’s chart. For each time point, mortality was assessed, as was the presence
of disease recurrence in patients still alive. Mortality was determined using the Municipal
ata RegisD
St
Statistical analysis To assess differences between age groups and differences in guideline adherence
between various subgroups, the SPSS (Statistical Package for the Social Sciences) version
16.0 was used. The chi‐square test was used for nominal and ordinal variables. For
continuous variables with a normal distribution, the Student t‐test was used; and
continuous variables with a non‐normal distribution the Mann‐Whitney test was used.
A logistic regression analysis was performed to determine factors associated with
treatment discordance. To determine which factors were associated with mortality, a Cox
regression analysis was performed. For both, a backward selection procedure was applied,
accepting a p‐value <0.05. The following factors were included: age at diagnosis, stage of
disease, tumour localisation, Charlson comorbidity score, and sex; for
a
110

Age‐related differences in head and neck cancer treatment
Results
65.3 years (range 23.6‐95.9 years); 220 patients
e frequently in
or prior malignancy (within
e years prior to inclusion) was observed in 9% of patients.
ent.
guidelines more often suffered from heart failure (12% vs. 2% in patients receiving
Patient and tumour characteristics Between January 1997 and December 2009, 757 new patients were seen by the
multidisciplinary head and neck cancer team. After exclusion of 153 patients (recurrent
disease or second primary tumour n=41, tumour location outside predefined area n=112),
a total of 604 patients were analysed. Patients and tumour characteristics are listed in
Table 1. Median age at diagnosis was
were aged 70 years or older (36%).
Tumour localisation varied with age; younger patients more often had oropharyngeal or
hypopharyngeal cancer, while cancer of the larynx and lip occurred mor
older patients (p<0.001). Stage of disease did not differ with age (p=0.47).
Data on comorbidity were available for 548 patients (91%). Mean Charlson index score
was 0.77 (SD 1.07) and increased over the age of 70 years. Table 2 lists the conditions
included in the Charlson index. Myocardial infarction was the most common comorbid
condition (11% of patients), followed by diabetes (9.5%), chronic pulmonary disease
.5%) and peripheral vascular disease (6.7%). A concurrent(7
fiv
Treatment choices Data on treatment was incomplete for three patients. Of the remaining 601 patients, 545
were treated in accordance with treatment guidelines (91%). Surgery was recommended
for 302 patients, and was performed in 276 (90%), but 3 patients only received local
treatment where locoregional treatment was recommended (1%). For radiotherapy, 310
out of 342 patients for whom it was recommended received full radiation treatment
(91%); 17 patients received only part of recommended dose (5%) and 20 did not receive
any radiotherapy (6%). Guidelines recommended either surgery or radiotherapy in 168
patients, of whom 60 received surgical therapy (36%), 72 radiotherapy (43%), 30 received
both (18%) and 6 had no therapy (4%). Chemotherapy was required in 97 patients
(concomitant n=73, induction n=24), and was given to 89 (92%), all of which received all
planned courses. Only 3% of patients (n=19) did not receive any form of treatm
Compliance to guidelines did not change in the course of the study period (p=0.763).
Increased age (odds ratio (OR) 1.40 95% confidence interval (CI) 1.04‐1.87 p=0.025), more
comorbidity (OR 1.68, 95%CI 1.32‐2.13 p<0.001) and more advanced disease (OR 1.83,
95%CI 1.46‐2.28, p<0.001) were independently associated with non‐adherence. This trend
was seen in all treatment modalities (Figure 1). Patients not treated in accordance with
111

Chapter 8
Table 1: Baseline characteristics per age group
All <70 years 70‐79 years 80+ years p‐value*
Number of patients 604 384 (63%) 148 (25%) 72 (12%)
% male 72.9% 74.5% 80.3% 50.0% 0.001
Mean Charlson score (SD) % without comorbidity % missing
0.77 (1.07) 55.8% 9.4%
0.60 (1.01)64.9%9.1%
1.16 (1.21)40.1%9.0%
1.03 (1.21) 40.3% 11.4%
0.001 <0.001
Tumour localisation Oropharynx Hypopharynx Lip Oral cavity Larynx
14.6% 5.8%
15.6% 34.8% 29.3%
18.8%7.6%
11.5%36.5%25.8%
10.1%2.0%
18.2%29.1%40.5%
2.8% 4.2%
31.9% 36.1% 25.0%
<0.001
Tumour stage In situ Stage I Stage II Stage III Stage IVab Stage IVc Stage unknown
1.7%
33.8% 18.8% 14.5% 27.3% 2.5% 1.3%
1.8%29.9%19.5%15.4%28.9%3.1%1.3%
2.0%40.5%14.9%14.2%24.3%2.7%1.4%
0%
40.3% 22.2% 11.1% 25.0%
0% 1.4%
0.47
* A ‐value < 0.05 is considered significant Table 2: Charlson comorbidity index
22, not including current cancer
Condition
Index factor
All patients
n=548
Treatment accordant with guidelines n=499
Treatment discordant with
guidelines n=49
p‐value**
Myocardial infarction 1 58 11% 55 11% 3 6% 0.21 Heart failure 1 14 3% 8 2% 6 12% 0.001 Peripheral vascular disease 1 36 7% 34 7% 2 4% 0.34 Cerebrovascular accident 1 23 4% 17 3% 6 12% 0.01 Dementia 1 14 3% 7 1% 7 14% <0.001 Chronic pulmonary disease 1 41 8% 37 7% 4 8% 0.51 Connective tissue disease 1 10 2% 9 2% 1 2% 0.61 Ulcer 1 10 2% 10 2% 0 0% 0.39 Chronic liver diseases or cirrhosis 1 6 1% 5 1% 1 2% 0.43 Diabetes mellitus 1 38 7% 35 7% 3 6% 0.55 Diabetes with organ complications 2 14 3% 12 2% 2 4% 0.36 Hemiplegia 2 3 1% 3 1% 0 0% 0.76 Kidney disease 2 10 2% 10 2% 0 0% 0.39 Cancer* 2 48 9% 39 8% 8 16% 0.05 Leukaemia or lymphoma 2 4 1% 3 1% 1 2% 0.31 Moderate to severe liver disease 3 6 1% 2 1% 4 8% 0.001 Metastases* 6 1 0% 1 0% 0 0% 0.91 AIDS 6 0 0% 0 0% 0 0% ‐ * not including current cancer ; ** a p‐value < 0.05 was considered significant (printed in bold)
112

Age‐related differences in head and neck cancer treatment
Figure 1: Association between baseline characteristics and guideline adherence a. Age
*In the treatment guidelines, chemotherapy is stated as “not mandatory” for patients aged 70 and over. b. Stage of disease
c. Comorbidity
113

Chapter 8
recommended treatment, p=0.001, Table 2), a cerebrovascular accident (12% vs. 3%,
p=0.01), dementia (14% vs. 1%, p<0.001), a previous malignancy (18% vs. 9%, p=0.05) and
moderate to severe liver dysfunction (8% vs. 0%, p=0.001).
For 44 out of the 62 patients not treated in accordance with guidelines, the motivation
behind this decision was stated in the patient’s chart. Reasons mentioned were
comorbidity in 20 patients (45%), poor general condition in 12 patients (27%), lack of
cooperation in two patients (5%), tumour characteristics in one patient (2%), while 14
patients stated they did not wish to undergo the recommended treatment (32%). In
patients aged < 70 years, comorbidity and lack of cooperation were the most important
reasons for non‐adherence, while in older patients, particularly in those over 80 years old,
discordance was more often due to patient’s refusal of treatment (two out of 386 patients
aged < 70 years (1%), four of 148 patients aged 70‐79 years (3%) and seven of 72 patients
ged 80 and over (10%); p=0.022). a
Outcome Median follow‐up in this study was 3.1 years (range 0‐5 years); five year follow‐up was
available for 64% of patients. Overall survival and cancer specific survival are listed in
Table 3. For patients not receiving standard treatment, death occurred most frequently
during the first year after diagnosis (one‐year overall survival 42%) while for patients that
did receive recommended treatment, mortality was more spread out (Figure 2).
Of patients still alive, the number of patients without disease recurrence was 90% at one
year (397 of 442 patients), 87% at two years (294 of 338) and 74% at five years (120 of
161), resulting in a disease‐free survival of 74%, 65% and 51% respectively. Disease
recurrence was only associated with stage of disease (OR 1.39, 95% CI 1.14‐1.50; p=0.001).
It was not associated with guideline discordance (p=0.511).
Data on cause of death was not retrievable for five patients (2%). Cause of death was
directly related to the head and neck cancer in 122 of the remaining 228 deceased
patients (54%). Other malignancies were cause of death in 52 patients (23%) and
cardiovascular disease was the major non‐oncological contributor (27 patients, 12%).
Cancer‐specific survival, stratified for guideline adherence, is listed in Table 3. Cause of
death did not differ for patients treated in accordance with guidelines compared to those
receiving discordant treatment (p=0.787).
In the multivariable Cox regression analysis, which included sex, age at diagnosis, stage of
disease, tumour localisation, Charlson comorbidity score, adherence to guidelines and
disease recurrence, higher age (hazard ratio (HR) 1.03, 95%CI 1.01‐1.04; p=0.009), more
advanced stage (HR 1.36, 95%CI 1.21‐1.53; p<0.001), recurrent disease (HR3.29, 95%CI
1.97‐5.52; p<0.001) and treatment discordant with guidelines (HR 3.22, 95%CI 2.15‐4.85:
p<0.001) were independently associated with cancer‐specific mortality.
114
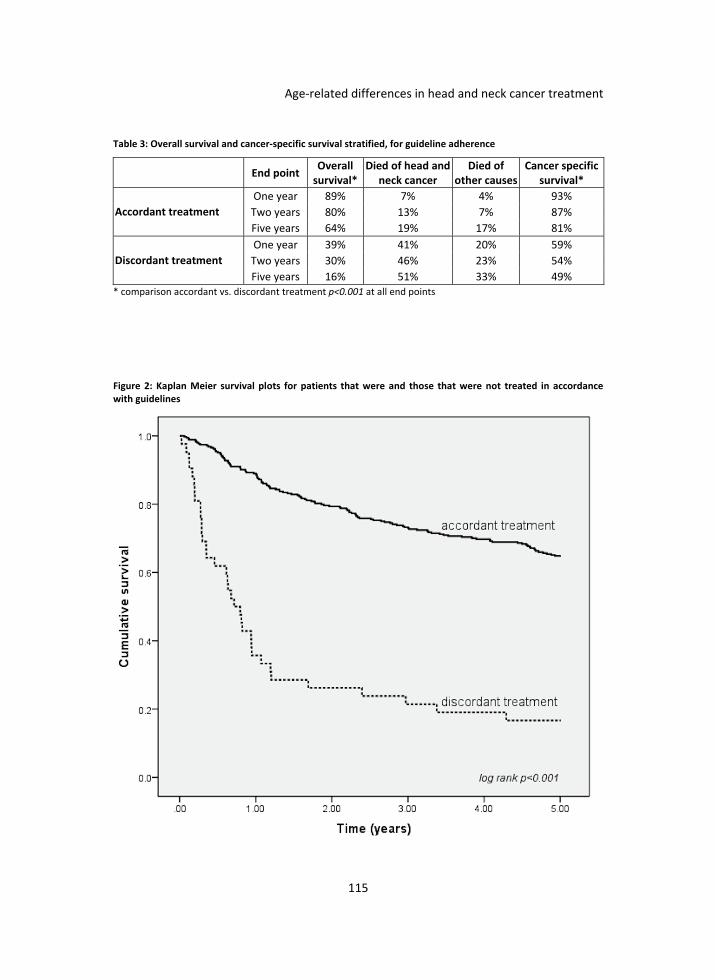
Age‐related differences in head and neck cancer treatment
Table 3: Overall survival and cancer‐specific survival stratified, for guideline adherence
End point Overall survival*
Died of head and neck cancer
Died of other causes
Cancer specific survival*
One year 89% 7% 4% 93%
Two years 80% 13% 7% 87% Accordant treatment
Five years 64% 19% 17% 81%
One year 39% 41% 20% 59%
Two years 30% 46% 23% 54% Discordant treatment
Five years 16% 51% 33% 49% * comparison accordant vs. discordant treatment p<0.001 at all end points
Figure 2: Kaplan Meier survival plots for patients that were and those that were not treated in accordance with guidelines
115

Chapter 8
Discussion In this study, we examined adherence to treatment guidelines in a cohort of 604
consecutive patients newly diagnosed with head and neck cancer and found that
guidelines were followed in over 90% of patients. Guideline adherence decreased in
patients aged > 70 years. Non‐adherence was also associated with stage and comorbidity.
After correction for potential confounders, non‐adherence resulted in significantly poorer
overall and cancer specific survival.
This study has several limitations. Because of its retrospective nature, the usual limitations
associated with data collection and missing values apply. In particular, data on
comorbidity were limited to what was recorded in patient’s medical charts; for 10% of
patients, no data were available. For the same reason, we were unable to include data
such as functional or socio‐economic status, which could potentially have affected
guideline compliance. As patient’s charts were used as a data source, data extraction was
not entirely blinded to outcome. In addition, although the received treatment was
compared to site‐ and stage‐specific treatment guidelines, there are various details of
treatment decision making that were not incorporated in the assessment of guideline‐
compliant treatment. Another potential limitation is that the patient sample was accrued
over an extended period of time; however, no major changes were made in the Dutch
treatment guidelines in the study period. Furthermore, it is difficult to determine
retrospectively whether the decision to modify treatment in a particular patient is
justifiable.
We are aware of only two previous studies that have compared actual treatment to
guidelines with stage‐specific treatment recommendations in newly diagnosed head and
neck cancer patients. Sanabria et al. reported guideline adherence in 312 patients with
head and neck cancer aged 70 and older and found 80% was treated in accordance to
guidelines.19 Derks et al. observed a guideline adherence of 62% in 78 patients aged 70
and older and 89% in 105 patients aged 45‐60 years of age.17 Likewise, we found age to be
an independent predictor of guideline discordance, but overall adherence rates were
better (80% for patients aged > 70 years versus 94% in younger patients).
A possible explanation for decreased guideline adherence in older patients is the
increased presence of comorbidity. This is particularly true in head and neck cancer,
because its association with smoking and alcohol consumption puts patients at risk for
other lifestyle‐related diseases. As has been shown in other studies,4,17,19 comorbidity
increased with age (Table 1) and was a major factor associated with treatment
discordance, both in the multivariate analysis as well as in the reasons for deviating from
the guideline stated in the patient’s chart. In previous studies, the presence of comorbid
diseases has been found to result in more complications and decreased tolerance of
surgery,15,23‐25 radiation therapy,14 and chemotherapy.26 Therefore, adjusting treatment in
116

Age‐related differences in head and neck cancer treatment
patients with significant comorbidity seems appropriate. Furthermore, in the first year
after diagnosis, we found that 20% of patients not treated in accordance with guidelines
died of causes other than the head and neck cancer, increasing to 33% of patients after
five years. In these patients, standard treatment could have been unnecessarily
aggressive. Despite this, cancer‐specific survival was severely compromised in patients
receiving discordant treatment (Table 3), suggesting the need for stricter guideline
adherence.
However, we also found that discordance with guidelines was often at patients’ request,
particularly in older patients: over 10% of those aged > 80 years refused the offered
treatment. Similarly, Derks et al. found that 9% of patients aged 70‐79 years and 18% of
those aged 80 years refused treatment.17 In another study, refusal increased from 2% in
patients younger than 75 years to 8% in those over 75 years.27 Refusal of treatment in
newly diagnosed older patients with cancer has been shown to be associated with
baseline functional impairment,28 or living alone.17,28 Furthermore, elderly patients often
prefer quality of life to length of life,17,29 and treatment‐related functional impairment is
feared more than death.30 As studies have shown that older patients experience poorer
outcomes for chewing,10 swallowing,31 speech10,31 and physical functioning,7,10,31 compared
to younger patients, and 32% of older patients experience incomplete recovery after one
year, this fear is not unrealistic.31
However, no studies are available comparing the quality of life and quality of death in
patients receiving discordant treatment to those receiving standard care. Future research
should focus not only on optimizing cancer‐specific survival through increasing guideline
adherence but more importantly on mapping out the short‐ and long‐term effects of head
and neck cancer and its treatment on quality of life. This information is much needed to
uide medical specialists and patients in their decision making. g
In conclusion, discordance with treatment guidelines was less than 10% at our centre, but
increased to 29% in patients aged 80 and over. It was independently associated with a
higher stage of disease and comorbidity and resulted in a significantly worse cancer‐
specific survival. Despite competing causes of death and the need to tailor treatment to
patients’ wishes, this suggests the need for greater guideline adherence. However,
research comparing short‐ and longer‐term quality of life after discordant versus standard
treatment is needed to help patients weigh the risks and benefits of treatment options.
117

Chapter 8
Appendix 1: Treatment guidelines per tumour localisation and stage of disease
Hypopharynx
Treatment recommendation Alternative treatment
Tis‐T2 n0 m0 Local radiotherapy, elective radiotherapy of the neck
T1, T2 n1 m0 Locoregional radiotherapy Locoregional surgery
T1, T2 n2 m0 Locoregional radiotherapy with neck dissection for rest tumour
T1,T2 n3 m0 Neck dissection, local radiation therapy, elective radiation of the neck
T3, T4 n0 m0 Chemoradiation* Surgery with post‐operative (chemo)radiation*
T3,T4 n1‐n3 m0 Chemoradiation* with neck dissection for rest tumour
Primary surgical therapy with post‐ operative (chemo)radiation*
Tany Nany m1 Chemoradiation*
Irresectable Chemoradiation*
* Chemotherapy is not mandatory for patients aged 70 and over.
Oropharynx
Treatment recommendation Alternative treatment
T1 n0 m0 Local surgery Local radiotherapy
T2 n0 m0 Local surgery with unilateral neck radiation Local radiotherapy with unilateral neck radiation
T1 ,T2 n1 m0 Local radiotherapy with unilateral neck radiation
T3,T4 n0 m0 Local surgery with unilateral neck dissection and locoregional neck radiation
T3,T4 n1 m0 Local surgery with local radiotherapy and bilateral neck radiation
Tany n2, n3 m0 Locoregional surgery with local radiotherapy and bilateral neck radiation
Tany Nany m1 Chemoradiation* Local radiotherapy with bilateral neck radiation
Irresectable Chemoradiation* Local radiotherapy with bilateral neck radiation
* Chemotherapy is not mandatory for patients aged 70 and over.
Oral cavity
Treatment recommendation Alternative treatment
Tany n0 m0 Local surgery with elective treatment of neck(radiation or surgery)
Tany n1 m0 Local surgery with unilateral neck dissection Local surgery with unilateral neck
radiotherapy
Tany n2‐n3 m0 Local surgery with bilateral neck dissection and bilateral neck radiation
Tany Nany m1 Chemoradiation*
Irresectable Chemoradiation*
* Chemotherapy is not mandatory for patients aged 70 and over.
118

Age‐related differences in head and neck cancer treatment
Larynx
Treatment recommendation Alternative treatment
T1 n0 m0 Local radiation therapy Local resection
T2 n0 m0 Local radiation therapy and neck radiation
T1,T2 n1 m0 Local radiation therapy and neck radiation
T1,T2 n2,n3 m0 Local radiotherapy with neck dissection and elective neck radiation
T3,T4 n0 m0 (Chemo)radiation* + treatment of neck (radiation or surgery)
T3,T4 n1 m0 (Chemo)radiation* with neck radiation Local surgery, (chemo)radiation* and treatment of neck (radiation/surgery)
T3,T4 n2,n3 m0 Locoregional (chemo)radiation* with neck dissection of rest tumour
Tany Nany m1 Chemoradiation*
* Chemotherapy is not mandatory for patients aged 70 and over.
Lip
Treatment recommendation Alternative treatment
T1‐3 n0 m0 Local surgery or local radiotherapy
T4 n0 m0 Local surgery and local radiotherapy
T1‐3 n1 m0 Local surgery or local radiotherapy with neck dissection
T1‐3 n2,3 m0 Local surgery or local radiotherapy with neck dissection and neck radiation
T4 n1 M0 Local surgery, neck dissection, local radiotherapy
T4 N2,3 m0 Local surgery with neck dissection ad locoregional radiation therapy
Tany Nany M1 (Chemo)radiation*
* Chemotherapy is not mandatory for patients aged 70 and over.
119

Chapter 8
References 1. Parkin DM. Global cancer statistics, 2002. CA Cancer J Clin 2005;55:74‐108. 2. www.ikcnet.nl. 2010. 3. Bernardi D, Barzan L, Franchin G et al. Treatment of head and neck cancer in elderly patients: state of the
art and guidelines. Crit Rev Oncol Hematol 2005;53:71‐80. 4. Reid BC, Alberg AJ, Klassen AC et al. Comorbidity and survival of elderly head and neck carcinoma patients.
Cancer 2001;92:2109‐2116. 5. Argiris A, Karamouzis MV, Raben D, Ferris RL. Head and neck cancer. Lancet 2008;371:1695‐1709. 6. Kamangar F, Dores G, Anderson W. Patterns of cancer incidence, mortality and prevalence across five
continents. J Clin Oncol 2006;24:2137‐2150. 7. van der Schroeff MP, Derks W, Hordijk GJ, de Leeuw RJ. The effect of age on survival and quality of life in
elderly head and neck cancer patients: a long‐term prospective study. Eur Arch Otorhinolaryngol 2007;264:415‐422.
8. Derks W, de L, Jr., Hordijk GJ, Winnubst JA. Elderly patients with head and neck cancer: short‐term effects of surgical treatment on quality of life. Clin Otolaryngol Allied Sci 2003;28:399‐405.
9. Derks W, de Leeuw RJ, Hordijk GJ, Winnubst JA. Quality of life in elderly patients with head and neck cancer one year after diagnosis. Head Neck 2004;26:1045‐1052.
10. Khafif A, Posen J, Yagil Y et al. Quality of life in patients older than 75 years following major head and neck surgery. Head Neck 2007;29:932‐939.
11. Sanabria A, Carvalho AL, Vartanian JG et al. Comorbidity is a prognostic factor in elderly patients with head and neck cancer. Ann Surg Oncol 2007;14:1449‐1457.
12. Derks W, de Leeuw RJ, Hordijk GJ. Elderly patients with head and neck cancer: the influence of comorbidity on choice of therapy, complication rate, and survival. Curr Opin Otolaryngol Head Neck Surg 2005;13:92‐96.
13. Pignon T, Horiot JC, et al. No age limit for radical radiotherapy in head and neck tumours. Eur J Cancer 1996;32A:2075‐2081.
14. Horiot JC. Radiation therapy and the geriatric oncology patient. J Clin Oncol 2007;25:1930‐1935. 15. Boruk M, Chernobilsky B, Rosenfeld RM, Har‐El G. Age as a prognostic factor for complications of major
head and neck surgery. Arch Otolaryngol Head Neck Surg 2005;131:605‐609. 16. Leon X, Quer M, Agudelo D, et al. Influence of age on laryngeal carcinoma. Ann Otol Rhinol Laryngol
1998;107:164‐169. 17. Derks W, de Leeuw L, Jr., Hordijk GJ, Winnubst JA. Reasons for non‐standard treatment in elderly patients
with advanced head and neck cancer. Eur Arch Otorhinolaryngol 2005;262:21‐26. 18. Sarini J, Fournier C, Lefebvre JL et al. Head and neck squamous cell carcinoma in elderly patients: a long‐
term retrospective review of 273 cases. Arch Otolaryngol Head Neck Surg 2001;127:1089‐1092. 19. Sanabria A, Carvalho AL, Vartanian JG et al. Factors that influence treatment decision in older patients
with resectable head and neck cancer. Laryngoscope 2007;117:835‐840. 20. Lewis CM, Hessel AC, Roberts DB et al. Prereferral head and neck cancer treatment: compliance with
national comprehensive cancer network treatment guidelines. Arch Otololaryngol Head Neck Surg 2010;136:1205‐11
21. Grenman R, Chevalier D, Gregoire V et al. Treatment of head and neck cancer: European concensus at the EUFOS congress in Vienna 2007. Eur Arch Otorhinolaryngol 2010;267:1619‐1621
22. Charlson ME, Pompei P, Ales KL, Mackenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987;40:373‐383.
23. Clayman GL, Eicher SA, Sicard MW et al. Surgical outcomes in head and neck cancer patients 80 years of age and older. Head Neck 1998;20:216‐223.
24. Sanabria A, Carvalho AL, Melo RL et al. Predictive factors for complications in elderly patients who underwent head and neck oncologic surgery. Head Neck 2008;30:170‐177.
26. de Cassia Braga RK, Kowalski LP. APACHE II, POSSUM, and ASA scores and the risk of perioperative complications in patients with oral or oropharyngeal cancer. Arch Otolaryngol Head Neck Surg 2003;129:739‐745.
25. Cohen EE, Lingen MW, Vokes EE. The expanding role of systemic therapy in head and neck cancer. J Clin Oncol 2004;22:1743‐1752.
26. Piccirillo JF. Importance of comorbidity in head and neck cancer. Laryngoscope 2000;110:593‐602.
120

Age‐related differences in head and neck cancer treatment
121
27. Kusaba R, Sakamoto K, Mori K et al. Laboratory data and treatment outcomes of head and neck tumor patients in the elderly. Auris Nasus Larynx 2001;28:161‐168.
28. Puts MT, Monette J, Girre V et al. Characteristics of older newly diagnosed cancer patients refusing cancer treatments. Support Care Cancer 2010;18:969‐974.
29. Meropol NJ, Egleston BL, Buzaglo JS et al. Cancer patient preferences for quality and length of life. Cancer 2008;113:3459‐3466.
30. Fried TR, Bradley EH, Towle VR, Allore H. Understanding the treatment preferences of seriously ill patients. N Engl J Med 2002;346:1061‐1066.
31. Derks W, De LR, Winnubst J, Hordijk GJ. Elderly patients with head and neck cancer: physical, social and psychological aspects after 1 year. Acta Otolaryngol 2004;124:509‐514.


Part III
Decision making in geriatric oncology


Chapter 9
The value of a comprehensive geriatric assessment for patient care in acutely hospitalized older patients with cancer
M.E. Hamaker, B.M. Buurman, B.C. Van Munster, I.M.J.A. Kuper,
C.H. Smorenburg, S.E. de Rooij
The Oncologist 2011;16:1403‐12

Chapter 9
Abstract Introduction: A comprehensive geriatric assessment systematically collects information on
geriatric conditions and is propagated in oncology as a useful tool when assessing older
cancer patients.
Objective: 1) to study the prevalence of geriatric conditions in cancer patients aged ≥65
years, acutely admitted to a general medicine ward, 2) to determine functional decline
and mortality within twelve months after admission, and 3) to assess which geriatric
conditions and cancer‐related variables are associated with twelve‐month‐mortality.
Method: An observational cohort study of 292 cancer patients ≥65 years, acutely admitted
to the general medicine and oncology ward of two university and one secondary teaching
hospital. Baseline assessment included patient characteristics, reason for admission,
comorbidity and geriatric conditions. Follow‐up at three and twelve months was aimed at
functional decline (loss of 1 in ADL‐activities) and mortality.
Results: Median age was 74.9 years, and 95% lived independently; 126 patients (43%) had
metastatic disease. A high prevalence of geriatric conditions was found for IADL
impairment (78%), depressive symptoms (65%), pain (65%), impaired mobility (48%),
malnutrition (46%) and ADL impairment (38%).
Functional decline was observed in 8% and 33% of patients at three and twelve months,
respectively. Mortality rates were 38% at three months and 64% at twelve months.
Mortality was associated with cancer‐related factors only.
Conclusion: In these acutely hospitalized older cancer patients, mortality was only
associated with cancer‐related factors. The prevalence of geriatric conditions in this
population was high. Future research is needed to elucidate if addressing these conditions
can improve quality of life.
126

CGA in hospitalized elderly cancer patients
Introduction Although malignant tumours occur at all ages, cancer disproportionately strikes individuals
aged 65 years and older.1 Data from the National Cancer Institute Surveillance,
Epidemiology, and End Results Program reveal that over half of all newly diagnosed cancer
patients and more than two‐thirds of cancer deaths are in this age group.2 In western
societies, the number of older cancer patients will increase substantially in the coming
decades as a result of increasing life expectancy and ageing of the population. Oncologists
are faced with the challenge of how to determine what treatment is suitable for their
older cancer patients, with their heterogeneity in comorbidity, physical reserve, disability
and geriatric conditions. Age and performance status are too limited to do justice to this
diversity,3,4 and as guidelines for cancer treatment are often based on trials from which
older patients and patients with comorbidity have been excluded,5 these guidelines
cannot automatically be extrapolated to all ages.
Therefore, the use of a comprehensive geriatric assessment (CGA) – a systematic
procedure to appraise the objective health status of older people, focusing on somatic,
functional and psychosocial domains ‐ is frequently propagated in oncology as the tool to
fill in these gaps.4,6‐11 It is thought that identifying those factors associated with poor
outcome will aid in prognostication and decision making regarding treatment for the
individual patient.10,12 Furthermore, modifying the conditions identified with a CGA could
improve outcome and health‐related quality of life,7,13,14 particularly since geriatric
conditions are often missed if they are not specifically looked for.7‐9,15
Although many editorials and review articles endorse the use of CGA in geriatric oncology,
publication of evidence supporting this assumption of an added value of systematic CGA
above usual care is far less frequent.4,5,7‐10,12,14,16‐19 In addition, due to heterogeneity in
study population (inpatients vs. outpatients) and study setting (oncology vs. geriatric
medicine vs. general medicine) as well as the large variation in the extensiveness of the
CGA administered, data remain fragmentary and inconclusive on the association between
CGA and outcome.
One setting in which CGA may be of added value is for older cancer patients requiring
acute hospitalization, for example when an acute illness reveals the presence of
malignancy or due to cancer‐ or treatment‐related complications in the course of the
disease. Independent of the reason for admission, choices need to be made about future
course of treatment during hospitalization. Furthermore, acutely ill patients could be at
increased risk for geriatric conditions and functional decline.
Therefore, we studied the value of a CGA for older cancer patients acutely admitted to the
general medicine and oncology departments of three hospitals. The aim of the present
study was threefold: 1) to study the prevalence of geriatric conditions in cancer patients
aged 65 years and older acutely admitted to a general medicine ward, 2) to determine
127

Chapter 9
functional decline and mortality within twelve months after admission and 3) to assess
which geriatric conditions and cancer‐related variables are associated with twelve‐month
ortality. m
Method
Patients This is an observational substudy of cancer patients who were included in the DEFENCE‐I
and ‐II studies (Development of strategies Enabling Frail Elderly New Complications to
Evade).20,21 The DEFENCE‐I study (n=647) was conducted at the Academic Medical Centre
Amsterdam (AMC), the Netherlands; inclusion ran from November 2002 until March
2006.20 The DEFENCE‐II study (n=639) ran from April 2006 until March 2008 in AMC,
University Medical Centre Utrecht, and Spaarne Hospital Hoofddorp.21
In these prospective cohort studies, all patients aged 65 years and older, acutely admitted
to the general medicine or oncology ward were included. Patients were excluded if 1) they
or their relatives did not give informed consent, 2) they were too ill to participate
according to their attending physician, 3) they came from another ward inside or outside
the hospital, 4) they were transferred to the intensive care unit, coronary care unit or
another ward inside or outside the hospital within 48 hours after admission, or 5) they
were unable to speak or understand Dutch. Inclusion had to take place within 48 hours
after admission. The Medical Ethics Committee of the AMC approved both studies.
In this substudy, only patients with a known malignancy at the time of admission or a
alignancy first diagnosed during admission were included. m
Data collection The methods of the two studies were similar: within 48 hours of admission, a
multidisciplinary evaluation was performed by a geriatric consultation team. This team
consisted of two medical specialists, a geriatric resident, a clinical nurse specialist and two
research nurses trained in geriatric medicine.
Data on social and demographic status were collected. Patients were assessed for the
following geriatric conditions: polypharmacy, malnutrition, incontinence, falls, the ability
to perform (instrumental) activities of daily living (ADL and IADL), and cognitive
impairment two weeks prior to admission, neurosensory deficits, mobility disorders, and
delirium. Furthermore, patients in the DEFENCE‐II study were assessed for the presence of
pain, constipation, pressure ulcers, health status, depressive symptoms and caregiver
burden. Appendix 1 lists the tools used in the assessment. All variables were
dichotomized, using the cut‐offs described in this appendix.
128

CGA in hospitalized elderly cancer patients
Medical history and oncologic treatment prior to, during and after hospital stay were
collected from patients’ medical records by a geriatrician. Based on the treatment during
and after hospitalization, patients were subdivided in two groups: those still receiving
active anti‐cancer treatment (both curative and palliative, i.e. chemotherapy, radiotherapy
and/or surgical therapy) and those receiving supportive or symptomatic care only. The
reason for admission was collected from the discharge report and classified as directly
tumour‐related, treatment‐related or due to another cause.
These reports were also used to derive the Charlson comorbidity index,32 excluding the
current malignancy. The Charlson score is a continuous variable, with scores range from 0‐
1 with higher scores indicating more or more severe comorbidities. 3
Follow up and definition of outcomes Follow‐up consisted of a telephone interview by a research nurse at three and twelve
months after discharge, in which the modified Katz ADL index was re‐administered.
Follow‐up was completed by the same person (patient or primary caregiver) interviewed
at baseline.
Functional decline was defined as a loss of one or more ADL activities at three or twelve
months as compared to premorbid function, two weeks prior to hospital admission. Data
n mortality were collected from the Municipal Data Registry. o
Statistical Analysis Patients receiving active treatment and those receiving supportive care only after
admission were compared with one another, for differences in age, comorbidity, the
presence of geriatric syndromes, as well as for mortality and functional decline. The chi‐
square test and risk analysis were used for nominal and ordinal variables, as well as for
continuous variables with a non‐normal distribution; for continuous variables with a
normal distribution, the Student t‐test was used.
To determine which baseline factors and geriatric conditions were associated with
mortality in the twelve months following admission, a Cox regression analysis was
performed. For each variable, the Cox proportional hazards assumption was tested using
the log minus log plot. Next, a univariate Cox‐regression analysis was performed to
determine which variables were associated with mortality in the twelve months following
admission. Factors with a p‐value <0.20 in the univariate analysis and with less than 20%
missing data, were included in the multivariate analysis. A backward selection procedure
was applied, accepting a p‐value of p<0.05. Kaplan Meier survival plots, with a log‐rank
analysis, were used to determine survival in the twelve months after admission.
The SPSS (Statistical Package for the Social Sciences) version 16.0 was used for the
analyses.
129

Chapter 9
Results
Characteristics of acutely hospitalized older cancer patients In total, 1286 patients were included in the two studies, of which 208 had a known, active
malignancy (16%), and 84 were diagnosed with cancer during admission (7%). Baseline
characteristics are listed in Table 1. Median age was 74.9 years (range 65.0 – 96.2 years)
and 95% of patients lived independently. A total of 27 different types of malignancies
were present (Appendix 2). A total of 126 patients (43%) had metastatic disease.
Table 1: Baseline characteristics of patients with receiving active oncological treatment or supportive care only* (data in n(%) unless otherwise specified)
All patients
n=292 Active treatment
n=150Supportive care
n=137 p‐
value**
Hospital .65 AMC 250 (87.1) 129 (86.0) 121 (88.3) UMCU 16 (5.6) 8 (5.3) 8 (5.8) Spaarne 21 (7.3) 13 (8.7) 8 (5.8)
Study .37 DEFENCE‐I 138 (47.3) 74 (49.3) 47 (46.7) DEFENCE‐II 154 (52.7) 76 (50.7) 49 (53.3)
Median age in years (range) 74.9 (65.0–96.2) 75.5 (65.0–94.7) 73.4 (65.2–96.2) .44 65‐74 years 210 (51.2) 104 (47.3) 101 (55.5) 75‐84 years 71 (34.5) 40 (36.7) 31 (32.1) 85+ years 11 (14.3) 6 (16.0) 5 (12.4)
Female sex 141 (48.8) 80 (53.3) 60 (43.8) .11
Years of education (SD) 10.2 (3.8) 9.5 (3.5) 10.9 (4.0) .003
Living independently 275 (95.0) 141 (94.0) 129 (96.3) .54
Median length of stay in days (range) 8 (1–80) 8 (2–80) 7 (1–42) .84
Charlson score (SD) 1.1 (1.1) 1.1 (0.9) 1.0 (1.2) .55
Number of comorbid conditions (SD) 1.1 (1.1) 1.0 (1.2) 1.1 (1.0) .44
Metastases at inclusion (42.7) 58 (38.7) 64 (47.1) .14
Newly diagnosed at admission (28.2) 68(45.3) 13 (9.5) <0.001
Known cancer diagnosis (71.8) (54.7) 124 (90.5) <0.001
Reason for admission Tumor‐related*** 193 (66.1) 101 (67.3) 91 (66.4) .99 Treatment‐related **** 49 (16.8) 25 (16.7) 24 (17.5) .01 Other 50 (17.1) 23 (15.3) 22 (16.1) .82 SD = standard deviation * due to missing follow‐up, we were unable to classify treatment in five patients. ** adjusted for age and sex; p‐value is considered significant at < 0.05 (in bold). *** tumour‐related causes for admission were asymptomatic jaundice or cholangitis (n=32), haemorrhage or anaemia (n=31), aspecific malaise (n=38), obstruction (n=26), dyspnoea (n=10) or pain (n=12) **** treatment‐related causes for acute admission were chemotherapy related complications (n=33), radiotherapy related complications(n=6), due to a complication of a diagnostic procedure (n=2) or due to a complication of a therapeutic surgical procedure (n=8)
130

CGA in hospitalized elderly cancer patients
Prevalence of geriatric conditions A high prevalence of geriatric conditions was seen, particularly of IADL impairment (77%),
pain (65%), depressive symptoms (65%), polypharmacy (48%), mobility problems (48%),
malnutrition (46%), high caregiver burden (44%) and ADL impairment (38%) (Table 2). On
average, patients had four geriatric conditions while only 9% had no geriatric conditions
The prevalence increased with age, as patients aged 65‐69 years had 2.9 conditions on
average, patients aged 70‐79 years had 4.1 conditions, and those aged 80 and older had
5.5 conditions (p<0.001). Mean Charlson comorbidity index, excluding the current
malignancy, was 1.1 (standard deviation 1.1). Table 2: Prevalence of geriatric conditions in patients receiving active oncological treatment or supportive care only*
All patients
n=292 Active treatment
n=150Supportive care
n=137 p‐value**
Somatic geriatric conditions n (%) Polypharmacy 129/270 (48.0) 67/139 (48.2) 62/131 (47.3) .80 Malnutrition 101/220 (46.0) 47/111 (42.3) 54/111 (48.6) .30 Pain*** 81/125 (64.8) 40/61 (65.6) 41/64 (64.1) .70 Constipation*** 33/149 (22.1) 17/76 (22.4) 16/73 (21.9) .94 Incontinence 66/261 (25.2) 40/138 (29.0) 26/123 (21.1) .29 Pressure ulcers*** 2/135 (1.4) 1/69 (1.4) 1/66 (1.5) .72 Falls 32/254 (12.7) 16/135 (11.9) 16/119 (13.4) .63
Functional geriatric conditions ADL impairment at baseline 104/273 (38.1) 57/142 (40.1) 47/131 (35.9) .94 IADL impairment at baseline 191/250 (76.9) 103/129 (79.8) 88/121 (72.7) .37 Neurosensory deficits 70/268 (26.0) 32/143 (22.4) 38/125 (30.4) .07 Mobility 131/275 (47.9) 78/145 (53.8) 53/130 (40.8) .13
Psychological geriatric conditions Global cognitive impairment 31/201 (15.1) 15/98 (15.3) 16/103 (15.5) .56 Depressive symptoms*** 79/121 (65.3) 40/59 (67.8) 39/162 (62.9) .66 Delirium 61/283 (21.5) 27/148 (18.2) 34/135 (25.2) .10 Low health status score*** 33/120 (28.5) 19/59 (32.2) 14/61 (23.0) .24
Social geriatric conditions High caregiver burden*** 47/108 (43.8) 26/51 (51.0) 21/57 (36.8) .12
Total number of geriatric conditions (SD)
4.0 (2.9) 4.2 (2.9) 4.1 (2.9) .51
Presence of 1 or more geriatric conditions
91.1 91.3 90.5 .80
* due to missing follow‐up data, we were unable to classify five patients ** adjusted for age and sex; p‐value is considered significant if < 0.05. *** only included in DEFENCE‐II study
131

Chapter 9
Differences between patients receiving active vs. supportive care We were unable to classify five patients as either receiving active or supportive care due
to missing follow‐up data. Of the remaining patients, 137 (48%) received only
symptomatic or supportive care; for newly diagnosed patients, this percentage was much
lower than for patients with a known cancer diagnosis (16% vs. 60%, p<0.001). Patients
receiving supportive care only had a higher level of education, and higher Charlson
comorbidity index. Interestingly, they did not differ in age (Table 1) or the presence of
geriatric conditions (Table 2) from those receiving active care.
Table 3: Cox‐regression analysis for mortality at twelve months
Univariate analysis Multivariate analysis *
Hazard ratio
95% confidence interval
p= * Hazard ratio
95% confidence interval
p= *
Age 1.01 .99 – 1.03 .48 ‐ Sex .91 .69 – 1.21 .50 ‐ Newly diagnosed cancer 1.18 .87 – 1.61 .29 Comorbidity 1.03 .90 – 1.17 .72 ‐ Metastatic disease 1.89 1.41 – 2.52 <0.001 1.67 1.23 – 2.29 <0.001 Tumor‐related admission 1.79 1.20 – 2.47 <0.001 1.57 1.12 – 2.21 .01 Supportive care only 1.14 .85 – 1.52 .38 Polypharmacy 1.10 .81 – 1.48 .55 Incontinence 1.13 .80 – 1.60 .48 Falls .96 .60 – 1.53 .87 ADL impairment at baseline
1.45 1.08 – 1.98 .02‐
IADL impairment at baseline
1.08 .75 – 1.56 .69
Neurosensory deficits .91 .65 – 1.29 .61 Mobility 1.12 .83 – 1.50 .46 Delirium 1.23 .87 – 1.74 .24
Variables not included in analysis due to >20% missing data
Malnutrition 1.27 .91 – 1.77 .16 Pain 1.11 .95 – 1.28 .18 Constipation 1.41 .88 – 2.28 .15 Pressure ulcers 5.29 1.26 – 22.19 .02 Global cognitive impairment
1.33 .83 – 2.13 .23
Depressive symptoms 1.23 .75 – 2.02 .40 Low health status score 1.24 .75 – 2.04 .41 Caregiver burden 1.32 .82 – 2.12 .25 * Variables with a p‐value <0.20 in the univariate analysis, and with less than 20% missing data, were included in the multivariate analysis; these variables are marked in bold in the p‐value column. Age, sex and comorbidity were also included as potential confounders. A backward selection procedure was applied; a forward analysis selected the same variables.
132

CGA in hospitalized elderly cancer patients
Figure 1: Kaplan Meier survival plotted in relation to active treatment vs. supportive care, after correcting for stage of disease and reason for admission
Outcomes Mortality rates were 11% in hospital, 38 % at three months and 64% at twelve months. Of
patients still alive at follow‐up, 8% experienced functional decline at three months, as
determined by a decline of one or more in ADL abilities in comparison to premorbid
function, two weeks prior to hospitalization. At twelve months, 33% of patients showed
functional decline
Table 3 shows the Cox‐regression analysis for factors associated with twelve‐month‐
mortality. Only metastatic disease (HR 1.67, 95% CI 1.23‐2.29) and a tumour‐related
reason for admission (HR 1.57, 95%CI 1.12‐2.21) were independent predictors of outcome,
while age, sex, and comorbidity were not. Active oncological treatment did not give any
significant survival benefit in comparison to supportive care only (Figure 1); at three
months, mortality rate was 36.7% for patients receiving active treatment vs. 38.7% in
those receiving supportive care only. At twelve months, mortality was 62.7% vs. 65.7%
respectively.
133

Chapter 9
Because several geriatric conditions were not included in the DEFENCE‐I study, we also
performed a separate multivariate analysis using only the data of the DEFENCE‐II study.
This analysis yielded similar results for factors associated with mortality within twelve
onths. m
Discussion To our knowledge, this is the first prospective, in‐patient study addressing the prevalence
of geriatric conditions and their association with outcome in acutely hospitalized older
cancer patients. Recent observations demonstrated that several geriatric conditions were
predictive of outcome in older cancer patients in out‐patient settings.6,11,12 In the present
study, we demonstrated that in our population of 292 acutely hospitalized older cancer
patients, most of whom were living independently prior to admission, geriatric conditions
were highly prevalent, but none of the elements of the CGA were associated with
mortality.
The high prevalence of geriatric conditions we found, was also seen in a hospital‐based,
retrospective study, which reported comparable rates of functional limitations, impaired
mobility, malnutrition and depression.17 Interestingly, we found no differences in the
presence of geriatric conditions between patients receiving active care, and those
receiving supportive care only. Also, receiving active oncologic treatment did not influence
mortality rates compared to receiving supportive care only. Of course, oncologic
treatment is not only aimed at improved survival but also improved quality of life, a factor
not incorporated in this study.
In our study, 8% of cancer patients experienced an increased ADL‐dependency three
months after discharge, and over 33% at twelve months. We found no prior studies that
addressed functional decline after acute hospitalization in older cancer patients. A study
by Covinsky et al. looked at loss of ADL abilities after hospitalization for any acute medical
illness in patients aged 70 and over – without specifically investigating cancer patients.33 In
their cohort, as many as 35‐50% of older patients experienced increased disability
(defined by a loss of one or more ADL‐abilities) three months after acute hospitalization.
The difference with our findings could be explained by differences in the study population,
as the cancer patients included in our analysis were younger, had less comorbidity, less
functional impairment and less cognitive impairment at baseline, all of which are factors
potentially associated with functional decline.34
For acutely hospitalized patients, the value of CGA in predicting mortality seems to be low.
We found that none of the geriatric conditions were associated with mortality within
twelve months of admission. This outcome differs from several other studies in an out‐
patient setting addressing the association between geriatric conditions and outcome;
age,12 comorbidity,12 ADL‐ and IADL‐dependency,11 and depression,6 were found to predict
134

CGA in hospitalized elderly cancer patients
mortality in older cancer patients in this setting. However, in these patients, geriatric
assessment was often administered prior to the onset of oncologic treatment with
curative intent. Therefore, patients were in a different phase of disease than the patients
in our study. Most likely, for these acutely admitted older cancer patients, the presence or
absence of geriatric conditions had little further impact on outcome, probably because of
the severity of the cancer and cancer‐related symptoms: 66% was admitted for a directly
tumour‐related reason, over 43% had metastases, 48% received only supportive care and
64% died within twelve months. This could also explain why mortality was not associated
with age or comorbidity.
In patients with a poor prognosis, the goal of care generally shifts from cure to palliation.
Potentially, identifying geriatric conditions at the time of hospital admission can provide
the treating physician with leads for improving quality of life. For example, in a study
comparing geriatric care for older patients with cancer to care as usual, geriatric care
improved quality of life, although there was no difference in survival.14 Because of the
high prevalence of geriatric conditions in our study, and the fact that geriatric conditions
are easily missed if not specifically looked for,7‐9,15 assessing patients for modifiable
geriatric conditions seems appropriate when aiming to optimize quality of hospital and
palliative care for older cancer patients.
There are several limitations to this study. First of all, the study population forms a
heterogeneous group, with different types of malignancies in different stages of disease.
Furthermore, because two of the three hospitals are tertiary referral centres, there is a
potential referral bias, resulting in a less frail population as well as an overrepresentation
of upper gastro‐intestinal tract tumours – for which the Academic Medical Centre is a
national centre – compared to regional hospitals. This potentially influences the
generalizability of our findings. For example, the low cancer‐specific survival rates of the
upper GI tract malignancies could have decreased the value of the CGA for predicting
mortality. A second limitation is that this is a post‐hoc analysis of two studies, whose
designs were highly but not entirely similar. Some geriatric conditions addressed in the
DEFENCE‐II study were not included in the DEFENCE‐I study, therefore resulting in a
missing data for these items. The effect on the outcomes of this study seems low,
however, as analyses with only the data from the DEFENCE‐II study did not lead to
different results. Due to the high mortality rates at three and twelve months, we were
nable to test which factors at baseline were associated with functional decline. u
In conclusion, our study demonstrates geriatric conditions are highly prevalent in older
cancer patients admitted for an acute illness. Based on prior literature, we assume that
using a CGA for older cancer patients acutely admitted to hospital may have added value
for improving quality of life. None of the elements of the CGA were of value in predicting
135

Chapter 9
mortality, as outcome in this population was only associated with cancer‐related factors.
To elucidate the exact role of CGA, future research comparing quality of life and outcome
in patients receiving either care as usual or specific interventions aimed at modifying the
geriatric conditions identified by a CGA, is needed.
136

CGA in hospitalized elderly cancer patients
Appendix 1: Tools used in the assessment for geriatric conditions
* Tools marked with an asterisk were only administered in the DEFENCE‐II study
Geriatric conditions
Measurement tool Source Range of scores
Cut‐off used
Somatic geriatric conditions Polypharmacy Number of different medications medical chart Continuous ≥ 5 Malnutrition Short Nutritional Assessment
Questionnaire (SNAQ)22* and / or Body Mass Index (BMI)
Patient medical chart
0 – 7 Continuous
≥ 2 < 20
Pain Visual Analogue Scale (VAS) 23* patient** 0 – 10 ≥ 4 Constipation Constipation on physical
examination at admission* medical chart yes or no Yes
Incontinence Presence of incontinence at admission
medical chart yes or no Yes
Falls Two or more falls in the past three months
patient yes or no Yes
Pressure ulcers Observation by the research nurse* nurse yes or no Yes
Functional geriatric conditions ADL functioning Katz ADL index score24 patient/
caregiver*** 0‐6 ≥ 1 is
impairment IADL functioning Modified Katz index25 patient/
caregiver*** 0‐9 ≥ 1 is
impairment Neurosensory deficits
Impairment of hearing and/or vision*, regardless of use of glasses or hearing aid
patient yes or no yes
Mobility Requiring help or the use of a walking aid for mobility
patient yes or no Yes
Health status Euroqol (EQ‐5D)26* patient** utility list of 5 items
present if scored “severe” ≥ 1
Psychological geriatric conditions Cognitive impairment
Informant Questionnaire COgnitive DEcline – Short Form (IQCODE‐SF)27
caregiver 1 – 5 ≥ 3.9
Depressive symptoms
Geriatric Depression Scale‐2 (GDS‐2)28*
patient** 0 – 2 2
Delirium Confusion Assessment Method29 nurse 0 – 4 item 1 and 2 present plus 3 and/or 4
Social geriatric conditions Caregiver burden Experienced Burden of Informal
Care (EDIZ)30* caregiver 0 – 9 ≥ 4
** Not administered if MMSE31 was <16
*** In the DEFENCE‐I study, the Katz was filled out by the patient if MMSE31 was >23. If it was lower, the
primary caregiver filled out the Katz. In the DEFENCE‐II study, the Katz was filled out by the patient if the MMSE was >20; filled out by the patient and double‐checked with the caregiver if MMSE was 16 to 20; and filled out by the caregiver only if MMSE was <16.
137

Chapter 9
Appendix 2: Overview of cancer diagnoses
Number of patients Pancreatic cancer 36 Colon cancer 32 Oesophageal cancer 26 Cholangiocarcinoma 23 Lymphoma 21 Breast cancer 18 Lung cancer 18 Prostate cancer 16 Stomach cancer 15 Bladder cancer 14 Leukaemia 12 Multiple myeloma 10 Rectum cancer 9 Other haematological 9 Ovarian cancer 7 Renal cell carcinoma 7 Unknown origin 5 Hepatocellular carcinoma 3 Melanoma 3 Laryngeal cancer 3 Sarcoma 2 Thyroid cancer 1 Carcinoid 1 Cervical cancer 1 Total: 292
138
CGA in hospitalized elderly cancer patients
References 1. Muss HB. Cancer in the elderly: a societal perspective from the United States. Clin Oncol (R Coll Radiol)
2009;21:92‐8
2. Yancik R, Ries LA. Cancer in older persons. Semin Oncol 2004;31:128‐36
3. Smorenburg CH, Sijp JR. [Breast cancer in the elderly]. Ned Tijdschr Oncol 2006;3:247‐52
4. Extermann M, Overcash J, Lyman GH et al. Comorbidity and functional status are independent in older cancer patients. J Clin Oncol 1998;16:1582‐7
5. Repetto L, Fratino L, Audisio RA et al. Comprehensive geriatric assessment adds information to the Eastern Cooperative Oncology group performance status in elderly cancer patients. J Clin Oncol 2002;20:494‐502
6. Maas HA, Janssen‐Heijnen ML, Olde Rikkert MG, Wymenga AN. Comprehensive geriatric assessment and its impact in oncology. Eur J Cancer 2007;43:2161‐9
7. Extermann M, Meyer J, McGinnis M et al. A comprehensive geriatric intervention detects multiple problems in older breast cancer patients. Crit Rev Hemaol Oncol 2004;49:69‐75
8. Flood KL, Carroll MB, Le CV et al. Geriatric syndromes in elderly patients admitted to an oncology‐acute care for elders unit. J Clin Oncol 2006;24:2298‐303
9. Terrett C, Albrand G, Droz JP, on behalf of the Geriatric Oncology Program. Multidimensional geriatric assessment reveals unkown medical problems in elderly cancer patients. J Clin Oncol 2004;22(14S)abstract 8167.
10. Zagonel V, Fratino L, Piselli et al. The comprehensive geriatric assessment predicts mortality among elderly cancer patients. Proc Am Soc Clin Oncol 2002;21:abstract 1458
11. Terret C, Zulian CG, Naiem A, Albrand G. Multidisciplinary approach to the geriatric oncology patient. J Clin Oncol 2007;25:1876‐81
12. Wedding U, Rohrig B, Klippstein A et al. Age, severe comorbidity and functional impairment independently contribute to poor survival in cancer patients. J cancer Res Clin Oncol 2007;133:945‐50
13. McCorkle R, Strumph NE, Nuamah IF et al. A specialized home care intervention improves survival among older post‐surgical cancer patients. J Am Geriatr Soc 2000;48:1707‐13
14. Rao AV, Hsieh F, Feussner JR, Cohen HJ. Geriatric evaluation and management units in the care of the frail elderly cancer patient. J Gerontol A Med Sci 2005;60A:798‐803
15. Inouye SK, Foreman MD, Mion LC et al. Nurses' recognition of delirium and its symptoms: comparison of nurse and researcher ratings. Arch Intern Med 2001 Nov 12;161(20):2467‐73
16. Serraino D, Fratino L, Zagonel V, for the GIOGer study group. Prevalence of functional dysability among elderly patients with cancer. Crit Rev Oncol Hematol 2001;39:269‐73
17. Retornaz F, Seux V, Pauly V, Soubeyrand J. Geriatric assessment and care for older cancer inpatients admitted in acute care for elders unit. Crit Rev Oncol Hematol 2008;68:165‐71
18. Retornaz F, Seux V, Sourial N et al. Comparison of the health and functional status between older inpatients with and without cancer admitted to a geriatric/internal medicine unit. J Gerontol A Med Sci 2007;62A:917‐22
19. Hurria A, Lichtman SM, Gardes J et al. Identifying vulnerable older adults with cancer. J Am Geriatr Soc 2007;55:1604‐8
20. Buurman BM, Munster BC van, Korevaar JC et al. Prognostication in acutely admitted older patients by nurses and physicians. J Gen Intern Med 2008;21:20‐29
21. Buurman BM, Hoogerduijn JG, van Gemert EA et al. Systematic Comprehensive Geriatric Assessment in older hospitalised patients at high and low risk for functional decline. [submitted]
22. Kruizenga HM, Seidell JC, de Vet HC et al. Development and validation of a hospital screening tool for malnutrition: the short nutritional assessment questionnaire (SNAQ). Clin Nutr 2005;24:75‐82
23. Collins SL, Moore RA, McQuay HJ. The visual analogue pain intensity scale: what is moderate pain in millimetres? Pain 1997;72:95‐7
24. Katz S, Ford AB, Moskowits RW et al. Studies of illness in the aged. The index of ADL: a standardized measure of biological and psychological function. JAMA 1963;185:914‐9
139

Chapter 9
140
25. Weinberger M, Samsa GP, Schmader K et al. Comparing proxy and patients' perceptions of patients' functional status: results from an outpatient geriatric clinic. J Am Geriatr Soc 1992;40:585‐8
26. The EuroQol Group. EuroQol‐a new facility for the measurement of health‐related quality of life. Health Policy 1990:16;199‐208.
27. Jorm AF, Jacomb PA. The Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE): socio‐demographic correlates, reliability, validity and some norms. Psychol Med 1989;19:1015‐22
28. Arroll B, Khin N, Kerse N. Screening for depression in primary care with two verbally asked questions: cross sectional study. BMJ 2003;327:1144‐6
29. Inouye SK, van Dyck CH, Alessi CA et al. Clarifying confusion: the confusion assessment method. A new method for detection of delirium. Ann Intern Med 1990;113:941‐8.
30. Pot AM, van DR, Deeg DJ. [Perceived stress caused by informal caregiving. Construction of a scale]. Tijdschr Gerontol Geriatr 1995;26:214‐9
31. Folstein MF, Folstein SE, McHugh PR. "Mini‐mental state". A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975;12:189‐98.
32. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987;40:373‐83.
33. Covinsky KE, Palmer RM, Fortinsky RH et al. Loss of independence in activities of daily living in older adults hopitalized with medical illnesses. J Am Geriatr Soc 2003;51:451‐8
34. Boyd CM, Ricks M, Fried LP et al. Functional decline and recovery of activities of daily living in hospitalized, disabled older women: the Women's Health and Aging Study I. J Am Geriatr Soc 2009;57:1757‐66

Chapter 10
Baseline comprehensive geriatric assessment is associated with toxicity and survival in elderly metastatic breast cancer patients receiving single‐agent chemotherapy
Results from the OMEGA study of the Dutch Breast Cancer Trialists’ Group
M.E. Hamaker, C. Seynaeve, A.N.M. Wymenga, H. van Tinteren, J.W.R. Nortier, E. Maartense, H. de Graaf, F.E. de Jongh, J.J. Braun, M. Los, J.G. Schrama,
A.E. van Leeuwen‐Stok, S.M. de Groot, C.H. Smorenburg
[submitted]

Chapter 10
Abstract Aim: To evaluate the association between baseline comprehensive geriatric assessment
(CGA) and toxicity in elderly metastatic breast cancer patients treated with first‐line
palliative chemotherapy.
Patients and Methods: Metastatic breast cancer patients (≥ 65 years) were randomized
between pegylated liposomal doxorubicin or capecitabine. CGA included instrumental
activities of daily living (IADL), cognition using the mini mental state examination (MMSE),
mood using the geriatric depression scale (GDS), comorbidity using the Charlson index,
polypharmacy and nutritional status using the body mass index. Frailty on CGA was
defined as 1+ of the following: IADL≤13, MMSE ≤23, GDS ≥5, BMI ≤20, ≥5 medications or
Charlson ≥2. The Groningen Frailty Index (GFI) was used as a frailty screening tool (cut‐off
for frailty ≥ 4).
Results: Of the 78 patients that were randomized (median age 75.5 years, range 65.8‐86.8
years), 73 were evaluable for CGA; 52 (71%) had one or more geriatric conditions. Only
19% of patients without geriatric conditions experienced grade 3‐4 chemotherapy‐related
toxicity compared to 56% of patients with two geriatric conditions and 80% of those with
three or more (p=0.03). Polypharmacy was the only individual factor associated with
toxicity (p=0.001). GFI had a sensitivity of 69% for frailty on CGA and a specificity of 76%,
and was not predictive of outcome.
Conclusion: In this study of elderly patients with metastatic breast cancer, the number of
geriatric conditions correlated with grade 3‐4 chemotherapy‐related toxicity, suggesting
that a CGA should be incorporated as a standard of care if chemotherapy is considered for
elderly cancer patients.
142

CGA predicts toxicity in elderly metastatic breast cancer patients
Introduction Although breast cancer occurs at all ages, it disproportionally strikes those aged 65 years
and older. In 2010, 17% of the Dutch population was aged 65 years and older,1 but 39% of
newly diagnosed breast cancers and 59% of breast cancer‐related deaths occurred in this
age group.2 With the imminent ageing of society, the number of older breast cancer
patients is expected to rise greatly in the coming decades. These patients have been
underrepresented in the clinical trials on which treatment recommendations have been
based.3,4 As a result, many questions remain regarding optimal treatment for older breast
cancer patients, including whether older patients derive the same benefit from
chemotherapy as younger patients, as well as how to determine whether an older patient
will be able to tolerate such treatment. As metastatic breast cancer is still an incurable
disease, major goals of chemotherapy especially in elderly patients are relief of symptoms
and prolongation of the time period with a reasonable quality of life.
Ageing is very much an individual process, in which differences in genetic predisposition
and life‐style will become apparent, intercurrent and chronic diseases as well as geriatric
conditions leave their mark, and the speed of decline of physiologic reserves varies from
person to person.5,6 As a result, the elderly form a highly heterogeneous population. To
allow for description of health status despite this heterogeneity in contributing factors,
geriatric medicine uses the concept of frailty,7 which can be seen as the final common
pathway of ageing resulting from the cumulative decline across multiple organ systems,
causing a diminished resistance to stressors. The presence of frailty can be determined
using the comprehensive geriatric assessment (CGA), which is a systematic procedure to
assess a patient’s health status, focusing on the somatic, psychosocial and functional
domains.8 An alternative approach is to use a short frailty screening tool specifically
designed for this purpose, such as the Groningen Frailty Index.9
Although it has been demonstrated that a CGA is helpful in identifying previously
unrecognized health issues in older cancer patients,5,10‐12 the exact role of the CGA or a
frailty screening tool in decision making regarding treatment for older cancer patients still
needs to be clarified. In this study, we evaluated the value of frailty according to CGA or
the GFI, as well as individual geriatric conditions, for predicting chemotherapy‐related
toxicity and overall survival in metastatic breast cancer patients treated with first‐line
alliative chemotherapy. p
Methods The Dutch Breast Cancer Trialists Group (BOOG) OMEGA study (trial number NTR897,
BOOG 2006‐02) is a multi‐centre, randomized clinical trial regarding the tolerance and
efficacy of first line, single‐agent palliative chemotherapy for metastatic breast cancer
143

Chapter 10
patients aged 65 years or older, with incorporation of a comprehensive geriatric
assessment.
Patients were recruited between April 2007 and September 2011, by 25 Dutch hospitals.
Eligibility criteria included: a) they were female, aged 65 years or older with proven
metastatic breast cancer and eligible for first‐line palliative chemotherapy for metastatic
breast cancer; b) with European Cooperative Oncology Group (ECOG) performance status
0 to 2, or 3 (in case of pain or another pre‐existent disabling disease was determinative of
performance); and c) had acceptable bone marrow, cardiac, liver and renal functions.
Patients were excluded in case of anthracycline or capecitabine resistance (i.e.
development of recurrent or metastatic disease while on adjuvant anthracycline or
capecitabine therapy, or within 12 months of the completion of this therapy in the
adjuvant setting) evidence of uncontrolled cerebral metastases, another malignancy
within the previous 5 years, or inability of providing informed consent or complying with
regular follow‐up. All patients gave informed consent prior to inclusion.
Eligible patients were subsequently randomized between pegylated liposomal doxorubicin
(Caelyx®) 45 mg/m2 administered intravenously once every four weeks for a maximum of
six cycles, or capecitabine 2000 mg/m2 (Xeloda®), given orally on days 1 to 14, every three
weeks for a maximum of eight cycles. Toxicity was graded according to the Common
Toxicity Criteria (CTC) of the National Cancer Institute (NCI), version 3.13 In addition to
baseline data on socio‐economic factors, performance status and quality of life (using the
QLQ‐C30)14 , this study included a baseline comprehensive geriatric assessment of the
following six geriatric conditions: comorbidity as assessed by the Charlson comorbidity
index (cut‐off score ≥2),15 functional status as assessed by the Lawton & Brody scale for
instrumental activities of daily living (IADL, cut‐offs for partial dependence 14‐27, full
functional dependence ≤13),16 number of medications being used (cut‐off for
polypharmacy ≥5), nutritional status using the body mass index (BMI, cut‐off for
undernutrition ≤20 kg/m2), cognition as assessed by the mini‐mental state examination
(MMSE, cut‐off for cognitive impairment ≤23),17 and mood as assessed by the geriatric
depression scale (GDS, cut‐off for severe depressive symptoms ≥10, moderate depressive
symptoms 5‐9).18 Frailty on CGA was defined as the presence of one or more of the
following: full IADL dependence, comorbidity score ≥2, polypharmacy, cognitive
impairment, undernutrition and/or moderate to severe depressive symptoms. In addition
to the CGA, the Groningen Frailty Index (GFI)9 was used as a frailty screening tool, with a
cut‐off of 4 or more for frailty. The GFI was designed in the Netherlands as a frailty
screening instrument, and consists of 15 questions covering physical functioning, visual
and hearing impairment, cognition, medication, social support and depression.9
144

CGA predicts toxicity in elderly metastatic breast cancer patients
Statistical analysis All variables were categorized into two or three groups, as appropriate. To assess
differences between groups, the chi‐square test was used. A p‐value of <0.05 was
considered significant.
A univariate logistic regression analysis was performed to test for association between
baseline characteristics and grade 3‐4 chemotherapy‐related toxicity; a subsequent
multivariable analysis was omitted due to the fact that only one factor was associated in
the univariate analysis. To determine which factors were associated with mortality, a
multivariable Cox regression analysis was performed. For each variable, the Cox
proportional hazards assumption was tested using the log minus log plot, after which
factors with a p‐value <0.10 in the univariate analysis were subsequently entered in the
multivariable analysis. In addition, Kaplan Meier survival plots with a log‐rank analysis
were used.
The SPSS (Statistical Package for the Social Sciences) version 19.0 was used for all analyses.
Table 1: Baseline characteristics of patients included in the OMEGA study
n= (%)
Number of patients 73
Chemotherapy arm Doxorubicin Capecitabine
37 (51%) 36 (49%)
Age 65‐69 years 70‐74 years 75‐80 years 80+ years
17 (23%) 16 (22%) 30 (41%) 10 (14%)
Marital status
Married Widowed Single Missing
42 (57%) 22 (30%) 8 (11%) 1 (1%)
Current living situation Independent Residential care Missing
69 (96%) 3 (3%) 1 (1%)
Performance status 0 1 2+
21 (29%) 36 (49%) 16 (22%)
Quality of life (global score)14 Poor (0‐33) Average (34‐66) Good (67‐100) Missing
15 (21%) 15 (21%) 42 (58%) 1 (1%)
145

Chapter 10
Results
Baseline characteristics In total, 78 patients were randomized. The study was prematurely closed due to slow
accrual and supply problems with liposomal doxorubicin. As five patients had missing
values in one or more CGA variables; these patients were excluded from further analyses.
Of the 73 remaining patients, 37 received liposomal doxorubicin and 36 capecitabine
(Table 1). Median age was 75.9 years (range 65.8‐86.8 years). Over half of patients was
married (42 patients, 57%) and almost all patients lived independently (69 patients, 96%).
Performance status was 0‐1 in 57 patients (78%) and 2 in 15 (21%). According to QLQ‐C30,
42 patients experienced good global quality of life (58%), 15 average (21%) and 15
patients expressed poor quality of life (21%) at baseline.
Results from the geriatric assessments are listed in Table 2. Comorbidity was limited, with
64 patients having a Charlson score of 0 or 1 (88%). Most common geriatric conditions
were partial IADL dependency (65 patients, 89%), polypharmacy (37 patients, 51%), and
depressive symptoms (24 patients, 33%), while undernutrition (5 patients, 7%) and
cognitive impairment (5 patients, 7%) were less prevalent. Overall, only 21 patients had no
geriatric conditions (29%), 31 patients had one geriatric condition (42%), 16 patients had
two (22%) and five patients (7%) had three or more of the six examined geriatric
conditions. Table 2: Baseline geriatric assessment
Geriatric condition n= (%)
Charlson comorbidity index15 0‐1 64 (88%) 2+ 9 (12%)
Polypharmacy 0‐4 types of medication 36 (49%) 5+ types of medication 37 (51%)
Body Mass index (BMI) Undernutrition (BMI <20 kg/m2) Normal (BMI 20‐30 kg/m2) Overweight (BMI >30 kg/m2)
4 (5%) 64 (88%) 5 (7%)
IADL16 Fully independent (28‐30 points) 8 (11%) Partially dependent (14‐27 points) 65 (89%) Fully dependent (≤13 points) 0
Cognition (MMSE17) No cognitive dysfunction (24+ points) 68 (93%) Cognitive dysfunction (≤23 points) 5 (7%)
Mood (GDS18) No depressive symptoms (0‐4 points) 49 (67%) Mild depressive symptoms (5‐9 points) 21 (29%) Severe depressive symptoms (10+ points) 3 (4%) IADL instrumental activities of daily living, MMSE mini mental state examination, GDS geriatric depression scale
146

CGA predicts toxicity in elderly metastatic breast cancer patients
Based on the GFI, 41 patients (56%) were considered frail. The GFI was not able to
accurately predict outcome of CGA. Of the 52 patients deemed frail according to the CGA
(one or more geriatric conditions present), 36 were also frail based on the GFI. Of the 21
patients without geriatric conditions, 5 were considered frail based on the GFI. Thus, the
GFI had a sensitivity of 69% for frailty on CGA and a specificity of 76%, with a positive
redictive value of 88% and negative predictive value of 50%. p
Toxicity Eight patients experienced no chemotherapy‐related toxicity (11%); maximum
chemotherapy‐related toxicity was grade 1 for 14 patients (19%), grade 2 for 24 (33%),
grade 3 for 26 (36%) and grade 4 in one patient (1%). The most frequently occurring grade
3‐4 toxicities for liposomal doxorubicin were fatigue (n=5), stomatitis (n=4) and hand‐foot
syndrome (n=4). For capecitabine, the most prevalent grade 3‐4 toxicities were fatigue
(n=5) and hand‐foot syndrome (n=6). The incidence of grade 3‐4 toxicity did not differ
between the two types of chemotherapy (odds ratio (OR) for capecitabine versus
liposomal doxorubicin 0.93, 95% confidence interval (CI) 0.32‐2.67, p=1.00).
Figure 1: Association between number of geriatric conditions and percentage of patients with grade 3‐4 toxicity
147

Chapter 10
Table 3: Association between baseline factors and grade 3‐4 chemotherapy‐related toxicity
Univariate analysis* % of patients experiencing grade 3‐4 toxicity OR 95% CI p=
Chemotherapy arm Doxorubicin Capecitabine
14/37 (38%)13/36 (36%)
10.93
0.32‐2.67
1.00
Age >75 years <75 years ≥ 75 years
12/33 (36%)15/40 (38%)
11.05
0.40‐2.73
0.92
Performance status 0 1 2+
5/21 (24%)15/36 (42%)7/16 (44%)
12.252.43
0.61‐9.65
0.49‐12.98
0.25 0.29
Comorbidity 0‐1 2+
22/64 (34%)5/9 (56%)
12.36
0.46‐13.16
0.28
Polypharmacy no yes
6/36 (17%)21/37 (57%)
16.38
1.99‐23.47
0.001
Nutritional status (BMI) ≤ 20 20‐30 ≥ 30
1/4 (25%)24/64 (38%)2/5 (40%)
11.791.85
0.13‐98.32 0.06‐156.5
1.00 1.00
IADL independent dependent
2/8 (25%)25/65 (38%)
11.86
0.30‐20.24
0.70
Cognition normal impairment
25/68 (37%) 2/5 (40%)
11.14
0.09‐10.71
1.00
Depressive symptoms no mild severe
15/49 (31%)11/21 (52%)1/3 (33%)
12.431.13
0.77‐8.10
0.02‐23.31
0.11 1.0
* As only one factor demonstrated a p‐value <0.10, no multivariate analysis was performed. OR odds ratio, CI confidence interval, IADL instrumental activities of daily living, BMI body mass index
The proportion of patients that experienced grade 3‐4 toxicity increased rapidly with
increasing number of geriatric conditions (Figure 1): only 19% of patients without geriatric
conditions experienced grade 3‐4 chemotherapy‐related toxicity compared to 56% of
patients with two geriatric conditions and 80% of those with three or more (p=0.03). The
number of geriatric conditions remained predictive after correcting for potential
confounders such as age, performance status and chemotherapy arm (p=0.04).
The association between individual CGA components and grade 3‐4 chemotherapy‐related
toxicity can be found in Table 3. Polypharmacy was the only individual factor predictive of
grade 3‐4 toxicity, which occurred in 57% of patients using five or more types
of.medication compared to 17% of patients using 4 or less, resulting in an OR of 6.38
(95%CI.1.99‐23.47, p=0.002); this association was not altered by correction for potential
confounders. In addition, GFI was not associated with toxicity (OR 1.98, 95%CI 0.67‐6.13,
p=0.22). Grade 3‐4 chemotherapy related toxicity was experienced by 44% of patients GFI‐
frail and 28% of GFI‐fit patients.
148

CGA predicts toxicity in elderly metastatic breast cancer patients
Table 4: Multivariable Cox regression analyses for mortality, both for cumulative frailty (based on total number of geriatric conditions) and for individual geriatric conditions
Univariate analysis Multivariable analysis
HR 95% CI p= * HR 95% CI p= *
Chemotherapy arm PEGdoxorubicin capecitabine
10.85 0.50‐1.47
0.57
Age <75 years ≥ 75 years
12.04 1.16‐3.57
0.01 12.27 1.25‐4.13
0.01
Performance status 0 1 2
11.212.82
0.62‐2.341.31‐6.07
0.01 11.111.81
0.55‐2.23 0.74‐4.42
0.78 0.19
Comorbidity 0‐1 2+
11.72 0.84‐3.53
0.14
Polypharmacy no yes
11.41 0.82‐2.44
0.21
Nutritional status (BMI)
≤ 20 20‐30 ≥ 30
10630.67
0.19‐2.040.15‐3.01
0.74
IADL independent dependent
12.1 0.85‐5.43
0.10
Cognition normal impairment
13.74 1.43‐9.73
0.004 11.88 0.65‐5.45
0.24
Depressive symptoms
none mild severe
10.933.89
0.49‐1.751.41‐13.28
0.05 10.743.67
0.34‐1.64 0.88‐15.3
0.46 0.07
* Variables with a p‐value <0.10 in the univariate analysis were included in the multivariate analysis; these variables are marked in bold in the univariate p‐value column. HR hazard ratio, CI confidence interval, IADL instrumental activities of daily living, BMI body mass index
Association between frailty and survival After a median follow‐up of 32 months, 56 patients died. Median survival for fit patients
was 19.9 months versus 10.3 months for frail patients (p=0.04, Figure 2a). However, after
correction for age, performance status and chemotherapy type, this association was no
longer significant (hazard ratio (HR) 1.70, 95%CI 0.75‐3.84, p=0.2).
Of the individual geriatric conditions, both cognitive impairment (HR 3.76, 95%CI 1.43‐
9.73, p=0.004) and severe depressive symptoms (HR 3.89, 95%CI 1.14‐13.28, p=0.05) were
associated with overall mortality (Table 4), as well as age and performance status. In the
multivariable model, age over 75 years remained associated with higher mortality (HR
2.27, 95%CI 1.25‐4.13,p=0.01, Figure 2b) while severe depressive symptoms showed a
borderline significant association (HR 3.67, 95%CI 0.88‐15.3, p=0.07).
GFI was not associated with survival (HR 1.06, 95%CI 0.61‐1.82, p=0.85).
149

Chapter 10
Figure 2: Kaplan Meier survival plots for overall survival A. Fit (no geriatric conditions) versus frail patients (one or more geriatric conditions)
B. Patients younger and older than 75 years
150

CGA predicts toxicity in elderly metastatic breast cancer patients
Discussion In this study of elderly metastatic breast cancer patients receiving first‐line single‐agent
palliative chemotherapy, the number of geriatric conditions was a strong independent
predictor of severe chemotherapy‐related toxicity. Of individual geriatric conditions, only
polypharmacy was associated with toxicity while all other conditions were not. In this
study, the frailty screening tool GFI was not predictive of toxicity. For survival, older age
was the most important predictive factor.
Frailty has been defined as the final common pathway of ageing, caused by the cumulative
decline across multiple organ systems, and resulting in a decreased resistance to
stressors,7 such as chemotherapy. This suggests that it is the accumulation of deficits that
is determinative of a patient’s vulnerability to the development of adverse outcomes
when exposed to stressors, while the particulars of each deficit are of secondary
importance. In line with this perspective, we found that the number of geriatric conditions
was associated with toxicity but this association was seen for only one of the six individual
geriatric conditions. This confirms that it is the accumulation of deficits in geriatric
domains – irrespective of which geriatric domains – that is contributing to the vulnerability
of patients to develop toxicity.
To our knowledge only two prior studies have investigated the value of geriatric
assessments in breast cancer patients receiving palliative chemotherapy for predicting
toxicity of chemotherapy.19‐21 Similar to our study, patients (n=152) in the PELICAN
study19,20 were randomized between capecitabine and liposomal doxorubicin. In
accordance with our findings, an association between overall frailty on CGA (defined as
the presence of one or more geriatric conditions, irrespective of which conditions) and
toxicity was also found and additionally, polypharmacy was the only individual geriatric
condition associated with toxicity. The DOGMES study21 assessed the association between
individual geriatric conditions and toxicity in 60 metastatic breast cancer patients
receiving liposomal doxorubicin; this study found comorbidity – in particular the presence
of diabetes – to be associated with hematologic toxicity. Assessment of polypharmacy was
not included in their study.
No prior studies have assessed the association between overall frailty on CGA and survival
in patients with metastatic breast cancer. However, this association has been addressed in
six studies which included patients with other cancer types or heterogeneous cohorts of
patients with multiple types of malignancies, different stages of disease and various
treatment regimens.22‐28 Despite these disparities, all six studies found that frailty
diagnosed by CGA was predictive of mortality, irrespective of the underlying geriatric
condition(s) that caused the frailty. While we also found an association between frailty on
CGA and survival, this association was no longer significant after correction for age and
performance status, possibly due to the small number of patients. Two prior studies have
151

Chapter 10
assessed the predictive value of individual geriatric conditions for survival in metastatic
breast cancer patients. One study found that IADL function and comorbidity (assessed
using the cumulative illness rating scale – geriatric version (CIRS‐G)29 which takes severity
of comorbidity into account) were predictive19,20 while the other found that no particular
geriatric condition was associated with mortality.30 Neither found an association between
depressive symptoms and survival.
The predictive value of a CGA for chemotherapy‐related toxicity suggests that for optimal
decision making regarding treatment risks and potential benefits, a CGA should be
incorporated into the standard assessment of all elderly cancer patients if chemotherapy
is considered. One important barrier to such routine implementation of CGA is the fact
that performing a CGA can be time‐consuming. This has led cancer specialists to search for
possible short‐cuts, such as the use of frailty screening tools.31 If such a tool had sufficient
predictive value for relevant outcome measures, it could replace the CGA altogether. The
Groningen Frailty Index, which was used in our study, is one of the tools currently being
examined in this context. We did not find an association between GFI and outcome;
however, two other studies using GFI did find an association with survival32 and toxicity33.
Therefore, the value of GFI for predicting outcome deserves further examination. In
addition to frailty screening tools, two tools aimed specifically at predicting toxicity of
chemotherapy have been developed in the past year, using clinical, geriatric and
biochemical parameters;34,35 further studies are now undertaken to validate these tools in
other patient cohorts and will eventually elucidate their predictive value compared to a
more extensive CGA.
Frailty screening tools have also been used to select which patients should proceed with a
CGA and for which patients more elaborate assessment is unnecessary. However, the
sensitivity of GFI for the presence of geriatric conditions on CGA was only 69%, with a
specificity of 77%. With a resultant negative predictive value of around 50%, this means
that over half of patients deemed fit according to the GFI will be found to have geriatric
conditions after CGA. Therefore, GFI does not appear to be an adequate frailty screening
tool in this setting. Thus far, none of the currently available frailty screening tools has
demonstrated sufficient discriminative power to separate fit older cancer patients that are
able to receive standard cancer treatment based upon the complete treatment schedule,
from vulnerable patients that should subsequently receive a CGA to guide tailoring of their
treatment regimen.36
This study using geriatric assessments in elderly metastatic breast cancer patients treated
with palliative chemotherapy has several limitations. When the study was designed, we
followed the recommendations formulated by the International Society of Geriatric
Oncology in 2005,37 which state that a CGA for older cancer patients should consist of
assessment of cognitive function, mood and some measure of functional status, such as
152

CGA predicts toxicity in elderly metastatic breast cancer patients
IADL or ADL. More recently, studies using an elaborate CGA have shown that ADL and IADL
function may both be of value, as other measures such as a formal assessment of
nutritional status and mobility32,38‐41 which we did not include. Furthermore, the
discrepancy between a high prevalence of polypharmacy but low Charlson index scores
suggests that this may not be the optimal tool for quantifying comorbidity burden; in
several recent studies, the CIRS‐G – which includes a broader scope of diseases and a
measure of their severity – was shown to be a more suitable tool.20,29,42‐45 In addition, due
to difficulties in the accrual of elderly patients, the patient cohort is relatively small. On
the other hand, an important strength of our study is the homogeneity of the study
population, as only patients with a single type of malignancy and similar stage of disease
were included using a limited number of treatment regimens.
Further research is needed to confirm the value of cumulative frailty in predicting toxicity
of chemotherapy. To avoid previous issues caused by heterogeneity in study populations,
such studies will be most useful in populations with a specific type of malignancy, a similar
hase of the treatment process and a limited number of treatment regimens. p
In conclusion, this randomized study on first‐line single‐agent chemotherapy in elderly
metastatic breast cancer patients, baseline CGA demonstrated a strong predictive value
for grade 3‐4 toxicity of chemotherapy, suggesting that if chemotherapy is considered for
elderly patients, a geriatric assessment should be routinely incorporated in the
ssessment and decision‐making process. a
Financial support: the OMEGA study received unrestricted financial support from the
Dutch Cancer Society and Amgen BV the Netherlands, Janssen‐Cilag BV the Netherlands,
MSD the Netherlands.
153

Chapter 10
References 1. www.cbs.nl. 3‐2‐2012. 2. www.cijfersoverkanker.nl. 2‐3‐2012. 3. Hutchins LF, Unger JM, Crowley JJ et al. Underrepresentation of patients 65 years of age or older in cancer‐
treatment trials. N Engl J Med 1999;341:2061‐2067. 4. Peto R, Davies C, Godwin J et al. Comparisons between different polychemotherapy regimens for early
breast cancer: meta‐analyses of long‐term outcome among 100,000 women in 123 randomised trials. Lancet 2012;379:432‐444.
5. Extermann M, Overcash J, Lyman GH et al. Comorbidity and functional status are independent in older cancer patients. J Clin Oncol 1998;16:1582‐1587.
6. Louwman WJ, Vulto JC, Verhoeven RH et al. Clinical epidemiology of breast cancer in the elderly. Eur J Cancer 2007;43:2242‐2252.
7. Ferrucci L, Guralnik JM, Studenski S et al. Designing randomized, controlled trials aimed at preventing or delaying functional decline and disability in frail, older persons: a consensus report. J Am Geriatr Soc 2004;52:625‐634.
8. Extermann M, Aapro M, Bernabei R et al. Use of comprehensive geriatric assessment in older cancer patients: recommendations from the task force on CGA of the International Society of Geriatric Oncology (SIOG). Crit Rev Oncol Hematol 2005;55:241‐252.
9. Slaets JP. Vulnerability in the elderly: frailty. Med Clin North Am 2006;90:593‐601. 10. Extermann M, Meyer J, McGinnis M et al. A comprehensive geriatric intervention detects multiple
problems in older breast cancer patients. Crit Rev Oncol Hematol 2004;49:69‐75. 11. Terret C, Albrand G, Droz JP. Multidisciplinary geriatric assessment reveals unknown medical problems in
elderly cancer patietns. J Clin Oncol 2004;22:a8167 12. Repetto L, Fratino L, Audisio RA et al l. Comprehensive geriatric assessment adds information to Eastern
Cooperative Oncology Group performance status in elderly cancer patients: an Italian Group for Geriatric Oncology Study. J Clin Oncol 2002;20:494‐502.
13. Trotti A, Colevas AD, Setser A et al. CTCAE v3.0: development of a comprehensive grading system for the adverse effects of cancer treatment. Semin Radiat Oncol 2003;13:176‐181.
14. Aaronson NK, Ahmedzai S, Bergman B et al. The European Organization for Research and Treatment of Cancer QLQ‐C30: a quality‐of‐life instrument for use in international clinical trials in oncology. J Natl Cancer Inst 1993;85:365‐376.
15. Charlson ME, Pompei P, Ales KL, Mackenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987;40:373‐383.
16. Lawton MP, Brody EM. Assessment of older people: self‐maintaining and instrumental activities of daily living. Gerontologist 1969;9:179‐186.
17. Folstein MF, Folstein SE, McHugh PR. "Mini‐mental state". A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975;12:189‐198.
18. Sheikh JI, Yesavage JA, Brooks JO et al. Proposed factor structure of the Geriatric Depression Scale. Int Psychogeriatr 1991;3:23‐28.
19. De Wit M, Honecker F, Wedding U et al. Incorporation of a comprehensive geriatric assessment (CGA) into a randomized phase III trial for metastatic breast cancer (MBC): The PELICAN study. Journal of Clinical Oncology Conference: 2010;Suppl 1:28.
20. De Wit M, Harbeck N, Scholz M et al. Incorporation of a Comprehensive Geriatric Assessment (CGA) into a randomized phase III trial for metastatic breast cancer: The PELICAN Study. Journal of Clinical Oncology Conference: 2009;Suppl1:20.
21. Sostelly A, Falandry C, Pejuade‐Lauraine E et al. Predicting chemotherapy induced hematotoxicity in elderly paients with metastatic breast cancer treated by pegylated liposomal doxorubicin. J.Clin.Oncol. e19740. 2011.
22. Arnoldi E, Dieli M, Mangia M et al. Comprehensive geriatric assessment in elderly cancer patients: an experience in an outpatient population. Tumori 2007; 93(1):23‐25.
23. Bamias A, Lainakis G, Kastritis E et al. Biweekly carboplatin/gemcitabine in patients with advanced urothelial cancer who are unfit for cisplatin‐based chemotherapy: report of efficacy, quality of life and geriatric assessment. Oncology 2007; 73(5‐6):290‐297.
154

CGA predicts toxicity in elderly metastatic breast cancer patients
155
24. Basso U, Tonti S, Bassi C et al. Management of Frail and Not‐Frail elderly cancer patients in a hospital‐based geriatric oncology program. Crit Rev Oncol Hematol 2008; 66(2):163‐170.
25. Basso U, Falci C, Brunello A et al. Prognostic value of multidimensional geriatric assessment on survival of a prospective cohort of 880 elderly cancer patients. J.Clin.Oncol. S9065. 2011.
26. Poon D, Lee HH, Chan LL et al An exploratory analysis of comprehensive geriatric assessment results and overall survival in 233 consecutive elderly cancer patients. Journal of Clinical Oncology 2009;27 (15 SUPPL 1):9504.
27. Tucci A, Ferrari S, Bottelli C et al. A comprehensive geriatric assessment is more effective than clinical judgment to identify elderly diffuse large cell lymphoma patients who benefit from aggressive therapy. Cancer 2009;115:4547‐4553.
28. Brunello A, Monfardini S, Falci C et al. Prognostic role of comprehensive geriatric assessment (CGA): a prospective study of a cohort of 1038 elderly cancer patients. J Geriatr Oncol 2011;Suppl 1:36.
29. Miller MD, Paradis CF, Houck PR et al. Rating chronic medical illness burden in geropsychiatric practice and research: application of the Cumulative Illness Rating Scale. Psychiatry Res 1992;41:237‐248.
30. Freyer G, Lortholary A, Delcambre C et al. Unexpected toxicities in elderly patients treated with oral idarubicin in metastatic breast cancer: the GINECO experience. Clin Oncol (R Coll Radiol) 2004; 16:17‐23.
31. Maas HA, Janssen‐Heijnen ML, Olde Rikkert MG et al. Comprehensive geriatric assessment and its clinical impact in oncology. Eur J Cancer 2007;43:2161‐2169.
32. Aaldriks AA, Maartense E, le CS et al. Predictive value of geriatric assessment for patients older than 70 years, treated with chemotherapy. Crit Rev Oncol Hematol 2011;79:205‐212.
33. Van Fraeyenhove F, Baitar A, De VM et al. Prediction of chemotherapy toxicity by the groningen frailty index (GFI) and the comprehensive geriatric assessment (CGA) in elderly cancer patients (PTS): An interim analysis. Annals of Oncology 2010;Oct suppl:185.
34. Extermann M, Boler I, Reich RR et al. Predicting the risk of chemotherapy toxicity in older patients: The Chemotherapy Risk Assessment Scale for High‐Age Patients (CRASH) score. Cancer 2012;118:3377‐86.
35. Hurria A, Togawa K, Mohile SG et al. Predicting chemotherapy toxicity in older adults with cancer: a prospective multicentre study. J Clin Oncol 2011;29:3457‐3465.
36. Hamaker ME, Jonker JM, de Rooij SE et al C. Frailty screening tools for predicting outcome of a comprehensive geriatric assessment in older cancer patients. Lancet oncology in print. 2012.
37. Extermann M, Aapro M, Bernabei R et al. Use of comprehensive geriatric assessment in older cancer patients: recommendations from the task force on CGA of the International Society of Geriatric Oncology (SIOG). Crit Rev Oncol Hematol 2005;55:241‐252.
38. Biesma B, Wymenga AN, Vincent A et al. Quality of life, geriatric assessment and survival in elderly patients with non‐small‐cell lung cancer treated with carboplatin‐gemcitabine or carboplatin‐paclitaxel: NVALT‐3 a phase III study. Ann Oncol 2011;22:1520‐1527.
39. Honecker FU, Wedding U, Rettig K et al. Use of the Comprehensive Geriatric Assessment (CGA) in elderly patients (pts) with solid tumors to predict mortality. Journal of Clinical Oncology 2009;27 suppl 1: 9549.
40. Kanesvaran R, Li H, Koo KN, Poon D. Analysis of prognostic factors of comprehensive geriatric assessment and development of a clinical scoring system in elderly asian patients with cancer. J Clin Oncol 2011;29:3620‐3627.
41. Ramsdale EE, Polite N, Bylow KA et al. Relationship between components of the comprehensive geriatric assessment, chemotherapy dose intensity, and overall survival in a colorectal cancer cohort age 65 and older. J Clin Oncol 2011;S9000.
42. Kristjansson SR, Jordhoy MS, Nesbakken A et al. Which elements of a comprehensive geriatric assessment (CGA) predict post‐operative complications and early mortality after colorectal cancer surgery? Journal of Geriatric Oncology 2010;1:57‐65
43. Marinello R, Marenco D, Roglia D et al. Predictors of treatment failures during chemotherapy: A prospective study on 110 older cancer patients. Arch Gerontol Geriatr 2009;48:222‐226.
44. Soubeyran P, Rainfray M, Mathoulin‐Pelissier S et al. Screening of elderly patients with cancer for early death risk. Results of a prospective multicentric study of 364 patients under chemotherapy. Crit Rev Oncol Hematol 2006;S23.
45. Wedding U, Rohrig B, Klippstein A et al. Age, severe comorbidity and functional impairment independently contribute to poor survival in cancer patients. J Cancer Res Clin Oncol 2007; 133:945‐950.


Chapter 11
The value of geriatric assessments in predicting treatment tolerance and all‐cause
mortality in older cancer patients
M.E. Hamaker, A.G. Vos, C.H. Smorenburg, S.E. de Rooij, B.C. van Munster
The Oncologist 2012 Aug 31. [Epub ahead of print]

Chapter 11
Abstract Background: Awareness on the use geriatric assessments for older cancer patients is
increasing. The aim of this review was to summarize all available evidence on the
association between geriatric assessments and relevant oncologic outcomes.
Method: A systematic search in Medline and Embase of studies on geriatric assessment in
oncology, focusing on the association between baseline assessment and outcome.
Results: Literature search identified 2008 reports; 51 publications from 37 studies were
selected for inclusion in the review. The quality of studies was heterogeneous and
generally poor. A median of five geriatric conditions was assessed per study (interquartile
range 4‐8). Little consistency was found in the results of the studies. Furthermore,
different tools appear to be predictive depending on the outcome measure: frailty,
nutritional status and comorbidity assessed by the CIRS‐G were predictive for all‐cause
mortality; frailty was predictive for toxicity of chemotherapy; cognitive impairment and
ADL‐impairment for chemotherapy completion; and IADL impairment for perioperative
complications.
Conclusion: Although various geriatric conditions appear to be of some value in predicting
outcome in elderly cancer patients, results are too inconsistent to guide treatment
decisions. Further research is needed to elucidate the role of geriatric assessments in the
oncologic decision‐making process for these patients.
158

Review CGA and outcome in older cancer patients
Introduction Although malignant tumours occur at all ages, cancer disproportionately strikes individuals
aged 65 years and older,1 and the number of elderly cancer patients will increase
substantially in the coming decades as a result of increasing life expectancy and ageing of
the population. Oncologists are faced with the challenge of determining the optimal
treatment for these patients, with their heterogeneity in comorbidity, physical reserve,
disability and geriatric conditions. In this context, a myriad of editorials and review articles
have been published, endorsing the use of a comprehensive geriatric assessment (CGA) in
geriatric oncology.2‐9 A CGA is a systematic procedure used to objectively appraise the
health status of older people, focusing on somatic, functional and psychosocial domains,2
aimed at constructing a multidisciplinary treatment plan. Its value in geriatric medicine
has been proven extensively,10 but outside this field, the evidence is more scarce.
Oncology studies comparing treatment choices in patients that are considered fit or frail
on the basis of a CGA have shown that frail patients receive less intensive treatment or
receive no treatment at all.11,12 Although this shows that standard medical assessment
overlaps in part with geriatric assessment, an additional value of the latter is its ability to
identify previously unrecognised but potentially modifiable health issues, such as
depressive symptoms, cognitive or functional impairment and malnutrition.4,5,7 In
addition, some studies are now using CGA to assess patients for trial eligibility or to
allocate them to alternative treatments regimens.13,14 However, the legitimacy of such
decision‐making protocols has been insufficiently proven thus far. It remains unclear how
to translate data from the CGA to clinical practice; should geriatric assessment only be
used to classify patients as fit, vulnerable or frail, or do individual geriatric conditions have
predictive value for relevant patient outcomes?
Therefore, the aim of this systematic review is to summarize all available evidence on the
association between CGA – its individual domains as well as the summarized assessment
of vulnerability – and clinically relevant outcomes, such as all‐cause mortality,
chemotherapy toxicity, chemotherapy completion, perioperative complications and
diotherapy tolerance. ra
Methods
Search strategy and article selection Our aim was to identify cohort studies which investigated the association between
baseline geriatric assessment and outcome in cancer patients, independent of age, cancer
type or stage of disease. For this purpose, a geriatric assessment was defined as an
assessment using validated assessment tools, composed of two or more of the following
distinct domains: cognitive function, mood/depression, nutritional status, activities of
159

Chapter 11
daily living (ADL), instrumental activities of daily living (IADL), comorbidity, polypharmacy,
mobility/falls, and frailty. Studies only using non‐validated assessment tools or non‐
validated subscales of validated assessment tools were excluded. We also excluded
studies that included other patient groups in addition to cancer patients, or studies using a
treatment protocol in which the outcome of the geriatric assessment determined
treatment choice.
For outcome, the following items were defined: all‐cause mortality, toxicity of
chemotherapy, chemotherapy completion, perioperative complications, and radiotherapy
completion and toxicity.
We performed the following search in both Medline and Embase on February 15th 2012:
(("Geriatric Assessment"[Mesh]) OR (geriatric assessment*[tiab])) AND
(("Neoplasms"[Mesh]) OR (neoplasm*[tiab] OR cancer*[tiab] OR tumour[tiab] OR
tumours[tiab] OR tumour[tiab] OR tumors[tiab] OR oncolog*[tiab] OR malignan*[tiab])).
No limits in age, language or publication date were applied to the search.
In addition, conference abstracts for the 2007 to 2011 scientific meetings of the American
Society of Clinical Oncology (ASCO), European Society of Medical Oncology (ESMO),
International Society of Geriatric Oncology (SIOG), American Geriatric Society (AGS) and
European Geriatric Medicine Society (EUGMS) were hand‐searched for studies on geriatric
assessments in cancer patients to identify additional eligible studies.
The titles and abstracts of all studies retrieved by the search were assessed by one
investigator (MH) to determine which were eligible for further investigation. All potentially
relevant articles were subsequently screened as full text by two authors (MH and AV). In
case only an abstract was available, we attempted to find a final report of the study by
searching Embase and Medline using the names of first, second and/or final authors as
well as key words from the title. Also, in case of insufficient data in the original
manuscript, the authors were contacted for additional information, for example on the
tools used in the geriatric assessment.
Finally, references of included publications were cross‐referenced to retrieve any
dditional relevant citations. a
Data extraction Data regarding study design and results were independently extracted by two
investigators (MH and AV) for each eligible study. Items that were extracted were the type
of study, study setting, study population (cancer type, cancer stage, cancer treatment),
content of geriatric assessment and assessment tools used, outcome measures examined,
methods of statistical analysis, and the reported results on the association between
geriatric assessments and the outcome measures.
160

Review CGA and outcome in older cancer patients
Quality assessment The methodological quality of each of the studies was independently assessed by two
reviewers (MH and AV). Disagreements among the reviewers was discussed during a
consensus meeting and in case of persisting disagreement, the assistance of a third
reviewer (BvM) was enlisted. We used a standardised list of 16 criteria to assess the
methodological quality of the included studies. This list was a modified version of the
checklist used by Kuijpers et al,15 based on the theoretical considerations and
ethodological aspects described by Altman16 (Appendix 1a). m
Data synthesis and analysis As a result of heterogeneity in study designs, diversity of patient populations and the wide
variety in content of the geriatric assessment, a formal meta‐analysis was not possible.
Therefore, we summarized the study results to describe our main outcomes of interest. If
necessary, reciprocal odds ratios or hazard ratios were calculated for optimizing
comparability of data. When applicable, subgroup summaries were made based on the
tools used in the assessment of the geriatric conditions.
Figure 1: Search results and study selection
All studies n=2008 Medline n= 893 Embase n= 962 Conference abstracts n= 153
Duplicates n=614
Exclusion n=1343 Not original research n=566 Not oncology n=340 No geriatric assessment n=148 No relevant outcome n=143 No association GA with outcome n=122 GA guided treatment n= 13 Study announcement only n= 3 Non‐cancer patients included n= 2 Assessment unclear n= 2 Non‐validated assessment tools n= 4 for individual domains
Cross referencing yielded no additional studies Inclusion: 51 publications from 37 studies
161

Chapter 11
Table 1: Characteristics of included studies
Author Publication year
Full text
Setting/department Study population
Aaldriks 17,18
2010, 2011 yes medical oncology dept various
Aparicio19,20
2011 no medical oncology/ gastroenterology dept
metastatic colon cancer
Arnoldi 21 2007 yes various various
Audisio22 2003 yes surgical oncology dept various
Bamias 23 2007 yes clinical therapeutics dept irresectable bladder cancer
Basso 24 2008 yes medical oncology ward various
Biesma 25‐27
2007, 2009, 2011 yes medical oncology dept NSCLC
Brunello 28,29
2010,2011 no medical oncology dept various
Brunello 30 2008 no medical oncology dept metastatic renal cell cancer
Castagneto 31 2004 yes oncology dept bladder cancer
De Wit 32,33
2009, 2010 no medical oncology dept metastatic breast cancer
Extermann36 2011 yes medical oncology dept various
Freyer 34 2005 yes medical oncology dept advanced ovarian cancer
Freyer 35 2004 yes medical oncology dept metastatic breast cancer
Hamaker 37 2011 yes general medicine ward various
Honecker 38 2009 no internet based registry various solid tumours
Hurria 39,40
2010, 2011 yes medical oncology dept various solid tumours
Hurria 41 2006 yes medical oncology dept breast/lung/prostate cancer
Kanesvaran 42‐44
2010, 2011, 2011 yes geriatric oncology clinic various
Karampeazis 45 2011 no medical oncology dept advanced NSCLC
Klepin46 2011 no medical oncology dept acute myologenous leukaemia
Kothari 47,48
2010, 2011 yes thoracic surgery dept various
Kristjansson 49‐51
2008, 2010, 2010 yes surgery dept colorectal cancer
Maione 52 2005 yes medical oncology dept advanced NSCLC
Marinello 53 2009 yes geriatric/oncology unit lung/colon/breast cancer
PACE‐participants 54,55
2006, 2008 yes surgical oncology dept various
Pilnik 56 2010 no medical oncology dept lung cancer
Poon 57 2009 no national cancer centre various
Ramsdale 58 2011 no oncology dept colorectal cancer
Sostelly 59 2011 no medical oncology dept metastatic breast cancer
Soubeyran 60 2006 no medical oncology dept various
Tahir 61 2010 no breast cancer clinic early breast cancer
Tredan 62 2006 yes medical oncology dept advanced ovarian cancer
Tucci 63 2009 yes medical oncology dept diffuse large cell lymphoma
v Fraeyenhove 64 2010 no medical oncology dept various
Wedding 65,66
2007, 2010 yes medical oncology ward various
Zagonel 67 2002 no medical oncology dept various
* CT chemotherapy CTRT chemoradiation ** M all‐cause mortality, tox chemotherapy toxicity,
162

Review CGA and outcome in older cancer patients
Table 1: Characteristics of included studies
Types of treatment*
Number of patients
Median age in years (range)
Number of assessed conditions
Summary score used
Outcome measures examined**
CT 202 77.2 (71‐92) 3 M CC
CT 123 80 (75‐91)
4 tox CC
various 153 76 (70‐91) 5 + M
surgery 72 77 (70‐92) 5 S
CT 32 75.5 (57‐84) 4 + M
CT 117 75 (70‐92) 7 M CC
CT 182 74 (70‐87) 8 M tox CC
CT 1038 77 (70‐92) 6 + M
CT 28 73.6 (70‐81) 7 + tox
CT 25 76 (71‐87) 3 M
CT 152 61 (22‐85) 4 + M tox CC
CT 518 75.5 (70‐92) 6 tox
CT 83 76 (70‐90) 3 M tox
CT 26 70+ 6 M
various 292 74.9 (65‐96) 8 M
various 1130 76.3 (69‐95) 7 M
CT 500 73 (65‐91) 5 tox
CT 20 75 (66‐84) 4 tox
unclear 249 77 (70‐94) 8 M
CT 131 74 (65‐92) 5 tox
CT 74 70 (±6.2) 4 M
surgery 60 76 (?) 5 S
surgery 182 80 (70‐94) 7 + M
CT 566 74 (70‐84) 3 M
CT 110 75 (70‐87) 4 M tox CC
surgery 460 76.9 (70‐95) 5 S
CT/CTRT 130 ? 4 tox
various 233 77 (70‐93) 7 + M
CT 38 72 (65‐89) 5 M CC
CT 60 ? 4 tox
CT 364 77.5 (70‐99) 7 M
unclear 124 82 (70‐94) 5 M
CT 155 75.5 (70‐90) 5 M
CT 84 73 (66‐89) 3 + M
CT 21 71.2 (66‐86) 8 + tox
CT 427 ?(18‐80+) 3 M
various 252 72 (65‐94) 2 M
CC chemotherapy completion, S surgery NSCLC = non‐small cell lung cancer
163

Chapter 11
Results
Study characteristics The literature search identified 1855 citations (893 from Medline and 962 from Embase),
of which 61 were duplicates. Hand‐searching of conference abstracts yielded another 153
potentially relevant publications. Details on the search and reasons for exclusion can be
found in Figure 1. After exclusion of 1343 publications, 51 publications from 37 studies
were included in this review.17‐67 Cross‐referencing yielded no additional results.
The characteristics of these 37 studies are summarized in Table 1. The first publication is
from 2002, but more than half of the studies were published in the last two years.17‐67 All
but one study consisted of prospective cohorts.24 The median sample size was 152
patients (range 20‐1130 patients).17‐67 Study populations were heterogeneous, with only
half focusing on a specific type of cancer,19,20,23,25‐27,30‐35,45,46,49‐52,56,58,59,61‐63 of which eleven
also focused on a specific cancer stage (30% of all studies).19,20,23,30,32‐35,45,52,59,61‐63
Furthermore, while 26 studies focused on chemotherapy (70%)17‐20,23‐36,39‐41,45,46,52,53,56,58‐
60,62‐66 and four studies focused on surgery (11%),22,47‐51,54,55 seven studies included
patients receiving multiple treatment modalities (19%).21,37,38,42‐44,57,61,67
The median number of geriatric conditions that were assessed was five (interquartile
range 4 – 8, Table 1).17‐67 Table 2 gives an overview of the geriatric conditions included in
the studies and the method of assessment,68‐93 a more detailed overview per study can be
found in Appendix 2. Ten studies summarized results of geriatric assessment in a summary
score (27%).21,23,24,28‐30,32,33,49‐51,57,63,64 Two used the cumulative number of geriatric
conditions57,64 as a summary and eight defined patients as frail if they were ADL‐
dependent, had 3 or more comorbidities (or one severe comorbid conditions) or one or
more geriatric conditions.21,23,24,28‐30,32,33,49‐51,63
The association between geriatric assessment and all‐cause mortality was assessed in 25
out of 37 studies (68%, Table 1),17,18,21,23‐29,31‐35,37,38,42‐44,46,49‐53,57,58,60‐67 chemotherapy
toxicity in 13 (35%)19,20,25‐27,30‐36,39‐41,45,53,56,59,64 and chemotherapy completion in seven
(19%).17‐20,24‐27,32,33,53,58 Four studies focused on the association between geriatric
assessment and perioperative complications (11%).22,47‐51,54,55 No studies were found on
eriatric assessment in relation to radiotherapy. g
Study quality The quality of the studies was heterogeneous, with a median score of 9 out of the sixteen
items on the quality checklist (interquartile range 7‐11). Reviewer agreement was >95%
for all aspects. In‐ and exclusion criteria and patient population were clearly described in
22 and 26 studies, respectively. The participation rate ‐ i.e. the percentage of potential
164

Review CGA and outcome in older cancer patients
Table 2: Content of geriatric assessments in included studies
Condition No. of studies assessing condition (%)
Assessment tool used for assessing condition
No. of studies using tool
Instrumental activities of daily living (IADL)
32 (86%) Lawton & Brody68 NEADL69 PAT‐D93
30 1 1
Comorbidity 32 (86%) Charlson70 CIRS‐G71 Satariano72 No. of conditions
12*
12 2 7
Activities of daily living (ADL) 31 (84%) Barthel73 Katz 74 OARS76 PAT‐D
93 Unclear
6 22 1 1 1
Cognition 26 (70%) MMSE75 IQcode77 Blessed
78 SPMSQ79
23* 2 1 1
Mood/depression 24 (65%) GDS80 HADS
81 PANAS82 SCID84 CES‐D
91
18* 4 1 1 1
Polypharmacy 13 (35%) No. of pills 12
Nutritional status 9 (24%) MNA83 Determine85 SNAQ86 NHI NHC
**
6 1 1 1
Mobility 9 (24%) TUG90 SPPB92
7 2
Frailty screening 6 (16%) GFI87 VES‐1388 Fried89
3 2 1
* some studies used more than one tool to assess the domain ** no reference available NEADL Nottingham extended activities of daily living, PAT‐D Pepper Assessment Tool for Disability, CIRS‐G cumulative illness rating scale‐geriatrics, OARS Older American Resources and Services, MMSE mini mental state examination, IQCODE informant questionnaire on cognitive decline in the elderly, SPMSQ short portable mental status questionnaire, GDS geriatric depression scale, HADS hospital anxiety and depression scale, SCID structured clinical interview for DSM IV CES‐D Centre for Epidemiologic Studies‐Depression scale MNA mini nutritional assessment, SNAQ short nutritional assessment questionnaire, NHI NHC national health initiative nutritional health checklist, TUG timed get‐up‐and‐go SPPB short physical performance battery, GFI Groningen frailty index, VES‐13 vulnerable elders scale‐13
165

Chapter 11
participants that received a geriatric assessment ‐ was only described in nine studies and
although 21 studies listed the duration of follow‐up, only eight described the number of
patients lost to follow‐up or compared completers with non‐completers. Only thirteen
studies described the completeness of data. Outcome reporting was of better quality, with
28 studies providing data from univariable analyses for the association of geriatric
assessments with outcome measures and 24 presenting some form of prognostic model.
However, reporting of associations was differed notably between studies, with some
presenting odds ratios, others hazard ratios and others only p‐values to indicate a
statistical significance without reporting on the actual odds/hazard ratio or confidence
interval. This complicated any comparison of data and hindered combining data for a
formal meta‐analysis. Furthermore, three studies did not appear to have sufficient
numbers for their multivariable analyses. Full results for the quality assessment can be
und in Appendix 1b. fo
All‐cause mortality The predictive value of geriatric assessments for all‐cause mortality was reported in 25
studies (Table 3). Six studies addressed the association of a summary score with mortality:
all six found that frail patients showed poorer overall survival (100%).21,23,24,28,29,57,63 In
these studies, median survival was between 1.6 and 3.7 times longer for fit patients
compared to frail subjects. Likewise, frailty assessed with a formal frailty screening tool
was found to be associated with mortality, in three out of four studies (75%).17,18,23,25,58
Nutritional status was found to be associated with mortality in all four studies in which it
was assessed (100%).17,18,42,50,58,60 For comorbidity, initial analysis revealed that only six out
of sixteen studies found an association with mortality (38%). However, when subdividing
according to the assessment method used, only one out of five studies using the Charlson
comorbidity index38 and none of the four studies using the number of comorbid conditions
found an association, while four out of five studies using the CIRS‐G found comorbidity
was associated with mortality (80%).33,50,53,60,65 For one study, the results for comorbidity
were not clearly reported. Of the 14 studies addressing cognitive function, only two found
an association between cognition and mortality.38,61 Only four out of fourteen studies
found an association between ADL‐impairment and mortality (29%),25,38,46,61,67 and six out
of sixteen reported finding an association for IADL‐impairment (38%).25,33,38,46,52,67 Results
for mood/depression, mobility and polypharmacy were inconclusive with approximately
equal numbers of studies that did and did not find an association. All of these results were
not altered when correcting for the assessment tool that was used.
166

Review CGA and outcome in older cancer patients
Table 3: Association of geriatric assessment with all‐cause mortality
Author
Number of
patients
Can
cer type
Summary score
Cognition
Mood/depression
Mobility
ADL
IADL
Nutritional status
Frailty screening
Comorbidity
Polypharmacy
De Wit 32,33
152 Breast + + + + – –
Freyer 35 26 Breast – – – – – –
Tahir 61 124 Breast + + – – + + – – – –
Kristjansson 49‐51
182 Colorectal – – – – – – – – + + + + – –
Ramsdale 58 38 Colorectal – – – – – – + + – –
Biesma 25‐27
182 Lung – – + + + + + + + + + ?
Maione 52 566 Lung – – + + – –
Tucci 63 84 Lymphoma +
Klepin46 74 AML – – ++ – – ++
Bamias 23 32 Bladder + –
Castagneto 31 25 Bladder – – –
Freyer 34 83 Ovarian – – – – + +
Tredan 62 151 Ovarian – – + + – – ± – –
Aaldriks 17,18
202 Various – – + + + +
Arnoldi 21 153 Various +
Basso 24 117 Various +
Brunello28 29 1038 Various + +
Hamaker 37 292 Various – – – – – – – – – – –
Honecker 38 1130 Various + + + + + + +
Kanesvaran 42‐44
249 Various – – + + – – – – + + – – – –
Marinello 53 110 Various – – – – – – + +
Poon 57 233 Various + + ±
Soubeyran 60 364 Various – – – – – – – – – – + + – –
Wedding 65,66
437 Various – – ± + +
Zagonel 67 252 Various + + + +
++ / ‐ ‐ : significant / no association in multivariable analysis, respectively. Of note, there was little uniformity across studies in the confounders and variables included in these analysis + / ‐: significant / no association in univariable analysis, respectively, no multivariable analysis performed or factor not included in multivariable analysis ?: association not described in the publication ±: association only present in subgroup of patients but not all patients (I)ADL: (instrumental) activities of daily living AML: acute myologenous leukaemia
167

Chapter 11
Toxicity of chemotherapy Results for toxicity of chemotherapy and chemotherapy completion are listed in Table 4.
For toxicity, the score summarizing geriatric assessment was found to be associated with
toxicity of chemotherapy in two out of three studies (66%), but these only reported
univariable results.33,64 Similarly, two out of three studies found an association between
toxicity and a frailty screening tool.56,64 For all other geriatric conditions, results were quite
variable across studies. Polypharmacy was associated with toxicity in two out of four.33,56
Comorbidity was associated with toxicity of chemotherapy in only three out of ten
studies.53,56,59 Method of assessing for comorbidity did not influence results. Toxicity of
chemotherapy was associated with impaired cognition in 17% of studies, depressed mood
in 13%, impaired mobility in 33%, ADL impairment in 0%, and IADL‐impairment in 18%,
spectively (Table 4). re
Chemotherapy completion For completion of chemotherapy, impaired cognitive function was found to be associated
with less completion or the need for dose reduction in two out of three studies (66%,
Table 4).17‐20 ADL‐impairment showed similar results (association in two out of three
studies).25,58 Furthermore, three out of five studies.33,53,58 found that comorbidity was
predictive of lower completion rates (60%). Two of these used the CIRS‐G and one the
Charlson comorbidity index to assess comorbidity; the two studies that did not find an
association both used the Charlson comorbidity index. One study addressed nutritional
status, and found an association in their multivariable analysis.17,18 Data was inconclusive
for the summary score (association in one of two studies, 50%), and negative for
epressed mood, impaired mobility, IADL impairment and the presence of frailty (Table 4). d
Perioperative complications Four studies addressed the association between geriatric assessment and perioperative
complications (Table 4). Only one study assessed the association of a summary score and
found it to be associated with perioperative complications (100%).49 This association was
found for IADL‐impairment in three out of the four studies.47,49,54 For depressed mood,
results were inconclusive with only two out of four studies finding an association.47,49 For
ADL‐impairment, polypharmacy, nutritional status, cognitive function and comorbidity, no
r little association was found. None of the studies used a frailty screening tool. o
Radiotherapy toxicity/completion No studies were identified that addressed the association between geriatric assessments
and toxicity or completion of radiotherapy. One study assessed patients receiving
chemotherapy or chemoradiation, but did not report separately on the latter group.56
168

Review CGA and outcome in older cancer patients
Table 4: Association of geriatric assessment with treatment complications/completion
Outcome
Author
Can
cer type
Number of
patients
Summary score
Cognition
Mood/depression
Mobility
ADL
IADL
Nutritional status
Frailty screening
Comorbidity
Polypharmacy
De Wit 32,33
Breast 152 + – – – +
Sostelly 59 Breast 60 – – – – – – + + + +
Aparicio 19,20
Colorectal 123 + + – – + + – –
Biesma 25‐27
Lung 182 + + – – – – – – – – – –
Karampeazis 45 Lung 131 – – – – –
Pilnik 56 Lung 130 – – + +
Brunello 30 Renal cell 28 –
Freyer 34 Ovarian 83 – – – – – –
Castagneto 31 Bladder 25 – – –
Extermann36 Various 518 ± – – ± ± – – – –
Hurria 39,40
Various 500 – – – – + + + + ?
Hurria 41 Various 20 – – – –
Marinello 53 Various 110 – – – – – – + +
CHEM
OTHER
APY
TOXICITY
Van Fraeyenhove 64 Various 21 + +
De Wit 32,33
Breast 152 – – – + –
Aparicio 19,20
Colorectal 123 + + – – – – – –
Ramsdale 58 Colorectal 38 – – + + + + ? – – + +
Biesma 25‐27
Lung 182 – – – – + + + + – – – –
Aaldriks 17,18
Various 202 + + + + – –
Basso 24 Various 117 + C
HEM
OTHER
APY
COMPLETION
Marinello 53 Various 110 – – – – – – + +
Kristjansson 49‐51
Colorectal 182 + + – – + + – – + + – – + + – –
Audisio 22 Various 72 – – + – –
Kothari 47,48
Various 60 + – + –
PER
IOPER
ATIVE
COMPLICATIONS
PACE‐participants 54
Various
460
– –
– –
– –
+ +
– –
++ / ‐ ‐ : significant / no association in multivariable analysis, respectively. Of note, there was little uniformity across studies in the confounders and variables included in these analysis + / ‐: significant / no association in univariable analysis, respectively; no multivariable analysis performed or factor not included in multivariable analysis ?: association not described in the publication ±: association only present in for a particular type of toxicity but not all toxicity (I)ADL: (instrumental) activities of daily living
169

Chapter 11
Discussion In this review on the value of geriatric assessments in predicting treatment tolerance and
all‐cause mortality in older cancer patients, little consistency was found between the
results of the various studies. Interestingly, different geriatric conditions appear to be
predictive for the primary outcome measures: frailty, nutritional status and comorbidity
(when measured with CIRS‐G) for all‐cause mortality; frailty for toxicity of chemotherapy;
cognitive function and ADL‐impairment for chemotherapy completion; and IADL‐
impairment for perioperative complications. However, the only truly consistent finding
was the association between a summary score of the geriatric assessment and mortality.
The studies included in this systematic review were heterogeneous in design, content and
reported outcomes. In addition, reporting was frequently too inadequate to assess
potential sources of bias. It was often unclear whether outcome of geriatric assessment
was known to the treating physician, allowing differences in overall survival to be caused
by the reception of suboptimal oncologic treatment based on the outcome of geriatric
assessment (and subsequently the assumption that patients would not be able to tolerate
standard treatment). Another potential bias is that the patients participating in studies
focusing on chemotherapy and surgery were already preselected as suitable for this
treatment by their physician. Thus, while many geriatric conditions were not predictive of
toxicity, one cannot conclude that patients should receive chemotherapy irrespective of –
for example – their cognitive status or IADL‐score.
These factors limited our possibilities of performing a formal meta‐analysis and drawing
definitive conclusions. One method to solve some of these issues would be to perform an
individual patient data analysis using the original data of included studies. A second
limitation of this review is that it focuses on studies assessing multiple geriatric conditions.
Studies focusing on single conditions or including multiple conditions but not identified as
geriatric assessment would not have been selected from Medline or Embase with our
search strategy. Despite these limitations, this review does provide a thorough overview
of the currently available evidence on the value of geriatric assessment for predicting
relevant outcomes in older cancer patients.
The results of this review have several clinical implications. First of all, although various
geriatric conditions appear to have some predictive value for each of the four outcome
measures, the lack of consistency in the findings does not support excluding patients from
certain treatment options based solely on their score on a geriatric assessment tool.
A second clinical implication of this review is that while current geriatric assessments used
in oncology primarily focus on cognitive function, mood/depression, and functional
limitations, less frequently examined geriatric conditions, such as malnutrition and
polypharmacy appear to be of similar or even greater predictive value and are potentially
modifiable; therefore, their assessment should not be omitted. Also, it appears that
170

Review CGA and outcome in older cancer patients
assessment of comorbidity without including a measure for the severity of these
conditions is not useful, and therefore, we recommend using the CIRS‐G rather that the
Charlson comorbidity index, despite that fact that the former is more time‐consuming.71,94
Interestingly, assessment of mobility – which is one of the cornerstones of geriatric
medicine – is rarely included. Given its predictive value in the general geriatric population,
this element of CGA deserves further exploration.95
Various factors may have contributed to the variation in the results of the included
studies. First of all, it appears that the choice of assessment tool influences outcome, as
illustrated by the fact that comorbidity assessed by CIRS‐G was associated with mortality
but when assessed with the Charlson, it was not. Heterogeneity in patient populations will
also have contributed to the variation in study outcomes: not only do different elements
of the CGA appear to be predictive depending on the outcome measure that is examined,
but it is possible that the specific characteristics and prognosis of a malignancy will also
affect the predictive value of various geriatric syndromes. All these factors mean that
finding that one optimal assessment tool that will be predictive of all outcome measures
in all patient populations and all treatment settings may not be feasible.
On the other hand, the results of our systematic review suggest that in predicting
outcome, it may be more important to determine whether or not a patient is frail than to
determine what makes him or her frail. This fits with the definition of frailty as the final
common pathway of ageing,96 where the presence of deficits in geriatric domains is the
determinative factor while the particulars of each deficit are of secondary importance. If
this be the case, a short frailty screening tool could potentially suffice in allocating a
patient to standard treatment of tailored care, and the time‐consuming process of a
formal geriatric assessment could be avoided.40,47,97 This does require that this tool has a
high sensitivity for frailty, allowing the assessor to trust that those patients deemed fit,
actually are fit.88 Those who are not, should then receive further assessment to ascertain
their ability to tolerate treatment. However, there is still much debate on the precise
definition of frailty and how it should be measured, and as yet, there is insufficient
evidence on the quality of the various screening tools in predicting fitness in this particular
setting to endorse one tool over the others.98
Ultimately, in limiting the use of a systematic geriatric assessment in oncology practice to
a decision‐making tool, the potential benefit of using the CGA to optimize care for elderly
patients with cancer is overlooked. For example, although a cognitive disorder does not
necessarily predict chemotherapy toxicity, it potentially means that a patient may not
respond adequately in case of complications, or will not take oncologic or supportive
medication as prescribed; these patients may require extra monitoring or home health
care. Similarly, addressing previously undiagnosed depressive symptoms or malnutrition
can improve a patient's resilience when undergoing treatment. A geriatric assessment
171

Chapter 11
could thus be seen as a starting point for further treatment and care, for improving not
only the outcomes addressed in this review, but also quality of life or functional capacity.
However, as a formal comprehensive geriatric assessment is time‐consuming, and a
geriatric consultation is often a scarce commodity, it may be useful to develop screening
tools that are particularly suitable for finding those patients at high risk for having geriatric
onditions that are modifiable or require intervention.99 c
In conclusion, this systematic review shows that although different geriatric conditions
appear to be predictive for each of the major outcome measures, currently available
evidence is too inconsistent to guide clinical decision making. Many questions remain
unanswered and will require further exploration. To elucidate the impact of the various
geriatric conditions on treatment tolerance and outcome for older cancer patients, future
clinical research should use broad geriatric assessments that address all geriatric
conditions, and include ‘geriatric’ outcome measures, such as functional capacity, in
addition to standard oncologic outcomes. Furthermore, research should focus on
validating screening tools that predict fitness rather than frailty, and on applying geriatric
assessment as an intervention aimed at optimizing a patient's resilience during treatment,
rather than as a decision‐making tool only.
172

Review CGA and outcome in older cancer patients
Appendix 1a: Criteria for quality assessment, based on Kuijpers et al15 and Altman
16
Criterion Score* Positive (+) if
Study population
A Inception cohort + – ? moment of inclusion is related to same point in the course of disease or treatment
B Descriptions of inclusion and exclusion criteria
+ ? clearly described
C Description of study population + ? setting, age and sex, cancer type and cancer treatment patients is described
Participation
D Participation rate + – ? less than 10% of potential patients did not receive geriatric assessment
E Information about participants vs. non‐participants
+ – description of non‐participants/reason for not participating is available
Follow‐up
F Prospective data collection + – ? prospective data collection or a historical cohort in which the determinants have been measured before the outcome was determined
G Duration + – length of follow‐up has been described
H Loss‐to‐follow‐up + – ? loss to follow‐up is less than 10%
I Information of completers vs. loss to follow up
+ – ? description of those patients lost to follow‐up is available
Geriatric assessment
J Standardized assessment of geriatric conditions
+ ? clear description of tools used for geriatric assessment and, if applicable, cut‐off values described
K Completeness of geriatric assessment data
+ – ? less than 10% missing data
Outcome
L Treatment decision blinded to outcome of geriatric assessment
+ – ? blinding process is clearly described
M Standardized assessment of relevant outcome criteria
+ – ? definitions of the used outcome measures are stated or standard definitions are used
N Outcome assessment blinded for baseline geriatric assessment
+ – ? blinding of outcome assessor for baseline geriatric assessment is mentioned
Data presentation
O Appropriate analysis + – ? univariable crude estimates are provided for the association of CGA (components) with outcome measure
P Prognostic model presented + – an attempt is made to determine a set of prognostic markers with the highest prognostic value
Q Sufficient numbers + – number of cases in the multivariable analysis is at least ten times the number of independent variables in the analysis
* evaluation is positive ( + ) if sufficient information is available and criteria in Appendix 1a are met; negative ( – ) if sufficient information is available but there is potential for bias due to inadequate design or conduct; ? signifies insufficient information for evaluating criterion. na = not applicable
173

Chapter 11
Appendix 1b: Quality assessment of included studies
Publication Study population Participation Follow‐up Geriatric assessment
Outcome Data presentation
Author
Inception cohort
Description of in–
and exclusion
Description of
patient population
Participation rate
Data on
participants vs.
Prospective data
collection
Description of
follow–up duration
Loss to follow–up
Data on completers
vs. lost to follow‐up
Standardized
assessmen
t of
geriatric conditions
Completeness of
data collection
Treatm
ent blinded
for GA outcome
Standardization of
outcome measures
Outcome
assessmen
t blinded
Appropriate
li
Prognostic m
odel
presented
Sufficient numbers
Aaldriks 17,18 + + + ? – + + ? – + + ? + ? + + +
Aparicio 19,20 + ? + – – + + ? – + ? ? + ? – + +
Arnoldi 21 – ? ? ? – + + ? – + ? ? + na + + +
Audisio 22 + + + + – + + + – + + ? + + + – na
PACE‐participants 54 + + + ? – + + ? – + ? + + ? + + +
Bamias 23 + + + + + + + ? – + ? + + ? + – na
Basso24 + + + + + – + ? – + ? ? + ? + – na
Biesma 25‐27 + + + + + + + ? – + + + + ? + + +
Brunello 28,29 – ? + ? – + + ? – + + ? + ? + + +
Brunello 30 + ? ? ? – + – ? – + + ? – ? ? – na
Castagento 31 + + + + – + + + + + + ? + ? – – na
De Wit 32,33 + ? + – – + – ? – ? ? + ? ? + + +
Extermann36 + + + + + + + + + – + + + ? + + +
Freyer 34 + + + ? – + – ? – + + ? + ? + + +
Freyer 35 + + + ? – + – ? – ? – ? + ? + – na
Hamaker 37 – + + ? – + + + – + – + + na + + +
Honecker 38 – ? + ? – + + ? – ? ? ? + ? + – na
Hurria 39,40 + ? ? ? – + – ? – + ? ? ? ? – + +
Hurria 41 + + + + + + – ? – + + ? + ? + – na
Kanesvaran 42‐44 + + ? ? – + – ? – + + ? + na + + +
Karampeazis 45 + ? ? ? – + – ? – ? ? ? + ? + – na
Klepin46 + + + ? – + + ? – + ? + + na ? + –
Kothari 47,48 + + + ? – + – ? – + ? + – + – – –
Kristjansson 49‐51 + + + – + + + + + + – + + ? + + +
Maione 52 + + + ? – + + ? – + + + + na + + +
Marinello 53 + + + ? – + + + + + + ? + ? + + +
Pilnik 56 ? + ? ? – + – ? – ? ? ? + ? ? – na
Poon 57 – ? ? ? – + – ? – ? ? ? + ? + + +
Ramsdale 58 + ? + ? – + – ? – ? ? ? + ? + + –
Sostelly 59 + ? ? ? – + – ? – ? ? ? + ? ? + ?
Soubeyran 60 + ? + ? – + – ? – ? ? ? + na + + +
Tahir 61 – ? ? ? – + + ? – + ? ? + na – + +
Tredan 62 + + + + + + – + + + – + + ? + + +
Tucci63 + + + + – + – + + + + ? + ? + – na
Van Fraeyenhove 64 + ? ? ? – + + ? – + ? ? + ? + – na
Wedding 65,66 + + + ? – + + ? – + – + + na + + +
Zagonel 67 + ? ? ? – + + ? – + ? ? + na + + +
na: not applicable
174

Review CGA and outcome in older cancer patients
Appendix 2: Content of geriatric assessments
Author
Cognition
Mood/
depression
Mobility
ADL
IADL
Nutritional
status
Frailty
screening
Comorbidity
Polypharmacy
Composition of
summary score
(if ap
plicab
le)*
Aaldriks 17,18
MMSE IQcode
MNA GFI
Aparicio 19,20
MMSE GDS Lawton Charlson
Arnoldi 21 MMSE GDS Barthel Lawton Charlson A
Audisio 22 MMSE GDS Katz Lawton Satariano
Bamias 23 Katz Lawton VES‐13 Charlson A
Basso 24 MMSE GDS Katz Lawton CIRS‐G + A
Biesma 25‐27
MMSE GDS15PANAS
TUG Katz Lawton GFI Charlson CIRS‐G
Brunello 28,29
MMSE GDS Katz Lawton CIRS‐G + A
Brunello 30 MMSE GDS Katz Lawton CIRS‐G + A
Castagneto 31 GDS Katz Lawton
De Wit 32,33
Barthel Lawton CIRS‐G + A
Extermann36 MMSE GDS Lawton MNA CIRS‐G +
Freyer 34 MMSE # +
Freyer 35 MMSE HADS TUG Lawton # +
Hamaker 37 IQcode Katz Lawton SNAQ Charlson +
Honecker 38 MMSE SCID TUG Barthel Lawton Charlson +
Hurria 39,40
Blessed HADS TUG OARS Lawton #
Hurria 41 GDS Katz Lawton Charlson
Kanesvaran 42‐44
MMSE GDS15 Katz Lawton Determine Charlson +
Karampeazis 45 MMSE GDS15 Katz Lawton CIRS‐G
Klepin46 CES‐D SPPB PAT‐D PAT‐D
Kothari 47,48
MMSE GDS15 Katz Lawton NHI NHC
Kristjansson 49‐51
MMSE GDS30 Barthel NEADL MNA CIRS‐G + A
Maione 52 Katz Lawton Charlson
Marinello 53 SPMSQ Katz Lawton CIRS‐G
PACE‐participants 54 MMSE GDS Katz Lawton Satariano
Pilnik 56 X Lawton # +
Poon 57 MMSE GDS TUG Katz Lawton MNA Charlson B
Ramsdale 58 MMSE SPPB Katz VES‐13 Charlson
Sostelly 59 HADS Katz Lawton Fried #
Soubeyran 60 MMSE GDS15 TUG Katz Lawton MNA CIRS‐G
Tahir 61 MMSE GDS Barthel Lawton #
Tredan 62 MMSE HADS Lawton # +
Tucci 63 Katz CIRS‐G A
Van Fraeyenhove 64 MMSE GDS TUG Katz Lawton MNA GFI Charlson B
Wedding 65,66
Barthel Lawton CIRS‐G
Zagonel 67 Katz Lawton
* composition of summary score: A – frail if ADL‐dependent, 3+ comorbidities or 1+ severe comorbidities, or 1+ geriatric conditions; B – number of geriatric conditions; x assessed but method not stated; # number of conditions See next page for further information
175

Chapter 11
Continuation of Appendix 2: NEADL Nottingham extended activities of daily living, PAT‐D Pepper Assessment Tool for Disability, CIRS‐G cumulative illness rating scale‐geriatrics, OARS Older American Resources and Services, MMSE mini mental state examination, IQCODE informant questionnaire on cognitive decline in the elderly, SPMSQ short portable mental status questionnaire, GDS geriatric depression scale, HADS hospital anxiety and depression scale, SCID structured clinical interview for DSM IV CES‐D Centre for Epidemiologic Studies‐Depression scale MNA mini nutritional assessment, SNAQ short nutritional assessment questionnaire, NHI NHC national health initiative nutritional health checklist, TUG timed get‐up‐and‐go SPPB short physical performance battery, GFI Groningen frailty index, VES‐13 vulnerable elders scale‐13
176

Review CGA and outcome in older cancer patients
References 1. Muss HB. Cancer in the elderly: a societal perspective from the United States. Clin Oncol (R Coll Radiol )
2009; 21:92‐98. 2. Extermann M, Aapro M, Bernabei R et al. Use of comprehensive geriatric assessment in older cancer
patients: recommendations from the task force on CGA of the International Society of Geriatric Oncology (SIOG). Crit Rev Oncol Hematol 2005;55:241‐252.
3. Rodin MB, Mohile SG. A practical approach to geriatric assessment in oncology. J Clin Oncol 2007;25:1936‐1944.
4. Extermann M, Overcash J, Lyman GH et al. Comorbidity and functional status are independent in older cancer patients. J Clin Oncol 1998;16:1582‐1587.
5. Extermann M, Meyer J, McGinnis M et al. A comprehensive geriatric intervention detects multiple problems in older breast cancer patients. Crit Rev Oncol Hematol 2004;49:69‐75.
6. Terret C, Zulian GB, Naiem A, Albrand G. Multidisciplinary approach to the geriatric oncology patient. J Clin Oncol 2007;25:1876‐1881.
7. Terret C, Albrand G, Droz JP. Multidisciplinary geriatric assessment reveals unknown medical problems in elderly cancer patients. J Clin Oncol 2004;22[14S]:8167.
8. Gosney M. Contribution of the geriatrician to the management of cancer in older patients. Eur J Cancer 2007; 43:2153‐2160.
9. Brunello A, Sandri R, Extermann M. Multidimensional geriatric evaluation for older cancer patients as a clinical and research tool. Cancer Treat Rev 2009;35:487‐492.
10. Ellis G, Whitehead MA, O'Neill D et al. Comprehensive geriatric assessment for older adults admitted to hospital. Cochrane Database Syst Rev 2011;7:CD006211.
11. Barthelemy P, Heitz D, Mathelin C et al. Adjuvant chemotherapy in elderly patients with early breast cancer. Impact of age and comprehensive geriatric assessment on tumor board proposals. Crit Rev Oncol Hematol 2011;79:196‐204.
12. Klepin HD, Gajra A, Hardt N et al. Predictors of primary dose reduction among patients aged 65 years and older receiving adjuvant chemotherapy. J Clin Oncol 2011:S9003.
13. Tirelli U, Fratino L, Balzarotti M et al. Comprehensive geriatric assessment‐adapted chemotherapy in elderly patients (>70 years) with diffuse large B‐Cell non‐hodgkin's lymphoma (DLBCL): Final results and long term follow‐up. Blood 2009;114.
14. Corre R, Chouaid C, Barlesi F et al. Study ESOGIA‐GFPC 08‐02: Phase III, randomized multicentre trial involving subjects over age 70 with stage IV non small cell lung cancer, comparing a "classical" strategy of treatment allocation, based on performance status and age, with an "optimized" strategy allocating the same treatments according to a simplified geriatric assessmnet screening scale plus a more thorough geriatric assessment if necessary. ASCO meeting abstract 2011;TPS219.
15. Kuijpers T, van der Windt DA, van der Heijden GJ, Bouter LM. Systematic review of prognostic cohort studies on shoulder disorders. Pain 2004;109:420‐431.
16. Altman DG. Systematic reviews of evaluations of prognostic variables. BMJ 2001;323:224‐228. 17. Aaldriks AA, Maartense E, le Cessie S et al. Predictive value of geriatric assessment for patients older than
70 years, treated with chemotherapy. Crit Rev Oncol Hematol 2011;79:205‐212. 18. Aaldriks AA, Maartense E, Giltay EJ et al. The impact of geriatric assessment on the outcome of older breast
cancer patients treated with chemotherapy. J Geriatr Oncol 2011;2suppl1:S29. 19. Aparicio T, Jouve JL, Teillet L et al. Geriatric factors to predict toxicity and dose‐intensity reduction in FFCD
2001‐02 phase III study comparing a first‐line chemotherapy of LV5FU2 or FOLFIRI in treatment of metastatic colorectal cancer in elderly patients. J Clin Oncol 2011;S9111.
20. Aparicio T, Jouve JL, Teillet F et al. Geriatric factors to predict toxicity and dose‐intensity reduction in FFCD 2001‐02 phase III study comparing a first line chemotherapy with LV5FU2 or FOLFIRI in treatment of metastatic colon cancer in elderly patients. J Geriatr Oncol 2011;2suppl1:S61.
21. Arnoldi E, Dieli M, Mangia M et al R. Comprehensive geriatric assessment in elderly cancer patients: an experience in an outpatient population. Tumori 2007;93:23‐25.
22. Audisio RA, Gennari R, Sunouchi K et al l. Preoperative assessment of cancer in elderly patients: a pilot study. Support Cancer Ther 2003;1:55‐60.
177

Chapter 11
23. Bamias A, Lainakis G, Kastritis E et al. Biweekly carboplatin/gemcitabine in patients with advanced urothelial cancer who are unfit for cisplatin‐based chemotherapy: report of efficacy, quality of life and geriatric assessment. Oncology 2007;73:290‐297.
24. Basso U, Tonti S, Bassi C et al. Management of Frail and Not‐Frail elderly cancer patients in a hospital‐based geriatric oncology program. Crit Rev Oncol Hematol 2008;66:163‐170.
25. Biesma B, Wymenga AN, Vincent A et al l. Quality of life, geriatric assessment and survival in elderly patients with non‐small‐cell lung cancer treated with carboplatin‐gemcitabine or carboplatin‐paclitaxel: NVALT‐3 a phase III study. Ann Oncol 2011;22:1520‐1527.
26. Wymenga M, Biesma B, Vincent A et al. Platinum‐based combination chemotherapy in the treatment of older non‐small cell lung cancer (NSCLC) patients (pts): Is there a role for Complete Geriatric Assessment (CGA)? Final results from the prospective multicentre NVALT‐3 study. Journal of Clinical Oncology 2009; e20547.
27. Wymenga M, Biesma B, Vincent A et al. Can baseline complete geriaric assessment predict toxicity in elderly non‐small cell lung cancer patients? J Clin Oncol 2007;S7537.
28. Brunello A, Monfardini S, Falci C et al. Prognostic role of comprehensive geriatric assessment (CGA): a prospective study of a cohort of 1038 elderly cancer patients. J Geriatr Oncol 2011;2Suppl1: S36.
29. Basso U, Falci C, Brunello A et al. Prognostic value of multidimensional geriatric assessment on survival of a prospective cohort of 880 elderly cancer patients. J Clin Oncol 2011;S9065.
30. Brunello A, Sacco C, Barile C et al. Sunitinib in elderly patients (>=70 years) with metastatic renal cell carcinoma (MRCC): Multicentre analysis of tolerability and efficacy. Annals of Oncology 2008;viii:209.
31. Castagneto B, Zai S, Marenco D et al l. Single‐agent gemcitabine in previously untreated elderly patients with advanced bladder carcinoma: response to treatment and correlation with the comprehensive geriatric assessment. Oncology 2004;67:27‐32.
32. De Wit M, Honecker F, Wedding U et al. Incorporation of a comprehensive geriatric assessment (CGA) into a randomized phase III trial for metastatic breast cancer (MBC): The PELICAN study. Journal of Clinical Oncology 2010;suppl:1.
33. De Wit M, Harbeck N, Scholz M et al. Incorporation of a Comprehensive Geriatric Assessment (CGA) into a randomized phase III trial for metastatic breast cancer: The PELICAN Study. Journal of Clinical Oncology 2009; 27:9551.
34. Freyer G, Geay JF, Touzet S et al l. Comprehensive geriatric assessment predicts tolerance to chemotherapy and survival in elderly patients with advanced ovarian carcinoma: a GINECO study. Ann Oncol 2005;16:1795‐1800.
35. Freyer G, Lortholary A, Delcambre C et al. Unexpected toxicities in elderly patients treated with oral idarubicin in metastatic breast cancer: the GINECO experience. Clin Oncol (R Coll Radiol ) 2004; 16:17‐23.
36. Extermann M, Boler I, Reich RR et al. Predicting the risk of chemotherapy toxicity in older patients: The Chemotherapy Risk Assessment Scale for High‐Age Patients (CRASH) score. Cancer 2012;118:3377‐86.
37. Hamaker ME, Buurman BM, van Munster BC, et al. The Value of a Comprehensive Geriatric Assessment for Patient Care in Acutely Hospitalized Older Patients with Cancer. Oncologist 2011;16:1403‐12
38. Honecker FU, Wedding U, Rettig K et al. Use of the Comprehensive Geriatric Assessment (CGA) in elderly patients (pts) with solid tumors to predict mortality. Journal of Clinical Oncology 2009;27:a9549.
39. Hurria A, Togawa K, Mohile SG et al. Predicting chemotherapy toxicity in older adults with cancer: A prospective 500 patient multicentre study. Journal of Clinical Oncology 2010;28:1.
40. Hurria A, Togawa K, Mohile SG, et al. Predicting chemotherapy toxicity in older adults with cancer: a prospective multicentre study. J Clin Oncol 2011;29:3457‐3465.
41. Hurria A, Fleming MT, Baker SD et al. Pharmacokinetics and toxicity of weekly docetaxel in older patients. Clin Cancer Res 2006;12:6100‐6105.
42. Kanesvaran R, Li H, Koo KN, Poon D. Analysis of prognostic factors of comprehensive geriatric assessment and development of a clinical scoring system in elderly asian patients with cancer. J Clin Oncol 2011;29:3620‐3627.
43. Kanesvaran R, Li H, Koo K, Poon D. An analysis of prognostic factors of comprehensive geriatric assessment (CGA) and development of a clinical scoring system in elderly Asian cancer patients. Journal of Clinical Oncology 2010;28:1.
44. Kanesvaran R, Koo KN, Chen W, Poon D. An analysis of the prognostic value of handgrip strength and its incorporation into the comprehensive geriatric assessment in elderly Asian patients with cancer. J Clin Oncol 2011: S9093.
178

Review CGA and outcome in older cancer patients
45. Karampeazis A, Vamvakas L, Agelaki S et al l. Baseline comprehensive geriatric assessment (CGA) and prediction of toxicity in eldelry non‐small cell lung cancer (NSCLC) patients receiving chemotherapy. J Clin Oncol 2011:e19656.
46. Klepin HD, Tooze JA, Geiger AM et al. Geriatric assessment predicts overall survival among older adults receiving induction chemotherapy for acute myologenous leukemia. J Geriatr Oncol 2011; 2suppl1:S32.
47. Kothari A, Phillips S, Bretl T et al Components of geriatric assessments predict thoracic surgery outcomes. J Surg Res 2011;166:5‐13.
48. Weigel T, Kothari A, Bretl T et al. An abbreviated thoracic onco geriatric assessment (TOGA) and its components predict outcomes of esophagectomies. Annals of Surgical Oncology 2010:17:S128.
49. Kristjansson SR, Nesbakken A, Jordhoy MS et al. Comprehensive geriatric assessment can predict complications in elderly patients after elective surgery for colorectal cancer: a prospective observational cohort study. Crit Rev Oncol Hematol 2010;76:208‐217.
50. Kristjansson SR, Jordhoy MS, Nesbakken A et al. Which elements of a comprehensive geriatric assessment (CGA) predict post‐operative complications and early mortality after colorectal cancer surgery? Journal of Geriatric Oncology 2010;1:57‐65.
51. Kristjansson SR, Nesbakken A, Jordhoy MS, Wyller TB. Comprehensive geriatric assessment predicts complications in elderly patients operated for colon cancer. Crit Rev Oncol Hematol 2008;68:S24.
52. Maione P, Perrone F, Gallo C et al. Pretreatment quality of life and functional status assessment significantly predict survival of elderly patients with advanced non‐small‐cell lung cancer receiving chemotherapy: a prognostic analysis of the multicentre Italian lung cancer in the elderly study. J Clin Oncol 2005;23:6865‐6872.
53. Marinello R, Marenco D, Roglia D et al. Predictors of treatment failures during chemotherapy: A prospective study on 110 older cancer patients. Arch Gerontol Geriatr 2009;48:222‐226.
54. Audisio RA, Pope D, Ramesh HS et al. Shall we operate? Preoperative assessment in elderly cancer patients (PACE) can help. A SIOG surgical task force prospective study. Crit Rev Oncol Hematol 2008;65:156‐163.
55. Ramesh HS, Pope D, Stotter A et al. Testing CGA components to predict 30 day surgery outcome in elderly cancer patients. Crit Rev Oncol Hematol 2006;S21.
56. Pilnik NG, Ibero MM, Carri D, Mareca O. Influence of some clinical parameters in the tolerance to treatment in elderly patients with advanced lung cancer. Journal of Clinical Oncology 2010;15suppl:1.
57. Poon D, Lee HH, Chan LL et al. An exploratory analysis of comprehensive geriatric assessment results and overall survival in 233 consecutive elderly cancer patients. Journal of Clinical Oncology 2009;27suppl1:9504.
58. Ramsdale EE, Polite N, Bylow KA et al. Relationship between components of the comprehensive geriatric assessment, chemotherapy dose intensity, and overall survival in a colorectal cancer cohort age 65 and older. J Clin Oncol 2011;S9000.
59. Sostelly A, Falandry C, Pejuade‐Lauraine E et al. Predicting chemotherapy induced hematotoxicity in elderly paients with metastatic breast cancer treated by pegylated liposomal doxorubicin. J Clin Oncol 2011:e19740.
60. Soubeyran P, Rainfray M, Mathoulin‐Pelissier S et al. Screening of elderly patients with cancer for early death risk. Results of a prospective multicentric study of 364 patienets under chemotherapy. Crit Rev Oncol Hematol 2006;S23.
61. Tahir M, Pretorius R, Robinson T et al. Optimising the management of breast cancer in older patients. European Journal of Surgical Oncology 2010;36:1117‐1118.
62. Tredan O, Geay JF, Touzet S et al. Carboplatin/cyclophosphamide or carboplatin/paclitaxel in elderly patients with advanced ovarian cancer? Analysis of two consecutive trials from the Groupe d'Investigateurs Nationaux pour l'Etude des Cancers Ovariens. Ann Oncol 2007;18:256‐262.
63. Tucci A, Ferrari S, Bottelli C et al. A comprehensive geriatric assessment is more effective than clinical judgment to identify elderly diffuse large cell lymphoma patients who benefit from aggressive therapy. Cancer 2009;115:4547‐4553.
64. Van Fraeyenhove F, Baitar A, De VM et al. Prediction of chemotherapy toxicity by the groningen frailty index (GFI) and the comprehensive geriatric assessment (CGA) in elderly cancer patients (PTS): An interim analysis. Annals of Oncology 2010;21
65. Wedding U, Rohrig B, Klippstein A et al. Age, severe comorbidity and functional impairment independently contribute to poor survival in cancer patients. J Cancer Res Clin Oncol 2007;133:945‐950.
66. Winkelmann N, Petersen I, Kiehntopf M et al. Results of comprehensive geriatric assessment effect survival in patients with malignant lymphoma. J Cancer Res Clin Oncol 2011;137:733‐738.
179

Chapter 11
67. Zagonel V, Fratino L, Piselli P et al. The comprehensive geriatric assessment predicts mortality among elderly cancer patients. Proc Am Thorac Soc 2002;21:abstract 1458.
68. Lawton MP, Brody EM. Assessment of older people: self‐maintaining and instrumental activities of daily living. Gerontologist 1969;9:179‐186.
69. Nouri FM, Lincoln NB. An extended activities of daily living index for stroke patients. Clin Rehabil 1987;1:301‐305.
70. Charlson ME, Pompei P, Ales KL, Mackenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987;40:373‐383.
71. Miller MD, Paradis CF, Houck PR et al. Rating chronic medical illness burden in geropsychiatric practice and research: application of the Cumulative Illness Rating Scale. Psychiatry Res 1992; 41:237‐248.
72. Satariano WA, Ragland DR. The effect of comorbidity on 3‐year survival of women with primary breast cancer. Ann Intern Med 1994;120:104‐110.
73. Barthel D. Functional evaluation: the Barthel index. Md State Med J 1965;14:61‐65. 74. Katz S, Ford AB, Moskowitz RW et al. Studies of illness in the aged. The index of ADL: a standardized
measure of biological and psychological function. JAMA 1962;185:914‐919. 75. Folstein MF, Folstein SE, McHugh PR. "Mini‐mental state". A practical method for grading the cognitive
state of patients for the clinician. J Psychiatr Res 1975;12:189‐198. 76. Fillenbaum GG, Smyer MA. The development, validity, and reliability of the OARS multidimensional
functional assessment questionnaire. J Gerontol 1981;36:428‐434. 77. Jorm AF, Jacomb PA. The Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE): socio‐
demographic correlates, reliability, validity and some norms. Psychol Med 1989;19:1015‐1022. 78. Blessed G, Tomlinson BE, Roth M. The association between quantitative measures of dementia and of
senile change in the cerebral grey matter of elderly subjects. Br J Psychiatry 1968; 114(512):797‐811. 79. Pfeiffer E. A short portable mental status questionnaire for the assessment of organic brain deficit in elderly
patients. J Am Geriatr Soc 1975;23:433‐441. 80. Sheikh JI, Yesavage JA, Brooks JO et al. Proposed factor structure of the Geriatric Depression Scale. Int
Psychogeriatr 1991;3:23‐28. 81. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand 1983;67:361‐370. 82. Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative
affect: the PANAS scales. J Pers Soc Psychol 1988;54:1063‐1070. 83. Vellas B, Guigoz Y, Garry PJ et al. The Mini Nutritional Assessment (MNA) and its use in grading the
nutritional state of elderly patients. Nutrition 1999;15:116‐122. 84. First MG, Spitzer RL, Gibbon M, Williams JB. Structured Clinical Interview for DSM‐IV Axis I Disorders.
Clinical version, administration booklet. New York: Biometrics Research Department, New York State Psychiatric Institute; 1997.
85. Posner BM, Jette AM, Smith KW, Miller DR. Nutrition and health risks in the elderly: the nutrition screening initiative. Am J Public Health 1993;83:972‐978.
86. Kruizenga HM, Seidell JC, de Vet HC et al. Development and validation of a hospital screening tool for malnutrition: the short nutritional assessment questionnaire (SNAQ). Clin Nutr 2005;24:75‐82.
87. Slaets JP. Vulnerability in the elderly: frailty. Med Clin North Am 2006;90:593‐601. 88. Saliba D, Orlando M, Wenger NS et al Identifying a short functional disability screen for older persons. J
Gerontol A Biol Sci Med Sci 2000;55:M750‐M756. 89. Fried LP, Tangen CM, Walston J et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci
Med Sci 2001;56:M146‐M156. 90. Mathias S, Nayak US, Isaacs B. Balance in elderly patients: the "get‐up and go" test. Arch Phys Med Rehabil
1986; 67:387‐389. 91. Radloff LS. The CES‐D scale. Applied Phychological Management 1977;1:385‐401. 92. Guralnik JM, Simonsick EM, Ferrucci L et al. A short physical performance battery assessing lower extremity
function: association with self‐reported disability and prediction of mortality and nursing home admission. J Gerontol 1994;49:M85‐M94.
93. Rejeski WJ, Ip EH, Marsh AP et al. Measuring disability in older adults: the International Classification System of Functioning, Disability and Health (ICF) framework. Geriatr Gerontol Int 2008;8:48‐54.
94. Lee L, Cheung WY, Atkinson E, Krzyzanowska MK. Impact of comorbidity on chemotherapy use and outcomes in solid tumors: a systematic review. J Clin Oncol 2011;29:106‐117.
95. Studenski S, Perera S, Patel K et al. Gait speed and survival in older adults. JAMA 2011;305:50‐58.
180

Review CGA and outcome in older cancer patients
181
96. Ferrucci L, Guralnik JM, Studenski S et al. Designing randomized, controlled trials aimed at preventing or delaying functional decline and disability in frail, older persons: a consensus report. J Am Geriatr Soc 2004;52:625‐634.
97. Overcash JA, Beckstead J, Moody L et al. The abbreviated comprehensive geriatric assessment (aCGA) for use in the older cancer patient as a prescreen: scoring and interpretation. Crit Rev Oncol Hematol 2006;59:205‐210.
98. Hamaker ME, Jonker JM, de Rooij SE et al. Frailty screening tools for predicting outcome of a comprehensive geriatric assessment in older cancer patients. Lancet oncology in print. 2012.
99. Maas HA, Janssen‐Heijnen ML, Olde Rikkert MG, Machteld Wymenga AN. Comprehensive geriatric assessment and its clinical impact in oncology. Eur J Cancer 2007;43:2161‐2169.


Chapter 12
Frailty screening tools for predicting outcome of a comprehensive geriatric assessment in older cancer patients:
a systematic review
M.E. Hamaker, J.M. Jonker, S.E. de Rooij, A.G. Vos, C.H. Smorenburg, B.C. van Munster
Lancet Oncology 2012;13:e437‐e444

Chapter 12
Abstract Aim: To assess which frailty screening tools demonstrate the best sensitivity and
specificity for predicting the presence of impairments on comprehensive geriatric
assessment (CGA) in older cancer patients.
Method: A systematic search in Medline and Embase and hand‐search of conference
abstracts, for studies on the association between frailty screening tools and CGA in older
cancer patients.
Results: Literature search identified 4440 reports, of which 22 publications from 14
studies, assessing seven different frailty screening tools, were included in the review.
Median sensitivity and specificity of the screening tools for frailty on CGA were
respectively: Vulnerable Elders Survey‐13 (VES‐13) 68%/78%, Geriatric 8 (G8) 87%/61%,
Triage Risk Screening tool (TRST, cut‐off 1+) 91%/±45%, Groningen Frailty Index (GFI) ±50%
/±75%, Fried frailty criteria, ±30%/±90%, Barber 59%/79%, and abbreviated CGA (aCGA)
51%/97%. However, even in case of the highest sensitivity, the negative predictive value
was only 60%.
Conclusion: G8 and TRST demonstrated the highest sensitivity for frailty, but had a poor
specificity and negative predictive value. These findings suggest that for now, it may be
beneficial for all older cancer patients to receive a complete geriatric assessment as the
currently available frailty screening tools have insufficient discriminative power in
selecting patients for further assessment.
184

Frailty screening tools in geriatric oncology
Introduction Although malignant tumours occur at all ages, cancer disproportionately strikes individuals
aged 65 years and older,1 and the number of elderly cancer patients will increase
substantially in the coming decades as a result of increasing life expectancy and ageing of
the population. Cancer specialists are faced with the challenge of determining the optimal
treatment for these patients, with their heterogeneity in comorbidity, physical reserve,
disability and geriatric conditions.
For this purpose, two concepts of geriatric medicine are being incorporated in geriatric
oncology: the concept of frailty and the comprehensive geriatric assessment. Frailty is
considered as a state of decreased physiological reserves, arising from cumulative deficits
in multiple physiological systems, resulting in a diminished resistance to stressors.2,3 As
cancer and its treatment both form significant stressors, requiring patients to encroach on
their reserves, the concept of frailty appears particularly relevant for older cancer
patients. As yet, there is no consensus on its operationalization. The original definition of
frailty as formulated by Fried et al. focuses primarily on physical weakness and wasting,
but many other definitions and criteria have been postulated, incorporating different
aspects of ageing that contribute to diminishing reserves.4‐6
In geriatric oncology, the comprehensive geriatric assessment (CGA) is used to detect
disabilities and geriatric conditions that potentially contribute to frailty. A CGA is a
systematic procedure used to objectively appraise the health status of older people,
focusing on somatic, functional and psychosocial domains,7 and its value in geriatric
medicine has been proven extensively.8 However, as a CGA is time‐consuming, research is
now focusing on screening tools to separate fit older cancer patients that are able to
receive standard cancer treatment based upon the complete treatment schedule, from
vulnerable patients that should subsequently receive a CGA to guide tailoring of their
treatment regimen.9
In this context, the sensitivity of a frailty screening tool is considered to be of prime
importance; this will allow the treating physician to trust that frail patients will correctly
be identified by the screening tool.10,11 However, to optimize the time‐saving potential of a
two‐stepped approach, a good specificity of the screening tool is also required to ensure
that the number of fit patients incorrectly identified as frail on the screening tool and thus
unnecessarily receive a CGA, will be limited. To determine which screening tool best
meets both criteria, we performed a systematic review to assess the sensitivity and
specificity of frailty screening tools in predicting the presence of impairments on a CGA.
185

Chapter 12
Methods
Search strategy and selection criteria Our aim was to identify cohort studies which investigated the association between an
established frailty screening tool and a more complete CGA in cancer patients,
independent of age, cancer type or stage of disease.
The following search was performed on December 28th 2011, in both Medline and
Embase: ((("Geriatric Assessment"[Mesh]) OR (gfi[tiab] OR groningen frailty index[tiab])
OR (tfi[tiab] OR tilburg frailty index[tiab]) OR (isar[tiab] OR identification seniors at
risk[tiab]) OR (G8[tiab]) OR (fried[tiab]) OR (barber[tiab]) OR (edmonton[tiab]) OR
(saop[tiab] OR senior adult oncology program[tiab]) OR (triage risk screening tool[tiab])
OR (runciman rowland questionnaires[tiab]) OR (ves 13 OR vulnerable elderly survey[tiab])
OR (abbreviated comprehensive geriatric assessment[tiab] OR acga[tiab]) OR (geriatric
assessment*[tiab])) OR ((screening tool*[tiab]) AND (elderl*[tiab] OR geriatri*[tiab] OR old
age[tiab]))) AND (("Neoplasms"[Mesh]) OR (neoplasm*[tiab] OR cancer*[tiab] OR
tumour[tiab] OR tumours[tiab] OR tumor[tiab] OR tumors[tiab] OR oncolog*[tiab] OR
malignan*[tiab])).
No language limits or date ranges were applied.
In addition, conference abstracts of the scientific meetings from 2007‐2011 of the
American Society of Clinical Oncology (ASCO), European Society of Medical Oncology
(ESMO), International Society of Geriatric Oncology (SIOG), American Geriatric Society
(AGS) and European Geriatric Medicine Society (EUGMS) were hand‐searched for studies
on CGA in cancer patients to identify additional eligible studies.
We defined a frailty screening tool as a tool designed to assess the concept of frailty,
irrespective of the population or purpose for which this tool is intended. A CGA was
defined as an assessment using validated assessment tools investigating at least three of
the following domains: cognitive function, mood/depression, nutritional status, activities
of daily living (ADL), instrumental activities of daily living (IADL), comorbidity,
polypharmacy, mobility/falls, and/or social support. Studies were not eligible for inclusion
in this review if the study cohort included non‐cancer patients. We also excluded studies if
the CGA was only performed in a subgroup of patients selected by the outcome of the
frailty screening tool(s). For studies which included more than one screening tool,
eligibility was assessed separately for each tool.
The titles and abstracts of all studies retrieved by the searches were assessed by one
reviewer (MH) to determine which warrant further examination. All potentially relevant
articles were subsequently screened as full text by two authors (MH and JJ). If only an
abstract was available, an effort was made to find the final report of the study by
searching Embase and Medline using the names of first, second and/or final authors as
186
Frailty screening tools in geriatric oncology
well as key words from the title. Also, in case of insufficient data in the original
manuscript, the authors were contacted for additional information, for example on the
ols used in the geriatric assessment or the cut‐off value of the screening tool. to
Data extraction Data regarding study design and results were independently extracted by two
investigators (MH and JJ) for each eligible study. Items that were extracted are the type of
study, study setting, study population (cancer type, cancer stage, cancer treatment, the
timing of screening), the frailty screening tools used including cut‐off values, the content
of the CGA and the assessment tools used, as well as the outcomes in terms of association
etween frailty screening tool and CGA. b
Quality assessment The methodological quality of each of the studies was also assessed independently by two
reviewers (MH and JJ), using the QUADAS‐2 tool (Quality Assessment of Studies of
Diagnostic Accuracy included in Systematic reviews, Appendix 1) as developed and revised
by Whiting et al.12,13 Disagreements among the reviewers were discussed during a
consensus meeting and in case of persisting disagreement, the assistance of a third
reviewer (BvM) was enlisted.
To address the suitability of the CGA to detect frailty, we used the definition formulated
by the International Society of Geriatric Oncology, which states that at minimum, a CGA
for older cancer patients should include assessment of functional status, cognition and
ood.7 m
Data synthesis and analysis We summarized the study results to describe our main outcomes of interest. If necessary,
sensitivity, specificity, positive and negative predictive values were calculated based on
the results listed in the publication, or – in case of insufficient published information – on
additional data obtained from the authors.
187

Chapter 12
Table 1: Studies on the association between frailty assessment and comprehensive geriatric assessment
Publication Patients
Author
Publication year
Abstract(A) or full
text (F)
Setting/departm
ent
Study population
Number of patients
% m
ale
Median age
in years
(range)
Baitar14‐16
2011 A Unclear Various cancer types 135 ? 77 (66‐97)
Kellen17 2010 F Medical
oncology/ general practice
Various cancer types, irrespective of stage of disease or treatment
113 60% 77 (SD 4)
Kenis18 2009 A Medical
oncology Newly diagnosed cancer or progressive disease, during admission
140 ? 76.5 (SD 5.1)
Kenis19 2011 A Medical
oncology Various cancer types, patients considered for start of chemotherapy
843 37% 76.9 (SD 5.1)
Kristjansson20 2008 A Surgery Pre‐operative patients with
colorectal cancer considered for surgery
74 46% 80 (71‐94)
Luciani21 2010 F Medical
oncology Various cancer types, prior to start first‐line chemotherapy
419 55% 76 (70‐97)
Mohile22,23
2007 F Medical oncology
Prostate cancer patients receiving hormonal treatment
50 100% 78 (70‐92)
Molina‐Garrido
24‐26
2010 F Medical oncology
Early stage breast cancer prior to start chemotherapy
41 0% 74.5 (SD 5.1)
Molina‐Garrido
27
2011 A Medical oncology
Unclear 58 ? Not stated
Monfardini28 2010 A Medical
oncology Patients with breast cancer newly referred to medical oncologist
150 ? 76 (70‐94)
Owusu29 2010 F Medical
oncology Various cancer types, first visit to outpatient clinic with newly diagnosed cancer
117 18% 72 (IQR 69‐80)
Pottel30‐32
2011 F Radiotherapy Head and neck cancer patients prior to start radiotherapy
51 84% 72 (65‐86)
Soubeyran33 2008 A Medical
oncology Various cancer types, prior to start of first‐line chemotherapy
364 59% 77 (70‐99)
Soubeyran34,3
5
2011 A Medical oncology
Unclear 1425 30% 78.2 (70‐98)
* A more detailed overview of the content of the geriatric assessment can be found in Appendix 3
188

Frailty screening tools in geriatric oncology
Table 1: Studies on the association between frailty assessment and comprehensive geriatric assessment
Screening tool Geriatric assessment (CGA)*
Frailty screening
tool used (cut‐off)
Cognition
Mood
ADL
IADL
Nutritional status
Social support
Comorbidity
Polypharmacy
Mobility/falls
Cut‐off value for
frailty on CGA (nr of
impairm
ents unless
otherw
ise stated)
GFI (4+) G8 (≤14)
+ + + + + + + + 2+
aCGA (1+)** VES13 (3+) GFI (4+)
+ + + + Cognitive impairment or 2+ more other impairments
GFI (4+) G8 (≤14) TRST (1+/2+)
+ + + + + + 2+
TRST (1+) G8 (≤14)
+ + + + + + + + 2+
Fried (3+)
+ + + + + + 1+
VES‐13 (3+)
+ + + + + + 1+
VES‐13 (3+)
+ + + + + + 2+
VES‐13 (3+) Barber (1+)
+ + + + + + + 2+
Fried (3+) VES‐13 (3+)
+ + + + + + + 2+
VES‐13 (3+)
+ + + + + + ADL‐dependent, 3+ comorbidities or 1+ severe comorbidities
VES‐13 (3+)
+ + + + + + + + 2+
G8 (≤14) VES‐13 (3+)
+ + + + + + 2+
G8 (≤14)
+ + + + + + + 1+
G8 (≤14) VES‐13 (3+)
+ + + + + + + 1+
** In the original aCGA publications, screening yielded subscores per domain but not an overall score. This cut‐off value in this study was defined by its researchers, based on the aggregated results of the subscores. GFI Groningen Frailty Index, G8 Geriatric 8, aCGA abbreviated comprehensive geriatric assessment, VES13 Vulnerable Elders’ Survey‐13, TRST Triage risk screening tool, (I)ADL instrumental activities of daily living
189

Chapter 12
Results
Characteristics of included studies The literature search yielded 3943 citations (1769 from Medline and 2174 from Embase)
and an additional 497 studies on geriatric assessment in cancer patients were identified in
conference abstracts. For one of the identified abstracts, the full text publication came out
after the search date; however, as this contained additional, useful information, we
included this manuscript as well. After exclusion of 1279 duplicates and 3139 studies for
other reasons (Appendix 2), a total of 22 publications from 14 studies were included in this
review.14‐35
The characteristics of these 14 studies are summarized in Table 1. The first publication is in
2007 but most were published in the past two years.14‐35 For seven studies, full text
reports were available,17,21‐26,29‐32 but for the seven remaining studies, conference
abstracts were the only publications.14‐16,18‐20,27,28,33‐35 Median sample size was 117 patients
(range 41‐1425). Median age of included patients ranged from 72 to 80 years.14‐35 All but
two studies20,30‐32 were performed in the medical oncology department. Half of the studies
included patients with various cancer types17‐19,21,27,29,33 while two did not elaborate on the
type of patients that were included,27,34,35 the other five studies focused on one cancer
type only (two on breast cancer,24‐26,28 and one each on prostate cancer,22,23 colorectal
cancer20 and head and neck cancer30‐32).
Seven different frailty screening tools were assessed: Vulnerable elders survey‐135 was the
most frequently examined (VES‐13, 9 studies) followed by the Geriatric 836 (G8, six
studies), Groningen Frailty Index4 (GFI, 3 studies), Triage Risk Screening Tool37 (TRST) and
Fried frailty criteria6 (2 studies each), and the abbreviated CGA38 (aCGA) and Barber24 (one
study each). Table 2 gives an overview of the domains these tools focus on, and their
relative weight. All tools address functional status, and most (five out of seven tools) also
focus on some aspect of psychosocial functioning, but for other geriatric conditions there
is much more variation (Table 2). The aCGA and G8 are the only tools designed specifically
for assessment of frailty in older cancer patients (Table 2).
The content of the CGA varied from four to eight geriatric conditions (Table 1); the median
number of examined conditions was seven.14‐35 All studies included assessment of
cognitive function and activities of daily living (ADL), although the method of assessment
varied.14‐35 Instrumental ADL functioning was examined in twelve studies,14‐17,19,21‐35 mood
in ten studies,14‐20,28‐35 nutritional status in nine,14‐16,19‐21,24‐27,30‐35 mobility/falls history in six
studies14‐16,19,29,33‐35 and social support in seven.14‐16,18,22‐29 Comorbidity was examined in
thirteen studies14‐16,18‐35 and polypharmacy in eight.18‐27,29 Frailty on CGA was defined as
the presence of one or more geriatric conditions in four studies20‐22,33‐35 and two or more
190

Frailty screening tools in geriatric oncology
Table 2: Relative weight of geriatric conditions in the frailty screening tools (in % of total points per tool)
Geriatric domains GFI4 G836 VES‐135 aCGA38 Fried6 Barber24 TRST37
Functional status 27% 11% 60% 60% 60% ADL impairment 13% 20% 33% IADL impairment 7% 40% 11% mobility/falls 7% 20%
Psychosocial domain
40% 11% 40%
Cognitive disorder
7% 27% 20%
Mood/anxiety 13% 13% Social support 20% 11%
Neuro‐sensory deficits
13% 22%
Nutritional status/weight loss
7% 46% 20%
Polypharmacy 7% 6% 20%
Comorbidity
Recent hospitalization
11% 20%
Geriatric syndromes 20%
Self‐reported health 7% 11% 10% 20% 11%
Age 11% 30%
Optimal score 0 17 0 * 0 0 0
Poorest score 15 0 10 * 5 9 5
Standard cut‐off value
4+ ≤14 3+ * 3+ 1+ 2+
Population for which tool was designed
Various Cancer patients
Community‐dwelling elderly
Cancer patients
No specific population
Primary care patients
Patients in emergency room
* no overall scoring of aCGA is available; subscores for each geriatric domain are calculated. GFI Groningen Frailty Index, G8 Geriatric 8, VES‐13 Vulnerable elders’ survey‐13, aCGA abbreviated comprehensive geriatric assessment, TRST triage risk screening tool; (I)ADL (instrumental) activities of daily living
in eight studies.14‐16,18,19,22‐27,29‐32 The remaining two studies applied other definitions,
assigning different weights to the various assessed conditions (Table 1).17,28
Study populations showed a wide variation in the prevalence of frailty as diagnosed by the
CGA; a median of 68% of patients was considered frail (range 28‐94%, Table 3).14‐35 This
wide range cannot be explained solely by differences in the cut‐off used for the definition
of frailty on CGA, as in studies using the cut‐off of 1+ prevalence of frailty ranged from 28
to 80%20‐22,33‐35 while in studies using a cut‐off of 2+, the range was 43% to 88%.14‐16,18,19,22‐
27,29‐32 According to frailty screening tools, the median prevalence of frailty was 49% (range
12‐83%).14‐35
191

Chapter 12
Quality assessment Results of the quality assessment can be found in Figure 1. Reviewer agreement was over
95% for all aspects. For patient selection, the risk of bias was generally considered low,
and little concerns existed about the applicability of selection criteria. Due to the lack of
information on the independent scoring of the frailty screening tool and the CGA, the risk
of bias was frequently unclear for both the index test as well as the reference test.
Variation in the content of the CGA resulted in some concerns about the applicability of
study results and may also have introduced risk of bias. Flow and timing of the studies
yielded few concerns. Full results of the quality assessment can be found in Appendix 1b.
Figure 1: Quality assessment of included studies, using the QUADAS‐2 assessment tool (Appendix 1a).
13 The
complete assessments per study can be found in Appendix 1b.
192

Frailty screening tools in geriatric oncology
Frailty screening tools vs. comprehensive geriatric assessment Table 3 gives an overview of the sensitivity and specificity of the frailty screening tools
compared to frailty as detected by CGA, while Figure 2 demonstrates the relationship
between sensitivity and false‐positives per screening tool. For the VES‐13, sensitivity
ranged from 39% to 88% with a median of 68%.17,21‐32,34,35 Thus, a median of 32% of frail
patients were not recognized as frail by the VES‐13. The specificity was better, ranging
from 62% to 100%, with a median of 78%. Thus, the VES‐13 yielded 22% false‐positives.
For the G8, the sensitivity ranged from 77% to 92%, with a median of 87% but the
specificity ranged from 39% to 75%, with a median of 61%.14‐16,18,19,30‐35 The TRST (using a
cut‐off of 1+) showed a sensitivity of 91% with a specificity of between 43 and 50%.18,19
For the GFI, sensitivity ranged from 39% to 62%, and the specificity was between 69% and
87%.14‐18 For the Fried frailty criteria, the sensitivity was between 25% and 37%, with a
specificity of 86% to 96%.20,27
Table 3: Sensitivity and specificity of frailty screening tools for outcome of (summarized) comprehensive geriatric assessment (CGA)
Screening tool
(cut‐off) Study
% frail on screening
tool
% frail on CGA
Sensitivity (%)
Specificity (%)
Positive predictive value (%)
Negative predictive value (%)
aCGA (1+) Kellen (2010)17 36 68 51 97 97 48
Barber (1+) Molina‐Garrido (2010)24‐26
42 56 59 79 77 63
Kristjansson (2008)20 12 38 25 96 78 67
Fried (3+) Molina Garrido (2011)
27 35 88 37 86 95 16
Baitar (2011)15 75 44 92 39 55 85
Kenis (2009)18 76 79 80 40 83 35
Kenis (2011)19 74 73 87 61 86 63
Pottel (2011)30‐32
67 69 86 75 88 71
Soubeyran (2008)33 82 94 85 65 97 22
G8 (≤14)
Soubeyran (2011)34,35
68 80 77 64 90 41
Baitar (2011)14,16
44 44 62 69 62 69
Kellen (2010)17 31 68 39 86 86 40 GFI (4+)
Kenis (2009)18 48 79 57 87 94 36
Kenis (2009)18 83 79 92 50 87 63
TRST (1+) Kenis (2011)
19 82 73 91 43 81 64
TRST (2+) Kenis (2009)18 50 79 64 100 100 43
Kellen (2010)17 49 68 61 78 85 48
Luciani (2010)21 54 28 87 62 45 93
Mohile (2007)22,23
50 60 73 86 89 67
Molina‐Garrido (2010)24‐26
29 56 55 100 100 66
Molina‐Garrido (2011)27 35 88 39 100 100 18
Monfardini (2010)28 46 44 68 71 65 74
Owusu (2010)29 56 43 88 69 68 88
Pottel (2011)30‐32
39 69 57 100 100 52
VES‐13 (3+)
Soubeyran (2011)34,35
60 80 69 74 92 37
GFI Groningen Frailty Index, G8 Geriatric 8, VES‐13 Vulnerable elders’ survey‐13, aCGA abbreviated comprehensive geriatric assessment, TRST triage risk screening tool
193

Chapter 12
Figure 2: Sensitivity and 1‐specificity of the screening tools for predicting outcome of comprehensive geriatric assessment
GFI Groningen Frailty Index, G8 Geriatric 8, VES‐13 Vulnerable elders’ survey‐13, aCGA abbreviated comprehensive geriatric assessment, TRST triage risk screening tool
Interestingly, as the prevalence of frailty in most study populations was high, even the
screening tools with the highest sensitivity to frailty still yielded negative predictive values
of around 60% (Table 3). This means that four out of every ten patients considered fit
fter frailty screening, will be diagnosed as frail after CGA. a
Frailty screening tools vs. individual geriatric conditions Although frailty screening tools are generally used to predict overall frailty, a few studies
have addressed the association between these tools and individual geriatric conditions
(Table 4); four studies addressed the latter association for VES‐13,17,22,23,29‐32 while one
study each looked at aCGA,17 GFI17 and G8.30‐32 Comparison of results is compromised,
however, by the different methods of presentation of the data.
Overall, VES‐13 appears to be most strongly associated with ADL and IADL functioning
(area under the curve (AUC) between 0.81 and 0.91, sensitivity between 67% and 83% and
specificity between 61% and 89%.)17,22,23,29‐32 Association between VES‐13 and cognitive
disorders, impaired mobility and malnutrition was fair (AUC 0.79‐0.81, 0.78‐0.87 and 0.78
194

Frailty screening tools in geriatric oncology
Table 4: Association between screening tools and individual geriatric domains
Screening tool
Study
Cognition
Mood
ADL
IADL
Nutritional status
Comorbidity
Social support
Mobility
Polypharmacy
aCGA Kellen (2010)
17
Sens 23% Spec 100%
Sens 69% Spec 92%
Sens 97% Spec 47%
Sens 92% Spec 69%
G8 Pottel (2011)
30‐32
AUC 0.73 AUC 0.78 AUC 0.71 AUC 0.67 AUC 0.95
AUC 0.74 AUC 0.74
GFI Kellen (2010)
17
Sens 47%Spec 76%
Sens 39% Spec 86%
Kellen (2010)
17
Sens 76% Spec 63%
Sens 67% Spec 89%
Mohile (2007)
22,23
Sens 75% Spec 58%
Sens 83% Spec 61%
Sens 76% Spec 68%
Sens 76% Spec 64%
Sens 33% Spec 46%
Sens 70% Spec 67%
Owusu (2010
29
AUC 0.81 AUC 0.66 AUC 0.81 AUC 0.91 AUC 0.73 AUC 0.57 AUC 0.78
AUC 0.72
VES‐13
Pottel (2011)
30‐32 AUC 0.79 AUC 0.74 AUC 0.87 AUC 0.86 AUC
0.78AUC 0.70 AUC
0.87
aCGA abbreviated comprehensive geriatric assessment, G8 Geriatric 8, GFI Groningen frailty index, VES‐13 Vulnerable Elders Survey‐13; AUC area under the curve
respectively) 22,23,29‐32 G8 showed a strong association with malnutrition (AUC 0.95), but
was of lesser value for predicting the presence of other geriatric conditions. 30‐32 aCGA
showed a strong association with ADL and IADL impairment (sensitivity 97% and 92%,
specificity 47% and 69% respectively), but the sensitivity for cognitive dysfunction or
depressive symptoms was low (23% and 69% respectively). 17 GFI demonstrated poor
sensitivity for functional impairment (ADL impairment 47%, IADL impairment 39%) but
asonable specificity (76% and 86% respectively). 17 re
Discussion A useful frailty screening tool in geriatric oncology should have a high sensitivity, thus
allowing the assessor to trust that those patients deemed fit actually are fit, and a
sufficient specificity so that the time‐consuming process of a full CGA is optimally
utilized.10,11,39 In this systematic review on the discriminative power of frailty screening
tools for outcome of full CGA, we found that those tools with the highest sensitivity lacked
specificity and vice versa. In addition, even for the screening tools with the highest
sensitivity, the negative predictive value (i.e. the proportion of patients considered fit on
the screening tool that were also considered fit after full CGA) was around 63%, meaning
over a third of patients were unjustly considered fit after frailty screening.
195

Chapter 12
Given the content of the frailty screening tools and the population and purpose for which
they were developed (Table 2), the lack of sensitivity of some of these screening tools
when used to predict outcome of CGA is hardly surprising. For example, the VES‐135 and
Fried frailty criteria6 focus strongly on functional status (Table 2). Therefore, it is not
surprising that these tools are not very successful in identifying impairments in other
geriatric domains. For other screening tools, such as the GFI, the lack of discriminative
power could be explained by the fact that they were designed to diagnose frailty in a
different patient population than that in which it is being used in geriatric oncology (Table
2). In fact, most of the screening tools that are being used in geriatric oncology were not
designed or validated for this particular setting; only the G8 and aCGA developed
specifically for use in older cancer patients. As the aCGA was designed to identify which
individual geriatric domains require further assessment, the lack of sensitivity for overall
frailty (median 51%) as well as for two of the four individual domains for which it was
designed (Table 4) is disappointing. Ultimately, the G8 and the TRST ‐ developed to assess
functional impairment in older patients admitted to the emergency department37 – had
the highest sensitivity for frailty on CGA (87 and 91% respectively) but both lacked
specificity (61% and 45% respectively).
Thus, no screening tool currently used in geriatric oncology combined adequate sensitivity
and specificity. In addition, for tools with the highest sensitivity, the percentage of
patients diagnosed as frail after screening was around 70%, and – based on the negative
predictive value of these tools – one‐third of the remaining 30% was incorrectly diagnosed
as fit. Considering these findings, the question rises whether there is any benefit in a two‐
stepped approach in which a CGA is preceded by a screening tool. The time‐saving
potential of this approach will be limited if the prevalence of frailty is high, and potentially
does not outweigh the risk of incorrectly identifying patients as fit and delivering care‐as‐
usual where a more cautious approach would have been better.
Another aspect for which the use of a screening tool prior to CGA could be beneficial is to
identify which geriatric domains require further assessment; this could save time by
allowing the CGA to be limited to those domains only. Several studies in this review
addressed this issue (Table 4); however, the available data are limited. In addition, these
studies examined the association between the entire screening tool and a specific geriatric
domain while it would be more useful to assess the sensitivity of each individual screening
question for the presence or absence of the specific geriatric conditions that the question
inquires after. This aspect warrants further exploration in future research.
This systematic review provides a valuable overview of all currently available evidence on
the use of frailty screening tools in geriatric oncology but it also has several limitations.
First of all, we limited our search to studies performed in older cancer patients, thus
excluding available evidence from other patient populations. However, the prevalence of
196

Frailty screening tools in geriatric oncology
geriatric conditions and frailty will differ greatly in various contexts and the discriminative
power of frailty screening tools should therefore be assessed in the context that it will be
used in. Another limitation of this review is that no full text reports have been published
for half of the included studies, and we had to rely on conference abstracts as the only
source of information on the execution and results of the study. In particular, this limited
our ability to analyse the predictive value of the frailty screening tools for individual
domains. Moreover, the content of the CGA differed considerably between studies, as did
the cut‐off value that was used to define frailty. The definition of frailty that is used will
influence the prevalence of frailty in a study population and similarly the sensitivity and
specificity of screening tools in predicting that frailty. This lack of golden standard for
assess frailty assessment decreased the comparability of study results and subsequently
hampered the execution of a formal meta‐analysis, thus leaving uncertainty about the
relative quality of the different screening tools for detecting frailty in older cancer
patients. In 2005, the International Society of Geriatric Oncology recommended that, at
minimum, frailty assessment for older cancer patients should include an evaluation of
functional status, cognition and mood.39 In wake of growing evidence that geriatric
conditions, such as nutritional status, polypharmacy, comorbidity and social support may
also be significant for older cancer patients, perhaps an update of these recommendations
should be undertaken. Moreover a consensus in the scales to use, including their cut‐off
values, would result in greater uniformity in clinical practice and research, and allow for
better comparison between studies and patient populations.
Ultimately, establishing whether a patient is fit or frail is not a goal in itself, but a method
for optimizing and tailoring oncologic and non‐oncologic treatment in elderly cancer
patients. Therefore, future research should focus on a more elaborate exploration of the
value of frailty and individual geriatric conditions for predicting and improving clinical
utcomes such as quality of life, survival, treatment tolerance and functional decline. o
In conclusion, although the Geriatric 8 and Triage Risk Screening Tool demonstrated the
best sensitivity for frailty on full CGA in older cancer patients, they had a poor specificity
and negative predictive value. Perhaps it will be possible to develop targeted screening
tools with better sensitivity and specificity once the relative importance of individual
geriatric domains and the benefit of appropriate interventions and follow‐up are fully
elucidated in this patient population. Until such a time, it may be beneficial for all older
patients to receive a complete geriatric assessment, since the two‐stepped approach –
using frailty screening tools to select patients for CGA – has insufficient discriminative
power.
197

Chapter 12
Appendix 1a: Quality Assessment of studies of Diagnostic Accuracy included in Systematic reviews‐2 (QUADAS‐
2) tool12,13
Domain 1: Patient Selection Risk of Bias: Could the selection of patients have introduced bias? 1: Was a consecutive or random sample of patients enrolled? 2: Was a case–control design avoided? 3: Did the study avoid inappropriate exclusions? Applicability: Are there concerns that the included patients and setting do not match the review question? Domain 2: Index Test Risk of Bias: Could the conduct or interpretation of the index test have introduced bias?
1: Were the index test results interpreted without knowledge of the results of the reference standard?
2: If a threshold was used, was it prespecified? Applicability: Are there concerns that the index test, its conduct, or its interpretation differ from the review question? Domain 3: Reference Standard Risk of Bias: Could the reference standard, its conduct, or its interpretation have introduced bias? 1: Is the reference standard likely to correctly classify the target condition?
For this purpose, we used the definition formulated by the International Society of Geriatric Oncology, which states that at minimum, a CGA for older cancer patients should include assessment of functional status, cognition and mood.
40 2: Were the reference standard results interpreted without knowledge of the results of the index test?
Applicability: Are there concerns that the target condition as defined by the reference standard does not match the research question? Domain 4: Flow and Timing Risk of Bias: Could the patient flow have introduced bias? 1: Was there an appropriate interval between the index test and reference standard? 2: Did all patients receive the same reference standard? 3: Were all patients included in the analysis?
198

Frailty screening tools in geriatric oncology
Appendix 1b: Overview of quality assessment according to the QUADAS‐2 tool per study
Risk of bias Concerns about applicability Author
Patient selection
Index test
Reference test
Flow and timing
Patient selection
Index test
Reference test
Baitar (2011)14‐16 Unclear Unclear Unclear Unclear Low Low Low
Kellen (2010)17 Low Unclear Unclear Low Low Low Low
Kenis (2009)18 Low Low Low Low Low Low Low
Kenis (2011)19 Low Unclear Unclear Low Low Low Low
Kristjansson (2008)20 Low Unclear Unclear Low Low Low Low
Luciani (2010)21 Low Unclear Unclear Low Low Low Low
Mohile (2007)22,23 Low High High Low Low Low High
Molina‐Garrido (2010)24‐26 Low Unclear High Low Low Low High
Molina‐Garrido (2011)27 Unclear Unclear High Low Unclear Low High
Monfardini (2010)28 Low Low Low Low Low Low Low
Owusu (2010)29 Low Unclear Unclear Low Low Low Low
Pottel (2011)30‐32 Low Unclear Unclear Low Low Low Low
Soubeyran (2008)33 Low High Unclear Unclear Low Low Low
Soubeyran (2011)34,35 Low Unclear Unclear High Low Low Low
Appendix 2: Search and study selection
All studies n= 4440 Medline n= 1769 Embase n= 2174 Conference abstracts n= 497
Duplicates n= 1279
Exclusion n= 3139 Not original research n= 747 Not oncology n= 444 No comprehensive geriatric assessment (CGA) n= 1340 No screening tool n= 566 No association screening tool with CGA n= 22 Non‐cancer patients included n= 8 CGA not performed in all patients n= 3 Substantial overlap with another publication n= 2 Insufficient data for analysis n= 5 Retrospective tool development n= 2
Inclusion: 22 publications from 14 studies
199

Chapter 12
Appendix 3: Complete overview of comprehensive geriatric assessment per study
Author
Frailty screening tool
used (cut‐off)
Cognition
Mood
ADL
IADL
Nutrition
Mobility/falls
Social
Comorbidity
Polypharmacy
Others
Baitar (2011)
14‐16
GFI (4+) G8 (≤14)
MMSE GDS Katz Lawton TUG MOS‐ SSS
Charlson
Kellen (2010)
17
aCGA (1+) VES13 (3+) GFI (4+)
MMSE GDS Barthel Lawton
Kenis (2009)
18
GFI (4+) G8 (≤14) TRST (1+/2+)
MMSE GDS Katz + + CIRS‐G + Age
Kenis (2011)
19
TRST (1+) G8 (≤14)
MMSE GDS Katz Lawton MNA Fall history
Charlson + Fatigue (Mob‐T)
Kristjansson (2008)
20
Fried (3+) MMSE GDS Barthel MNA CIRS‐G +
Luciani (2010)
21
VES‐3 (3+) MMSE Katz Lawton MNA CIRS‐G + Social status
Mohile (2007)
22,23
VES‐3 (3+) SPMSQ, Pfeiffer
Katz Lawton MOS‐SSS
Charlson + SPPB
Molina‐ Garrido (2010)
24‐26
VES‐3 (3+) Barber (1+)
Pfeiffer Barthel Lawton NSI Gijon Charlson +
Molina‐ Garrido (2011)
27
Fried (3+) VES‐13 (3+)
Pfeiffer Barthel Lawton NSI Gijon Charlson +
Monfardini (2010)
28
VES‐3 (3+)
MMSE GDS Katz Lawton CIRS‐G +
Owusu (2010)
29
VES‐3 (3+)
MMSE GDS Katz Lawton TUG, fall history
MOS‐SSS
Charlson + Visual/hearing impairment
Pottel (2011)
30‐32
G8 (≤14) VES‐3 (3+)
MMSE GDS Katz Lawton MNA Tinetti CIRS‐G
Soubeyran (2008)
33
G8 (≤14) MMSE GDS Katz Lawton MNA TUG CIRS‐G Quality of life (QLQ‐C30)
Soubeyran (2011)
34,35
G8 (≤14) VES‐3 (3+)
MMSE GDS Katz Lawton MNA TUG CIRS‐G
GFI Groningen Frailty Index, G8 Geriatric 8, VES‐13 Vulnerable elders survey‐13, aCGA abbreviated comprehensive geriatric assessment, TRST triage risk screening tool + assessed without the use of a specific assessment tool (I)ADL instrumental activities of daily living, MMSE mini mental state examination, SPMSQ short portable mental status questionnaire, GDS geriatric depression scale, MNA mini nutritional assessment, NSI nutrition screening initiative TUG Timed up and go, MOS‐SSS medical outcomes study – social support survey CIRS‐G cumulative illness rating scale‐geriatric, SPPB short physical performance battery QLQ‐C30 quality of life questionnaire
200

Frailty screening tools in geriatric oncology
References 1. Muss HB. Cancer in the elderly: a societal perspective from the United States. Clin Oncol (R Coll Radiol )
2009;21:92‐98. 2. Ferrucci L, Guralnik JM, Studenski S et al. Designing randomized, controlled trials aimed at preventing or
delaying functional decline and disability in frail, older persons: a consensus report. J Am Geriatr Soc 2004;52:625‐634.
3. Rockwood K, Mitnitski A. Frailty defined by deficit accumulation and geriatric medicine defined by frailty. Clin Geriatr Med 2011;27:17‐26.
4. Slaets JP. Vulnerability in the elderly: frailty. Med Clin North Am 2006;90:593‐601. 5. Saliba D, Orlando M, Wenger NS et al. Identifying a short functional disability screen for older persons. J
Gerontol A Biol Sci Med Sci 2000;55:M750‐M756. 6. Fried LP, Tangen CM, Walston J et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci
Med Sci 2001;56:M146‐M156. 7. Extermann M, Aapro M, Bernabei R et al. Use of comprehensive geriatric assessment in older cancer
patients: recommendations from the task force on CGA of the International Society of Geriatric Oncology (SIOG). Crit Rev Oncol Hematol 2005;55:241‐252.
8. Ellis G, Whitehead MA, O'Neill D et al. Comprehensive geriatric assessment for older adults admitted to hospital. Cochrane Database Syst Rev 2011;7:CD006211.
9. Maas HA, Janssen‐Heijnen ML, Olde Rikkert MG, Machteld Wymenga AN. Comprehensive geriatric assessment and its clinical impact in oncology. Eur J Cancer 2007;43:2161‐2169.
10. Molina‐Garrido MJ, Guillen‐Ponce C. Overvaluation of the vulnerable elders survey‐13 as a screening tool for vulnerability. J Clin Oncol 2011;29:3201‐3202.
11. Falci C, Brunello A, Monfardini S. Detecting functional impairment in older patients with cancer: is vulnerable elders survey‐13 the right prescreening tool? An open question. J Clin Oncol 2010;28:e665‐e666.
12. Whiting P, Rutjes AW, Reitsma JB et al. The development of QUADAS: a tool for the quality assessment of studies of diagnostic accuracy included in systematic reviews. BMC Med Res Methodol 2003;3:25.
13. Whiting PF, Rutjes AW, Westwood ME et al l. QUADAS‐2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med 2011;155:529‐536.
14. Baitar A, Van Fraeyenhove F, Galdermans D et al. Evaluation of the groningen frailty indicator as a screening tool for frailty in older cancer patients (PTS). European Journal of Cancer 2011:46:S282.
15. Baitar A, Vandebroek A, De DE et al. Evaluation of the g8 questionnaire as a screening tool for frailty in older cancer patients (PTS). European Journal of Cancer 2011;47:S275.
16. Schrijvers D, Baitar A, de Vos M et al P. Evaluation of the Groningen Frailty Index as a screening tool in elderly patients (PTS): an interim analysis. Annals of Oncology 2010;21(Suppl 8):556PD.
17. Kellen E, Bulens P, Deckx L et al. Identifying an accurate pre‐screening tool in geriatric oncology. Crit Rev Oncol Hematol 2010;75:243‐248.
18. Kenis C, Schuermans H, van Cutsem E et al. Screening for a geriatric risk profile in older cancer patients; a comparative study of the predictive validity of three screening tools. Crit Rev Oncol Hematol 2009;72(suppl 1):S22.
19. Kenis C, Decoster L, Vanpuyvelde K et al l. Comparison of two screening tols in older cancer patients. J Geriatr Oncol 2011;2(suppl 1):S39.
20. Kristjansson SR, Jordhoy MS, Nesbakken A, Wyller TB. A comparison of two methods to measuring frailty in elderly patients with colorectal cancer. Crit Rev Oncol Hematol 2008;68(suppl1):S30.
21. Luciani A, Ascione G, Bertuzzi C et al l. Detecting disabilities in older patients with cancer: comparison between comprehensive geriatric assessment and vulnerable elders survey‐13. J Clin Oncol 2010;28:2046‐2050.
22. Mohile SG, Bylow K, Stadler WW, Rodin M. A pilot study of the Vulnerable Elders Survey (VES‐13) as compared to Comprehensive Geriatric Assessment (CGA) to examine geriaric domains in elder prostate cancer patients at risk for decline. J Clin Oncol 2006;24(suppl):8539.
23. Mohile SG, Bylow K, Dale W et al. A pilot study of the vulnerable elders survey‐13 compared with the comprehensive geriatric assessment for identifying disability in older patients with prostate cancer who receive androgen ablation. Cancer 2007;109:802‐810.
24. Molina‐Garrido MJ, Guillen‐Ponce C. Comparison of two frailty screening tools in older women with early breast cancer. Crit Rev Oncol Hematol 2011;79:51‐64.
201

Chapter 12
202
25. Molina‐Garrido M, Guillen‐Ponce C, Santiago J et al. Barber test as a screening tool in multidimensional geriatric evaluation in elderly women with early breast cancer. J Clin Oncol 2009;155:e20645.
26. Molina‐Garrido MJ, Guillen‐Ponce C, Guirado‐Risueno M et al Usefulness of the Barber test is compared with the comprehensive geriatric assessment for identifying disability in outpatients older than 65 years with breast cancer who receive chemotherapy. Crit Rev Oncol Hematol 2008;68(suppl2):S33.
27. Molina‐Garrido M, Guillen‐Ponce C, Munoz M et al. A comparison of the fried criteria and the VES‐13 questionnaire as screening instruments for frail elderly patients diagnosed with cancer. European Geriatric Medicine 2011;2(suppl 1):S34.
28. Monfardini S, Basso U, Fiduccia P et al. Can the short screening test Vulnerable Elders Survey 13 (VES‐13) substitute for the time‐consuming comprehensive geriatric assessment (CGA) to identify vulnerable/frail elderly breast cancer patients? Journal of Clinical Oncology 2010;28.
29. Owusu C, Koroukian SM, Schluchter M et al. Screening older cancer patients for a Comprehensive Geriatric Assessment: A comparison of three instruments. J Geriatr Oncol 2011;28:121‐129.
30. Pottel L, Boterberg T, Pottel H et al. Determination of an adequate screening tool for identification of vulnerable elderly head and neck cancer patients treated with radio(chemo)therapy. J Clin Oncol 2011;di:10.1016/j/jgo.2011.11.006.
31. Debruyne PR, Boterberg T, Pottel H et al. Can the Vulnerable Elders Survey‐13 and/or the G8 adequatley identify elderly patients with head and neck cancer in need of a comprehensive geriatric assessment? J Clin Oncol 2011:e19670.
32. Pottel L, Boterberg T, Pottel H et al l. Could the combined test "VES‐13 + (max‐G8) represent an interesting alternative screening tool for identification of potential vulnerable elderly head and neck cancer patients? J Geriatr Oncol 2011;2(suppl1):S21.
33. Soubeyran P, Bellera CA, Gregoire F et al. Validation of a screening test for elderly patients in oncology. J Clin Oncol 2008;26(15S):20568.
34. Soubeyran P, Bellera C, Goyard J et al. Validation of the G8 geriatric screening tool for elderly cancer patients and comparions with the VES‐13: final results of the ONCODAGE project. J Geriatr Oncol 2011;2(S1):S17.
35. Soubeyran P, Bellera C, Goyard J et al. Validation of the G8 screening tool in geriatric oncology; the ONCODAGE project. J Clin Oncol 2011;29(15S):9001.
36. Bellera C, Rainfray M, Mathoulin‐Pelissier S, Soubeyran I. Validation of a screening tool in geriatric oncology: the Oncodage project. Crit Rev Oncol Hematol 2008;68(suppl):O2.
37. Meldon SW, Mion LC, Palmer RM et al. A brief risk‐stratification tool to predict repeat emergency department visits and hospitalizations in older patients discharged from the emergency department. Acad Emerg Med 2003;10:224‐232.
38. Overcash JA, Beckstead J, Moody L et al. The abbreviated comprehensive geriatric assessment (aCGA) for use in the older cancer patient as a prescreen: scoring and interpretation. Crit Rev Oncol Hematol 2006;59:205‐210.
39. Extermann M, Aapro M, Bernabei R et al. Use of comprehensive geriatric assessment in older cancer patients: recommendations from the task force on CGA of the International Society of Geriatric Oncology (SIOG). Crit Rev Oncol Hematol 2005;55:241‐252.
40. Extermann M, Aapro M, Bernabei R et al. Use of comprehensive geriatric assessment in older cancer patients: recommendations from the task force on CGA of the International Society of Geriatric Oncology (SIOG). Crit Rev Oncol Hematol 2005;55:241‐252.

Part IV
General discussion, summary
and acknowledgements


Chapter 13 General discussion

Chapter 13
Introduction In this thesis, we addressed current treatment practices and decision making in elderly
cancer patients as well as the consequences of these decisions for clinical outcome. In
addition, we investigated the value of a comprehensive geriatric assessment in the
decision‐making process for these patients. In this final chapter, the results of these
studies will be placed in a broader perspective and some issues and implications of these
ndings will be discussed, including some directions for future research. fi
Research in elderly cancer patients: clinical trials and observational cohort studies If we want to know the optimal treatment for older cancer patients, we must design
studies that specifically target these patients, as it is incorrect to assume that optimal
treatment for a younger patient population will be just as suitable for the older group.
However, designing clinical trials for elderly patients is complicated by multiple factors,
including the heterogeneity of the population resulting in a great variability in the ability
to tolerate treatment, as well as hesitance of older patients to participate in a trial,
especially in case of randomization (Chapter 5). These factors may affect the accrual of
elderly patients, or mean the patients that are included in clinical trials do not form a
representative sample of the target population. Therefore, studies in real‐life populations
are needed to supplement trial data.
One option is to use observational cohorts as was done in this thesis, where we examined
cohorts of patients with breast cancer, colon cancer and head and neck cancer, to address
the issue of guideline adherence and differences in treatment choices between younger
and older patients (Chapter 1‐3 and 6‐8). These have provided us with data on real‐life
clinical practice and in particular, on the reasons why certain treatment choices are made;
these data could not have been obtained in a clinical trial format. However, as all these
studies were done retrospectively, data on potentially relevant confounders such as the
presence of geriatric syndromes or decreased functional capacity were not available. Since
these data could also have influenced treatment choices or prognosis, it will be useful to
repeat these studies prospectively, with incorporation of baseline data on frailty and
geriatric syndromes. In fact, it could be argued that for any research in elderly cancer
patients – irrespective of the chosen study design – reporting of geriatric baseline data is
as important as the tumour‐related data or other patient characteristics. Without these
data, it is not possible to compare study results or extrapolate their findings to the
dividual patient.1 in
206

General Discussion
Non‐standard or sub‐standard treatment: more than mere semantics For decades, the issue of guideline adherence for the elderly was barely addressed in
oncologic literature, as older age was a generally accepted contra‐indication for cancer
treatment. In the last decades of the twentieth century, cancer specialists came to realize
that this automatic exclusion of older patients did not do them justice.2 In wake of studies
demonstrating that standard cancer treatment could be given successfully to selected
elderly,3 older patients not receiving standard care were stated to receive “substandard”
or even “inappropriate” treatment.2,4 However, despite the obviously positive
development that age itself is no longer considered to be a criterion on which to base
decisions, it should be emphasized that for the elderly patient discordance with standard
practice or guideline‐recommended treatment does not automatically imply that
treatment is suboptimal. As discussed in Chapters 1‐4 and 6‐8, valid reasons for deviation
from guidelines exist. Furthermore, although there is general consensus that age should
not be the primary reason for withholding treatment,5,6 it would be unfair to say that age
does not matter at all. For instance, the process of ageing means that a person gradually
loses some of his or her physiological reserves, influencing their treatment tolerance. In
addition, much cancer treatment is aimed at preventing future cancer‐related
complications; as ageing limits the remaining life‐expectancy of a patient, it may also limit
the benefit of such treatment.
Using the terms “substandard treatment” or “undertreatment” to describe non‐standard
treatment suggests that any tailoring of treatment to the patient’s situation should be
avoided. However, overtreatment of frail elderly patients may be as harmful as
undertreatment. Therefore, tailor‐made care should be the standard of care for older
patients. The important questions that remain are what factors should guide such tailoring
nd how to reliably determine and balance potential benefit with potential harm. a
Using geriatric concepts in oncology With this in mind, cancer specialists are looking towards the concepts and methods of
geriatric medicine. One such concept is frailty, which is a state of decreased physiological
reserves, arising from cumulative decline across multiple physiological systems, resulting
in a diminished resistance to stressors;7 it can be seen as the final common pathway of
ageing. As both cancer and its treatment form significant stressors, which require patients
to encroach on their reserves, the concept of frailty appears particularly relevant for older
cancer patients. Another geriatric concept that has been adopted in oncology is the
comprehensive geriatric assessment (CGA), which is a systematic appraisal of the health
status of older individuals, focusing on somatic as well as psychosocial and functional
domains;8 it is used to detect disabilities and geriatric conditions that potentially
contribute to frailty.
207

Chapter 13
However, whereas geriatricians consider the CGA to be the entirety of their consultation
with a patient, focusing on as many as twenty geriatric conditions,9,10 in geriatric oncology
the term CGA is used to describe any procedure in which one or more screening tests for
individual geriatric conditions is used. For example, the International Society of Geriatric
Oncology, in their 2005 guidelines for the use of geriatric tools in the assessment of older
cancer patients,11 states that a CGA should consist of a mini‐mental state examination
(MMSE), geriatric depression scale (GDS) and Katz activities of daily living (ADL) scale. In
other studies that describe using a CGA for older cancer patients, this consisted of only
one ADL or instrumental ADL scale.12 However, malnutrition, polypharmacy, addressed
and unaddressed comorbidity and mobility disorders have also been demonstrated to be
quite common in older cancer patients (Chapter 9 and 10) and deserve evaluation.
Limiting a CGA to only a few geriatric conditions could mean that relevant frailty remains
unrecognized, as it has been demonstrated that many geriatric conditions are easily
missed if they are not specifically looked for.13 For example, one study comparing the
physician’s assessment of a patient’s fitness for chemotherapy with the assessment as
done by a CGA, revealed that 20% of patients deemed fit by their oncologist had more
than three geriatric conditions.14
These newly identified health issues could form the starting point for interventions aimed
at optimizing quality of life, survival and treatment tolerance. Studies that incorporated a
geriatric consultation into standard oncologic care for older cancer patients found that
over 70% of patients subsequently receive at least one non‐oncologic intervention.15‐17
The effect of such interventions remains to be evaluated, as thus far only one study has
addressed this issue. In this study by Rao et al. adding geriatric care to standard in‐patient
cancer care for 99 hospitalized elderly cancer patients resulted in a significant decrease in
the amount of emotional limitations, social dysfunction and bodily pain that these
patients experienced at three months; the effect on pain was still significant one year after
hospital discharge.18 This aspect of CGA in cancer care certainly warrants further
investigation.
Another purpose for which CGA could be used in geriatric oncology is to guide treatment
decisions. Cancer treatment should be tailored to the estimated remaining life‐
expectancy, and as demonstrated in Chapter 10 and 11, frailty – defined by the presence
of one or more geriatric conditions – is an independent predictor of survival, even after
correcting for age, cancer type, stage and treatment choice. Interestingly, the presence of
frailty seems to be more important than the individual geriatric conditions that cause the
frailty, supporting the concept of frailty as a final common pathway of the ageing process.
In addition to predicting survival, frailty also appears to be of value in predicting treatment
tolerance, in particular toxicity of chemotherapy (Chapter 10 and 11), but these findings
still require further confirmation. Despite this uncertainty, studies that have incorporated
208

General Discussion
CGA into standard cancer care demonstrate that knowledge of the presence of geriatric
conditions resulted in an altered treatment plan in 21‐49% of patients;15‐17,19 these
alterations consisted of temporary delays to optimize non‐oncologic issues as well as both
decreased and increased intensity of treatment, meaning that some patients actually were
less frail than initially thought by the cancer specialist.
In summary, the value of CGA has been proven for identifying previously unrecognized
health issues, which can guide treatment decisions and can also be used to implement
multidisciplinary interventions to optimize a patient’s health status and quality of life. We
therefore strongly urge all cancer specialists to incorporate a CGA into the standard
ssessment of all older cancer patients. a
Frailty screening tools An important obstacle to incorporating the CGA into oncologic practice is the fact it is time
consuming. This has understandably led cancer specialists to search for a short screening
tool or checklist that could stratify patients as fit or unfit for treatment, rendering a full
assessment unnecessary.20 An alternative approach is to use the tool to select patients for
further assessment.21 However, currently available screening tools lack discriminative
power and the prevalence of one or more geriatric conditions is so high that almost all
older cancer patients will potentially benefit from further assessment (Chapter 12). As
capturing the heterogeneity and nuances of the elderly cancer population in a few simple
questions is unlikely to become a reality, future research should focus on other ways in
which the full CGA with subsequent interventions could be incorporated into the cancer
care process. Although this will be time consuming, it will be balanced out by the gains in
terms of avoiding under‐ and overtreatment, preventing complications and adverse
eatment outcomes as well as improving quality of life. tr
Patient preferences and decision making Another factor that could influence treatment decisions for older cancer patients is a
patient’s personal preferences. In several studies included in this thesis (Chapter 1‐4 and
8), patient preference was an important reason for non‐adherence to treatment
guidelines. In addition, patient’s refusal of trial participation was an important factor in
the poor accrual for our clinical trial on chemotherapy for metastatic breast cancer
(Chapter 5). It is possible that elderly patients truly do not want cancer treatment, and are
unwilling to participate in trials. However, older patients tend to take a more passive role
in the decision‐making process,22 and because they are less likely to access alternative
sources of information,23 their decisions will be greatly influenced by the information that
he or she has been offered by the cancer specialist.24 In addition, studies have shown that
the endorsement of a clinical trial by the treating physician greatly increases the likelihood
209

Chapter 13
of trial participation.25,26 Therefore, an interesting but as yet unanswered question is how
much of what is stated to be the patient’s preference is actually a reflection of the
physician’s preference.
Various studies have demonstrated that to the older patient, quality of life and
maintaining functional independence are much more important than overall survival.27
However, these types of outcome measures are generally not included in clinical trials.28 In
order for future studies to supply truly relevant information for the older patient, we
highly recommend incorporating geriatric outcome measures, such as cognitive function
and functional capacity, as well as quality‐adjusted survival analyses like the TWiST, the
ime Without Symptoms or Toxicity.29 T
Directions for future research and patient care Given the currently available data on the value of CGA in geriatric oncology, we believe
that some form of geriatric assessment should be incorporated into standard cancer care
for older patients. However, the precise role of the comprehensive geriatric assessment
for both patient care and decision making needs to be determined. A further exploration
of the ability of CGA to predict treatment tolerance is warranted; however, to avoid
previous issues with heterogeneity in patient population and limited content of CGA,
these studies should be conducted in single‐tumour cohorts and include a broad range of
geriatric conditions. Another important research question still to be addressed is whether
implementing interventions aimed at the conditions identified by CGA can improve a
patient’s ability to tolerate treatment, and in line with this, whether this will improve
quality of life and/or survival.
As stated before, research that addresses older cancer patients should incorporate
baseline frailty information. Given the heterogeneity of the elderly population, these data
allow for comparison between studies and enable translation of outcomes to the
individual patient. In addition, future studies in older cancer patients should focus not only
on survival and somatic treatment complications, but also include relevant patient‐
centred outcome measures to allow weighing the benefits with the risks of a particular
eatment for the individual patient. tr
In conclusion, for older cancer patients, tailor‐made care should be the standard of care,
striking the golden mean between undertreatment and overtreatment and fully taking
into account the heterogeneity of this patient population. The comprehensive geriatric
assessment will provide invaluable information about a patient’s overall health status, but
its exact place within the decision‐making process still remains to be defined.
210

General Discussion
References 1. Audisio RA, Van LB. When reporting on older patients with cancer, frailty information is needed. Annals of
Surgical Oncology 2011;18:4‐5 2. Byrne A, Carney DN. Cancer in the elderly. Curr Probl Cancer 1993;17:145‐218. 3. Valentini V, Morganti AG, Luzi S et al. Is chemoradiation feasible in elderly patients? A study of 17 patients
with anorectal carcinoma. Cancer 1997;80:1387‐1392. 4. Bergman L, Dekker G, van Kerkhoff EH et al. Influence of age and comorbidity on treatment choice and
survival in elderly patients with breast cancer. Breast Cancer Res Treat 1991;18:189‐198. 5. Audisio RA, Bozzetti F, Gennari R, et al. The surgical management of elderly cancer patients;
recommendations of the SIOG surgical task force. Eur J Cancer 2004;40:926‐938. 6. Lichtman SM, Wildiers H, Chatelut E et al. International Society of Geriatric Oncology Chemotherapy
Taskforce: evaluation of chemotherapy in older patients‐‐an analysis of the medical literature. J Clin Oncol 2007;25:1832‐1843.
7. Ferrucci L, Guralnik JM, Cavazzini C et al l. The frailty syndrome: a critical issue in geriatric oncology. Crit Rev Oncol Hematol 2003;46:127‐137.
8. Extermann M, Aapro M, Bernabei R et al. Use of comprehensive geriatric assessment in older cancer patients: recommendations from the task force on CGA of the International Society of Geriatric Oncology (SIOG). Crit Rev Oncol Hematol 2005;55:241‐252.
9. Buurman BM, Hoogerduijn JG, de Haan RJ et al l. Geriatric conditions in acutely hospitalized older patients: prevalence and one‐year survival and functional decline. PLoS One 2011;6:e26951.
10. Ellis G, Langhorne P. Comprehensive geriatric assessment for older hospital patients. Br Med Bull 2004; 71:45‐59.
11. Extermann M, Aapro M, Bernabei R et al. Use of comprehensive geriatric assessment in older cancer patients: recommendations from the task force on CGA of the International Society of Geriatric Oncology (SIOG). Crit Rev Oncol Hematol 2005;55:241‐252.
12. Extermann M, Overcash J, Lyman GH et al. Comorbidity and functional status are independent in older cancer patients. J Clin Oncol 1998;16:1582‐1587.
13. Extermann M, Meyer J, McGinnis M et al. A comprehensive geriatric intervention detects multiple problems in older breast cancer patients. Crit Rev Oncol Hematol 2004; 49:69‐75.
14. Wedding U, Kodding D, Pientka L et al. Physicians' judgement and comprehensive geriatric assessment (CGA) select different patients as fit for chemotherapy. Crit Rev Oncol Hematol 2007; 64:1‐9.
15. Chaibi P, Magne N, Breton S et al l. Influence of geriatric consultation with comprehensive geriatric assessment on final therapeutic decision in elderly cancer patients. Crit Rev Oncol Hematol 2011;79:302‐307.
16. Caillet P, Canoui‐Poitrine F, Vouriot J et al. Comprehensive Geriatric Assessment in the Decision‐Making Process in Elderly Patients With Cancer: ELCAPA Study. J Clin Oncol 2011;29:3636‐3642.
17. Horgan AM, Leighl NB, Coate L et al. Impact and Feasibility of a Comprehensive Geriatric Assessment in the Oncology Setting: A Pilot Study. Am J Clin Oncol 2011.
18. Rao AV, Hsieh F, Feussner JR, Cohen HJ. Geriatric evaluation and management units in the care of the frail elderly cancer patient. J Gerontol A Biol Sci Med Sci 2005;60:798‐803.
19. Girre V, Falcou MC, Gisselbrecht M et al. Does a geriatric oncology consultation modify the cancer treatment plan for elderly patients? J Gerontol A Biol Sci Med Sci 2008; 63:724‐730.
20. Extermann M, Boler I, Reich RR et al. Predicting the risk of chemotherapy toxicity in older patients: The Chemotherapy Risk Assessment Scale for High‐Age Patients (CRASH) score. Cancer 2012;118:3377‐86.
21. Overcash JA, Beckstead J, Moody L et al. The abbreviated comprehensive geriatric assessment (aCGA) for use in the older cancer patient as a prescreen: scoring and interpretation. Crit Rev Oncol Hematol 2006;59:205‐210.
22. Fallowfield L. Participation of patients in decisions about treatment for cancer. BMJ 2001;323:1144. 23. Pinquart M, Duberstein PR. Information needs and decision‐making processes in older cancer patients. Crit
Rev Oncol Hematol 2004;51:69‐80. 24. Pierce PF. Deciding on breast cancer treatment: a description of decision behavior. Nurs Res 1993;42:22‐28. 25. Townsley CA, Chan KK, Pond GR et al. Understanding the attitudes of the elderly towards enrolment into
cancer clinical trials. BMC Cancer 2006;6:34.
211

Chapter 13
212
26. Wright JR, Whelan TJ, Schiff S et al. Why cancer patients enter randomized clinical trials: exploring the factors that influence their decision. J Clin Oncol 2004;22:4312‐4318.
27. Yellen SB, Cella DF, Leslie WT. Age and clinical decision making in oncology patients. J Natl Cancer Inst 1994;86:1766‐1770.
28. Reuben DB, Tinetti ME. Goal‐oriented patient care‐‐an alternative health outcomes paradigm. N Engl J Med 2012;366:777‐779.
29. Goldhirsch A, Gelber RD, Simes RJ et al. Costs and benefits of adjuvant therapy in breast cancer: a quality‐adjusted survival analysis. J Clin Oncol 1989;7:36‐44.

Chapter 14
Summary / Samenvatting

Chapter 14
Summary: Decision making in geriatric oncology
In Western societies, the population is ageing. Between 2012 and 2030, the proportion of
Dutch inhabitants aged 75 years and over will double. This will have significant
implications for health care, as many diseases that predominantly affect the elderly will
become more prevalent. This is also true for cancer.
Optimal cancer care for the elderly ideally strikes the golden mean between
overtreatment and undertreatment and must be tailored to the individual patient. Cancer
specialists are now collaborating with geriatricians to optimize this decision‐making
process. The aim of this thesis was to study current treatment practice in older cancer
patients with breast cancer, colon cancer and head and neck cancer (Part I and II) and to
investigate the potential value of geriatric concepts and methods in this decision‐making
process (Part III).
In Part I, current treatment practice and decision making is studied in older patients with
breast cancer. In Chapter 1, we examined a cohort of 166 patients aged 70 years and
older, newly diagnosed with breast cancer between 2002 and 2004 at the Medical Centre
Alkmaar (MCA). We found that 74% of these patients were diagnosed and treated in
accordance with national guidelines. However, guideline adherence decreased with age:
only 40% of patients aged 90 years and older received guideline recommended treatment
compared to 88% of patients aged 70‐79 years. The deviations from guidelines were
primarily deliberate adjustments to comorbid diseases and the patient’s preferences.
To assess whether implementation of a weekly, multidisciplinary breast cancer meeting to
discuss all new patients in 2006 improved guideline adherence, we extended the previous
study until 2007 and focused on the 232 patients aged 70 years and older who were
diagnosed with an early stage of breast cancer within that period (Chapter 2). For early
stage breast cancer, surgery is the primary treatment. However, contrary to what we
expected to find, the percentage of patients that received surgery decreased from 94% in
2002 to 76% in 2007 and this decrease was even more explicit in patients aged 80 years
and older, in which this proportion decreased from 80% to 33%. Although guideline
adherence was not altered by the initiation of the multidisciplinary meetings, we did find
that awareness of guidelines improved over time and discordance was more clearly
motivated in the patient’s charts.
In Chapter 3, we took a more detailed look at a cohort of 187 patients aged 75 years and
older with early breast cancer for which surgery was omitted despite guideline
recommendations, diagnosed between 1990 and 2008 at five Dutch hospitals. Most of
these patients received hormone treatment instead. Earlier studies have demonstrated
that this kind of treatment can prevent disease progression in many patients for some
years. However, for patients with a limited life‐expectancy, a temporary solution may
214

Summary / Samenvatting
suffice. In our study, patients lived for an average of 2.1 years after the breast cancer was
diagnosed. We found that 34% of patients died of breast cancer; this is quite similar to
what is seen in studies of older breast cancer patients receiving guideline recommended
treatment. For 21% of the patients in our study, breast cancer was stated as an underlying
disease in patients who died of other causes. However, for the remaining patients, breast
cancer was not thought to be relevant at the time of death, suggesting that hormone
treatment had been successful in suppressing the cancer for the remainder of the
patient’s lifetime. Interestingly, in one‐third of patients, omission of surgery was not for
medical reasons but at the patient’s own request.
Chapters 1 to 3 focus on treatment decisions that were made in the hospital or out‐
patient clinic. However, this does require referral to a hospital by the primary care
physician. In Chapter 4, we sent out a questionnaire to elderly‐care physicians (ECPs), who
provide the primary care for patients living in nursing homes, to inquire after their
decisions regarding patients with possible breast cancer. Almost 60% of respondents
stated that they had encountered at least one such patient in the past year; of these, one‐
third was not referred to a hospital. The most important reasons for not referring the
patient were end‐stage dementia, the patient’s or family’s preference and limited life‐
expectancy. Referral was often felt to be too burdensome for these very vulnerable
patients. In this chapter, potential alternatives to hospital‐based care are discussed.
Optimal decision making is based on evidence that is obtained from clinical trials focusing
specifically on the target population, in which treatment is randomly assigned so that
potential confounding and bias is as limited as possible. However, even when a clinical
trial is designed for older patients, it may be difficult to accrue sufficient numbers of
patients. We encountered this issue in the OMEGA study of the Dutch Breast Cancer
Trialists’ Group (BOOG), which was designed for frail older patients with metastatic breast
cancer (for more detail, see Chapter 10), and therefore examined possible obstacles to
accrual (Chapter 5). The primary barrier we identified was that a patient’s overall health
status was considered either too fit or too frail for inclusion, as well as the patient’s refusal
to participate or preference for a particular type of treatment. These findings demonstrate
how difficult it is to design a study for older cancer patients and emphasize the need for
educating patients on the potential benefits of trial participation.
In Part II, current treatment practices and decision making is studied in two other types of
cancer: colon cancer and head and neck cancer. In Chapter 6, we compared treatment for
colon cancer in 183 patients aged 70 years and older with 103 patients younger than 70
years. Of the older patients, 91% received surgery in accordance with guidelines compared
to 100% of the younger age group. For chemotherapy, these proportions were 32% and
85% respectively. The primary reason for deviation from guidelines was age, as well as
comorbidity and poor general health. Despite the fact that only fit patients received
215

Chapter 14
standard treatment, older patients experienced more post‐operative complications and
mortality than younger patients; for chemotherapy, toxicity was equal despite careful
selection and less aggressive regimens for older patients. These results suggest that older
age does affect the ability of a patient to tolerate treatment and can therefore not be
discounted in the decision‐making process.
There are many different causes for iron deficiency but in 2‐15% of patients, it is caused by
gastro‐intestinal cancer. To diagnose such cancers, endoscopy is needed, which is a
burdensome examination; if cancer is found, surgery is often the next step. As not all
patients are fit enough for surgery, or do not want this treatment, it is sometimes decided
to forego further examination when iron‐deficiency is found. In Chapter 7, we looked at a
group of 471 patients aged 80 years and older with iron‐deficiency anaemia, diagnosed at
the laboratory of the Gelre hospital in Apeldoorn. For 59% of these patients, no anaemia‐
related diagnostic procedures were performed. This was more likely in case of female sex,
older age, less severe anaemia and in the absence of gastrointestinal symptoms. Initial
work‐up revealed 46 malignancies (9 upper and 37 lower gastrointestinal tract). In
addition to these, another 16 patients were diagnosed with colon cancer during follow‐up,
primarily in patients who received no initial diagnostic procedures. Of these patients, 9
were subsequently treated surgically; for these patients, the delay in diagnosis could have
resulted in disease progression and thus decreased the likelihood of curative treatment or
increased the risk of complications. By contrast, a delay in diagnosis is less relevant if the
underlying disease is incurable or requires treatment that is considered too burdensome
for the individual patient. Median survival varied greatly, depending on the initial
diagnosis. For colon cancer patients receiving surgery, perioperative mortality was high
(15%) but after 1.3 years, benefit of surgical treatment became apparent.
Chapter 8 focuses on 606 patients with head and neck cancer of all ages, diagnosed and
treated at the Medical Centre Alkmaar. Head and neck cancer can have tremendous
impact on a patient’s quality of life, as the disease affects some of our most basic body
functions, such as breathing, swallowing and speech. However, the burden of treatment
can be just as great. An additional complicating factor is that head and neck cancer is
often related to alcohol use and smoking and as a result, patients frequently suffer from
multiple lifestyle‐related diseases simultaneously. These diseases can affect the ability of
patient to tolerate treatment. In our study, we found that 91% of patients were treated in
accordance with guidelines. Primary reasons for discordant treatment were comorbidity
and lack of cooperation in patients aged younger than 70 years and patient’s refusal of
treatment for older patients. Five‐year overall survival was 64% for patients treated in
accordance with guidelines, compared to only 15% in case of discordant treatment,
emphasizing the importance of guideline adherence in these patients.
216

Summary / Samenvatting
In Part III, the value of two concepts of geriatric medicine is examined for oncologic
decision making. One such concept is frailty, which is a state of diminished functional
reserves, caused by a cumulative decline across multiple organ systems, resulting in a
decreased resistance to stressors. Frailty can be seen as the final common pathway of
ageing. As both cancer and its treatment represent significant stressors, which require a
patient to use their reserves to get through it, the concept of frailty seems particularly
relevant to oncology. A second concept is the comprehensive geriatric assessment or CGA,
which is a systematic assessment of a patient’s health status, focusing on their physical,
functional and psychosocial well‐being. It can be used to detect the presence of geriatric
syndromes, such as dementia, depression, malnutrition, disability, impaired mobility etc.,
as well as frailty.
In Chapter 9, the CGA is used in a group of 292 patients aged 65 years and older, with any
type of cancer, acutely admitted to the internal medicine wards of three hospitals. In
these patients, we saw that geriatric syndromes were frequently present in older cancer
patients. For example, almost half of patients suffered from polypharmacy (the use of
more than five types of medications), impaired mobility and malnutrition, while more than
two‐thirds suffered from depressive symptoms, functional limitations and pain. Detecting
these conditions can form a starting point for interventions aimed at optimizing general
health and quality of life. However, the prognosis of these patients was not associated
with these geriatric conditions; for survival, having metastatic disease or cancer‐related
complications that required hospital admission were much more important factors.
Chapter 10 describes the results of the OMEGA study, in which 78 patients aged 65 years
and older with metastatic breast cancer were treated with two types of palliative
chemotherapy. Metastatic breast cancer cannot be cured, and therefore the aim of this
treatment is to prolong survival and maintain an optimal quality of life. By contrast,
serious toxicity of chemotherapy can decrease quality of life and is potentially fatal.
Therefore, predicting toxicity can be quite useful in deciding which patients should or
should not receive palliative chemotherapy. In our study, all patients received a CGA at
baseline. We found that the chance of experiencing serious toxicity due to the
chemotherapy increased steadily with the number of geriatric conditions that a patient
had, rising from 18% in patients without geriatric problems, to over 50% in case two
conditions were present and over 80% in case of three or more.
Chapters 11 is a systematic review of other studies that have assessed the predictive value
of CGA for survival and treatment tolerance, both for chemotherapy as well as oncologic
surgery. We found 37 other studies that addressed this issue; however, little consistency
was found in their results. It appears that different geriatric syndromes were useful for
predicting each of the different outcome measures: frailty (defined as having one or more
geriatric syndromes), nutritional status and comorbidity were predictive of survival; frailty
217

Chapter 14
was also predictive of toxicity of chemotherapy; cognitive impairments and difficulties in
performing the basic daily activities (such as eating, washing or using the toilet) were
associated with not completing all planned cycles of chemotherapy; and difficulties in
performing instrumental daily activities (such as using the telephone or taking medication)
were associated with perioperative complications. The inconsistency in study results could
be caused by the great variety in the study populations (in terms of tumour types, stage of
disease and treatment modalities) that were included in the different studies. Thus,
although various geriatric conditions appear to be of some value for predicting outcome in
elderly cancer patients, the results as yet are too inconsistent to guide treatment
decisions.
Performing a CGA is time‐consuming, which has led cancer specialists to search for short
frailty screening tools that can be used to select which patients should receive a full
assessment. We performed a systematic review to determine the sensitivity and
specificity of the currently available screening tools for the outcome of the complete CGA
(Chapter 12). We identified 14 studies, assessing seven different frailty screening tools.
We found that the Geriatric 8 (G8) and Triage Risk Screening Tool had the best sensitivity
for frailty on full CGA, but these tools lacked specificity; similarly, tools with a good
specificity for frailty, such as the Fried Criteria and abbreviated CGA (aCGA) severely
lacked sensitivity. These findings suggests that all older patients should receive a complete
geriatric assessment as the two‐stepped approach – using frailty screening tools to select
patients for CGA – has insufficient discriminative power.
The general discussion in Chapter 13 elaborates on the observed results and discusses the
plications of these findings for patient care and for future research. im
In conclusion, the studies in this thesis have shown that for older cancer patients, tailor‐
made care should be the standard of care, striking the golden mean between
undertreatment and overtreatment and fully taking into account the heterogeneity of this
patient population. The comprehensive geriatric assessment will provide valuable
information about a patient’s overall health status, but its exact place within the decision‐
making process still remains to be defined.
218

Summary / Samenvatting
Samenvatting: Besluitvorming in de geriatrische oncologie
In een vergrijzend Nederland zal het aantal inwoners ouder dan 75 jaar in de komende 20
jaar verdubbelen, met grote gevolgen voor de gezondheidszorg. Zo zullen allerlei ziekten
die vooral ouderen treffen, waaronder kanker, steeds vaker voorkomen. Een optimale
kankerbehandeling van de oudere patiënt moet aangepast zijn aan het individu; alleen zo
kan de balans gevonden worden tussen onderbehandeling en overbehandeling.
Dit proefschrift gaat over het zoeken van die balans. In de eerste twee delen is gekeken
naar de huidige besluitvorming en invulling van de zorg voor oudere patiënten met
borstkanker, darmkanker en hoofd‐halskanker. Het laatste deel van dit proefschrift
beschrijft de toegevoegde waarde van een geriatrische werkwijze in het complexe
besluitvormingsproces rond de kankerbehandeling bij ouderen. Geriaters zijn
ziekenhuisspecialisten die zich richten op het zorgvuldig in kaart brengen en optimaliseren
van de gezondheid van oudere patiënten met meervoudige gezondheidsproblematiek.
Deel I richt zich op borstkanker bij ouderen. Hoofdstuk 1 beschrijft een groep van 166
patiënten van 70 jaar en ouder, bij wie tussen 2002 en 2004 in het Medisch Centrum
Alkmaar borstkanker werd vastgesteld. Daarbij bleek dat 74% van deze patiënten
overeenkomstig de Nederlandse behandelrichtlijnen werd onderzocht en behandeld.
Echter, hoe ouder de patiënt, hoe vaker van de geadviseerde behandeling werd
afgeweken: slechts 40% van de patiënten boven de 90 jaar werd behandeld volgens de
richtlijnen. Het afwijken van de richtlijnen gebeurde veelal bewust, vanwege bijkomende
ziekten of de voorkeur van de patiënt.
Om te beoordelen of het invoeren van een wekelijkse, multidisciplinaire
borstkankerbespreking in 2006 een verbetering gaf in het volgen van de richtlijn, werd het
voorgaande onderzoek verlengd tot 2007, waarbij de studie zich beperkte tot de 232
patiënten ouder dan 70 jaar bij wie een vroeg stadium van borstkanker werd vastgesteld
(Hoofdstuk 2). Bij een vroeg stadium van borstkanker staat chirurgie centraal in de
behandeling. In tegenstelling tot wat verwacht was, daalde het percentage patiënten dat
werd geopereerd van 94% in 2002 tot 76% in 2007. Deze daling was het meest
uitgesproken bij patiënten boven de 80 jaar: voor hen daalde het percentage van
respectievelijk 80% naar 33%. Hoewel het volgen van de richtlijn niet verbeterde door de
invoering van de borstkankerbespreking, bleken behandelaars de richtlijn wel bewuster te
hanteren; afwijkingen hiervan werden ook beter werd gemotiveerd in de patiëntenstatus.
In Hoofdstuk 3 is meer gedetailleerd gekeken naar een groep van 187 borstkanker‐
patiënten, van 75 jaar en ouder, bij wie van de geadviseerde chirurgische behandeling
werd afgezien. Het merendeel van deze patiënten kreeg als vervanging hormonale
behandeling. Eerder onderzoek heeft uitgewezen dat deze behandeling de borstkanker
219

Chapter 14
tijdelijk kan onderdrukken maar het niet kan genezen; echter, voor patiënten met een
beperkte levensverwachting kan een tijdelijke oplossing soms volstaan. De patiënten in
ons onderzoek leefden gemiddeld nog 2,1 jaar nadat de borstkanker was vastgesteld en
34% overleed ten gevolge ervan. Voor bijna de helft van de patiënten was de borstkanker
klinisch niet relevant op het moment van overlijden. Dit suggereert dat de
hormoontherapie de kanker voldoende heeft onderdrukt voor de resterende levensjaren
van de patiënt. Hormonale behandeling lijkt dus een effectief en veilig alternatief voor
opereren bij geselecteerde oudere patiënten, maar er moet wel rekening gehouden
worden met de mogelijke negatieve gevolgen van het weglaten van chirurgie op de
langere termijn, bijv. doordat de tumor ongevoelig wordt voor de hormoonbehandeling.
Een interessant bijkomend gegeven is dat bij één‐derde van de patiënten het weglaten
van de operatie niet om medische redenen gebeurde maar op verzoek van de patiënt.
Hoofdstuk 1 tot en met 3 hebben betrekking op de behandeling van borstkanker in het
ziekenhuis. Daaraan vooraf gaat een verwijzing naar het ziekenhuis. Hoofdstuk 4 beschrijft
de uitkomsten van een enquête gericht op het verwijsbeleid van specialisten
ouderengeneeskunde bij verdenking op borstkanker. Specialisten ouderengeneeskunde
zijn de artsen die de basiszorg leveren aan patiënten die verblijven in een verpleeghuis.
Bijna 60% van de respondenten meldde in het afgelopen jaar tenminste één patiënt met
een mogelijke borstkanker te hebben behandeld; hiervan werd een‐derde niet
doorverwezen voor nadere diagnostiek of behandeling. De belangrijkste redenen daarvoor
waren een eindstadium van dementie, de wens van de patiënt of de familie en een
beperkte levensverwachting. Het bezoek aan het ziekenhuis werd veelal te belastend
geacht voor deze kwetsbare patiëntengroep. In dit hoofdstuk worden ook mogelijke
alternatieven voor ziekenhuiszorg besproken.
Medici baseren hun behandelkeuzes bij voorkeur op bewijzen verkregen uit klinische
studies. Het sterkste bewijs komt uit zogeheten gerandomiseerde studies, waarbij
patiënten niet op basis van patiëntkenmerken maar juist door toeval aan een bepaalde
behandeling worden toegewezen. Dit zorgt ervoor dat mogelijke bijkomende factoren en
patiënteigenschappen zo gelijkmatig mogelijk over de verschillende behandelgroepen
verdeeld worden. Om diverse redenen, waaronder ethische, is deze vorm van onderzoek
niet altijd mogelijk. In dat geval zijn beschrijvende studies, zoals weergegeven in de
voorgaande hoofdstukken, een alternatief; deze kunnen waardevolle aanvullende
informatie verschaffen. Ook als het wel mogelijk is om een gerandomiseerde studie te
ontwerpen, kan het moeilijk zijn om hiervoor voldoende patiënten te werven. Dat was ook
het geval bij de OMEGA studie, die werd opgezet voor kwetsbare ouderen met een
uitgezaaide vorm van borstkanker (zie ook Hoofdstuk 10). Vanwege teleurstellende
patiëntenaantallen werd onderzoek ingezet naar mogelijk obstakels in het werven van
patiënten (Hoofdstuk 5). Het belangrijkste obstakel bleek te zijn dat de conditie van de
220
Summary / Samenvatting
patiënt als te goed of te slecht werd beschouwd voor deelname. Daarnaast wilden veel
patiënten zelf niet mee doen, of hadden zij een sterke voorkeur voor één van de twee
behandelopties waardoor randomisatie van de behandeling niet gewenst was. Deze
uitkomsten laten zien hoe moeilijk het is om een goede studie te ontwerpen voor ouderen
en benadrukken de noodzaak van voorlichting aan patiënten over het belang van
deelname aan wetenschappelijk onderzoek.
In Deel II is de huidige behandeling en besluitvorming bij twee andere soorten kanker
onderzocht: darmkanker en hoofd‐halskanker. In Hoofdstuk 6 werd de behandeling van
darmkanker bij 183 patiënten ouder dan 70 jaar vergeleken met die van 103 patiënten
jonger dan 70 jaar. Van de oudere patiënten kreeg 91% een chirurgische behandeling
zoals geadviseerd door de richtlijnen, vergeleken met 100% van de jongere patiënten.
Voor chemotherapie waren deze percentages respectievelijk 32% en 85%. De belangrijkste
redenen om af te wijken van de richtlijnen waren leeftijd, bijkomende ziektes en de
algehele conditie van de patiënt. Ondanks het feit dat alleen vitale patiënten de standaard
behandeling kregen, ontwikkelden ouderen patiënten meer complicaties na de operatie
en was de sterfte in de eerste maand na de ingreep aanzienlijk hoger. Bij chemotherapie
traden evenveel bijwerkingen op ondanks zorgvuldige selectie van geschikte patiënten en
minder agressieve behandeling voor de oudere patiënten. Deze resultaten tonen aan dat
leeftijd wel degelijk van belang is voor het vermogen van de patiënt om een behandeling
te doorstaan; dit aspect mag dus niet buiten beschouwing kunnen worden gelaten in de
besluitvorming.
Eén van de symptomen van darmkanker is ijzergebrek. Omdat ijzer een belangrijke
bouwstof is van rode bloedcellen, zal ijzergebrek uiteindelijk leiden tot bloedarmoede, ook
wel anemie genoemd. Bij 2‐15% van de patiënten met ijzergebreksanemie is kanker in het
maagdarmkanaal de oorzaak. Kanker veroorzaakt schade aan de binnenkant van de maag
of darm, waar al dan niet ongemerkt bloed uit kan siepelen; hierdoor raakt de
ijzervoorraad in het lichaam uitgeput. Om deze vormen van kanker vast te stellen wordt
de binnenkant van het maagdarmkanaal bekeken tijdens een zogeheten coloscopie (darm)
of gastroscopie (maag). Als daarbij kanker wordt vastgesteld, is chirurgisch ingrijpen de
volgende stap. Omdat niet alle patiënten fit genoeg zijn voor een operatie, of deze
behandeling niet willen, wordt soms afgezien van verdere diagnostiek als een
ijzergebreksanemie wordt vastgesteld. In Hoofdstuk 7 is gekeken naar een groep van 471
patiënten van 80 jaar en ouder waarbij in het laboratorium van het Gelre ziekenhuis in
Apeldoorn ijzergebreksanemie werd vastgesteld. Bij 59% van deze patiënten werd geen
verder onderzoek verricht; dit gebeurde vaker bij vrouwen, bij een hogere leeftijd, bij
minder ernstige bloedarmoede en bij het ontbreken van maagdarmklachten. Bij 61
patiënten werd maagdarmkanker vastgesteld, waarvan 16 pas in tweede instantie omdat
aanvankelijk was gekozen werd voor een terughoudend diagnostisch beleid. Bij patiënten
221

Chapter 14
met darmkanker was de sterfte ten gevolge van de operatie 15% en pas na 1.3 jaar werd
de toegevoegde waarde van opereren ten opzichte van patiënten bij wie van deze
operatie werd afgezien zichtbaar in de overlevingsgrafieken.
Hoofdstuk 8 richt zich op 606 patiënten met hoofd‐halskanker, die behandeld werden in
het Medisch Centrum Alkmaar. Hoofd‐halskanker heeft vaak een ingrijpend effect op de
kwaliteit van leven van een patiënt, omdat het een verstoring kan geven van heel basale
lichaamsfuncties zoals slikken, ademen en spreken. De belasting van de behandeling kan
echter ook zeer groot zijn. Een bijkomende complicerende factor is dat hoofd‐halskanker
vaak een gevolg is van alcoholmisbruik en roken. Hierdoor treden in deze patiëntengroep
vaak gelijktijdig meerdere levensstijl‐gerelateerde ziekten op; deze ziekten kunnen de
belastbaarheid van de patiënten sterk beïnvloeden. In ons onderzoek zagen wij dat 91%
van alle patiënten behandeld werd volgens de richtlijnen, met een leeftijdsgerelateerde
afname. De belangrijkste redenen om van de richtlijnen af te wijken bij jongere patiënten
waren bijkomende ziektes en gebrek aan medewerking van de patiënt terwijl voor oudere
patiënten het afwijken van de richtlijn vooral op verzoek van de patiënt gebeurde. Na vijf
jaar was 64% van de patiënten die volgens de richtlijn werden behandeld nog in leven,
maar slechts 15% van de patiënten met een afwijkende behandeling; dit toont aan hoe
belangrijk het volgen van de richtlijnen voor deze patiëntengroep is.
In Deel III is de mogelijke toegevoegde waarde onderzocht van twee concepten uit de
geriatrie voor de oncologische besluitvorming. Het eerste concept is frailty, ofwel
kwetsbaarheid; in de geriatrie wordt dit gedefinieerd als een toestand van verminderde
reserves, die ontstaat door de opeenstapeling van veroudering van diverse
orgaansystemen, met als gevolg een verminderd vermogen om ziektes op te vangen.
Omdat zowel kanker als kankerbehandeling een forse belasting betekenen voor het
lichaam en een patiënt dwingen om zijn reserves bij te zetten, lijkt het concept van frailty
bijzonder relevant in de oncologie. Een tweede concept is het uitgebreid geriatrisch
onderzoek, ofwel comprehensive geriatric assessment (CGA), waarbij op een
systematische wijze de gezondheidstoestand van een patiënt in kaart wordt gebracht, met
aandacht voor lichamelijke, psychologische, sociale en functionele aspecten. Het wordt
gebruikt om geriatrische problemen op te sporen, zoals dementie, stemmingsstoornissen,
ondervoeding, beperkingen in de zelfredzaamheid of mobiliteit en ook frailty.
In Hoofdstuk 9 werd dit CGA gebruikt in een groep van 292 patiënten van 65 jaar en ouder
met een actieve vorm van kanker die via de spoedeisende hulp werden opgenomen op
één van de interne geneeskunde afdelingen van drie ziekenhuizen. Hierbij bleek dat
geriatrische problematiek veelvuldig voorkomt. Bij bijna de helft van deze patiënten was
sprake van ondervoeding, mobiliteitsproblemen, een overbelaste mantelzorger en
polyfarmacie (het gebruik van meer dan vijf verschillende soorten medicatie) terwijl bij
meer dan twee‐derde sprake was van stemmingsstoornissen, pijn en beperkte
222

Summary / Samenvatting
zelfredzaamheid. Het opsporen van deze aandoeningen kan een aangrijpingspunt zijn voor
het optimaliseren van de gezondheidstoestand en de kwaliteit van leven van een patiënt.
Ons onderzoek toonde echter ook aan dat voor deze specifieke patiëntenpopulatie
geriatrische factoren niet bepalend zijn voor de prognose; hiervoor zijn
kankergerelateerde factoren van veel groter belang.
Hoofdstuk 10 beschrijft de resultaten van de OMEGA studie, waarin 78 patiënten van 65
jaar en ouder met uitgezaaide borstkanker werden behandeld met twee soorten
chemotherapie. Genezing van uitgezaaide kanker is niet mogelijk en het doel van deze
chemotherapie is dan ook vooral om de kwaliteit van leven in de resterende levenstijd te
verbeteren. Omdat ernstige bijwerkingen van de chemotherapie die kwaliteit juist nadelig
kunnen beïnvloeden en tot vroegtijdig overlijden kunnen leiden, zou het waardevol zijn als
vooraf voorspeld kon worden bij welke patiënten ernstige bijwerkingen te verwachten
zijn. In ons onderzoek kregen alle patiënten voor aanvang van de chemotherapie een CGA.
Daarbij werd gezien dat de kans op ernstige bijwerkingen bijna lijnrecht steeg met het
aantal geriatrische aandoeningen bij de patiënt; van patiënten zonder zulke aandoeningen
had slechts 18% ernstige bijwerkingen, maar dit percentage steeg naar 50% bij twee
geriatrische aandoeningen en 80% bij drie of meer. Bovendien bleek ook de overleving van
de patiënten gerelateerd aan geriatrische problematiek.
Hoofdstuk 11 geeft een overzicht van 37 eerder gepubliceerde studies naar de
voorspellende waarde van het CGA voor overleving en belastbaarheid – zowel wat betreft
chemotherapie als chirurgie ‐ die tot nu toe verricht zijn bij oudere kankerpatiënten.
Helaas zijn de uitkomsten van deze 37 studies tegenstrijdig. Daarnaast lijkt het erop dat
verschillende factoren voorspellend zijn per bestudeerde uitkomstmaat: frailty
(gedefinieerd als de aanwezigheid van één of meer geriatrische problemen), ondervoeding
en comorbiditeit waren voorspellend voor overleving; frailty was ook voorspellend voor
de toxiciteit van chemotherapie; cognitieve stoornissen en beperkingen in de
zelfredzaamheid waren voorspellend voor het voltooien van alle geplande chemokuren;
en beperkingen in de zelfredzaamheid waren voorspellend voor complicaties na
oncologische operaties. Het gebrek aan eenduidigheid in de resultaten van deze studies
zou het gevolg kunnen zijn van het brede scala aan patiëntenpopulaties waarin deze
onderzoeken verricht werden. Al met al lijken geriatrische problemen wel voorspellende
waarde te hebben voor de oudere patiënt met kanker maar is het nog te vroeg om de
besluitvorming rond de kankerbehandeling uitsluitend hierop te baseren.
Omdat het uitvoeren van een CGA tijdrovend is, zijn kankerbehandelaars op zoek gegaan
naar een korte vragenlijst of screening tool die gebruikt kan worden om patiënten te
selecteren voor uitgebreider onderzoek. De ideale screeningstool heeft een zeer hoge
sensitiviteit, wat betekent dat alle kwetsbare patiënten geïdentificeerd worden, en ook
een hoge specificiteit, wat betekent dat zo min mogelijk fitte patiënten ten onrechte als
223

Chapter 14
224
kwetsbaar worden aangewezen. Hoofdstuk 12 geeft een overzicht van de 14 studies die
tot op heden over dit onderwerp verricht zijn. De Geriatric 8 (G8) en Triage Risk Screening
Tool hadden de beste sensitiviteit voor kwetsbaarheid, maar misten specificiteit;
omgekeerd hadden die vragenlijsten met een goede specificiteit een te geringe
sensitiviteit. Gezien deze uitkomsten lijkt een een twee‐traps‐CGA, waarin een
screeningstool wordt gebruikt om patiënten te selecteren voor uitgebreider onderzoek,
niet haalbaar met de nu beschikbare vragenlijsten.
In Hoofdstuk 13 wordt uitgebreider ingegaan op de resultaten van de voorgaande
onderzoeken en besproken welke consequenties deze hebben voor de patiëntenzorg en
toekomstig onderzoek. Samenvattend blijkt uit de studies in dit proefschrift dat zorg op
maat de norm zou moeten zijn in de behandeling van ouderen met kanker, waarbij de
balans gezocht wordt tussen onderbehandeling en overbehandeling en waarbij rekening
wordt gehouden met de verscheidenheid aan patiënten die in deze populatie wordt
gezien. Het uitgebreid geriatrisch onderzoek kan belangrijke aanvullende informatie
verschaffen over de gezondheidstoestand van de patiënt maar de exacte rol die dit
onderzoek kan vervullen in de besluitvorming rond de behandeling van ouderen met
kanker moet nog worden bepaald.



Author Affiliations

Author Affiliations
T. Acampo, MD Department of Geriatric Medicine, Gelre Hospitals, Apeldoorn
W.P. Achterberg, MD PhD Department of public Health and Primary Care, Leiden University Medical Centre, Leiden
E. Bastiaannet, MSc PhD Department of Surgery and Department of Gerontology and Geriatrics, Leiden University Medical Centre, Leiden
E. Boven, MD PhD Department of Medical Oncology, Vrije Universiteit Medical Centre, Amsterdam
J.J. Braun, MD PhD Department of Internal Medicine Vlietland Hospital, Schiedam
N.G. Breeuwsma, MD Department of Pathology, Medical Centre Alkmaar, Alkmaar
R.J. Bun, MD Department of Oral and Maxillofacial Surgery, Medical Centre Alkmaar, Alkmaar
B.M. Buurman, MSc PhD Department of Internal Medicine, section of Geriatric Medicine, Academic Medical Centre, Amsterdam
D. Evers, MD Department of Internal Medicine, Haga Hospital, the Hague
L. van der Geest Comprehensive Cancer Centre, the Hague
H. de Graaf, MD PhD Department of Medical Oncology, Medical Centre Leeuwarden, Leeuwarden
S.M. de Groot Dutch Breast Cancer Trialists' Group BOOG/Comprehensive Cancer Centre, Amsterdam
V.C. Hamelinck, MSc Department of Surgery and Department of Gerontology and Geriatrics, Leiden University Medical Centre, Leiden
F.E. de Jongh, MD PhD Department of Internal Medicine, Ikazia Hospital, Rotterdam
J.M. Jonker, MD Department of Geriatric Medicine, Slotervaart Hospital, Amsterdam
I.M.J.A. Kuper, MD Department of Geriatric Medicine, Slotervaart Hospital, Amsterdam
G.T. de Kuyper, MD Department of Otolaryngology, Medical Centre Alkmaar, Alkmaar
A.E. van Leeuwen‐Stok, PhD Dutch Breast Cancer Trialists' Group BOOG, Amsterdam
G.J. Liefers, MD PhD Department of Surgery, Leiden University Medical Centre, Leiden
228

Author Affiliations
M. Los, MD PhD Department of Internal Medicine, St. Antonius Hospital, Nieuwegein
E. Maartense, MD PhD Department of Internal Medicine, Reinier de Graaf Hospital, Delft
B.C. van Munster, MD PhD Department of Internal Medicine, section of Geriatric Medicine, Academic Medical Centre, Amsterdam
Department of Geriatric Medicine, Gelre Hospitals, Apeldoorn
J.W.R. Nortier, MD PhD Department of Medical Oncology, Leiden University Medical Centre, Leiden
H.A. Paling, MD Department of Geriatric Medicine, Gelre Hospitals, Apeldoorn
J.E.A. Portielje, MD PhD Department of Internal Medicine, Haga Hospital, The Hague
A. Pronk, MD PhD Department of Surgery, Diakonessenhuis, Utrecht
J.A. Remijn, PhD Department of Clinical Chemistry and Hematology, Gelre Hospitals, Apeldoorn
S.E. de Rooij, MD PhD Department of Internal Medicine, section of Geriatric Medicine, Academic Medical Centre, Amsterdam
J.G. Schrama, MD PhD Department of Internal Medicine, Spaarne Hospital, Hoofddorp
W.H. Schreurs, MD PhD Department of Surgery, Medical Centre Alkmaar, Alkmaar
C. Seynaeve, MD PhD Department of Medical Oncology, Erasmus University Medical Centre – Daniel den Hoed Cancer Centre, Rotterdam
M. Soesan, MD Department of Internal Medicine, Slotervaart Hospital, Amsterdam
H.J. van Slooten, MD PhD Department of Pathology, Medical Centre Alkmaar, Alkmaar
C.H. Smorenburg, MD PhD Department of Internal Medicine, Medical Centre Alkmaar, Alkmaar
H. van Tinteren Antoni van Leeuwenhoek Hospital/NKI, Amsterdam
C.R. Tulner, MD PhD Department of Geriatric Medicine, Slotervaart Hospital, Amsterdam
S.A.C van Tuyl, MD PhD Department of Gastro‐enterology, Diakonessenhuis, Utrecht
229
Author Affiliations
230
J.M. Uppelschoten, MD Department of Radiotherapy, Medical Centre Alkmaar, Alkmaar
A.G. Vos, MD Department of Internal Medicine, Diakonessenhuis, Utrecht
W. van de Water, MD Department of Surgery, Leiden University Medical Centre, Leiden
B.M. Wiarda, MD Department of Radiology, Medical Centre Alkmaar, Alkmaar
M. Wymenga, MD PhD
Department of Medical Oncology, Medisch Spectrum Twente, Enschede
E.S. van der Zaag, MD PhD Department of Surgery, Gelre Hospitals, Apeldoorn
A.M. Zeilemaker, MD Department of Surgery, Rijnland Hospital, Leiderdorp

Curriculum Vitae

232

Curriculum Vitae
Marije Emilie Hamaker was born on January 26th 1976 in Assen, the Netherlands. For most
of her youth, she lived in a little village in Drenthe called Lhee, but spent her early teens in
Hilo, Hawaii. After graduating from high school in 1994, she spent a year travelling to
South America and teaching at a primary school in Zimbabwe. From 1995 to 1996 she
studied psychology and cultural anthropology at the University of Amsterdam before
finally getting into medical school in 1996 at the same university. She completed her
medical training in 2003. Having considered almost every specialty she came into contact
with as a medical student, Marije finally settled on geriatric medicine, first as an AGNIO
and then as of 2005, as a resident. During a rotation at the oncology department of the
Medical Centre Alkmaar, she met Carolien Smorenburg, whose enthusiasm for geriatric
oncology was the inspiration for this thesis.
Since completing her training as a geriatrician in the fall of 2009, Marije has been working
at the Diakonessenhuis in Utrecht and Zeist. She is the secretary of the special interest
group Geriatric Oncology of the Dutch Society for Geriatric Medicine (NVKG) and a
member of the Dutch Geriatric Oncology Foundation (GeriOnNe).

234

Acknowledgements
(Dankwoord)

Acknowledgements (Dankwoord)
Als achtjarig meisje leerde ik voor het eerst over statistiek van mijn grootvader, Hugo
Christiaan Hamaker (1905‐1993). Hij had een grote bak met gele en rode kraaltjes en een
schep met 10 bij 10 gaatjes. Spelenderwijs bracht hij mij daarmee de beginselen bij van
steekproeven nemen en kansberekening. Zo leerde ik dat statistiek iets leuks is (en niet
lleen maar moeilijk en ongrijpbaar). Wellicht is het toen allemaal begonnen. a
Het vervolg liet wel een tijdje op zich wachten. Hoewel het toeval in de wetenschap zo
veel mogelijk moet worden buitengesloten, was dit proefschrift zonder toeval niet tot
stand gekomen. Terugkijkend op de zes jaar waarin dit boekje zich langzaam vulde – eerst
als losse stukjes onderzoek en sinds 2010 als officieel promotietraject – realiseer ik mij dat
het vooral toevallige ontmoetingen zijn geweest die mij tot dit hier hebben gebracht. Je
kunt nog zo veel willen, of nog zo hard werken, maar zonder de juiste mensen kom je er
iet. Bij een aantal van hen wil ik graag stilstaan. n
Carolien Smorenburg – wie had kunnen denken dat er een proefschrift voort zou komen
uit mijn terloopse vraag in het najaar van 2006 of je nog ideeën had voor “iets” met
kanker en ouderen. Jouw enthousiasme voor de geriatrische oncologie blijft inspirerend.
Maar daarnaast ben jij voor mij een voorbeeld geweest van het soort dokter dat ik wilde
worden. Jouw vermogen om zonder veel woorden je betrokkenheid en empathie op een
patiënt over te brengen vind ik nog altijd heel bijzonder. Dank je wel voor je gulheid en
lles wat jij voor mij mogelijk hebt gemaakt. a
Professor Sophia de Rooij – dankzij jou (of is het nu u?) had ik in de zomer van 2009
onverwachts een promotieplan. Eigenlijk kwam ik praten over een ander onderzoek maar
jij was duidelijk: met al twee gepubliceerde studies binnen de geriatrische oncologie was
het zonde om met iets nieuws te beginnen. Ik was die dag voor het eerst getuige van jouw
creativiteit en indrukwekkende vermogen om vage ideeën om te zetten in concrete
onderzoeksvoorstellen: binnen een paar minuten had ik een blaadje vol met plannen. Het
duurde even voordat onze wederzijdse verwachtingen over de invulling van onze
samenwerking op één lijn zaten maar we zijn een goed team geworden. Heel leuk dat ik je
p de valreep als promotor mag noteren! o
Barbara van Munster – wat ben ik blij dat jij je aan mij hebt opgedrongen! Dank je wel
voor al je steun, vertrouwen en begeleiding, voor je uitleg over de politiek van het
publiceren en vooral voor je kritische blik. Jouw vermogen om de vinger te leggen op de
zwakke plekken in mijn plannen en artikelen is de kwaliteit van dit proefschrift en van mij
als onderzoeker zeer ten goede gekomen. Uiteindelijk kregen we er een “methodologically
236

Acknowledgements (Dankwoord)
impeccable” van een reviewer voor terug, een compliment dat vooral jou toekomt. Er
ggen nog diverse plannen op de plank en ik verheug mij op onze verdere samenwerking. li
Professor Marcel Levi – dank u wel dat u deze promotie mogelijk heeft gemaakt. Hoewel
uw naamverbintenis met dit proefschrift aanvankelijk vooral praktische redenen had,
realiseerde ik mij pas later hoe betrokken u bent bij de discussie over (te lang)
doorbehandelen vs onderbehandelen. Ik verheug mij erop die discussie op 30 november
oort te zetten. v
Ik wil graag alle leden van de leescommissie hartelijk bedanken voor hun bereidheid dit
anuscript inhoudelijk te beoordelen en te opponeren. m
Bij het opstellen van een lijstje met mede‐auteurs besefte ik mij pas met hoeveel
verschillende mensen ik heb mogen werken: het bleken er uiteindelijk 44 te zijn! Allemaal
heel veel dank voor de prettige samenwerking. In het bijzonder wil ik noemen: Judith
Jonker, oud‐collega, sparring partner, mede‐auteur en vriendin: het is leuk hoe we al deze
aspecten hebben weten te combineren. Dat er nog vele gezellige etentjes, onderzoeks‐
projecten en nieuwe inzichten mogen volgen! Esther Bastiaannet, ik kon aanvankelijk
moeilijk geloven dat iemand zo zonder dubbele agenda wetenschap kon bedrijven. Het
was me een waar genoegen om met je samen te werken en ideeën uit te wisselen. To be
continued...? Alinda Vos: wat heb jij hard gewerkt voor die review, daar kan ik je niet
genoeg voor bedanken. Je bent een groot talent en ik ben heel benieuwd waar dat
allemaal toe gaat leiden. Johanneke Portielje, ik hoop op nog vele stevige, vruchtbare
discussies en samenwerkingsprojecten binnen en buiten GeriOnNe. Ook wil ik Bianca
Buurman en alle medewerkers van de DEFENCE studie bedanken voor het mogen
gebruiken van hun data, evenals Caroline Seynaeve, Elise van Leeuwen, Harm van
interen, Steffen de Groot en alle medewerkers van de OMEGA studie. T
Ja
n Willem Broek – heel veel dank voor de prachtige lay‐out! Ben er superblij mee.
Voor alle leden van de special interest group Geriatrische Oncologie: het ontwikkelen van
een geriatrische visie op oncologische zorg en deze naar buiten brengen blijkt niet altijd
eenvoudig maar samen staan we sterk! Het is elke keer weer leuker om daarover van
gedachten te wisselen. Dank daarvoor, en dank ook voor jullie input bij de review over de
voorspellende waarde van het CGA. Dr. Huub Maas – als partner‐in‐crime in de
geriatrische oncologie ben je steeds aan de zijlijn aanwezig geweest. Dank je wel voor het
geven van het goede voorbeeld! Ons artikel is er niet echt van gekomen dus bij deze nog
237

Acknowledgements (Dankwoord)
maar eens een porretje. Truus Schuurman – in 2003 was jij als mijn zaalsupervisor in het
Slotervaartziekenhuis het bewijs dat een pittig karakter en hoge hakken prima samengaan
met de zorg voor kwetsbare ouderen. Ik vind het heel leuk dat wij elkaar nu via de SIG
eer tegen zijn gekomen. w
Dr. Victor Umans – zonder de stimulans om (toch enigszins tegen mijn zin) in 2006 met dat
case‐report over het Eisenmenger syndroom aan de slag te gaan, waren mijn
wetenschappelijke ambities waarschijnlijk in hun winterslaap verzonken gebleven.
Grappend zei ik toen dat als er ooit een proefschrift zou komen u een eervolle vermelding
verdiende maar ik denk niet dat één van ons in die mogelijkheid geloofde. Bij dezen wil ik
nogmaals heel hartelijk danken voor dat zetje richting onderzoek. u
Mijn (oud)collega’s uit het Medisch Centrum Alkmaar en het AMC: het was fijn om altijd
gezelligheid te vinden als ik langskwam voor een afspraak of om statussen in te zien. Dank
wel daarvoor! je
Dan al mijn collega’s in het Diakonessenhuis: wat heb ik het getroffen! Prettige collega’s,
goede sfeer, een geweldig team om in te werken… Wat wil een mens nog meer? Richard
Faaij, ik heb veel respect voor de ruimte die jij mij het gegeven om me te bemoeien met
“jouw kindje”. Dank je wel voor al je flexibiliteit die het voortzetten van mijn
promotietraject mogelijk heeft gemaakt. Meike Prins, ooit mijn coassistent, toen
vriendinnen geworden, nu mijn collega en wie weet volgend jaar ook mijn maat: ik
verheug mij bijzonder op onze samenwerking in het uitbouwen van ons geriatrisch
centrum midden‐Nederland. Peter Thunnissen, René van der Griend en Daan ten Bokkel
Huinink: doen jullie mee? Frans Boerenboom, Bas van Tuyl en Apollo Pronk: op het
snijvlak van jullie specialismen en het mijne ligt een goudmijn aan onderzoeksvragen. Ik
verheug mij op de kans om dit samen verder te verkennen. Femke Meulendijks, Patricia
Hamers, Lizelot(t)e van Beek: heel leuk om het stokje nu aan jullie door te geven! Rob
Gallas, jij verdient een speciale vermelding: jouw overtuiging dat het voor mij niet
haalbaar zou zijn om starten als vrijgevestigde te combineren met promotieonderzoek, is
uitermate prikkelend geweest en mijn wens jouw ongelijk te bewijzen heeft mij door
eerdere moedeloze momenten heen geholpen. m
Bij de verdediging van mijn proefschrift word ik bijgestaan door mijn paranimfen: Nadine
Vieleers en Karen Farrington. Lieve Nadine – het was geen vriendschap op het eerste
gezicht toen wij elkaar ontmoeten tijdens de introductieweek van geneeskunde in 1996.
Gelukkig bleken onze cultuurverschillen prima overbrugbaar door een
gemeenschappelijke interesse in reality series en ATWT en je bent een van mijn beste
238

Acknowledgements (Dankwoord)
239
vriendinnen geworden. Het blijft voor mij bijzonder dat jij lang voordat ik het wilde horen
al besloten had dat geriatrie het beste bij mij paste. Ik geloof nog steeds niet dat ik daar
zelf ooit aan gedacht zou hebben. Zonder jou was er voor mij geen geriatrie geweest en
dus ook geen geriatrische oncologie: dat alleen zou reden genoeg zijn geweest om je te
vragen mijn paranimf te zijn… Lieve Karen – in gedachten zie ik ons nog zitten (eind 1995)
bij jou op de bank, papieren op schoot, rode pen in de hand, geconcentreerde
(gepijnigde?) blik, krassend in elkaars werkstukken. Elke drie weken moesten wij vijf
A4tjes volschrijven over een antropologisch boek en dus hebben we heel wat keren zo
gezeten. Samen met jou leerde ik de lol van het schrijven en aangezien onze docent vooral
keek naar het uiterlijk van het werkstuk, verdien jij veel van de eer van alles wat ik toen
geleerd heb. Om die reden, en alles wat we in de 17 jaar vriendschap erna hebben
gedeeld, wilde ik graag dat jij mijn paranimf zou zijn. Dank jullie beiden voor jullie
riendschap en steun, en natuurlijk ook de hulp bij het maken van de stellingen. v
Twee andere vriendinnen mogen hier niet ontbreken: Karien Hoogenboezem – in alle
drukte van opleiding, stages, onderzoek en werk ben jij met je gezin al vele jaren het
rustpunt. Na zo’n weekje kletsen, spelletjes spelen en knuffelen met mijn neefjes kan ik
weer met nieuwe energie aan de slag. Het is heerlijk een plek te hebben waar ik mij zo
welkom weet. Anneke Geel – it’s so great to have my friend of over 25 years here for this
occasion. Thank you so much for coming! I just realized that the day of my defense will be
the first time that all four of my oldest friends are together in one place. Makes the day
xtra special… e
Voor mijn ouders: jullie zijn een prachtig bewijs dat leeftijd niets zegt over hoe oud je
bent. Dank je wel voor alles wat jullie me hebben meegegeven. Het voelt goed om te
weten dat ik altijd op jullie kan rekenen. En natuurlijk ook bedankt voor de hulp met de
Nederlandse samenvatting. Jasper, het was zo fijn op te groeien met iemand zoals jij als
grote broer. Dat zou ik ieder meisje gunnen. Lief dat je vanuit Lagos komt om erbij te zijn.
_ _ _ _ _ _
Een promotie lijkt een afsluiting. Dat is het ook wel, natuurlijk. Maar er liggen nog zoveel
onbeantwoorde vragen … Hoe meer we kunnen, des te prangender wordt de vraag of we
dat ook moeten inzetten, en zo ja, wanneer en bij wie. Alle reden voor mij om door te
gaan met onderzoek. Wie doet er mee?
