debate advances in hf ofili
TRANSCRIPT

Advances in Heart Failure For African Americans:
Paradigm Shift or Paradigm Drift?
Elizabeth O. Ofili, MD, MPH, FACC
Professor of Medicine (Cardiology)
Senior Associate Dean, Clinical and Translational Research
Director, Clinical Research Center
Morehouse School of Medicine
Atlanta, Georgia
Email: [email protected]

ATLANTA UNIVERSITY CENTER
combined faculty of ~ 1000 with a student enrollment
of over 10,000, from across the US and over 50 countries

I N S T I T U T E O F M E D I C I N E (IOM)
Shaping the Future for Health
National Academy of Sciences; 2002. http://www.nap.edu/catalog/10260.html

Health Disparities
A health disparity is a difference in health outcomes across subgroups
of the population. Health disparities are often linked to social, economic,
or environmental disadvantages (e.g., less access to good jobs, unsafe
neighborhoods, lack of affordable transportation options).
Health disparities adversely affect groups of people who have
systematically experienced greater obstacles to health on the basis of
their racial or ethnic group, religion, socioeconomic status, gender, age,
mental health, cognitive, sensory, or physical disability, sexual
orientation or gender identity, geographic location, or other
characteristics historically linked to discrimination or exclusion.
“Of all the forms of inequality, injustice in health care is the most shocking and inhumane.” Martin Luther
King, Jr
“Missing Persons: Minorities in the Health Professions” Louis Sullivan, President Emeritus Morehouse
School of Medicine, 17th Secretary, US Department of Health and Human Services
“What If We Were Equal?” “ If we closed the Black-White Mortality Gap, over 83,000 dealths per year will
be eliminated” David Satcher, 16th US Surgeon General; Past President, Morehouse School of Medicine

What is Health Equity
Healthy People 2020 defines health equity as "attainment of the highest level of health for all people. Achieving health equity requires valuing everyone equally with focused and ongoing societal efforts to address avoidable inequalities, historical and contemporary injustices, and the elimination of health and health care disparities."
Achieving health equity requires valuing everyone equally with focused and ongoing societal efforts to address avoidable inequalities, historical and contemporary injustices, . . .
. . . To eliminate health and health care disparities and attain the highest level of health for all people.“
Equality vs. Equity

Heart Failure Disparities in
African American Patients
• The Prevalence of HF is higher in African Americans than in Caucasians
• HF has a more malignant natural history in African American patients
– Occurs at an earlier age1
– Associated with more advanced left ventricular disease at diagnosis1
• Differing etiology in African Americans
– More likely to be associated with a history of hypertension1
– Incidence of myocardial infarct is consistently lower1
• Worse prognosis in African Americans
– Higher rate of hospitalization than in Caucasian patients2
– Higher mortality rate than in Caucasians2
1. Yancy CW. J Card Fail. 2000;6:183-186.
2. Yancy CW. J Card Fail. 2003;9:S210-S215.

Modifiable risk
factors
Hypertension, diabetes, obesity, LVH, smoking, and chronic
kidney disease are more common in AAs
Neurohormonal
imbalances
and endothelial
dysfunction
Derangements in the renin-angiotensin-aldosterone and
adrenergic axes as well as impaired endothelial function
are more common in AAs
Genetic
polymorphisms
Racial disparity may be the result of several polymorphisms
associated with the risk of HF (beta 1 adrenergic receptor,
alpha 2c receptor, aldosterone synthase, G protein,
transforming growth factor beta, nitric oxide [NO] synthase,
and transthyretin)
Socioeconomic
factors and quality of
care
Low socioeconomic status and discrimination from health
care providers serve as barriers to attaining treatment goals
in AAs
Why Are African Americans More at Risk for
Heart Failure? • Mechanism of HF and responses to pharmacologic therapy among AAs may
differ from those among other races1-3
1. Bahrami H, Kronmal R, Bluemke DA, et al. Differences in the incidence of congestive heart failure by ethnicity: the multi-ethnic study of atherosclerosis. Arch Intern Med. 2008;168(19):2138-2145.
2. Yancy CW. Heart failure in African Americans: unique etiology and pharmacologic treatment responses. J Natl Med Assoc. 2003;95(1):1-9.
3. Yancy CW. Heart failure in African Americans: a cardiovascular enigma. J Card Fail. 2000;6(3):183-186. 4. Sharma A, Colvin-Adams M, Yancy CW. Heart failure in African Americans:
Disparities can be overcome. Cleve Clin J Med. 2014;81(5):301-311.
Sourced from Sharma A, Colvin-Adams M, Yancy CW.. Heart failure in African Americans: Disparities can be overcome. Cleve Clin J Med. 2014;81(5):301-311.4

Heart Failure is Associated with
Neurohormonal Excess and Nitric Oxide
Insufficiency
Endothelial Nitric Oxide Neurohormones
Neurohormonal Antagonists
• Beta Blockers
• Renin-Angiotensin Antagonists
• Aldosterone Blockers
Nitric Oxide Enhancment (NOE)
• Fixed-dose combination ISDN/HYD
• Omapatrilat ( Dual ACE and NEP inh)
• Angiotensin-Neprilysin Anatagonist


N=1050
Fixed-dose I/H 518 463 407 359 313 251 13
Placebo 532 466 401 340 285 232 24
Taylor AL et al. N Engl J Med. 2004;351:2049-2057.
Days Since Baseline Visit Date
A-HeFT: All-Cause Mortality
0 100 200 300 400 500 600 85
90
95
100 S
urvi
val (
%)
P=0.01
Fixed Dose Isosorbide/Hydralazine
Placebo
Hazard ratio=0.57 43% Decrease
Primary Efficacy Endpoint – Composite score: All-Cause Mortality;
First HF Hospitalization; Change in QoL at 6 months relative to baseline

n=32
6.2
All-Cause
Mortality (%)
P=0.012
Placebo + Standard Therapies FDC I/H + Standard Therapies
First HF
Hospitalization (%)
P<0.001 P<0.01
Patient Reported
Functional Status
n=130
24.4 10.2
n=54
10
30
20
-8
0
0
15
10
5 16.4
n=85
n=532
n=518 -4
-2
-6
Taylor AL et al. N Engl J Med. 2004;351:2052.
AHeFT: Trial Summary N=1050
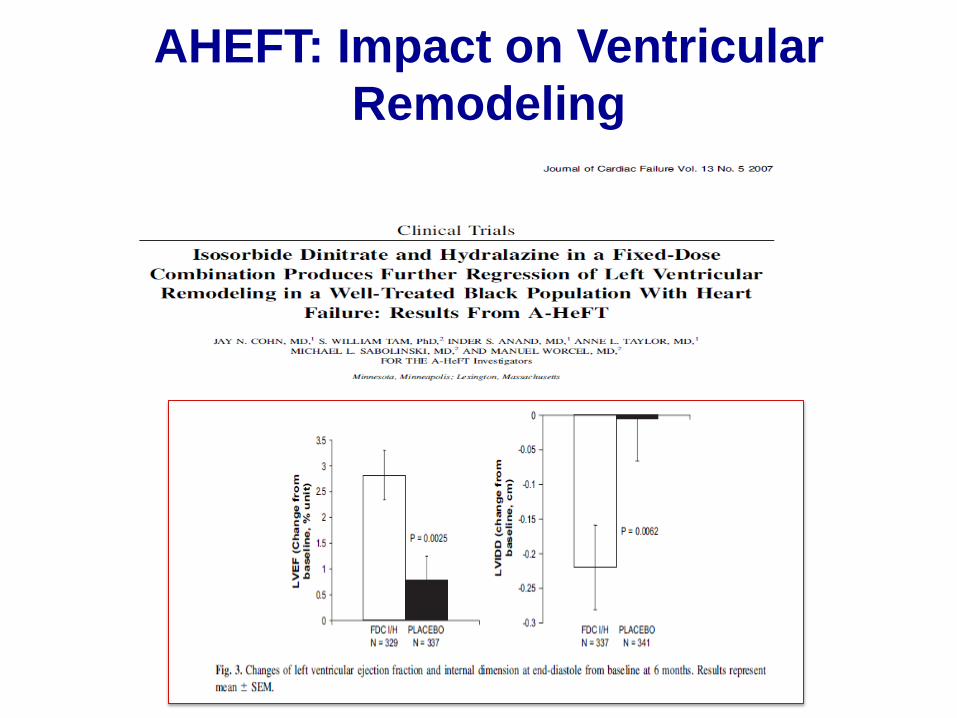
AHEFT: Impact on Ventricular
Remodeling

2013 ACC/AHA Guideline: HYD and ISDN
The combination of HYD and ISDN is
recommended for African Americans with
NYHA class III–IV HFrEF on GDMT – IA
A combination of HYD and ISDN can be
useful with HFrEF who cannot be given ACE-
Is or ARBs – IIa B
Yancy CW et al. J Am Coll Cardiol. 2013:62:e147-e239.

Ten Years After AHEFT: Have We
Advanced Health Equity?

Any degree of uncertainty a physician may have
relative to the condition of a patient can contr ibute
to disparities in treatment.
Smedley B. et al, IOM March 2002
McMur ray J. et al NEJM 2014;371(11):993-1004

0
16
32
40
24
8
Enalapril (n=4212)
360 720 1080 0 180 540 900 1260
Days After Randomization
4187
4212
3922
3883
3663
3579
3018
2922
2257
2123
1544
1488
896
853
249
236
LCZ696
Enalapril
Patients at Risk
1117
Kap
lan
-Meie
r E
sti
mate
of
Cu
mu
lati
ve R
ate
s (
%)
914
LCZ696 (n=4187)
PARADIGM-HF: Cardiovascular Death or Heart Failure Hospitalization (Primary Endpoint)
HR = 0.80 (0.73-0.87)
P = 0.0000002
Packer M., et al. For PARADIGM Investigators

LCZ696 (n=4187)
Enalapril (n=4212)
P Value
Prospectively identified adverse events
Symptomatic hypotension 588 388 < 0.001
Serum potassium > 6.0 mmol/l 181 236 0.007
Serum creatinine ≥ 2.5 mg/dl 139 188 0.007
Cough 474 601 < 0.001
Discontinuation for adverse event 449 516 0.02
Discontinuation for hypotension 36 29 NS
Discontinuation for hyperkalemia 11 15 NS
Discontinuation for renal
impairment 29 59 0.001
Angioedema (adjudicated)
Medications, no hospitalization 16 9 NS
Hospitalized; no airway
compromise 3 1 NS
Airway compromise 0 0 ----
PARADIGM-HF: Adverse Events Commentary: The trial randomized only patients who successfully completed a single-blind run-in phase consisting of enalapril for two weeks
and then LCZ699 for twice that long—all after being stable for at least a month on either an ACE inhibitor or
angiotensin-receptor blocker (ARB). Of the 10 521 entering the run-in phase, >2000 dropped out, mostly because they couldn't
tolerate one of the two agents, often because of hypotension
Packer M., et al. For PARADIGM Investigators

Paradigm
Shifts in
Heart-Failure
Therapy — A
Timeline
Sacks et al
NEJM;
September 11,
2014 Vol. 371
No. 11

Dr Lynne Warner Stevenson(Boston MA): "I don't believe it is time [for ARNIs] to
replace ACE inhibitors or ARBs," given all the patients who didn't tolerate the drug
or didn't meet the inclusion criteria”
"The advent of LCZ[696] enriches our respect for the complexity of our patients'
individual responses. I'm not really sure which actions of ACE inhibitors are the
most important for which patients. I'm not [even] sure which actions of beta-
blockers are most important for which patients. And I'm certainly not sure of all the
hormones affected by LCZ[696] or which are going to be the most important for
each patient. These results should inspire us to do new research on these
kinds of individual responses and the challenge of optimizing our therapies
in patient-centered ways,”
"I don't think that LCZ[696] is ready for a level I indication; that is a higher bar,”
Dr John Cleland( London, UK): “Eight thousand patients is a lot, but not enough
to answer every question about the new agent; We are going to need more clinical
trials.”
PARADIGM-HF at HFSA Sessions: September 25, 2014
MEDSCAPE-News from the: Heart Failure Society of America (HFSA) 18th Annual Scientific Meeting

September 11, 2014; 371:1062-1064

Advances in Heart Failure For African
Americans: Paradigm Shift or Paradigm Drift? • A decade after the landmark AHEFT Trial, African American
patients are not receiving guideline based medical therapy
• Clinical trials of novel heart failure therapies should integrate guideline based therapies across ALL demographic groups of heart failure patients, including African Americans
Advancing heart failure treatment for African American patients requires a Paradigm shift to advance health equity
Ofili2015

Equality vs. Equity in Heart Failure Care ONE size for ALL Clinical trials Without Race/Ethnicity impact on efficacy/ side effects
Right size Clinical trial of novel drug incorporate evidence based Background therapy

Thank you!!!!
www.msm.edu
Mission: Leading the Creation and Advancement of Health Equity #1 in Social Mission among US medical schools (Annals of Internal
Medicine, June 2010) Announcing: Association of Black Cardiologists/Morehouse School of Medicine Cardiovascular Disease Registry