dear fda survey participant - cloud object storage | store ... · 18/05/2016 · dear fda survey...
TRANSCRIPT
Dear FDA Survey Participant:
Thank you so much for sharing your perspective on the FDA’s interactions with drug
sponsors. Expertise like yours is key to the success of this survey initiative, and your
feedback will provide a vital window into how sponsors view the FDA.
As you know, PDUFA 6 negotiations took place this past fall, and the data from this survey
allowed BIO’s negotiators to share with FDA the real world experiences and opinions of drug
sponsors. Last fall’s negotiations kicked off a months-long process that will culminate with
the legislative reauthorization of PDUFA before it expires in 2017. Communications between
FDA and drug sponsors will be a key focus of PDUFA 6, and the data and commentary from
our FDA survey will enhance BIO’s efforts to support an effective 21st century FDA.
This report provides you, and the FDA, with an interim survey analysis based on our April 15
data pull. In order to keep you informed, we have included in this report a data slide deck
as well as an analysis of participants’ open-end responses.
UPCOMING EVENTS
Webinar: BIO is hosting a webinar on May 18 to reveal the interim results of the
survey. The webinar will also feature a presentation from CDER staff on
FDA’s recent Draft Guidance on Best Practices for Communication Between
IND Sponsors and FDA During Drug Development.
Data Pull: We will be conducting another data pull before the end of this year. We will
also periodically check in on the data as we remain engaged with the FDA and
Congress in the run-up to PDUFA reauthorization. You can continue to share
your experiences at fdasurvey.bio.org.
CALL TO ACTION
As your clinical programs move through the development process, I would like to encourage
you to continue providing feedback in order to help us better identify what is working and
where improvements are needed at the FDA. You can add new clinical programs and
phase-specific journals at any time, and you can always log-in to update program and
journals already in the system. Your input will allow us to better compare differences
between Centers and Review Divisions and effect change at the FDA.
Thank you again for your participation!
Sincerely,
E. Cartier Esham, Ph.D.
Executive Vice President, Emerging Companies
BIO

TABLE OF CONTENTS
OVERVIEW OF INTERIM FINDINGS
Executive Summary of Interim Findings 5
Slide Presentation – Interim Findings Based on August 2015 Data Pull 8
COMPARISON OF PERFORMANCE RATINGS BETWEEN
CENTERS & REVIEW DIVISIONS
Slide Presentation – Summary Charts: Center/Division Ratings 23
CDER 29
CDER Division of Oncology Products 33
CDER Division of Neurology Products 36
CDER Division of Hematology Products 39
CDER Division of Metabolism and Endocrinology Products 42
CDER Division of Gastroenterology and Inborn Error Products 45
CBER & CBER Division of Cellular and Gene Therapies 48
CDRH: Preliminary Results 53
APPENDICES: COMPREHENSIVE LIST OF ADDITIONAL COMMENTS
Appendix 1: CDER 57
Appendix 2: CBER 76
Appendix 3: CDER Division of Oncology Products 81
Appendix 4: CDER Division of Neurology Products 86
Appendix 5: CDER Division of Hematology Products 92
Appendix 6: CDER Division of Metabolism and Endocrinology Products 95
Appendix 7: CDER Division of Gastroenterology and Inborn Error Products 100
Appendix 8: CDRH 104
OVERVIEW OF
INTERIM FINDINGS

Executive Summary of Interim Findings SUMMARY OF PARTICIPATION Since launching the survey tool in August 2014, we have steadily increased participation numbers. Currently, we have:
433 users (survey participants registered) representing 295 companies 436 programs (descriptive information for individual clinical development programs) 451 journals (information about FDA/sponsor interactions for individual clinical
development programs during each stage of development) We have excellent representation from emerging, mid-sized, and large biopharmaceutical companies across all stages of development and review divisions. Currently, we have the most representation from programs under review by the following divisions:
CDER Division of Oncology Products (20%) CDER Division of Neurology Products (11%) CDER Division of Gastroenterology and Inborn Error Products (9%) CBER Division of Cellular and Gene Therapies (8%) CDER Division of Metabolism and Endocrinology Products (8%) CDER Division of Hematology Products (7%)
Throughout the survey, participants are asked to provide detailed feedback on their interactions with the FDA via phase-specific program journals. These journals are available for each phase of development through which a program passes on its way toward NDA/BLA submission. Currently, we have the most phase-specific feedback from clinical program journals from the following review divisions:
CDER Division of Oncology Products (20%) CDER Division of Neurology Products (15%) CDER Division of Hematology Products (9%) CDER Division of Metabolism and Endocrinology Products (7%) CDER Division of Gastroenterology and Inborn Error Products (7%) CBER Division of Cellular and Gene Therapies (6%)
SUMMARY OF KEY FINDINGS Overall Communications
Approximately half of the survey participants rated their interactions with FDA as Very Beneficial and half indicated that there was room for improvement.
o These ratings were consistent across each stage of clinical development. CBER had a higher percentage of participants that rated their overall communications
with FDA as Very Beneficial (60%), as compared to CDER (47%). The Division of Oncology Products was the most represented Division overall, and it
tied with the Division of Hematology Products for the highest ratings for overall communications of any Review Division (54% Very Beneficial).
The Division of Cellular and Gene Therapies was the most represented CBER Division and had the 3rd highest ratings for overall communications of any Review Division (50% Very Beneficial).
Among the top 5 CDER Divisions represented, the Division of Oncology Products and the Division of Hematology Products had the highest ratings for overall communications (54% Very Beneficial). No survey participant rated either Division as Not At All Beneficial.
5

Among the top 5 CDER Divisions represented, the Division of Gastroenterology and Inborn Error Products had the highest percentage of respondents rating overall communications as Not At All Beneficial (12%) and tied for the highest percentage reporting Not Very Beneficial overall communications with the Division of Metabolism and Endocrinology Products (19%).
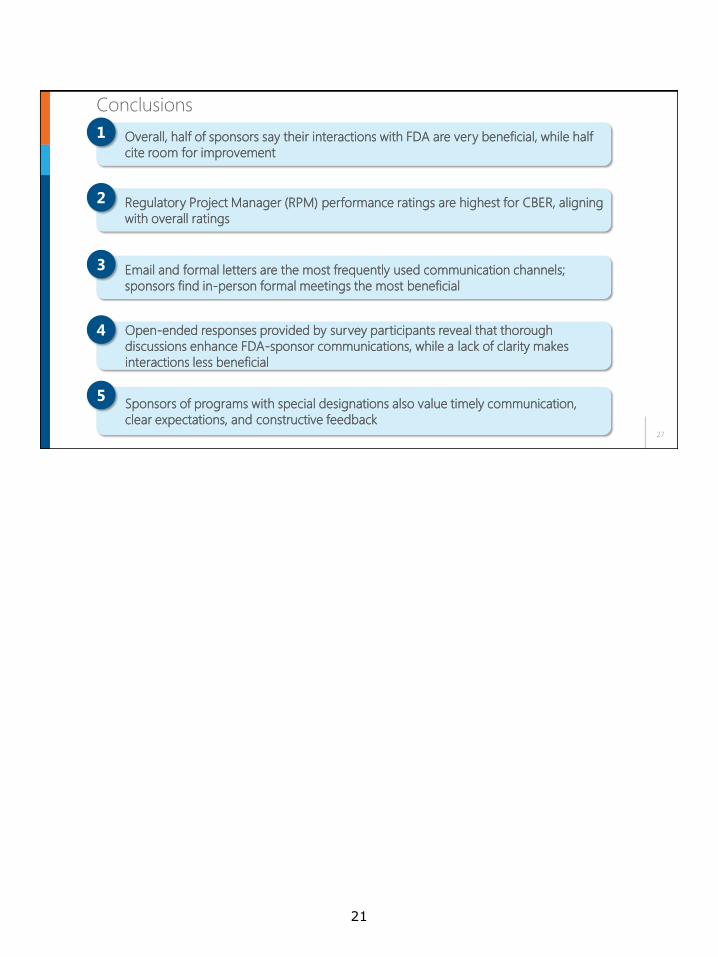
Ratings of overall communications for Orphan Drug clinical programs (49% Very Beneficial) were very similar to the ratings for all clinical programs (48% Very Beneficial).
Regulatory Project Manager
CBER had a higher percentage of participants that rated their interactions with their Regulatory Project Manager (RPM) as Very Beneficial (70%), as compared to CDER (53%).
The Division of Cellular and Gene Therapies had the highest RPM ratings across all Divisions (69% Very Beneficial). Among the top 5 CDER Divisions represented, the Division of Oncology Products had the highest RPM ratings (60% Very Beneficial).
The Division of Neurology Products had the lowest percentage of respondents rate their interactions with their RPM as Very Beneficial (43%). The Neurology Division also had the highest percentage of respondents rating their RPM interactions as Not At All Beneficial (2%).
Ratings of interactions with RPMs for Orphan Drug clinical programs (57% Very Beneficial) were similar to the ratings for all clinical programs (54% Very Beneficial).
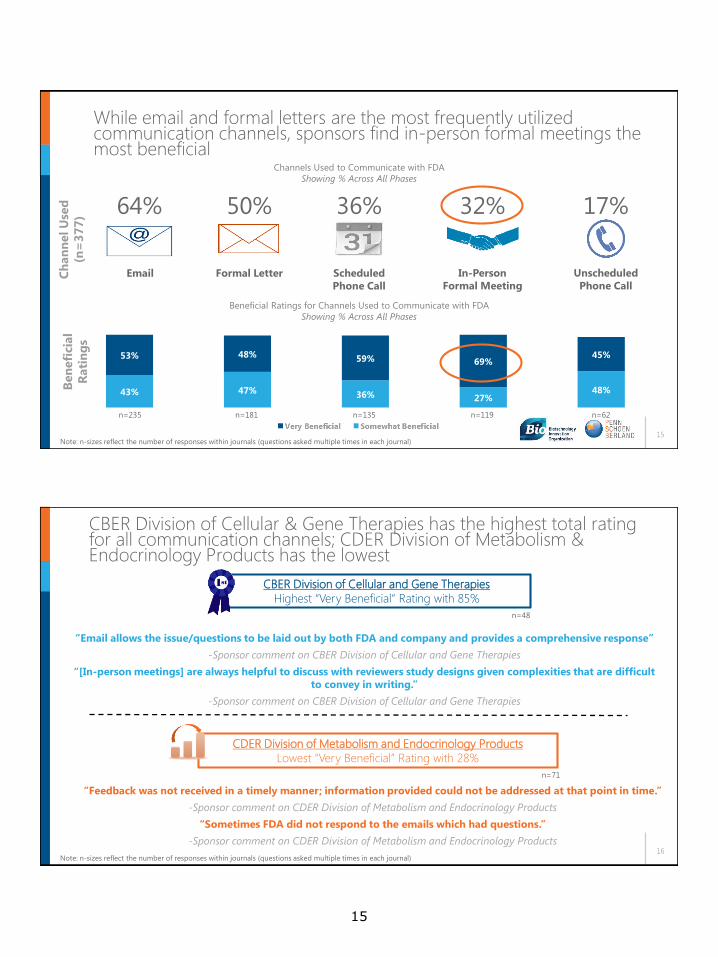
Communication Channels and Issue Resolution Email and formal letters are the most frequently used forms of communication, but
in-person formal meetings are rated by far the most beneficial. In-person formal meetings had the highest performance ratings (69% Very Beneficial), as compared to 53% Very Beneficial for emails and 48% Very Beneficial for formal letters.
o The Division of Oncology Products had the highest combined performance ratings for all formal meetings (Type B, Type C, and other in-person formal meetings), with 78% of respondents rating these meetings Very Beneficial.
CBER had a significantly higher percentage of responses rating utilization of communication channels as Very Beneficial (83%), as compared to CDER (52%).
The Division of Cellular and Gene Therapies had the highest percentage of responses rating utilization of communication channels as Very Beneficial (85%) among the top Review Divisions represented. The Division of Gastroenterology and Inborn Error Products had the highest percentage of responses rating utilization of communication channels as Not At All Beneficial (9%).
Among the top 5 CDER Divisions represented, the Division of Oncology Products had the highest number of responses rating utilization of communication channels as Very Beneficial (60%).
While clinical programs that had an Orphan Drug designation did not differ much from the overall communications ratings for all programs, they did have a higher percentage of responses that rated utilization of communication channels as Very Beneficial (67% vs. 55%).
The most frequently used comments that supported Very Beneficial ratings for communication channels cited interactions that were thorough, helpful, constructive, timely, and collaborative. Additionally, effective use of multiple communication channels to resolve issues in an effective and timely manner was consistently cited as a reason for high performance ratings (e.g., follow up phone calls after an in-person meeting).
o Survey participants reporting they had meetings with the FDA in advance of an upcoming phase of development had noticeably higher percentages
6

ranking their overall communications with FDA as Very Beneficial during that phase.
The most frequent comments citing areas for improvement were the need to improve clarity as well as an inability to obtain and/or delays in obtaining responses to specific questions. Additionally, inconsistent feedback and inability to engage in scientific dialogue to resolve issues were consistently cited as reasons for low performance ratings.
7

1
WIN N IN G K N OWLEDGET M
WIN N IN G K N OWLEDGET M
OVERVIEW OF INTERIM FINDINGS
Based on data as of April 2016
FDA/Sponsor Interactions During Drug DevelopmentMay 18, 2016
2
295
Companies
433
Users
436
Programs
451
Journals
Current Participation
• Companies refers to the number of companies participating in the study
• Users are the participants from all the various companies involved in the study
• Some companies have multiple users (different people or divisions) and some users have multiple
programs
• Programs correspond to a user's product(s) in clinical development
• Journals for programs provide information on interactions with FDA during a specific phase of development
8

3
63%11%
6%
2% 17%
Company Size
100 employees or fewer
101-250 employees
251-500 employees
501-1000 employees
>1000 employees
Companies of all sizes and phases of development are
represented
128
114 111
98
Pre-IND Phase 1 Phase 2 Phase 3
Journal Participation
Journals
18%
23%
25%
24%
10%
Current Phase of Programs
Pre-IND
Phase 1
Phase 2
Phase 3
NDA/BLA pending submission
n=434 programs
• 77% of programs are NMEs
• Both NDAs (54%) and BLAs (40%) program applications are represented
n=175 companiesn=451 journals
4
20%
11%
9%
8%8%7%
37%
CDER Division of Oncology Products
CDER Division of Neurology Products
CDER Division of Gastroenterology and
Inborn Error Products
CBER Division of Cellular and Gene
Therapies
CDER Division of Metabolism and
Endocrinology Products
CDER Division of Hematology Products
Other Divisions
A broad mix of review divisions is represented in the study
n=407* programs
20%
15%
7%6%7%
9%
36%
Programs by Review Division
Showing % Out of All Programs
Note: Some n-sizes in the following slides are small, and should be taken directionally, and some anecdotally.
Journals by Review Division
Showing % Out of All Journals
n=451 journals
Other Divisions:
CBER Division of Bacterial, Parasitic, and Allergenic Products
CBER Division of Blood Applications
CBER Division of Hematology
CBER Division of Human Tissues
CBER Division of Vaccines and Related Product Applications
CBER Division of Viral Products
CDER Division of Anesthesia, Analgesia, and Addiction Products
CDER Division of Anti-Infective Products
CDER Division of Anti-Viral Products
CDER Division of Bone, Reproductive, and Urologic Products
CDER Division of Cardiovascular and Renal Products
CDER Division of Dermatology and Dental Products
CDER Division of Medical Imaging Products
CDER Division of Psychiatry Products
CDER Division of Pulmonary, Allergy, and Rheumatology Products
CDER Division of Transplant and Ophthalmology Products
CDRH Office of Device Evaluation
CDRH Office of In Vitro Diagnostics and Radiological Health
n=433 programs
87
49
38
36
34
30
Number of Programs Participating
159
9

5
Key Findings and
Supporting Data
6
Key Findings
Overall, half of sponsors say their interactions with FDA are very beneficial, while half
cite room for improvement
Regulatory Project Manager (RPM) performance ratings are highest for CBER, aligning
with overall ratings
Open-ended responses provided by survey participants reveal that thorough
discussions enhance FDA-sponsor communications, while a lack of clarity makes
interactions less beneficial
1
2
4
Email and formal letters are the most frequently used communication channels;
sponsors find in-person formal meetings the most beneficial
3
Sponsors of programs with special designations also value timely communication,
clear expectations, and constructive feedback
5
10

7
Overall, half of sponsors say their interactions
with FDA are very beneficial, while half cite
room for improvement
● This trend is evident across CBER, CDER, and CDRH and
among the top 6 review divisions
○ CBER has the highest Very Beneficial rating (60%)
○ CDER Division of Oncology Products and CDER
Division of Hematology Products have the highest
Very Beneficial rating (54%)
○ CDER Division of Neurology Products has the lowest
Very Beneficial rating (33%)
1
8
Half of sponsors rate overall interactions with FDA as Very
Beneficial; half see room for improvement
4% 5% 3% 3% 3%7% 7% 6%
10%6%
41%34% 44%
46%
42%
48%53%
48%41%
49%
Total
(n=397)
Pre-IND
(n=111)
Phase 1
(n=108)
Phase 2
(n=92)
Phase 3
(n=86)
How would you rate your overall interactions with FDA during the <phase> stage?
Very Beneficial
Somewhat Beneficial
Not Very Beneficial
Not at all Benefical
Room to
improve
Note: n-sizes reflect the number of journals
11

9
CBER has higher overall performance ratings than CDER
4%5%7% 12%
35%
41%47%
60%47%
41%
CBER
(n=43)
CDER
(n=350)
CDRH
(n=17)
How would you rate your overall interactions with FDA during the <phase> stage?
Showing % Across All Phases
Very Beneficial
Somewhat Beneficial
Not Very Beneficial
Not at all Benefical
Note: n-sizes reflect the number of journals
The feedback on CBER is more positive than CDER (i.e., more “Very Beneficial”
ratings), albeit on a smaller sample of CBER respondents
10
CDER Division of Oncology Products and CDER Division of Hematology Products have the highest performance ratings
12%5%4% 8% 5%
19%
19%
5%
42% 38% 45%
37%
31%
57%
54% 54% 50%44%
38% 33%
CDER Division of
Oncology Products
(n=83)
CDER Division of
Hematology Products
(n=37)
CBER Division of
Cellular and Gene
Therapies
(n=22)
CDER Division of
Metabolism and
Endocrinology
(n=27)
CDER Division of
Gastroenterology and
Inborn Error Products
(n=26)
CDER Division of
Neurology Products
(n=58)
How would you rate your overall interactions with FDA during the <phase> stage?
Showing % Across All Phases
Very Beneficial
Somewhat Beneficial
Not Very Beneficial
Not at all Benefical
Note: n-sizes reflect the number of journals
12

11
Regulatory Project Manager (RPM)
performance ratings are highest for CBER,
aligning with overall ratings
● CBER Division of Cellular and Gene Therapies has the
highest RPM performance rating (69% Very Beneficial)
● CDER Division of Neurology has the lowest RPM
rating of the top 6, with only 43% saying Very
Beneficial
2
12
RPM ratings are highest for CBER, aligning with overall ratings
1%8%4%
5%
26%
41%42%
70%
53% 50%
CBER
(n=23)
CDER
(n=222)
CDRH
(n=12)
Very
Beneficial
Somewhat
Beneficial
Not Very
Beneficial
Not at all
Benefical
How would you rate your interactions with your FDA Regulatory Project Manager?
Showing % Across All Phases
Note: n-sizes reflect the number of journals
CBER Division of Cellular
and Gene Therapies had
the highest RPM rating
(69% Very Beneficial)
Of the top 6 review
divisions, CDER Division of
Neurology has the most
room to improve for RPM
rating with only 43% saying
Very Beneficial
13

13
RPMs are generally well-rated and sponsors value RPM responsiveness, but there is still room for improvement in timeliness and experience
“The regulatory project manager was able to provide information or direct contact with the appropriate
FDA review team members to address any questions or issues.”
-Sponsor comment on CBER Division of Cellular and Gene Therapies
“The project manager is very responsive to emails and phone calls.”
-Sponsor comment on CDER Division of Neurology Products
“Clear and timely communications.”
-Sponsor comment on CDER Division of Oncology Products
“Getting a timely response from FDA RPMs to email or phone contacts has become a significant problem.”
-Sponsor comment on CBER Division of Cellular and Gene Therapies
“Other than logistics (e.g. date/time of meeting) the RPM is often not aware of discussions within the
review team.”
-Sponsor comment on CDER Transplant and Ophthalmology Products
“Our project manager is an MPH without obvious specific oncology pharmaceutical experience. We found
some of the comments made to be arbitrary.”
-Sponsor comment on CDER Division of Oncology Products
Neg
ati
ve
Feed
back
Po
siti
ve
Feed
back
14
Email and formal letters are the most
frequently used communication channels;
sponsors find in-person formal meetings
most beneficial
● 69% of survey participants rate in-person formal
meetings as Very Beneficial compared to only 53% for
emails and 48% for formal letters
● CBER Division of Cellular and Gene Therapies has the
highest total communication channels ratings (85%
Very Beneficial)
3
14
15
43% 47% 36% 27%48%
53% 48% 59% 69%45%
While email and formal letters are the most frequently utilized communication channels, sponsors find in-person formal meetings the most beneficial
Channels Used to Communicate with FDA
Showing % Across All Phases
Ben
efi
cia
l
Rati
ng
s
Beneficial Ratings for Channels Used to Communicate with FDA
Showing % Across All Phases
n=235 n=181 n=119n=135 n=62
Note: n-sizes reflect the number of responses within journals (questions asked multiple times in each journal)
Email Formal Letter Unscheduled
Phone Call
Ch
an
nel U
sed
(n=
37
7)
64% 50% 17%
Scheduled
Phone Call
36%
In-Person
Formal Meeting
32%
16
CBER Division of Cellular & Gene Therapies has the highest total rating for all communication channels; CDER Division of Metabolism & Endocrinology Products has the lowest
Note: n-sizes reflect the number of responses within journals (questions asked multiple times in each journal)
CBER Division of Cellular and Gene Therapies
Highest “Very Beneficial” Rating with 85%
CDER Division of Metabolism and Endocrinology Products
Lowest “Very Beneficial” Rating with 28%
“Email allows the issue/questions to be laid out by both FDA and company and provides a comprehensive response”
-Sponsor comment on CBER Division of Cellular and Gene Therapies
“[In-person meetings] are always helpful to discuss with reviewers study designs given complexities that are difficult
to convey in writing.”
-Sponsor comment on CBER Division of Cellular and Gene Therapies
“Feedback was not received in a timely manner; information provided could not be addressed at that point in time.”
-Sponsor comment on CDER Division of Metabolism and Endocrinology Products
“Sometimes FDA did not respond to the emails which had questions.”
-Sponsor comment on CDER Division of Metabolism and Endocrinology Products
n=48
n=71
15

17
Pre-phase meetings increase overall communications ratings, yet
many respondents did not think a meeting was necessary at the time
Of those who did not have a meeting, 8 in 10 say it
was because they did not think it was necessary
2% 6%5%
10%
40%
43%
53%40%
Meeting
(n=253)
No Meeting
(n=143)
Overall Ratings of Communications with FDA
Showing % Had Meeting Prior to Any Phase vs. Did Not
Have Meeting Prior to Any Phase
Very
Beneficial
Somewhat
Beneficial
Not Very
Beneficial
Not At All
Beneficial
n=143*
Note: n-sizes reflect the number of journals
*n-size reflects sponsors who provided both a reason for not having a meeting and an overall communications rating
18
69%
31%Total
Yes No Not applicable, received a response
0% contacted the
Enhanced Communications Team
n=51
No respondents have contacted the Enhanced Communications Team; many did not know it existed
If you did not receive a response to your procedural
or simple clarifying question within the expected or
agreed timeframe, did you contact the new
Enhanced Communications team?
Why did you not contact the new Enhanced
Communications team?Asked of Those Who Answered No
100%
53% did not know it existed
13% did not think it would be helpful
7% were concerned review team would view
contacting FDA staff outside their team negatively
n=15
Note: n-sizes reflect the number of journals
16

19
Open-ended responses provided by
survey participants reveal that thorough
discussions enhance FDA-sponsor
communications, while a lack of clarity
makes interactions less beneficial
● The most beneficial communications with FDA are
thorough, constructive, timely, or collaborative, and
they allow sponsors to detect problems early
● Less beneficial communications with FDA are untimely
or unclear, and may make scheduling meetings
difficult
4
2020
7%
10%
19%
32%
32%
Most of the positive comments about communications mention thorough discussions and constructive feedback
Note: n-sizes reflect the number of positive comments mentioning the feedback above
n=215
“The FDA has been very responsive, provide
thorough comments and guidance”-Sponsor comment on CDER Division of Neurology Products
“FDA provided important information about general concerns
that needed to be addressed to support clinical development.”-Sponsor comment on CDER Division of Gastroenterology and Inborn Error Products
“Open dialogue and clear understanding of FDA’s expectations for
phase 2b and phase 3 clinical trial design for Crohn's disease.” – Sponsor comment on CDER Division of Gastroenterology and Inborn Error Products
A review of comments shows that
thorough discussion helps lead to
beneficial ratings
Constructive feedback is highly
valued in FDA interactions
Timely responses support
successful FDA communication
Sponsors highly value
collaboration with FDA
Early detection of potential issues
can save valuable time
“The teleconferences were helpful in clarifying the FDA’s concerns
and allowing us to express our perspective on the issues.”-Sponsor comment on CDER Division of Cardiovascular and Renal Products
Reasons for Beneficial Ratings
Showing % of mentions referring to the following positive feedback
“Good input from the review division on ways to streamline the
clinical program. With this input we’re able to move quickly into
start of program following meeting (EOP2).” - Sponsor comment on CDER Division of Anti-Infective Products
17

2121
17%
10%
32%
41%
Unclear communications are the top reason for negative comments
“FDA designation of a combination product at the end
of an IND review caused significant delays.”
-Sponsor comment on CDER Division of Gastroenterology
and Inborn Error Products
n=71
“FDA hadn't clearly stated their understanding/expectation of the
'use' of the proposed drug which lead to delay in trial design.”
-Sponsor comment on CDER Division of Neurology Products
“Getting time with FDA is difficult. The project managers
are generally very responsive but it takes them quite a
while to schedule a meeting or get the appropriate parties
available for a formal or informal teleconference.”
-Sponsor comment on CDER Division of Gastroenterology and
Inborn Error Products
Notes: n-sizes reflect total number of negative comments about specific areas of feedback; “17%” not to scale
Many sponsors want FDA to be
more clear in their
communications
Some sponsors experienced
delays that they attributed to
untimely communication
Difficulty scheduling meetings
and cancellations limit the value
of sponsor-FDA interactions
Other
Reasons for Beneficial Ratings
Showing % of mentions referring to the following negative feedback
22
Sponsors of programs with special
designations also value timely
communication, clear expectations, and
constructive feedback
● Orphan Drug sponsors report high beneficial ratings
for overall communications, RPMs, and
communication channels
● Sponsors value the frequent communication of the
Fast Track program, but need more clarity about
criteria and benefits of the program
● Sponsors want more clarity about criteria required to
obtain Breakthrough Therapy designation
5
18
23
Special Designations and Approvals
Special Designation # of Programs With Responses
Orphan Drug Program 44
Fast Track Designation 35
Accelerated Approval 4
Breakthrough Therapy Designation 7
Genetically Targeted Program 9
Note: n-sizes reflect the number of programs
24
2%
41%
57%
1%9%
40%
49%
3%
30%
67%
2%5%
40%
54%
2%4%
40%
55%
4%
7%
41%
48%
Overall Communications Ratings Regulatory Project Manager Ratings Total Communication Channels Ratings
n=75 n=51
Orphan Drugsn=158*
Orphan Drugs Orphan Drugsn=397
All Programsn=248
All Programsn=732*
All Programs
Orphan Drug sponsors provide high beneficial ratings for multiple
aspects of FDA communications
Note: n-sizes reflect the number of journals
*n-sizes reflect the number of responses within journals (questions asked multiple times in each journal)
19

25
12%
21%
27%
39% More frequent
communications
Rolling Review
FDA more flexible
Other
9%
56%
35%
Fast Track
(n=34)
Very Beneficial
Somewhat Beneficial
Not Very Beneficial
Not at all Benefical
n=33
Sponsors value the frequent communication of the Fast Track program,
but need more clarity about criteria and benefits of the program
Overall, how would you rate the Fast Track program?Asked of Those Who Received a Fast Track Designation
What is the most beneficial aspect of the Fast Track program?Asked of Those Who Received a Fast Track Designation
How could the Fast Track program be improved?
“The indication granted for Fast Track are overly specific and can lead to a
company having to make multiple requests for Fast Track as the indication
broadens or narrows, particularly when FT designation is granted earlier in
development before additional clinical data helps refine the patient population
that can benefit.”
-Sponsor comment on CBER Division of Cellular and Gene Therapies
“Better define the expectation of what the program is supposed to offer.”
-Sponsor comment on CDER Division of Anesthesia, Analgesia, and Addiction Products
Note: n-sizes reflect the number of programs
26
Sponsors want more clarity about criteria required to obtain
Breakthrough Therapy designation
“Better information on what constitutes a BTD product. Better understand of the benefits of BTD,
especially as it relates to more frequent FDA interactions.”
-Sponsor comment on CDER Division of Hematology Products
“Agency should continue to provide guidance and direction on what criteria need to be met to achieve BT
designation.”
-Sponsor comment on CDER Division of Pulmonary, Allergy, and Rheumatology Products
“Update the BTD guidance to state that for the oncology division, they will require more substantial
clinical evidence than currently stated in the guidance”
-Sponsor comment on CDER Division of Oncology Products
“More clarity is needed around the actual expectations, appear to be some inconsistencies around how
they make the determination. Underlying questions is what is the threshold for their determination of
"substantial improvement.”
-Sponsor comment on CDER Division of Oncology Products
20
27
Conclusions
Overall, half of sponsors say their interactions with FDA are very beneficial, while half
cite room for improvement
Regulatory Project Manager (RPM) performance ratings are highest for CBER, aligning
with overall ratings
Open-ended responses provided by survey participants reveal that thorough
discussions enhance FDA-sponsor communications, while a lack of clarity makes
interactions less beneficial
1
2
4
Email and formal letters are the most frequently used communication channels;
sponsors find in-person formal meetings the most beneficial
3
Sponsors of programs with special designations also value timely communication,
clear expectations, and constructive feedback
5
21

COMPARISON OF PERFORMANCE RATINGS
BETWEEN CENTERS & REVIEW DIVISIONS

1
WIN N IN G K N OWLEDGET M
WIN N IN G K N OWLEDGET M
COMPARISON OF PERFORMANCE
RATINGS BETWEEN CENTERS &
REVIEW DIVISIONS
Summary Charts: Center/Division Ratings for
Overall Communications and Individual
Communication Channels
FDA/Sponsor Interactions During Drug DevelopmentMay 18, 2016
2
Overall Communications Ratings
How would you rate your overall interactions with FDA?
Overall
CommunicationsCDER CBER CDRH
CDER
Division of
Oncology
Products
CDER
Division of
Neurology
Products
CDER Division of
Gastroenterology
and Inborn Error
Products
CDER
Division of
Hematology
Products
CDER Division of
Metabolism and
Endocrinology
Products
CBER Division of
Cellular and
Gene Therapies
Orphan Drug
Designation
N-Size 350 43 17 83 58 26 37 27 22 75
Very Beneficial 47% 60% 41% 54% 33% 38% 54% 44% 50% 49%
Somewhat Beneficial 41% 35% 47% 42% 57% 31% 38% 37% 45% 40%
Not very Beneficial 7% 5% 12% 4% 5% 19% 8% 19% 5% 9%
Not at all Beneficial 4% 0% 0% 0% 5% 12% 0% 0% 0% 1%
Showing % across all phases for ratings of overall communications with FDA
23
3
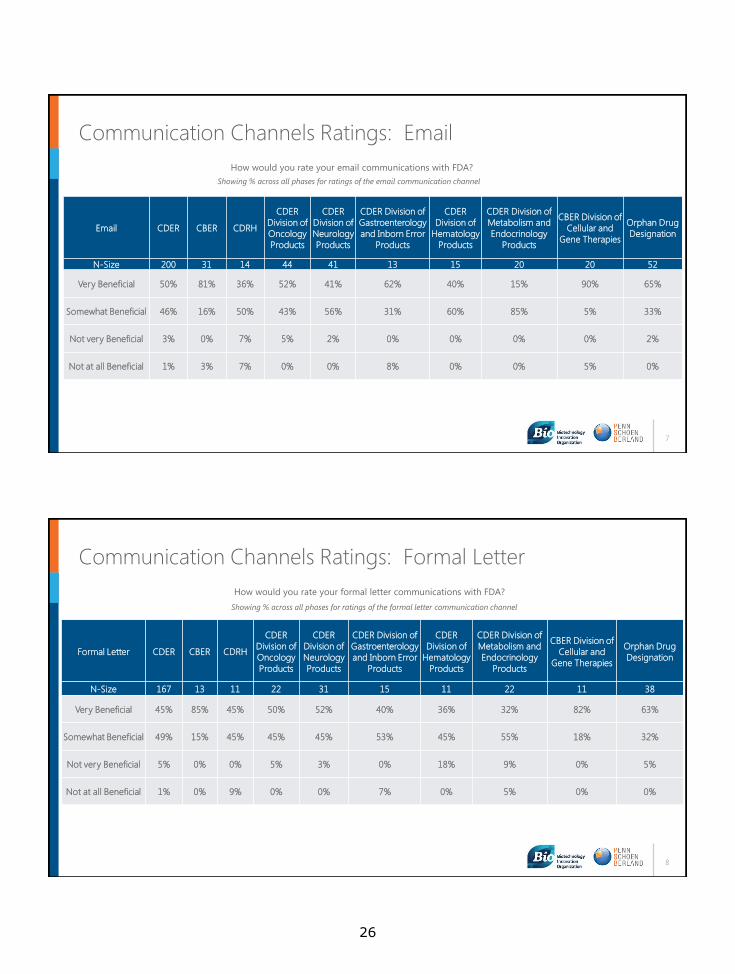
Regulatory Project Manager Communications Ratings
How would you rate your interactions with your FDA Regulatory Project Manager?
Regulatory Project
ManagerCDER CBER CDRH
CDER
Division of
Oncology
Products
CDER
Division of
Neurology
Products
CDER Division of
Gastroenterology
and Inborn Error
Products
CDER
Division of
Hematology
Products
CDER Division of
Metabolism and
Endocrinology
Products
CBER Division of
Cellular and
Gene Therapies
Orphan Drug
Designation
N-Size 222 23 12 53 42 14 22 18 13 51
Very Beneficial 53% 70% 50% 60% 43% 57% 45% 50% 69% 57%
Somewhat Beneficial 41% 26% 42% 32% 55% 36% 55% 44% 31% 41%
Not very Beneficial 5% 4% 0% 8% 0% 7% 0% 6% 0% 0%
Not at all Beneficial 1% 0% 8% 0% 2% 0% 0% 0% 0% 2%
Showing % across all phases for ratings of communications with the Regulatory Project Manager
4
Total Communication Channels Ratings
How would you rate your <communication channel> communications with FDA?
Total
CommunicationsCDER CBER CDRH
CDER
Division of
Oncology
Products
CDER
Division of
Neurology
Products
CDER Division of
Gastroenterology
and Inborn Error
Products
CDER
Division of
Hematology
Products
CDER Division of
Metabolism and
Endocrinology
Products
CBER Division of
Cellular and
Gene Therapies
Orphan Drug
Designation
N-Size 640 76 53 110 118 54 48 71 48 158
Very Beneficial 52% 83% 49% 60% 47% 54% 42% 28% 85% 67%
Somewhat Beneficial 43% 16% 43% 37% 49% 37% 54% 61% 12% 30%
Not very Beneficial 4% 0% 4% 3% 3% 0% 4% 10% 0% 3%
Not at all Beneficial 2% 1% 4% 0% 1% 9% 0% 1% 2% 0%
Showing % across all phases for ratings of all communications channels combined
*Communication channels include: email, unscheduled phone calls, scheduled
phone calls, formal letters, and in-person formal meetings
24

5
WIN N IN G K N OWLEDGET M
WIN N IN G K N OWLEDGET M
NEED MORE INFORMATION:
Communication Channels Ratings
FDA/Sponsor Interactions During Drug DevelopmentMay 18, 2016
6
How would you rating your <meeting> with FDA?
All Meetings Ratings CDER CBER CDRH
CDER
Division of
Oncology
Products
CDER
Division of
Neurology
Products
CDER Division of
Gastroenterology
and Inborn Error
Products
CDER
Division of
Hematology
Products
CDER Division of
Metabolism and
Endocrinology
Products
CBER Division of
Cellular and
Gene Therapies
Orphan Drug
Designation
N-Size 303 26 28 45 43 26 23 45 17 70
Very Beneficial 65% 69% 71% 78% 56% 62% 65% 53% 59% 73%
Somewhat Beneficial 28% 23% 25% 22% 40% 35% 30% 36% 29% 21%
Not very Beneficial 5% 8% 4% 0% 5% 4% 0% 11% 12% 6%
Not at all Beneficial 2% 0% 0% 0% 0% 0% 4% 0% 0% 0%
Showing % across all phases for ratings of all meetings combined
Ratings for All Formal Meetings (Type B, Type C, & In-Person Formal Meetings)
25
7
Communication Channels Ratings: Email
How would you rate your email communications with FDA?
Email CDER CBER CDRH
CDER
Division of
Oncology
Products
CDER
Division of
Neurology
Products
CDER Division of
Gastroenterology
and Inborn Error
Products
CDER
Division of
Hematology
Products
CDER Division of
Metabolism and
Endocrinology
Products
CBER Division of
Cellular and
Gene Therapies
Orphan Drug
Designation
N-Size 200 31 14 44 41 13 15 20 20 52
Very Beneficial 50% 81% 36% 52% 41% 62% 40% 15% 90% 65%
Somewhat Beneficial 46% 16% 50% 43% 56% 31% 60% 85% 5% 33%
Not very Beneficial 3% 0% 7% 5% 2% 0% 0% 0% 0% 2%
Not at all Beneficial 1% 3% 7% 0% 0% 8% 0% 0% 5% 0%
Showing % across all phases for ratings of the email communication channel
8
Communication Channels Ratings: Formal Letter
Formal Letter CDER CBER CDRH
CDER
Division of
Oncology
Products
CDER
Division of
Neurology
Products
CDER Division of
Gastroenterology
and Inborn Error
Products
CDER
Division of
Hematology
Products
CDER Division of
Metabolism and
Endocrinology
Products
CBER Division of
Cellular and
Gene Therapies
Orphan Drug
Designation
N-Size 167 13 11 22 31 15 11 22 11 38
Very Beneficial 45% 85% 45% 50% 52% 40% 36% 32% 82% 63%
Somewhat Beneficial 49% 15% 45% 45% 45% 53% 45% 55% 18% 32%
Not very Beneficial 5% 0% 0% 5% 3% 0% 18% 9% 0% 5%
Not at all Beneficial 1% 0% 9% 0% 0% 7% 0% 5% 0% 0%
How would you rate your formal letter communications with FDA?
Showing % across all phases for ratings of the formal letter communication channel
26

9
Communication Channels Ratings: Scheduled Phone Call
Scheduled Phone Call CDER CBER CDRH
CDER
Division of
Oncology
Products
CDER
Division of
Neurology
Products
CDER Division of
Gastroenterology
and Inborn Error
Products
CDER
Division of
Hematology
Products
CDER Division of
Metabolism and
Endocrinology
Products
CBER Division of
Cellular and
Gene Therapies
Orphan Drug
Designation
N-Size 111 17 12 22 19 10 9 10 8 31
Very Beneficial 58% 82% 42% 73% 63% 50% 44% 30% 88% 68%
Somewhat Beneficial 36% 18% 50% 27% 37% 30% 56% 40% 12% 32%
Not very Beneficial 4% 0% 8% 0% 0% 0% 0% 30% 0% 0%
Not at all Beneficial 3% 0% 0% 0% 0% 20% 0% 0% 0% 0%
How would you rate your scheduled phone call communications with FDA?
Showing % across all phases for ratings of the scheduled phone call communication channel
10
Communication Channels Ratings: In-person Formal Meeting
In-person Formal
MeetingCDER CBER CDRH
CDER
Division of
Oncology
Products
CDER
Division of
Neurology
Products
CDER Division of
Gastroenterology
and Inborn Error
Products
CDER
Division of
Hematology
Products
CDER Division of
Metabolism and
Endocrinology
Products
CBER Division of
Cellular and
Gene Therapies
Orphan
Drug
Designation
N-Size 108 7 10 14 14 12 11 11 4 23
Very Beneficial 67% 100% 80% 86% 57% 67% 55% 45% 100% 83%
Somewhat Beneficial 29% 0% 20% 14% 29% 33% 45% 45% 0% 9%
Not very Beneficial 4% 0% 0% 0% 14% 0% 0% 9% 0% 9%
Not at all Beneficial 1% 0% 0% 0% 0% 0% 0% 0% 0% 0%
How would you rate your in-person formal meeting communications with FDA?
Showing % across all phases for ratings of the in-person formal meeting communication channel
27

11
Communication Channels Ratings: Unscheduled Phone Call
How would you rate your unscheduled phone call communications with FDA?
Unscheduled Phone
CallCDER CBER CDRH
CDER
Division of
Oncology
Products
CDER
Division of
Neurology
Products
CDER Division of
Gastroenterology
and Inborn Error
Products
CDER
Division of
Hematology
Products
CDER Division of
Metabolism and
Endocrinology
Products
CBER Division of
Cellular and
Gene Therapies
Orphan Drug
Designation
N-Size 54 8 6 8 13 4 2 8 5 14
Very Beneficial 41% 75% 50% 50% 15% 50% 0% 25% 60% 57%
Somewhat Beneficial 52% 25% 50% 50% 77% 25% 100% 62% 40% 43%
Not very Beneficial 4% 0% 0% 0% 0% 0% 0% 12% 0% 0%
Not at all Beneficial 4% 0% 0% 0% 8% 25% 0% 0% 0% 0%
Showing % across all phases for ratings of the unscheduled phone call communication channel
28
CDER
363 programs under review 397 phase-specific journals
The CDER Division reviewing the most programs in this survey is the Division of Oncology Products (n=87), followed by the Division of Neurology Products (n=49), the Division of Gastroenterology and Inborn Error Products (n=38), the Division of Metabolism and Endocrinology Products (n=34), and the Division of Hematology Products (n=30). The responses within these top 5 Divisions provide the basis for our analysis throughout this report. The remaining clinical programs (n=125) are being reviewed by the following CDER Divisions: Dermatology and Dental Products; Cardiovascular and Renal Products; Anti-Viral Products; Anti-Infective Products; Anesthesia, Analgesia, and Addiction Products; Bone, Reproductive, and Urologic Products; Medical Imaging Products; Pulmonary, Allergy, and Rheumatology Products; Psychiatry Products; and Transplant and Ophthalmology Products. CDER participants representing the Division of Oncology Products submitted the most phase-specific journals (n=88), followed by the Division of Neurology Products (n=67), the Division of Hematology Products (n=39), the Division of Metabolism and Endocrinology Products (n=31), and the Division of Gastroenterology and Inborn Error Products (n=31). CDER participants provided the most feedback about their phase-specific experiences in the Pre-IND stage of development (n=109). Phase 1 (n=102) and Phase 2 (n=100) were represented evenly, while Phase 3 (n=86) had the fewest responses. OVERALL COMMUNICATIONS Forty-seven percent of survey participants with clinical development programs under review by CDER rated their overall communications as Very Beneficial, while 41% said Somewhat Beneficial, 7% said Not Very Beneficial, and 4% said Not At All Beneficial. Survey participants that had beneficial interactions with the FDA described communications that were straightforward, constructive, and obtained in a timely manner. Survey participants cited a lack of consistency in feedback and an inability to engage in scientific dialogue to discuss FDA’s positions/concerns as reasons for lower performance ratings. Beneficial
“Responses were timely and helpful.” – Cardiovascular and Renal Products “Thorough, complete, clear.” – Cardiovascular and Renal Products “The FDA has been very responsive, provided thorough comments and guidance.”
– Anesthesia, Analgesia, and Addiction Products “Constructive comments were received.” – Bone, Reproductive and Urologic Products “FDA provided clear guidance and shared its current thinking of drug development
for the disease area.” – Pulmonary, Allergy, and Rheumatology Products “Communications were straightforward.” – Psychiatry Products
Room for Improvement
“Feedback and guidance has been variable and did not always follow prior precedent in this space.” – Anesthesia, Analgesia, and Addiction Products
“The FDA didn't highlight the key clinical issue prior to review.” – Pulmonary, Allergy, and Rheumatology Products
29

“Team received inconsistent comments and feedback from the Agency throughout the review process: different levels of management provided different comments.” – Transplant and Ophthalmology Products
“FDA did not provide rationale for positions.” – Transplant and Ophthalmology Products
“We did not feel that FDA was willing to engage in any substantial dialogue via email without formal communication. Emails were not helpful other than as a means of communication.” – Anti-Viral Products
REGULATORY PROJECT MANAGER Approximately half of survey respondents within CDER rated interactions with their Regulatory Project Manager (RPM) as Very Beneficial (53%). Forty-one percent rated them as Somewhat Beneficial and 6% rated them as Not Very Beneficial or Not At All Beneficial. Survey participants that had beneficial interactions with their RPM described interactions that were collaborative and communications that were obtained in a timely manner. Survey participants that had less beneficial interactions with their RPM cited issues with inexperienced RPMs, inability to engage in dialogue with the review team, and a lack of responsiveness as reasons for lower performance ratings. Beneficial
“Easy to communicate with and sought to understand sponsor perspective.” – Cardiovascular and Renal Products
“Very communicative, collaborative, and transparent.” – Anesthesia, Analgesia, and Addiction Products
“Our Regulatory Project Manager is very responsive and the review team provides us timely feedback.” – Psychiatry Products
Room for Improvement
“Somewhat formal and procedure oriented.” – Anti-Viral Products “Not responsive and information not always adequate, not much experience.”
– Anesthesia, Analgesia, and Addiction Products “Always very helpful, responds quickly most of the time. However, other than
logistics (e.g. date/time of meeting) the RPM is often not aware of discussions within the review team.” – Transplant and Ophthalmology Products
COMMUNICATION CHANNELS AND ISSUE RESOLUTION Respondents were asked to rate specific communication channels through which they interacted with FDA: emails, unscheduled phone calls, scheduled phone calls, formal letters, and in-person formal meetings. Respondents within CDER rated these communication channels, collectively, as 52% Very Beneficial, 43% Somewhat Beneficial, 4% Not Very Beneficial, and 2% Not At All Beneficial. When we examine the utilization of specific communication channels, email is the most utilized channel of communication within CDER, followed by formal letters, scheduled phone calls, in-person meetings, and unscheduled phone calls. In terms of rating the usefulness of specific communication channels, in-person formal meetings had the highest percentage of CDER participants rating interactions as Very Beneficial (67%). Scheduled phone calls were the second highest rated channel (58% Very Beneficial), followed by emails (50%), formal letters (45%), and unscheduled phone calls (41%).
30
When we examine combined ratings for formal meetings (Type B, Type C, and other in-person formal meetings), we see a high percentage of Very Beneficial ratings (65%). Survey participants that rated communication channels positively describe effective use of multiple communication channels to obtain constructive and proactive feedback. They cite information that is conveyed in a timely manner, interactions that enable scientific dialogue, and efficient resolution of issues as reasons for high performance ratings. Conversely, survey participants that cited room for improvement in their usage of communication channels described issues in obtaining timely responses, communications that lacked clarity, feedback that was inconsistent, and an inability to engage in scientific dialogue with FDA as reasons for low performance ratings. Beneficial Utilization of Communication Channels
“Email communications were used in support of a Type C meeting, both before and after the meeting. The Type C meeting was prior to Phase 2b. We had very good interaction and innovative thinking about the study endpoint. The Division Director was very open and also helped guide some of the other reviewers to think similarly.” – Cardiovascular and Renal Products
“FDA was very engaged and gave good feedback and appropriate rationale for their thinking. They were helpful and willing to have additional discussions.” – Anti-Viral Products
“Emails were timely and helpful in gaining agreement prior to submission of formal amendments.” – Anti-Viral Products
“Good input from the review division on ways to streamline the clinical program. With this input we’re able to move quickly into start of program following meeting (EOP2).” – Anti-Infective Products
“FDA provided constructive and detailed preliminary feedback in advance of our face to face meeting which helped to hone the conversation to the key issues and was able to ensure these could be discussed within the allotted meeting time.” – Psychiatry Products
“Very open dialogue about dosing via email and scheduled phone call for one of proposed studies.” – Psychiatry Products
“FDA responded in a timely manner to our emails and provided us guidance for submitting carcinogenicity protocols.” – Psychiatry Products
“Live discussions with the DTOP are always preferred. Preliminary comments ahead of the meeting are always most helpful.” – Transplant and Ophthalmology Products
Beneficial Utilization of Communication Channels to Resolve Issues
“Agency was responsive to discussions around alternate means to populate information required for complete IND submission.” – Cardiovascular and Renal Products
“EOP2 meeting had a lot of topics to cover and little time to get through everything. Based on FDA input at the meeting we had questions on whether revisions we'd made to clinical trials would be satisfactory. We were able to quickly resolve with email communication. FDA was quick to respond.” – Anti-Infective Products
“Biomarker topic was discussed in a separate meeting (separate from EOP2) per FDA advice (Very Beneficial).” – Pulmonary, Allergy, and Rheumatology Products
“Clarified deficiencies in proposed program and helped us develop a path forward to address FDA comments/concerns (EOP2).” – Pulmonary, Allergy, and Rheumatology Products
“FDA was very responsive to query about clinical trial endpoints and enrollment criteria.” – Transplant and Ophthalmology Products
31
Room for Improving Utilization of Communication Channels “In general each of these (communication channels) interactions has the potential to
clarify FDA expectations and they usually do. What we seek is from the FDA is clarity (based on reasonable scientific rationale) and consistency. In our experience the Agency does a fair job on the former but has been disappointing on the latter. In addition the issue of ease of access is a substantial one. While we would like to have more in the way of informal discussions, to date this has been difficult to achieve.” – Anesthesia, Analgesia, and Addiction Products
“FDA changed expectations from pre-IND to those required for IND filing - Had to fix inconsistent advice received during pre-IND.” – Anti-Viral Products
“Not responsive in a timely manner to providing comments on the clinical trial protocols, even though these had been available and on file for some time. Review was delayed until interim safety data were provided to the agency for review.” – Anti-Viral Products
“When Type C meeting is carried out as written response – agency should consider allowing sponsor to ask follow up questions – sometimes recommendations listed in response are confusing and not straight forward causing a lot of questions about how to best move forward.” – Pulmonary, Allergy, and Rheumatology Products
“Lack of ability to have dialogue when responses are limited to written format, especially when proposed approach is denied.” – Pulmonary, Allergy, and Rheumatology Products
“We received an information request in (Fall) 2012, responded to the Agency about a week later, and then didn't receive a follow-up response from FDA until (Early) 2013, at which time the study had significantly progressed.” – Psychiatry Products
Room for Improving Utilization of Communication Channels to Resolve Issues
“FDA was unable to provide guidance on structural endpoints given current state of field (at EOP2).” – Dermatology and Dental Products
“We subscribed to their suggestions, submitted an SPA, and they ignored their own counsel when we completed the study (EOP2).” – Anesthesia, Analgesia, and Addiction Products
“(FDA) was open to discussing options during meeting. Timeliness suffered when consult review (from another division) was required on one issue. Would have been useful to have both Review divisions provide unified feedback, which was not the case in this instance.” – Pulmonary, Allergy, and Rheumatology Products
“Requests regarding pediatrics seem slower than those for adult indications.” – Pulmonary, Allergy, and Rheumatology Products
“3 month delay waiting for FDA feedback regarding clinical study dosing plan before could start study.” – Psychiatry Products
32
CDER Division of Oncology Products
87 programs under review 88 phase-specific journals
The most common stages of development for feedback on interactions with the Division of Oncology Products were Phase 1 (34%) and Pre-IND (28%). The remaining journals were split between Phase 2 (23%) and Phase 3 (15%). OVERALL COMMUNICATIONS Among the top 5 represented CDER Review Divisions (Oncology, Neurology, Hematology, Metabolism & Endocrinology, and Gastroenterology & Inborn Error), Oncology tied with Hematology for the highest performance rating for overall communications (54% Very Beneficial). Comments from survey participants who rated overall communications as Very Beneficial describe interactions that were collaborative and communications that were clear and obtained in a timely manner. Clinical programs being reviewed by the Oncology Division had the second highest percentage rating overall communications as Somewhat Beneficial (42%) among the top 5 CDER Review Divisions. The Division did not have any survey participants rate overall communications as Not At All Beneficial and only 4% rated them as Not Very Beneficial. Comments cited inconsistent feedback and multiple rounds of communications required to obtain necessary information as reasons for lower performance ratings. Beneficial
“FDA was responsive.” “All communications were very clear and responses from FDA were timely.” “Collaborative environment – FDA was responsive and sent preliminary comments
early and all additional questions were addressed during in-person meeting.” “All communications were very clear and responses from FDA were timely.”
Room for Improvement
“Reviewer's comments and responses to questions were inconsistent with the same division precedents and inconsistent with clinical practice.”
“FDA was responsive to emails. However, it took several rounds of emails before they indicated that our revisions were acceptable.”
REGULATORY PROJECT MANAGER The CDER Division of Oncology’s Regulatory Project Manager (RPM) ratings were the highest among the top 5 represented CDER Review Divisions, with 60% of respondents rating their interactions with RPMs as Very Beneficial. Survey participants that rated interactions with their RPM as Very Beneficial described interactions that were responsive and communications that were clear. However, Oncology also had the highest percentage of survey participants rating their interactions with RPMs as Not Very Beneficial (8%) compared to all Centers and Review Divisions analyzed.
33

Survey participants that rated interactions with their RPM as Not Very Beneficial cited lack of experience and lack of substantive feedback as reasons for low performance ratings. Beneficial
“Clear and timely communication.” “FDA project manager was very responsive to all forms of communication.” “Very Responsive”
Room for Improvement
“Did not seem to have oncology pharmaceutical experience, some comments seemed arbitrary.”
“Regulatory Project Manager primarily handled work flow. Friendly and efficient but no further input was available.”
“Very inexperienced Regulatory Project Manager assigned” COMMUNICATION CHANNELS AND ISSUE RESOLUTION Among the top 5 represented CDER Review Divisions, Oncology had the highest percentage of responses that rated utilization of communication channels (email, unscheduled phone calls, scheduled phone calls, formal letters, and in-person meetings) as Very Beneficial (60%). Survey participants that rated utilization of communication channels as Very Beneficial describe communications that were clear and timely, processes that enabled effective use of multiple communication channels to gain clarity on questions, and feedback and interactions that were effective and efficient in resolving issues. Nearly half of the responses in the Division of Oncology rated utilization of communication channels as Somewhat Beneficial (37%) or Not Very Beneficial (3%). Communications that were inconsistent, inability to gain clarity on FDA responses and resolve issues, and delays in obtaining time-sensitive feedback were common reasons attributed to lower performance ratings. When we examine ratings of specific communication channels, Oncology had by far the highest combined formal meeting (Type B, Type C, and other in-person formal meetings) performance ratings among all Centers and Review Divisions examined (78% Very Beneficial). Comments from survey participants that rated combined formal meetings as Very Beneficial described interactions that provided clear feedback and communications that were helpful in advancing clinical development programs. Survey participants cited inconsistent feedback and scheduling/timing difficulties as reasons for lower combined formal meeting performance ratings. We do not have enough responses to discuss trends for other individual communication channels at this time. Beneficial Utilization of Communication Channels
“FDA was very responsive to emails and sponsor was able to reply with comments and clarifications to protocols in a timely manner.”
“FDA clarified considerations for their position and provided clear feedback on sponsor proposals during scheduled phone call.”
34

“Written communications (email and letters) were clear with specified timelines and actions required.”
“Pre-IND meeting responses were clear and helpful in protocol design.” “Received concrete feedback from agency in End of Phase 2 meeting.”
Beneficial Utilization of Communication Channels to Resolve Issues
“Clear and rapid communications on protocol design changes via email and formal letter.”
“FDA provided beneficial advice during scheduled call on safety observations.” “Timely response to request for extension to address CMC comments received during
IND assessment” “Communications have been beneficial regarding the phase 1 protocol and the input
from the Division was very helpful in finalizing a couple of issues in the protocol.” “Input on Phase 3 trial design; clinical pharmacology program was beneficial” “Emails, scheduled calls and formal letters useful to address FDA’s comments in a
timely manner and modify protocol accordingly” Room for Improving Utilization of Communication Channels
“Written responses were unhelpful, insufficient detail provided.” “Reviewer's comments and responses to questions were inconsistent with the same
division precedents and inconsistent with clinical practice.” “FDA cancelled our End of Phase 2 meeting without explanation and rescheduled us
several months later. An Advisory Committee meeting in between resulted in a change of FDA policy on approvable endpoints for our indication.”
Room for Improving Utilization of Communication Channels to Resolve Issues
“FDA did not provide opportunity to discuss recommended changes (by FDA) to study designs”
“FDA reviewers raised concerns that were not based on the preclinical package. An abundance of caution is welcome but if unnecessary testing increases the cost of Phase 1 and lowers patient interest and/or compliance, we all lose.”
“Reviewers indicated certain generic concerns that were not justified by the IND preclinical package (i.e. CV risk monitoring in the absence of any CV risk findings in the preclinical package).”
“Submitted IND sequence document to eCTD regarding changes to dosing regimen but no response from FDA – assumption is everything is acknowledged and approved but not certain”
“FDA addressed questions asked but time was limited and issues arising during the discussion could not be addressed as they were not on the agenda requiring a follow-up call.”
35
CDER Division of Neurology Products
49 programs under review 67 phase-specific journals
Phase-specific feedback from clinical development programs being reviewed by the Division of Neurology Products was spread evenly across the four stages of development – Pre-IND (27%), Phase 1 (24%), Phase 2 (27%), and Phase 3 (22%). OVERALL COMMUNICATIONS The Division of Neurology Products had the lowest percentage of survey participants rating their overall communications as Very Beneficial (33%) among the top 5 represented CDER Review Divisions. Comments from survey participants who rated overall communications as Very Beneficial describe communications that were timely and provided constructive feedback. The Division of Neurology had the highest percentage of respondents rate their overall communications as Somewhat Beneficial (57%) compared to all of the Centers and Review Divisions analyzed. The Division of Neurology had the 2nd highest percentage of respondents rate overall communications as Not at All Beneficial (5%) among the top 5 CDER Review Divisions analyzed. This percentage is in line with what we see across all CDER clinical development programs combined (4% Not At All Beneficial). The inability to discuss new approaches to clinical trial designs, problems reaching agreement on scientific issues, and uncertainty about expertise of reviewers on certain specialty issues were common reasons cited for lower performance ratings. Beneficial
“Constructive feedback.” “(Communications) helped shape the development path forward” “Responses received in timely manner.” “At the Pre-IND Phase FDA was very helpful and responsive to the questions about
scope of pre-IND testing.” Room for Improvement
“The Agency gave good overall feedback, although it did not appear that there was adequate understanding of the finer aspects of the orphan disease and the constraints thereof.”
“FDA does not make it easy to discuss new strategies for clinical trial designs (for orphan diseases), with Sponsors.”
“Transitioning of Divisional Leadership, as well as lack of consensus in scientific development of this area contribute to some uncertainty regarding FDA position on certain issues related to drug development in this therapeutic area.”
REGULATORY PROJECT MANAGER Among the top 5 CDER Review Divisions represented, the Division of Neurology Products had the lowest percentage of survey participants that rated interactions with their Regulatory Project Manager (RPM) as Very Beneficial (43%).
36

Survey participants that rated their interactions as Very Beneficial described timely and responsive communications with their RPM. Among the top 5 CDER Review Divisions represented, Neurology had the highest percentage of respondents that rated interactions with their RPM as Somewhat Beneficial (55%, tied with Hematology). Neurology was the only Division among the top 5 CDER Divisions that had respondents rate their RPM interactions as Not At All Beneficial (2%). Survey participants that rated their interactions as Somewhat Beneficial and Not At All Beneficial cited the need to interact with the review division to obtain information and issues that arose from having multiple RPMs as reasons for lower performance ratings. Beneficial
“Very responsive to emails.” “Timely confirmation of submitted documents.” “Responsive, helpful.” “In general, our project manager is very responsive and helpful.”
Room for Improvement
“In some instances he/she needs to follow up with the review division for information, which can limit the usefulness of the interactions.”
“There were multiple Regulatory Project Managers during the conduct of the Phase 3 program. Some had better communication styles/abilities than others.”
COMMUNICATION CHANNELS AND ISSUE RESOLUTION Among the top 5 CDER Review Divisions represented, the Division of Neurology Products had the 3rd highest percentage of responses rating utilization of communication channels as Very Beneficial (47%). Survey participants that rated utilization of communication channels as Very Beneficial described communications that were timely and thorough as well as interactions that enabled feedback on critical development program issues. The Division of Neurology Products had the 3rd highest percentage of responses that rated utilization of communication channels as Somewhat Beneficial (49%). The need for more timely feedback, the inability to discuss issues, and multiple communications required to obtain responses to questions were reasons given for lower performance ratings. When we examine ratings of specific communication channels, 56% of Neurology respondents rated combined formal meetings (Type B, Type C, and other in-person formal meetings) as Very Beneficial. This represents the 2nd lowest percentage among the top 5 CDER Review Divisions represented. Survey participants that rated in-person meetings as Very Beneficial described positive meetings that enabled scientific dialogue and allowed for the resolution of issues. Participants also praised meetings that provided feedback that was helpful in advancing clinical development programs. We do not have enough responses to discuss trends for other individual communication channels at this time.
37
Beneficial Utilization of Communication Channels “FDA was very responsive to the emails and telephone calls querying how to
reference pre-clinical studies conducted on behalf of another disease state.” “FDA provided beneficial information during scheduled phone call.” “Written responses to questions posed in pre-meeting briefing package were
thorough.” “FDA provided thorough written response to the questions posed in the pre-meeting
briefing package. The responses were received 2 days prior to their target for response.”
“We have received a lot of feedback on our study protocols and analysis plans by the reviewers.”
Beneficial Utilization of Communication Channels to Resolve Issues
“The FDA (Division Neurology Products) responded to our very specific questions posed for our Phase 3 protocol regardless of the method of communication.”
“The communications received from FDA regarding the Pediatric Study Plan were very helpful and allowed us to address all of the issues and receive an initial agreement.”
“Agreement on primary endpoint – prompt response and confirmation of endpoint enabled sponsor to proceed in a timely manner.”
“The Clinical Hold Letter outlined all items where additional information was requested.”
Room for Improving Utilization of Communication Channels “It would be very helpful if the division would respond in a timely fashion to email or
general correspondence, which are not under a clock (formal meeting). Sometimes there are small but significant questions that come up during the development that needs FDA input that can be accomplished by email/phone contact.”
“Difficult to discuss/receive any feedback during a conversation that was not set up with RPM in advance.”
Room for Improving Utilization of Communication Channels to Resolve Issues
“Provided multiple written submissions for requested CMC information and protocol amendments prior to lifting clinical hold.”
“Responses to the Special Protocol Assessment requests were not beneficial as we were unable to obtain agreement with the Division prior to initiating our Phase 3 trial.”
38
CDER Division of Hematology Products
30 programs under review 39 phase-specific journals
A majority of phase-specific journals submitted about the Division of Hematology Products were in the Pre-IND (41%) or Phase 1 (36%) stages of development. The remaining clinical program journals represented feedback about Phase 2 (15%) and Phase 3 (8%). OVERALL COMMUNICATIONS Among the top 5 CDER Review Divisions represented (Oncology, Neurology, Hematology, Metabolism & Endocrinology, and Gastroenterology & Inborn Error), Hematology tied with Oncology for the highest performance rating for overall communications (54% Very Beneficial). Comments from survey participants who rated overall communications as Very Beneficial described interactions with FDA as collaborative and communications as instructive and proactive. The Division of Hematology did not have any survey participants rate overall communications as Not At All Beneficial and had the 3rd lowest percentage of survey participants that rated overall communications as Not Very Beneficial (8%). Comments cited issues with inexperienced reviewers and lack of scientific dialogue as reasons for low performance ratings. Beneficial
“Collaborative tone.” “FDA agreed to review additional information prior to submission.” “The review division is collaborative and reasonable. The review teams have
provided instructive feedback.”
Room for Improvement “Some comments appeared to be from inexperienced reviewers.” “Was using non-traditional approach and CMC reviewer just said “follow guidance” –
not enough for FDA to hold a meeting must be an active participant – reviewer could have been more informative and identified pitfalls with the approach we were using.”
REGULATORY PROJECT MANAGER The Division of Hematology had the 2nd lowest ratings of respondents’ Regulatory Project Manager (RPM) among the top 5 CDER Review Divisions represented, with 45% rating their interactions as Very Beneficial. Survey participants that rated their interactions as Very Beneficial described interactions that were responsive and communications that were clear and instructive. The Division of Hematology had the highest percentage of respondents rating interactions with their RPM as Somewhat Beneficial (55%). No survey participants rated interactions as Not Very Beneficial or Not At All Beneficial. Survey participants cited issues with DOP2 Project Managers as reasons for lower performance ratings.
39

Beneficial “Prompt and clear responses to questions.” “RPM very responsive.” “Comments and concerns regarding the regulatory risk and regulatory path were
beneficial.”
Room for Improvement “Interactions with DOP2 have been problematic – delays in requests and lack of
coordination with Project Manager.” “Project manager from DOP2 is not responsive.”
COMMUNICATION CHANNELS AND ISSUE RESOLUTION Hematology had the 2nd lowest percentage of responses that rated utilization of communication channels (email, unscheduled phone calls, schedule phone calls, formal letters, and in-person meetings) as Very Beneficial (42%) among the top 5 CDER Review Divisions represented. Survey participants that rated utilization of communication channels as Very Beneficial describe communications that were clear and direct. They also describe effective use of multiple communication channels and collaborative discussions that enabled efficient resolution of issues. The Division of Hematology had the 2nd highest percentage of responses among the top 5 CDER Divisions that rated their utilization of communication channels as Somewhat Beneficial (54%) and had the 2nd highest percentage of respondents that rated communication channels as Not Very Beneficial (4%). Survey participants cited lack of responsiveness and inability to engage in productive dialogue to resolve issues as reasons for lower performance ratings. When we examine specific communication channels, Hematology had the 2nd highest percentage of survey participants that rated combined formal meetings (Type B, Type C, and other in-person formal meetings) as Very Beneficial (65%) among the top 5 CDER Divisions. We do not have enough responses to discuss trends for other individual communication channels at this time. Beneficial Utilization of Communication Channels
“(During In-Person Meeting) Questions asked were specific and detailed. FDA provided direct responses that provided clarity and direction.”
“FDA provided clear feedback during scheduled phone call.” Beneficial Utilization of Communication Channels to Resolve Issues
“FDA communicated issues about starting dose and study design by email – after initial teleconference to clarify issues and submission of revised proposal, had a productive teleconference and worked out a revised study design that met everyone’s needs – helped to have FDA clinical reviewers with clear development experience.”
“Very responsive discussion (via email) regarding the safety signal observed.” “General agreement reached on patient population, primary endpoint, important
parameters for trial design, and planned size of the overall safety database (at EOP2).”
40

“We reached agreement on key aspects of the study design. It was a collaborative discussion (at EOP2).”
Room for Improving Utilization of Communication Channels
“Lack of opportunity for dialogue during hold meetings.” “A response was not received (Formal Letter) until the final protocol was submitted.” “The division has changed their process for creating minutes of meetings. They have
gone from generating the minutes during the meeting to doing them post-meeting. This has resulted in substantially increased times to receive final meeting minutes.
Room for Improving Utilization of Communication Channels to Resolve Issues
“(Pre-IND meeting) CMC reviewer was not informative and ultimately led to a clinical hold.”
“Telecons regarding clinical hold requested by FDA were too short and communication was one way. Time for a two way dialogue would have been very beneficial.”
41

CDER Division of Metabolism and Endocrinology Products
34 programs under review 31 phase-specific journals
A plurality of the clinical program journals within the Division of Metabolism and Endocrinology Products provide feedback on the Phase 3 stage of development (39%). Participants also submitted phase-specific journals about Pre-IND (19%), Phase 1 (16%), and Phase 2 (26%). OVERALL COMMUNICATIONS Overall communication ratings for the Division of Metabolism and Endocrinology Products were a mixed bag. Among the top 5 CDER Divisions represented, the Division of Metabolism and Endocrinology had the 3rd highest percentage of respondents rating their overall communications as Very Beneficial (44%) but also tied with the Division of Gastroenterology and Inborn Error Products for the highest percentage ranking communications as Not Very Beneficial (19%). Survey participants that rated overall communications favorably described pragmatic review teams and communications that provided clear and constructive information that helped advance clinical development programs. Survey participants cited inconsistent feedback and delays in obtaining responses as reasons for lower performance ratings. Beneficial
“In general, the review team and the leadership take a very pragmatic approach to development, balancing the need for sound data on which to base decisions with the importance of ensuring the studies are feasible.”
“Consistently provided clarification of what was needed to reach agreement and move program forward.”
“Provided clarity on path forward.” Room for Improvement
“Timeliness of responses was problematic.” “FDA comments within the different divisions were not consistent.”
REGULATORY PROJECT MANAGER The Division of Metabolism and Endocrinology had the 3rd lowest percentage of respondents ranking interactions with their Regulatory Project Manager (RPM) as Very Beneficial (50%) among the top 5 CDER Review Divisions represented. Forty-four percent of participants rated their interactions as Somewhat Beneficial and 6% rated them as Not Very Beneficial (the 3rd highest percentage among the top 5 CDER Divisions analyzed). Beneficial
“Our RPM is easily accessible and provides solid feedback and guidance on ensuring a smooth review process. Very knowledgeable and good communicator.”
“Willingness of FDA Regulatory Project Manager to email copies of FDA letters being sent by post was highly appreciated.”
42

Room for Improvement “Project Manager was often unable to be reached or did not reply to emails or phone
calls.” “Our previous RPM was aloof and difficult to reach and was not diligent with following
up.” “Project manager generally had to be called or e-mailed more than once to get a
response.” COMMUNICATION CHANNELS AND ISSUE RESOLUTION Among the top 5 CDER Review Divisions, Metabolism and Endocrinology had by far the lowest percentage of responses that rated utilization of communication channels (emails, unscheduled phone calls, scheduled phone calls, formal letters, and in-person meetings) as Very Beneficial (28%). The Division of Metabolism and Endocrinology had the highest percentage of responses that rated communication channels as Somewhat Beneficial (61%) and Not Very Beneficial (10%) among all the Centers and Review Divisions analyzed. Survey participants that rated utilization of communication channels favorably described effective use of multiple communication channels to obtain constructive and proactive feedback, communications that were clear, and the ability to engage in scientific dialogue as reasons for positive performance ratings. Survey participants cited lack of responsiveness, inconsistent feedback, and FDA changing positions as reasons for lower performance ratings. When we examine specific communication channels, Metabolism and Endocrinology had the lowest percentage of survey participants that rated their combined formal meetings (Type B, Type C, and other in-person formal meetings) as Very Beneficial (53%) and the highest percentage that rated them as Not Very Beneficial (11%) compared to other CDER Review Divisions analyzed. We do not have enough responses to discuss trends for other individual communication channels at this time. Beneficial Utilization of Communication Channels
“FDA listened with great interest, asked good questions and provided feedback on path forward (In-person Meeting).”
“Ability to have a live discussion to be able to ask clarifying questions provides a significant benefit.”
“Provided multiple opportunities for discussion prior to start of trial - FDA requested sponsor submit protocol and SAP for review and comment prior to initiating trial – contacted sponsor w/in 2 weeks and provided opportunity to meet with FDA in 5 days; at end of meeting FDA requested an additional teleconference to discuss path forward.”
Beneficial Utilization of Communication Channels to Resolve Issues
“Feedback on interpretation of data was helpful and provided opportunity to discuss data and expectations and reach an understanding of a path forward.”
“Key agreements reached involved the entry criteria (for a condition with a complicated diagnosis), sample size and duration of the trials needed to support approval for chronic condition.”
“FDA provided clear feedback and opinions on the trial design and objectives agreement regarding trial design.”
43
Room for Improving Utilization of Communication Channels “FDA was not very responsive to unscheduled phone calls and e-mails however
responses, once received, were helpful.” “There were multiple rounds of discussion and written feedback; when we were able
to get on the phone it was much easier to resolve our issues.” “Sometimes FDA did not respond to the emails which had questions.”
Room for Improving Utilization of Communication Channels to Resolve Issues
“Agreement and advice received from agency during EOP2 meeting changed significantly after completion of the pivotal study.”
“The Division was initially not willing to engage in early discussions on pediatric development plan, which was problematic reconciling with requirements in EU to initiate the pediatric program.”
“Agency responses related to clinical pharmacology questions were quite delayed.”
44

CDER Division of Gastroenterology and Inborn Error Products
38 programs under review 31 phase-specific journals
Pre-IND journals make up a plurality (32%) of the phase-specific feedback about the Division of Gastroenterology and Inborn Error Products. Phase 2 (23%) and Phase 3 (26%) were evenly represented in the survey, while Phase 1 had the fewest responses (19%). OVERALL COMMUNICATIONS The CDER Division of Gastroenterology and Inborn Error Products had the 2nd lowest percentage of survey participants rating overall communications as Very Beneficial (38%) among the top 5 CDER Review Divisions represented. The Division of Gastroenterology and Inborn Error Products had the highest percentage of respondents rate their overall communications as Not At All Beneficial (12%) and tied for the highest percentage rating them as Not Very Beneficial (19%) compared to all Centers and Review Divisions analyzed. Comments from survey participants who rated overall communications as Very Beneficial describe overall interactions with FDA as collaborative and responsive as well as specific communications that were timely, clear, and helpful in setting expectations and proactively identifying issues. Comments from survey participants who gave unfavorable ratings describe communications that were delayed and inconsistent, as well as a general difficulty reaching agreement on scientific issues as common reasons for lower performance ratings. Beneficial
“Division is very responsive and collaborative.” “No delays caused by FDA.” “FDA provided important information about general concerns that needed to be
addressed to support clinical development.” “FDA did not provide detailed input on proposed clinical trial design but made us
aware of specific concerns that needed to be addressed in the clinical development program.”
Room for Improvement
“Designation as combination product caused significant delays.” “FDA changing their mind on primary endpoint; not accepting science based
rationales; not understanding the indication and challenges.” “Our review division does not seem to understand the challenges of developing drugs
for rare diseases. They also have changed their advice to us on major issues - which has been challenging to us. They do not seem to appear to understand the indications they are in charge of and do not read our briefing documents completely.”
“FDA not current on some aspects of their own guidance. Subsequently, lack of dialogue to find a pragmatic solution.”
45
REGULATORY PROJECT MANAGER Survey participants in the Division of Gastroenterology and Inborn Error Products did not consistently provide rankings for their Regulatory Project Managers (RPMs). Preliminary results show that ratings for Gastroenterology and Inborn Error RPMs were rated the 2nd highest among the 5 CDER Review Divisions analyzed (57% Very Beneficial). No survey respondent rated interactions with their RPM as Not At All Beneficial, but 36% rated their RPM as Somewhat Beneficial and 7% said Not Very Beneficial. Survey participants that rated their interactions with their RPM as Very Beneficial mainly commented on responsiveness. Survey participants that cited room for improvement described difficulty in communicating with the RPM and issues obtaining responses from their review team as the reasons for lower performance ratings. Beneficial
“Very responsive to emails and phone calls.” “Our new RPM is fantastic - very communicative, pleasant and appears to try to
answer questions as best as he can.” “Our new RPM is great – he responds immediately to questions and provides
information.” Room for Improvement
“Working with project manager is typically efficient but can’t reach members of the review team for specific questions where direct communication would be beneficial.”
“RPM very friendly and responsive but not empowered to act without feedback from review team.”
“Very little communication; never picked up the phone and slow to respond to email and when the RPM did, it was not helpful.”
COMMUNICATION CHANNELS AND ISSUE RESOLUTION Among the top 5 CDER Review Divisions represented, the Division of Gastroenterology and Inborn Error Products had the 2nd highest percentage of responses rating utilization of communication channels as Very Beneficial (54%). Survey participants that rated utilization of communication channels as Very Beneficial described communications that were timely and constructive. They also described interactions that were collaborative and enabled substantive feedback. The Division of Gastroenterology and Inborn Error Products had the highest percentage of responses that rated utilization of communication channels as Not At All Beneficial (9%). Reasons given for these ratings include communications that lacked clarity and/or required multiple rounds of communications to obtain answers to questions. Respondents also described situations where FDA positions changed and issues that were not identified in a timely manner. When we examine ratings of specific communication channels, 62% of Gastroenterology and Inborn Error respondents rated combined formal meetings (Type B, Type C, and other in-person formal meetings) as Very Beneficial. This was the 3rd highest percentage among the top 5 CDER Review Divisions represented. Several survey participants that rated in-personal formal meetings as Very Beneficial described their meetings as the most productive communication channel.
46

We do not have enough responses to discuss trends for other individual communication channels at this time. Beneficial Utilization of Communication Channels
“Responded to emails promptly.” “Scheduled phone calls allowed us to have a conversation with the Reviewers to
better understand their positions and explain our rationale.” “The review division was quite collaborative at the in-person meetings (e.g. stayed
over time).” “Received feedback on proposed development program.”
Beneficial Utilization of Communication Channels to Resolve Issues “Comments regarding non-clinical studies have been helpful.” “FDA very responsive to formal request for feedback regarding IND-enabling toxicity
study design.” “Very open dialogue between FDA and sponsor - very clear guidance given on clinical
trial endpoints for Phase 2b and Phase 3 trials in Crohn's disease.” Room for Improving Utilization of Communication Channels
“Formal written responses have been unclear and required follow up for clarification.” “Did not provide clarity or reasons for information requested and no feedback was
provided at the end of the scheduled call.” “6 month – 1 year delay incurred due to no guidance from FDA during Pre-IND
meeting about combination product designation which required substantially more information.”
“Getting time with appropriate people difficult – takes a long time to get a meeting.” Room for Improving Utilization of Communication Channels to Resolve Issues
“It took two meetings and several correspondences/communications to reach consensus.”
“Clinical hold issues were not identified by FDA in pre-IND meeting – hold issues arose.”
“(Previously) we met to discuss our Phase 3 plan and our primary endpoint was agreed upon in writing. Then in the EOP2 meeting they told us this was not acceptable and we would need to use an outcome that would take us years to develop. They were also not aligned as a department…”
47
CBER
72 programs under review 49 phase-specific journals
Half of CBER clinical programs in this survey are being reviewed by the CBER Division of Cellular and Gene Therapies (n=36). The remaining clinical development programs (n=36) are being reviewed by the following CBER Divisions: Bacterial, Parasitic, and Allergenic Products; Blood Applications; Hematology; Human Tissues; Vaccines and Related Product Applications; and Viral Products. CBER participants representing the Division of Cellular and Gene Therapies also submitted half of the Center’s phase-specific journals (n=25). Across all CBER Divisions, Pre-IND (37%) and Phase 1 (24%) journals were the most common, followed by Phase 2 (18%) and Phase 3 (20%). OVERALL COMMUNICATIONS While the number of CBER clinical program journals (n=49) is far less than the total number of CDER journals (n=397), it is worth noting that CBER participants rated their overall communications with FDA significantly higher than any other Center or Review Division (60% Very Beneficial). No survey participant rated overall communications with CBER as Not At All Beneficial.
Division of Cellular and Gene Therapies: The Division of Cellular and Gene Therapies had the 3rd highest ratings for overall communications (50% Very Beneficial) compared to the top 5 CDER Review Divisions represented.
Comments from survey participants that rated overall communications favorably describe interactions that were collaborative and communications that were specific and focused on proactively identifying or resolving issues. CBER had the lowest percentage of participants rate their overall communications as Somewhat Beneficial (35%) and Not Very Beneficial (5%) as compared to CDER and CDRH. Delays in responses and inability to discuss scientific issues with review team were common reasons cited for low performance ratings.
Division of Cellular and Gene Therapies: The Division of Cellular and Gene Therapies had the 2nd highest percentage of respondents rate their interactions as Somewhat Beneficial (45%) compared to the top 5 represented CDER Review Divisions. No Cellular and Gene Therapies survey participant rated their overall communications with the Division as Not At All Beneficial.
Comments from survey participants cite delays and issues reaching understanding and/or agreement on scientific issues as reasons for low performance ratings. Beneficial Division of Cellular and Gene Therapies
“FDA clear in communications and quite responsive” – Cellular and Gene Therapies “FDA was responsive and willing to collaborate” – Cellular and Gene Therapies “Sense of partnership in discussions without crossing boundaries” – Cellular and
Gene Therapies “FDA always available and willing to help” – Cellular and Gene Therapies
48

Other CBER Divisions “Efficient and on-point” – Vaccines and Related Product Applications “Very collaborative, focused on science of product and patient safety” – Vaccines and
Related Product Applications “Interactions with FDA anticipated new elements that would need attention as
sponsor moved forward with development” – Vaccines and Related Product Applications
“All communications have been beneficial with this Division” – Viral Products “A lot of communication and interactions” – Viral Products
Room for Improvement Division of Cellular and Gene Therapies
“Slow to respond to requests to discuss some of their concerns” – Cellular and Gene Therapies
“Length of time it can take to get a response to an issue” – Cellular and Gene Therapies
Other CBER Divisions “FDA's initial lack of understanding technology” – Viral Products
REGULATORY PROJECT MANAGER We did not consistently receive ratings or comments on Regulatory Project Managers (RPMs) from CBER clinical development programs. Preliminary results show that CBER had the highest percentage of respondents rate interactions with their RPM as Very Beneficial (70%) compared to CDER respondents (53%).
Division of Cellular and Gene Therapies: The Division of Cellular and Gene Therapies had the highest ratings for interactions with the RPM (69% Very Beneficial) compared to the other top represented Review Divisions.
The positive RPM comments from CBER participants cite the ability to work with RPM to obtain feedback and proactive identification of issues. Commenters cite a need for multiple communications to obtain necessary information and general lack of responsiveness as reasons for lower performance ratings. Beneficial Division of Cellular and Gene Therapies
“The regulatory project manager was able to provide information or direct contact with the appropriate FDA review team members to address any questions or issues.” – Cellular and Gene Therapies
Other CBER Divisions
“Effective in providing feedback to questions and making sponsor aware of FDA needs” – Vaccines and Related Product Applications
“Our project manager has been very responsive and helpful.” – Vaccines and Related Product Applications
Room for Improvement Division of Cellular and Gene Therapies
“Getting a timely response from RPMs to email or phone contacts has become a significant problem” – Cellular and Gene Therapies
“One issue that comes up is that we have the same RPM for multiple programs, many of which are progressing at same time, More often than not, we do not receive
49

timely responses from the RPM when contacted by email or phone. It requires multiple contacts to obtain a response, which is frustrating. We recognize that in general FDA staff are under resourced and workload issues can significantly slow down a sponsor's ability to progress its program, particularly since there is no FDA policy for timeframe to respond to informal inquiries” – Cellular and Gene Therapies
“In general, the reviewers are helpful, but the regulatory project managers who arrange meetings, document discussions are not responsive in a timely manner, or don't accurately document discussions which is frustrating” – Cellular and Gene Therapies
Other CBER Divisions
“Difficult to reach and unresponsive” - Vaccines and Related Product Applications COMMUNICATION CHANNELS AND ISSUE RESOLUTION CBER had a significantly higher percentage of responses that rated utilization of communication channels (email, unscheduled phone calls, scheduled phone calls, formal letters and in-person meetings) as Very Beneficial (83%) compared to CDER (52%). No survey participant within CBER rated utilization of communication channels as Not Very Beneficial and only 1% said Not At All Beneficial.
Division of Cellular and Gene Therapies: The Division of Cellular and Gene Therapies had the highest percentage of responses that rated utilization of communication channels Very Beneficial (85%) as compared to all of the other top represented Review Divisions.
We did not have enough responses to comment on trends for individual communication channels. However, those that rated utilization of communication channels as Very Beneficial described communications that were responsive, clear, and helpful in answering questions. They also describe interactions that were collaborative, balanced, and helpful in resolving simple and complex issues. CBER had the lowest percentage of respondents that rated utilization of communication channels as Somewhat Beneficial (16%). Within the Division of Cellular and Gene Therapies, only 12% of respondents rated utilization of communication channels as Somewhat Beneficial. Reasons cited for these lower performance ratings include delays in obtaining responses to questions, inconsistent feedback, and inability to discuss and/or resolve scientific issues. Beneficial Utilization of Communication Channels Division of Cellular and Gene Therapies
“FDA was very responsive to request for End of Phase 1 meeting” – Cellular and Gene Therapies
“Overall communication for our specific programs, as well as communication on more general topics related to the field of gene therapy (in particular during events sponsored by FDA) has been very helpful to answer our questions and provide general guidance.” – Cellular and Gene Therapies
“Clear feedback in written format, followed by productive conversation to gain clarity.” – Cellular and Gene Therapies
“Generally, always helpful to discuss with reviewers study designs given complexities that are difficult to convey in writing” – Cellular and Gene Therapies
50

Other CBER Divisions “Meeting pre-reads and questions submitted by email were resolved and no
scheduled meeting required” – Vaccines and Related Product Applications “Discussions were always fair with give and take on both sides. No significant
unresolved issues” – Vaccines and Related Product Applications “All issues resolved via email and scheduled calls” – Vaccines and Related Product
Applications “Pre-IND meeting was productive and informative” – Viral Products
Beneficial Utilization of Communication Channels to Resolve Issues Division of Cellular and Gene Therapies
“Comments on required protocol changes were helpful” – Cellular and Gene Therapies
“Obtaining answers to issues that came up (Very Beneficial)” – Cellular and Gene Therapies
“Helpful advising on development of complicated assays required for this project” – Cellular and Gene Therapies
“FDA needed clarity on intent of a proposed interim analysis and allowed us to clarify” – Cellular and Gene Therapies
Other CBER Divisions
“All issues resolved via email and scheduled calls” – Vaccines and Related Product Applications
“Email communications about design of toxicology very helpful” – Viral Products “Discussions on trial design were helpful. Questions from FDA on CMC issues were
reflective of concern that we were aware of upcoming expectations (i.e. potency assays).” – Vaccines and Related Product Applications
Room for Improving Utilization of Communication Channels Division of Cellular and Gene Therapies
“There was no discussion of study design specifics (EOP2)” – Cellular and Gene Therapies
“The final version of the meeting minutes were nearly identical to draft version received, despite fact extensive discussion and agreement occurred, which was documented in internal company minutes (submitted in advance of receiving FDA "official" minutes). Receiving FDA minutes that do not reflect the actual discussion, calls in the question of what the purpose of having a meeting with the FDA achieves.” – Cellular and Gene Therapies
“We requested a face-to-face meeting, but were only given a written response only meeting. The comments received were useful, but there was no chance to discuss” – Cellular and Gene Therapies
Other CBER Divisions
“We have conducted 2 Phase 3 trials and submitted our BLA with the expectation based on communication with FDA that our safety database would be adequate. We filed our BLA and received a CRL because the database was too small. We are conducting a third Phase 3 trial” – Vaccines and Related Product Applications
“We have used several methods to get input into our Phase 3 trial design. We sent a draft protocol and received comments from FDA after 3 months. We have asked questions via email with some questions being answered but others required a scheduled phone call. The biggest problem has been that we thought we had an agreement on an important aspect of the study but months later FDA reversed its opinion.” – Vaccines and Related Product Applications
51
“FDA delayed the first FDA stating they would not approve the IND. Then after 1 year FDA called and said they were ready but we were not at that time and funding became an issue” – Viral Products
Room for Improving Utilization of Communication Channels to Resolve Issues Division of Cellular and Gene Therapies
“Company was forced to design a study at Agency's insistence that was unlikely to be successful” – Cellular and Gene Therapies
“FDA clinical reviewers had strong ideas as to appropriate endpoints and duration which were not completely aligned with company and/or key opinion leaders” – Cellular and Gene Therapies
Other CBER Divisions
“While interactions have been somewhat beneficial, we have received communications that are not science based or it seems the review division did not understand the science behind our proposals.” – Vaccines and Related Product Applications
“Ongoing discussions about a primary endpoint that meets all criteria for a primary endpoint which they tell us is only exploratory (Not Very Beneficial)” – Vaccines and Related Product Applications
52
CDRH: Preliminary Results
17 programs under review 19 phase-specific journals
CDRH was the primary Center reviewing just 4% of clinical development programs in the survey data set. CDRH participants also accounted for 4% of the clinical program journals submitted. A plurality of CDRH journal submissions were in the Phase 3 stage of development (42%). The remaining journals were spread across Pre-IND (26%), Phase 1 (16%), and Phase 2 (16%). OVERALL COMMUNICATIONS We do not have a high number of CDRH clinical development programs represented. Preliminary results indicate that CDRH has a lower percentage of survey participants that rated their overall communications with FDA as Very Beneficial (41%) compared to CDER and CBER. It also has the highest percentage of participants rating overall communications as Somewhat Beneficial (47%) and Not Very Beneficial (12%). Survey participants that rated their overall communications favorably described interactions that were collaborative and responsive. Survey participants cited a lack of preparation by FDA before in-person meetings and inability to effectively discuss complex issues as reasons for lower performance ratings. Beneficial
“FDA was very timely in responding to the request for information for a Regulatory Project Manager.”
“CDRH review division was collaborative, responsive and seemed genuinely interested in helping us advance our program.”
“Our program started under CDER and was subsequently shifted to CDRH. The CDRH review division was significantly more responsive and helpful at addressing questions in an informal manner. This was very helpful and allowed for a collaborative working relationship with the division.”
“FDA was responsive to our questions and satisfied to be contacted ahead of any application.”
“CDRH is more collaborative and available on an informal basis compared to CDER.”
Room for Improvement “FDA not well prepared for in-person meetings, had not read pre-meeting materials.” “FDA deferred key information requests sponsor identified prior to in-person
meeting.” “Email and written correspondence were generally not effective. Issues are
frequently too complex to resolve in back and forth emails and letters. Also very inefficient.”
REGULATORY PROJECT MANAGER CDRH survey respondents did not consistently rate or comment on interactions with their Regulatory Project Manager (RPM). Preliminary data shows that 50% of CDRH participants rated their interactions as Very Beneficial (lower than CDER and CBER), 42% rated them as Somewhat Beneficial (higher than CDER and CBER), and 8% rated them as Not At All Beneficial (higher than CDER and CBER).
53
Beneficial “Project manager made efforts to expedite meetings and decision-making.”
Room for Improvement
“Eager to assist but held little decision-making authority – most of time spent was as a go-between with sponsor and reviewers.”
“Project manager was helpful but had difficulty getting access to actual reviewers for timely discussion on key protocol design issues.”
“No answer to email.” COMMUNICATION CHANNELS AND ISSUE RESOLUTION CDRH responses rating utilization of communications were similar to CDER, with 49% rating them as Very Beneficial, 43% as Somewhat Beneficial, 4% rating them as Not Very Beneficial, and 4% as Not At All Beneficial. When we examine preliminary results of combined ratings for Type B, Type C, and other in-person meetings, CDRH has a similar percentage of responses rating them as Very Beneficial (71%) when compared to CDER and CBER (65% and 69%, respectively). Survey participants commented that while in-person meetings were constructive and enabled scientific dialogue, emails were not helpful in obtaining feedback. We do not have enough responses to discuss individual communication channels at this time. Beneficial Utilization of Communication Channels
“Face-to-face meetings allowed more in-depth dialogue and better opportunities to assure agreement on key issues versus short teleconferences and written communications.”
“Unless meeting was in person or by formal FDA letter – very little constructive information is conveyed – Face to face meetings were most helpful.”
Beneficial Utilization of Communication Channels to Resolve Issues
“FDA helpful in providing constructive input on protocol design and sample size requirements for Ph 1 study.”
“(EOP2) Meeting helped establish concurrence on protocol design and primary endpoints.”
“DGEIP was very helpful in guiding the program with respect to primary and secondary endpoints for Phase 2b and Phase 3.”
“Type A meeting ultimately resulted in removal of clinical hold.” Room for Improving Utilization of Communication Channels
“Email was not very helpful. Unless the correspondence was a formal FDA letter, it seemed that our reviewers were unwilling to commit to key decisions via email. This resulted in further delays while the company waited to receive actual letter.”
Room for Improving Utilization of Communication Channels to Resolve Issues
“HFE discussions on biologic/device combination were very challenging. Received different input from CDRH, OSE and DMEP at different times, and uncertain how to address FDA concerns. Was not clear what standard was for demonstrating safe use and what an acceptable use error profile was, and whether results could be considered to be at level of residual risk or not. Difficulty reconciling clinical safe use vs. HFE safe use.”
54

“All (clinical hold) discussions were subject to 30 and 60 day clocks – created delays.”
“Needed help on detailed requirement on device approval pathway.”
55

APPENDICES: COMPREHENSIVE LIST OF ADDITIONAL COMMENTS
APPENDIX 1: CDER ADDITIONAL COMMENTS Below is a comprehensive list of additional comments from survey respondents with clinical development programs being reviewed by CDER. For comments from the top 5 CDER Review Divisions (Oncology, Neurology, Hematology, Metabolism & Endocrinology, and Gastroenterology & Inborn Error), see Appendices 3-7. OVERALL COMMUNICATIONS Beneficial
“Responses were timely and helpful.” – Cardiovascular and Renal Products “Thorough, complete, clear.” – Cardiovascular and Renal Products “The FDA has been very responsive, provided thorough comments and guidance.”
– Anesthesia, Analgesia, and Addiction Products “Constructive comments were received.” – Bone, Reproductive and Urologic Products “FDA provided clear guidance and shared its current thinking of drug development
for the disease area.” – Pulmonary, Allergy, and Rheumatology Products “Communications were straightforward.” – Psychiatry Products “FDA was very helpful and clearly answered our questions. We were able to cancel
our teleconference with FDA because they so clearly answered our questions in their written response.” – Dermatology and Dental Products
“Agency provided very specific feedback regarding clinical study design.” – Dermatology and Dental Products
“Constructive feedback.” – Cardiovascular and Renal Products “Timely preliminary feedback.” – Cardiovascular and Renal Products “Interactions were thorough, scientifically driven and in a collaborative atmosphere.”
– Cardiovascular and Renal Products “Feedback useful and clarifying.” – Cardiovascular and Renal Products “Responses and feedback were timely.” – Cardiovascular and Renal Products “Proactive in reaching out to sponsors.” – Cardiovascular and Renal Products “Interactions were productive and collaborative.” – Cardiovascular and Renal
Products “FDA did not cause any delays.” – Anti–Infective Products “Good guidance on new programs (QIDP) and in the revised guidance for antibiotic
development.” – Anti–Infective Products “The division has been very responsive.” – Anti–Infective Products “We have multiple INDs but with the same compound. The FDA has provided us with
guidance to streamline our filings.” – Anesthesia, Analgesia, and Addiction Products “More timely feedback would be helpful.” – Bone, Reproductive and Urologic Products “Timely response (response in 3 business days before due date).” – Pulmonary,
Allergy, and Rheumatology Products “FDA is generally responsive and guidance provided is generally helpful.”
– Pulmonary, Allergy, and Rheumatology Products “FDA comments are generally beneficial.” – Pulmonary, Allergy, and Rheumatology
Products “FDA’s comments in response to questions were generally adequate to allow us to
proceed. Risks were identified and incorporated into other internal decision-making elements.” – Pulmonary, Allergy, and Rheumatology Products
“The interactions with the FDA Division of Pulmonary, Allergy and Rheumatology Products, for this particular development program, have been uncharacteristically challenging...there is a perception on our part that certain reviewers are lacking any objectivity in their assessment of the information we have provided.” – Pulmonary, Allergy, and Rheumatology Products
57

“Most communications were straight forward and no issues noted by FDA or sponsor.” – Psychiatry Products
“FDA comments are generally helpful.” – Dermatology and Dental Products “Reviewers were reasonable and responsive.” – Pulmonary, Allergy, and
Rheumatology Products “FDA is responsive and helpful.” – Transplant and Ophthalmology Products “FDA responsive.” – Transplant and Ophthalmology Products “Agency provided very specific feedback regarding clinical study design.” –
Dermatology and Dental Products “They let us proceed; raised some other nonclinical issues without a clinical hold and
were good about explaining why they were insisting on certain aspects of their requirements.” – Cardiovascular and Renal Products
“Following the pre-IND meeting, FDA had some non-hold comments that were helpful and we have made submissions to address those points. They were constructive and showed an openness to evaluating the matter. They were also very rapid in their responses, even though these were not clinical hold issues.” – Cardiovascular and Renal Products
“Face-to-face meetings and telecons have been more beneficial than written responses only, since the rationale behind responses can be discussed.” – Cardiovascular and Renal Products
“Very collaborative and productive communications. FDA also provided helpful feedback and guidance to improve the Phase III program. Providing preliminary comments 10 days in advance of the meeting was very helpful. Offering guidance to improve the program was also helpful. FDA was open to alternative proposals.” – Cardiovascular and Renal Products
“Allowed alignment on key aspects of Phase 3 study; they also provided good feedback on their expectations. Endpoints, statistics, study operations (dropouts, DMC)” – Cardiovascular and Renal Products
“FDA communications during Phase 3 were beneficial. FDA was willing to work with us on designing streamlined trials that would be adequate for registration. FDA End of Phase 2 meetings were very helpful in designing the Phase 3 studies to meet FDA's needs for registration.” – Cardiovascular and Renal Products
“The dialogue was open and FDA was being as helpful as they could with the design of the study. They were also prompt in replying and agreeable to telecons.” – Cardiovascular and Renal Products
“FDA indicated they were conducting outside analysis to verify the analyses we were sending them. In the end the Agency sponsored a scientific meeting with the NKF that addressed this issue in a comprehensive manner. Subsequent to that meeting, we received approval for our new endpoint.” – Cardiovascular and Renal Products
“Interactions with Analgesia Division have been very collaborative.” – Anesthesia, Analgesia, and Addiction Products
“Provided guidance on clinical study design and requirements” – Anesthesia, Analgesia, and Addiction Products
“They were responsive to our questions in a timely manner.” – Pulmonary, Allergy, and Rheumatology Products
“We received FDA comments on the protocol regarding the bridging strategy…The response to our proposed strategy to bridging the two devices is clear.” – Pulmonary, Allergy, and Rheumatology Products
“FDA is generally responsive and guidance provided is generally helpful.” – Pulmonary, Allergy, and Rheumatology Products
“FDA comments are generally beneficial.” – Pulmonary, Allergy, and Rheumatology Products
58

“Assistance on compassionate use was very helpful.” – Pulmonary, Allergy, and Rheumatology Products
“Beneficial interactions included written agreements, SPA process, QIDO designation.” – Anti-Infective Products
“The division has been very responsive.” – Anti-Infective Products “FDA very responsive to our requests” – Anti-Viral Products “FDA gave clear expectations in pre-IND communications about what would be
needed for the IND enabling study and into Phase 2. The communication was quite comprehensive and helpful although we have a few points that needed clarification.” – Dermatology and Dental Products
“Interactions on this program have thus far been quite helpful.” – Dermatology and Dental Products
“We had one teleconference to discuss an IND Safety Report. The reviewers asked good questions and listened to our thoughts. They were reasonable in their review and we were able to come to agreement on a path forward. We also had a breakthrough designation request denied. They were very helpful in their response, sharing their thoughts transparently and we will be able to reapply once we have further data.” – Anesthesia, Analgesia, and Addiction Products
“The discussion was very collaborative and supportive. The FDA review team was focused on supporting the program to be able to move it forward- completely aligned with our goal. Disagreements were put on the table with the objective to "resolve to be able to move forward with development”.” – Anesthesia, Analgesia, and Addiction Products
“We were able to get some issues resolved quickly” – Dermatology and Dental Products
“After being granted Breakthrough Designation, the picture changed dramatically. We were assigned senior staff, have had very collaborative discussions and have been offered rapid turnaround on any questions that we may have.” – Anesthesia, Analgesia, and Addiction Products
“FDA comments and meeting discussion was timely and clear” – Dermatology and Dental Products
Room for Improvement
“The FDA didn't highlight the key clinical issue prior to review.” - Pulmonary, Allergy, and Rheumatology Products
“Team received inconsistent comments and feedback from the Agency throughout the review process: different levels of management provided different comments.” – Transplant and Ophthalmology Products
“FDA did not provide rationale for positions.” – Transplant and Ophthalmology Products
“We did not feel that FDA was willing to engage in any substantial dialogue via email without formal communication. Emails were not helpful other than as a means of communication.” – Anti-Viral Products
“Reviewers did not want to be bothered to provide feedback.” – Dermatology and Dental Products
“FDA changed expectations btw pre-IND meeting and IND application review thus delaying Ph1, but, forthcoming in providing longer term expectations.” – Anti-Viral Products
“Correspondence required follow-ups (not clear).” – Anti-Viral Products “Feedback and guidance has been variable and did not always follow prior precedent
in this space.” – Anesthesia, Analgesia, and Addiction Products “Inconsistent – hard to predict how they will view issues and interpret data.” –
Anesthesia, Analgesia, and Addiction Products
59
“3-6 month delay due to waiting for FDA feedback, more information requested by FDA and FDA changing positions on what was required.” – Anesthesia, Analgesia, and Addiction Products
“Anyone dealing with this division of the FDA will find them to be elusive, deceptive and in violation of the FDA governing laws.” – Anesthesia, Analgesia, and Addiction Products
“Provided comment to protocol design but did not respond to sponsor response.” – Pulmonary, Allergy, and Rheumatology Products
“Key issue was not clearly communicated by review division.” – Pulmonary, Allergy, and Rheumatology Products
“Program was required to change Divisions (Neurology to Psychiatry) but no official communication regarding change was provided by either division.” – Psychiatry Products
“Inconsistencies in FDA interactions caused delays in the program.” - Transplant and Ophthalmology Products
“Additional rationale and perspective from the Division would be helpful. - Transplant and Ophthalmology Products
“It took several weeks after contacting the Division to respond to our questions about our pre-IND meeting request. Once requested, our Pre-IND meeting could not be scheduled in within the 60 days of our request but rather around 100 days. Communications with the Division can best be described as sluggish.” – Anesthesia, Analgesia, and Addiction Products
“Change of requirements” – Bone, Reproductive, and Urologic Products “Did not respond to our response.” – Pulmonary, Allergy, and Rheumatology
Products “Request regarding pediatric indications seems slower than topics on adult
indications.” – Pulmonary, Allergy, and Rheumatology Products “The recommendation for alternative approaches is not clear.” – Pulmonary, Allergy,
and Rheumatology Products “We provided our response, however did not hear back from the Agency.”
– Pulmonary, Allergy, and Rheumatology Products “Interactions with the Agency have at times very disappointing.” – Pulmonary,
Allergy, and Rheumatology Products “Further discussion on endpoints would have been helpful in a formal meeting setting
as no formal FDA guidance is available.” – Pulmonary, Allergy, and Rheumatology Products
“While we received adequate general advice concerning our proposed clinical development program, the feedback obtained during our Pre-NDA meeting was much more pointed and indicated very little of the flexibility we had been given to make certain decisions about our Phase 3 program, were actually being translated into a positive assessment of the Phase 3 data or even some of the underlying principles around the use of the class of drug in an asthmatic population.” – Pulmonary, Allergy, and Rheumatology Products
“The lack of specificity around some elements of the Phase 3 program that were deeply troubling the FDA at the time of the EoP2 meeting and subsequent Type C meeting, were not clearly communicated as substantial risks to the clinical development program.” – Pulmonary, Allergy, and Rheumatology Products
“The FDA didn't highlight the key clinical issue prior to review.” – Pulmonary, Allergy, and Rheumatology Products
“Pediatric study plan - procedural requirements on amendments, what is required and how it relates to the BLA submission and approval. Request for feedback was sent through formal submission. FDA response has yet to be received.” – Pulmonary, Allergy, and Rheumatology Products
60

“Key issue was not clearly communicated by review division.” – Pulmonary, Allergy, and Rheumatology Products
“It is recommended that FDA reviewers identify themselves, ie which Divisions they are from, before comments are provided to the Sponsor as advice given could be different for drug and device development.” – Pulmonary, Allergy, and Rheumatology Products
“For this particular submission, the Review Division has appeared to be less interested in the actual data that has been developed in Phase 3 and more interested in trying to re-hash some topics that were relevant 10 years ago.” – Pulmonary, Allergy, and Rheumatology Products
“The interactions with the FDA Division of Pulmonary, Allergy, and Rheumatology Products, for this particular development program, have been uncharacteristically challenging...there is a perception on our part that certain reviewers are lacking any objectivity in their assessment of the information we have provided.” – Pulmonary, Allergy, and Rheumatology Products
“Had to deal with earlier changing of the process and guidelines after initial Phase 3 had started” – Anti-Infective Products
“The written and verbal feedback was somewhat beneficial” – Anesthesia, Analgesia, and Addiction Products
“We have tried on several occasions to have verbal discussions. We have offered informal off-the-record type discussion and also requested formal discussions and have had none. It is understandable that the Division personnel are very busy however a discussion could help. We only want to answer their questions and give them all of the information they need. We have gone so far as to submit a Breakthrough Designation Request so that we can get some feedback even if it is in the form of a denial response. We don't see any reason to go through the communications office since that is unlikely to help by adding another layer.” – Anesthesia, Analgesia, and Addiction Products
“Some members of the review team had not read the full package and were unaware of some critical elements of the program. We were able to sort it out with post meeting communication that was efficient and did not result in a delay to the program but it was frustrating nonetheless.” – Dermatology and Dental Products
“Response was clear, but delayed for quite some time. It is not clear whether a consult from the Division was delayed or whether the COA group took a very long time to respond. In the end, we did get a satisfactory response.” – Dermatology and Dental Products
“If FDA had more informal, collaborative discussions with sponsors so that sponsors could understand their thinking on the project, then they wouldn't get so many "futile" requests” – Anesthesia, Analgesia, and Addiction Products
REGULATORY PROJECT MANAGER (RPM) Beneficial
“Easy to communicate with and sought to understand sponsor perspective.” – Cardiovascular and Renal Products
“Very communicative, collaborative, and transparent.” – Anesthesia, Analgesia, and Addiction Products
“Our Regulatory Project Manager is very responsive and the review team provides us timely feedback.” – Psychiatry Products
“Appropriate for what sponsor was requesting.” – Dermatology and Dental Products “Quick to provide feedback and great to work with.” – Cardiovascular and Renal
Products “Extremely responsive and provided timely feedback.” – Cardiovascular and Renal
Products
61

“The PM did a great job of channeling information so that we could have the most productive face to face meeting possible.” – Cardiovascular and Renal Products
“Adequate, responsive, no issues.” – Anti-Viral Products “Somewhat formal and procedure oriented, but helpful in facilitating meetings, etc.,
and quite responsive.” – Anti-Viral Products “Very responsive and clear, easy to speak with.” – Anti-Infective Products “So far, So good.” – Anti-Infective Products “A lot of experience and very responsive.” – Anesthesia, Analgesia, and Addiction
Products “The project manager is very communicative and realistic. He has a collaborative
attitude.” – Anesthesia, Analgesia, and Addiction Products “The Regulatory Project Manager has generally been helpful in scheduling
interactions.” – Anesthesia, Analgesia, and Addiction Products “PM is very responsive to our emails.” – Anesthesia, Analgesia, and Addiction
Products “The PM was very responsive and communicated well by email. We have received a
lot of feedback on our study protocols and analysis plans by the reviewers.” – Anesthesia, Analgesia, and Addiction Products
“Helped improve efficiency.” – Bone, Reproductive and Urologic Products “Very responsive.” – Pulmonary, Allergy, and Rheumatology Products “Appropriate for what sponsor was requesting.” – Pulmonary, Allergy, and
Rheumatology Products “Very responsive and helpful.”– Pulmonary, Allergy, and Rheumatology Products “Excellent communications with the PM since 2014 including those leading up to End
of Phase 2 meeting.” – Psychiatry Products “PM is very responsive to our emails.” – Psychiatry Products “We have received a lot of feedback on our study protocols and analysis plans by the
reviewers.” – Psychiatry Products “Project manager has been excellent and very helpful in facilitating the multiple
meetings, teleconferences, and correspondence throughout the entire process.” – Cardiovascular and Renal Products
“The FDA Regulatory Project Manager is very responsive and collaborative. She provides feedback in a timely manner and is very easy to work with.” – Cardiovascular and Renal Products
“The Cardiorenal Division is responsive. They respond to questions in a timely manner and on occasion have been willing to have informal teleconferences to discuss an issue.” – Cardiovascular and Renal Products
“She’s excellent.” – Anti-Viral Products “Division brought appropriate level and other division participants to discuss plan”
– Anesthesia, Analgesia, and Addiction Products “The Regulatory Project Manager has generally been helpful in scheduling
interactions.” – Pulmonary, Allergy, and Rheumatology Products “Appropriate for what sponsor was requesting.” – Pulmonary, Allergy, and
Rheumatology Products “Feedback received from the four-sided meeting with CDER and CDRH and the
meeting was extremely useful.” – Pulmonary, Allergy, and Rheumatology Products “She’s excellent.” – Anti-Viral Products “She’s responsive and a "straight shooter."” – Anti-Infective Products “Regulatory PM has always been very responsive and cooperative” – Anti-Viral
Products “We have always worked to optimize communications with the Regulatory Project
Managers in DPARP” – Pulmonary, Allergy, and Rheumatology Products
62
“Our previous project manager was very communicative and realistic. He had a collaborative attitude.”– Anesthesia, Analgesia, and Addiction Products
“With Breakthrough Designation we were assigned a new PM. She is fantastic.” – Anesthesia, Analgesia, and Addiction Products
“Overall, interactions have been very beneficial. Responses have been comprehensive and generally clear. We have had some frustration as noted in prior comments, but these issues were resolved expeditiously.” – Dermatology and Dental Products
Room for Improvement
“Somewhat formal and procedure oriented.” – Anti-Viral Products “Not responsive and information not always adequate, not much experience.”
– Anesthesia, Analgesia, and Addiction Products “Always very helpful, responds quickly most of the time. However, other than
logistics (e.g. date/time of meeting) the RPM is often not aware of discussions within the review team.” – Transplant and Ophthalmology Products
“Inept, deceptive…” – Anesthesia, Analgesia, and Addiction Products “Written feedback denied proposed PRO, but written responses did not provide venue
to explore options.” – Pulmonary, Allergy, and Rheumatology Products “[After an initial RPM that was very communicative], the next project manager was
much less communicative.” – Anesthesia, Analgesia, and Addiction Products “Many delays in scheduling meetings, cancellation of scheduled meeting, etc.”
– Anesthesia, Analgesia, and Addiction Products “Although our interactions with the Division overall have gone well and we ultimately
get what we need, our project manager has changed multiple times and getting timely response a challenge at times.” – Dermatology and Dental Products
“Interactions to date have been good, but always formal. Would be nice to be able to have informal or follow-up clarifications that have not been allowed.” – Dermatology and Dental Products
“The project manager changes frequently and isn't terribly responsive.” – Dermatology and Dental Products
SPECIFIC COMMUNICATION CHANNELS Email: Beneficial
“Email good for communication with Project Manager.” – Cardiovascular and Renal Products
“FDA responded in a timely manner to our emails and provided us guidance for submitting carcinogenicity protocols.” – Psychiatry Products
“Emails were timely and helpful in gaining agreement prior to submission of formal amendments.” – Anti-Viral Products
“Response by email facilitated quick response time and minimized delays.” – Anti-Viral Products
“The email was mostly as means of communication with the RPM and also receiving feedback or any questions in a timely manner.” – Anti-Viral Products
“Email is helpful informal communication tool to alert FDA PM of upcoming submissions, plans, and to touch base when not readily available by phone.” – Anti-Viral Products
“Received a timely notification of completion of FDA review – but notification was duplicative with both electronic and paper delivery.” – Anti-Infective Products
“FDA was very responsive to emails regarding placement of non-IND protocols in eCTD structure, QIDP questions specific to indication and Fast Track, and IRB waiver agreement.” – Anti-Infective Products
63

“The email and formal letters have clearly documented our interactions”. – Anesthesia, Analgesia, and Addiction Products
“During IND had a few follow-up questions that were answered easily via email.” – Anesthesia, Analgesia, and Addiction Products
“FDA responded in a timely manner to our emails and provided us guidance for submitting carcinogenicity protocols.” – Anesthesia, Analgesia, and Addiction Products
“Email is useful for straightforward questions and answers. However, there is a limitation on explanation or discussion that can be communicated through email.” – Pulmonary, Allergy, and Rheumatology Products
“Division was responsive to email communications/clarifications on trials designs following EOP2 meeting. Allowed quick resolution of outstanding queries.” – Anti-Infective Products
“FDA provided beneficial feedback via email and formal letters on clinical study plan.” – Psychiatry Products
“Very responsive to emails and phone calls.” – Psychiatry Products “Email served well for communication with RPM.” – Cardiovascular and Renal
Products “Emails: FDA was very responsive to our emails but they were generally regarding
minor items” – Cardiovascular and Renal Products “Email is useful for straight forward questions and answers. They provide
opportunities for sponsors to better understand FDA's thinking and also to clarify questions and comments.” – Pulmonary, Allergy, and Rheumatology Products
“Used for informal discussions, introducing questions, status updates and near term activities (e.g. radar screen of what they can expect coming from us)” – Anesthesia, Analgesia, and Addiction Products
Room for Improvement
“Emails and unscheduled calls helpful for status of submissions or responses – not for substantive information.” – Cardiovascular and Renal Products
“There is a limitation on explanation or discussion that can be communicated through email.” – Pulmonary, Allergy, and Rheumatology Products
Formal Letters: Beneficial
“Formal letters seem to most effectively capture concerns and agreements.” – Cardiovascular and Renal Products
“Written response provided most of the info requested around study design issues.” – Anesthesia, Analgesia, and Addiction Products
“FDA provided constructive feedback on submitted questions and also provided valuable insight on clinical study design.” – Bone, Reproductive and Urologic Products
“Clearly answered questions via written response, no telecon needed.” – Dermatology and Dental Products
“Timely responses. We received the response 3 business days earlier than the due date.” – Pulmonary, Allergy, and Rheumatology Products
“We received an advice letter with very helpful comments” – Anesthesia, Analgesia, and Addiction Products
“The follow-up letter gave clear advice on the outstanding issue we needed input on.” – Dermatology and Dental Products
“Written response is pending but based on prior interactions, expect that it will at least be somewhat (or even very) beneficial” – Dermatology and Dental Products
64
“In the last 1.5 years or so, the Derm Division has been very accepting and responsive of our request for written responses to Type C meeting requests. The written responses have been very helpful.” – Dermatology and Dental Products
Room for Improvement
“Written correspondence via formal letter were helpful, but less so as this did not allow for on the spot discussion/input.” – Anti-Viral Products
“Lack of ability to have dialogue when responses are limited to written format, especially when proposed approach is denied.” – Pulmonary, Allergy, and Rheumatology Products
“This was in the context of an interim analysis. There was a lot of back and forth with formal letters with the statistical group and it was clear that the Agency reviewers were not fully understanding what we were trying to communicate to them. We precipitated a teleconference with the stats group, and this was initially not very helpful – later the Stats Div lead stepped in and helped summarize the discussion and the Agency's position (they in fact agreed with our proposal, which made it seem as if the initial correspondence was due to lack of full understanding on their part), and this was very helpful.” – Anti-Infective Products
“There have been a few written communications that have been informative but would have been better if accompanied by a teleconference to explain the thinking behind the written document.” – Anesthesia, Analgesia, and Addiction Products
“Formal letter Response to proposed strategy to bridge 2 devices is clear but recommendations for alternative approach is not clear.” – Pulmonary, Allergy, and Rheumatology Products
“FDA changed expectations from pre-IND to those required for IND filing - Had to fix inconsistent advice received during pre-IND.” – Anti-Viral Products
“Not responsive in a timely manner to providing comments on the clinical trial protocols, even though these had been available and on file for some time. Review was delayed until interim safety data were provided to the agency for review.” – Anti-Viral Products
“Received comments on protocol via formal letter but did not get feedback on our response.” – Pulmonary, Allergy, and Rheumatology Products
“Written feedback denied proposed PRO, but written responses did not provide venue to explore options.” – Pulmonary, Allergy, and Rheumatology Products
“We received an information request in (Fall) 2012, responded to the Agency about a week later, and then didn't receive a follow-up response from FDA until (Early) 2013, at which time the study had significantly progressed.” – Psychiatry Products
“Written comments often lacked clear rational for disagreements, which often leaves the sponsor with more questions.” – Transplant and Ophthalmology Products
“Minutes did not contain enough detail, follow- up was required – delayed IND submission time.” – Bone, Reproductive, and Urologic Products
Unscheduled Phone Calls: Beneficial
“FDA very responsive to questions during unscheduled call.” – Cardiovascular and Renal Products
“Used email and unscheduled calls to keep the Division informed about the program. Particularly following protocol specified safety reviews and their outcome.” – Anti-Infective Products
Room for Improvement
“Emails and unscheduled calls helpful for status of submissions or responses – not for substantive information.” – Cardiovascular and Renal Products
65

Scheduled Phone Calls: Beneficial
“Several scheduled phone calls were held to resolve issues (re: Clinical hold).” – Cardiovascular and Renal Products
“Very open dialogue about dosing via email and scheduled phone call for one of proposed studies.” – Psychiatry Products
“Scheduled phone call was in response to a clinical hold issue for CMC. The reviewers were very helpful in advising on our plan to respond.” – Cardiovascular and Renal Products
“Teleconference to for us to understand their (clinical hold) concerns and discuss our plan to respond.” – Cardiovascular and Renal Products
“Phone calls were focused on getting Ph 2a initiative and negotiating agency expectations to enable Ph 2a to start.” – Anti-Viral Products
“We appreciate more in person discussions (Telecons) with the Agency (vs. written feedback).” – Anti-Viral Products
“Scheduled teleconference calls with the Division were very beneficial.” – Anti-Viral Products
“Scheduled phone call clarified comments received via email; provided insights into FDA mindset on the issues.” – Anti-Viral Products
“We had one teleconference to discuss an IND Safety Report. The reviewers asked good questions and listened to our thoughts. They were reasonable in their review and we were able to come to agreement on a path forward. We also had a breakthrough designation request denied. They were very helpful in their response, sharing their thoughts transparently and we will be able to reapply once we have further data.” – Anesthesia, Analgesia, and Addiction Products
“Division proposed telecon, which proved highly productive and instructive to us, instead of face-to-face pre-IND meeting when big storm was predicted.” – Bone, Reproductive and Urologic Products
“Scheduled phone call and meeting are beneficial. They provide opportunities for sponsors to better understand FDA's thinking and also to clarify questions and comments.” – Pulmonary, Allergy, and Rheumatology Products
“During teleconference, FDA very open and receptive to sponsor recommendation of clinical study plan.” – Psychiatry Products
“Teleconference were most helpful.” – Transplant and Ophthalmology Products “Telecons have been more beneficial than written responses only, since the rationale
behind responses can be discussed.” – Cardiovascular and Renal Products “Clear path forward provided by FDA in PreIND meeting tcon” – Pulmonary, Allergy,
and Rheumatology Products Room for Improvement
“Timing of preliminary comments (1-2 days ahead of meeting) make it difficult to convert meetings from F2F to teleconference - especially if team has already traveled.” – Transplant and Ophthalmology Products
“Scheduled phone calls are somewhat beneficial but sometimes lack clarity in final outcomes (people hear what they want to hear).” – Cardiovascular and Renal Products
In-Person Meetings: Beneficial
“FDA granted meetings, were responsive, gave constructive feedback.” – Anti-Viral Products
66

“FDA was very engaged and gave good feedback and appropriate rationale for their thinking. They were helpful and willing to have additional discussions.” – Anti-Viral Products
“Live discussions with the DTOP are always preferred. Preliminary comments ahead of the meeting are always most helpful.” – Transplant and Ophthalmology Products
“Good input from the review division on ways to streamline the clinical program. With this input we’re able to move quickly into start of program following meeting (EOP2).” – Anti-Infective Products
“Discussed pediatric plans (rated very beneficial).” – Dermatology and Dental Products
“Achieved clarity on various safety assessments that would be needed to satisfy FDA concerns during in-person meeting.” – Cardiovascular and Renal Products
“FDA response to BD submission prior to face-to-face meeting helped make meeting more focused/productive.” – Cardiovascular and Renal Products
“Face to face discussion in an open way regarding clinical endpoint was most helpful.” – Cardiovascular and Renal Products
“Received good advice from FDA and come to agreement on study design (EOP2).” – Cardiovascular and Renal Products
“The type C meeting was prior to phase 2b. We had very good interaction and innovative thinking about the study endpoint. The Division Director was very open and also helped guide some of the other reviewers to think similarly.” – Cardiovascular and Renal Products
“FDA was collaborative and meeting was extremely productive.” – Cardiovascular and Renal Products
“Discussed pediatric plans (rated very beneficial).” – Cardiovascular and Renal Products
“Division provided preliminary comments 10 days in advance of meeting, which was very helpful to prepare company responses and utilized responses to discuss with FDA during the meeting. FDA also found that providing the responses in advance was helpful and they were well prepared to provide feedback. The meeting was very efficient.” – Cardiovascular and Renal Products
“Planning pediatric pathway – FDA gave good feedback on expectations/requirements prior to initiation of studies and how they would consider risk/benefit for pediatric population – also brought in an ethicist to help.” – Anti-Viral Products
“The face to face meeting was helpful with a good deal of interaction and good discussion. We also received FDA internal feedback prior to the meeting, albeit just ~36 h prior to the actual meeting. Nonetheless, receiving feedback prior to the meeting allows for a much better discussion at the meeting itself.” – Anti-Viral Products
“Prior to having Ph 1 data, discussion regarding overall program direction was very beneficial to gain view of future clinical development plan.” – Anti-Infective Products
“During the face-to-face meeting, FDA was very responsive to our questions and provided excellent guidance on possible Phase 3 study designs including examples and sample size estimations.” – Anti-Infective Products
“Able to get clarity on issue and path forward.” – Anti-Infective Products “End of Ph 2 meeting included totally new trial design that was count to previous FDA
guidance – it was based on the old study design and the written correspondence from FDA was in constant conflict with itself.” – Anesthesia, Analgesia, and Addiction Products
“FDA provided clarity on what additional info was needed.” – Anesthesia, Analgesia, and Addiction Products
67
“(We) received valuable input on our Phase 3 development plan (during EOP2).” – Anesthesia, Analgesia, and Addiction Products
“Face-to-face EOP2 meeting was the most productive interaction with the Agency.” – Anesthesia, Analgesia, and Addiction Products
“DAAAP has a clear understanding of the therapeutic area we're working in and provided constructive and helpful perspective in our meeting with them.” – Anesthesia, Analgesia, and Addiction Products
“FDA provided constructive and detailed preliminary feedback in advance of our face to face meeting which helped to hone the conversation to the key issues and was able to ensure these could be discussed within the allotted meeting time.” – Psychiatry Products
“Formal meetings have involved good dialogue based on sound scientific rationale resulting in clarification of Agency expectations.” – Anesthesia, Analgesia, and Addiction Products
“Face to face EOP2 meeting (Type B) (rated Very Beneficial).” – Pulmonary, Allergy, and Rheumatology Products
“Discussed pediatric plans (Very Beneficial).” – Pulmonary, Allergy, and Rheumatology Products
“Feedback received from the four-sided meeting with CDER and CDRH and the meeting was extremely useful.” – Pulmonary, Allergy, and Rheumatology Products
“FDA provided clear feedback to Sponsor's proposal to move the program forward and explained its position on the issue.” – Pulmonary, Allergy, and Rheumatology Products
“FDA provided clear feedback to Sponsor's proposals.” – Pulmonary, Allergy, and Rheumatology Products
“Provided additional guidance/points to consider for complete Phase 3 program.” – Pulmonary, Allergy, and Rheumatology Products
“FDA provided comprehensive pre-meeting comments, and meeting was limited to the two topics not resolved through the pre-meeting responses.” – Pulmonary, Allergy, and Rheumatology Products
“All interactions with the Division on this program have been very helpful. The most helpful have been our Pre-IND and Type C Meetings, as has the Division's timely feedback and review of our protocol.” – Psychiatry Products
“EOP2 meeting especially beneficial.” – Psychiatry Products “Good feedback in preliminary responses to End of Phase 2 questions and good
discussion during End of Phase 2 meeting.” – Psychiatry Products “Meeting addressed the FDA concerns and there were clear deliverables the sponsor
needed to provide the agency with an agreed upon timeline.” – Psychiatry Products “Preliminary comments prior to meeting (Pre-IND meeting) succinct.” – Transplant
and Ophthalmology Products “Guidance, agreement on trial design and objective for outcome (EOP2).”
– Transplant and Ophthalmology Products “Clear guidance and understanding was reached (EOP3).” – Transplant and
Ophthalmology Products “Face to face meetings are usually very beneficial with this division.” – Transplant
and Ophthalmology Products “DTOP discussions are always beneficial and highly preferred over written
comments.” – Transplant and Ophthalmology Products “Meetings are granted very timely, preliminary comments were received prior to the
meeting.” – Transplant and Ophthalmology Products “It was collaborative; the Agency heard our point of view, was constructive”
– Cardiovascular and Renal Products
68

“Agreement on clinical study design; agreement on targeted AE collection; reporting” – Cardiovascular and Renal Products
“Reached agreement on most aspects of Phase 3 design” – Cardiovascular and Renal Products
“Overall discussion was positive” – Cardiovascular and Renal Products “FDA provided clarification on end of Phase 2 meeting minutes. They also provided
feedback on specific aspects of the protocol prior to finalization.” – Cardiovascular and Renal Products
“Discussed different patient populations and ways to make the clinical trial useful as a supportive pivotal trial.” – Cardiovascular and Renal Products
“Face-to-face meetings have been more beneficial than written responses only, since the rationale behind responses can be discussed.” – Cardiovascular and Renal Products
“FDA provided clarity for the content of clinical data.” – Cardiovascular and Renal Products
“FDA provided feedback on study designs.” – Cardiovascular and Renal Products “The meeting enabled a development discussion outside of the Type B meeting
venue.” – Cardiovascular and Renal Products “Provided guidance for the design of our Phase 2b trial.” – Cardiovascular and Renal
Products “Face to face meetings were the most beneficial.” – Bone, Reproductive, and Urologic
Products “Face to face EOP2 meeting (Type B) was the most beneficial.” – Pulmonary, Allergy,
and Rheumatology Products “FDA provided comprehensive pre-meeting comments, and meeting was limited to
the two topics not resolved through the pre-meeting responses.” – Pulmonary, Allergy, and Rheumatology Products
“Formal meetings have involved good dialogue based on sound scientific rationale resulting in clarification of Agency expectations.” – Pulmonary, Allergy, and Rheumatology Products
“FDA was very responsive to request for EOP1 meeting.” – Anti-Infective Products “Meeting was extremely helpful and collaborative” – Anesthesia, Analgesia, and
Addiction Products Room for Improvement
“Pre-IND meeting was too restrictive on time (30 min. telecom) even though IND opening program was in Ph2 – could not get clarification.” – Dermatology and Dental Products
“When Type C meeting is carried out as written response – agency should consider allowing sponsor to ask follow up questions – sometimes recommendations listed in response are confusing and not straight forward causing a lot of questions about how to best move forward.” – Pulmonary, Allergy, and Rheumatology Products
“EOP2 meeting limited communications to date.” – Cardiovascular and Renal Products
“Had same issue with EOP2 as had with pre-IND meeting – FDA agreed with our plan, but expressed lack of some understanding with regard to what it takes to conduct studies in orphan diseases, especially in terms of follow up, placebo-controlled studies, numbers of patients.” – Cardiovascular and Renal Products
“FDA was unable to provide guidance on structural endpoints given current state of field (EOP2).” – Cardiovascular and Renal Products
“3-6 month delay because pre-IND advice was not accepted after IND submission and required and amendment.” – Anti-Viral Products
69

“Requested pre-IND mtg via formal request, which was denied. We were not able to discuss clinical development plans with the Division prior to filing the IND.” – Anti-Viral Products
“We had two face to face meetings with the division. FDA wasn't well prepared for the first meeting and advised us to get external input on our proposed study and request another meeting. The second meeting was more productive but we are still waiting for FDA feedback on the comparator.” – Anesthesia, Analgesia, and Addiction Products
“They unreasonably stacked the decks against the product at an advisory panel.” – Anesthesia, Analgesia, and Addiction Products
“Had meetings with the Agency where they were not well prepared, were not open to understanding the science and had come to conclusions prior to the meeting based on less than solid considerations.” – Anesthesia, Analgesia, and Addiction Products
“They said one thing and did another.” – Anesthesia, Analgesia, and Addiction Products
“They ignored the positive results of their own audit.” – Anesthesia, Analgesia, and Addiction Products
“Pre-IND meeting feedback from Division altered some aspects of proposed protocol and had mixed effects on timing.” – Bone, Reproductive and Urologic Products
“The meeting did not clearly identify the key concerns from the Agency.” – Pulmonary, Allergy, and Rheumatology Products
“The tone and climate of the meeting was very (uncharacteristically) emotional and combative on the FDA's part. The feedback that was provided did not appear to take into account a significant body of information about the drug in a separate (but strongly allied) indication or take into account the extensive totality of information that had been obtained in randomized, double-blind clinical studies within the target patient population (all of which were positive, and with one minor exception, statistically and clinically positive).” – Pulmonary, Allergy, and Rheumatology Products
“In a multi-division meeting, it is recommended that FDA reviewers identifies themselves, i.e. which Divisions they are from, before comments are provided to the Sponsor as advice given could be different for drug and device development.” – Pulmonary, Allergy, and Rheumatology Products
“When type C meeting is carried as written response, the Agency may consider allowing the sponsor to ask follow up questions. Sometimes, the recommendation listed in the response is not straight forward—even confusing. With only one round of communication with the review division, it causes a lot of questions and confusion for moving forward with agency's comments.” – Pulmonary, Allergy, and Rheumatology Products
“We've had meetings with the Agency where they were not well prepared, were not open to understanding the science and had come to conclusions prior to the meeting based on less than solid considerations.” – Pulmonary, Allergy, and Rheumatology Products
“The meeting did not clearly identify the key concerns from the Agency.” – Pulmonary, Allergy, and Rheumatology Products
“The tone and climate of the meeting was very (uncharacteristically) emotional and combative on the FDA's part. The feedback that was provided did not appear to take into account a significant body of information about the drug in a separate (but strongly allied) indication or take into account the extensive totality of information that had been obtained in randomized, double-blind clinical studies within the target patient population (all of which was positive, and with one minor exception, statistically and clinically positive).” – Pulmonary, Allergy, and Rheumatology Products
70

“Pre-IND meeting feedback was reasonably beneficial.” – Anesthesia, Analgesia, and Addiction Products
ISSUE RESOLUTION Beneficial
“Gained agreement on nonclinical and clinical plan (at EOP2).” – Dermatology and Dental Products
“Agency was responsive to discussions around alternate means to populate information required for complete IND submission.” – Cardiovascular and Renal Products
“EOP2 meeting had a lot of topics to cover and little time to get through everything. Based on FDA input at the meeting we had questions on whether revisions we'd made to clinical trials would be satisfactory. We were able to quickly resolve with email communication. FDA was quick to respond.” – Anti-Infective Products
“Biomarker topic was discussed in a separate meeting (separate from EOP2) per FDA advice (Very Beneficial).” – Pulmonary, Allergy, and Rheumatology Products
“Clarified deficiencies in proposed program and helped us develop a path forward to address FDA comments/concerns (EOP2).” – Pulmonary, Allergy, and Rheumatology Products
“FDA was very responsive to query about clinical trial endpoints and enrollment criteria.” – Transplant and Ophthalmology Products
“Feedback on the protocol (was very beneficial).” – Cardiovascular and Renal Products
“They let us proceed; raised some other nonclinical issues without a clinical hold and were good about explaining why they were insisting on certain aspects of their requirements. ).” – Cardiovascular and Renal Products
“We had a pre-IND meeting which was after we completed the Phase 1 in the UK and after we had submitted the Phase 2 protocol in the UK. The meeting with the FDA division was helpful to set the stage for filing of the IND and getting an understanding of what their areas of concern were. We successfully filed the IND and then had an EOP2 meeting about a year later.” – Cardiovascular and Renal Products
“Excellent feedback on study design; selection of primary endpoints; dose selection; and choice of active comparator and protocol amendment.” – Cardiovascular and Renal Products
“Provided valuable feedback on trial design and approval path.” – Cardiovascular and Renal Products
“Assistance on compassionate use was very helpful.” – Cardiovascular and Renal Products
“Having a TC to discuss study designs to address hold issues was helpful.” – Anti-Viral Products
“IND review written comments had additional comments on Ph 1 protocol which were resolved in a timely manner via email which were followed up with formal responses.” – Anti-Viral Products
“Efficient communications during initial IND submission.” – Anti-Infective Products “Received FAST Track and QIDP status for GAIN in a timely fashion – Agency very
responsive on discussions around safety study requirements.” – Anti-Infective Products
“After proceed acknowledgement – questions were raised and resolved quickly.” – Anti-Infective Products
“Able to reach agreement on Ph 2 efficacy endpoint (EOP1).” – Anti-Infective Products
71

“Biomarker topic was discussed in a separate meeting (separate from EOP2) per FDA advice (Very Beneficial).” – Pulmonary, Allergy, and Rheumatology Products
“Clarified deficiencies in proposed program and helped us develop a path forward to address FDA comments/concerns (EOP2).” – Pulmonary, Allergy, and Rheumatology Products
“Change in study design was communicated through IND amendment with a protocol amendment.” – Pulmonary, Allergy, and Rheumatology Products
“The recommendation for the Phase 3 study design was clear.” – Pulmonary, Allergy, and Rheumatology Products
“The recommendation for the phase 3 study was clear (EOP2).” – Pulmonary, Allergy, and Rheumatology Products
“Used email, scheduled phone calls and formal letters and understood FDA’s concerns and amended protocol to lift clinical hold.” – Psychiatry Products
“FDA provided directions on how to modify protocol in order to removed clinical hold (later was placed on partial clinical hold with clinical dosing and duration limitation but that was later removed).” – Psychiatry Products
“We got positive feedback on the duration of the chronic tox studies we were proposing, as well as on the patient population to be included in the Phase 2 study.” – Psychiatry Products
“Clear requirements were discussed. Despite disagreement between DTOP/sponsor, a clear understanding was reached.” – Transplant and Ophthalmology Products
“Response to the pre-IND questions were clear and enabled us to cancel the teleconference” – Dermatology and Dental Products
“Response from FDA prior to the face-to-face meeting was helpful to make discussion more focused during meeting.” – Cardiovascular and Renal Products
“The Division has been very responsive to all of our questions and the pre-NDA meeting dialogue helped us determine what and how the date should be presented in the NDA.” – Cardiovascular and Renal Products
“The letters we received communicated the agency’s concerns which we addressed in follow-up submissions. The teleconferences were helpful in clarifying the FDA's concerns and allowing us to express our perspective on the issues. Since changing a clinical endpoint had a major effect on the entire industry there was a lot of dialogue required. The overall process, while long, was very productive and collaborative.” – Cardiovascular and Renal Products
“We had asked FDA to review specific aspects of the protocol outside of a SPA and they were responsive and provided the requested feedback.” – Cardiovascular and Renal Products
“FDA provided feedback on changes to a protocol prior to issuing the official amendment. We requested FDA clarification on end of Phase 2 meeting minutes. We also requested clarification on how to procedurally submit documents FDA had requested.” – Cardiovascular and Renal Products
“Type C written comments received provided sufficient agreement on the overall target population, background therapy and study design.” – Pulmonary, Allergy, and Rheumatology Products
“FDA comments in response to questions were generally adequate to allow us to proceed...risks were identified and incorporated into other (internal) decision-making elements.” – Pulmonary, Allergy, and Rheumatology Products
“FDA comments received were generally helpful in guiding our internal decision-making (trial designs, etc.) for adolescent/pediatric studies.” – Pulmonary, Allergy, and Rheumatology Products
“Reached agreement on phase 2 efficacy endpoint.” – Anti-Infective Products “Alignment on type and details of studies to support NDA.” – Anti-Infective Products
72

“Rapid alignment on operations and strategy of getting phase 3 program running.” – Anti-Infective Products
“Pre-IND meeting communication was very helpful. We were granted a meeting but did not need to have the PIND meeting as all our questions were answered through written communication.” – Dermatology and Dental Products
“Written feedback on questions posed in pre-IND meeting package [were most helpful FDA communications]” – Anesthesia, Analgesia, and Addiction Products
“Once FDA realized they had missed a critical element and we clarified our position, they responded in writing in a manner that was acceptable and did so in an efficient manner.” – Dermatology and Dental Products
Room for Improvement
“FDA was unable to provide guidance on structural endpoints given current state of field (at EOP2).” – Dermatology and Dental Products
“We subscribed to their suggestions, submitted an SPA, and they ignored their own counsel when we completed the study (EOP2).” – Anesthesia, Analgesia, and Addiction Products
“(FDA) was open to discussing options during meeting. Timeliness suffered when consult review (from another division) was required on one issue. Would have been useful to have both Review divisions provide unified feedback, which was not the case in this instance.” – Pulmonary, Allergy, and Rheumatology Products
“Requests regarding pediatrics seem slower than those for adult indications.” – Pulmonary, Allergy, and Rheumatology Products
“3 month delay waiting for FDA feedback regarding clinical study dosing plan before could start study.” – Psychiatry Products
“Resolved problems that arose from inconsistency in pre-IND advice and resolved IND non-hold comments.” – Anti-Viral Products
“In general each of these (communication channels) interactions has the potential to clarify FDA expectations and they usually do. What we seek is from the FDA is clarity (based on reasonable scientific rationale) and consistency. In our experience the Agency does a fair job on the former but has been disappointing on the latter. In addition the issue of ease of access is a substantial one. While we would like to have more in the way of informal discussions, to date this has been difficult to achieve.” – Anesthesia, Analgesia, and Addiction Products
“While they engaged in the dialog (during Teleconference), they were not very helpful in thinking outside the box given that 2 studies had indicated a positive trend in the data, the drug was very safe and this is for a VERY high unmet medical need condition where the label could have been restricted etc. They were insistent that yet another study be conducted (which was impossible to do given that we had already conducted a worldwide study in over 30 lung transplant centers) with a huge effort. The FDA was dismissive and did not show any interest in working with the sponsor to make this doable. It has led to the program not being developed further at this time (IND is inactive).” – Anti-Viral Products
“Denial of TCs was not helpful.”– Anti-Viral Products “Initial communications with FDA were helpful and engaging and beneficial (we had
several conversations and face to face meetings on this programs); but at the end, FDA was not willing to be innovative and helpful. When FDA was presented with an encouraging dataset in an adult orphan population with a high unmet medical need, the FDA was not open-minded or willing to engage in any accelerated approval pathways or otherwise innovative ways of approaching the data to help the adult population for a condition that is recognized as life threatening and had no treatment options. We had taken a clinical expert with us who reiterated our thinking and emphasized why this drug was needed and had promise, and his opinions were not
73
considered. The Division brought in a consult from the Pulmonary Div., which changed the tone of the meeting (relative to previous interactions) and was essentially unhelpful. This consultant dominated the conversation and was very dismissive of the data and the proposal.” – Anti-Viral Products
“FDA did not have sufficient information to assess risk/benefit - additional nonclinical information was requested (delayed) 8-12 months b/c clinical hold.” – Anti-Viral Products
“Denying TCs and requesting package with questions for written feedback caused further delay (on clinical hold).” – Anti-Viral Products
“IND was placed on hold and FDA requested additional information.” – Anti-Viral Products
“Primary communications during Phase 2 are being lead by government sponsor; therefore, we have no direct line of sight to effectiveness of communications in subsequent agency interactions.” – Anti-Infective Products
“Many players involved in animal rule product decisions - not always clear what part of the government is driving certain issues.” – Anti-Infective Products
“Submission of study protocols for review took too long to get feedback based on our business needs and sometimes got comments back > 60 days after we had already started the study.” – Anesthesia, Analgesia, and Addiction Products
“We were assured the drug would be approved, and they sent a CRL one week before the PDUFA date.” – Anesthesia, Analgesia, and Addiction Products
“We were placed on clinical hold as a result of a single SAE which is well described in the literature in this condition and with the current SOC. In fact the label for the current product provides a stand alone paragraph that discusses this AE. It was clear from our one way discussion with the Division that they had limited, possibly no, familiarity with this information, yet proceeded to place us on hold.” – Anesthesia, Analgesia, and Addiction Products
“Pediatric study plan - procedural requirements on amendments, what is required and how it relates to the BLA submission and approval. Request for feedback was sent through formal submission. FDA response has yet to be received.” – Pulmonary, Allergy, and Rheumatology Products
“The lack of specificity around some elements of the Phase 3 program that were deeply troubling the FDA at the time of the EoP2 meeting and subsequent Type C meeting, were not clearly communicated as substantial risks to the clinical development program.” – Pulmonary, Allergy, and Rheumatology Products
“In our pre-IND meeting FDA agreed that proper control for our improved medicine would be current standard of care. We completed the Ph 2 trial demonstrating superiority of our product vs SOC and proceeded to end of Ph 2 meeting with FDA (DPARP) where they informed us that upon reflection they had changed their minds and decided that the proper control should be placebo. This cost us at least a year in development and multiple millions of dollars.” – Pulmonary, Allergy, and Rheumatology Products
“While we received adequate general advice concerning our proposed clinical development program, the feedback obtained during our Pre-NDA meeting was much more pointed and indicated very little of the flexibility we had been given to make certain decisions about our Phase 3 program.” – Pulmonary, Allergy, and Rheumatology Products
“For this particular submission, the Review Division has appeared to be less interested in the actual data that has been developed in Phase 3 and more interested in trying to re-hash some topics that were relevant 10 years ago.” – Pulmonary, Allergy, and Rheumatology Products
“Received a partial clinical hold based on a nonclinical finding and limited duration of clinical dosing.” – Psychiatry Products
74

“Label negotiations started late and sponsor received no rationale in areas of disagreement. We held a call a few days later, to discuss the Division’s (Transplant and Ophthalmology Products) position, we started late, were delayed in trying to understand the Divisions position which led to high activity very close to the action date.” – Transplant and Ophthalmology Products
“SPA comments were brief and lacked clear rationale for disagreement on 1 important point. Lack of clarity led to uncertainty and additional question from the sponsor.’ – Transplant and Ophthalmology Products
“Since we were proposing a new endpoint, a series of additional discussions were required prior to reaching final agreement in a SPA. This process took about 2 years.” – Cardiovascular and Renal Products
“We had approximately 6 teleconferences with the Agency and made multiple submissions including 3 SPA submissions prior to reaching agreement.” – Cardiovascular and Renal Products
“FDA was unable to provide guidance on structural endpoints given current state of the field.” – Cardiovascular and Renal Products
“This was in the context of an interim analysis. There was a lot of back and forth with formal letters with the statistical group and it was clear that the Agency reviewers were not fully understanding what we were trying to communicate to them. We precipitated a teleconference with the stats group, and this was initially not very helpful because of language barriers (the FDA statistician was of a different nationality and was very difficult to understand), but then the Stats Div lead stepped in and helped summarize the discussion and the Agency's position (they in fact agreed with our proposal, which made it seem as if the initial correspondence was due to lack of full understanding on their part), and this was very helpful.” – Anti-Viral Products
“Lack of ability to have dialogue when responses are limited to written format, especially when proposed approach is denied.” – Pulmonary, Allergy, and Rheumatology Products
“There have been a few written communications that have been informative but would have been better if accompanied by a teleconference to explain the thinking behind the written document.” – Anesthesia, Analgesia, and Addiction Products
75
APPENDIX 2: CBER ADDITIONAL COMMENTS Below is a comprehensive list of additional comments from survey respondents with clinical development programs being reviewed by CBER. OVERALL COMMUNICATIONS Beneficial
“Helpful feedback and productive communication.” – Cellular and Gene Therapies “All expectations met.” – Vaccines and Related Product Applications “FDA clear in communications and quite responsive” – Cellular and Gene Therapies “FDA was responsive and willing to collaborate” – Cellular and Gene Therapies “Sense of partnership in discussions without crossing boundaries” – Cellular and
Gene Therapies “FDA always available and willing to help” – Cellular and Gene Therapies “Efficient and on-point” – Vaccines and Related Product Applications “Very collaborative, focused on science of product and patient safety” – Vaccines and
Related Product Applications “Interactions with FDA anticipated new elements that would need attention as
sponsor moved forward with development” – Vaccines and Related Product Applications
“All communications have been beneficial with this Division” – Viral Products “A lot of communication and interactions” – Viral Products “Overall communication for our specific programs, as well as communication on more
general topics related to the field of gene therapy (in particular during events sponsored by FDA) has been very helpful to answer our questions and provide general guidance.” – Cellular and Gene Therapies
“We hadn't realized that a six month follow-up of vaccines was standard. Communications were early enough that there was no disruption to study or imposition on study subjects.” – Vaccines and Related Product Applications
“Continuous dialogue.” – Blood Applications Room for Improvement
“Slow to respond to requests to discuss some of their concerns” – Cellular and Gene Therapies
“Length of time it can take to get a response to an issue” – Cellular and Gene Therapies
“FDA's initial lack of understanding technology” – Viral Products “While interactions have been somewhat beneficial, we have received
communications that are not science based or it seems the review division did not understand the science behind our proposals.” – Vaccines and Related Product Applications
“The review division has made requests that have been out of the ordinary including requests to review CRFs, the CRF completion guidance, charters for DSMB and our Safety Evaluation and Adjudication Committee. Their oversight of our trial has been surprisingly intrusive.” – Vaccines and Related Product Applications
“During Pre-IND meeting FDA required expensive animal studies prior to beginning trial in U.S. – Australian regulator approved the study under a Clinical Trial Notification” – Blood Applications
“FDA had an initial lack of understanding of the technology.” – Blood Applications
76
REGULATORY PROJECT MANAGER Beneficial
“Effective in providing feedback to questions and making sponsor aware of FDA needs” – Vaccines and Related Product Applications
“The regulatory project manager was able to provide information or direct contact with the appropriate FDA review team members to address any questions or issues.” – Cellular and Gene Therapies
“Our project manager has been very responsive and helpful.” – Vaccines and Related Product Applications
“Excellent communication with medical reviewer” – Cellular and Gene Therapies Room for Improvement
“Getting a timely response from RPMs to email or phone contacts has become a significant problem” – Cellular and Gene Therapies
“One issue that comes up is that we have the same RPM for multiple programs, many of which are progressing at same time, More often than not, we do not receive timely responses from the RPM when contacted by email or phone. It requires multiple contacts to obtain a response, which is frustrating. We recognize that in general FDA staff are under resourced and workload issues can significantly slow down a sponsor's ability to progress its program, particularly since there is no FDA policy for timeframe to respond to informal inquiries” – Cellular and Gene Therapies
“In general, the reviewers are helpful, but the regulatory project managers who arrange meetings, document discussions are not responsive in a timely manner, or don't accurately document discussions which is frustrating” – Cellular and Gene Therapies
“Difficult to reach and unresponsive” - Vaccines and Related Product Applications SPECIFIC COMMUNICATION CHANNELS Email: Beneficial
“Email allows the issue/questions to be laid out by both FDA and company and provide a comprehensive response.” – Cellular and Gene Therapies
“FDA has been reasonably responsive to our emails. Sometimes, responses take several weeks, but since there is no time frame for response, it has been within expectations.” – Vaccines and Related Product Applications
“All issues resolved via email and scheduled calls” – Vaccines and Related Product Applications
“Formal meetings and e-mails are most helpful.” – Cellular and Gene Therapies “FDA was quick to respond via e-mail.” – Cellular and Gene Therapies “Most beneficial: e-mail and telephone communications” – Cellular and Gene
Therapies “Email communications about design of toxicology very helpful – meeting was
productive and informative.” – Blood Applications
Room for Improvement “FDA has been reasonably responsive to our emails. Sometimes, responses take
several weeks, but since there is no time frame for response, it has been within expectations.” – Vaccines and Related Product Applications
Formal Letters: Beneficial
“Clear timely feedback both written and via teleconference.” – Cellular and Gene Therapies
77

“Written comments (email and phone) sufficient to meet our needs and meet FDA needs.” – Vaccines and Related Product Applications
Scheduled Phone Calls: Beneficial
“All issues resolved via email and scheduled calls” – Vaccines and Related Product Applications
“Most beneficial: e-mail and telephone communications” – Cellular and Gene Therapies
“Meetings/conference calls were most useful” – Cellular and Gene Therapies “Type C meeting held by conference call addressed questions raised in the briefing
document on the study design” – Cellular and Gene Therapies In-Person Meetings: Beneficial
“Formal pre-IND meeting minutes were helpful to clarify the patient population to include in clinical trial.” – Cellular and Gene Therapies
“Additional lab testing (Delay - A few months) - Instructions on testing to be performed (Beneficial).” – Vaccines and Related Product Applications
“Criteria of acceptance were clearly outlined (Type C mtg).” – Viral Products “FDA was very responsive to request for End of Phase 1 meeting” – Cellular and
Gene Therapies “Generally, always helpful to discuss with reviewers study designs given complexities
that are difficult to convey in writing” – Cellular and Gene Therapies “Clear feedback in written format, followed by productive conversation to gain
clarity.” – Cellular and Gene Therapies “Meeting pre-reads and questions submitted by email were resolved and no
scheduled meeting required” – Vaccines and Related Product Applications “Discussions were always fair with give and take on both sides. No significant
unresolved issues” – Vaccines and Related Product Applications “Pre-IND meeting was productive and informative” – Viral Products “Formal meetings and e-mails are most helpful.” – Cellular and Gene Therapies “It provided the framework for the Phase 2 clinical trial to be conducted.” – Cellular
and Gene Therapies “Received answers to the questions posed in the briefing document that adequately
addressed the issues.” – Cellular and Gene Therapies “Criteria of acceptance were clearly outlined.” – Blood Applications “Meetings/conference calls were most useful” – Cellular and Gene Therapies “Issues raised in the briefing document were addressed to our satisfaction; The FDA
recommended we hold a Facility Type C meeting prior to BLA submission and we did” – Cellular and Gene Therapies
Room for Improvement
“A lot of discussion, but worried the FDA will change the approach at some point.” – Viral Products
“There was no discussion of study design specifics (EOP2)” – Cellular and Gene Therapies
“The final version of the meeting minutes were nearly identical to draft version received, despite fact extensive discussion and agreement occurred, which was documented in internal company minutes (submitted in advance of receiving FDA "official" minutes). Receiving FDA minutes that do not reflect the actual discussion, calls in the question of what the purpose of having a meeting with the FDA achieves.” – Cellular and Gene Therapies
78
“We requested a face-to-face meeting, but were only given a written response only meeting. The comments received were useful, but there was no chance to discuss” – Cellular and Gene Therapies
“We had submitted the Phase 2 protocol to the FDA months before but did not get a response. It was not until we had a NIC RAC meeting that the FDA indicated that we should have an EOPI meeting and that they had questions regarding our plans.” – Cellular and Gene Therapies
“A lot of discussion, but worried the FDA will change the approach at some point.” – Blood Applications
“Had actually 3 meetings. Delay first to FDA stating they would not approve the IND. Then after 1 year FDA called and said they were ready. Then we were not ready. Then funding became an issue.” – Blood Applications
ISSUE RESOLUTION Beneficial
“Helpful advising on development of complicated assays required for this project.” – Cellular and Gene Therapies
“Protocol review (by FDA) was mostly helpful.” – Vaccines and Related Product Applications
“Agency provided agreement to proceed to Phase 3 (EOP2).” – Cellular and Gene Therapies
“All issues were resolved fairly readily.” – Vaccines and Related Product Applications “Comments on required protocol changes were helpful” – Cellular and Gene
Therapies “Obtaining answers to issues that came up (Very Beneficial)” – Cellular and Gene
Therapies “Helpful advising on development of complicated assays required for this project”
– Cellular and Gene Therapies “FDA needed clarity on intent of a proposed interim analysis and allowed us to
clarify” – Cellular and Gene Therapies “All issues resolved via email and scheduled calls” – Vaccines and Related Product
Applications “Email communications about design of toxicology very helpful” – Viral Products “Discussions on trial design were helpful. Questions from FDA on CMC issues were
reflective of concern that we were aware of upcoming expectations (i.e. potency assays).” – Vaccines and Related Product Applications
“FDA was able to answer specific questions clarifying the information they required for the study.” – Cellular and Gene Therapies
“For the EOP1 meeting we received good feedback from the agency on our clinical protocol. They offered an informal review of the protocol after revisions based on the meeting.” – Cellular and Gene Therapies
“After submitting a safety amendment the FDA was responsive to our request for a timely review so that enrollment could be re-initiated.” – Cellular and Gene Therapies
“All issues raised were addressed either by e-mail, via phone calls or formal letter” – Cellular and Gene Therapies
Room for Improvement
“FDA stated a BLA submission would result in an RTF (EOP3).” – Cellular and Gene Therapies
“The review division has made requests that have been out of the ordinary including requests to review CRFs, the CRF completion guidance, charters for DSMB and our Safety Evaluation and Adjudication Committee. Their oversight of our trial has been surprisingly intrusive.” – Vaccines and Related Product Applications
79
“During Pre-IND meeting FDA required expensive animal studies prior to beginning trial in U.S. – Australian regulator approved the study under a Clinical Trial Notification.” – Viral Products
“We have conducted 2 Phase 3 trials and submitted our BLA with the expectation based on communication with FDA that our safety database would be adequate. We filed our BLA and received a CRL because the database was too small. We are conducting a third Phase 3 trial” – Vaccines and Related Product Applications
“We have used several methods to get input into our Phase 3 trial design. We sent a draft protocol and received comments from FDA after 3 months. We have asked questions via email with some questions being answered but others required a scheduled phone call. The biggest problem has been that we thought we had an agreement on an important aspect of the study but months later FDA reversed its opinion.” – Vaccines and Related Product Applications
“FDA delayed the first FDA stating they would not approve the IND. Then after 1 year FDA called and said they were ready but we were not at that time and funding became an issue” – Viral Products
“Company was forced to design a study at Agency's insistence that was unlikely to be successful” – Cellular and Gene Therapies
“FDA clinical reviewers had strong ideas as to appropriate endpoints and duration which were not completely aligned with company and/or key opinion leaders” – Cellular and Gene Therapies
“Ongoing discussions about a primary endpoint that meets all criteria for a primary endpoint which they tell us is only exploratory (Not Very Beneficial)” – Vaccines and Related Product Applications
“The reviewer did not follow-up on their offer of informal review of the protocol. Although it was sent by e-mail, there was no response or feedback given by the FDA.” – Cellular and Gene Therapies
“Could not reach agreement on acceptable proposal to change the study design” – Cellular and Gene Therapies
80
APPENDIX 3: CDER DIVISION OF ONCOLOGY PRODUCTS ADDITIONAL COMMENTS
Below is a comprehensive list of additional comments from survey respondents with clinical development programs being reviewed by CDER Division of Oncology Products. OVERALL COMMUNICATIONS Beneficial
“FDA was responsive.” “All communications were very clear and responses from FDA were timely.” “Collaborative environment – FDA was responsive and sent preliminary comments
early and all additional questions were addressed during in-person meeting.” “All communications were very clear and responses from FDA were timely.” “The interactions allowed both the company and FDA to work through potential
issues. Although the initial IND was put on clinical hold, other issues were resolved prior to IND submission.”
“When giving "heads up" for an upcoming submission for breakthrough designation, was asked to provide preliminary submission and a teleconference to discuss the potential to qualify before the formal submission, saving a lot of time and effort on both parts. The Division also provided a worksheet for a compassionate use request to help the investigator prepare for an investigator IND. Keeping in touch via email informally helps prepare FDA for forthcoming communications.”
“FDA Review Division provided timely and thoughtful input during discussions” “Senior staff participated on our teleconference – this was highly respectful for our
small company and we appreciated their candor” “Since hiring a head of regulatory affairs, multiple communications have occurred re:
opportunities to discuss Fast Track, Breakthrough Therapy Designation, EOP1 meeting. FDA is highly responsive, clear and interactive”
“Comparability meeting we discussed progress, enrollment and anticipated completion”
“Very supportive, collaborative and partnered effectively to meet patient needs and expedited development of an important drug”
“FDA very collaborative and supportive of the development program” “Division of Oncology provided additional insights around patient populations, which
made the endpoint more acceptable for registration purposes.” “The FDA was responsive and informative with suggestions on trial design, patient
population, and other issues.” “[FDA] addressed all questions”
Room for Improvement
“Reviewer's comments and responses to questions were inconsistent with the same division precedents and inconsistent with clinical practice.”
“FDA was responsive to emails. However, it took several rounds of emails before they indicated that our revisions were acceptable.”
“FDA would not respond favorably to a request for Fast Track designation in the IND” “FDA did not think a dose escalation was necessary when clearly it was because the
drug had not been used in combination with chemotherapy and radiation therapy. Investigators felt that dose escalation was necessary to protect the patients”
“The clinical reviewer made remarks about findings shared, as irrelevant—contrary to the opinion of key leading cancer specialists”
“Some of FDA’s comments were not clear, and required clarification (unlike our experience with EMA)”
81
“Written response from FDA was “maybe,” without further explanation” REGULATORY PROJECT MANAGER (RPM) Beneficial
“Clear and timely communication.” “FDA project manager was very responsive to all forms of communication.” “Very Responsive” “The project manager was responsive, informative, and followed through on requests
for information and responses.” “FDA PM was very communicative, helpful and collaborative throughout the whole
development program.” “Very responsive, and when she left, she connected me with the new PM to ensure
communication flow was continued.” “Regulatory Project Manager was extremely interactive and helpful in working
through issues” “The FDA project manager is responsive and consults with her team as needed. Our
communications are respectful and timely.” “FDA PM was critical to ensure timely FDA feedback”
Room for Improvement
“Did not seem to have oncology pharmaceutical experience, some comments seemed arbitrary.”
“Regulatory Project Manager primarily handled work flow. Friendly and efficient but no further input was available.”
“Very inexperienced Regulatory Project Manager assigned” “Requested respect for reviewers even if they were wrong” “Regulatory Project Manager did not provide any input other than how to handle
submission.” “The PM pointed out that the reviewers should be respected even if they were
wrong” SPECIFIC COMMUNICATION CHANNELS Email: Beneficial
“FDA was very responsive to emails and sponsor was able to reply with comments and clarifications to protocols in a timely manner.”
“FDA was responsive to questions posed over email regarding separate or combined INDs for 2 investigational drugs separately and in combination (combination drug filing issues)”
“Email communication very helpful to expedite program” “Written communications (email and letters) were clear with specified timelines and
actions required” “Timely response to emails when could not reach via phone” “Email more useful communication tool as it is real-time communication” “FDA was very responsive to emails and sponsor was able to reply with comments
and clarifications to protocols in a timely manner so as not go to on hold prior to IND approval”
“Combo (Onco/CDRH) – FDA very responsive to emails regarding pre-IND and IND interactions and FDA feedback”
“Rapid and complete responses to email” “Email requests for comment were addresses in a timely manner and were able to
discuss clinical hold issue via scheduled call and gain clarity on issues in person formal meetings.”
82

“Timely email communication in between formal communications” “All correspondence was done by email, very cordial and allowed us to move quickly
into Ph2, submitted documents formally after confirmation by email that they were acceptable.”
Formal Letters: Beneficial
“Formal communications laid out a clear pathway to IND approval” “Clear and rapid communications on protocol design changes via email and formal
letter” “Letter with FDA suggestions and comments to protocol [has been most helpful]”
Room for Improvement
“Written feedback left room for interpretation – clarification would have been beneficial”
“Written responses were unhelpful, insufficient detail provided.” “Letter with FDA suggestions caused delays to revise clinical program”
Unscheduled Phone Calls: Room for Improvement
“Unscheduled phone call only served to set up a scheduled call where questions were answered”
Scheduled Phone Calls: Beneficial
“Scheduled teleconference very helpful” “FDA clarified considerations for their position and provided clear feedback on
sponsor proposals during scheduled phone call” “FDA provided beneficial advice during scheduled call on safety observations” “Eight months prior to the end-of-phase 2 meeting, there was a formal Type B
teleconference with FDA to discuss the general clinical development program for NSCLC. This helped in the planning of the pivotal Phase 3 study leading up to the end-of phase 2.”
“Teleconference to discuss potential safety issue and agree on steps to mitigate risk to patients without program delay was beneficial”
“Formal teleconferences to discuss strategy and development plans allowed for continued alignment”
In-Person Meetings: Beneficial
“FDA provided clear feedback on all questions from Type C meeting.” “Pre-IND meeting responses were clear and helpful in protocol design” “Type B meeting for pre-breakthrough was very helpful” “Type B – pre-IND meeting very helpful” “Face-to-face meeting with Division head was helpful after FDA changed its position.” “Input on Phase 3 trial design; clinical pharmacology program.” “Face-to-face meeting with Division head was helpful after FDA changed its position.” “FDA provided clear feedback on all questions from Type C meeting” “In person meeting was more helpful as it allowed discussion of broad outline of a
registration program.” “DOP1 was very clear and communicative about what they wanted from this trial to
lead to potential approval.” “Feedback facilitated progress into Phase 3”
83
“FDA Division head presence provided clarity that staff were not willing to provide.” “Received concrete feedback from agency in End of Phase 2 meeting” “Type C meeting informed the program.” “Pre-NDA/BLA meeting was very collaborative” “FDA provided complete answers in Type C meeting to all of our questions and made
additional comments” “Face to face interactions were extremely helpful” “FDA excited and suggested breakthrough and fast track development, rapid
development plan to get drug to patients. Very collaborative.” “Useful conversation around companion diagnostic development. Parallel
conversation was conducted with CDRH around this same period of time (regarding companion diagnostic).”
“Ensured alignment on key study parameters and patient population, endpoints and interim analyses”
“We requested a pre-IND meeting and received beneficial answers to all of our questions to enable an IND filing.”
“Ensured the current progress of CMC and manufacturing were acceptable and met FDA expectations for initial commercial product”
“Type C meetings provided additional guidance on trial design aspects.” “Protocol finalization” “FDA provided complete answers to all of our questions and made additional
comments.” “Type C - preclin meeting beneficial”
Room for Improvement
“Reviewer's comments on the phase 3 program at EOP2 was inconsistent with the same division's precedents and inconsistent with clinical practice”
“Division director was absent in pre-IND and EOP2 meetings which may avoid potential inconsistencies in different reviewers' opinions within the same division”
“FDA cancelled our End of Phase 2 meeting without explanation and rescheduled us several months later. An Advisory Committee meeting in between resulted in a change of FDA policy on approvable endpoints for our indication.”
“Division director was absent in Pre-IND and End of Phase 2 meetings whose presence may have helped avoid inconsistencies in different reviewers' opinions within the same division.”
ISSUE RESOLUTION Beneficial
“Clear and rapid communications on protocol design changes via email and formal letter.”
“FDA provided beneficial advice during scheduled call on safety observations.” “Timely response to request for extension to address CMC comments received during
IND assessment” “Communications have been beneficial regarding the phase 1 protocol and the input
from the Division was very helpful in finalizing a couple of issues in the protocol.” “Input on Phase 3 trial design; clinical pharmacology program was beneficial” “Emails, scheduled calls and formal letters useful to address FDA’s comments in a
timely manner and modify protocol accordingly” “Modifications to program were made based on FDA feedback during end of Ph 1
meeting which were helpful” “If had a pre-IND meeting to discuss and agree on protocol – would have saved the
need for many interactions after IND filing” “Came back for Type C meeting to discuss protocol revisions.”
84

“We discussed the acceptability of adapting the final analysis plan with future data from other ongoing studies (i.e. still ongoing Phase 2 studies) after the start of the pivotal Phase 3 study.”
“Type C meeting was used for Protocol finalization” “Modifications to program were made based on FDA feedback during end of Phase 1
meeting which were helpful.” “Protocol amendments were submitted and accepted by FDA.” “The email responses to the question in the pre-IND meeting requests provided FDA
expectations and preliminary issues identified that could be further discussed at the scheduled teleconference. A productive discussion allowed for resolution and further required data to support an initial IND.”
“Formal correspondences were extremely helpful as were draft FDA responses prior to face to face meetings. This allowed a more focused discussion on key topics/issues.”
“FDA wanted to ensure we had adequate safety data prior to starting phase 3, so we provided it informally via email and formally via official letter.”
Room for Improvement
“FDA reviewers raised concerns that were not based on the preclinical package. An abundance of caution is welcome but if unnecessary testing increases the cost of Phase 1 and lowers patient interest and/or compliance, we all lose.”
“Reviewers indicated certain generic concerns that were not justified by the IND preclinical package (i.e. CV risk monitoring in the absence of any CV risk findings in the preclinical package).”
“Submitted IND sequence document to eCTD regarding changes to dosing regimen but no response from FDA – assumption is everything is acknowledged and approved but not certain”
“FDA addressed questions asked but time was limited and issues arising during the discussion could not be addressed as they were not on the agenda requiring a follow-up call.”
“FDA did not provide opportunity to discuss recommended changes (by FDA) to study designs.”
“Investigators felt strongly that a dose escalation was needed to protect patients b/c drug had not been used in combination with chemo and radiation therapy but FDA did not agree”
“Meeting allowed us to get back on track after FDA changed its position from its earlier written guidance!”
85

APPENDIX 4: CDER DIVISION OF NEUROLOGY PRODUCTS ADDITIONAL COMMENTS
Below is a comprehensive list of additional comments from survey respondents with clinical development programs being reviewed by CDER Division of Neurology Products. OVERALL COMMUNICATIONS Beneficial
“Good discussion, Helpful.” “I feel all interactions with the Division are beneficial.” “Constructive feedback.” “(Communications) helped shape the development path forward” “Responses received in timely manner.” “At the Pre-IND Phase FDA was very helpful and responsive to the questions about
scope of pre-IND testing.” “Detailed and helpful development comments and questions were included in the IND
clearance letter. This type of feedback regarding future development needs are invaluable. Receiving this specific advice very early also enables the sponsor to research and improve on areas of weaknesses in the program. In this way, the sponsor can respond to these questions thoughtfully, at a time when they judge they have sufficient data to address the Agency's questions.”
“The FDA has been very responsive, provide thorough comments and guidance. We have multiple INDs but with the same compound. The FDA has provided us with guidance to streamline our filings.”
“Overall our communication has been helpful Hopefully it will continue as our program continues.”
“The discussion with FDA was very good and helpful. It helped in planning the phase 3 program.”
“IND review was very fast (27 days), with only 1 request for additional (CMC) information”
Room for Improvement
“It would be very beneficial if the reviewers had a clear and detailed response to sponsor questions especially when sponsor is seeking guidance from the Review division on development pathway. This in my opinion will help the reviewers when they review the regulatory submissions.”
“FDA hadn't clearly stated their understanding/expectation of the 'use' of the proposed drug which lead to delay in trial design.”
“The risk/benefit assessment/requirements does not appear to be commensurate with the high unmet medical and patient requirements for these rare diseases.”
“The Agency gave good overall feedback, although it did not appear that there was adequate understanding of the finer aspects of the orphan disease and the constraints thereof.”
“FDA does not make it easy to discuss new strategies for clinical trial designs (for orphan diseases), with Sponsors.”
“Transitioning of Divisional Leadership, as well as lack of consensus in scientific development of this area contribute to some uncertainty regarding FDA position on certain issues related to drug development in this therapeutic area.”
“Certain review divisions seem to be disconnected from feedback of both patients and industry. It would be beneficial if FDA focused more resources on addressing these areas of disconnect with sponsors and patient communities to better serve public interest.”
86

“There seemed to be a surprising lack of preparation or unwillingness on the Neuro division's part to discuss specifics for an expedited development program in the orphan space for an indication with no approved treatments.”
“Answers to the clinical questions would have been more helpful if they were not so vague and more indication-specific. For a small biotech developing drugs in the orphan space, very specific clinical advice is helpful in early development.”
“I always get a response, although in general it’s not before multiple attempts and up to two weeks before anything is acknowledged. We do tend to get concise feedback - as much as you can expect within the timelines allowed. I guess we shouldn't expect more?”
REGULATORY PROJECT MANAGER (RPM) Beneficial
“RPM is very responsive to our emails.” “FDA RPM responsive via email and telephone conversation regarding status and
when the sponsor could expect FDA feedback.” “RPM is very responsive to our emails.” “The RPM was very responsive and communicated well by email.” “Very responsive to emails.” “Timely confirmation of submitted documents.” “Responsive, helpful.” “In general, our project manager is very responsive and helpful.” “We are working with a great, experienced RPM.” “Our FDA project manager in the Division of Neurology Products is very responsive
and transparent. She contacted us and let us know what to expect and when.” “FDA was very timely in responding to the request for information for a Regulatory
Project Manager.” Room for Improvement
“In some instances he/she needs to follow up with the review division for information, which can limit the usefulness of the interactions.”
“There were multiple Regulatory Project Managers during the conduct of the Phase 3 program. Some had better communication styles/abilities than others.”
“There is a tremendous variability among the various RPMs at the Agency which effects the review timeliness at the Agency.”
SPECIFIC COMMUNICATION CHANNELS Email: Beneficial
“FDA responded to email request to confirm the Regulatory Project Manager contact information.”
“Very responsive to emails.” “FDA was very responsive to the emails and telephone calls querying how to
reference pre-clinical studies conducted on behalf of another disease state.” “Used email to communicate with Project Manager only.” “Email used for clarifying questions regarding acceptability of endpoint.” “Email correspondence was used to ask and respond to clarifying questions regarding
the acceptability of the primary endpoint. Responses were prompt and agreement on the primary endpoint was reached within two weeks.”
“FDA responsive to email request for scheduled phone call.” “FDA was responsive to the emails about the scope of the clinical trial design “Feedback on Phase 2 study design received within 2 months of request for
comment/advice.”
87

“FDA response was received in a timely manner and fully addressed the question asked within our New Protocol submission.”
“Request for Agency Feedback on protocol design question included in New Protocol submission.”
“They responded to formal letters by way of email confirmation and emails by way of emails as appropriate.”
“FDA responded in a timely manner to our emails and provided us guidance for submitting carcinogenicity protocols.”
“FDA was responsive to emails about clarifications regarding the endpoint.” Room for Improvement
“It would be helpful if FDA would respond to our general correspondence that helps planning.”
“It would be very helpful if the division would respond in a timely fashion to email or general correspondence, which are not under a clock (formal meeting). Sometimes there are small but significant questions that come up during the development that needs FDA input that can be accomplished by email/phone contact.”
“Difficult to discuss/receive any feedback during a conversation that was not set up with RPM in advance.”
Formal Letters: Beneficial
“Clinical Hold letter outlined all items where additional information was needed.” “The formal letter addressed the Maximum Feasible Dose in our tox studies and
clarified issues.” “Most Beneficial: Type C written feedback.” “They responded to formal letters by way of email confirmation and emails by way of
emails as appropriate.” “FDA responded quickly to the formal letters we submitted” “FDA was responded in great detail to the formal letters we submitted”
Room for Improvement
“Received a clinical hold letter in response to filing IND.” “Unhelpful FDA Communications: Issuance of a Written Request Letter with new
pediatric assessment dates and FDA Deferral denial of pediatric assessment dates that referenced the original assessment dates in the NDA approval letter in error.”
“Formal letters were mainly standard communications such as annual reports, protocol amendments, new investigators etc. (not very beneficial).”
Unscheduled Phone Calls: Beneficial
“FDA was very responsive to the emails and telephone calls querying how to reference pre-clinical studies conducted on behalf of another disease state.”
“Feedback on Phase 2 study design received within 2 months of request for comment/advice. FDA PM responsive via email and telephone conversation regarding status and when the sponsor could expect FDA feedback.”
Scheduled Phone Calls: Beneficial
“FDA provided beneficial information during the phone call.”
88

In-Person Meetings: Beneficial
“FDA sent meeting minutes prior to in-person meeting, which was very helpful.” “Discussed the feasibility of applying for Fast Track at the time of IND filing. Clarified
that this would impact the 30-day clock for the IND review.” “Type B face-to-face pre-IND meeting was very interactive.” “Ph 1 study not done in U.S. but FDA was willing to engage and understood our plan
and enabled continuation of Ph 2 study and engagement again a few months later for a EOP 2 meeting.”
“Written responses to questions posed in pre-meeting briefing package were thorough.”
“Meeting was interactive and provided clarity to questions asked.” “FDA preliminary comments to the questions posed to FDA were clear and a meeting
to discuss them was not required and was subsequently cancelled.” “The most helpful communications were our Type C Meetings, IRT review, and
response regarding transitioning to DSUR.” “Most beneficial: The Face to face meeting and the detailed preliminary feedback we
received.” “FDA provided thorough written response to the questions posed in the pre-meeting
briefing package. The responses were received 2 days prior to their target for response.”
“We have received a lot of feedback on our study protocols and analysis plans by the reviewers.”
“It was helpful that Dr. Temple attended the meeting and set the tone.” “Provided feedback specific to our questions.” “FDA provided direction on the pivotal protocol, statistical analysis plan and
appropriate patients.” “FDA provided feedback on the proposed design of the Phase 2 study which were
were able to incorporate in advance of protocol submission.” “The Division's preliminary responses were very clear such that we received the
feedback that we needed and were able to cancel the scheduled teleconference and have the Preliminary Comments serve as the official record of the meeting.”
“Helped sponsor with planning the phase 2 program.” “The face-to-face discussions with the Agency provided clarity and direction that
allowed the program to move forward.” “It was good to discuss face-to-face with FDA the issues and resolve concerns, seek
clarification.” “At least we were able to clarify certain issues related to our development program.” “The in-person meetings were most beneficial.” “The discussion with FDA was very good and helpful. It helped in planning the phase
3 program.” “This was a pre-IND meeting for us because we went to FDA after we had completed
the Phase 1 and also had some data in patients from the Phase 2. This was helpful to introduce the program, and to set the stage for the plan for filing of the IND as well as for the EOP2 meeting which happened just a few months later. FDA was willing to be engaged, understood our plan and gave good feedback that enabled continuation of our Phase 2 study and engagement of the Div again for the EOP2 meeting a few months later”
“Received valuable input on our Phase 3 development plan” “The Agency gave good overall feedback.” “FDA gave us good feedback during our Pre-IND meeting with the Agency”
89

Room for Improvement “6 month delay so far…” “The lack of clear guidance during the Pre-IND meeting was disconcerting. Type B
meetings are always encouraged by the Agency, so they should always be invaluable. This meeting was a Pre-IND meeting for a Phase II IND-initiating study, where specific advice would have been more meaningful and helpful to our development program.”
“In a Pre-IND meeting FDA gave us only mediocre feedback during our Pre-IND meeting with the Agency. As a small company developing drugs in a rare, orphan disease, the answers to the clinical questions would have been more helpful if they were not so vague. For instance, if the Agency could share common development problems that are not drug or company-specific, that would be very valuable to small biotechs developing drugs in this space.”
ISSUE RESOLUTION Beneficial
“Agreement was reached on the Phase 3 protocol.” “Discussion with FDA at F2F meeting enabled clarification/resolution of certain
issues/sticking points in preliminary response received from FDA.” “All nonclinical issues were addressed after the clinical hold.” “Responses prompt and agreement on primary endpoint reached within 2 weeks.” “The Agency clearly communicated the requirements for a pediatric PK study.” “FDA was timely and provided responsive content via email regarding amending
Phase 1 clinical protocol.” “The FDA was in agreement with the pre-clinical and phase 1/2 study designs.” “The FDA (Division Neurology Products) responded to our very specific questions
posed for our Phase 3 protocol regardless of the method of communication.” “The communications received from FDA regarding the Pediatric Study Plan were
very helpful and allowed us to address all of the issues and receive an initial agreement.”
“Agreement on primary endpoint – prompt response and confirmation of endpoint enabled sponsor to proceed in a timely manner.”
“The Clinical Hold Letter outlined all items where additional information was requested.”
“Phone call was helpful to understand FDA requests on changes to study design.” “Emails were exchanged with FDA to clarify some issues regarding the study
endpoint.” “The Hold comments were very specific, which made it easier to address the specific
issues regarding the Hold.” “We had several Type A meetings to get to a Special Protocol Agreement on our
Phase 3 protocol prior to starting it.” “The FDA responded to an amendment to our protocol which was under SP-
Agreement by way of email with a very concise, specific answer.” “Written responses in response to pre-IND Type C meeting confirmed our proposed
regulatory path and confirmed the proposed PK bridging study is probably sufficient (pending data review, of course)”
Room for Improvement “Biostatistical questions were submitted in writing as time ran out during the Type B
meeting for discussion. In addition, a Pediatric Study plan was submitted, had requests for additional information and received initial agreement from the Division. Protocol Assessments were submitted for the proposed Phase 3 protocol and No Agreement letters were received from the Division.”
90

“Provided multiple written submissions for requested CMC information and protocol amendments prior to lifting clinical hold.”
“Responses to the Special Protocol Assessment requests were not beneficial as we were unable to obtain agreement with the Division prior to initiating our Phase 3 trial.”
“The FDA’s response was beneficial, but it was not without multiple emails and phone calls from us as well as an email from our CEO to the Medical Director assigned to our program.”
91

APPENDIX 5: CDER DIVISION OF HEMATOLOGY PRODUCTS ADDITIONAL COMMENTS
Below is a comprehensive list of additional comments from survey respondents with clinical development programs being reviewed by CDER Division of Hematology Products. OVERALL COMMUNICATIONS Beneficial
“We have benefited from the interactions and have been able to incorporate the feedback into the development program. We hope that the incorporation of the agency feedback will facilitate the subsequent processes.”
“Collaborative tone.” “FDA agreed to review additional information prior to submission.” “The review division is collaborative and reasonable. The review teams have
provided instructive feedback.” “We have benefited from the interactions and have been able to incorporate the
feedback into the development program. We hope that the incorporation of the agency feedback will facilitate the subsequent processes.”
Room for Improvement
“Some comments appeared to be from inexperienced reviewers.” “Was using non-traditional approach and CMC reviewer just said “follow guidance” –
not enough for FDA to hold a meeting must be an active participant – reviewer could have been more informative and identified pitfalls with the approach we were using.”
“FDA seemed irritated by some of the questions we asked, despite them being standard questions for a pre-IND. FDA also questioned our concern for patient safety.”
“Comments in passing after meeting concluded by FDA lead during meeting were that were not consistent with the minutes, causing confusion”
“Management is emphasizing FDA comments made at Type B meetings that were not minuted. This is creating some regulatory confusion”
REGULATORY PROJECT MANAGER (RPM) Beneficial
“Prompt and clear responses to questions.” “RPM very responsive.” “Comments and concerns regarding the regulatory risk and regulatory path were
beneficial.” “Very responsive.” “Reg PM was helpful with timely response to questions” “Pleasant interactions, requests for information and provided clear timelines” “Responsive and timely interaction with clear direction on next steps”
Room for Improvement
“Interactions with DOP2 have been problematic – delays in requests and lack of coordination with Project Manager.”
“Project manager from DOP2 is not responsive.” “The email and phone calls allowed active communication with the RPM, but she was
not cooperative and 'talked down' to us about the regulatory process (which we have a lot of experience on); and made it very difficult to understand why we were getting very different feedback and interactions from two RPMs from the SAME division! We suspect that this is either due to the RPM or the medical reviewer or both.”
92

“There have been several changes in the PM during the program” SPECIFIC COMMUNICATION CHANNELS Email: Room for Improvement
“Several emails exchanged to get full understanding of FDA comment/request.” Formal Letters: Beneficial
“Formal letter provided somewhat beneficial comments to protocol prior to initiating Ph 1.”
“Comments were received and in response to the comments revisions were incorporated into a protocol amendment.”
Room for Improvement
“A response was not received (Formal Letter) until the final protocol was submitted.” Scheduled Phone Calls: Beneficial
“FDA provided value feedback during phone call on required consultation on study inclusion criteria following due to AE.”
“FDA provided clear feedback during scheduled phone call.” In-Person Meetings: Beneficial
“Questions asked were specific and detailed. FDA provided direct responses that provided clarity and direction.”
“All were helpful. Type B EOP2, Type A for SPA, and Type C during Phase 3 were all invaluable to ensuring clinical study conduct and data analyses would meet FDA expectations/needs for evaluation of the compound.”
“Feedback was very clear and did not require further FDA interaction.” “Requested meeting to discuss manufacturing issues but meeting was denied – FDA
did provide written response that clarified questions about manufacturing.” “Had 2 pre-IND mtgs. – 1 with CDER and 1 with CBER –both collaborative.” “Obtained written response prior to meeting.” “Beneficial pre-IND meeting.” “Pre-IND meeting was very helpful.” “Advice requested on a second trial and response was timely” “Collaborative environment, FDA was responsive and sent preliminary comments
early. All additional questions were addressed during the in-person meeting.” Room for Improvement
“Lack of opportunity for dialogue during hold meetings.” “The division has changed their process for creating minutes of meetings. They have
gone from generating the minutes during the meeting to doing them post-meeting. This has resulted in substantially increased times to receive final meeting minutes. It is more efficient for the project manager to draft the minutes on the screen during the meetings so that the review team can weigh in real time and the sponsor has a more accurate understanding of what will be in the minutes.”
“Meeting was denied.” “Please reconsider the meeting minute process to reintroduce the generation of
meeting minutes during the meetings.”
93

ISSUE RESOLUTION Beneficial
“FDA communicated issues about starting dose and study design by email – after initial teleconference to clarify issues and submission of revised proposal, had a productive teleconference and worked out a revised study design that met everyone’s needs – helped to have FDA clinical reviewers with clear development experience.”
“Very responsive discussion (via email) regarding the safety signal observed.” “General agreement reached on patient population, primary endpoint, important
parameters for trial design, and planned size of the overall safety database (at EOP2).”
“We reached agreement on key aspects of the study design. It was a collaborative discussion (at EOP2).”
“Review division was communicative once placed on hold – gave clear direction on what was needed to address hold.”
“Protocol was vetted with FDA through special protocol assessment (SPA). SPA agreement was reached.”
“Reached agreement on study design as part of the SPA process.” “Reaching SPA agreement (prior to starting Ph 3) provided us with the confidence
that FDA endorsed our plans for our Phase 3 study.” “Provided comments to protocol.” “Had a clarification meeting after clinical hold decision that was very helpful.” “Answers to manufacturing questions were helpful.” “An EOP1 to discuss a phase 3 study design followed by a Type C to resolve any
remaining questions following incorporation of feedback from FDA and EMA. This was a helpful suggestion from the medical reviewer.”
“Discussions helpful re: revised study design.” “FDA RPM communicated frequently about logistics and acknowledgement of the
meeting request, etc.; in the face to face pre-IND meeting, FDA was very good in giving feedback on CMC aspects, nonclinical studies, as well as the study design. They were prepared, had read the materials and were open minded. It was a good discussion.”
“Requested Type C to discuss contents of filing. Written communication was sufficient and meeting was canceled.”
Room for Improvement
“(Pre-IND meeting) CMC reviewer was not informative and ultimately led to a clinical hold.”
“Telecons regarding clinical hold requested by FDA were too short and communication was one way. Time for a two way dialogue would have been very beneficial.”
“Clear direction prior to hold could have prevented clinical hold.” “FDA did provide current thinking on endpoints but their guidance did not seem
exactly in line with clinical practice.” “Our perception was that the review team had not thoroughly reviewed the (clinical
hold) package.” “It is not the mode of communication per se, but the quality of the communication -
the tone, the talking down, and the quality of the response from the review team (question on study design not answered; just told that it would be reviewed when we send the IND)”
94

APPENDIX 6: CDER DIVISION OF METABOLISM AND ENDOCRINOLOGY PRODUCTS
ADDITIONAL COMMENTS Below is a comprehensive list of additional comments from survey respondents with clinical development programs being reviewed by CDER Division of Metabolism and Endocrinology Products. OVERALL COMMUNICATIONS Beneficial
“We are very happy about all the FDA interactions we had so far for this program. FDA had granted all our meeting requests and provided their responses within the PDUFA user fee date, sometimes even a few days earlier.”
“In general, the review team and the leadership take a very pragmatic approach to development, balancing the need for sound data on which to base decisions with the importance of ensuring the studies are feasible.”
“Consistently provided clarification of what was needed to reach agreement and move program forward.”
“Provided clarity on path forward.” “The division was clearly very engaged and willing to work with us.” “Overall, our interactions have been very positive.” “Communications pre-Phase 3 safety and efficacy studies were useful.” “Formal FDRR interactions involving Sr. FDA Officials proved to be most helpful” “Were able to discuss proposed pediatric trial design directly with division director” “Interactions with senior FDA officials were significantly more useful and eventually
resulted in a path forward”
Room for Improvement “Timeliness of responses was an issue.” “Feedback was not received in a timely manner; information provided could not be
addressed at that point in time.” “Lack of transparency, multiple unrealistic pre-clinical requests.” “Email and unscheduled calls were used primarily as communication tool to organize
written feedback and F2F meetings. Written feedback from formal letter (i.e. instead of granting formal Type C meeting FDA provided written feedback) was used often by Division. Overall was helpful to address outstanding concerns, although process was lengthy to get FDA feedback, and often led to follow-up questions with lengthy response times.”
“Timeliness of responses was problematic.” “FDA comments within the different divisions were not consistent.” “The information we got on our PSP was completely contradicted at our EOP2A
meeting.” “Discussions post-CRL were very challenging as FDA did not have internal alignment
when discussing trial options and design elements with the sponsor.” “EOR meeting was particularly unsatisfying as internal FDA alignment did not exist
before meeting with the Sponsor.” “Response time was definitely an ongoing issue during review and study conduct.
This was especially the case with respect to questions regarding PK studies.” “Responses were not very timely”
95

REGULATORY PROJECT MANAGER Beneficial
“Our RPM is easily accessible and provides solid feedback and guidance on ensuring a smooth review process. Very knowledgeable and good communicator.”
“Willingness of FDA Regulatory Project Manager to email copies of FDA letters being sent by post was highly appreciated.”
“Current RPM is great” Room for Improvement
“Project Manager was often unable to be reached or did not reply to emails or phone calls.”
“Our previous RPM was aloof and difficult to reach and was not diligent with following up.”
“Project Manager was often only able to be reached via e-mail, often needing more than one e-mail”
“Project manager generally had to be called or e-mailed more than once to get a response”
SPECIFIC COMMUNICATION CHANNELS Email: Beneficial
“FDA provided clarifications via email regarding food effect and PK studies.” “The phone call discussed possibility of addressing a question related to study
datasets via an email instead of through a formal letter. The question and background information was sent via email and was addressed without needing submission of a formal letter.”
“Very responsive to email and phone calls – even acknowledgement of receiving calls is very helpful.”
“Relatively quick turn-around/response time to email questions and requests for information”
Room for Improvement
“FDA was not very responsive to unscheduled phone calls and e-mails however responses, once received, were helpful.”
“Sometimes FDA did not respond to the emails which had questions.” Formal Letters: Beneficial
“Formal correspondence (meeting minutes, FDA response to questions) are most helpful.”
“Letters and TCs were comprehensive and timely.” “Formal letter addressed comments from earlier discussions related to the first 2
Phase 3 trials.” Room for Improvement
“There were multiple rounds of discussion and written feedback; when we were able to get on the phone it was much easier to resolve our issues.”
Unscheduled Phone Calls: Room for Improvement
“FDA was not very responsive to unscheduled phone calls and e-mails however responses, once received, were helpful.”
96

Scheduled Phone Calls: Beneficial
“The two conference calls were sufficient to attain agreement on key study design elements such that an in-person meeting was not necessary.”
In-Person Meetings: Beneficial
“FDA listened with great interest, asked good questions and provided feedback on path forward (In-person Meeting).”
“Ability to have a live discussion to be able to ask clarifying questions provides a significant benefit.”
“Provided multiple opportunities for discussion prior to start of trial - FDA requested sponsor submit protocol and SAP for review and comment prior to initiating trial – contacted sponsor w/in 2 weeks and provided opportunity to meet with FDA in 5 days; at end of meeting FDA requested an additional teleconference to discuss path forward.”
“We were able to come to an agreement for the trial design.” “The EOP2 meeting was beneficial as we obtained the Agency’s comments on all
aspects of the program and FDA’s input was much appreciated by the company.” “First discussion with FDA regarding program. Feedback led to additional discussions
around other clinical protocols (discussed 2nd phase 3 study prior to initiation of the 1st phase 3 study).”
“DMEP provided responses to sponsor questions which addressed many of the outstanding issues which allowed the Phase 3a to proceed. This did result in modifying the Ph3a program to address the Agencies.”
“(In-person meeting provided) clarification on their (FDA) position.” “We had a few Type C meeting request with the division, all the cases we received
the Agency's written responses with 75 days. FDA's feedback was very beneficial to move the program forward.”
“Most helpful: ability to discuss proposed pediatric trial design directly with division director.”
“Most helpful: End of Phase 2 meeting, type C procedural meeting, and pre-BLA meeting.”
“(In-person meeting) clarified data requirements for submitting the file to FDA.” “Due to contradictory agency advice (between EOP2 and preNDA), preNDA meeting
concluded without resolution of all issues. Follow up interactions with the agency (post-preNDA meeting) were assigned Type C meeting time frame.”
“We had Type C meeting for WR for different area of the project. It was very beneficial for the project to move forward.”
“Getting the feedback by a defined time allowed us to plan the follow-up activities.” “The in-person formal meeting was critical because of Sponsor shift in direction on
the desired indication. Key agreements reached in the meeting and confirmed in a subsequent telephone call included patient population, study design, and sample size.”
“FDA was prepared and they gave us good input.” “Meeting held to ensure phase 3 clinical trials would meet agency expectations.” “Engaged reviewers” “They took the time to review the protocol and supporting document and were able
to provide good responses to the questions we posed.”
97

Room for Improvement “Refusal to meet” “We had a number of meetings. Most were useful however a number of them
resulted in an identified need to escalate to FDA Sr. Officials.” “The company sought to engage in a Target Product Profile (TPP) meeting with
DMEP, to explore labeling and to aid in preparing for EOP2 meeting and development of Phase 3a program. The meeting was denied as the Division determined it was premature to engage in such discussions.”
“FDA was willing to engage on follow-up items from the EOP2 meeting however responses were not very timely.”
“Our EOR meeting was especially challenging as FDA was unable to agree internally, before meeting with the Sponsor, on the key aspects of a CVOT study that would allow for product approval. Eventually the Sponsor utilized the FDRR process.”
“Received written comments that were somewhat beneficial but did not provide a direct answer to our questions.”
ISSUE RESOLUTION Beneficial
“Feedback on interpretation of data was helpful and provided opportunity to discuss data and expectations and reach an understanding of a path forward.”
“Key agreements reached involved the entry criteria (for a condition with a complicated diagnosis), sample size and duration of the trials needed to support approval for chronic condition.”
“FDA provided clear feedback and opinions on the trial design and objectives agreement regarding trial design.”
“Additional preclinical testing and quality requirements in clinical trial design was required: (Delay) 6-9 months - FDA responded to questions submitted by email prior to submission of package.”
“Very helpful on endpoint discussions.” “Agreement (reached) regarding protocol modifications.” “FDA indicated additional studies were required and provided feedback on design of
studies.” “Communications were beneficial in providing clarity around phase 3a program and
resolving outstanding concerns FDA raised while phase 3a was ongoing.” “Gave clear reasons for hold (delay less than 6 months).” “IND review written comments had additional comments on the Phase 1 protocol,
which were resolved in a more timely manner using emails. These were followed up with formal responses. Phone calls were focused on getting the Phase 2a study initiated, and negotiating agency expectations to enable 2a start.”
“We had observed an AE that we communicated to the FDA. There was good interaction and constructive feedback and good understanding by FDA on the reasons behind what we were proposing and our next steps.”
“Questions asked were answered completely and resulted in a cancellation, requested by the Sponsor, of the face-to-face meeting.”
“Formal letters/submissions were helpful in follow-up to phone calls; meetings regarding study design and to address questions regarding the SPA.”
Room for Improvement
“Partial clinical hold – quality matters had to be updated when process changed: delayed 5 years.”
“Alignment on trials designs, study populations and endpoints was reached however the primary endpoints agreed at Phase II were not allowed to be included in the Full Prescribing Information at the time of final label negotiations.”
98

“The FDA had raised some concerns with part of the 3a program which were still outstanding after the EOP2 meeting. Additional correspondence (email/telephone/written response) and formal Type C meetings were held to address these issues.”
“Additional communications were conducted regarding the program that were not necessary prior to phase 3 start.”
“The Division was initially not willing to engage in early discussions on pediatric development plan, which was problematic reconciling with requirements in EU to initiate the pediatric program. After further discussion with the FDA they did provide preliminary feedback.”
“Between EOP2 and pre-NDA, there were several changes to division staff, and this may have contributed to inconsistency of agency advice.”
“We ended up following the FDRR process during the NDA review. The Review Division was consistently unable to provide clarity on viable options for moving forward. Interactions with Sr. FDA Officials were significantly more useful.”
“Regarding pre-specified meta-analysis, FDA position consistent with accepting meta-analysis results if for safety concern, but not accepting for comparative claims between products.”
Least helpful: Immunogenicity written responses; multiple rounds of written communications slowed down progress compared to phone communications
“HFE discussions on biologic/device combination were very challenging. Received different input from CDRH, OSE and DMEP at different times, and uncertain how to address FDA concerns. Was not clear what standard was for demonstrating safe use and what an acceptable use error profile was, and whether results could be considered to be at level of residual risk or not. Difficulty reconciling clinical safe use vs. HFE safe use.”
“The meeting was helpful in lifting the clinical hold but ultimately the concern that had triggered the partial hold was reduced when it was subsequently found that the nonclinical finding that had given rise to the concern was common for a number of products in that animal species. That is, a lengthy delay was incurred for what was ultimately found to be a nonissue.”
“PK questions to FDA had extended timeframes for feedback.” “Agreement and advice received from agency during EOP2 was changed significantly
after completion of pivotal study.” “Multiple rounds of meetings and communications regarding immunogenicity could
have been avoided if addressed appropriately in a formal forum earlier.” “Agreement and advice received from agency during EOP2 meeting changed
significantly after completion of the pivotal study.” “Agreement and advice given by the agency during the EOP2 meeting was changed
significantly after completion of the Phase 3 study.” “Agency responses related to clinical pharmacology questions were quite delayed.” “Most meetings were useful on some level; however significant (and creative)
forward progress only seemed to be made after the Sponsor identified the need to escalate to FDA Senior Officials”
99

APPENDIX 7: CDER DIVISION OF GASTROENTEROLOGY AND INBORN ERROR
PRODUCTS ADDITIONAL COMMENTS Below is a comprehensive list of additional comments from survey respondents with clinical development programs being reviewed by CDER Division of Gastroenterology and Inborn Error Products. OVERALL COMMUNICATIONS Beneficial
“Division is very responsive and collaborative.” “No delays caused by FDA.” “FDA provided important information about general concerns that needed to be
addressed to support clinical development.” “FDA did not provide detailed input on proposed clinical trial design but made us
aware of specific concerns that needed to be addressed in the clinical development program.”
“Creating an avenue by which to compress the clinical program” “They provided an aggressive path for the clinical development of the asset”
Room for Improvement
“Designation as combination product caused significant delays.” “FDA changing their mind on primary endpoint; not accepting science based
rationales; not understanding the indication and challenges.” “Our review division does not seem to understand the challenges of developing drugs
for rare diseases. They also have changed their advice to us on major issues - which has been challenging to us. They do not seem to appear to understand the indications they are in charge of and do not read our briefing documents completely.”
“FDA not current on some aspects of their own guidance. Subsequently, lack of dialogue to find a pragmatic solution.”
“Not all FDA reviewers were prepared for the pre-IND meeting and admitted to not reading the briefing book. The feedback given on the protocol design was not specific enough to understand exactly where their concerns were. Also, FDA did not have the correct reviewers present for pre-IND as we proposed a study in pediatric patients, yet no pediatricians were part of the pre-IND review.”
“FDA was very responsive and collegial, but their perspective and expectations on our development program changed significantly in the few-month interval between the pre-IND meeting and the IND submission. A wholesale change in review team membership may have exacerbated the inconsistencies encountered. This experience left us with a level of uncertainty regarding agreements reached with FDA, which increases the risk to product development.”
REGULATORY PROJECT MANAGER (RPM) Beneficial
“Project Manager was very responsive during IND review.” “RPM has always been responsive.” “Very responsive to emails and phone calls.” “Our new RPM is fantastic - very communicative, pleasant and appears to try to
answer questions as best as he can.”
100

“Our new RPM is great – he responds immediately to questions and provides information.”
“Seems to be action oriented, with desire to get all parties aligned” “Action oriented”
Room for Improvement
“Our RPM at the time was terrible in communicating with us. We got vague answers and very late responses to questions.”
“Working with project manager is typically efficient but can’t reach a members of the review team for specific questions where direct communication would be beneficial.”
“We responded to a couple of RFIs. At this time, our RPM at the time was terrible in communicating with us. We got vague answers and very late responses to questions. (This was up until now, mid 2014).”
“Working with project manager is typically efficient but can’t reach members of the review team for specific questions where direct communication would be beneficial.”
“RPM very friendly and responsive but not empowered to act without feedback from review team.”
“Very little communication; never picked up the phone and slow to respond to email and when the RPM did, it was not helpful.”
“Our old RPM was terrible. Very little communication; never picked up the phone and slow to respond to email and when she did, it was not helpful.”
SPECIFIC COMMUNICATION CHANNELS Email: Beneficial
“Email helped finding out status of FDA review.” “Email was beneficial to exchange information with the FDA quickly.” “Responded to emails promptly.” “Email communication was beneficial since we were able to get FDA feedback on a
specific matter very quickly.” Room for Improvement
“Very limited feedback was received by phone or email.” Formal Letters: Beneficial
“Letters provided clear responses to questions.” Room for Improvement
“Formal written responses have been unclear and required follow up for clarification.” Unscheduled Phone Calls: Beneficial
“FDA helpful on phone regarding pre-IND meeting planning and to determine if face-to-face or just written responses required.”
Scheduled Phone Calls: Beneficial
“Scheduled phone calls allowed us to have a conversation with the Reviewers to better understand their positions and explain our rationale.”
“Their comments are somewhat helpful to amend the current protocol design.”
101

Room for Improvement “Scheduled phone calls have been less productive.” “Did not provide clarity or reasons for information requested and no feedback was
provided at the end of the scheduled call.” “Very limited feedback was received by phone or email.”
In-Person Meetings: Beneficial
“The review division was quite collaborative at the in-person meetings (e.g. stayed over time).”
“Received feedback on proposed development program.” “Obtained clarity on Phase 3 study design and endpoint expectations to support
registration.” “In-person meetings are more productive.” “Most beneficial: EOP2 meeting, Special Protocol Assessments, Type C meetings.” “In-person meetings most productive.” “In-person meetings are the most productive.” “In-person meetings were the most helpful.” “(In person meeting provided) an opportunity to obtain FDA feedback on endpoint
requirements before requesting a Type B meeting.” “The meeting will address the clinical development plan, the supporting pre-clinical
safety program and the CMC aspects of the clinical supply.” “The f2f meeting was beneficial since the FDA pre-meeting comments were clear and
thorough and the discussion was collaborative and productive. It was also helpful in that FDA representatives from different functions and Offices were present, enabling us the opportunity to hear many different perspectives, and for them to hear each other.”
“Mapped out an aggressive clinical development path” Room for Improvement
“We had a turn over with different reviewers than those that were part of pre-IND meeting and review of Ph 1 study protocol resulting in differing opinions.”
“Due to time needed to address the general concerns raised, there was inadequate time to address specific trial design questions.”
“We’ve had mixed benefits.” “6 month – 1 year delay incurred due to no guidance from FDA during Pre-IND
meeting about combination product designation which required substantially more information.”
“Getting time with appropriate people difficult – takes a long time to get a meeting.” ISSUE RESOLUTION Beneficial
“Comments regarding non-clinical studies have been helpful.” “FDA very responsive to formal request for feedback regarding IND-enabling toxicity
study design.” “Very open dialogue between FDA and sponsor - very clear guidance given on clinical
trial endpoints for Phase 2b and Phase 3 trials in Crohn's disease.” “Type C written response addressed high level questions about registration endpoint
requirements. Helped the team design Ph3 study and preserved the Type B meeting that discussed the details of the Ph3 design and other development program questions.”
102

“The FDA highlighted the opportunity to accelerate the clinical plan by running the adequate and well controlled trial "concurrently" with the Phase 1/2a study. This has a dramatic impact on the corporate strategy.”
“Advocated that we advance into an adequate and well controlled study and skip the POC Phase 2 trial”
“FDA responded favorably to our proposed pre-clinical safety program.” “DGEIP was very helpful in guiding the program with respect to primary and
secondary endpoints for phase 2b and phase 3” “FDA correspondence addressed our questions point by point. The agency was clear
that an ISS would be required; however, an ISE was not required based on the proposed NDA submission plan.”
Room for Improvement
“Although the Division was clear on the intent to change the Crohn's Disease registration endpoints, the implementation was abrupt and lacked thorough public review of endpoint validation and feasibility data by stakeholders.”
“More information is required to finalize protocol.” “Extremely frustrating. The Division had not read the whole briefing book and the
appendices which had comprehensive information, rationales and data support. They also did a 180 on us. (Previously) we met to discuss our Phase 3 plan and our primary endpoint was agreed upon in writing. Then in the EOP2 meeting they told us this was not acceptable and we would need to use an outcome that would take us years to develop. They were also not aligned as a department. In the last 5 minutes of the meeting, the high-level officer came in and said he did not agree with what the division had just agreed to. The clinical reviewer did not understand the rare disease indication, the challenges or impact of our drug. We also received the FDAs Preliminary comments all 20 pages just 24 hours before the meeting. We spend months preparing the briefing book and preparing for the meeting; and get so little back from them.”
“It took two meetings and several correspondences/communications to reach consensus.”
“Clinical hold issues were not identified by FDA in pre-IND meeting – hold issues arose.” “(Previously) we met to discuss our Phase 3 plan and our primary endpoint was
agreed upon in writing. Then in the EOP2 meeting they told us this was not acceptable and we would need to use an outcome that would take us years to develop. They were also not aligned as a department…”
“FDA cited the protocol design as the reason for the clinical hold. There were two fundamental concerns: the number of invasive assessments (in peds and adults) and how the information received in adults would inform treatment in children. These concerns were not made clear enough during the pre-IND meeting and only brought up after we had submitted the IND.; We opted to withdraw the IND as not to go on clinical hold.”
“FDA could have been more prepared during the pre-IND meeting and been more clear in their comments on how they wanted us to revise the protocol. They should have offered to work with us on the protocol before we submitted the IND to prevent a clinical hold issue after submission. They didn't have the correct reviewers at the pre-IND meeting (i.e. pediatricians). FDA should provide feedback that is more clear and direct (i.e. easier to interpret).”
“Potential modifications to protocol inclusion/exclusion criteria during trial to address patient recruitment challenges were not accepted by Division with seemingly no possibility to dialogue whereas same protocol amendments were readily accepted by all other regulatory agencies globally (EU, Canada).”
“FDA was responsive to formal written correspondence only.”
103
APPENDIX 8: CDRH ADDITIONAL COMMENTS Below is a comprehensive list of additional comments from survey respondents with clinical development programs being reviewed by CDRH.
SPECIFIC COMMUNICATION CHANNELS Email: Room for Improvement
“Email provided limited value and often led to additional questions.” “FDA did not answer out email.” “Email was largely ineffective.”
Formal Letters: Beneficial
“Formal letter provided the most detailed information that enabled the company to move forward with Phase 2 plans. Phone calls were marginally useful to help provide clarification on key study design issues.”
In-Person Meetings: Beneficial
“Face-to-face meetings were most constructive.” “Face-to-face meetings were most productive and helpful.” “Face-to-face meetings always resulted in better understanding of complex issues.” “In-Person meetings more effective than phone calls.”
104