deactivating peripheral nerve triggers: a surgical solution to
TRANSCRIPT
WILLIAM G. AUSTEN JR., MD
CHIEF, DIVISION OF PLASTIC & RECONSTRUCTIVE SURGERY
CHIEF, DIVISION OF BURN SURGERY
MGH TRUSTEES CHAIR
Massachusetts General Hospital, Harvard Medical School
Deactivating Peripheral Nerve Triggers:
A Surgical Solution to Refractory Headaches
Founder of Cytrellis Biosystems
DISCLOSURES

WE CAN ONLY KNOW THAT WE
KNOW NOTHING
-TOLSTOY
SOCRATIC PARADOX
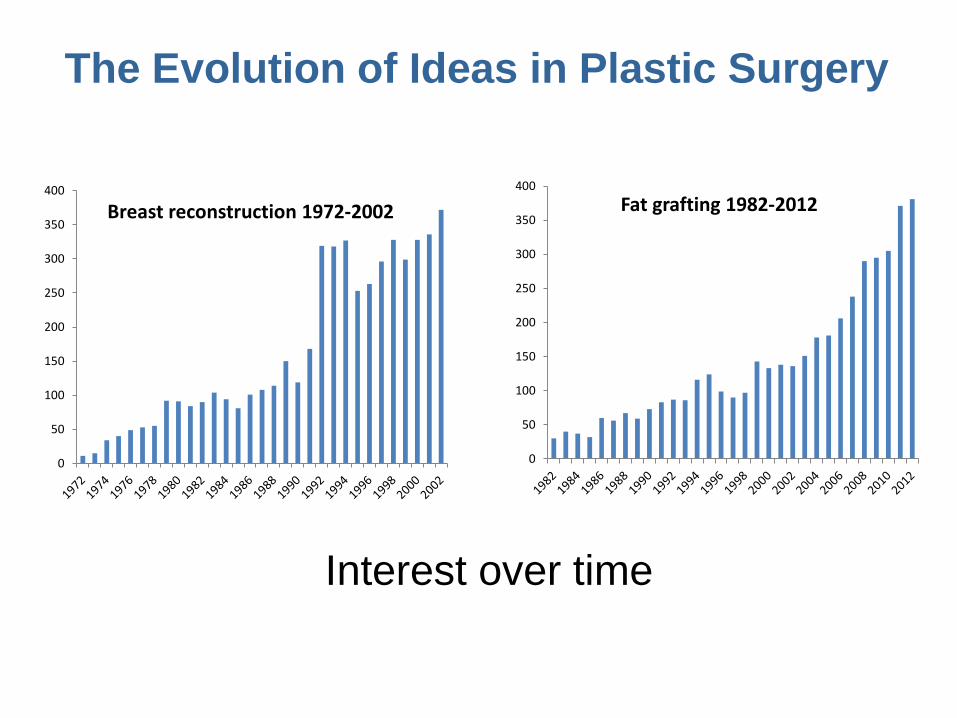
The Evolution of Ideas in Plastic Surgery
0
50
100
150
200
250
300
350
400
Fat grafting 1982-2012
0
50
100
150
200
250
300
350
400
Breast reconstruction 1972-2002
Interest over time
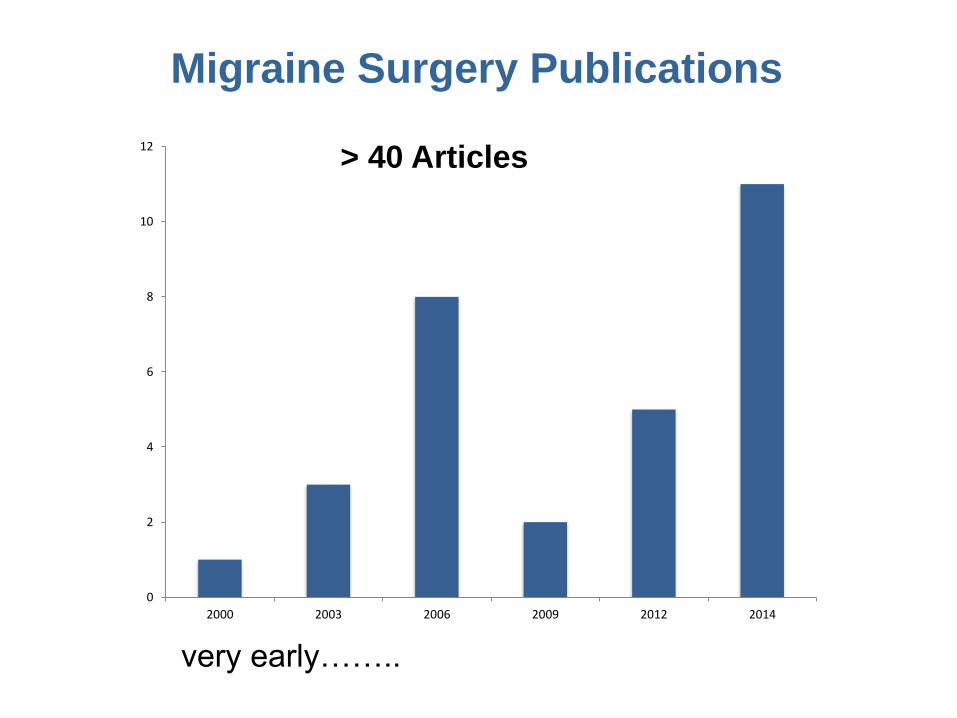
Migraine Surgery Publications
0
2
4
6
8
10
12
2000 2003 2006 2009 2012 2014
very early……..
> 40 Articles
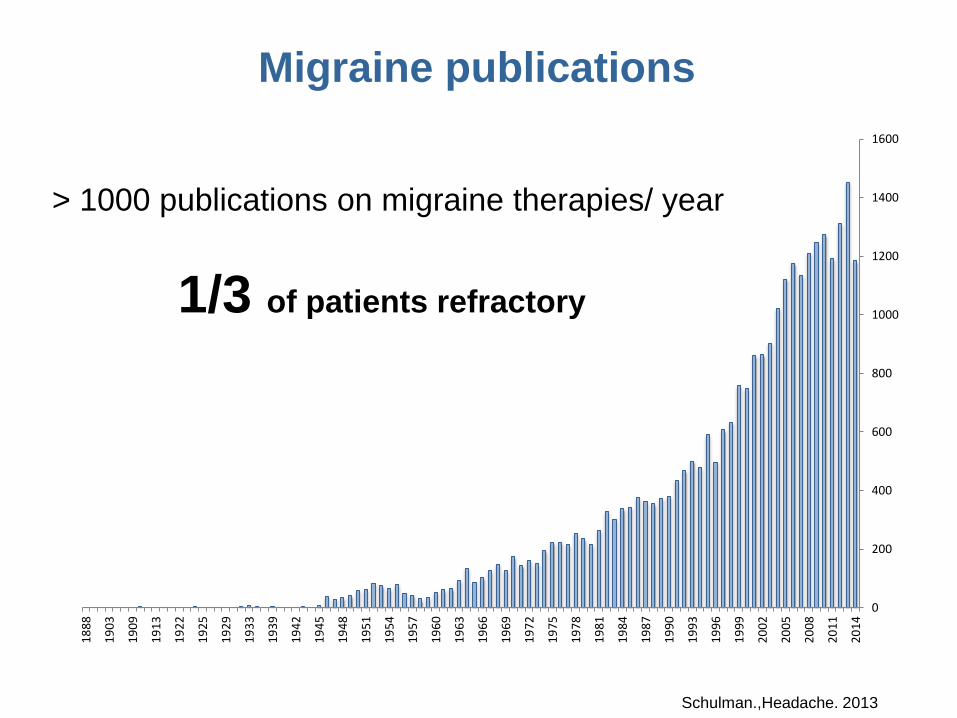
> 1000 publications on migraine therapies/ year
1/3 of patients refractory
0
200
400
600
800
1000
1200
1400
1600
20
14
20
11
20
08
20
05
20
02
19
99
19
96
19
93
19
90
19
87
19
84
19
81
19
78
19
75
19
72
19
69
19
66
19
63
19
60
19
57
19
54
19
51
19
48
19
45
19
42
19
39
19
33
19
29
19
25
19
22
19
13
19
09
19
03
18
88
Migraine publications
Schulman.,Headache. 2013

0
200
400
600
800
1000
1200
1400
1600
20
14
20
11
20
08
20
05
20
02
19
99
19
96
19
93
19
90
19
87
19
84
19
81
19
78
19
75
19
72
19
69
19
66
19
63
19
60
19
57
19
54
19
51
19
48
19
45
19
42
19
39
19
33
19
29
19
25
19
22
19
13
19
09
19
03
18
88
Migraine publications
SHOULD WE THINK ABOUT
ALTERNATIVES ?
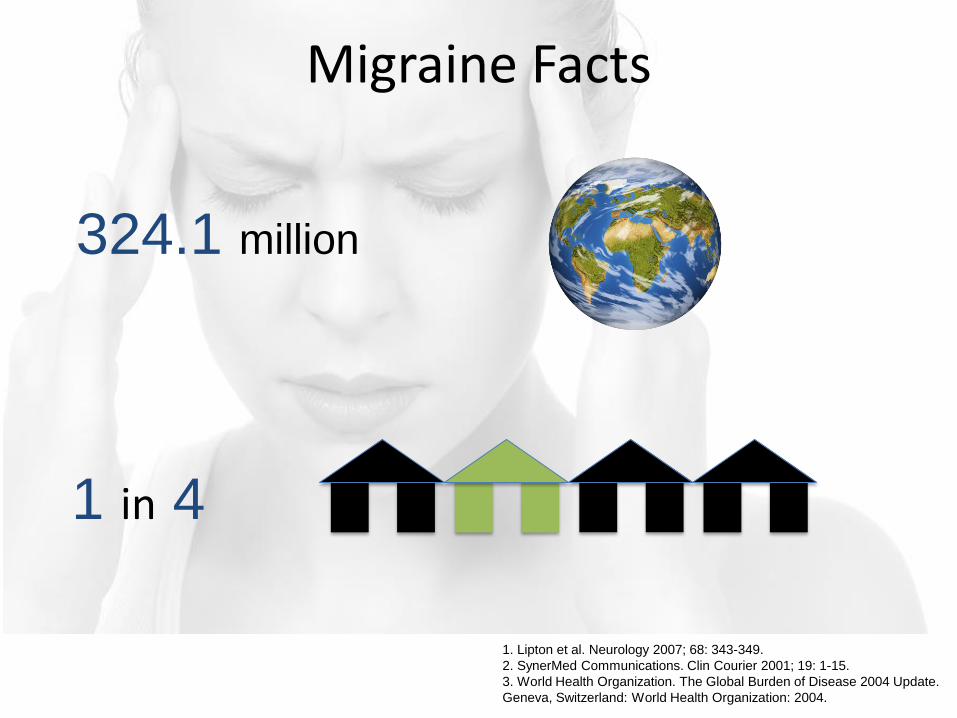
Migraine Facts
324.1 million
1 in 4
1. Lipton et al. Neurology 2007; 68: 343-349.
2. SynerMed Communications. Clin Courier 2001; 19: 1-15.
3. World Health Organization. The Global Burden of Disease 2004 Update.
Geneva, Switzerland: World Health Organization: 2004.

Significance
35MILLION Americans
3 : 1
1. Stewart et al. J Clin Epidemiol 1995
2. Stewart et al. Cephalalgia 2008
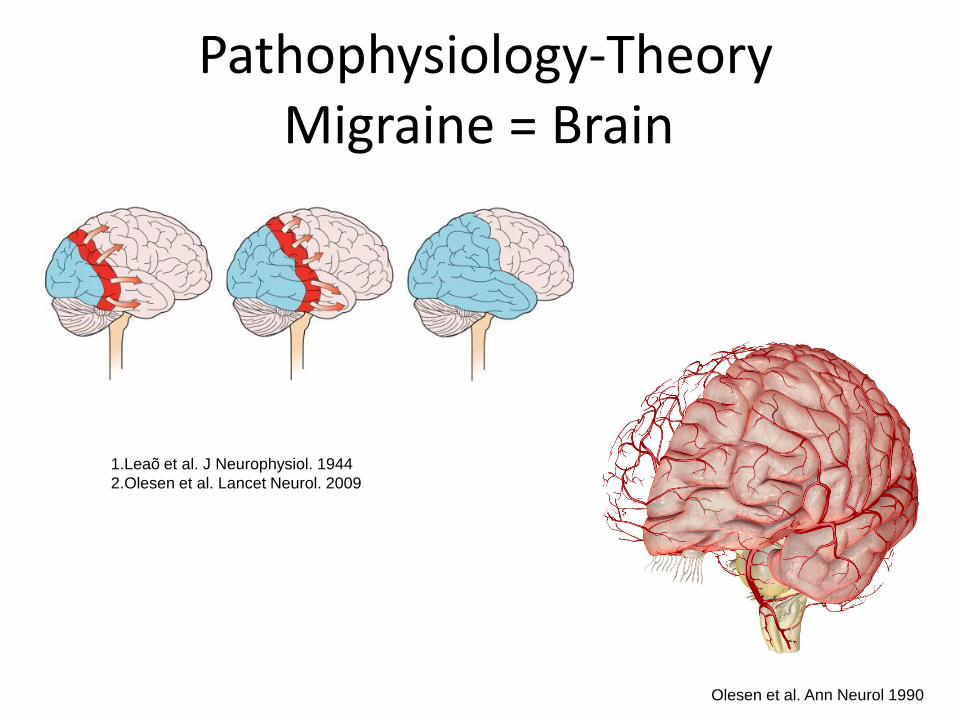
Pathophysiology-TheoryMigraine = Brain
Olesen et al. Ann Neurol 1990
1.Leaõ et al. J Neurophysiol. 1944
2.Olesen et al. Lancet Neurol. 2009

Why Surgery ?
Observation

Migraine Therapies
Side Effects
Contraindications
NON- Responders
1. Dodick et al. Headache 2005
2. Blumenfeld et al. Headache 2013

New Developments- Late 1990s
Botulinum Toxin for the Treatment of Migraine
2010
FDA approved

Observation- 2000
Dr. Bahman Guyuron
349 brow- lift patients
- 79% migraine improved
? CARPAL TUNNEL SYNDROME OF THE HEAD ?

Pathophysiology
Nerve Irritation
(muscle, fascia, bone, vessels)
Substance P/ Cytokines
Inflammation/Pain

Theory
1. Janis et. al, PRS 2010
2. Janis et. al, PRS 2010
3. Janis et. al, PRS 2012

Frontal
Temporal
Occipital
Nasal
1. Janis et. al, PRS 2010
2. Janis et. al, PRS 2010
3. Janis et. al, PRS 2012
2005
92%>50% reduction of migraine
2009
2005
PLACEBO CONTROLLED TRIAL WITH SHAM SURGERY
83.7% real surgery
57.7% sham surgery
>50% reduction of migraine
2009
2005
PLACEBO CONTROLLED TRIAL WITH SHAM SURGERY
57.1 % real surgery
3.8 % sham surgery
TOTAL ELIMINATION OF
MIGRAINES
2011
88% >50% reduction of migraine

2015
Clinical Data
> 50% improvement between 62- 95%

Oct
2008
Looking back on my own practice…

Gathering a Team
2009
2009
The 1st Year
NEW
CONSULTS
SURGERY1
5

2010NEW
CONSULTS
SURGERY2
7
The 2nd Year

Patient recruitment
Skepticism - Neurology
Patient selection
Insurance coverage
Challenges

Importance of Media
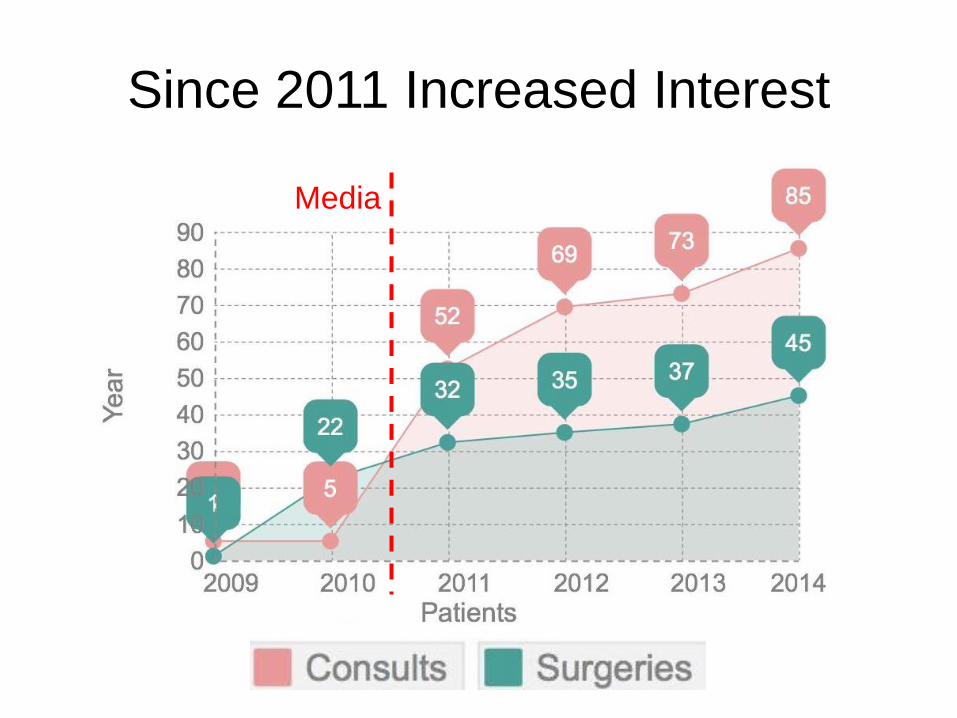
Since 2011 Increased Interest
Media

Patient recruitment
Skepticism - Neurology
Patient selection
Insurance coverage
Challenges

The art of identification
1. Establish diagnosis in refractory patient
1. Identification of specific trigger points
1. Clinical evaluation & diagnostic testing
Patient must HAVE BEEN followed by a NEUROLOGIST

The art of identification
1. Establish diagnosis in refractory patient
1. Identification of specific trigger points
1. Clinical evaluation & diagnostic testing
Patient must HAVE BEEN followed by a NEUROLOGIST

The art of identification
1. Establish diagnosis in refractory patient
1. Identification of specific trigger points
1. Clinical evaluation & diagnostic testing
Patient must HAVE BEEN followed by a NEUROLOGIST
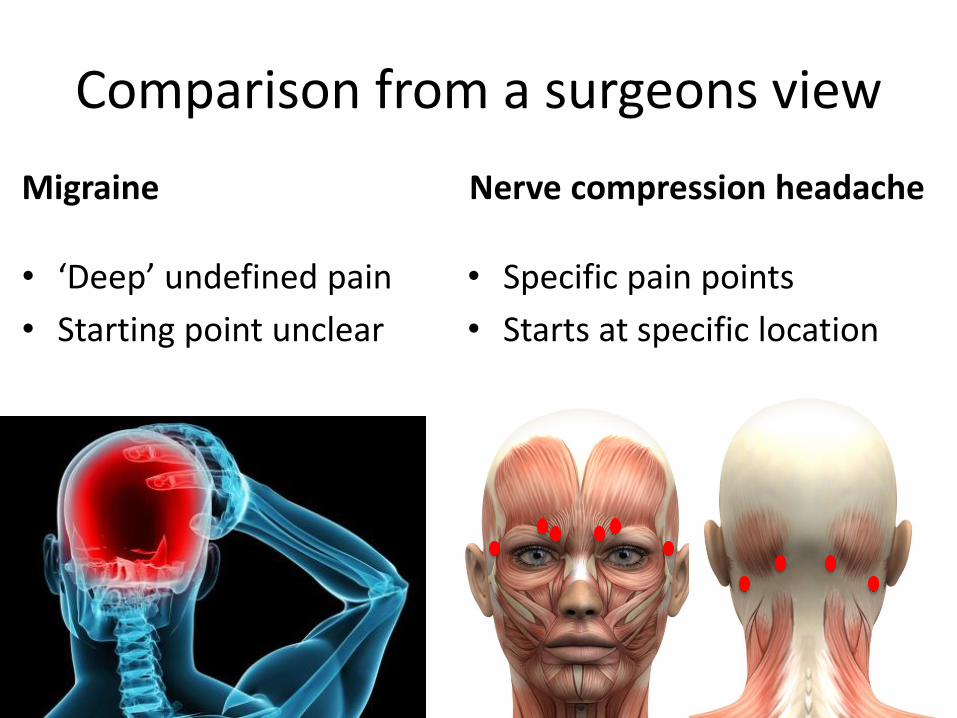
Comparison from a surgeons view
Migraine
• ‘Deep’ undefined pain
• Starting point unclear
Nerve compression headache
• Specific pain points
• Starts at specific location
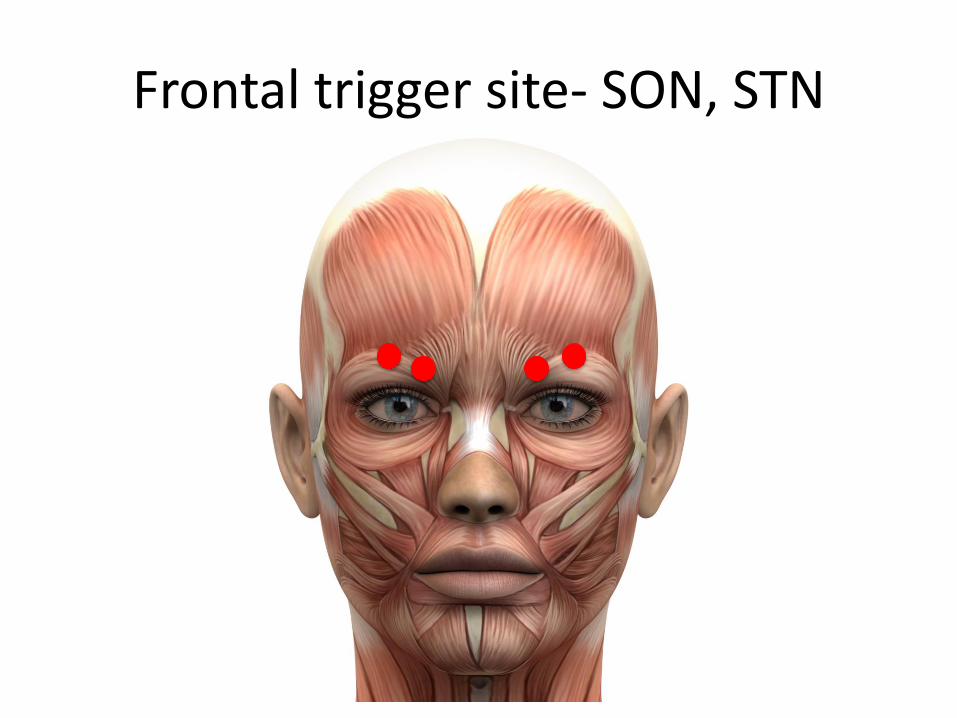
Frontal trigger site- SON, STN
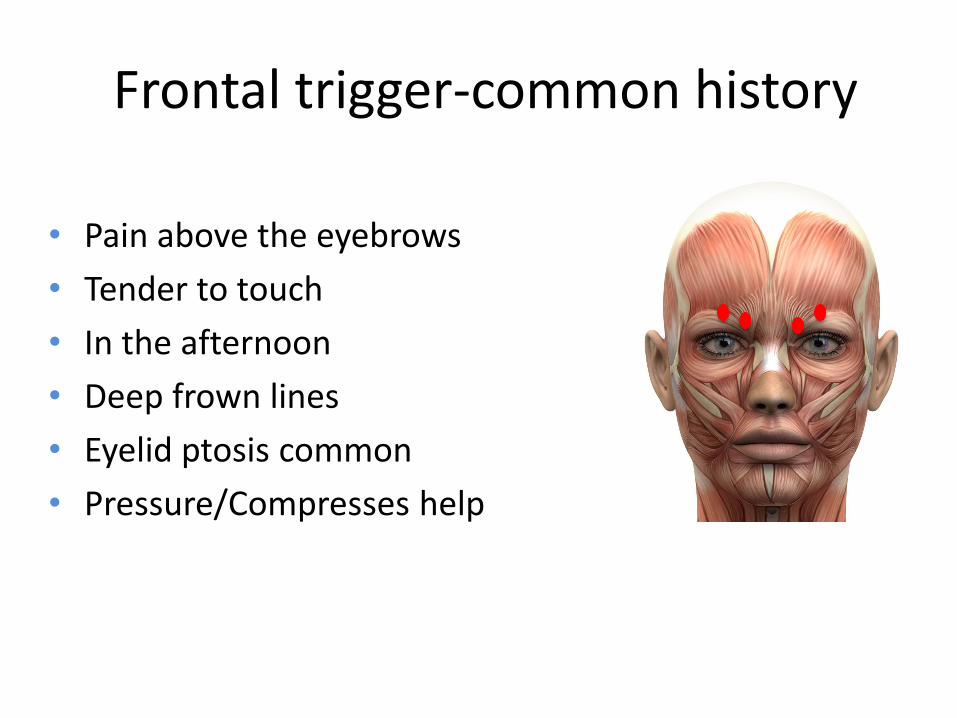
Frontal trigger-common history
• Pain above the eyebrows
• Tender to touch
• In the afternoon
• Deep frown lines
• Eyelid ptosis common
• Pressure/Compresses help
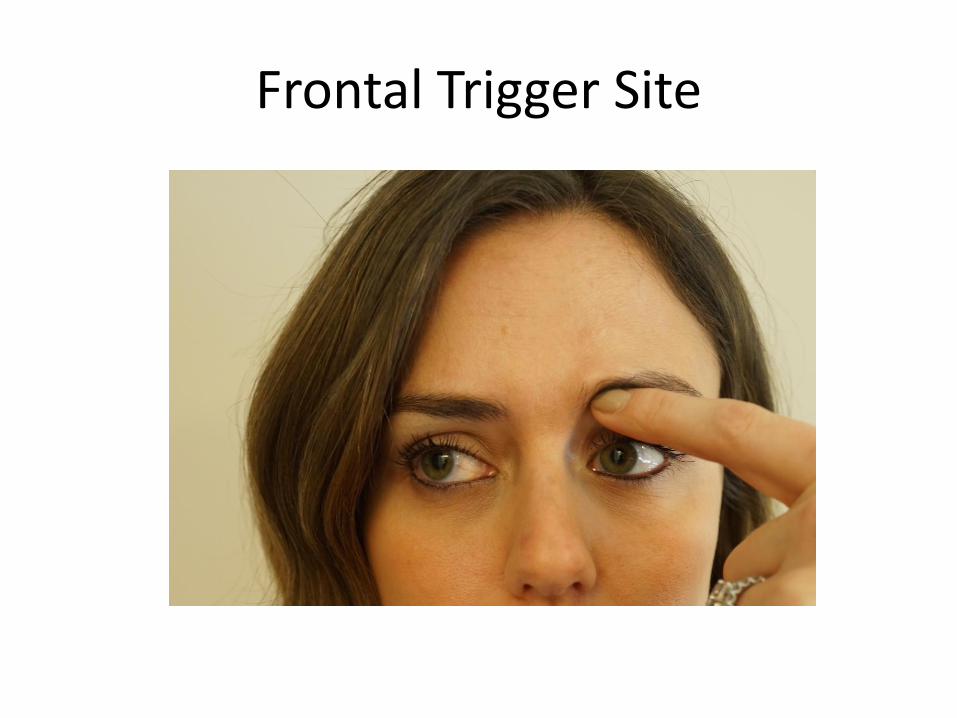
Frontal Trigger Site
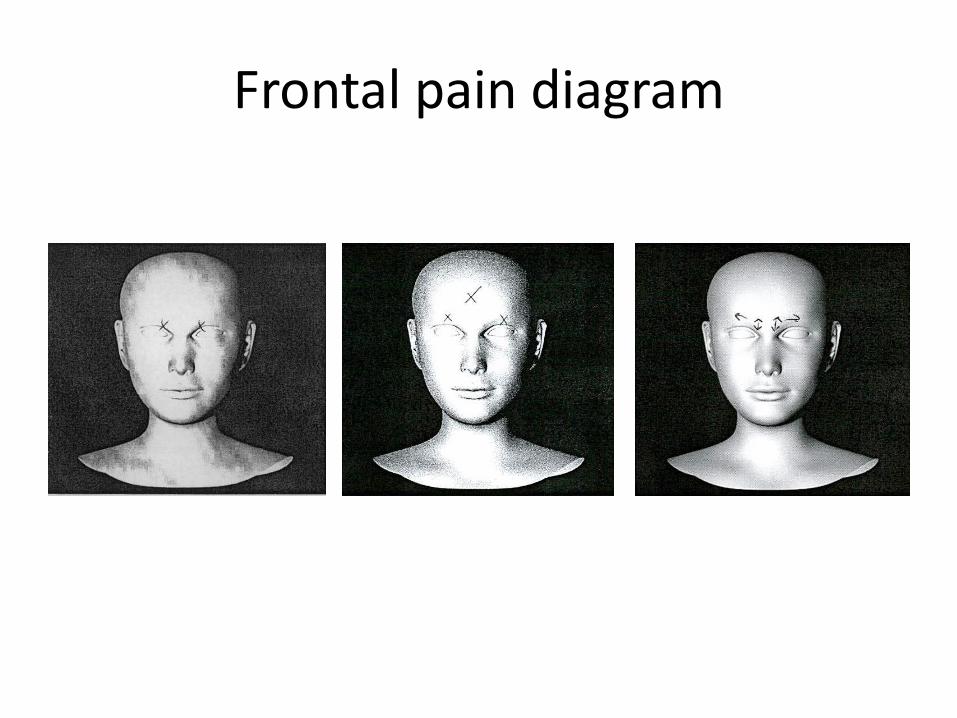
Frontal pain diagram

Abnormal frontal pain diagram
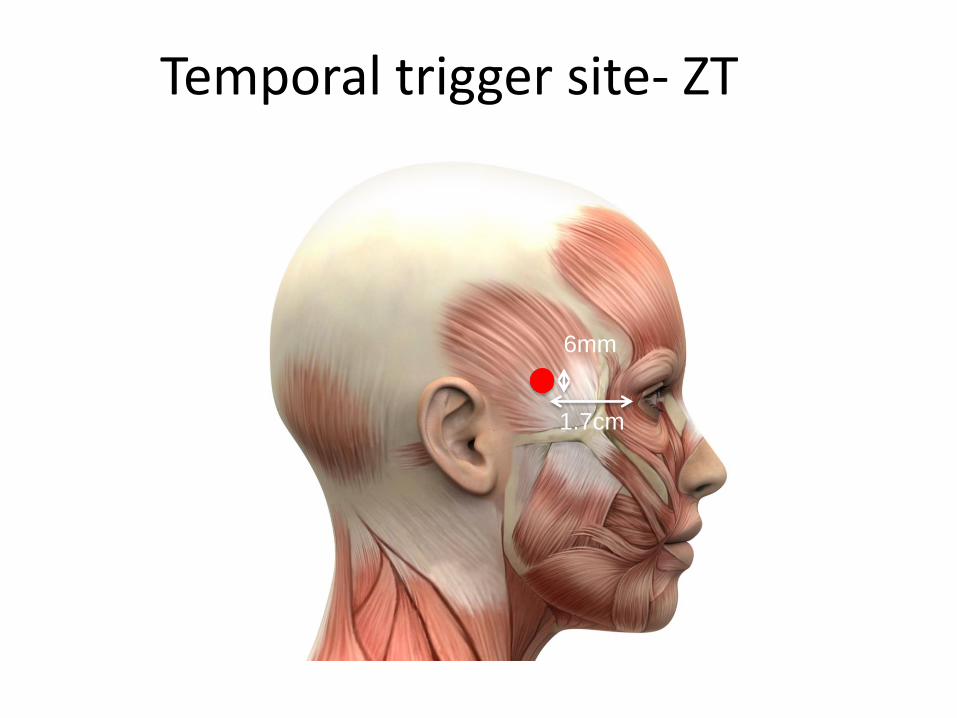
Temporal trigger site- ZT
1.7cm
6mm

Temporal trigger- common history
• Pain starts at temple
• Patients wake up with pain
• Bruxism very common
• Often throbbing pain
• Pressure/ compresses help

Temporal trigger site
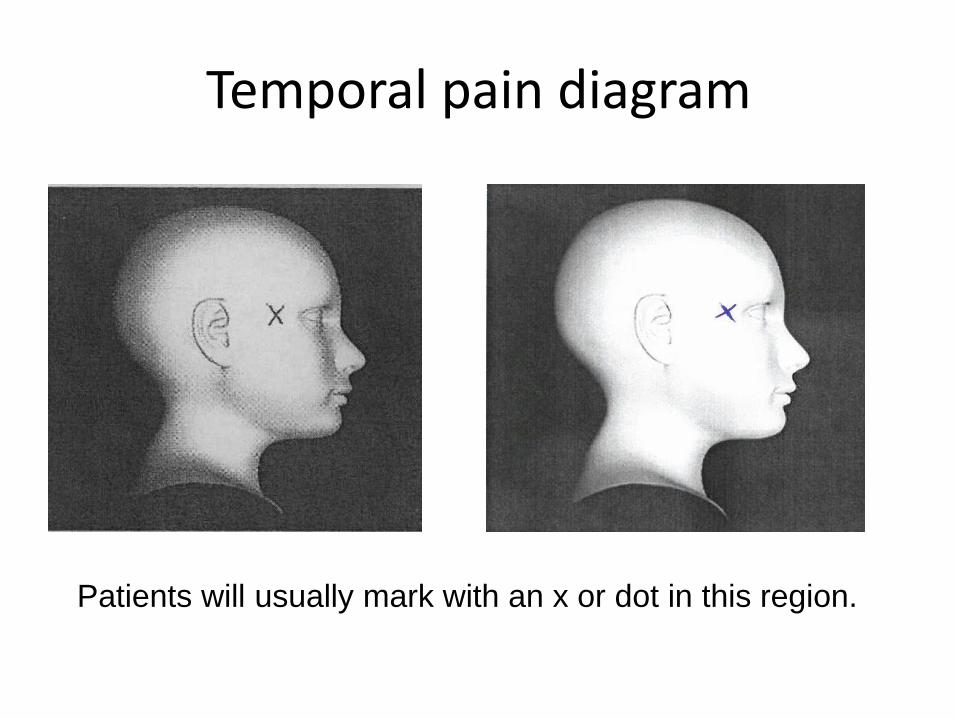
Temporal pain diagram
Patients will usually mark with an x or dot in this region.
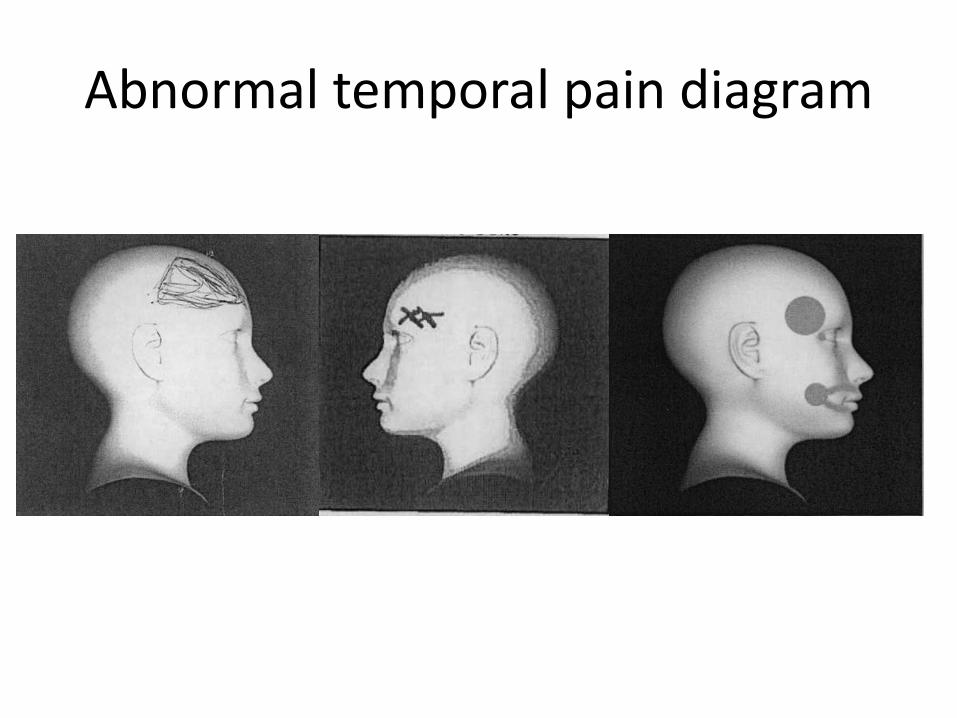
Abnormal temporal pain diagram

Occipital trigger site- GON
occipital
protuberance
3cm
1.5cm
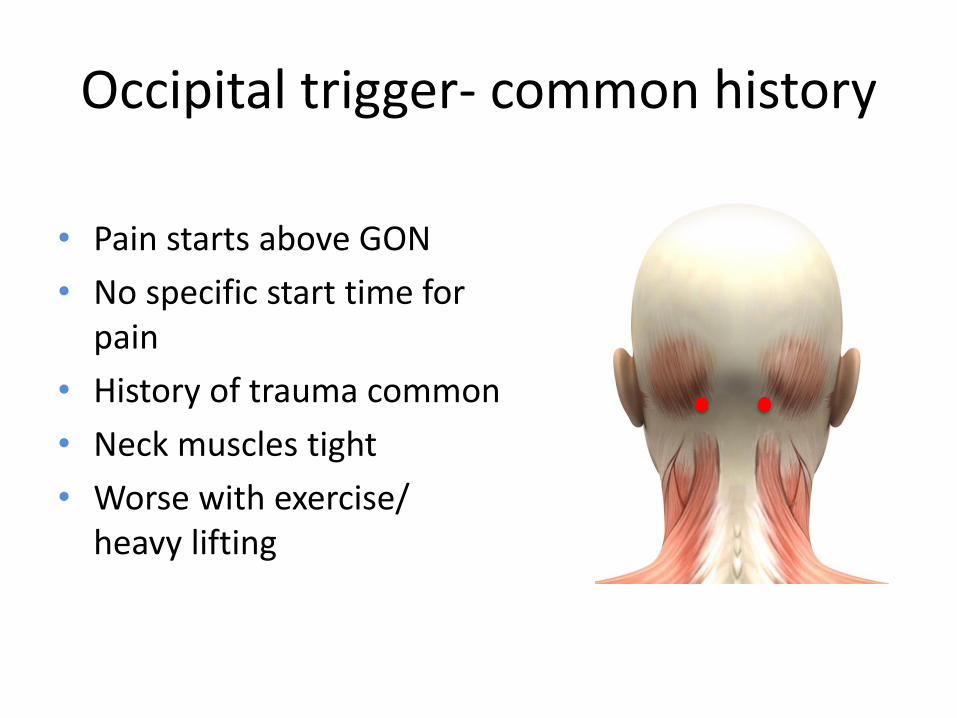
Occipital trigger- common history
• Pain starts above GON
• No specific start time for pain
• History of trauma common
• Neck muscles tight
• Worse with exercise/ heavy lifting

Occipital trigger site
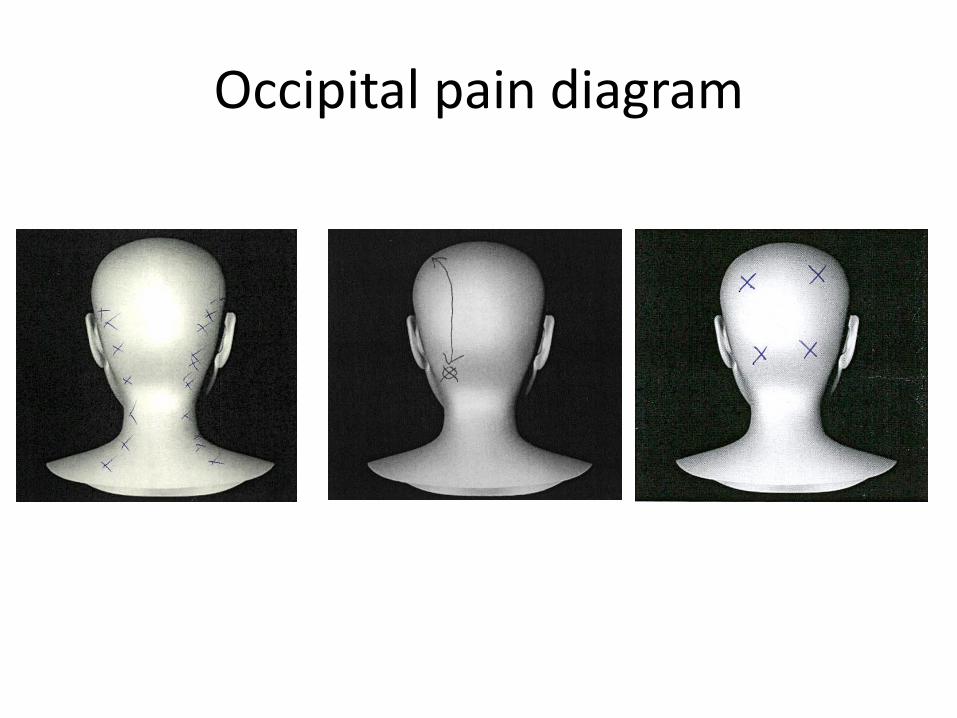
Occipital pain diagram
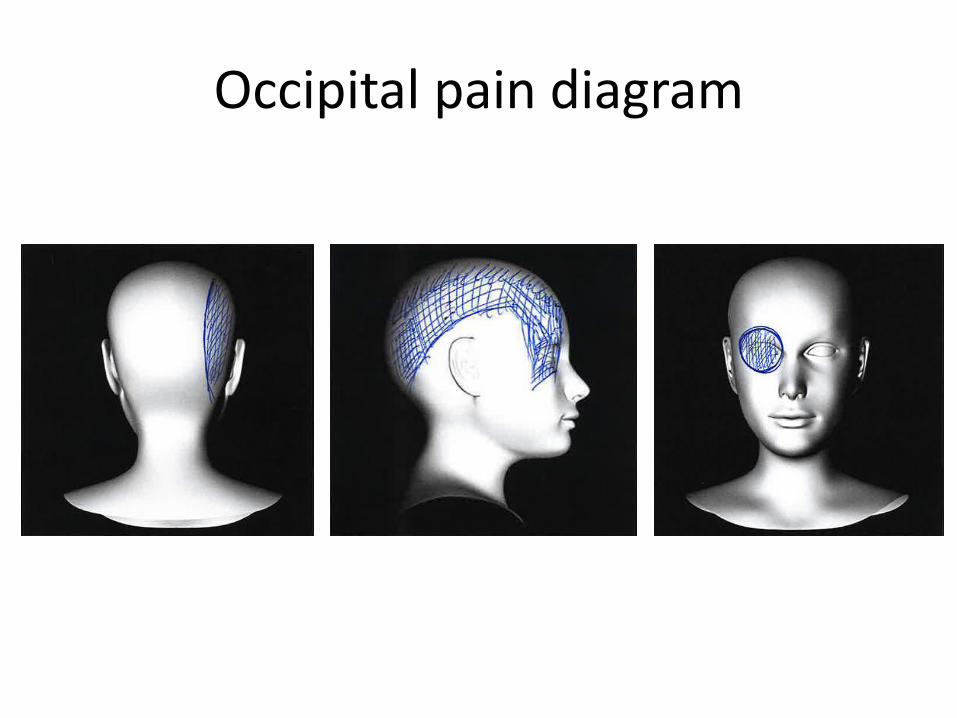
Occipital pain diagram
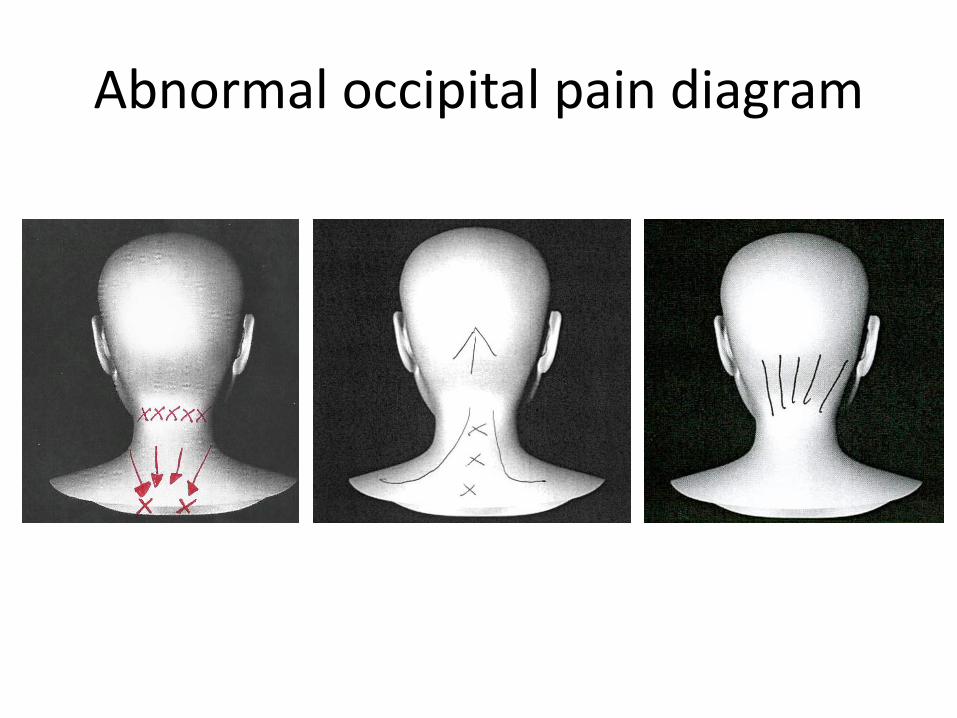
Abnormal occipital pain diagram

Rhinogenic trigger site
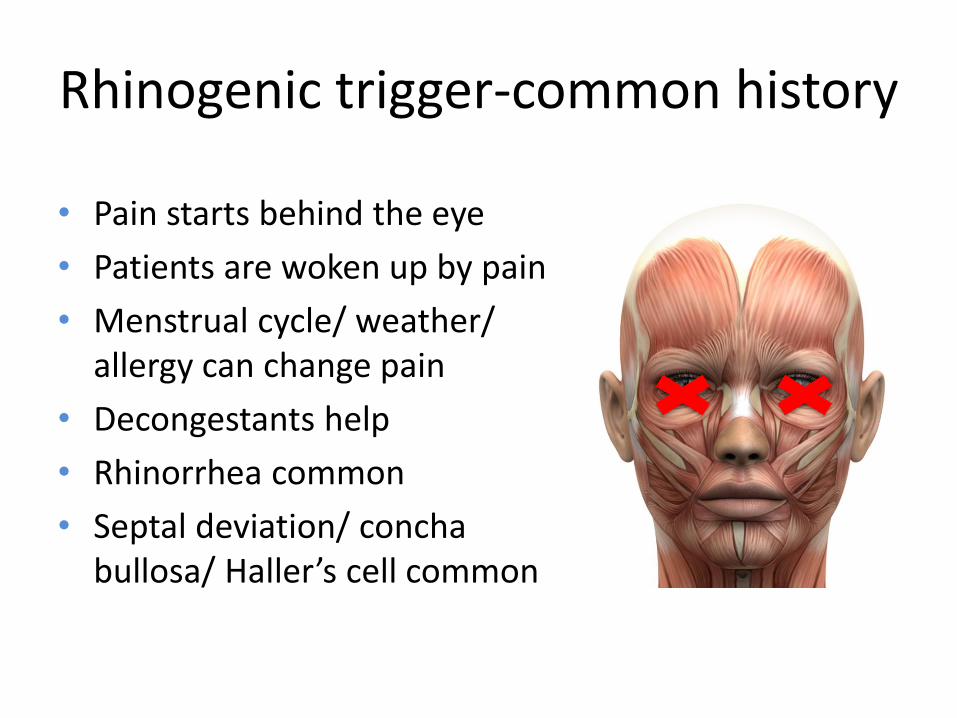
Rhinogenic trigger-common history
• Pain starts behind the eye
• Patients are woken up by pain
• Menstrual cycle/ weather/ allergy can change pain
• Decongestants help
• Rhinorrhea common
• Septal deviation/ concha bullosa/ Haller’s cell common

Rhinogenic pain diagram
The art of identification
1. Establish diagnosis in refractory patient
1. Identification of specific trigger points
1. Clinical evaluation & diagnostic testing
Patient must HAVE BEEN followed by a NEUROLOGIST
Botox/ Nerve blocks?
Doppler Ultrasound
Arterial versus non- arterial trigger
• Especially useful in identification of
minor triggers
• Too early to understand impact
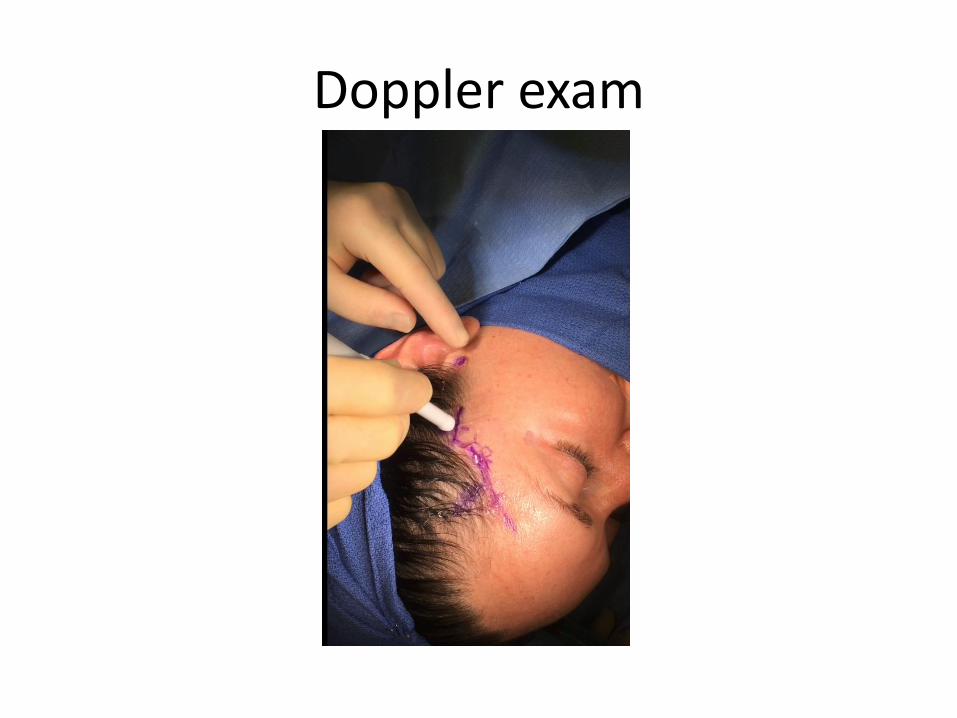
Doppler exam

CT scan
Detection of nasal pathology
Deviated Septum/
Concha Bullosa
Haller Cell

History/ Nerve Block and/or Botox Injection/ Doppler/ Imaging
to identify trigger sites
✔✖
NEUROLOGYPAIN SERVICE ENT
Two Pathways

Posterior triggers GON/LON
Ducic et al. Plast. Recon. Surg. 2009
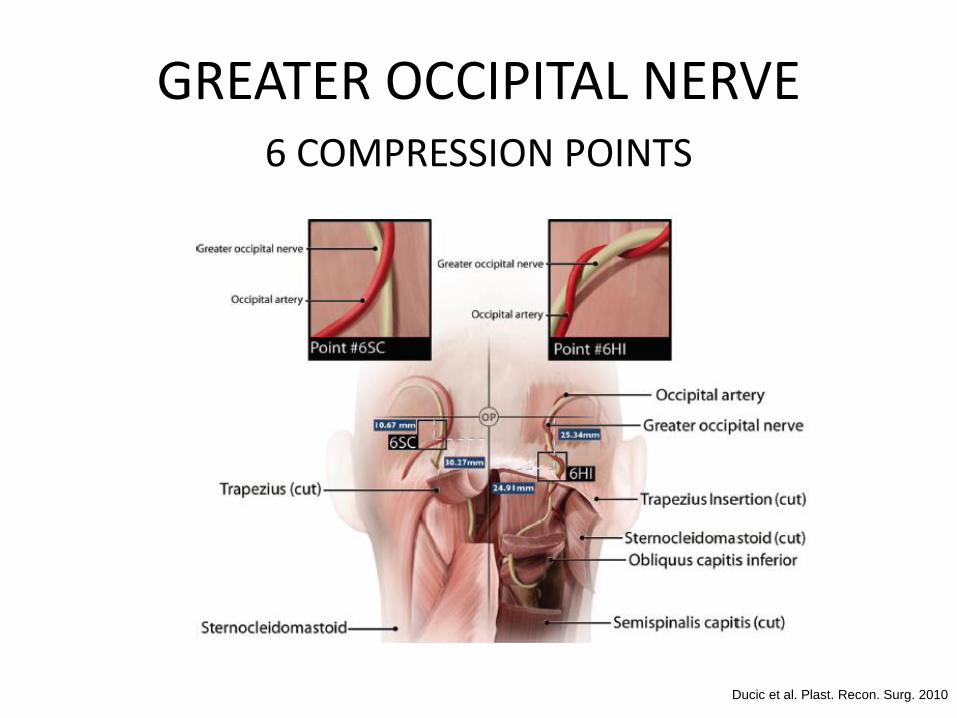
GREATER OCCIPITAL NERVE6 COMPRESSION POINTS
Ducic et al. Plast. Recon. Surg. 2010

Injection local
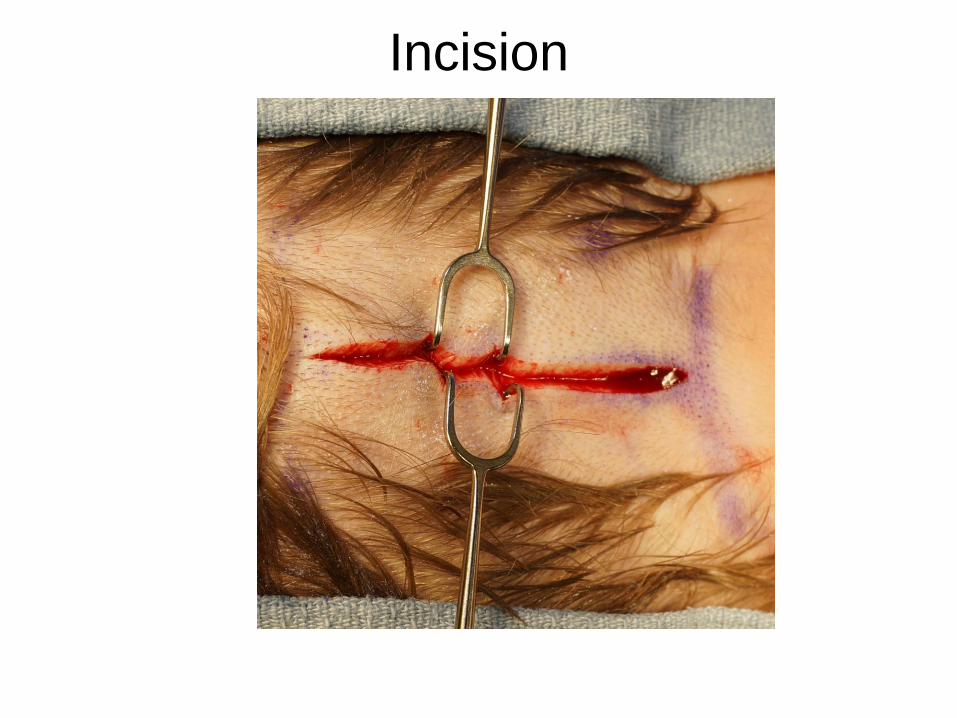
Incision
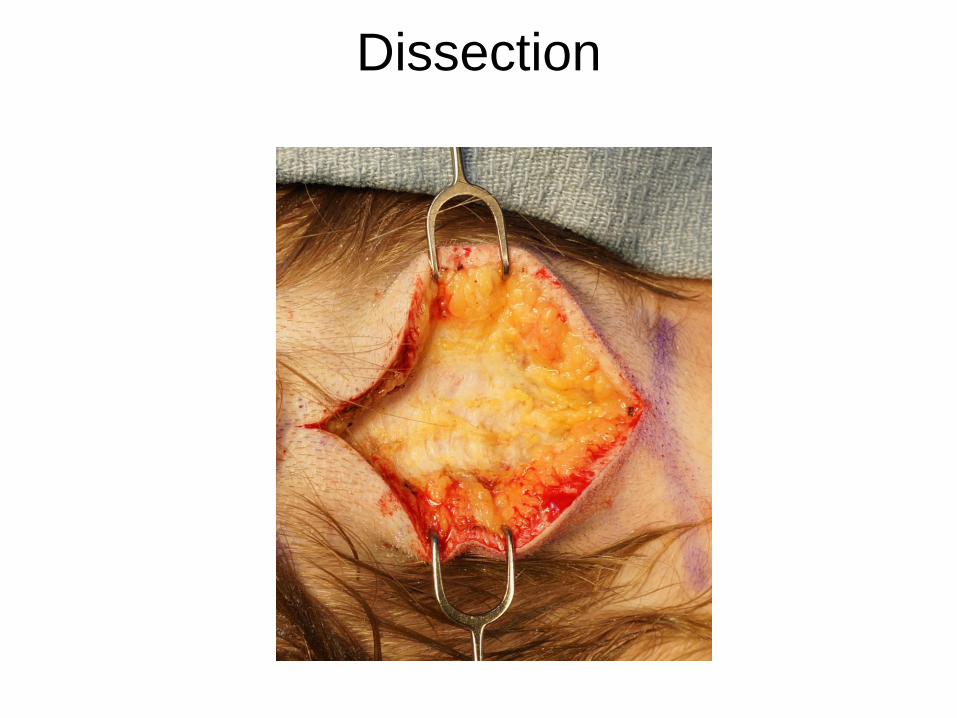
Dissection

Fascia elevation

Fascia elevation

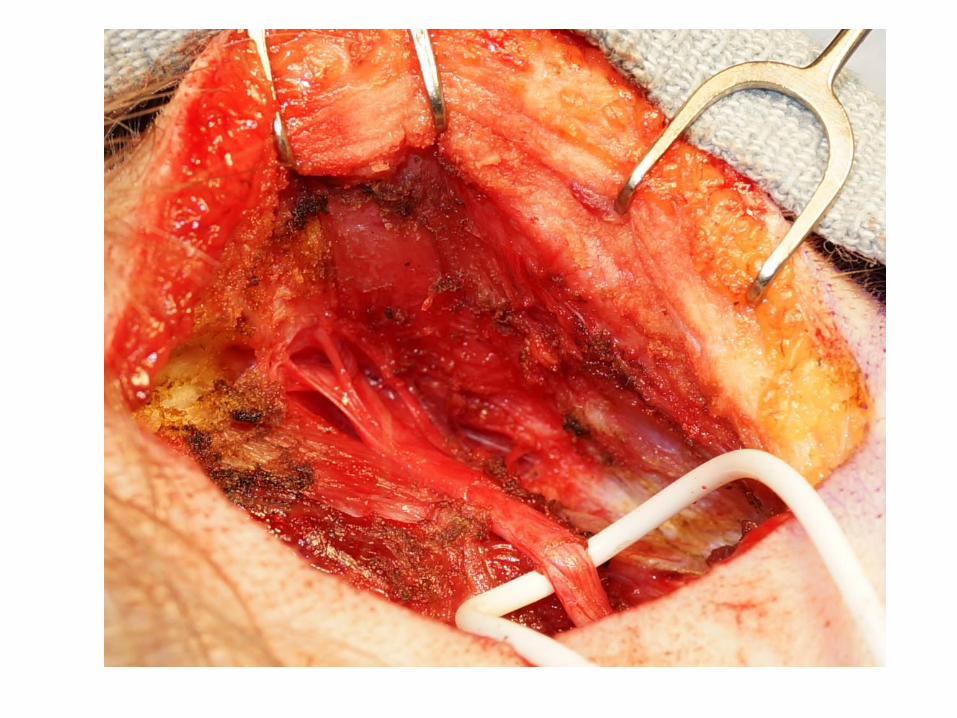
GON exposure

GON
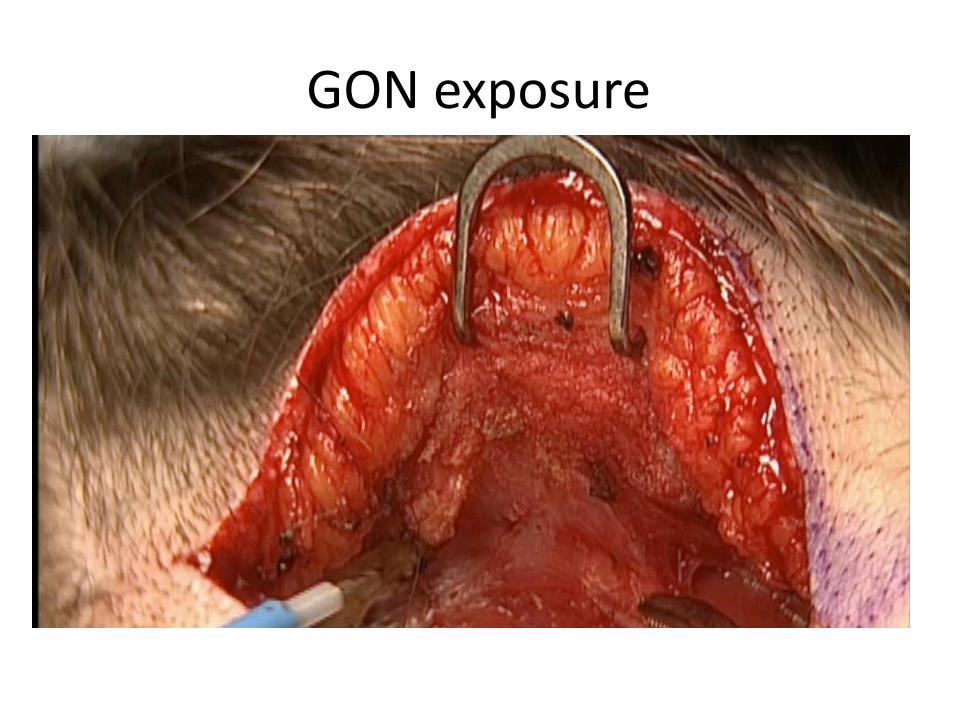
GON exposure

Muscle removal

Muscle removal


Post fascia and muscle removal

OCCIPITAL ARTERY
GON

Adipose fat flap

Complete release

Closure and drain
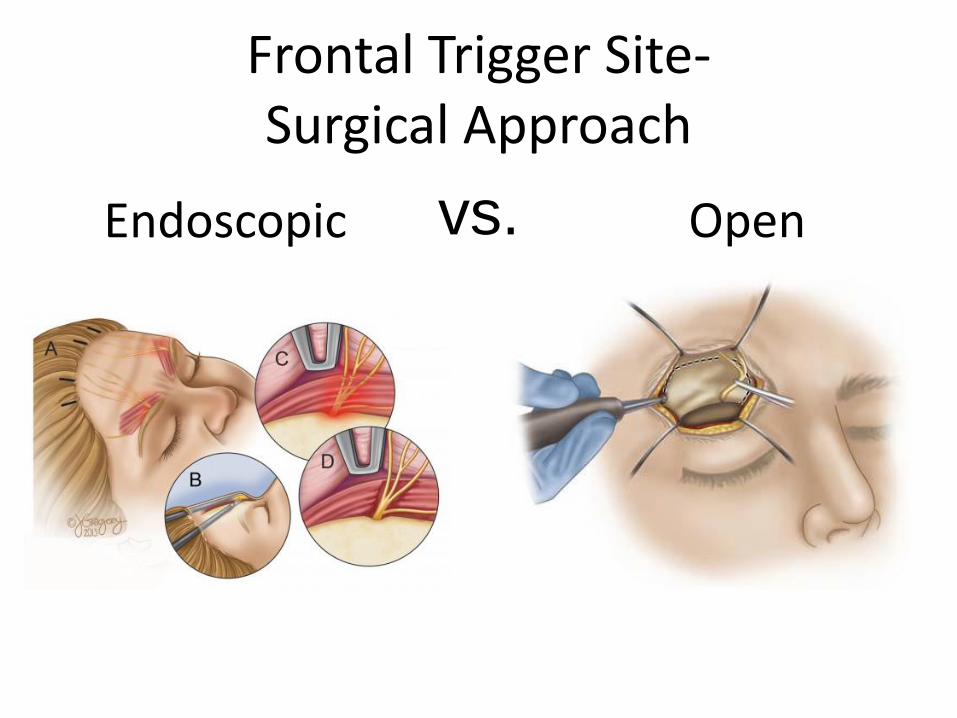
Frontal Trigger Site-Surgical Approach
Endoscopic Openvs.

Anatomy SON/STN
Liu et al.. Plast Reconstr Surg. 2011.

Removal Upper Eyelid Skin

Dissection to the Orbital Rim

Dissection to the orbital rim

Identification of Nerves

Supraorbital
Nerve
Supratrochlear
Nerve
Frontal Trigger Site- SON/STN

Fascial band versus supraorbital foramen
Falluco, M et al.. Plast Reconstr Surg. 2012.

Foraminectomy

Supraorbital Foramen

Two nerves exiting through foramen

Very high supraorbital foramen
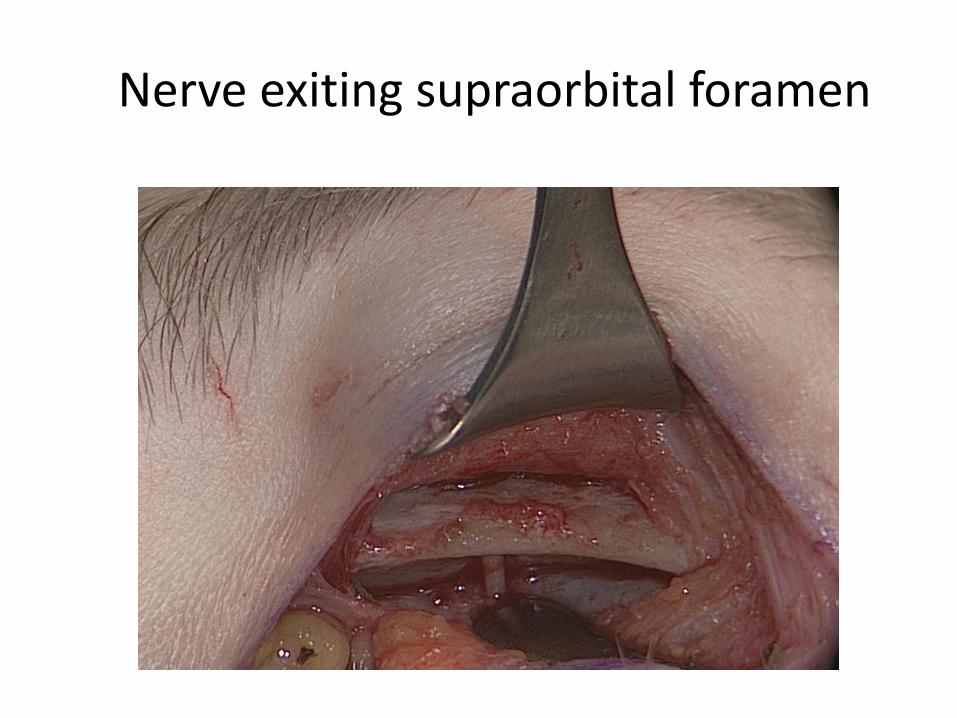
Nerve exiting supraorbital foramen
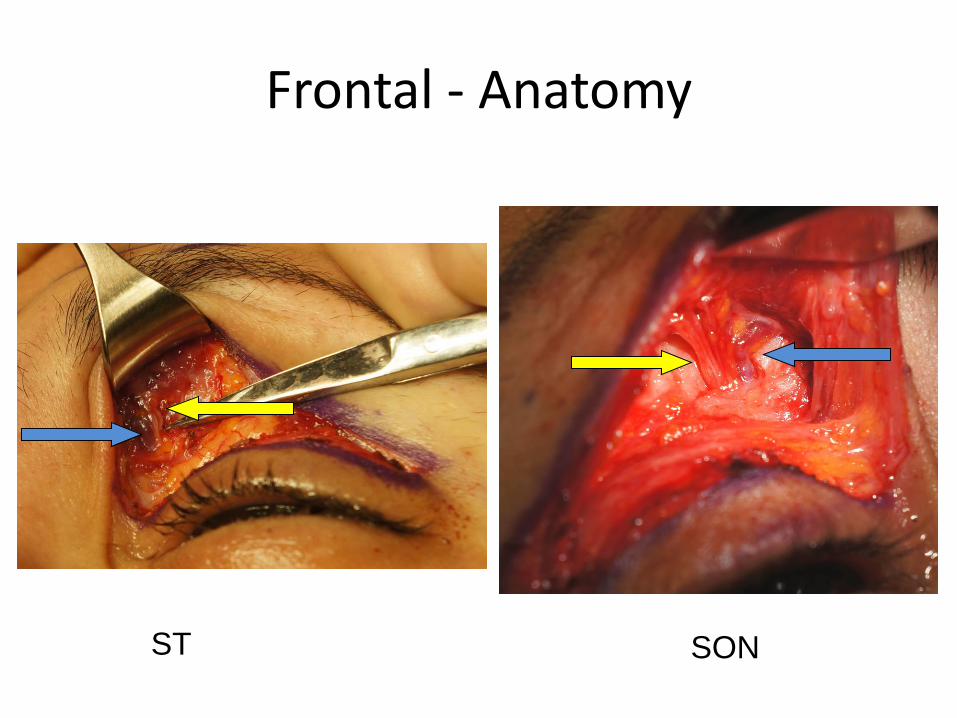
Frontal - Anatomy
ST SON

Aberrant Nerve
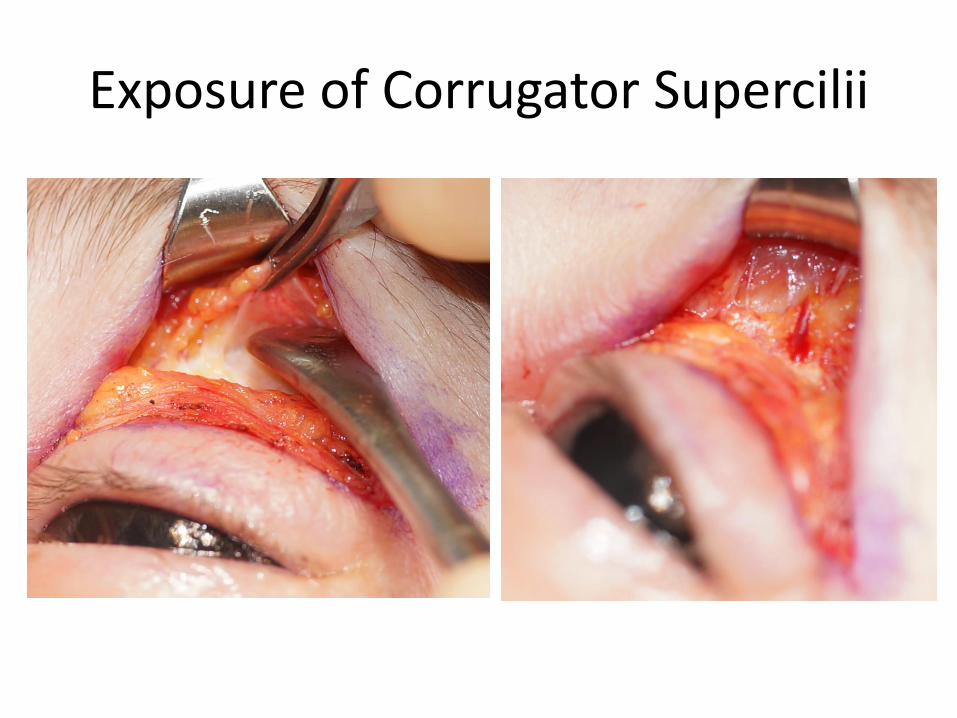
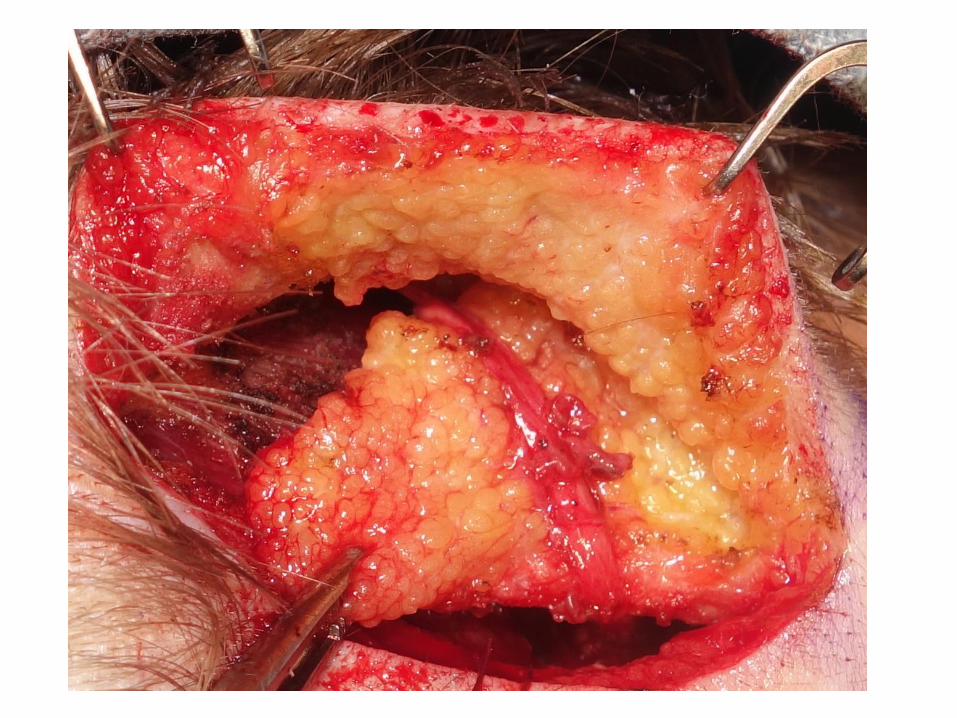
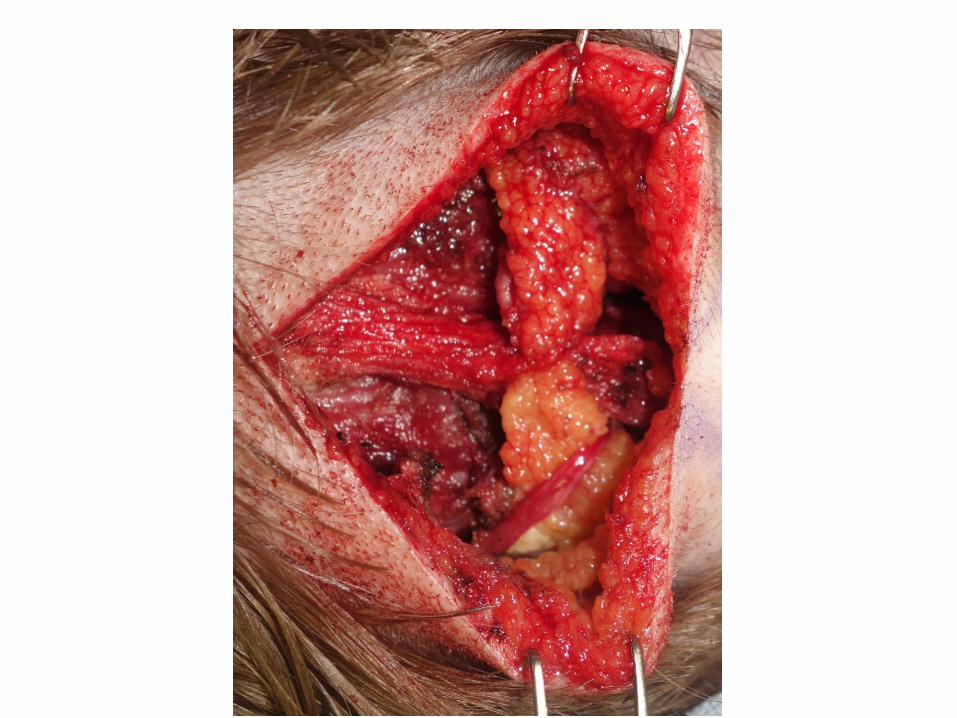
Exposure of Corrugator Supercilii
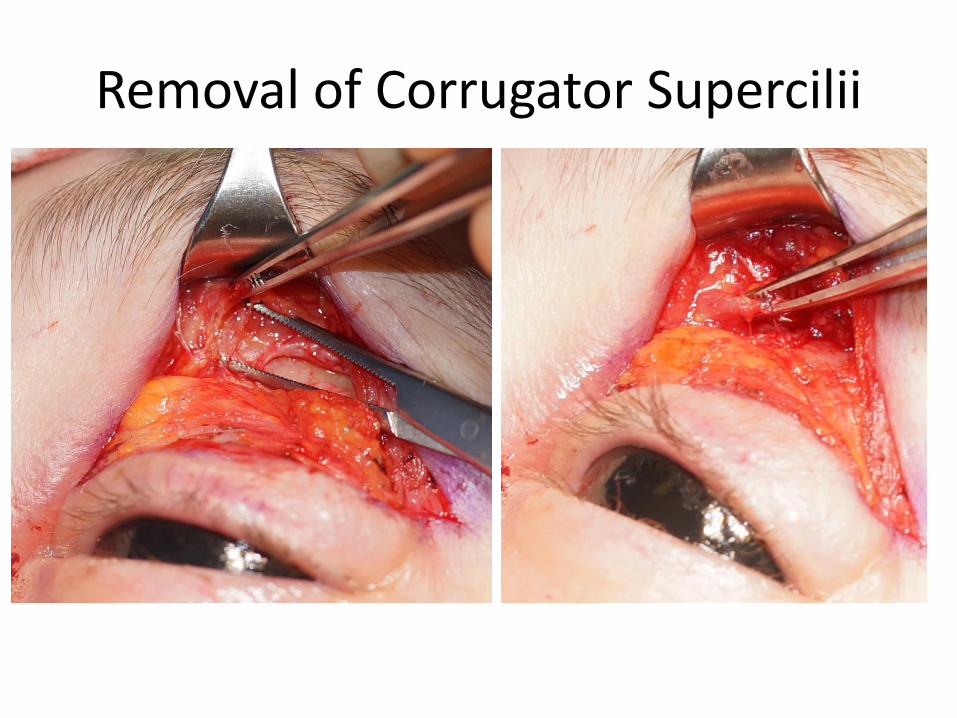
Removal of Corrugator Supercilii
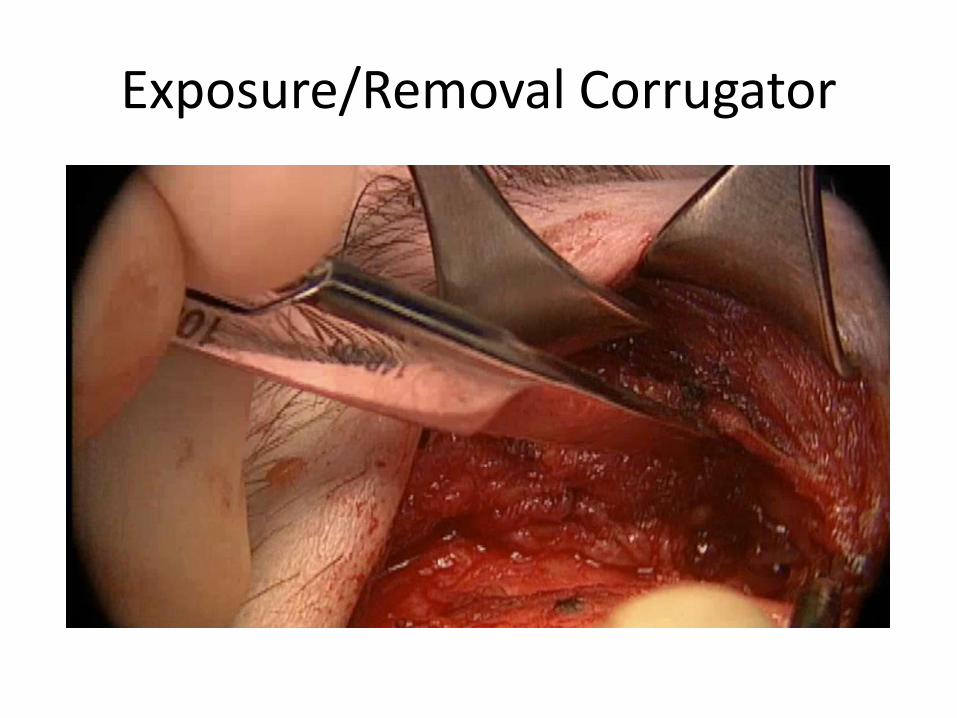
Exposure/Removal Corrugator
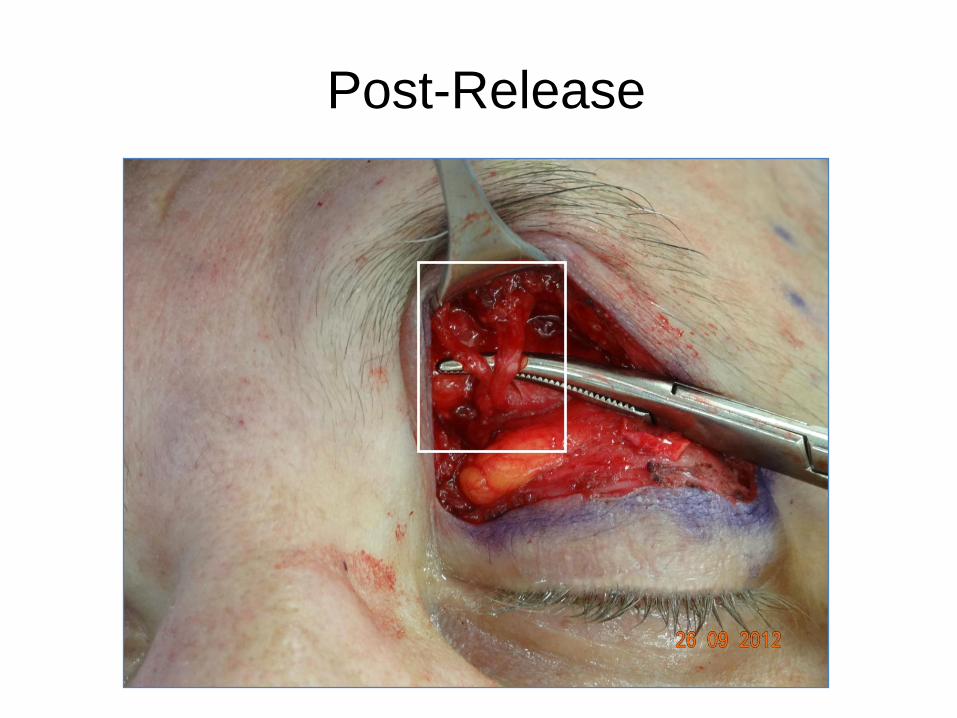
Post-Release
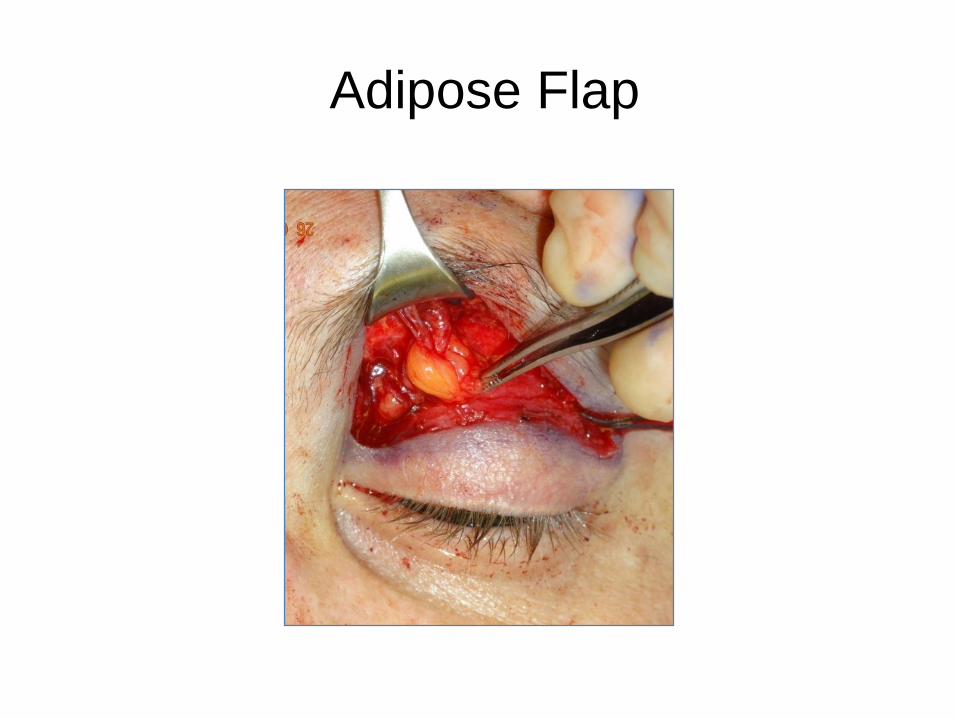
Adipose Flap

Adipose Flap

Zygomaticotemporal nerve
Janis et al.. Plast Reconstr Surg. 2010.

Temporal Trigger Site
Endoscopic
Totonchi et al.. Plast Reconstr Surg. 2005.

Blepheroplasty approach to ZT

Dissection to sentinel Vein
sentinel vein

Identification and removal ZT
sentinel vein
zygomatico-
temporal
nerve

Video ZT release
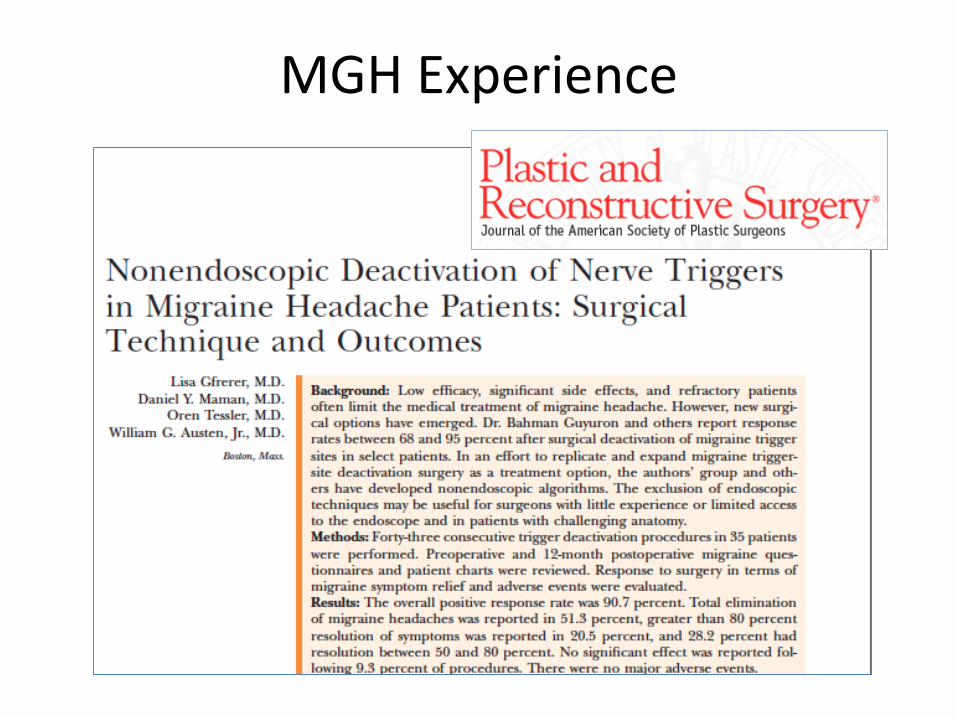
MGH Experience

Results Migraine Headache Frequency
Preop 18.5
Postop 3.7
p<0.01
Frequency (d)

Results Migraine Headache Duration
Preop 16.8
Postop 4.8
p<0.01
Duration (h)
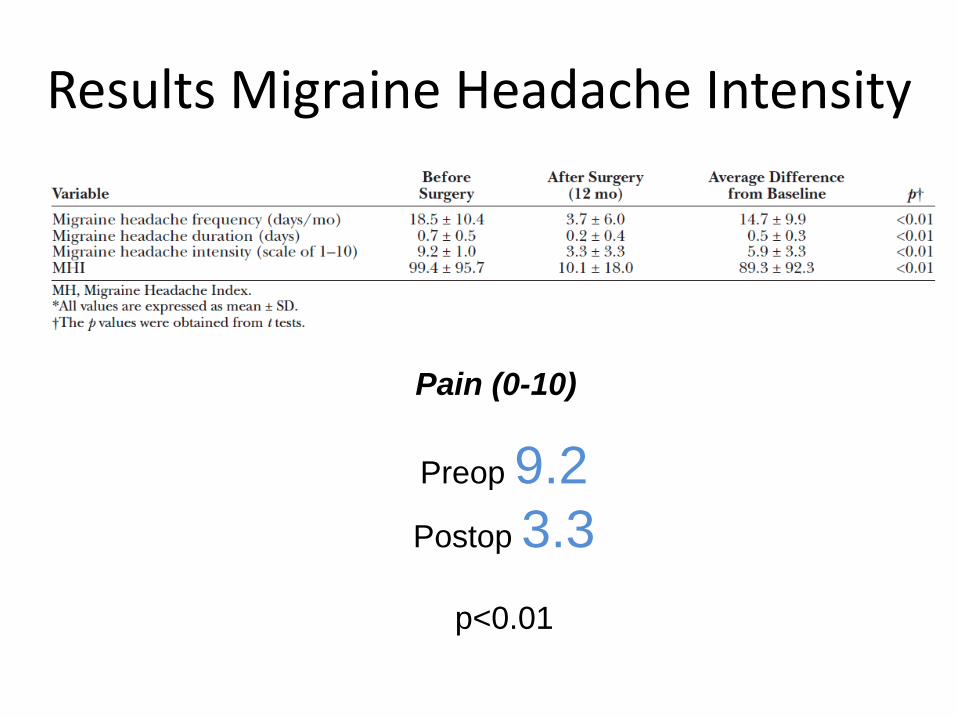
Results Migraine Headache Intensity
Preop 9.2
Postop 3.3
p<0.01
Pain (0-10)

Results Migraine Headache Index
Migraine headache index =
Frequency (d) Duration (1/24) Severity (0-10)
Preop 99.4
postop 10.1
p<0.01
-90%

Post- Surgical Response Rates
> 50%
< 50%
90.9%
9.3%Migraine
Headache Index
Improvement

Positive Response Distribution
100%
> 80%
50- 80%51.3%
28.2%
20.5%
Migraine
Headache Index
Improvement

PATIENTS DO VERY WELL POST OPERATIVELY
Post-Operative Management
Happy Patients…Happy Doctors!
Neuropraxia
Shooting nerve pain/ numbness
Acute migraine attack
Hypertrophic scar
Additional surgery
Low Incidence of Adverse Events
Post-Op pain medication plan
Neurologist and PCP
Pain Specialist
Encourage:
• Patient to contact
Neurologist
• Patient to speak about their
surgery and result
Post-Op Management
From
art…
To
science…

What are the important questions?
Screening?
Evaluate/ communicate results?
Working? How well?
Migraine Q
Screening Evaluation

Questions are a powerful tool

Current Migraine Questionnaires
Migraine Specific Quality of
Life Questionnaire
The migraine work and productivity loss questionnaire
PHQ
9

Screening Tool for doctors
5
Migraine Q

Evaluation Tool for patients Migraine Q

PHQ
2
For Migraine
Prospective questionnaire study
Migraine
Headache
Index
& Chronic Pain
Pain Self Efficacy
Questionnaire

Preliminary Results Questionnaires
mean values; unpublished data
* p<0.01
**
Migraine Headache Frequency (days per month)
*
*

Preliminary Results Questionnaires
mean values; unpublished data
* p<0.01
**
Migraine Headache Duration (hours)

Preliminary Results Questionnaires
mean values; unpublished data
* p<0.01
**
Migraine Headache Severity (0-10)
**

Preliminary Results Questionnaires
mean values; unpublished data
* p<0.01
**
Migraine Headache Index
Frequency (d) Duration (1/24) Severity (0-10)
*
*
-85.7%
-93.5%

Comparison % improvement
8.4%
91.6%
Improvement
90.9%
9.3%
Improvement
prospective retrospective
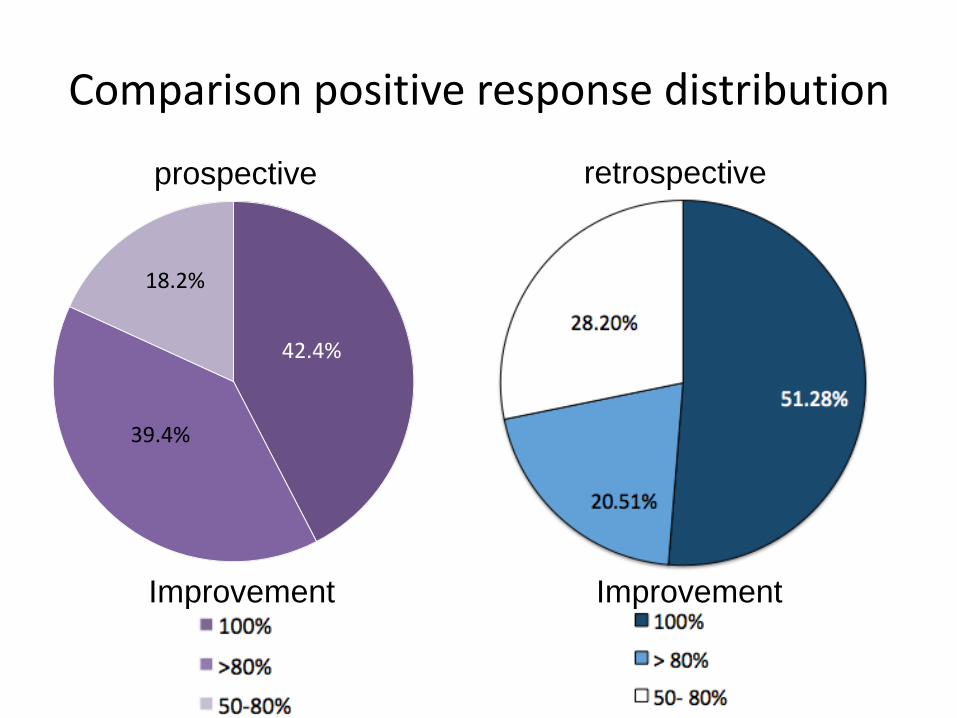
Comparison positive response distribution
39.4%
18.2%
Improvement
prospective retrospective
Improvement
42.4%
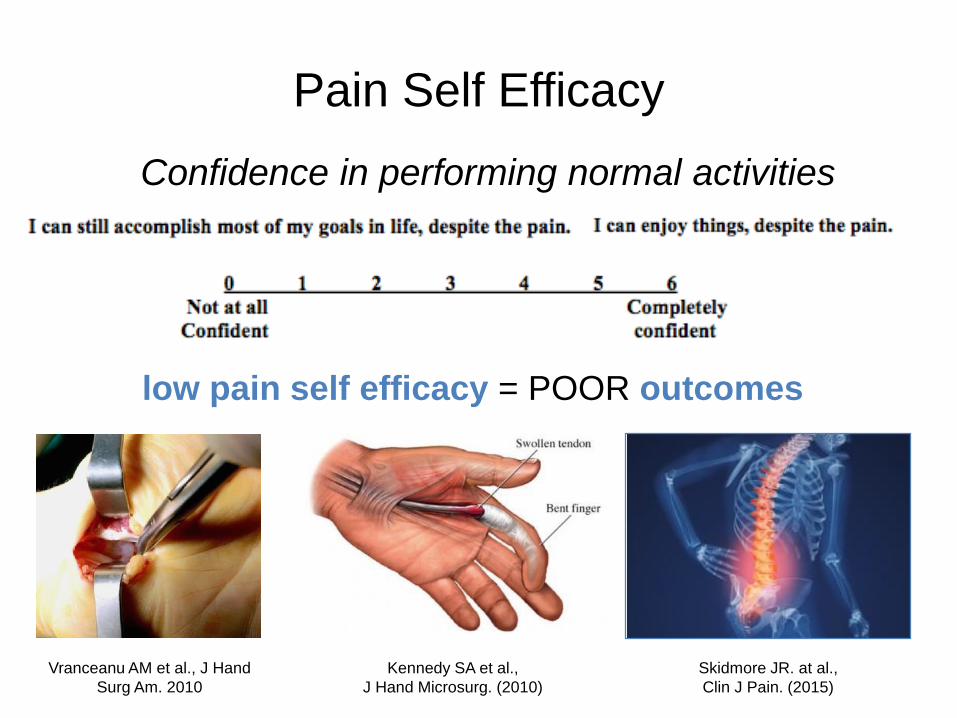
Pain Self Efficacy
Confidence in performing normal activities
low pain self efficacy = POOR outcomes
Kennedy SA et al.,
J Hand Microsurg. (2010)
Vranceanu AM et al., J Hand
Surg Am. 2010
Skidmore JR. at al.,
Clin J Pain. (2015)

Pain Self Efficacy
Treatment Comparison
Jan Paul Briet et al., Phys Ther. (2014) Maughan et. al., Eur Spine J. (2010)
Pre- Treatment Scores
MigraineMigraine
Chronic Back Pain
Carpal Tunnel Syndrome
unpublished

Pain Self Efficacy
Treatment Comparison
Jan Paul Briet et al., Phys Ther. (2014) Maughan et. al., Eur Spine J. (2010)
Post- Treatment Scores
unpublished
Carpal Tunnel Pre
Carpal Tunnel Post
Chronic Back Pain Pre
Chronic Back Pain Post
Migraine Pre
Migraine Post +147%
+13%
+8%

Age of onset mattersMean age at onset 23.9 ± 14.4 (Range 2-61)
Age of onset >40
p<0.05
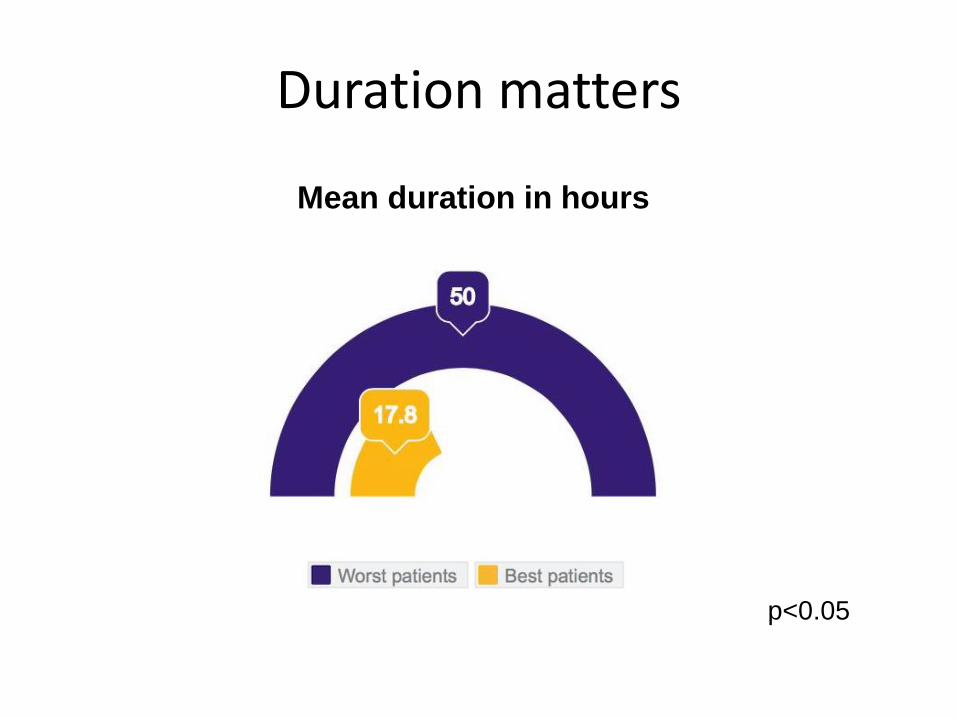
Duration matters
p<0.05
Mean duration in hours

Predictive Variables
Patients do better… when bothered by…
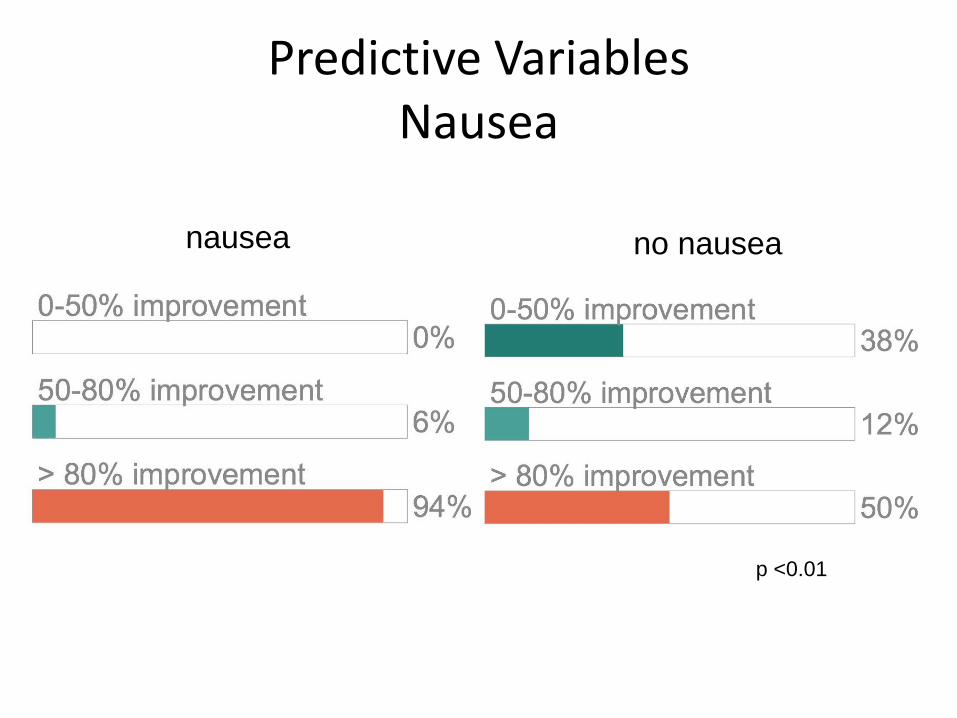
Predictive Variables Nausea
nausea no nausea
p <0.01
Predictive Variables
Patients do better… when relieved by…
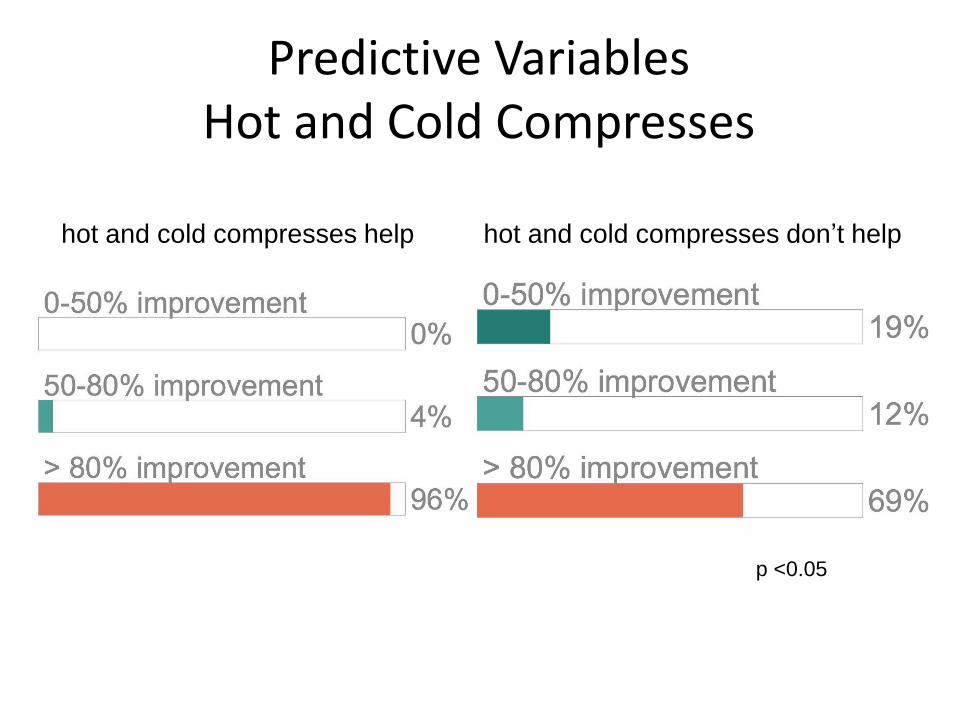
Predictive Variables Hot and Cold Compresses
hot and cold compresses help hot and cold compresses don’t help
p <0.05
What are the important questions?
Pathomechanism
Imaging
…

Migraine Tissue Bank
.. First Migraine Tissue Bank to our knowledge
Pathomechanism

Thermal Imaging
Can we predict nerve compression and
surgery outcomes?
Imaging

Thermal Image
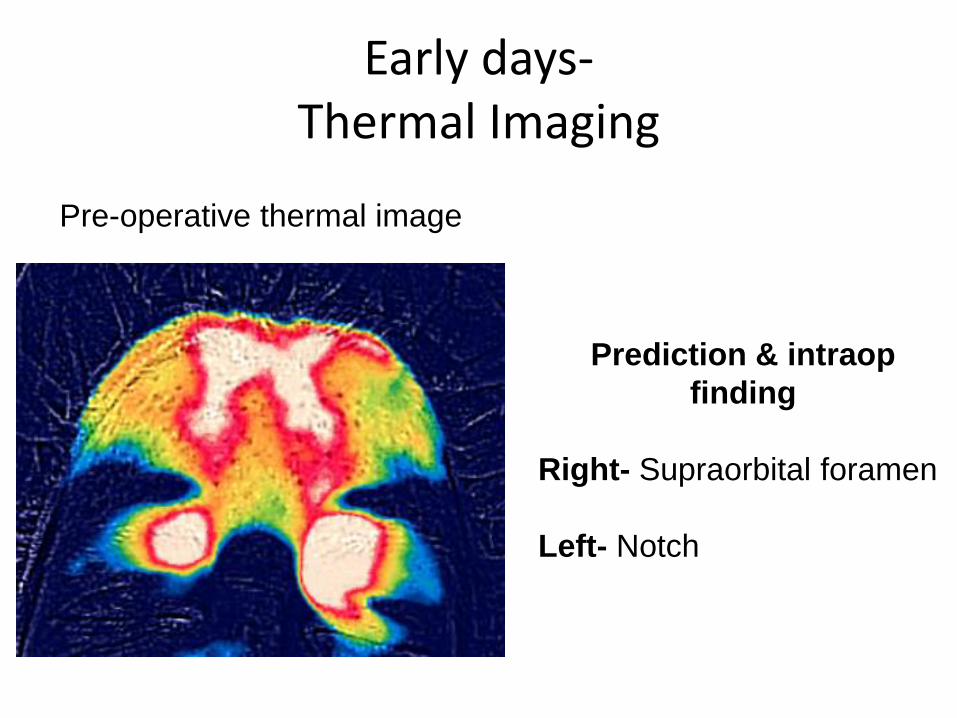
Early days-Thermal Imaging
Pre-operative thermal image
Prediction & intraop
finding
Right- Supraorbital foramen
Left- Notch
WILLIAM G. AUSTEN JR., MD
CHIEF, DIVISION OF PLASTIC & RECONSTRUCTIVE SURGERY
CHIEF, DIVISION OF BURN SURGERY
MGH TRUSTEES CHAIR
Massachusetts General Hospital, Harvard Medical School
Deactivating Peripheral Nerve Triggers:
A Surgical Solution to Refractory Headaches