danish fracture database – dfdb -...
TRANSCRIPT

Danish Fracture Database – DFDB.DK
Herlev Sygehus 04.03.2015
Kirill Gromov, MD, PhD, - e-mail: [email protected]

”Web-based prospective quality monitoring of fracture related surgery”
Evaluation: Rates of reoperation
Operative parameters
Purpose of DFDB
2

Why assessment of quality is relevant:
Life time prevalence of getting a fracture is 38.2 %
20,000 fracture related surgeries are estimated to be carried out annually in DK
No prospective data for assessing the quality of fracture related surgery in general has previously been collected
Assessment of Quality
3
Need for registry based research
• Observational data • Treatment guidelines • Implant monitoring

6 years ago: Paper and pen-based database tested at
Aabenraa Hospital
2 years ago: Web-based database initiated at Hvidovre and
Odense Hospitals, Dept. of Orthopaedics
Now: 21 departments in total
Administration and statistics
» Steering group with
annual meetings
Michael Brix Anders Troelsen
History of DFDB
5

21 departments n ≈ 35,000 operations
Kolding
Aabenraa
Herlev
Bispebjerg
Esbjerg
Holbæk
Viborg
Horsens
Aalborg & Farsø
Randers
Hvidovre
Odense
Rigshospitalet
Slagelse
Køge
Nykøbing F.
Hillerød
Århus
Vejle
Gentofte
Participating departments
6
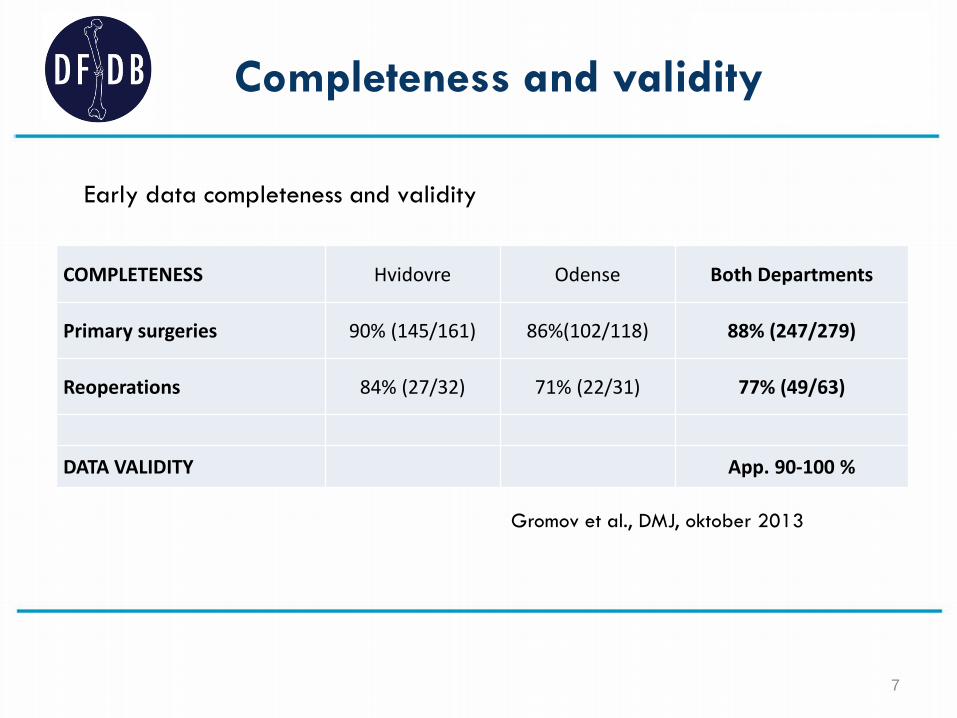
Early data completeness and validity
COMPLETENESS Hvidovre Odense Both Departments
Primary surgeries 90% (145/161) 86%(102/118) 88% (247/279)
Reoperations 84% (27/32) 71% (22/31) 77% (49/63)
DATA VALIDITY App. 90-100 %
Gromov et al., DMJ, oktober 2013
Completeness and validity
7

> 8000 entries / 6 months
History of data entries
DFDB
8

• DFDB.dk online registration, developed by PROCORDO®
• 2 min per registration
• Filled out by the surgeon immediately after surgery
• Patient, trauma and surgery related factors are registered
• Reoperations are linked with primary operations
Structure
9
• Departments own their own data
• Department can use data for quality monitoring, research etc.
• Departments can veto use of data in projects by other departments
• Departments deliver data for annual report at the DOS congress
• All rules followed, all is reported to The Danish Data Protection Agency
• Alle departments have a person responsible for data who is also member of the steering group
Data
10

User featers
• Status messages • Surgical log


• Landsdækkende database (ansøgning til SSI indsendt)
• Flere forskningsprojekter
• Implantat sporing
Fremtid
13

Forskningsprojekter
• 4 artikler i Pubmed • 1 accepteret til JBJS – surgical delay.
– Danish Fracture Database Collaboration ordning.
• Flere på vej ???
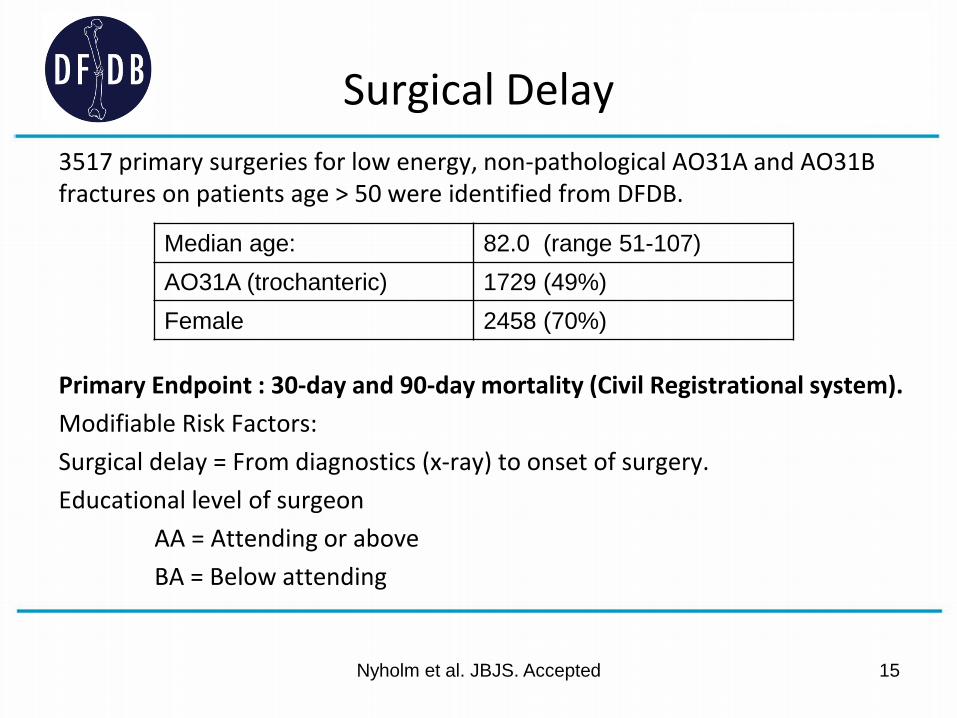
Surgical Delay 3517 primary surgeries for low energy, non-pathological AO31A and AO31B fractures on patients age > 50 were identified from DFDB. Primary Endpoint : 30-day and 90-day mortality (Civil Registrational system). Modifiable Risk Factors: Surgical delay = From diagnostics (x-ray) to onset of surgery. Educational level of surgeon AA = Attending or above BA = Below attending
Nyholm et al. JBJS. Accepted 15
Median age: 82.0 (range 51-107) AO31A (trochanteric) 1729 (49%) Female 2458 (70%)

16
Mortality
Surgical delay
Surgical Delay

Logistical regression* *Adjusted for age, gender, ASA score, fracture type, treatment, educationale level of surgeon/surgical delay
Surgical delay
30-day mortality risk (OR)
90-day mortality risk (OR)
≥12 vs <12h 1.45* 1.10
≥24 vs <24h 1.34* 1.23*
≥36 vs <36h 1.32 1.21*
≥48 vs <48h 1.56* 1.36
≥72 vs <72h 1.23 1.09
Surgical delay
30-day mortality risk (OR)
90-day mortality risk (OR)
<12 h 1 1
12-24 h 1.33 1.02
24-36 h 1.60* 1.22
36-48 h 1.37 1.08
48-72 h 2.61* 1.83*
≥72 h 1.67 1.18
Educatilnal level of surgeon
30-day mortality risk (OR)
90-day mortality risk (OR)
AA 1 1 BA 1.28* 1.26*

Conclusions
Short surgical delay (<12h) reduces risk of 30-day mortality.
The effect is less pronounced at 90-day mortality.
Junior surgeons should be supervised.

19
IMPLANTATSPORING Hvidovre Hospital
Intelligent implantat sporing &
klassifikation
Kirill Gromov, læge, PhD, - e-mail: [email protected]

Kirill Gromov, læge, PhD, - e-mail: [email protected]
Implantat sporing Behov
20
”Det anvendte implantat skal kunne identificeres entydigt og specifikt ved angivelse af implantatets
navn og model, størrelse af implantatet, fabrikantens navn, serienummer eller LOT
efterfulgt af batchkode”
1) Hvad har vi opereret patienten med? • Reoperationer • Recalls
2) Hvordan går det med det nye implantat?
• Kontinuerlig kvalitets monitorering

Kirill Gromov, læge, PhD, - e-mail: [email protected] 21
Implantat sporing idag
1) Hvad har vi opereret patienten med? • Reoperationer • Recalls

Kirill Gromov, læge, PhD, - e-mail: [email protected] 22
Implantat sporing idag
2) Hvordan går det med det nye implantat?
• Kontinuerlig kvalitets monitorering

• Nem tilgængelig og med landsdækkende potentiale
• Løbende monitorering med ”early warnings” • Intelligent implantat sporing med
klassifikation
23
Implantat sporing i fremtiden
Kirill Gromov, læge, PhD, - e-mail: [email protected]

Hvorfor klassificere?
Er det ikke nok at kende firmaet og lot nummeret nummeret?
24 Kirill Gromov, læge, PhD, - e-mail: [email protected]

1978
Ford Pinto – ”Barbecue that seats four”
25 Kirill Gromov, læge, PhD, - e-mail: [email protected]

Defekt produktion, design eller noget helt tredje?
26 Kirill Gromov, læge, PhD, - e-mail: [email protected]

27
2010

Defekt produktion, design eller noget helt tredje?
28 Kirill Gromov, læge, PhD, - e-mail: [email protected]


• Sammenligning på tværs af producenter
• Mulighed for at kigge på flere faktorer samtidigt
• Identificering af fejl i designet • Mulige farlige ”kombinationer”
30
Implantatklassifikation giver større viden
Kirill Gromov, læge, PhD, - e-mail: [email protected]

Cladestik ved implantatregistrering
• Klassificeres første gang af kirurgen • En implantat skal kun klassificeres en gang • Alle implantater klassificeres • Valideres af superbruger
31 Kirill Gromov, læge, PhD, - e-mail: [email protected]

Overlevelses kurver
32

Overlevelses kurver
33

Aktuel status på Marvsøm
• Hvad er evidensen for brug af forskellige implantater til proximal femur frakturer?

Begrænsninger:
– Engelsksproget – publiceret 1990 eller senere. – Trochantær eller collum fem (dvs. ikke pipkin eller distalt for troc.
minor) – Primære hoftefracture – Ikke patologisk – Angive failure of implant – Min.follow-up 1 år – Klart angive implantat

Søm
Implant N (studies)
N (patients) Prospective
N (patients) Retrospective
N (patients) total
Gamma3 12 759 259 1018
IMHS 7 210 352 562
InterTan 5 585 10 595
PFN 13 785 183 968
PFNA 20 887 686 1573 PTN 0 0 0 0

•HUSK AT REGISTRERE I DFDB