daniel s. sitar, bscpharm, phd, fcp email: sitar@cc ... approaches to pain... · daniel s. sitar,...
TRANSCRIPT
Daniel S. Sitar, BScPharm, PhD, FCP
Email: [email protected]
Professor Emeritus University of Manitoba
Editor: Journal of Clinical Pharmacology
March 8, 2011
DEFINITIONS
Pain: The unpleasant sensory and emotional
experience associated with a noxious event, including, tissue damage or inflammation
Nociception: The process of encoding and sensing
tissue injury and inflammation
Significant developmental/maturational changes
Analgesia: Relief of the perception of pain
Accompanying sedation unintended
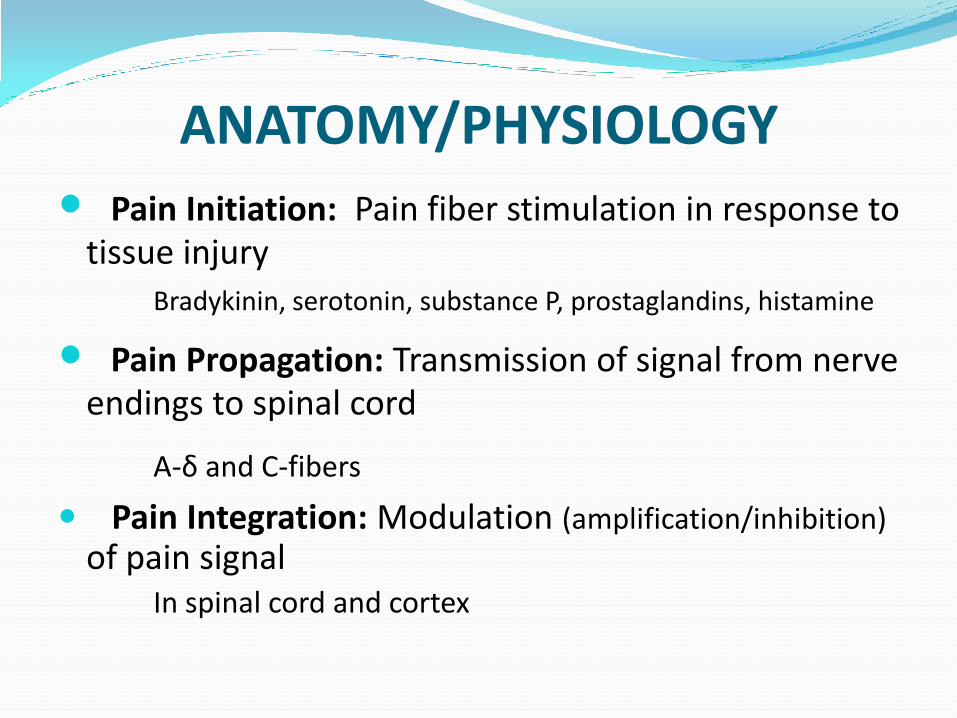
ANATOMY/PHYSIOLOGY
Pain Initiation: Pain fiber stimulation in response to tissue injury
Bradykinin, serotonin, substance P, prostaglandins, histamine
Pain Propagation: Transmission of signal from nerve endings to spinal cord
A-δ and C-fibers
Pain Integration: Modulation (amplification/inhibition)
of pain signalIn spinal cord and cortex

THE GOLD STANDARD OF PAIN ASSESSMENT IS SELF REPORT - BUT HARDLY FEASIBLE IN COGNITIVELY IMPAIRED PERSONS
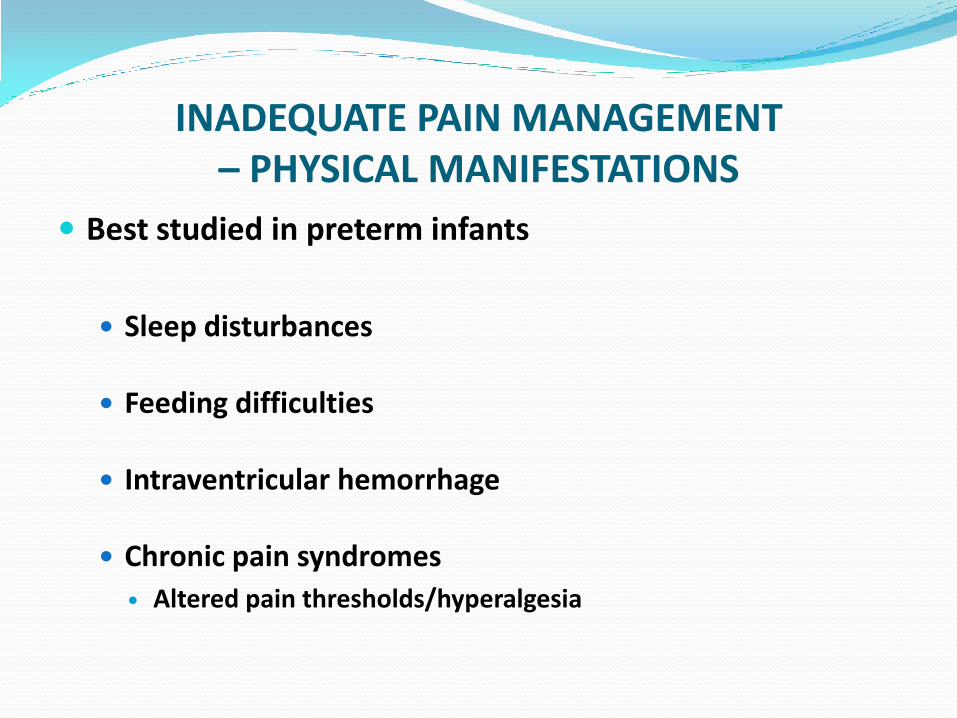
INADEQUATE PAIN MANAGEMENT – PHYSICAL MANIFESTATIONS
Best studied in preterm infants
Sleep disturbances
Feeding difficulties
Intraventricular hemorrhage
Chronic pain syndromes
Altered pain thresholds/hyperalgesia
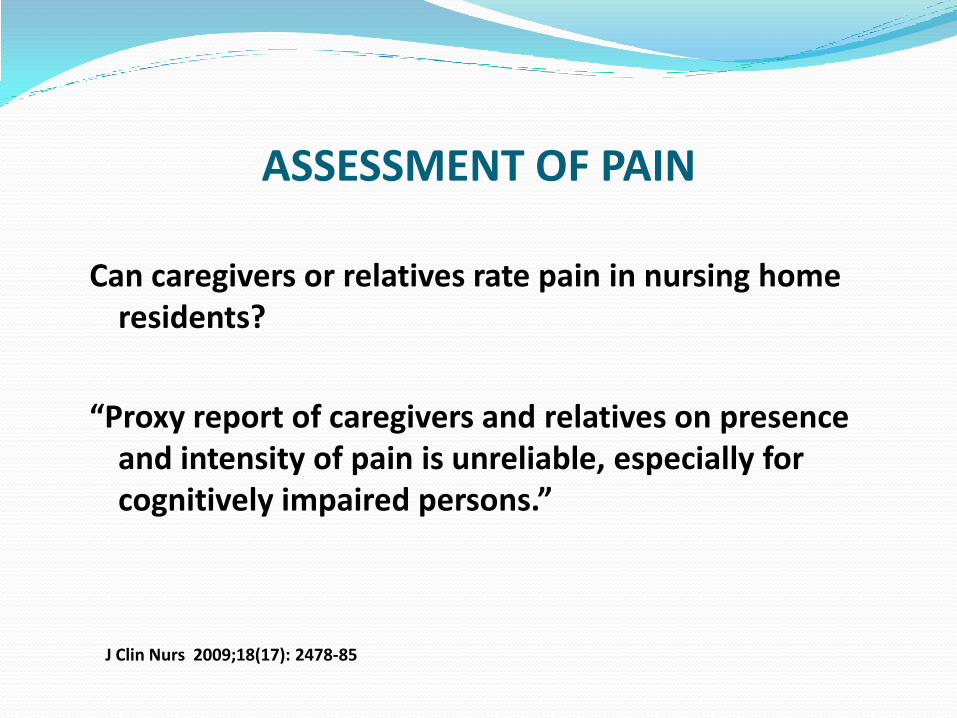
ASSESSMENT OF PAIN
Can caregivers or relatives rate pain in nursing home residents?
“Proxy report of caregivers and relatives on presence and intensity of pain is unreliable, especially for cognitively impaired persons.”
J Clin Nurs 2009;18(17): 2478-85
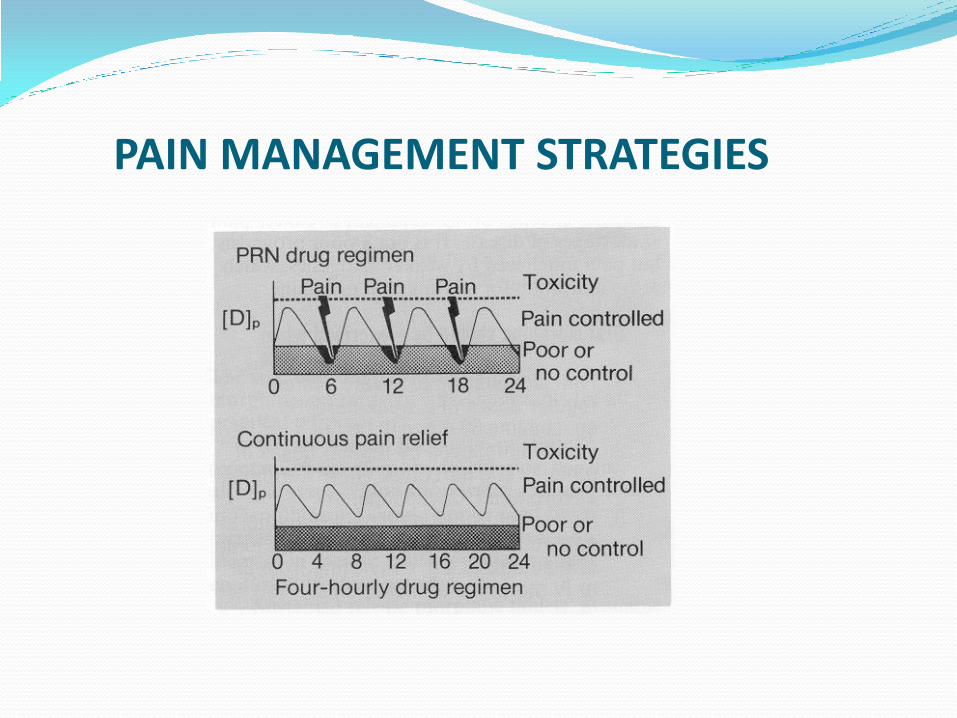
PAIN MANAGEMENT STRATEGIES
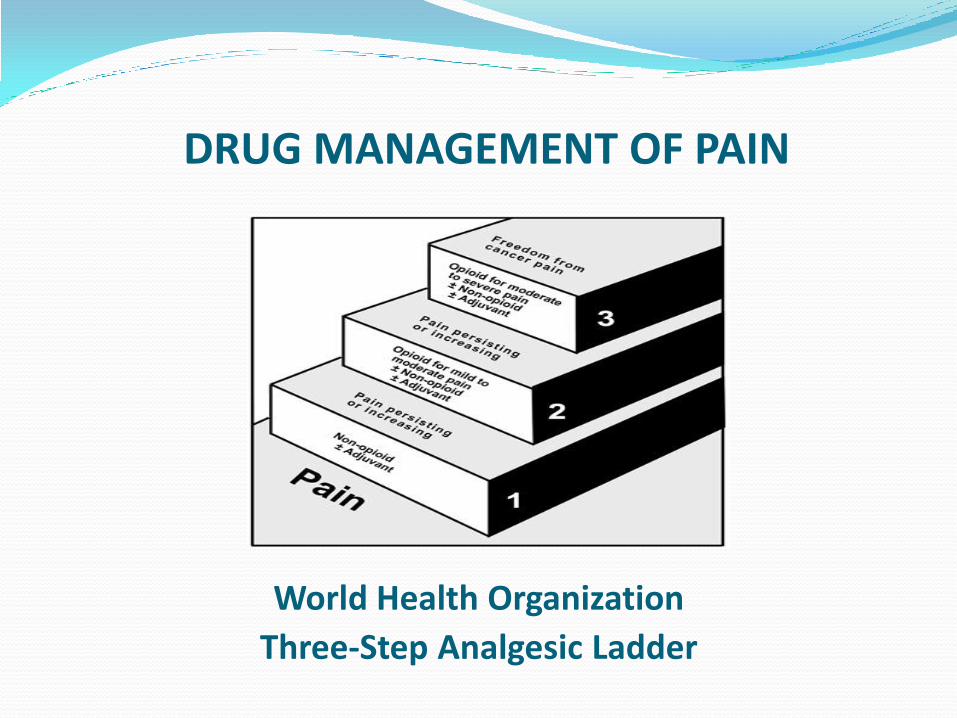
DRUG MANAGEMENT OF PAIN
World Health Organization
Three-Step Analgesic Ladder

Figure 1: Percentage of Seniors Who Reported Having 1 or More of 11 Chronic
Conditions, for Canada and by Province (Age–Sex Standardized)
N.W.T.Y.T.
Nun.
B.C.Alta.
Sask. Man.
Ont.
Que.
N.B.N.S.
N.L.
P.E.I.
Canada
75% 82%*
76% 70%
75%
81%
79%
85%*
81%
76%
74%
Canadian Survey of Experiences With Primary Health Care, 2008, Statistics Canada;Canadian Institute for Health Information. –from Jan 2011 CIHI Report
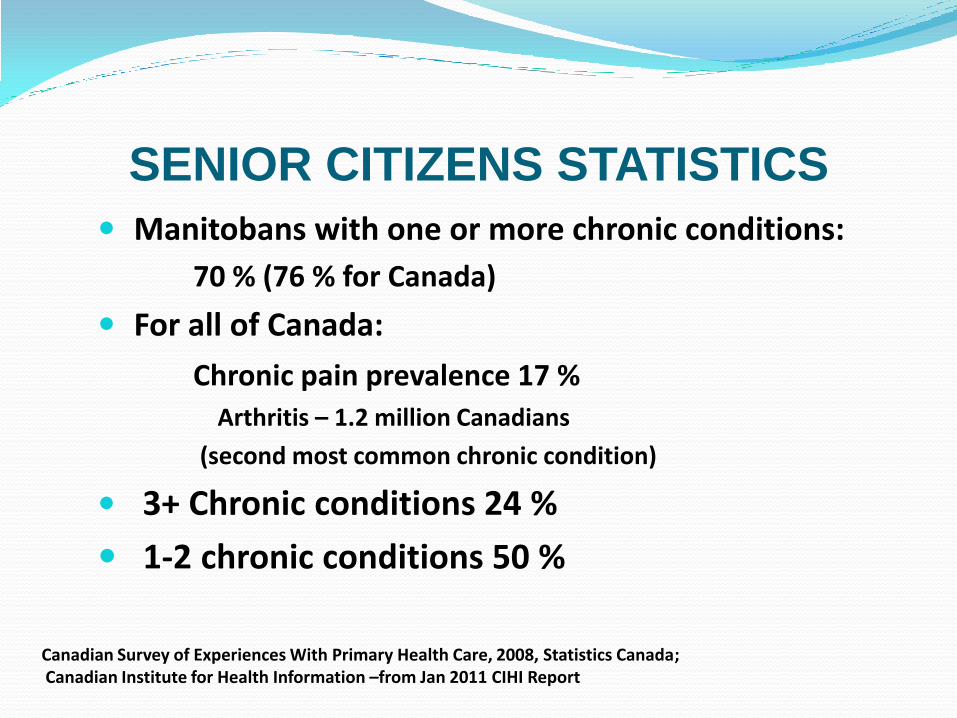
SENIOR CITIZENS STATISTICS
Manitobans with one or more chronic conditions:
70 % (76 % for Canada)
For all of Canada:
Chronic pain prevalence 17 %
Arthritis – 1.2 million Canadians
(second most common chronic condition)
3+ Chronic conditions 24 %
1-2 chronic conditions 50 %
Canadian Survey of Experiences With Primary Health Care, 2008, Statistics Canada;Canadian Institute for Health Information –from Jan 2011 CIHI Report
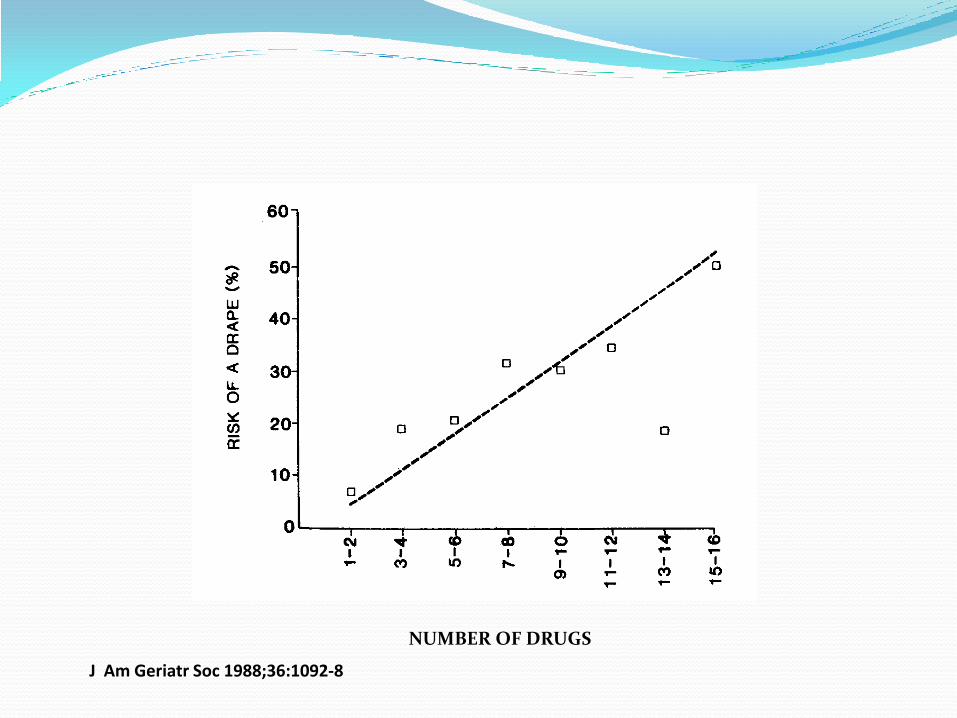
NUMBER OF DRUGS
J Am Geriatr Soc 1988;36:1092-8
Choices for Analgesia
• Nonopioid
• Opioid
• Co-analgesics

OTC ANALGESICS - CANADA
Acetylsalicylic acid (ASA)
Acetaminophen (Paracetamol – UK)
Ibuprofen
Naproxen
Combination products with codeine phosphate
– up to 8 mg/tablet - Not recommended

Biopharm Drug Disposit 1986;7:21-5

Acetaminophen is not an NSAID
PHARMACOLOGY OF ACETAMINOPHEN
• Rapidly and completely absorbed
• Peak plasma concentrations in 30 to 60 minutes
• Half-life of 2 hours in adults
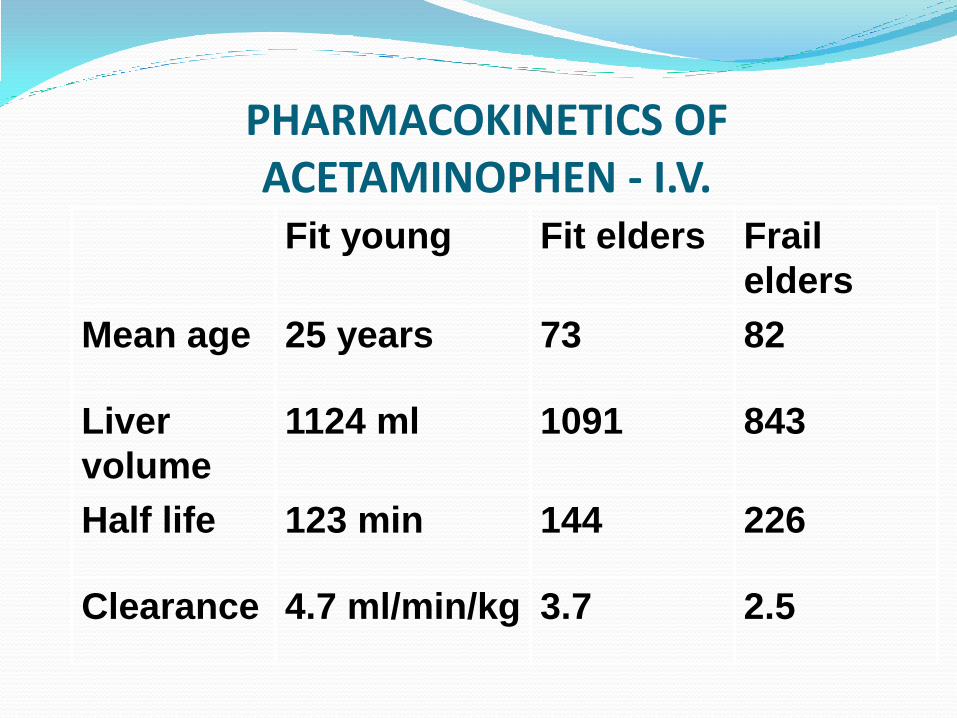
PHARMACOKINETICS OF ACETAMINOPHEN - I.V.
Fit young Fit elders Frail
elders
Mean age 25 years 73 82
Liver
volume
1124 ml 1091 843
Half life 123 min 144 226
Clearance 4.7 ml/min/kg 3.7 2.5
RATIONAL NONOPIOID ANALGESIC COMBINATIONS
ASA + Acetaminophen
ASA + Caffeine
Acetaminophen + Caffeine
ASA + Acetaminophen + Caffeine
DRUG USE PRINCIPLE Don’t mix NSAIDs
Increased cardiovascular risk
Illogical therapeutic approach due to same mechanism of action
PROBLEMS WITH NONOPIOID DRUGS FOR PAIN MANAGEMENT
Cardiovascular – NSAIDS
Bleeding – NSAIDS
Hypertension – NSAIDS
Hepatotoxicity – mostly with acetaminophen
Kidney toxicity – both NSAIDs and acetaminophen
Brain toxicity – mostly with NSAIDs
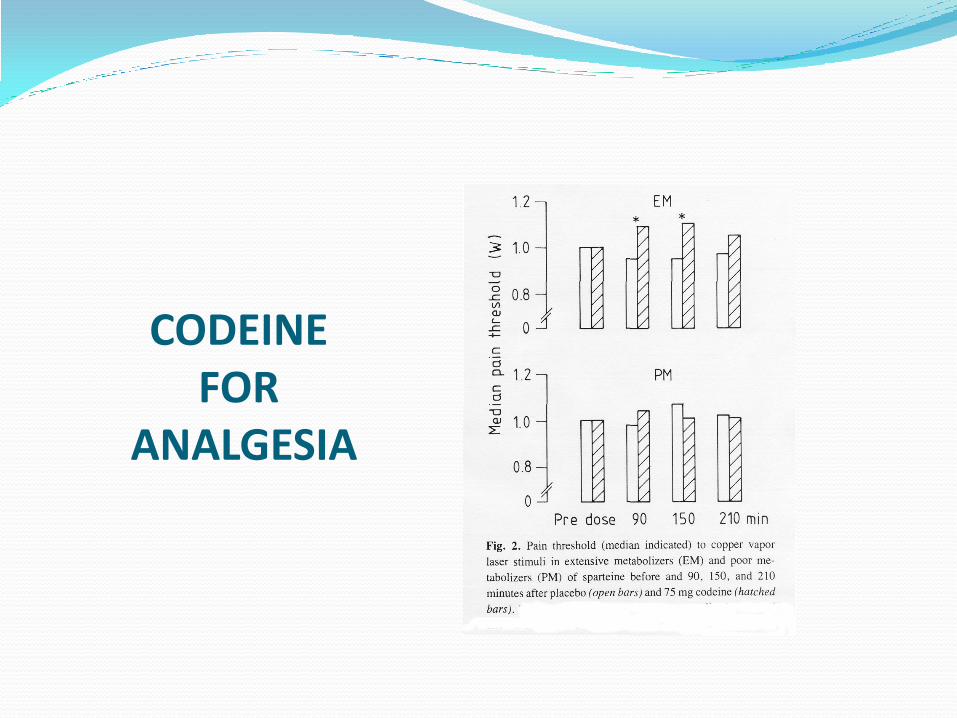
CODEINE FOR
ANALGESIA

CYP2D6 AND ETHNICITY
Population % Poor Metabolizers
Caucasian 5 - 10
Canadian Native Indian 1.1
Inuit 3.3
Chinese 1
African 0 - 20
Int J Clin Pharmacol Ther 2000;38:61
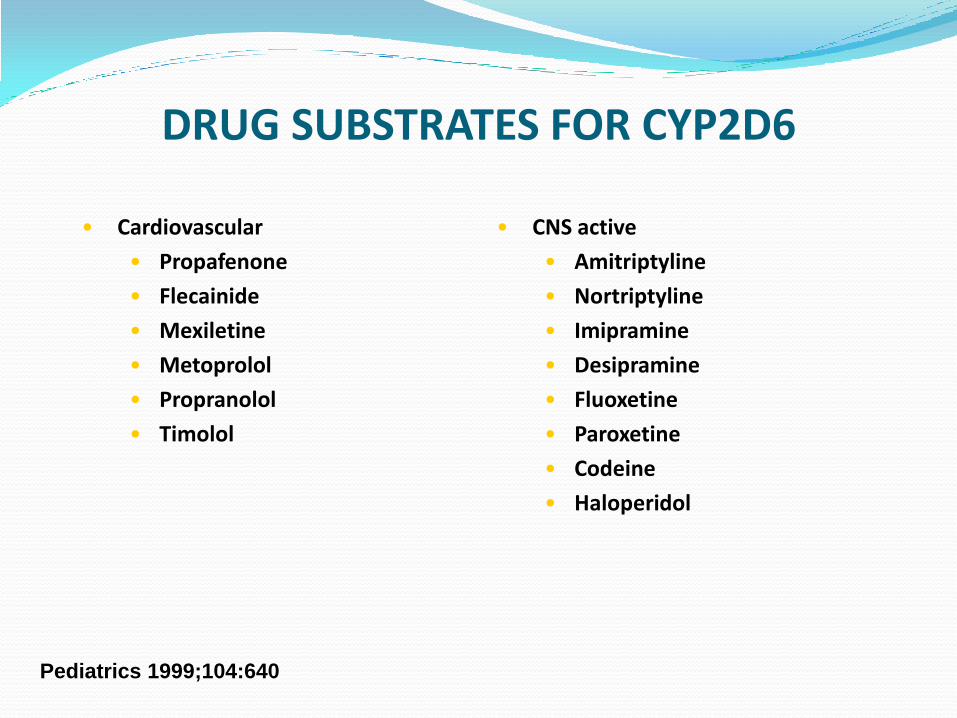
DRUG SUBSTRATES FOR CYP2D6
• Cardiovascular
• Propafenone
• Flecainide
• Mexiletine
• Metoprolol
• Propranolol
• Timolol
• CNS active
• Amitriptyline
• Nortriptyline
• Imipramine
• Desipramine
• Fluoxetine
• Paroxetine
• Codeine
• Haloperidol
Pediatrics 1999;104:640
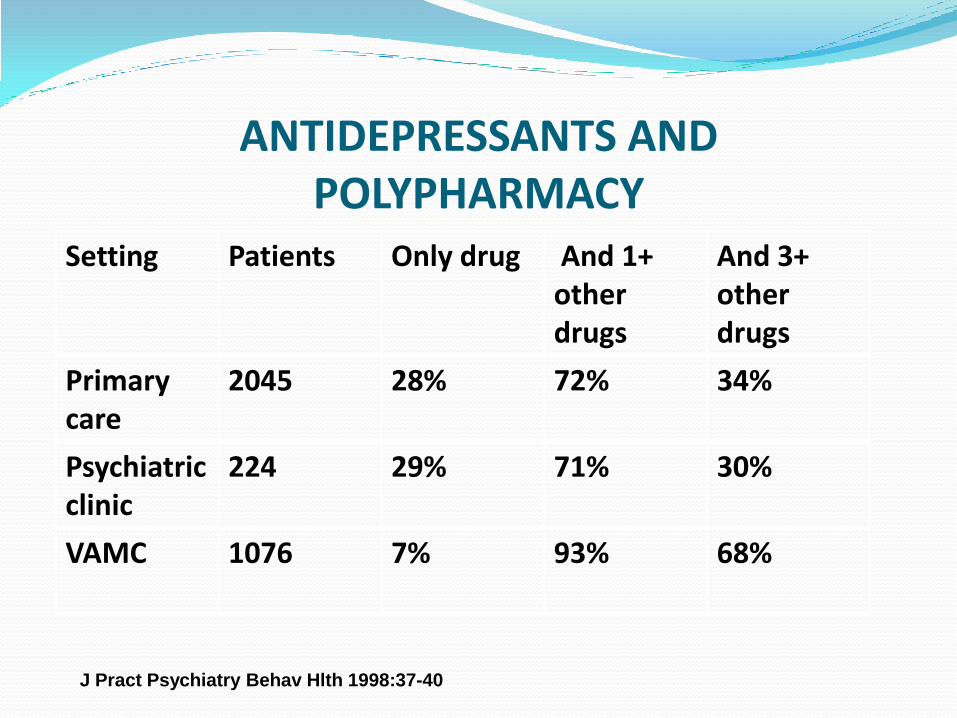
ANTIDEPRESSANTS AND POLYPHARMACY
Setting Patients Only drug And 1+ other drugs
And 3+ other drugs
Primary care
2045 28% 72% 34%
Psychiatric clinic
224 29% 71% 30%
VAMC 1076 7% 93% 68%
J Pract Psychiatry Behav Hlth 1998:37-40

ISSUES WITH OPIOID ANALGESICS Respiratory Depression
Constipation
Bladder Evacuation Difficulties
ADVERSE PERSON EVENTS AFTER CODEINE
• Consistent with literature on lack of analgesic effect of codeine in persons lacking CYP2D6
• Same incidence of adverse events regardless of analgesic efficacy (sedation, dizziness etc. but not nausea)
• Beware: large placebo response in effectiveness of analgesics
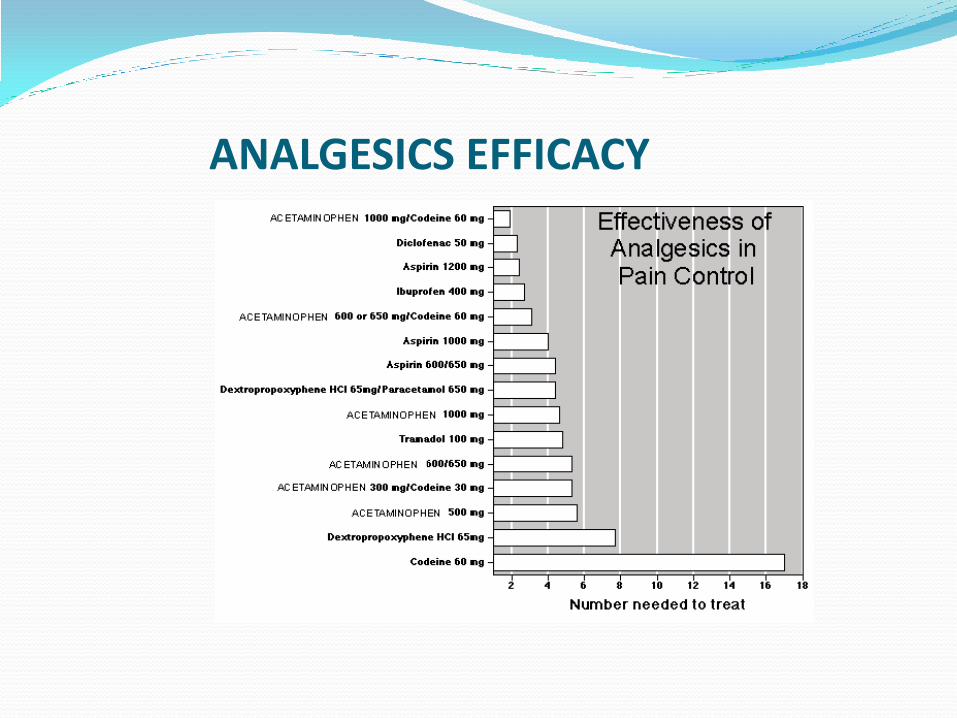
ANALGESICS EFFICACY
March 9, 2011
TYLENOL® WITH CODEINE ORDERS
• One tablet “T3” equals 2 tablets of plain acetaminophen
• Tylenol #1® has an ineffective dose of codeine
• Analgesic range should be allowed:
e.g. 2 tablets Tylenol #2 or #3® QID
as a regular dose
March 9, 2011
TYLENOL ORDERS
Tylenol #3 1-2 tabs OH4 prn
CONCLUSIONS
• Acute and chronic pain are very prevalent and an important issue for person satisfaction
• Simple analgesics are among the most frequently used medications
• Clinicians need to carefully monitor analgesic use (and abuse) and optimize regimens using pharmacologic principles