cytogenetics updatehaematology.org.my/afh2010/slides/16b.pdf · • deletion of 13q observed in 20%...
TRANSCRIPT

Ph
Nowell and Hungerford, 1960

922
Janet Rowley showed the Ph chromosome to be a balanced rearrangement: t(9;22)


Acute lymphoblastic leukaemia

EFS of patients treated on UK MRC ALL97 by cytogenetic subgroup
Moorman et al, Blood, 2007

t (12;21)(p13;q22)
• 4 year old boy presented with sudden onset of tiredness and bruising
• FBE showed blasts in PB
46,XY,del(12)(p13)[22]

HEH karyogram

High hyperdiploidy in paediatric ALL• Hyperdiploidy in acute lymphoblastic leukaemia associated with
consistent pattern of trisomies and often four copies of chromosome 21
• FISH for trisomies of 4, 10 and 17
ETV6/RUNX1
CEP4, 10, 17
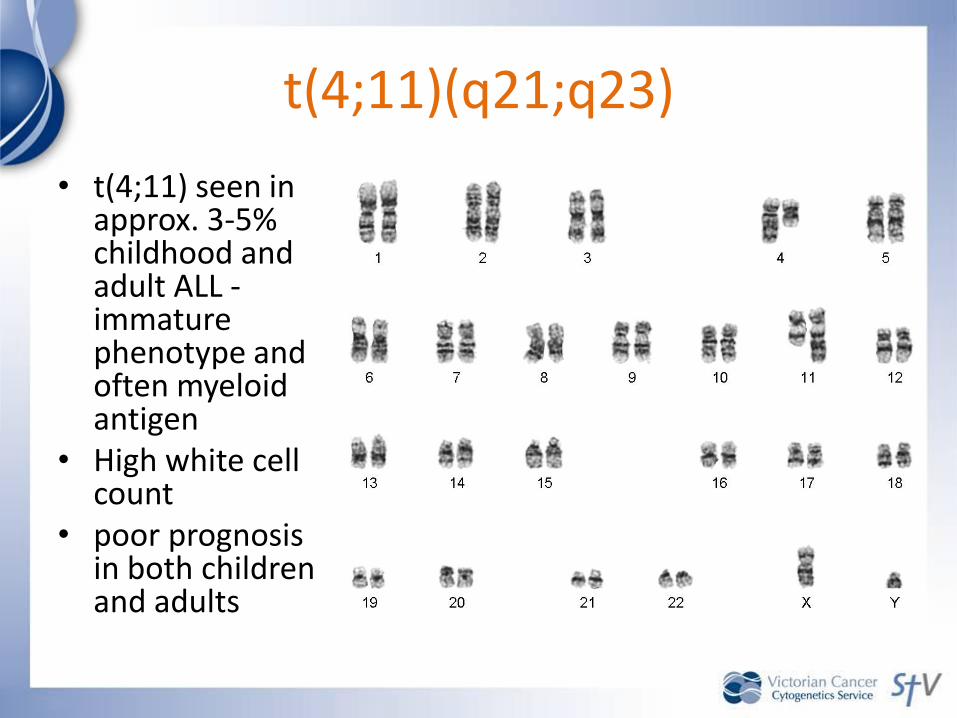
t(4;11)(q21;q23)
• t(4;11) seen in approx. 3-5% childhood and adult ALL -immature phenotype and often myeloid antigen
• High white cell count
• poor prognosis in both children and adults

Ph+ ALL
• 15-30% adult ALL but only about 3% childhood ALL
• either p190 or p210 fusion product seen
• associated with a dismal prognosis in both adults and children
• transplant candidates• Some promising
results with imatinibtherapy

t(17;19)(q22;p13) with TCF3-HLF fusion
• t(17;19)(q22;p13) gives rise to the TCF3-HLF fusion
• It is a variant of t(1;19)(q23;p13), TCF3-PBX1 fusion.
• Very rare
• Extremely poor outcome in paediatric series
• Usually visible by cytogenetic analysis but may be confirmed using the dual colour breakapart probe specific for TCF3 (E2A)
• Report of t(17;19) in 23 adults showed no difference in overall survival compared with negative patients (Burmeister et al, Haematologica, 2010)

Multiple copies of RUNX1 clustered on a marker chromosome

intrachromosomal amplification of chromosome 21 (iAMP21)
• 2% childhood ALL - pre-B immunophenotype,
• significantly older (median 9 years vs 5 years),
• lower white cell count (median 3.9 vs 12.4)
• significantly inferior EFS at 5 years : 29% versus 78% and overall survival 71% versus 87% respectively.
• 3-fold increase in relapse risk,
• New patients with iAMP21 on UK MRC ALL2003 trial high-risk arm and considered for bone marrow transplantation in first CR.
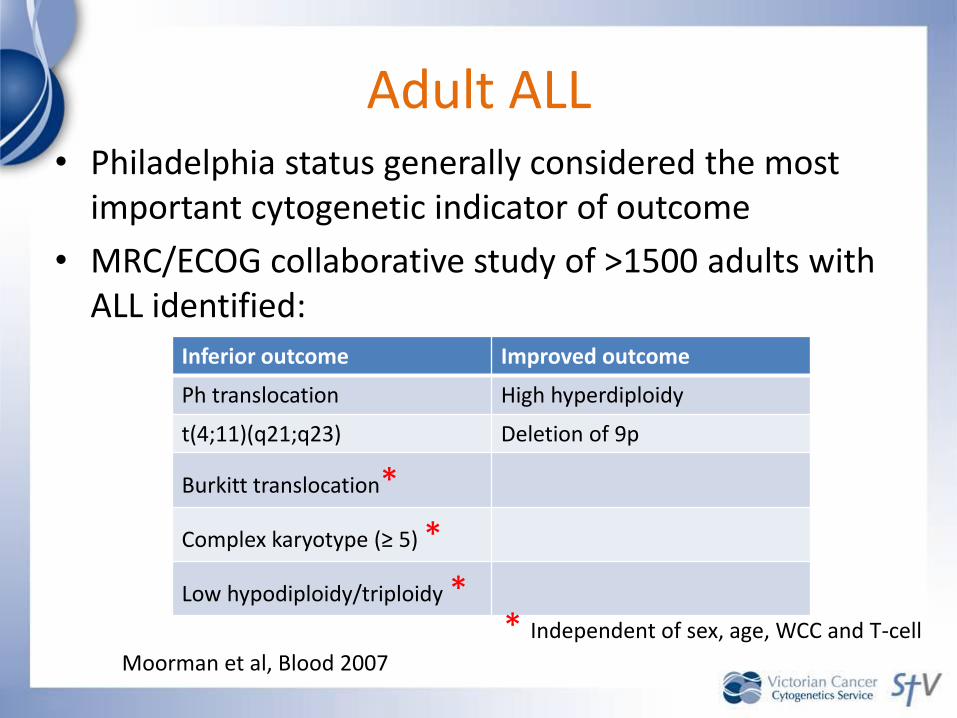
Adult ALL• Philadelphia status generally considered the most
important cytogenetic indicator of outcome
• MRC/ECOG collaborative study of >1500 adults with ALL identified:
Inferior outcome Improved outcome
Ph translocation High hyperdiploidy
t(4;11)(q21;q23) Deletion of 9p
Burkitt translocation*
Complex karyotype (≥ 5) *
Low hypodiploidy/triploidy *
Moorman et al, Blood 2007
* Independent of sex, age, WCC and T-cell

WHO 2008 classification of AML:AML with recurrent genetic abnormalities
• AML with t(8;21); RUNX1-RUNX1T1
• AML with inv(16) or t(16;16); CBFB-MYH11
• APL with t(15;17); PML-RARA*
• AML with t(9;11); MLLT3-MLL#
• AML with t(6;9); DEK-NUP214
• AML with inv(3); RPN1-EVI1
• AML (megakaryoblastic) with t(1;22); RBM15-MKL1

Acute Myeloid Leukaemia with t(8;21); RUNX1-RUNX1T1
Cytogenetically Normal AML (CN-AML)
Figure 1. Pie chart illustrating the molecular heterogeneity of cytogenetically normal AML based on mutations in the NPM1, CEBPA, MLL, FLT3(ITD and TKD mutations at codons D835 and I836), NRAS, and WT1 genes. Data are derived from mutational analysis of 485 younger adult patients with cytogenetically normal AML from AMLSG.
Dohner et al, Blood, 115: 453-474, 2010
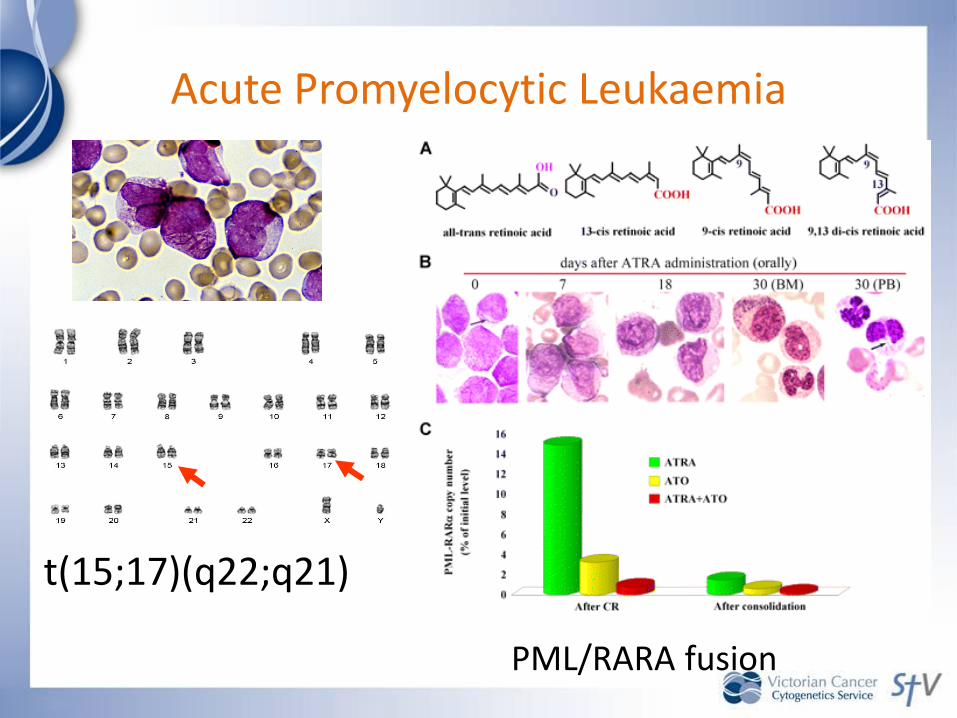
Acute Promyelocytic Leukaemia
t(15;17)(q22;q21)
PML/RARA fusion

Rare variants:
t(11;17)(q23;q21) – RARA/PLZFt(5;17)(q35;q21) – RARA/NPMt(11;17)(q13;q21) – RARA/NuMAinterstitial del(17q) – RARA/STAT5b
PML/RARA probe RARA with PRKAR1A BAC probe
PRKAR1A-RARA fusion in variant APL, Catalano et al, Blood 2007

Inversion 16
AML M4Eo
Fusion of CBFB on 16q22 and MYH11 gene on 16p13
AML with maturation with Auer rods & eosinophilia.Fuses the RUNX1 gene on 21 with the RUNX1T1 (CBFA2T1, ETO) gene on 8q22

Probe for inversion 16: CBFB/MYH11 dual fusion translocation probe (Cytocell Aquarius Probe)

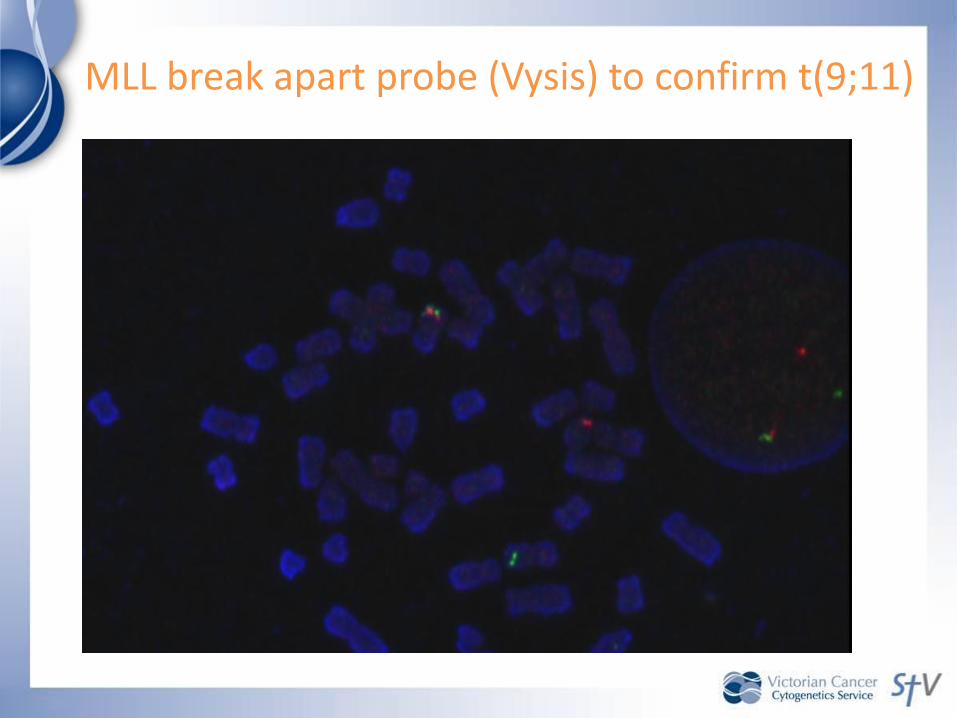
MLL break apart probe (Vysis) to confirm t(9;11)

11q23 abnormalities
• Rearrangements of MLL observed in high-risk paediatric, adult and therapy-related acute leukaemias
• At least 104 different MLL rearrangements reported with 64 of the translocation partner genes
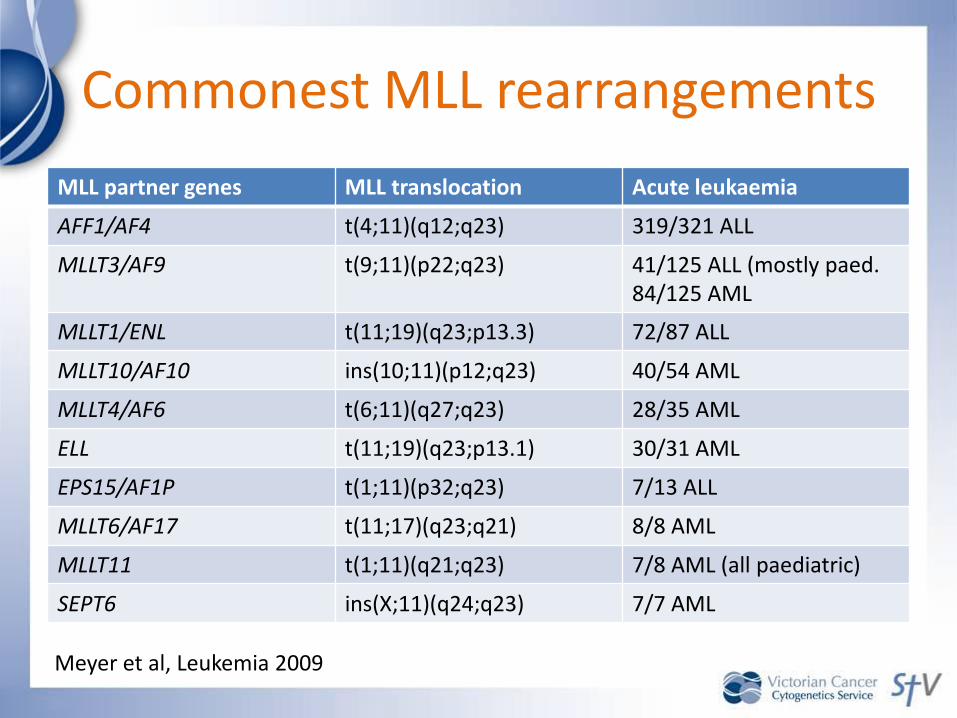
Commonest MLL rearrangements
MLL partner genes MLL translocation Acute leukaemia
AFF1/AF4 t(4;11)(q12;q23) 319/321 ALL
MLLT3/AF9 t(9;11)(p22;q23) 41/125 ALL (mostly paed. 84/125 AML
MLLT1/ENL t(11;19)(q23;p13.3) 72/87 ALL
MLLT10/AF10 ins(10;11)(p12;q23) 40/54 AML
MLLT4/AF6 t(6;11)(q27;q23) 28/35 AML
ELL t(11;19)(q23;p13.1) 30/31 AML
EPS15/AF1P t(1;11)(p32;q23) 7/13 ALL
MLLT6/AF17 t(11;17)(q23;q21) 8/8 AML
MLLT11 t(1;11)(q21;q23) 7/8 AML (all paediatric)
SEPT6 ins(X;11)(q24;q23) 7/7 AML
Meyer et al, Leukemia 2009

Overall survival curve for patients with 11q23/MLL-rearranged pediatric AML grouped on the basis of different
translocation partners
t(1;11)
t(10;11)
Balgobind et al, Blood 2009, Vol. 114, No. 12, pp. 2489-2496

10
p13 (AF10)
11
q14 (CALM)
q23 (MLL)
Recent case: 23 year man presented with AML

FISH required to diagnose t(10;11)
• Type of rearrangement and breakpoints are variable.
• Observed in both ALL and AML
• A significant proportion result in an MLL-AF10fusion (strongly associated with M5/M5a).
• Two other possible transcripts also described.– CALM-AF10 (seen in both T-ALL and immature
AML)
– Rarely MLL-ABI-1 (two cases reported)

Van Limbergen et al (2002) proposed 4 recombination patterns for the MLL/AF10:
• Type 1: inversion of MLL then t with 10p13.
• Type 2: inversion of MLL then ins into 10p13.
• Type 3: inversion of AF10 then t with 11q23.
• Type 4: inversion of AF10 then ins into 11q23.
• Morphologically, our case appeared to be a type 2 inversion / insertion but…

MLL break apart probe: normal result →
assumed to be CALM-AF10 fusion formed by translocation

MRC % SWOG/ECOG %
Good Inv(16)/t(16;16) ;
t(15;17), t(8;21) +/-
other abn;
21
%
Inv(16)/t(16;16) ;
t(15;17)+/- other abn;
t(8;21) without del(9q)
or Cx
20%
Intermediate Normal, 11q23 abn,
+8, del(9q), del(7q),
+21, +22, all others
62
%
Normal, +8, +6, -Y,
del(12p)
46%
Poor Del(5q)/-5, -7, abn
3q, and Complex (≥5
unrelated abn)
t(6;9)*, t(9;22)*
17
%
Del(5q)/-5, -7/del(7q),
abn 3q, 9q, 11q, 20q,
21q, 17p, t(6;9), t(9;22)
and Complex (≥3
unrelated abn)
30%
Unknown N/A All other abn 4%
Prognosis categories in AML
Ref: Slovak et al, Blood, 96: 4075, 2000; Grimwade et al, Blood, 92: 2322, 1998
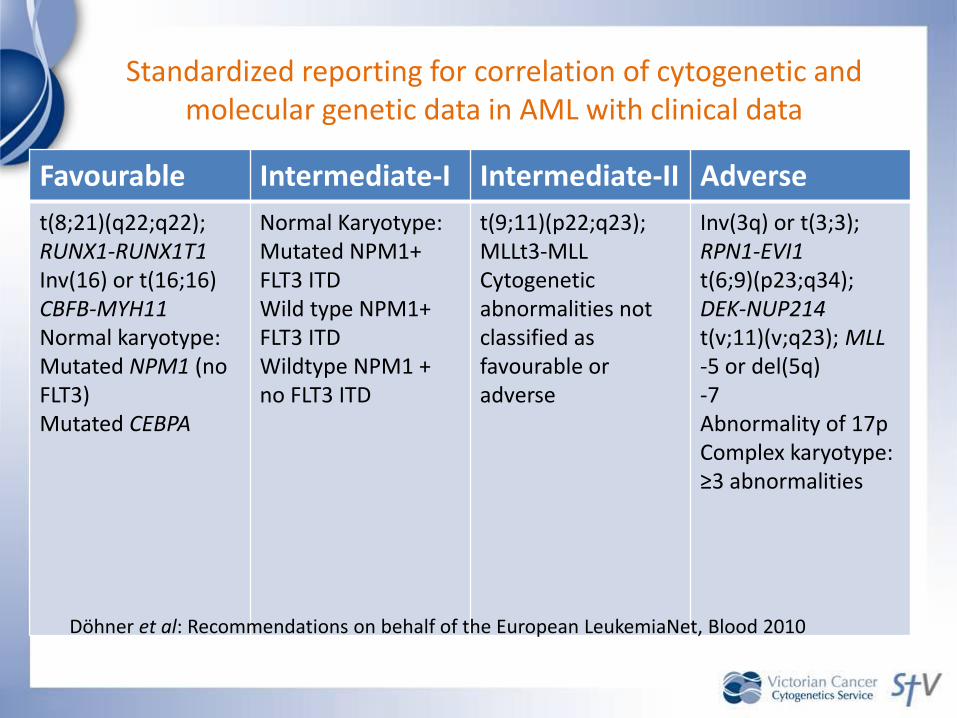
Standardized reporting for correlation of cytogenetic and molecular genetic data in AML with clinical data
Favourable Intermediate-I Intermediate-II Adverse
t(8;21)(q22;q22);RUNX1-RUNX1T1Inv(16) or t(16;16) CBFB-MYH11Normal karyotype:Mutated NPM1 (no FLT3)Mutated CEBPA
Normal Karyotype:Mutated NPM1+ FLT3 ITDWild type NPM1+ FLT3 ITDWildtype NPM1 + no FLT3 ITD
t(9;11)(p22;q23); MLLt3-MLLCytogeneticabnormalities not classified as favourable or adverse
Inv(3q) or t(3;3); RPN1-EVI1t(6;9)(p23;q34); DEK-NUP214t(v;11)(v;q23); MLL-5 or del(5q)-7Abnormality of 17pComplex karyotype:≥3 abnormalities
Döhner et al: Recommendations on behalf of the European LeukemiaNet, Blood 2010

Acquired uniparental disomy in CN-AML
Bollinger et al, Leukemia (2010) 24, 438–449

FISH protocol for AML:
• FISH for t(15;17), inversion 16, t(8;21) or an MLL translocation if morphological or cytogenetic evidence to suggest the presence of a either a standard or variant aberration
• FISH for inversion 16 in all follow-up cases

IPSS for MDS: Survival and AML evolutionScore Value
Prognostic
variable
0 0.5 1.0 1.5 2.0
BM blasts (%) <5 5-10 - 11-20 21-30
Karyotype# Good Intermediate Poor
Cytopenias* 0/1 2/3
# Good: normal, -Y, del(5q), del(20q)
Poor: complex (3) or chromosome 7 abn.Intermediate: other abnormalities
Ref: Greenberg et al, Blood 89: 2079-2088, 1997
* Cytopenias: Hb <100g/L, Neutrophils <1.8x109/L,
Platelets <100x109/L

WPSS for MDS
Variable 0 1 2 3
WHO category RA, RARS, 5q- RCMD, RCMD-RS
RAEB-1 RAEB-2
Karyotype Good Intermediate Poor −
Transfusion requirement *
No Regular − −
Risk groups: Very low score = 0Low score = 1Intermediate score = 2High score = 3-4Very high score = 5-6
* Transfusion dependency = at least one RBC transfusion every 8 weeks over 4 months
Ref: Malcovati et al, JCO, 25: 3503, 2007

Detlef Haase: Updated risk features in MDS
Prog.
group
Chromosome
abnormalities
Time to
25% AML
Survival
(months)
Fav. 5q-, 12p-, 20q-, +21, -Y,
11q-, t(11q23), normal,
5q- plus one other abn
71.9 51
Inter1 +1q, 3q21/q26 abn, +8,
t(7q), +19, -21, any other
single* or double abn
16 29
Inter2 -X, -7/7q-, -7/7q- plus one
other abn, complex = 3
abn
6 15.6
Unfav. Complex > 3 abn 2.8 5.9
* Most common group – ie rare abnormalities

FIP1L1
LNX RPL21 CHIC2
MORF4
GSH2
PDGFRA
KIT KDR
cen tel
Deleted region (800 kb)
4q12 region
Ref: Cools et al, NEJM, 2003
RPCI11-120K16 RCPI11-3H20 RCPI11-24O10
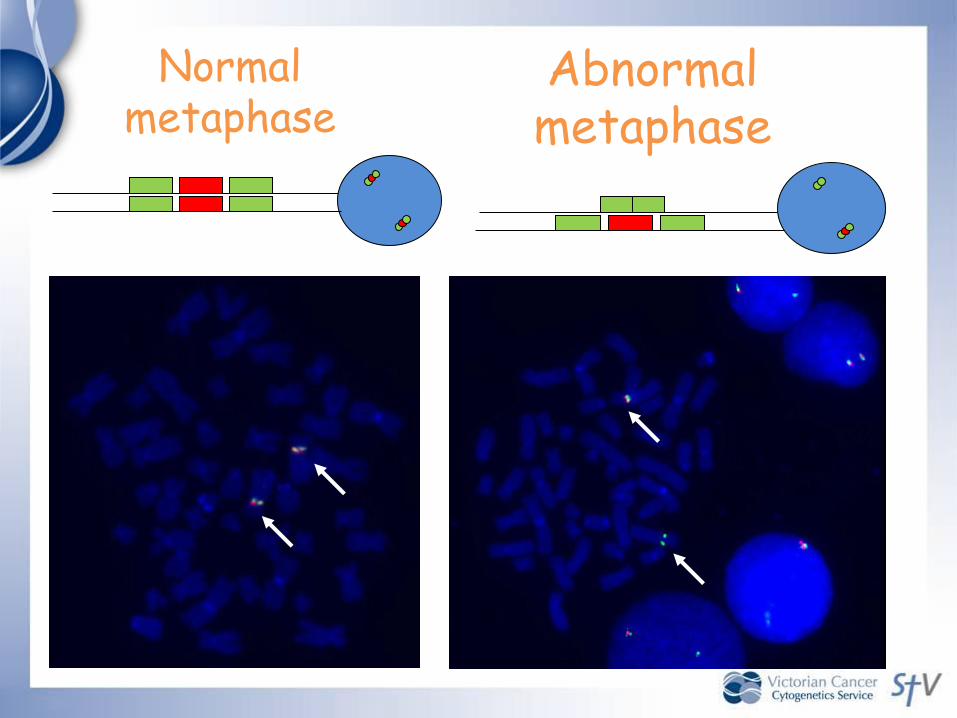
Normal metaphase
Abnormal metaphase

Myeloma cytogenetics
• Chromosome abnormalities detected by both conventional cytogenetics and by fluorescence in situ hybridization (FISH) have been associated with prognosis in multiple myeloma
• Conventional cytogenetic analysis relies on obtaining dividing cells in culture and analysing the chromosome abnormalities
• Use of FISH allows abnormalities to be detected even in non-dividing cells

Common cytogenetic abnormalities• Deletion of 13q observed in 20% by CC and 50% by FISH• An IGH translocation at 14q32 with an oncogene observed in 50% patients with myeloma.
• Translocations resulting in dys-regulation of oncogene –thought to be primary oncogenic events.
IGH partner gene Chromosomallocation
Incidence Prognostic significance
Cyclin D1 11q13 15% -
Cyclin D2 12p13 <1% -
Cyclin D3 6p21 2% -
MAF 16q23 5% Poor
MAFB 20q12 2% -
MAFA 8q24.3 <1% -
MMSET/FGFR3 4p16 15% Poor

Myeloma & FISH
• FISH analysis does not distinguish between the abnormal plasma cell population and other nucleated cells in the bone marrow
• The European Myeloma Network recommendations for FISH in myeloma 2007 state that “it is not acceptable to report FISH results in myeloma without either concentrating the plasma cells or employing some means of plasma cell identification so that only these cells are scored” .

Identifying Labelled Plasma Cells
• cIg labelling:
• Classic PC
morphology
• Antibody labelling
within cytoplasm
• Easily
distinguishable
from other cells

Myeloma cytogenetic/FISH testing
• Conventional cytogenetic analysis: poor prognosis abnormalities:
Hypodiploidy
loss of 13q
• FISH: t(4;14)
t(14;16)
Deletion of 17p (TP53)

FISH in CLLCytogenetic
abnormality
No. cases (325) Median Survival
(months)
Deletion 13q 55% 133
Deletion 11q 18% 79
Trisomy 12q 16% 114
Deletion 17p* 7% 32
Normal Karyotype 18% 111
* Independent prognostic indicator (Dohner et al; Krober et al; Oscier et al 2002)

Monoallelic vs biallelic del(13q)
• Loss of one 13q14 (D13S319) signal is the commonest genetic abnormality in CLL
• As a sole aberration, it predicts a relatively indolent course
• However, it is not uncommon to find a clone with loss of both 13q14 alleles
• Does this carry the same prognostic significance as loss of only one allele?

Chena et al, European J Haematology 2008:
• Studied 103 CLL patients with FISH panels to detect trisomy12, deletions of ATM (11q22), 13q14 and 13q34 (D13S319 and LAMP1) and TP53 (17p13)
• 6/103 (6%) showed biallelic 13q14 loss as sole abnormality and 32/103 (31%) with monoallelicloss
• 6/6 vs 12/32 showed disease progression
• Treatment free survival was 28.5 months vs 49 months

Is it CLL or Mantle cell lymphoma?

11 14 t(11;14)
Cyclin D1
MCL characterised by t(11;14)(q13;q32)
•Causes cyclin D1 upregulation (BCL1, PRAD1, CCND1)
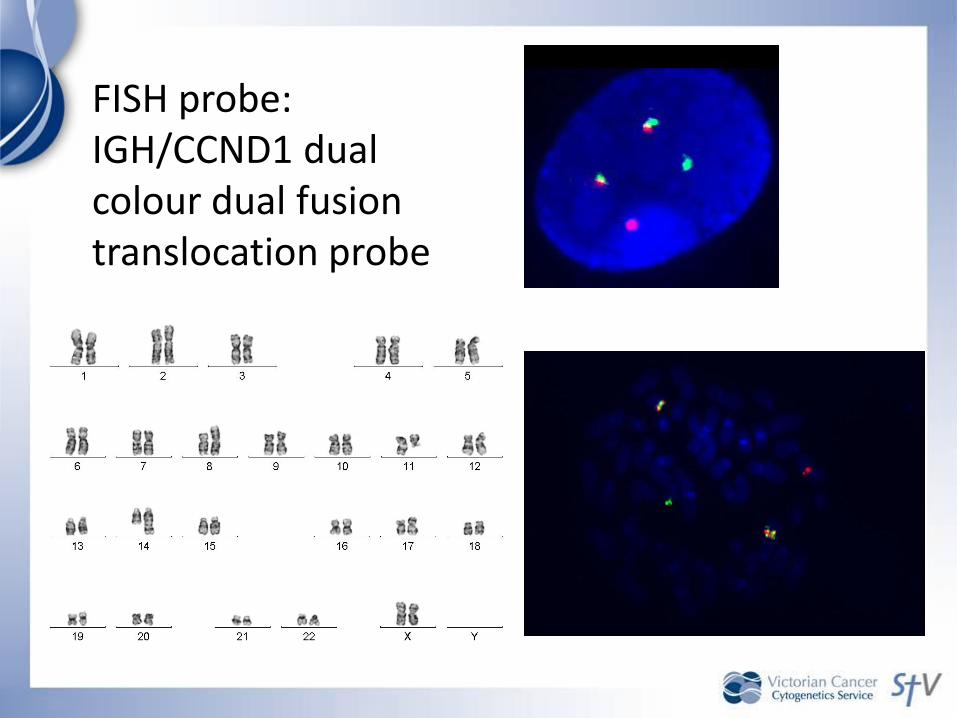
FISH probe: IGH/CCND1 dual colour dual fusion translocation probe

“double hit” lymphomas
• Rare neoplasms characterised by highly aggressive clinical behaviour, complex karyotypesand pathological features overlapping BL, DLBCL and B-lymphoblastic lymphoma/leukaemia
• May have history of FL
• 93 cases over 3 studies: 48 B-cell lymphomas unclassifiable, 45 DLBCL*, 1 B-LBL, 1 FL
• commonly: stage 3-4 disease; high LDH levels; extra nodal disease; BM involvement; CNS disease Niitsu et al, Leukemia 2009
Snuderl et al, Am J Surg Pathol 2010 Johnson et al, 2009

MYC break apart probeDual fusion IGH/BCL2
probe

“Double – hit” lymphoma
• More commonly t(8;22) rather than t(8;14) or non-Ig / MYC translocations plus higher number of chromosomal aberrations
• At 5 years, only 6 survivors and 32 died within 6 months of MYC translocation (Johnson et al)
• Median overall survival 4.5 months inferior to both BL and IPI matched DLBCL (Snuderl et al)
Niitsu et al, Leukemia 2009Snuderl et al, Am J Surg Pathol 2010 Johnson et al, 2009

Dual translocations in DLBCL
Niitsu et al, Leukemia 2009

Acknowledgements: Staff of the VCCS
Cris BatziosKaren BinnionRebecca BowenMelissa CurtisPina D’AchilleCaroline DobrzelakLee HarrisonVeronica HoctorKinjal JoshiRuth MacKinnon Bruce MercerTrish MichaelMegan NolanSrilakshmi NutalapatiFran O’MalleySarah PoileKathleen RayerouxAnne RobertsonDora StamatonikolosLan TaMeg WallJoanne WhiteAdrian Zordan