cyrus mehta ph.d. and lingyun liu ph.d cytel inc., cambridge ma
DESCRIPTION
Adaptive Designs to Demonstrate Risk Reduction in Cardiovascular Outcome Trials A Case Study of the EXAMINE Trial. Cyrus Mehta Ph.D. and Lingyun Liu Ph.D Cytel Inc., Cambridge MA. The EXAMINE Trial. Multicenter randomized double blind placebo controlled study of Alogliptin a DPP4 inhibitor - PowerPoint PPT PresentationTRANSCRIPT

Adaptive Designs to Demonstrate Risk Reduction in Cardiovascular Outcome Trials
A Case Study of the EXAMINE Trial
Cyrus Mehta Ph.D. and Lingyun Liu Ph.DCytel Inc., Cambridge MA

FDA and Industry: September 23, 2014 2
• Multicenter randomized double blind placebo controlled study of Alogliptin a DPP4 inhibitor
• Designed to rule out excess risk of CV outcomes in very high risk T2DM patients
• Primary Endpoint: composite of first occurrence of CV death, MI or stroke (MACE)
• FDA Guidance: estimate upper bound of 95% RCI for the hazard ratio of Alogliptin/Placebo• if < 1.8: submit pre-marketing NDA for alogliptin• if < 1.3: CV safety demonstrated
The EXAMINE Trial

FDA and Industry: September 23, 2014 3
EXAMINE: Group Sequential Design
1.8
1.3
1
80 100 125 150
550 650
550 650
• O’Brien-Fleming spending function
• Sample size: 5400
• Events: 150 for 1.8 and 650 for 1.3
• Enrolment 2 years
• Trial duration 4.25 years
• 94% power for 1.8 for true HR=1
• 91% power for 1.3 for true HR=1
Only 53% power to claim superiority if true HR=0.85

FDA and Industry: September 23, 2014 4
EXAMINE: Study Results
Non-
inferiority HR 1.8
Non-
inferiority HR 1.3
Superior
ity HR 1
83 100 125 150
550 650
550 650
• Total enroll: 5383
• IA1: 83 events• Upper bound of RCI: 1.51• Submitted NDA
• IA2: 550 events• HR: 0.96• Upper bound RCI: 1.17• Stopped to claim non-inferiority
• White et. al. published in NEJM
Trial could have continued to 650 events in hopes of showing superiorityWhy stop at 550 and accept a non-inferiority claim?

FDA and Industry: September 23, 2014 5
Trial was underpowered for Superiority
Hazard Ratio 80% Power 90% Power
Events Sample Size Events Sample Size
0.8 631 5253 845 70340.85 1189 9644 1592 12913
0.9 2829 22377 3787 29954
0.95 11933 92116 15975 123317
Deterrents to an up-front superiority design• Don’t know what HR to target• HR = 0.8 unlikely• HR > 0.85 leads to very large trial with high risk of failure
Sample size requirements for a trial powered to show superiority(assumes 2 years accrual and 3 additional years of follow-up)

FDA and Industry: September 23, 2014 6
• SAVOR-TIMI Trial (NEJM 2013)• Designed up front for superiority• Planned for 1040 events and 16,500 patients• 85% power to detect HR=0.83• O’Brien-Fleming boundary at 50% information
• After enrolling 16,492 patients with 2.1 years median follow-up and 1222 MACE events, the trial failed to show superiority
• Could have designed a smarter trial!
The Risks of Powering Up-Front for Superiority

FDA and Industry: September 23, 2014 7
• Power for non-inferiority with 650 events and 5400 patients
• At interim analysis (IA-550), re-power for superiority by increasing the number of events and sample size provided:1. NI criterion is met (RCI bound < 1.3)2. CP(Sup) is in a “promising zone”
Less risky to allow switching from NI to Superiority objective at interim analysis
FDA and Industry: September 23, 2014 8
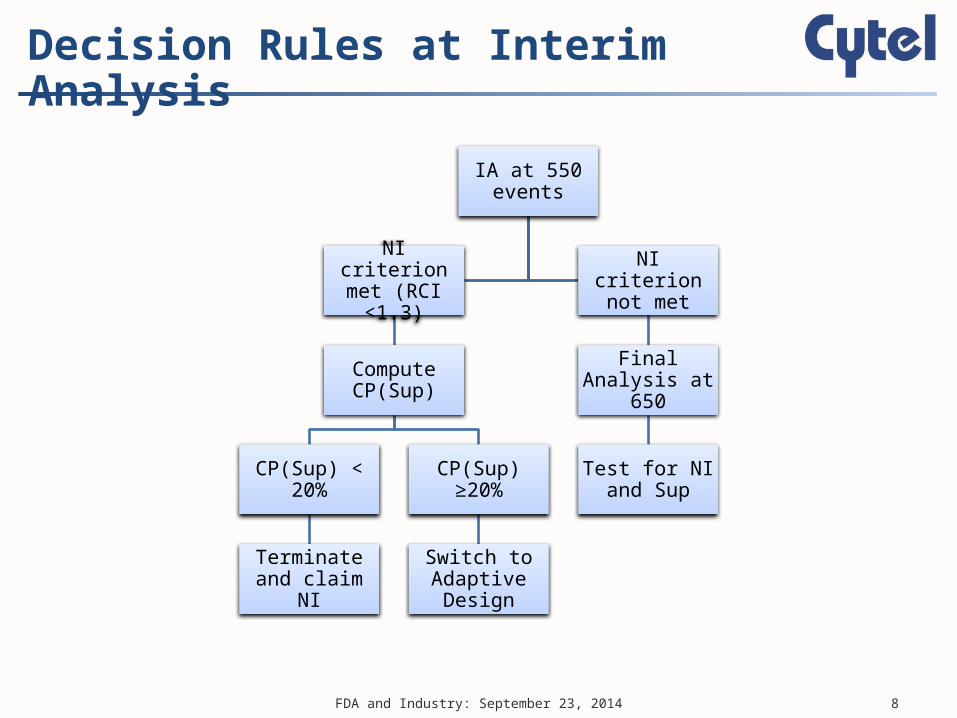
Decision Rules at Interim Analysis
IA at 550 events
NI criterion met (RCI <1.3)
Compute CP(Sup)
CP(Sup) < 20%
Terminate and claim NI
CP(Sup) ≥20%
Switch to Adaptive Design
NI criterion not met
Final Analysis at 650
Test for NI and Sup

FDA and Industry: September 23, 2014 9
The Path to an Adaptive Switch
IA at 550 events
NI criterion met (RCI <1.3)
Compute CP(Sup)
CP(Sup) < 20%
Terminate and claim NI
CP(Sup) ≥20%
Switch to Adaptive Design
NI criterion not met
Final Analysis at 650
Test for NI and Sup

FDA and Industry: September 23, 2014 10
Switch to Adaptive Design
Unfavorable Zone 20%<CP(Sup)<50%
Go to 650 events
Promising Zone50%≤CP(Sup)<90%
Increase events to 1300Incr sample size to 10,800
Go to 650 events
Criteria for adaptive increase of events and sample size

FDA and Industry: September 23, 2014 11
Zones for Decision Making to Claim Superiority after NI Boundary is Crossed
Stop and claim NI: CP(sup)<20%
Unfavorable Zone: 20% ≤CP(sup)<50%Carry on with no change
Promising Zone: 50% <CP(sup)≤90%Double the events and sample size
Favorable Zone: CP(sup)>90%Carry on with no change

FDA and Industry: September 23, 2014 12
• Since promising zone starts at 50% conditional power, no special adjustment needed for the adaptive increase in events (Chen, DeMets and Lan, 2004)
• Thus one can use the classical RCI for a group sequential superiority trial
where D is the number of MACE events at the final analysis (here 650)
No adjustment necessary for adaptation
Dα 2
ln(HR) c

FDA and Industry: September 23, 2014 13
Results: If IA-550 is in Promising Zone
0.8 0.85 0.9 0.95 10
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
Hazard Ratio
Pow
er

FDA and Industry: September 23, 2014 14
Operating Characteristics if HR=0.85
• NI claim is assured• Sup claim has good prospects too
• 40% chance at IA with 550 events• 0.12x0.37= 4% chance at 650 events (no adaptation)• 0.11*0.96=11% chance at 1300 events (adaptation)
• If adaptation occurs, 96% chance of showing Sup

FDA and Industry: September 23, 2014 15
Operating Characteristics if HR=1
• NI claim has at least 90% power (per design) with 76% chance of early stop• Very little (<2%) chance of showing superiority• Only 2% chance of expanding the trial by doubling sample size and events

FDA and Industry: September 23, 2014 16
• All design details are included in DMC charter• DMC buys into design at the kick-off meeting, but
reserves right to exercise clinical judgment• Although the trial is expanded only if the IA at 550
events shows promise of superiority:• Actual interim decision should only be conveyed on
need to know basis (to drug supply and IVRS teams)• Investigators may be told only that this adaptive design
has a maximum sample size of 13,000 patients and possibility of showing superiority
• Double blind design also important to avoid bias
Operational Considerations

FDA and Industry: September 23, 2014 17
• No anti-glycemic agent has shown protection to CV risk
• Huge up-side to being the first on the market• Traditional superiority design requires:
• large up-front commitment of resources• considerable optimism about underlying HR
• SAVOR-TIMI example underscores the risks• Start with modest expectations and expand
only if interim results are promising
Concluding Remarks