curricula health management crash training courseold.iss.it/binary/ures/cont/hmtc.1161243999.pdf ·...
TRANSCRIPT

WHO South Sudan Istituto Superiore di Sanità
CURRICULA
HEALTH MANAGEMENT
CRASH TRAINING COURSE
HMCTC
Rumbek 9 October- 4 November 2006
Under the Project: “WHO Cap2004 SUD-04/H17
Strengthening training facilities for nurses and allied sciences and capacity building of HMs”

ii
CURRICULA
HEALTH MANGEMENT CRASH TRAINING
COURSE - HMCTC
Working Group Components:
Monywir Arop, MOH, Sudan
Alfonso Mazzaccara, ISS, Rome
Viola Vallini, ISS, Rome
Alessandra Torsello, ISS, Rome
Laura Masiello, ISS, Rome
Abdullahi M. Ahmed, WHO Sudan

iii
TABLE OF CONTENTS
LIST OF ACRONYMS. 4
1. SUMMARY 5
2. BACKGROUND. 6
3. THE RELEVANCE OF HMCTC FOR HMs. 8
4. REQUIREMENTS AND CRITERIA FOR PARTICIPATION. 9
5. OBJECTIVES. 10
6. STRUCTURE OF THE HMCTC PROGRAMME. 11
7. THE TEACHING-LEARNING METHOD. 24
8. REFERENCES. 27
Annex I – The Programming. 29
Annex II – Pedagogical Contract: participants’ rights and duties 33
Annex III – Facilitator check list 35
Annex IV – Coordinator check list 36
Annex V – SWOT Analysis 37
Annex VI – Training Costs. 38

LIST OF ACRONYMS
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 4
LIST OF ACRONYMS.
CHWs Community Health Workers
HCDS Health Care Delivery System
HMs Health Managers
HMCTC Health Management Crash Training Course
HMIS Health Management Information System
HRs Human Resources
HSM Health Services Management
HSs Health Services
ISS Istituto Superiore di Sanità
NHS National Health System
MCQ Multiple Choice Questionnaire
MM Monitoring Meeting
MOH Ministry of Health
PM Planning Meeting
PHPC Provisional Health Personnel Council
PBL Problem Based Learning
PHC Primary Health Care
PSM Problem Solving Meeting
SOH Secretary of Health
SPLM/A Sudan People Liberation Movement/Army
TNA Training Need Assessment
WHO World Health Organization

1. SUMMARY
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 5
1. SUMMARY
Following the ruinous effects of the two decades long civil war, South Sudan is now facing the
enormous challenge of the reconstruction of its severely affected institutions, facilities and
infrastructures. The healthcare system, in particular, is today neither adequate nor equitably
distributed throughout the country and suffers from a severe shortage of personnel with the
required professional qualification. This complex situation implies that most of the healthcare
services in South Sudan are currently provided by NGOs, with the support of international
development agencies and foreign governments.
A great effort is then envisaged towards the provision of capacity building to the existing local
health personnel on such issues as: services management, communities’ health needs
assessment, staff supervision and monitoring of quality of services.
On the basis of the above, the TNA that was conducted by ISS in September-November 2005,
targeting the health personnel that was available in accessible areas of South Sudan,
highlighted that awareness of HMs’ responsibilities is currently very poor and most of the survey
respondents do not feel confident with planning, monitoring and evaluation issues.
The emerging need to upgrade the qualification of the existing health personnel has conducted
ISS to evaluate the proposal of a crash training course focused on basic managerial skills,
consisting of 5 residential modules designed to provide participants with fundamental elements
and concepts relative to health policy and function of health management, situation analysis,
planning, implementation, monitoring and evaluation.

2. BACKGROUND
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 6
2. BACKGROUND.
2.1. HSs Delivery in South Sudan.
The recently ended two decades of civil war in South Sudan caused violence and massive
displacement of population and severely affected all the main productive sectors of the country.
The overall demolition of the healthcare system and the consequent harsh deterioration of the
HCSD and infrastructures, in particular, were among the worst effects of this extremely complex
situation.
As a consequence:
The existing health care facilities are neither adequate nor equitably distributed throughout
the country;
There is great shortage of qualified health personnel, with the exception of few high level
cadres;
Most of the healthcare services and training of health personnel are currently provided by
NGOs, with the support of international development agencies and foreign governments.
Since the signing of the peace agreement in January 2005, the SPLM/A has embarked on
strategic development initiatives for political and socio-economic recovery and future
development.
Within the health sector, a great effort is envisaged towards the provision of quality healthcare
services at all levels to the estimated 8 million people in South Sudan and to the additional 3
million refugees in the neighbouring countries.
As a consequence of the creation of the New Sudan and the decentralization process within the
health reform, there is a great need of providing capacity building to the existing personnel on
such issues as: HSM, communities’ health needs assessment, staff supervision and support,
stimulation of community participation to the effective allocation of health resources, monitoring
of quality and managing of change.
2.2. Human Resource for health and TNA in South Sudan.
Due to both the brief and the poor quality of previous training and the several years of practice
in extremely difficult circumstances, almost all the health workers in South Sudan urgently need
to receive intensive training and an upgrading of their professional knowledge.
The total trained health workforce is estimated today at 4,600, two thirds of which are CHWs1.
The highly qualified staff are today expatriates in Kenya and Uganda. Many skilled Sudanese
have attended only one or two years of respective 3-years phased-training programmes. In
1 Jam Sudan Capacity Building & Institutional Development Vol. III 2005

2. BACKGROUND
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 7
most cases, even formal qualifications were attained through sub-standardized training
programmes. Some cadres have been trained abroad.
In order to establish proper standards with regard to contents and length of training
programmes and curriculum, the PHPC was created in the early 1990s. In 2002, the PHPC
became a permanent structure with a management board called Health Personnel Council.
A TNA survey, by means of individual interviews, was conducted by ISS in September-
November 2005, targeting the local health personnel that were available in some areas of South
Sudan selected on the basis of accessibility and security criteria.
Two different questionnaires were developed in order to assess the training needs of high and
middle health cadres, aimed at collecting such data as: candidate’s profile, job related
responsibilities and consequent gap between effective and desired skills, perceived educational
needs, existing skills in teaching methodologies.
The analysis of the collected data highlighted that:
Overall, the extent of awareness of HMs’ responsibilities is very poor;
Most of the survey respondents do not feel confident with planning, monitoring and
evaluation of HSs;
The awareness of the importance of HMIS and its use is generally limited;
The training level of the health personnel is generally very basic;
All HMs perceive the lack of qualified staff and equipment, the inadequate transport facilities
and the low services utilization as the main constraints affecting their effective performance
in HSs delivery;
Overall, the major training needs result in the areas of HSM, including health financing,
leadership and coordination between county and MOH, communication skills and health
promotion.

3. THE RELEVANCE OF HMCTC FOR HMs
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 8
3. THE RELEVANCE OF HMCTC FOR HMs.
The Ministry of Health of the New Sudan had developed a health policy and its implementation
plan. The policy document provided guidelines on the current and future direction on training of
health personnel and delivery of health care services in the country. The health policy had the
following three major areas that were identified as useful for the planning and implementation of
health care services in the country:
a) health services management;
b) health services provision;
c) health human resources development.
In order to achieve the objectives of providing quality and cost effective health care services,
human resources development was a critical success factor. The health policy recognised the
existing gaps in human resources development that need to be filled and spelt out the actions
required in planning and production of health resources resources.
In light of what above indicated, the GOS need to initiate national continuing professional
development programmes in order to update and refresh the skills of health providers and
managers and to upgrade their knowledge base and competencies, which will result into an
improvement in the organization of quality health care and delivery of the related services to
communities.
HMs need to acquire the skills required to manage HSs, including the assessment of the health
needs of the communities, the supervision of staff, the stimulation of community participation to
the effective allocation of HRs and the monitoring of quality.

4. REQUIREMENTS AND CRITERIA FOR PARTICIPATION
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 9
4. REQUIREMENTS AND CRITERIA FOR PARTICIPATION.
The HMCTC is open to graduate and non-graduate health personnel with management
responsibilities at county, hospital and PHC level. Candidates are required at least 3 years work
experience and to be confident with the English language.
REQUIREMENTS
Management responsibilities County, Hospital or PHC
Work experience 3 year
Language Confident with English
Participants will be eligible among the NHS personnel. NGOs local health personnel are also
invited to attend the course.
Previous participation to management courses and partnership or collaboration with
international organizations could be considered as further selection criteria.
Female participation to the training course is strongly encouraged and an equitable
geographical and age distribution of attendees will be considered as a success factor of the
initiative.
Criteria Weight
NHS + + + + +
Local NGOs + + +
Previous participation to management courses +
Collaboration with international organizations +

5. OBJECTIVES
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 10
5. OBJECTIVES.
The HMCTC aims at improving the knowledge and skills of health workers in planning,
managing and evaluating a given health service depending on the background and specific
professional level of individual participants.
At the end of the training programme, participants will be able to:
Describe the main features of HSs organisation and health policies and reforms in
South Sudan;
Appreciate what planning is and how it can be used effectively as a basic management
technique;
Plan, monitor and evaluate HSs in accordance with national health plans and strategies
and considering local priorities, resources and constraints;
Make effective oral and written communications.

6 STRUCTURE OF THE HMTC PROGRAMME
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 11
6. STRUCTURE OF THE HMCTC PROGRAMME.
The proposed duration of the HMCTC Programme is 4 weeks, based upon individual and self-
contained module curricula of 1 week each.
The HMCTC Programme consists of 5 residential modules designed to explore the health policy
framework in South Sudan and to provide participants with elements and concepts concerning
planning and management of HSs.
The modules 1; 2; 3 are structured in 2 units content meanwhile modules 4 and 5 are structured
in 1 unit content.
All of them delivered with the PBL approach in practical sessions, will be weighted according to
its duration in weeks (i.e. 1 week duration = 1 credit week). In order to obtain the credits,
participants will have to pass the tests foreseen per each module.
In order to achieve the HMCTC, participants are required to complete the residential modules (4
credits weeks)
The structure of HMCTC Programme is summarised in table I.
Table I - HMCTC Programme
Modules Credits
(weeks)
1 - Health policy and function of health management 1
2 - Situation Analysis 1
3 - Health Planning 1
4 – Implementation 0,5
5 - Monitoring and Evaluation 0,5
Total 4
Besides the managerial skills, a health manager needs to acquire communication skills. After
focusing on theoretical concepts and models about the nature of communication, within
different modules, participants will acquire tools and skills in interacting with people at different
levels, preparing and presenting papers, reports and plans. This module entails continuous
monitoring of participants' progress from the start to the end of the course.
6.1. Modules outline
Rationale, objectives, content, time framework, participants’ assessment and main references of
the modules are shown in the following pages.
6. STRUCTURE OF THE HMCTC PROGRAMME
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 12
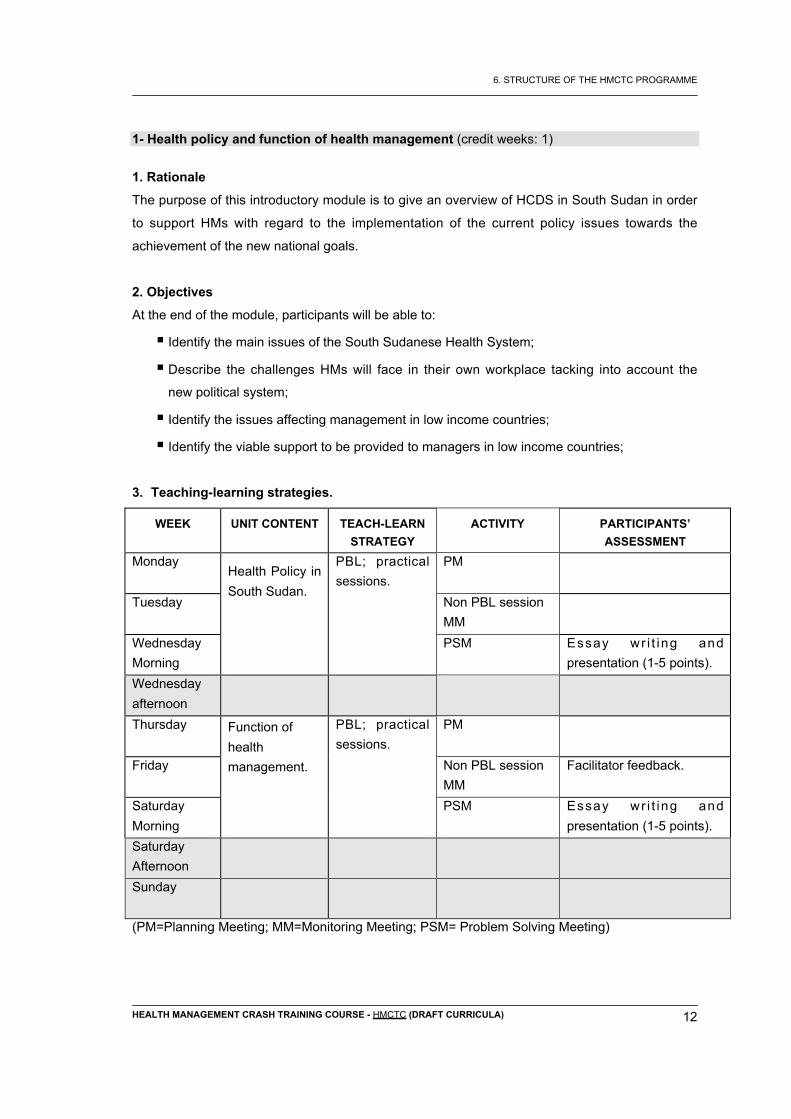
1- Health policy and function of health management (credit weeks: 1)
1. Rationale
The purpose of this introductory module is to give an overview of HCDS in South Sudan in order
to support HMs with regard to the implementation of the current policy issues towards the
achievement of the new national goals.
2. Objectives
At the end of the module, participants will be able to:
Identify the main issues of the South Sudanese Health System;
Describe the challenges HMs will face in their own workplace tacking into account the
new political system;
Identify the issues affecting management in low income countries;
Identify the viable support to be provided to managers in low income countries;
3. Teaching-learning strategies.
WEEK UNIT CONTENT TEACH-LEARN
STRATEGY
ACTIVITY PARTICIPANTS’
ASSESSMENT
Monday PM
Tuesday Non PBL session
MM
Wednesday
Morning
Health Policy in
South Sudan.
PBL; practical
sessions.
PSM Essay wr i t ing and
presentation (1-5 points).
Wednesday
afternoon
Thursday PM
Friday
Function of
health
management.
PBL; practical
sessions.
Non PBL session
MM
Facilitator feedback.
Saturday
Morning
PSM Essay wr i t ing and
presentation (1-5 points).
Saturday
Afternoon
Sunday
(PM=Planning Meeting; MM=Monitoring Meeting; PSM= Problem Solving Meeting)

6. STRUCTURE OF THE HMCTC PROGRAMME
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 13
4. List of reading materials.
4.1. Learning materials
Books
McMahon R, et al., “On being in charge. A guide to management in primary health care”, WHO,
Geneva 1992. Pages: 13- 27. (Pages amount: 15)
Articles
1. Jam Sudan Capacity Building & Institutional Development, Vol. III 2005.
Pages 24-34; 169-174; 183-190. (Pages amount: 22)
2. Country Cooperation Strategy for WHO and Sudan: 2003–2007
Pages 1-14
3. Health Policy and Management. Chapter 3. Annual Report 2004, WHO.
Pages 1-10
4. South Sudan Interim Health Policy 2006-2011, December 2005 – South Sudan Federal
Ministry of Health. Pages 1-36
5. Sudan Health Status Report, WB/AFTH3 2003
Pages 9-12; 60-66; 88-94 (Pages amount: 18)
6. Policy Document for Health in post conflict Sudan. Republic of Sudan, Federal Ministry of
Health, 2003.
Pages 1-5
7. Management, Leadership and partnership for District Health, WHO Regional Office for
Africa, 2004. Module 2, unit 1: Important management and leadership concepts, pages: 1-8.
Http: //www.afro.who.int/dsd/dhm-training/index.htm
4.2 Consultation material.
Articles and journals (if available a web link):
British Medical Journal: http://www.bmj.com.
Health Policy and Planning: http://heapol.oupjournals.org.
5. Resources Persons.
MOH South Sudan: Monwyiir Arop

6. STRUCTURE OF THE HMCTC PROGRAMME
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 14
2-Situation Analysis (credit weeks: 1)
1. Rationale.
Quantitative methods (epidemiology) are a fundamental tool in planning and evaluation of HSs,
from identifying priority health issues to allocating resources effectively and efficiently.
Epidemiology is the study of the distribution, frequency and determinants of health problems
and diseases in the human population. The purpose of epidemiology with the support of
statistical techniques is to obtain, interpret and use the health information needed for planning,
managing and evaluating all the activities required to promote health and prevent diseases. In
the absence of such epidemiological data there is a tendency to tackle public health problems
through indiscriminate mass intervention. Such an approach is not only wasteful but has often
proved to be ineffective.
In order to plan interventions, HMs will need the epidemiological and statistical skills required by
the following tasks:
Define population by age/sex structure, migration and vital statistics;
Assess the health status of the population and high risk groups, particularly important
causes of morbidity and mortality;
Collect health data through routine services, surveillance, epidemics and surveys;
Produce health information by analysis of data;
Decide on the priority health problems;
Use health information in order to select proper initiatives;
Estimate increase in access and coverage;
Determine changes in health status in the district population.
In particular the descriptive (diseases distribution and frequency) and evaluation epidemiology
(measure of the effectiveness of different HSs and programmes) can be extremely useful and
should be widely used by HMs.
This module will enable participants to use basic data as a tool for assessing population health
needs.
2. Objectives.
At the end of the module participants will be able to:
Register and collect the data related to the field situation;
Analyse and interpret these data;
Transmit and present the above data;
Understand the uses of epidemiological information in planning and evaluation of HSs.

6. STRUCTURE OF THE HMCTC PROGRAMME
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 15
3. Teaching-learning strategies.
WEEK UNIT CONTENT TEACH-LEARN
STRATEGY
ACTIVITY PARTICIPANTS’
ASSESSMENT
Monday PM
Tuesday Non PBL session
MM
Wednesday
Morning
Data
management.
PBL; practical
sessions.
PSM Essay wr i t ing and
presentation (1-5 points).
Wednesday
Afternoon
Thursday PM
Friday
The use of data
in planning and
evaluation.
PBL; practical
sessions.
Non PBL session
MM
Facilitator feedback.
Saturday
Morning
PSM Essay wr i t ing and
presentation (1-5 points).
Saturday
Afternoon
Sunday
(PM=Planning Meeting; MM=Monitoring Meeting; PSM=Problem Solving Meeting)
4. List of reading materials.
4.1. Learning materials.
Books
Vaughan JP, Morrow RH. Manual of epidemiology for district health management. WHO,
Geneva 1989 (Pages 71-153).
Articles
How to conduct a rapid situation analysis. Mc Coy D. Bammford L. Health Fund Trust; South
Africa – 1998. (Pages. 1-49).
4.2. Consultation material.
Books
1. Coggon D., Rose G., Barker D.J.P. Epidemiology for uninitiated. BMJ Publishing Group,
2003.
2. Swinscow T D V Statistics at square one. BMJ Publishing Group, 1997.

6. STRUCTURE OF THE HMCTC PROGRAMME
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 16
Articles and journals (if available a web link):
British Medical Journal: http://www.bmj.com.
The International Journal of Epidemiology: http://ije.oupjournals.org.
American Journal of Epidemiology: http://www3.oup.co.uk/aje.
5. Resources Persons.
WHO South Sudan: Amos Paul Bassi

6. STRUCTURE OF THE HMCTC PROGRAMME
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 17
3-Planning and health management (credit weeks: 1)
1. Rationale
Planning is one of the main responsibilities of HMs aimed at ensuring both the current and
future availability of resources and their efficient utilization towards the realization of defined
objectives. The basis for planning is the dilemma of scarce resources coupled with vast health
care needs, thus implying a need of making decisions about how the HMs will use its resource
in the future. After learning the differences between strategic and operational planning,
participants will have an overview of the "Project cycle" approach and its steps: situation
analysis; problem identification; priority setting; planning, management, monitoring, assessment
and evaluation of activities.
2. Objectives.
At the end of this module participants will able to:
Use available data for problem identification;
Define general and specific objectives;
Plan an activity by setting priorities according to the available resources;
Chose the most appropriate strategies to reach the defined objective.
1. Teaching-learning strategies.
WEEK UNIT CONTENT TEACH-LEARN
STRATEGY
ACTIVITY PARTICIPANTS’
ASSESSMENT
Monday PM
Tuesday Non PBL session
MM
Wednesday
Morning
Problem
identification
and Objective
definition.
PBL; practical
sessions.
PSM Essay wr i t ing and
presentation (1-5 points).
Wednesday
afternoon
Thursday PM
Friday
Priority setting
and decision
making.
PBL; practical
sessions.
Non PBL session
MM
Facilitator feedback.
Saturday
Morning
PSM Essay wr i t ing and
presentation (1-5 points).
Saturday
Afternoon
Sunday
(PM=Planning Meeting; MM=Monitoring Meeting; PSM=Problem Solving Meeting)

6. STRUCTURE OF THE HMCTC PROGRAMME
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 18
4. List of reading materials
4.1. Reading Materials.
Books
1. Project Cycle Management Guidelines – European Commission; (2004).158 pages.
2. Planning and implementation of District Health Services. WHO – Regional Office for Africa
Brazzaville, 2004. pages. 24 - 31.
Articles
1. Problem tree. WB – 2001 2 pages
http://web.mit.edu/urbanupgrading/upgrading/issues-tools/tools/problem-tree.html
2. SWOC - FAO 8 pages
http://www.fao.org//docrep/005/y4401e/y4401e0d.htm
4.2. Consultation Materials.
Books
1. McMahon R, et al. On being in charge. A guide to management in primary health care.
WHO, Geneva 1992.
2. A. Green. An introduction to Health planning in developing countries. 2002.
Articles and journals (if available a web link):
British Medical Journal: http://www.bmj.com.
Health Policy and Planning: http://heapol.oupjournals.org.
5. Resources Persons.
ISS Alfonso Mazzaccara.

6. STRUCTURE OF THE HMCTC PROGRAMME
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 19
4 - Implementation through HRs and Communication Skills (credit weeks: 0,5)
1. Rationale.
HRs are estimated to represent up to 75% of the healthcare systems expenditures in many
countries. As such, if HRs are poorly planned, the implications for the health service itself can
be extremely serious.
Despite the above, data relative to HRs management are still poor in South Sudan. Common
problems affecting HRs in South Sudan include the following:
Small number of trained and available personnel;
High concentration of health staff in urban hospital settings and shortages in rural
areas;
Inappropriate use of personnel;
Unproductive or demoralised staff.
In recognition of this, management of HRs will be a core module within the HMCTC programme.
The module aims at providing participants with the knowledge and skills required for managing
health personnel, from leading a team in a supportive way to organising team activities and from
assessing manpower demand and supply to developing a human resource plan.
Participants will gain knowledge and skills on different methods of implementing selected
programmes and activities.
2. Objectives.
At the end of this module participants will be able to:
Prepare a job description;
Discuss a task analysis;
Design a tree diagram;
Carry out effective supervision of health workers;
Introduce change and resolve conflicts among staff;
Foster good communication among health workers;
Run a meeting.

6. STRUCTURE OF THE HMCTC PROGRAMME
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 20
3. Teaching-learning strategies.
WEEK UNIT CONTENT TEACH-LEARN
STRATEGY
ACTIVITY PARTICIPANTS’
ASSESSMENT
Monday PM
Tuesday Non PBL session
MM
Facilitator feedback.
Wednesday
Implementation
o f p lanned
activities
through the
appropriate
HRs and using
appropriate
communication
skills.
PBL; practical
sessions.
PSM Essay wr i t ing and
presentation (1-5 points).
(PM=Planning Meeting; MM=Monitoring Meeting; PSM=Problem Solving Meeting)

6. STRUCTURE OF THE HMCTC PROGRAMME
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 21
4. List of reading materials
4.1. Reading Materials.
Articles and Report
1. Management, Leadership and partnership for District Health, WHO Regional Office for
Africa, 2004. Module 3, Unit 1: “Management of Human Resources for Health”, pages: 1-
18; Communication pp. 6-10; Supervision pp. 12-16; Managing Interpersonal Conflict pp.
17-18;
Unit 6: “Managing Time and Space" pp. 49-54
Http: //www.afro.who.int/dsd/dhm-training/index.htm.
2. Working together for health. WHO, 2006. "Working in conflict and post conflict
environments". Pages 1-4.
Http: //www.who.int/whr/2006/06_chap2_en.pdf
3. Leading, ISS reading material, 2006, pages: 1-2.
4. Identifying Communication Styles for success, ISS reading material, Rome, 2006, pages:
1-3.
5. Conflict resolution: a communication tool for change, ISS reading material, Rome, 2006,
pages: 1-3.
6. Internal communication strategies, ISS reading material, Rome, 2006, pages: 1-3.
7. Conflict and cooperation in workplace, ISS reading material, Rome, 2006, pages: 1- 2.
8. Conflict resolution, ISS reading material, Rome, 2006, pages: 1- 3.
9. Human resources for health, WHO-WPRO,p.1
Consultation Books
1. Teaching for better learning, Abbatt, F.R. WHO 1992;
2. McMahon R, et al. “On being in charge. A guide to management in primary health care”.
WHO, Geneva 1992.
Journals
BioMed Central - Online journal http://www.human-resources-health.com/
5. Resources Persons.
___________________________

6. STRUCTURE OF THE HMCTC PROGRAMME
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 22
5-Monitoring and Evaluation (credit weeks: 0,5)
1. Rationale.
HMs should be acquainted with the planning process and be able to manage and evaluate HSs
from assessing community health needs, to deciding on priorities, setting objectives, selecting
indicators, identifying activities and responsibilities and allocating resources effectively.
Participants will gain knowledge and skills on different methods of monitoring and evaluation
and their central role in health care delivery.
2. Objectives.
At the end of the module the participant will be able to:
Monitor the work progresses according to schedule;
Monitor inputs: material, financial and information resources for public and private
health services;
Monitor outputs: quality of private and public HSs performance according to local
standards;
Evaluate the achievement of health team in services delivered and their impact in
reducing the priority health problems of the community;
Evaluate the efficient use of the health team resources;
Ensure community participation in monitoring and evaluating HSs.
3. Teaching-learning strategies.
WEEK UNIT CONTENT TEACH-LEARN
STRATEGY
ACTIVITY PARTICIPANTS’
ASSESSMENT
Thursday PM
Friday
PBL; practical
sessions.
Non PBL session
MM
Facilitator feedback.
Saturday
Morning
Building a set
of indicators for
monitoring.Eval
uate HSs:
quantitative
and qualitative
approach.
PSM Essay wr i t ing and
presentation (1-5 points).
Saturday
Sunday
(PM=Planning Meeting; MM=Monitoring Meeting; PSM=Problem Solving Meeting)

6. STRUCTURE OF THE HMCTC PROGRAMME
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 23
4. List of reading materials.
4.1. Reading Materials.
Books
Planning and implementation of District Health Services. WHO – Regional Office for Africa
Brazzaville, 2004. pg. 41-43
Participatory Monitoring and Evaluation. A strategy for organization strengthening. F.W. Mulwa,
S.N. Nguluu. 2003. Pages.38-42, 52-64, 99-113.
Articles and Report
1. Monitoring and evaluation some tools, methods & approaches. WB –2004. (26 pages)
4.2. Consultation Materials.
Books
McMahon R, et al. On being in charge. A guide to management in primary health care - WHO,
Geneva 1992.
Articles and journals (if available a web link):
1. International Journal for quality in Health care. http://intqhc.oxfordjournals.org/
2. Framework for programme evaluation, Execut ive Board, WHO, 2000
http://who.int/gb/ebwha/pdf-files/EB107/eeid3.pdf. (4 pages)
Resource Person.
__________________________

6. STRUCTURE OF THE HMCTC PROGRAMME
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 24
7. THE TEACHING-LEARNING METHOD.
The teaching-learning method adopted finds its main and distinctive pillar in the PBL approach
(1, 2, 3, 4, 5). PBL, at its most fundamental level, is an instructional method characterised by
the use of "real world" problems as a context for participants to learn critical thinking and
problem solving skills, and acquire knowledge of the essential concepts of the course. Using
PBL, participants acquire life long learning skills, which include the ability, to find and use
appropriate learning resources. The process used in PBL is the following:
1. Participants are presented with a problem (case, research paper, video tape, for example).
Participants (in small groups, 6-8 people) organise their ideas and previous knowledge
related to the problem, and attempt to define the broad nature of the problem.
2. Throughout discussion, participants pose questions, called "learning issues," on aspects of
the problem that they do not understand. These learning issues are recorded by the group.
Participants are continually encouraged to define what they know - and more importantly -
what they don't know.
3. Participants rank, in order of importance, the learning issues generated in the session. They
decide which questions will be followed up by the whole group, and which issues can be
assigned to individuals, who later present to the rest of the group. Participants and
instructor also discuss what resources will be needed in order to research the learning
issues, and where they could be found.
4. When participants reconvene, they explore the previous learning issues, integrating their
new knowledge into the context of the problem. Participants are also encouraged to
summarise their knowledge and connect new concepts to old ones. They continue to define
new learning issues as they progress through the problem. Participants soon see that
learning is an ongoing process, and that there will always be (even for the teacher) learning
issues to be explored.
Tutor/facilitator plays a central role in the PBL process, guiding and supporting the participants
as they "learn how to learn." Each student PBL group has a dedicated tutor whose role is to
stimulate discussion, hone the students' ability to analyse and critique the information they bring
to group discussions, and monitor the group process. A Tutor’s Guide will help tutors in
facilitating the PBL sessions.

6. STRUCTURE OF THE HMCTC PROGRAMME
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 25
A Participants’ Guide, including the module cover page, the objectives and the problems will be
provided to the participants at the beginning of each unit.
A Facilitator Guide, including the general and specific objectives, the problems and the main
lectures will be provided to the facilitator at the beginning of the course to engineering the
method and to guide in a coherent a homogenous way the facilitator.
A part from PBL, non-PBL activities, such as lectures, seminars, audiovisuals, simulation
games, informatics sessions, and exercises will be also adopted.
7.1. Monitoring and evaluation.
Monitoring and evaluation is essential for the success of any training programme. It will deal
with the implementation of the programme and the performance of the participants.
Formal evaluation will be implemented to ensure the possibility to certify at the end of the
course the achievement of the defined objective.
Formative evaluation will be implemented to stimulate the progress of the participant using self,
pair and facilitator feedback.
7.1.1. Evaluation of programme.
Due to the “pilot” value of the first course an anonymous MCQ test will be provided to the
participant at the beginning and at the end of the course to assess the participant increasing of
knowledge.
At the same time the satisfaction of the customers will be assessed by a questionnaire:
From the inception to the implementation of the training programs, a systematic monitoring of its
adequacy and how it will meet participants’ needs will be conducted. At the end of each module,
tutors will prepare and distribute a questionnaire to all participants.
The questionnaire will cover the following areas:
– Extent to which the learning objectives have been achieved
– Relevance of course contents with regard to planned learning objectives
– Quality of teaching methods
– Tutors’ professionalism, availability and courtesy
– Availability, quantity and quality of learning materials
– Time allocated for the different steps of PBL
– Ameliorative proposals.
6. STRUCTURE OF THE HMCTC PROGRAMME
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 26
7.1.2. Participants’ assessment
As in any programme utilising PBL, the following assessment tools will be used -
Formal evaluation:
a. Individual written test: includes multiple choice, true/false questions aimed at assessing
knowledge and skills gained, as certifying assessment.
The suggested evaluation scale is as follow:
1= Unsatisfactory; 2= Below average; 3= Average; 4= Very good; 5=Excellent
The pass mark is 3.
b. Oral presentation skills assessment: short oral presentation on a topic relevant to the
objectives of the module. This is aimed at assessing presentation skills. Handouts will be
distributed in the framework of an ad-hoc seminar.
Formative Evaluation
a. Weekly peer and facilitator feedback: aimed at monitoring group-work skills.
b. Final feedback by facilitator: aimed at assessing participant's ability to work effectively in a
group. It provides feedback on individual basis
c. Peer evaluation will be ensured asking to the participants, starting from the third week to
create an assessment grid to use during the problem-solving meeting.
d. Self-evaluation will be ensured anonymously through the MCQ pre-post test.

8. REFERENCES
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 27
8. REFERENCES.
1. Aronson B. Improving online access to medical information for low-income countries. New England
Journal of Medicine, 2004, 350:966–968. http://content.nejm.org/cgi/reprint/350/10/966.pdf
2. Barrows HS. Designing a Problem Based Curriculum for the Pre-Clinical years. Springer
Publishing Company, New York 1985.
3. Barrows HS, Tamblyn RM. Problem-Based Learning: An Approach to Medical Education.
Springer Publishing Company, New York 1980.
4. Boud D, Felleti G. The Challenge of Problem-Based Learning. Kogan, London 1991.
5. Woods D R. Problem-Based Learning: How to Gain the Most from PBL. Donald R. Woods
Publisher, Hamilton, Ontario, Canada 1994.
6. Bouhuijs PAJ, Schmidt HG, Van Berkel HJM. Problem-Based Learning as an Educational
Strategy. Network Publications, Maastricht, 1993.
7. Butler R, Inman D, Lobb D. Problem-based learning and the medical school: another case
of the emperor’s new clothes? Advances in Physiology Education, 2005, 29:194–196.
http://advan.physiology.org/cgi/reprint/29/4/194
8. Dolmans DH, De Grave W, Wolfhagen IH, van der Vleuten CP. Problem-based learning:
future challenges for educational practice and research. Medical Education, 2005,
39:732–741. http://www.blackwell-synergy.com/doi/abs/10.1111/j.1365-2929.2005.02205.x
9. Evaluation of the Prime Minister’s Lady Health Worker Programme. Oxford, Oxford Policy
Management, 2002 (http://www.opml.co.uk/social_policy/health/cn1064_lhw.html),
10. Freire P. Education for critical consciousness. London Sheed and Ward, 1973.
11. Guilbert, J.J. Educational Handbook for Health Personnel Geneva, WHO, 1992.
12. Kaufman A. Implementing Problem-Based Learning Education. Springer Publishing
Company, New York 1985.
13. Knowles, M. (1984). The Adult Learner: A Neglected Species (3rd Ed.). Houston, TX: Gulf
Publishing.
14. Knowles, M. (1984). Andragogy in Action. San Francisco: Jossey-Bass Scherpbier AJJA,
15. Huddart J, Picazo OF, Duale S. The health sector human resource crisis in Africa: an issues
paper. Washington, DC, United States Agency for International Development, Bureau for
Africa, Office of Sustainable Development, 2003.
16. Littlewood S, Ypinazar V, Margolis SA, Scherpbier A, Spencer J, Dornan T. Early practical
experience and the social responsiveness of clinical education: systematic review. BMJ,
2005, 331:387–391. http://www.pubmedcentral.gov/articlerender.fcgi?tool=pubmed&pubmedid=16096306
17. Slovensky DJ, Paustian PE. Preparing for diversity management strategies: teaching tactics
for an undergraduate healthcare management program. Journal of Health Administration
8. REFERENCES
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 28
Education, 2005, 22:189–199.
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=15960
025&dopt=Abstract
18. Sturmberg JP, Reid S, Khadra MH. A longitudinal, patient-centred, integrated curriculum: facilitating
community-based education in a rural clinical school. Education for Health: Change in Learning and
Practice, 2002, 15:294–304.
http://taylorandfrancis.metapress.com/(sifmkwvf2xyfrln5jomw3j55)/app/home/contribution.asp?refer
rer=parent&backto=issue,3,22;journal,11,19;linkingpublicationresults,1:104574,1
19. Van Der Vleuten CPM, Rethans JJ, Van der Steeg AFW. Advances in Medical Education.
Kluwer Academic Publishers, Dordrecht, Netherlands 1997.
20. Walsh A. The tutor in problem-based learning: a novice’s guide. Hamilton, McMasterUniversity,
2005. http://www.fhs.mcmaster.ca/facdev/tutorPBL.pdf
Some Institutions involved in PBL.
Bowman Gray School of Medicine http://isnet.is.wfu.edu/bgsm/library/hughes.html.
McMaster University http://www-hsl.mcmaster.ca/faculty/workshops.html.
Maastricht University http://www.unimaas.nl/pbl/.
Harverd University Harvard Medical School - the "new pathway".

Annex 1 - The Programming
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 29
Annex I – The Programming.
HMCTC - Pilot Study
Where: Rumbek
When: May/June
Who: Staff: 1 Project Coordinator (9 weeks)
Skills required: Post-Graduate diploma; 10 years minimum work experience,
preferbly in Africa; Relevant experience in team and project coordination,
managing logistics and administration; Specific skills: fluency in English,
knowledge of the area preferable.
The job holders:
The organization will meet the person in charge for WHO/South Sudan
office to get information about the present situation in South Sudan in terms
of logistics issues such as transport, flights schedules etc;
Jointly with WHO person in charge will meet the Director of Sudanese
Human Resources Department to finalize the already agreed criteria for
selecting participants to the Crash Training and, to get a complete list
(name, title and location) of the selected participants;
Will be responsible for procuring and purchasing “in loco” training material
and equipment (if needed). The list of material and equipment will be
provided before her/his leaving;
Will ensure a safe and prompt transportation of material and equipment to
the field (through air transportation planning);
Will be responsible for travel and accommodation arrangement of
participants and expatriates by air transportation planning;
Will establish and maintain regular communication with WHO/Nairobi/South
Sudan office and, with ISS/Rome office;

Annex 1 - The Programming
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 30
Who: Staff: 1 Course Coordinator (5 weeks)
Skills required:
Post-Graduate diploma; 10 years minimum training work experience, preferably
in Africa; Relevant experience in team and project coordination, managing
training courses and modules; Specific skills: fluency in English, knowledge of
the area preferable.
The job holders:
To draft the program and the context of the Training course, on the basis of
the TNA;
To manage and prepare with ISS staff and facilitators the learning material
(for each module: introduction; problem; reading material, seminar, the
assessment system; participant and facilitator guide);
To coordinate the Training course;
To manage and organize facilitators activities;
To coordinate facilitators and participants in the field;
To understand participants and facilitators needs;
To solve-problems between participants and facilitators;
To advise and help facilitators;
To manage the participants assessment;
To manage the module assessment;
To asses facilitators performance and give suggestions;
To improve the organization and coordination of the Training course on the
basis of the lessons learned.

Annex 1 - The Programming
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 31
Who: Staff 3 Facilitators (5 weeks each)
Skills required:
Post-Graduate diploma; 3 years minimum work experience, preferably in Africa;
Course on PBL methodology; Pevious experience in team and project
coordination; Specific skills: fluency in English, knowledge of the area
preferable.
Tasks:
The job holders:
• To collaborate with the ISS staff to the production of the learning material
(for each module: introduction; problem; reading material, seminar, the
assessment system; participant and facilitator guide)
• To facilitate the participants learning process
• To collaborate with the coordinator during the field work
• To participate to the participants assessment
• To participate to the module assessment
• To modify on the basis of the lessons learned the learning material for the
following course.
Who: Trainee A maximum of 24 participants

Annex 1 - The Programming
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 32
HMCTC – Courses
How On the basis of the course evaluation, according to the lessons learned a
maximum of 1-2 courses will be developed
Where: To define
When: October/November
Who trainers: 1 Project Coordinator (9 weeks)
Tasks:
The same mentioned above more eventual new elements to consider on
the basis of the lessons learned during the pilot course.
1 Course Quality Manager (5 weeks)
Tasks:
To coordinate with each course coordinator the Training course;
To manage and organize coordinators activities;
To standardize the methodology among the different coordinator
To solve-problems between coordinators and facilitators;
To advise and help coordinators;
To manage the coordinator supervision;
To standardize the module assessment;
To supervise coordinator performance and give suggestions;
To improve the organization and coordination of the Training course on
the basis of the lessons learned.
3 Course Coordinator
Tasks:
The same mentioned above more eventual new elements to consider on
the basis of the lessons learned during the pilot course
6 Facilitators
Tasks:
The same mentioned above more eventual new elements to consider on
the basis of the lessons learned during the pilot course
Who Trainee A maximum of 16 participants for each course

Annex II – Pedagogical Contract
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 33
Annex II – Pedagogical Contract: participants’ rights and duties
Structure of HMCTC and timing
The participants will receive a course (HMCTC) of 5 residential modules designed to explore the
health policy framework in South Sudan and will be provided with the fundamental elements
and concepts concerning planning and management of HSs.
Each module will be weighted according to its duration in weeks (i.e. 1 week duration = 1 credit
week). Each module will be structured in 2 units content, delivered with the PBL approach in
practical sessions.
In order to obtain the credits, participants will have to pass the written tests foreseen per each
module.
In order to achieve the HMCTC, participants are required to complete the residential modules (5
credits weeks).
Presence of participants to the entire course program is considered compulsory, in order to
obtain the final certificates of attendance from the MoH of GoSS.
Material
The participant will receive at the beginning of the course a Participants’ Guide, including the
module cover page, the objectives of the course.
The problems of each week will be provided to the participants at the beginning of each unit.
The participant will receive a mean of 10 pages for each individual study hour as reading
material.
The participants task will be to prioritise among this material choosing the main relevant topics
to study for the problem-solving meeting.
A part from PBL, non-PBL activities, such as lectures, seminars, audiovisuals, simulation
games, informatics sessions, exercises will be provided to the participants.
Participants Monitoring and Evaluation
The assessment of the participants will be based on Formal evaluation necessary to certify at
the end of the course the achievement of the defined objective.
Formative evaluation will be implemented to stimulate the progress of the participant using self,
pair and facilitator feedback.

Annex II – Pedagogical Contract
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 34
Participants’ assessment
The participants will be assessed, as in any PBL programme, utilising different assessment
tools:
Formal evaluation:
a. Individual written test: includes multiple choice, true/false questions aimed at assessing
knowledge and skills gained, as certifying assessment.
The suggested evaluation scale is as follow:
1= Unsatisfactory; 2= Below average; 3= Average; 4= Very good; 5=Excellent
The pass mark is 3.
b. Oral presentation skills assessment: short oral presentation on a topic relevant to the
objectives of the module. This is aimed at assessing presentation skills. Handouts will
be distributed in the framework of an ad-hoc seminar.
Formative Evaluation:
c. Weekly peer and facilitator feedback: aimed at monitoring group-work skills. Has a
formative purpose.
d. Final feedback by facilitator: aimed at assessing participant's ability to work effectively
in a group. It provides feedback on individual basis and has also formative purposes.
e. Peer evaluation: will be ensured asking to the participants, starting from the third week
to create an assessment grid to use during the problem-solving meeting.
f. Self-evaluation: will be ensured anonymously through the MCQ pre-post test.
Evaluation of programme.
The participant satisfaction will be assessed using a MCQ test.
It will be provided at the beginning and at the end of the course
The participant needs will be monitored through the facilitator commitment using for each unit a
questionnaire.
The questionnaire will cover the following areas:
– Extent of the learning objectives achieved
– Relevance of course contents with regard to planned learning objectives
– Quality of teaching methods
– Tutors’ professionalism, availability and courtesy
– Availability, quantity and quality of learning materials
– Time allocated for the different steps of PBL
– Ameliorative proposals

Annex III – Facilitator check list
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 35
Annex III – Facilitator check list
Material
Participant list
General objective list (course)
Specific objective list (for each module)
Learning material
Problems
Reading material
Participants guide
Facilitator guide
PBL methodology’s guidelines
Phase’s list
Questions to favourite the passage from a phase to the other one
Evaluation tools
Peer feedback format
Facilitator feedback format
Peer evaluation format

Annex IV – Coordinator check list
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 36
Annex IV – Coordinator check list
Material
Seminar presentation
Role playing guide
The Participant assessment guide (criteria assessment)
Facilitator criteria assessment
Evaluation tools
MCQ unit assessment
Participant presentation assessment criteria
MCQ pre-post test course and self evaluation

Annex V – SWOT Analysis
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 37
Annex V – SWOT Analysis
S W Relevance of HMCTC to current training
needs of health personnel in South Sudan.
Curricula designed on the basis of local
situation.
PBL as an interactive and participatory
training methodology of continuing education.
Intensive nature of programmed training.
Long-lasting lack of exposure of health
personnel to continuing education and
professional upgrading initiatives.
Limited awareness of the importance of HSM
and its use by potential participants to
HMCTC.
Limited knowledge of managerial language
and terminology by candidate participants to
HMCTC.
Limited time span to deepen management
concepts.
O T January 2005 peace agreement between
SPLM/A and the Government of Khartoum;
SPLM/A’s concern in fostering strategic
development initiatives aimed at political and
socio-economic recovery of South Sudan;
Continuing institutional interest in the
reconstruction of the heath care system and in
the development of quality health care
services in South Sudan;
Provision of healthcare services and training
by NGOs;
Perceived need of intensive training and
professional qualification of existing health
personnel;
Logistics
Post-conflict environment.
Overall poor extent of awareness of health
personnel responsibilities.
Potential political aspects linked to managing
human resources (i.e.: potential difficulties in
reintegrating health workers from different
political factions, tribes or sects)
Low level of coordination between County
and MOH.

Annex VI – Training Costs
HEALTH MANAGEMENT CRASH TRAINING COURSE - HMCTC (DRAFT CURRICULA) 38
Annex VI – Training Costs.
The cost of one-week training per participant, calculated in US$, is, distributed as follows:
ITEM COST (US$)
Tuition
(Registration, tutorials, access to the library and computers, stationary)
Welfare
(Full board accommodation)
The cost of the HMCTC programme (5 weeks) per participant, calculated in US$, is, distributed
as follows:
ITEM COST (US$)
Tuition
(Registration, tutorials, access to the library and computers, stationary)
Welfare
(Full board accommodation)
Travel
(Displacement cost)