current practices and future vision on metabolite ... · on metabolite profiling and quantification...
TRANSCRIPT

Current practices and future vision on metabolite profiling and
quantification in GSK
Graeme Young – September EBF Workshop, Brussels 2015
Property of GlaxoSmithKline

Overview
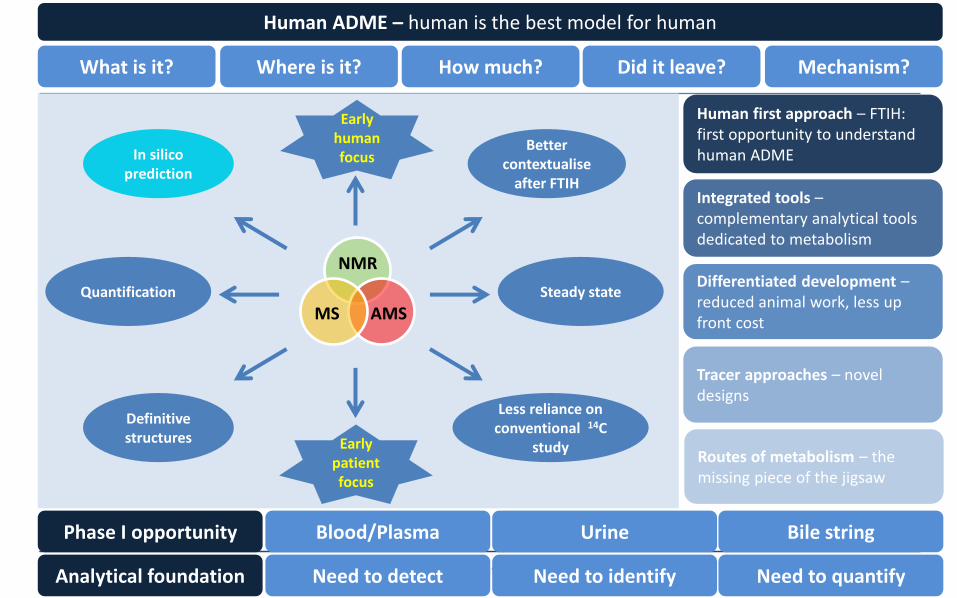
• GSK strategy – Human First ! [“Human is the best model for human”]
• Cold metabolism – the “free data” concept
• Cold metabolism + 14C tracer
• Specific assays……absolute quantification with authentic standards
• Long winded approach – use of 14C for multiple species metabolite profiling
• Future vision
Presentation title 3
Steady state Quantification
Definitive structures
In silico prediction
Better contextualise
after FTIH
Mechanism? Did it leave? How much? Where is it? What is it?
Early human focus
Human ADME – human is the best model for human
NMR
AMS MS
Tracer approaches – novel designs
Human first approach – FTIH: first opportunity to understand human ADME
Differentiated development – reduced animal work, less up front cost
Integrated tools – complementary analytical tools dedicated to metabolism
Bile string Urine Blood/Plasma Phase I opportunity
Less reliance on conventional 14C
study Routes of metabolism – the missing piece of the jigsaw
Need to quantify Need to identify Need to detect Analytical foundation
Early patient focus

Problems with historical approach
in silico Too many options; how
predictable for human
especially circulation
in vitro “artificial” system;
good for routes
~70% predictable
Not routinely used to select
toxicology species
Pre-clinical in vivo
Resource intensive
ID, quant. on non-human mets.
What are likely to be relevant?
Conventional Human Radiolabel Study
HRS Circulating metabolites
Routes of excretion
% urine % faeces
complex ethics Phase 2b/3
Body Burden %dose/metabolite & % unextracted
Single dose Human dose

What can we do in humans earlier? – the “free data” concept
Human Non-radiolabel Circulating metabolites
Routes of excretion
% urine
Single & Repeat dose
Faeces!
duodenal Bile*
*Entero-Test® ; GSK has used this approach in > 12 clinical studies (most in early clinical)
Guiney WJ, Beaumont C, Thomas SR, Robertson DC, McHugh SM, Koch A, Richards D. Use of Entero-Test, a simple approach for non-invasive clinical evaluation of the biliary disposition of drugs. Br J Clin Pharmacol 2011; 72: 133-42.

Cold metabolism….”free data”

NMR based cold metabolism approach
DRUG
30
PLASMA
70
Re
spo
nse
HPLC fractionation
Pool or bulk sample
Concentrate/extract sample
NMR NMR of fractions
% Quantify
Time
MET. M1
Dear GJ, Roberts AD, Beaumont C, North SE. Evaluation of preparative high performance liquid chromatography and cryoprobe-nuclear magnetic resonance spectroscopy for the early quantitative estimation of drug metabolites in human plasma. J. Chromatogr. B 2008; 876: 182–90.

Cold metabolism : healthy subject example
Glucuronidation is major route of elimination
• Contribution of oxidative metabolism (CYP3A4) unclear from in vitro data
• Human bile was analysed in early clinical development (non-invasive bile string)
• The primary pathway of metabolism was identified as O-glucuronidation
• Data used to inform on DDI risk strategy
Bloomer JC, Nash M, Webb A, Miller BE, Lazaar AL, Beaumont C, Guiney WJ. Assessment of potential drug interactions by characterization of human drug metabolism pathways using non-invasive bile sampling. Br J Clin Pharmacol 2013; 75: 488–96.

Cold metabolism example : patient focussed
• Sitamaquine is an orally active 8-aminoquinoline - shown potential for treatment
of Visceral leishmaniasis (VL) in Africa and India
• Despite potential for sitamaquine in treating VL, notable toxicity has been demonstrated in non-clinical species and clinically relevant exposure is only achieved in one species (the rat)
N
NH
O
N

• Animal welfare/ethical issues preclude further animal studies with sitamaquine
and development has been via carefully conducted clinical studies in patients with
VL, with intensive safety monitoring
• Also precludes a Human Radiolabel Study (HRS) in healthy volunteers
• In vivo human metabolism data generated via cold metabolism approach
urine and plasma examined by NMR and MS to determine the nature and
amounts of metabolite
Cold metabolism example : patient focussed

Minimum Body Burden
Major circulating
Major metabolic route
Renal Clearance
Cold metabolism example : Sitamaquine – Patient focussed

Cold metabolism + 14C tracer

Cold metabolism + 14C tracer
• Design using tracers of 13C- or 14C-labelled drug
tracer choice dictated by assay sensitivity and study endpoints IV 13C- or 14C-tracer dosed concomittant to Oral therapeutic dose
• Repeat dose 14C study designs are now feasible
often low ionising radiation exposure; <1µCi dose
• IV microtracer study design* adopted by many Pharma supplementary benefit of 14C over the “cold metabolism” approach provides the “what is it?” and the “how much?” providing valuable PK/ADME information particularly for early stage assets
* Approaches to intravenous clinical pharmacokinetics: Recent developments with isotopic microtracers, Lappin G., The Journal of Clinical Pharmacology 2015, on-line advance version, 1–13.

Cold metabolism + 14C tracer: example
0
200
400
600
800
1000
1200
1400
1600
1800
2000
2200
2400
2600
2800
3000
3200
0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75
Time after oral dose (hours)
Me
an
Co
nce
ntr
atio
n o
f SR
T2
10
4 in
Pla
sma
(n
g/m
L)
Oral (dose of 250mg)
IV data from 14C tracer of 100ug
(Normalised to 250mg)
Provided by AMS (parent isolation by UPLC)
Provided by LC/MS
0.00
0.02
0.04
0.06
0.08
0.10
0.12
0 5 10 15 20 25 30 35 40
Time (min.)
dpm
/200
uL H
PLC
Fra
ctio
n
Parent; drug
M17
M16
M21,M22
M27
M26
M19 M18
M8
F%
Human PK
Metabolism
• combining MS, NMR, AMS

Cold metabolism + 14C tracer - Metabolism
• Data from metabolic profiling “informs” for further development strategies
– provide useful data for safety assessment and clinical study designs
assessment of total observed drug related material in urine from PO therapeutic route dose (NMR)
• Each technology (AMS, LC/MS & NMR ) provides different insights
14C use allows assessment of eg. extraction recoveries
more comprehensive comparison of metabolism in animals and human
definition of full structural ID and amounts
specific assay for isolated metabolite (by “LC+AMS”) also possible

Synthetic standards – specific assays

Frequency of occurrence……quantitative metabolite assays (within bioanalytical group)
• Proportion of [in-house] clinical assays which included metabolites
In 2015 (Jan to August) it was ~5%
Interestingly - in 2008 (Jan to August ) it was ~15% [larger data set than 2015]
on the decrease? ; pragmatism on the rise?
possible impact of “differential development” ?
Specific assays by LC/MS

The longwinded approach….

The longwinded approach….
• Human ADME support produced evidence of two “major” metabolites – known instability issue - dilute and shoot approach and AMS applied
0
0.1
0.2
0.3
0.4
0.5
0 10 20 30
dp
m
Time (mins)
.
Parent
M2/others
M4
M2/others ~8% M4 = 11%
Human ADME data Plasma Pool
0
0.1
0.2
0 20 40 60
dp
m
Time (mins)
.
M2
M2 resolved and no longer considered a major metabolite.
Human ADME data Plasma Pool
• Synthesis of metabolite standards not viable

0
0.1
0.2
0.3
0.4
0.5
0 10 20 30
dp
m
Time (mins)
.
Parent
M2/others
M4
M2/others ~8% M4 = 11%
Human ADME data Plasma Pool
0
0.1
0.2
0 20 40 60
dp
m
Time (mins)
.
M2
M2 resolved and no longer considered a major metabolite.
Human ADME data Plasma Pool
Elapsed Time > 1 Year
The longwinded approach….
• Follow-on dosing of 14C-drug to rodent and non-rodent
• Cover estimates made based on quantification via profiling

Future Vision
• Drug to target – human tissue sampling
leaning towards imaging for more intact tissue assessment
moving from qualitative to more quantitative [mimetic model approach]*
• Increased use of microtracer approaches ; combined power of AMS, MS, NMR
access to key matrix – bile sampling [particularly useful with IV admin.]
• Greater focus on patients rather than healthy subjects…….
Future vision….
* A Mimetic Tissue Model for the Quantification of Drug Distributions by MALDI Imaging Mass Spectrometry, Groseclose M.R. and Castellino S., Anal.Chem., 2013 , 85 (21):10099-106.

GSK Clinical studies (incl. patients) – drug to site of action/tissue of interest
Skin cores…. healthy skin and lesions
Important Note – even when we have shown that drug appears to be close to the target site or site of toxicity (real or inferred) ; has not necessarily lead to efficacy or provided clear link to toxicity …but at least one step (maybe several) closer to supporting the “pillars of success” than eg. analysis of drug in blood plasma……
* Hair sampling…
drug therapy
adherence
monitoring?
Urine bladder…..
Dermal
distbn. of
Drug XX
*Brain tumour sampling…
Cancer drug to
target tissue
*Lung lavage…
Pulmonary PK of
drug and active
metabolite(s)
Lung lavage…
Seminal fluid analysis…
* Potential/planned
Drug Z risk
assessment
Colon and rectum analysis..
Drug X to target
tissue
Skeletal muscle analysis…
Drug Y to target
tissue
*Polydendritic cells…
Delivery to
target cells in
systemic
Pulmonary PK for IV
antibiotic & multiple
inhaled cpds.
Cerebrospinal fluid5…
Fosdevirine safety
“investigation”
5. Central nervous system distribution and metabolism of fosdevirine (GSK2248761), a non-nucleoside reverse transcriptase inhibitor : an LC-MS and matrix-assisted laser desorption/ionization imaging MS investigation into central nervous system toxicity, Catellino S. et al., Chem. Res. Toxicol., 2013, 26, 241-251.
6. Safety, Pharmacokinetic, and Functional Effects of the Nogo-A Monoclonal Antibody in Amyotrophic Lateral Sclerosis: A Randomized, First-In-Human Clinical Trial, Meininger V et al., www.plosone.org, 2014, 9(5).
Skeletal muscle6 analysis…
Ozanezumab to
target tissue
safety
“investigation”

Summary • Human in vivo data as first intent – metabolism in animals later
• What is the metabolite structure and how much ?
access to human bile and urine
circulating metabolites are only one part of the story [assessing body/tissue burden]
mechanism of metabolite formation is important
IV µtracer design with ADME endpoints provides opportunities for early human IV PK and Abs. Bio. + Met ID/Quant
Drug to target – human tissue sampling
Greater focus on patients rather than healthy subjects…….
Summary

Acknowledgements • GSK DMPK colleagues present and past including -
Stephanie North, Gordon Dear, Andy Roberts, Claire Beaumont, Billy Guiney,
Steve Thomas, Steve Castellino, David Wagner, Jill Pirhalla, Ernie Schubert, Igor
Goljer, Steve Corless, Clive Felgate, Adrian Pereira, Mike Tucker
• Xceleron (AMS CRO), Vitalea Science (AMS CRO), PRA, SIMBEC, Quotient and Comprehensive Development for support of the IV µtracer studies • The patients and healthy volunteer subjects who participated in the clinical studies*
* The human biological samples were sourced ethically and their research use was in accord with the terms of the informed consents


Back-ups

1.52.02.53.03.54.04.55.05.56.06.57.07.58.08.5 ppm
Metabolite signal masked by noise
0.00 2.50 5.00 7.50 10.00 12.50 15.00 17.50 20.00 22.50 25.00 27.50 30.00 32.50 35.00 37.50 40.00 42.50Time1
100
%
0
100
%
14.61
12.55
13.40
16.17
12.5311.19
10.79
10.28
9.69
7.274.173.84 8.55
12.70
12.94
13.14
600/700 NMR - cryoprobes
UPLC/MS Mass defect filtering
NMR Approach Oral dose > 50 mg
~ 5 μg drug in plasma pool
Mass Spectrometry Approach Oral dose 1-50 mg

Technology improvements - Entero-Test ®
• FTIH metabolism focus Provides steady state systemic metabolites
Urinary metabolites
Biliary excretion is often a major route of elimination
Not easy to get bile out of humans
• Entero-Test® (absorbent string) provides easy non-invasive mechanism to collect human bile (used on several FTIH studies); ~ 1mL sampled
• Bile ; extremely dirty matrix – reliant on technology platforms to maximise data value

Assess data from SD human plasma
Are there any metabolites >5% oDRM*
Assess data from residual rodent TK plasma
Are human metabolites of concern present?
Plan RD rodent study to coincide with RD human
(if insufficient TK plasma available )
Assess data from residual norodent TK plasma
Are human metabolites of concern present?
Consider options for RD non-rodent study to
coincide with RD human (if insufficient TK plasma
available )
Await RD human data
Alternative options may be considered
Await RD human data
No concerns at this time
YES
NO
YES
YES
NO
NO
Step 1: LC/MS of residual rodent & non-rodent TK plasma (no data processing)
Step 2: Quantitative & qualitative assessment of SD human plasma
Assess data from RD human plasma
Are there any metabolites >5% oDRM*
Assess data from residual rodent & non-rodent TK
plasma
Are human metabolites of concern present ?
Generate & use appropriate non-clinical plasma to
assess exposure multiples with human
(LC/MS peak area ratios)
Discuss alternative options with SA
eg. alternative non-clinical species; dosing of
metabolite No further action required
at this stage
YES
NO
YES#
NO
Step 3: Quantitative & qualitative assessment of RD Human Plasma
* Or metabolites of safety concern based on chemical structure
If insufficient cover
#Stability of metabolites assessed first if residual TK plasma to be used

Additional References
• The use of isotopes in the determination of absolute bioavailability of drugs in humans, Lappin G., Rowland M., and Garner R.C., Expert Opin. Drug Metab. Toxicol., 2006, 2(3), 419-426
[Provides a good comparison of the pros and cons to use of stable label versus radioisotopes for absolute bioavailability studies]
• Accelerator MS: its role as a frontline bioanalytical technique, Seymour M., Bioanalysis, 2011, 3(24), 2817-2823. [Mentions use of IV tracer following repeated oral administration to provide kinetics at steady state, and clearly outlines the advantages
of concomitant dosing versus the traditional cross-over design]
• When opportunity met aspirational goals: accelerator MS, microdosing and absolute bioavailability studies , Arnold ME and LaCreta
F., Bioanalysis, 2012, 4(15), 1831-1834. [Acknowledges “renewed requirement” for defining absolute bioavailability in humans and provides support for the technology that now makes this more facile for many molecules]
• Microdosing: A Critical Assessment of Human Data, Rowland M., J. Pharm. Sci., 2012, Published online in WileyOnline Library
(wileyonlinelibrary.com). DOI 10.1002/jps.23290. [Recent position piece on the general microdosing approach , including concomitant dosing by PO and IV routes]
• Human ADME Properties of Drug Molecules: a Plethora of Approaches, Beaumont C., Young GC, Cavalier T. and Young M, Br. J.Clin.
Pharmacol., 78:6, 1185-1200. [Variety of cold, tracer and alternative approaches discussed]

‘Human first’ strategy to assess victim DDI risk
Acknowledgements: Aarti Patel and Claire Beaumont

Determining Absolute Bioavailability (F%) in Humans
Variable PK in human?
Early assessment of F%
- permeability limited?
- first pass metabolism?
F> 20 (?)%
Yes
No Yes
Consider
Termination of
Development #
Consider addition of
other ADME endpoints
No
High % (>85%ǂ)
of parent drug
excreted
unchanged in
human urine?
No Yes
Conduct Abs. Bio.
study prior to
submission of
regulatory file?
Investigative Regulatory Requirement
Defer to later stage of
development
(prior to submission)
Develop
recommendation for
waiver of Abs. Bio.
study ? High clearance
(>70% LBF)?
No further
formulation effort Worth pursuing formulation development to decrease
variability
- address solubility and dissolution rate issues
- reduce dose burden; cost of goods improvement
No Yes
# Unless drug targetted to have low bioavailability eg. local action in GI tract, or pro-drug ǂ Per FDA BCS guidance draft 2015

Pooling
• Urine
– Equal volumes from all subjects (0-24h) combined to generate a 500 mL pool
• Plasma
– Combined across subjects and time points in a time adjusted manner to create a sample representative of the AUC 0-24h (70 mL)
NMR
Time
Resp
on
se
30 METABOLITE
70 DRUG
% PLASMA/ URINE
(1) Pooling
(2) Extraction
(3) Fractionation
(4) Identification
(5) Quantification
UPLC MS

Extraction
• Urine
– 500 mL lyophilised
– Reconstituted in 50 mL of 10% aqueous methanol
• Plasma
– Protein precipitated with acetonitrile. Supernatants combined, dried under N2 and reconstituted in 50 mL of 10% aqueous methanol
NMR
Time
Resp
on
se
30 METABOLITE
70 DRUG
% PLASMA/ URINE
(1) Pooling
(2) Extraction
(3) Fractionation
(4) Identification
(5) Quantification
UPLC MS

HPLC
• HPLC scaled from analytical where possible
• Typically 10 mm – 21.2mm i.d. columns
• Column eluent is fractionated at 15 s intervals to give a reasonable compromise between maintaining chromatographic resolution and limiting fraction numbers
• On-line MS to aid structural elucidation
NMR
Time
Resp
on
se
30 METABOLITE
70 DRUG
% PLASMA/ URINE
(1) Pooling
(2) Extraction
(3) Fractionation
(4) Identification
(5) Quantification
UPLC MS

NMR
• HPLC fraction are dried and reconstituted or analysed directly if using D2O mobile phase
• 10 - 100 μg of metabolite may be isolated from urine allowing for the usual selection of NMR experiments to determine structure
• Metabolites isolated from plasma are typically lower (<10μg) NMR will be limited to 1D proton only
• To reach acceptable detection limits in plasma cryoprobes are essential
NMR
Time
Resp
on
se
30 METABOLITE
70 DRUG
% PLASMA/ URINE
(1) Pooling
(2) Extraction
(3) Fractionation
(4) Identification
(5) Quantification
UPLC MS