current evidence in ablative therapy for hepatocellular carcinoma joint hospital surgical grand...
TRANSCRIPT

Current Evidence in Ablative Therapy for Hepatocellular Carcinoma
Joint Hospital Surgical Grand Round
Dr Chu Ka Wan
Queen Mary Hospital

• 70% presented as unresectable hepatocellular carcinoma (HCC)– Inadequate liver function– Multifocal HCC– Proximity to major vessels
• 5-year recurrence rate > 50% after “curative” hepatectomy
Grazi GL et al. Aliment Pharmacol Ther 2003
Inoue K et al. Liver Transpl 2004
Llovet JM et al. Lancet 2003

HIFU

Local Ablative Therapy for Hepatocellular Carcinoma
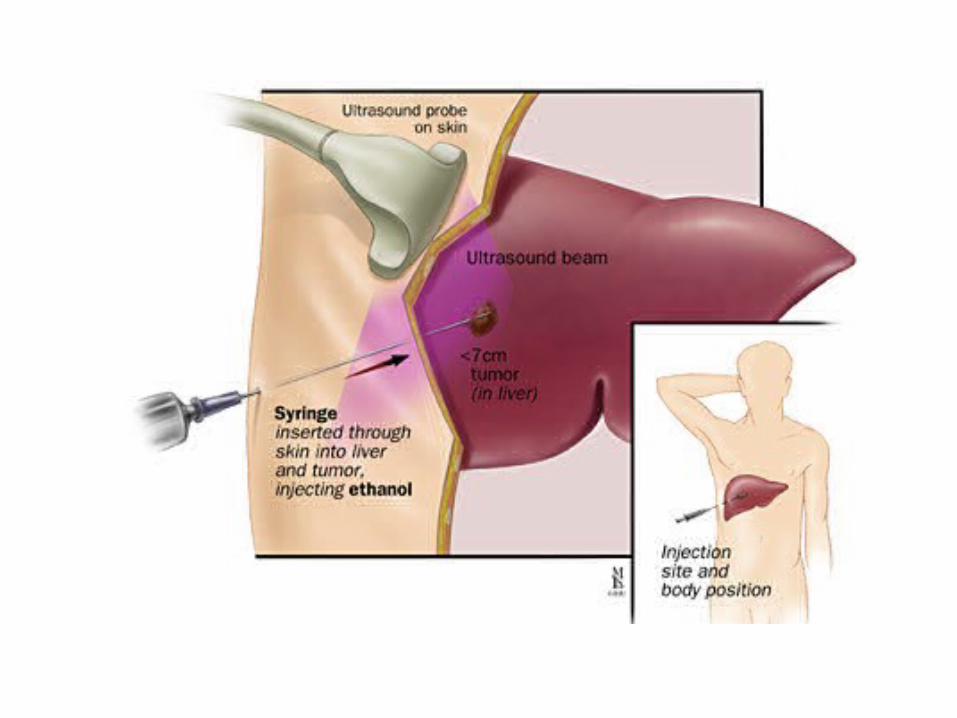
• Percutaneous ethanol injection (PEI)
• Cryoablation
• Microwave coagulation therapy
• Radio-frequency ablation (RFA)
• High-intensity Focused Ultrasound Ablation (HIFU)
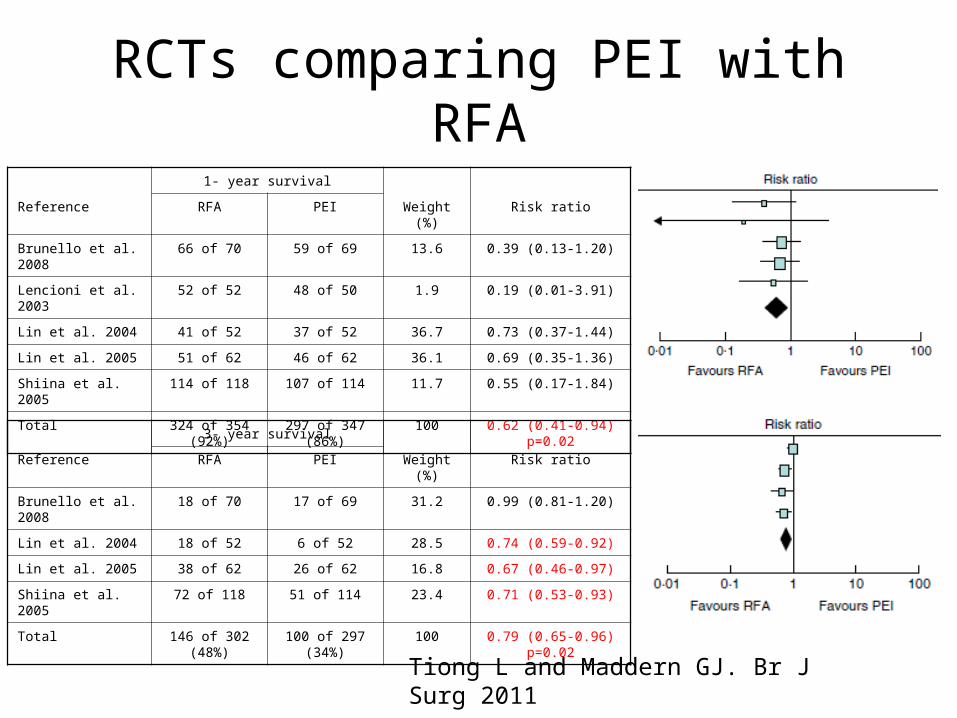
1- year survival
Reference RFA PEI Weight (%) Risk ratio
Brunello et al. 2008 66 of 70 59 of 69 13.6 0.39 (0.13-1.20)
Lencioni et al. 2003 52 of 52 48 of 50 1.9 0.19 (0.01-3.91)
Lin et al. 2004 41 of 52 37 of 52 36.7 0.73 (0.37-1.44)
Lin et al. 2005 51 of 62 46 of 62 36.1 0.69 (0.35-1.36)
Shiina et al. 2005 114 of 118 107 of 114 11.7 0.55 (0.17-1.84)
Total 324 of 354 (92%)
297 of 347 (86%)
100 0.62 (0.41-0.94) p=0.02
3- year survival
Reference RFA PEI Weight (%) Risk ratio
Brunello et al. 2008 18 of 70 17 of 69 31.2 0.99 (0.81-1.20)
Lin et al. 2004 18 of 52 6 of 52 28.5 0.74 (0.59-0.92)
Lin et al. 2005 38 of 62 26 of 62 16.8 0.67 (0.46-0.97)
Shiina et al. 2005 72 of 118 51 of 114 23.4 0.71 (0.53-0.93)
Total 146 of 302 (48%)
100 of 297 (34%)
100 0.79 (0.65-0.96) p=0.02
Tiong L and Maddern GJ. Br J Surg 2011
RCTs comparing PEI with RFA
• RCTs comparing PEI and RFA:– More local tumour recurrence– More treatment sessions required
• Allowing treatment of tumours near sensitive organs
• No “heat-sink” effect adjacent to vessels
• Applicability is limited
• Inferior compared with RFA


Cohorts comparing cryoablation with RFA
• Prosepctive cohort• Study period 1992-1998• Mean follow-up 15 months• HCC and metastatic
tumours (41:105)• Laparotomy with intra-
operative ultrasound
• Tumour recurrence:– 3 of 138 in RFA– 12 of 88 in cryoablation
Cryoablation RFA P
Number of patients (tumour nodules)
54 (88) 92 (138)
Local recurrence 13.6% 2.2% 0.01
Complications
Haemorrhage
Perihepatic abscess
Intrahepatic abscess
Renal insufficiency
Symptomatic pleural effusion
Pneumothorax / injured diaphragm
27 (40.7%)
2 (3.7%)
2 (3.7%)
10 (18.5%)
2 (3.7%)
8 (14.8%)
2 (3.7%)
3 (3.3%)
1 (1.2%)
2 (2.4%)
0
0
0
0
<0.001
Death 1 0
Pearson AS et al. Am J Surg. 1999
• High complication rate reported by multiple studies– Higher haemorrhagic complication
• Ablation zone of probes is generally smaller than RFA
• The zone of complete lethality lies a variable distance inside the edge of the ice ball
• Being questioned for its use in HCCPearson AS et al. Am J Surg. 1999
Xu KC et al. World J Gastroenterol 2009
Adam R et al. Arch Surg 2002
• Antenna• 60W, 915MHz generator• Fiber optic temperature monitor
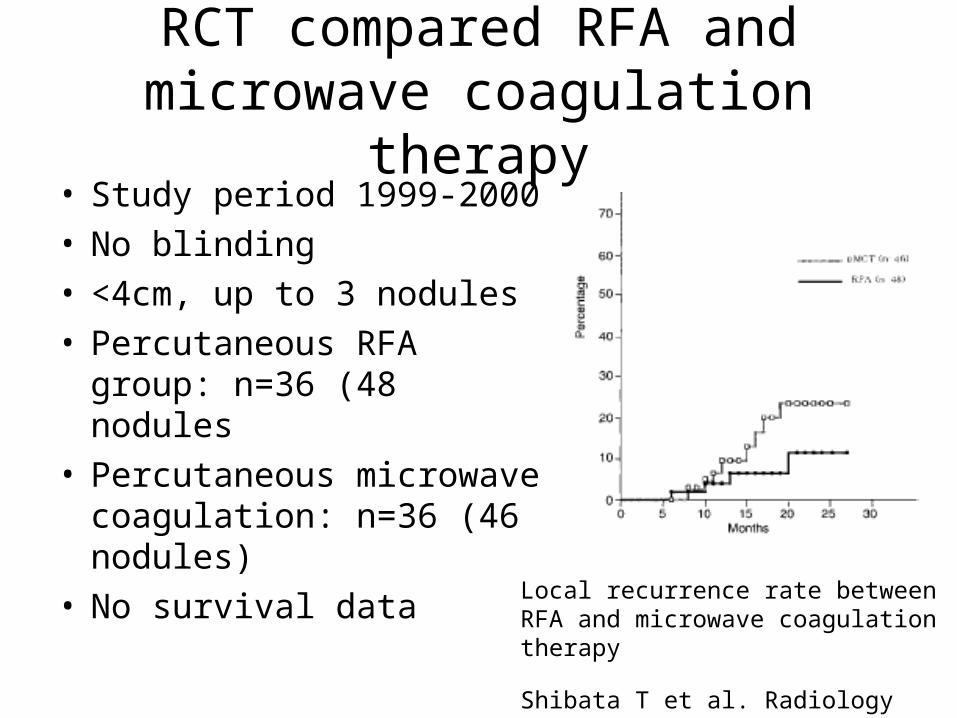
RCT compared RFA and microwave coagulation therapy
• Study period 1999-2000• No blinding• <4cm, up to 3 nodules• Percutaneous RFA group:
n=36 (48 nodules• Percutaneous microwave
coagulation: n=36 (46 nodules)
• No survival data
Shibata T et al. Radiology 2002
Local recurrence rate between RFA and microwave coagulation therapy
• Higher temperature in shorter treatment time
• Less affected by heat-sink effect
• Ground pads are not required
• Unmatched series reported inferior survival compared with RFA
• Complication rate similar as RFA
Ohmoto K et al. J Gastroenterol Hepatol 2009

Radiofrequency ablation
• Alternating electrical current• Frequency 200k-20M Hz in the range of
radio-waves• Electric power 10 W to 200 W• Circuit completed with grounding pads• Agitation of ionic dipolar molecules
producing frictional heating• Coagulative necrosis and tissue
desiccation
Strasberg S et al. Curr Probl Surg 2003

RFA vs resection for small HCC
RCT compared RFA with hepatectomy (Guangzhou)
• RCT (blinding not possible)
• Study period 1999-2004
• Solitary HCC < 5cm
• Percutaneous RFA n=71 (per-protocol)
• Hepatectomy n=88
• Both intention-to-treat and per-protocol analysis
Chen MS et al. Ann Surg 2006

Overall and disease-free survivals with percutaneous RFA and hepatectomy for HCC<3cm (p>0.05)
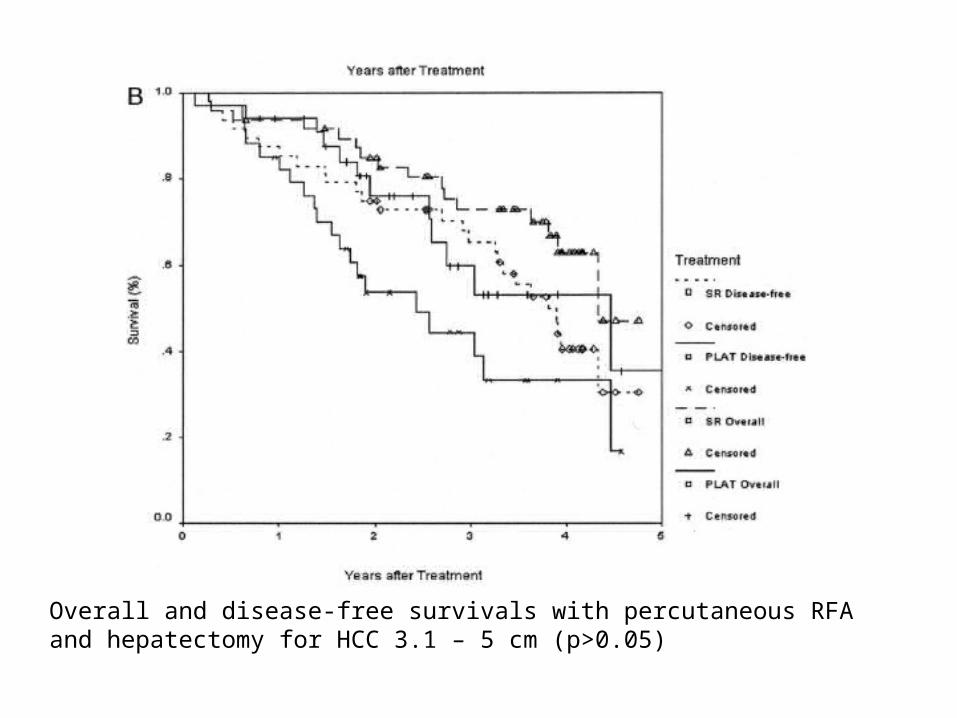
Overall and disease-free survivals with percutaneous RFA and hepatectomy for HCC 3.1 – 5 cm (p>0.05)

RCT compared RFA with hepatectomy (Chengdu)
• RCT
• Study period 2003-2005
• Solitary HCC<5cm / up to 3 nodules, each <3cm
• Percutaneous RFA n=115
• Hepatectomy n=115
• Intention to treat analysis
Huang J et al. Ann Surg 2010

Overall survivals with percutaneous RFA and hepatectomy for HCC conforming to Milan Criteria (p=0.001)

Overall survivals with percutaneous RFA and hepatectomy for HCC ≤ 3cm (p=0.03)
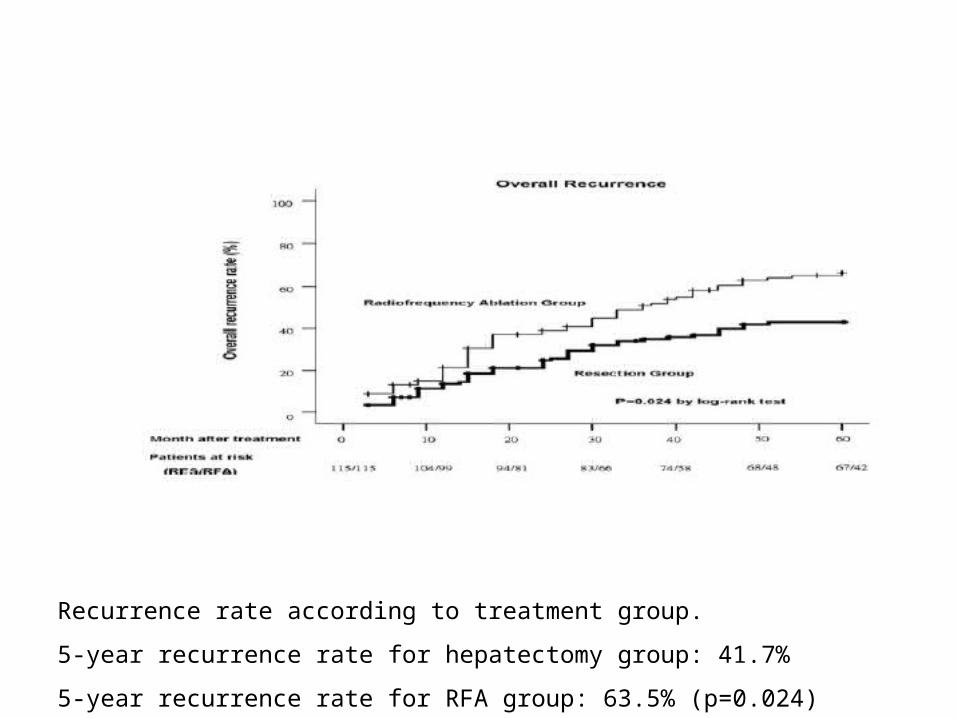
Recurrence rate according to treatment group.
5-year recurrence rate for hepatectomy group: 41.7%
5-year recurrence rate for RFA group: 63.5% (p=0.024)
RFA vs resection for recurrent HCC
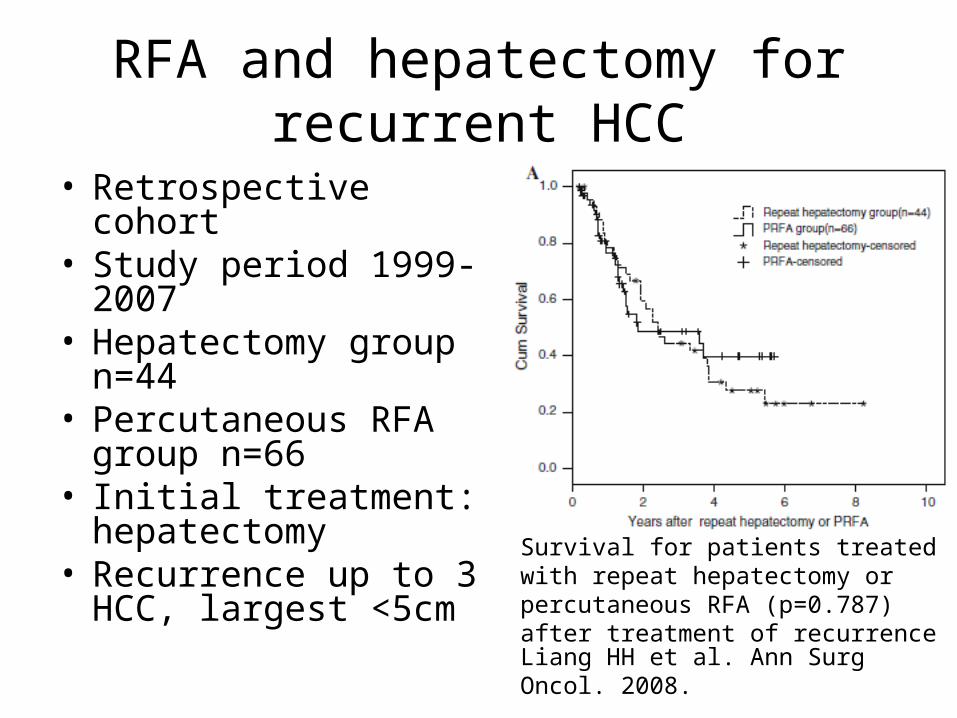
RFA and hepatectomy for recurrent HCC
• Retrospective cohort• Study period 1999-
2007• Hepatectomy group
n=44• Percutaneous RFA
group n=66• Initial treatment:
hepatectomy• Recurrence up to 3
HCC, largest <5cm
Liang HH et al. Ann Surg Oncol. 2008.
Survival for patients treated with repeat hepatectomy or percutaneous RFA (p=0.787) after treatment of recurrence

• Retrospective cohort• Study period 2001-
2008• Hepatectomy group
n=29• RFA group n=45
(open n=23, percutaneous n=22)
• Size up to 6cm
Chan AC et al. World J Surg. 2012.
Survival for patients treated with repeat hepatectomy or percutaneous RFA (p non-significant) after treatment of recurrence
RFA and hepatectomy for recurrent HCC

HIFU
No heat sink effect
HIFU
• Unresectable HCC
• Primary or recurrent
• <10cm
• No extrahepatic metastasis
• Fit general anaesthesia

• Prospective controlled trial
• Unresectable HCC• Alternately enrolled into
2 treatment group• Study period 1998-2000• Mean tumour size 4-
14cm, number 1-4• TACE group: n=26• TACE + HIFU: n=24
TACE + HIFU
TACE
Survival of patient treated with TACE alone and TACE + HIFU, p=0.007
Wu F et al. Radiology 2005
Summary
• A meta-analysis of 5 RCTs indicated RFA was better than PEI
• Cryoablation causes more complication than RFA
• Comparison between RFA and microwave coagulation therapy was inconclusive
• HIFU as a non-invasive tool with limited evidence

Summary (RFA)
Indication Current evidence
Unresectable HCC RFA-TACE was found to be superior to TACE alone
Resectable HCC Still considered inferior to hepatectomy
Recurrence HCC Comparable to hepatectomy (retrospective cohort)
Ruptured HCC
Cheng BQ et al. JAMA 2008
Manikam J et al. Hepatogastroenterology 2009
