cu - ucm-biblioteca complutensebiblioteca.ucm.es/intranet/doc20127.pdf · cu second quarter, 2012...
TRANSCRIPT

Cu
SECOND Quarter, 2012
VOLUME 27 NUMBER 2
Summer
birroculus
Paul E. Romano, MD, MSO Founder
Founding Editor Editor-in-Chief
StrabOL cv CUarterb; Simms-romano' s
The First and Original Scientific e-Periodical Devoted to Binocular Vision and Strabismus
*Scientists for the Abrogation of -Statistical Significance = v.05"
MIMS III: REPORT: Strabology and COMMENT on the 38 th Meeting of the American Association for Pediatric
Ophthalmology & Strabismus, San Antonio, Texas 2012
*** ORIGINAL EVIDENCE-BASED SCIENTIFIC ARTICLES ***
KHAN: An Analysis of 5 Duane's Retraction Syndrome Patients with Preoperative Abnormal Face Turn Reversal and/or Worsening after Standard Horizontal Eye Muscle Surgery
LARIA, SHOKIDA, TATARCHUCK, PINERO and X. GONZALEZ: New Diplopic Restrictive Strabismus as a Sequela after Conjunctival Surgery for Conjunctival Lesions: A Series of 3 Cases, Management and Outcome
ARNOLD RW, ARNOLD AW, EBY and ALESHIRE: Lay Person Slit Lamp Detection of Iritis in Absence of an Eye 1111.D.: Test of a Portablo Model of Cells and Flare
*** CASE REPORT With Management and Outcome***
DAGHERI, TAVAKOLI and RAFAATI: Diplopic Mechanical Restrictive Strabismus due to Orbital Wall Fracture and Medial Rectus Muscle Entrapment After Endoscopic Dacryocystorhinostomy, with Optic Nerve Deficit
LEAD EDITORIAL: Restrictive (Mechanical) Strabismus: An Epidemic? DNA or Not; Twins Faces, Texas, DRS, lritis
HYDE PARK EDITORIAL: Conscience and Consciousness
CITED IN INDEX MEDICUS
CITED ONLINE
I in EM BASE CITED ONLINE' CITED IN
I in M E D L I N E 'INDEX BINDCULUS

An extensive source of products for
Eye Care Professionals
Fun Designer Eye Patches • Call for Free Patient Samples • Non-toxic • Latex Free • Ilypo-Allergenic • Breathable • Awressiec Adhesive • Blackout layer provides for total
occlusion • Thinner occlusion is gentle
on eye lashes-
For more than 24 years the
Fresnel Prism and Lens Co. has
been offering products to assist
in the diagnostic and therapeutic
issues offered by eyecare specialists.
We are still a small personal office
and look forward to working with
you to ensure you receive just what
you need.
7-Ring Trial Set • Allow accurate testing of large
oculomotor imbalances • Fits all standard trial frames • Lightweight.- made of thin optical
quality acrylic Available as two sets providing a full range of prisms
• More accurate evaluation of large-angle deviations Indispenseable as a tool for the proper evaluation of ocular motility distturbances
• Each set includes a display box
3M Press-On Optics • Ultra-thin prisms and spheres -
measure only 1 mm thick • M:ty be CUE to fit most frame sizes
and shapes and adhere to misting lenses with only water
• Aspheric Lenses - plus and minus and as D-sctments
• Diplopia (3rd -4th and 6th nerve
palsies. following cataract surgery tnyasthenia gravis MS Graves Disease )
• Phorias (symptomatic or &compensated phorias)
CIE ERESNEL PRISM AND LENS CO.
Bangerter Occlusion Foils & Bars
1-800-544-4760 www. fresnel-prism.com [email protected]

Prisms in the Northern Lights
The Science of Orthoptics
• •
XI Ith International
Orthoptic Congress June 26-29 / 2012
Westin Harbour Castle
Toronto Ontario Canada
10A INTERNATIONAL
ORTHOPTIC
ASSOCIATION
www.torontoioacongress.org

BINOCULAR VISION & STRABOLOGY QUARTERLY, Simms-Romano’s: Print Version ISSN 2160-5351 (formerly 1088-6281)LIMITED PRINT version for libraries, since the 2007 addition of identical electronic Internet ONLINE version, ISSN 2160-5904,
The "loftiest scientific journal in the world" is published 9100 feet above sea level, in the Rocky Mountains, in the shadow ofthe American Continental D iv ide, Summit County, Colorado, by BINOCULUS PUBLISHING, PO Box 3727, 740 Piney AcresCircle, D illon, CO 80435-3727 USA; FAX 970-262-2768. Email: judyatbv@ vail.net. A Medical Scientific online E-Periodical(w ith continuation of lim ited print version for libraries.
W ebmaster: Ryan Soderberg, W ebez.net Internet Services, D illon, Colorado. Official publication date of this issue April 1,2012 D istribution date by June 30, 2011. This is a Simms-Romano Enterprise (Simms is the maiden name of the founder’smother, R .N., a Daughter of the American Revolution, (DAR), honored here as the laudable custom in many other worldcultures; his father was Battalion Surgeon for the 33 Infantry Division in World W ar II, serving from 1942-1945, in the Pacific;rd
scheduled to invade Japan, when Hiroshima saved his life and those of many other Americans and Japanese.).
COPYRIGHT 2012. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means,electronic or mechanical, including xerographic copy, photocopy, recording, or an information storage and retrieval system,without permission in writing from the publisher, except as specifically allowed by law (each paid subscriber may print one hardcopy of each issue, for personal use only, by simply executing the “print” command on their computer/printer).
EDITORIAL OFFICE / MANUSCRIPTS: Please send by email to the Editor, Binocular Vision & Strabology Quarterly, atperxbvq@ colorado.net, w ith a copy to judyatbv@ vail.net. Instructions for Authors may be found on the website(binocularvision.net) or by contacting judyatbv@ vail.net and a PDF will be sent to you. Letters to the Editor are considered "forpublication" unless otherw ise indicated and may be edited and condensed as space dictates.
ADVERTISING: Please direct inquiries to BINOCULUS PUBLISHING, PO Box 3727, 740 Piney Acres C ircle, D illon CO 80435-3727 USA. Tel & FAX 970-262-2768. Media kit and rates on request.
SUBSCRIPTIONS: For 2012 Please send orders w ith check or money order payable in US $ funds to Binoculus Publishing, POBox 3727, 740 Piney Acres C ircle, D illon CO 80435-3727 USA. Visa, Mastercard and American Express are accepted. Tosubscribe or order, Fax 970-262-2768. Email: Judy Robinson < judyatbv@ vail.net> O r order on the (secured) website at www.binocularvision.net (Personal, one year subscriptions only)
Individual: Per four issue online electronic annual volume only: $68 a year for a three year subscription (total $US 204=3x68),$78 a year for a two year subscription ($US 156 =2x78), $84 for a one year subscription. Special reduced ratesavailable for Certified Orthoptists, see International Orthoptic Association.com Rendered by quarterly email hot link.
Library/Institution: One year online electronic subscription $US 512, online electronic version only. For an additional secondsubscription in print, $US475 ....
Open online access store: binocularvision.net. Single Issues $US 47, individual articles $US 7-37
Back print issues (1985-2010) $US 36, if available only) Some past Bound Volumes are available thru’ 2005.
Disclaimer: The ideas/opinions expressed in Binocular Vision & Strabology Quarterly do not necessarily reflect those of thepublisher or editorial staff. BV&Sq makes every effort to maintain accuracy; however, cannot guarantee accuracy of contents.or claims of advertisers. Readers should consult the author or manufacturer before using any product appearing in BV&Sq.
The designation of individual issues is by the quarter, not the season, because seasons are never the same, but opposite, inthe Northern and Southern hemispheres. The seasons are however designated on the cover with the Northern season on thetop and, inverted below, the current season in the Southern hemisphere.
Binocular Vision & Strabology Quarterly Simms-Romano’s© E D IT O R IA L B O A R D SECOND Quarter of 2012, Volume 27 (No:2) Page 76
Leonard AptRobert W. ArnoldKyle ArnoldiE.S. Avetisov, RussiaJohn D. BakerP. Vital Berard, FranceFrank Billson, AustraliaMichael C. BrodskyJorge A. Caldeira, BrazilAlberto O. Ciancia, ArgentinaKenneth J. CiuffredaDavid K. CoatsJeffrey CooperJan-T.H.N. de Faber, NetherlandsJay M. EnochRobert W. EnzenauerCaleb GonzalezMichael H. Gräf, GermanyDavid GuytonEugene M. HelvestonRichard W. HertleCreig S. HoytRobert S. JampelEdward Khawam, Lebanon
Lionel Kowal, AustraliaStephen P. Kraft, CanadaMalcolm L. MazowHenry S. MetzJoel MillerJames L. Mims IIIScott E. OlitskyGian Paolo Paliaga, ItalyEvelyn A. PaysseJ.V. Plenty, United KingdomZane F. PollardJulio Prieto-Diaz, ArgentinaMichael X. RepkaJames D. ReynoldsDavid L. Romero-Apis, MexicoAlan B. ScottKurt SimonsAnnette Spielmann, FranceDavid R. Stager, Sr.Martin J. Steinbach, CanadaDavid S.I. Taylor, EnglandGuillermo Velez, ColombiaM. Edward Wilson, Jr.Kenneth W. Wright
EMERITUS
Shinobu Awaya, JapanHenderson Almeida, BrazilBruno Bagolini†, ItalyAlbert W. BiglanEileen BirchWilliam N. Clarke, CanadaJohn S. Crawford†, CanadaRobert A. Crone, NetherlandsEugene R. Folk†David A. HilesDavid HubelBela JuleszHerbert Kaufmann, GermanyPhilip Knapp†Burton J. KushnerJoseph Lang†, SwitzerlandJohn P. Lee†, EnglandPinhas Nemet, IsraelEdward L. RaabRobert D. ReineckeWilliam E. ScottR. Lawrence Tychsen
“... the belief that one’s view of reality is the only reality is the most dangerous of all delusions ...”-Watzlawick, 1976
ISSN 2160-5351 (Print)EDITOR ISSN 2160-5904 (Online) SECOND Quarter of 2012
Paul E. Romano, M.D., M.S.O TABLE OF CONTENTS Volume 27, Number 2
MEDLINE Abbr. Binocul Vis Strabolog Q Simms Romano NLM ID: 101556982
79 Correspondence; People & Places; News & Announcements
80 Editorial: Restrictive (Mechanical) Strabismus: An epidemic? DNA or Not, Twins Faces,
Texas, DRS, Iris Monitoring
88 Strabology Report and COMMENT on the 38th Annual Meeting of the AAPOS
James L. Mims III, M.D.
*** ORIGINAL “EVIDENCE-BASED” SCIENTIFIC ARTICLES ***
108 An Analysis of 5 Duane’s Retraction Syndrome Patients with Preoperative Abnormal FaceTurn Reversal and/or Worsening after Standard Horizontal Eye Muscle Surgery
Arif O. Khan, M.D.
113 New Diplopic Restrictive Strabismus as a Sequela After Conjunctival Surgery forConjunctival Lesions: A Series of 3 Cases, Management and Outcome.C. Laria, M.D., PhD, F. Shokida, M.D., MSc, P. Tatarchuck. M.D., D.P. Piñero, PhD and X. Gonzalez, M.D.
129 Lay Person Slit Lamp Detection of Iritis in Absence of an Eye M.D.: Test of a PortableModel of Cells and FlareRobert W. Arnold, M.D., Andrew W. Arnold, Eryn Eby and Jennifer Aleshire
*** CASE REPORT with Management, Outcome and Literature Review ***
122 Diplopic Mechanical Restrictive Strabismus due to Orbital Medial Wall Fracture andMedial Rectus Muscle Entrapment after Endoscopic Dacryocystorhinostomy, withOptic Nerve DeficitAbbas Bagheri, M.D., Mehdi Tavakoli, M.D. and Nasrin Rafaati, M.D.
135 Abstracts of the Current Literature
138 Hyde Park Editorial: CONSCIENCE and CONSCIOUSNESS: Close Words, but R#1 is StillStereo 3D BV via the Egocenter.....
Index of Advertisers: Fresnel Prism and Lens Co. Page 74International Orthoptic Association Page 75Richmond Products Page 77

Binocular Vision & Strabology People and Places, News and Announcements SECOND Quarter of 2012
Quarterly, Simms-Romano’s© Correspondence Volume 27 (No.2):
A Medical Scientific e-Periodical Page 79
-79-
Correspondence
RE: Mims III. HISTORY OF MEDICINE:Ocular Disorders of the Mona Lisa andOther Famous Paintings. BVSQ 2012;27(1):35-38
To: James L. Mims III, M.D.
From: Judy Robinson, CO
QUESTION: The other day I heard ona TV financial channel a person talking aboutbeing to the Louvre and how he had beenthere. He was taking some photographs andwas told, not so gently, to put his camera awayas picture taking was not allowed. When heasked why, the guard said it was disrespectfuland then followed him around to be sure hedidn’t take any more. Presuming you took thephotos in your report, we are even moreimpressed.
In Reply From: James L. Mims III, M.D.
To: Judy Robinson, CO
They didn’t bother me or mycompanion in the Louvre. We used smallcameras and no flash. We weren’t the onlyones taking photos. Yes, I took over 100photos of the paintings in the Louvre. Wewere nearly worshipfully respectful andmaybe the guards sensed that. Also, all artmuseums won’t allow photos in the touringshows. Maybe that was the problem for thisfellow you report.
Ed Note: We commented that the Mona Lisa’ssmile slightly suggested an ipsilateral 7th N.Palsy too.
B.J. Kushner reminded us in San Antoniothat’s a Moebius Syndrome... -per
Meeting Announcements
THIS Coming WEEK: Tuesday 26 June -Friday 29 June, 2012
Toronto, Ontario, Canada
Quadrenniel Meeting of the InternationalOrthoptic Association. SEE AD inside frontcover, on page 75
This FALL:
Milan, Italy September 7-9, 2012. 2nd WorldCongress of Paediatric Ophthalmology andStrabismus.
Contact: www.wcpos.org
Shanghai, China October 14-16, 2012. 3rd
I n t e r n a t i o n a l R O P C o n g r e s s .http://rop2012.org Contact: Lisa Erbring 215-590-4594 or Graham Quinn, Chairman of theScientific Committee
Contact Email: [email protected]
Chicago, Illinois November 9, 2012. Pre-AAO Pediatric Ophthalmology Day. Hostedby the Wright Foundation and the Universityof Illinois at Chicago. Hubel and Wiesel.Special lecture with question and answersession. Contact Stacy Lassman.
Contact Email: [email protected]
NEXT YEAR (2014):
Kyoto, Japan December 1-4, 2014. XIIthI n t e r n at i o n a l S t r a b i s m o l og i c a lAssociation. Quadrenniel Meeting. Hostedby the Japanese Association of Strabismus.Local Organizer: Miho Sato.
Contact www.isa2014.jp

Binocular Vision & Strabology Editorial: Restrictive (Mechanical) Strabismus: An Epidemic? SECOND Quarter of 2012Quarterly, Simms-Romano’s© DNA or Not, Twins Faces, Texas, DRS, Iritis Monitoring Volume 27 (No 2)A Medical Scientific Eye e-Periodical P. E. Romano, MD, MS Ophthalmology Pages 80-87
- 80 -
EDITORIAL: Restrictive (mechanical) Strabismus:an epidemic? DNA or Not, TWINS FACES, Texas,DRS, Iritis Monitoring
Reminder: It’s not too late to arrangeto go, next week, to the quadrenniel metingof the IOA in Toronto Canada (TuesdayJUNE 26 - Friday JUNE 29). See theadvertisement on page 75 inside the frontcover, website for more info.
Strabology: Restrictive (mechanical)Strabismus:
In the last three issues of thispublication, there has been almost anepidemic of reports of cases on this subject;primarily how to fix those very complex,severe and difficult cases - a total of 5 reportson a total of 22 plus cases!
1. Ahmed R, Coats DK, Yen MT. Periosteal flapfixation of the globe for surgical treatment of severerestrictive strabismus. A report of Eight Cases withoutcomes. Binocul Vis Strabolog Q Simms Romano2012;27: 230-235.
2. Bagheri A, Erfanian-Salim R, Salour H,Yazdani S. Globe fixation with homologous temporalisfascia transplant for treatment of restrictive esotropiastrabismus: An interventional case report and review of theliterature. Binocul Vis Strabology Q Simms Romano 2012;27: 236-242.
3. Akbari MR, Jafari AK, Ameri A, Anvari F,Eshraghi B, Masoomian B. Successful extraocular musclere-resection for a strabismus surgery complication: A“snapped” [severed, inadvertently] and retrieved inferiorrectus muscle; A case report. Binocul Vis Strabolog QSimms Romano 2012; 27:41-45.
4. Khawam E, Fahed D.. Review: Oculomotorcranial nerve palsies: Symptoms, problems and non-surgical preoperative management of the resultant
complex incomitant strabismus and monocular andbinocular vision disturbances. Binocul Vis Strabolog Q
Simms Romano 2012: 27:23-34.[Surgical considerationswill appear in a tandem review to be published in one ofthe next issues -ed]
5. Romano PE. Stage III IntraoperativeAdjustment (IOA) of eye muscle surgery (under generalanesthesia) for neuroparalytic and mechanical (restrictive)incomitant strabismus: Report of results in a series:Outcomes in 20 eye muscle surgeries in twelve patients..Binocul Vis Strabolog Q Simms Romano 2012; 27:46-50
6. Laria C, Shokida F, Tatarchuck P, Piñero DP,Gonzalez X. New diplopic restrictive strabismus as asequela after conjunctival surgery for conjunctival lesions:A series of 3 cases, management and outcome. Binocul VisStrabolog Q Simms Romano 2012; 27:113-121.
7. Bagheri A, Tavakoli M, Rafaati N. Diplopicmechanical restrictive strabismus due to orbital medialwall fracture and medial rectus muscle entrapment afterendoscopic dacryocystorhinostomy, with optic nervedeficit. Binocul Vis Strabolog Q Simms Romano 2012:27:122-128.
After we had received the first four ofthem, it did make me go back and look at myprior work on the subject that nobody hadreferenced and realize that it had only beenpublished in the transactions of the meetingthat I first presented it at. Never submitted itfurther. I had retired from academic medicine.I never was a very good salesman and didn’tunderstand that you must be if want anyone toaccept or adopt your ideas or advances. LikeKelman. Or better yet, Parks, who inventedthat new and absolutely sure marketing thing,“pediatric ophthalmology”!

Binocular Vision & Strabology Editorial: Restrictive (Mechanical) Strabismus: An Epidemic? SECOND Quarter of 2012Quarterly, Simms-Romano’s© DNA or Not, Twins Faces, Texas, DRS, Iritis Monitoring Volume 27 (No 2)A Medical Scientific Eye e-Periodical P. E. Romano, MD, MS Ophthalmology Pages 80-87
- 81 -
So we published it here in the firstissue of this year, especially after we hadreceived for consideration a couple moresimilar papers.....
That’s another dozen cases in all, forwhich we had performed 20 surgeries. Thenthe last two papers added another four cases.
With that addition of two more reportson restrictive strabismus published in thisissue, we reviewed these papers for theetiology of the strabismus....
They were divided between those thatwere originally severe cranial nerve palsieswhich had not adequately responded to moreconventional eye muscle surgeries (andmechanical type residual deviations) andthose that were the sequelae or complicationsof prior ophthalmic surgery not pertaining tothe eye muscles or ocular motility per se...
We can’t do much to avoid or preventthe first group but we would call upon ourcolleagues to help us avoid the secondgroup.... The report in this issue, in the abovereference list number 6 offers a number ofsuggestions which they used to correct boththe secondary strabismus and to avoid it in thefirst place....
Editorial Followup: DNA or not;More Epigenetic Medical Problems:
More on epigenetics from yourfinancial newspaper including therecognition as we proposed in the last issueof BV&SQ that school myopia is anepigenetic, not solely a genetic, disease:
Then, SOME VERY SERIOUSREASONS FOR EVERYBODY TO AVOIDSTRESS on themselves and giving it to
others . . . ; IT SHORTENS YOURTELOMERES! (I.e., your life).
From our favorite Medical “journal”The Wall Street Journal Saturday/SundayMay 12-13, 2012 by Matt Ridley. HowDickensian Childhoods Leave GeneticScars. “Being maltreated as a child canperhaps affect you for life. It now seems theharm might reach into your very DNA. Tworecently published studies found evidence ofchanges to the genetic material in people withexperience of maltreatment. These are the tipof an iceberg of discoveries in the still largelymysterious field of ‘epigenetic’ epidemiology- the alteration of gene expression in waysthat affect later health. ... genes aren’tsupposed to change, so you can pass them onto generations untainted by your ownmistakes. It now seems they can at leastacquire marks of experience during life,affecting how much they are ‘expressed’. ...shorter telomeres in children who stayed inBucharest orphanages, compared with thosein foster families. The Duke scientists havemeasured the effect of exposure to bullying,beating or domestic violence between themother and her partner on telemere lengthbetween the ages of 5 and 10 ... On average,the telemeres did shrink faster in those thatexperiences violence than in other children. ...the loss of a parent or maltreatment as a childresults in greater ‘methylation’ of some spotsnear a gene tied to stress response inadulthood. Methylation, the addition of amethyl group of atoms to one DNA ‘letter’,[which occurs throughout life -ed] tends toreduce the activity of nearby genes. ... geneticdeterminism is not necessarily a lifesentence, as those who wear glasses forshortsightedness [EdBOLD] or take a growth

Binocular Vision & Strabology Editorial: Restrictive (Mechanical) Strabismus: An Epidemic? SECOND Quarter of 2012Quarterly, Simms-Romano’s© DNA or Not, Twins Faces, Texas, DRS, Iritis Monitoring Volume 27 (No 2)A Medical Scientific Eye e-Periodical P. E. Romano, MD, MS Ophthalmology Pages 80-87
- 82 -
hormone for growth problems can attest. Thesame will almost certainly be true forepigenetic determinism: Understanding themechanism should bring forward possiblecures.”
More examples: From my personalexperience and exposure to auto racing: Somany children seem to enjoy the same sort ofsuccess racing cars that their fathers did, itseems. And a lot of that talent just has to begenetic. My talent in that area was totallynatural. I loved it from the start and was prettydarn good at, winning my very first race withease, and then winning more and severalchampionships. Today’s champs startedracing go karts when they are three year olds,but my first exposure was in the spring of myfreshman year in medical school at the age of21. Paul Newman was 46 when he started hisracing career. But so many seem to have asmuch as talent as their fathers did eventhough you only get half your genetic materialfrom a father. I think epigenetics is the answerto this inherited ability.
Sit down for this next example Ipropose. After watching a variety ofpathologic psychos try to kill their way toworld domination, I am sure that is an organicbrain disease, but an ACQUIRED one, but sostrong, it is as if their genetics as humanbeings have radically changed. And theycannot in anyway ever recognize or admit tothe wrongfulness of their actions. (Is rightand wrong only epigenetic? See Hype Park138). You don’t suppose those changes arealso epigenetic, do you? That might explaintheir total acquired inhumanity...
Kids do tend to follow their parentsinto life and many seem to enjoy success likejust only one of their parents did, and in many
occupations which do require some specialtalent or ability...
Of course we never hear much aboutthe ones who don’t repeat one of their parentssuccesses... but some of the extraordinarytalent passed on from one parent looks like agood example of something more than simplegenetics, like epigenetics. I think you oftensee that also in athletic or musical endeavors,especially female singers...
Epigenetics Far Out: The world ischanging and radically, and as severely herein the old USA as anywhere. It is moving sofar away from the values we grew up with. Ithink the epigenetc input in childhood mustbe and is very, very different today. It’s as ifno one under about 40 has any of the needs Ilearned to live with and for. But isn’t that truefor every succeeding generation? It isdisarming in so many ways. And we disarmedour parents. What our parents and societyexpected of me behavior wise when I grew upis totally different today.... “Pay-Back” time?
Epigenetics “rules” your longevitythrough stress so be good to those aroundyou. And the single most important “rule”about how to influence others around you isto “set a good example”. Too bad so few ingovernment seem to understand that. Theirrule is instead “do as I say, not as I do”.
Followup on The Mona Lisa: checkCorrespondence on preceding page 79.
Binocular Vision & Strabology Editorial: Restrictive (Mechanical) Strabismus: An Epidemic? SECOND Quarter of 2012Quarterly, Simms-Romano’s© DNA or Not, Twins Faces, Texas, DRS, Iritis Monitoring Volume 27 (No 2)A Medical Scientific Eye e-Periodical P. E. Romano, MD, MS Ophthalmology Pages 80-87
- 83 -
This was from the AMA daily bulletinabout a month ago....
This was good news for me as I havealways been a coffee-holic, and drink a pot ora quart or two of the stuff everyday. It helpsme to manage my bipolar depression, more sosince I have been on those depressing betablockers for a decade now for myarrhythmias, (and even my new pacemakerdoesn’t relieve me of that burden at all). Ibecome a beta blocker zombie if I don’t , andespecially later in the working day... I am notsure what a lethal dose is, but I do overdosenot infrequently or occasionally and an overcaffeinated brain is no fun and no work either.Nor has it produced any Superman or ArnoldShwarznegger type changes in my muscles
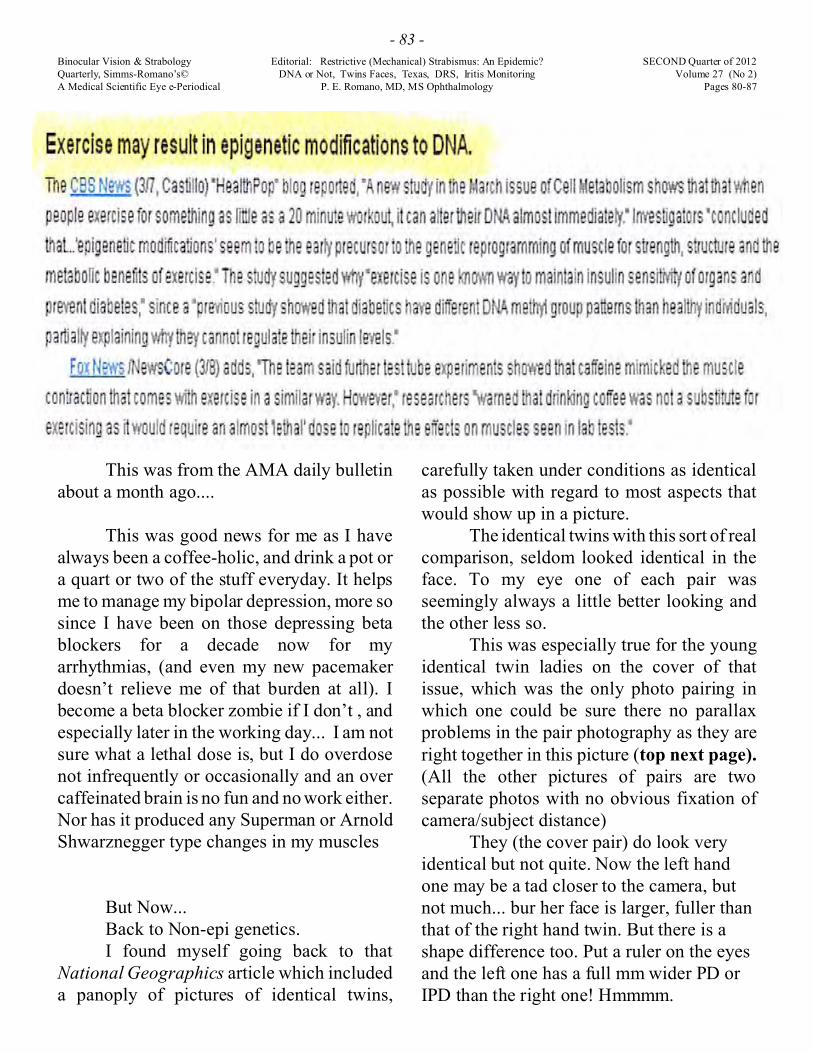
But Now...Back to Non-epi genetics.I found myself going back to that
National Geographics article which includeda panoply of pictures of identical twins,
carefully taken under conditions as identicalas possible with regard to most aspects thatwould show up in a picture.
The identical twins with this sort of realcomparison, seldom looked identical in theface. To my eye one of each pair wasseemingly always a little better looking andthe other less so.
This was especially true for the youngidentical twin ladies on the cover of thatissue, which was the only photo pairing inwhich one could be sure there no parallaxproblems in the pair photography as they areright together in this picture (top next page).(All the other pictures of pairs are twoseparate photos with no obvious fixation ofcamera/subject distance)
They (the cover pair) do look veryidentical but not quite. Now the left handone may be a tad closer to the camera, butnot much... bur her face is larger, fuller thanthat of the right hand twin. But there is ashape difference too. Put a ruler on the eyesand the left one has a full mm wider PD orIPD than the right one! Hmmmm.

Binocular Vision & Strabology Editorial: Restrictive (Mechanical) Strabismus: An Epidemic? SECOND Quarter of 2012Quarterly, Simms-Romano’s© DNA or Not, Twins Faces, Texas, DRS, Iritis Monitoring Volume 27 (No 2)A Medical Scientific Eye e-Periodical P. E. Romano, MD, MS Ophthalmology Pages 80-87
- 84 -
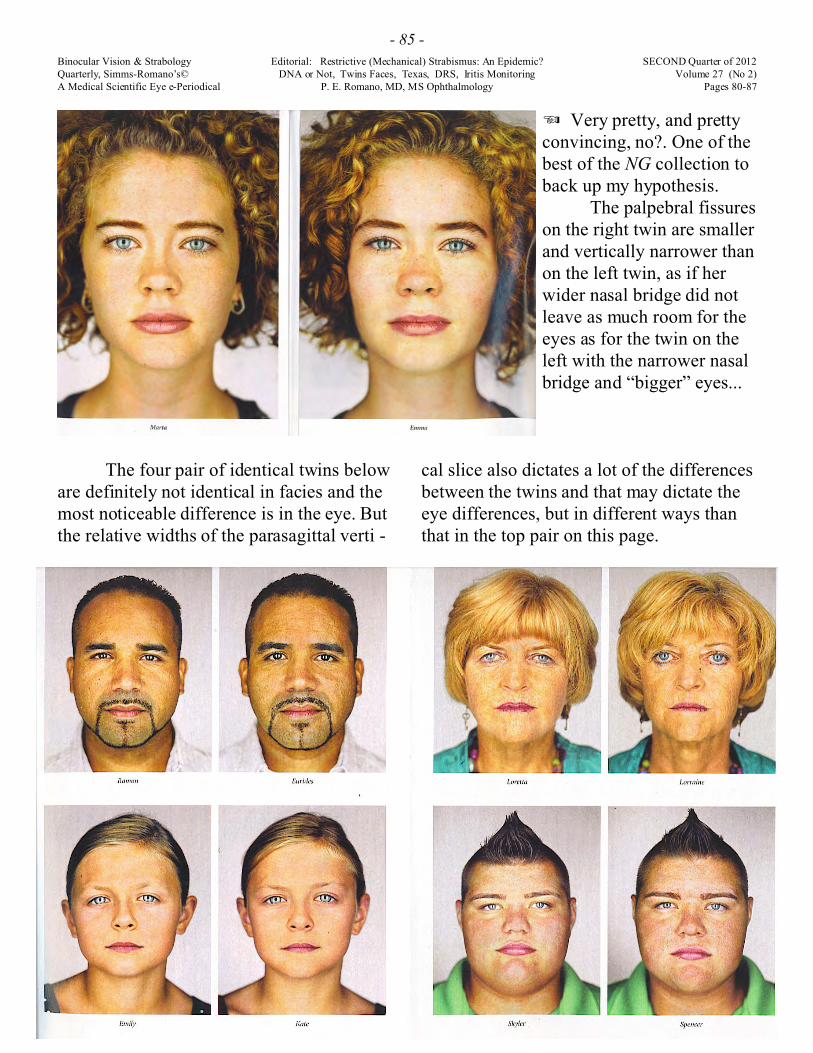
I was also able to convince myselfthat the left twin had slightly larger headwidth, nasal bridge, nasal tip and lips andchin and that it wasn’t just a matter of herpossibly being perhaps a little closer to thecamera than the right twin.
But National Geographic had givenus lots of pictures of identical twin pairs to
look at a few samples of which are on thefollowing pages, and after perusing them, Iwas further able to confirm my hypothesisthat the facial appearance differencebetween them was in each case a matter ofthe thickness of the parasagittal “slice” ofthe face. (See next page)
Binocular Vision & Strabology Editorial: Restrictive (Mechanical) Strabismus: An Epidemic? SECOND Quarter of 2012Quarterly, Simms-Romano’s© DNA or Not, Twins Faces, Texas, DRS, Iritis Monitoring Volume 27 (No 2)A Medical Scientific Eye e-Periodical P. E. Romano, MD, MS Ophthalmology Pages 80-87
- 85 -
The four pair of identical twins beloware definitely not identical in facies and themost noticeable difference is in the eye. Butthe relative widths of the parasagittal verti -
7 Very pretty, and prettyconvincing, no?. One of thebest of the NG collection toback up my hypothesis.
The palpebral fissureson the right twin are smallerand vertically narrower thanon the left twin, as if herwider nasal bridge did notleave as much room for theeyes as for the twin on theleft with the narrower nasalbridge and “bigger” eyes...
cal slice also dictates a lot of the differencesbetween the twins and that may dictate theeye differences, but in different ways thanthat in the top pair on this page.

Binocular Vision & Strabology Editorial: Restrictive (Mechanical) Strabismus: An Epidemic? SECOND Quarter of 2012Quarterly, Simms-Romano’s© DNA or Not, Twins Faces, Texas, DRS, Iritis Monitoring Volume 27 (No 2)A Medical Scientific Eye e-Periodical P. E. Romano, MD, MS Ophthalmology Pages 80-87
- 86 -
Here’s another quartet of NG identical twins
There is in embrogenesis a time whenthese features arise from each of the twosides of the embryo, much like the limbs do,and fuse in the midline to form the face ofthe embryo. This sagittal line in the middleof the face is also in Tessier’s establishedand accepted classification of boney cleftsof the human head, as cleft # 14, the last ofthem, counting them as he does from theside of the head toward the midline..
This occurs very early in fetal life,like about when mom finally is pretty sureshe has missed a period and starts to suspectshe is pregnant. Since these are identicaltwins in the same womb, finding a reasonfor such differences in identical
with the same range of width differences:
twins sounds nigh to impossible but it canmake a significant difference in theappearance of the face. Here comes that newword “like” again.
And looking again when it occurs, aslant or a different slant of the palpebralfissures is a significant, easily noteddifference in the twins.
In each of these pairs it is too easy tofind one face more attractive than the other.We leave that to the geneticists to worryabout, but they can add that to their someday “wish list”. In the meantime if you haveto deal with twins, this sort of carefulphotography and analysis might help you tolearn how to tell them apart.

Binocular Vision & Strabology Editorial: Restrictive (Mechanical) Strabismus: An Epidemic? SECOND Quarter of 2012Quarterly, Simms-Romano’s© DNA or Not, Twins Faces, Texas, DRS, Iritis Monitoring Volume 27 (No 2)A Medical Scientific Eye e-Periodical P. E. Romano, MD, MS Ophthalmology Pages 80-87
- 87 -
In this Issue
Texas !
Mims III JL. Strabology Report andCOMMENT on the 38th Annual Meeting ofthe AAPOS Binocul Vis Strabolog Q SimmsRomano’s 2012; 27(2):88-107.
Thank you, thank you, thank you Jimfor playing local host in San Antonio for ourannual meeting!
And thank you, thank you, thank youfor another huge detailed report on thestrabology presentations there, and yourcomments on them. We don’t know how youdo it. It is such a wonderful piece of work,and you seem to have references or personalexperience or both on every topic. Yourimmense and documented work for all thistime are so appreciated.
Khan AO. An Analysis of 5 Duane’sRetraction Syndrome Patients withPreoperative Abnormal Face TurnReversal and/or Worsening after StandardHorizontal Eye Muscle Surgery. BinoculVis Strabolog Q Simms Romano’s 2012: 27(2) 108-112.
Laria C, Shokida F, Tatarchuck P, Piñero,Gonzalez X. New Diplopia RestrictiveStrabismus as a Sequela AfterConjunctival Surgery for ConjunctivalLesions: A Series of 3 Cases, Managementand Outcome. Binocul Vis Strabolog QSimms Romano’s 2012; 27(2):113-121
Bagheri A, Tavakoli M, Rafaati N. DiplopicMechanical Restrictive Strabismus due to
Ortical Medial Wall Fracture and MedialRectus Muscle Entrapment afterEndoscopic Dacryocystorhinostomy, withOptic Nerve Deficit. Binocul Vis StrabologQ Simms Romano 2012; 27(2): 129-134,
These last two are all cases of compoundmonocular binocular ocular misalignment.How’s that for a term describing an alignmentproblem primarily in the movement and/orabsolute position of one eye, but thiscontributes to a binocular misalignment andboth problems need remediation but together.That is why it is so and most difficult todetermine exactly what to do and especiallyhow much to do, to get the best binocularalignment for the patient.... Our results from our experience 25 years agoas finally published for indexing in the lastissue here are better than those in theaforementioned group of papers on”restrictive strabismus”. And all theprinciples of our IOA III system are confirmedstill valid in the most recently publishedpapers using our IOA techniques (See articleproper in last issue for those references).
Arnold RW, Arnold AW, Eby E, Aleshire.Lay Person Slit Lamp Detection of Iritis inAbsence of an Eye M.D. : Test of a PortableModel of Cells and Flare. Binocul VisStrabology Q Simms Romano’s 2012; 27(2)129-134
The focus here is vast: how do you takecare of patients in remote locations who needregular medical monitoring? How equipmentdependent is the monitoring needed? What ismore important: the equipment or who mansthe equipment? These authors seek a solutionto iritis monitoring!
See you again in the fall -per

Binocular Vision & Strabology Strabology Report & COMM ENT on the 38th AAPOS Meeting Second Quarter of 2012
Quarterly, Simms R oma no’s© James L . M ims, III, MD Volume 26 (No.2)
A Medical Scientif ic ePeriodical Grand Hyatt Hotel, San Antonio, Texas Pages 88-107
88
Strabology Report & COMMENT on the 38th Annual Meeting of the
American Association forPediatric Ophthalmology and Strabology
Grand Hyatt Hotel, San Antonio, Texas, March 24-28, 2012
Meeting Reported by: James L. Mims III, M.D.Local Resident, Native, Host and Reporter
Scientific Program Chair: Stephen P. Christiansen, M.D.President: Steven E. Rubin, M.D.
Scientific Meeting Coordinator: Maria A. Schweers, CO
(EdNote: Author and resident host, Mims, Below, also, as usual, has sent a batch of his neat superbphotos. This year we are able to radically and randomly distribute them individually throughout thetext, [relieved of old serious costs of color by the web and by ink jet printing] so it will be harder tomiss who you missed. -or important comments by Mims on various contributions. This is finally sortof a “Facebook” for AAPOS meetings, which the editor actually started to do about 20 years agowhen AAPOS membership was growing too fast to keep up, but we never got it off the ground (toobad! but I was too busy and old! to do a Mark Z.). The larger, full name tags AAPOS adopted thisyear help ID ing pics. Maybe they could make them even more legible next year...) (Editorialcomments from here on ....are by the author (Mims) and are in italics.) -PER, ed.
Remember the Alamo!
My mother always told me to thank thehost as I was leaving a party, and, following hersage advice I want to say THANK YOU,AAPOS; I had a really nice time at your party!Thank you especially JenniferHull and Rebekka Stout, AAOc o - o r d i n a t o r s , S c i e n t i f i cProgram Chair Stephen P.Christiansen, MD and ExecutiveVice President Christie L.Morse, MD. Because youproduced a flawless meeting, Iwas able to push the envelope(gently) and have a really greattime. If the meeting had beenanything but flawless, some ofmy antics would have come off
as merely stupid. More on live dog surgery (livesurgeon, mechanical dog) and the exhibit of the
first textbooks of strabismus surgery later. Afterlisting the new officers and mentioning thenamed lectures, this report will detail exciting
and genuinely new basic scienceunder s tand ing o f com m o no b s e r v a ti o n s i n P e d i a tr icstrabismus. After that we shallcont inue our t radit ion ofgrouping summaries of thescientific papers, posters, andw o r k s h o p s p e r t a in i n g t ostrabismus and strabology
New Officers
The new President ofAAPOS, starting July 1, 2012,

Binocular Vision & Strabology Strabology Report & COMM ENT on the 38th AAPOS Meeting Second Quarter of 2012
Quarterly, Simms R oma no’s© James L . M ims, III, MD Volume 26 (No.2)
A Medical Scientif ic ePeriodical Grand Hyatt Hotel, San Antonio, Texas Pages 88-107
89
... will be K. David Epley, MD. The new Vice-President will be Sharon F. Freedman, MD. Thenew Vice-President Elect will be SherwinIsenberg, M.D. Robert E. Wiggins, Jr. MDcontinues as the Secretary-Treasurer. Stephen P.Christiansen, MD will continue as the TheSecretary for Program and the ScientificProgram Committee Chair. Christie L. MorseMD continues as our Executive Vice President.Previous Directors-at-Large who will remain intheir positions include Mary Louise Z. CollinsMD and R. Michael Siatkowski, MD. The onenew Director-At-Large is Derek T. Sprunger,MD.
Costenbader and Knapp Lectures
The Costenbader Lecture was given byex AAPOS President Michael X. Repka MD.
He went beyond the title, “StrabismusAmong Aged Medicare Beneficiaries”, to point
out that although up to 6% of Medicarebeneficiaries have some form of strabismus,only a fraction of one percent receivestrabismus surgery each year. [Is it the lowreimbursement of the Medicare Fee Schedulefor strabismus surgery, or is that old folks don’tcare that much?]{ed note: the RV disappearswith age for both surgeon and patient!}
Host City San Antonio’s crown jewel: The Riverwalk; runs right next to our Hyatt hotel

Binocular Vision & Strabology Strabology Report & COMM ENT on the 38th AAPOS Meeting Second Quarter of 2012
Quarterly, Simms R oma no’s© James L . M ims, III, MD Volume 26 (No.2)
A Medical Scientif ic ePeriodical Grand Hyatt Hotel, San Antonio, Texas Pages 88-107
90
The 2012 Knapp lecture, “The OtherSide of Strabismus”, was given by John J.Sloper, FRCOphth, a clinician who was the firstto describe changes in the layers of the LateralGeniculate Nucleus corresponding to thevisually deprived eye (atrophy). More recently,he documented deficient hand-eye co-ordinationin children with amblyopia. He has founddefects in the brain corresponding to thepresumably normal fellow (“non-amblyopic”)eye as well.
Risk Factors for Wrong Site or WrongMuscle: Errors in Strabismus Surgery
The program committee sagaciouslychose a study (survey) of 1103 strabismussurgeons, of whom 173 (33%) self-reportedhaving operated on the wrong eye or the wrongmuscle at some time in their careers. The rate ofthis kind of error was 1 in 2506 surgeries.Surgeons performing fewer than the median1500 surgeries had an error rate 5.9 timeshigher. Running more than one operatingroom was error-prone (p = 0.02). Indiscussion from the floor a it was emphasizedthat marking on the face is not required toreduce errors of this type to zero if a formal“time out” is observed in the O.R. prior to thestart of the surgery, with empowering of allmembers of the operating team to speak up if
they suspect an impending error. [I personallyhave never experienced one such error in over5000 surgeries, and the Methodist HospitalSystem in San Antonio has written into itsbylaws that there shall be no requirement formarking the face of children who are to undergostrabismus surgery. A colleague in another cityhas described losing a patient who had X’s onwritten on both sides of the face in the pre-opholding area for a bilateral medial rectusrecession. This was the 4th case of the day, andfearful parents “freaked out” and left thehospital.](Paper 2 at 2012 AAPOS, “HumanError in Strabismus Surgery” by Tina RutarMD, Elizabeth Shen BA, Travis C Porco PhDMPH, all of UCSF.)
Contracture as an Explanation of SomeClinical Observations in Pediatric Stra-bology
Thirty-five years ago I asked MarshallParks why there was no head tilt in primaryoveraction of the Inferior Oblique (PrimaryOAIO), and he replied that he did not know.Logically if the IO is pulling too hard (as itwould be if hypertrophied and/or chronicallyhyper-innervated), there should be a head tilt tothe opposite side. In private discussions and inthe workshop entitled “Ocular Motor Plasticityin Strabismus” Burton Kushner MD contendedthat if the primarily overacting IO were merely

Binocular Vision & Strabology Strabology Report & COMM ENT on the 38th AAPOS Meeting Second Quarter of 2012
Quarterly, Simms R oma no’s© James L . M ims, III, MD Volume 26 (No.2)
A Medical Scientif ic ePeriodical Grand Hyatt Hotel, San Antonio, Texas Pages 88-107
91
contractured, then there would be no head tilt.In this ongoing debate, Mims had to admit thatwhile he was certain that primarily overactinginferior oblique muscles in very young childrenwith primary OAIO were larger in diameterthan secondarily overacting inferior obliquemuscles in adults with superior oblique palsies,he really didn’t know if adults in general haveinferior oblique muscles that are smaller thanthose in young children. All agree that primarilyoveracting IO have not been studied by Demer’sMRI techniques, because little kids won’t co-operate well enough. Meanwhile, anotheraudience member, David Guyton MD remindedeveryone that the extorsion, which is known toprecede clinical primary OAIO, would elevatethe MR insertion enough to produce the clinicalpicture of OAIO.
Further possibilities of the importance ofcontracture were raised by Mims. First, he hasobserved that about 50% of young children
receiving a 9 m recession of one LR for X(T)will seem to be undercorrected if measured at 3to 8 weeks post-op, but that most of these willdemonstrate orthotropia and orthophoria ortruly small exophorias at 4 months post-op.Mims asked Linda McLoon PhD if her studiesof muscle metabolic activity early afterstrabismus surgery would supp ort thehypothesis that the operated lateral rectusmuscle underwent full contracture weeks earlierthan the unoperated antagonist medial rectusmuscle. Mims called this the “stirring up thejuices” hypothesis. McLoon replied that, yes,the operated muscle had much morereorganizational activity (is much moremetabolically active) than the unoperatedantagonist in the early post-operative period.
Kushner and Mims had already agreed thatanother common observation could beexplained by this difference in rate ofcontracture post-operatively between theoperated agonist and the unoperated antagonist.This observation is that among a series ofinfantile esotropes all receiving a bilateralmedial rectus recession according to astatistically rigorous dose-response curve basedon results at 6 week post-op, the infants with thelarger angles will tend to have a recurrent ET by4 months post-op, even though they were

Binocular Vision & Strabology Strabology Report & COMM ENT on the 38th AAPOS Meeting Second Quarter of 2012
Quarterly, Simms R oma no’s© James L . M ims, III, MD Volume 26 (No.2)
A Medical Scientif ic ePeriodical Grand Hyatt Hotel, San Antonio, Texas Pages 88-107
92
orthotropic at 6 weeks post-op. (Tran HM,Mims III JL, Wood RC. A new dose-responsecurve for bilateral medial rectus recessions forinfantile esotropia. J AAPOS 2002; 6:112-119.)This observation, also, could be explained bythe longer LR in the infants with larger ETangles pre-op, which would take longer toundergo full contracture than the correspondingrecessed medial rectus muscles.
[In this publication, BVS&Q, we havepreviously discussed how progression of the sizeof an unoperated esotropia from age 5 mos toage 12 mos, could be explained by progressivecontracture of the medial rectus muscles. (MimsIII JL. Further implications of probablechanges in medial rectus innervation aftersurgery for infantile esotropia. Binocul VisStrabismus Q 2009; 24(No.4):228-232.) If,after all, a muscle reorganizes itself internallyto achieve a normal linear density ofsarcomeres according to the average length ofthat muscle in a 24-hour period, then thechronically hyper-innervated MR is shorteneduntil a steady state is reached between thehype r- inne rvat i o n a nd the shor tenedsarcomeres (down their length-tension curve).When the contractured muscle then approachesa more nearly normal linear density ofsarcomeres, then it will once again pull harderfor a given level of hyperinnervation, andproduce an even larger angle of esotropia. This
neatly explains why the angle of ET growslarger over time in most babies.]
In this same workshop, Vallabh Das PhDreported recordings from the motor cortex inmonkeys with sensory induced esotropia. (Heuses opaque contact lenses and alternated themdaily in the first few months of life, and reliablyinduces esotropia.) He reports that A & Vpatterns can be explained entirely by hisrecordings in the motor cortex. (David Stager JrMD made the workshop even more interestingby giving a pre- and post- workshop quiz for theaudience with the audience responding withremote-control devices (just like the adultcataract surgeons do).
In the body of the workshop, LindaMcLoon emphasized variability and constantremodeling and Stephen Christiansen MDemphasized neural gain and CNS plasticity.

Binocular Vision & Strabology Strabology Report & COMM ENT on the 38th AAPOS Meeting Second Quarter of 2012
Quarterly, Simms R oma no’s© James L . M ims, III, MD Volume 26 (No.2)
A Medical Scientif ic ePeriodical Grand Hyatt Hotel, San Antonio, Texas Pages 88-107
93
Can the Fascicles of Extraocular MusclesEasily Side Over One and Another? (andwhy it matters)
Extending their blockbuster revelationslast year of separate innervation to the superiorand inferior halves (roughly) of medial rectusmuscles, Robert A. Clark MD and Joseph L.Demer MD PhD reported than their MRI studiess u g g e s t ed d i f f er en t i al co m p ar tm en ta lcontractility of the medial rectus in normals insupraduction but not infraduction. Theyhypothesize that this contributes to the torsionalstability of the eye as it looks upward. In the
formally presented discussion of this paper,Linda McLoon PhD presented 4 major pointsthat would refute this paper’s findings. In paneldiscussion (and in my 30-minute discussion withthis author later), Clark refuted all 4 of herpoints.
McLoon Clark1. Histological study reveals stout interconnections 1. Biomechanical study of fresh musclesbetween muscle fascicles. Reveals easy slippage.*
2. On upgaze, the upper border of the MR is 2. Both upper and lower borders of the MRshorter and the lower border is longer, thus are longer on upgaze, increased explaining Clark’s findings as merely passive contractility is seen only in the upper half changes. of the MR
3. Classical EMG recordings reveal no changes 3. Recordings have not been made at theon upgaze. Upper half vs. the lower half.
4. The 3rd nerve nucleus is incompatible with 4. No, it isn’t.differential contractility of the upper and lowerhalves of the MR.
* a Best-of-Show Blue Ribbon Award Winning Poster: “Mechanical Study of Compartmentalizationin Passive Bovine Extraocular Muscles (EOMs). By Andrew Shin MS, Lawrence Yoo PhD, andJoseph L. Demer MD PhD.
[Stay tuned for the future resolution of this Battle of the Titans of EOM physiology and histology.]

Binocular Vision & Strabology Strabology Report & COMM ENT on the 38th AAPOS Meeting Second Quarter of 2012
Quarterly, Simms R oma no’s© James L . M ims, III, MD Volume 26 (No.2)
A Medical Scientif ic ePeriodical Grand Hyatt Hotel, San Antonio, Texas Pages 88-107
94
Papers & Posters That Will ImpactMy Practice of Strabismus Surgery
Deepak Mangla MS, John W Simon MD,and Jitka Zobal-Ratner MD compared twogroups of 17 patients treated for consecutiveexotropia. In this presentation, Mangla et alcompared two groups of 17 such patients withsimilar preoperative deviations. Postoperativedeviations were 11.4 prim diopters in theadvancement group and 11.9 prism diopters inthe resection group, and a somewhat higherproportion of the advancement group achievedbinocular re-alignment within 10 diopters oforthotropia (65% vs 47%for resection).
I shall continue my current practices. Also, Ishall continue to have the usual concerns abouteliminating concurrent IO or SO overaction.Note: I no longer perform bilateral SOtenotomies for lambda pattern consecutiveexotropia because it tends to produce esotropiain down gaze. Instead, I perform bilateralRosenbaum posterior tenectomies of the SOtendon at its insertion, as described in theRosenbaum Santiago textbook, leaving only theanterior 1 mm of the SO tendon intact. Usually,to prevent worsening or unleashing DVD, I willsimultaneously recess both SR 10 mm with 3mm of nasal transposition. I probably couldn’tdo this routinely were it not for my private dutyscrub nurse, Susan Seekatz, who has been kindenough to work with me for 28 years.]
Three other posters verified previousprejudices. For many years, for angles of lessthan 30 prism diopters, I have been content witha 9 mm recession of the ipsilateral LR forpatients with organic amblyopia, and recessionsof 6 mm with PFS [myopexy] for esotropes withdense and intractable amblyopia. Luisa MHopker MD and David R Weakley MD
compared 42 patients with sensory strabismuswho received a one-muscle recession with 41who received recess-resect. Of these 83, 36 hadsensory ET and 47/83 had sensory XT. With amean age of 65 months and a mean follow-up of35 months, success (within 10 PD) wasachieved in 74% of one-muscle procedures and54% of recess-resection procedures. [Hopker

Binocular Vision & Strabology Strabology Report & COMM ENT on the 38th AAPOS Meeting Second Quarter of 2012
Quarterly, Simms R oma no’s© James L . M ims, III, MD Volume 26 (No.2)
A Medical Scientif ic ePeriodical Grand Hyatt Hotel, San Antonio, Texas Pages 88-107
95
and Weakley did not add the PFS [myopexy] tothe MR recession as originally suggested byMalcolm Mazow MD, but I am convinced that itis important to add the PFS [myopexy] in thepresence of eccentric fixation.]
Another prejudice verified was theimportance of removal of the scleral buckle incases of strabismus appearing after retinaldetachment surgery. Jee Ho Chang MD PhD,Amy K Hutchinson MD, Monica Zhang, andScott R. Lambert MD found a “statisticallysignificant” difference (62.5 % success withbuckle removal and only 11.1% success withoutbuckle removal, p < 0.05).
Yet another prejudice [Ednote: AuthorMims likes this word “prejudice” and uses it alot but he is only being pre-emptive againstcounter attacks because he doesn’t really meanhe is what the dictionary says about this term: “1. An unfavorable opinion or feeling formedbeforehand... without knowledge, thought orreason. 2. Any pre-conceived opinion...3.Unreasonable feelings, opinions, or attitudes,esp. of a hostile nature...” -PER ]
...verified was ignoring most verticals whenplanning strabismus surgery for primaryintermittent exotropia. This was verified byMichael C Struck MD and Timothy J. DaleyMD, who reviewed the charts of 21 consecutivepatients with 5 or more prism diopters of
hypertropia in the setting of intermittentexotropia. At 6 months post-op, 9/11 patientswith hypertropia who underwent horizontalmuscle surgery alone were binocularly“aligned” (82%), whereas only 3/10 of patientswith combined ver tical surgery were“successful” (30%). Five of the ten receivingsimultaneous vertical and horizontal surgeryhad an “overcorrection” of the verticaldeviation!
One of my prejudices in regard to theineffectiveness of a certain procedure was alsoverified. Preeti A Patil DNB, Mahmoud ElSahn, Salma Khayali, Shira L Robbins MD, andDavid B. Granet MD transposed the lateralhalves of the vertical rectus muscles combinedwith Scott Foster lateral fixation sutures in 4patients with sixth Cranial Nerve palsy, and hadlarge average 15 prism diopters residualdeviations.

Binocular Vision & Strabology Strabology Report & COMM ENT on the 38th AAPOS Meeting Second Quarter of 2012
Quarterly, Simms R oma no’s© James L . M ims, III, MD Volume 26 (No.2)
A Medical Scientif ic ePeriodical Grand Hyatt Hotel, San Antonio, Texas Pages 88-107
96
[I am aware of three patients who hadthis procedure by excellent surgeons elsewherewho also had gross undercorrections.Personally, I really like David Coats MD et al(who published a nice diagram of thisprocedure in BV&SQ: Coats DK, Brady-McCreery, Paysse EA: Split rectus musclem o d i f i e d F o s t e r a u g m e n t e d p a r t i a ltransp osit ion proced ure fo r par alyt i cstrabismus. Binocul Vis Strabismus Q 2001;16:281-284 and David Granet MD, the seniorauthor of this poster, but I simply think thisprocedure is inadequately effective.]
[EdNote: we again (sorry...) recommend forall these surgeons and patients our stage III(endoperative) intraoperative adjustment of eyemuscle surgery, guided by the surgicallyachieved binocular re-alignment, see LeadEditorial this issue, pages 80-87 and the priorfirst issue of this publication for 2012, for ourspecific guidelines, article on pages 46-50]
Third Nerve Palsy and INO (Internuclearophthalmoplegia) Surgical Treatments
Linda R. Dagi MD and David G. HunterMD, PhD performed split nasal transposition ofthe lateral rectus to the insertion of the medialrectus with postop’ adjustment in 3 children,two with unilateral and one with bilateralcomplete 3rd Nerve palsies and produced no newvertical deviations while improving the XTfrom a median of 35 ET pre-operatively (range,30-135) to a post-operative range 0 to 10ET.
Ahmed Gomaa MD of Cairo joinedMonte Del Monte MD in presenting 5 patientswith 3rd N palsy and aberrant regeneration suchthat the blepharoptosis resolved in adduction.They performed a large LR recession and MRresection in the other eye with “good” results.[This is not the first time this has been reportedin this rare type of patient. I have seen andoperated, with similar success, one case in 34years of practice.]
Niraj R Nathan and Sean P Donahue MDPhD managed 5 cases of internuclear ophthal-moplegia with a nasal Jensen procedure andlarge recessions of the lateral rectus musclesand were “happy” with the results.
Superior Oblique Palsy
Elias Traboulsi MD, Reecha SachdevaMD, Paul Rychwalski MD, and Andreas

Binocular Vision & Strabology Strabology Report & COMM ENT on the 38th AAPOS Meeting Second Quarter of 2012
Quarterly, Simms R oma no’s© James L . M ims, III, MD Volume 26 (No.2)
A Medical Scientif ic ePeriodical Grand Hyatt Hotel, San Antonio, Texas Pages 88-107
97
Marcotty MD compared results of surgicaltreatment of SOP in 42 who had undergonerecession of the IO vs 45 receiving myectomyof the IO. Those patients receiving myectomyhad less post-op HT in primary gaze (p = 0.002)if the deviation was less than 20 HT in theprimary position pre-op, but surgery on the IOalone was generally insufficient for deviationsabove 20HT.
[Note: I will not change to myectomies asdescribed, having seen three cases of ET in upgaze after myectomies. Instead, I shall continueto perform a procedure originally described ata Texas Society for Pediatric Ophthalmology byMonte Stavis MD 20 years ago. This includes atriangular myectomy of the posterior insertionalfibers, and attachment of the anteriorinsertional fibers 5 mm posterior to the lateralend of the insertion of the inferior rectus. Thisrarely produces ET in up gaze and in 2 cases Ihave retrieved the IO and advanced it toeliminate an ET in up gaze. I have performedthis procedure over 200 times, usually forprimary OAIO, but occasionally for SOP.]
Reza Nabie MD, Minoo Azadeh, andDima Andalib MD performed “graded”recessions of the IO in 32 patients withunilateral SOP with primary position deviationsof up to 25 HT and reported good results forpatients with deviations less that 20 HT. Theirsuccess rate was 89% for deviations of 16-20HT, but only 50% for deviations of 21 – 25 HT.[Benefits of grading vs performing the sameprocedure in every case are not proven in thistype of study.]
Karen Hendler MD, Federico G VelezMD, Arthur Rosenbaum MD, Joseph L DemerMD PhD, Guillermo Velez MD, and Stacy LPineles MD combined their experience insurgical treatment of laterally incomitanthypertropias, with 25 patients receivingrecessions of the IO and 21 receiving smallrecessions of the IR. They reported 8%overcorrections in central gaze in the IO groupand 14% overcorrections in the IR group.Significantly, no patient in the IO group wasovercorrected in down gaze, but 19 % [!] wereovercorrected in down gaze in the IR group.
[I sincerely hope all of these authorswere measuring carefully in 9 cardinalpositions and performing the Intraoperative 3-Step Test, or at least the Plager Test beforedeciding to perform a weakening procedure onthe IO. (Mims III JL. The triple forced ductiont e st ( s ) for th ed i a g n o s i s a n dt r e a t m e n t o fsuperior obliquepalsy. Binocul VisS t r a b i s m u s Q2003; 18(1):15-24.)]

Binocular Vision & Strabology Strabology Report & COMM ENT on the 38th AAPOS Meeting Second Quarter of 2012
Quarterly, Simms R oma no’s© James L . M ims, III, MD Volume 26 (No.2)
A Medical Scientif ic ePeriodical Grand Hyatt Hotel, San Antonio, Texas Pages 88-107
98
The Effect of Medial vs Lateral RectusSurgery on Distance-Near Incomitance
Steve Archer MD has been dubbed thestatistical conscience of AAPOS, a title he welldeserves. His definitive paper on this, “Theeffect of medial versus lateral rectus musclesurgery on distance-near incomitance”. JAAPOS 2009; 13:20-26, should have been thelast word on this subject: When you recess orresect the lateral rectus, you do not get moreeffect on the distance deviation than the neardeviation, and when you recess or resect themedial rectus, you do not get more effect on thenear deviation than the distance deviation, ineither case, unless that is what the patienthappens to need from your surgery. His analysiswas based on over 600 patients.
The 23 patients Reported and studiedhere by A Pauls Grigorian MD, BritaDeacon MD, Scott Lowery MD,Katherine J Fray CO, Shawn L BrownBS CO COMT and Paul H PhillipsMD added little, except that theylooked at results unusually early, atonly one week post-op.
[One example is that if you geta recurrent high AC/A ET years after
a bilateral medial rectus recession, the bestsurgery is a unilateral LR resection of 7.5 mmusually, as originally suggested by BurtonKushner MD at the 2004 AAPOS meeting, andconfirmed in large series by Nelson et al in2006. Thus unilateral LR resection is muchbetter than doing anything else to a medialrectus in recurrent high ACA ET, such asmarginal myotomies (the 70’s, proven not to bea good idea by von Noorden), posterior fixationsutures (the 80’s, tough to deal with if you get aconsecutive XT later), or re-recessions (the90’s, at least 27% late consecutive XT inchildren as published by the Stager group in JAAPOS.) Another good example is recurrentXT with a larger deviation at distance than atnear after previous bilateral lateral rectusrecessions of 6 or more mm. Resection of oneMR 5 mm works really well. (Mims III JL.Outcome of 5 mm resection of one medial rectusmuscle for recurrent exotropia. Binocul VisStrabismus Q 2003; 18(3):143-150).]
In a similar vein, Zia Chaudhuri MSFRCS(Glasg) and Joseph L Demer MD PhDfound that MR recession was as effective as LRresection in divergence paralysis esotropia
(DPE). 6 patients with DPE had MRIand all demonstrated LR sag as thecause of the strabismus. This is due to athinning and atrophy of the membraneconnecting the LR and the SR asdescribed in detail by Demer last year.They found, however, that recession ofthe MR, “physiological antagonist ofthe sagging LR, provided binocular

Binocular Vision & Strabology Strabology Report & COMM ENT on the 38th AAPOS Meeting Second Quarter of 2012
Quarterly, Simms R oma no’s© James L . M ims, III, MD Volume 26 (No.2)
A Medical Scientif ic ePeriodical Grand Hyatt Hotel, San Antonio, Texas Pages 88-107
99
single vision without convergence insufficiencyat near”, and was more convenient for laterintraoperative adjustment under topicalanesthesia than was LR resection.
Winner of the 2012 “I told you so”Award
Kirsta L. Schoeff DO, Zia ChaudhuriFRCS MS, and Joseph L Demer MD PhDmeasured horizontal rectus EOM size andcontractility in concomitant esotropia and foundthat both the MR and the LR had supernormalsize and contractility. Greater MR contractilitycould either reflect greater MR neural drive inesotropia or merely reflect the larger horizontalductions in the MRI scanner enabled by thestrabismus. LR function was not reduced in sizeor function in these patients with concomitantesotropia. [Told you so? Well, maybe this iscompatible with the notion that medial rectusmuscles in esotropia are hyperinnervated untilwe do something to make the eyes straight, elicitFUSION, and normalize the innervation of themedial rectus. (Mims III JL, Miller AM,Schoolfield J. The exoshift under anesthesiacorrelates with probable changes in medialrectus innervation after surgery for infantileesotropia. Binocul Vis Strabismus Q 2008;23(4):215-226.)] Unilateral aphakia and
Strabismus
Erick D. Bothun MD,Jul ie C le v e land MSPH ,Michael J Lynn MS, StephenP Christiansen MD, DeborahK Vanderveen MD, Saniel ENeely MD, Stacey J KrugerMD, and Scott Lambert MDparticipated in a study of 114infants operated for unilateralcongeni tal cataract w ithrandom assignment to IOLimplantation or contact lensesfor the optical treatment ofunilateral aphakia. Strabismus

Binocular Vision & Strabology Strabology Report & COMM ENT on the 38th AAPOS Meeting Second Quarter of 2012
Quarterly, Simms R oma no’s© James L . M ims, III, MD Volume 26 (No.2)
A Medical Scientif ic ePeriodical Grand Hyatt Hotel, San Antonio, Texas Pages 88-107
100
developed in the first year of follow-up among38 (67%) of the pseudophakic infants and 42(75%) of the infants treated with contactlenses.(p=0.59) The younger cohort at the timeof surgery developed less strabismus (29 of 50,58%) than the older cohort (51 of 64,80%0(p<0.01).
Prematurity and Reoperations
Lani T. Hoang MD, Carolyn Wu MD,and Deborah K VanderVeen MD studiedstrabismus surgical results in 24 patients bornprematurely. Mean gestational age/birthweightwas 29 weeks/1037 grams in the “success”group (56% of the 24) vs. 26 weeks/805 gramsin the “failure” group (44% of the 24). Thus, themore premature, the greater the need for secondsurgeries.
Is Strabismus Surgery Worth the Cost?
Miriam Ehrenberg MD, Bharti RNihalani MD, Christina E Cain MPH, PatriceMelvin MPH, and Linda R Dagi MD studied733 patients undergoing strabismus surgery andassigned one of four reasonable goals to eachsurgery. These goals were: (1) binocular visionfunction with some level of stereopsis (2)restoration of eye contact (3) diplopia control,or (4) torticolis management. The politicallycorrect term they used for these study goals was“Goal-determined, Risk-Stratified OutcomesAnalysis”. One of these goals was achieved in84% of their patients.
Kelly MacKenzie, Hayley James, CharisAu, Jo Hancox, Daniel Ezra, Gillian GWAdams MD, and Stanton Newman studied thepsychological status of adults with strabismusseeking surgical correction and found that thesize of the deviation was not as important ashow the patient felt about having a noticeablestrabismus and their expectations for improvingsocial relationships after the strabismus wascorrected. (48 pa t ien ts , psychologicalquestionnaires)
Robert C Cheeseman MBBCh, VickiWong, Jane Young, Ian B Marsh, and Jon MDurnian performed a prospective study of thechange in patient’s quality of life followingstrab i smus surgery using the A S-20questionnaire. Among 63 patients with medianage 35 years, the median AS-20 score of 40improved to 70 post-operatively, indicating thatsuccessful strabismus surgery had a highly

Binocular Vision & Strabology Strabology Report & COMM ENT on the 38th AAPOS Meeting Second Quarter of 2012
Quarterly, Simms R oma no’s© James L . M ims, III, MD Volume 26 (No.2)
A Medical Scientif ic ePeriodical Grand Hyatt Hotel, San Antonio, Texas Pages 88-107
101
positive impact on thesepatients quality of life.
David A Leske MS,Sarah R Hatt DBO, LauraLiebermann, and Jonathan MHo lm es M D soug ht toimprove the adult strabismus-20 (AS-20) questionnaire andfound a closer correlation withstrabismus surgical successesusing a Rasch-modified AS-20, due to anemphasis on the psychosocial subscale.
[However, nothing beats the $ 1.4million in lifetime income loss crediblyestimated resu lting from UN correctedstrabismus, etc. in Beauchamp CL, Felius J,Beauchamp GR. “The economic value added(EVA) resulting from medical care off u n c t i o n a l a m b l y o p i a , s t r ab i s m u s ,(pathologies of binocular vision) andasthma”. Binocul Vis Strabismus Q 2010;25(4):206-216 when you are trying to justifystrabismus surgery. Thank you Cynthia, Joost,George, Paul, and Judy! [EdNote: you don’tsuppose the economic difference to the patientby normalization has anything to do with theirQuality of Life, per se, do you? Maybe it justmakes them FEEL better! $ 1.4 million worthof feeling better! Maybe there just reallyshould be a big fat full lifetime governmententitlement for everyone who is NOT beautifulor good looking! Or see the wonderfulBrazilian alternative in Hyde Park Editorialpages 138-152 -PER ]
Can You Save Money by PerformingUnnecessary Surgery?
The answer, clearly, is yes, if inperforming the first surgery of a potential 2 or3, the total of your failure percentage plus thepercentage of unnecessary surgeries (due topotential for spontaneous resolution of theproblem without surgery) is smaller than thefailure percentage experienced if you wait until
all the patients with a reasonable potential forspontaneous resolution have resolved.
One example is unilateral recession ofone LR 9 mm in children with X(T) performedat age 18 mos. The long term failure rate is20%, when the surgery is performed at this age,but you might be operating on as many as 10%“unnecessarily”. If you were to wait until 6years of age and perform bilateral lateral rectusrecessions, you then incur 3 penalties: (1)poorer outcome in stereopsis; (2) initial costslightly higher due to longer O.R. time and feefor two instead of one muscle surgery; and (3) are-operation rate of 40%. ( But early surgery’s10% + 20% = < 40%).
This is a fairly well-recognized example(at least in most of Texas and in Philadelphia)of how “unnecessary” surgery can beeconomical and therefore in the public’s best

Binocular Vision & Strabology Strabology Report & COMM ENT on the 38th AAPOS Meeting Second Quarter of 2012
Quarterly, Simms R oma no’s© James L . M ims, III, MD Volume 26 (No.2)
A Medical Scientif ic ePeriodical Grand Hyatt Hotel, San Antonio, Texas Pages 88-107
102
interest economically. This conclusion wasvalidated by several discussions at thismeeting.
A similar analysis of office probings forNLD obstruction vs. waiting to perform theinitial probing under anesthesia in those fewfor whom the obs truc t ion d id notspontaneously resolve; by PEDIG; led to theconclusion that the early office probings costsociety less, even though many infants wouldbe probed who would have recovered laterspontaneously, (Ednote: in retrospect thatstrikes me, in this case, as a major moralwrong, as it sounds as if it writes off all therisks, psychic trauma, inconvenience andother human costs of the unnecessary surgeryand the benefits of general anesthesia.Although our current government wouldagree with PEDIG, since cost to them is theirsole and only consideration when it comes tothe practice of medicine.-PER)
Infantile Esotropia, Something to WorryAbout long term again, or not.
The wonderful long-term results ofesotropes straight at age 14 years and stillstraight at age 30 years (116/117) reported byJack Baker MD at previous AAPOS meetingswas diminished by Mohamed S. Soliman MD,Alan B Richards MD, and John D HinrichsenMD. These authors found 6 patients withprevious infantile esotropia who developeddiplopia between ages 13 and 33 years of age.The number of surgeries per patient rangedfrom 2 – 6 (mean was 4). All had experiencedconsecutive exotropia requiring surgery. 3 haddeviations of 6 prism diopters or less, and 3had 10 – 15 ET. As usual Kushner hadreported on this flaw in the diamondpreviously. (Kushner BJ. Recently acquireddiplopia in adults with longstand ingst rabismus. Arch Op hth almol 2001;119:1795-1801.)

Binocular Vision & Strabology Strabology Report & COMM ENT on the 38th AAPOS Meeting Second Quarter of 2012
Quarterly, Simms R oma no’s© James L . M ims, III, MD Volume 26 (No.2)
A Medical Scientif ic ePeriodical Grand Hyatt Hotel, San Antonio, Texas Pages 88-107
103
Anterior Orbitotomy for “Lost” orTransected Medial Rectus Muscles
Stacey L Pineles MD, Jessica LaursenMD, Robert Goldberg MD, Joseph L DemerMD, and Federico G Velez MD tabulated thefunctional results of repairs by anteriororbitotomy performed in cases of MRtransection or avulsion. 5 of 9 patients achievedsingle binocular vision in the primary position.They did not claim better functional results thanother treatments, but 5 of 9 patients are reallyhappy.
Assorted Observations in Strabismus
Michael S. Abrams MD pointed out thatlarge loose prisms, such as those we all use inperforming the alternate cover and cover-uncover tests, can fit into the clips in an adulttrial frame, and will stay in place for longenough for the adult to “experience” correction.
[My experience is that this is a waste of time;one day of straight eyes will enable 97% ofadults to adapt to straight eyes without diplopiaaccording to separate large series reported by
Bill Scott MD and by Burton J Kushner MD.]
Marlo Galli CO and Gregg T LuederMD found that patients who undergo prismadaptation testing will either simply fuse withthe large prisms or “eat” the prisms and returnto their original angle in addition to the prismsthey are wearing. [PAT isn’t necessary for highsurgical success rates. If you measure distanceconvergence fusional amplitudes with a prismbar they are almost always equal to the neardeviation. Do it (your surgical dosage) for thenear angle and you have a high success ratewithout PAT or even without doing the fusionalvergence amplitudes. The distance fusionalamplitudes in this context (high AC/A ET) havebeen termed “the maximum motor fusion test.”(Mims III JL, Wood RC. The maximum motorfusion test: a parameter for surgery foracquired esotropia. J AAPOS 2000; 4(4):211-216.]
Surgical Alternatives for Exo-Duane’swith Severe Co-contraction
Pradeep Sharma MD, Ruchi Tomer MD,Vimla Menon MS, and Rohit Saxena MEperformed periosteal fixation of the lateralrectus in 6 patients and combined this with splitvertical rectus lateral transpositions in 7

Binocular Vision & Strabology Strabology Report & COMM ENT on the 38th AAPOS Meeting Second Quarter of 2012
Quarterly, Simms R oma no’s© James L . M ims, III, MD Volume 26 (No.2)
A Medical Scientif ic ePeriodical Grand Hyatt Hotel, San Antonio, Texas Pages 88-107
104
additional cases of exo-Duane’s. In addition tomeasurements in 9 cardinal positions, theymeasured adduction and abduction using asynoptophore, the extent of binocular singlevision using a perimeter,Hertel exophthalmometryand palpebral fissuremeasurements at 1 week,1 month, and 3 monthspos t -op . T h ey w ereimpressed that spli tvertical rectus transferimproved the extent ofthe single binocular field,but the very small furtherimprovem ent in theprimary position angle made me question this.You can make the right patient with this type ofproblem really happy simply by extirpating theoffending lateral rectus. Spectacular casestreated with extirpation of the offending lateralrectus have been presented at the Texas Societyfor Pediatric Ophthalmology by O.B. JacksonMD and Susan Berry MD.
Russians Secretive about their DifferentStrabismus Surgery Dosage
When Igor E Asnauryan PhD, MohamadEl Sada, Victoria O Balasanyn Md PhD and ErikAznauryan of Cairo and Yasnic Vzor ofMoscow presented a “mathematical model forthe calculation of the horizontal parameters forhorizontal strabismus surgery” everyone wasinitially excited, until Burton J Kushner MD in
formal discussion pointed out that thecomputer p rogram was proprietary(“private” and not available for his neededcritical analysis) and was for only “recess-resect” procedures in which the “resection”was actually a muscle plication instead ofthe resection prevalent elsewhere so thispresentation was Not helpful for the rest ofthe world and us.
Elsewhere: Rachel Bloom MD, NormanMedow MD, and Iliana B Friedman MD
sent a survey to all physician members of theAAPOS and segregated results of types ofsurgeries performed by those practicing in theUSA and those practicing outside the USA.
(Interestingly, inv i e w o f th eplications usedin the paperc i t e d in th eprevious paper,above, 97% ofs u r g e o n swo rldw ide doresections, notp l i c a t i o n s . )When amblyopiais not severe,
bilateral surgery is preferred by 87% of USsurgeons, but only 70% of non-US surgeons.Worldwide, 70% do not use any adjustablesutures. Only 2% use post-op oral antibioticsworldwide. [I.V. antibiotics after anesthesiainduction and prior to surgical incision is nowvirtually universal in the U.S.] Post-opendophthalmitis occurring at least once in asurgeon’s career was similar worldwide, about9% of those reporting. [Thank God I’ve neverhad one!]
The 170 year old First Textbooks ofStrabismus Surgery
The first Saturday afternoon of themeeting, in the registration hall, in specialplastic display cases, Mims displayed [? HISORIGINAL COLLECTOR COPIES OF ?

Binocular Vision & Strabology Strabology Report & COMM ENT on the 38th AAPOS Meeting Second Quarter of 2012
Quarterly, Simms R oma no’s© James L . M ims, III, MD Volume 26 (No.2)
A Medical Scientif ic ePeriodical Grand Hyatt Hotel, San Antonio, Texas Pages 88-107
105
]the first monographs published with diagramsof strabismus surgery. These five works werethe first published in Germany (Dieffenbach),
France, Great Britain, Boston, and Richmond.They were all published in 1840 – 1842. WhatFun!
Binocular Vision & Strabology Strabology Report & COMM ENT on the 38th AAPOS Meeting Second Quarter of 2012
Quarterly, Simms R oma no’s© James L . M ims, III, MD Volume 26 (No.2)
A Medical Scientif ic ePeriodical Grand Hyatt Hotel, San Antonio, Texas Pages 88-107
106
(Your Reporter’s Poster:)
A Surprisingly Simple Way to Control,Remotely, Strabismus Eye ExaminationLane Distance Fixation Toys that Singand Dance (instead of barking)
Dressed in surgical scrubs, Mimsperformed live mechanical dog surgery todemonstrate... this, his meeting poster on how todo it yourself!.
Cover test and alternate cover testmeasurements with good distance fixation[and control of accommodation -ed] aredemanding but essential tests in themanagement of pediatric strabismus.**Historically, barking dog toys provided the briefmoment of attention and fixation needed fromthe child. New mechanical toys that sing anddance could provide valuable additional secondsof attention but have proven difficult to controlremotely with appropriate power from standardwall current sources.
The availability of 8X "Ultimate" verylong lasting lithium batteries has changed theparadigm for the brief momentary powersources for these toys. Surprisingly, dissectionexploration of the newer toys reveals that thethere is a press-on, press-off switch in the limbor paw which is connected to the interior byonly two small gauge wires (instead of acomputer!). If these two are briefly connected(touched one to the other), the toy turns on oroff, (which is ALL we need!).
Equations for direct current indicate thatlarger gauge wires (such as 16 or 14) have lessresistance than smaller wires with little drop involtage over the remote 6-meter distance of eyetargets in a standard eye lane (and folding it updoesn't work with strabismic kids.). So we usedthat to extend the wires and switch from the toyto the examiner's position.
In addition to detailed photographs of themodification method in the poster, an 8 minutemovie with 27 toys was also shown during
during poster viewing hours, demonstratinghistorical toys and the new toys that sing anddance and the surprisingly simple surgicaltechnique for invading the toys and accessingthe wires and connecting them to a remote-control switch. Widely available inexspensivetoys that sing and dance can now be used fordistance fixation devices in the pediatricstrabismus exam. One toy can be easilyexchanged for another; the toys can even beseasonally appropriate. Or several different oreven identical toys can be displayed andalternated with separate switches.
Ednote: parting shot (Your ed’s life has beenon the line medically four or five times in thelast dozen years, and one of these times it willbe too late, so we take our opportunities whenthey appear.): we had to add to Jim’s fantasticreport and clever engineering the following:
**and for the surgeon, very time consumingin addition to being quite difficult, especiallywith some children, toddlers and infants. Dr.Mims and many others emulate or weretaught by Marshall Parks to do this all bythemselves and Dr. Mims has published manyof the manual tricks that enable him to do thissinglehanded. It is not surprising that heseldom has the time or energy to also performthe various tests for binocular vision (personalcommunication).
Others, like your editor, have encounteredearly in their careers talented and trainedorthoptists, commonly females with “theright” or superior genes to deal with children,and appreciated their tremendous ability tohelp in the thorough and completeexamination of strabismic children. In ourclinical practice we found the male/femalecombo to work one way or the other for themost resistant children in obtaining bothm easu rem ents of the deviat ion andbinocularity.
We note this now, as with the recentconversion of strabology to pediatric

Binocular Vision & Strabology Strabology Report & COMM ENT on the 38th AAPOS Meeting Second Quarter of 2012
Quarterly, Simms R oma no’s© James L . M ims, III, MD Volume 26 (No.2)
A Medical Scientif ic ePeriodical Grand Hyatt Hotel, San Antonio, Texas Pages 88-107
107
ophthalmology, it seems to have made manylike Dr. Mims to have never learned about orhave forgotten orthoptists, or feared themmuch like its inventor who worried they wouldcompete with Eye MDs like optometrists did.But trained orthoptists are still available andare now trained to do near everything else too.But you cannot expect as expert help fromsomeone who has not spent a lot of time intraining in a strabology clinic.
If you are thinking of hiring an orthoptist,they (The International Orthoptic Association)are having their quadrenniel meeting inToronto in just a few weeks in June. (See theirad inside front cover of this issue.)
Ednote: As, unofficial local host, Dr.Mims also made up and copied for distributionduring the meeting, several handouts whichwere also given out to all the attendees,describing the best tourist attractions andrestaurants in the area around the Grand HyattHotel. He even arranged the Rio Raxi nighttouring (see prior pages).
The next, 2013, annual AAPOS meeting will beheld at the Westin Copley Place in Boston.Meeting Dates: April 3-7, 2013.t
DISCLAIMER: While the reporter hasendeavored to be as accurate as possible inreporting in the presentation sat this meeting,the reader is strongly advised to confirm anyinformation in this report before acting on it orapplying it to patients.
Binocular Vision & Strabology An Analysis of 5 Duane’s Retraction Syndrome Patients W ith Preoperative Second Quarter of 2012
Qu arter ly Sim ms Rom ano’s © Abno rma l Face Turn Reversa l / W orsening after Standa rd Horizonta l Eye M uscle Surg ery Volume 27 (No. 2)
A Medical Scientif ic ePeriodical Arif O. Khan, MD PAGES 108-112
-108-
Original Scientific Article
An Analysis of 5 Duane’s Retraction Syndrome PatientsWith Preoperative Abnormal Face Turn Reversal and/orWorsening after Standard Horizontal Eye MuscleSurgery
ARIF O. KHAN, M.D.From the Division of Pediatric Ophthalmology, King Khaled Eye Specialist Hospital,
Riyadh, Saudia Arabia.
ABSTRACT: Background/Purpose: Although horizontal extraocular muscle rectus recessionis an accepted treatment for abnormal face turn (AFT) in Duane’s Retraction Syndrome (DRS),in some situations it can worsen or reverse the AFT. Patients referred to the author with thiscomplication over a 4 year period (2002-2006) were reviewed to identify potential risk factors.
Methods: Retrospective medical record review of DRS patients referred because ofreversal and/or worsening of the preoperative AFT immediately after technically uncomplicatedhorizontal rectus eye muscle recession surgery.
Results: All five patients (5-9 years old, all girls) preoperatively had unilateral DRS (fourType I, one Type III), with significant co-contraction during attempted ipsilateral adduction,orthotropia in the preoperative AFT, normal vision in both eyes, and no other ophthalmicfindings. Four patients had significant postoperative AFT reversal: three DRS Type I patientswith original primary position esotropia of 20 prism diopters or less who developedpostoperative primary position exotropia after large ipsilateral medial rectus recession (twobilateral, one unilateral), and one DRS Type III patient whose primary position exotropiapersisted after moderate bilateral lateral rectus recessions with a posterior fixation myopexysuture to the the contralateral medial rectus muscle. The fifth patient had postoperativeworsening of the original AFT: she was a DRS Type I patient with original primary positionesotropia of 40 prism diopters who still had significant undercorrected primary position esotropiaafter large bilateral medial rectus recessions.
Conclusions: The amount of ipsilateral medial rectus recession for treatment of AFT inesotropic unilateral Type I DRS should be limited if significant preoperative co-contraction ispresent and the degree of primary position esotropia is small; otherwise, a significant reversalof the AFT may occur. Surgical matching of the DRS eye’s duction limitation in the unaffectedeye (e.g., by posterior fixation suture or large recession) can potentially lead to a compensatoryface turn in the direction of the duction limitation in the context of post-operative significantprimary position strabismus.
Received for consideration December 4, 2011; accepted for publication January 3, 2012Correspondence: Division of Pediatric Ophthalmology, King Khaled Eye Specialist Hospital, POBox7191, Riyadh 11464, Saudi Arabia. Email: [email protected]

Binocular Vision & Strabology An Analysis of 5 Duane’s Retraction Syndrome Patients W ith Preoperative Second Quarter of 2012
Qu arter ly Sim ms Rom ano’s © Abno rma l Face Turn Reversa l / W orsening after Standa rd Horizonta l Eye M uscle Surg ery Volume 27 (No. 2)
A Medical Scientif ic ePeriodical Arif O. Khan, MD PAGES 108-112
-109-
INTRODUCTION:
Duane’s Retraction Syndrome (DRS) isa form of congenital incomitant strabismuscharacterized by co-contraction of the medialand lateral rectus muscles in the affectedeye(s) during adduction (1).
A common goal of initial strabismussurgery in unilateral DRS is reduction of theabnormal face turn (AFT) which patientsoften adopt to maintain binocularity (2). Oneaccepted surgical approach is horizontal rectusmuscle recession in the affected eye with orwithout surgery in the unaffected eye to matchthe duction deficient of the affected eye (3-6).
For example, in esotropic DRS Type I,medial rectus recession for the primaryposition esotropia can be performed in theDRS eye while a large medial rectus recessionand/or placement of a posterior fixation suturecan be performed in the contralateral eye tomatch the DRS eye’s abduction defect – thiswould theoretically put the contralateral eye in“fixation duress,” and promote abduction inthe DRS eye (rather than adduction, theposition in which co-contraction occurs).However, poor outcomes have infrequentlybeen reported with this approach (7,8,9).
The purpose of this study is to review aseries of patients with DRS who were referredbecause of poor outcomes after this surgicalapproach, in order to try to identify potentialrisk factors for this paradoxical outcome.
METHODS
A retrospective medical chart reviewwas performed for five unilateral DRSpatients who had uncomplicated rectus musclerecession as initial surgical treatment for asignificant AFT but had undesirable resultsthat were evident immediately post-operatively.
These patients had been referred to theauthor between 2002 and 2006.
RESULTS
All five patients (5-9 years old, all girls)had unilateral DRS (four esotropic Type I, oneexotropic Type III), normal vision in eithereye, and no significant ophthalmic findingsother than the findings associated with DRS.
Preoperatively, in their affected eye allpatients had obvious lid fissure narrowing andglobe retraction during adduction. In addition,during adduction of the affected eye upshootswere demonstrable if the eye was slightlysupraducted and dow nsh oots weredemonstrable if the eye was slightlyinfraducted. Otherwise, there was no verticalstrabismus. All five patients were orthotropicin (at) their preoperative AFTs (Table).Surgeries were performed as planned with nointraoperative complications. Intraoperativeforced ductions were positive for restriction inthe affected eyes in abduction for theesotropic patients and in both abduction andadduction for the exotropic patient.
Postoperative examinations were withintwo weeks of the surgery. All patients wereorthotropic in (at) their postoperative newAFTs. Patient data is summarized in theTable, top, next page.

Binocular Vision & Strabology An Analysis of 5 Duane’s Retraction Syndrome Patients W ith Preoperative Second Quarter of 2012
Qu arter ly Sim ms Rom ano’s © Abno rma l Face Turn Reversa l / W orsening after Standa rd Horizonta l Eye M uscle Surg ery Volume 27 (No. 2)
A Medical Scientif ic ePeriodical Arif O. Khan, MD PAGES 108-112
-110-
TABLE: Patient Data in 5 Cases of Duane’s Retraction Syndrome after ConventionalHorizontal Eye Muscle Surgery
Legend for Table:
C: Case number; DRS: Duane’s Retraction Syndrome: mm: millimeters; M:male; F:female; R: right, L: left; MR: medial rectus muscle; LR: lateral rectus muscle; pfs:posterior fixation suture [myopexy] (placed 12 mm posterior to the insertion); ET:esotropia; XT: exotropia.
Binocular Vision & Strabology An Analysis of 5 Duane’s Retraction Syndrome Patients W ith Preoperative Second Quarter of 2012
Qu arter ly Sim ms Rom ano’s © Abno rma l Face Turn Reversa l / W orsening after Standa rd Horizonta l Eye M uscle Surg ery Volume 27 (No. 2)
A Medical Scientif ic ePeriodical Arif O. Khan, MD PAGES 108-112
-111-
DISCUSSION
The review of the accumulated data ledto the following hypothesis:
The use of rectus muscle “dose-response” tables, while appropriate for thetreatment of most traditional primary positionstrabismus, is not appropriate for the surgicalmanagement of DRS with significant co-contraction.
Patient #1 had an amount of ipsilateralmedial rectus recession that may have beenappropriate for a traditional (non-DRS) fusingpatient with the amount of primary positionesotropia that was measured in the context ofan abduction deficit; however, this amount ofmedial rectus recession led to adductionlimitation and a significant postoperative AFTin the opposite direction. This is presumablybecause the amount of recession in theesotropic DRS Type I eye gave a relativeadvantage to the ipsilateral lateral rectusmuscle during the remaining co-contractionthat occurred during attempted adduction ofthat eye. This relative mechanical advantageof the lateral rectus muscle then led to acompensatory face turn opposite to themuscle’s direction of action in order tomaintain binocularity.
Similar results occurred in Patients #2& #3, both of whom had ipsilateral medialrectus recession for esotropic DRS Type I inaddition to a contralateral medial rectusrecession, and can be explained by the samemechanism. Although this phenomenon hasbeen previously recognized following largemedial rectus recessions in DRS eyes (3,7,8),not all authors limit their medial rectusrecess ions fo r D RS ey es (2 .10 ).Intraoperative “tightness” of the medial rectusmuscle in the affected eye of a patient withesotropic DRS is another relative indication
for limiting the amount of medial rectusrecession (11).
Like Patients #2 & #3, Patient #4underwent medial rectus recession in both theDRS eye and the unaffected eye. However,Patient #4 experienced a worsening of thepreoperative left AFT (rather than a reversal).This phenomenon has also been previouslyrecognized (7) and seems to be because amatched duction limitation in the contralateral(non-DRS) eye can promote a compensatoryface turn in the direction of the ductionlimitation in order to maintain binocularity inthe setting of postoperative primary positionstrabismus. Presumably Patient #4 did notdevelop a face turn reversal like Patients #2  because the amount of medial rectusrecession in the DRS eye was not enough tocorrect the relatively large primary positionesotropia; contralateral medial rectusrecession in this setting seems to havepromoted the original AFT (7).
The concept that duction limitation inthe contralateral (non-DRS) eye can promotea compensatory face turn in the direction ofduction limitation in the context of primaryposition strabismus is also illustrated byPatient #5’s course. In addition to bilaterallateral rectus recessions, Patient #5 had aposterior fixation suture placed in the medialrectus muscle of the contralateral (non-DRS)eye in order to match the abduction defect inthe DRS and thus “theoretically” promoteabduction in the DRS eye (and thus minimizeco-contraction, which occurred duringadduction of that eye). However, in the settingof undercorrected primary position exotropia,the result of this treatment was a face turntoward the induced duction defect rather thanpromotion of abduction in the DRS eye (7).
Although good results have been

Binocular Vision & Strabology An Analysis of 5 Duane’s Retraction Syndrome Patients W ith Preoperative Second Quarter of 2012
Qu arter ly Sim ms Rom ano’s © Abno rma l Face Turn Reversa l / W orsening after Standa rd Horizonta l Eye M uscle Surg ery Volume 27 (No. 2)
A Medical Scientif ic ePeriodical Arif O. Khan, MD PAGES 108-112
-112-
described for horizontal rectus musclerecession in the DRS eye with or withoutsurgery in the unaffected eye to match theduction deficient of the DRS eye (2-5,11),poor results can sometimes occur in situationssuggested by the current case series. Theamount of ipsilateral medial rectus recessionfor treatment of AFT in esotropic unilateralType I DRS should be limited if significantpreoperative co-contraction is present and thedegree of primary position esotropia is small;otherwise, a significant reversal of face turnmay occur. Surgical matching of the DRSeye’s duction limitation in the unaffected eyecan lead to a compensatory face turn in thedirection of the duction limitation when thereis significant, persistent, postoperative pri-mary position strabismus.
REFERENCES
1. Huber A. Electrophysiology of theretraction syndromes. Br J Ophthalmol1974;58(3):293-300. 2. Pressman SH, Scott WE. Surgical treatmentof Duane's syndrome. Ophthalmology1986;93(1):29-38.3. Kraft SP. A surgical approach for Duanesyndrome. J P edia tr O ph tha lm olStrabismus 1988;25(3):119-30.4. Saunders RA, Wilson ME, Bluestein EC,Sinatra RB. Surgery on the normal eye inDuane retraction syndrome. J PediatrOphthalmol Strabismus 1994;31(3):162-9.5. Lingua RW, Walonker F. Use of posteriorfixation suture in type 1 Duane’s syndrome. JOcular Therapeu tics and Surgery1985;4:107-11.6. Farvardin M, Rad AH, Ashrafzadeh A.Results of bilateral medial rectus musclerecession in unilateral esotropic Duanesyndrome. J AAPOS. 2009 Aug;13(4):339-42.7. Nelson LB. Severe adduction deficiency
following a large medial rectus recession inDu ane’s retraction syndrome. ArchOphthalmol 1986;104:859-62.8. Kushner BJ, Arthur BW, Mazow ML, et al.Grand Rounds #51: A case of consecutiveexotropia after medial rectus recession forDuane syndrome. Binocul Vis Strabismus Q1998;13(3):188-92.9. Greenberg MF, Pollard ZF. Poor resultsafter recession of both medial rectus musclesin unilateral small-angle Duane's syndrome,type I. J AAPOS 2003;7(2):142-5.10. Biedner BZ. Medial rectus re-recession forunacceptable head-turn and esotropia inDuane’s retraction syndrome. OphthalmicSurg Lasers 1997;28(9):762-4.11. Kubota N, Takahashi H, Hayashi T, et al.Outcome of surgery in 124 cases of Duane'sRetraction Syndrome (DRS) treated byintraoperatively graduated recession of themedial rectus for esotropic DRS, and of thelateral rectus for exotropic DRS. Binocul VisStrabismus Q 2001;16(1):15-22.
Binocular Vision & Strabology Ne w D iplopic Re atric tive Stra bismus Afte r Con junctiva l Su rge ry. Second Quarter of 2012
Quarterly, Simms R oma no’s© L.C. Laria , MD, PhD, F . Shok ida, MD, MSc, P . Tatarchuck , MD Volume 27 (No.2)
A Medical Scientif ic ePeriodical D.P., P iñero , PhD and X. González, MD Pages 113-121
-113-
Original Scientific Article
New Diplopic Restrictive STRABISMUS as a sequelaAFTER CONJUNCTIVAL SURGERY for conjunctivallesions: A series of 3 cases, managment and outcome.
C. LARIA, MD, PHD1, F. SHOKIDA, MD,MSc,2,
P. TATARCHUCK, MD3 , D.P. PIÑERO, PHD1,4, X. GONZÁLEZ, MD2
From 1 Pediatric Ophthalmology & Strabismus Unit. Oftalmar. Medimar InternacionalHospital. Alicante. Spain, 2 Strabismus and Pediatric Ophthalmology Unit. Italian Hospitalof Buenos Aires. Argentina, 3 Clínica de Ojos Mar Del Plata. Buenos Aires. Argentina, and4 Departamento de Óptica, Farmacología y Anatomía. Universidad de Alicante. Spain.
ABSTRACT: Objective: To present three clinical cases of diplopia secondary to conjunctivalsurgery (for tumor of caruncle and recurrent pterygium surgery).
Patients & Methods: Clinical data of three patients with binocular diplopia andincomitant esotropia associated with compensatory torticollis and duction limitation are shownand discussed. In all cases, a complete ophthalmological examination was performed includingocular motility study, duction test and preoperative evaluation under general anesthesia.
Results: The forced duction test was positive in all cases, confirming the diagnosis ofrestrictive strabismus. Uneventful surgery was performed in all cases in which conjunctivaladherences to eye orbit bones were eliminated and the involved extraocular muscle was isolatedand freed.
Furthermore, some additional treatments were applied to avoid recurrency(subconjunctival and topical corticosteroids, amniotic membrane and therapeutic contact lens).One case presented postoperatively a new conjunctival adherence in spite of such anti-recurrencytreatment although with no significant motility alterations associated.
Conclusions: Conjunctival surgery can cause fibrosis and conjunctival adherences leadingto restrictive strabismus. The surgical procedure for solving this problem must be performed withspecial care to avoid complications and recurrencies. The use of antimetabolites or amnioticmembrane seems to be recommendable to ensure a satisfactory postoperative outcome.
Received for consideration December 1, 2011; accepted for publication January 21, 2012
The authors have no proprietary or commercial interest in the medical devices that are involvedin this manuscript. Correspondence: Dr. Carlos Laria, Oftalmar, Department of Ophthalmology, MedimarInternational Hospital, Avda. Denia, 78, 03016 Alicante, Spain. Email: [email protected]
Binocular Vision & Strabology Ne w D iplopic Re atric tive Stra bismus Afte r Con junctiva l Su rge ry. Second Quarter of 2012
Quarterly, Simms R oma no’s© L.C. Laria , MD, PhD, F . Shok ida, MD, MSc, P . Tatarchuck , MD Volume 27 (No.2)
A Medical Scientif ic ePeriodical D.P., P iñero , PhD and X. González, MD Pages 113-121
-114-
INTRODUCTION
The presence of restrictive strabismusafter multiple conjunctival surgical proceduresor after very complex surgeries is acomplication that should be considered. It isnot a rare condition after pterygium surgery inpatients that have undergone several surgicalprocedures due to recurrencies (1-3).
Likewise, this complication may alsoappear after more aggressive surgicalprocedures such as conjunctival tumourremoval. The motor alterations associated tothis type of strabismus may be due to directaffectation of extraocular muscles withlimitation of the field of action of a specificmuscle (2,3) or to an adherential processsecondary to the presence of fibrotic areaslimiting the contralateral movement of the eye(4).
We present three cases of restrictivestrabismus after conjunctival surgery, oneafter excision of a conjunctival tumour and theother two after multiple pterygium surgicalexcisions.
CASE REPORTS
Clinical Case 1
A 68-year woman attended to our clinicwith complaints of diplopia. The patientcompensated partially for this diplopia byturning the head. As ophthalmologicalantecedents, the patient referred surgery forthe removal of a caruncle tumour in the lefteye (Figure 1 A, top left, next page) one yearbefore, with the perception of a constantdiplopia immediately after surgery. Thiscondition was diagnosed as a post-surgical VInerve palsy. At our examination, the patienthad a decimal visual acuity of 0.9 in botheyes, and a Goldman intraocular pressure of16 and 18 mm Hg in right and left eyes,
respectively. The biomicroscopic examshowed a conjunctival scar in the nasal area ofthe left eye and an incipient phacosclerosis inboth eyes. No abnormalities were detected inthe fundus examination. Regarding ocularmotility, a left eye esotropia of 15 prismdiopters was present in the primary position,with abduction (-4), and supra- andinfradduction limitations (-2) (Figure 2A, top,next subsequent page). The patient presentedcompensatory head position with headrotation to the left. Furthermore, the forcedduction test was positive for all directions,especially for abduction.
Surgery was planned for the correctionof this strabismus. First, the left eye medialrectus muscle was carefully examined. A greatamount of fibrotic adherential tissue betweenthe muscle and the orbitary wall was found(Figure 1B, top right next page). Thesefibrotic adherences were then removed withspecial attention to the different anatomicalplanes. The forced duction test was repeatedduring dissection until it was finally negative.After this, 0.5 ml of triamcinolone acetonide(Trigon Depot, Bristol-Myers Squibb, Madrid,Spain) was injected subconjunctivally.
Motor exercises were prescribedpostoperatively (prism vergence exercises andBrock’s string) as well as a combination oftopical steroid and antibiotic (Tobradex,Alcon, Fort Worth, Texas, USA) to beapplied four times daily for two weeks andtwo times daily during the following twopostoperative weeks.
After the first postoperative month, thisprophylactic treatment was substituted bynon-steroidal anti-inflammatory drops(Dicloabak, Laboratorios Thea, Barcelona,Spain) to be applied during one additionalmonth three times daily. Furthermore, the use

Binocular Vision & Strabology Ne w D iplopic Re atric tive Stra bismus Afte r Con junctiva l Su rge ry. Second Quarter of 2012
Quarterly, Simms R oma no’s© L.C. Laria , MD, PhD, F . Shok ida, MD, MSc, P . Tatarchuck , MD Volume 27 (No.2)
A Medical Scientif ic ePeriodical D.P., P iñero , PhD and X. González, MD Pages 113-121
-115-
Figure 1. (Laria et al): A- Clinical case 1, caruncle tumour, preoperative; B- Clinical case 1,adherences between medial rectus and orbit wall, surgery; C- Clinical case 2, amnioticmembrane transplantation and “Illig” contact lens, surgery; D- Clinical case 2, newconjunctival adherence after contact lens withdrawal, postoperative; E- Clinical case 3,pterygium recurrency in right eye; F- Clinical case 3, pterygium recurrency in left eye.

Binocular Vision & Strabology Ne w D iplopic Re atric tive Stra bismus Afte r Con junctiva l Su rge ry. Second Quarter of 2012
Quarterly, Simms R oma no’s© L.C. Laria , MD, PhD, F . Shok ida, MD, MSc, P . Tatarchuck , MD Volume 27 (No.2)
A Medical Scientif ic ePeriodical D.P., P iñero , PhD and X. González, MD Pages 113-121
-116-
Figure 2. (Laria et al): A- Clinical case 1, positions, preoperative; B- Clinical case 1, positions, 2-month postoperative;C- Clinical case 2, positions, preoperative; D-.Clinical case 2, positions, 1-month postoperative;E- Clinical case 3, positions, preoperative; F- Clinical case 3, positions, postoperative.
...of artificial tears was recommendedduring all this postoperative period (Systane,Novartis AG, Basel, Switzerland). Twomonths after surgery, orthotropia was present,with no torticollis, excellent conjunctivalhealing, and slight abduction limitation (-1) inthe left eye (see also Figure 2B, top right,below)
Clinical Case 2
A 47 year-old presented to our clinicwith strabismus and diplopia in dextroversionthat can be compensated by turning the headhorizontally to the right. As antecedents, the
patient reported that he had undergone 11pterygium surgeries performed by differentsurgeons in the right eye. In the last threesurgeries, mitomycin C 0.3% was appliedduring two minutes in the affected area, witha subsequent conjunctival autografting.Furthermore, conjunctival biopsy wasnegative for pemphigoid in two occasions.The patient reported a significant worseningof the diplopia after the last surgicalprocedures.
At our examination, the patient had adecimal visual acuity of 1.0 and 0.8 in rightand left eyes, respectively. The Goldman

Binocular Vision & Strabology Ne w D iplopic Re atric tive Stra bismus Afte r Con junctiva l Su rge ry. Second Quarter of 2012
Quarterly, Simms R oma no’s© L.C. Laria , MD, PhD, F . Shok ida, MD, MSc, P . Tatarchuck , MD Volume 27 (No.2)
A Medical Scientif ic ePeriodical D.P., P iñero , PhD and X. González, MD Pages 113-121
-117-
intraocular pressure was of 16 and 18 mm Hgin right and left eyes, respectively. Thebiomicroscopic exam showed large amountsof scar tissue in the nasal conjunctival area ofthe left eye, with the presence ofsymblepharon. No abnormalities weredetected in the fundus examination. Regardingocular motility, a right eye esotropia of 25prism diopters was present in the primaryposition, with abduction (-4), and supra- andinfradduction limitations (-2). The patientpresented compensatory head position withhorizontal head rotation to the right (Figure1C, prior page 115, middle frame, left,).Furthermore, the forced duction test waspositive for all type of ductions, especially forthe abduction.
Surgery was planned for the correctionof this strabismus. A great amount of fibroticadherential tissue was found between themedial rectus, and the bulbar and palpebralconjunctiva. This tissue was carefullyeliminated until the forced duction test wasnegative. The symblepharon was separated ascompletely as possible, with elimination of alladherences to the muscle. Afterwards, amedial rectus recession and a lateral rectusmiectomy were pe rformed . As theconjunctival tissue of the affected area couldnot be repaired, it was covered with anamniotic membrane graft to avoid potentialrecurrencies (Figure 1C see page 115). Inaddition, an “Illig” contact lens was adapted(see aforementioned Figure 1C).
In the immediate postoperative period,the patient was left with a residual exotropiaof 5 prism diopters and adduction limitation (-2), considering the potential development ofrecurrencies. A combination of topical steroidand antibiotic (Ciloxadex, Alcon, Fort Worth,Texas, USA) was prescribed to be appliedfour times daily during the first postoperative
2 weeks. Furthermore, the use of artificialtears was recommended during all this period(Systane, Novartis AG, Basel, Switzerland).After contact lens removal, a recurrency of theconjunctival adherence appeared (Figure 1D).In spite of it, the patient showed a satisfactorypostoperative outcome, with a slightadduction limitation (-1) in the right eye (seeFigure 2D, prior page 116, right middleframe), no diplopia in primary position andthe absence of torticollis. This situation wasmaintained during the initial 6 months afterour surgery.
At 12 months postoperatively,orthotropia without torticollis was present, butwith an abduction limitation due to therecurrency of the symblepharon. Theconjunctival biopsy was repeated one moretime and it was positive for “mucousmembrane pemphigoid”. For this, Orali m m u n o s u p p r e s s o r t r e a t m e n t w i t hmethotrexate 10 mg/week (Ervemin, IVAXArgentina) was then initiated and maintainedto this date.
Clinical Case 3
A 58 year-old man attended to ourclinic with diplopia secondary to multiplesurgeries for bilateral pterygium removal. Henormally uses a prism of 7 prism diopters baseout that however does not compensate for hisdiplopia. The patient reported that theperception of double vision was initiallyintermittent and it worsened progressively.Specifically, he described that the perceptionof constant diplopia began 1 week after thesecond pterygium surgery in the left eye. Oneyear after this surgical procedure, anotherpterygium surgery was performed in the righteye with amniotic membrane graft, but thepterygium relapsed two months after.

Binocular Vision & Strabology Ne w D iplopic Re atric tive Stra bismus Afte r Con junctiva l Su rge ry. Second Quarter of 2012
Quarterly, Simms R oma no’s© L.C. Laria , MD, PhD, F . Shok ida, MD, MSc, P . Tatarchuck , MD Volume 27 (No.2)
A Medical Scientif ic ePeriodical D.P., P iñero , PhD and X. González, MD Pages 113-121
-118-
At our examination, the patientpresented a decimal visual acuity of 1.0 inboth eyes with spherocylindrical correction(Right eye: +2.00 -1.00 x 80º; Left eye: +1.50-0.50 x 90º). In the ocular motilityexamination, an incomitant esotropia of 15prism diopters in primary position wasobserved. This deviation increased to 20 prismdiopters with right hypotropia of 12 prismdiopters in levoversion, and decreased to 10prism diopters in dextroversion. In addition,an A-pattern was observed, with 20 prismdiopters of esotropia in supraversion and adeviation of significantly less magnitude ininfraversion (See on prior page 116, Figure2E, lower left frame). The biomicroscopicexam showed a thickened nasal conjunctiva inthe right eye with vascularisation, the absenceof semilunar fold and the presence of ahyperemic caruncle and a relapsed pterygium.In the left eye, a relapsed pterygium was alsoobserved, but with a less degree ofconjunctival hyperemia compared to the righteye (See on prior page 115, Figure 1E andF, bottom row).
Surgery was planned in the left eye. Itpresented a positive forced duction test for theabduction. In addition, a limbar area withstrong adherences of the conjunctiva to sclerawas found as well as a medial rectus adheredto the conjunctiva, with infiltration, fat andfibrosis until the septum. After dissecating andreleasing the adherences, a 2-mm recession ofthe medial rectus was performed by using thetechnique of the delayed adjustable suturewith implantation of a silicone sheet (Silastic)under the muscle. Triamcinolone acetonidewas then injected in the internal-superiorangle.
In the immediate postoperative period,the diplopia disappeared in primary position.A combination of topical steroid and
antibiotic (Ciloxadex, Alcon, Fort Worth,Texas, USA) was prescribed to be applied fourtimes daily during the first postoperative 2weeks. Furthermore, cyclosporine 0.05%(Lacrinmune, Bausch & Lomb Argentina) wasprescribed to be applied two times daily duringthe first postoperative 6 months. Thesatisfactory immediate postoperative outcomewas maintained during the first postoperativeyear (See Figure 2F on page 116 lower rightframe), with only the presence of diplopia inextreme left gaze due to a residual esotropia of7 prism diopters in this position.
DISCUSSION
The diplopia after anterior segmentsurgery can be monocular or binocular. Thepresence of postsurgical monocular diplopia isnormally related to irregular astigmatism aftercorneal surgery (6). However, the postsurgicalbinocular diplopia may be due to a directtrauma over the adjacent muscle (1-3) as wellas to the presence of adherential tissue leadingto a subsequent motor restriction (4). Thedifferential diagnosis of these two conditionsleading to postsurgical binocular diplopia isbased on the ocular motility exploration (SeeFlow chart in Figure 3, next page). Thedirect damage of an extraocular muscle willoriginate a limitation in the field of actioncorresponding to the affected muscle, whereasan adherential restriction will mainly affect thecontralateral field of action, although otherfields may be also limited depending on thelevel of fibrosis. In this last condition,incomitant esotropia may also appear, with alarger deviation when the affected eye isfixating (7).
The forced duction test is also crucialfor the diagnosis because a negative outcomeconfirms the absence of restrictions and then

Binocular Vision & Strabology Ne w D iplopic Re atric tive Stra bismus Afte r Con junctiva l Su rge ry. Second Quarter of 2012
Quarterly, Simms R oma no’s© L.C. Laria , MD, PhD, F . Shok ida, MD, MSc, P . Tatarchuck , MD Volume 27 (No.2)
A Medical Scientif ic ePeriodical D.P., P iñero , PhD and X. González, MD Pages 113-121
-119-
Figure 3. (Laria et al): Diagnostic diagram of the differential diagnosis
of new diplopia after anterior segment surgery, and its management.
of an adherential problem. In theclinical cases reported here, a negative forcedduction test was achieved after the eliminationof the adherential tissue generating therestriction, with necessity of additional musclesurgery in two cases, as reported by otherauthors (7). The potential generation of new
adherences should be considered during thepostoperative follow-up. The use ofconjunctival autograft transplantations hasbeen proposed. as a procedure to avoidrecurrences with these type of surgeries (8).

Binocular Vision & Strabology Ne w D iplopic Re atric tive Stra bismus Afte r Con junctiva l Su rge ry. Second Quarter of 2012
Quarterly, Simms R oma no’s© L.C. Laria , MD, PhD, F . Shok ida, MD, MSc, P . Tatarchuck , MD Volume 27 (No.2)
A Medical Scientif ic ePeriodical D.P., P iñero , PhD and X. González, MD Pages 113-121
-120-
The clinical case 2 reported here showsa right eye esotropia causing a very significantdiscomfort to the patient, because this eyewas the dominant eye. Incomitancy waspresent for lateral gazes as well as for fixationchanges between eyes. In this specific case,the conjunctival affected area was coveredwith an amniotic membrane due to theimpossibility of repairing the conjunctivaltissue. Likewise, an “Illig” contact lens wasadapted to protect against recurrences ofadherences and symblepharon. The earlycontact lens withdrawal due to abundantsecretions not tolerated by the patientfacilitated the partial recurrence of thesymblepharon which did not howevergenerate significant restrictions. The patientpresented postoperatively with no torticollisand orthotropia in primary position. For thisreason, we preferred to wait and see theevolution. It was especially curious that twobiopsies were negative and only the thirdbiopsy after the last conjunctival surgery waspositive for mucous membrane pemphigoid.
The third clinical case shown reports adiplopia caused by a recurrent pterygium (9),with the more significant disturbances whenthe fixating eye was operated on, with thesubsequent mechanical restrictive limitations.This case was solved by eliminating theadherences and by the topical use ofantimetabolites for 6 months. In contrast toother authors (8), the first clinical casereported here showed another case of diplopiadue to a restrictive strabismus in which theelimination of the adherences was enough tosolve the problem, with no necessity of anadditional muscle surgery.
In general, the surgery in restrictivestrabismus after conjunctival surgery must bevery meticulous. The different anatomicalplanes must be respected as maximum as
possible in order to avoid new adherentialprocesses (10,11) and the damage the medialrectus muscle (12). Furthermore, it should beconsidered that the strabismus surgery in thesecases is not concluded until obtaining anegative outcome with the forced duction test.Another factor to consider is the intra- andpostoperative treatment to avoid therecurrency of the adherential process.Intraoperatively, special care must be takenwith the conjunctival closure to prevent futurenew restrictions. Currently, there is still adebate regarding the applicability of theintraoperative use of mitomycin C (13),subconjunctival or periorbitary corticosteroidsand even the possibility of autografts (7) oramniotic membrane transplantations, as in theclinical case 2 reported here, to avoidrecurrencies. More scientific evidence aboutthe mechanism of action and efficacy of thistype of treatments are necessary in the future.We considered that in cases like thosepresented in the current case report, the short-term and long-term monitoring is necessary toevaluate if new adherences are created andtheir motor impact. Thus, the clinician will beable to plan as soon as possible new surgeriesif required to avoid motor restriction withsignificant clinical impact.
In conclusion, a very meticulousprocedure should be always followed inanterior segment surgery during themanipulation of the different anatomicalplanes to avoid the creation of postoperativerestrictive phenomena. The forced duction testis a crucial test for confirming the diagnosis ofa restrictive condition. The potentialrecurrency of adherential processes should bealways considered. The treatment to applyshould be customized according to thespecific features of each condition.
Binocular Vision & Strabology Ne w D iplopic Re atric tive Stra bismus Afte r Con junctiva l Su rge ry. Second Quarter of 2012
Quarterly, Simms R oma no’s© L.C. Laria , MD, PhD, F . Shok ida, MD, MSc, P . Tatarchuck , MD Volume 27 (No.2)
A Medical Scientif ic ePeriodical D.P., P iñero , PhD and X. González, MD Pages 113-121
-121-
REFERENCES
1. Jenkins PF, Stavis MI, Jenkins DE III.Esotropia following pterygium surgery.Binocul Vis Strabismus Q . 2002; 17: 227-8.2. Raab EL, Metz HS, Ellis FD. Medial rectusinjury after pterigium excision. ArchOphthalmol. 1989; 107: 1428.3. Ugrin MC, Molinari A. Disinsertion of themedial rectus following pterygium surgery:signs and management. Strabismus. 1999; 7:147-52.4. Vrabec MP, Weisenthal RW, Elsing SH.Subconjunctival fibrosis after conjunctivalautograft. Cornea. 1993; 12: 181-3.5. Shokida MF. Silicone sheet for delayedadjustable suture strabismus. OphthalmicSurgery 1993; 24: 486-8.6. Walland MJ, Stevens JD, Steele AD. Theeffect of recurrent pterygium on cornealtopography. Cornea 1994; 13: 463-4.7. Ela-Dalman N, Velez F, Rosenbaum AL.Incomitant esotropia following pterygiumexcision surgery. Arch Ophthalmol 2007;125: 369-73.
8. Kenyon KR, Wagoner MD, Hettinger ME.Conjunctival autograft transplantation foradvanced and recurrent pterygium.Ophthalmology 1985; 92: 1461-70.9. Guo S, Wagner R, Gewirtz M, Maxwell D,Pokorny K, Tutela A, Caputo A, Zarbin M.Diplopia and strabismus following ocularsurgeries. Surv Ophthalmol 2010; 55: 335-58.10. Ludwig IH, Chow AY. Scar remodelingafter strabismus surgery. J AAPOS 2000; 4:326-32.11. Ludwig IH, Jacob JT, Gillian B, Dean A.Scar stretch as a cause of consecutiveesotropia - development of an animal model .Invest Ophthalmol Vis Sci 1998; 39: S554.12. Ugrin MC, Molinari A. Desinsertion ofthe medial rectus following pterygiumsurgery. Strabismus 1999; 7: 147-52.13. Miyai T, Hara R, Nejima R, Miyata K,Yonemura T, Amano S. Limbal allograftamniotic membrane transplantation andintraoperative mitomycin C for recurrentpterygium. Ophthalmology 2005; 112: 1263-7.
Diplopic Mechanical Restrictive Strabismus Due To
Binocular Vision & Strabology Orbital Medial Wall Fracture and Medial Rectus Muscle Entrapment Second Quarter of 2012
Quarterly, Simm s Romano’s © Following Endoscopic Dacryocystorhinostomy Volume 27 (No.2)
A Medical Scientific ePeriodical A. Bagher i, MD, M. Tavakoli, MD and N. Rafaati, MD PAGES 122-128
-122-
Case Report, With Management and Outcome
Diplopic Mechanical Restrictive Strabismus due toOrbital Medial Wall Fracture and Medial Rectus MuscleEntrapment After Endoscopic Dacryocystorhinostomy,with Optic Nerve Deficit
ABBAS BAGHERI, M.D., MEHDI TAVAKOLI, M.D. andNASRIN RAFAATI, M.D.
From the Ophthalmic Research Center, Shahid Beheshti University of Medical Sciences, Tehran,Iran.
ABSTRACT: Purpose: To report a patient with medial rectus muscle entrapment as acomplication of endoscopic dacryocystorhinostomy (EDCR).
Method: A 34 year old female was referred with diplopia 18 days after EDCR for thetreatment of primary nasolacrimal duct obstruction. She had a large angle left exotropia inprimary position as well as a complete limitation of adduction and partial limitation of abductionof left eye. CT scan showed large fracture of the medial orbital wall in which the medial rectusmuscle was entrapped. She underwent multiple procedures in order to release the entrappedmuscle as well as management of the diplopia .
Result: Finally the patient had 10 PD exotropia in primary position but could fuse witha small face turn.
Conclusion: Orbital wall fracture with medial rectus extraocular muscle entrapment asa complication of EDCR should be kept in mind.
Received for consideration January 4, 2012; accepted for publication February 26, 2012.
Acknowledgment: The authors wish to thank M. Hadi Tavakoli MSc for his great role in theEnglish edition of the manuscript.
Correspondence to: Abbas Bagheri MD, Ophthalmic Research Center, Labbafinejad MedicalCenter, Pasdaran Ave. Boostan 9 St. Tehran, Iran. 16666, Fax: +98 21 22590607Email: [email protected]
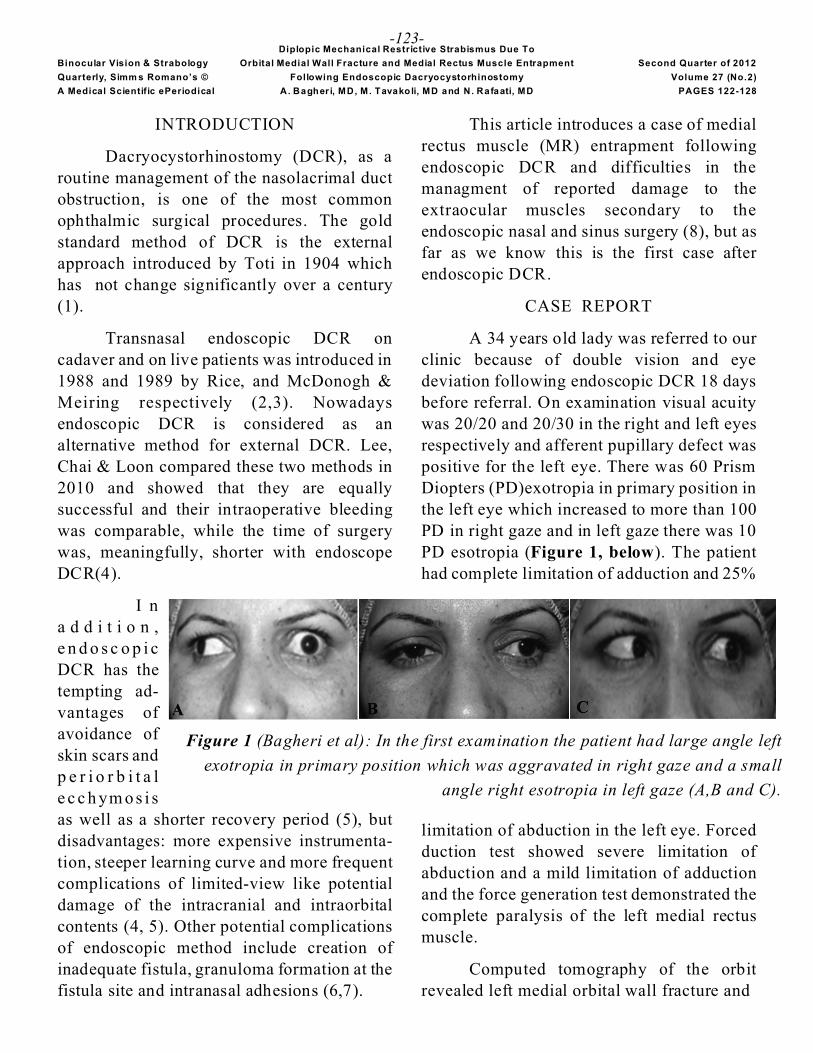
Diplopic Mechanical Restrictive Strabismus Due To
Binocular Vision & Strabology Orbital Medial Wall Fracture and Medial Rectus Muscle Entrapment Second Quarter of 2012
Quarterly, Simm s Romano’s © Following Endoscopic Dacryocystorhinostomy Volume 27 (No.2)
A Medical Scientific ePeriodical A. Bagher i, MD, M. Tavakoli, MD and N. Rafaati, MD PAGES 122-128
-123-
INTRODUCTION
Dacryocystorhinostomy (DCR), as aroutine management of the nasolacrimal ductobstruction, is one of the most commonophthalmic surgical procedures. The goldstandard method of DCR is the externalapproach introduced by Toti in 1904 whichhas not change significantly over a century(1).
Transnasal endoscopic DCR oncadaver and on live patients was introduced in1988 and 1989 by Rice, and McDonogh &Meiring respectively (2,3). Nowadaysendoscopic DCR is considered as analternative method for external DCR. Lee,Chai & Loon compared these two methods in2010 and showed that they are equallysuccessful and their intraoperative bleedingwas comparable, while the time of surgerywas, meaningfully, shorter with endoscopeDCR(4).
I na d d i t i o n ,e n d o s c o p i cDCR has thetempting ad-vantages ofavoidance ofskin scars andp e r i o r b i t a le c c h ym o s i sas well as a shorter recovery period (5), butdisadvantages: more expensive instrumenta-tion, steeper learning curve and more frequentcomplications of limited-view like potentialdamage of the intracranial and intraorbitalcontents (4, 5). Other potential complicationsof endoscopic method include creation ofinadequate fistula, granuloma formation at thefistula site and intranasal adhesions (6,7).
This article introduces a case of medialrectus muscle (MR) entrapment followingendoscopic DCR and difficulties in themanagment of reported damage to theextraocular muscles secondary to theendoscopic nasal and sinus surgery (8), but asfar as we know this is the first case afterendoscopic DCR.
CASE REPORT
A 34 years old lady was referred to ourclinic because of double vision and eyedeviation following endoscopic DCR 18 daysbefore referral. On examination visual acuitywas 20/20 and 20/30 in the right and left eyesrespectively and afferent pupillary defect waspositive for the left eye. There was 60 PrismDiopters (PD)exotropia in primary position inthe left eye which increased to more than 100PD in right gaze and in left gaze there was 10PD esotropia (Figure 1, below). The patienthad complete limitation of adduction and 25%
limitation of abduction in the left eye. Forcedduction test showed severe limitation ofabduction and a mild limitation of adductionand the force generation test demonstrated thecomplete paralysis of the left medial rectusmuscle.
Computed tomography of the orbitrevealed left medial orbital wall fracture and
Figure 1 (Bagheri et al): In the first examination the patient had large angle left
exotropia in primary position which was aggravated in right gaze and a small
angle right esotropia in left gaze (A,B and C).

Diplopic Mechanical Restrictive Strabismus Due To
Binocular Vision & Strabology Orbital Medial Wall Fracture and Medial Rectus Muscle Entrapment Second Quarter of 2012
Quarterly, Simm s Romano’s © Following Endoscopic Dacryocystorhinostomy Volume 27 (No.2)
A Medical Scientific ePeriodical A. Bagher i, MD, M. Tavakoli, MD and N. Rafaati, MD PAGES 122-128
-124-
Figure 2 (Bagheri et al): Axial (A) and coronal (B) CT scan of the orbit demonstrate the leftmedial orbital wall fracture and major entrapment of the medial rectus muscle.
medial rectus muscle entrapment in thefracture site of the left orbit (Figure2, above).
We repaired the medial wall fracture
Figure 3 (Bagheri et al): (A) Axial and
with a silastic sheet and released the entrapped(muscle via a medial canthal skin incisionFigure 3, see below).
(B) coronal CT following repair and release.

Diplopic Mechanical Restrictive Strabismus Due To
Binocular Vision & Strabology Orbital Medial Wall Fracture and Medial Rectus Muscle Entrapment Second Quarter of 2012
Quarterly, Simm s Romano’s © Following Endoscopic Dacryocystorhinostomy Volume 27 (No.2)
A Medical Scientific ePeriodical A. Bagher i, MD, M. Tavakoli, MD and N. Rafaati, MD PAGES 122-128
-125-
At the end of operation, we injected 20units of Dysport (botulinum toxin A) in theleft lateral rectus. The next day the exotropiadecreased to 25 PD and diplopia improvedsignificantly, but adduction was still severelylimited. With loss of the effect of botulinumtoxin after 6 months, the left exotropiaincreased to 50 PD again and the diplopiarecurred. The patient then underwent a secondsurgical procedure: split half tendontransposition of the medial half of the superiorand inferior rectus muscles to the medialrectus with 6 mm resection. Also the leftlateral rectus muscle was recessed 10 mm and20 units of Dysport injected again in thismuscle. After 3 months, the patient againdeveloped left exotropia of about 30 PD; sowe performed a third operation: a left lateralrectus disinsertion and released this muscleinto Tenon’s space after also cutting off about10 mm of its length (myectomy). We alsofixed the globe with a scleral traction suture tothe medial wall for 5 days after operation.Exotropia decreased to 10 PD and, for thefirst time, the patient could fuse in primaryposition with a small angle right face turn.This improvement in primary position wasobtained and accompanied by a near completeloss of abduction in addition to adduction(see Figure 4, below).
In addition to strabismus the patient haddecreased vision and positive afferentpupillary defect at presentation. Furtherevaluation showed optic atrophy and a deeparcuate superior visual field defect in the lefteye (Figure 5, below,). Vision and binocularalignment were stable after 6 months of thelast operation.
Figure 5 (Bagheri et al): Visual field of theleft eye demonstrates a deep arcuate scotomain the superior half of the field.
Figure 4 (Bagheri et al): One month after the last operation, the patient had small angle
exotropia at primary position but she was able to fuse with a small face turn (A,B and C).

Diplopic Mechanical Restrictive Strabismus Due To
Binocular Vision & Strabology Orbital Medial Wall Fracture and Medial Rectus Muscle Entrapment Second Quarter of 2012
Quarterly, Simm s Romano’s © Following Endoscopic Dacryocystorhinostomy Volume 27 (No.2)
A Medical Scientific ePeriodical A. Bagher i, MD, M. Tavakoli, MD and N. Rafaati, MD PAGES 122-128
-126-
DISCUSSION
Traumatic medial orbital wall fractureis less common than inferior orbital wallfracture but it can be seen even in a minororbital trauma and may be associated withmedial rectus muscle entrapment (8). Medialrectus entrapment is a known complication oforbital trauma and endoscopic surgeries ofparanasal sinuses (9) but, according to ourliterature search, medial rectus entrapment andtraumatic injury of the optic nerve have notever been reported following endoscopicDCR.
Occasionally, intranasal surgeries fortreatment of nasal polyps or anteriorethmoidectomy lead to MR damage (9). Inaddition, endoscopic sinus procedures,especially when performed on the middle andposterior ethmoidal air cells may increase therisk of injury to the extraocular musclesespecially medial rectus (10).
Although damage to the MR duringendoscopic sinus surgery is an uncommoncomplication (11), it should be consideredwhen the patient has diplopia after thisoperation and the adduction is limited.
The probable mechanisms for MRdamage during operation include directcutting of the muscle, damage to the nerve orvessels of the muscle, adhesion of the muscleto the adjacent tissues and finally entrapmentof the muscle in the defect of the orbital wall(12). In our patient, the positive forcedduction test in abduction and adduction was inbenefit of left MR entrapment and thecontracture of the left lateral rectus secondaryto exotropia. The mechanism for weakness offorce generation in left MR seemed to be thedamage to the motor nerves of the medialrectus or the damage to the myofibrils of the
MR itself.
Huang et al (11) classified the injuriesto the MR following endoscopic sinus surgeryinto 4 patterns:
In the first pattern the patient has largeexotropia and complete adduction limitationwhile the abduction is normal and themechanism is complete transection of themidportion of the medial rectus (paralyticpattern);
In the second pattern, in which theexotropia is moderate to severe and both theabduction and the adduction are defective, themechanism is contusion of the MR associatedwith MR entrapment (paralytic/ restrictivepattern);
In the third pattern, the patient has mildesotropia and severe abduction limitation, andits mechanism is pure MR entrapment withoutits contusion (restrictive pattern); and
The fourth pattern consists of a milddeviation of the eye secondary to musclecontusion but there is not entrapment or nervedamage (paretic pattern) (11). Our patient wassimilar to the second pattern, although theabduction was relatively good. Optic nervedamage suggests that the posterior fibers ofthe MR muscle may be involved consideringthe proximity of these fibers with the opticnerve. Because of the damage to the posteriorfibers of the medial rectus which is near theoptic nerve, damage to the optic nerve wasalso explained.
CT scan is an important tool toevaluate the bony defects of the orbit and theposition of the soft tissues in relation to bonyorbit. Sometimes exact evaluation of softtissues, especially extraocular muscles is not

Diplopic Mechanical Restrictive Strabismus Due To
Binocular Vision & Strabology Orbital Medial Wall Fracture and Medial Rectus Muscle Entrapment Second Quarter of 2012
Quarterly, Simm s Romano’s © Following Endoscopic Dacryocystorhinostomy Volume 27 (No.2)
A Medical Scientific ePeriodical A. Bagher i, MD, M. Tavakoli, MD and N. Rafaati, MD PAGES 122-128
-127-
possible because of hemorrhage and edema. Inthis condition MRI would be more helpful(13). MRI also can show the extent of thedamage to the muscles.
Most authors believe that in MR muscleentrapment early intervention is indicated(14). Smith et al believe that early surgery forthe fractures and muscle entrapment canprevent fibrosis of the muscle and help relievediplopia (15). Huang and colleagues (13)stated that early intervention (within 2-3weeks) for the muscle entrapment followingendoscopic sinus surgery is easier to performand may prevent fibrosis.
It is notable that in planning forstrabismus surgery after releasing theentrapped muscle, one has to wait for theparalysis to improve spontaneously beforedoing extensive procedures like transpositionsurgery. This protocol was considered in thiscase. Occasionally when the paralysis iscomplete, transposition is not enough and wehave to cripple the antagonist muscle, as wedid (16, 17).
CONCLUSION
In conclusion we suggest that orbitalwall trauma and medial rectus muscleentrapment and also concurrent optic nervedamage are included in the list of thecomplications of endoscopic DCR. Inaddition, in management of the patients withstrabismus following this condition, similar tothe entrapment following other endoscopicnasal and sinus procedures, one should try torelease the entrapped muscle immediately andremember that the muscle damage may havecomplex mechanisms which need anappropriate management.
REFERENCES
1. Toti A. Nuovo metodo conservatore di curaradicalle delle suppurazioni chronicle delsacco lacrimale. Clin Mod Firenze 1904;10:385-389.2. Rice DH. Endoscopic intranasaldacryocystorhinostomy results in fourpatients. Arch Otolaryngol Head Neck Surg1990;116:1061.3. McDonogh M, Meiring JH. Endoscopictransnasal dacr yocy storh inos tom y. JLaryngol Otol 1989; 103:585-7.4. Lee DW, Chai CH, Loon SC. Primaryexternal dacryocystorhinostomy versusprimary endonasal dacrycystorhinostomy: areview. Clin Experiment Ophthalmol 2010;38: 418-426.5 . E l i e R E . E n d o s c o p i cdacryocys torhinostom y. Curr OpinOtolaryngol Head Neck Surg 1999; 7:446. Fayet B, Racy E, Assouline M.Complications of standardized endonasaldacryocystorhinostomy with unciformectomy.Ophthalmology 2004;111:837-45.7. Sonkhya N, Mishra P.Endoscopictransnasal dacryocystorhinostomy with nasalmucosal and posterior lacrimal sac flap. JLaryngol Otol 2009;123: 320-6. Epub 2008Oct 28. 8. Hall LS, MD, Mccann JD, Goldberg RA, etal. Strabismus after orbital fractures and sinussurgery. In: Rosenbaum AL, Santiago AP,(eds). Clinical Strabismus Management,Principles and Surgical techniques.Philadelphia: W.B. Saunders, 1999:3199. Mirsky RG, Saunders RA. A case ofisolated medial wall fracture with medialrectus entrapment following seemingly trivialtrauma. J Pediatr Ophthalmol Strabismus1979;16:287-90.10. Rosenbaum AL, Astle WF. Superioroblique and inferior rectus muscle injuryfollowing frontal and intranasal sinus surgery.

Diplopic Mechanical Restrictive Strabismus Due To
Binocular Vision & Strabology Orbital Medial Wall Fracture and Medial Rectus Muscle Entrapment Second Quarter of 2012
Quarterly, Simm s Romano’s © Following Endoscopic Dacryocystorhinostomy Volume 27 (No.2)
A Medical Scientific ePeriodical A. Bagher i, MD, M. Tavakoli, MD and N. Rafaati, MD PAGES 122-128
-128-
J Pediatr Ophthalmol Strabismus 1985;22:194-202.11. Huang CM, Meyer DR, Patrinely JR,Soparkar CN, Dailey RA, Maus M, et al.Medial rectus muscle injuries associated withfunctional endoscopic sinus surgery:characterization and management. OphthalPlast Reconstr Surg 2003;19:25-37.12. Dunya IM, Salman SD, Shore JW.Ophthalmic complications of endoscopicethmoid surgery and their management. Am JOtolaryngol 1996; 17:32213. Shin GS, Demer JL, Rosenbaum AL. Highresolution, dynamic, magnetic resonanceimaging in complicated strabismus. J PediatrOphthalmol Strabismus 1996; 33: 282-90.14. Brannan PA, Kersten RC, Kulwin DR.Isolated medial orbital wall fractures with
medial rectus muscle incarceration. OphthalPlast Reconstr Surg 2006; 22:178-83.15.Smith B, Lisman RD, Simonton J, DellaRocca R. Volkmann's contracture of theextraocular muscles following blow outfracture. Plast Reconstructive Surg 1984;74:200-16.16. Velez FG, Thacker N, Britt MT, AlcornD, Foster RS, Rosenbaum AL. Rectus muscleorbital wall fixation: a reversible profoundweakening procedure. J AAPOS2004;8:473-80.17. Morad Y, Kowal L, Scott AB. Lateralrectus muscle disinsertion and reattachmentto the lateral orbital wall. Br JOphthalmol 2005; 89:983-5.

Binocular Vision & Strabology Lay Person Slit Lamp Detection of Ir itis in Absence of an Eye MD: Second Quarter of 2012
Quarterly, Simms R oma no's© Eva luation o f a Slit Lamp Mo del o f Ce lls and Flare Volume 27 (No.2)
A Medical Scientif ic ePeriodical R.W . Arno ld, MD , A.W . Arno ld, E. Eby and J . Alesh ire GALLEY PAGES 129-134
-129-
Original Scientific Article
Lay Person Slit Lamp Detection of Iritis in Absence ofan Eye MD: Test of a Portable Model of Cells and Flare
ROBERT W. ARNOLD, M.D, ANDREW W. ARNOLD, ERYN EBY, and JENNIFER ALESHIRE
From Ophthalmic Associates, Anchorage, Alaska
ABSTRACT: Background: Asymptomatic - or minimally so, eye conditions like uveitis,iritis, and glaucoma are silent stealthily blinding diseases, especially when present in children.The iritis that accompanies Juvenile Idiopathic or Rheumatoid Arthritis (JIA or JRA) ischaracteristically asymptomatic. Children with these must be examined regularly androutinely(see Reference 1 and Table) on an opthalmologic biomicroscopic slit lamp for themicroscopic cells (and aqueous flare) which occurr in the anterior chamber of the eye, signalingthe presence of iritis, and an immediate need for anti-inflammatory agents. Such an exam is alsoindicated when the so afflicted develop most any symptoms of a new or recurrent eye problem.
Slit lamp iritis determination remains challenging. It virtually requires a major, notportable, table mounted and expensive biomicroscope. And the examiner designated inschedules (1) is a trained ophthalmolgist,, an "Eye M.D.". Both.
There are times and places throughout the world where and when a slit lamp may beavailable but there is no Eye MD (or qualified ophthalmic technician or assistant) available ina timely manner to timely examine for iritis when such is needed as noted.
However, there are theoretical advantages if a parent could detect iritis in their J I A childif a slit lamp were available, if they had been trained to use it and recognize iritis cells and flare.
Methods: A portable model of varying iritis severity was developed. Parents of JIApatients were instructed on slit lamp use and then attempted to match unknown models of iritisseverity with known training models of varying concentrations of cells and flare.
Results: Twelve parents ranked the 5 unknowns with an average summed deviation fromexpected of 2.2 +/-2 grade levels (out of 12). This was a good and useful degree of training.
Conclusion: We were able to teach lay adults to match a model of iritis severity on a slitlamp. We would suggest that where needed, they could provide urgent and more convenient andfaster diagnosis and treatment of recurrent iritis and also augment recommended scheduled EyeMD screening for iritis in JIA patients providing an effectively higher level of care, quality oflife, and reduction in loss of vision for JIA victims at lower cost and greater facility for thepatients, their caregivers and society as a whole.
Received for consideration March 05, 2012; accepted for publication April 9, 2012.Presented as a poster at the annual meeting of the AAPOS, Orlando, Florida 2010.
Correspondence: Robert W. Arnold, M.D., Pediatric Ophthalmology and Strabismus, Ophthalmic Pediatrics,542 W 2nd Ave., Anchorage AK . Fax: 907-264-2687 Email: [email protected]
The authors, as of this time, have no financial interest in this work.
Binocular Vision & Strabology Lay Person Slit Lamp Detection of Ir itis in Absence of an Eye MD: Second Quarter of 2012
Quarterly, Simms R oma no's© Eva luation o f a Slit Lamp Mo del o f Ce lls and Flare Volume 27 (No.2)
A Medical Scientif ic ePeriodical R.W . Arno ld, MD , A.W . Arno ld, E. Eby and J . Alesh ire GALLEY PAGES 129-134
-130-
BACKGROUND
Asymptomatic - or minimally so, eyeconditions like uveitis, iritis and glaucoma aresilent stealthily blinding diseases, especiallywhen present in children. The iritis thataccompanies Juvenile Idiopathic orRheumatoid Arthritis (JIA or JRA) ischaracteristically asymptomatic. Childrenwith these must be examined regularly androutinely(see Reference 1 and Table) on anopthalmologic biomicroscopic slit lamp forthe microscopic cells (and aqueous flare)which occurr in the anterior chamber of theeye, signaling the presence of iritis, and animmediate need for anti-inflammatory agents.Such an exam is also indicated when the soafflicted develop most any symptoms of anew or recurrent eye problem.
Slit lamp iritis determination remainschallenging. It virtually requires a major, notportable, table mounted and expensivebiomicroscope. And the examiner designatedin schedules (1) is a trained ophthalmolgist,,an "Eye M.D.". Both.
There are times and places throughoutthe world where and when a slit lamp may beavailable but there is no Eye MD (or qualifiedophthalmic technician or assistant) availablein a timely manner to timely examine for iritiswhen such is needed as noted.
INTRODUCTION
How does one learn how to detect andgrade iritis? Iritis observation is difficultbecause patients are often exquisitelyphotophobic and the slit lamp adjustmentsmust be optimized in order to visualize 7micron white cells floating in the aqueoushumor. First-year ophthalmology residentswith patient mentors wait for days and weeks
to find exemplary clinical cases. Familyphysicians and Emergency Specialists havefar less opportunity to hone slit lamp skills.
The iritis that accompanies JuvenileIdiopathic Arthritis (JIA or JRA) ischaracteristically asymptomatic. Potentiallyblinding sequelae such as cataract, synechiaeand glaucoma can result from undetectediritis, or with excess corticosteroid therapy.Balancing short term side-effects with costand inconvenience, the American Academy ofPediatrics (AAP) and rheumatologists haveproduced scheduling guidelines for pediatricophthalmology slit lamp examinations for allsuspected JIA patients based on gender, ageand other factors (1).
A different, systemic/ocular condition,diabetes mellitus, previously requiredscheduled doctor and lab visits, whereascurrent home monitoring of serum glucoseaffords tighter therapeutic control andsubstantially less blindness.
We postulate better control andoutcomes for JI&RA iritis could result fromaugmenting (not supplanting) regularophthalmic exams by adding some homemonitoring of iritis severity.
Therefore, we developed a model forslit lamp grading of iritis. This study is a pilotstudy to determine whether we could teachparents, lay volunteers to accurately matchmodel severity using an eye slit lamp.
METHODS
With approval from IRB at ProvidenceHospital, parents and friends of JIA patientsparticipated in the initial assessment of amodel of iritis severity mounted on acommunity slit lamp. Each observed aneducational video about iritis and white cell

Binocular Vision & Strabology Lay Person Slit Lamp Detection of Ir itis in Absence of an Eye MD: Second Quarter of 2012
Quarterly, Simms R oma no's© Eva luation o f a Slit Lamp Mo del o f Ce lls and Flare Volume 27 (No.2)
A Medical Scientif ic ePeriodical R.W . Arno ld, MD , A.W . Arno ld, E. Eby and J . Alesh ire GALLEY PAGES 129-134
-131-
grading and then was familiarized with slitlamp adjustment and use in less than an hour.
Then, after consent, each observed amodel of iritis severity and attempted tomatch them to randomly assorted unknownsin a similar model.
Development of the Model:
Off-white, fine particulate matter wasfiltered, dissolved in purified water andtreated with ethanol to make a non-toxic,sterile suspension. From this, variedconcentrations were placed in small clearglass vials to approximate different grades ofiritis from grade 1 to grade 4 (highconcentration). An additional vial held purewater to represent grade zero aqueous humor.
Figure 1 (Arnold et al): Two iritis kits: top with labeled known concentrations of suspendedwhite particles (oak) and bottom with color-coded unknowns in nylon housing. Malleablewires suspend the kits from the forehead rest of any slit lamp.

Binocular Vision & Strabology Lay Person Slit Lamp Detection of Ir itis in Absence of an Eye MD: Second Quarter of 2012
Quarterly, Simms R oma no's© Eva luation o f a Slit Lamp Mo del o f Ce lls and Flare Volume 27 (No.2)
A Medical Scientif ic ePeriodical R.W . Arno ld, MD , A.W . Arno ld, E. Eby and J . Alesh ire GALLEY PAGES 129-134
-132-
Five vials were then placed in a kit that couldbe suspended from the forehead rest of anyslit lamp (Figure 1, prior page 131). Onetype of kit had the five vials labeled as to theconcentration (0-4), and a second was colorcoded to represent "unknowns". Aneducational video was made comparing actualslit lamp examinations of patients with iritis,to views of the model. See video at:
http://vimeo.com/robertarnold/homeiritiskit)
RESULTS
Twelve individuals, average age 42years, ranked all 5 unknowns at a slit lamp.The average summed deviation from expectedwas 2.2 +/- 2 grade levels, on a potential 12point spread, with 5 scoring a perfect 0, andthe worst scoring 4 (switching just twolevels). The average deviation for grade zeroiritis was just 0.2 grade levels (Figure 2, nextpage).
CONCLUSION
To our knowledge, there is no model ofclinical iritis for teaching, yet. Our proposedmethod of slit lamp familiarization, videoviewing and then observation of an iritismodel could enhance teaching about silt lampdetction of anter io r chamber cellconcentration.
Lay adults were able to reliably matchcorresponding varied concentrations ofsuspensions of fine, white particles in a modelresembling iritis. While their agreement wasnot perfect, these results encourage furtherinvestigations as to whether parents andfriends would be able to accurately grade iritisin JIA patients. A community service clinic,or organization such as the Lions Club, could
potentially maintain a slit lamp for family use.More frequent, lay monitoring of uveitismight afford an enhanced balance oftreatment and follow-up formal eyeexaminations.
REFERENCE
1. Cassidy J, Kivlin J, Lindsley C, NoctonJ. Ophthalmologic examinations in childrenwith juvenile rheumatoid arthritis. Pediatrics2006;117:1843-5.
Please see Table (from the AmericanAcademy of Pediatrics), page 134

Binocular Vision & Strabology Lay Person Slit Lamp Detection of Ir itis in Absence of an Eye MD: Second Quarter of 2012
Quarterly, Simms R oma no's© Eva luation o f a Slit Lamp Mo del o f Ce lls and Flare Volume 27 (No.2)
A Medical Scientif ic ePeriodical R.W . Arno ld, MD , A.W . Arno ld, E. Eby and J . Alesh ire GALLEY PAGES 129-134
-133-
Figure 2 (Arnold et al): Results of slit lamp comparisons by lay individuals of known andunknown iritis kits for 12 individuals who had watched an educational video, then familiarizedthemselves with slit lamp use in less than one hour.

Binocular Vision & Strabology Lay Person Slit Lamp Detection of Ir itis in Absence of an Eye MD: Second Quarter of 2012
Quarterly, Simms R oma no's© Eva luation o f a Slit Lamp Mo del o f Ce lls and Flare Volume 27 (No.2)
A Medical Scientif ic ePeriodical R.W . Arno ld, MD , A.W . Arno ld, E. Eby and J . Alesh ire GALLEY PAGES 129-134
-134-

Binocular Vision & Strabology ABSTRACTS SECO ND Quarter of 201 2
Quarterly, Simm s-Roman o’s© Volume 27 (No 2)
A Medical Scienti fic e-Periodical Pages135-136
-135-
Vision / Visual Acuity / Amblyopia
Abnormal Radial Deformation Hyperacuity inChildren with Strabismic Am blyopia.Subramanian V, Morale SE, Want Y-Z, BirchEE. Invest Ophthalmol Vis Sci 2012, April 24.[Authors Conclusions]
The demonstrated feasibility of radialdeformation stimuli for forced-choice preferentiallooking testing and the sensitivity and specificityof the small radius radial deformation hyperacuitystimulus for amblyopia support the potential toutilize this test to detect and monitor amblyopia ininfants and preschool children.([email protected])
School-Based Approaches to the Correction ofRefractive Error in Children. Sharma A,Congdon N, Patel M, Gilbert C. SurvOphthalmol 2012; 57:272-283. [AuthorsAbstract Condensed]
The World Health Organization estimatesthat 13 million children aged 5-15 yearsworldwide are visually impaired from uncorrectedrefractive error. ... School -based vision screeningcarried out by teachers, [etc may remedy this] ... .Barriers to [this]... include the cost and quality ofavailable refractive care and mistaken beliefsthat glasses will harm children’s eyes. Furtherresearch .. needed.. cost-effectiveness...and impactof education to promote acceptance... Schoolvision programs should be integrated intocomprehensive efforts to promote health childrenand their families. ([email protected])
Anisometropia in Children from Infancy to 15Years. Deng L. Gw iazda JE. InvestOphthalmol Vis Sci 2012 [Authors Conclusions]
The prevalence of anisometropia increasesbetween 5 and 15 years, when some children’seyes grow longer and become myopic. However,anisometropia was found to accompany bothmyopia and hyperopia, suggesting that othermechanisms in addition to excessive eye growthmay exist for anisometropia development,especially in hyperopia. (Dept Vision Science,New England College Optometry, 424 Beacon St,Boston MA 02115)
Push-Pull Training Reduces Foveal SensoryEye Dominance Within the Early VisualChannels. U JP, He ZJ, Ooi TL. Vis Res 2012;61:48-59 [Highlights from AAO Science Direct]
!Foveal sensory eye dominance (SED) isreduced by the push-pull training protocol. !Thepush-pull protocol excites the weak eye whileinhibiting the strong eye. !The learning effect(reduced SED) transfers within the sameorientation channel. !The learning effecttransfers to a spatial frequency 1 octave higherthan trained. !The learning also transfers to otheruntrained binocular tasks.
Strabismus Pathophysiology
Measuring the Accommodative Response witha Double-Pass System: Comparison with theHartmann-Shack Technique. Vis Res 2012;62:26-34 [AAOs Science Direct]
Highlights: !Accommodation responsewas measured with double-pass and Hartmann-Shack systems. !No significant differences werefound among metrics. !No significantdifferences were found in the results obtainedwith both techniques. !Slightly higheraccommodative responses than those previouslypublished were found in this study. !Double-passmight be a helpful tool for accommodativeresponse measurement based on retinal imagequality. [No Author Information]
Responses of Cells in the Midbrain Near-Response Area in Monkeys with Strabismus.Das VE. Invest Ophthalmol Vis Sci 2012; May3 [Author Abstract]
Purpose: To investigate whether neuronalactivity within the supraoculomotor area (SOA-monosynaptically connected to medial rectusmotonerurons and encode vergence angle) ofstrabismic monkeys was correlated with the angleof horizontal misalignment and therefore helps todefine the state of strabismus. Methods: Single-cell neural activity was recorded from SOAneurons in two monkeys with exotropia as theyperformed eye movement tasks during monocularviewing. Results: Horizontal strabismus anglevaried depending on eye of fixation (Dissociated

Binocular Vision & Strabology ABSTRACTS SECO ND Quarter of 201 2
Quarterly, Simm s-Roman o’s© Volume 27 (No 2)
A Medical Scienti fic e-Periodical Pages135-136
-136-
Horizontal Deviation) and the activity of SOAcells (n=35) varied in correlation with the angle ofstrabismus. Both near-response (cells that showedlarger firing rates for smaller angles of exotropia)and far-response (cells that showed lower firingrates for smaller angles of exotropia) cells wereidentified. SOA cells showed no modulation ofactivity with changes in conjugate eye position astested during smooth-pursuit thereby verifyingthat the responses were related to binocularmisalignment. SOA cell activity was also notcorrelated with change in horizontal misalignmentdue to A-patterns of strabismus. Comparison ofSOA population activity in strabismic animals andnormal monkeys (described in the literature) showthat both neural thresholds and neural sensitivitiesare altered in the strabismic animals compared tothe normals. Conclusions: SOA cell activity isimportant in determining the state of horizontalstrabismus possibly by altering vergence tone inextraocular muscle. The lack of correlated SOAactivity with changes in misalignment due to A/Vpatterns suggest that circuits mediating horizontalstrabismus angle and those that mediate A/Vpatterns are different. ([email protected]>
Related Neuro-Ophthalmology
Paroxysmal Tonic Upgaze in Normal Children:A Case Series and a Review of the Literature.Salmina C, Taddeo I, Falesi M, Weber P,Bianchetti M, Ramelli CP. Eu J PediatriNeurol, May 16, 2012 [Authors AbstractCondensed]
... neurodevelopmentally normal children...The duration... was highly variable:.. lastedbetween 3 s and 10 min in 50% of the cases, ...5 sto 30 min and long... 10 s to 2 h. The frequencyranged from one every 3 months to 10 per day. ...onset under 2 years of age,..eventual improvementand recovery, and impaired movementcoordination [in some]. (Dr. Mario Bianchetti,Dept Pediatrics, Mendrisio and BellinzonaHospitals and University of Bern, Switzerland).
Perception of Depth
Integration Time for the Perception of Depthfrom Motion Parallax. Nawrot M, Stroyan K.Vis Res 2012; 59:64-71 [from AAO Science
Direct Highlights]
!Perception of depth from motionparallax occurs with brief stimulus presentations(30ms). !A high-contrast pattern mask caninterrupt this with an SOA less than 70-75 ms.!The masking interval might be tied to thelatency of eye movement processing.!Mechanisms serving the perception of depthfrom motion parallax are not necessarilysluggish. [from Authors Abstract] ... that relativedepth discrimination can be performed withpresentations as brief as 16.6 ms, with only twostimulus frames providing both retinal imagemotion and the stimulus window motion forpursuit (mean range = 16.6-33.2 ms). ... neuralmechanisms serving depth from motion parallaxgenerate a depth estimate much more quicklythan previously believed. ... (Mark Nawrot,Center for Visual Neuroscience, DeptPsychology, North Dakota State University,Fargo ND 58108)
Binocular Vision / Eye Movements
Stereopsis and Binocular Rivalry are Based onPerceived rather than Physical Orientations.Chopin A, Mamassian P, Blake R. Vis Res2012; 63:63-68. [Highlights from AAO’sScience Direct]
!Orienta tion d ispari ty be tweendichoptically viewed lines can yield 3D slant. !Orientation disparities exceeding a limit producerivalry, not 3D slant,. !Illusory line tilt can beinduced by short lines placed on a long line(Zoollner). ! Illusory tilt influences disparitiesdefining the transition from slant to rivalry. !Rivalry and stereopsis rely on illusory rather thandisplayed orientations.
Reconsidering Yarbus: A Failure to PredictObservers’ Task from Eye Movement PatternsVis Res 2012; 62:1-8 [from AAOs ScienceDirect] Highlights: !Yarbus (1967)showed that eye movement patterns lookdifferent depending on task. !We used patternclassification to see if task could be predictedfrom eye movements. !Both classifiers andhuman observers failed to predict task.

Binocular Vision & Hyde Park Editorial B: ’B’LOG SECO ND Quarter of 2012
Strabology Quarterly S-r’s © Vo lum e 27 (No.2 ): A Medical Scienti fic EYE e-Periodical Pages: 137-152
- 137 -
HYDE PARK EDITORIAL: The Editor's Soapbox, Sandbox & B'LOG(Prehistoric) Since 1985
CONSCIENCE and CONSCIOUSNESS: Close Words,BUT R#1 is still Stereo 3D BV via the Egocenter; also:Cameron, SpecsX4, Brazil, Lying, Losing a +61% GAIN.
Stereoscopic 3 Dimensional depth perception vision remains
the Acme, Epitome and GOAL of all of both (monocular) vision and
Binocular Vision.
It’s the Very Foundation
of Ego-Centric Localization,
Your Very Own Cornerstone of
SPACE and your unique world
for you, and us, live in 3D.
Those first two words, “Conscience andConsciousness” are only a couple of inchesseparated in the dictionary. They even havevirtual equivalence in more remote “obsolete”meanings. But primary meanings differentiatewell: respectively: “right and wrong” versus;“awake, aware” But “conscience” is in the newsmuch lately, invaded by our president with thecudgel of insurance covering his anti-religious
anti religion intentions. The Catholic church and others cry “FOUL!” that this, his latest healthcare insuranceploy, is an incursion on CONSCIENCE. That conscience Is somehow sacred and inviolate as a deep inbornfeeling of right and wrong, that is therefore always RIGHT (for each person), as if it were virtually genetic.Maybe yes, some of those feelings are related to human individual and species survival, but... we think allthose deeply held “beliefs” are not genetic, not DNA... they are most or all epigenetic at the most, the resultof teaching and training, not as adults with choice, but as young children, choiceless, helpless subjects. Mostformative: Parents! Next, religion: And where do all the rapidly reproducing Muslims get their “conscience”:Those Madrassas, where they get compulsory intensive learning of the Quran, including who to hate and kill.I think they learned this technique from the Catholics, who, I understood, stood by the creed: “ Give me a childfor the first seven years of their life and we have them, for life.” Both literally and figuratively, as it turns out now;and they are still in denial at all the upper responsible levels: “U.S. Bishops Still Stonewall on Sex Abuse... TenYears after the ‘Dallas Charter’, church leaders keep dodging accountability.” by David Gibson, Wall StreetJournal, Friday June 8 2012 “Opinion” p.A13.Maybe the sexual revolution will provide a cure for this ancientwrong-doing. It’s very Uphill!, the Vatican missed it, opposes anyone fiddling with all their “rules” about sex.
Theoretically in most of the world you can pick and choose your religion, but when you’re indoctrinatedfrom early childhood and surrounded from then on, it ain’t easy.... and Religion has been with us forever,apparently, (“the opiate of the masses”) even though the basic human need for it seems to dissipate as ourknowledge and understanding of the universe expands. But as Morgan Liddick, a local columnist, recentlypointed out, Catholicism’s mission is concerned with ephemeral other worldly objectives (saving our souls) andcould care less about us other than reproducing Catholics. Similarly for Islam, with their rage extending to theirholy book. Some of it may be ebbing (and also is our society’s moral foundation) but you should see the $ fivemillion dollar church just completed in our little ski tourist mountain community...
Or is that just ?Evidence of conscious conscience?

Binocular Vision & Hyde Park Editorial B: ’B’LOG SECO ND Quarter of 2012
Strabology Quarterly S-r’s © Vo lum e 27 (No.2 ): A Medical Scienti fic EYE e-Periodical Pages: 137-152
- 138 -
Binocular Vision & Hyde Park Editorial B: ’B’LOG SECO ND Quarter of 2012
Strabology Quarterly S-r’s © Vo lum e 27 (No.2 ): A Medical Scienti fic EYE e-Periodical Pages: 137-152
- 139 -

Binocular Vision & Hyde Park Editorial B: ’B’LOG SECO ND Quarter of 2012
Strabology Quarterly S-r’s © Vo lum e 27 (No.2 ): A Medical Scienti fic EYE e-Periodical Pages: 137-152
- 140 -
Re prior pages: That amazing 3D Director- Producer Cameron is some venturesome guy. He did go down to the Titanic himself,to take some of those 3D pictures of the wreck. Most recently his submarine adventures were in NationalGeographic where he took his one man submarine down to the bottom (to take 3 D pictures) in that deepestplace in the ocean on earth, the Marianna’s trench 7 miles down, That’s more down than Mount Everest is Up!!!!
PS on egocenters: in the POV (egocenter Point ofView) like a map, there is only physical geography, NO people(other than the POV)..... because every other living thing has its own egocenter and-there would be conflicts?-there is no room for another universe?-other ideas?
The POV of your egocenter is the binoculus !!!!

Binocular Vision & Hyde Park Editorial B: ’B’LOG SECO ND Quarter of 2012
Strabology Quarterly S-r’s © Vo lum e 27 (No.2 ): A Medical Scienti fic EYE e-Periodical Pages: 137-152
- 141 -
3D TVs may soon be bargains:The above are stale, but the latest I had. But LOOK at that 42" LG at the bottom for less than $ 600. I paid almostthat much for my first 32" flat screen which only lasted a few weeks beyond the warranty. The current price isundoubtedly even lower. The newest TVs recently announced will probably be 3D but they will also be your new computer andinternet browser screen whenever you want it to be, and will in addition , like your auto system, respond to yourvoice commands and maybe also hand motions. I can hardly wait! I still cant stroke my latest camera screen veryadroitly when reviewing the pictures I have just taken, and my touch panel on the computer keyboard consistentlywants to translate anything that is not a perfect tactile touch into a signal to move all over the place, and to carryout somebody else’s (Bill Gates’) commands !!!!
Whoops, I see that X-Box, at least, has the hand signals already, and now can be adapted to act like yourinternet contact so I guess some people, especially gamers may have that already.
Whoops whoops: Wall Street Journal Tuesday 05 June 2012 B3: “...Smartglass” New Gaming...Will LetTablet or Phone stream Content to a Television (screen).” Apple is working on Airplay to work with theirexpected Apple TV.

Binocular Vision & Hyde Park Editorial B: ’B’LOG SECO ND Quarter of 2012
Strabology Quarterly S-r’s © Vo lum e 27 (No.2 ): A Medical Scienti fic EYE e-Periodical Pages: 137-152
- 142 -
H2.Strabology etcHow did we miss this? The crowding phenomenon is something we all learned very early in ophthalmology...If Uncrowding helps so much here (it almost looks like a cure for some parts of these disorders?), would it helpin the treatment of AMBLYOPIA ?!!! to say nothing of other types of reading and learning disabilities.....????
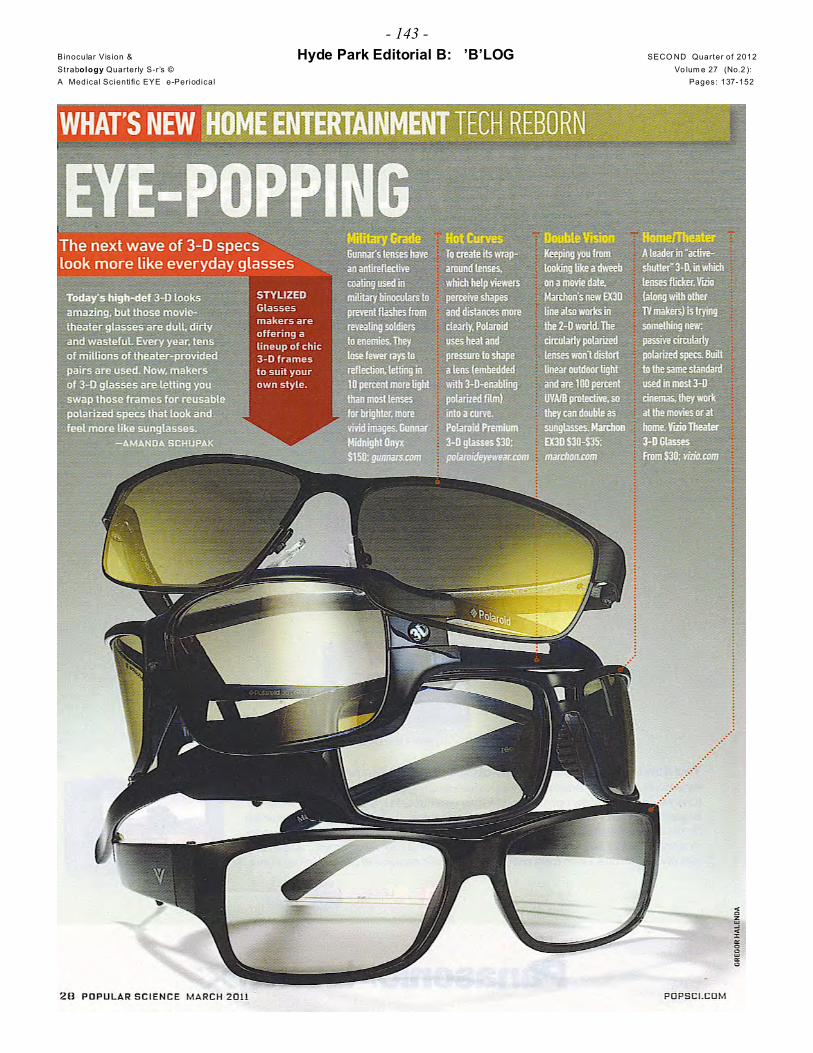
Binocular Vision & Hyde Park Editorial B: ’B’LOG SECO ND Quarter of 2012
Strabology Quarterly S-r’s © Vo lum e 27 (No.2 ): A Medical Scienti fic EYE e-Periodical Pages: 137-152
- 143 -

Binocular Vision & Hyde Park Editorial B: ’B’LOG SECO ND Quarter of 2012
Strabology Quarterly S-r’s © Vo lum e 27 (No.2 ): A Medical Scienti fic EYE e-Periodical Pages: 137-152
- 144 -
a decade ago, actually, 2000, I presented a paper at the annual Wilmer Eye Institute alumni meeting about theincreasing threat of anisometropia to binocular vision, especially the increasing side effect of various ophthalmicsurgical procedures on refraction...
To get the attention of my audience I mounted the speaker’s podium with a very miniature TV monitorI found somewhere that was about an inch or so cube, temporarily mounted to the outside corner of my eyeglasses frame, and started my talk by saying that here is the future of vision and binocular vision, pointing to thesmall TV device and describing it as a minute computer monitor.
I didn’t at the time realize how accurate that prediction was! This “viewfinder” (below) was in a recent issue of “Popular Mechanics, and in the lower right inset detail,
it uses the goggle frame to house a micro mini monitor in the lower frame optical projected into the field of view.This is intended for skiers so the goggle is a natural vehicle.
This was before... Google, and others did it for NOT skiers, but not “before” by much.

Binocular Vision & Hyde Park Editorial B: ’B’LOG SECO ND Quarter of 2012
Strabology Quarterly S-r’s © Vo lum e 27 (No.2 ): A Medical Scienti fic EYE e-Periodical Pages: 137-152
- 145 -
Right and right Below: Sergey Brin cofounder of Google wearing new Google spectacle frame which containsan internet computer, and the monitor, for which, the picture is by an optical system (see diagram on the next
page) displayed by reflection - like a“heads-up” pilot or driver display, onthe inside of the spectacle lens. Fromthe Wall Street Journal April 2 andMay22,2012.

Binocular Vision & Hyde Park Editorial B: ’B’LOG SECO ND Quarter of 2012
Strabology Quarterly S-r’s © Vo lum e 27 (No.2 ): A Medical Scienti fic EYE e-Periodical Pages: 137-152
- 146 -
Binocular Vision & Hyde Park Editorial B: ’B’LOG SECO ND Quarter of 2012
Strabology Quarterly S-r’s © Vo lum e 27 (No.2 ): A Medical Scienti fic EYE e-Periodical Pages: 137-152
- 147 -
Now we know why there is that new fad that started a year or so ago, for just wearing spectacle rims, with nolenses. Remember our neato headline:
“Rimless Glasses used to be the ne plus ultra, Now it is GLASS-LESS RIMS”
That was a secret campaign by Google and these other folks working on the aforementioned computer spectaclesbecause they knew people were going to have to wear an essentially naked spectacle frame to sell them to usetheir new device, which would require wearing spectacles all the time! Even the military is trying to make their spectacles less ugly!:
\ not Sergey but better....
Apple’s NEW Retina display: what’s that? Is appleinvading Ophthalmology????Not quite: but the new I pad has so many much morepixel resolution than prior devices, anybody’s! Numerically, it (the I pad screen) has 2 million morepixels than an HD TV screen. That is said or supposedlyis as high a resolution as the human retina (is that right?)And more important, at what viewed distance???”? thatinfo doesn’t seem available.... But that is why Steve andthey call it (and named it) a “retina display”. It is goingto be on the i-phone too...???? Reviews of the newscreen are quite positive....

Binocular Vision & Hyde Park Editorial B: ’B’LOG SECO ND Quarter of 2012
Strabology Quarterly S-r’s © Vo lum e 27 (No.2 ): A Medical Scienti fic EYE e-Periodical Pages: 137-152
- 148 -
We SCOOPED the WSJ by a quarter on this identical idea which ran in our last issue,or maybe OUR article was picked up and “copied” by them.....????
This article did recommend to make your smartphone camera even smarter anda good equal: These Three essential camera apps:
Camera+ : the effects masterHipstamatic: the analog spiritAwesome Camera: Everything but the kitchen sink.
Sounds like we are turning everyone into a professional photographer.Thanks to: we now have so much memory, you can save anything and everything? Andlike a pro, just save the knock-outs.Us older photogs know that Saving is more of a curse than a blessing.
But the youngest generation has nothing else to do: No jobs, no home, no moneyand the guys don’t even have any interest in cars. (See AGAIN our last issue here h9,“kids don’t want cars” page 79, also confirmed in the mass news today April 3,)
And the latest cameras capture all the light rays for infinite 3D !!!!
Nikon and Target disagree: they are still buying huge9x11 ! glossy print ads like this:
And these cover girls: (Right->) they alllook the same and they all look like all the starson the TV shows. They may not have the samemake up person and plastic surgeon, but they allfollow the same recipe. It’s confusing !
This one is from a feature in CR abuses ofadvertising. This is an ad for mascara, but the tinyfootnote says her luscious lashes are not hers orthe mascara but that ”lash inserts were added....”
NEXT PAGE: more looking and seeing.... Beauty IS NOW AGOVERNMENT RIGHT AND BENEFIT in Brazil!:The next page is an AP release. Is this the future of our world? As we saidin the lead editorial, is good looks now become another inalienable,government mandated and and subsidized human right ?

Binocular Vision & Hyde Park Editorial B: ’B’LOG SECO ND Quarter of 2012
Strabology Quarterly S-r’s © Vo lum e 27 (No.2 ): A Medical Scienti fic EYE e-Periodical Pages: 137-152
- 149 -

Binocular Vision & Hyde Park Editorial B: ’B’LOG SECO ND Quarter of 2012
Strabology Quarterly S-r’s © Vo lum e 27 (No.2 ): A Medical Scienti fic EYE e-Periodical Pages: 137-152
- 150 -
Note that there are twice as many factors on the side of “Increasing Dishonesty”than there are for “Decreasing”it! Also the “Decrease” factors are what OTHERS must impose upon you! I don’t’ see that’s there any roomat all for politicians in here. Especially when in the campaigning for office mode. Slightly better afterwards ?....But then the biggest and boldest liar I have ever come across in my life holds the office of U.S. President now.Some think lawyers go to law school to get washed of everything in the above diagram and when you get yourLLD Anything goes after that...except losing.. . And they do want to be the #1 and only real profession. That’swhy they are destroying our medical profession with all their laws and regulations. Life is their football it seems.Or” life IS all politics” as “it is for [BO]” (WSJ quote).

Binocular Vision & Hyde Park Editorial B: ’B’LOG SECO ND Quarter of 2012
Strabology Quarterly S-r’s © Vo lum e 27 (No.2 ): A Medical Scienti fic EYE e-Periodical Pages: 137-152
- 151 -
9. Public Safety, cars: DANGER: Imperial government gets worse and worse all the time. The
rest of this article was 3/4 of a full page, gave some history of this horror, but otherwise
was no help to defend yourself from this further abuse of government. Don’t Say NO (or
anything) more than you have to. Prepare to prove in court everything that you do say.
Ask for a lawyer now! Take the Fifth !? Say “I don’t remember... I don’t know”... If you
need an example, Roger Clemens is our current poster boy. Martha Stewart with her
serious jail time is our saint, our Joan of Arc. She was tried in the public media kangaroo
court and couldn’t disprove the accusations so she was guilty! Make the government
workers unhappy and they can do this to anybody....

Binocular Vision & Hyde Park Editorial B: ’B’LOG SECO ND Quarter of 2012
Strabology Quarterly S-r’s © Vo lum e 27 (No.2 ): A Medical Scienti fic EYE e-Periodical Pages: 137-152
- 152 -
9. Public service, safety, continued: “Protect Yourself at ALL TIMES”
FEELING poor? You’ve got lots of company: 99.44% OF US failed to protect themselves from OURGOVERNMENT INSTIGATED CRASH-DISASTER. WSJ noted Tuesday June 12, that the net worth ofAmericans in 2010 after the dust of the democrat government sponsored (Bill and Hillary and Barney) mortgagecrisis settled was down to $77,000. That was down from $124,000 in 2007 before the crisis, DOWN - 40%.(~43/124)But you have to invert the fraction to see the size of that government induced bubble: so that is 124 minus 77 =47 over 77= 47/77 = BUBBLE UP +61% = the TRUE size of the democrat’s unlawful idealogy created realestate bubble.... 61% is the VERY REAL LOSS you actually suffered and still feel because THAT’S HOW FARYOU THOUGHT YOU WERE AHEAD OF YOURSELF AND YOU WERE! THAT WAS CORRECT.+ 61%!
“Trust Me, Watch Out for Almost Everyone,” Music Teachers, osteopaths, cabbies. No Thanks. I’ll put my faith in cobblers and dental technicians....” by JoeQueenan,” Moving Targets”, column Wall Street Journal Saturday 02 June 2012.Pedestrian safety: NEXT: WATCH OUT FOR SCHOOL BUSES !!!
From the National Motorists Association Newsletter, December 25, 2011 by John Bowman, NMACommunications Director. The Numbers Tell the Story ... Again. “... stop-arm cameras on school buses.These systems are designed to photograph drivers who pass by stopped school buses while they load or unloadchildren. ... So how many Montgomery County school children were killed by careless motorists speeding byschool buses in 2009? None, according to NHTSA. Overall, there were two school bus-related pedestrianfatalities in Maryland in 2009, but those were caused by the bus. The article doesn’t mention that. Nationally,NHTSA fatality numbers for school bus/pedestrian fatalities exhibit a similar pattern over the last few years. So,from 2006-2009, 83% of school bus/pedestrian fatalities were caused by the bus.
Are Normally Sighted, Visually Impaired, and Blind Pedestrians Accurate and Reliable at Making StreetCrossing Decision? Hassan SE. Invest Ophthalmol Vis Sci 2012; 53:2593-2600 [Author’s Conclusions]
... visually impaired pedestrians can make accurate and reliable street crossing decisions like those ofnormally sighted pedestrians. When using auditory information only, all subjects significantly overestimated thevehicular gap time. Our finding that blind pedestrians performed significantly worse than either the normallysighted or visually impaired subjects under the hearing only condition suggested that they may benefit fromtraining to improve their detection ability and/or interpretation of vehicular gap times. [Ed: They should alsocarry and wave white walking sticks when crossing] [email author: [email protected]] -per