csam webinar on marijuana 7-23-14
TRANSCRIPT

Medicine Law
Public Health Public Policy
Clearing the Air: Marijuana's Effects on Health
Itai Danovitch, MD, MBA President, California Society of AddicBon Medicine
Chairman, Dept. of Psychiatry & Behavioral Neurosciences Cedars Sinai Medical Center

Overview & ObjecBves
• What impact does marijuana have on health? – Does marijuana have demonstrated medical benefits?
– Does marijuana have any significant harms?
– Is marijuana really addicBve?
• What impact does marijuana policy have on public health?

Disclosures
• Financial Conflicts of Interest – I have no relaBonships with enBBes producing, markeBng, re-‐selling,
or distribuBng health care goods or services consumed by, or used on, paBents.
• Off-‐Label Medica8ons
– There are no FDA approved medicaBons for the treatment of marijuana use disorders. Any medicaBon I discuss during this presentaBon is off label with respect to treatment of marijuana use disorder.

• Cannabis saBva
• Forms – Marijuana (0.5-‐5%) – Sinsemilla (7.5-‐14%) – Hashish (2-‐8%) – Hash oil (15-‐70%)
QuesBon 1: What is marijuana?

Mechoulam; Gaoni. A total synthesis of dl-‐D1-‐tetrahydrocannabinol, the acBve consBtuent of hashish. J Amer Chem Soc. 1965
30-‐80 cannabinoids

264
257
CB1
e1 e2
e3
i1 i2 i3
472 amino acids
174
179
CB2
e1 e2
e3
i1 i2
i3
Extracellular
360 amino acids
THC acts at cannabinoid receptors
Howlec AC. 2002. Pharmacol Rev. ClassificaBon of cannabinoid receptors
THC mimics anandamide
Devane; Mechoulam. 1992. Science. IsolaBon and structure of a brain consBtuent that binds to the cannabinoid receptor

Retrograde Signaling
Guzman-‐2003-‐Nature-‐Cannabinoids-‐ potenBal anBcancer agents
Presynap8c Neuron
Postsynap8c Neuron

CB1 receptors are widespread in the CNS

Endocannabinoid effects
• Mood • Sensory PercepBon • Memory • Arousal • AcenBon • ExecuBve funcBon • Psychomotor acBvity
• NocicepBon • AppeBte • GastrointesBnal • Stress reacBvity • Immune funcBon • ReproducBve physiology

Purified THC does not replicate effect of whole marijuana
Izzo. Mechoulam. 2009. TIPS. Non psychotropic plant cannabinoids: new therapeuBc opportuniBes from an ancient herb

• FDA/DEA: Schedule I A. The drug or other substance has a high potenBal for abuse.
B. The drug or other substance has no currently accepted medical use in treatment in the United States.
C. There is a lack of accepted safety for use of the drug or other substance under medical supervision.
QuesBon 2: Does marijuana have demonstrated medical benefits?
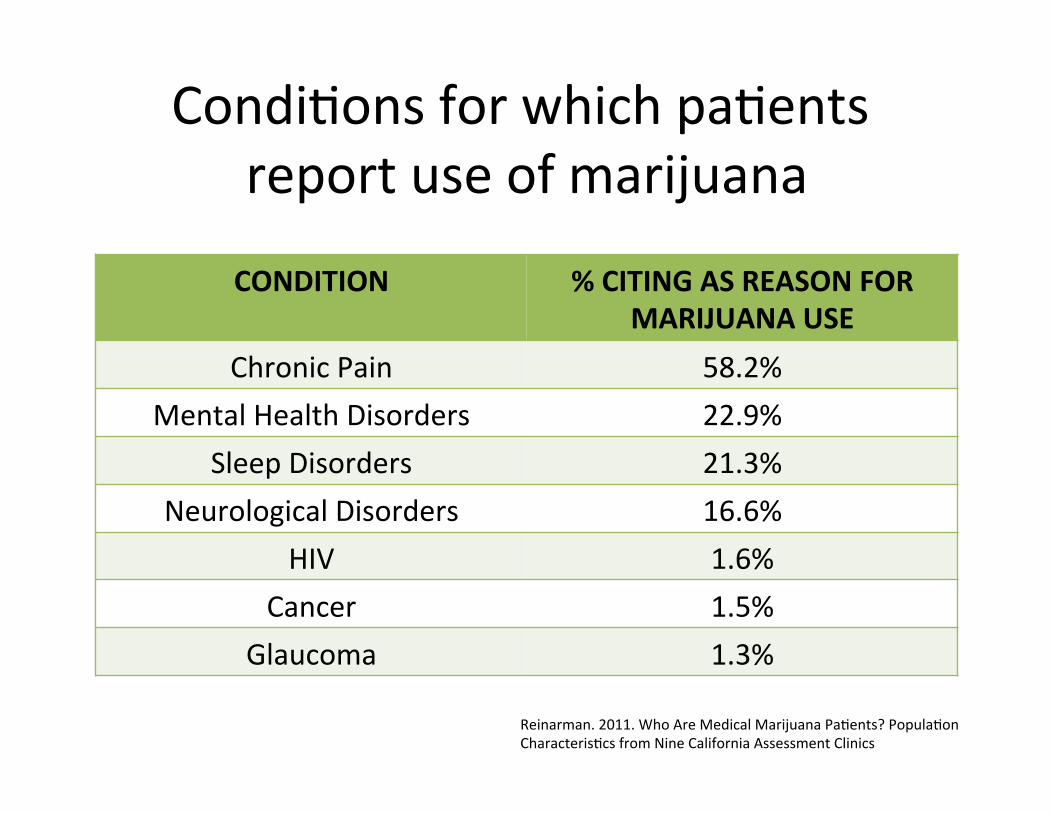
CondiBons for which paBents report use of marijuana
CONDITION % CITING AS REASON FOR MARIJUANA USE
Chronic Pain 58.2% Mental Health Disorders 22.9%
Sleep Disorders 21.3% Neurological Disorders 16.6%
HIV 1.6% Cancer 1.5%
Glaucoma 1.3%
Reinarman. 2011. Who Are Medical Marijuana PaBents? PopulaBon CharacterisBcs from Nine California Assessment Clinics

Safety and efficacy demonstrated in some condiBons
• Nausea • Emesis • Appe6te • Cachexia • Pain
1. Ben Amar. 2006. Cannabinoids In Medicine-‐ A Review Of Their TherapeuBc PotenBal-‐ 76 Studies 2. Grant. 2010. CMCR Report to the Legislature 3. hcp://medicalmarijuana.procon.org/view.resource.php?resourceID=000884#double ; 7-‐23-‐14
Peer-‐Reviewed Studies on Marijuana or Marijuana Extracts Pro Neutral Con Totals
Type of Study # of studies % of total # of studies % of total # of studies % of total # of studies % of total
I. Double-Blind Human Studies
12 54.54% 7 31.82% 3 13.64% 22 100%
II. Human Studies 24 30.38% 25 31.65% 30 37.97% 79 100%
TOTALS 36 35.64% 32 31.68% 33 32.67% 101 100%
• Spas6city • Seizures • Intraocular
pressure • Inflamma6on
• *HIV Associated Neuropathic Pain • *Chemotherapy associated toxicity • *MulBple Sclerosis SpasBcity • *Chronic Neuropathic Pain

Consensus Statements ü Purified THC does not replicate
whole marijuana ü Safety and efficacy in some
condiBons ü Physician & paBent protecBons ü Call for well-‐controlled research ü Call for re-‐scheduling
v Smoking is not a safe delivery system
v MedicaBons should be subject to approval process of FDA
v If prescribed, physicians must adhere to: – Good faith history & physical, treatment
planning, informed consent, monitoring, and documentaBon
– Adequate training, and consultaBon as necessary
1. NIH. 1997. Workshop on the Medical UBlity of Marijuana 2. IOM. 1998. Marijuana and Medicine: Assessing the Science
Base 3. ACP. 2008. SupporBng Research Into The TherapeuBc Role
Of Marijuana
1. AMA. 2009. House of Delegates Report 2. APA. 2013. PosiBon statement on Marijuana as Medicine 3. ASAM. 2010. Public policy statement on Medical Marijuana 4. AAAP. 2002. Medical Use of Marijuana
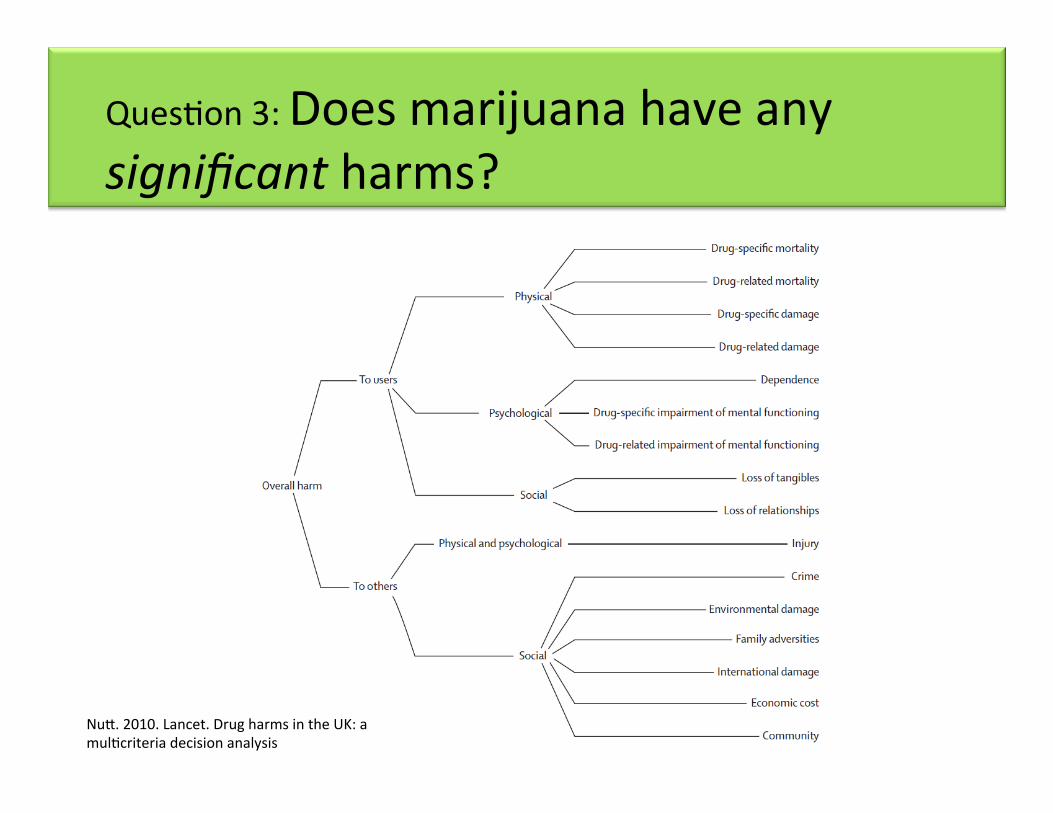
QuesBon 3: Does marijuana have any significant harms?
Nuc. 2010. Lancet. Drug harms in the UK: a mulBcriteria decision analysis

Social Risks
• EducaBonal acainment • School failure • Employment • OccupaBon • Income • Welfare dependence
*New Zealand birth cohort
1. Fergusson. 2008. Cannabis use and later life outcomes 2. Macleod. 2004. Lancet. Psychological and social sequelae of cannabis
and other illicit drug use by young people: a systemaBc review of longitudinal, general populaBon studies

Risk of PSYCHOSIS among high frequency users of marijuana
Risk of PSYCHOSIS among individuals who had ever used marijuana
Psychological Risks
1. Psychosis
2. Affect
3. AddicBon
Risk of DEPRESSION among high frequency users of marijuana
Risk of ANXIETY among high frequency users of marijuana
Moore. 2007. Lancet. Cannabis use and risk of psychoBc or affecBve mental health outcomes: a systemaBc review

Physical Risks
• Pulmonary • Cancer • Cardiac • ReproducBve
• Brain
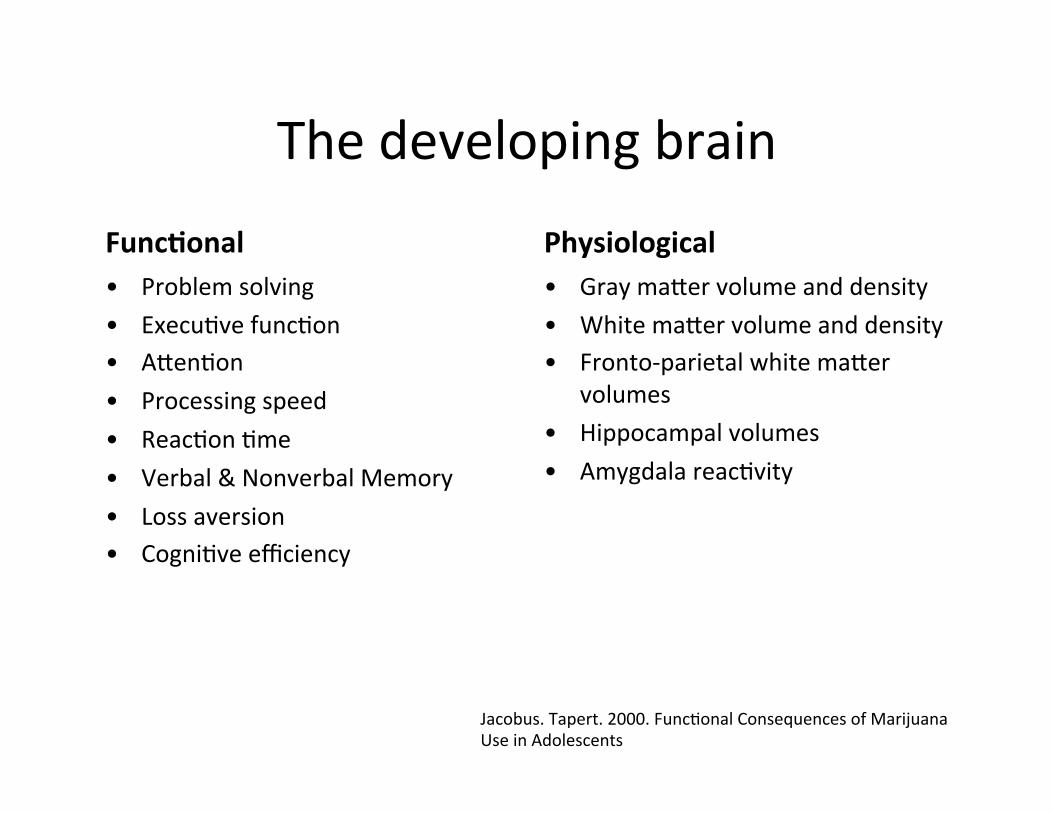
The developing brain
Func8onal • Problem solving • ExecuBve funcBon • AcenBon • Processing speed • ReacBon Bme • Verbal & Nonverbal Memory • Loss aversion • CogniBve efficiency
Physiological • Gray macer volume and density • White macer volume and density • Fronto-‐parietal white macer
volumes • Hippocampal volumes • Amygdala reacBvity
Jacobus. Tapert. 2000. FuncBonal Consequences of Marijuana Use in Adolescents

Marijuana dependence associated with change in IQ
Avg IQ (99.8 to 100.6)
Avg IQ (93.9 to 99.7)
Meier. 2012. Persistent cannabis users show neuropsychological decline from childhood to midlife

Risks to others • Impaired Driving
Asbridge. BMJ. 2012. Acute cannabis consumpBon and motor vehicle collision risk: systemaBc review of observaBonal studies and meta-‐analysis

• Impaired Driving
• Unresolved QuesBons – Complement vs Subs6tute – Accidental intoxica6ons – Second hand smoke
Risks to others

Nuc. 2010. Lancet. Drug harms in the UK: a mulBcriteria decision analysis

QuesBon 4: Is marijuana really addicBve?
• ProposiBon 19: SecBon 2—Findings, intent and purposes – A.5. “Cannabis is not physically
addic8ve, does not have long term toxic effects on the body...”

Evidence for Marijuana Use Disorder
1. Neurobiology 2. Pre-‐Clinical 3. Clinical 4. Epidemiology
Ventral tegmental area (VTA)
Nucleus accumbens
2008 NSDUH Survey 2008 NIDA Monitoring The Future
Common Presen8ng Symptoms • Inability to stop using (93%) • Feeling bad about use(87%) • ProcrasBnaBng (86%) • Loss of self confidence (76%) • Memory loss (67%) • Withdrawal symptoms (51%) Stephens et al. 1993. Adult marijuana users seeking treatment.
• LifeBme Use – 103.2 million people (42.4%) > 12 – 42% high school seniors
• Annual Use – 25.8 million people (10.6%) > 12 – 32.4% high school seniors
• Daily Use – 3.1 million people (1.3%) > 12 – 5% high school seniors
• Dependence – 8-‐9% of users – 17% of users <18

Chronic THC" Control"
Romero. 1997. Effect of chronic exposure to delta9-‐tetrahydrocannabinoloin cannabinoid receptor binding and mRNA levels in several rat brain regions.
Physical dependence

Budney. 2004. AJP. Review of the validity and significance of cannabis withdrawal syndrome
Withdrawal Symptoms • Common
– Aggression/ Anger – Restlessness – Decreased appeBte/ Weight loss – Sleep difficulBes/ Bad dreams – Irritability – Nervousness/Anxiety
• Less Common – Chills – Depressed Mood – Stomach Pain – Shakiness – SweaBng

Risk of having “any” mental health disorder
Comorbid disorder
Subjects with marijuana dependence Percent SE
Any mood disorder 60.5 2.8
Major depression 47.0 2.6 Dysthymia 20.3 2.4 Mania 23.6 2.5 Hypomania 10.2 1.7
Any anxiety disorder 48.5 2.7
Panic disorder with agoraphobia
8.8 2.0
Panic disorder without agoraphobia
13.7 1.6
Social phobia 21.3 2.3 Specific phobia 27.2 2.9 Generalized anxiety disorder
20.8 2.6
• Non-‐Dependent Frequent Users • OR = 5.35, P<.001
• Dependent Frequent Users • OR = 14.97, P<.001
Conway KP. 2006. JCP. LifeBme comorbidity of DSM-‐IV mood and anxiety disorders and specific drug use disorders: results from the NaBonal Epidemiologic Survey on Alcohol and Related CondiBons
VanDerPol. 2013. Mental health differences between frequent cannabis users with and without dependence and the general populaBon

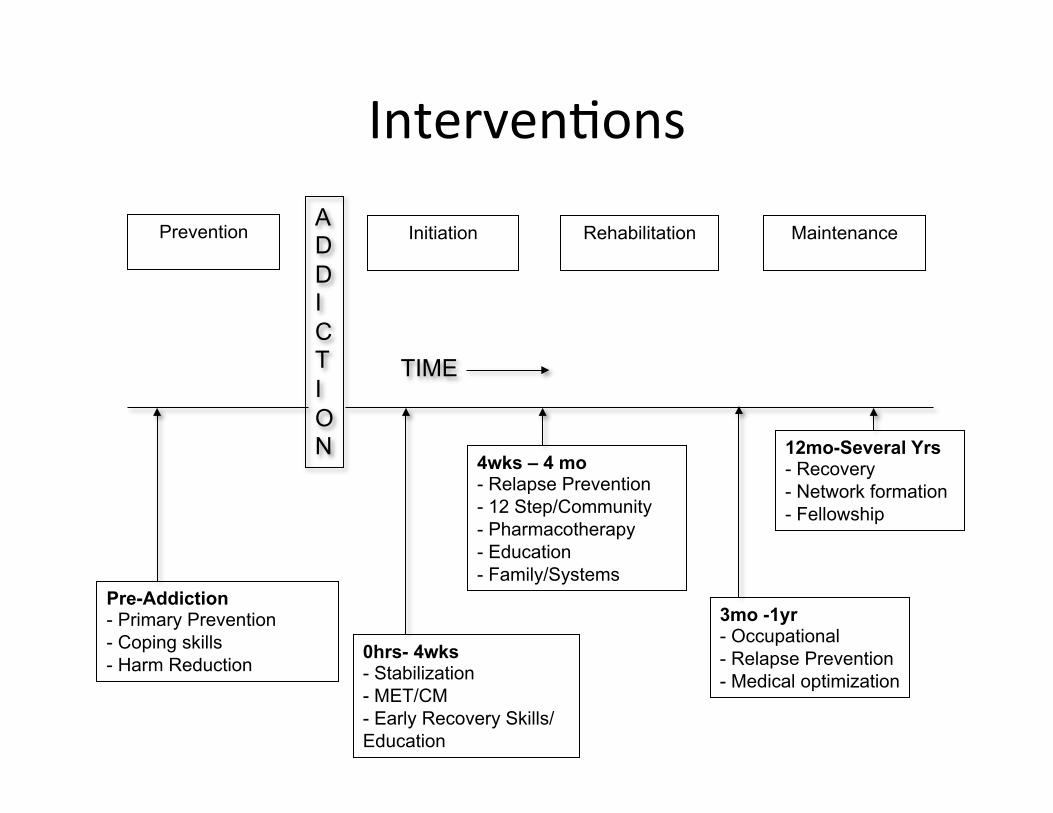
Maintenance
Pre-Addiction - Primary Prevention - Coping skills - Harm Reduction
0hrs- 4wks - Stabilization - MET/CM - Early Recovery Skills/ Education
4wks – 4 mo - Relapse Prevention - 12 Step/Community - Pharmacotherapy - Education - Family/Systems
12mo-Several Yrs - Recovery - Network formation - Fellowship
ADDICTION
Rehabilitation
TIME
3mo -1yr - Occupational - Relapse Prevention - Medical optimization
IntervenBons
Initiation
Prevention

QuesBon 5: What impact does marijuana policy have on public health?
CriminalizaBon LegalizaBon
Harms to Others
Harms to Users
Increased Use
IncarceraBon
Black Market
InterdicBon

Approval is increasing % favorin
g legalizaB
on, by gene
raBo
n

Availability is increasing

Use is increasing
NSDUH; Burns. 2013. StaBsBcs on cannabis users skew percepBons of cannabis use

Potency is increasing

Consumption Increased availability
Decreased price
Decreased percep8on of
risk Commodi8za8on
Special Interests
Conflicts of interest
ImplicaBons
RAND. Altered State? Assessing How Marijuana LegalizaBon in California Could Influence Marijuana ConsumpBon and Public Budgets. 2010.

Is there a middle ground?
CriminalizaBon LegalizaBon
Harms to others
Harms to users
Increased Use
IncarceraBon
Black Market
InterdicBon
?
PrevenBon
Harm reducBon
Public health

Natural experiments in drug policy
Uruguay
Central government
Price set to street value
($1)
Washington
State liquor control board
25% tax ($15)
Colorado
Dept. of revenue
Price set by market

Public Health Concerns I. PrevenBon
ü At-‐risk populaBons (youth; pregnancy; mental illness) II. Treatment
ü Access; Quality III. Product
ü Contents; Contaminants; Mis-‐labeling; MarkeBng IV. Industry
ü Oversight; Standards; Growth V. Monitoring
ü Impaired driving; SensiBve professions VI. Research
ü Document Impact of Policy VII. Revenue
ü Allocated first to address goals above
CSAM Statement on Marijuana LegalizaBon 2010

Medicine Law
Public Health Public Policy
Thank You
Itai Danovitch, MD President, California Society of AddicBon Medicine
Chairman, Dept. of Psychiatry & Behavioral Neurosciences Cedars Sinai Medical Center


APPENDIX

Reducing Harms to Public Health
Targets • Access and use by youth • Impaired driving • AddicBon • Contaminants, and
mislabeling • Concurrent use with alcohol • Public consumpBon
Strategies • Increase prices • Create state monopoly • Establish licensing • Restrict products • Restrict markeBng • Restrict public consumpBon • Measure and prevent
impaired driving
Pacula. 2014. Developing public health regulations for marijuana: lessons from alcohol and tobacco

IntervenBons
• Psychotherapy – Individual (MET; CBT; CM; SEP) – Group – Family/Systems (FSN; ACRA; MDFT)
• Pharmacotherapy – IntoxicaBon – Withdrawal – Relapse
• Community – EducaBon/PrevenBon – Self-‐help/12 Step – Sober Living/TherapeuBc Community
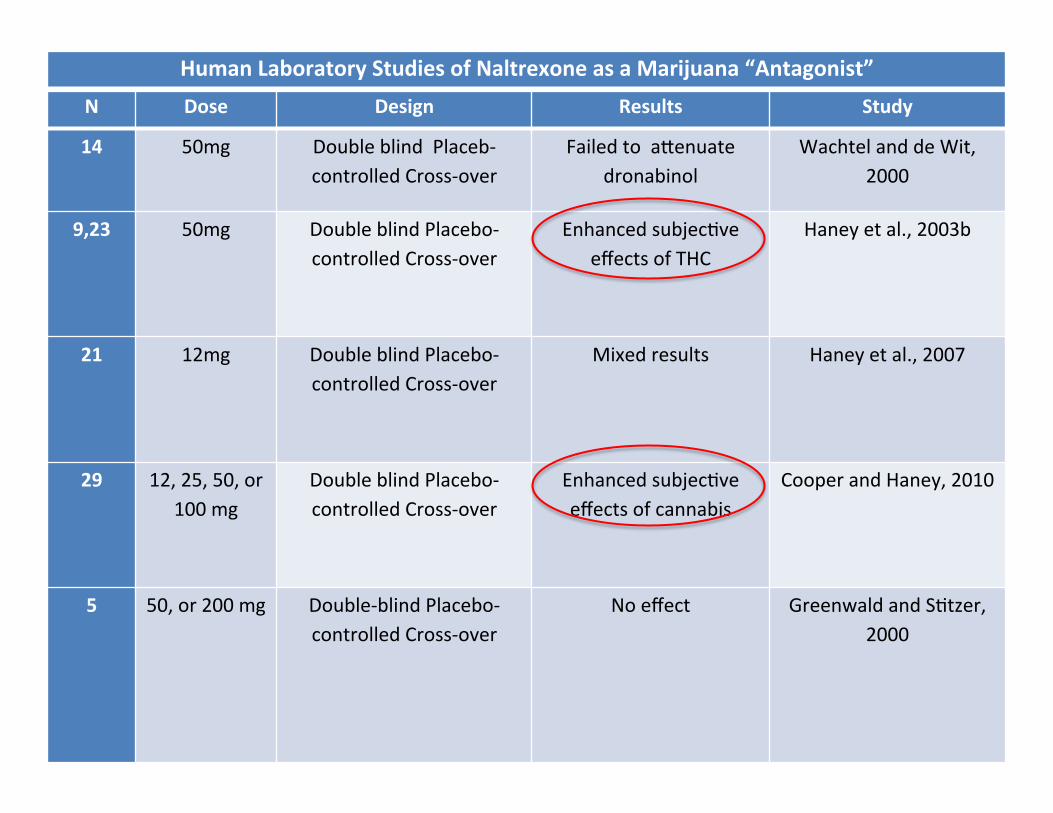
N Dose Design Results Study
14 50mg Double blind Placeb-‐controlled Cross-‐over
Failed to acenuate dronabinol
Wachtel and de Wit, 2000
9,23 50mg Double blind Placebo-‐controlled Cross-‐over
Enhanced subjecBve effects of THC
Haney et al., 2003b
21 12mg Double blind Placebo-‐controlled Cross-‐over
Mixed results Haney et al., 2007
29 12, 25, 50, or 100 mg
Double blind Placebo-‐controlled Cross-‐over
Enhanced subjecBve effects of cannabis
Cooper and Haney, 2010
5 50, or 200 mg Double-‐blind Placebo-‐controlled Cross-‐over
No effect Greenwald and SBtzer, 2000
Human Laboratory Studies of Naltrexone as a Marijuana “Antagonist”

Human studies of pharmacotherapy for marijuana withdrawal Human experimental laboratory studies
Bupropion 10 300mg Randomized Double-‐blind Placebo-‐controlled Cross-‐
over
Worsened withdrawal
Haney et al., 2001
Nefazodone 7 450mg Randomized Double-‐blind Placebo-‐controlled Cross-‐
over
Improved anxiety Haney et al., 2003a
Fluoxe8ne 22 20-‐40mg Randomized Double-‐blind Placebo-‐controlled Cross-‐
over
Reduced cannabis use
Cornelius et al., 2005
Baclofen or
Mirtazapine
11 30, 60, 90 mg
30mg
Randomized Double-‐blind Placebo-‐controlled Cross-‐
over
No effect Haney et al., 2010
Divalproex 7 1500mg Randomized Double-‐blind Placebo-‐controlled Cross-‐
over
Worsened withdrawal
Haney et al., 2004
Oral THC 11 10mg Randomized Double-‐blind Placebo-‐controlled cross-‐over
Reduced withdrawal Haney et al., 2004
Lofexidine+ THC 8 2.4mg 60mg Placebo-‐controlled Reduced withdrawal Haney et al., 2008
Outpa8ent clinical studies Oral THC 8 30, 90 mg Randomized Double-‐blind
Placebo-‐controlled Cross-‐over
Reduced withdrawal Budney et al., 2007
Lithium 9 600-‐900 mg Open label Reduced withdrawal Bowen et al., 2005
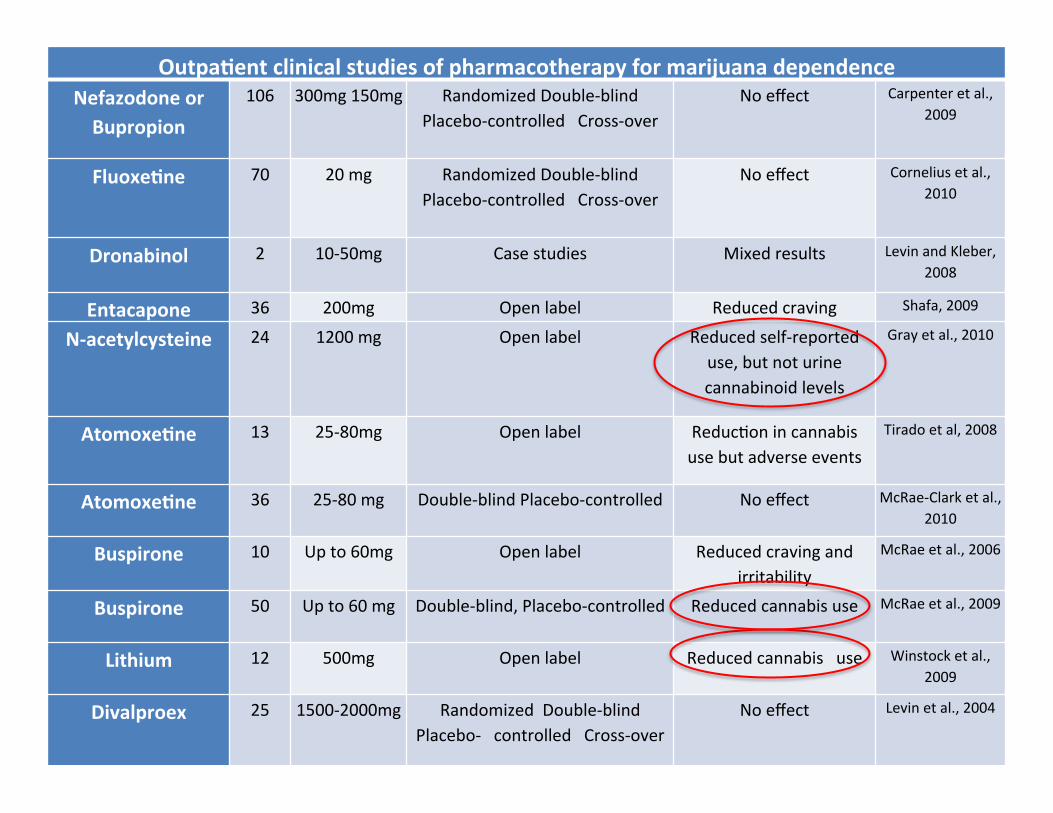
Outpa8ent clinical studies of pharmacotherapy for marijuana dependence Nefazodone or Bupropion
106 300mg 150mg Randomized Double-‐blind Placebo-‐controlled Cross-‐over
No effect Carpenter et al., 2009
Fluoxe8ne 70 20 mg Randomized Double-‐blind Placebo-‐controlled Cross-‐over
No effect Cornelius et al., 2010
Dronabinol 2 10-‐50mg Case studies Mixed results Levin and Kleber, 2008
Entacapone 36 200mg Open label Reduced craving Shafa, 2009
N-‐acetylcysteine 24 1200 mg Open label Reduced self-‐reported use, but not urine cannabinoid levels
Gray et al., 2010
Atomoxe8ne 13 25-‐80mg Open label ReducBon in cannabis use but adverse events
Tirado et al, 2008
Atomoxe8ne 36 25-‐80 mg Double-‐blind Placebo-‐controlled No effect McRae-‐Clark et al., 2010
Buspirone 10 Up to 60mg Open label Reduced craving and irritability
McRae et al., 2006
Buspirone 50 Up to 60 mg Double-‐blind, Placebo-‐controlled Reduced cannabis use McRae et al., 2009
Lithium 12 500mg Open label Reduced cannabis use Winstock et al.,2009
Divalproex 25 1500-‐2000mg Randomized Double-‐blind Placebo-‐ controlled Cross-‐over
No effect Levin et al., 2004

MedicaBon ImplicaBons
“B” THC replacement can reduce withdrawal symptoms
“B” Naltrexone is ineffecBve
“C” Lithium reduces withdrawal symptoms and decreases relapse
“C” Buspirone reduces withdrawal symptoms and relapse
“D” Mirtazapine no effect
“?” GabapenBn; QueBapine; N-‐Acetylcysteine

Psychotherapy For Cannabis Dependence
• Individual – MET – CBT – CM – SEP
• Group – MET – CBT
• Family and Systems – FSN – ACRA – MDFT
• Community – 12 Step – TC/SL

Findings • Many features in common
• Ambivalence tends to be high
• External reinforcers associated with early absBnence
• Skills acquisiBon and self-‐efficacy associated with maintenance
NCPIC. 2009. Management of cannabis use disorder and related issues

Therapy ImplicaBons
“A” Cannabis dependence can generally be treated in an outpaBent sezng, using MET/CBT
“A” The addiBon of CM to MET/CBT improves outcomes “B” ConBnued care and follow-‐up are vital “C” Comorbid dependencies are common and can be treated
simultaneously, e.g. nicoBne dependence with NRT “C” Courses of one to nine sessions have been tested with posiBve
results. OpBmum number of sessions is unknown

0 2 4 6 8
10 12 14 16 18 20
Met/Met Val/Met Val/Val
% with
schizoph
reniform
disorder at a
ge 26
COMT Genotype
no adolescent cannabis use adolescent cannabis use
Caspi. 2005. Biol. Psychiatry. ModeraBon of the effect of adolescent-‐onset cannabis use on adult psychosis by a funcBonal polymorphism in the catechol-‐O-‐methyltransferase gene
Adolescent Cannabis Use Increases the Risk for Adult Psychosis in GeneBcally Vulnerable Individuals
Maintenance
Pre-Addiction - Primary Prevention - Coping skills - Harm Reduction
0hrs- 4wks - Stabilization - MET/CM - Early Recovery Skills/ Education
4wks – 4 mo - Relapse Prevention - 12 Step/Community - Pharmacotherapy - Education - Family/Systems
12mo-Several Yrs - Recovery - Network formation - Fellowship
ADDICTION
Rehabilitation
TIME
3mo -1yr - Occupational - Relapse Prevention - Medical optimization
IntervenBons
Initiation
Prevention

Safety and efficacy demonstrated in some condiBons
DB-‐RCTs • HCV & Ca Chemotherapy
Toxicity • HIV Associated Neuropathic
Pain • Chronic Neuropathic Pain • MulBple Sclerosis SpasBcity
Consensus Statements ü Purified THC does not replicate
whole marijuana ü Safety and efficacy in some
condiBons ü Physician & paBent protecBons ü Call for research ü Call for re-‐scheduling
1. Koppel. 2014. SystemaBc Review-‐Efficacy and safety of medical marijuana in selected neurologic disorders
2. Hazekamp. 2010. Review on clinical studies with cannabis and cannabinoids 2005-‐2009
3. Grant. 2010. CMCR Report to the Legislature
1. Na8onal Ins8tute of Health (1997) Workshop on the Medical UBlity of Marijuana
2. Ins8tute of Medicine (1998) Marijuana and Medicine: Assessing the Science Base
3. American College of Physicians (2008) SupporBng Research Into The TherapeuBc Role Of Marijuana
4. American Medical Associa8on (2009) House of Delegates Report