craniofacial morphology and nasopharyngeal dimensions … 47-52 zetu ijmd 1-2013… · ·...
TRANSCRIPT

International Journal of Medical Dentistry 47
CRANIOFACIAL MORPHOLOGY AND NASOPHARYNGEAL DIMENSIONS IN MOUTH BREATHING PATIENTS
AbstractMaxillofacial structures and mouth breathing patients
constitute an especially interesting topic in orthodontic literature. The present study aims at determining the pos-sible correlations between the anteroposterior and vertical dimensions of the pharynx and the craniofacial morphol-ogy in these patients.
Materials and method. Prior to the orthodontic treat-ment, measurements were performed on 90 teleradiogra-phies of some children aged between 8 and 13, with Class I, II and III anomalies, after which the anteroposterior and vertical dimensions of the pharynx and the skeletal cranio-facial morphology were statistically compared.
Results and discussion. Correlations have been estab-lished between the nasopharyngeal and craniofacial variables. Nasopharyngeal depth increases in skeletal Class II- and decreases in skeletal Class III-cases, while the discrepancy is represented by either the ANB angle or AOBO value. No significant differences between ages were recorded.
Conclusions. Obstruction of the nasopharynx can be – in some specific cases – statistically significant, being related to a specific craniofacial morphology.
Keywords: craniofacial morphology, nasopharynx.
INTRODUCTION
The influence of oral breathing on the maxil-lofacial structures has been and continues to be a subject of special interest in orthodontic litera-ture [1,2]. In this respect, early noticing of any postnasal obstruction is very important [3]. Using a simple radiological film as a profile cephalometry, the orthodontist can accomplish a complete pharyngeal analysis, thus obtaining very precise information. On these films one can evaluate: the soft and hard palate and the posi-tion to the anterior arch of the atlas bone, the anteroposterior and vertical dimensions of the
CRANIOFACIAL MORPHOLOGY AND NASOPHARYNGEAL DIMENSIONS IN MOUTH BREATHING PATIENTS
Irina Nicoleta ZETU1, Raluca Maria MOCANU2, A. OGODESCU3, M.D. COBZEANU4, Adriana BĂLAN5
1. Assoc.Prof.,Dept.OrthodonticsandDentofacialOrthopedics,“Gr.T.Popa”UniversityofMedicineandPharmacy,Iaşi2. Res.PhDStudent,Dept.OrthodonticsandDentofacialOrthopedics,“Gr.T.Popa”UniversityofMedicineandPharmacy,Iaşi3. Lecturer,Dept.Paedodontics-Orthodontics,“VictorBabeş”UniversityofMedicineandPharmacy,Timişoara4. Assoc.Prof.,“Gr.T.Popa”UniversityofMedicineandPharmacy,Iaşi5. Assoc.Prof.,Dept.Paedodontics,“Gr.T.Popa”UniversityofMedicineandPharmacy,IaşiCorresponding author: Raluca Maria Mocanu, e-mail: [email protected]
nasopharynx, the quantity and distribution of the nasal polyps [4]. Also, the craniofacial mor-phology, the dimension and position of the skel-etal bases, the position and relation of maxilla and mandible in both anteroposterior and verti-cal plane can be visualized on the cephalometry. The radiological structures allow pharynx’ exploration from the cave to the laringopharynx. The radiological image of the pharynx, of longi-tudinal transparency, assures projection from the cranial basis to the sixth cervical vertebra. The aim of this study was therefore to statistically compare the anteroposterior and vertical dimen-sions of the pharynx and the skeletal craniofacial morphology in mouth breathing patients.
MATERIALS AND METHOD
The study was developed on 90 pre-treatment teleradiographies of mouth-breathing patients aged between 8-13, with no difference of race or sex. For statistical analysis, the boys received number 1 and the girls – number 2. According to the 90 teleradiographies, 30 patients presented class I malocclusion, 30 – class II malocclusion and the remaining 30 – class III malocclusion. Selection of the skeletal class was made by the AOBO value:
• Class I- AOBO between –2 mm and +2 mm• Class II- AOBO > +2 mm• Class III- AOBO < – 2 mmFilm analysis made use of 18 points and 5 lines
and planes, as described in figures 1 and 2.
Orthodontics
48 volume 3 • issue 1 January / March 2013 • pp. 47-52
Irina Nicoleta Zetu, Raluca Maria Mocanu, A. Ogodescu, M.D. Cobzeanu, Adriana Bălan
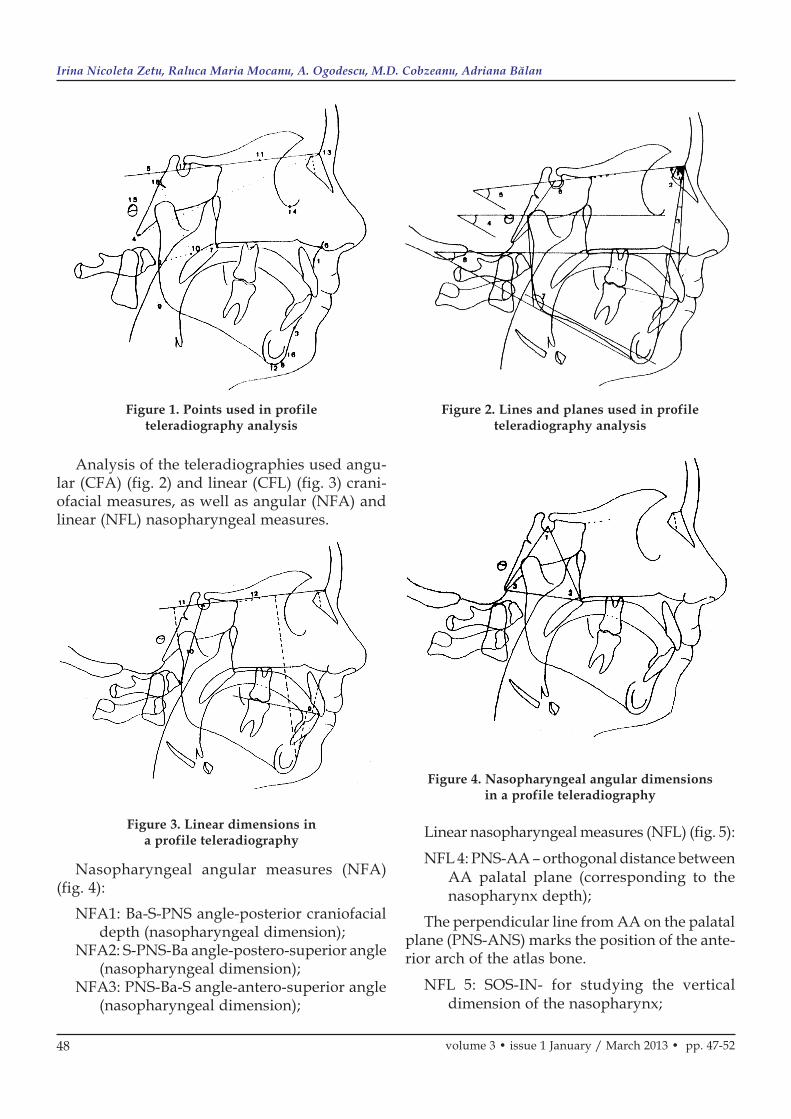
Analysis of the teleradiographies used angu-lar (CFA) (fig. 2) and linear (CFL) (fig. 3) crani-ofacial measures, as well as angular (NFA) and linear (NFL) nasopharyngeal measures.
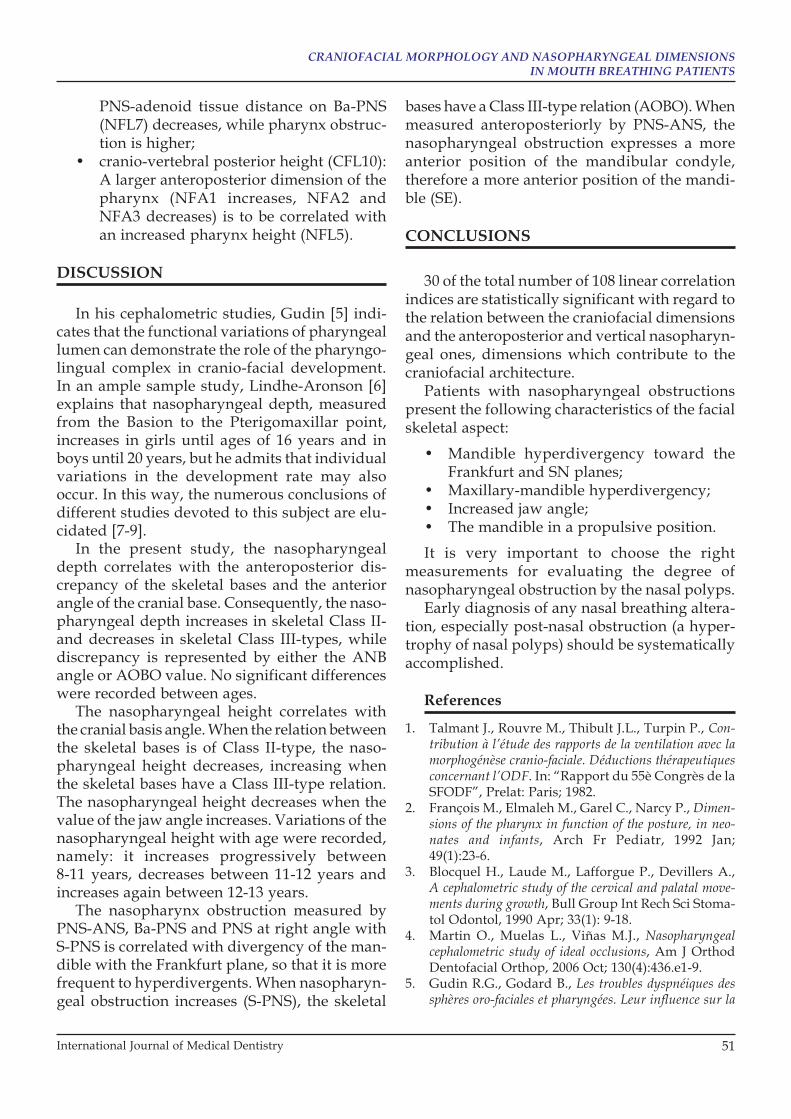
Figure 3. Linear dimensions in a profile teleradiography
Nasopharyngeal angular measures (NFA) (fig. 4):
NFA1: Ba-S-PNS angle-posterior craniofacial depth (nasopharyngeal dimension);
NFA2: S-PNS-Ba angle-postero-superior angle (nasopharyngeal dimension);
NFA3: PNS-Ba-S angle-antero-superior angle (nasopharyngeal dimension);
Figure 4. Nasopharyngeal angular dimensions in a profile teleradiography
Linear nasopharyngeal measures (NFL) (fig. 5):NFL 4: PNS-AA – orthogonal distance between
AA palatal plane (corresponding to the nasopharynx depth);
The perpendicular line from AA on the palatal plane (PNS-ANS) marks the position of the ante-rior arch of the atlas bone.
NFL 5: SOS-IN- for studying the vertical dimension of the nasopharynx;
Figure 1. Points used in profile teleradiography analysis
Figure 2. Lines and planes used in profile teleradiography analysis

International Journal of Medical Dentistry 49
CRANIOFACIAL MORPHOLOGY AND NASOPHARYNGEAL DIMENSIONS IN MOUTH BREATHING PATIENTS
Perpendicular line from SOS on the BANA plane, until the PNS-AA line; this point repre-sents the inferior skeletal nasopharynx limit of this plane.
NFL6: AD0 – distance between PNS and the closest adenoid tissue measured on the PNS-ANS line;
NFL7: AD1 – distance between PNS and the closest adenoid tissue measured on the Ba-PNS line;
NFL8: AD2 – distance between PNS and the closest adenoid tissue measured on the perpendicular line from PNS to S-Ba;
NFL9: AD3 – distance between PNS and the closest adenoid tissue measured on the S-PNS line.
NFL6, NFL7, NFL8 and NFL9 measure the pharyngeal obstruction on various levels; if these distances decrease, the degree of obstruc-tion is higher.
20 quantitative variables (11 craniofacial measures and 9 nasopharyngeal measures) and a qualitative variable (sex) have been introduced in the study.
Figure 5. Nasopharyngeal size linearly measured in a profile teleradiography
The tests performed for the statis tical analysis of the results were: Student, Kruskal-Wallis or Mann-Whitney, X2 or Fischer, non-parametric Kendall tests, as well as para metric Pearson tests. Table 1 summarizes the descriptive study of the variables.
Table 1. Descriptive study of the variables

50 volume 3 • issue 1 January / March 2013 • pp. 47-52
Irina Nicoleta Zetu, Raluca Maria Mocanu, A. Ogodescu, M.D. Cobzeanu, Adriana Bălan
RESULTS
Table 2 summarizes the correlations between nasopharyngeal and craniofacial variables.
Correlations between nasopharynx and:• discrepancy of bases expressed by the
ANB angle (CFA3): when the ANB angle increases, both the anteroposterior dimen-sion of the pharynx (NFA1) and the naso-pharyngeal depth (NFL4) increase;
• discrepancy of bases expressed by the AOBO distance (CFL9): when the AOBO distance increases, the nasopharyngeal depth (NFL4) increases, too. Also, the dis-tance between the closest adenoid tissue measured on S-PNS (NFL9) and pharynx obstruction is reduced;
• anterior angle of the cranial basis (CFA6): when this angle is augmented, the antero-posterior dimension and the depth of the pharynx also increase, however the height is diminished.
• the anteroposterior position of the mandi-ble –SE (CFL11): when the SE value is higher (the mandible is in anterior posi-tion), the depth of the nasopharynx increases (NFL4 and NFL1 increase; NFA3 decreases); when the distance between PNS
and the closest adenoid tissue measured on the PNS-ANS line (NFL6) is reduced, pharynx obstruction is increased.
Correlations between nasopharynx measure-ments and:
• the vertical direction expressed by the FMA angle (CFA4): when the FMA angle increases (significant hyperdivergency), the PNS-adenoid tissue distance measured on both PNS-ANS and Ba-PNS is reduced, pharynx obstruction is significantly higher, and both the anteroposterior dimen sion (NFA1) and pharynx depth (NFL4) decrease;
• the vertical direction expressed by the GoGn/SN angle (CFA5): when the GoGn/SN angle increases (significant hyper-divergency), the PNS-adenoid tissue dis-tance (measured on both PNS-ANS and Ba-PNS) is reduced, while the degree of pharynx obstruction is higher;
• jaw angle (CFA7): when the jaw angle increases, the vertical dimension of the pharynx (NFL5) decreases, the PNS-ade-noid tissue distance on PNS-ANS (NFL6), Ba-PNS (NFL7) and S-PNS (NFL9) is reduced and pharynx obstruction is higher;
• maxillary-mandible divergence angle (CFA8): when this angle increases, the
Table 2. Correlations between nasopharyngeal and craniofacial variables
International Journal of Medical Dentistry 51
CRANIOFACIAL MORPHOLOGY AND NASOPHARYNGEAL DIMENSIONS IN MOUTH BREATHING PATIENTS
PNS-adenoid tissue distance on Ba-PNS (NFL7) decreases, while pharynx obstruc-tion is higher;
• cranio-vertebral posterior height (CFL10): A larger anteroposterior dimension of the pharynx (NFA1 increases, NFA2 and NFA3 decreases) is to be correlated with an increased pharynx height (NFL5).
DISCUSSION
In his cephalometric studies, Gudin [5] indi-cates that the functional variations of pharyngeal lumen can demonstrate the role of the pharyngo-lingual complex in cranio-facial development. In an ample sample study, Lindhe-Aronson [6] explains that nasopharyngeal depth, measured from the Basion to the Pterigomaxillar point, increases in girls until ages of 16 years and in boys until 20 years, but he admits that individual variations in the development rate may also occur. In this way, the numerous conclusions of different studies devoted to this subject are elu-cidated [7-9].
In the present study, the nasopharyngeal depth correlates with the anteroposterior dis-crepancy of the skeletal bases and the anterior angle of the cranial base. Consequently, the naso-pharyngeal depth increases in skeletal Class II- and decreases in skeletal Class III-types, while discrepancy is represented by either the ANB angle or AOBO value. No significant differences were recorded between ages.
The nasopharyngeal height correlates with the cranial basis angle. When the relation between the skeletal bases is of Class II-type, the naso-pharyngeal height decreases, increasing when the skeletal bases have a Class III-type relation. The nasopharyngeal height decreases when the value of the jaw angle increases. Variations of the nasopharyngeal height with age were recorded, namely: it increases progressively between 8-11 years, decreases between 11-12 years and increases again between 12-13 years.
The nasopharynx obstruction measured by PNS-ANS, Ba-PNS and PNS at right angle with S-PNS is correlated with divergency of the man-dible with the Frankfurt plane, so that it is more frequent to hyperdivergents. When nasopharyn-geal obstruction increases (S-PNS), the skeletal
bases have a Class III-type relation (AOBO). When measured anteroposteriorly by PNS-ANS, the nasopharyngeal obstruction expresses a more anterior position of the mandibular condyle, therefore a more anterior position of the mandi-ble (SE).
CONCLUSIONS
30 of the total number of 108 linear correlation indices are statistically significant with regard to the relation between the craniofacial dimensions and the anteroposterior and vertical nasopharyn-geal ones, dimensions which contribute to the craniofacial architecture.
Patients with nasopharyngeal obstructions present the following characteristics of the facial skeletal aspect:
• Mandible hyperdivergency toward the Frankfurt and SN planes;
• Maxillary-mandible hyperdivergency;• Increased jaw angle;• The mandible in a propulsive position.It is very important to choose the right
measure ments for evaluating the degree of nasopharyngeal obstruction by the nasal polyps.
Early diagnosis of any nasal breathing altera-tion, especially post-nasal obstruction (a hyper-trophy of nasal polyps) should be systematically accomplished.
References
1. Talmant J., Rouvre M., Thibult J.L., Turpin P., Con-tribution à l’étude des rapports de la ventilation avec la morphogénèse cranio-faciale. Déductions thérapeutiques concernant l’ODF. In: “Rapport du 55è Congrès de la SFODF”, Prelat: Paris; 1982.
2. François M., Elmaleh M., Garel C., Narcy P., Dimen-sions of the pharynx in function of the posture, in neo-nates and infants, Arch Fr Pediatr, 1992 Jan; 49(1):23-6.
3. Blocquel H., Laude M., Lafforgue P., Devillers A., A cephalometric study of the cervical and palatal move-ments during growth, Bull Group Int Rech Sci Stoma-tol Odontol, 1990 Apr; 33(1): 9-18.
4. Martin O., Muelas L., Viñas M.J., Nasopharyngeal cephalometric study of ideal occlusions, Am J Orthod Dentofacial Orthop, 2006 Oct; 130(4):436.e1-9.
5. Gudin R.G., Godard B., Les troubles dyspnéiques des sphères oro-faciales et pharyngées. Leur influence sur la

52 volume 3 • issue 1 January / March 2013 • pp. 47-52
Irina Nicoleta Zetu, Raluca Maria Mocanu, A. Ogodescu, M.D. Cobzeanu, Adriana Bălan
morphologie craniofaciale et leur rapport avec la posture mandibulaire en période de croissance, Rev. Orthop. Dento Faciale, 1989; 23(4):407-425.
6. Linder-Aronson S., Henrikson C.O., Radiocephalo-metric analysis of anteroposterior nasopharyngeal dimen-sions in 6-to 12-year-old mouth breathers compared with nose breathers, ORL J Otorhinolaryngol Relat Spec, 1973; 35(1):19-29.
7. Poole M.N., Engel G.A., Chaconas S.J., Nasopharyn-geal cephalometrics, Oral Surg Oral Med Oral Pathol, 1980 Mar; 49(3):266-71.
8. Tourné L.P., Growth of the pharynx and its physiologic implications, Am J Orthod Dentofacial Orthop, 1991 Feb; 99(2):129-39.
9. Mihail Dan Cobzeanu, Vasile Costinescu, Course of Ear, Nose and Throat Diseases, Vasiliana ’98 Publish-ing House, 2001, ISBN 973-8148-22-5.