cps council presentation may 2016
TRANSCRIPT

Community Pharmacy ScotlandCouncil Meeting May 2016
#cpscouncil#cpselections

HousekeepingHarry McQuillan
CEO

Username: xxxx
Password:xxxx
WiFi Connection

Apologies for Absence
Amanda Henderson

Introduction and Welcome
Harry McQuillanCEO

Agenda for the Day
• Ratification of Amended Articles of Association
• Election of Office Bearers and Board
• Roles and Responsibilities
• Financial Package 16/17
• High Cost Medicine Session
• GPhC – Consultation on standards for pharmacy professionals
• Prescription for Excellence – Direction of Travel

Amended Articles of Association

Amended Articles of Association
• Ratification of Amended Articles of Association
• Please refer to your handout

Election of Office Bearers

Election of Chair

Nominations
● One nomination received
• Martin Green

Election of Vice-Chair

Nominations
● Two nominations received:
● John Currie
● Stephen Watkins

Election of Board

Board Election Process
● Each member of the elected pharmacy contractor group (nonCCA), including deputies, is entitled to vote● You may vote for SEVEN or fewer candidates● Voting is achieved by placing a cross (X) in the space alongside the name of a candidate for whom you wish to vote● Voting papers having marks alongside more than seven candidates or upon which the voters intentions are not clear will be disallowed

Voting Form - Correct
Voting Form - Wrong

Board Election

Candidates
Name Name
Sally Arnison Alasdair Macintyre
John Connolly Dara O’Malley
John Currie James Semple
Philip Galt Campbell Shimmins
Karen Gordon Catriona Sinclair
Colin Fergusson

Time to decide

Decision Time

Results
Name Votes Name Votes
Sally Arnison Alasdair Macintyre
John Connolly Dara O’Malley
John Currie James Semple
Philip Galt Campbell Shimmins
Karen Gordon Catriona Sinclair
Colin Fergusson
Community Pharmacy Scotland Board Session 2016-2019
Name Name
Martin Green (Chair)
(Vice Chair)

Council Meeting
Roles and Responsibilities of Council
Matt BarclayDirector of Operations

Roles and Responsibilities of Council
• Promote, represent and safeguard the rights and interests of all pharmacy contractors in the provision of pharmaceutical services
• Negotiate the terms and conditions for the provision of those services
• Inform, advise and assist pharmacy contractors
• Educate and inform the public on the services provided by pharmacy contractors

Roles and Responsibilities of Council
• Promote and increase the profile of community pharmacy to a wide range of external bodies, stakeholders and decision makers
• Take forward the opinions of pharmacy contractors on matters affected the provision of services
• Put forward the views of the CPHBs and feedback to the CPHBs
Roles and Responsibilities of Council
• Represent the interests of community pharmacy at conferences, meetings and forums
• Represent the views of pharmacy contractors on consultations and proposed legislative changes
• Ensure that sufficient funds are raised by making such levies upon pharmacy contractors to ensure the furtherance of the objects of the Council

Roles and Responsibilities of Council
• Duty to elect or nominate members to the Board at the first meeting of a new session
• Once formed from the members of Council, it is important that the Board conforms to any rules and restrictions, being not inconsistent with the provisions of the Articles of Association, that may be imposed on it by the Council
Roles and Responsibilities of Council
• Council and Board can delegate any of its work to sub committees and appoint, remove and reappoint members to such committees
• The Council shall determine the constitution, powers and duties of each CPHB and ensure that one of the key duties of a CPHB is to elect representatives to the next session of Council
• Council forwards views to the Board and ensures that feedback comes back from the Board
Roles and Responsibilities of Council
• Duty of the Council and the Board to ensure that pharmacy is represented on appropriate committees and organisations to promote the interests of community pharmacy
• The Council has a duty to practise, further and protect the objects of the Council as laid down in the Articles of Association

Attendance at Meetings
• Two meetings per year and one shall be the annual general meeting
• Any voting member of Council not able to attend a general meeting can nominate another pharmacist having like eligibility to attend and vote on their behalf – counts towards a quorum

Attendance at Meetings
• Council can co-opt additional members from time to time – must be pharmacy contractors or representatives of pharmacy contractors, whose expertise or experience would be of assistance – cannot vote
• Similar co-option allowed to Board for a period of less than the duration of a session of the Council

Minutes of Council Meeting
Chair
Minutes of the meeting held on 11th November 2015
• Propose
• Second

Matters arising from the minutes

Financial Settlement 2016/17
Chair

Negotiations with SG
• We started out by talking about the principles we wanted to achieve in our negotiations
• Key objectives were to secure an environment which supported stability and predictability
• Mindful of the pending Scottish parliamentary election• SG had new negotiating team• SG then sent their first offer letter in January• We were underwhelmed
Initial Offer
• Global Sum was to remain the same• Reimbursement for Part 7 and MSA were to remain unchanged for
2016/17 until contractors had repaid to Boards all that was owed.• The non Global Sum element of £1.3m (for clinics, grants etc) was
to stay the same• In general SG wanted to look at how it could re-energise CMS and
how the money in the existing global sum could be spent to deliver political priorities
Next Steps
• CPS pointed out it was not possible to leave all MSA unchanged as whatever happened over the course of the year would impact upon the starting point for 2017/18
• More work had to take place on the MSA elements including outcome for 2015/16 where we had run into problems
• Doctors, dentists and nurses had been given a 1% pay rise so why was pharmacy excluded?
• What about the burden caused by introduction of the Living Wage?

Outcomes
• SG agreed to allow an uplift in respect of pay for low paid workers and £1m has been added to the global sum taking it to £178.359m for the year 2016/17
• This money came from the MSA for 2015/16
• It was also agreed that a further £2m would be made available on a non-recurring basis and that this money sat outside the Global Sum

Outcomes – Drug Tariff
• Pregabalin has been added to Part 7 at the Lyrica price pending the outcome of the Pfizer court case
• PSD will no longer differentiate between tablet and caplet formulations when pricing prescriptions for co-codamol and paracetamol presentations
• Volume growth for the year has been estimated at 2.5%• Some modulation has occurred where prices were well adrift from
the market place but otherwise prices have been left unchanged• Claw back rates have both been reduced – 3.0% for Part 7 and
6.18% for non Part 7

Distribution of Monies
• For most payment lines there will be no immediate change
• There is some money unallocated in the global sum – previous overpayments have been worked off and there will be no flu payments this year
• There is another £2m sitting outside the global sum
• CPS has proposed that the money should come out under three headings

Distribution Proposals
• A new fixed experiential payment should be made to contractors who provide placements for students – contractors would have to sign up to receive it
• The money previously paid for the supply of flu vaccines should be used to support the introduction of a new vaccination service and possibly used initially to cover training
• The remaining money should be used to fund a salary/regulatory burden payment

Future Work
• Should we look to negotiate a longer term deal?
• Offers stability while we reassess the long term future of some payments
• What about the payments for CMS? For O and D?
• Is there the possibility for new payments after the PfE refresh?

High Cost Medicine Session
Mark FeeneyHead of Policy and Development

Why?
● Contractors suffering large fluctuations in cash flow
● Frequent operational issues with service
● Feeling in the network the service was significantly underfunded

Timeline
● Summer 2015 :CPS raises concerns with SG about DAAs
● Autumn 2015 :CP GG+C inform HB service is at risk
● December 2015 :CPS inform DOPs of need for urgent action
● January 2016 :CPS push for meeting with DOPs group
● February 2016 :First face to Face meeting with DOPs group
Timeline
● March 2016 :Further meeting with DOPs groupCPS write to all local CP committees advising withdrawal from service
● April 2016 :Final meeting with DOPs groupWithdrawal date changed to 1st of August
● May 2016 :Local negotiations start

Reflections

CPS Brand Values

Lunch

GPhC Consultation into new standards for Pharmacy Professionals
Lynsey ClelandGPhC Director for Scotland

Prescription for ExcellenceDirection of Travel
CEO

Prescription for Excellence CPO’s 5 Themes
● Pharmaceutical Care
● Safer Use of Medicines
● Evidence Base and Outcomes
● Strategic Engagement
● Pharmacy Profession and Professionalism

Prescription for Excellence
• Undergoing a “refresh” process at present
• CPS expecting a revised publication
• Revised project management structure in place
• Blueprint working group established
• Technology & Workforce subgroup

Moving from actions to outcomes
Commitments / Actions Outputs Outcomes
out-
put
no. broad specific Patient need Patient need Patient need Patient need Patient centred Patient centred Access Access Access Access delivery / sustainability
delivery /
sustainability delivery / sustainability
delivery /
sustainability
delivery /
sustainability
delivery /
sustainability
delivery /
sustainability
delivery /
sustainability
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
services
designed
around patient
needs
Patients
receive
appropriate
pharm care
Reduction in
admission
rates / ALOS
reduction in
harm from
medicines
improved patient
confidence and
satisfation in
service
Improved
patient
adherence to
medicines
patients access and
are routed to pharm
services appropriate
to their needs
increase in the
availability and
use of pharm
care services
Increased
clinical capacity
(pharm wf) /
capacity in the
system
Access to
required
information to
deliver services
pharm care services
embedded /
pharmacist integrated
within MDTs
Technology &
enhanced
service
delivery
Decreased unwanted
varation / increased
consistency in service
delivery
reduction in
waste of
medicines
services are
sustainable
and financially
viable
IJB allocate
resources
Recognition of
pharmacy role
/ pharm care
on IJB agenda
Improved
governance
arrangements
Planning and operating Model
We will introduce new planning and contracting
requirements for the delivery of pharmaceutical
care services
• Develop and agree role of pharmaceutical care
service plan in identifying need
2
Nationally agreed standards of
service
Appropriate / functional
care service plan(s).
Acceptable service
solutions
CSPs ensure
need is met
CSPs
ensure need
is met
secondary
outcome
secondary
outcome
secondary
outcome
secondary
outcome
direct outcome of
CSP implementation
direct outcome of
CSP
implementation
direct outcome of
CSP
implementation
direct outcome of CSP
implementation
variation reduced if
rolled out coherently
secondary
outcome
secondary
outcome
19
National planning framework that is
fit for purpose
CSPs ensure
need is met
CSPs
ensure need
is met
secondary
outcome
secondary
outcome
secondary
outcome
secondary
outcome
direct outcome of
CSP implementation
direct outcome of
CSP
implementation
direct outcome of
CSP
implementation
direct outcome of CSP
implementation
variation reduced if
rolled out coherently
secondary
outcome
secondary
outcome
• Ensure articulated population care needs inform
and shape service design and delivery1
Processes which ensure continuity
and consistency of service provision
needs based delivery
models
models ensure
need is met
models
ensure need
is met
secondary
outcome
secondary
outcome
secondary
outcome
secondary
outcome
direct outcome of del
models
direct outcome of
del models
direct outcome of
del models
direct outcome of del
models
variation reduced if
rolled out coherently
secondary
outcome
secondary
outcome
appropriate pathways for
decisions /
communication
enabler to
achieve right
decisions?
enabler to
achieve right
decisions?
enabler to achieve
right decisions?
direct outcome of
pathways?
direct outcome of
pathways?
direct outcome of
pathways?
secondary
outcome
secondary
outcome
• Implement new contract arrangements
delivering pharmaceutical care services18
Contract arrangements that are fit
for delivering future pharm care and
services
Contract arrangements
in place
if specified in
contract
if specified in
contract
secondary
outcome
secondary
outcome if specified in contract
if varation addressed in
contract
secondary
outcome
secondary
outcome
role of IJB
determined
in contract?
covered in
contract
appropriate enablers /
levers
if specified in
contract
if specified in
contract ? ?
if varation addressed in
contract
one lever
being role of
IJB? ?
3
pharma care services are
embedded in MDTs
if MDT is appr.
Model
if MDT is
appr. Model
capacity through
MDTs output or outcome?
• Introduce standard reports to assess levels of
PCS and effectiveness of delivery1
Processes which ensure continuity
and consistency of service provision
Bundles of standard
reports
bundles provide
required info
2
Nationally agreed standards of
service
standards
ensure need is
met
standards
ensure need
is met
secondary
outcome
secondary
outcome
secondary
outcome
secondary
outcome
variation reduced if
rolled out coherently
secondary
outcome
secondary
outcome
• Establish new reimbursement and
remuneration arrangements for PCS in the Drug
Tariff1
Processes which ensure continuity
and consistency of service provision
appropriate
reimbursement &
remuneration
arrangements
fin sust.
Ensured
arrangement
s with IJB?
• Review governance arrangements for safe
delivery of pharmaceutical care and use of
medicines in the community 1
Processes which ensure continuity
and consistency of service provision
appropriate governance
arrangements
stipulated in
governance arr.
stipulated in
governance
arr.
stipulated in
governance arr.
2
Nationally agreed standards of
service
stipulated in
governance arr.
stipulated in
governance
arr.
stipulated in
governance arr.
Outcomes to feed directly into high-level strategic objectives (Outcome Dependency Model)
Underlying benefits summary with possible measures, evaluation approach
Commitments / Actions
from Blueprint
Translate into agreed set of
outputsLink to overarching set of outcomes
Anticipated causal relationship

Outputs
3 – Pharmaceutical care services are embedded in MDTs
14 - increased patient trust in pharm care services
OutcomesActions
develop existing working practices and expectations to integrate
pharmacists into multidisciplinary teams working across all settings
Commitments
We will:
•Develop proactive approaches to pharmacists working across sectors – initiating /taking responsibility for small improvements•Improve communication between community pharmacy and other healthcare professionals to improve patient care•Understand and address barriers to Community Pharmacy working as equal healthcare partners – e.g. access to patient records•Develop integrated seamless pharmaceutical care pathways•Support Directors of Pharmacy to lead change and necessary communication to install new ways of working between pharmacists and other healthcare professions• DN: [something needed about final check culture -how to give pharmacists confidence to accept / move away from this element of supply]
Patient Need
1 2
Access Delivery / Sustainability
9 11
Patient Need
1 - services designed around patient needs
2 - Patients receive appropriate pharm care
3 - Reduction in admission rates/ALOS
4 - reduction in harm from medicines
Patient Centred
5 - improved patient confidence and satisfaction in service
6 - Improved patient adherence to medicines
Access
7 - patients access and are routed to pharm services appropriate to their needs
8 - increase in the availability and use of pharm care services
9 - Increased clinical capacity (pharm wf) / capacity in the system
10 - Access to required information to deliver services
Delivery/Sustainability
11 - pharm care services embedded / pharmacist integrated within MDTs
12 - Technology & enhanced service delivery
13 - Decreased unwanted variation / increased consistency in service delivery
14 - reduction in waste of medicines
15 - services are sustainable and financially viable
16 - IJB allocate resources
17 - Recognition of pharmacy role / pharm care on IJBagenda
18 - Improved governance arrangements
Patient Centred
5 6
Access Delivery / Sustainability
7
Design of Pharmaceutical Care Services (1)
increase the availability of pharmaceutical care services and
expertise in medicines in multidisciplinary settings
•Develop service delivery models that: utilise the full community pharmacy network in; increase pharmacist management of common clinical conditions in partnership with GPs; increase pharmacist role in pharmaco-vigilance; provide medication reviews to improve patient outcomes
•Extend CMS and MAS
•Develop clinics to be delivered in community pharmacy to support continuity of care
•Improve access to pharmaceutical care in care homes, care at home, hospital at home.
•Integrate pharmacist into the multidisciplinary team –both managed service pharmacist and community pharmacist
•Consider opportunities for service delivery by all community pharmacists, not just independent prescribers
•Scope and address resource requirements for delivery of pharmaceutical care and medication reviews across primary and secondary care
•Consider how SMC process links to future service delivery model
•Develop role of technology to enable remote consultations
•Explore use of telehealth from specialist secondary care pharmacy staff
7 - A clear national specification for pharm care services
1 - Processes which ensure continuity and consistency of service provision
9 - Improved capacity / capability of CP services
19 - National planning framework that is fit for purpose
10 - Improved capacity & capability in pharm care delivery
Patient Need
1 2
Access Delivery / Sustainability
8 13
Patient Need
1 2
Access Delivery / Sustainability
7 8 9 11 16 18
Patient Centred
5
Access
8 9
Patient Need
1 2
Access Delivery / Sustainability
7 8 9 11
Patient Need
1 2
Access Delivery / Sustainability
8 9

Technology & Workforce
• Only live original workstream
• Agreed the test areas to be considered
• Tests robotic technology – viability cut off point advice
• Tests scanning technology – improved safety aspect
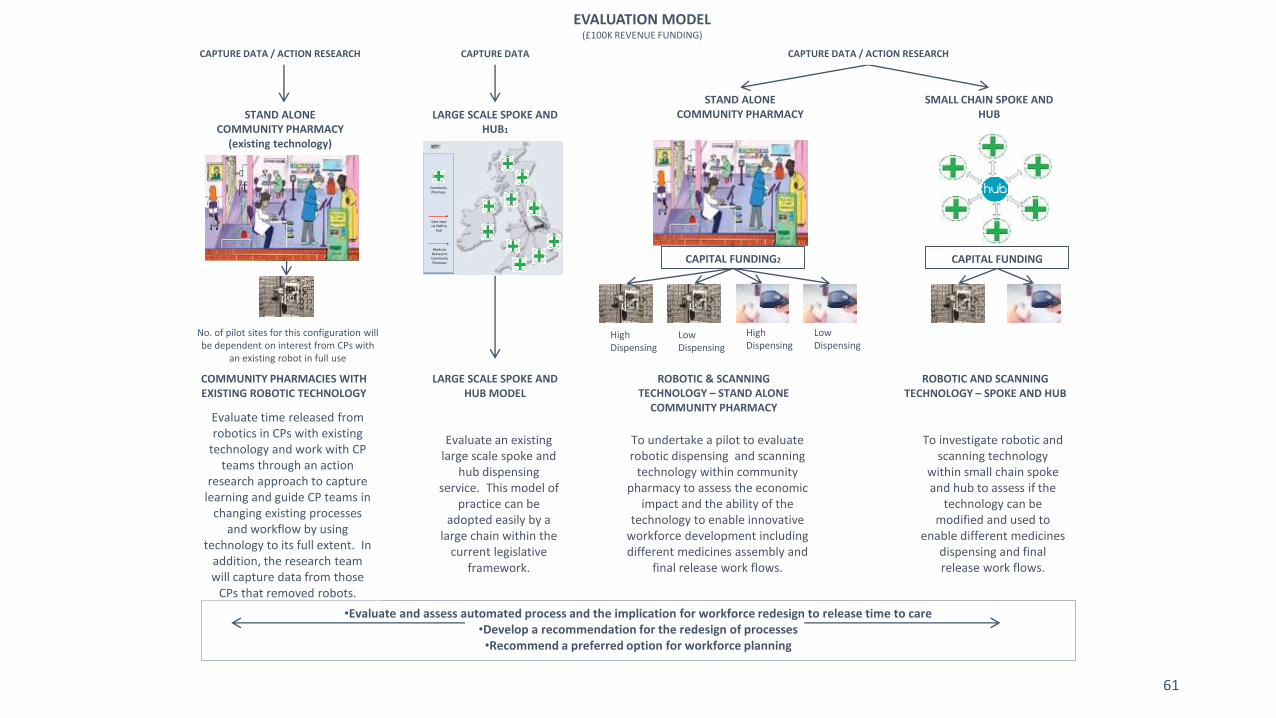
EVALUATION MODEL(£100K REVENUE FUNDING)
•Evaluate and assess automated process and the implication for workforce redesign to release time to care•Develop a recommendation for the redesign of processes•Recommend a preferred option for workforce planning
61
SMALL CHAIN SPOKE AND HUB
ROBOTIC & SCANNING TECHNOLOGY – STAND ALONE
COMMUNITY PHARMACY
ROBOTIC AND SCANNING TECHNOLOGY – SPOKE AND HUB
To undertake a pilot to evaluate robotic dispensing and scanning
technology within community pharmacy to assess the economic
impact and the ability of the technology to enable innovative
workforce development including different medicines assembly and
final release work flows.
To investigate robotic and scanning technology
within small chain spoke and hub to assess if the
technology can be modified and used to
enable different medicines dispensing and final release work flows.
STAND ALONE COMMUNITY PHARMACY
CAPITAL FUNDING2 CAPITAL FUNDING
Community Pharmacy
Data input via PMR to
Hub
Medicine Delivery to Community Pharmacy
LARGE SCALE SPOKE AND HUB1
Evaluate an existing large scale spoke and
hub dispensing service. This model of
practice can be adopted easily by a
large chain within the current legislative
framework.
STAND ALONE COMMUNITY PHARMACY
(existing technology)
No. of pilot sites for this configuration will be dependent on interest from CPs with
an existing robot in full use
COMMUNITY PHARMACIES WITH EXISTING ROBOTIC TECHNOLOGY
Evaluate time released from robotics in CPs with existing
technology and work with CP teams through an action
research approach to capture learning and guide CP teams in
changing existing processes and workflow by using
technology to its full extent. In addition, the research team will capture data from those
CPs that removed robots.
LARGE SCALE SPOKE AND HUB MODEL
CAPTURE DATA / ACTION RESEARCH CAPTURE DATA
High Dispensing
Low Dispensing
High Dispensing
Low Dispensing
CAPTURE DATA / ACTION RESEARCH

Technology & Workforce
Automated Dispensing Robot – Low Volume Dispensing Standalone Community
Pharmacy (installation before 31st March 2017)
Automated Dispensing Robot - High Volume Dispensing Standalone Community
Pharmacy (installation before 31st March 2017)
Automated Dispensing Robot –
Spoke and Hub Operating Model (installation before 31st March 2018)
Scanning Technology –
Low Volume Dispensing Standalone Community Pharmacy (installation before 31st
March 2017)
Scanning Technology –
High Volume Dispensing Standalone Community Pharmacy (installation before 31st
March 2017)
Scanning Technology –
Spoke and Hub Operating Model (installation before 31st March 2017)

Technology & Workforce
• Now at the initial Grant Application Process stage
• Opened 2nd May
• Closes 27th May
• Screening Process follows
• National decision re grant allocation

Prescription for Excellence
• CPS is now being invited to participate
• Practicalities of implementation being considered
• Acceptance of a major role for Community Pharmacy

AOB