cpc cardiology department sms medical college jaipur
TRANSCRIPT
SMS Medical College JaipurCPC Meetings
Conducted By Medical Education Unit
SMSMC-CPCThe TEAM
bull DR HEMANT MALHOTRA CONVENER (9829062040 drmalhotrahemantgmailcom)
bull DR PUNEET SAXENA Dept of Medicine (9414079182 puneetsaxena96yahoocoin)
bull DR ARADHANA SINGH Dept of Medicine (9166916692 aradhanas610yahoocom)
bull DR MONICA JAIN Dept of Pharmacology (9828786533 monicajain07yahoocom)
bull VENUE AUDITORIUM OF THE SMS HOSPITAL (audio-visual IC ndash Dr PD Meena Dept Of Medicine)
bull Day amp date 2nd Friday of every monthbull Time 1230 pm to 130 pmbull ATTENDENCE TO BE COMPULSORY FOR ALL FACULTY
MEMBERS OF THE INSTITUION ndash PHODs TO ENSURE SMOOTH FUNCTIONING OF ALL PATIENT SERVICES
bull Audience all faculty members of the SMSMC all senior residents ex-faculty members
SMSMC-CPC
SMSMC-CPCFormat
bull Dates allotted to each department for the full calendar yearbull No cancellation permitted other than if Friday is a GHbull Mutual exchange with another dept permitted with info to and
permission from office of the P amp Cbull First 15 mins of presentation to include highlights of work done in the
dept major publications awards honours amp achievements of the deptbull Subsequent 30 mins to include multi-speciality case presentation of
interest to as many depts As possible ndash presentation by multiple faculty amp multiple depts encouraged (example - case presentation by dept of Medicine radiological findings by dept of Radio-diagnosis surgical finding by dept of Surgery histo-path diagnosis by dept of pathology dd amp treatment by dept of oncology)
bull Last 15 mins for q amp a
Next CPC
Dept of Neurology12 August 2016
INTRODUCTION
ProfDr S M Sharma Add PrincipalHOD Dept of Cardiology
Department of CardiologySawai Man Singh Medical College
Hospital Jaipur
History
bull Department of cardiology is one of the esteemed department of SMS Medical college
bull Started in 1992 as a separate Cardiology unit in the department of Medicine under guidance of Dr Amrit Khalsa and Dr V S Baldwa
bull When coronary intervention was being developed in western world in Nineties First Cath lab of the department established in 1992
bull Separate Department of Cardiology established in 1995 under Prof Dr Madhok with 50 beds alloted
bull DM cardiology course started in the department in 1999 with two students and subsequently seats increased to eight in 2010
bull Separate ICCU started in 2005 with 12 beds facility in main ICCU and 10 beds in semi ICCU
bull In 2006 new Cath lab established having capabilities of diverse interventional procedures and EP facility
bull Third Unit in cardiology started in 2008 and also OPD days increased from four to seven days a week
bull New 3-D echo machine Holter monitors and TMT machines were added in the department in 2009
bull In 2013 another gem added with establishment of second cath lab having facilities such as IVUS FFR Dyna CT imaging IABP DSA booster facility which is helping to provide world class cardiac and peripheral intervention
bull In 2014 fourth unit startedbull Recently renovation of Post Catheterisation
Recovery Area(PCRA) dedicated to post cath patients completed which increased its bed capacity from 7 to 21
PRESENT SCENARIO OF THE DEPARTMENTbull No of consultants-12 bull These include 7 Professors 1 Associate Professor 3 Asst Professors and 1 MO
bull Prof Dr Anoop Jainbull Prof Dr Shashi Mohan Sharma(PHOD)bull Prof Dr Rajeev Bagarhattabull Prof Dr V V Agarwalbull Prof Dr Vijay Pathakbull Prof Dr Chandrabhan Meenabull Prof Dr Deepak Maheshwaribull Asso Prof Dr Neeraj Chaturvedibull Asst Prof Dr Sohan Kumar Sharmabull Asst Prof Dr Ritesh Guptabull Asst Prof Dr Omprakash Khojabull Dr Sunil Sharma MO
bull No of Residents- 24 (8 each year)
bull No of DET( Diploma in ECG Technician) students- 20 per yearbull No of equipment- - Two cath labs with state of the art equipment like IVUS FFR CT+3D imaging IABP Rotablator EP system Electrocautery etc - One 3-D Echo machine and four 2-D echo machines distributed in Echo lab Cath lab ICCU and Emergency dept - 2 TMT machines - 11 Holter Devices
CATH LAB 1
CATH LAB 2
CATH LAB CONSOLE
ECHO LAB
bull OPD runs 7 days a weekbull 24 hours Cardiology Emergency services with
round the clock presence of DM residentbull No of patients visited Cardiology department
last year Numbers
No of patients attending OPD 96160
No of Indoor admissions 10808
No of 2D-Echo 19183
No of Holter monitoring 954
No of TMT 5749
No of Cath Interventions 8834
bull We are also providing Super speciality services to Seth S R Goyal satellite hospital Sethi colony Jaipur- 3 days a week
bull Primary PCI is being done round the clock and this facility is present in only few Govt Hospitals anywhere in India Also the Door to balloon time in our hospital is around 70 min which is well under the international recommendations of less than 90 min
bull An exhaustive DM Cardiology teaching programme is going on in the department five days a week with full participation of students and consultants
bull Our students who come for DM get excellent exposure to clinical and interventional work which sets them not only at par but I take pride in saying that they are even better than their counterparts in leading premier institutes of the country This is the reason why most of them are very well settled now and are doing very well wherever they are
bull Our department also offers Diploma for ECG Technician(DET) course in which 20 students get admitted yearly
Research Activities
Research Activities
Average no of studies done per year 22
Average no of papers published in reputed national amp international journals per year
14
In last 6 years our students have published around 100 research papers in national and international reputed journals
Presently work in the department is covering all major aspects of cardiology includingbull PTCA + STENTING including complex angioplastiesbull Primary PCIbull Rotablationbull IVUS FFRbull Carotid and other peripheral angioplastiesbull Renal angioplastiesbull BMVBPV BAVbull ASD VSD PDA Device closurebull Permanent pacemaker implantations including Dual chamber and MRI
compatible pacemakersbull AICDbull CRT-P CRT-Dbull EPS and RFAbull Arterial Embolizationbull Endomyocardial biopsy
bull These are comparable to most of the leading Govt Institutes anywhere in India
bull We are also trying to upgrade our facilities in the field of structural heart disease which includes endovascular treatment of aortic aneurysm dissection paravalvular leak closure TAVI etc
bull Lastly the Honorable CM has sanctioned a new Cath lab for our department in the present budget which will be installed soon A new 3-D Echo machine is being installed in next 2-3 months This will further improve the working in the department for better care of the poor patients
THANK YOU
CPC caseDepartment Cardiology
8th July 2016
Presenter Dr Rakesh Kumar Ola Dr Daulat Singh Meena
Cardiology discussant Dr Sohan K Sharma Assistant Prof Deptt Cardiology
Respiratory discussant Dr Sheetu Singh Assistant Prof Chest amp TB
Medicine discussant Dr Ashutosh Daga Resident Deptt Of Medicine ProfDrHemant Malhotra PHOD Deptt Of Medicine
Radiology discussant Dr Sachin Lamba Resident RadiologyDr RK Yadav Astt Prof Radiology
Pathology discussant Dr Neetu Aggarwal Sr Resident PathologyDr Anita Harsh Assoc Prof Pathology
Case Presenter
Dr Rakesh Kumar OlaIIIrd Year Resident
Department of Cardiology
Presenting complaints
A 38y old male resident of Jhalawar-Rajasthan presented with complaints of bull Fever on and off-12 monthsbull Cough- 12 monthsbull Weight loss-12 monthsbull Shortness of breath on exertion- 6 months bull Bilateral lower limb swelling- 15-20 days
History of presenting illness
Asymptomatic till 12 month back when he developed - Fever bull Insidious bull Low grade bull Intermittent typebull Each episode lasted for 10-15 daysbull Not associated with chills and rigor bull No diurnal variation bull Relieved by medications
History of presenting illness
Cough -12 monthbull Non-productive coughbull On and Off bull Each episode lasted for 20-30 days bull Cough was not associated with hemoptysis
chest heaviness noisy breathing and post-nasal discharge
bull No postural diurnal or seasonal variation
History of presenting illness
Weight loss -12 monthbull Patient had ho of significant weight loss of
5kg in last 12 months associated with easy fatigability
History of presenting illness
Shortness of breath-6 monthsbull Insidious onset bull Patient initially complain SOB on more than ordinary
activity and it progressively increased over 5 months and from last one month patient having SOB on less than ordinary physical activity (NYHA grade I to III ) but not at rest
bull SOB was not worsen by lying down and had no HO of episodic breathlessness during night
bull No postural or diurnal or seasonal variation
History of presenting illness
Bilateral lower limb swelling- 15-20 daysbull Lower limb swelling started from ankle joint
and progressed up to knee joint bull Not associated with morning facial puffiness
and abdominal fullnessbull No pain tenderness or warmth of lower limb
History of presenting illness
No history of bull Personal or family history of atopy or allergy like
itching skin lesions urticaria noisy breathing or seasonal variations
bull History of joint pains oral ulcersbull Travel out of statebull History of drugs or radiation exposurebull Occupational exposure of dust or smoke
History of presenting illness
No history of bull Recurrent episodes of diarrhoea abdominal pain
dysphagia or icterusbull Chest pain bull Palpitationbull Loss of consciousness bull Ho of focal neurological deficit
Past medical history
bull Patient had history of recurrent admissions and received treatment for enteric fever and malaria though patient had no relief in symptoms from same
bull No HO of DM HTN Tuberculosisbull No Ho any surgical intervention in past
Personal history
bull Laborerbull Studied up to 10th standardbull Smokerbull Non alcoholicbull Married bull Normal sleep appetite bowel and bladder
habitsbull Diet - vegetarian
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
SMSMC-CPCThe TEAM
bull DR HEMANT MALHOTRA CONVENER (9829062040 drmalhotrahemantgmailcom)
bull DR PUNEET SAXENA Dept of Medicine (9414079182 puneetsaxena96yahoocoin)
bull DR ARADHANA SINGH Dept of Medicine (9166916692 aradhanas610yahoocom)
bull DR MONICA JAIN Dept of Pharmacology (9828786533 monicajain07yahoocom)
bull VENUE AUDITORIUM OF THE SMS HOSPITAL (audio-visual IC ndash Dr PD Meena Dept Of Medicine)
bull Day amp date 2nd Friday of every monthbull Time 1230 pm to 130 pmbull ATTENDENCE TO BE COMPULSORY FOR ALL FACULTY
MEMBERS OF THE INSTITUION ndash PHODs TO ENSURE SMOOTH FUNCTIONING OF ALL PATIENT SERVICES
bull Audience all faculty members of the SMSMC all senior residents ex-faculty members
SMSMC-CPC
SMSMC-CPCFormat
bull Dates allotted to each department for the full calendar yearbull No cancellation permitted other than if Friday is a GHbull Mutual exchange with another dept permitted with info to and
permission from office of the P amp Cbull First 15 mins of presentation to include highlights of work done in the
dept major publications awards honours amp achievements of the deptbull Subsequent 30 mins to include multi-speciality case presentation of
interest to as many depts As possible ndash presentation by multiple faculty amp multiple depts encouraged (example - case presentation by dept of Medicine radiological findings by dept of Radio-diagnosis surgical finding by dept of Surgery histo-path diagnosis by dept of pathology dd amp treatment by dept of oncology)
bull Last 15 mins for q amp a
Next CPC
Dept of Neurology12 August 2016
INTRODUCTION
ProfDr S M Sharma Add PrincipalHOD Dept of Cardiology
Department of CardiologySawai Man Singh Medical College
Hospital Jaipur
History
bull Department of cardiology is one of the esteemed department of SMS Medical college
bull Started in 1992 as a separate Cardiology unit in the department of Medicine under guidance of Dr Amrit Khalsa and Dr V S Baldwa
bull When coronary intervention was being developed in western world in Nineties First Cath lab of the department established in 1992
bull Separate Department of Cardiology established in 1995 under Prof Dr Madhok with 50 beds alloted
bull DM cardiology course started in the department in 1999 with two students and subsequently seats increased to eight in 2010
bull Separate ICCU started in 2005 with 12 beds facility in main ICCU and 10 beds in semi ICCU
bull In 2006 new Cath lab established having capabilities of diverse interventional procedures and EP facility
bull Third Unit in cardiology started in 2008 and also OPD days increased from four to seven days a week
bull New 3-D echo machine Holter monitors and TMT machines were added in the department in 2009
bull In 2013 another gem added with establishment of second cath lab having facilities such as IVUS FFR Dyna CT imaging IABP DSA booster facility which is helping to provide world class cardiac and peripheral intervention
bull In 2014 fourth unit startedbull Recently renovation of Post Catheterisation
Recovery Area(PCRA) dedicated to post cath patients completed which increased its bed capacity from 7 to 21
PRESENT SCENARIO OF THE DEPARTMENTbull No of consultants-12 bull These include 7 Professors 1 Associate Professor 3 Asst Professors and 1 MO
bull Prof Dr Anoop Jainbull Prof Dr Shashi Mohan Sharma(PHOD)bull Prof Dr Rajeev Bagarhattabull Prof Dr V V Agarwalbull Prof Dr Vijay Pathakbull Prof Dr Chandrabhan Meenabull Prof Dr Deepak Maheshwaribull Asso Prof Dr Neeraj Chaturvedibull Asst Prof Dr Sohan Kumar Sharmabull Asst Prof Dr Ritesh Guptabull Asst Prof Dr Omprakash Khojabull Dr Sunil Sharma MO
bull No of Residents- 24 (8 each year)
bull No of DET( Diploma in ECG Technician) students- 20 per yearbull No of equipment- - Two cath labs with state of the art equipment like IVUS FFR CT+3D imaging IABP Rotablator EP system Electrocautery etc - One 3-D Echo machine and four 2-D echo machines distributed in Echo lab Cath lab ICCU and Emergency dept - 2 TMT machines - 11 Holter Devices
CATH LAB 1
CATH LAB 2
CATH LAB CONSOLE
ECHO LAB
bull OPD runs 7 days a weekbull 24 hours Cardiology Emergency services with
round the clock presence of DM residentbull No of patients visited Cardiology department
last year Numbers
No of patients attending OPD 96160
No of Indoor admissions 10808
No of 2D-Echo 19183
No of Holter monitoring 954
No of TMT 5749
No of Cath Interventions 8834
bull We are also providing Super speciality services to Seth S R Goyal satellite hospital Sethi colony Jaipur- 3 days a week
bull Primary PCI is being done round the clock and this facility is present in only few Govt Hospitals anywhere in India Also the Door to balloon time in our hospital is around 70 min which is well under the international recommendations of less than 90 min
bull An exhaustive DM Cardiology teaching programme is going on in the department five days a week with full participation of students and consultants
bull Our students who come for DM get excellent exposure to clinical and interventional work which sets them not only at par but I take pride in saying that they are even better than their counterparts in leading premier institutes of the country This is the reason why most of them are very well settled now and are doing very well wherever they are
bull Our department also offers Diploma for ECG Technician(DET) course in which 20 students get admitted yearly
Research Activities
Research Activities
Average no of studies done per year 22
Average no of papers published in reputed national amp international journals per year
14
In last 6 years our students have published around 100 research papers in national and international reputed journals
Presently work in the department is covering all major aspects of cardiology includingbull PTCA + STENTING including complex angioplastiesbull Primary PCIbull Rotablationbull IVUS FFRbull Carotid and other peripheral angioplastiesbull Renal angioplastiesbull BMVBPV BAVbull ASD VSD PDA Device closurebull Permanent pacemaker implantations including Dual chamber and MRI
compatible pacemakersbull AICDbull CRT-P CRT-Dbull EPS and RFAbull Arterial Embolizationbull Endomyocardial biopsy
bull These are comparable to most of the leading Govt Institutes anywhere in India
bull We are also trying to upgrade our facilities in the field of structural heart disease which includes endovascular treatment of aortic aneurysm dissection paravalvular leak closure TAVI etc
bull Lastly the Honorable CM has sanctioned a new Cath lab for our department in the present budget which will be installed soon A new 3-D Echo machine is being installed in next 2-3 months This will further improve the working in the department for better care of the poor patients
THANK YOU
CPC caseDepartment Cardiology
8th July 2016
Presenter Dr Rakesh Kumar Ola Dr Daulat Singh Meena
Cardiology discussant Dr Sohan K Sharma Assistant Prof Deptt Cardiology
Respiratory discussant Dr Sheetu Singh Assistant Prof Chest amp TB
Medicine discussant Dr Ashutosh Daga Resident Deptt Of Medicine ProfDrHemant Malhotra PHOD Deptt Of Medicine
Radiology discussant Dr Sachin Lamba Resident RadiologyDr RK Yadav Astt Prof Radiology
Pathology discussant Dr Neetu Aggarwal Sr Resident PathologyDr Anita Harsh Assoc Prof Pathology
Case Presenter
Dr Rakesh Kumar OlaIIIrd Year Resident
Department of Cardiology
Presenting complaints
A 38y old male resident of Jhalawar-Rajasthan presented with complaints of bull Fever on and off-12 monthsbull Cough- 12 monthsbull Weight loss-12 monthsbull Shortness of breath on exertion- 6 months bull Bilateral lower limb swelling- 15-20 days
History of presenting illness
Asymptomatic till 12 month back when he developed - Fever bull Insidious bull Low grade bull Intermittent typebull Each episode lasted for 10-15 daysbull Not associated with chills and rigor bull No diurnal variation bull Relieved by medications
History of presenting illness
Cough -12 monthbull Non-productive coughbull On and Off bull Each episode lasted for 20-30 days bull Cough was not associated with hemoptysis
chest heaviness noisy breathing and post-nasal discharge
bull No postural diurnal or seasonal variation
History of presenting illness
Weight loss -12 monthbull Patient had ho of significant weight loss of
5kg in last 12 months associated with easy fatigability
History of presenting illness
Shortness of breath-6 monthsbull Insidious onset bull Patient initially complain SOB on more than ordinary
activity and it progressively increased over 5 months and from last one month patient having SOB on less than ordinary physical activity (NYHA grade I to III ) but not at rest
bull SOB was not worsen by lying down and had no HO of episodic breathlessness during night
bull No postural or diurnal or seasonal variation
History of presenting illness
Bilateral lower limb swelling- 15-20 daysbull Lower limb swelling started from ankle joint
and progressed up to knee joint bull Not associated with morning facial puffiness
and abdominal fullnessbull No pain tenderness or warmth of lower limb
History of presenting illness
No history of bull Personal or family history of atopy or allergy like
itching skin lesions urticaria noisy breathing or seasonal variations
bull History of joint pains oral ulcersbull Travel out of statebull History of drugs or radiation exposurebull Occupational exposure of dust or smoke
History of presenting illness
No history of bull Recurrent episodes of diarrhoea abdominal pain
dysphagia or icterusbull Chest pain bull Palpitationbull Loss of consciousness bull Ho of focal neurological deficit
Past medical history
bull Patient had history of recurrent admissions and received treatment for enteric fever and malaria though patient had no relief in symptoms from same
bull No HO of DM HTN Tuberculosisbull No Ho any surgical intervention in past
Personal history
bull Laborerbull Studied up to 10th standardbull Smokerbull Non alcoholicbull Married bull Normal sleep appetite bowel and bladder
habitsbull Diet - vegetarian
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
bull VENUE AUDITORIUM OF THE SMS HOSPITAL (audio-visual IC ndash Dr PD Meena Dept Of Medicine)
bull Day amp date 2nd Friday of every monthbull Time 1230 pm to 130 pmbull ATTENDENCE TO BE COMPULSORY FOR ALL FACULTY
MEMBERS OF THE INSTITUION ndash PHODs TO ENSURE SMOOTH FUNCTIONING OF ALL PATIENT SERVICES
bull Audience all faculty members of the SMSMC all senior residents ex-faculty members
SMSMC-CPC
SMSMC-CPCFormat
bull Dates allotted to each department for the full calendar yearbull No cancellation permitted other than if Friday is a GHbull Mutual exchange with another dept permitted with info to and
permission from office of the P amp Cbull First 15 mins of presentation to include highlights of work done in the
dept major publications awards honours amp achievements of the deptbull Subsequent 30 mins to include multi-speciality case presentation of
interest to as many depts As possible ndash presentation by multiple faculty amp multiple depts encouraged (example - case presentation by dept of Medicine radiological findings by dept of Radio-diagnosis surgical finding by dept of Surgery histo-path diagnosis by dept of pathology dd amp treatment by dept of oncology)
bull Last 15 mins for q amp a
Next CPC
Dept of Neurology12 August 2016
INTRODUCTION
ProfDr S M Sharma Add PrincipalHOD Dept of Cardiology
Department of CardiologySawai Man Singh Medical College
Hospital Jaipur
History
bull Department of cardiology is one of the esteemed department of SMS Medical college
bull Started in 1992 as a separate Cardiology unit in the department of Medicine under guidance of Dr Amrit Khalsa and Dr V S Baldwa
bull When coronary intervention was being developed in western world in Nineties First Cath lab of the department established in 1992
bull Separate Department of Cardiology established in 1995 under Prof Dr Madhok with 50 beds alloted
bull DM cardiology course started in the department in 1999 with two students and subsequently seats increased to eight in 2010
bull Separate ICCU started in 2005 with 12 beds facility in main ICCU and 10 beds in semi ICCU
bull In 2006 new Cath lab established having capabilities of diverse interventional procedures and EP facility
bull Third Unit in cardiology started in 2008 and also OPD days increased from four to seven days a week
bull New 3-D echo machine Holter monitors and TMT machines were added in the department in 2009
bull In 2013 another gem added with establishment of second cath lab having facilities such as IVUS FFR Dyna CT imaging IABP DSA booster facility which is helping to provide world class cardiac and peripheral intervention
bull In 2014 fourth unit startedbull Recently renovation of Post Catheterisation
Recovery Area(PCRA) dedicated to post cath patients completed which increased its bed capacity from 7 to 21
PRESENT SCENARIO OF THE DEPARTMENTbull No of consultants-12 bull These include 7 Professors 1 Associate Professor 3 Asst Professors and 1 MO
bull Prof Dr Anoop Jainbull Prof Dr Shashi Mohan Sharma(PHOD)bull Prof Dr Rajeev Bagarhattabull Prof Dr V V Agarwalbull Prof Dr Vijay Pathakbull Prof Dr Chandrabhan Meenabull Prof Dr Deepak Maheshwaribull Asso Prof Dr Neeraj Chaturvedibull Asst Prof Dr Sohan Kumar Sharmabull Asst Prof Dr Ritesh Guptabull Asst Prof Dr Omprakash Khojabull Dr Sunil Sharma MO
bull No of Residents- 24 (8 each year)
bull No of DET( Diploma in ECG Technician) students- 20 per yearbull No of equipment- - Two cath labs with state of the art equipment like IVUS FFR CT+3D imaging IABP Rotablator EP system Electrocautery etc - One 3-D Echo machine and four 2-D echo machines distributed in Echo lab Cath lab ICCU and Emergency dept - 2 TMT machines - 11 Holter Devices
CATH LAB 1
CATH LAB 2
CATH LAB CONSOLE
ECHO LAB
bull OPD runs 7 days a weekbull 24 hours Cardiology Emergency services with
round the clock presence of DM residentbull No of patients visited Cardiology department
last year Numbers
No of patients attending OPD 96160
No of Indoor admissions 10808
No of 2D-Echo 19183
No of Holter monitoring 954
No of TMT 5749
No of Cath Interventions 8834
bull We are also providing Super speciality services to Seth S R Goyal satellite hospital Sethi colony Jaipur- 3 days a week
bull Primary PCI is being done round the clock and this facility is present in only few Govt Hospitals anywhere in India Also the Door to balloon time in our hospital is around 70 min which is well under the international recommendations of less than 90 min
bull An exhaustive DM Cardiology teaching programme is going on in the department five days a week with full participation of students and consultants
bull Our students who come for DM get excellent exposure to clinical and interventional work which sets them not only at par but I take pride in saying that they are even better than their counterparts in leading premier institutes of the country This is the reason why most of them are very well settled now and are doing very well wherever they are
bull Our department also offers Diploma for ECG Technician(DET) course in which 20 students get admitted yearly
Research Activities
Research Activities
Average no of studies done per year 22
Average no of papers published in reputed national amp international journals per year
14
In last 6 years our students have published around 100 research papers in national and international reputed journals
Presently work in the department is covering all major aspects of cardiology includingbull PTCA + STENTING including complex angioplastiesbull Primary PCIbull Rotablationbull IVUS FFRbull Carotid and other peripheral angioplastiesbull Renal angioplastiesbull BMVBPV BAVbull ASD VSD PDA Device closurebull Permanent pacemaker implantations including Dual chamber and MRI
compatible pacemakersbull AICDbull CRT-P CRT-Dbull EPS and RFAbull Arterial Embolizationbull Endomyocardial biopsy
bull These are comparable to most of the leading Govt Institutes anywhere in India
bull We are also trying to upgrade our facilities in the field of structural heart disease which includes endovascular treatment of aortic aneurysm dissection paravalvular leak closure TAVI etc
bull Lastly the Honorable CM has sanctioned a new Cath lab for our department in the present budget which will be installed soon A new 3-D Echo machine is being installed in next 2-3 months This will further improve the working in the department for better care of the poor patients
THANK YOU
CPC caseDepartment Cardiology
8th July 2016
Presenter Dr Rakesh Kumar Ola Dr Daulat Singh Meena
Cardiology discussant Dr Sohan K Sharma Assistant Prof Deptt Cardiology
Respiratory discussant Dr Sheetu Singh Assistant Prof Chest amp TB
Medicine discussant Dr Ashutosh Daga Resident Deptt Of Medicine ProfDrHemant Malhotra PHOD Deptt Of Medicine
Radiology discussant Dr Sachin Lamba Resident RadiologyDr RK Yadav Astt Prof Radiology
Pathology discussant Dr Neetu Aggarwal Sr Resident PathologyDr Anita Harsh Assoc Prof Pathology
Case Presenter
Dr Rakesh Kumar OlaIIIrd Year Resident
Department of Cardiology
Presenting complaints
A 38y old male resident of Jhalawar-Rajasthan presented with complaints of bull Fever on and off-12 monthsbull Cough- 12 monthsbull Weight loss-12 monthsbull Shortness of breath on exertion- 6 months bull Bilateral lower limb swelling- 15-20 days
History of presenting illness
Asymptomatic till 12 month back when he developed - Fever bull Insidious bull Low grade bull Intermittent typebull Each episode lasted for 10-15 daysbull Not associated with chills and rigor bull No diurnal variation bull Relieved by medications
History of presenting illness
Cough -12 monthbull Non-productive coughbull On and Off bull Each episode lasted for 20-30 days bull Cough was not associated with hemoptysis
chest heaviness noisy breathing and post-nasal discharge
bull No postural diurnal or seasonal variation
History of presenting illness
Weight loss -12 monthbull Patient had ho of significant weight loss of
5kg in last 12 months associated with easy fatigability
History of presenting illness
Shortness of breath-6 monthsbull Insidious onset bull Patient initially complain SOB on more than ordinary
activity and it progressively increased over 5 months and from last one month patient having SOB on less than ordinary physical activity (NYHA grade I to III ) but not at rest
bull SOB was not worsen by lying down and had no HO of episodic breathlessness during night
bull No postural or diurnal or seasonal variation
History of presenting illness
Bilateral lower limb swelling- 15-20 daysbull Lower limb swelling started from ankle joint
and progressed up to knee joint bull Not associated with morning facial puffiness
and abdominal fullnessbull No pain tenderness or warmth of lower limb
History of presenting illness
No history of bull Personal or family history of atopy or allergy like
itching skin lesions urticaria noisy breathing or seasonal variations
bull History of joint pains oral ulcersbull Travel out of statebull History of drugs or radiation exposurebull Occupational exposure of dust or smoke
History of presenting illness
No history of bull Recurrent episodes of diarrhoea abdominal pain
dysphagia or icterusbull Chest pain bull Palpitationbull Loss of consciousness bull Ho of focal neurological deficit
Past medical history
bull Patient had history of recurrent admissions and received treatment for enteric fever and malaria though patient had no relief in symptoms from same
bull No HO of DM HTN Tuberculosisbull No Ho any surgical intervention in past
Personal history
bull Laborerbull Studied up to 10th standardbull Smokerbull Non alcoholicbull Married bull Normal sleep appetite bowel and bladder
habitsbull Diet - vegetarian
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
SMSMC-CPCFormat
bull Dates allotted to each department for the full calendar yearbull No cancellation permitted other than if Friday is a GHbull Mutual exchange with another dept permitted with info to and
permission from office of the P amp Cbull First 15 mins of presentation to include highlights of work done in the
dept major publications awards honours amp achievements of the deptbull Subsequent 30 mins to include multi-speciality case presentation of
interest to as many depts As possible ndash presentation by multiple faculty amp multiple depts encouraged (example - case presentation by dept of Medicine radiological findings by dept of Radio-diagnosis surgical finding by dept of Surgery histo-path diagnosis by dept of pathology dd amp treatment by dept of oncology)
bull Last 15 mins for q amp a
Next CPC
Dept of Neurology12 August 2016
INTRODUCTION
ProfDr S M Sharma Add PrincipalHOD Dept of Cardiology
Department of CardiologySawai Man Singh Medical College
Hospital Jaipur
History
bull Department of cardiology is one of the esteemed department of SMS Medical college
bull Started in 1992 as a separate Cardiology unit in the department of Medicine under guidance of Dr Amrit Khalsa and Dr V S Baldwa
bull When coronary intervention was being developed in western world in Nineties First Cath lab of the department established in 1992
bull Separate Department of Cardiology established in 1995 under Prof Dr Madhok with 50 beds alloted
bull DM cardiology course started in the department in 1999 with two students and subsequently seats increased to eight in 2010
bull Separate ICCU started in 2005 with 12 beds facility in main ICCU and 10 beds in semi ICCU
bull In 2006 new Cath lab established having capabilities of diverse interventional procedures and EP facility
bull Third Unit in cardiology started in 2008 and also OPD days increased from four to seven days a week
bull New 3-D echo machine Holter monitors and TMT machines were added in the department in 2009
bull In 2013 another gem added with establishment of second cath lab having facilities such as IVUS FFR Dyna CT imaging IABP DSA booster facility which is helping to provide world class cardiac and peripheral intervention
bull In 2014 fourth unit startedbull Recently renovation of Post Catheterisation
Recovery Area(PCRA) dedicated to post cath patients completed which increased its bed capacity from 7 to 21
PRESENT SCENARIO OF THE DEPARTMENTbull No of consultants-12 bull These include 7 Professors 1 Associate Professor 3 Asst Professors and 1 MO
bull Prof Dr Anoop Jainbull Prof Dr Shashi Mohan Sharma(PHOD)bull Prof Dr Rajeev Bagarhattabull Prof Dr V V Agarwalbull Prof Dr Vijay Pathakbull Prof Dr Chandrabhan Meenabull Prof Dr Deepak Maheshwaribull Asso Prof Dr Neeraj Chaturvedibull Asst Prof Dr Sohan Kumar Sharmabull Asst Prof Dr Ritesh Guptabull Asst Prof Dr Omprakash Khojabull Dr Sunil Sharma MO
bull No of Residents- 24 (8 each year)
bull No of DET( Diploma in ECG Technician) students- 20 per yearbull No of equipment- - Two cath labs with state of the art equipment like IVUS FFR CT+3D imaging IABP Rotablator EP system Electrocautery etc - One 3-D Echo machine and four 2-D echo machines distributed in Echo lab Cath lab ICCU and Emergency dept - 2 TMT machines - 11 Holter Devices
CATH LAB 1
CATH LAB 2
CATH LAB CONSOLE
ECHO LAB
bull OPD runs 7 days a weekbull 24 hours Cardiology Emergency services with
round the clock presence of DM residentbull No of patients visited Cardiology department
last year Numbers
No of patients attending OPD 96160
No of Indoor admissions 10808
No of 2D-Echo 19183
No of Holter monitoring 954
No of TMT 5749
No of Cath Interventions 8834
bull We are also providing Super speciality services to Seth S R Goyal satellite hospital Sethi colony Jaipur- 3 days a week
bull Primary PCI is being done round the clock and this facility is present in only few Govt Hospitals anywhere in India Also the Door to balloon time in our hospital is around 70 min which is well under the international recommendations of less than 90 min
bull An exhaustive DM Cardiology teaching programme is going on in the department five days a week with full participation of students and consultants
bull Our students who come for DM get excellent exposure to clinical and interventional work which sets them not only at par but I take pride in saying that they are even better than their counterparts in leading premier institutes of the country This is the reason why most of them are very well settled now and are doing very well wherever they are
bull Our department also offers Diploma for ECG Technician(DET) course in which 20 students get admitted yearly
Research Activities
Research Activities
Average no of studies done per year 22
Average no of papers published in reputed national amp international journals per year
14
In last 6 years our students have published around 100 research papers in national and international reputed journals
Presently work in the department is covering all major aspects of cardiology includingbull PTCA + STENTING including complex angioplastiesbull Primary PCIbull Rotablationbull IVUS FFRbull Carotid and other peripheral angioplastiesbull Renal angioplastiesbull BMVBPV BAVbull ASD VSD PDA Device closurebull Permanent pacemaker implantations including Dual chamber and MRI
compatible pacemakersbull AICDbull CRT-P CRT-Dbull EPS and RFAbull Arterial Embolizationbull Endomyocardial biopsy
bull These are comparable to most of the leading Govt Institutes anywhere in India
bull We are also trying to upgrade our facilities in the field of structural heart disease which includes endovascular treatment of aortic aneurysm dissection paravalvular leak closure TAVI etc
bull Lastly the Honorable CM has sanctioned a new Cath lab for our department in the present budget which will be installed soon A new 3-D Echo machine is being installed in next 2-3 months This will further improve the working in the department for better care of the poor patients
THANK YOU
CPC caseDepartment Cardiology
8th July 2016
Presenter Dr Rakesh Kumar Ola Dr Daulat Singh Meena
Cardiology discussant Dr Sohan K Sharma Assistant Prof Deptt Cardiology
Respiratory discussant Dr Sheetu Singh Assistant Prof Chest amp TB
Medicine discussant Dr Ashutosh Daga Resident Deptt Of Medicine ProfDrHemant Malhotra PHOD Deptt Of Medicine
Radiology discussant Dr Sachin Lamba Resident RadiologyDr RK Yadav Astt Prof Radiology
Pathology discussant Dr Neetu Aggarwal Sr Resident PathologyDr Anita Harsh Assoc Prof Pathology
Case Presenter
Dr Rakesh Kumar OlaIIIrd Year Resident
Department of Cardiology
Presenting complaints
A 38y old male resident of Jhalawar-Rajasthan presented with complaints of bull Fever on and off-12 monthsbull Cough- 12 monthsbull Weight loss-12 monthsbull Shortness of breath on exertion- 6 months bull Bilateral lower limb swelling- 15-20 days
History of presenting illness
Asymptomatic till 12 month back when he developed - Fever bull Insidious bull Low grade bull Intermittent typebull Each episode lasted for 10-15 daysbull Not associated with chills and rigor bull No diurnal variation bull Relieved by medications
History of presenting illness
Cough -12 monthbull Non-productive coughbull On and Off bull Each episode lasted for 20-30 days bull Cough was not associated with hemoptysis
chest heaviness noisy breathing and post-nasal discharge
bull No postural diurnal or seasonal variation
History of presenting illness
Weight loss -12 monthbull Patient had ho of significant weight loss of
5kg in last 12 months associated with easy fatigability
History of presenting illness
Shortness of breath-6 monthsbull Insidious onset bull Patient initially complain SOB on more than ordinary
activity and it progressively increased over 5 months and from last one month patient having SOB on less than ordinary physical activity (NYHA grade I to III ) but not at rest
bull SOB was not worsen by lying down and had no HO of episodic breathlessness during night
bull No postural or diurnal or seasonal variation
History of presenting illness
Bilateral lower limb swelling- 15-20 daysbull Lower limb swelling started from ankle joint
and progressed up to knee joint bull Not associated with morning facial puffiness
and abdominal fullnessbull No pain tenderness or warmth of lower limb
History of presenting illness
No history of bull Personal or family history of atopy or allergy like
itching skin lesions urticaria noisy breathing or seasonal variations
bull History of joint pains oral ulcersbull Travel out of statebull History of drugs or radiation exposurebull Occupational exposure of dust or smoke
History of presenting illness
No history of bull Recurrent episodes of diarrhoea abdominal pain
dysphagia or icterusbull Chest pain bull Palpitationbull Loss of consciousness bull Ho of focal neurological deficit
Past medical history
bull Patient had history of recurrent admissions and received treatment for enteric fever and malaria though patient had no relief in symptoms from same
bull No HO of DM HTN Tuberculosisbull No Ho any surgical intervention in past
Personal history
bull Laborerbull Studied up to 10th standardbull Smokerbull Non alcoholicbull Married bull Normal sleep appetite bowel and bladder
habitsbull Diet - vegetarian
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
Next CPC
Dept of Neurology12 August 2016
INTRODUCTION
ProfDr S M Sharma Add PrincipalHOD Dept of Cardiology
Department of CardiologySawai Man Singh Medical College
Hospital Jaipur
History
bull Department of cardiology is one of the esteemed department of SMS Medical college
bull Started in 1992 as a separate Cardiology unit in the department of Medicine under guidance of Dr Amrit Khalsa and Dr V S Baldwa
bull When coronary intervention was being developed in western world in Nineties First Cath lab of the department established in 1992
bull Separate Department of Cardiology established in 1995 under Prof Dr Madhok with 50 beds alloted
bull DM cardiology course started in the department in 1999 with two students and subsequently seats increased to eight in 2010
bull Separate ICCU started in 2005 with 12 beds facility in main ICCU and 10 beds in semi ICCU
bull In 2006 new Cath lab established having capabilities of diverse interventional procedures and EP facility
bull Third Unit in cardiology started in 2008 and also OPD days increased from four to seven days a week
bull New 3-D echo machine Holter monitors and TMT machines were added in the department in 2009
bull In 2013 another gem added with establishment of second cath lab having facilities such as IVUS FFR Dyna CT imaging IABP DSA booster facility which is helping to provide world class cardiac and peripheral intervention
bull In 2014 fourth unit startedbull Recently renovation of Post Catheterisation
Recovery Area(PCRA) dedicated to post cath patients completed which increased its bed capacity from 7 to 21
PRESENT SCENARIO OF THE DEPARTMENTbull No of consultants-12 bull These include 7 Professors 1 Associate Professor 3 Asst Professors and 1 MO
bull Prof Dr Anoop Jainbull Prof Dr Shashi Mohan Sharma(PHOD)bull Prof Dr Rajeev Bagarhattabull Prof Dr V V Agarwalbull Prof Dr Vijay Pathakbull Prof Dr Chandrabhan Meenabull Prof Dr Deepak Maheshwaribull Asso Prof Dr Neeraj Chaturvedibull Asst Prof Dr Sohan Kumar Sharmabull Asst Prof Dr Ritesh Guptabull Asst Prof Dr Omprakash Khojabull Dr Sunil Sharma MO
bull No of Residents- 24 (8 each year)
bull No of DET( Diploma in ECG Technician) students- 20 per yearbull No of equipment- - Two cath labs with state of the art equipment like IVUS FFR CT+3D imaging IABP Rotablator EP system Electrocautery etc - One 3-D Echo machine and four 2-D echo machines distributed in Echo lab Cath lab ICCU and Emergency dept - 2 TMT machines - 11 Holter Devices
CATH LAB 1
CATH LAB 2
CATH LAB CONSOLE
ECHO LAB
bull OPD runs 7 days a weekbull 24 hours Cardiology Emergency services with
round the clock presence of DM residentbull No of patients visited Cardiology department
last year Numbers
No of patients attending OPD 96160
No of Indoor admissions 10808
No of 2D-Echo 19183
No of Holter monitoring 954
No of TMT 5749
No of Cath Interventions 8834
bull We are also providing Super speciality services to Seth S R Goyal satellite hospital Sethi colony Jaipur- 3 days a week
bull Primary PCI is being done round the clock and this facility is present in only few Govt Hospitals anywhere in India Also the Door to balloon time in our hospital is around 70 min which is well under the international recommendations of less than 90 min
bull An exhaustive DM Cardiology teaching programme is going on in the department five days a week with full participation of students and consultants
bull Our students who come for DM get excellent exposure to clinical and interventional work which sets them not only at par but I take pride in saying that they are even better than their counterparts in leading premier institutes of the country This is the reason why most of them are very well settled now and are doing very well wherever they are
bull Our department also offers Diploma for ECG Technician(DET) course in which 20 students get admitted yearly
Research Activities
Research Activities
Average no of studies done per year 22
Average no of papers published in reputed national amp international journals per year
14
In last 6 years our students have published around 100 research papers in national and international reputed journals
Presently work in the department is covering all major aspects of cardiology includingbull PTCA + STENTING including complex angioplastiesbull Primary PCIbull Rotablationbull IVUS FFRbull Carotid and other peripheral angioplastiesbull Renal angioplastiesbull BMVBPV BAVbull ASD VSD PDA Device closurebull Permanent pacemaker implantations including Dual chamber and MRI
compatible pacemakersbull AICDbull CRT-P CRT-Dbull EPS and RFAbull Arterial Embolizationbull Endomyocardial biopsy
bull These are comparable to most of the leading Govt Institutes anywhere in India
bull We are also trying to upgrade our facilities in the field of structural heart disease which includes endovascular treatment of aortic aneurysm dissection paravalvular leak closure TAVI etc
bull Lastly the Honorable CM has sanctioned a new Cath lab for our department in the present budget which will be installed soon A new 3-D Echo machine is being installed in next 2-3 months This will further improve the working in the department for better care of the poor patients
THANK YOU
CPC caseDepartment Cardiology
8th July 2016
Presenter Dr Rakesh Kumar Ola Dr Daulat Singh Meena
Cardiology discussant Dr Sohan K Sharma Assistant Prof Deptt Cardiology
Respiratory discussant Dr Sheetu Singh Assistant Prof Chest amp TB
Medicine discussant Dr Ashutosh Daga Resident Deptt Of Medicine ProfDrHemant Malhotra PHOD Deptt Of Medicine
Radiology discussant Dr Sachin Lamba Resident RadiologyDr RK Yadav Astt Prof Radiology
Pathology discussant Dr Neetu Aggarwal Sr Resident PathologyDr Anita Harsh Assoc Prof Pathology
Case Presenter
Dr Rakesh Kumar OlaIIIrd Year Resident
Department of Cardiology
Presenting complaints
A 38y old male resident of Jhalawar-Rajasthan presented with complaints of bull Fever on and off-12 monthsbull Cough- 12 monthsbull Weight loss-12 monthsbull Shortness of breath on exertion- 6 months bull Bilateral lower limb swelling- 15-20 days
History of presenting illness
Asymptomatic till 12 month back when he developed - Fever bull Insidious bull Low grade bull Intermittent typebull Each episode lasted for 10-15 daysbull Not associated with chills and rigor bull No diurnal variation bull Relieved by medications
History of presenting illness
Cough -12 monthbull Non-productive coughbull On and Off bull Each episode lasted for 20-30 days bull Cough was not associated with hemoptysis
chest heaviness noisy breathing and post-nasal discharge
bull No postural diurnal or seasonal variation
History of presenting illness
Weight loss -12 monthbull Patient had ho of significant weight loss of
5kg in last 12 months associated with easy fatigability
History of presenting illness
Shortness of breath-6 monthsbull Insidious onset bull Patient initially complain SOB on more than ordinary
activity and it progressively increased over 5 months and from last one month patient having SOB on less than ordinary physical activity (NYHA grade I to III ) but not at rest
bull SOB was not worsen by lying down and had no HO of episodic breathlessness during night
bull No postural or diurnal or seasonal variation
History of presenting illness
Bilateral lower limb swelling- 15-20 daysbull Lower limb swelling started from ankle joint
and progressed up to knee joint bull Not associated with morning facial puffiness
and abdominal fullnessbull No pain tenderness or warmth of lower limb
History of presenting illness
No history of bull Personal or family history of atopy or allergy like
itching skin lesions urticaria noisy breathing or seasonal variations
bull History of joint pains oral ulcersbull Travel out of statebull History of drugs or radiation exposurebull Occupational exposure of dust or smoke
History of presenting illness
No history of bull Recurrent episodes of diarrhoea abdominal pain
dysphagia or icterusbull Chest pain bull Palpitationbull Loss of consciousness bull Ho of focal neurological deficit
Past medical history
bull Patient had history of recurrent admissions and received treatment for enteric fever and malaria though patient had no relief in symptoms from same
bull No HO of DM HTN Tuberculosisbull No Ho any surgical intervention in past
Personal history
bull Laborerbull Studied up to 10th standardbull Smokerbull Non alcoholicbull Married bull Normal sleep appetite bowel and bladder
habitsbull Diet - vegetarian
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber

INTRODUCTION
ProfDr S M Sharma Add PrincipalHOD Dept of Cardiology
Department of CardiologySawai Man Singh Medical College
Hospital Jaipur
History
bull Department of cardiology is one of the esteemed department of SMS Medical college
bull Started in 1992 as a separate Cardiology unit in the department of Medicine under guidance of Dr Amrit Khalsa and Dr V S Baldwa
bull When coronary intervention was being developed in western world in Nineties First Cath lab of the department established in 1992
bull Separate Department of Cardiology established in 1995 under Prof Dr Madhok with 50 beds alloted
bull DM cardiology course started in the department in 1999 with two students and subsequently seats increased to eight in 2010
bull Separate ICCU started in 2005 with 12 beds facility in main ICCU and 10 beds in semi ICCU
bull In 2006 new Cath lab established having capabilities of diverse interventional procedures and EP facility
bull Third Unit in cardiology started in 2008 and also OPD days increased from four to seven days a week
bull New 3-D echo machine Holter monitors and TMT machines were added in the department in 2009
bull In 2013 another gem added with establishment of second cath lab having facilities such as IVUS FFR Dyna CT imaging IABP DSA booster facility which is helping to provide world class cardiac and peripheral intervention
bull In 2014 fourth unit startedbull Recently renovation of Post Catheterisation
Recovery Area(PCRA) dedicated to post cath patients completed which increased its bed capacity from 7 to 21
PRESENT SCENARIO OF THE DEPARTMENTbull No of consultants-12 bull These include 7 Professors 1 Associate Professor 3 Asst Professors and 1 MO
bull Prof Dr Anoop Jainbull Prof Dr Shashi Mohan Sharma(PHOD)bull Prof Dr Rajeev Bagarhattabull Prof Dr V V Agarwalbull Prof Dr Vijay Pathakbull Prof Dr Chandrabhan Meenabull Prof Dr Deepak Maheshwaribull Asso Prof Dr Neeraj Chaturvedibull Asst Prof Dr Sohan Kumar Sharmabull Asst Prof Dr Ritesh Guptabull Asst Prof Dr Omprakash Khojabull Dr Sunil Sharma MO
bull No of Residents- 24 (8 each year)
bull No of DET( Diploma in ECG Technician) students- 20 per yearbull No of equipment- - Two cath labs with state of the art equipment like IVUS FFR CT+3D imaging IABP Rotablator EP system Electrocautery etc - One 3-D Echo machine and four 2-D echo machines distributed in Echo lab Cath lab ICCU and Emergency dept - 2 TMT machines - 11 Holter Devices
CATH LAB 1
CATH LAB 2
CATH LAB CONSOLE
ECHO LAB
bull OPD runs 7 days a weekbull 24 hours Cardiology Emergency services with
round the clock presence of DM residentbull No of patients visited Cardiology department
last year Numbers
No of patients attending OPD 96160
No of Indoor admissions 10808
No of 2D-Echo 19183
No of Holter monitoring 954
No of TMT 5749
No of Cath Interventions 8834
bull We are also providing Super speciality services to Seth S R Goyal satellite hospital Sethi colony Jaipur- 3 days a week
bull Primary PCI is being done round the clock and this facility is present in only few Govt Hospitals anywhere in India Also the Door to balloon time in our hospital is around 70 min which is well under the international recommendations of less than 90 min
bull An exhaustive DM Cardiology teaching programme is going on in the department five days a week with full participation of students and consultants
bull Our students who come for DM get excellent exposure to clinical and interventional work which sets them not only at par but I take pride in saying that they are even better than their counterparts in leading premier institutes of the country This is the reason why most of them are very well settled now and are doing very well wherever they are
bull Our department also offers Diploma for ECG Technician(DET) course in which 20 students get admitted yearly
Research Activities
Research Activities
Average no of studies done per year 22
Average no of papers published in reputed national amp international journals per year
14
In last 6 years our students have published around 100 research papers in national and international reputed journals
Presently work in the department is covering all major aspects of cardiology includingbull PTCA + STENTING including complex angioplastiesbull Primary PCIbull Rotablationbull IVUS FFRbull Carotid and other peripheral angioplastiesbull Renal angioplastiesbull BMVBPV BAVbull ASD VSD PDA Device closurebull Permanent pacemaker implantations including Dual chamber and MRI
compatible pacemakersbull AICDbull CRT-P CRT-Dbull EPS and RFAbull Arterial Embolizationbull Endomyocardial biopsy
bull These are comparable to most of the leading Govt Institutes anywhere in India
bull We are also trying to upgrade our facilities in the field of structural heart disease which includes endovascular treatment of aortic aneurysm dissection paravalvular leak closure TAVI etc
bull Lastly the Honorable CM has sanctioned a new Cath lab for our department in the present budget which will be installed soon A new 3-D Echo machine is being installed in next 2-3 months This will further improve the working in the department for better care of the poor patients
THANK YOU
CPC caseDepartment Cardiology
8th July 2016
Presenter Dr Rakesh Kumar Ola Dr Daulat Singh Meena
Cardiology discussant Dr Sohan K Sharma Assistant Prof Deptt Cardiology
Respiratory discussant Dr Sheetu Singh Assistant Prof Chest amp TB
Medicine discussant Dr Ashutosh Daga Resident Deptt Of Medicine ProfDrHemant Malhotra PHOD Deptt Of Medicine
Radiology discussant Dr Sachin Lamba Resident RadiologyDr RK Yadav Astt Prof Radiology
Pathology discussant Dr Neetu Aggarwal Sr Resident PathologyDr Anita Harsh Assoc Prof Pathology
Case Presenter
Dr Rakesh Kumar OlaIIIrd Year Resident
Department of Cardiology
Presenting complaints
A 38y old male resident of Jhalawar-Rajasthan presented with complaints of bull Fever on and off-12 monthsbull Cough- 12 monthsbull Weight loss-12 monthsbull Shortness of breath on exertion- 6 months bull Bilateral lower limb swelling- 15-20 days
History of presenting illness
Asymptomatic till 12 month back when he developed - Fever bull Insidious bull Low grade bull Intermittent typebull Each episode lasted for 10-15 daysbull Not associated with chills and rigor bull No diurnal variation bull Relieved by medications
History of presenting illness
Cough -12 monthbull Non-productive coughbull On and Off bull Each episode lasted for 20-30 days bull Cough was not associated with hemoptysis
chest heaviness noisy breathing and post-nasal discharge
bull No postural diurnal or seasonal variation
History of presenting illness
Weight loss -12 monthbull Patient had ho of significant weight loss of
5kg in last 12 months associated with easy fatigability
History of presenting illness
Shortness of breath-6 monthsbull Insidious onset bull Patient initially complain SOB on more than ordinary
activity and it progressively increased over 5 months and from last one month patient having SOB on less than ordinary physical activity (NYHA grade I to III ) but not at rest
bull SOB was not worsen by lying down and had no HO of episodic breathlessness during night
bull No postural or diurnal or seasonal variation
History of presenting illness
Bilateral lower limb swelling- 15-20 daysbull Lower limb swelling started from ankle joint
and progressed up to knee joint bull Not associated with morning facial puffiness
and abdominal fullnessbull No pain tenderness or warmth of lower limb
History of presenting illness
No history of bull Personal or family history of atopy or allergy like
itching skin lesions urticaria noisy breathing or seasonal variations
bull History of joint pains oral ulcersbull Travel out of statebull History of drugs or radiation exposurebull Occupational exposure of dust or smoke
History of presenting illness
No history of bull Recurrent episodes of diarrhoea abdominal pain
dysphagia or icterusbull Chest pain bull Palpitationbull Loss of consciousness bull Ho of focal neurological deficit
Past medical history
bull Patient had history of recurrent admissions and received treatment for enteric fever and malaria though patient had no relief in symptoms from same
bull No HO of DM HTN Tuberculosisbull No Ho any surgical intervention in past
Personal history
bull Laborerbull Studied up to 10th standardbull Smokerbull Non alcoholicbull Married bull Normal sleep appetite bowel and bladder
habitsbull Diet - vegetarian
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber

History
bull Department of cardiology is one of the esteemed department of SMS Medical college
bull Started in 1992 as a separate Cardiology unit in the department of Medicine under guidance of Dr Amrit Khalsa and Dr V S Baldwa
bull When coronary intervention was being developed in western world in Nineties First Cath lab of the department established in 1992
bull Separate Department of Cardiology established in 1995 under Prof Dr Madhok with 50 beds alloted
bull DM cardiology course started in the department in 1999 with two students and subsequently seats increased to eight in 2010
bull Separate ICCU started in 2005 with 12 beds facility in main ICCU and 10 beds in semi ICCU
bull In 2006 new Cath lab established having capabilities of diverse interventional procedures and EP facility
bull Third Unit in cardiology started in 2008 and also OPD days increased from four to seven days a week
bull New 3-D echo machine Holter monitors and TMT machines were added in the department in 2009
bull In 2013 another gem added with establishment of second cath lab having facilities such as IVUS FFR Dyna CT imaging IABP DSA booster facility which is helping to provide world class cardiac and peripheral intervention
bull In 2014 fourth unit startedbull Recently renovation of Post Catheterisation
Recovery Area(PCRA) dedicated to post cath patients completed which increased its bed capacity from 7 to 21
PRESENT SCENARIO OF THE DEPARTMENTbull No of consultants-12 bull These include 7 Professors 1 Associate Professor 3 Asst Professors and 1 MO
bull Prof Dr Anoop Jainbull Prof Dr Shashi Mohan Sharma(PHOD)bull Prof Dr Rajeev Bagarhattabull Prof Dr V V Agarwalbull Prof Dr Vijay Pathakbull Prof Dr Chandrabhan Meenabull Prof Dr Deepak Maheshwaribull Asso Prof Dr Neeraj Chaturvedibull Asst Prof Dr Sohan Kumar Sharmabull Asst Prof Dr Ritesh Guptabull Asst Prof Dr Omprakash Khojabull Dr Sunil Sharma MO
bull No of Residents- 24 (8 each year)
bull No of DET( Diploma in ECG Technician) students- 20 per yearbull No of equipment- - Two cath labs with state of the art equipment like IVUS FFR CT+3D imaging IABP Rotablator EP system Electrocautery etc - One 3-D Echo machine and four 2-D echo machines distributed in Echo lab Cath lab ICCU and Emergency dept - 2 TMT machines - 11 Holter Devices
CATH LAB 1
CATH LAB 2
CATH LAB CONSOLE
ECHO LAB
bull OPD runs 7 days a weekbull 24 hours Cardiology Emergency services with
round the clock presence of DM residentbull No of patients visited Cardiology department
last year Numbers
No of patients attending OPD 96160
No of Indoor admissions 10808
No of 2D-Echo 19183
No of Holter monitoring 954
No of TMT 5749
No of Cath Interventions 8834
bull We are also providing Super speciality services to Seth S R Goyal satellite hospital Sethi colony Jaipur- 3 days a week
bull Primary PCI is being done round the clock and this facility is present in only few Govt Hospitals anywhere in India Also the Door to balloon time in our hospital is around 70 min which is well under the international recommendations of less than 90 min
bull An exhaustive DM Cardiology teaching programme is going on in the department five days a week with full participation of students and consultants
bull Our students who come for DM get excellent exposure to clinical and interventional work which sets them not only at par but I take pride in saying that they are even better than their counterparts in leading premier institutes of the country This is the reason why most of them are very well settled now and are doing very well wherever they are
bull Our department also offers Diploma for ECG Technician(DET) course in which 20 students get admitted yearly
Research Activities
Research Activities
Average no of studies done per year 22
Average no of papers published in reputed national amp international journals per year
14
In last 6 years our students have published around 100 research papers in national and international reputed journals
Presently work in the department is covering all major aspects of cardiology includingbull PTCA + STENTING including complex angioplastiesbull Primary PCIbull Rotablationbull IVUS FFRbull Carotid and other peripheral angioplastiesbull Renal angioplastiesbull BMVBPV BAVbull ASD VSD PDA Device closurebull Permanent pacemaker implantations including Dual chamber and MRI
compatible pacemakersbull AICDbull CRT-P CRT-Dbull EPS and RFAbull Arterial Embolizationbull Endomyocardial biopsy
bull These are comparable to most of the leading Govt Institutes anywhere in India
bull We are also trying to upgrade our facilities in the field of structural heart disease which includes endovascular treatment of aortic aneurysm dissection paravalvular leak closure TAVI etc
bull Lastly the Honorable CM has sanctioned a new Cath lab for our department in the present budget which will be installed soon A new 3-D Echo machine is being installed in next 2-3 months This will further improve the working in the department for better care of the poor patients
THANK YOU
CPC caseDepartment Cardiology
8th July 2016
Presenter Dr Rakesh Kumar Ola Dr Daulat Singh Meena
Cardiology discussant Dr Sohan K Sharma Assistant Prof Deptt Cardiology
Respiratory discussant Dr Sheetu Singh Assistant Prof Chest amp TB
Medicine discussant Dr Ashutosh Daga Resident Deptt Of Medicine ProfDrHemant Malhotra PHOD Deptt Of Medicine
Radiology discussant Dr Sachin Lamba Resident RadiologyDr RK Yadav Astt Prof Radiology
Pathology discussant Dr Neetu Aggarwal Sr Resident PathologyDr Anita Harsh Assoc Prof Pathology
Case Presenter
Dr Rakesh Kumar OlaIIIrd Year Resident
Department of Cardiology
Presenting complaints
A 38y old male resident of Jhalawar-Rajasthan presented with complaints of bull Fever on and off-12 monthsbull Cough- 12 monthsbull Weight loss-12 monthsbull Shortness of breath on exertion- 6 months bull Bilateral lower limb swelling- 15-20 days
History of presenting illness
Asymptomatic till 12 month back when he developed - Fever bull Insidious bull Low grade bull Intermittent typebull Each episode lasted for 10-15 daysbull Not associated with chills and rigor bull No diurnal variation bull Relieved by medications
History of presenting illness
Cough -12 monthbull Non-productive coughbull On and Off bull Each episode lasted for 20-30 days bull Cough was not associated with hemoptysis
chest heaviness noisy breathing and post-nasal discharge
bull No postural diurnal or seasonal variation
History of presenting illness
Weight loss -12 monthbull Patient had ho of significant weight loss of
5kg in last 12 months associated with easy fatigability
History of presenting illness
Shortness of breath-6 monthsbull Insidious onset bull Patient initially complain SOB on more than ordinary
activity and it progressively increased over 5 months and from last one month patient having SOB on less than ordinary physical activity (NYHA grade I to III ) but not at rest
bull SOB was not worsen by lying down and had no HO of episodic breathlessness during night
bull No postural or diurnal or seasonal variation
History of presenting illness
Bilateral lower limb swelling- 15-20 daysbull Lower limb swelling started from ankle joint
and progressed up to knee joint bull Not associated with morning facial puffiness
and abdominal fullnessbull No pain tenderness or warmth of lower limb
History of presenting illness
No history of bull Personal or family history of atopy or allergy like
itching skin lesions urticaria noisy breathing or seasonal variations
bull History of joint pains oral ulcersbull Travel out of statebull History of drugs or radiation exposurebull Occupational exposure of dust or smoke
History of presenting illness
No history of bull Recurrent episodes of diarrhoea abdominal pain
dysphagia or icterusbull Chest pain bull Palpitationbull Loss of consciousness bull Ho of focal neurological deficit
Past medical history
bull Patient had history of recurrent admissions and received treatment for enteric fever and malaria though patient had no relief in symptoms from same
bull No HO of DM HTN Tuberculosisbull No Ho any surgical intervention in past
Personal history
bull Laborerbull Studied up to 10th standardbull Smokerbull Non alcoholicbull Married bull Normal sleep appetite bowel and bladder
habitsbull Diet - vegetarian
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
bull Separate ICCU started in 2005 with 12 beds facility in main ICCU and 10 beds in semi ICCU
bull In 2006 new Cath lab established having capabilities of diverse interventional procedures and EP facility
bull Third Unit in cardiology started in 2008 and also OPD days increased from four to seven days a week
bull New 3-D echo machine Holter monitors and TMT machines were added in the department in 2009
bull In 2013 another gem added with establishment of second cath lab having facilities such as IVUS FFR Dyna CT imaging IABP DSA booster facility which is helping to provide world class cardiac and peripheral intervention
bull In 2014 fourth unit startedbull Recently renovation of Post Catheterisation
Recovery Area(PCRA) dedicated to post cath patients completed which increased its bed capacity from 7 to 21
PRESENT SCENARIO OF THE DEPARTMENTbull No of consultants-12 bull These include 7 Professors 1 Associate Professor 3 Asst Professors and 1 MO
bull Prof Dr Anoop Jainbull Prof Dr Shashi Mohan Sharma(PHOD)bull Prof Dr Rajeev Bagarhattabull Prof Dr V V Agarwalbull Prof Dr Vijay Pathakbull Prof Dr Chandrabhan Meenabull Prof Dr Deepak Maheshwaribull Asso Prof Dr Neeraj Chaturvedibull Asst Prof Dr Sohan Kumar Sharmabull Asst Prof Dr Ritesh Guptabull Asst Prof Dr Omprakash Khojabull Dr Sunil Sharma MO
bull No of Residents- 24 (8 each year)
bull No of DET( Diploma in ECG Technician) students- 20 per yearbull No of equipment- - Two cath labs with state of the art equipment like IVUS FFR CT+3D imaging IABP Rotablator EP system Electrocautery etc - One 3-D Echo machine and four 2-D echo machines distributed in Echo lab Cath lab ICCU and Emergency dept - 2 TMT machines - 11 Holter Devices
CATH LAB 1
CATH LAB 2
CATH LAB CONSOLE
ECHO LAB
bull OPD runs 7 days a weekbull 24 hours Cardiology Emergency services with
round the clock presence of DM residentbull No of patients visited Cardiology department
last year Numbers
No of patients attending OPD 96160
No of Indoor admissions 10808
No of 2D-Echo 19183
No of Holter monitoring 954
No of TMT 5749
No of Cath Interventions 8834
bull We are also providing Super speciality services to Seth S R Goyal satellite hospital Sethi colony Jaipur- 3 days a week
bull Primary PCI is being done round the clock and this facility is present in only few Govt Hospitals anywhere in India Also the Door to balloon time in our hospital is around 70 min which is well under the international recommendations of less than 90 min
bull An exhaustive DM Cardiology teaching programme is going on in the department five days a week with full participation of students and consultants
bull Our students who come for DM get excellent exposure to clinical and interventional work which sets them not only at par but I take pride in saying that they are even better than their counterparts in leading premier institutes of the country This is the reason why most of them are very well settled now and are doing very well wherever they are
bull Our department also offers Diploma for ECG Technician(DET) course in which 20 students get admitted yearly
Research Activities
Research Activities
Average no of studies done per year 22
Average no of papers published in reputed national amp international journals per year
14
In last 6 years our students have published around 100 research papers in national and international reputed journals
Presently work in the department is covering all major aspects of cardiology includingbull PTCA + STENTING including complex angioplastiesbull Primary PCIbull Rotablationbull IVUS FFRbull Carotid and other peripheral angioplastiesbull Renal angioplastiesbull BMVBPV BAVbull ASD VSD PDA Device closurebull Permanent pacemaker implantations including Dual chamber and MRI
compatible pacemakersbull AICDbull CRT-P CRT-Dbull EPS and RFAbull Arterial Embolizationbull Endomyocardial biopsy
bull These are comparable to most of the leading Govt Institutes anywhere in India
bull We are also trying to upgrade our facilities in the field of structural heart disease which includes endovascular treatment of aortic aneurysm dissection paravalvular leak closure TAVI etc
bull Lastly the Honorable CM has sanctioned a new Cath lab for our department in the present budget which will be installed soon A new 3-D Echo machine is being installed in next 2-3 months This will further improve the working in the department for better care of the poor patients
THANK YOU
CPC caseDepartment Cardiology
8th July 2016
Presenter Dr Rakesh Kumar Ola Dr Daulat Singh Meena
Cardiology discussant Dr Sohan K Sharma Assistant Prof Deptt Cardiology
Respiratory discussant Dr Sheetu Singh Assistant Prof Chest amp TB
Medicine discussant Dr Ashutosh Daga Resident Deptt Of Medicine ProfDrHemant Malhotra PHOD Deptt Of Medicine
Radiology discussant Dr Sachin Lamba Resident RadiologyDr RK Yadav Astt Prof Radiology
Pathology discussant Dr Neetu Aggarwal Sr Resident PathologyDr Anita Harsh Assoc Prof Pathology
Case Presenter
Dr Rakesh Kumar OlaIIIrd Year Resident
Department of Cardiology
Presenting complaints
A 38y old male resident of Jhalawar-Rajasthan presented with complaints of bull Fever on and off-12 monthsbull Cough- 12 monthsbull Weight loss-12 monthsbull Shortness of breath on exertion- 6 months bull Bilateral lower limb swelling- 15-20 days
History of presenting illness
Asymptomatic till 12 month back when he developed - Fever bull Insidious bull Low grade bull Intermittent typebull Each episode lasted for 10-15 daysbull Not associated with chills and rigor bull No diurnal variation bull Relieved by medications
History of presenting illness
Cough -12 monthbull Non-productive coughbull On and Off bull Each episode lasted for 20-30 days bull Cough was not associated with hemoptysis
chest heaviness noisy breathing and post-nasal discharge
bull No postural diurnal or seasonal variation
History of presenting illness
Weight loss -12 monthbull Patient had ho of significant weight loss of
5kg in last 12 months associated with easy fatigability
History of presenting illness
Shortness of breath-6 monthsbull Insidious onset bull Patient initially complain SOB on more than ordinary
activity and it progressively increased over 5 months and from last one month patient having SOB on less than ordinary physical activity (NYHA grade I to III ) but not at rest
bull SOB was not worsen by lying down and had no HO of episodic breathlessness during night
bull No postural or diurnal or seasonal variation
History of presenting illness
Bilateral lower limb swelling- 15-20 daysbull Lower limb swelling started from ankle joint
and progressed up to knee joint bull Not associated with morning facial puffiness
and abdominal fullnessbull No pain tenderness or warmth of lower limb
History of presenting illness
No history of bull Personal or family history of atopy or allergy like
itching skin lesions urticaria noisy breathing or seasonal variations
bull History of joint pains oral ulcersbull Travel out of statebull History of drugs or radiation exposurebull Occupational exposure of dust or smoke
History of presenting illness
No history of bull Recurrent episodes of diarrhoea abdominal pain
dysphagia or icterusbull Chest pain bull Palpitationbull Loss of consciousness bull Ho of focal neurological deficit
Past medical history
bull Patient had history of recurrent admissions and received treatment for enteric fever and malaria though patient had no relief in symptoms from same
bull No HO of DM HTN Tuberculosisbull No Ho any surgical intervention in past
Personal history
bull Laborerbull Studied up to 10th standardbull Smokerbull Non alcoholicbull Married bull Normal sleep appetite bowel and bladder
habitsbull Diet - vegetarian
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
bull In 2014 fourth unit startedbull Recently renovation of Post Catheterisation
Recovery Area(PCRA) dedicated to post cath patients completed which increased its bed capacity from 7 to 21
PRESENT SCENARIO OF THE DEPARTMENTbull No of consultants-12 bull These include 7 Professors 1 Associate Professor 3 Asst Professors and 1 MO
bull Prof Dr Anoop Jainbull Prof Dr Shashi Mohan Sharma(PHOD)bull Prof Dr Rajeev Bagarhattabull Prof Dr V V Agarwalbull Prof Dr Vijay Pathakbull Prof Dr Chandrabhan Meenabull Prof Dr Deepak Maheshwaribull Asso Prof Dr Neeraj Chaturvedibull Asst Prof Dr Sohan Kumar Sharmabull Asst Prof Dr Ritesh Guptabull Asst Prof Dr Omprakash Khojabull Dr Sunil Sharma MO
bull No of Residents- 24 (8 each year)
bull No of DET( Diploma in ECG Technician) students- 20 per yearbull No of equipment- - Two cath labs with state of the art equipment like IVUS FFR CT+3D imaging IABP Rotablator EP system Electrocautery etc - One 3-D Echo machine and four 2-D echo machines distributed in Echo lab Cath lab ICCU and Emergency dept - 2 TMT machines - 11 Holter Devices
CATH LAB 1
CATH LAB 2
CATH LAB CONSOLE
ECHO LAB
bull OPD runs 7 days a weekbull 24 hours Cardiology Emergency services with
round the clock presence of DM residentbull No of patients visited Cardiology department
last year Numbers
No of patients attending OPD 96160
No of Indoor admissions 10808
No of 2D-Echo 19183
No of Holter monitoring 954
No of TMT 5749
No of Cath Interventions 8834
bull We are also providing Super speciality services to Seth S R Goyal satellite hospital Sethi colony Jaipur- 3 days a week
bull Primary PCI is being done round the clock and this facility is present in only few Govt Hospitals anywhere in India Also the Door to balloon time in our hospital is around 70 min which is well under the international recommendations of less than 90 min
bull An exhaustive DM Cardiology teaching programme is going on in the department five days a week with full participation of students and consultants
bull Our students who come for DM get excellent exposure to clinical and interventional work which sets them not only at par but I take pride in saying that they are even better than their counterparts in leading premier institutes of the country This is the reason why most of them are very well settled now and are doing very well wherever they are
bull Our department also offers Diploma for ECG Technician(DET) course in which 20 students get admitted yearly
Research Activities
Research Activities
Average no of studies done per year 22
Average no of papers published in reputed national amp international journals per year
14
In last 6 years our students have published around 100 research papers in national and international reputed journals
Presently work in the department is covering all major aspects of cardiology includingbull PTCA + STENTING including complex angioplastiesbull Primary PCIbull Rotablationbull IVUS FFRbull Carotid and other peripheral angioplastiesbull Renal angioplastiesbull BMVBPV BAVbull ASD VSD PDA Device closurebull Permanent pacemaker implantations including Dual chamber and MRI
compatible pacemakersbull AICDbull CRT-P CRT-Dbull EPS and RFAbull Arterial Embolizationbull Endomyocardial biopsy
bull These are comparable to most of the leading Govt Institutes anywhere in India
bull We are also trying to upgrade our facilities in the field of structural heart disease which includes endovascular treatment of aortic aneurysm dissection paravalvular leak closure TAVI etc
bull Lastly the Honorable CM has sanctioned a new Cath lab for our department in the present budget which will be installed soon A new 3-D Echo machine is being installed in next 2-3 months This will further improve the working in the department for better care of the poor patients
THANK YOU
CPC caseDepartment Cardiology
8th July 2016
Presenter Dr Rakesh Kumar Ola Dr Daulat Singh Meena
Cardiology discussant Dr Sohan K Sharma Assistant Prof Deptt Cardiology
Respiratory discussant Dr Sheetu Singh Assistant Prof Chest amp TB
Medicine discussant Dr Ashutosh Daga Resident Deptt Of Medicine ProfDrHemant Malhotra PHOD Deptt Of Medicine
Radiology discussant Dr Sachin Lamba Resident RadiologyDr RK Yadav Astt Prof Radiology
Pathology discussant Dr Neetu Aggarwal Sr Resident PathologyDr Anita Harsh Assoc Prof Pathology
Case Presenter
Dr Rakesh Kumar OlaIIIrd Year Resident
Department of Cardiology
Presenting complaints
A 38y old male resident of Jhalawar-Rajasthan presented with complaints of bull Fever on and off-12 monthsbull Cough- 12 monthsbull Weight loss-12 monthsbull Shortness of breath on exertion- 6 months bull Bilateral lower limb swelling- 15-20 days
History of presenting illness
Asymptomatic till 12 month back when he developed - Fever bull Insidious bull Low grade bull Intermittent typebull Each episode lasted for 10-15 daysbull Not associated with chills and rigor bull No diurnal variation bull Relieved by medications
History of presenting illness
Cough -12 monthbull Non-productive coughbull On and Off bull Each episode lasted for 20-30 days bull Cough was not associated with hemoptysis
chest heaviness noisy breathing and post-nasal discharge
bull No postural diurnal or seasonal variation
History of presenting illness
Weight loss -12 monthbull Patient had ho of significant weight loss of
5kg in last 12 months associated with easy fatigability
History of presenting illness
Shortness of breath-6 monthsbull Insidious onset bull Patient initially complain SOB on more than ordinary
activity and it progressively increased over 5 months and from last one month patient having SOB on less than ordinary physical activity (NYHA grade I to III ) but not at rest
bull SOB was not worsen by lying down and had no HO of episodic breathlessness during night
bull No postural or diurnal or seasonal variation
History of presenting illness
Bilateral lower limb swelling- 15-20 daysbull Lower limb swelling started from ankle joint
and progressed up to knee joint bull Not associated with morning facial puffiness
and abdominal fullnessbull No pain tenderness or warmth of lower limb
History of presenting illness
No history of bull Personal or family history of atopy or allergy like
itching skin lesions urticaria noisy breathing or seasonal variations
bull History of joint pains oral ulcersbull Travel out of statebull History of drugs or radiation exposurebull Occupational exposure of dust or smoke
History of presenting illness
No history of bull Recurrent episodes of diarrhoea abdominal pain
dysphagia or icterusbull Chest pain bull Palpitationbull Loss of consciousness bull Ho of focal neurological deficit
Past medical history
bull Patient had history of recurrent admissions and received treatment for enteric fever and malaria though patient had no relief in symptoms from same
bull No HO of DM HTN Tuberculosisbull No Ho any surgical intervention in past
Personal history
bull Laborerbull Studied up to 10th standardbull Smokerbull Non alcoholicbull Married bull Normal sleep appetite bowel and bladder
habitsbull Diet - vegetarian
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
PRESENT SCENARIO OF THE DEPARTMENTbull No of consultants-12 bull These include 7 Professors 1 Associate Professor 3 Asst Professors and 1 MO
bull Prof Dr Anoop Jainbull Prof Dr Shashi Mohan Sharma(PHOD)bull Prof Dr Rajeev Bagarhattabull Prof Dr V V Agarwalbull Prof Dr Vijay Pathakbull Prof Dr Chandrabhan Meenabull Prof Dr Deepak Maheshwaribull Asso Prof Dr Neeraj Chaturvedibull Asst Prof Dr Sohan Kumar Sharmabull Asst Prof Dr Ritesh Guptabull Asst Prof Dr Omprakash Khojabull Dr Sunil Sharma MO
bull No of Residents- 24 (8 each year)
bull No of DET( Diploma in ECG Technician) students- 20 per yearbull No of equipment- - Two cath labs with state of the art equipment like IVUS FFR CT+3D imaging IABP Rotablator EP system Electrocautery etc - One 3-D Echo machine and four 2-D echo machines distributed in Echo lab Cath lab ICCU and Emergency dept - 2 TMT machines - 11 Holter Devices
CATH LAB 1
CATH LAB 2
CATH LAB CONSOLE
ECHO LAB
bull OPD runs 7 days a weekbull 24 hours Cardiology Emergency services with
round the clock presence of DM residentbull No of patients visited Cardiology department
last year Numbers
No of patients attending OPD 96160
No of Indoor admissions 10808
No of 2D-Echo 19183
No of Holter monitoring 954
No of TMT 5749
No of Cath Interventions 8834
bull We are also providing Super speciality services to Seth S R Goyal satellite hospital Sethi colony Jaipur- 3 days a week
bull Primary PCI is being done round the clock and this facility is present in only few Govt Hospitals anywhere in India Also the Door to balloon time in our hospital is around 70 min which is well under the international recommendations of less than 90 min
bull An exhaustive DM Cardiology teaching programme is going on in the department five days a week with full participation of students and consultants
bull Our students who come for DM get excellent exposure to clinical and interventional work which sets them not only at par but I take pride in saying that they are even better than their counterparts in leading premier institutes of the country This is the reason why most of them are very well settled now and are doing very well wherever they are
bull Our department also offers Diploma for ECG Technician(DET) course in which 20 students get admitted yearly
Research Activities
Research Activities
Average no of studies done per year 22
Average no of papers published in reputed national amp international journals per year
14
In last 6 years our students have published around 100 research papers in national and international reputed journals
Presently work in the department is covering all major aspects of cardiology includingbull PTCA + STENTING including complex angioplastiesbull Primary PCIbull Rotablationbull IVUS FFRbull Carotid and other peripheral angioplastiesbull Renal angioplastiesbull BMVBPV BAVbull ASD VSD PDA Device closurebull Permanent pacemaker implantations including Dual chamber and MRI
compatible pacemakersbull AICDbull CRT-P CRT-Dbull EPS and RFAbull Arterial Embolizationbull Endomyocardial biopsy
bull These are comparable to most of the leading Govt Institutes anywhere in India
bull We are also trying to upgrade our facilities in the field of structural heart disease which includes endovascular treatment of aortic aneurysm dissection paravalvular leak closure TAVI etc
bull Lastly the Honorable CM has sanctioned a new Cath lab for our department in the present budget which will be installed soon A new 3-D Echo machine is being installed in next 2-3 months This will further improve the working in the department for better care of the poor patients
THANK YOU
CPC caseDepartment Cardiology
8th July 2016
Presenter Dr Rakesh Kumar Ola Dr Daulat Singh Meena
Cardiology discussant Dr Sohan K Sharma Assistant Prof Deptt Cardiology
Respiratory discussant Dr Sheetu Singh Assistant Prof Chest amp TB
Medicine discussant Dr Ashutosh Daga Resident Deptt Of Medicine ProfDrHemant Malhotra PHOD Deptt Of Medicine
Radiology discussant Dr Sachin Lamba Resident RadiologyDr RK Yadav Astt Prof Radiology
Pathology discussant Dr Neetu Aggarwal Sr Resident PathologyDr Anita Harsh Assoc Prof Pathology
Case Presenter
Dr Rakesh Kumar OlaIIIrd Year Resident
Department of Cardiology
Presenting complaints
A 38y old male resident of Jhalawar-Rajasthan presented with complaints of bull Fever on and off-12 monthsbull Cough- 12 monthsbull Weight loss-12 monthsbull Shortness of breath on exertion- 6 months bull Bilateral lower limb swelling- 15-20 days
History of presenting illness
Asymptomatic till 12 month back when he developed - Fever bull Insidious bull Low grade bull Intermittent typebull Each episode lasted for 10-15 daysbull Not associated with chills and rigor bull No diurnal variation bull Relieved by medications
History of presenting illness
Cough -12 monthbull Non-productive coughbull On and Off bull Each episode lasted for 20-30 days bull Cough was not associated with hemoptysis
chest heaviness noisy breathing and post-nasal discharge
bull No postural diurnal or seasonal variation
History of presenting illness
Weight loss -12 monthbull Patient had ho of significant weight loss of
5kg in last 12 months associated with easy fatigability
History of presenting illness
Shortness of breath-6 monthsbull Insidious onset bull Patient initially complain SOB on more than ordinary
activity and it progressively increased over 5 months and from last one month patient having SOB on less than ordinary physical activity (NYHA grade I to III ) but not at rest
bull SOB was not worsen by lying down and had no HO of episodic breathlessness during night
bull No postural or diurnal or seasonal variation
History of presenting illness
Bilateral lower limb swelling- 15-20 daysbull Lower limb swelling started from ankle joint
and progressed up to knee joint bull Not associated with morning facial puffiness
and abdominal fullnessbull No pain tenderness or warmth of lower limb
History of presenting illness
No history of bull Personal or family history of atopy or allergy like
itching skin lesions urticaria noisy breathing or seasonal variations
bull History of joint pains oral ulcersbull Travel out of statebull History of drugs or radiation exposurebull Occupational exposure of dust or smoke
History of presenting illness
No history of bull Recurrent episodes of diarrhoea abdominal pain
dysphagia or icterusbull Chest pain bull Palpitationbull Loss of consciousness bull Ho of focal neurological deficit
Past medical history
bull Patient had history of recurrent admissions and received treatment for enteric fever and malaria though patient had no relief in symptoms from same
bull No HO of DM HTN Tuberculosisbull No Ho any surgical intervention in past
Personal history
bull Laborerbull Studied up to 10th standardbull Smokerbull Non alcoholicbull Married bull Normal sleep appetite bowel and bladder
habitsbull Diet - vegetarian
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
bull No of DET( Diploma in ECG Technician) students- 20 per yearbull No of equipment- - Two cath labs with state of the art equipment like IVUS FFR CT+3D imaging IABP Rotablator EP system Electrocautery etc - One 3-D Echo machine and four 2-D echo machines distributed in Echo lab Cath lab ICCU and Emergency dept - 2 TMT machines - 11 Holter Devices
CATH LAB 1
CATH LAB 2
CATH LAB CONSOLE
ECHO LAB
bull OPD runs 7 days a weekbull 24 hours Cardiology Emergency services with
round the clock presence of DM residentbull No of patients visited Cardiology department
last year Numbers
No of patients attending OPD 96160
No of Indoor admissions 10808
No of 2D-Echo 19183
No of Holter monitoring 954
No of TMT 5749
No of Cath Interventions 8834
bull We are also providing Super speciality services to Seth S R Goyal satellite hospital Sethi colony Jaipur- 3 days a week
bull Primary PCI is being done round the clock and this facility is present in only few Govt Hospitals anywhere in India Also the Door to balloon time in our hospital is around 70 min which is well under the international recommendations of less than 90 min
bull An exhaustive DM Cardiology teaching programme is going on in the department five days a week with full participation of students and consultants
bull Our students who come for DM get excellent exposure to clinical and interventional work which sets them not only at par but I take pride in saying that they are even better than their counterparts in leading premier institutes of the country This is the reason why most of them are very well settled now and are doing very well wherever they are
bull Our department also offers Diploma for ECG Technician(DET) course in which 20 students get admitted yearly
Research Activities
Research Activities
Average no of studies done per year 22
Average no of papers published in reputed national amp international journals per year
14
In last 6 years our students have published around 100 research papers in national and international reputed journals
Presently work in the department is covering all major aspects of cardiology includingbull PTCA + STENTING including complex angioplastiesbull Primary PCIbull Rotablationbull IVUS FFRbull Carotid and other peripheral angioplastiesbull Renal angioplastiesbull BMVBPV BAVbull ASD VSD PDA Device closurebull Permanent pacemaker implantations including Dual chamber and MRI
compatible pacemakersbull AICDbull CRT-P CRT-Dbull EPS and RFAbull Arterial Embolizationbull Endomyocardial biopsy
bull These are comparable to most of the leading Govt Institutes anywhere in India
bull We are also trying to upgrade our facilities in the field of structural heart disease which includes endovascular treatment of aortic aneurysm dissection paravalvular leak closure TAVI etc
bull Lastly the Honorable CM has sanctioned a new Cath lab for our department in the present budget which will be installed soon A new 3-D Echo machine is being installed in next 2-3 months This will further improve the working in the department for better care of the poor patients
THANK YOU
CPC caseDepartment Cardiology
8th July 2016
Presenter Dr Rakesh Kumar Ola Dr Daulat Singh Meena
Cardiology discussant Dr Sohan K Sharma Assistant Prof Deptt Cardiology
Respiratory discussant Dr Sheetu Singh Assistant Prof Chest amp TB
Medicine discussant Dr Ashutosh Daga Resident Deptt Of Medicine ProfDrHemant Malhotra PHOD Deptt Of Medicine
Radiology discussant Dr Sachin Lamba Resident RadiologyDr RK Yadav Astt Prof Radiology
Pathology discussant Dr Neetu Aggarwal Sr Resident PathologyDr Anita Harsh Assoc Prof Pathology
Case Presenter
Dr Rakesh Kumar OlaIIIrd Year Resident
Department of Cardiology
Presenting complaints
A 38y old male resident of Jhalawar-Rajasthan presented with complaints of bull Fever on and off-12 monthsbull Cough- 12 monthsbull Weight loss-12 monthsbull Shortness of breath on exertion- 6 months bull Bilateral lower limb swelling- 15-20 days
History of presenting illness
Asymptomatic till 12 month back when he developed - Fever bull Insidious bull Low grade bull Intermittent typebull Each episode lasted for 10-15 daysbull Not associated with chills and rigor bull No diurnal variation bull Relieved by medications
History of presenting illness
Cough -12 monthbull Non-productive coughbull On and Off bull Each episode lasted for 20-30 days bull Cough was not associated with hemoptysis
chest heaviness noisy breathing and post-nasal discharge
bull No postural diurnal or seasonal variation
History of presenting illness
Weight loss -12 monthbull Patient had ho of significant weight loss of
5kg in last 12 months associated with easy fatigability
History of presenting illness
Shortness of breath-6 monthsbull Insidious onset bull Patient initially complain SOB on more than ordinary
activity and it progressively increased over 5 months and from last one month patient having SOB on less than ordinary physical activity (NYHA grade I to III ) but not at rest
bull SOB was not worsen by lying down and had no HO of episodic breathlessness during night
bull No postural or diurnal or seasonal variation
History of presenting illness
Bilateral lower limb swelling- 15-20 daysbull Lower limb swelling started from ankle joint
and progressed up to knee joint bull Not associated with morning facial puffiness
and abdominal fullnessbull No pain tenderness or warmth of lower limb
History of presenting illness
No history of bull Personal or family history of atopy or allergy like
itching skin lesions urticaria noisy breathing or seasonal variations
bull History of joint pains oral ulcersbull Travel out of statebull History of drugs or radiation exposurebull Occupational exposure of dust or smoke
History of presenting illness
No history of bull Recurrent episodes of diarrhoea abdominal pain
dysphagia or icterusbull Chest pain bull Palpitationbull Loss of consciousness bull Ho of focal neurological deficit
Past medical history
bull Patient had history of recurrent admissions and received treatment for enteric fever and malaria though patient had no relief in symptoms from same
bull No HO of DM HTN Tuberculosisbull No Ho any surgical intervention in past
Personal history
bull Laborerbull Studied up to 10th standardbull Smokerbull Non alcoholicbull Married bull Normal sleep appetite bowel and bladder
habitsbull Diet - vegetarian
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
CATH LAB 1
CATH LAB 2
CATH LAB CONSOLE
ECHO LAB
bull OPD runs 7 days a weekbull 24 hours Cardiology Emergency services with
round the clock presence of DM residentbull No of patients visited Cardiology department
last year Numbers
No of patients attending OPD 96160
No of Indoor admissions 10808
No of 2D-Echo 19183
No of Holter monitoring 954
No of TMT 5749
No of Cath Interventions 8834
bull We are also providing Super speciality services to Seth S R Goyal satellite hospital Sethi colony Jaipur- 3 days a week
bull Primary PCI is being done round the clock and this facility is present in only few Govt Hospitals anywhere in India Also the Door to balloon time in our hospital is around 70 min which is well under the international recommendations of less than 90 min
bull An exhaustive DM Cardiology teaching programme is going on in the department five days a week with full participation of students and consultants
bull Our students who come for DM get excellent exposure to clinical and interventional work which sets them not only at par but I take pride in saying that they are even better than their counterparts in leading premier institutes of the country This is the reason why most of them are very well settled now and are doing very well wherever they are
bull Our department also offers Diploma for ECG Technician(DET) course in which 20 students get admitted yearly
Research Activities
Research Activities
Average no of studies done per year 22
Average no of papers published in reputed national amp international journals per year
14
In last 6 years our students have published around 100 research papers in national and international reputed journals
Presently work in the department is covering all major aspects of cardiology includingbull PTCA + STENTING including complex angioplastiesbull Primary PCIbull Rotablationbull IVUS FFRbull Carotid and other peripheral angioplastiesbull Renal angioplastiesbull BMVBPV BAVbull ASD VSD PDA Device closurebull Permanent pacemaker implantations including Dual chamber and MRI
compatible pacemakersbull AICDbull CRT-P CRT-Dbull EPS and RFAbull Arterial Embolizationbull Endomyocardial biopsy
bull These are comparable to most of the leading Govt Institutes anywhere in India
bull We are also trying to upgrade our facilities in the field of structural heart disease which includes endovascular treatment of aortic aneurysm dissection paravalvular leak closure TAVI etc
bull Lastly the Honorable CM has sanctioned a new Cath lab for our department in the present budget which will be installed soon A new 3-D Echo machine is being installed in next 2-3 months This will further improve the working in the department for better care of the poor patients
THANK YOU
CPC caseDepartment Cardiology
8th July 2016
Presenter Dr Rakesh Kumar Ola Dr Daulat Singh Meena
Cardiology discussant Dr Sohan K Sharma Assistant Prof Deptt Cardiology
Respiratory discussant Dr Sheetu Singh Assistant Prof Chest amp TB
Medicine discussant Dr Ashutosh Daga Resident Deptt Of Medicine ProfDrHemant Malhotra PHOD Deptt Of Medicine
Radiology discussant Dr Sachin Lamba Resident RadiologyDr RK Yadav Astt Prof Radiology
Pathology discussant Dr Neetu Aggarwal Sr Resident PathologyDr Anita Harsh Assoc Prof Pathology
Case Presenter
Dr Rakesh Kumar OlaIIIrd Year Resident
Department of Cardiology
Presenting complaints
A 38y old male resident of Jhalawar-Rajasthan presented with complaints of bull Fever on and off-12 monthsbull Cough- 12 monthsbull Weight loss-12 monthsbull Shortness of breath on exertion- 6 months bull Bilateral lower limb swelling- 15-20 days
History of presenting illness
Asymptomatic till 12 month back when he developed - Fever bull Insidious bull Low grade bull Intermittent typebull Each episode lasted for 10-15 daysbull Not associated with chills and rigor bull No diurnal variation bull Relieved by medications
History of presenting illness
Cough -12 monthbull Non-productive coughbull On and Off bull Each episode lasted for 20-30 days bull Cough was not associated with hemoptysis
chest heaviness noisy breathing and post-nasal discharge
bull No postural diurnal or seasonal variation
History of presenting illness
Weight loss -12 monthbull Patient had ho of significant weight loss of
5kg in last 12 months associated with easy fatigability
History of presenting illness
Shortness of breath-6 monthsbull Insidious onset bull Patient initially complain SOB on more than ordinary
activity and it progressively increased over 5 months and from last one month patient having SOB on less than ordinary physical activity (NYHA grade I to III ) but not at rest
bull SOB was not worsen by lying down and had no HO of episodic breathlessness during night
bull No postural or diurnal or seasonal variation
History of presenting illness
Bilateral lower limb swelling- 15-20 daysbull Lower limb swelling started from ankle joint
and progressed up to knee joint bull Not associated with morning facial puffiness
and abdominal fullnessbull No pain tenderness or warmth of lower limb
History of presenting illness
No history of bull Personal or family history of atopy or allergy like
itching skin lesions urticaria noisy breathing or seasonal variations
bull History of joint pains oral ulcersbull Travel out of statebull History of drugs or radiation exposurebull Occupational exposure of dust or smoke
History of presenting illness
No history of bull Recurrent episodes of diarrhoea abdominal pain
dysphagia or icterusbull Chest pain bull Palpitationbull Loss of consciousness bull Ho of focal neurological deficit
Past medical history
bull Patient had history of recurrent admissions and received treatment for enteric fever and malaria though patient had no relief in symptoms from same
bull No HO of DM HTN Tuberculosisbull No Ho any surgical intervention in past
Personal history
bull Laborerbull Studied up to 10th standardbull Smokerbull Non alcoholicbull Married bull Normal sleep appetite bowel and bladder
habitsbull Diet - vegetarian
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
CATH LAB 2
CATH LAB CONSOLE
ECHO LAB
bull OPD runs 7 days a weekbull 24 hours Cardiology Emergency services with
round the clock presence of DM residentbull No of patients visited Cardiology department
last year Numbers
No of patients attending OPD 96160
No of Indoor admissions 10808
No of 2D-Echo 19183
No of Holter monitoring 954
No of TMT 5749
No of Cath Interventions 8834
bull We are also providing Super speciality services to Seth S R Goyal satellite hospital Sethi colony Jaipur- 3 days a week
bull Primary PCI is being done round the clock and this facility is present in only few Govt Hospitals anywhere in India Also the Door to balloon time in our hospital is around 70 min which is well under the international recommendations of less than 90 min
bull An exhaustive DM Cardiology teaching programme is going on in the department five days a week with full participation of students and consultants
bull Our students who come for DM get excellent exposure to clinical and interventional work which sets them not only at par but I take pride in saying that they are even better than their counterparts in leading premier institutes of the country This is the reason why most of them are very well settled now and are doing very well wherever they are
bull Our department also offers Diploma for ECG Technician(DET) course in which 20 students get admitted yearly
Research Activities
Research Activities
Average no of studies done per year 22
Average no of papers published in reputed national amp international journals per year
14
In last 6 years our students have published around 100 research papers in national and international reputed journals
Presently work in the department is covering all major aspects of cardiology includingbull PTCA + STENTING including complex angioplastiesbull Primary PCIbull Rotablationbull IVUS FFRbull Carotid and other peripheral angioplastiesbull Renal angioplastiesbull BMVBPV BAVbull ASD VSD PDA Device closurebull Permanent pacemaker implantations including Dual chamber and MRI
compatible pacemakersbull AICDbull CRT-P CRT-Dbull EPS and RFAbull Arterial Embolizationbull Endomyocardial biopsy
bull These are comparable to most of the leading Govt Institutes anywhere in India
bull We are also trying to upgrade our facilities in the field of structural heart disease which includes endovascular treatment of aortic aneurysm dissection paravalvular leak closure TAVI etc
bull Lastly the Honorable CM has sanctioned a new Cath lab for our department in the present budget which will be installed soon A new 3-D Echo machine is being installed in next 2-3 months This will further improve the working in the department for better care of the poor patients
THANK YOU
CPC caseDepartment Cardiology
8th July 2016
Presenter Dr Rakesh Kumar Ola Dr Daulat Singh Meena
Cardiology discussant Dr Sohan K Sharma Assistant Prof Deptt Cardiology
Respiratory discussant Dr Sheetu Singh Assistant Prof Chest amp TB
Medicine discussant Dr Ashutosh Daga Resident Deptt Of Medicine ProfDrHemant Malhotra PHOD Deptt Of Medicine
Radiology discussant Dr Sachin Lamba Resident RadiologyDr RK Yadav Astt Prof Radiology
Pathology discussant Dr Neetu Aggarwal Sr Resident PathologyDr Anita Harsh Assoc Prof Pathology
Case Presenter
Dr Rakesh Kumar OlaIIIrd Year Resident
Department of Cardiology
Presenting complaints
A 38y old male resident of Jhalawar-Rajasthan presented with complaints of bull Fever on and off-12 monthsbull Cough- 12 monthsbull Weight loss-12 monthsbull Shortness of breath on exertion- 6 months bull Bilateral lower limb swelling- 15-20 days
History of presenting illness
Asymptomatic till 12 month back when he developed - Fever bull Insidious bull Low grade bull Intermittent typebull Each episode lasted for 10-15 daysbull Not associated with chills and rigor bull No diurnal variation bull Relieved by medications
History of presenting illness
Cough -12 monthbull Non-productive coughbull On and Off bull Each episode lasted for 20-30 days bull Cough was not associated with hemoptysis
chest heaviness noisy breathing and post-nasal discharge
bull No postural diurnal or seasonal variation
History of presenting illness
Weight loss -12 monthbull Patient had ho of significant weight loss of
5kg in last 12 months associated with easy fatigability
History of presenting illness
Shortness of breath-6 monthsbull Insidious onset bull Patient initially complain SOB on more than ordinary
activity and it progressively increased over 5 months and from last one month patient having SOB on less than ordinary physical activity (NYHA grade I to III ) but not at rest
bull SOB was not worsen by lying down and had no HO of episodic breathlessness during night
bull No postural or diurnal or seasonal variation
History of presenting illness
Bilateral lower limb swelling- 15-20 daysbull Lower limb swelling started from ankle joint
and progressed up to knee joint bull Not associated with morning facial puffiness
and abdominal fullnessbull No pain tenderness or warmth of lower limb
History of presenting illness
No history of bull Personal or family history of atopy or allergy like
itching skin lesions urticaria noisy breathing or seasonal variations
bull History of joint pains oral ulcersbull Travel out of statebull History of drugs or radiation exposurebull Occupational exposure of dust or smoke
History of presenting illness
No history of bull Recurrent episodes of diarrhoea abdominal pain
dysphagia or icterusbull Chest pain bull Palpitationbull Loss of consciousness bull Ho of focal neurological deficit
Past medical history
bull Patient had history of recurrent admissions and received treatment for enteric fever and malaria though patient had no relief in symptoms from same
bull No HO of DM HTN Tuberculosisbull No Ho any surgical intervention in past
Personal history
bull Laborerbull Studied up to 10th standardbull Smokerbull Non alcoholicbull Married bull Normal sleep appetite bowel and bladder
habitsbull Diet - vegetarian
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber

CATH LAB CONSOLE
ECHO LAB
bull OPD runs 7 days a weekbull 24 hours Cardiology Emergency services with
round the clock presence of DM residentbull No of patients visited Cardiology department
last year Numbers
No of patients attending OPD 96160
No of Indoor admissions 10808
No of 2D-Echo 19183
No of Holter monitoring 954
No of TMT 5749
No of Cath Interventions 8834
bull We are also providing Super speciality services to Seth S R Goyal satellite hospital Sethi colony Jaipur- 3 days a week
bull Primary PCI is being done round the clock and this facility is present in only few Govt Hospitals anywhere in India Also the Door to balloon time in our hospital is around 70 min which is well under the international recommendations of less than 90 min
bull An exhaustive DM Cardiology teaching programme is going on in the department five days a week with full participation of students and consultants
bull Our students who come for DM get excellent exposure to clinical and interventional work which sets them not only at par but I take pride in saying that they are even better than their counterparts in leading premier institutes of the country This is the reason why most of them are very well settled now and are doing very well wherever they are
bull Our department also offers Diploma for ECG Technician(DET) course in which 20 students get admitted yearly
Research Activities
Research Activities
Average no of studies done per year 22
Average no of papers published in reputed national amp international journals per year
14
In last 6 years our students have published around 100 research papers in national and international reputed journals
Presently work in the department is covering all major aspects of cardiology includingbull PTCA + STENTING including complex angioplastiesbull Primary PCIbull Rotablationbull IVUS FFRbull Carotid and other peripheral angioplastiesbull Renal angioplastiesbull BMVBPV BAVbull ASD VSD PDA Device closurebull Permanent pacemaker implantations including Dual chamber and MRI
compatible pacemakersbull AICDbull CRT-P CRT-Dbull EPS and RFAbull Arterial Embolizationbull Endomyocardial biopsy
bull These are comparable to most of the leading Govt Institutes anywhere in India
bull We are also trying to upgrade our facilities in the field of structural heart disease which includes endovascular treatment of aortic aneurysm dissection paravalvular leak closure TAVI etc
bull Lastly the Honorable CM has sanctioned a new Cath lab for our department in the present budget which will be installed soon A new 3-D Echo machine is being installed in next 2-3 months This will further improve the working in the department for better care of the poor patients
THANK YOU
CPC caseDepartment Cardiology
8th July 2016
Presenter Dr Rakesh Kumar Ola Dr Daulat Singh Meena
Cardiology discussant Dr Sohan K Sharma Assistant Prof Deptt Cardiology
Respiratory discussant Dr Sheetu Singh Assistant Prof Chest amp TB
Medicine discussant Dr Ashutosh Daga Resident Deptt Of Medicine ProfDrHemant Malhotra PHOD Deptt Of Medicine
Radiology discussant Dr Sachin Lamba Resident RadiologyDr RK Yadav Astt Prof Radiology
Pathology discussant Dr Neetu Aggarwal Sr Resident PathologyDr Anita Harsh Assoc Prof Pathology
Case Presenter
Dr Rakesh Kumar OlaIIIrd Year Resident
Department of Cardiology
Presenting complaints
A 38y old male resident of Jhalawar-Rajasthan presented with complaints of bull Fever on and off-12 monthsbull Cough- 12 monthsbull Weight loss-12 monthsbull Shortness of breath on exertion- 6 months bull Bilateral lower limb swelling- 15-20 days
History of presenting illness
Asymptomatic till 12 month back when he developed - Fever bull Insidious bull Low grade bull Intermittent typebull Each episode lasted for 10-15 daysbull Not associated with chills and rigor bull No diurnal variation bull Relieved by medications
History of presenting illness
Cough -12 monthbull Non-productive coughbull On and Off bull Each episode lasted for 20-30 days bull Cough was not associated with hemoptysis
chest heaviness noisy breathing and post-nasal discharge
bull No postural diurnal or seasonal variation
History of presenting illness
Weight loss -12 monthbull Patient had ho of significant weight loss of
5kg in last 12 months associated with easy fatigability
History of presenting illness
Shortness of breath-6 monthsbull Insidious onset bull Patient initially complain SOB on more than ordinary
activity and it progressively increased over 5 months and from last one month patient having SOB on less than ordinary physical activity (NYHA grade I to III ) but not at rest
bull SOB was not worsen by lying down and had no HO of episodic breathlessness during night
bull No postural or diurnal or seasonal variation
History of presenting illness
Bilateral lower limb swelling- 15-20 daysbull Lower limb swelling started from ankle joint
and progressed up to knee joint bull Not associated with morning facial puffiness
and abdominal fullnessbull No pain tenderness or warmth of lower limb
History of presenting illness
No history of bull Personal or family history of atopy or allergy like
itching skin lesions urticaria noisy breathing or seasonal variations
bull History of joint pains oral ulcersbull Travel out of statebull History of drugs or radiation exposurebull Occupational exposure of dust or smoke
History of presenting illness
No history of bull Recurrent episodes of diarrhoea abdominal pain
dysphagia or icterusbull Chest pain bull Palpitationbull Loss of consciousness bull Ho of focal neurological deficit
Past medical history
bull Patient had history of recurrent admissions and received treatment for enteric fever and malaria though patient had no relief in symptoms from same
bull No HO of DM HTN Tuberculosisbull No Ho any surgical intervention in past
Personal history
bull Laborerbull Studied up to 10th standardbull Smokerbull Non alcoholicbull Married bull Normal sleep appetite bowel and bladder
habitsbull Diet - vegetarian
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber

ECHO LAB
bull OPD runs 7 days a weekbull 24 hours Cardiology Emergency services with
round the clock presence of DM residentbull No of patients visited Cardiology department
last year Numbers
No of patients attending OPD 96160
No of Indoor admissions 10808
No of 2D-Echo 19183
No of Holter monitoring 954
No of TMT 5749
No of Cath Interventions 8834
bull We are also providing Super speciality services to Seth S R Goyal satellite hospital Sethi colony Jaipur- 3 days a week
bull Primary PCI is being done round the clock and this facility is present in only few Govt Hospitals anywhere in India Also the Door to balloon time in our hospital is around 70 min which is well under the international recommendations of less than 90 min
bull An exhaustive DM Cardiology teaching programme is going on in the department five days a week with full participation of students and consultants
bull Our students who come for DM get excellent exposure to clinical and interventional work which sets them not only at par but I take pride in saying that they are even better than their counterparts in leading premier institutes of the country This is the reason why most of them are very well settled now and are doing very well wherever they are
bull Our department also offers Diploma for ECG Technician(DET) course in which 20 students get admitted yearly
Research Activities
Research Activities
Average no of studies done per year 22
Average no of papers published in reputed national amp international journals per year
14
In last 6 years our students have published around 100 research papers in national and international reputed journals
Presently work in the department is covering all major aspects of cardiology includingbull PTCA + STENTING including complex angioplastiesbull Primary PCIbull Rotablationbull IVUS FFRbull Carotid and other peripheral angioplastiesbull Renal angioplastiesbull BMVBPV BAVbull ASD VSD PDA Device closurebull Permanent pacemaker implantations including Dual chamber and MRI
compatible pacemakersbull AICDbull CRT-P CRT-Dbull EPS and RFAbull Arterial Embolizationbull Endomyocardial biopsy
bull These are comparable to most of the leading Govt Institutes anywhere in India
bull We are also trying to upgrade our facilities in the field of structural heart disease which includes endovascular treatment of aortic aneurysm dissection paravalvular leak closure TAVI etc
bull Lastly the Honorable CM has sanctioned a new Cath lab for our department in the present budget which will be installed soon A new 3-D Echo machine is being installed in next 2-3 months This will further improve the working in the department for better care of the poor patients
THANK YOU
CPC caseDepartment Cardiology
8th July 2016
Presenter Dr Rakesh Kumar Ola Dr Daulat Singh Meena
Cardiology discussant Dr Sohan K Sharma Assistant Prof Deptt Cardiology
Respiratory discussant Dr Sheetu Singh Assistant Prof Chest amp TB
Medicine discussant Dr Ashutosh Daga Resident Deptt Of Medicine ProfDrHemant Malhotra PHOD Deptt Of Medicine
Radiology discussant Dr Sachin Lamba Resident RadiologyDr RK Yadav Astt Prof Radiology
Pathology discussant Dr Neetu Aggarwal Sr Resident PathologyDr Anita Harsh Assoc Prof Pathology
Case Presenter
Dr Rakesh Kumar OlaIIIrd Year Resident
Department of Cardiology
Presenting complaints
A 38y old male resident of Jhalawar-Rajasthan presented with complaints of bull Fever on and off-12 monthsbull Cough- 12 monthsbull Weight loss-12 monthsbull Shortness of breath on exertion- 6 months bull Bilateral lower limb swelling- 15-20 days
History of presenting illness
Asymptomatic till 12 month back when he developed - Fever bull Insidious bull Low grade bull Intermittent typebull Each episode lasted for 10-15 daysbull Not associated with chills and rigor bull No diurnal variation bull Relieved by medications
History of presenting illness
Cough -12 monthbull Non-productive coughbull On and Off bull Each episode lasted for 20-30 days bull Cough was not associated with hemoptysis
chest heaviness noisy breathing and post-nasal discharge
bull No postural diurnal or seasonal variation
History of presenting illness
Weight loss -12 monthbull Patient had ho of significant weight loss of
5kg in last 12 months associated with easy fatigability
History of presenting illness
Shortness of breath-6 monthsbull Insidious onset bull Patient initially complain SOB on more than ordinary
activity and it progressively increased over 5 months and from last one month patient having SOB on less than ordinary physical activity (NYHA grade I to III ) but not at rest
bull SOB was not worsen by lying down and had no HO of episodic breathlessness during night
bull No postural or diurnal or seasonal variation
History of presenting illness
Bilateral lower limb swelling- 15-20 daysbull Lower limb swelling started from ankle joint
and progressed up to knee joint bull Not associated with morning facial puffiness
and abdominal fullnessbull No pain tenderness or warmth of lower limb
History of presenting illness
No history of bull Personal or family history of atopy or allergy like
itching skin lesions urticaria noisy breathing or seasonal variations
bull History of joint pains oral ulcersbull Travel out of statebull History of drugs or radiation exposurebull Occupational exposure of dust or smoke
History of presenting illness
No history of bull Recurrent episodes of diarrhoea abdominal pain
dysphagia or icterusbull Chest pain bull Palpitationbull Loss of consciousness bull Ho of focal neurological deficit
Past medical history
bull Patient had history of recurrent admissions and received treatment for enteric fever and malaria though patient had no relief in symptoms from same
bull No HO of DM HTN Tuberculosisbull No Ho any surgical intervention in past
Personal history
bull Laborerbull Studied up to 10th standardbull Smokerbull Non alcoholicbull Married bull Normal sleep appetite bowel and bladder
habitsbull Diet - vegetarian
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
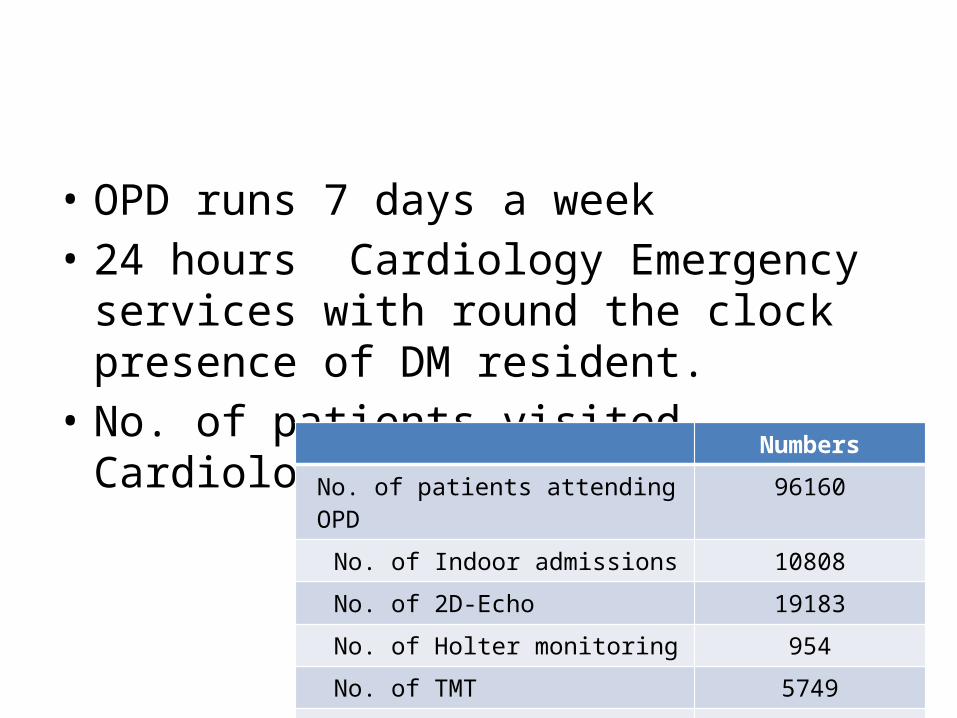
bull OPD runs 7 days a weekbull 24 hours Cardiology Emergency services with
round the clock presence of DM residentbull No of patients visited Cardiology department
last year Numbers
No of patients attending OPD 96160
No of Indoor admissions 10808
No of 2D-Echo 19183
No of Holter monitoring 954
No of TMT 5749
No of Cath Interventions 8834
bull We are also providing Super speciality services to Seth S R Goyal satellite hospital Sethi colony Jaipur- 3 days a week
bull Primary PCI is being done round the clock and this facility is present in only few Govt Hospitals anywhere in India Also the Door to balloon time in our hospital is around 70 min which is well under the international recommendations of less than 90 min
bull An exhaustive DM Cardiology teaching programme is going on in the department five days a week with full participation of students and consultants
bull Our students who come for DM get excellent exposure to clinical and interventional work which sets them not only at par but I take pride in saying that they are even better than their counterparts in leading premier institutes of the country This is the reason why most of them are very well settled now and are doing very well wherever they are
bull Our department also offers Diploma for ECG Technician(DET) course in which 20 students get admitted yearly
Research Activities
Research Activities
Average no of studies done per year 22
Average no of papers published in reputed national amp international journals per year
14
In last 6 years our students have published around 100 research papers in national and international reputed journals
Presently work in the department is covering all major aspects of cardiology includingbull PTCA + STENTING including complex angioplastiesbull Primary PCIbull Rotablationbull IVUS FFRbull Carotid and other peripheral angioplastiesbull Renal angioplastiesbull BMVBPV BAVbull ASD VSD PDA Device closurebull Permanent pacemaker implantations including Dual chamber and MRI
compatible pacemakersbull AICDbull CRT-P CRT-Dbull EPS and RFAbull Arterial Embolizationbull Endomyocardial biopsy
bull These are comparable to most of the leading Govt Institutes anywhere in India
bull We are also trying to upgrade our facilities in the field of structural heart disease which includes endovascular treatment of aortic aneurysm dissection paravalvular leak closure TAVI etc
bull Lastly the Honorable CM has sanctioned a new Cath lab for our department in the present budget which will be installed soon A new 3-D Echo machine is being installed in next 2-3 months This will further improve the working in the department for better care of the poor patients
THANK YOU
CPC caseDepartment Cardiology
8th July 2016
Presenter Dr Rakesh Kumar Ola Dr Daulat Singh Meena
Cardiology discussant Dr Sohan K Sharma Assistant Prof Deptt Cardiology
Respiratory discussant Dr Sheetu Singh Assistant Prof Chest amp TB
Medicine discussant Dr Ashutosh Daga Resident Deptt Of Medicine ProfDrHemant Malhotra PHOD Deptt Of Medicine
Radiology discussant Dr Sachin Lamba Resident RadiologyDr RK Yadav Astt Prof Radiology
Pathology discussant Dr Neetu Aggarwal Sr Resident PathologyDr Anita Harsh Assoc Prof Pathology
Case Presenter
Dr Rakesh Kumar OlaIIIrd Year Resident
Department of Cardiology
Presenting complaints
A 38y old male resident of Jhalawar-Rajasthan presented with complaints of bull Fever on and off-12 monthsbull Cough- 12 monthsbull Weight loss-12 monthsbull Shortness of breath on exertion- 6 months bull Bilateral lower limb swelling- 15-20 days
History of presenting illness
Asymptomatic till 12 month back when he developed - Fever bull Insidious bull Low grade bull Intermittent typebull Each episode lasted for 10-15 daysbull Not associated with chills and rigor bull No diurnal variation bull Relieved by medications
History of presenting illness
Cough -12 monthbull Non-productive coughbull On and Off bull Each episode lasted for 20-30 days bull Cough was not associated with hemoptysis
chest heaviness noisy breathing and post-nasal discharge
bull No postural diurnal or seasonal variation
History of presenting illness
Weight loss -12 monthbull Patient had ho of significant weight loss of
5kg in last 12 months associated with easy fatigability
History of presenting illness
Shortness of breath-6 monthsbull Insidious onset bull Patient initially complain SOB on more than ordinary
activity and it progressively increased over 5 months and from last one month patient having SOB on less than ordinary physical activity (NYHA grade I to III ) but not at rest
bull SOB was not worsen by lying down and had no HO of episodic breathlessness during night
bull No postural or diurnal or seasonal variation
History of presenting illness
Bilateral lower limb swelling- 15-20 daysbull Lower limb swelling started from ankle joint
and progressed up to knee joint bull Not associated with morning facial puffiness
and abdominal fullnessbull No pain tenderness or warmth of lower limb
History of presenting illness
No history of bull Personal or family history of atopy or allergy like
itching skin lesions urticaria noisy breathing or seasonal variations
bull History of joint pains oral ulcersbull Travel out of statebull History of drugs or radiation exposurebull Occupational exposure of dust or smoke
History of presenting illness
No history of bull Recurrent episodes of diarrhoea abdominal pain
dysphagia or icterusbull Chest pain bull Palpitationbull Loss of consciousness bull Ho of focal neurological deficit
Past medical history
bull Patient had history of recurrent admissions and received treatment for enteric fever and malaria though patient had no relief in symptoms from same
bull No HO of DM HTN Tuberculosisbull No Ho any surgical intervention in past
Personal history
bull Laborerbull Studied up to 10th standardbull Smokerbull Non alcoholicbull Married bull Normal sleep appetite bowel and bladder
habitsbull Diet - vegetarian
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
bull We are also providing Super speciality services to Seth S R Goyal satellite hospital Sethi colony Jaipur- 3 days a week
bull Primary PCI is being done round the clock and this facility is present in only few Govt Hospitals anywhere in India Also the Door to balloon time in our hospital is around 70 min which is well under the international recommendations of less than 90 min
bull An exhaustive DM Cardiology teaching programme is going on in the department five days a week with full participation of students and consultants
bull Our students who come for DM get excellent exposure to clinical and interventional work which sets them not only at par but I take pride in saying that they are even better than their counterparts in leading premier institutes of the country This is the reason why most of them are very well settled now and are doing very well wherever they are
bull Our department also offers Diploma for ECG Technician(DET) course in which 20 students get admitted yearly
Research Activities
Research Activities
Average no of studies done per year 22
Average no of papers published in reputed national amp international journals per year
14
In last 6 years our students have published around 100 research papers in national and international reputed journals
Presently work in the department is covering all major aspects of cardiology includingbull PTCA + STENTING including complex angioplastiesbull Primary PCIbull Rotablationbull IVUS FFRbull Carotid and other peripheral angioplastiesbull Renal angioplastiesbull BMVBPV BAVbull ASD VSD PDA Device closurebull Permanent pacemaker implantations including Dual chamber and MRI
compatible pacemakersbull AICDbull CRT-P CRT-Dbull EPS and RFAbull Arterial Embolizationbull Endomyocardial biopsy
bull These are comparable to most of the leading Govt Institutes anywhere in India
bull We are also trying to upgrade our facilities in the field of structural heart disease which includes endovascular treatment of aortic aneurysm dissection paravalvular leak closure TAVI etc
bull Lastly the Honorable CM has sanctioned a new Cath lab for our department in the present budget which will be installed soon A new 3-D Echo machine is being installed in next 2-3 months This will further improve the working in the department for better care of the poor patients
THANK YOU
CPC caseDepartment Cardiology
8th July 2016
Presenter Dr Rakesh Kumar Ola Dr Daulat Singh Meena
Cardiology discussant Dr Sohan K Sharma Assistant Prof Deptt Cardiology
Respiratory discussant Dr Sheetu Singh Assistant Prof Chest amp TB
Medicine discussant Dr Ashutosh Daga Resident Deptt Of Medicine ProfDrHemant Malhotra PHOD Deptt Of Medicine
Radiology discussant Dr Sachin Lamba Resident RadiologyDr RK Yadav Astt Prof Radiology
Pathology discussant Dr Neetu Aggarwal Sr Resident PathologyDr Anita Harsh Assoc Prof Pathology
Case Presenter
Dr Rakesh Kumar OlaIIIrd Year Resident
Department of Cardiology
Presenting complaints
A 38y old male resident of Jhalawar-Rajasthan presented with complaints of bull Fever on and off-12 monthsbull Cough- 12 monthsbull Weight loss-12 monthsbull Shortness of breath on exertion- 6 months bull Bilateral lower limb swelling- 15-20 days
History of presenting illness
Asymptomatic till 12 month back when he developed - Fever bull Insidious bull Low grade bull Intermittent typebull Each episode lasted for 10-15 daysbull Not associated with chills and rigor bull No diurnal variation bull Relieved by medications
History of presenting illness
Cough -12 monthbull Non-productive coughbull On and Off bull Each episode lasted for 20-30 days bull Cough was not associated with hemoptysis
chest heaviness noisy breathing and post-nasal discharge
bull No postural diurnal or seasonal variation
History of presenting illness
Weight loss -12 monthbull Patient had ho of significant weight loss of
5kg in last 12 months associated with easy fatigability
History of presenting illness
Shortness of breath-6 monthsbull Insidious onset bull Patient initially complain SOB on more than ordinary
activity and it progressively increased over 5 months and from last one month patient having SOB on less than ordinary physical activity (NYHA grade I to III ) but not at rest
bull SOB was not worsen by lying down and had no HO of episodic breathlessness during night
bull No postural or diurnal or seasonal variation
History of presenting illness
Bilateral lower limb swelling- 15-20 daysbull Lower limb swelling started from ankle joint
and progressed up to knee joint bull Not associated with morning facial puffiness
and abdominal fullnessbull No pain tenderness or warmth of lower limb
History of presenting illness
No history of bull Personal or family history of atopy or allergy like
itching skin lesions urticaria noisy breathing or seasonal variations
bull History of joint pains oral ulcersbull Travel out of statebull History of drugs or radiation exposurebull Occupational exposure of dust or smoke
History of presenting illness
No history of bull Recurrent episodes of diarrhoea abdominal pain
dysphagia or icterusbull Chest pain bull Palpitationbull Loss of consciousness bull Ho of focal neurological deficit
Past medical history
bull Patient had history of recurrent admissions and received treatment for enteric fever and malaria though patient had no relief in symptoms from same
bull No HO of DM HTN Tuberculosisbull No Ho any surgical intervention in past
Personal history
bull Laborerbull Studied up to 10th standardbull Smokerbull Non alcoholicbull Married bull Normal sleep appetite bowel and bladder
habitsbull Diet - vegetarian
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
Research Activities
Research Activities
Average no of studies done per year 22
Average no of papers published in reputed national amp international journals per year
14
In last 6 years our students have published around 100 research papers in national and international reputed journals
Presently work in the department is covering all major aspects of cardiology includingbull PTCA + STENTING including complex angioplastiesbull Primary PCIbull Rotablationbull IVUS FFRbull Carotid and other peripheral angioplastiesbull Renal angioplastiesbull BMVBPV BAVbull ASD VSD PDA Device closurebull Permanent pacemaker implantations including Dual chamber and MRI
compatible pacemakersbull AICDbull CRT-P CRT-Dbull EPS and RFAbull Arterial Embolizationbull Endomyocardial biopsy
bull These are comparable to most of the leading Govt Institutes anywhere in India
bull We are also trying to upgrade our facilities in the field of structural heart disease which includes endovascular treatment of aortic aneurysm dissection paravalvular leak closure TAVI etc
bull Lastly the Honorable CM has sanctioned a new Cath lab for our department in the present budget which will be installed soon A new 3-D Echo machine is being installed in next 2-3 months This will further improve the working in the department for better care of the poor patients
THANK YOU
CPC caseDepartment Cardiology
8th July 2016
Presenter Dr Rakesh Kumar Ola Dr Daulat Singh Meena
Cardiology discussant Dr Sohan K Sharma Assistant Prof Deptt Cardiology
Respiratory discussant Dr Sheetu Singh Assistant Prof Chest amp TB
Medicine discussant Dr Ashutosh Daga Resident Deptt Of Medicine ProfDrHemant Malhotra PHOD Deptt Of Medicine
Radiology discussant Dr Sachin Lamba Resident RadiologyDr RK Yadav Astt Prof Radiology
Pathology discussant Dr Neetu Aggarwal Sr Resident PathologyDr Anita Harsh Assoc Prof Pathology
Case Presenter
Dr Rakesh Kumar OlaIIIrd Year Resident
Department of Cardiology
Presenting complaints
A 38y old male resident of Jhalawar-Rajasthan presented with complaints of bull Fever on and off-12 monthsbull Cough- 12 monthsbull Weight loss-12 monthsbull Shortness of breath on exertion- 6 months bull Bilateral lower limb swelling- 15-20 days
History of presenting illness
Asymptomatic till 12 month back when he developed - Fever bull Insidious bull Low grade bull Intermittent typebull Each episode lasted for 10-15 daysbull Not associated with chills and rigor bull No diurnal variation bull Relieved by medications
History of presenting illness
Cough -12 monthbull Non-productive coughbull On and Off bull Each episode lasted for 20-30 days bull Cough was not associated with hemoptysis
chest heaviness noisy breathing and post-nasal discharge
bull No postural diurnal or seasonal variation
History of presenting illness
Weight loss -12 monthbull Patient had ho of significant weight loss of
5kg in last 12 months associated with easy fatigability
History of presenting illness
Shortness of breath-6 monthsbull Insidious onset bull Patient initially complain SOB on more than ordinary
activity and it progressively increased over 5 months and from last one month patient having SOB on less than ordinary physical activity (NYHA grade I to III ) but not at rest
bull SOB was not worsen by lying down and had no HO of episodic breathlessness during night
bull No postural or diurnal or seasonal variation
History of presenting illness
Bilateral lower limb swelling- 15-20 daysbull Lower limb swelling started from ankle joint
and progressed up to knee joint bull Not associated with morning facial puffiness
and abdominal fullnessbull No pain tenderness or warmth of lower limb
History of presenting illness
No history of bull Personal or family history of atopy or allergy like
itching skin lesions urticaria noisy breathing or seasonal variations
bull History of joint pains oral ulcersbull Travel out of statebull History of drugs or radiation exposurebull Occupational exposure of dust or smoke
History of presenting illness
No history of bull Recurrent episodes of diarrhoea abdominal pain
dysphagia or icterusbull Chest pain bull Palpitationbull Loss of consciousness bull Ho of focal neurological deficit
Past medical history
bull Patient had history of recurrent admissions and received treatment for enteric fever and malaria though patient had no relief in symptoms from same
bull No HO of DM HTN Tuberculosisbull No Ho any surgical intervention in past
Personal history
bull Laborerbull Studied up to 10th standardbull Smokerbull Non alcoholicbull Married bull Normal sleep appetite bowel and bladder
habitsbull Diet - vegetarian
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
Presently work in the department is covering all major aspects of cardiology includingbull PTCA + STENTING including complex angioplastiesbull Primary PCIbull Rotablationbull IVUS FFRbull Carotid and other peripheral angioplastiesbull Renal angioplastiesbull BMVBPV BAVbull ASD VSD PDA Device closurebull Permanent pacemaker implantations including Dual chamber and MRI
compatible pacemakersbull AICDbull CRT-P CRT-Dbull EPS and RFAbull Arterial Embolizationbull Endomyocardial biopsy
bull These are comparable to most of the leading Govt Institutes anywhere in India
bull We are also trying to upgrade our facilities in the field of structural heart disease which includes endovascular treatment of aortic aneurysm dissection paravalvular leak closure TAVI etc
bull Lastly the Honorable CM has sanctioned a new Cath lab for our department in the present budget which will be installed soon A new 3-D Echo machine is being installed in next 2-3 months This will further improve the working in the department for better care of the poor patients
THANK YOU
CPC caseDepartment Cardiology
8th July 2016
Presenter Dr Rakesh Kumar Ola Dr Daulat Singh Meena
Cardiology discussant Dr Sohan K Sharma Assistant Prof Deptt Cardiology
Respiratory discussant Dr Sheetu Singh Assistant Prof Chest amp TB
Medicine discussant Dr Ashutosh Daga Resident Deptt Of Medicine ProfDrHemant Malhotra PHOD Deptt Of Medicine
Radiology discussant Dr Sachin Lamba Resident RadiologyDr RK Yadav Astt Prof Radiology
Pathology discussant Dr Neetu Aggarwal Sr Resident PathologyDr Anita Harsh Assoc Prof Pathology
Case Presenter
Dr Rakesh Kumar OlaIIIrd Year Resident
Department of Cardiology
Presenting complaints
A 38y old male resident of Jhalawar-Rajasthan presented with complaints of bull Fever on and off-12 monthsbull Cough- 12 monthsbull Weight loss-12 monthsbull Shortness of breath on exertion- 6 months bull Bilateral lower limb swelling- 15-20 days
History of presenting illness
Asymptomatic till 12 month back when he developed - Fever bull Insidious bull Low grade bull Intermittent typebull Each episode lasted for 10-15 daysbull Not associated with chills and rigor bull No diurnal variation bull Relieved by medications
History of presenting illness
Cough -12 monthbull Non-productive coughbull On and Off bull Each episode lasted for 20-30 days bull Cough was not associated with hemoptysis
chest heaviness noisy breathing and post-nasal discharge
bull No postural diurnal or seasonal variation
History of presenting illness
Weight loss -12 monthbull Patient had ho of significant weight loss of
5kg in last 12 months associated with easy fatigability
History of presenting illness
Shortness of breath-6 monthsbull Insidious onset bull Patient initially complain SOB on more than ordinary
activity and it progressively increased over 5 months and from last one month patient having SOB on less than ordinary physical activity (NYHA grade I to III ) but not at rest
bull SOB was not worsen by lying down and had no HO of episodic breathlessness during night
bull No postural or diurnal or seasonal variation
History of presenting illness
Bilateral lower limb swelling- 15-20 daysbull Lower limb swelling started from ankle joint
and progressed up to knee joint bull Not associated with morning facial puffiness
and abdominal fullnessbull No pain tenderness or warmth of lower limb
History of presenting illness
No history of bull Personal or family history of atopy or allergy like
itching skin lesions urticaria noisy breathing or seasonal variations
bull History of joint pains oral ulcersbull Travel out of statebull History of drugs or radiation exposurebull Occupational exposure of dust or smoke
History of presenting illness
No history of bull Recurrent episodes of diarrhoea abdominal pain
dysphagia or icterusbull Chest pain bull Palpitationbull Loss of consciousness bull Ho of focal neurological deficit
Past medical history
bull Patient had history of recurrent admissions and received treatment for enteric fever and malaria though patient had no relief in symptoms from same
bull No HO of DM HTN Tuberculosisbull No Ho any surgical intervention in past
Personal history
bull Laborerbull Studied up to 10th standardbull Smokerbull Non alcoholicbull Married bull Normal sleep appetite bowel and bladder
habitsbull Diet - vegetarian
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
bull These are comparable to most of the leading Govt Institutes anywhere in India
bull We are also trying to upgrade our facilities in the field of structural heart disease which includes endovascular treatment of aortic aneurysm dissection paravalvular leak closure TAVI etc
bull Lastly the Honorable CM has sanctioned a new Cath lab for our department in the present budget which will be installed soon A new 3-D Echo machine is being installed in next 2-3 months This will further improve the working in the department for better care of the poor patients
THANK YOU
CPC caseDepartment Cardiology
8th July 2016
Presenter Dr Rakesh Kumar Ola Dr Daulat Singh Meena
Cardiology discussant Dr Sohan K Sharma Assistant Prof Deptt Cardiology
Respiratory discussant Dr Sheetu Singh Assistant Prof Chest amp TB
Medicine discussant Dr Ashutosh Daga Resident Deptt Of Medicine ProfDrHemant Malhotra PHOD Deptt Of Medicine
Radiology discussant Dr Sachin Lamba Resident RadiologyDr RK Yadav Astt Prof Radiology
Pathology discussant Dr Neetu Aggarwal Sr Resident PathologyDr Anita Harsh Assoc Prof Pathology
Case Presenter
Dr Rakesh Kumar OlaIIIrd Year Resident
Department of Cardiology
Presenting complaints
A 38y old male resident of Jhalawar-Rajasthan presented with complaints of bull Fever on and off-12 monthsbull Cough- 12 monthsbull Weight loss-12 monthsbull Shortness of breath on exertion- 6 months bull Bilateral lower limb swelling- 15-20 days
History of presenting illness
Asymptomatic till 12 month back when he developed - Fever bull Insidious bull Low grade bull Intermittent typebull Each episode lasted for 10-15 daysbull Not associated with chills and rigor bull No diurnal variation bull Relieved by medications
History of presenting illness
Cough -12 monthbull Non-productive coughbull On and Off bull Each episode lasted for 20-30 days bull Cough was not associated with hemoptysis
chest heaviness noisy breathing and post-nasal discharge
bull No postural diurnal or seasonal variation
History of presenting illness
Weight loss -12 monthbull Patient had ho of significant weight loss of
5kg in last 12 months associated with easy fatigability
History of presenting illness
Shortness of breath-6 monthsbull Insidious onset bull Patient initially complain SOB on more than ordinary
activity and it progressively increased over 5 months and from last one month patient having SOB on less than ordinary physical activity (NYHA grade I to III ) but not at rest
bull SOB was not worsen by lying down and had no HO of episodic breathlessness during night
bull No postural or diurnal or seasonal variation
History of presenting illness
Bilateral lower limb swelling- 15-20 daysbull Lower limb swelling started from ankle joint
and progressed up to knee joint bull Not associated with morning facial puffiness
and abdominal fullnessbull No pain tenderness or warmth of lower limb
History of presenting illness
No history of bull Personal or family history of atopy or allergy like
itching skin lesions urticaria noisy breathing or seasonal variations
bull History of joint pains oral ulcersbull Travel out of statebull History of drugs or radiation exposurebull Occupational exposure of dust or smoke
History of presenting illness
No history of bull Recurrent episodes of diarrhoea abdominal pain
dysphagia or icterusbull Chest pain bull Palpitationbull Loss of consciousness bull Ho of focal neurological deficit
Past medical history
bull Patient had history of recurrent admissions and received treatment for enteric fever and malaria though patient had no relief in symptoms from same
bull No HO of DM HTN Tuberculosisbull No Ho any surgical intervention in past
Personal history
bull Laborerbull Studied up to 10th standardbull Smokerbull Non alcoholicbull Married bull Normal sleep appetite bowel and bladder
habitsbull Diet - vegetarian
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber

THANK YOU
CPC caseDepartment Cardiology
8th July 2016
Presenter Dr Rakesh Kumar Ola Dr Daulat Singh Meena
Cardiology discussant Dr Sohan K Sharma Assistant Prof Deptt Cardiology
Respiratory discussant Dr Sheetu Singh Assistant Prof Chest amp TB
Medicine discussant Dr Ashutosh Daga Resident Deptt Of Medicine ProfDrHemant Malhotra PHOD Deptt Of Medicine
Radiology discussant Dr Sachin Lamba Resident RadiologyDr RK Yadav Astt Prof Radiology
Pathology discussant Dr Neetu Aggarwal Sr Resident PathologyDr Anita Harsh Assoc Prof Pathology
Case Presenter
Dr Rakesh Kumar OlaIIIrd Year Resident
Department of Cardiology
Presenting complaints
A 38y old male resident of Jhalawar-Rajasthan presented with complaints of bull Fever on and off-12 monthsbull Cough- 12 monthsbull Weight loss-12 monthsbull Shortness of breath on exertion- 6 months bull Bilateral lower limb swelling- 15-20 days
History of presenting illness
Asymptomatic till 12 month back when he developed - Fever bull Insidious bull Low grade bull Intermittent typebull Each episode lasted for 10-15 daysbull Not associated with chills and rigor bull No diurnal variation bull Relieved by medications
History of presenting illness
Cough -12 monthbull Non-productive coughbull On and Off bull Each episode lasted for 20-30 days bull Cough was not associated with hemoptysis
chest heaviness noisy breathing and post-nasal discharge
bull No postural diurnal or seasonal variation
History of presenting illness
Weight loss -12 monthbull Patient had ho of significant weight loss of
5kg in last 12 months associated with easy fatigability
History of presenting illness
Shortness of breath-6 monthsbull Insidious onset bull Patient initially complain SOB on more than ordinary
activity and it progressively increased over 5 months and from last one month patient having SOB on less than ordinary physical activity (NYHA grade I to III ) but not at rest
bull SOB was not worsen by lying down and had no HO of episodic breathlessness during night
bull No postural or diurnal or seasonal variation
History of presenting illness
Bilateral lower limb swelling- 15-20 daysbull Lower limb swelling started from ankle joint
and progressed up to knee joint bull Not associated with morning facial puffiness
and abdominal fullnessbull No pain tenderness or warmth of lower limb
History of presenting illness
No history of bull Personal or family history of atopy or allergy like
itching skin lesions urticaria noisy breathing or seasonal variations
bull History of joint pains oral ulcersbull Travel out of statebull History of drugs or radiation exposurebull Occupational exposure of dust or smoke
History of presenting illness
No history of bull Recurrent episodes of diarrhoea abdominal pain
dysphagia or icterusbull Chest pain bull Palpitationbull Loss of consciousness bull Ho of focal neurological deficit
Past medical history
bull Patient had history of recurrent admissions and received treatment for enteric fever and malaria though patient had no relief in symptoms from same
bull No HO of DM HTN Tuberculosisbull No Ho any surgical intervention in past
Personal history
bull Laborerbull Studied up to 10th standardbull Smokerbull Non alcoholicbull Married bull Normal sleep appetite bowel and bladder
habitsbull Diet - vegetarian
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
CPC caseDepartment Cardiology
8th July 2016
Presenter Dr Rakesh Kumar Ola Dr Daulat Singh Meena
Cardiology discussant Dr Sohan K Sharma Assistant Prof Deptt Cardiology
Respiratory discussant Dr Sheetu Singh Assistant Prof Chest amp TB
Medicine discussant Dr Ashutosh Daga Resident Deptt Of Medicine ProfDrHemant Malhotra PHOD Deptt Of Medicine
Radiology discussant Dr Sachin Lamba Resident RadiologyDr RK Yadav Astt Prof Radiology
Pathology discussant Dr Neetu Aggarwal Sr Resident PathologyDr Anita Harsh Assoc Prof Pathology
Case Presenter
Dr Rakesh Kumar OlaIIIrd Year Resident
Department of Cardiology
Presenting complaints
A 38y old male resident of Jhalawar-Rajasthan presented with complaints of bull Fever on and off-12 monthsbull Cough- 12 monthsbull Weight loss-12 monthsbull Shortness of breath on exertion- 6 months bull Bilateral lower limb swelling- 15-20 days
History of presenting illness
Asymptomatic till 12 month back when he developed - Fever bull Insidious bull Low grade bull Intermittent typebull Each episode lasted for 10-15 daysbull Not associated with chills and rigor bull No diurnal variation bull Relieved by medications
History of presenting illness
Cough -12 monthbull Non-productive coughbull On and Off bull Each episode lasted for 20-30 days bull Cough was not associated with hemoptysis
chest heaviness noisy breathing and post-nasal discharge
bull No postural diurnal or seasonal variation
History of presenting illness
Weight loss -12 monthbull Patient had ho of significant weight loss of
5kg in last 12 months associated with easy fatigability
History of presenting illness
Shortness of breath-6 monthsbull Insidious onset bull Patient initially complain SOB on more than ordinary
activity and it progressively increased over 5 months and from last one month patient having SOB on less than ordinary physical activity (NYHA grade I to III ) but not at rest
bull SOB was not worsen by lying down and had no HO of episodic breathlessness during night
bull No postural or diurnal or seasonal variation
History of presenting illness
Bilateral lower limb swelling- 15-20 daysbull Lower limb swelling started from ankle joint
and progressed up to knee joint bull Not associated with morning facial puffiness
and abdominal fullnessbull No pain tenderness or warmth of lower limb
History of presenting illness
No history of bull Personal or family history of atopy or allergy like
itching skin lesions urticaria noisy breathing or seasonal variations
bull History of joint pains oral ulcersbull Travel out of statebull History of drugs or radiation exposurebull Occupational exposure of dust or smoke
History of presenting illness
No history of bull Recurrent episodes of diarrhoea abdominal pain
dysphagia or icterusbull Chest pain bull Palpitationbull Loss of consciousness bull Ho of focal neurological deficit
Past medical history
bull Patient had history of recurrent admissions and received treatment for enteric fever and malaria though patient had no relief in symptoms from same
bull No HO of DM HTN Tuberculosisbull No Ho any surgical intervention in past
Personal history
bull Laborerbull Studied up to 10th standardbull Smokerbull Non alcoholicbull Married bull Normal sleep appetite bowel and bladder
habitsbull Diet - vegetarian
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
Case Presenter
Dr Rakesh Kumar OlaIIIrd Year Resident
Department of Cardiology
Presenting complaints
A 38y old male resident of Jhalawar-Rajasthan presented with complaints of bull Fever on and off-12 monthsbull Cough- 12 monthsbull Weight loss-12 monthsbull Shortness of breath on exertion- 6 months bull Bilateral lower limb swelling- 15-20 days
History of presenting illness
Asymptomatic till 12 month back when he developed - Fever bull Insidious bull Low grade bull Intermittent typebull Each episode lasted for 10-15 daysbull Not associated with chills and rigor bull No diurnal variation bull Relieved by medications
History of presenting illness
Cough -12 monthbull Non-productive coughbull On and Off bull Each episode lasted for 20-30 days bull Cough was not associated with hemoptysis
chest heaviness noisy breathing and post-nasal discharge
bull No postural diurnal or seasonal variation
History of presenting illness
Weight loss -12 monthbull Patient had ho of significant weight loss of
5kg in last 12 months associated with easy fatigability
History of presenting illness
Shortness of breath-6 monthsbull Insidious onset bull Patient initially complain SOB on more than ordinary
activity and it progressively increased over 5 months and from last one month patient having SOB on less than ordinary physical activity (NYHA grade I to III ) but not at rest
bull SOB was not worsen by lying down and had no HO of episodic breathlessness during night
bull No postural or diurnal or seasonal variation
History of presenting illness
Bilateral lower limb swelling- 15-20 daysbull Lower limb swelling started from ankle joint
and progressed up to knee joint bull Not associated with morning facial puffiness
and abdominal fullnessbull No pain tenderness or warmth of lower limb
History of presenting illness
No history of bull Personal or family history of atopy or allergy like
itching skin lesions urticaria noisy breathing or seasonal variations
bull History of joint pains oral ulcersbull Travel out of statebull History of drugs or radiation exposurebull Occupational exposure of dust or smoke
History of presenting illness
No history of bull Recurrent episodes of diarrhoea abdominal pain
dysphagia or icterusbull Chest pain bull Palpitationbull Loss of consciousness bull Ho of focal neurological deficit
Past medical history
bull Patient had history of recurrent admissions and received treatment for enteric fever and malaria though patient had no relief in symptoms from same
bull No HO of DM HTN Tuberculosisbull No Ho any surgical intervention in past
Personal history
bull Laborerbull Studied up to 10th standardbull Smokerbull Non alcoholicbull Married bull Normal sleep appetite bowel and bladder
habitsbull Diet - vegetarian
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
Presenting complaints
A 38y old male resident of Jhalawar-Rajasthan presented with complaints of bull Fever on and off-12 monthsbull Cough- 12 monthsbull Weight loss-12 monthsbull Shortness of breath on exertion- 6 months bull Bilateral lower limb swelling- 15-20 days
History of presenting illness
Asymptomatic till 12 month back when he developed - Fever bull Insidious bull Low grade bull Intermittent typebull Each episode lasted for 10-15 daysbull Not associated with chills and rigor bull No diurnal variation bull Relieved by medications
History of presenting illness
Cough -12 monthbull Non-productive coughbull On and Off bull Each episode lasted for 20-30 days bull Cough was not associated with hemoptysis
chest heaviness noisy breathing and post-nasal discharge
bull No postural diurnal or seasonal variation
History of presenting illness
Weight loss -12 monthbull Patient had ho of significant weight loss of
5kg in last 12 months associated with easy fatigability
History of presenting illness
Shortness of breath-6 monthsbull Insidious onset bull Patient initially complain SOB on more than ordinary
activity and it progressively increased over 5 months and from last one month patient having SOB on less than ordinary physical activity (NYHA grade I to III ) but not at rest
bull SOB was not worsen by lying down and had no HO of episodic breathlessness during night
bull No postural or diurnal or seasonal variation
History of presenting illness
Bilateral lower limb swelling- 15-20 daysbull Lower limb swelling started from ankle joint
and progressed up to knee joint bull Not associated with morning facial puffiness
and abdominal fullnessbull No pain tenderness or warmth of lower limb
History of presenting illness
No history of bull Personal or family history of atopy or allergy like
itching skin lesions urticaria noisy breathing or seasonal variations
bull History of joint pains oral ulcersbull Travel out of statebull History of drugs or radiation exposurebull Occupational exposure of dust or smoke
History of presenting illness
No history of bull Recurrent episodes of diarrhoea abdominal pain
dysphagia or icterusbull Chest pain bull Palpitationbull Loss of consciousness bull Ho of focal neurological deficit
Past medical history
bull Patient had history of recurrent admissions and received treatment for enteric fever and malaria though patient had no relief in symptoms from same
bull No HO of DM HTN Tuberculosisbull No Ho any surgical intervention in past
Personal history
bull Laborerbull Studied up to 10th standardbull Smokerbull Non alcoholicbull Married bull Normal sleep appetite bowel and bladder
habitsbull Diet - vegetarian
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber

History of presenting illness
Asymptomatic till 12 month back when he developed - Fever bull Insidious bull Low grade bull Intermittent typebull Each episode lasted for 10-15 daysbull Not associated with chills and rigor bull No diurnal variation bull Relieved by medications
History of presenting illness
Cough -12 monthbull Non-productive coughbull On and Off bull Each episode lasted for 20-30 days bull Cough was not associated with hemoptysis
chest heaviness noisy breathing and post-nasal discharge
bull No postural diurnal or seasonal variation
History of presenting illness
Weight loss -12 monthbull Patient had ho of significant weight loss of
5kg in last 12 months associated with easy fatigability
History of presenting illness
Shortness of breath-6 monthsbull Insidious onset bull Patient initially complain SOB on more than ordinary
activity and it progressively increased over 5 months and from last one month patient having SOB on less than ordinary physical activity (NYHA grade I to III ) but not at rest
bull SOB was not worsen by lying down and had no HO of episodic breathlessness during night
bull No postural or diurnal or seasonal variation
History of presenting illness
Bilateral lower limb swelling- 15-20 daysbull Lower limb swelling started from ankle joint
and progressed up to knee joint bull Not associated with morning facial puffiness
and abdominal fullnessbull No pain tenderness or warmth of lower limb
History of presenting illness
No history of bull Personal or family history of atopy or allergy like
itching skin lesions urticaria noisy breathing or seasonal variations
bull History of joint pains oral ulcersbull Travel out of statebull History of drugs or radiation exposurebull Occupational exposure of dust or smoke
History of presenting illness
No history of bull Recurrent episodes of diarrhoea abdominal pain
dysphagia or icterusbull Chest pain bull Palpitationbull Loss of consciousness bull Ho of focal neurological deficit
Past medical history
bull Patient had history of recurrent admissions and received treatment for enteric fever and malaria though patient had no relief in symptoms from same
bull No HO of DM HTN Tuberculosisbull No Ho any surgical intervention in past
Personal history
bull Laborerbull Studied up to 10th standardbull Smokerbull Non alcoholicbull Married bull Normal sleep appetite bowel and bladder
habitsbull Diet - vegetarian
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
History of presenting illness
Cough -12 monthbull Non-productive coughbull On and Off bull Each episode lasted for 20-30 days bull Cough was not associated with hemoptysis
chest heaviness noisy breathing and post-nasal discharge
bull No postural diurnal or seasonal variation
History of presenting illness
Weight loss -12 monthbull Patient had ho of significant weight loss of
5kg in last 12 months associated with easy fatigability
History of presenting illness
Shortness of breath-6 monthsbull Insidious onset bull Patient initially complain SOB on more than ordinary
activity and it progressively increased over 5 months and from last one month patient having SOB on less than ordinary physical activity (NYHA grade I to III ) but not at rest
bull SOB was not worsen by lying down and had no HO of episodic breathlessness during night
bull No postural or diurnal or seasonal variation
History of presenting illness
Bilateral lower limb swelling- 15-20 daysbull Lower limb swelling started from ankle joint
and progressed up to knee joint bull Not associated with morning facial puffiness
and abdominal fullnessbull No pain tenderness or warmth of lower limb
History of presenting illness
No history of bull Personal or family history of atopy or allergy like
itching skin lesions urticaria noisy breathing or seasonal variations
bull History of joint pains oral ulcersbull Travel out of statebull History of drugs or radiation exposurebull Occupational exposure of dust or smoke
History of presenting illness
No history of bull Recurrent episodes of diarrhoea abdominal pain
dysphagia or icterusbull Chest pain bull Palpitationbull Loss of consciousness bull Ho of focal neurological deficit
Past medical history
bull Patient had history of recurrent admissions and received treatment for enteric fever and malaria though patient had no relief in symptoms from same
bull No HO of DM HTN Tuberculosisbull No Ho any surgical intervention in past
Personal history
bull Laborerbull Studied up to 10th standardbull Smokerbull Non alcoholicbull Married bull Normal sleep appetite bowel and bladder
habitsbull Diet - vegetarian
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
History of presenting illness
Weight loss -12 monthbull Patient had ho of significant weight loss of
5kg in last 12 months associated with easy fatigability
History of presenting illness
Shortness of breath-6 monthsbull Insidious onset bull Patient initially complain SOB on more than ordinary
activity and it progressively increased over 5 months and from last one month patient having SOB on less than ordinary physical activity (NYHA grade I to III ) but not at rest
bull SOB was not worsen by lying down and had no HO of episodic breathlessness during night
bull No postural or diurnal or seasonal variation
History of presenting illness
Bilateral lower limb swelling- 15-20 daysbull Lower limb swelling started from ankle joint
and progressed up to knee joint bull Not associated with morning facial puffiness
and abdominal fullnessbull No pain tenderness or warmth of lower limb
History of presenting illness
No history of bull Personal or family history of atopy or allergy like
itching skin lesions urticaria noisy breathing or seasonal variations
bull History of joint pains oral ulcersbull Travel out of statebull History of drugs or radiation exposurebull Occupational exposure of dust or smoke
History of presenting illness
No history of bull Recurrent episodes of diarrhoea abdominal pain
dysphagia or icterusbull Chest pain bull Palpitationbull Loss of consciousness bull Ho of focal neurological deficit
Past medical history
bull Patient had history of recurrent admissions and received treatment for enteric fever and malaria though patient had no relief in symptoms from same
bull No HO of DM HTN Tuberculosisbull No Ho any surgical intervention in past
Personal history
bull Laborerbull Studied up to 10th standardbull Smokerbull Non alcoholicbull Married bull Normal sleep appetite bowel and bladder
habitsbull Diet - vegetarian
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
History of presenting illness
Shortness of breath-6 monthsbull Insidious onset bull Patient initially complain SOB on more than ordinary
activity and it progressively increased over 5 months and from last one month patient having SOB on less than ordinary physical activity (NYHA grade I to III ) but not at rest
bull SOB was not worsen by lying down and had no HO of episodic breathlessness during night
bull No postural or diurnal or seasonal variation
History of presenting illness
Bilateral lower limb swelling- 15-20 daysbull Lower limb swelling started from ankle joint
and progressed up to knee joint bull Not associated with morning facial puffiness
and abdominal fullnessbull No pain tenderness or warmth of lower limb
History of presenting illness
No history of bull Personal or family history of atopy or allergy like
itching skin lesions urticaria noisy breathing or seasonal variations
bull History of joint pains oral ulcersbull Travel out of statebull History of drugs or radiation exposurebull Occupational exposure of dust or smoke
History of presenting illness
No history of bull Recurrent episodes of diarrhoea abdominal pain
dysphagia or icterusbull Chest pain bull Palpitationbull Loss of consciousness bull Ho of focal neurological deficit
Past medical history
bull Patient had history of recurrent admissions and received treatment for enteric fever and malaria though patient had no relief in symptoms from same
bull No HO of DM HTN Tuberculosisbull No Ho any surgical intervention in past
Personal history
bull Laborerbull Studied up to 10th standardbull Smokerbull Non alcoholicbull Married bull Normal sleep appetite bowel and bladder
habitsbull Diet - vegetarian
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
History of presenting illness
Bilateral lower limb swelling- 15-20 daysbull Lower limb swelling started from ankle joint
and progressed up to knee joint bull Not associated with morning facial puffiness
and abdominal fullnessbull No pain tenderness or warmth of lower limb
History of presenting illness
No history of bull Personal or family history of atopy or allergy like
itching skin lesions urticaria noisy breathing or seasonal variations
bull History of joint pains oral ulcersbull Travel out of statebull History of drugs or radiation exposurebull Occupational exposure of dust or smoke
History of presenting illness
No history of bull Recurrent episodes of diarrhoea abdominal pain
dysphagia or icterusbull Chest pain bull Palpitationbull Loss of consciousness bull Ho of focal neurological deficit
Past medical history
bull Patient had history of recurrent admissions and received treatment for enteric fever and malaria though patient had no relief in symptoms from same
bull No HO of DM HTN Tuberculosisbull No Ho any surgical intervention in past
Personal history
bull Laborerbull Studied up to 10th standardbull Smokerbull Non alcoholicbull Married bull Normal sleep appetite bowel and bladder
habitsbull Diet - vegetarian
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber

History of presenting illness
No history of bull Personal or family history of atopy or allergy like
itching skin lesions urticaria noisy breathing or seasonal variations
bull History of joint pains oral ulcersbull Travel out of statebull History of drugs or radiation exposurebull Occupational exposure of dust or smoke
History of presenting illness
No history of bull Recurrent episodes of diarrhoea abdominal pain
dysphagia or icterusbull Chest pain bull Palpitationbull Loss of consciousness bull Ho of focal neurological deficit
Past medical history
bull Patient had history of recurrent admissions and received treatment for enteric fever and malaria though patient had no relief in symptoms from same
bull No HO of DM HTN Tuberculosisbull No Ho any surgical intervention in past
Personal history
bull Laborerbull Studied up to 10th standardbull Smokerbull Non alcoholicbull Married bull Normal sleep appetite bowel and bladder
habitsbull Diet - vegetarian
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
History of presenting illness
No history of bull Recurrent episodes of diarrhoea abdominal pain
dysphagia or icterusbull Chest pain bull Palpitationbull Loss of consciousness bull Ho of focal neurological deficit
Past medical history
bull Patient had history of recurrent admissions and received treatment for enteric fever and malaria though patient had no relief in symptoms from same
bull No HO of DM HTN Tuberculosisbull No Ho any surgical intervention in past
Personal history
bull Laborerbull Studied up to 10th standardbull Smokerbull Non alcoholicbull Married bull Normal sleep appetite bowel and bladder
habitsbull Diet - vegetarian
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
Past medical history
bull Patient had history of recurrent admissions and received treatment for enteric fever and malaria though patient had no relief in symptoms from same
bull No HO of DM HTN Tuberculosisbull No Ho any surgical intervention in past
Personal history
bull Laborerbull Studied up to 10th standardbull Smokerbull Non alcoholicbull Married bull Normal sleep appetite bowel and bladder
habitsbull Diet - vegetarian
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber

Personal history
bull Laborerbull Studied up to 10th standardbull Smokerbull Non alcoholicbull Married bull Normal sleep appetite bowel and bladder
habitsbull Diet - vegetarian
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
Family history
bull No significant family history
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
Examination findingsGeneral physical examination Patient was conscious cooperative and well oriented to time place and person Pallor Present Icterus Absent Clubbing Absent Cyanosis Absent Lymphadenopathy Absent BL pedal edema Present (pitting) Neck veins Engorged and JVP
raised 6 cm above sternal angle with two prominent positive and two prominent negative wave seen
BMI 19 kgm2
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
Vitals Pulse = 96min (regular normal volume and character with
no vessel wall thickening no RR or RF delay all peripheral pulses felt )
Respiratory rate = 24min abdomino-thoracic
bull Blood pressure = 10072mmHg measured in right and left
arm in supine position and 10876 mmHg in right and left
lower limb in prone position no postural variation Temp ndash 984degF taken orally SpO2 = 95 on room air
Examination findings
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
Respiratory system examinationInspectionbull Chest symmetrical amp bilateral equal chest movementsbull Trachea centralbull No scars sinuses and dilated veinsPalpationbull Inspectory findings are confirmed
Percussionbull Bilateral equal resonant note
Auscultationbull Bilateral equal vesicular breath soundsbull Fine end-inspiratory crepitation present in bilateral infra-
scapular areas
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
CVS system examinationInspection bull Chest is bilaterally symmetrical no precordial bulge seenbull Apex impulse visualised in 5th LICS just medial to mid clavicular linebull No scar sinus fistula visible veins
Palpation Apex beat in Lt 5thIC just medial to mid clavicular line
Percussion LHB―gt Apex RHB ―gtretrosternal Left 2nd IC resonateAuscultation S1 S2 normal No added sound
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
Abdominal examination
Inspection non distended no venous prominence no scar PalpationLiver- 4cm below right costal margin at Right MCL soft
tender rounded regular margin smooth surface with systolic pulsation and no bruit liver span of 16cm
Spleen ndash Just palpable soft and non tenderAuscultationbull Normal bowel sound +
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
Summary bull A 38 year old male presented with intermittent fever cough
and Weight loss- 12 month followed by dyspnea on exertion which progressed from NYHA I to NYHA III over 6 months and now admitted with worsening of dyspnea and bilateral lower limb swelling -15-20 days
bull On examination pallor engorged neck vein bl pitting pedal edema and BL end-inspiratory crepts present with hepato-splenomegaly
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
Provisional Differential Diagnosis
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
bull Investigations
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
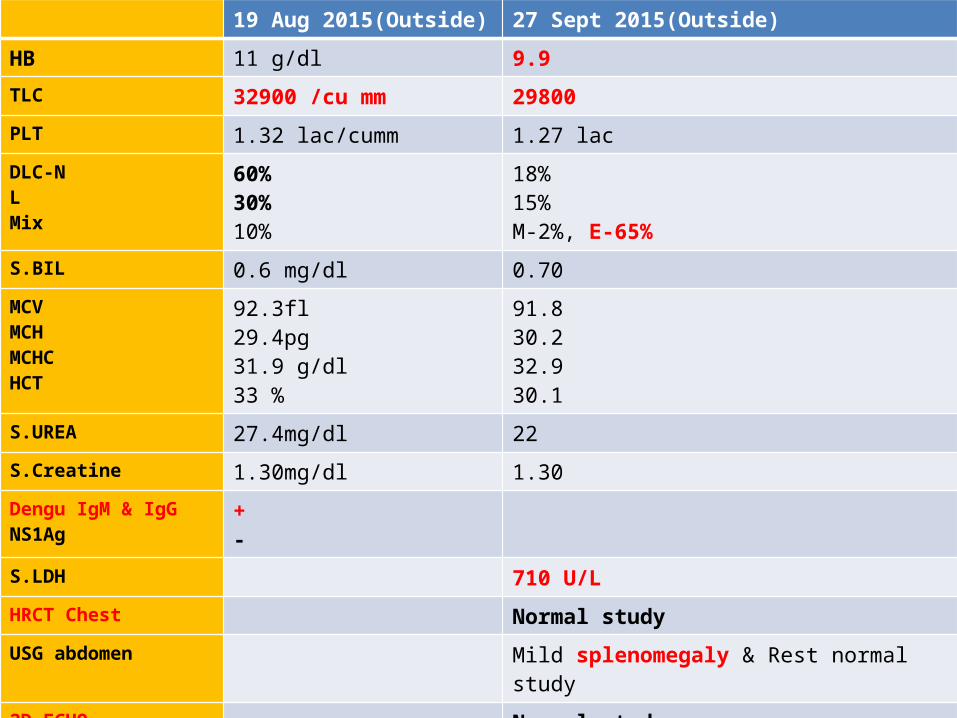
19 Aug 2015(Outside) 27 Sept 2015(Outside)
HB 11 gdl 99TLC 32900 cu mm 29800PLT 132 laccumm 127 lacDLC-NLMix
603010
1815M-2 E-65
SBIL 06 mgdl 070MCVMCHMCHCHCT
923fl294pg319 gdl33
918302329301
SUREA 274mgdl 22SCreatine 130mgdl 130Dengu IgM amp IgGNS1Ag
+-
SLDH 710 ULHRCT Chest Normal study USG abdomen Mild splenomegaly amp Rest normal study
2D ECHO Normal studyPBF Mild anisocytosis NCNC leukocytosis with
eosinophilia No parasite seen
30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber

30 MAY 2016(SMS) 30 may 2016(SMS)
HB 96 gdl CRP Positive TLC 2165 X 103 microl RA Factor NegativePLT 45 x 103 microl Dengue-IgM IgG Negative
DLC-NLEBMAbsolute Eosinophil Count-ESR-
1815650214 x 103microl33 mm
HCVHBsAg Negative
Widal Negative
SIgE 339 IUML
Stool examinationTwo sample
NAD
SBIL 06 mgdl SLDH 773 ULMCVMCHMCHCHCT
93fl338pg364 gdl264
CPK MB 683 UL
HI V Negative
SUREA 71 mgdl SCaSPh 88288 mgdlSCreatine 106 mgdl SCortisol 1750 ugdlLFT-SBILSGOTSGPTALP T Protein SAlb
20 mgdl241UL247UL78 IUL5231
PBF NCNC mild anisocytosis leukocytosis with eosinophilia with reduce platelets no parasite seen
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
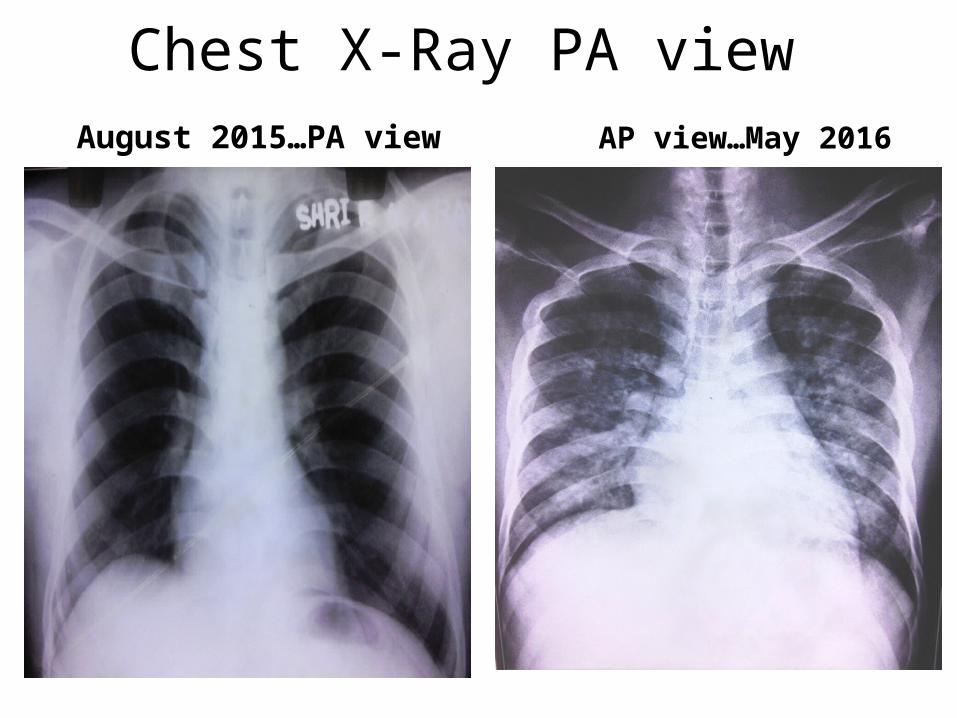
Chest X-Ray PA view August 2015hellipPA view AP viewhellipMay 2016
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
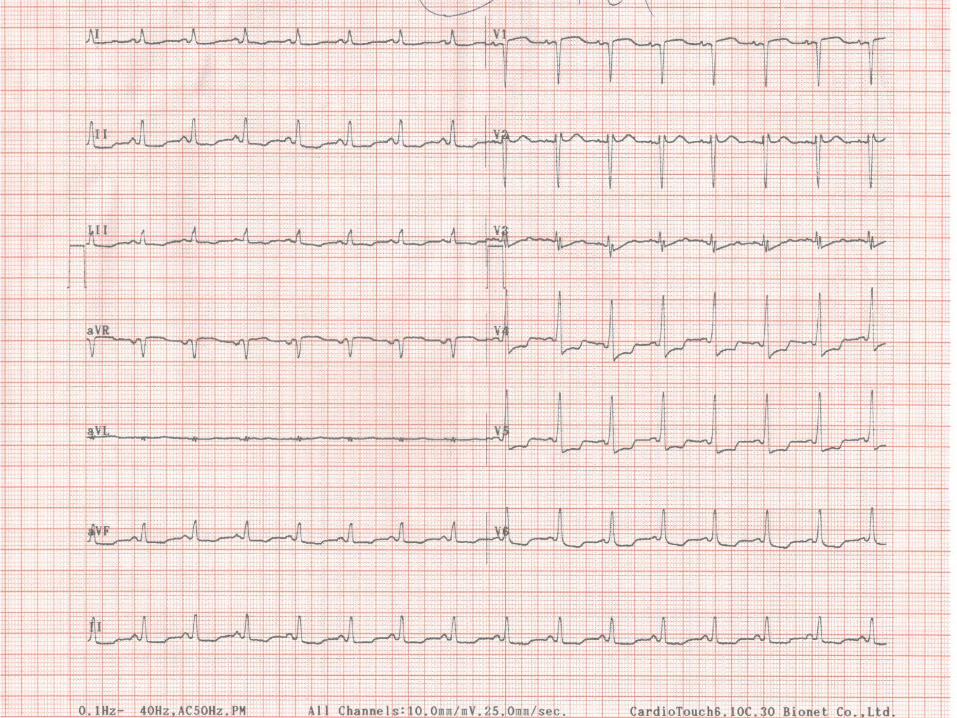
Conclude bull 38 year old male having 12 months history of progressive
dyspnea fever cough weight loss and pedal edema with recent worsening examination revealed bilateral pneumonitis right sided heart failure with hepato- splenomegaly and investigations showed hyper-eoisinopihillia
bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber

bull Differential diagnosis
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
Cause of hyper-eosinophilia 1 Reactive eosinophilia-bull Allergy- Drug reactions Asthmabull Parasitic infections- Strongyloidiasis Schistosomiasis Filariasis Toxocariasisbull Infectious disease- HIV chronic infections recovery from a bacterial infection bull Pulmonary diseases-eosinophilic pneumonia Loefflerrsquos pneumonia ABPA
hypersensitivity pneumonitisbull Collagen vascular disease-Churg Strauss syndrome Hypereosinophilic syndrome
Sarcoidosisbull Eosinophil-associated gastrointestinal disorders-eosinophilic esophagitis celiac
disease inflammatory bowel disease bull Malignant diseases-Hodgkin lymphoma non-Hodgkin lymphomas especially T-cell
lymphomas carcinomas (especially metastatic diseases) bull T-cell hypereosinophilic syndrome ie T-HES -Clonal expansion of
immunophenotypically aberrant T cells without overt lymph-proliferative diseasebull Endocrine hypo-functions- Addison disease
Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber

Cause of hyper-eosinophilia
2 Clonal eosinophilia-3 Acute myeloid leukemia 4 Chronic myeloid disorders a Molecularly defined
bull i BCRABL+ chronic myeloid leukemia bull ii PDGFRA-rearranged eosinophilic disorder bull iii PDGFRB-rearranged eosinophilic disorder bull iv KIT-mutated systemic mastocytosis bull v 8p11 syndrome (FGFR1 rearrangements)
b Clinicopathologically assigned
bull i Chronic myeloproliferative neoplasms (including chronic eosinophilic leukemia not otherwise specified (NOS) and mastocytosis)
bull ii Myelodysplastic syndromes bull iii Myelodysplastic myeloproliferative syndromes
3 Familial eosinophilia- family history of persistence hyper-eosinophillia of unknown cause
4 Idiopathic HES
DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber

DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PRELIMINANRY
INVESTIGATIONS
bull Allergic disorder-Asthma atopic dermatitisbull Drug hypersensitivity-Sulphonamides Antirheumatics Anticonvulsants
and Allopurinolbull Helminthic and parasitic infestationbull Eosinophil-associated gastrointestinal disorders-Primary
and secondary eosinophilic esophagitis celiac disease and IBDChronic pancreatitis
bull Radiation exposurebull Hypoadrenalismbull HIV
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
Respiratory discussion
Dr Sheetu Singh Assistant Prof
Department of chest amp TB
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber

Acute eosinophilic pneumonia
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
Acute eosinophilic pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestationsbull Raised blood eosinophil levels (may be
normal)
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
Allergic bronchopulmonary aspergillosis (ABPA)
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoea
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
POINTS AGAINSTbull History of asthma and atopy is ABSENTbull Presence of systemic manifestations
Allergic bronchopulmonary aspergillosis (ABPA)
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
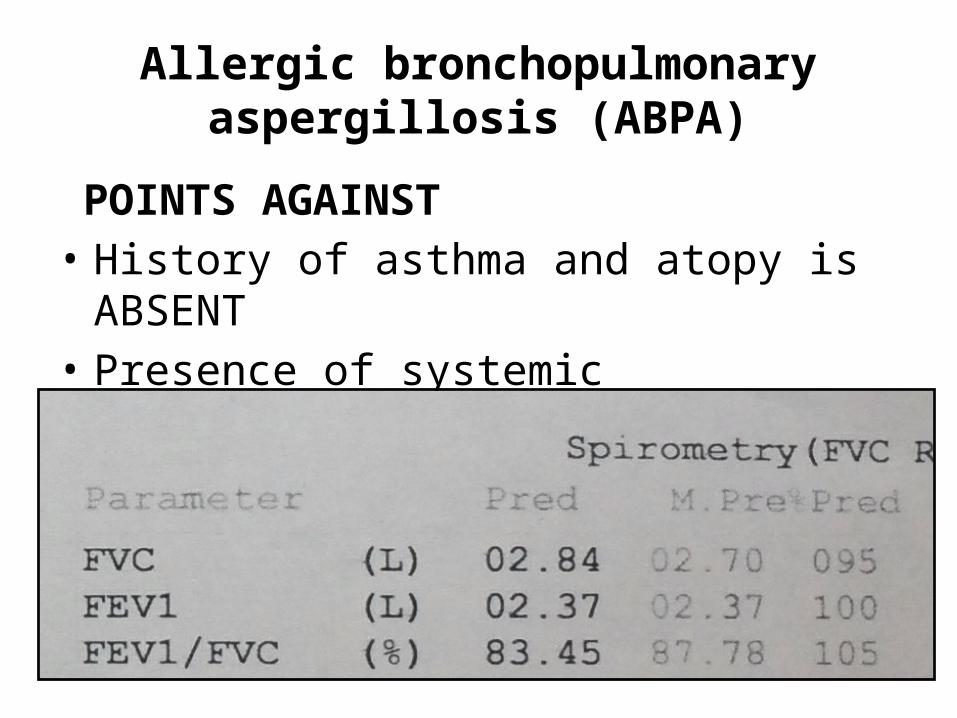
Skin prick test for Aspergillus
Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber

Churg Strauss syndrome
POINTS IN FAVOR bull Symptoms- Cough amp dyspnoeabull Systemic manifestations
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
Churg Strauss syndrome
POINTS AGAINSTbull History of asthma and atopy atleast 10 y prior
to onset of systemic featuresbull Spirometry is normal
bull p-ANCA - Negative
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
Loefflerrsquos pneumonia
POINTS IN FAVOR bull Cough and dyspnoea
Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber

Loefflerrsquos pneumonia
POINTS AGAINSTbull Chronic presentationbull Presence of systemic manifestations
bull Stool for ova amp cyst - negative
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull ABPAbull Churg Strauss syndromebull Hypereosinophilic syndromebull Sarcoidosisbull Hypersensitivity pneumonitisbull Autoimmune and Connective tissue disorderbull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
PULMONARY INFILTRATES WITH
EOSINOPHILIA
How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber

How to proceed
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
Algorithm of management
CECT chest with HR
cutsBronchoscopy
Broncho-alveolar lavage
+Transbronchial
lung biopsy
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
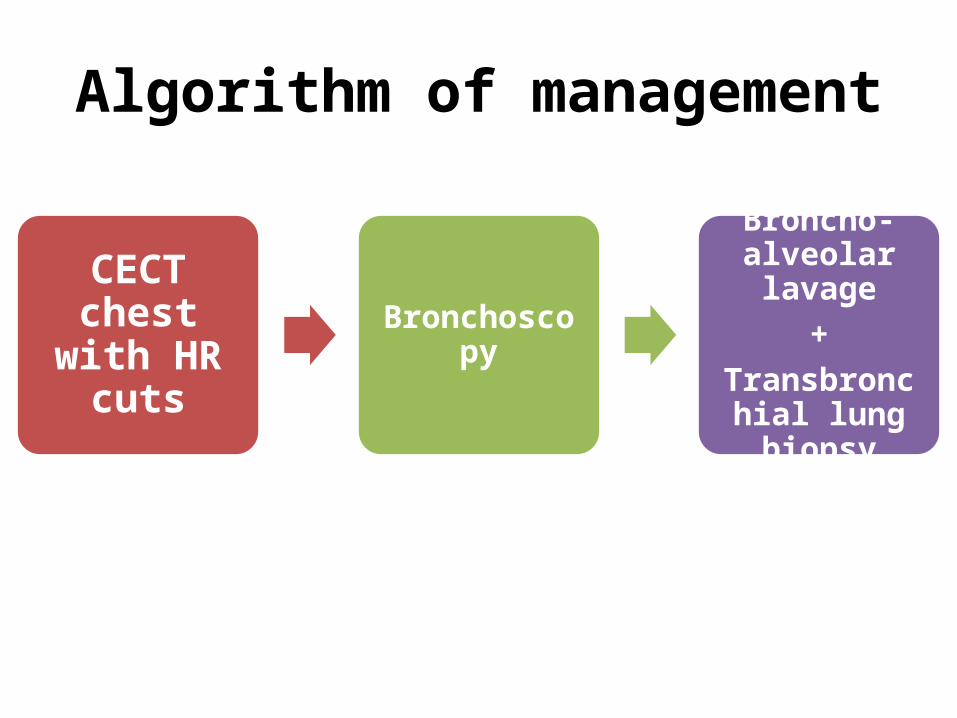
Medicine discussion
Dr Ashutosh Daga ( IIIrd year Resident)ProfDrHemant Malhotra PHOD Deptt Of Medicine
DEPARTMENT OF MEDICINE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber

bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber

INVESTIGATIONS REQUIRED
bull SIgE- 339 IUMLbull ANA-Negativebull RA Factor-Negative
bull SB12 level- gt2000 pgml
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
Autoimmune and Connective tissue disorder
POINTS IN FAVOURbull Multisystem involvement bull Haematological
manifestations
POINTS AGAINSTbull No history of joint pain oral
ulcers red eyesopthalmoplegiablurring of vision skin lesions or rash along with a normal physical examination
bull Normal RF and ANA titres rules out connective tissue disorders and autoimmune causes less likely
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
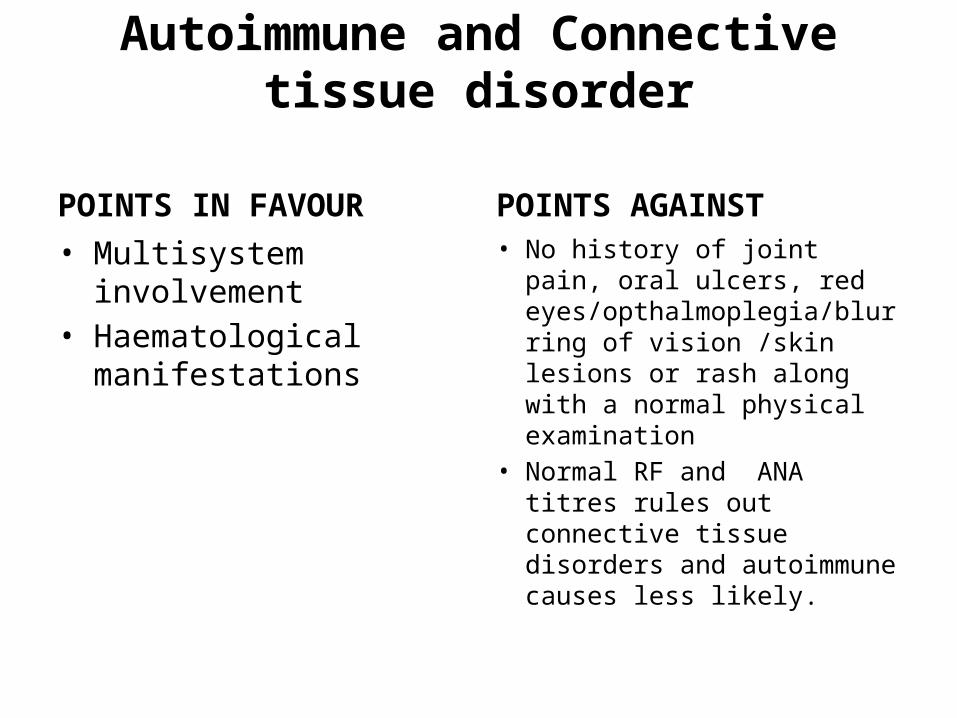
LEUKEMIAS
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Pulmonary involvementbull Hepatosplenomegaly
POINTS IN AGAINSTbull No blast seen in peripheral
bloodbull PBF not showing various
stage development of white blood maturation as in CML
bull No lymphadenopathybull Splenomegaly not massive
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
TUMOURS ASSOCIATED
POINTS IN FAVOURbull Shortness of breathbull Systemic manifestationsbull Pulmonary involvementbull Hepatosplenomegaly
POINTS AGAINSTbull No evident mass lesion in
X-RAY chest bull No palpable
lymphadenopathy bull Age of presentationbull No haemoptysis
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
POINTS IN FAVOURbull Fever and systemic
symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia
bull Hepatosplenomegaly
POINTS AGAINSTbull PBF not suggestive of any
dysplasia polycythemia
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
LYMPHOPROLIFERATIVE TYPE HES
POINTS IN FAVOUR
bull Pulmonary symptoms more common as compared to myeloproliferative type
bull Fever and systemic symptoms
bull Leukocytosis with thrombocytopenia and eosinophilia in PBF
bull Hepatosplenomegaly
POINTS AGAINST
bull Normal S-IgEbull No Itching eczemabull No Urticaria angioedemabull Pulmonary symptomsbull More aggressive clinical
presentationbull Cardiac involvementbull Increase serum vitamin B12
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
POINTS IN FAVOUR POINTS AGAINSTbull Pulmonary involvement
less common as compared to lymphoproliferative type of HES
bull Fever and systemic symptomsbull Leukocytosis with
thrombocytopenia and eosinophilia in PBF
bull Cardiac involvementbull Hepatosplenomegalybull Increase serum vitamin B12 bull More aggressive clinical
phenotypebull Normal IgE Levels
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomasbull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
bull Next investigation
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber

INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysis
Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber

Radiological discussion
Dr Sachin Lamba ( IIIrd Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
Chest X-Ray PA view -normal
SEPT 152015 SEPT 212015
CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber

CECT Chest ndashnormal(on sept 222015)
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
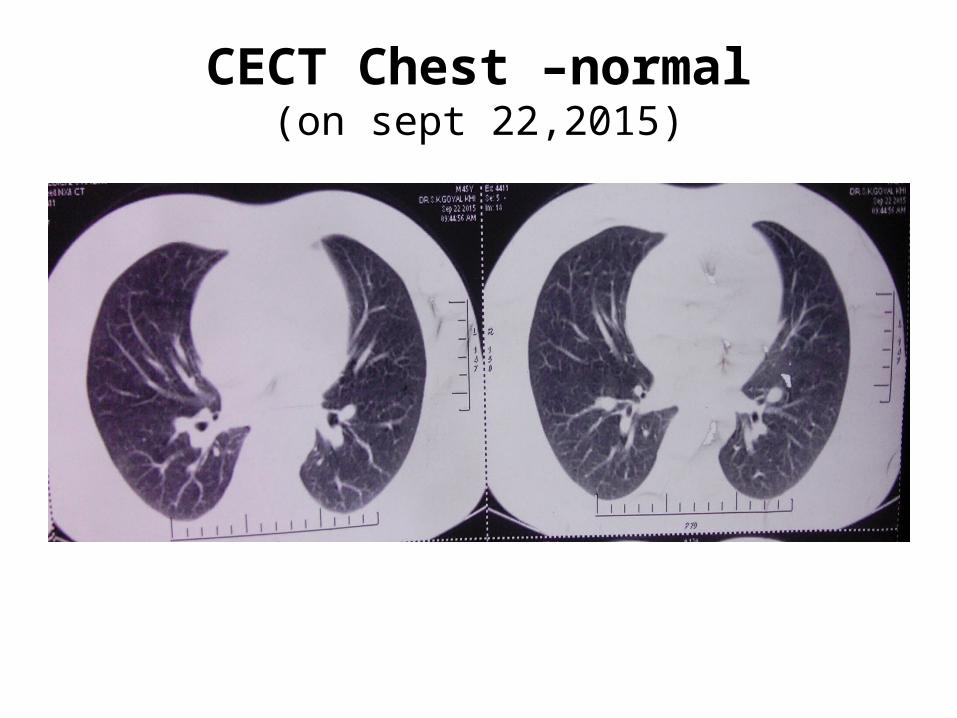
Chest radiographs showing bilateral multiple patchy air space hazy opacities in bilateral lung zones
PA View (MAY 222016) AP View (MAY 272016)
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
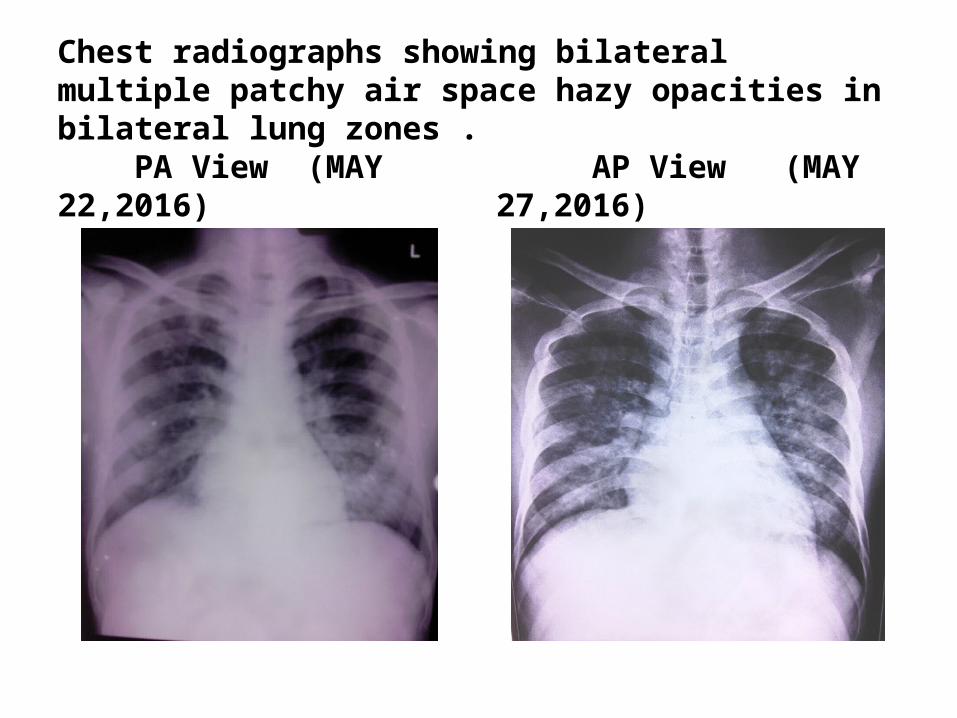
HRCT (Axial and Coronal) is showing multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and bilateral pleural effusion ( on May 302016)
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
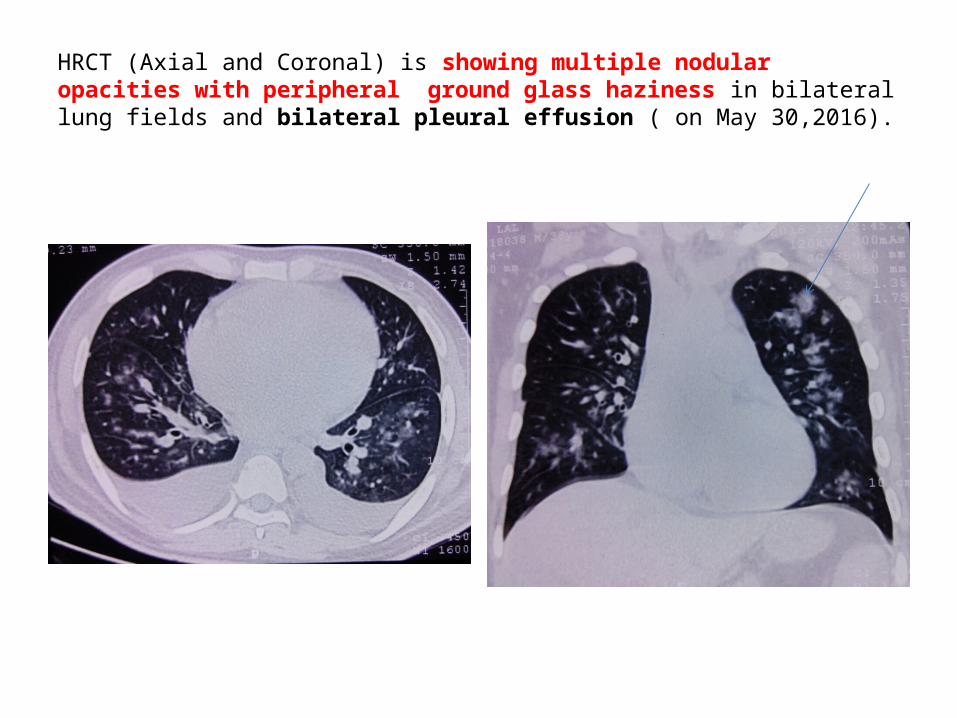
CECT chest is showing sub-centimetric mediastinal lymph nodes
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
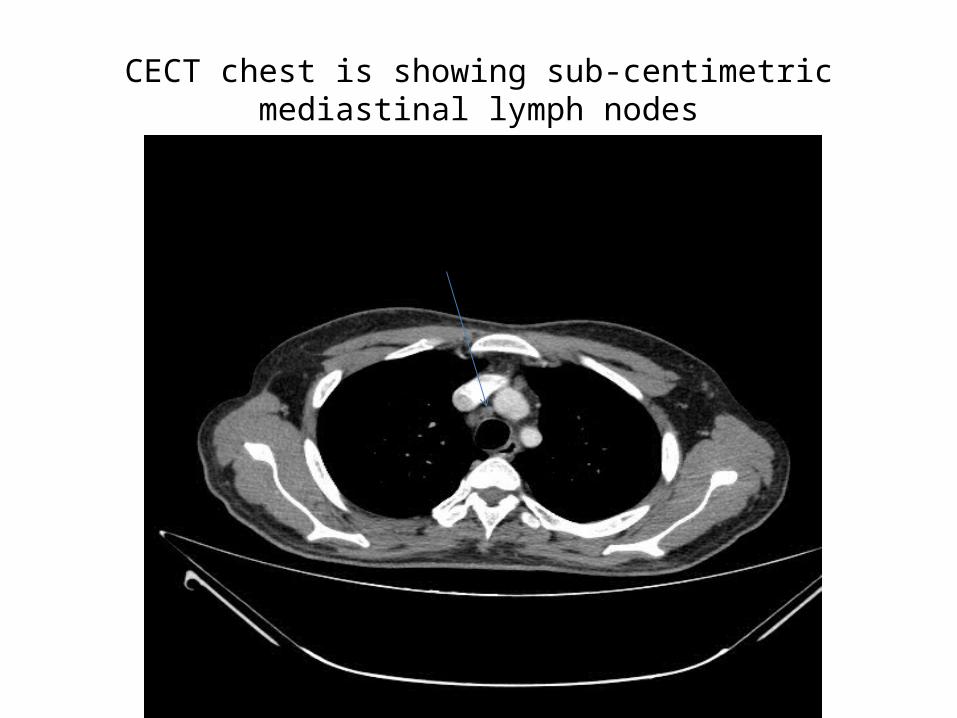
CECT abdomen revealed mild hepatosplenomegalyThere was no evidence of abdominal lymphadenopathy and any mass lesion
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
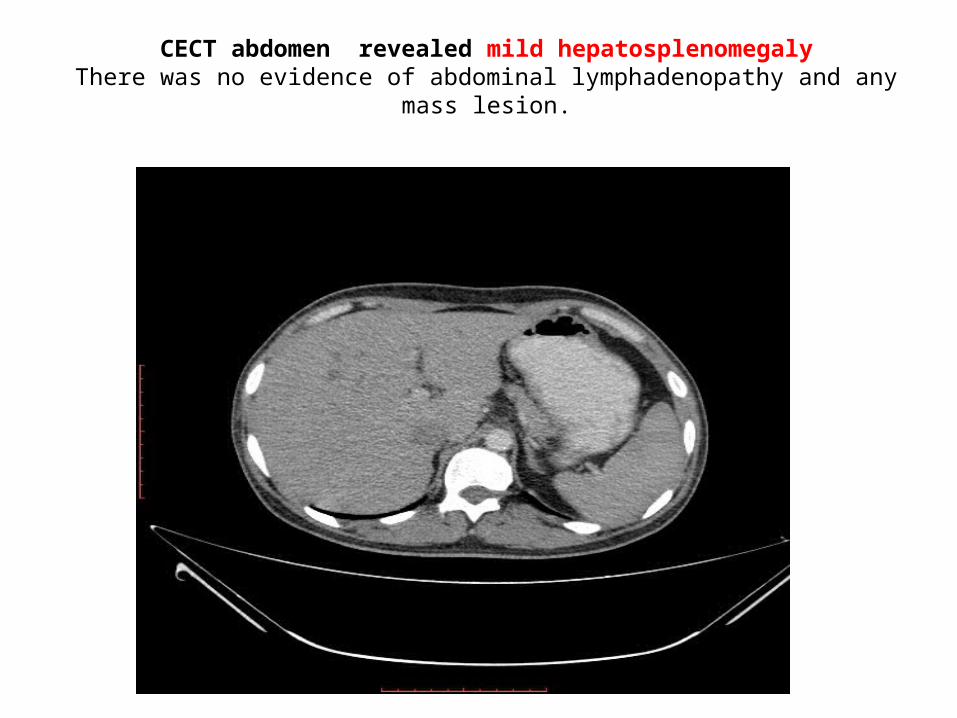
Differential diagnosis of nodules with ground glass pattern with eosinophilia
bull Eosinophilic lung diseases -Simple pulmonary eosinophilia -Idiopathic hypereosinophilic syndrome -Acute eosinophilic pneumonia -Chronic eosinophilic pneumonia -Churg-strauss syndrome -Eosinophilic drug reactionbull Sarcoidosisbull Hypersensitivity pneumonitis
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
Hypersensitivity pneumonitis
POINTS IN FAVOUR
Patchy ground glass opacities
POINTS AGAINST
bull Absence of centrilobular nodules
bull Absence of areas of air trapping
bull Absence of fibrosis
Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber

Chronic eosinophilic pneumonia
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-Involvement of other organs
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
SARCOIDOSIS
bull POINTS IN FAVOUR
-Patchy ground glass opacities
bull POINTS AGAINST
-No lymphadenopathy-Distribution of nodules
not perilymphatic
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
TUMOURS ASSOCIATED
bull CECT Chest and Abdomen are showing no evidence of bulky lymphadenopathy or any mass lesion so possibility of tumour associated pathology is less likely
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
Hypereosinophilic syndrome
POINTS IN FAVOUR bull Patchy ground glass
opacitiesbull Peripheral middle and
upper lobe predominance
bull Involvment of other organs
bull POINTS AGAINSTbull NONE
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Hypereosinophilic syndromebull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Chronic eosinophilic leukemia bull Tumor associated-Adenocarcinomas Squamous carcinomas Large cell lung carcinomas bull Other MPNMDS associated with eosinophiliabull Infiltrative cardiomyopathy bull Chronic Constrictive cardiomyopathy
DIFFERENTIALS DIAGNOSIS
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
Cardiology discussion
Dr Sohan k SharmaAssistant Prof
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
Next investigations
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
2D ECHO on done 21 sept 2105 showing normal 2D echo and Doppler study
Normal apical 4 chamber
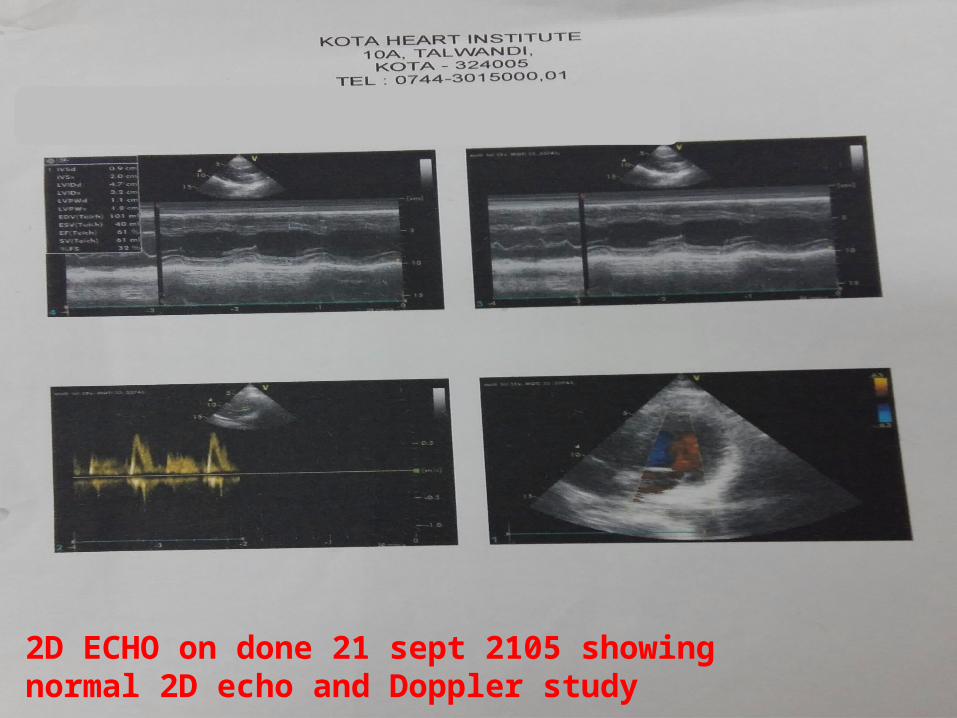
Normal apical 4 chamber
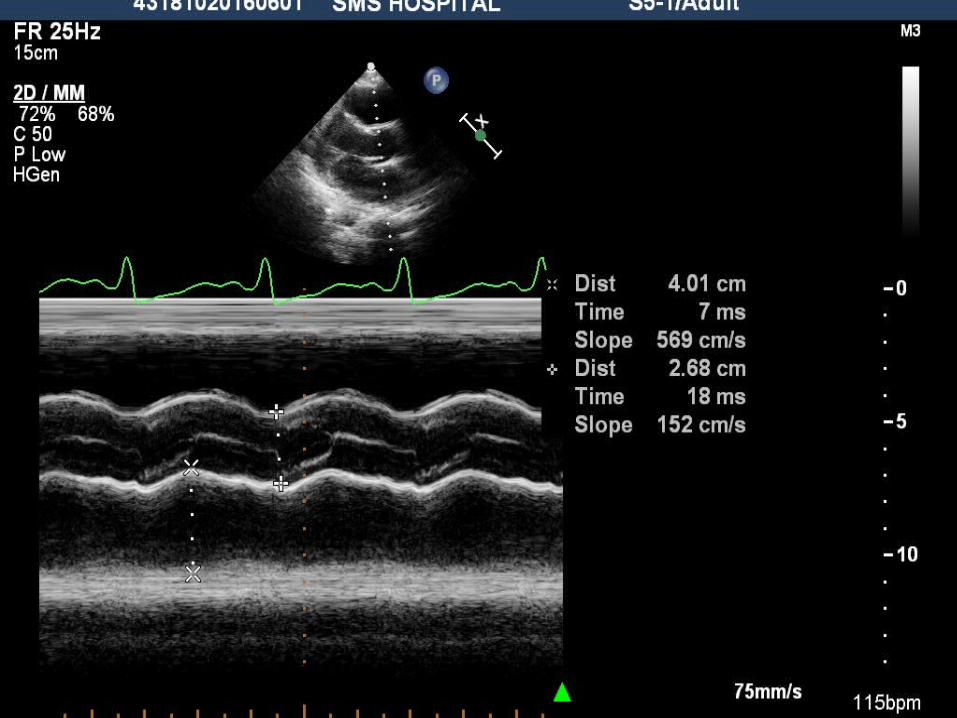
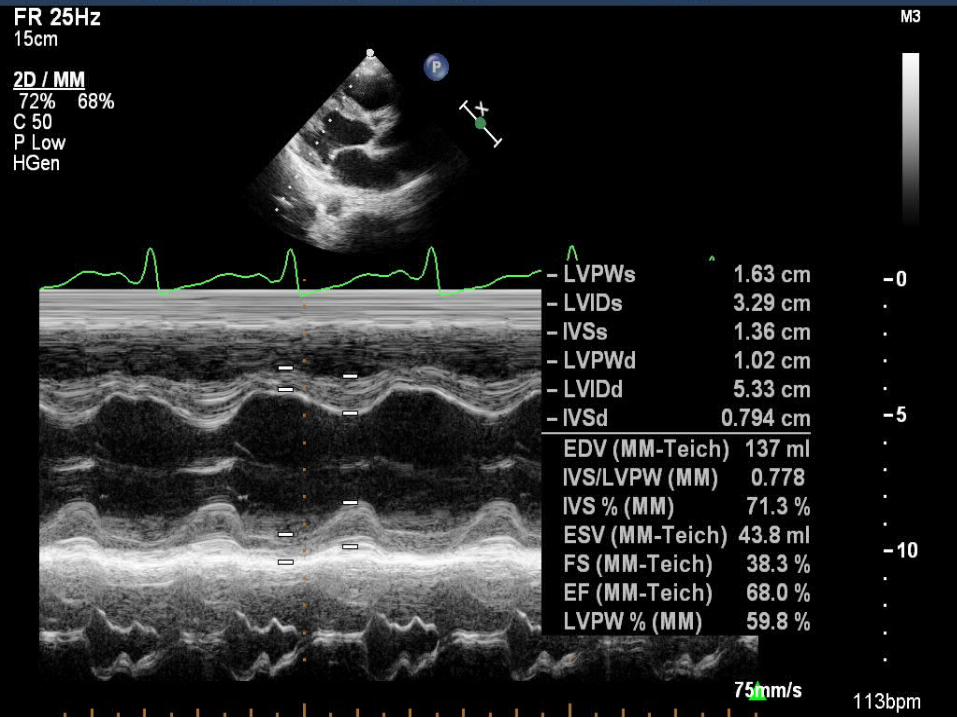
Restrictive physiology
Point in favorbull LV size and systolic function
preserved bull Biventricular apices obliterated bull Bi-atrial enlargement bull AV valves incompetencebull EgtgtA EA ratio (25) bull Medial ersquo lt 39 cms bull Respiratory variation of mitral E
velocity lt 10
Point against
bull EA ratio gt2bull PAH absent bull Pericardium can be normal in 10-
15bull ECHO has limited value in cases of
non-calcified pericardium and in presence of severe myocardial disease and preload dependence
bull Next investigations
bull Cardiac CATH study
LV Pressure tracing
LVEDP=22mmHg
RV pressure tracing
RVEDP=8mmHg
RVSP=37mmHg
RVEDPRVSP=lt13
RA Pressure tracing
PA pressure tracing
Normal LV angiogram

Restrictive physiology
Point in favorbull LV size and systolic function
preserved bull Biventricular apices obliterated bull Bi-atrial enlargement bull AV valves incompetencebull EgtgtA EA ratio (25) bull Medial ersquo lt 39 cms bull Respiratory variation of mitral E
velocity lt 10
Point against
bull EA ratio gt2bull PAH absent bull Pericardium can be normal in 10-
15bull ECHO has limited value in cases of
non-calcified pericardium and in presence of severe myocardial disease and preload dependence
bull Next investigations
bull Cardiac CATH study
LV Pressure tracing
LVEDP=22mmHg
RV pressure tracing
RVEDP=8mmHg
RVSP=37mmHg
RVEDPRVSP=lt13
RA Pressure tracing
PA pressure tracing
Normal LV angiogram

bull Next investigations
bull Cardiac CATH study
LV Pressure tracing
LVEDP=22mmHg
RV pressure tracing
RVEDP=8mmHg
RVSP=37mmHg
RVEDPRVSP=lt13
RA Pressure tracing
PA pressure tracing
Normal LV angiogram
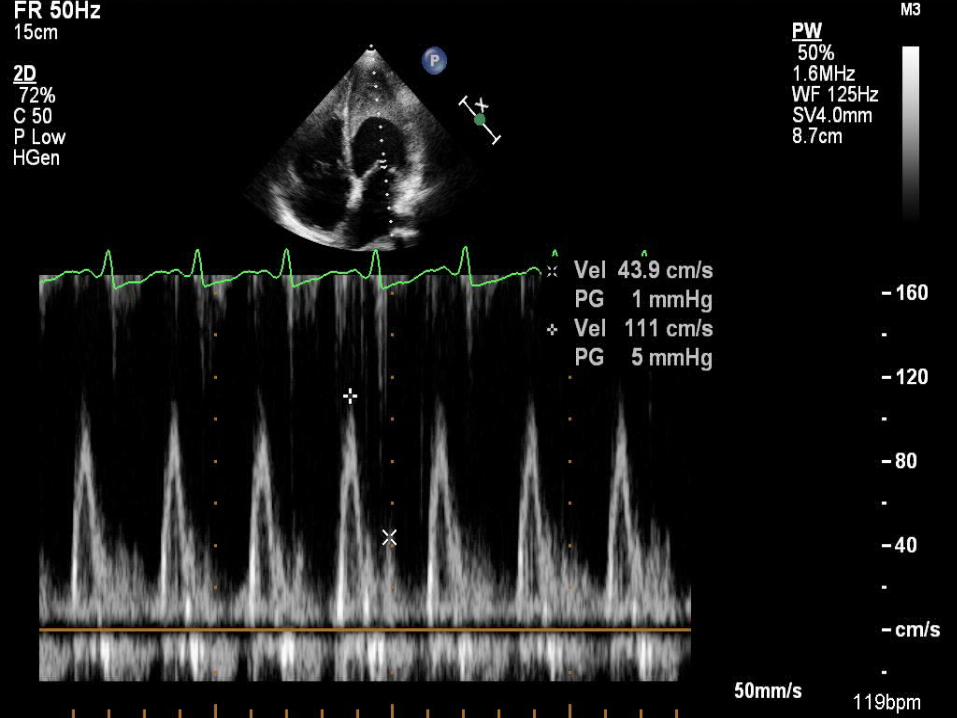
bull Cardiac CATH study
LV Pressure tracing
LVEDP=22mmHg
RV pressure tracing
RVEDP=8mmHg
RVSP=37mmHg
RVEDPRVSP=lt13
RA Pressure tracing
PA pressure tracing
Normal LV angiogram
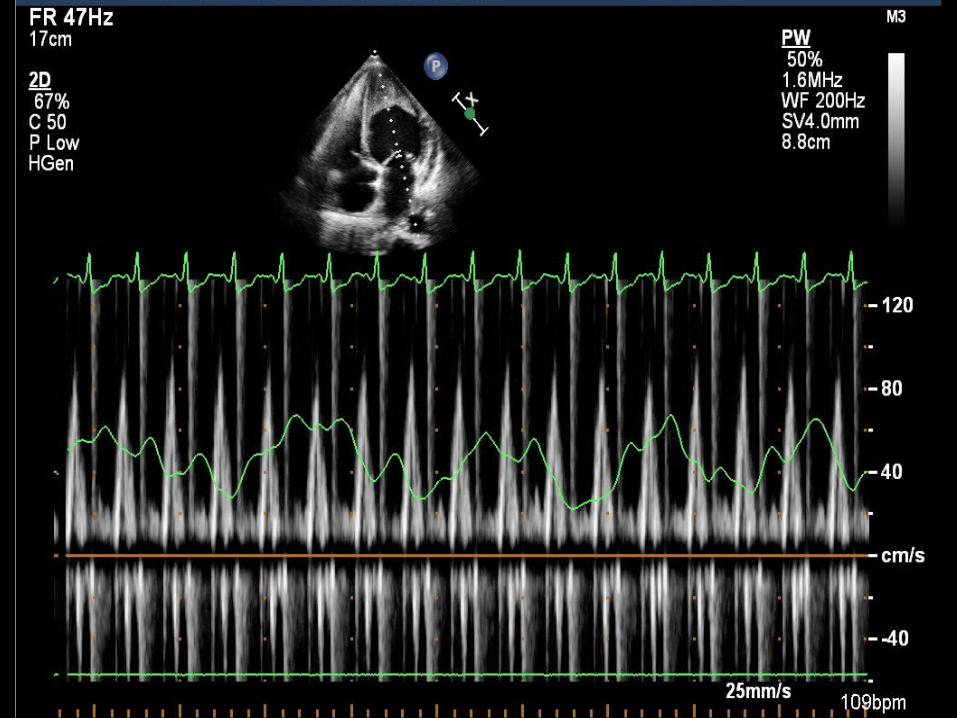
LV Pressure tracing
LVEDP=22mmHg
RV pressure tracing
RVEDP=8mmHg
RVSP=37mmHg
RVEDPRVSP=lt13
RA Pressure tracing
PA pressure tracing
Normal LV angiogram

RV pressure tracing
RVEDP=8mmHg
RVSP=37mmHg
RVEDPRVSP=lt13
RA Pressure tracing
PA pressure tracing
Normal LV angiogram
RA Pressure tracing
PA pressure tracing
Normal LV angiogram
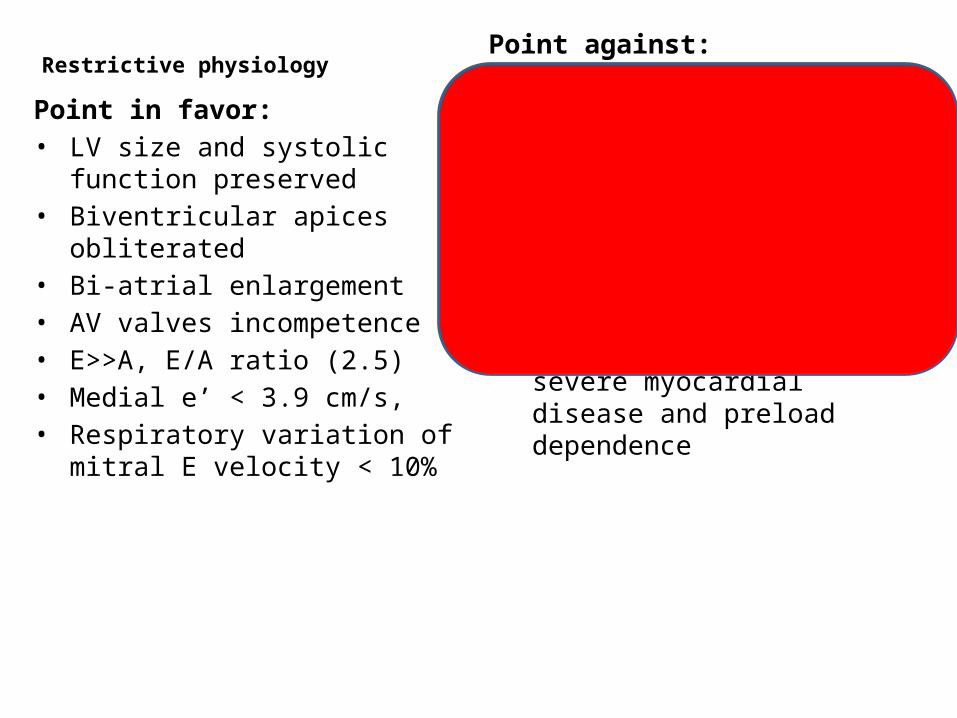
PA pressure tracing
Normal LV angiogram
Normal LV angiogram
LV angiogram

RV angiogram

CATH study analysis
Restrictive physiology bull LVEDP-RVEDP=16bull RVEDPRVSP=021bull BL ventricular apical
obliteration
CCPbull PASP= 41 bull PA pressure can be explain by
biventricular involvement
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Etiological diagnosis
Infiltrative cardiomyopathy
Endomyocardial biopsy
bull Endomyocardial biopsy was done and sample sent for histopathological evaluation
bull Cardiac MRI
Radiological discussion
Dr Sachin Lamba ( 3rd year Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Bright blood 2 chamber cine MRI is showing left ventricular apical hypointensity with left atrial dilatation
Bright blood 4 chamber cine MRI is showing left ventricular apical hypointensity with bi-atrial dilatation
Early post contrast MR images are showing subendocardial enhancement in nonvascular distribution (straight arrows) and a large left ventricular apical hypointensity ( curved arrows)
Delayed post contrast MR images are showing subendocardial enhancement in a nonvascular distribution ( straight arrows) as well as a large left ventricular apical hypointensity which did not take contrast proving it to be thrombus ( block arrows)Additionally wash out of contrast from normal myocardium (curved arrows) can be noted
Differential diagnosis of delayed contrast enhancement at cardiac MR imaging by location
Amyloidosis
bull POINTS IN FAVOUR -Subendocardial
enhancement is common
bull POINTS AGAINST -Subendocardial
enhancement is not global -Presence of intra -
ventricular thrombus
Endomyocardial fibrosisLoefflers endocarditis
bull POINTS IN FAVOUR-Subendocardial
enhancement is not global
-Presence of intra -ventricular thrombus
bull POINTS AGAINST-None
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP
Etiological diagnosis
Infiltrative cardiomyopathy
bull EMFbull Lofflers endocarditis
Endomyocardial fibrosis(MF) Point in favorbull More common in tropical country countries(India and Brazil)bull Associated with restrictive physiology with ventricular apical
obliteration bull Biventricular involvement present in 75 cases
Point againstbull Insidious onset and gradual progression bull Hypereosinophilia is uncommon bull Ecg- atrial fibrillation right axis deviation is more common bull Not associated with systemic illness
Lofflers endocarditisPoint in favorbull Predominantly in malebull Onset is common between second ndash fourth decade bull Onset is acute bull More aggressive coursebull Commonly present with fever cough and weight lossbull Associated with severe hypereosinophilliabull Associated with restrictive physiology with ventricular apical
obliteration bull Bi-ventricular involvement -100bull Ecg ndashsinus rhythm ST depressionbull Associated with systemic illness with multi-organ involvement Point againstbull More common in temperate countries
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Etiological diagnosis
bull EMFbull Lofflers endocarditis
Diagnosis
bull Lofflers endocarditis with systemic hyper- eosinophilia
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Tumor associated-Adenocarcinomas bull Squamous carcinomasbull Large cell lung carcinomas bull Chronic Constrictive cardiomyopathybull Infiltrative cardiomyopathy bull Hypereosinophilic syndromebull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Chronic eosinophilic leukemia bull Other MPNMDS associated with eosinophilia
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysisbull BAL and lung biopsy
Pathological Discussion
Dr Neetu AgrawalSenior Demonstrator
Under guidance
Dr Anita HarshAssociate Professor
Department of Pathology
COMPLETE BLOOD COUNTSRBC 332 X 106 μlHGB 96 gdlHCT 306 MCV 922 fLMCH 289 pgMCHC 314 gdlWBC 2165 X 103 microlDLC Neutrophils - 18 Lymphocytes - 15 Monocytes - 02 Eosinophils - 65 Basophils - 00PLT 45 x 103 microlAbsolute Eosinophil Count- 14 x 103microl
Peripheral blood film shows predominantly normocytic normochromic RBCs with few macrocytes Eosinophilic leukocytosis showing hypersegmentation amp cytoplasmic vacoulization Platelets are reduced(40x Leishman stain)
Bone marrow aspirates markedly diluted with peripheral blood showing eosinophils
Bone marrow aspirate showing eosinophilic myelocyte band cell amp one hypersegmented
Eosinophil with cytoplasmic vacoulization
Trephine marrow biopsy showing bony trabeculae amp hypercellular hematopoietic tissue
(10xHampE stain)
Bone marrow biopsy showing myeloid hyperplasia with increased eosinophils and eosinophilic precursors few blasts with open nuclear chromatin amp
prominent nucleoli normoblastic erythropoiesis and megakaryocytes (40xHampE stain)
Bone marrow biopsy shows predominantly eosinophilic precursors and eosinophils with granular pink red cytoplasm (40x HampE stain)
Bone marrow biopsy showing different stages of eosinophil maturation with
hypersegmented and ring eosinophil (100x HampE stain)
Bone marrow biopsy showing focal increased reticulin with few course fibres grade 2 ( 4x reticulin stain)
bull PBF ndash Eosinophilic leukocytosisbull BM Aspiration ndash Diluted bull BMB - Myeloid hyperplasia with increased
Eosinophil and its precursors and abnormal forms
bull No increase in blastsbull Increased fibrosis (MF2)
The WHO defined Myeloid malignancies associated with clonal eosinophilia ruled out by CBC PBF amp BM examination are ndash AML with inv 16 ndash no blast in PBF Blasts ˂ 20 in BM Polycythemia vera - Hb lt 165 gdl HCT lt 49 no trilineage hyperplasia on BMB Essential thrombocythemia ndash PLT decreased no increase in megakaryocytes on BMB Primary Myelofibrosis ndash No megakaryocytic proliferation and atypia CMML ndash Monocytosis absent Monocytes lt 10 of WBC count aCML - neutrophils and their precursors are not increased Systemic Mastocytosis ndash Mast cells are not seen
Myeloid neoplasms associated with eosinophilia and rearrangement
of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
Chronic eosinophilic leukemia NOS
Idiopathic Hypereosinophilic syndrome
DIFFERENTIAL DIAGNOSIS 1 Myeloid neoplasms associated with eosinophilia and rearrangement of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
2 Chronic eosinophilic leukemia NOS
3 Idiopathic Hypereosinophilic syndrome
These disorders can not be differentiated on the basis of morphology Molecularcytogenetic analysis was suggested for further categorization
Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
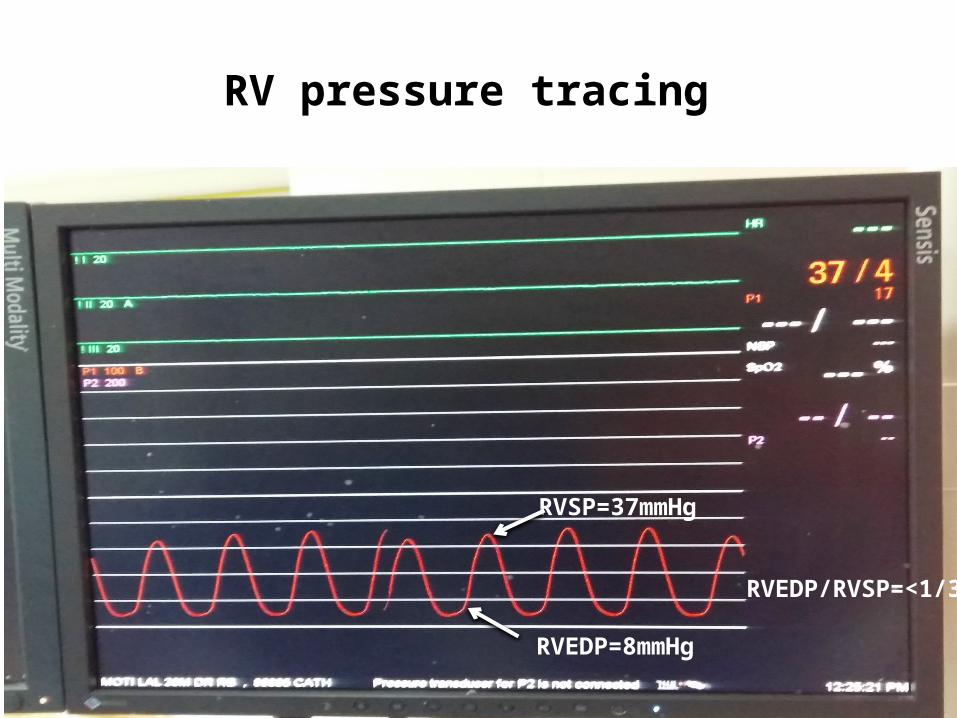
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Etiological diagnosis
Infiltrative cardiomyopathy
Endomyocardial biopsy
bull Endomyocardial biopsy was done and sample sent for histopathological evaluation
bull Cardiac MRI
Radiological discussion
Dr Sachin Lamba ( 3rd year Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Bright blood 2 chamber cine MRI is showing left ventricular apical hypointensity with left atrial dilatation
Bright blood 4 chamber cine MRI is showing left ventricular apical hypointensity with bi-atrial dilatation
Early post contrast MR images are showing subendocardial enhancement in nonvascular distribution (straight arrows) and a large left ventricular apical hypointensity ( curved arrows)
Delayed post contrast MR images are showing subendocardial enhancement in a nonvascular distribution ( straight arrows) as well as a large left ventricular apical hypointensity which did not take contrast proving it to be thrombus ( block arrows)Additionally wash out of contrast from normal myocardium (curved arrows) can be noted
Differential diagnosis of delayed contrast enhancement at cardiac MR imaging by location
Amyloidosis
bull POINTS IN FAVOUR -Subendocardial
enhancement is common
bull POINTS AGAINST -Subendocardial
enhancement is not global -Presence of intra -
ventricular thrombus
Endomyocardial fibrosisLoefflers endocarditis
bull POINTS IN FAVOUR-Subendocardial
enhancement is not global
-Presence of intra -ventricular thrombus
bull POINTS AGAINST-None
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP
Etiological diagnosis
Infiltrative cardiomyopathy
bull EMFbull Lofflers endocarditis
Endomyocardial fibrosis(MF) Point in favorbull More common in tropical country countries(India and Brazil)bull Associated with restrictive physiology with ventricular apical
obliteration bull Biventricular involvement present in 75 cases
Point againstbull Insidious onset and gradual progression bull Hypereosinophilia is uncommon bull Ecg- atrial fibrillation right axis deviation is more common bull Not associated with systemic illness
Lofflers endocarditisPoint in favorbull Predominantly in malebull Onset is common between second ndash fourth decade bull Onset is acute bull More aggressive coursebull Commonly present with fever cough and weight lossbull Associated with severe hypereosinophilliabull Associated with restrictive physiology with ventricular apical
obliteration bull Bi-ventricular involvement -100bull Ecg ndashsinus rhythm ST depressionbull Associated with systemic illness with multi-organ involvement Point againstbull More common in temperate countries
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Etiological diagnosis
bull EMFbull Lofflers endocarditis
Diagnosis
bull Lofflers endocarditis with systemic hyper- eosinophilia
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Tumor associated-Adenocarcinomas bull Squamous carcinomasbull Large cell lung carcinomas bull Chronic Constrictive cardiomyopathybull Infiltrative cardiomyopathy bull Hypereosinophilic syndromebull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Chronic eosinophilic leukemia bull Other MPNMDS associated with eosinophilia
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysisbull BAL and lung biopsy
Pathological Discussion
Dr Neetu AgrawalSenior Demonstrator
Under guidance
Dr Anita HarshAssociate Professor
Department of Pathology
COMPLETE BLOOD COUNTSRBC 332 X 106 μlHGB 96 gdlHCT 306 MCV 922 fLMCH 289 pgMCHC 314 gdlWBC 2165 X 103 microlDLC Neutrophils - 18 Lymphocytes - 15 Monocytes - 02 Eosinophils - 65 Basophils - 00PLT 45 x 103 microlAbsolute Eosinophil Count- 14 x 103microl
Peripheral blood film shows predominantly normocytic normochromic RBCs with few macrocytes Eosinophilic leukocytosis showing hypersegmentation amp cytoplasmic vacoulization Platelets are reduced(40x Leishman stain)
Bone marrow aspirates markedly diluted with peripheral blood showing eosinophils
Bone marrow aspirate showing eosinophilic myelocyte band cell amp one hypersegmented
Eosinophil with cytoplasmic vacoulization
Trephine marrow biopsy showing bony trabeculae amp hypercellular hematopoietic tissue
(10xHampE stain)
Bone marrow biopsy showing myeloid hyperplasia with increased eosinophils and eosinophilic precursors few blasts with open nuclear chromatin amp
prominent nucleoli normoblastic erythropoiesis and megakaryocytes (40xHampE stain)
Bone marrow biopsy shows predominantly eosinophilic precursors and eosinophils with granular pink red cytoplasm (40x HampE stain)
Bone marrow biopsy showing different stages of eosinophil maturation with
hypersegmented and ring eosinophil (100x HampE stain)
Bone marrow biopsy showing focal increased reticulin with few course fibres grade 2 ( 4x reticulin stain)
bull PBF ndash Eosinophilic leukocytosisbull BM Aspiration ndash Diluted bull BMB - Myeloid hyperplasia with increased
Eosinophil and its precursors and abnormal forms
bull No increase in blastsbull Increased fibrosis (MF2)
The WHO defined Myeloid malignancies associated with clonal eosinophilia ruled out by CBC PBF amp BM examination are ndash AML with inv 16 ndash no blast in PBF Blasts ˂ 20 in BM Polycythemia vera - Hb lt 165 gdl HCT lt 49 no trilineage hyperplasia on BMB Essential thrombocythemia ndash PLT decreased no increase in megakaryocytes on BMB Primary Myelofibrosis ndash No megakaryocytic proliferation and atypia CMML ndash Monocytosis absent Monocytes lt 10 of WBC count aCML - neutrophils and their precursors are not increased Systemic Mastocytosis ndash Mast cells are not seen
Myeloid neoplasms associated with eosinophilia and rearrangement
of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
Chronic eosinophilic leukemia NOS
Idiopathic Hypereosinophilic syndrome
DIFFERENTIAL DIAGNOSIS 1 Myeloid neoplasms associated with eosinophilia and rearrangement of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
2 Chronic eosinophilic leukemia NOS
3 Idiopathic Hypereosinophilic syndrome
These disorders can not be differentiated on the basis of morphology Molecularcytogenetic analysis was suggested for further categorization
Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
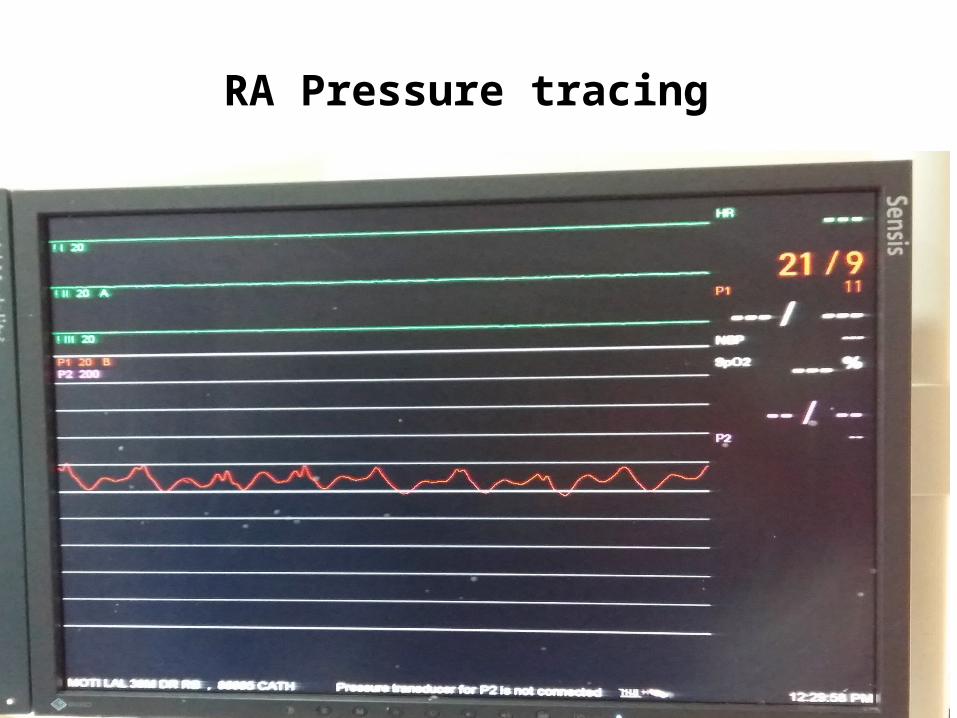
Endomyocardial biopsy
bull Endomyocardial biopsy was done and sample sent for histopathological evaluation
bull Cardiac MRI
Radiological discussion
Dr Sachin Lamba ( 3rd year Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Bright blood 2 chamber cine MRI is showing left ventricular apical hypointensity with left atrial dilatation
Bright blood 4 chamber cine MRI is showing left ventricular apical hypointensity with bi-atrial dilatation
Early post contrast MR images are showing subendocardial enhancement in nonvascular distribution (straight arrows) and a large left ventricular apical hypointensity ( curved arrows)
Delayed post contrast MR images are showing subendocardial enhancement in a nonvascular distribution ( straight arrows) as well as a large left ventricular apical hypointensity which did not take contrast proving it to be thrombus ( block arrows)Additionally wash out of contrast from normal myocardium (curved arrows) can be noted
Differential diagnosis of delayed contrast enhancement at cardiac MR imaging by location
Amyloidosis
bull POINTS IN FAVOUR -Subendocardial
enhancement is common
bull POINTS AGAINST -Subendocardial
enhancement is not global -Presence of intra -
ventricular thrombus
Endomyocardial fibrosisLoefflers endocarditis
bull POINTS IN FAVOUR-Subendocardial
enhancement is not global
-Presence of intra -ventricular thrombus
bull POINTS AGAINST-None
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP
Etiological diagnosis
Infiltrative cardiomyopathy
bull EMFbull Lofflers endocarditis
Endomyocardial fibrosis(MF) Point in favorbull More common in tropical country countries(India and Brazil)bull Associated with restrictive physiology with ventricular apical
obliteration bull Biventricular involvement present in 75 cases
Point againstbull Insidious onset and gradual progression bull Hypereosinophilia is uncommon bull Ecg- atrial fibrillation right axis deviation is more common bull Not associated with systemic illness
Lofflers endocarditisPoint in favorbull Predominantly in malebull Onset is common between second ndash fourth decade bull Onset is acute bull More aggressive coursebull Commonly present with fever cough and weight lossbull Associated with severe hypereosinophilliabull Associated with restrictive physiology with ventricular apical
obliteration bull Bi-ventricular involvement -100bull Ecg ndashsinus rhythm ST depressionbull Associated with systemic illness with multi-organ involvement Point againstbull More common in temperate countries
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Etiological diagnosis
bull EMFbull Lofflers endocarditis
Diagnosis
bull Lofflers endocarditis with systemic hyper- eosinophilia
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Tumor associated-Adenocarcinomas bull Squamous carcinomasbull Large cell lung carcinomas bull Chronic Constrictive cardiomyopathybull Infiltrative cardiomyopathy bull Hypereosinophilic syndromebull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Chronic eosinophilic leukemia bull Other MPNMDS associated with eosinophilia
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysisbull BAL and lung biopsy
Pathological Discussion
Dr Neetu AgrawalSenior Demonstrator
Under guidance
Dr Anita HarshAssociate Professor
Department of Pathology
COMPLETE BLOOD COUNTSRBC 332 X 106 μlHGB 96 gdlHCT 306 MCV 922 fLMCH 289 pgMCHC 314 gdlWBC 2165 X 103 microlDLC Neutrophils - 18 Lymphocytes - 15 Monocytes - 02 Eosinophils - 65 Basophils - 00PLT 45 x 103 microlAbsolute Eosinophil Count- 14 x 103microl
Peripheral blood film shows predominantly normocytic normochromic RBCs with few macrocytes Eosinophilic leukocytosis showing hypersegmentation amp cytoplasmic vacoulization Platelets are reduced(40x Leishman stain)
Bone marrow aspirates markedly diluted with peripheral blood showing eosinophils
Bone marrow aspirate showing eosinophilic myelocyte band cell amp one hypersegmented
Eosinophil with cytoplasmic vacoulization
Trephine marrow biopsy showing bony trabeculae amp hypercellular hematopoietic tissue
(10xHampE stain)
Bone marrow biopsy showing myeloid hyperplasia with increased eosinophils and eosinophilic precursors few blasts with open nuclear chromatin amp
prominent nucleoli normoblastic erythropoiesis and megakaryocytes (40xHampE stain)
Bone marrow biopsy shows predominantly eosinophilic precursors and eosinophils with granular pink red cytoplasm (40x HampE stain)
Bone marrow biopsy showing different stages of eosinophil maturation with
hypersegmented and ring eosinophil (100x HampE stain)
Bone marrow biopsy showing focal increased reticulin with few course fibres grade 2 ( 4x reticulin stain)
bull PBF ndash Eosinophilic leukocytosisbull BM Aspiration ndash Diluted bull BMB - Myeloid hyperplasia with increased
Eosinophil and its precursors and abnormal forms
bull No increase in blastsbull Increased fibrosis (MF2)
The WHO defined Myeloid malignancies associated with clonal eosinophilia ruled out by CBC PBF amp BM examination are ndash AML with inv 16 ndash no blast in PBF Blasts ˂ 20 in BM Polycythemia vera - Hb lt 165 gdl HCT lt 49 no trilineage hyperplasia on BMB Essential thrombocythemia ndash PLT decreased no increase in megakaryocytes on BMB Primary Myelofibrosis ndash No megakaryocytic proliferation and atypia CMML ndash Monocytosis absent Monocytes lt 10 of WBC count aCML - neutrophils and their precursors are not increased Systemic Mastocytosis ndash Mast cells are not seen
Myeloid neoplasms associated with eosinophilia and rearrangement
of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
Chronic eosinophilic leukemia NOS
Idiopathic Hypereosinophilic syndrome
DIFFERENTIAL DIAGNOSIS 1 Myeloid neoplasms associated with eosinophilia and rearrangement of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
2 Chronic eosinophilic leukemia NOS
3 Idiopathic Hypereosinophilic syndrome
These disorders can not be differentiated on the basis of morphology Molecularcytogenetic analysis was suggested for further categorization
Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
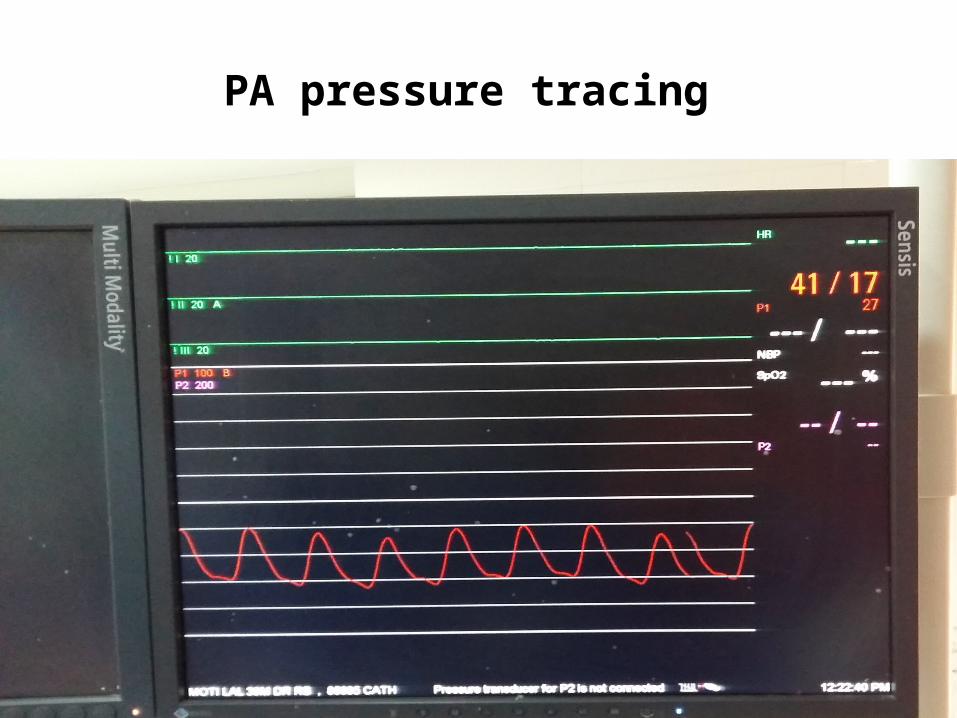
bull Cardiac MRI
Radiological discussion
Dr Sachin Lamba ( 3rd year Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Bright blood 2 chamber cine MRI is showing left ventricular apical hypointensity with left atrial dilatation
Bright blood 4 chamber cine MRI is showing left ventricular apical hypointensity with bi-atrial dilatation
Early post contrast MR images are showing subendocardial enhancement in nonvascular distribution (straight arrows) and a large left ventricular apical hypointensity ( curved arrows)
Delayed post contrast MR images are showing subendocardial enhancement in a nonvascular distribution ( straight arrows) as well as a large left ventricular apical hypointensity which did not take contrast proving it to be thrombus ( block arrows)Additionally wash out of contrast from normal myocardium (curved arrows) can be noted
Differential diagnosis of delayed contrast enhancement at cardiac MR imaging by location
Amyloidosis
bull POINTS IN FAVOUR -Subendocardial
enhancement is common
bull POINTS AGAINST -Subendocardial
enhancement is not global -Presence of intra -
ventricular thrombus
Endomyocardial fibrosisLoefflers endocarditis
bull POINTS IN FAVOUR-Subendocardial
enhancement is not global
-Presence of intra -ventricular thrombus
bull POINTS AGAINST-None
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP
Etiological diagnosis
Infiltrative cardiomyopathy
bull EMFbull Lofflers endocarditis
Endomyocardial fibrosis(MF) Point in favorbull More common in tropical country countries(India and Brazil)bull Associated with restrictive physiology with ventricular apical
obliteration bull Biventricular involvement present in 75 cases
Point againstbull Insidious onset and gradual progression bull Hypereosinophilia is uncommon bull Ecg- atrial fibrillation right axis deviation is more common bull Not associated with systemic illness
Lofflers endocarditisPoint in favorbull Predominantly in malebull Onset is common between second ndash fourth decade bull Onset is acute bull More aggressive coursebull Commonly present with fever cough and weight lossbull Associated with severe hypereosinophilliabull Associated with restrictive physiology with ventricular apical
obliteration bull Bi-ventricular involvement -100bull Ecg ndashsinus rhythm ST depressionbull Associated with systemic illness with multi-organ involvement Point againstbull More common in temperate countries
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Etiological diagnosis
bull EMFbull Lofflers endocarditis
Diagnosis
bull Lofflers endocarditis with systemic hyper- eosinophilia
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Tumor associated-Adenocarcinomas bull Squamous carcinomasbull Large cell lung carcinomas bull Chronic Constrictive cardiomyopathybull Infiltrative cardiomyopathy bull Hypereosinophilic syndromebull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Chronic eosinophilic leukemia bull Other MPNMDS associated with eosinophilia
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysisbull BAL and lung biopsy
Pathological Discussion
Dr Neetu AgrawalSenior Demonstrator
Under guidance
Dr Anita HarshAssociate Professor
Department of Pathology
COMPLETE BLOOD COUNTSRBC 332 X 106 μlHGB 96 gdlHCT 306 MCV 922 fLMCH 289 pgMCHC 314 gdlWBC 2165 X 103 microlDLC Neutrophils - 18 Lymphocytes - 15 Monocytes - 02 Eosinophils - 65 Basophils - 00PLT 45 x 103 microlAbsolute Eosinophil Count- 14 x 103microl
Peripheral blood film shows predominantly normocytic normochromic RBCs with few macrocytes Eosinophilic leukocytosis showing hypersegmentation amp cytoplasmic vacoulization Platelets are reduced(40x Leishman stain)
Bone marrow aspirates markedly diluted with peripheral blood showing eosinophils
Bone marrow aspirate showing eosinophilic myelocyte band cell amp one hypersegmented
Eosinophil with cytoplasmic vacoulization
Trephine marrow biopsy showing bony trabeculae amp hypercellular hematopoietic tissue
(10xHampE stain)
Bone marrow biopsy showing myeloid hyperplasia with increased eosinophils and eosinophilic precursors few blasts with open nuclear chromatin amp
prominent nucleoli normoblastic erythropoiesis and megakaryocytes (40xHampE stain)
Bone marrow biopsy shows predominantly eosinophilic precursors and eosinophils with granular pink red cytoplasm (40x HampE stain)
Bone marrow biopsy showing different stages of eosinophil maturation with
hypersegmented and ring eosinophil (100x HampE stain)
Bone marrow biopsy showing focal increased reticulin with few course fibres grade 2 ( 4x reticulin stain)
bull PBF ndash Eosinophilic leukocytosisbull BM Aspiration ndash Diluted bull BMB - Myeloid hyperplasia with increased
Eosinophil and its precursors and abnormal forms
bull No increase in blastsbull Increased fibrosis (MF2)
The WHO defined Myeloid malignancies associated with clonal eosinophilia ruled out by CBC PBF amp BM examination are ndash AML with inv 16 ndash no blast in PBF Blasts ˂ 20 in BM Polycythemia vera - Hb lt 165 gdl HCT lt 49 no trilineage hyperplasia on BMB Essential thrombocythemia ndash PLT decreased no increase in megakaryocytes on BMB Primary Myelofibrosis ndash No megakaryocytic proliferation and atypia CMML ndash Monocytosis absent Monocytes lt 10 of WBC count aCML - neutrophils and their precursors are not increased Systemic Mastocytosis ndash Mast cells are not seen
Myeloid neoplasms associated with eosinophilia and rearrangement
of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
Chronic eosinophilic leukemia NOS
Idiopathic Hypereosinophilic syndrome
DIFFERENTIAL DIAGNOSIS 1 Myeloid neoplasms associated with eosinophilia and rearrangement of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
2 Chronic eosinophilic leukemia NOS
3 Idiopathic Hypereosinophilic syndrome
These disorders can not be differentiated on the basis of morphology Molecularcytogenetic analysis was suggested for further categorization
Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
Radiological discussion
Dr Sachin Lamba ( 3rd year Resident)
Guided byndash Dr Rajkumar Yadav Sir Assistant Professor
DEPARTMENT OF RADIODIAGNOSIS AND MODERN IMAGING
Bright blood 2 chamber cine MRI is showing left ventricular apical hypointensity with left atrial dilatation
Bright blood 4 chamber cine MRI is showing left ventricular apical hypointensity with bi-atrial dilatation
Early post contrast MR images are showing subendocardial enhancement in nonvascular distribution (straight arrows) and a large left ventricular apical hypointensity ( curved arrows)
Delayed post contrast MR images are showing subendocardial enhancement in a nonvascular distribution ( straight arrows) as well as a large left ventricular apical hypointensity which did not take contrast proving it to be thrombus ( block arrows)Additionally wash out of contrast from normal myocardium (curved arrows) can be noted
Differential diagnosis of delayed contrast enhancement at cardiac MR imaging by location
Amyloidosis
bull POINTS IN FAVOUR -Subendocardial
enhancement is common
bull POINTS AGAINST -Subendocardial
enhancement is not global -Presence of intra -
ventricular thrombus
Endomyocardial fibrosisLoefflers endocarditis
bull POINTS IN FAVOUR-Subendocardial
enhancement is not global
-Presence of intra -ventricular thrombus
bull POINTS AGAINST-None
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP
Etiological diagnosis
Infiltrative cardiomyopathy
bull EMFbull Lofflers endocarditis
Endomyocardial fibrosis(MF) Point in favorbull More common in tropical country countries(India and Brazil)bull Associated with restrictive physiology with ventricular apical
obliteration bull Biventricular involvement present in 75 cases
Point againstbull Insidious onset and gradual progression bull Hypereosinophilia is uncommon bull Ecg- atrial fibrillation right axis deviation is more common bull Not associated with systemic illness
Lofflers endocarditisPoint in favorbull Predominantly in malebull Onset is common between second ndash fourth decade bull Onset is acute bull More aggressive coursebull Commonly present with fever cough and weight lossbull Associated with severe hypereosinophilliabull Associated with restrictive physiology with ventricular apical
obliteration bull Bi-ventricular involvement -100bull Ecg ndashsinus rhythm ST depressionbull Associated with systemic illness with multi-organ involvement Point againstbull More common in temperate countries
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Etiological diagnosis
bull EMFbull Lofflers endocarditis
Diagnosis
bull Lofflers endocarditis with systemic hyper- eosinophilia
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Tumor associated-Adenocarcinomas bull Squamous carcinomasbull Large cell lung carcinomas bull Chronic Constrictive cardiomyopathybull Infiltrative cardiomyopathy bull Hypereosinophilic syndromebull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Chronic eosinophilic leukemia bull Other MPNMDS associated with eosinophilia
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysisbull BAL and lung biopsy
Pathological Discussion
Dr Neetu AgrawalSenior Demonstrator
Under guidance
Dr Anita HarshAssociate Professor
Department of Pathology
COMPLETE BLOOD COUNTSRBC 332 X 106 μlHGB 96 gdlHCT 306 MCV 922 fLMCH 289 pgMCHC 314 gdlWBC 2165 X 103 microlDLC Neutrophils - 18 Lymphocytes - 15 Monocytes - 02 Eosinophils - 65 Basophils - 00PLT 45 x 103 microlAbsolute Eosinophil Count- 14 x 103microl
Peripheral blood film shows predominantly normocytic normochromic RBCs with few macrocytes Eosinophilic leukocytosis showing hypersegmentation amp cytoplasmic vacoulization Platelets are reduced(40x Leishman stain)
Bone marrow aspirates markedly diluted with peripheral blood showing eosinophils
Bone marrow aspirate showing eosinophilic myelocyte band cell amp one hypersegmented
Eosinophil with cytoplasmic vacoulization
Trephine marrow biopsy showing bony trabeculae amp hypercellular hematopoietic tissue
(10xHampE stain)
Bone marrow biopsy showing myeloid hyperplasia with increased eosinophils and eosinophilic precursors few blasts with open nuclear chromatin amp
prominent nucleoli normoblastic erythropoiesis and megakaryocytes (40xHampE stain)
Bone marrow biopsy shows predominantly eosinophilic precursors and eosinophils with granular pink red cytoplasm (40x HampE stain)
Bone marrow biopsy showing different stages of eosinophil maturation with
hypersegmented and ring eosinophil (100x HampE stain)
Bone marrow biopsy showing focal increased reticulin with few course fibres grade 2 ( 4x reticulin stain)
bull PBF ndash Eosinophilic leukocytosisbull BM Aspiration ndash Diluted bull BMB - Myeloid hyperplasia with increased
Eosinophil and its precursors and abnormal forms
bull No increase in blastsbull Increased fibrosis (MF2)
The WHO defined Myeloid malignancies associated with clonal eosinophilia ruled out by CBC PBF amp BM examination are ndash AML with inv 16 ndash no blast in PBF Blasts ˂ 20 in BM Polycythemia vera - Hb lt 165 gdl HCT lt 49 no trilineage hyperplasia on BMB Essential thrombocythemia ndash PLT decreased no increase in megakaryocytes on BMB Primary Myelofibrosis ndash No megakaryocytic proliferation and atypia CMML ndash Monocytosis absent Monocytes lt 10 of WBC count aCML - neutrophils and their precursors are not increased Systemic Mastocytosis ndash Mast cells are not seen
Myeloid neoplasms associated with eosinophilia and rearrangement
of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
Chronic eosinophilic leukemia NOS
Idiopathic Hypereosinophilic syndrome
DIFFERENTIAL DIAGNOSIS 1 Myeloid neoplasms associated with eosinophilia and rearrangement of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
2 Chronic eosinophilic leukemia NOS
3 Idiopathic Hypereosinophilic syndrome
These disorders can not be differentiated on the basis of morphology Molecularcytogenetic analysis was suggested for further categorization
Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
Bright blood 2 chamber cine MRI is showing left ventricular apical hypointensity with left atrial dilatation
Bright blood 4 chamber cine MRI is showing left ventricular apical hypointensity with bi-atrial dilatation
Early post contrast MR images are showing subendocardial enhancement in nonvascular distribution (straight arrows) and a large left ventricular apical hypointensity ( curved arrows)
Delayed post contrast MR images are showing subendocardial enhancement in a nonvascular distribution ( straight arrows) as well as a large left ventricular apical hypointensity which did not take contrast proving it to be thrombus ( block arrows)Additionally wash out of contrast from normal myocardium (curved arrows) can be noted
Differential diagnosis of delayed contrast enhancement at cardiac MR imaging by location
Amyloidosis
bull POINTS IN FAVOUR -Subendocardial
enhancement is common
bull POINTS AGAINST -Subendocardial
enhancement is not global -Presence of intra -
ventricular thrombus
Endomyocardial fibrosisLoefflers endocarditis
bull POINTS IN FAVOUR-Subendocardial
enhancement is not global
-Presence of intra -ventricular thrombus
bull POINTS AGAINST-None
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP
Etiological diagnosis
Infiltrative cardiomyopathy
bull EMFbull Lofflers endocarditis
Endomyocardial fibrosis(MF) Point in favorbull More common in tropical country countries(India and Brazil)bull Associated with restrictive physiology with ventricular apical
obliteration bull Biventricular involvement present in 75 cases
Point againstbull Insidious onset and gradual progression bull Hypereosinophilia is uncommon bull Ecg- atrial fibrillation right axis deviation is more common bull Not associated with systemic illness
Lofflers endocarditisPoint in favorbull Predominantly in malebull Onset is common between second ndash fourth decade bull Onset is acute bull More aggressive coursebull Commonly present with fever cough and weight lossbull Associated with severe hypereosinophilliabull Associated with restrictive physiology with ventricular apical
obliteration bull Bi-ventricular involvement -100bull Ecg ndashsinus rhythm ST depressionbull Associated with systemic illness with multi-organ involvement Point againstbull More common in temperate countries
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Etiological diagnosis
bull EMFbull Lofflers endocarditis
Diagnosis
bull Lofflers endocarditis with systemic hyper- eosinophilia
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Tumor associated-Adenocarcinomas bull Squamous carcinomasbull Large cell lung carcinomas bull Chronic Constrictive cardiomyopathybull Infiltrative cardiomyopathy bull Hypereosinophilic syndromebull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Chronic eosinophilic leukemia bull Other MPNMDS associated with eosinophilia
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysisbull BAL and lung biopsy
Pathological Discussion
Dr Neetu AgrawalSenior Demonstrator
Under guidance
Dr Anita HarshAssociate Professor
Department of Pathology
COMPLETE BLOOD COUNTSRBC 332 X 106 μlHGB 96 gdlHCT 306 MCV 922 fLMCH 289 pgMCHC 314 gdlWBC 2165 X 103 microlDLC Neutrophils - 18 Lymphocytes - 15 Monocytes - 02 Eosinophils - 65 Basophils - 00PLT 45 x 103 microlAbsolute Eosinophil Count- 14 x 103microl
Peripheral blood film shows predominantly normocytic normochromic RBCs with few macrocytes Eosinophilic leukocytosis showing hypersegmentation amp cytoplasmic vacoulization Platelets are reduced(40x Leishman stain)
Bone marrow aspirates markedly diluted with peripheral blood showing eosinophils
Bone marrow aspirate showing eosinophilic myelocyte band cell amp one hypersegmented
Eosinophil with cytoplasmic vacoulization
Trephine marrow biopsy showing bony trabeculae amp hypercellular hematopoietic tissue
(10xHampE stain)
Bone marrow biopsy showing myeloid hyperplasia with increased eosinophils and eosinophilic precursors few blasts with open nuclear chromatin amp
prominent nucleoli normoblastic erythropoiesis and megakaryocytes (40xHampE stain)
Bone marrow biopsy shows predominantly eosinophilic precursors and eosinophils with granular pink red cytoplasm (40x HampE stain)
Bone marrow biopsy showing different stages of eosinophil maturation with
hypersegmented and ring eosinophil (100x HampE stain)
Bone marrow biopsy showing focal increased reticulin with few course fibres grade 2 ( 4x reticulin stain)
bull PBF ndash Eosinophilic leukocytosisbull BM Aspiration ndash Diluted bull BMB - Myeloid hyperplasia with increased
Eosinophil and its precursors and abnormal forms
bull No increase in blastsbull Increased fibrosis (MF2)
The WHO defined Myeloid malignancies associated with clonal eosinophilia ruled out by CBC PBF amp BM examination are ndash AML with inv 16 ndash no blast in PBF Blasts ˂ 20 in BM Polycythemia vera - Hb lt 165 gdl HCT lt 49 no trilineage hyperplasia on BMB Essential thrombocythemia ndash PLT decreased no increase in megakaryocytes on BMB Primary Myelofibrosis ndash No megakaryocytic proliferation and atypia CMML ndash Monocytosis absent Monocytes lt 10 of WBC count aCML - neutrophils and their precursors are not increased Systemic Mastocytosis ndash Mast cells are not seen
Myeloid neoplasms associated with eosinophilia and rearrangement
of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
Chronic eosinophilic leukemia NOS
Idiopathic Hypereosinophilic syndrome
DIFFERENTIAL DIAGNOSIS 1 Myeloid neoplasms associated with eosinophilia and rearrangement of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
2 Chronic eosinophilic leukemia NOS
3 Idiopathic Hypereosinophilic syndrome
These disorders can not be differentiated on the basis of morphology Molecularcytogenetic analysis was suggested for further categorization
Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
Bright blood 4 chamber cine MRI is showing left ventricular apical hypointensity with bi-atrial dilatation
Early post contrast MR images are showing subendocardial enhancement in nonvascular distribution (straight arrows) and a large left ventricular apical hypointensity ( curved arrows)
Delayed post contrast MR images are showing subendocardial enhancement in a nonvascular distribution ( straight arrows) as well as a large left ventricular apical hypointensity which did not take contrast proving it to be thrombus ( block arrows)Additionally wash out of contrast from normal myocardium (curved arrows) can be noted
Differential diagnosis of delayed contrast enhancement at cardiac MR imaging by location
Amyloidosis
bull POINTS IN FAVOUR -Subendocardial
enhancement is common
bull POINTS AGAINST -Subendocardial
enhancement is not global -Presence of intra -
ventricular thrombus
Endomyocardial fibrosisLoefflers endocarditis
bull POINTS IN FAVOUR-Subendocardial
enhancement is not global
-Presence of intra -ventricular thrombus
bull POINTS AGAINST-None
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP
Etiological diagnosis
Infiltrative cardiomyopathy
bull EMFbull Lofflers endocarditis
Endomyocardial fibrosis(MF) Point in favorbull More common in tropical country countries(India and Brazil)bull Associated with restrictive physiology with ventricular apical
obliteration bull Biventricular involvement present in 75 cases
Point againstbull Insidious onset and gradual progression bull Hypereosinophilia is uncommon bull Ecg- atrial fibrillation right axis deviation is more common bull Not associated with systemic illness
Lofflers endocarditisPoint in favorbull Predominantly in malebull Onset is common between second ndash fourth decade bull Onset is acute bull More aggressive coursebull Commonly present with fever cough and weight lossbull Associated with severe hypereosinophilliabull Associated with restrictive physiology with ventricular apical
obliteration bull Bi-ventricular involvement -100bull Ecg ndashsinus rhythm ST depressionbull Associated with systemic illness with multi-organ involvement Point againstbull More common in temperate countries
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Etiological diagnosis
bull EMFbull Lofflers endocarditis
Diagnosis
bull Lofflers endocarditis with systemic hyper- eosinophilia
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Tumor associated-Adenocarcinomas bull Squamous carcinomasbull Large cell lung carcinomas bull Chronic Constrictive cardiomyopathybull Infiltrative cardiomyopathy bull Hypereosinophilic syndromebull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Chronic eosinophilic leukemia bull Other MPNMDS associated with eosinophilia
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysisbull BAL and lung biopsy
Pathological Discussion
Dr Neetu AgrawalSenior Demonstrator
Under guidance
Dr Anita HarshAssociate Professor
Department of Pathology
COMPLETE BLOOD COUNTSRBC 332 X 106 μlHGB 96 gdlHCT 306 MCV 922 fLMCH 289 pgMCHC 314 gdlWBC 2165 X 103 microlDLC Neutrophils - 18 Lymphocytes - 15 Monocytes - 02 Eosinophils - 65 Basophils - 00PLT 45 x 103 microlAbsolute Eosinophil Count- 14 x 103microl
Peripheral blood film shows predominantly normocytic normochromic RBCs with few macrocytes Eosinophilic leukocytosis showing hypersegmentation amp cytoplasmic vacoulization Platelets are reduced(40x Leishman stain)
Bone marrow aspirates markedly diluted with peripheral blood showing eosinophils
Bone marrow aspirate showing eosinophilic myelocyte band cell amp one hypersegmented
Eosinophil with cytoplasmic vacoulization
Trephine marrow biopsy showing bony trabeculae amp hypercellular hematopoietic tissue
(10xHampE stain)
Bone marrow biopsy showing myeloid hyperplasia with increased eosinophils and eosinophilic precursors few blasts with open nuclear chromatin amp
prominent nucleoli normoblastic erythropoiesis and megakaryocytes (40xHampE stain)
Bone marrow biopsy shows predominantly eosinophilic precursors and eosinophils with granular pink red cytoplasm (40x HampE stain)
Bone marrow biopsy showing different stages of eosinophil maturation with
hypersegmented and ring eosinophil (100x HampE stain)
Bone marrow biopsy showing focal increased reticulin with few course fibres grade 2 ( 4x reticulin stain)
bull PBF ndash Eosinophilic leukocytosisbull BM Aspiration ndash Diluted bull BMB - Myeloid hyperplasia with increased
Eosinophil and its precursors and abnormal forms
bull No increase in blastsbull Increased fibrosis (MF2)
The WHO defined Myeloid malignancies associated with clonal eosinophilia ruled out by CBC PBF amp BM examination are ndash AML with inv 16 ndash no blast in PBF Blasts ˂ 20 in BM Polycythemia vera - Hb lt 165 gdl HCT lt 49 no trilineage hyperplasia on BMB Essential thrombocythemia ndash PLT decreased no increase in megakaryocytes on BMB Primary Myelofibrosis ndash No megakaryocytic proliferation and atypia CMML ndash Monocytosis absent Monocytes lt 10 of WBC count aCML - neutrophils and their precursors are not increased Systemic Mastocytosis ndash Mast cells are not seen
Myeloid neoplasms associated with eosinophilia and rearrangement
of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
Chronic eosinophilic leukemia NOS
Idiopathic Hypereosinophilic syndrome
DIFFERENTIAL DIAGNOSIS 1 Myeloid neoplasms associated with eosinophilia and rearrangement of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
2 Chronic eosinophilic leukemia NOS
3 Idiopathic Hypereosinophilic syndrome
These disorders can not be differentiated on the basis of morphology Molecularcytogenetic analysis was suggested for further categorization
Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-

Early post contrast MR images are showing subendocardial enhancement in nonvascular distribution (straight arrows) and a large left ventricular apical hypointensity ( curved arrows)
Delayed post contrast MR images are showing subendocardial enhancement in a nonvascular distribution ( straight arrows) as well as a large left ventricular apical hypointensity which did not take contrast proving it to be thrombus ( block arrows)Additionally wash out of contrast from normal myocardium (curved arrows) can be noted
Differential diagnosis of delayed contrast enhancement at cardiac MR imaging by location
Amyloidosis
bull POINTS IN FAVOUR -Subendocardial
enhancement is common
bull POINTS AGAINST -Subendocardial
enhancement is not global -Presence of intra -
ventricular thrombus
Endomyocardial fibrosisLoefflers endocarditis
bull POINTS IN FAVOUR-Subendocardial
enhancement is not global
-Presence of intra -ventricular thrombus
bull POINTS AGAINST-None
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP
Etiological diagnosis
Infiltrative cardiomyopathy
bull EMFbull Lofflers endocarditis
Endomyocardial fibrosis(MF) Point in favorbull More common in tropical country countries(India and Brazil)bull Associated with restrictive physiology with ventricular apical
obliteration bull Biventricular involvement present in 75 cases
Point againstbull Insidious onset and gradual progression bull Hypereosinophilia is uncommon bull Ecg- atrial fibrillation right axis deviation is more common bull Not associated with systemic illness
Lofflers endocarditisPoint in favorbull Predominantly in malebull Onset is common between second ndash fourth decade bull Onset is acute bull More aggressive coursebull Commonly present with fever cough and weight lossbull Associated with severe hypereosinophilliabull Associated with restrictive physiology with ventricular apical
obliteration bull Bi-ventricular involvement -100bull Ecg ndashsinus rhythm ST depressionbull Associated with systemic illness with multi-organ involvement Point againstbull More common in temperate countries
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Etiological diagnosis
bull EMFbull Lofflers endocarditis
Diagnosis
bull Lofflers endocarditis with systemic hyper- eosinophilia
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Tumor associated-Adenocarcinomas bull Squamous carcinomasbull Large cell lung carcinomas bull Chronic Constrictive cardiomyopathybull Infiltrative cardiomyopathy bull Hypereosinophilic syndromebull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Chronic eosinophilic leukemia bull Other MPNMDS associated with eosinophilia
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysisbull BAL and lung biopsy
Pathological Discussion
Dr Neetu AgrawalSenior Demonstrator
Under guidance
Dr Anita HarshAssociate Professor
Department of Pathology
COMPLETE BLOOD COUNTSRBC 332 X 106 μlHGB 96 gdlHCT 306 MCV 922 fLMCH 289 pgMCHC 314 gdlWBC 2165 X 103 microlDLC Neutrophils - 18 Lymphocytes - 15 Monocytes - 02 Eosinophils - 65 Basophils - 00PLT 45 x 103 microlAbsolute Eosinophil Count- 14 x 103microl
Peripheral blood film shows predominantly normocytic normochromic RBCs with few macrocytes Eosinophilic leukocytosis showing hypersegmentation amp cytoplasmic vacoulization Platelets are reduced(40x Leishman stain)
Bone marrow aspirates markedly diluted with peripheral blood showing eosinophils
Bone marrow aspirate showing eosinophilic myelocyte band cell amp one hypersegmented
Eosinophil with cytoplasmic vacoulization
Trephine marrow biopsy showing bony trabeculae amp hypercellular hematopoietic tissue
(10xHampE stain)
Bone marrow biopsy showing myeloid hyperplasia with increased eosinophils and eosinophilic precursors few blasts with open nuclear chromatin amp
prominent nucleoli normoblastic erythropoiesis and megakaryocytes (40xHampE stain)
Bone marrow biopsy shows predominantly eosinophilic precursors and eosinophils with granular pink red cytoplasm (40x HampE stain)
Bone marrow biopsy showing different stages of eosinophil maturation with
hypersegmented and ring eosinophil (100x HampE stain)
Bone marrow biopsy showing focal increased reticulin with few course fibres grade 2 ( 4x reticulin stain)
bull PBF ndash Eosinophilic leukocytosisbull BM Aspiration ndash Diluted bull BMB - Myeloid hyperplasia with increased
Eosinophil and its precursors and abnormal forms
bull No increase in blastsbull Increased fibrosis (MF2)
The WHO defined Myeloid malignancies associated with clonal eosinophilia ruled out by CBC PBF amp BM examination are ndash AML with inv 16 ndash no blast in PBF Blasts ˂ 20 in BM Polycythemia vera - Hb lt 165 gdl HCT lt 49 no trilineage hyperplasia on BMB Essential thrombocythemia ndash PLT decreased no increase in megakaryocytes on BMB Primary Myelofibrosis ndash No megakaryocytic proliferation and atypia CMML ndash Monocytosis absent Monocytes lt 10 of WBC count aCML - neutrophils and their precursors are not increased Systemic Mastocytosis ndash Mast cells are not seen
Myeloid neoplasms associated with eosinophilia and rearrangement
of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
Chronic eosinophilic leukemia NOS
Idiopathic Hypereosinophilic syndrome
DIFFERENTIAL DIAGNOSIS 1 Myeloid neoplasms associated with eosinophilia and rearrangement of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
2 Chronic eosinophilic leukemia NOS
3 Idiopathic Hypereosinophilic syndrome
These disorders can not be differentiated on the basis of morphology Molecularcytogenetic analysis was suggested for further categorization
Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
Delayed post contrast MR images are showing subendocardial enhancement in a nonvascular distribution ( straight arrows) as well as a large left ventricular apical hypointensity which did not take contrast proving it to be thrombus ( block arrows)Additionally wash out of contrast from normal myocardium (curved arrows) can be noted
Differential diagnosis of delayed contrast enhancement at cardiac MR imaging by location
Amyloidosis
bull POINTS IN FAVOUR -Subendocardial
enhancement is common
bull POINTS AGAINST -Subendocardial
enhancement is not global -Presence of intra -
ventricular thrombus
Endomyocardial fibrosisLoefflers endocarditis
bull POINTS IN FAVOUR-Subendocardial
enhancement is not global
-Presence of intra -ventricular thrombus
bull POINTS AGAINST-None
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP
Etiological diagnosis
Infiltrative cardiomyopathy
bull EMFbull Lofflers endocarditis
Endomyocardial fibrosis(MF) Point in favorbull More common in tropical country countries(India and Brazil)bull Associated with restrictive physiology with ventricular apical
obliteration bull Biventricular involvement present in 75 cases
Point againstbull Insidious onset and gradual progression bull Hypereosinophilia is uncommon bull Ecg- atrial fibrillation right axis deviation is more common bull Not associated with systemic illness
Lofflers endocarditisPoint in favorbull Predominantly in malebull Onset is common between second ndash fourth decade bull Onset is acute bull More aggressive coursebull Commonly present with fever cough and weight lossbull Associated with severe hypereosinophilliabull Associated with restrictive physiology with ventricular apical
obliteration bull Bi-ventricular involvement -100bull Ecg ndashsinus rhythm ST depressionbull Associated with systemic illness with multi-organ involvement Point againstbull More common in temperate countries
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Etiological diagnosis
bull EMFbull Lofflers endocarditis
Diagnosis
bull Lofflers endocarditis with systemic hyper- eosinophilia
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Tumor associated-Adenocarcinomas bull Squamous carcinomasbull Large cell lung carcinomas bull Chronic Constrictive cardiomyopathybull Infiltrative cardiomyopathy bull Hypereosinophilic syndromebull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Chronic eosinophilic leukemia bull Other MPNMDS associated with eosinophilia
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysisbull BAL and lung biopsy
Pathological Discussion
Dr Neetu AgrawalSenior Demonstrator
Under guidance
Dr Anita HarshAssociate Professor
Department of Pathology
COMPLETE BLOOD COUNTSRBC 332 X 106 μlHGB 96 gdlHCT 306 MCV 922 fLMCH 289 pgMCHC 314 gdlWBC 2165 X 103 microlDLC Neutrophils - 18 Lymphocytes - 15 Monocytes - 02 Eosinophils - 65 Basophils - 00PLT 45 x 103 microlAbsolute Eosinophil Count- 14 x 103microl
Peripheral blood film shows predominantly normocytic normochromic RBCs with few macrocytes Eosinophilic leukocytosis showing hypersegmentation amp cytoplasmic vacoulization Platelets are reduced(40x Leishman stain)
Bone marrow aspirates markedly diluted with peripheral blood showing eosinophils
Bone marrow aspirate showing eosinophilic myelocyte band cell amp one hypersegmented
Eosinophil with cytoplasmic vacoulization
Trephine marrow biopsy showing bony trabeculae amp hypercellular hematopoietic tissue
(10xHampE stain)
Bone marrow biopsy showing myeloid hyperplasia with increased eosinophils and eosinophilic precursors few blasts with open nuclear chromatin amp
prominent nucleoli normoblastic erythropoiesis and megakaryocytes (40xHampE stain)
Bone marrow biopsy shows predominantly eosinophilic precursors and eosinophils with granular pink red cytoplasm (40x HampE stain)
Bone marrow biopsy showing different stages of eosinophil maturation with
hypersegmented and ring eosinophil (100x HampE stain)
Bone marrow biopsy showing focal increased reticulin with few course fibres grade 2 ( 4x reticulin stain)
bull PBF ndash Eosinophilic leukocytosisbull BM Aspiration ndash Diluted bull BMB - Myeloid hyperplasia with increased
Eosinophil and its precursors and abnormal forms
bull No increase in blastsbull Increased fibrosis (MF2)
The WHO defined Myeloid malignancies associated with clonal eosinophilia ruled out by CBC PBF amp BM examination are ndash AML with inv 16 ndash no blast in PBF Blasts ˂ 20 in BM Polycythemia vera - Hb lt 165 gdl HCT lt 49 no trilineage hyperplasia on BMB Essential thrombocythemia ndash PLT decreased no increase in megakaryocytes on BMB Primary Myelofibrosis ndash No megakaryocytic proliferation and atypia CMML ndash Monocytosis absent Monocytes lt 10 of WBC count aCML - neutrophils and their precursors are not increased Systemic Mastocytosis ndash Mast cells are not seen
Myeloid neoplasms associated with eosinophilia and rearrangement
of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
Chronic eosinophilic leukemia NOS
Idiopathic Hypereosinophilic syndrome
DIFFERENTIAL DIAGNOSIS 1 Myeloid neoplasms associated with eosinophilia and rearrangement of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
2 Chronic eosinophilic leukemia NOS
3 Idiopathic Hypereosinophilic syndrome
These disorders can not be differentiated on the basis of morphology Molecularcytogenetic analysis was suggested for further categorization
Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
Differential diagnosis of delayed contrast enhancement at cardiac MR imaging by location
Amyloidosis
bull POINTS IN FAVOUR -Subendocardial
enhancement is common
bull POINTS AGAINST -Subendocardial
enhancement is not global -Presence of intra -
ventricular thrombus
Endomyocardial fibrosisLoefflers endocarditis
bull POINTS IN FAVOUR-Subendocardial
enhancement is not global
-Presence of intra -ventricular thrombus
bull POINTS AGAINST-None
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP
Etiological diagnosis
Infiltrative cardiomyopathy
bull EMFbull Lofflers endocarditis
Endomyocardial fibrosis(MF) Point in favorbull More common in tropical country countries(India and Brazil)bull Associated with restrictive physiology with ventricular apical
obliteration bull Biventricular involvement present in 75 cases
Point againstbull Insidious onset and gradual progression bull Hypereosinophilia is uncommon bull Ecg- atrial fibrillation right axis deviation is more common bull Not associated with systemic illness
Lofflers endocarditisPoint in favorbull Predominantly in malebull Onset is common between second ndash fourth decade bull Onset is acute bull More aggressive coursebull Commonly present with fever cough and weight lossbull Associated with severe hypereosinophilliabull Associated with restrictive physiology with ventricular apical
obliteration bull Bi-ventricular involvement -100bull Ecg ndashsinus rhythm ST depressionbull Associated with systemic illness with multi-organ involvement Point againstbull More common in temperate countries
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Etiological diagnosis
bull EMFbull Lofflers endocarditis
Diagnosis
bull Lofflers endocarditis with systemic hyper- eosinophilia
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Tumor associated-Adenocarcinomas bull Squamous carcinomasbull Large cell lung carcinomas bull Chronic Constrictive cardiomyopathybull Infiltrative cardiomyopathy bull Hypereosinophilic syndromebull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Chronic eosinophilic leukemia bull Other MPNMDS associated with eosinophilia
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysisbull BAL and lung biopsy
Pathological Discussion
Dr Neetu AgrawalSenior Demonstrator
Under guidance
Dr Anita HarshAssociate Professor
Department of Pathology
COMPLETE BLOOD COUNTSRBC 332 X 106 μlHGB 96 gdlHCT 306 MCV 922 fLMCH 289 pgMCHC 314 gdlWBC 2165 X 103 microlDLC Neutrophils - 18 Lymphocytes - 15 Monocytes - 02 Eosinophils - 65 Basophils - 00PLT 45 x 103 microlAbsolute Eosinophil Count- 14 x 103microl
Peripheral blood film shows predominantly normocytic normochromic RBCs with few macrocytes Eosinophilic leukocytosis showing hypersegmentation amp cytoplasmic vacoulization Platelets are reduced(40x Leishman stain)
Bone marrow aspirates markedly diluted with peripheral blood showing eosinophils
Bone marrow aspirate showing eosinophilic myelocyte band cell amp one hypersegmented
Eosinophil with cytoplasmic vacoulization
Trephine marrow biopsy showing bony trabeculae amp hypercellular hematopoietic tissue
(10xHampE stain)
Bone marrow biopsy showing myeloid hyperplasia with increased eosinophils and eosinophilic precursors few blasts with open nuclear chromatin amp
prominent nucleoli normoblastic erythropoiesis and megakaryocytes (40xHampE stain)
Bone marrow biopsy shows predominantly eosinophilic precursors and eosinophils with granular pink red cytoplasm (40x HampE stain)
Bone marrow biopsy showing different stages of eosinophil maturation with
hypersegmented and ring eosinophil (100x HampE stain)
Bone marrow biopsy showing focal increased reticulin with few course fibres grade 2 ( 4x reticulin stain)
bull PBF ndash Eosinophilic leukocytosisbull BM Aspiration ndash Diluted bull BMB - Myeloid hyperplasia with increased
Eosinophil and its precursors and abnormal forms
bull No increase in blastsbull Increased fibrosis (MF2)
The WHO defined Myeloid malignancies associated with clonal eosinophilia ruled out by CBC PBF amp BM examination are ndash AML with inv 16 ndash no blast in PBF Blasts ˂ 20 in BM Polycythemia vera - Hb lt 165 gdl HCT lt 49 no trilineage hyperplasia on BMB Essential thrombocythemia ndash PLT decreased no increase in megakaryocytes on BMB Primary Myelofibrosis ndash No megakaryocytic proliferation and atypia CMML ndash Monocytosis absent Monocytes lt 10 of WBC count aCML - neutrophils and their precursors are not increased Systemic Mastocytosis ndash Mast cells are not seen
Myeloid neoplasms associated with eosinophilia and rearrangement
of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
Chronic eosinophilic leukemia NOS
Idiopathic Hypereosinophilic syndrome
DIFFERENTIAL DIAGNOSIS 1 Myeloid neoplasms associated with eosinophilia and rearrangement of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
2 Chronic eosinophilic leukemia NOS
3 Idiopathic Hypereosinophilic syndrome
These disorders can not be differentiated on the basis of morphology Molecularcytogenetic analysis was suggested for further categorization
Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
Amyloidosis
bull POINTS IN FAVOUR -Subendocardial
enhancement is common
bull POINTS AGAINST -Subendocardial
enhancement is not global -Presence of intra -
ventricular thrombus
Endomyocardial fibrosisLoefflers endocarditis
bull POINTS IN FAVOUR-Subendocardial
enhancement is not global
-Presence of intra -ventricular thrombus
bull POINTS AGAINST-None
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP
Etiological diagnosis
Infiltrative cardiomyopathy
bull EMFbull Lofflers endocarditis
Endomyocardial fibrosis(MF) Point in favorbull More common in tropical country countries(India and Brazil)bull Associated with restrictive physiology with ventricular apical
obliteration bull Biventricular involvement present in 75 cases
Point againstbull Insidious onset and gradual progression bull Hypereosinophilia is uncommon bull Ecg- atrial fibrillation right axis deviation is more common bull Not associated with systemic illness
Lofflers endocarditisPoint in favorbull Predominantly in malebull Onset is common between second ndash fourth decade bull Onset is acute bull More aggressive coursebull Commonly present with fever cough and weight lossbull Associated with severe hypereosinophilliabull Associated with restrictive physiology with ventricular apical
obliteration bull Bi-ventricular involvement -100bull Ecg ndashsinus rhythm ST depressionbull Associated with systemic illness with multi-organ involvement Point againstbull More common in temperate countries
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Etiological diagnosis
bull EMFbull Lofflers endocarditis
Diagnosis
bull Lofflers endocarditis with systemic hyper- eosinophilia
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Tumor associated-Adenocarcinomas bull Squamous carcinomasbull Large cell lung carcinomas bull Chronic Constrictive cardiomyopathybull Infiltrative cardiomyopathy bull Hypereosinophilic syndromebull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Chronic eosinophilic leukemia bull Other MPNMDS associated with eosinophilia
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysisbull BAL and lung biopsy
Pathological Discussion
Dr Neetu AgrawalSenior Demonstrator
Under guidance
Dr Anita HarshAssociate Professor
Department of Pathology
COMPLETE BLOOD COUNTSRBC 332 X 106 μlHGB 96 gdlHCT 306 MCV 922 fLMCH 289 pgMCHC 314 gdlWBC 2165 X 103 microlDLC Neutrophils - 18 Lymphocytes - 15 Monocytes - 02 Eosinophils - 65 Basophils - 00PLT 45 x 103 microlAbsolute Eosinophil Count- 14 x 103microl
Peripheral blood film shows predominantly normocytic normochromic RBCs with few macrocytes Eosinophilic leukocytosis showing hypersegmentation amp cytoplasmic vacoulization Platelets are reduced(40x Leishman stain)
Bone marrow aspirates markedly diluted with peripheral blood showing eosinophils
Bone marrow aspirate showing eosinophilic myelocyte band cell amp one hypersegmented
Eosinophil with cytoplasmic vacoulization
Trephine marrow biopsy showing bony trabeculae amp hypercellular hematopoietic tissue
(10xHampE stain)
Bone marrow biopsy showing myeloid hyperplasia with increased eosinophils and eosinophilic precursors few blasts with open nuclear chromatin amp
prominent nucleoli normoblastic erythropoiesis and megakaryocytes (40xHampE stain)
Bone marrow biopsy shows predominantly eosinophilic precursors and eosinophils with granular pink red cytoplasm (40x HampE stain)
Bone marrow biopsy showing different stages of eosinophil maturation with
hypersegmented and ring eosinophil (100x HampE stain)
Bone marrow biopsy showing focal increased reticulin with few course fibres grade 2 ( 4x reticulin stain)
bull PBF ndash Eosinophilic leukocytosisbull BM Aspiration ndash Diluted bull BMB - Myeloid hyperplasia with increased
Eosinophil and its precursors and abnormal forms
bull No increase in blastsbull Increased fibrosis (MF2)
The WHO defined Myeloid malignancies associated with clonal eosinophilia ruled out by CBC PBF amp BM examination are ndash AML with inv 16 ndash no blast in PBF Blasts ˂ 20 in BM Polycythemia vera - Hb lt 165 gdl HCT lt 49 no trilineage hyperplasia on BMB Essential thrombocythemia ndash PLT decreased no increase in megakaryocytes on BMB Primary Myelofibrosis ndash No megakaryocytic proliferation and atypia CMML ndash Monocytosis absent Monocytes lt 10 of WBC count aCML - neutrophils and their precursors are not increased Systemic Mastocytosis ndash Mast cells are not seen
Myeloid neoplasms associated with eosinophilia and rearrangement
of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
Chronic eosinophilic leukemia NOS
Idiopathic Hypereosinophilic syndrome
DIFFERENTIAL DIAGNOSIS 1 Myeloid neoplasms associated with eosinophilia and rearrangement of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
2 Chronic eosinophilic leukemia NOS
3 Idiopathic Hypereosinophilic syndrome
These disorders can not be differentiated on the basis of morphology Molecularcytogenetic analysis was suggested for further categorization
Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-

Endomyocardial fibrosisLoefflers endocarditis
bull POINTS IN FAVOUR-Subendocardial
enhancement is not global
-Presence of intra -ventricular thrombus
bull POINTS AGAINST-None
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP
Etiological diagnosis
Infiltrative cardiomyopathy
bull EMFbull Lofflers endocarditis
Endomyocardial fibrosis(MF) Point in favorbull More common in tropical country countries(India and Brazil)bull Associated with restrictive physiology with ventricular apical
obliteration bull Biventricular involvement present in 75 cases
Point againstbull Insidious onset and gradual progression bull Hypereosinophilia is uncommon bull Ecg- atrial fibrillation right axis deviation is more common bull Not associated with systemic illness
Lofflers endocarditisPoint in favorbull Predominantly in malebull Onset is common between second ndash fourth decade bull Onset is acute bull More aggressive coursebull Commonly present with fever cough and weight lossbull Associated with severe hypereosinophilliabull Associated with restrictive physiology with ventricular apical
obliteration bull Bi-ventricular involvement -100bull Ecg ndashsinus rhythm ST depressionbull Associated with systemic illness with multi-organ involvement Point againstbull More common in temperate countries
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Etiological diagnosis
bull EMFbull Lofflers endocarditis
Diagnosis
bull Lofflers endocarditis with systemic hyper- eosinophilia
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Tumor associated-Adenocarcinomas bull Squamous carcinomasbull Large cell lung carcinomas bull Chronic Constrictive cardiomyopathybull Infiltrative cardiomyopathy bull Hypereosinophilic syndromebull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Chronic eosinophilic leukemia bull Other MPNMDS associated with eosinophilia
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysisbull BAL and lung biopsy
Pathological Discussion
Dr Neetu AgrawalSenior Demonstrator
Under guidance
Dr Anita HarshAssociate Professor
Department of Pathology
COMPLETE BLOOD COUNTSRBC 332 X 106 μlHGB 96 gdlHCT 306 MCV 922 fLMCH 289 pgMCHC 314 gdlWBC 2165 X 103 microlDLC Neutrophils - 18 Lymphocytes - 15 Monocytes - 02 Eosinophils - 65 Basophils - 00PLT 45 x 103 microlAbsolute Eosinophil Count- 14 x 103microl
Peripheral blood film shows predominantly normocytic normochromic RBCs with few macrocytes Eosinophilic leukocytosis showing hypersegmentation amp cytoplasmic vacoulization Platelets are reduced(40x Leishman stain)
Bone marrow aspirates markedly diluted with peripheral blood showing eosinophils
Bone marrow aspirate showing eosinophilic myelocyte band cell amp one hypersegmented
Eosinophil with cytoplasmic vacoulization
Trephine marrow biopsy showing bony trabeculae amp hypercellular hematopoietic tissue
(10xHampE stain)
Bone marrow biopsy showing myeloid hyperplasia with increased eosinophils and eosinophilic precursors few blasts with open nuclear chromatin amp
prominent nucleoli normoblastic erythropoiesis and megakaryocytes (40xHampE stain)
Bone marrow biopsy shows predominantly eosinophilic precursors and eosinophils with granular pink red cytoplasm (40x HampE stain)
Bone marrow biopsy showing different stages of eosinophil maturation with
hypersegmented and ring eosinophil (100x HampE stain)
Bone marrow biopsy showing focal increased reticulin with few course fibres grade 2 ( 4x reticulin stain)
bull PBF ndash Eosinophilic leukocytosisbull BM Aspiration ndash Diluted bull BMB - Myeloid hyperplasia with increased
Eosinophil and its precursors and abnormal forms
bull No increase in blastsbull Increased fibrosis (MF2)
The WHO defined Myeloid malignancies associated with clonal eosinophilia ruled out by CBC PBF amp BM examination are ndash AML with inv 16 ndash no blast in PBF Blasts ˂ 20 in BM Polycythemia vera - Hb lt 165 gdl HCT lt 49 no trilineage hyperplasia on BMB Essential thrombocythemia ndash PLT decreased no increase in megakaryocytes on BMB Primary Myelofibrosis ndash No megakaryocytic proliferation and atypia CMML ndash Monocytosis absent Monocytes lt 10 of WBC count aCML - neutrophils and their precursors are not increased Systemic Mastocytosis ndash Mast cells are not seen
Myeloid neoplasms associated with eosinophilia and rearrangement
of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
Chronic eosinophilic leukemia NOS
Idiopathic Hypereosinophilic syndrome
DIFFERENTIAL DIAGNOSIS 1 Myeloid neoplasms associated with eosinophilia and rearrangement of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
2 Chronic eosinophilic leukemia NOS
3 Idiopathic Hypereosinophilic syndrome
These disorders can not be differentiated on the basis of morphology Molecularcytogenetic analysis was suggested for further categorization
Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
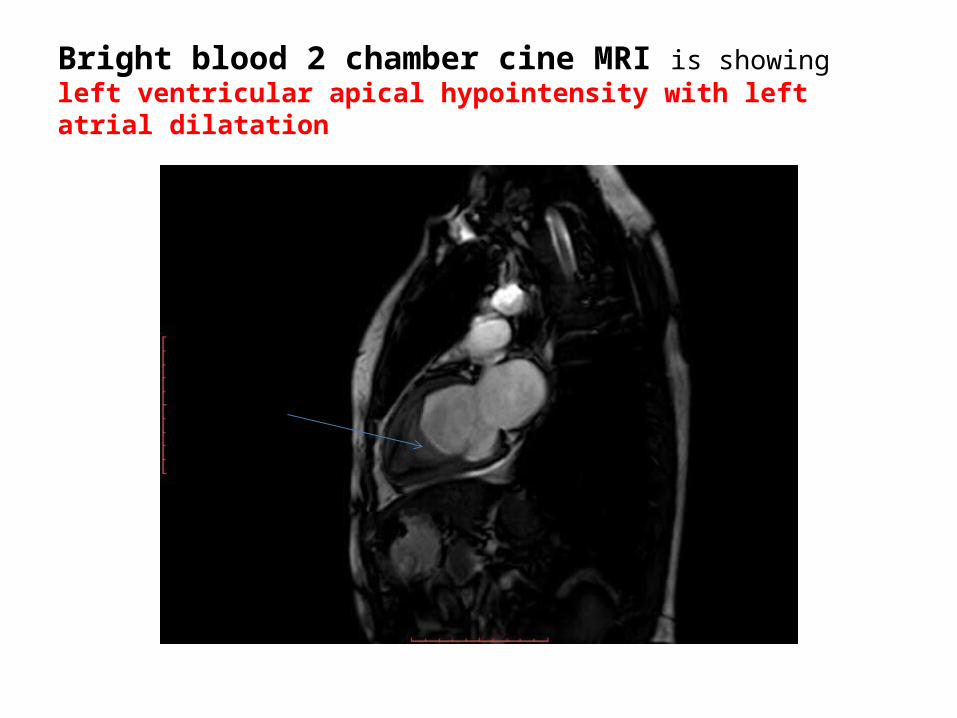
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP
Etiological diagnosis
Infiltrative cardiomyopathy
bull EMFbull Lofflers endocarditis
Endomyocardial fibrosis(MF) Point in favorbull More common in tropical country countries(India and Brazil)bull Associated with restrictive physiology with ventricular apical
obliteration bull Biventricular involvement present in 75 cases
Point againstbull Insidious onset and gradual progression bull Hypereosinophilia is uncommon bull Ecg- atrial fibrillation right axis deviation is more common bull Not associated with systemic illness
Lofflers endocarditisPoint in favorbull Predominantly in malebull Onset is common between second ndash fourth decade bull Onset is acute bull More aggressive coursebull Commonly present with fever cough and weight lossbull Associated with severe hypereosinophilliabull Associated with restrictive physiology with ventricular apical
obliteration bull Bi-ventricular involvement -100bull Ecg ndashsinus rhythm ST depressionbull Associated with systemic illness with multi-organ involvement Point againstbull More common in temperate countries
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Etiological diagnosis
bull EMFbull Lofflers endocarditis
Diagnosis
bull Lofflers endocarditis with systemic hyper- eosinophilia
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Tumor associated-Adenocarcinomas bull Squamous carcinomasbull Large cell lung carcinomas bull Chronic Constrictive cardiomyopathybull Infiltrative cardiomyopathy bull Hypereosinophilic syndromebull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Chronic eosinophilic leukemia bull Other MPNMDS associated with eosinophilia
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysisbull BAL and lung biopsy
Pathological Discussion
Dr Neetu AgrawalSenior Demonstrator
Under guidance
Dr Anita HarshAssociate Professor
Department of Pathology
COMPLETE BLOOD COUNTSRBC 332 X 106 μlHGB 96 gdlHCT 306 MCV 922 fLMCH 289 pgMCHC 314 gdlWBC 2165 X 103 microlDLC Neutrophils - 18 Lymphocytes - 15 Monocytes - 02 Eosinophils - 65 Basophils - 00PLT 45 x 103 microlAbsolute Eosinophil Count- 14 x 103microl
Peripheral blood film shows predominantly normocytic normochromic RBCs with few macrocytes Eosinophilic leukocytosis showing hypersegmentation amp cytoplasmic vacoulization Platelets are reduced(40x Leishman stain)
Bone marrow aspirates markedly diluted with peripheral blood showing eosinophils
Bone marrow aspirate showing eosinophilic myelocyte band cell amp one hypersegmented
Eosinophil with cytoplasmic vacoulization
Trephine marrow biopsy showing bony trabeculae amp hypercellular hematopoietic tissue
(10xHampE stain)
Bone marrow biopsy showing myeloid hyperplasia with increased eosinophils and eosinophilic precursors few blasts with open nuclear chromatin amp
prominent nucleoli normoblastic erythropoiesis and megakaryocytes (40xHampE stain)
Bone marrow biopsy shows predominantly eosinophilic precursors and eosinophils with granular pink red cytoplasm (40x HampE stain)
Bone marrow biopsy showing different stages of eosinophil maturation with
hypersegmented and ring eosinophil (100x HampE stain)
Bone marrow biopsy showing focal increased reticulin with few course fibres grade 2 ( 4x reticulin stain)
bull PBF ndash Eosinophilic leukocytosisbull BM Aspiration ndash Diluted bull BMB - Myeloid hyperplasia with increased
Eosinophil and its precursors and abnormal forms
bull No increase in blastsbull Increased fibrosis (MF2)
The WHO defined Myeloid malignancies associated with clonal eosinophilia ruled out by CBC PBF amp BM examination are ndash AML with inv 16 ndash no blast in PBF Blasts ˂ 20 in BM Polycythemia vera - Hb lt 165 gdl HCT lt 49 no trilineage hyperplasia on BMB Essential thrombocythemia ndash PLT decreased no increase in megakaryocytes on BMB Primary Myelofibrosis ndash No megakaryocytic proliferation and atypia CMML ndash Monocytosis absent Monocytes lt 10 of WBC count aCML - neutrophils and their precursors are not increased Systemic Mastocytosis ndash Mast cells are not seen
Myeloid neoplasms associated with eosinophilia and rearrangement
of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
Chronic eosinophilic leukemia NOS
Idiopathic Hypereosinophilic syndrome
DIFFERENTIAL DIAGNOSIS 1 Myeloid neoplasms associated with eosinophilia and rearrangement of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
2 Chronic eosinophilic leukemia NOS
3 Idiopathic Hypereosinophilic syndrome
These disorders can not be differentiated on the basis of morphology Molecularcytogenetic analysis was suggested for further categorization
Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
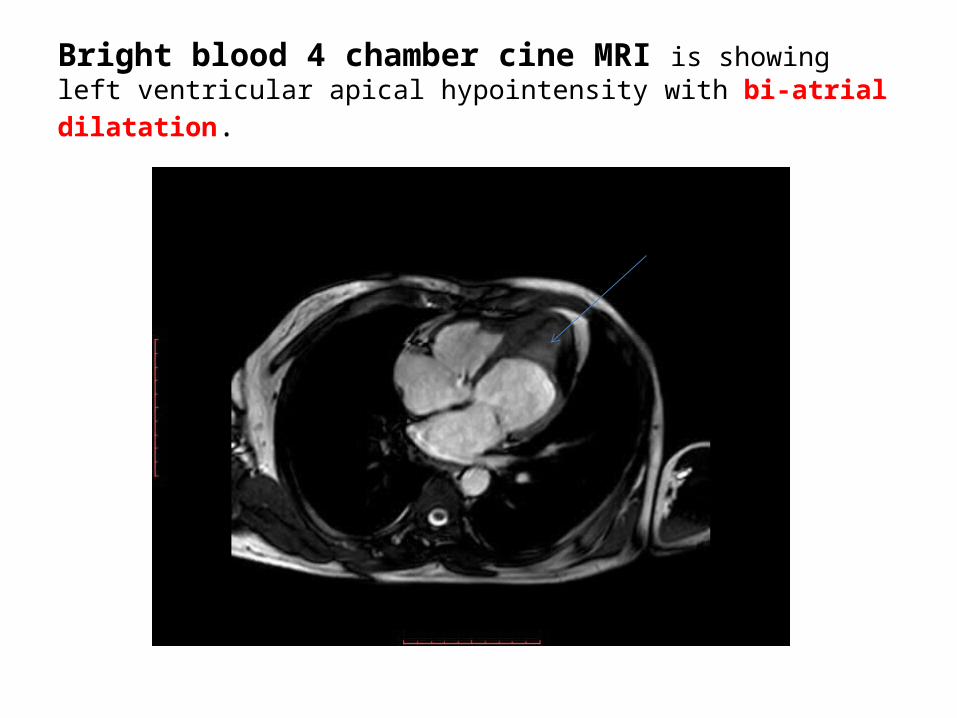
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP
Etiological diagnosis
Infiltrative cardiomyopathy
bull EMFbull Lofflers endocarditis
Endomyocardial fibrosis(MF) Point in favorbull More common in tropical country countries(India and Brazil)bull Associated with restrictive physiology with ventricular apical
obliteration bull Biventricular involvement present in 75 cases
Point againstbull Insidious onset and gradual progression bull Hypereosinophilia is uncommon bull Ecg- atrial fibrillation right axis deviation is more common bull Not associated with systemic illness
Lofflers endocarditisPoint in favorbull Predominantly in malebull Onset is common between second ndash fourth decade bull Onset is acute bull More aggressive coursebull Commonly present with fever cough and weight lossbull Associated with severe hypereosinophilliabull Associated with restrictive physiology with ventricular apical
obliteration bull Bi-ventricular involvement -100bull Ecg ndashsinus rhythm ST depressionbull Associated with systemic illness with multi-organ involvement Point againstbull More common in temperate countries
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Etiological diagnosis
bull EMFbull Lofflers endocarditis
Diagnosis
bull Lofflers endocarditis with systemic hyper- eosinophilia
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Tumor associated-Adenocarcinomas bull Squamous carcinomasbull Large cell lung carcinomas bull Chronic Constrictive cardiomyopathybull Infiltrative cardiomyopathy bull Hypereosinophilic syndromebull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Chronic eosinophilic leukemia bull Other MPNMDS associated with eosinophilia
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysisbull BAL and lung biopsy
Pathological Discussion
Dr Neetu AgrawalSenior Demonstrator
Under guidance
Dr Anita HarshAssociate Professor
Department of Pathology
COMPLETE BLOOD COUNTSRBC 332 X 106 μlHGB 96 gdlHCT 306 MCV 922 fLMCH 289 pgMCHC 314 gdlWBC 2165 X 103 microlDLC Neutrophils - 18 Lymphocytes - 15 Monocytes - 02 Eosinophils - 65 Basophils - 00PLT 45 x 103 microlAbsolute Eosinophil Count- 14 x 103microl
Peripheral blood film shows predominantly normocytic normochromic RBCs with few macrocytes Eosinophilic leukocytosis showing hypersegmentation amp cytoplasmic vacoulization Platelets are reduced(40x Leishman stain)
Bone marrow aspirates markedly diluted with peripheral blood showing eosinophils
Bone marrow aspirate showing eosinophilic myelocyte band cell amp one hypersegmented
Eosinophil with cytoplasmic vacoulization
Trephine marrow biopsy showing bony trabeculae amp hypercellular hematopoietic tissue
(10xHampE stain)
Bone marrow biopsy showing myeloid hyperplasia with increased eosinophils and eosinophilic precursors few blasts with open nuclear chromatin amp
prominent nucleoli normoblastic erythropoiesis and megakaryocytes (40xHampE stain)
Bone marrow biopsy shows predominantly eosinophilic precursors and eosinophils with granular pink red cytoplasm (40x HampE stain)
Bone marrow biopsy showing different stages of eosinophil maturation with
hypersegmented and ring eosinophil (100x HampE stain)
Bone marrow biopsy showing focal increased reticulin with few course fibres grade 2 ( 4x reticulin stain)
bull PBF ndash Eosinophilic leukocytosisbull BM Aspiration ndash Diluted bull BMB - Myeloid hyperplasia with increased
Eosinophil and its precursors and abnormal forms
bull No increase in blastsbull Increased fibrosis (MF2)
The WHO defined Myeloid malignancies associated with clonal eosinophilia ruled out by CBC PBF amp BM examination are ndash AML with inv 16 ndash no blast in PBF Blasts ˂ 20 in BM Polycythemia vera - Hb lt 165 gdl HCT lt 49 no trilineage hyperplasia on BMB Essential thrombocythemia ndash PLT decreased no increase in megakaryocytes on BMB Primary Myelofibrosis ndash No megakaryocytic proliferation and atypia CMML ndash Monocytosis absent Monocytes lt 10 of WBC count aCML - neutrophils and their precursors are not increased Systemic Mastocytosis ndash Mast cells are not seen
Myeloid neoplasms associated with eosinophilia and rearrangement
of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
Chronic eosinophilic leukemia NOS
Idiopathic Hypereosinophilic syndrome
DIFFERENTIAL DIAGNOSIS 1 Myeloid neoplasms associated with eosinophilia and rearrangement of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
2 Chronic eosinophilic leukemia NOS
3 Idiopathic Hypereosinophilic syndrome
These disorders can not be differentiated on the basis of morphology Molecularcytogenetic analysis was suggested for further categorization
Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-

Endomyocardial fibrosis(MF) Point in favorbull More common in tropical country countries(India and Brazil)bull Associated with restrictive physiology with ventricular apical
obliteration bull Biventricular involvement present in 75 cases
Point againstbull Insidious onset and gradual progression bull Hypereosinophilia is uncommon bull Ecg- atrial fibrillation right axis deviation is more common bull Not associated with systemic illness
Lofflers endocarditisPoint in favorbull Predominantly in malebull Onset is common between second ndash fourth decade bull Onset is acute bull More aggressive coursebull Commonly present with fever cough and weight lossbull Associated with severe hypereosinophilliabull Associated with restrictive physiology with ventricular apical
obliteration bull Bi-ventricular involvement -100bull Ecg ndashsinus rhythm ST depressionbull Associated with systemic illness with multi-organ involvement Point againstbull More common in temperate countries
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Etiological diagnosis
bull EMFbull Lofflers endocarditis
Diagnosis
bull Lofflers endocarditis with systemic hyper- eosinophilia
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Tumor associated-Adenocarcinomas bull Squamous carcinomasbull Large cell lung carcinomas bull Chronic Constrictive cardiomyopathybull Infiltrative cardiomyopathy bull Hypereosinophilic syndromebull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Chronic eosinophilic leukemia bull Other MPNMDS associated with eosinophilia
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysisbull BAL and lung biopsy
Pathological Discussion
Dr Neetu AgrawalSenior Demonstrator
Under guidance
Dr Anita HarshAssociate Professor
Department of Pathology
COMPLETE BLOOD COUNTSRBC 332 X 106 μlHGB 96 gdlHCT 306 MCV 922 fLMCH 289 pgMCHC 314 gdlWBC 2165 X 103 microlDLC Neutrophils - 18 Lymphocytes - 15 Monocytes - 02 Eosinophils - 65 Basophils - 00PLT 45 x 103 microlAbsolute Eosinophil Count- 14 x 103microl
Peripheral blood film shows predominantly normocytic normochromic RBCs with few macrocytes Eosinophilic leukocytosis showing hypersegmentation amp cytoplasmic vacoulization Platelets are reduced(40x Leishman stain)
Bone marrow aspirates markedly diluted with peripheral blood showing eosinophils
Bone marrow aspirate showing eosinophilic myelocyte band cell amp one hypersegmented
Eosinophil with cytoplasmic vacoulization
Trephine marrow biopsy showing bony trabeculae amp hypercellular hematopoietic tissue
(10xHampE stain)
Bone marrow biopsy showing myeloid hyperplasia with increased eosinophils and eosinophilic precursors few blasts with open nuclear chromatin amp
prominent nucleoli normoblastic erythropoiesis and megakaryocytes (40xHampE stain)
Bone marrow biopsy shows predominantly eosinophilic precursors and eosinophils with granular pink red cytoplasm (40x HampE stain)
Bone marrow biopsy showing different stages of eosinophil maturation with
hypersegmented and ring eosinophil (100x HampE stain)
Bone marrow biopsy showing focal increased reticulin with few course fibres grade 2 ( 4x reticulin stain)
bull PBF ndash Eosinophilic leukocytosisbull BM Aspiration ndash Diluted bull BMB - Myeloid hyperplasia with increased
Eosinophil and its precursors and abnormal forms
bull No increase in blastsbull Increased fibrosis (MF2)
The WHO defined Myeloid malignancies associated with clonal eosinophilia ruled out by CBC PBF amp BM examination are ndash AML with inv 16 ndash no blast in PBF Blasts ˂ 20 in BM Polycythemia vera - Hb lt 165 gdl HCT lt 49 no trilineage hyperplasia on BMB Essential thrombocythemia ndash PLT decreased no increase in megakaryocytes on BMB Primary Myelofibrosis ndash No megakaryocytic proliferation and atypia CMML ndash Monocytosis absent Monocytes lt 10 of WBC count aCML - neutrophils and their precursors are not increased Systemic Mastocytosis ndash Mast cells are not seen
Myeloid neoplasms associated with eosinophilia and rearrangement
of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
Chronic eosinophilic leukemia NOS
Idiopathic Hypereosinophilic syndrome
DIFFERENTIAL DIAGNOSIS 1 Myeloid neoplasms associated with eosinophilia and rearrangement of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
2 Chronic eosinophilic leukemia NOS
3 Idiopathic Hypereosinophilic syndrome
These disorders can not be differentiated on the basis of morphology Molecularcytogenetic analysis was suggested for further categorization
Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
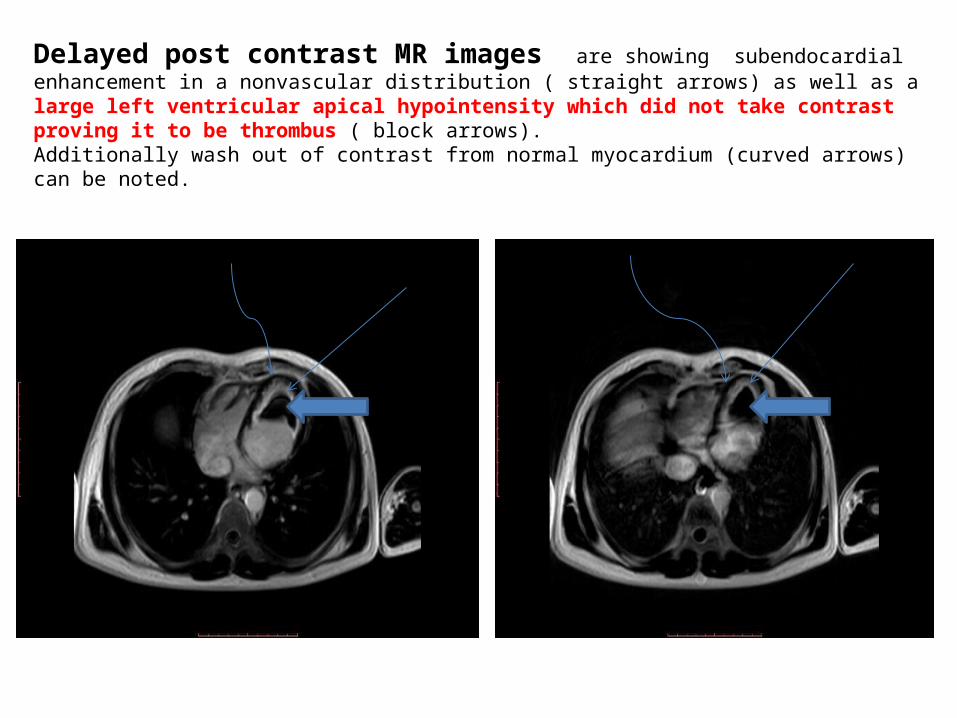
Lofflers endocarditisPoint in favorbull Predominantly in malebull Onset is common between second ndash fourth decade bull Onset is acute bull More aggressive coursebull Commonly present with fever cough and weight lossbull Associated with severe hypereosinophilliabull Associated with restrictive physiology with ventricular apical
obliteration bull Bi-ventricular involvement -100bull Ecg ndashsinus rhythm ST depressionbull Associated with systemic illness with multi-organ involvement Point againstbull More common in temperate countries
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Etiological diagnosis
bull EMFbull Lofflers endocarditis
Diagnosis
bull Lofflers endocarditis with systemic hyper- eosinophilia
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Tumor associated-Adenocarcinomas bull Squamous carcinomasbull Large cell lung carcinomas bull Chronic Constrictive cardiomyopathybull Infiltrative cardiomyopathy bull Hypereosinophilic syndromebull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Chronic eosinophilic leukemia bull Other MPNMDS associated with eosinophilia
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysisbull BAL and lung biopsy
Pathological Discussion
Dr Neetu AgrawalSenior Demonstrator
Under guidance
Dr Anita HarshAssociate Professor
Department of Pathology
COMPLETE BLOOD COUNTSRBC 332 X 106 μlHGB 96 gdlHCT 306 MCV 922 fLMCH 289 pgMCHC 314 gdlWBC 2165 X 103 microlDLC Neutrophils - 18 Lymphocytes - 15 Monocytes - 02 Eosinophils - 65 Basophils - 00PLT 45 x 103 microlAbsolute Eosinophil Count- 14 x 103microl
Peripheral blood film shows predominantly normocytic normochromic RBCs with few macrocytes Eosinophilic leukocytosis showing hypersegmentation amp cytoplasmic vacoulization Platelets are reduced(40x Leishman stain)
Bone marrow aspirates markedly diluted with peripheral blood showing eosinophils
Bone marrow aspirate showing eosinophilic myelocyte band cell amp one hypersegmented
Eosinophil with cytoplasmic vacoulization
Trephine marrow biopsy showing bony trabeculae amp hypercellular hematopoietic tissue
(10xHampE stain)
Bone marrow biopsy showing myeloid hyperplasia with increased eosinophils and eosinophilic precursors few blasts with open nuclear chromatin amp
prominent nucleoli normoblastic erythropoiesis and megakaryocytes (40xHampE stain)
Bone marrow biopsy shows predominantly eosinophilic precursors and eosinophils with granular pink red cytoplasm (40x HampE stain)
Bone marrow biopsy showing different stages of eosinophil maturation with
hypersegmented and ring eosinophil (100x HampE stain)
Bone marrow biopsy showing focal increased reticulin with few course fibres grade 2 ( 4x reticulin stain)
bull PBF ndash Eosinophilic leukocytosisbull BM Aspiration ndash Diluted bull BMB - Myeloid hyperplasia with increased
Eosinophil and its precursors and abnormal forms
bull No increase in blastsbull Increased fibrosis (MF2)
The WHO defined Myeloid malignancies associated with clonal eosinophilia ruled out by CBC PBF amp BM examination are ndash AML with inv 16 ndash no blast in PBF Blasts ˂ 20 in BM Polycythemia vera - Hb lt 165 gdl HCT lt 49 no trilineage hyperplasia on BMB Essential thrombocythemia ndash PLT decreased no increase in megakaryocytes on BMB Primary Myelofibrosis ndash No megakaryocytic proliferation and atypia CMML ndash Monocytosis absent Monocytes lt 10 of WBC count aCML - neutrophils and their precursors are not increased Systemic Mastocytosis ndash Mast cells are not seen
Myeloid neoplasms associated with eosinophilia and rearrangement
of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
Chronic eosinophilic leukemia NOS
Idiopathic Hypereosinophilic syndrome
DIFFERENTIAL DIAGNOSIS 1 Myeloid neoplasms associated with eosinophilia and rearrangement of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
2 Chronic eosinophilic leukemia NOS
3 Idiopathic Hypereosinophilic syndrome
These disorders can not be differentiated on the basis of morphology Molecularcytogenetic analysis was suggested for further categorization
Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
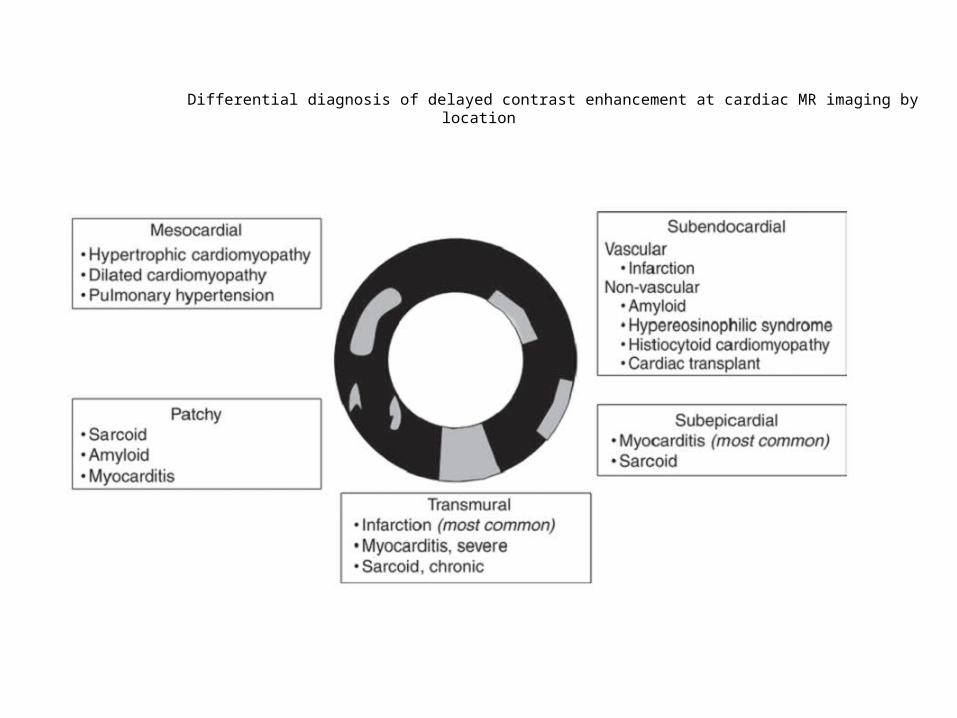
Cardiovascular involvement differentials
Restrictive physiology
bull RCMP bull CCP
Etiological diagnosis
bull EMFbull Lofflers endocarditis
Diagnosis
bull Lofflers endocarditis with systemic hyper- eosinophilia
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Tumor associated-Adenocarcinomas bull Squamous carcinomasbull Large cell lung carcinomas bull Chronic Constrictive cardiomyopathybull Infiltrative cardiomyopathy bull Hypereosinophilic syndromebull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Chronic eosinophilic leukemia bull Other MPNMDS associated with eosinophilia
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysisbull BAL and lung biopsy
Pathological Discussion
Dr Neetu AgrawalSenior Demonstrator
Under guidance
Dr Anita HarshAssociate Professor
Department of Pathology
COMPLETE BLOOD COUNTSRBC 332 X 106 μlHGB 96 gdlHCT 306 MCV 922 fLMCH 289 pgMCHC 314 gdlWBC 2165 X 103 microlDLC Neutrophils - 18 Lymphocytes - 15 Monocytes - 02 Eosinophils - 65 Basophils - 00PLT 45 x 103 microlAbsolute Eosinophil Count- 14 x 103microl
Peripheral blood film shows predominantly normocytic normochromic RBCs with few macrocytes Eosinophilic leukocytosis showing hypersegmentation amp cytoplasmic vacoulization Platelets are reduced(40x Leishman stain)
Bone marrow aspirates markedly diluted with peripheral blood showing eosinophils
Bone marrow aspirate showing eosinophilic myelocyte band cell amp one hypersegmented
Eosinophil with cytoplasmic vacoulization
Trephine marrow biopsy showing bony trabeculae amp hypercellular hematopoietic tissue
(10xHampE stain)
Bone marrow biopsy showing myeloid hyperplasia with increased eosinophils and eosinophilic precursors few blasts with open nuclear chromatin amp
prominent nucleoli normoblastic erythropoiesis and megakaryocytes (40xHampE stain)
Bone marrow biopsy shows predominantly eosinophilic precursors and eosinophils with granular pink red cytoplasm (40x HampE stain)
Bone marrow biopsy showing different stages of eosinophil maturation with
hypersegmented and ring eosinophil (100x HampE stain)
Bone marrow biopsy showing focal increased reticulin with few course fibres grade 2 ( 4x reticulin stain)
bull PBF ndash Eosinophilic leukocytosisbull BM Aspiration ndash Diluted bull BMB - Myeloid hyperplasia with increased
Eosinophil and its precursors and abnormal forms
bull No increase in blastsbull Increased fibrosis (MF2)
The WHO defined Myeloid malignancies associated with clonal eosinophilia ruled out by CBC PBF amp BM examination are ndash AML with inv 16 ndash no blast in PBF Blasts ˂ 20 in BM Polycythemia vera - Hb lt 165 gdl HCT lt 49 no trilineage hyperplasia on BMB Essential thrombocythemia ndash PLT decreased no increase in megakaryocytes on BMB Primary Myelofibrosis ndash No megakaryocytic proliferation and atypia CMML ndash Monocytosis absent Monocytes lt 10 of WBC count aCML - neutrophils and their precursors are not increased Systemic Mastocytosis ndash Mast cells are not seen
Myeloid neoplasms associated with eosinophilia and rearrangement
of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
Chronic eosinophilic leukemia NOS
Idiopathic Hypereosinophilic syndrome
DIFFERENTIAL DIAGNOSIS 1 Myeloid neoplasms associated with eosinophilia and rearrangement of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
2 Chronic eosinophilic leukemia NOS
3 Idiopathic Hypereosinophilic syndrome
These disorders can not be differentiated on the basis of morphology Molecularcytogenetic analysis was suggested for further categorization
Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
Diagnosis
bull Lofflers endocarditis with systemic hyper- eosinophilia
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Tumor associated-Adenocarcinomas bull Squamous carcinomasbull Large cell lung carcinomas bull Chronic Constrictive cardiomyopathybull Infiltrative cardiomyopathy bull Hypereosinophilic syndromebull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Chronic eosinophilic leukemia bull Other MPNMDS associated with eosinophilia
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysisbull BAL and lung biopsy
Pathological Discussion
Dr Neetu AgrawalSenior Demonstrator
Under guidance
Dr Anita HarshAssociate Professor
Department of Pathology
COMPLETE BLOOD COUNTSRBC 332 X 106 μlHGB 96 gdlHCT 306 MCV 922 fLMCH 289 pgMCHC 314 gdlWBC 2165 X 103 microlDLC Neutrophils - 18 Lymphocytes - 15 Monocytes - 02 Eosinophils - 65 Basophils - 00PLT 45 x 103 microlAbsolute Eosinophil Count- 14 x 103microl
Peripheral blood film shows predominantly normocytic normochromic RBCs with few macrocytes Eosinophilic leukocytosis showing hypersegmentation amp cytoplasmic vacoulization Platelets are reduced(40x Leishman stain)
Bone marrow aspirates markedly diluted with peripheral blood showing eosinophils
Bone marrow aspirate showing eosinophilic myelocyte band cell amp one hypersegmented
Eosinophil with cytoplasmic vacoulization
Trephine marrow biopsy showing bony trabeculae amp hypercellular hematopoietic tissue
(10xHampE stain)
Bone marrow biopsy showing myeloid hyperplasia with increased eosinophils and eosinophilic precursors few blasts with open nuclear chromatin amp
prominent nucleoli normoblastic erythropoiesis and megakaryocytes (40xHampE stain)
Bone marrow biopsy shows predominantly eosinophilic precursors and eosinophils with granular pink red cytoplasm (40x HampE stain)
Bone marrow biopsy showing different stages of eosinophil maturation with
hypersegmented and ring eosinophil (100x HampE stain)
Bone marrow biopsy showing focal increased reticulin with few course fibres grade 2 ( 4x reticulin stain)
bull PBF ndash Eosinophilic leukocytosisbull BM Aspiration ndash Diluted bull BMB - Myeloid hyperplasia with increased
Eosinophil and its precursors and abnormal forms
bull No increase in blastsbull Increased fibrosis (MF2)
The WHO defined Myeloid malignancies associated with clonal eosinophilia ruled out by CBC PBF amp BM examination are ndash AML with inv 16 ndash no blast in PBF Blasts ˂ 20 in BM Polycythemia vera - Hb lt 165 gdl HCT lt 49 no trilineage hyperplasia on BMB Essential thrombocythemia ndash PLT decreased no increase in megakaryocytes on BMB Primary Myelofibrosis ndash No megakaryocytic proliferation and atypia CMML ndash Monocytosis absent Monocytes lt 10 of WBC count aCML - neutrophils and their precursors are not increased Systemic Mastocytosis ndash Mast cells are not seen
Myeloid neoplasms associated with eosinophilia and rearrangement
of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
Chronic eosinophilic leukemia NOS
Idiopathic Hypereosinophilic syndrome
DIFFERENTIAL DIAGNOSIS 1 Myeloid neoplasms associated with eosinophilia and rearrangement of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
2 Chronic eosinophilic leukemia NOS
3 Idiopathic Hypereosinophilic syndrome
These disorders can not be differentiated on the basis of morphology Molecularcytogenetic analysis was suggested for further categorization
Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
bull Acute eosinophilic pneumoniabull Chronic eosinophilic pneumoniabull Loefflerrsquos pneumoniabull Allergic bronchopulmonary aspergillosis (ABPA)bull Churg Strauss syndrome bull Sarcoidosis bull Hypersensitivity pneumonitis bull Autoimmune and Connective tissue disorder bull Lymphomas (particularly Hodgkins T- and B-cell lymphomas)bull Tumor associated-Adenocarcinomas bull Squamous carcinomasbull Large cell lung carcinomas bull Chronic Constrictive cardiomyopathybull Infiltrative cardiomyopathy bull Hypereosinophilic syndromebull Leukemia (Acute myelogenous leukemias most commonly B cell ALL)bull Chronic eosinophilic leukemia bull Other MPNMDS associated with eosinophilia
DIFFERENTIALS DIAGNOSIS
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysisbull BAL and lung biopsy
Pathological Discussion
Dr Neetu AgrawalSenior Demonstrator
Under guidance
Dr Anita HarshAssociate Professor
Department of Pathology
COMPLETE BLOOD COUNTSRBC 332 X 106 μlHGB 96 gdlHCT 306 MCV 922 fLMCH 289 pgMCHC 314 gdlWBC 2165 X 103 microlDLC Neutrophils - 18 Lymphocytes - 15 Monocytes - 02 Eosinophils - 65 Basophils - 00PLT 45 x 103 microlAbsolute Eosinophil Count- 14 x 103microl
Peripheral blood film shows predominantly normocytic normochromic RBCs with few macrocytes Eosinophilic leukocytosis showing hypersegmentation amp cytoplasmic vacoulization Platelets are reduced(40x Leishman stain)
Bone marrow aspirates markedly diluted with peripheral blood showing eosinophils
Bone marrow aspirate showing eosinophilic myelocyte band cell amp one hypersegmented
Eosinophil with cytoplasmic vacoulization
Trephine marrow biopsy showing bony trabeculae amp hypercellular hematopoietic tissue
(10xHampE stain)
Bone marrow biopsy showing myeloid hyperplasia with increased eosinophils and eosinophilic precursors few blasts with open nuclear chromatin amp
prominent nucleoli normoblastic erythropoiesis and megakaryocytes (40xHampE stain)
Bone marrow biopsy shows predominantly eosinophilic precursors and eosinophils with granular pink red cytoplasm (40x HampE stain)
Bone marrow biopsy showing different stages of eosinophil maturation with
hypersegmented and ring eosinophil (100x HampE stain)
Bone marrow biopsy showing focal increased reticulin with few course fibres grade 2 ( 4x reticulin stain)
bull PBF ndash Eosinophilic leukocytosisbull BM Aspiration ndash Diluted bull BMB - Myeloid hyperplasia with increased
Eosinophil and its precursors and abnormal forms
bull No increase in blastsbull Increased fibrosis (MF2)
The WHO defined Myeloid malignancies associated with clonal eosinophilia ruled out by CBC PBF amp BM examination are ndash AML with inv 16 ndash no blast in PBF Blasts ˂ 20 in BM Polycythemia vera - Hb lt 165 gdl HCT lt 49 no trilineage hyperplasia on BMB Essential thrombocythemia ndash PLT decreased no increase in megakaryocytes on BMB Primary Myelofibrosis ndash No megakaryocytic proliferation and atypia CMML ndash Monocytosis absent Monocytes lt 10 of WBC count aCML - neutrophils and their precursors are not increased Systemic Mastocytosis ndash Mast cells are not seen
Myeloid neoplasms associated with eosinophilia and rearrangement
of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
Chronic eosinophilic leukemia NOS
Idiopathic Hypereosinophilic syndrome
DIFFERENTIAL DIAGNOSIS 1 Myeloid neoplasms associated with eosinophilia and rearrangement of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
2 Chronic eosinophilic leukemia NOS
3 Idiopathic Hypereosinophilic syndrome
These disorders can not be differentiated on the basis of morphology Molecularcytogenetic analysis was suggested for further categorization
Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
INVESTIGATIONS REQUIREDbull CECT abdomen and chest bull Cardiac evaluation for signs of right side heart failurebull Bone marrow aspiration and biopsybull Cytogenetic analysis of bone marrow aspiratebull Molecular analysis on peripheral blood cells for clonality of
myeloproliferative neoplasms( PDGFR FGFR rearrangements etchellip)
bull Immunophenotyping and molecular analysis for blood T cells receptor clonality
bull BCR-ABL mutation analysisbull BAL and lung biopsy
Pathological Discussion
Dr Neetu AgrawalSenior Demonstrator
Under guidance
Dr Anita HarshAssociate Professor
Department of Pathology
COMPLETE BLOOD COUNTSRBC 332 X 106 μlHGB 96 gdlHCT 306 MCV 922 fLMCH 289 pgMCHC 314 gdlWBC 2165 X 103 microlDLC Neutrophils - 18 Lymphocytes - 15 Monocytes - 02 Eosinophils - 65 Basophils - 00PLT 45 x 103 microlAbsolute Eosinophil Count- 14 x 103microl
Peripheral blood film shows predominantly normocytic normochromic RBCs with few macrocytes Eosinophilic leukocytosis showing hypersegmentation amp cytoplasmic vacoulization Platelets are reduced(40x Leishman stain)
Bone marrow aspirates markedly diluted with peripheral blood showing eosinophils
Bone marrow aspirate showing eosinophilic myelocyte band cell amp one hypersegmented
Eosinophil with cytoplasmic vacoulization
Trephine marrow biopsy showing bony trabeculae amp hypercellular hematopoietic tissue
(10xHampE stain)
Bone marrow biopsy showing myeloid hyperplasia with increased eosinophils and eosinophilic precursors few blasts with open nuclear chromatin amp
prominent nucleoli normoblastic erythropoiesis and megakaryocytes (40xHampE stain)
Bone marrow biopsy shows predominantly eosinophilic precursors and eosinophils with granular pink red cytoplasm (40x HampE stain)
Bone marrow biopsy showing different stages of eosinophil maturation with
hypersegmented and ring eosinophil (100x HampE stain)
Bone marrow biopsy showing focal increased reticulin with few course fibres grade 2 ( 4x reticulin stain)
bull PBF ndash Eosinophilic leukocytosisbull BM Aspiration ndash Diluted bull BMB - Myeloid hyperplasia with increased
Eosinophil and its precursors and abnormal forms
bull No increase in blastsbull Increased fibrosis (MF2)
The WHO defined Myeloid malignancies associated with clonal eosinophilia ruled out by CBC PBF amp BM examination are ndash AML with inv 16 ndash no blast in PBF Blasts ˂ 20 in BM Polycythemia vera - Hb lt 165 gdl HCT lt 49 no trilineage hyperplasia on BMB Essential thrombocythemia ndash PLT decreased no increase in megakaryocytes on BMB Primary Myelofibrosis ndash No megakaryocytic proliferation and atypia CMML ndash Monocytosis absent Monocytes lt 10 of WBC count aCML - neutrophils and their precursors are not increased Systemic Mastocytosis ndash Mast cells are not seen
Myeloid neoplasms associated with eosinophilia and rearrangement
of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
Chronic eosinophilic leukemia NOS
Idiopathic Hypereosinophilic syndrome
DIFFERENTIAL DIAGNOSIS 1 Myeloid neoplasms associated with eosinophilia and rearrangement of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
2 Chronic eosinophilic leukemia NOS
3 Idiopathic Hypereosinophilic syndrome
These disorders can not be differentiated on the basis of morphology Molecularcytogenetic analysis was suggested for further categorization
Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-

Pathological Discussion
Dr Neetu AgrawalSenior Demonstrator
Under guidance
Dr Anita HarshAssociate Professor
Department of Pathology
COMPLETE BLOOD COUNTSRBC 332 X 106 μlHGB 96 gdlHCT 306 MCV 922 fLMCH 289 pgMCHC 314 gdlWBC 2165 X 103 microlDLC Neutrophils - 18 Lymphocytes - 15 Monocytes - 02 Eosinophils - 65 Basophils - 00PLT 45 x 103 microlAbsolute Eosinophil Count- 14 x 103microl
Peripheral blood film shows predominantly normocytic normochromic RBCs with few macrocytes Eosinophilic leukocytosis showing hypersegmentation amp cytoplasmic vacoulization Platelets are reduced(40x Leishman stain)
Bone marrow aspirates markedly diluted with peripheral blood showing eosinophils
Bone marrow aspirate showing eosinophilic myelocyte band cell amp one hypersegmented
Eosinophil with cytoplasmic vacoulization
Trephine marrow biopsy showing bony trabeculae amp hypercellular hematopoietic tissue
(10xHampE stain)
Bone marrow biopsy showing myeloid hyperplasia with increased eosinophils and eosinophilic precursors few blasts with open nuclear chromatin amp
prominent nucleoli normoblastic erythropoiesis and megakaryocytes (40xHampE stain)
Bone marrow biopsy shows predominantly eosinophilic precursors and eosinophils with granular pink red cytoplasm (40x HampE stain)
Bone marrow biopsy showing different stages of eosinophil maturation with
hypersegmented and ring eosinophil (100x HampE stain)
Bone marrow biopsy showing focal increased reticulin with few course fibres grade 2 ( 4x reticulin stain)
bull PBF ndash Eosinophilic leukocytosisbull BM Aspiration ndash Diluted bull BMB - Myeloid hyperplasia with increased
Eosinophil and its precursors and abnormal forms
bull No increase in blastsbull Increased fibrosis (MF2)
The WHO defined Myeloid malignancies associated with clonal eosinophilia ruled out by CBC PBF amp BM examination are ndash AML with inv 16 ndash no blast in PBF Blasts ˂ 20 in BM Polycythemia vera - Hb lt 165 gdl HCT lt 49 no trilineage hyperplasia on BMB Essential thrombocythemia ndash PLT decreased no increase in megakaryocytes on BMB Primary Myelofibrosis ndash No megakaryocytic proliferation and atypia CMML ndash Monocytosis absent Monocytes lt 10 of WBC count aCML - neutrophils and their precursors are not increased Systemic Mastocytosis ndash Mast cells are not seen
Myeloid neoplasms associated with eosinophilia and rearrangement
of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
Chronic eosinophilic leukemia NOS
Idiopathic Hypereosinophilic syndrome
DIFFERENTIAL DIAGNOSIS 1 Myeloid neoplasms associated with eosinophilia and rearrangement of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
2 Chronic eosinophilic leukemia NOS
3 Idiopathic Hypereosinophilic syndrome
These disorders can not be differentiated on the basis of morphology Molecularcytogenetic analysis was suggested for further categorization
Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
COMPLETE BLOOD COUNTSRBC 332 X 106 μlHGB 96 gdlHCT 306 MCV 922 fLMCH 289 pgMCHC 314 gdlWBC 2165 X 103 microlDLC Neutrophils - 18 Lymphocytes - 15 Monocytes - 02 Eosinophils - 65 Basophils - 00PLT 45 x 103 microlAbsolute Eosinophil Count- 14 x 103microl
Peripheral blood film shows predominantly normocytic normochromic RBCs with few macrocytes Eosinophilic leukocytosis showing hypersegmentation amp cytoplasmic vacoulization Platelets are reduced(40x Leishman stain)
Bone marrow aspirates markedly diluted with peripheral blood showing eosinophils
Bone marrow aspirate showing eosinophilic myelocyte band cell amp one hypersegmented
Eosinophil with cytoplasmic vacoulization
Trephine marrow biopsy showing bony trabeculae amp hypercellular hematopoietic tissue
(10xHampE stain)
Bone marrow biopsy showing myeloid hyperplasia with increased eosinophils and eosinophilic precursors few blasts with open nuclear chromatin amp
prominent nucleoli normoblastic erythropoiesis and megakaryocytes (40xHampE stain)
Bone marrow biopsy shows predominantly eosinophilic precursors and eosinophils with granular pink red cytoplasm (40x HampE stain)
Bone marrow biopsy showing different stages of eosinophil maturation with
hypersegmented and ring eosinophil (100x HampE stain)
Bone marrow biopsy showing focal increased reticulin with few course fibres grade 2 ( 4x reticulin stain)
bull PBF ndash Eosinophilic leukocytosisbull BM Aspiration ndash Diluted bull BMB - Myeloid hyperplasia with increased
Eosinophil and its precursors and abnormal forms
bull No increase in blastsbull Increased fibrosis (MF2)
The WHO defined Myeloid malignancies associated with clonal eosinophilia ruled out by CBC PBF amp BM examination are ndash AML with inv 16 ndash no blast in PBF Blasts ˂ 20 in BM Polycythemia vera - Hb lt 165 gdl HCT lt 49 no trilineage hyperplasia on BMB Essential thrombocythemia ndash PLT decreased no increase in megakaryocytes on BMB Primary Myelofibrosis ndash No megakaryocytic proliferation and atypia CMML ndash Monocytosis absent Monocytes lt 10 of WBC count aCML - neutrophils and their precursors are not increased Systemic Mastocytosis ndash Mast cells are not seen
Myeloid neoplasms associated with eosinophilia and rearrangement
of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
Chronic eosinophilic leukemia NOS
Idiopathic Hypereosinophilic syndrome
DIFFERENTIAL DIAGNOSIS 1 Myeloid neoplasms associated with eosinophilia and rearrangement of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
2 Chronic eosinophilic leukemia NOS
3 Idiopathic Hypereosinophilic syndrome
These disorders can not be differentiated on the basis of morphology Molecularcytogenetic analysis was suggested for further categorization
Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
Peripheral blood film shows predominantly normocytic normochromic RBCs with few macrocytes Eosinophilic leukocytosis showing hypersegmentation amp cytoplasmic vacoulization Platelets are reduced(40x Leishman stain)
Bone marrow aspirates markedly diluted with peripheral blood showing eosinophils
Bone marrow aspirate showing eosinophilic myelocyte band cell amp one hypersegmented
Eosinophil with cytoplasmic vacoulization
Trephine marrow biopsy showing bony trabeculae amp hypercellular hematopoietic tissue
(10xHampE stain)
Bone marrow biopsy showing myeloid hyperplasia with increased eosinophils and eosinophilic precursors few blasts with open nuclear chromatin amp
prominent nucleoli normoblastic erythropoiesis and megakaryocytes (40xHampE stain)
Bone marrow biopsy shows predominantly eosinophilic precursors and eosinophils with granular pink red cytoplasm (40x HampE stain)
Bone marrow biopsy showing different stages of eosinophil maturation with
hypersegmented and ring eosinophil (100x HampE stain)
Bone marrow biopsy showing focal increased reticulin with few course fibres grade 2 ( 4x reticulin stain)
bull PBF ndash Eosinophilic leukocytosisbull BM Aspiration ndash Diluted bull BMB - Myeloid hyperplasia with increased
Eosinophil and its precursors and abnormal forms
bull No increase in blastsbull Increased fibrosis (MF2)
The WHO defined Myeloid malignancies associated with clonal eosinophilia ruled out by CBC PBF amp BM examination are ndash AML with inv 16 ndash no blast in PBF Blasts ˂ 20 in BM Polycythemia vera - Hb lt 165 gdl HCT lt 49 no trilineage hyperplasia on BMB Essential thrombocythemia ndash PLT decreased no increase in megakaryocytes on BMB Primary Myelofibrosis ndash No megakaryocytic proliferation and atypia CMML ndash Monocytosis absent Monocytes lt 10 of WBC count aCML - neutrophils and their precursors are not increased Systemic Mastocytosis ndash Mast cells are not seen
Myeloid neoplasms associated with eosinophilia and rearrangement
of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
Chronic eosinophilic leukemia NOS
Idiopathic Hypereosinophilic syndrome
DIFFERENTIAL DIAGNOSIS 1 Myeloid neoplasms associated with eosinophilia and rearrangement of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
2 Chronic eosinophilic leukemia NOS
3 Idiopathic Hypereosinophilic syndrome
These disorders can not be differentiated on the basis of morphology Molecularcytogenetic analysis was suggested for further categorization
Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
Bone marrow aspirates markedly diluted with peripheral blood showing eosinophils
Bone marrow aspirate showing eosinophilic myelocyte band cell amp one hypersegmented
Eosinophil with cytoplasmic vacoulization
Trephine marrow biopsy showing bony trabeculae amp hypercellular hematopoietic tissue
(10xHampE stain)
Bone marrow biopsy showing myeloid hyperplasia with increased eosinophils and eosinophilic precursors few blasts with open nuclear chromatin amp
prominent nucleoli normoblastic erythropoiesis and megakaryocytes (40xHampE stain)
Bone marrow biopsy shows predominantly eosinophilic precursors and eosinophils with granular pink red cytoplasm (40x HampE stain)
Bone marrow biopsy showing different stages of eosinophil maturation with
hypersegmented and ring eosinophil (100x HampE stain)
Bone marrow biopsy showing focal increased reticulin with few course fibres grade 2 ( 4x reticulin stain)
bull PBF ndash Eosinophilic leukocytosisbull BM Aspiration ndash Diluted bull BMB - Myeloid hyperplasia with increased
Eosinophil and its precursors and abnormal forms
bull No increase in blastsbull Increased fibrosis (MF2)
The WHO defined Myeloid malignancies associated with clonal eosinophilia ruled out by CBC PBF amp BM examination are ndash AML with inv 16 ndash no blast in PBF Blasts ˂ 20 in BM Polycythemia vera - Hb lt 165 gdl HCT lt 49 no trilineage hyperplasia on BMB Essential thrombocythemia ndash PLT decreased no increase in megakaryocytes on BMB Primary Myelofibrosis ndash No megakaryocytic proliferation and atypia CMML ndash Monocytosis absent Monocytes lt 10 of WBC count aCML - neutrophils and their precursors are not increased Systemic Mastocytosis ndash Mast cells are not seen
Myeloid neoplasms associated with eosinophilia and rearrangement
of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
Chronic eosinophilic leukemia NOS
Idiopathic Hypereosinophilic syndrome
DIFFERENTIAL DIAGNOSIS 1 Myeloid neoplasms associated with eosinophilia and rearrangement of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
2 Chronic eosinophilic leukemia NOS
3 Idiopathic Hypereosinophilic syndrome
These disorders can not be differentiated on the basis of morphology Molecularcytogenetic analysis was suggested for further categorization
Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
Bone marrow aspirate showing eosinophilic myelocyte band cell amp one hypersegmented
Eosinophil with cytoplasmic vacoulization
Trephine marrow biopsy showing bony trabeculae amp hypercellular hematopoietic tissue
(10xHampE stain)
Bone marrow biopsy showing myeloid hyperplasia with increased eosinophils and eosinophilic precursors few blasts with open nuclear chromatin amp
prominent nucleoli normoblastic erythropoiesis and megakaryocytes (40xHampE stain)
Bone marrow biopsy shows predominantly eosinophilic precursors and eosinophils with granular pink red cytoplasm (40x HampE stain)
Bone marrow biopsy showing different stages of eosinophil maturation with
hypersegmented and ring eosinophil (100x HampE stain)
Bone marrow biopsy showing focal increased reticulin with few course fibres grade 2 ( 4x reticulin stain)
bull PBF ndash Eosinophilic leukocytosisbull BM Aspiration ndash Diluted bull BMB - Myeloid hyperplasia with increased
Eosinophil and its precursors and abnormal forms
bull No increase in blastsbull Increased fibrosis (MF2)
The WHO defined Myeloid malignancies associated with clonal eosinophilia ruled out by CBC PBF amp BM examination are ndash AML with inv 16 ndash no blast in PBF Blasts ˂ 20 in BM Polycythemia vera - Hb lt 165 gdl HCT lt 49 no trilineage hyperplasia on BMB Essential thrombocythemia ndash PLT decreased no increase in megakaryocytes on BMB Primary Myelofibrosis ndash No megakaryocytic proliferation and atypia CMML ndash Monocytosis absent Monocytes lt 10 of WBC count aCML - neutrophils and their precursors are not increased Systemic Mastocytosis ndash Mast cells are not seen
Myeloid neoplasms associated with eosinophilia and rearrangement
of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
Chronic eosinophilic leukemia NOS
Idiopathic Hypereosinophilic syndrome
DIFFERENTIAL DIAGNOSIS 1 Myeloid neoplasms associated with eosinophilia and rearrangement of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
2 Chronic eosinophilic leukemia NOS
3 Idiopathic Hypereosinophilic syndrome
These disorders can not be differentiated on the basis of morphology Molecularcytogenetic analysis was suggested for further categorization
Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
Trephine marrow biopsy showing bony trabeculae amp hypercellular hematopoietic tissue
(10xHampE stain)
Bone marrow biopsy showing myeloid hyperplasia with increased eosinophils and eosinophilic precursors few blasts with open nuclear chromatin amp
prominent nucleoli normoblastic erythropoiesis and megakaryocytes (40xHampE stain)
Bone marrow biopsy shows predominantly eosinophilic precursors and eosinophils with granular pink red cytoplasm (40x HampE stain)
Bone marrow biopsy showing different stages of eosinophil maturation with
hypersegmented and ring eosinophil (100x HampE stain)
Bone marrow biopsy showing focal increased reticulin with few course fibres grade 2 ( 4x reticulin stain)
bull PBF ndash Eosinophilic leukocytosisbull BM Aspiration ndash Diluted bull BMB - Myeloid hyperplasia with increased
Eosinophil and its precursors and abnormal forms
bull No increase in blastsbull Increased fibrosis (MF2)
The WHO defined Myeloid malignancies associated with clonal eosinophilia ruled out by CBC PBF amp BM examination are ndash AML with inv 16 ndash no blast in PBF Blasts ˂ 20 in BM Polycythemia vera - Hb lt 165 gdl HCT lt 49 no trilineage hyperplasia on BMB Essential thrombocythemia ndash PLT decreased no increase in megakaryocytes on BMB Primary Myelofibrosis ndash No megakaryocytic proliferation and atypia CMML ndash Monocytosis absent Monocytes lt 10 of WBC count aCML - neutrophils and their precursors are not increased Systemic Mastocytosis ndash Mast cells are not seen
Myeloid neoplasms associated with eosinophilia and rearrangement
of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
Chronic eosinophilic leukemia NOS
Idiopathic Hypereosinophilic syndrome
DIFFERENTIAL DIAGNOSIS 1 Myeloid neoplasms associated with eosinophilia and rearrangement of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
2 Chronic eosinophilic leukemia NOS
3 Idiopathic Hypereosinophilic syndrome
These disorders can not be differentiated on the basis of morphology Molecularcytogenetic analysis was suggested for further categorization
Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
Bone marrow biopsy showing myeloid hyperplasia with increased eosinophils and eosinophilic precursors few blasts with open nuclear chromatin amp
prominent nucleoli normoblastic erythropoiesis and megakaryocytes (40xHampE stain)
Bone marrow biopsy shows predominantly eosinophilic precursors and eosinophils with granular pink red cytoplasm (40x HampE stain)
Bone marrow biopsy showing different stages of eosinophil maturation with
hypersegmented and ring eosinophil (100x HampE stain)
Bone marrow biopsy showing focal increased reticulin with few course fibres grade 2 ( 4x reticulin stain)
bull PBF ndash Eosinophilic leukocytosisbull BM Aspiration ndash Diluted bull BMB - Myeloid hyperplasia with increased
Eosinophil and its precursors and abnormal forms
bull No increase in blastsbull Increased fibrosis (MF2)
The WHO defined Myeloid malignancies associated with clonal eosinophilia ruled out by CBC PBF amp BM examination are ndash AML with inv 16 ndash no blast in PBF Blasts ˂ 20 in BM Polycythemia vera - Hb lt 165 gdl HCT lt 49 no trilineage hyperplasia on BMB Essential thrombocythemia ndash PLT decreased no increase in megakaryocytes on BMB Primary Myelofibrosis ndash No megakaryocytic proliferation and atypia CMML ndash Monocytosis absent Monocytes lt 10 of WBC count aCML - neutrophils and their precursors are not increased Systemic Mastocytosis ndash Mast cells are not seen
Myeloid neoplasms associated with eosinophilia and rearrangement
of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
Chronic eosinophilic leukemia NOS
Idiopathic Hypereosinophilic syndrome
DIFFERENTIAL DIAGNOSIS 1 Myeloid neoplasms associated with eosinophilia and rearrangement of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
2 Chronic eosinophilic leukemia NOS
3 Idiopathic Hypereosinophilic syndrome
These disorders can not be differentiated on the basis of morphology Molecularcytogenetic analysis was suggested for further categorization
Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
Bone marrow biopsy shows predominantly eosinophilic precursors and eosinophils with granular pink red cytoplasm (40x HampE stain)
Bone marrow biopsy showing different stages of eosinophil maturation with
hypersegmented and ring eosinophil (100x HampE stain)
Bone marrow biopsy showing focal increased reticulin with few course fibres grade 2 ( 4x reticulin stain)
bull PBF ndash Eosinophilic leukocytosisbull BM Aspiration ndash Diluted bull BMB - Myeloid hyperplasia with increased
Eosinophil and its precursors and abnormal forms
bull No increase in blastsbull Increased fibrosis (MF2)
The WHO defined Myeloid malignancies associated with clonal eosinophilia ruled out by CBC PBF amp BM examination are ndash AML with inv 16 ndash no blast in PBF Blasts ˂ 20 in BM Polycythemia vera - Hb lt 165 gdl HCT lt 49 no trilineage hyperplasia on BMB Essential thrombocythemia ndash PLT decreased no increase in megakaryocytes on BMB Primary Myelofibrosis ndash No megakaryocytic proliferation and atypia CMML ndash Monocytosis absent Monocytes lt 10 of WBC count aCML - neutrophils and their precursors are not increased Systemic Mastocytosis ndash Mast cells are not seen
Myeloid neoplasms associated with eosinophilia and rearrangement
of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
Chronic eosinophilic leukemia NOS
Idiopathic Hypereosinophilic syndrome
DIFFERENTIAL DIAGNOSIS 1 Myeloid neoplasms associated with eosinophilia and rearrangement of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
2 Chronic eosinophilic leukemia NOS
3 Idiopathic Hypereosinophilic syndrome
These disorders can not be differentiated on the basis of morphology Molecularcytogenetic analysis was suggested for further categorization
Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
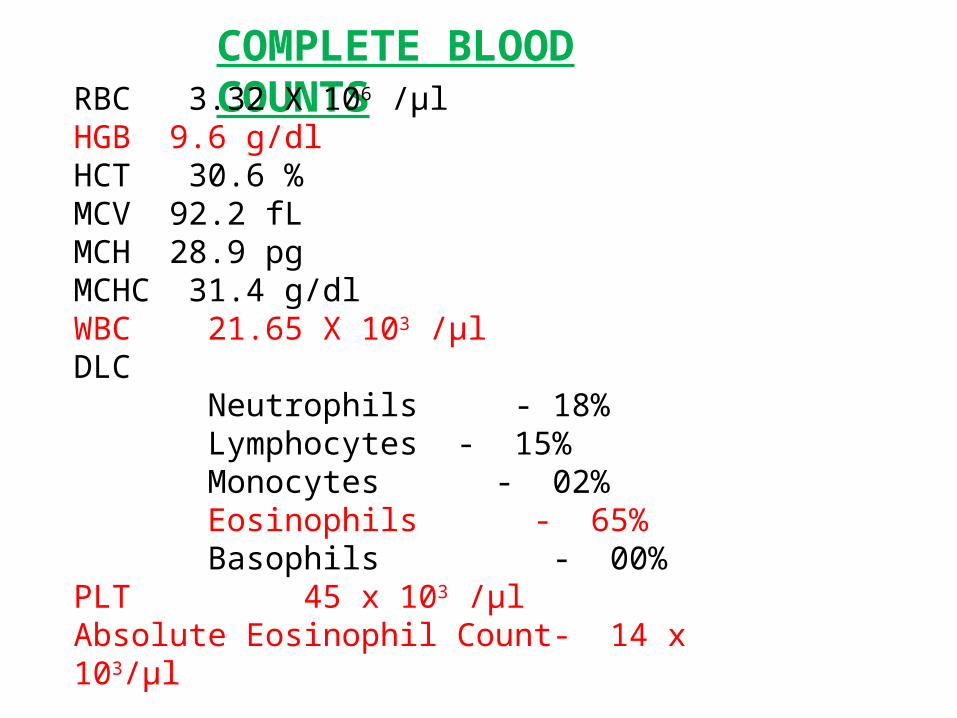
Bone marrow biopsy showing different stages of eosinophil maturation with
hypersegmented and ring eosinophil (100x HampE stain)
Bone marrow biopsy showing focal increased reticulin with few course fibres grade 2 ( 4x reticulin stain)
bull PBF ndash Eosinophilic leukocytosisbull BM Aspiration ndash Diluted bull BMB - Myeloid hyperplasia with increased
Eosinophil and its precursors and abnormal forms
bull No increase in blastsbull Increased fibrosis (MF2)
The WHO defined Myeloid malignancies associated with clonal eosinophilia ruled out by CBC PBF amp BM examination are ndash AML with inv 16 ndash no blast in PBF Blasts ˂ 20 in BM Polycythemia vera - Hb lt 165 gdl HCT lt 49 no trilineage hyperplasia on BMB Essential thrombocythemia ndash PLT decreased no increase in megakaryocytes on BMB Primary Myelofibrosis ndash No megakaryocytic proliferation and atypia CMML ndash Monocytosis absent Monocytes lt 10 of WBC count aCML - neutrophils and their precursors are not increased Systemic Mastocytosis ndash Mast cells are not seen
Myeloid neoplasms associated with eosinophilia and rearrangement
of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
Chronic eosinophilic leukemia NOS
Idiopathic Hypereosinophilic syndrome
DIFFERENTIAL DIAGNOSIS 1 Myeloid neoplasms associated with eosinophilia and rearrangement of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
2 Chronic eosinophilic leukemia NOS
3 Idiopathic Hypereosinophilic syndrome
These disorders can not be differentiated on the basis of morphology Molecularcytogenetic analysis was suggested for further categorization
Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
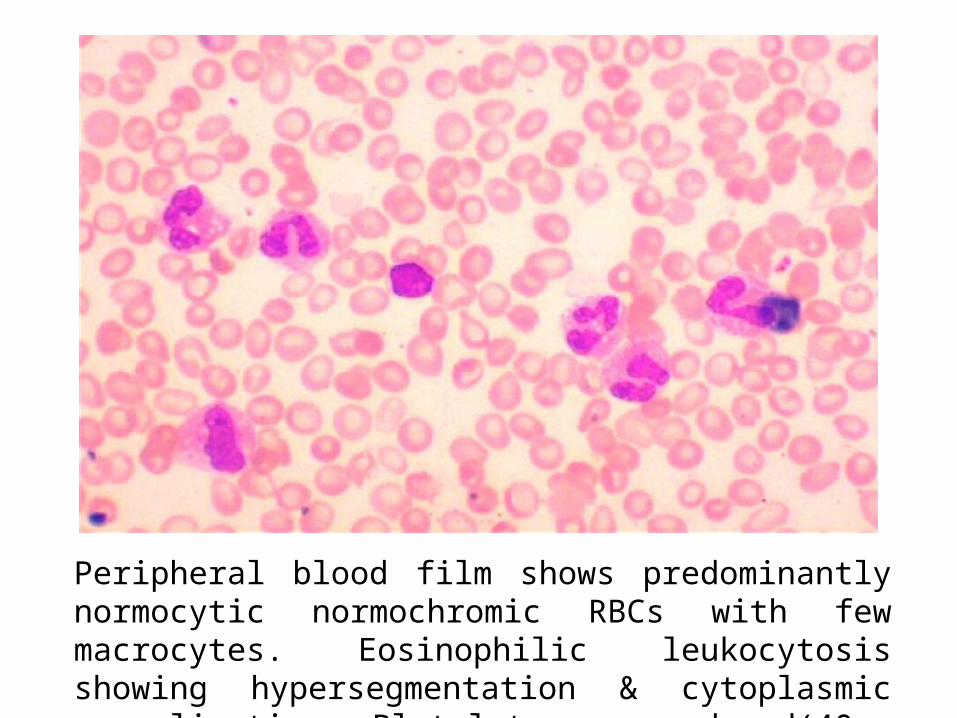
Bone marrow biopsy showing focal increased reticulin with few course fibres grade 2 ( 4x reticulin stain)
bull PBF ndash Eosinophilic leukocytosisbull BM Aspiration ndash Diluted bull BMB - Myeloid hyperplasia with increased
Eosinophil and its precursors and abnormal forms
bull No increase in blastsbull Increased fibrosis (MF2)
The WHO defined Myeloid malignancies associated with clonal eosinophilia ruled out by CBC PBF amp BM examination are ndash AML with inv 16 ndash no blast in PBF Blasts ˂ 20 in BM Polycythemia vera - Hb lt 165 gdl HCT lt 49 no trilineage hyperplasia on BMB Essential thrombocythemia ndash PLT decreased no increase in megakaryocytes on BMB Primary Myelofibrosis ndash No megakaryocytic proliferation and atypia CMML ndash Monocytosis absent Monocytes lt 10 of WBC count aCML - neutrophils and their precursors are not increased Systemic Mastocytosis ndash Mast cells are not seen
Myeloid neoplasms associated with eosinophilia and rearrangement
of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
Chronic eosinophilic leukemia NOS
Idiopathic Hypereosinophilic syndrome
DIFFERENTIAL DIAGNOSIS 1 Myeloid neoplasms associated with eosinophilia and rearrangement of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
2 Chronic eosinophilic leukemia NOS
3 Idiopathic Hypereosinophilic syndrome
These disorders can not be differentiated on the basis of morphology Molecularcytogenetic analysis was suggested for further categorization
Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-

bull PBF ndash Eosinophilic leukocytosisbull BM Aspiration ndash Diluted bull BMB - Myeloid hyperplasia with increased
Eosinophil and its precursors and abnormal forms
bull No increase in blastsbull Increased fibrosis (MF2)
The WHO defined Myeloid malignancies associated with clonal eosinophilia ruled out by CBC PBF amp BM examination are ndash AML with inv 16 ndash no blast in PBF Blasts ˂ 20 in BM Polycythemia vera - Hb lt 165 gdl HCT lt 49 no trilineage hyperplasia on BMB Essential thrombocythemia ndash PLT decreased no increase in megakaryocytes on BMB Primary Myelofibrosis ndash No megakaryocytic proliferation and atypia CMML ndash Monocytosis absent Monocytes lt 10 of WBC count aCML - neutrophils and their precursors are not increased Systemic Mastocytosis ndash Mast cells are not seen
Myeloid neoplasms associated with eosinophilia and rearrangement
of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
Chronic eosinophilic leukemia NOS
Idiopathic Hypereosinophilic syndrome
DIFFERENTIAL DIAGNOSIS 1 Myeloid neoplasms associated with eosinophilia and rearrangement of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
2 Chronic eosinophilic leukemia NOS
3 Idiopathic Hypereosinophilic syndrome
These disorders can not be differentiated on the basis of morphology Molecularcytogenetic analysis was suggested for further categorization
Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
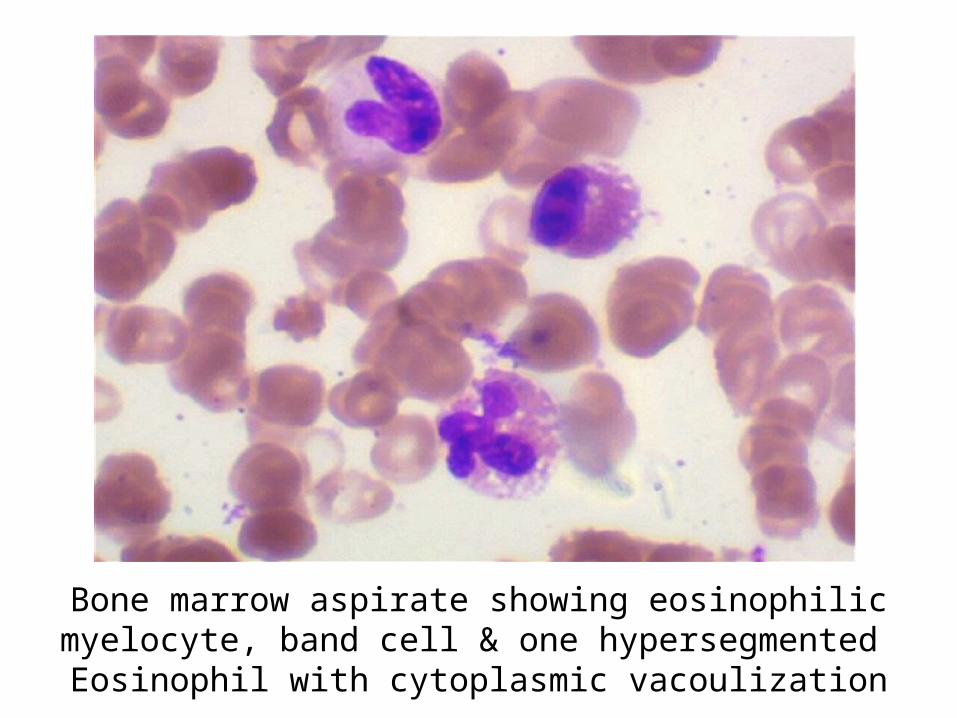
The WHO defined Myeloid malignancies associated with clonal eosinophilia ruled out by CBC PBF amp BM examination are ndash AML with inv 16 ndash no blast in PBF Blasts ˂ 20 in BM Polycythemia vera - Hb lt 165 gdl HCT lt 49 no trilineage hyperplasia on BMB Essential thrombocythemia ndash PLT decreased no increase in megakaryocytes on BMB Primary Myelofibrosis ndash No megakaryocytic proliferation and atypia CMML ndash Monocytosis absent Monocytes lt 10 of WBC count aCML - neutrophils and their precursors are not increased Systemic Mastocytosis ndash Mast cells are not seen
Myeloid neoplasms associated with eosinophilia and rearrangement
of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
Chronic eosinophilic leukemia NOS
Idiopathic Hypereosinophilic syndrome
DIFFERENTIAL DIAGNOSIS 1 Myeloid neoplasms associated with eosinophilia and rearrangement of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
2 Chronic eosinophilic leukemia NOS
3 Idiopathic Hypereosinophilic syndrome
These disorders can not be differentiated on the basis of morphology Molecularcytogenetic analysis was suggested for further categorization
Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
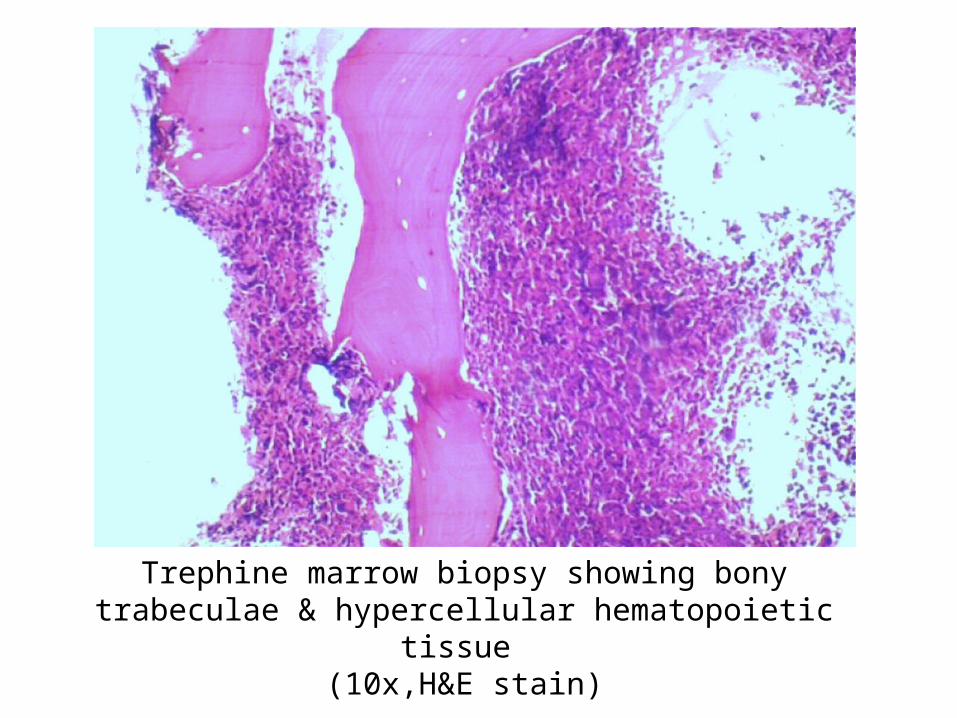
DIFFERENTIAL DIAGNOSIS 1 Myeloid neoplasms associated with eosinophilia and rearrangement of PDGFRA PDGFRB or FGFR1 or with PCM1-JAK2
2 Chronic eosinophilic leukemia NOS
3 Idiopathic Hypereosinophilic syndrome
These disorders can not be differentiated on the basis of morphology Molecularcytogenetic analysis was suggested for further categorization
Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-

Molecular analysis for BCR-ABL was negative
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
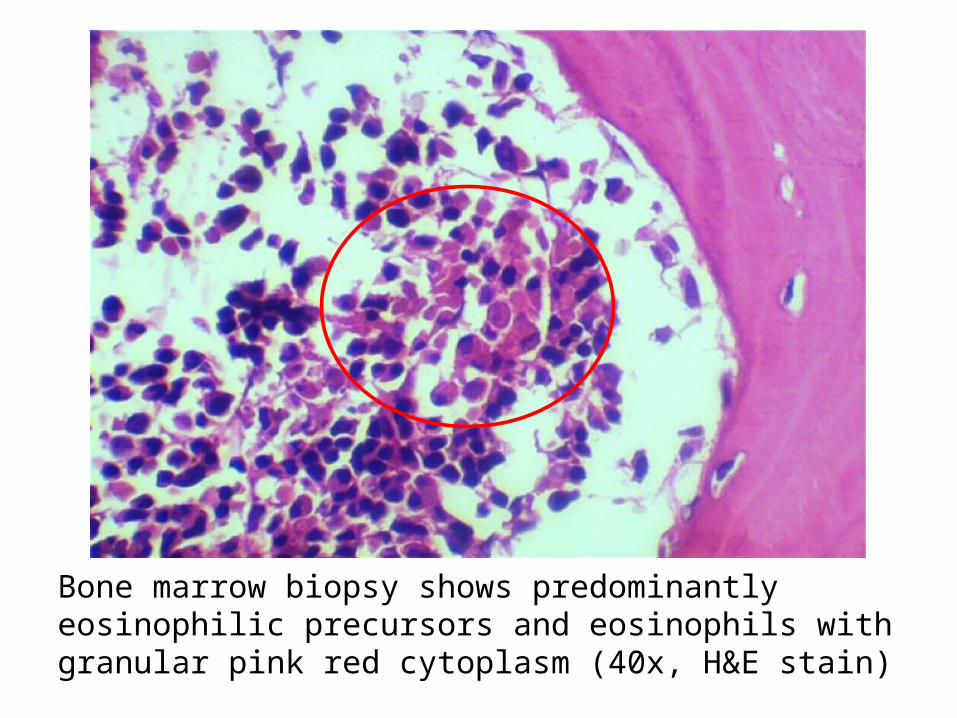
Molecular analysis for FIP1L1-PDGFRA rearrangement was done and detected positive
DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-

DIAGNOSIS
Myeloid neoplasm with eosinophilia and FIP1L1-PDGFRA rearrangement presenting as chronic eosinophilic leukemia or(Chronic eosinophilic leukemia with FIP1L1-PDGFRA rearrangement)
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
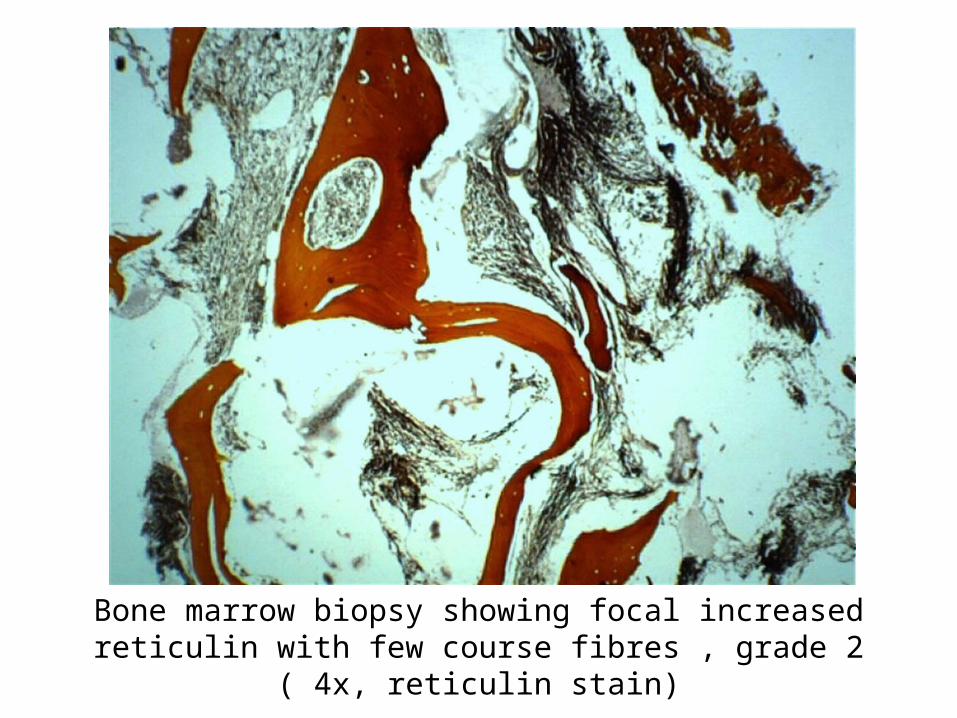
bull BRONCHOALVEOLAR LAVAGE FLUID
Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-

Bronchoalveolar Lavage fluid shows many pigment laden macrophages histiocytes amp
Few lymphocytes No eosinophil seen
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
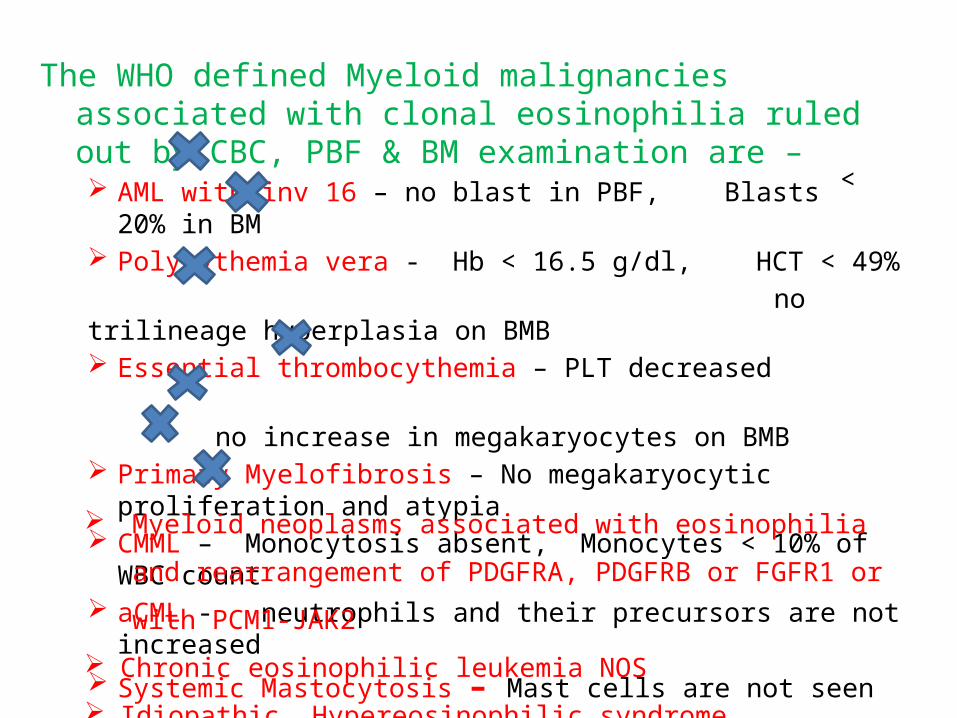
bullLUNG BIOPSY
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
Lung biopsy shows mild destruction of lung parenchyma with thickening of septa mild mononuclear cell infiltration amp patchy areas of fibrosis - favours UIP(10xHampE stain)
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
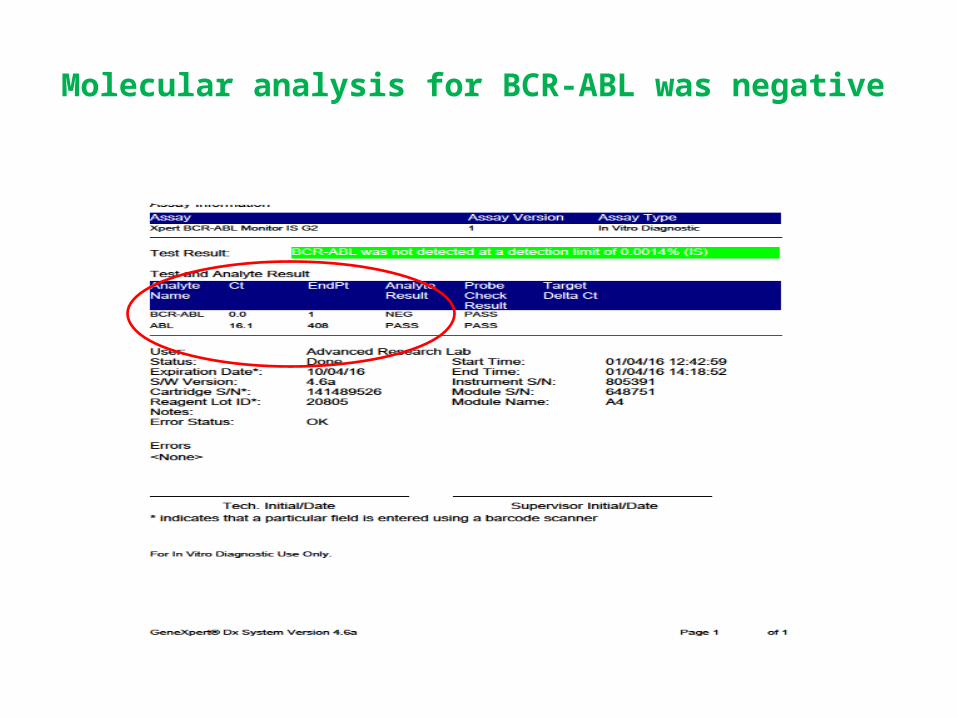
Focal area on lung biopsy showing histiocytes amp lymphocytes (40xHampE stain)
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
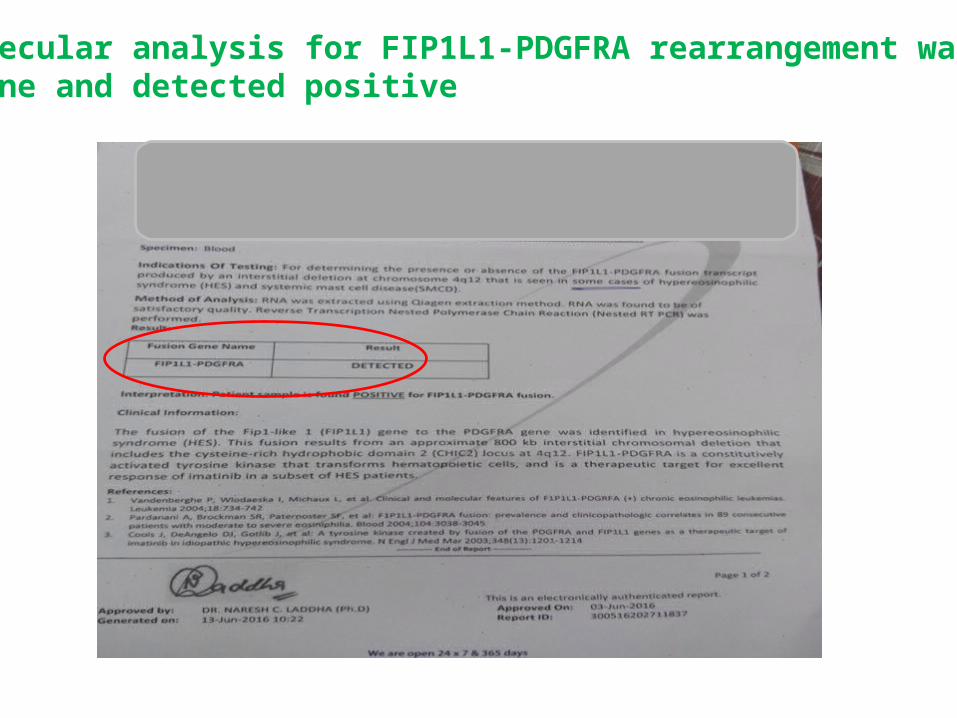
Lung biopsy shows blue stained areas of patchy fibrosis (10xMassonrsquos Trichome stain)
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
UIP Pattern of fibrosis
bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-

bullENDOMYOCARDIAL BIOPSY
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
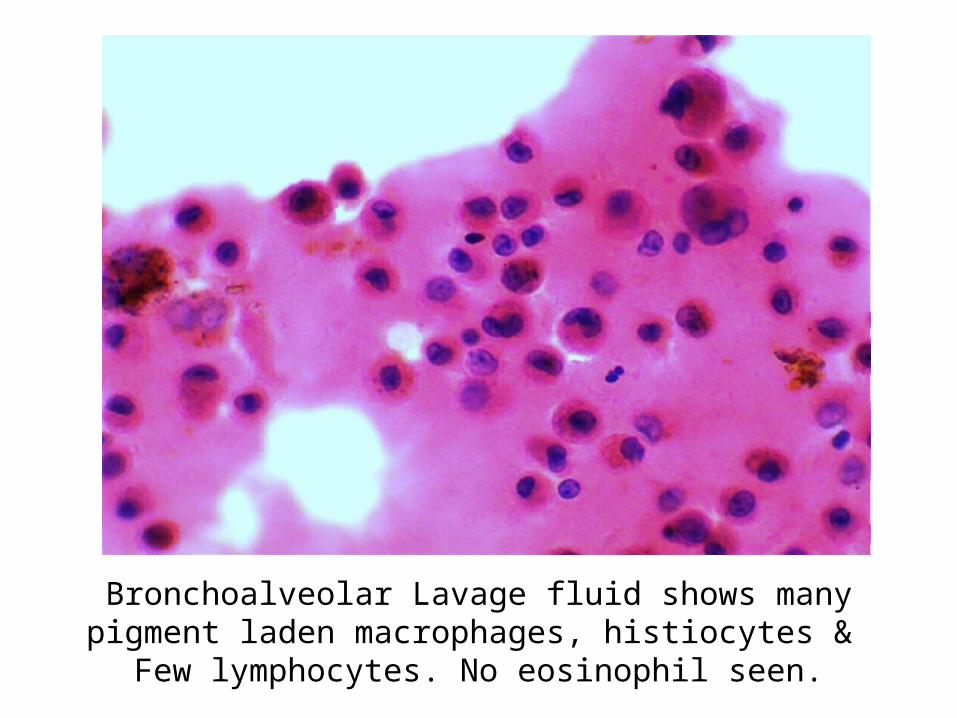
Endomyocardial biopsy showing only haemorrhage and blood clots (10xHampE stain)
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
CONCLUSION
Chronic Eosinophilic leukemia with FIP1L1 ndash PDGFRA rearrangement with organ involvement
Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-

Case Presenter
Dr Daulat Singh MeenaIIIrd Year Resident
Department of Cardiology
Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-

Case summary 38 year old male having 12 months history of progressive dyspnea fever cough weight loss and pedal edema examination reveal bilateral pneumonitis right sided heart failure with hepatosplenomegaly and investigations showed hypereosinophilia with elevated B12 and CPKMB
bull HRCT - Multiple nodular opacities with peripheral ground glass haziness in bilateral lung fields and pleural effusion- secondary to hypereosinophilia
bull ECHOCATHMRI- RCMP with biventricular apical obliteration with severe TR and moderate MR ndash Loffer endocarditis
bull PBF- Eosinophilic leukocytosis BMB - Myeloid hyperplasia with increased Eosinophil with no increase in blasts cells
bull Lung biopsy- favours UIPbull FIP1L1-PDGFRA rearrangement- positive
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
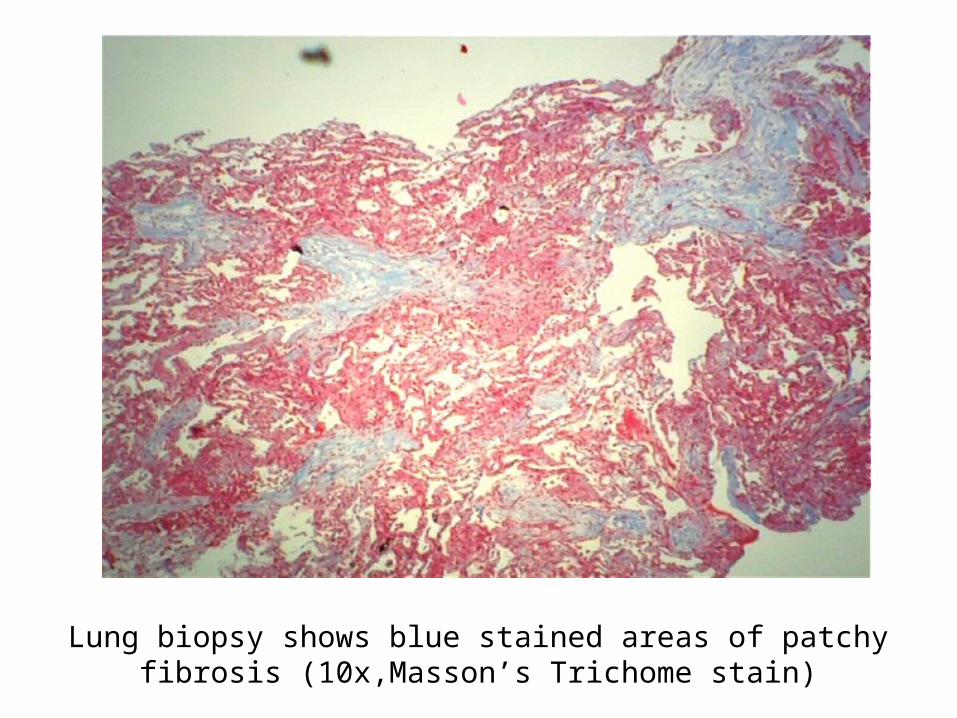
Final Diagnosis
bull Chronic eosinophilic leukemia with Fip-1 like 1-platelet derived growth factor receptor alpha (FIP 1L1-PDGRA) mutation with Lofflers endocarditis with pneumonitis
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
CEL-FIP1L1-PDGFRA fusion gene
bull FIP1L1-PDGFRA fusion gene detectable in 5 to 15 of all cases with clonal HE
bull The most common presenting signs and symptoms were weakness and fatigue (26) cough (24) dyspnea (16)
bull The organ most frequently affected are the heart and it also involve skin the nervous system and the respiratory and gastrointestinal tract up to 20 cases
bull FP mutation positive patient will have more aggressive course and severe fibrotic complications including endomyocardial fibrosis restrictive pulmonary disease and myelofibrosis
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
bullThe associations among eosinophilia active carditis and multiorgan involvement were first described by Loeffler in 1936
1Necrotic stage (early stage)
2Thrombotic stage
3Fibrotic stage (late stage) Restrictive myopathy
AV valvular regurgitationRight and left heart failure
Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-

Management of Loffler endocarditis
Symptomatic ndash ndash Diuretics Ace inhibitors B-blocker and anticoagulation (in case
with history of embolic phenomena or presence of LV clot)
Surgical Endocardiectomy - ndash Heart failure refractory to medical therapyndash Operative mortality rate of 15-29
AV valve repair and replacendash Patient with severe AV valvular regurgitation may be subject to
replacement or repair depending on the involvement of the subchordal apparatus
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
Follow upndash Once patient have hematological remission patient should be followed up in every 3-6
months for hematological and clinical evaluation
Prognosis CEL WITH FIP 1L1-PDGFRA positive
ndash Imatinib in PDGFRA disease really changed the natural history of HE Patients passed from a 2-year survival of 55 without imatinib to a 10-year survival of 90 with imatinib
Loffler endocarditis- ndash Substantially better survival rates in patients who presented in early stage of diseasendash 35-50 2-year mortality rate in patients presented with advanced myocardial fibrosis
Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-

Follow up bull Pt started on Tab Imatinib 400mg OD with Steroids 1mgkgbull 27th may 2016 20june2016bull `RBC 332 X 10^6Ulbull HGB 96 gdl 100 bull HCT 306 313bull MCV 922fL 928fL bull MCH 289pg 295pgbull MCHC 314gdl 318gdlbull WBC 2165 X 10^3ul 42X 10^3ulbull DLC bull neutrophils -18 573bull Lymphocytes - 15 382bull Monocytes - 02 24bull Eosinophils - 65 14bull Basophils - 00 07bull PLT 45 x 10^3uL 11lac
bull Absolute Eosinophil Count- 14 x 10^3ul 60ul
Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-

Chest X-Ray PA view AP viewhellipMay 2016 PA viewhellipJune 2016
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
HRCT Chest
May 2016 June 2016
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
Take home massage bull Not all cases of hypereosinophilia are reactive and secondary
to parasite infestation
bull Clinical suspicion of myloproliferative neoplasm with hypereosinophilia is essential for early diagnosis to limit morbidity and mortality associated with cardiac involvement
bull Imatinib is drug of choice in presence of PDGRFAB positive mutation which suggest importance of mutation analysis
bull Steroids should always added in patients with elevated serum troponin level andor ECHO finding suggestive cardiac involvement to prevent acute myocardial necrosis
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-
- SMS Medical College Jaipur CPC Meetings Conducted By Medical
- SMSMC-CPC The TEAM
- SMSMC-CPC
- SMSMC-CPC Format
- Next CPC
- INTRODUCTION
- History
- Slide 8
- Slide 9
- PRESENT SCENARIO OF THE DEPARTMENT
- Slide 11
- CATH LAB 1
- Slide 13
- CATH LAB CONSOLE
- ECHO LAB
- Slide 16
- Slide 17
- Research Activities
- Slide 19
- Slide 20
- Slide 21
- CPC case Department Cardiology 8th July 2016
- Case Presenter
- Presenting complaints
- History of presenting illness
- History of presenting illness (2)
- History of presenting illness (3)
- History of presenting illness (4)
- History of presenting illness (5)
- History of presenting illness (6)
- History of presenting illness (7)
- Past medical history
- Personal history
- Family history
- Examination findings
- Slide 36
- Respiratory system examination
- CVS system examination
- Abdominal examination
- Summary
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Chest X-Ray PA view
- Slide 46
- Conclude
- Slide 48
- Cause of hyper-eosinophilia
- Cause of hyper-eosinophilia (2)
- DIFFERENTIALS RULED OUT ON THE BASIS OF CLINICAL HISTORY AND PR
- Slide 52
- Respiratory discussion
- PULMONARY INFILTRATES WITH EOSINOPHILIA
- Acute eosinophilic pneumonia
- Acute eosinophilic pneumonia (2)
- Allergic bronchopulmonary aspergillosis (ABPA)
- Allergic bronchopulmonary aspergillosis (ABPA) (2)
- Skin prick test for Aspergillus
- Churg Strauss syndrome
- Churg Strauss syndrome (2)
- Loefflerrsquos pneumonia
- Loefflerrsquos pneumonia (2)
- PULMONARY INFILTRATES WITH EOSINOPHILIA (2)
- How to proceed
- Algorithm of management
- Medicine discussion
- Slide 68
- INVESTIGATIONS REQUIRED
- Autoimmune and Connective tissue disorder
- LEUKEMIAS
- TUMOURS ASSOCIATED
- OTHER MPNMDS ASSOCIATED WITH EOSINOPHILLIA
- LYMPHOPROLIFERATIVE TYPE HES
- MYELOPROLIFERATIVE HYPEREOSINOPHILIC SYNDROMES
- Slide 76
- Slide 77
- INVESTIGATIONS REQUIRED (2)
- Radiological discussion
- Chest X-Ray PA view -normal
- CECT Chest ndashnormal (on sept 222015)
- Chest radiographs showing bilateral multiple patchy air space h
- HRCT (Axial and Coronal) is showing multiple nodular opacities
- CECT chest is showing sub-centimetric mediastinal lymph nodes
- CECT abdomen revealed mild hepatosplenomegaly There was no ev
- Differential diagnosis of nodules with ground glass pattern wi
- Slide 87
- Chronic eosinophilic pneumonia
- SARCOIDOSIS
- TUMOURS ASSOCIATED (2)
- Hypereosinophilic syndrome
- Slide 92
- Cardiology discussion
- Cardiovascular involvement differentials
- Slide 95
- Slide 96
- Slide 97
- Slide 98
- Normal apical 4 chamber
- Slide 100
- Slide 101
- Slide 102
- Slide 103
- Slide 104
- Slide 105
- Slide 106
- Slide 107
- Slide 108
- Slide 109
- LV Pressure tracing
- RV pressure tracing
- RA Pressure tracing
- PA pressure tracing
- Normal LV angiogram
- LV angiogram
- RV angiogram
- CATH study analysis
- Cardiovascular involvement differentials (2)
- Endomyocardial biopsy
- Slide 120
- Radiological discussion (2)
- Bright blood 2 chamber cine MRI is showing left ventricular api
- Bright blood 4 chamber cine MRI is showing left ventricular ap
- Early post contrast MR images are showing subendocardial enhan
- Delayed post contrast MR images are showing subendocardial e
- Differential diagnosis of delayed contrast e
- Amyloidosis
- Endomyocardial fibrosisLoefflers endocarditis
- Case Presenter
- Cardiovascular involvement differentials (3)
- Endomyocardial fibrosis(MF)
- Lofflers endocarditis
- Cardiovascular involvement differentials (4)
- Diagnosis
- Slide 135
- INVESTIGATIONS REQUIRED (3)
- Pathological Discussion
- Slide 138
- Slide 139
- Bone marrow aspirates markedly diluted with peripheral blood sh
- Bone marrow aspirate showing eosinophilic myelocyte band cell
- Trephine marrow biopsy showing bony trabeculae amp hypercellular
- Bone marrow biopsy showing myeloid hyperplasia with increased e
- Bone marrow biopsy shows predominantly eosinophilic precursors
- Bone marrow biopsy showing different stages of eosinophil
- Bone marrow biopsy showing focal increased reticulin with few c
- Slide 147
- Slide 148
- Slide 149
- Slide 150
- Slide 151
- Slide 152
- Slide 153
- Bronchoalveolar Lavage fluid shows many pigment laden macrophag
- Slide 155
- Lung biopsy shows mild destruction of lung parenchyma with thic
- Focal area on lung biopsy showing histiocytes amp lymphocytes (40
- Lung biopsy shows blue stained areas of patchy fibrosis (10xMa
- Slide 159
- Slide 160
- Endomyocardial biopsy showing only haemorrhage and blood clots
- Slide 162
- Case Presenter (2)
- Case summary
- Final Diagnosis
- CEL-FIP1L1-PDGFRA fusion gene
- Slide 167
- Slide 168
- Management of Loffler endocarditis
- Slide 170
- Follow up
- Chest X-Ray PA view (2)
- HRCT Chest
- Take home massage
- Slide 175
- Slide 176
- Slide 177
-