cp unknown reeba omman, pgy-1 dr. girish venkataraman dr. philip dechristopher
TRANSCRIPT

CP UNKNOWN
Reeba Omman, PGY-1
Dr. Girish Venkataraman
Dr. Philip DeChristopher

59/M PB smear from core lab for path review: Funny looking immature cells?

What should be the next step in the work up?1.Review the entire smear2.Flow? 3.Review the chart-for what?4.Pick up the phone and call clinician with blasts in blood?

• 59 y/o hispanic male DLBCL of stomach in 01/2010
• Completed 6 cycles of CHOP 6/2010• Follow up EGD 9/9/2011 suggestive of
recurrent disease• 10/2011 – PET scan shows increased uptake in
fundus and adjacent lymph node• s/p one cycle of ICE (ifosfamide, etoposide
and carboplatin) finished 3 weeks ago• Presents for cycle 2 of ICE
Clinical History-11/16/2011

• LymphomaLymphoma• LeukemiaLeukemia• Systemic/Organ specific Systemic/Organ specific
infectioninfection–Bacterial, fungal, viralBacterial, fungal, viral
• DrugsDrugs–G-CSFG-CSF–Valproic acid, GanciclovirValproic acid, Ganciclovir

Toxic granulation with Dohle bodies
Additional areas of the same smear

Toxic Vacuolization
Additional areas of the same smear

Left shift leukocytosis

More pertinent patient History
• Patient asymptomatic, afebrile, blood cultures negative
• On Neulasta (Peg-G-CSF) since 10/30/2011
• Diagnosis:– G-CSF related toxic changes and rare blasts in
peripheral blood smear
What is G-CSF?
• Granulocyte Colony Stimulating Factor– Glycoprotein– Growth factor– Cytokine
• Produced by endothelium, macrophages and other immune cells
• G-CSF receptor present on precursor cells in the bone marrow– Initiates proliferation and differentiation into mature
granulocytes– Stimulates bone marrow cell release into circulation
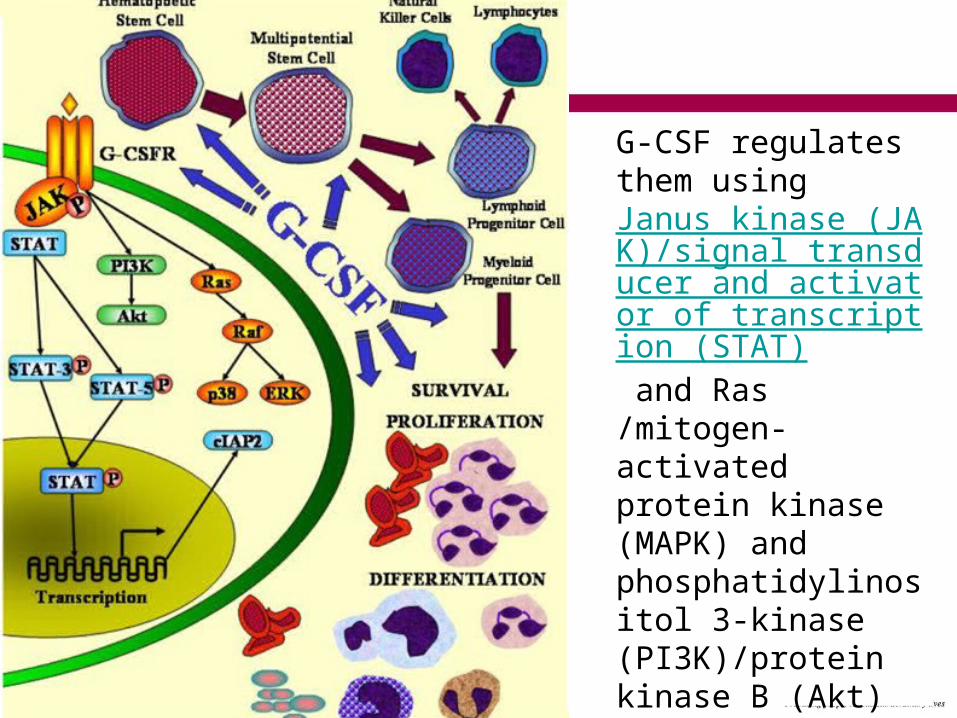
G-CSF regulates them using Janus kinase (JAK)/signal transducer and activator of transcription (STAT) and Ras /mitogen-activated protein kinase (MAPK) and phosphatidylinositol 3-kinase (PI3K)/protein kinase B (Akt) signal transduction pathway.

• FILGRASTIM (G-CSF) regulates the production of neutrophils within the bone marrow and affects neutrophil progenitor proliferation, differentiation and functional activation
• PEGFILGRASTIM (Pegylated G-CSF) – pegylated form of recombinant filgrastim– covalently binding 20-kD pegylated molecule to the N-
terminus of filgrastim• SAGRAMOSTIM (GM-CSF) stimulates myelopoiesis
generally, and neutrophils and monocytes specifically
Types of Colony Stimulating Factors

Two important G-CSF uses
1. MOST COMMON: Post chemotherapy febrile neutropenia
– 2006 ASCO Update on CSF use – Evidence Based Clinical Practice Guideline
• When the risk of febrile neutropenia is 20% and no other equally effective regimen is available
– Age
– Medical History
– Disease characteristics
– Myelotoxicity of the chemotherapy regimen
– Does not compromise dose intensity
– Reduces dose delays
2. Potent inducer of hematopoietic stem cell mobilization for stem cell transplantation (SCT)

G-CSF (Filgrastim)
Pegylated G-CSF (Pegfilgrastim)
GM-CSF (Sargramostim)
Clinical Use -after 24 hrs
-daily dose for 7-14 days
-lasts 24 hrs
-for inpatients
-one dose
-2 weeks
-for outpatients (billing issue)
-similar to G-CSF
-rare
-after BM transplant if patient has invasive fungal infection (increases monocytes)
G-CSF and post chemotherapy FN


Left Shift Leukocytosis

Toxic Granulation
• Large purple or dark blue granules– Similar to primary granules of
promyelocytes, metamyelocytes, bands and segmented neutrophils
– That are retained in mature neutrophils
– More deeply staining than normal
• Due to enhanced lysosomal enzyme production and packaging
– Associated conditions:• Infection, trauma, burns

Dohle Body
• In association with neutrophil activation: toxic granulation and vacuolization
• Single or multiple blue to gray blue inclusions of variable size and shape
• Denatured aggregates of free ribosomes or stacks of rough endoplasmic reticulum
• Usually in neutrophils, bands and metamyelocytes
• Associated conditions:– May-Hegglin anomaly, Alder’s
anomaly, infection, trauma, burns, pregnancy

Toxic Vacuolization
• Round clear spaces in cytoplasm– Sites of digestion of
phagocytized material
• Larger and more numerous; may coalesce and appear to disrupt the cytoplasm
• More prominent vs. degenerating neutrophils
• Associated conditions:– May-Hegglin anomaly,
Alder’s anomaly, infection, trauma, burns and pregnancy
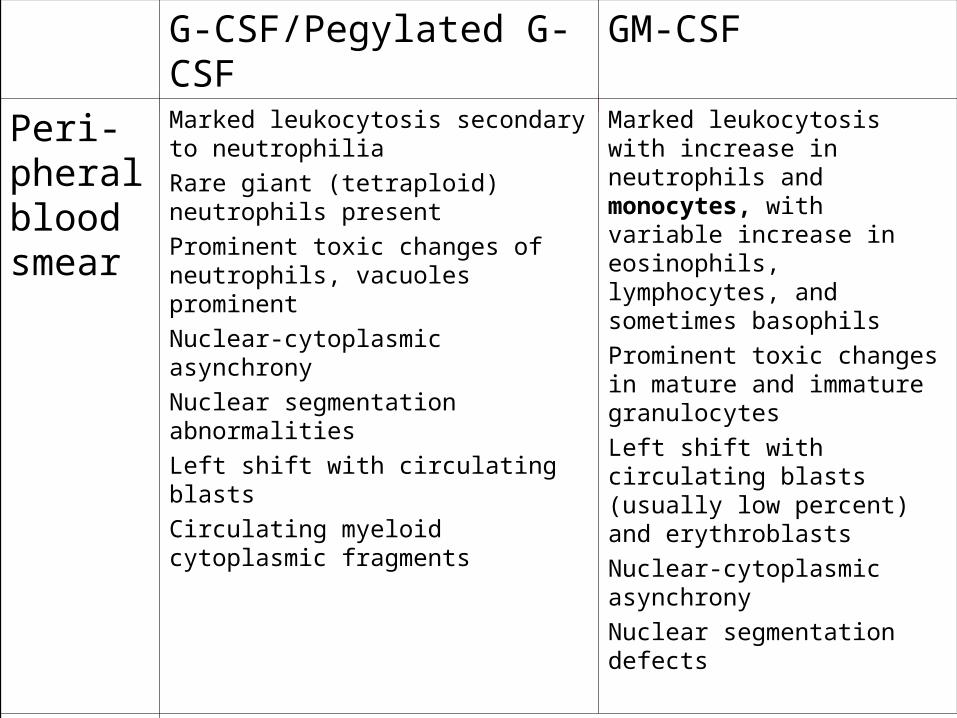
G-CSF/Pegylated G-CSF GM-CSF
Peri-pheral blood smear
Marked leukocytosis secondary to neutrophilia
Rare giant (tetraploid) neutrophils present
Prominent toxic changes of neutrophils, vacuoles prominent
Nuclear-cytoplasmic asynchrony
Nuclear segmentation abnormalities
Left shift with circulating blasts
Circulating myeloid cytoplasmic fragments
Marked leukocytosis with increase in neutrophils and monocytes, with variable increase in eosinophils, lymphocytes, and sometimes basophils
Prominent toxic changes in mature and immature granulocytes
Left shift with circulating blasts (usually low percent) and erythroblasts
Nuclear-cytoplasmic asynchrony
Nuclear segmentation defects
Bone marrow
Early: interstitial foci of granulocyte precursors in hypocellular bone marrow
Increased cellularity with left shift in hematopoietic elements
Promyelocytic hyperplasia with reactive features during early phase of therapy
Pronounced toxic changes of immature and mature granulocytic elements
Occasional binucleate promyelocytes and myelocytes
Rare: fibrosis with bony changes, acute bone marrow necrosis
Histiocytic proliferation (GM-CSF plus G-CSF)

Peripheral blood stem cell mobilization (PBSC)
• Advantage of PBSCs over steady-state marrow stem cells has more rapid hematologic reconstitution following transplantation
• G-CSF is standard mobilizing agent (other agents are chemotherapy and chemokines)– Mobilizes more CD34+ with less toxicity – G-CSF > Peg G-CSF

G-CSF and PBSC Mobilization
• On Day 4 or 5 after G-CSF therapy, peripheral blood CD34 level is measured
• If CD34 level is above (5-20 CD34 cells/uL), apheresis begins
• Poor mobilization factors:– Increasing age, increasing cycles and regimens of
chemotherapy, prior radiation to active marrow sites, prior treatment with purine analogues, female gender
• Side effects:– Injection site erythema, bone pain, HA, fever, splenic
rupture (rare)

• Advantages
– Predictability of apheresis
• CD34 cells enter circulation on 4th or 5th day
– Combination of G-CSF and GM-CSF is good for “poor mobilizer” population
• 10 or more cycles of chemotherapy, platinum-based chemotherapy, radiation to marrow sites
G-CSF and PBSC Mobilization

Pheresis collection post G-CSF therapy Pheresis collection post G-CSF therapy

References• 2006 Update of ASCO Practice Guideline Recommendations for the Use of
White Blood Cell Growth Factors: Guideline Summary. Journal of Oncology Practice, vol 2. July 2006.
• ASH Image Bank. American Society of Hematology Publications. http://imagebank.hematology.org/
• “Blast crisis: Differential Diagnosis” BMJ Publishing Group Limited 2011. http://bestpractice.bmj.com/best-practice/monograph/1026/diagnosis/differential.html
• “Benign White Cell Disorders: Leukocytosis” Pathology Thread. University of Virginia School of Medicine. http://www.med-ed.virginia.edu/courses/path/innes/wcd/leukocytosis.cfm
• Glassy, Eric F. Color Atlas of Hematology. CAP Hematology and Clinical Microscopy Resource Committee. 1998.
• Wingard et al. Hematopoietic Stem Cell Transplantation. AABB. Bethesda, Maryland. 2009.
• “Neuroprotective effect of Granulocyte colony stimulating factor” Frontiers in Bioscience 12, 712-724, January 1. 2007.http://www.bioscience.org/2007/v12/af/2095/fulltext.asp?bframe=viewer.htm&doi=yes