coverage guidelines prosthetics - baptist health plan · prosthetics (mp)”. implantable fda...
TRANSCRIPT
Prosthetics Created: 09/01/04
Updated: 06/02/15 (mba); 05/10/12; 02/26/08; 03/20/07; 11/21/05 Coded: 08/30/15 (sbm)
Page 1 of 30
Copyright 2012 Healthcare Research & Resolutions. This information is not intended to replace the advice of a healthcare professional or an attorney.
Coverage Guidelines
Prosthetics
Disclaimer:
Please note that Baptist Health Plan updates Coverage Guidelines throughout the year. A printed version may not be most up to date version available. The health plan reserves the right to review and update this policy as needed. Refer to the website to ascertain that you are utilizing the most current available version. Clinical guideline policies are not intended to serve as treatment guidelines or treatment recommendation. Treating providers must use their own clinical judgment in rendering care to their patient population.
For self-funded plans, consult individual plan documents. If there is a conflict between this policy and a self-funded plan document, the provisions of the plan document will govern. In addition, coverage for Medicare Advantage members may differ. This is a result of applicable coverage statements by the Center for Medicare & Medicaid Services (CMS). The National Coverage Determinations, Local Coverage Determinations, and Local Medical Review Policies may be found at the CMS website: http://www.cms.gov. Please note that for all plans, the member’s health plan benefits that are in effect on the rendered date of service must be used in coverage determinations.
Breast prostheses are discussed in the Coverage Guideline titled “Breast Surgeries”.
Myoelectric prostheses are discussed in the Coverage Guideline titled “Myoelectric Prosthetics (MP)”.
Implantable FDA approved prosthetics being used as part of an approved surgical procedure are not addressed in this paper.
DEFINITION
A prosthetic is an artificial substitute for a body part or a material inserted into tissue for functional, cosmetic, or therapeutic purposes. Prostheses may be functional, as in the case of arms, legs, feet, and ankles or hip and knee replacement joints, or cosmetic, as in the case of an artificial eye or breast prosthesis. Implanted prosthetics tend to be used therapeutically and are surgically inserted or grafted into the body.i
The terms Medically Necessary (or Medical Necessity) are defined by the Plan as the services or supplies required and/or furnished by a Provider to identify or treat a Member’s illness or injury and which, as determined by the Plan, are:
• Consistent with the symptom or diagnosis and treatment of the Member’s condition, disease, ailment, or injury;
Prosthetics Created: 09/01/04
Updated: 06/02/15 (mba); 05/10/12; 02/26/08; 03/20/07; 11/21/05 Coded: 08/30/15 (sbm)
Page 2 of 30
Copyright 2012 Healthcare Research & Resolutions. This information is not intended to replace the advice of a healthcare professional or an attorney.
• Appropriate with regard to standards of good medical practice;
• Not solely for the convenience of a Member or Provider; and
• The most appropriate supply or level of service that can be safely provided to the Member. When applied to the care of an Inpatient, it further means that the Member’s medical symptoms or condition require that the services cannot be safely provided as an Outpatient.
Examples of available prosthetics include but may not be limited to:
• Ankle
• Arm
• Breast Prosthesis
• Ears
• Eyes
• Facial Prosthesis (such as nose, lips)
• Fingers / Thumbs / Toes
• Foot
• Hand / Partial Hand
• Hip
• Knee
• Leg
• Testicles
• Wigs
Although some prosthetics are used to restore functionality or body structure, others are purely cosmetic.
COVERAGE CRITERIA
In accordance with the Centers for Medicare and Medicaid Services, the Plan considers ostomy supplies and urinary collection and retention systems, and tracheostomy supplies to be related to the functioning of a prosthetic. Therefore, ostomy and urinary supplies are subject to the “Plan’s” provisions for prosthetics.
Prosthetic purchases and replacements require pre-certification.
Medically Necessary Prosthetics
The initial purchase, fitting, necessary adjustments, repairs, and replacements of prosthetics that replace a limb or a permanently inoperative or malfunctioning external body part may be considered medically necessary as detailed below:
• A preparatory (initial) prosthesis for the first several weeks or months following surgery until

Prosthetics Created: 09/01/04
Updated: 06/02/15 (mba); 05/10/12; 02/26/08; 03/20/07; 11/21/05 Coded: 08/30/15 (sbm)
Page 3 of 30
Copyright 2012 Healthcare Research & Resolutions. This information is not intended to replace the advice of a healthcare professional or an attorney.
the stump has stabilized and the “permanent” or definitive prosthesis is provided
• Training is usually necessary for optimum prosthetic performance and comfort. Early training is provided by the prosthetist during the fitting trials. Additional training by a physical therapist is available up to the COC provisions limit for physical therapy visits.
• Purchase, fitting, necessary adjustments, and repairs of prosthetic devices and supplies to restore minimal basic function or replace all or part of the function of a permanently inoperative or malfunctioning body part or an absent body part (including contiguous tissue)
• Replacement of a prosthetic device required by a change in medical condition or to accommodate growth
• Replacement of a prosthetic that is non-functional due to normal wear and tear and is no longer serviceable
• Prostheses must be ordered or provided by, or under the direction of a physician
• Batteries useful to, and required for approved prosthetics
If more than one prosthetic device can meet the Member’s functional needs, only the most cost-effective prosthetic device is considered medically necessary.
The following specific prosthetics may be medically necessary when criteria are met:
• Eye – includes one enlargement or reduction of the prosthesis in addition to polishing and resurfacing twice a year
• Facial – including ears
• Lower limb – (a basic prosthetic for a Member at a K1 level usually includes a SACH foot and a single axis, constant friction knee) – when ALL the following criteria are met:
� Prosthesis is needed for ambulation
� Member can be expected to reach or maintain functional use within a reasonable period of time
� Medical records are available documenting current functional capabilities and rehabilitation potential is based on the K levels outlined below in the Medical Background section of this document
• SPECIFIC lower limb information:
� Ankle – Member is at a functional level (see chart below in Medical Background section) of:
o K2 or above may be eligible for an axial rotation unit
o K3 or above may be eligible for an endoskeletal ankle/foot or a power-assist ankle system
� Foot – Member is at a functional level of:
o K1 or above may be eligible for an external keel SACH (Solid Ankle Cushion

Prosthetics Created: 09/01/04
Updated: 06/02/15 (mba); 05/10/12; 02/26/08; 03/20/07; 11/21/05 Coded: 08/30/15 (sbm)
Page 4 of 30
Copyright 2012 Healthcare Research & Resolutions. This information is not intended to replace the advice of a healthcare professional or an attorney.
Heel) foot or a single axis ankle/foot or a flexible-keel foot or a multiaxial ankle/foot
o K2 or above may be eligible for a flexible-keel foot or multi-axial ankle/foot
o K3 or above functional level may be eligible for a flex foot system. Energy storing foot, multi-axial ankle/foot, dynamic response or flex-walk system
� Knee – Member is at a functional level of:
o K1 or above may be eligible for a single axis constant friction knee and other basic knee systems
o K3 or above may be eligible for a fluid or pneumatic knee
o K4 or above may be eligible for a high-activity knee control frame
• Upper Extremity
� A body-powered upper extremity prosthesis may be medically necessary when this type of prosthesis meets the functional needs to perform normal activities of daily living (ADLs)
• Testicular ii
Prosthetics that may NOT be medically necessary, or are excluded by the Plan, and/or may be considered experimental/investigational include but may not be limited to:
• Batteries that are considered common household items and are readily available over-the-counter
• Batteries necessary for use in non-covered prosthetics
• Replacement of a prosthetic device that has been lost or stolen, or was broken by carelessness, abuse or lack of maintenance is excluded by the Plan
• Replacement of a prosthetic for appearance or for a newer model with additional features is excluded by the Plan
• Dental appliances, other than those required in treatment of TMJ or CMJ, are excluded by the Plan (To be considered medically necessary dental appliances used in the treatment of TMJ/CMJ must not be designed to change the position of the teeth. If an appliance changes the position of the Member’s teeth it is considered to be an orthodontic treatment and is excluded by the Plan regardless of medical necessity.)
• For Members who do not have the ability or potential to ambulate or transfer safely with or without assistance, and when a prosthesis would not enhance their quality of life or mobility, a prosthetic is excluded by the Plan
• A second prosthetic for back-up purposes is excluded by the Plan
• Wigs are excluded by the Plan
• A user-adjustable heel height feature for a foot prosthesis

Prosthetics Created: 09/01/04
Updated: 06/02/15 (mba); 05/10/12; 02/26/08; 03/20/07; 11/21/05 Coded: 08/30/15 (sbm)
Page 5 of 30
Copyright 2012 Healthcare Research & Resolutions. This information is not intended to replace the advice of a healthcare professional or an attorney.
• Proprio Foot (Össur)iii
• Test (diagnostic) sockets for immediate post-surgical or early-fitted prostheses
• The Vacuum Assisted Socket System (VASS), a device used in conjunction with artificial limbs. VASS is considered experimental and investigational. Despite use of VASS the pain and wound healing did not significantly differ from the control group. iv
• Microprocessor-controlled leg prostheses such as the OttoBock C-Leg or the Össur Rheo Knee
A Member’s potential functional ability when provided with a lower limb prosthetic may be determined by the following K Levels. These levels, as defined by Medicare, determine the prosthetic most appropriate for the Member.
K-Level Outcome Measures in Lower Limb Prostheticsv
K-Level Description
K0 Member does not have the ability or potential to ambulate or transfer safely with or without assistance and a prosthesis does not enhance their quality of life or mobility. Therefore, a Member at this level would not be eligible for a prosthesis.
K1 Member has the ability or potential to use a prosthesis for transfers or ambulation on level surfaces at a fixed cadence. A Member at this level is considered a typical limited community ambulatory.
K2 Member has the ability or potential for ambulation with the ability to traverse low-level environmental barriers such as curbs, stairs, or uneven surfaces. A Member at this level is considered a typical community ambulatory
K3 Member has the ability or potential for ambulation with variable cadence. At this level a Member is considered a typical community ambulatory with the ability to traverse most environmental barriers and may have vocational, therapeutic, or exercise activity that demands prosthetic use beyond simple locomotion.
K4 Member has the ability or potential for prosthetic ambulation that exceeds basic ambulation skills, exhibiting high impact stress, or energy levels. This K-level is typical of the prosthetic demands of a child, active adult or an athlete.
Upper limb prostheses are classified as follows:
Body powered – A body harness and cable system provides functional manipulation. The voluntary movement of the shoulder and/or limb stump extends the cable system transmitting force to the device to control hand, forearm and elbow movement.
Passive – The lightest system is a mostly cosmetic prosthesis. It must be repositioned manually by the opposite arm.
Prosthetics Created: 09/01/04
Updated: 06/02/15 (mba); 05/10/12; 02/26/08; 03/20/07; 11/21/05 Coded: 08/30/15 (sbm)
Page 6 of 30
Copyright 2012 Healthcare Research & Resolutions. This information is not intended to replace the advice of a healthcare professional or an attorney.
REGULATORY INFORMATION
Kentucky – No legislative mandates were found for coverage of prosthetics.
Indiana – No legislative mandates were found for coverage of prosthetics.
Tennessee – No legislative mandates were found for coverage of prosthetics.
Prosthetic devices are subject to regulation by the U.S. Food and Drug Administration (FDA) as medical devices.
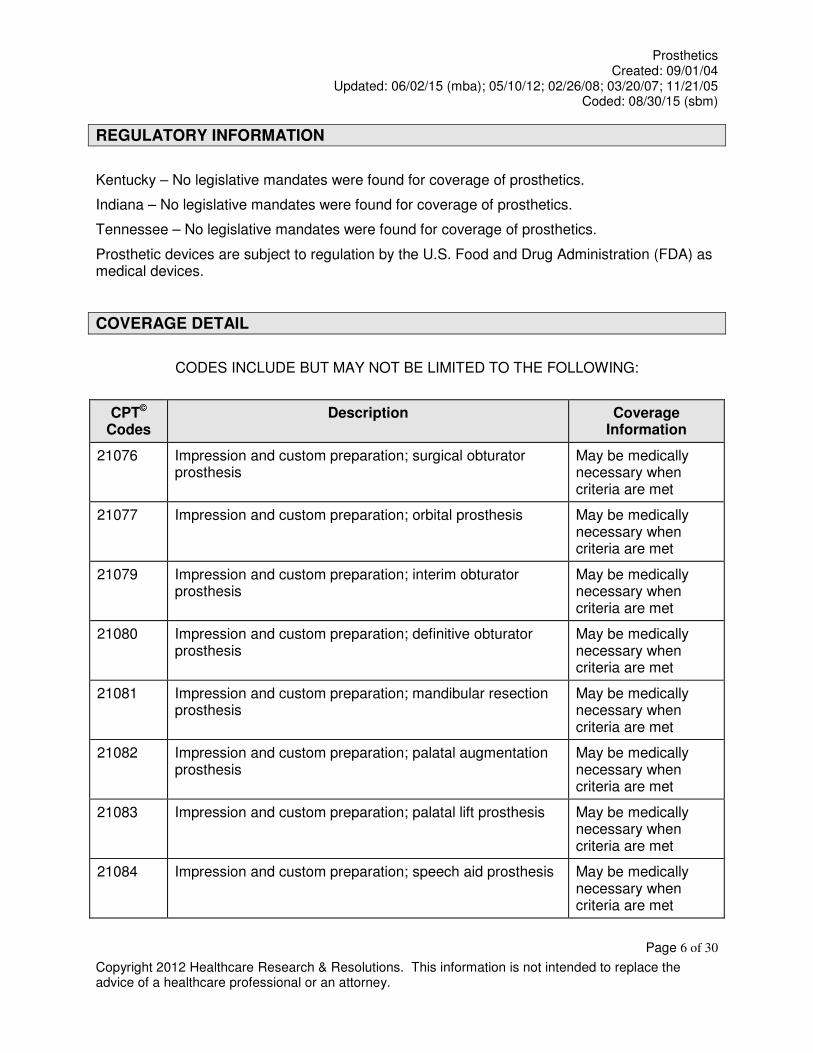
COVERAGE DETAIL
CODES INCLUDE BUT MAY NOT BE LIMITED TO THE FOLLOWING:
CPT© Codes
Description Coverage Information
21076 Impression and custom preparation; surgical obturator prosthesis
May be medically necessary when criteria are met
21077 Impression and custom preparation; orbital prosthesis May be medically necessary when criteria are met
21079 Impression and custom preparation; interim obturator prosthesis
May be medically necessary when criteria are met
21080 Impression and custom preparation; definitive obturator prosthesis
May be medically necessary when criteria are met
21081 Impression and custom preparation; mandibular resection prosthesis
May be medically necessary when criteria are met
21082 Impression and custom preparation; palatal augmentation prosthesis
May be medically necessary when criteria are met
21083 Impression and custom preparation; palatal lift prosthesis May be medically necessary when criteria are met
21084 Impression and custom preparation; speech aid prosthesis May be medically necessary when criteria are met
Prosthetics Created: 09/01/04
Updated: 06/02/15 (mba); 05/10/12; 02/26/08; 03/20/07; 11/21/05 Coded: 08/30/15 (sbm)
Page 7 of 30
Copyright 2012 Healthcare Research & Resolutions. This information is not intended to replace the advice of a healthcare professional or an attorney.
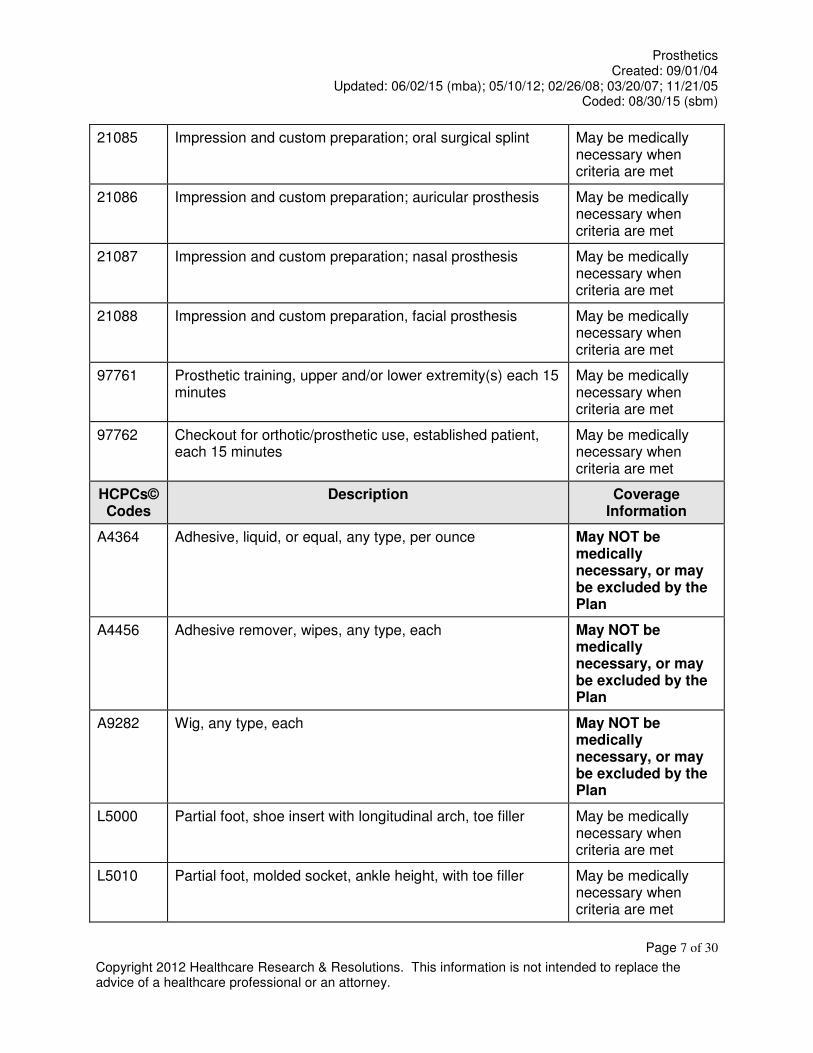
21085 Impression and custom preparation; oral surgical splint May be medically necessary when criteria are met
21086 Impression and custom preparation; auricular prosthesis May be medically necessary when criteria are met
21087 Impression and custom preparation; nasal prosthesis May be medically necessary when criteria are met
21088 Impression and custom preparation, facial prosthesis May be medically necessary when criteria are met
97761 Prosthetic training, upper and/or lower extremity(s) each 15 minutes
May be medically necessary when criteria are met
97762 Checkout for orthotic/prosthetic use, established patient, each 15 minutes
May be medically necessary when criteria are met
HCPCs© Codes
Description Coverage Information
A4364 Adhesive, liquid, or equal, any type, per ounce May NOT be medically necessary, or may be excluded by the Plan
A4456 Adhesive remover, wipes, any type, each May NOT be medically necessary, or may be excluded by the Plan
A9282 Wig, any type, each May NOT be medically necessary, or may be excluded by the Plan
L5000 Partial foot, shoe insert with longitudinal arch, toe filler May be medically necessary when criteria are met
L5010 Partial foot, molded socket, ankle height, with toe filler May be medically necessary when criteria are met

Prosthetics Created: 09/01/04
Updated: 06/02/15 (mba); 05/10/12; 02/26/08; 03/20/07; 11/21/05 Coded: 08/30/15 (sbm)
Page 8 of 30
Copyright 2012 Healthcare Research & Resolutions. This information is not intended to replace the advice of a healthcare professional or an attorney.
L5020 Partial foot, molded socket, tibial tubercle height, with toe filler
May be medically necessary when criteria are met
Ankle
L5050 Ankle, Symes, molded socket, solid ankle cushion heel (SACH) foot
May be medically necessary when criteria are met
L5060 Ankle, Symes, metal frame, molded leather socket, articulated ankle/foot
May be medically necessary when criteria are met
Below Knee
L5100 Below knee, molded socket, shin, SACH foot May be medically necessary when criteria are met
L5105 Below knee, plastic socket, joints and thigh lacer, SACH foot
May be medically necessary when criteria are met
Knee Disarticulation
L5150 Knee disarticulation (or through knee), molded socket, external knee joints, shin, SACH foot
May be medically necessary when criteria are met
L5160 Knee disarticulation (or through knee), molded socket, bent knee configuration, external knee joints, shin, SACH foot
May be medically necessary when criteria are met
Above Knee
L5200 Above knee, molded socket, single axis constant friction knee, shin, SACH foot
May be medically necessary when criteria are met
L5210 Above knee, short prosthesis, no knee joint (“stubbies”), with foot blocks, no ankle joints, each
May be medically necessary when criteria are met
L5220 Above knee, short prosthesis, no knee joint (“stubbies”), with articulated ankle/foot, dynamically aligned, each
May be medically necessary when criteria are met
L5230 Above knee, for proximal femoral focal deficiency, constant friction knee, shin, SACH foot
May be medically necessary when criteria are met
Hip Disarticulation
L5250 Hip disarticulation, Canadian type; molded socket, hip joint, May be medically

Prosthetics Created: 09/01/04
Updated: 06/02/15 (mba); 05/10/12; 02/26/08; 03/20/07; 11/21/05 Coded: 08/30/15 (sbm)
Page 9 of 30
Copyright 2012 Healthcare Research & Resolutions. This information is not intended to replace the advice of a healthcare professional or an attorney.
single axis constant friction knee, shin, SACH foot necessary when criteria are met
L5270 Hip disarticulation, tilt table type; molded socket, locking hip joint, single axis constant friction knee, shin, SACH foot
May be medically necessary when criteria are met
Hemipelvectomy
L5280 Hemipelvectomy, Canadian type: molded socket, hip joint, single axis constant friction knee, shin, SACH foot
May be medically necessary when criteria are met
L5301 Below knee, molded socket, shin, SACH foot, endoskeletal system
May be medically necessary when criteria are met
L5321 Above knee, molded socket, open end, SACH foot, endoskeletal system, single axis knee
May be medically necessary when criteria are met
L5331 Hip disarticulation, Canadian type; molded socket, endoskeletal system, hip joint, single axis knee, SACH foot
May be medically necessary when criteria are met
L5341 Hemipelvectomy, Canadian type; molded socket, endoskeletal system, hip joint, single axis knee, SACH foot
May be medically necessary when criteria are met
Immediate Postsurgical or Early Fitting Procedures
L5400 Immediate postsurgical or early fitting, application of initial rigid dressing, including fitting, alignment and suspension, and one cast change, below knee
May be medically necessary when criteria are met
L5410 Immediate postsurgical or early fitting, application of initial rigid dressing, including fitting, alignment and suspension, below knee, each additional cast change and realignment
May be medically necessary when criteria are met
L5420 Immediate postsurgical or early fitting, application of initial rigid dressing, including fitting, alignment and suspension and one cast change “AK” or knee disarticulation
May be medically necessary when criteria are met
L5430 Immediate postsurgical or early fitting, application of initial rigid dressing, including fitting, alignment and suspension, “AK” or knee disarticulation, each additional cast change and realignment
May be medically necessary when criteria are met
L5450 Immediate postsurgical or early fitting, application of nonweight bearing rigid dressing, below knee
May be medically necessary when criteria are met
L5460 Immediate postsurgical or early fitting, application of nonweight bearing rigid dressing, above knee
May be medically necessary when

Prosthetics Created: 09/01/04
Updated: 06/02/15 (mba); 05/10/12; 02/26/08; 03/20/07; 11/21/05 Coded: 08/30/15 (sbm)
Page 10 of 30
Copyright 2012 Healthcare Research & Resolutions. This information is not intended to replace the advice of a healthcare professional or an attorney.
criteria are met
Initial Prosthesis
L5500 Initial, below knee “PTB” type socket, non-alignable system, pylon, no cover, SACH foot, plaster socket, direct formed
May be medically necessary when criteria are met
L5505 Initial, above knee – knee disarticulation, ischial level socket, non-alignable system, pylon, no cover, SACH foot, plaster socket, direct formed
May be medically necessary when criteria are met
Preparatory Prosthesis
L5510 Preparatory, below knee “PTB” type socket, non-alignable system, pylon, no cover, SACH foot, plaster socket, molded to model
May be medically necessary when criteria are met
L5520 Preparatory, below knee “PTB” type socket, non-alignable system, pylon, no cover, SACH foot, thermoplastic or equal, direct formed
May be medically necessary when criteria are met
L5530 Preparatory, below knee “PTB” type socket, non-alignable system, pylon, no cover, SACH foot, thermoplastic or equal, molded to model
May be medically necessary when criteria are met
L5535 Preparatory, below knee “PTB” type socket, non-alignable system, pylon, no cover, SACH foot, prefabricated, adjustable open end socket
May be medically necessary when criteria are met
L5540 Preparatory, below knee “PTB” type socket, non-alignable system, pylon, no cover, SACH foot, laminated socket, molded to model
May be medically necessary when criteria are met
L5560 Preparatory above knee – knee disarticulation, ischial level socket, non-alignable system, pylon, no cover, SACH foot, plaster socket, molded to model
May be medically necessary when criteria are met
L5570 Preparatory above knee – knee disarticulation, ischial level socket, non-alignable system, pylon, no cover, SACH foot, thermoplastic or equal, direct formed
May be medically necessary when criteria are met
L5580 Preparatory above knee – knee disarticulation, ischial level socket, non-alignable system, pylon, no cover, SACH foot, thermoplastic or equal, molded to model
May be medically necessary when criteria are met
L5585 Preparatory above knee – knee disarticulation, ischial level socket, non-alignable system, pylon, no cover, SACH foot, prefabricated adjustable open end socket
May be medically necessary when criteria are met
L5590 Preparatory above knee – knee disarticulation, ischial level socket, non-alignable system, pylon, no cover, SACH foot, laminated socket, molded to model
May be medically necessary when criteria are met

Prosthetics Created: 09/01/04
Updated: 06/02/15 (mba); 05/10/12; 02/26/08; 03/20/07; 11/21/05 Coded: 08/30/15 (sbm)
Page 11 of 30
Copyright 2012 Healthcare Research & Resolutions. This information is not intended to replace the advice of a healthcare professional or an attorney.
L5595 Preparatory, hip disarticulation – Hemipelvectomy, pylon, no cover, SACH foot, thermoplastic or equal, molded to patient model
May be medically necessary when criteria are met
L5600 Preparatory, hip disarticulation – Hemipelvectomy, pylon, no cover, SACH foot, laminated socket, molded to patient model
May be medically necessary when criteria are met
Additions: Lower Extremity
L5610 Addition to lower extremity, endoskeletal system, above knee, hydracadence system
May be medically necessary when criteria are met
L5611 Addition to lower extremity, endoskeletal system, above knee – knee disarticulation, 4-bar linkage, with friction swing phase control
May be medically necessary when criteria are met
L5613 Addition to lower extremity, endoskeletal system, above knee – knee disarticulation, 4-bar linkage, with hydraulic swing phase control
May be medically necessary when criteria are met
L5614 Addition to lower extremity, endoskeletal system, above knee – knee disarticulation, 4-bar linkage, with pneumatic swing phase control
May be medically necessary when criteria are met
L5616 Addition to lower extremity, endoskeletal system, above knee, universal multiplex system, friction swing phase control
May be medically necessary when criteria are met
L5617 Addition to lower extremity, quick change self-aligning unit, above or below knee, each
May be medically necessary when criteria are met
L5618 Addition to lower extremity, test socket, Symes May be medically necessary when criteria are met
L5620 Addition to lower extremity, test socket, below knee May be medically necessary when criteria are met
L5622 Addition to lower extremity, test socket, knee disarticulation May be medically necessary when criteria are met
L5624 Addition to lower extremity, test socket, above knee May be medically necessary when criteria are met
L5626 Addition to lower extremity, test socket, hip disarticulation May be medically necessary when criteria are met

Prosthetics Created: 09/01/04
Updated: 06/02/15 (mba); 05/10/12; 02/26/08; 03/20/07; 11/21/05 Coded: 08/30/15 (sbm)
Page 12 of 30
Copyright 2012 Healthcare Research & Resolutions. This information is not intended to replace the advice of a healthcare professional or an attorney.
L5628 Addition to lower extremity, test socket, Hemipelvectomy May be medically necessary when criteria are met
L5629 Addition to lower extremity, below knee, acrylic socket May be medically necessary when criteria are met
L5630 Addition to lower extremity, Symes type, expandable wall socket
Medically necessary when criteria are met
L5631 Addition to lower extremity, above knee or knee disarticulation, acrylic socket
Medically necessary when criteria are met
L5632 Addition to lower extremity, Symes type, “PTB” brim design socket
May be medically necessary when criteria are met
L5634 Addition to lower extremity, Symes type, posterior opening (Canadian) socket
May be medically necessary when criteria are met
L5636 Addition to lower extremity, Symes type, medial opening socket
May be medically necessary when criteria are met
L5637 Addition to lower extremity, below knee, total contact May be medically necessary when criteria are met
L5638 Addition to lower extremity, below knee, leather socket May be medically necessary when criteria are met
Additions: Socket Variations
L5639 Addition to lower extremity, below knee, wood socket May be medically necessary when criteria are met
L5640 Addition to lower extremity, knee disarticulation, leather socket
May be medically necessary when criteria are met
L5642 Addition to lower extremity, above knee, leather socket May be medically necessary when criteria are met
L5643 Addition to lower extremity, hip disarticulation, flexible inner socket, external frame
May be medically necessary when criteria are met
L5644 Addition to lower extremity, above knee, wood socket May be medically necessary when
Prosthetics Created: 09/01/04
Updated: 06/02/15 (mba); 05/10/12; 02/26/08; 03/20/07; 11/21/05 Coded: 08/30/15 (sbm)
Page 13 of 30
Copyright 2012 Healthcare Research & Resolutions. This information is not intended to replace the advice of a healthcare professional or an attorney.
criteria are met
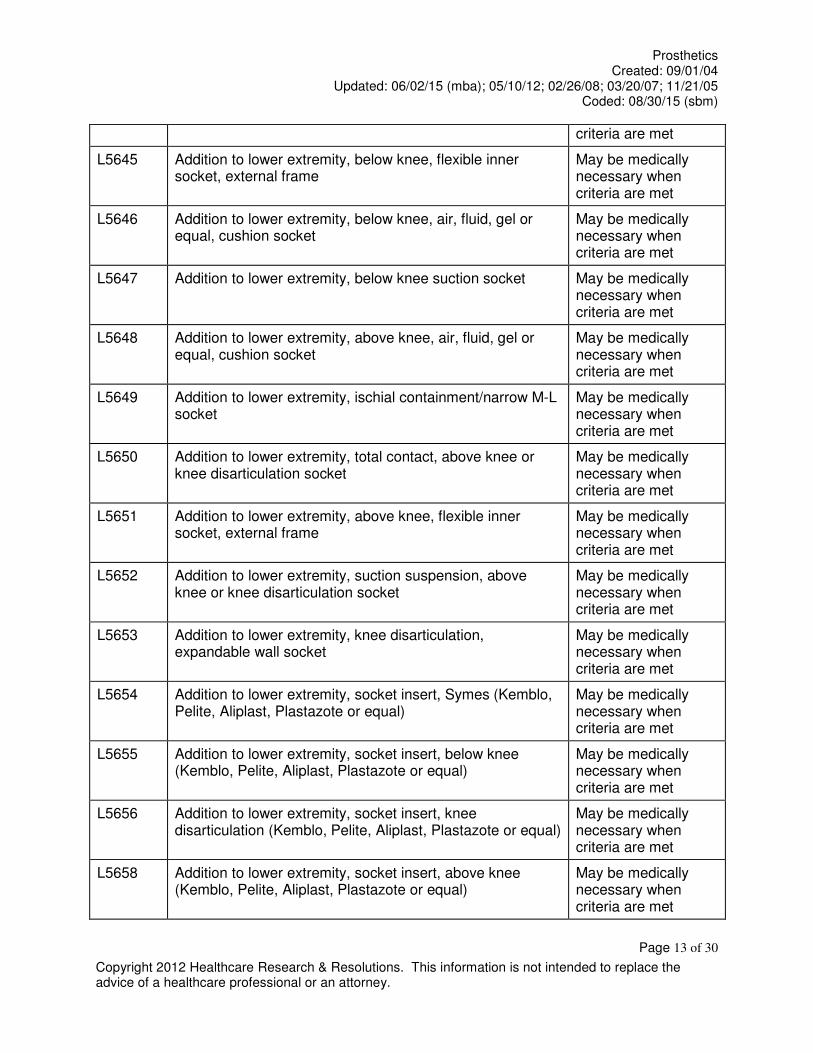
L5645 Addition to lower extremity, below knee, flexible inner socket, external frame
May be medically necessary when criteria are met
L5646 Addition to lower extremity, below knee, air, fluid, gel or equal, cushion socket
May be medically necessary when criteria are met
L5647 Addition to lower extremity, below knee suction socket May be medically necessary when criteria are met
L5648 Addition to lower extremity, above knee, air, fluid, gel or equal, cushion socket
May be medically necessary when criteria are met
L5649 Addition to lower extremity, ischial containment/narrow M-L socket
May be medically necessary when criteria are met
L5650 Addition to lower extremity, total contact, above knee or knee disarticulation socket
May be medically necessary when criteria are met
L5651 Addition to lower extremity, above knee, flexible inner socket, external frame
May be medically necessary when criteria are met
L5652 Addition to lower extremity, suction suspension, above knee or knee disarticulation socket
May be medically necessary when criteria are met
L5653 Addition to lower extremity, knee disarticulation, expandable wall socket
May be medically necessary when criteria are met
L5654 Addition to lower extremity, socket insert, Symes (Kemblo, Pelite, Aliplast, Plastazote or equal)
May be medically necessary when criteria are met
L5655 Addition to lower extremity, socket insert, below knee (Kemblo, Pelite, Aliplast, Plastazote or equal)
May be medically necessary when criteria are met
L5656 Addition to lower extremity, socket insert, knee disarticulation (Kemblo, Pelite, Aliplast, Plastazote or equal)
May be medically necessary when criteria are met
L5658 Addition to lower extremity, socket insert, above knee (Kemblo, Pelite, Aliplast, Plastazote or equal)
May be medically necessary when criteria are met

Prosthetics Created: 09/01/04
Updated: 06/02/15 (mba); 05/10/12; 02/26/08; 03/20/07; 11/21/05 Coded: 08/30/15 (sbm)
Page 14 of 30
Copyright 2012 Healthcare Research & Resolutions. This information is not intended to replace the advice of a healthcare professional or an attorney.
L5661 Addition to lower extremity, socket insert, multidurometer, Symes
May be medically necessary when criteria are met
L5665 Addition to lower extremity, socket insert, multidurometer, below knee
May be medically necessary when criteria are met
L5666 Addition to lower extremity, below knee, cuff suspension May be medically necessary when criteria are met
L5668 Addition to lower extremity, below knee, molded distal cushion
May be medically necessary when criteria are met
L5670 Addition to lower extremity, below knee, molded supracondylar suspension (“PTS” or similar)
May be medically necessary when criteria are met
L5671 Addition to lower extremity, below knee/above knee suspension locking mechanism (shuttle, lanyard or equal), excludes socket insert
May be medically necessary when criteria are met
L5672 Addition to lower extremity, below knee, removable medial brim suspension
May be medically necessary when criteria are met
Additions: Socket Insert and Suspension
L5673 Addition to lower extremity, below knee/above knee, custom fabricated from existing mold or prefabricated, socket insert, silicone gel, elastomeric or equal, for use with locking mechanism
May be medically necessary when criteria are met
L5676 Addition to lower extremity, below knee, knee joints, single axis, pair
May be medically necessary when criteria are met
L5677 Addition to lower extremity, below knee, knee joints, polycentric, pair
May be medically necessary when criteria are met
L5678 Addition to lower extremity, below knee, joint covers, pair May be medically necessary when criteria are met
L5679 Addition to lower extremity, below knee/above knee, custom fabricated, socket insert, silicone gel, elastomeric or equal, not for use with locking mechanism
May be medically necessary when criteria are met
L5680 Addition to lower extremity, below knee, thigh lacer, nonmolded
May be medically necessary when

Prosthetics Created: 09/01/04
Updated: 06/02/15 (mba); 05/10/12; 02/26/08; 03/20/07; 11/21/05 Coded: 08/30/15 (sbm)
Page 15 of 30
Copyright 2012 Healthcare Research & Resolutions. This information is not intended to replace the advice of a healthcare professional or an attorney.
criteria are met
L5681 Addition to lower extremity, below knee/above knee, custom fabricated socket insert for congenital or atypical traumatic amputee, silicone gel, elastomeric or equal, for use with or without locking mechanism, initial only (for other than initial, use code L5673 or L5679)
May be medically necessary when criteria are met
L5682 Addition to lower extremity, below knee, thigh lacer, gluteal/ischial, molded
May be medically necessary when criteria are met
L5683 Addition to lower extremity, below knee/above knee, custom fabricated socket insert for other that congenital or atypical traumatic amputee, silicone gel, elastomeric or equal, for use with or without locking mechanism, initial only (for other than initial, use code L5673 or L5679
May be medically necessary when criteria are met
L5684 Addition to lower extremity, below knee fork strap May be medically necessary when criteria are met
L5685 Addition to lower extremity prosthesis, below knee, suspension/sealing sleeve, with or without valve, any material, each
May be medically necessary when criteria are met
L5686 Addition to lower extremity, below knee, back check (extension control)
May be medically necessary when criteria are met
L5688 Addition to lower extremity, below knee, waist belt, webbing
May be medically necessary when criteria are met
L5690 Addition to lower extremity, below knee, waist belt, padded and lined
May be medically necessary when criteria are met
L5692 Addition to lower extremity, above knee, pelvic control belt, light
May be medically necessary when criteria are met
L5694 Addition to lower extremity, above knee, pelvic control belt, padded and lined
May be medically necessary when criteria are met
L5695 Addition to lower extremity, above knee, pelvic control, sleeve suspension, neoprene or equal, each
May be medically necessary when criteria are met
L5696 Addition to lower extremity, above knee or knee disarticulation, pelvic joint
May be medically necessary when criteria are met

Prosthetics Created: 09/01/04
Updated: 06/02/15 (mba); 05/10/12; 02/26/08; 03/20/07; 11/21/05 Coded: 08/30/15 (sbm)
Page 16 of 30
Copyright 2012 Healthcare Research & Resolutions. This information is not intended to replace the advice of a healthcare professional or an attorney.
L5697 Addition to lower extremity, above knee or knee disarticulation, pelvic band
May be medically necessary when criteria are met
L5698 Addition to lower extremity, above knee or knee disarticulation, Silesian bandage
May be medically necessary when criteria are met
L5699 All lower extremity prostheses, shoulder harness May be medically necessary when criteria are met
Replacements
L5700 Replacement, socket, below knee, molded to patient model
May be medically necessary when criteria are met
L5701 Replacement, socket, above knee/knee disarticulation, including attachment plate, molded to patient model
May be medically necessary when criteria are met
L5702 Replacement, socket, hip disarticulation, including hip joint, molded to patient model
May be medically necessary when criteria are met
L5703 Ankle, Symes, molded to patient model, socket without SACH foot, replacement only
May be medically necessary when criteria are met
L5704 Custom shaped protective cover, below knee May be medically necessary when criteria are met
L5705 Custom shaped protective cover, above knee May be medically necessary when criteria are met
L5706 Custom shaped protective cover, knee disarticulation May be medically necessary when criteria are met
L5707 Custom shaped protective cover, hip disarticulation May be medically necessary when criteria are met
L5710 Addition, exoskeletal knee-shin system, single axis, manual lock
May be medically necessary when criteria are met
L5711 Addition, exoskeletal knee-shin system, single axis, manual lock, ultra-light material
May be medically necessary when criteria are met

Prosthetics Created: 09/01/04
Updated: 06/02/15 (mba); 05/10/12; 02/26/08; 03/20/07; 11/21/05 Coded: 08/30/15 (sbm)
Page 17 of 30
Copyright 2012 Healthcare Research & Resolutions. This information is not intended to replace the advice of a healthcare professional or an attorney.
L5712 Addition, exoskeletal knee-shin system, single axis, friction swing and stance phase control (safety knee)
May be medically necessary when criteria are met
L5714 Addition, exoskeletal knee-shin system, single axis, variable friction swing phase control
May be medically necessary when criteria are met
Additions: Exoskeletal Knee-Shin System
L5716 Addition, exoskeletal knee-shin system, polycentric, mechanical stance phase lock
May be medically necessary when criteria are met
L5718 Addition, exoskeletal knee-shin system, polycentric, friction swing and stance phase control
May be medically necessary when criteria are met
L5722 Addition, exoskeletal knee-shin system, single axis, pneumatic swing, friction stance phase control
May be medically necessary when criteria are met
L5724 Addition, exoskeletal knee-shin system, single axis, fluid swing phase control
May be medically necessary when criteria are met
L5726 Addition, exoskeletal knee-shin system, single axis, external joints, fluid swing phase control
May be medically necessary when criteria are met
L5728 Addition, exoskeletal knee-shin system, single axis, fluid swing and stance phase control
May be medically necessary when criteria are met
L5780 Addition, exoskeletal knee-shin system, single axis, pneumatic/hydra pneumatic swing phase control
May be medically necessary when criteria are met
L5781 Addition to lower limb prosthesis, vacuum pump, residual limb volume management and moisture evacuation system
May be medically necessary when criteria are met
L5782 Addition to lower limb prosthesis, vacuum pump, residual limb volume management and moisture evacuation system, heavy duty
May be medically necessary when criteria are met
Component Modification
L5785 Addition, exoskeletal system, below knee, ultra-light material (titanium, carbon fiber or equal)
May be medically necessary when criteria are met
L5790 Addition, exoskeletal system, above knee, ultra-light material (titanium, carbon fiber or equal)
May be medically necessary when

Prosthetics Created: 09/01/04
Updated: 06/02/15 (mba); 05/10/12; 02/26/08; 03/20/07; 11/21/05 Coded: 08/30/15 (sbm)
Page 18 of 30
Copyright 2012 Healthcare Research & Resolutions. This information is not intended to replace the advice of a healthcare professional or an attorney.
criteria are met
L5795 Addition, exoskeletal system, hip disarticulation, ultra-light material (titanium, carbon fiber or equal)
May be medically necessary when criteria are met
Additions: Endoskeletal Knee-Shin System
L5810 Addition, endoskeletal knee-shin system, single axis, manual lock
Medically necessary when criteria are met
L5811 Addition, endoskeletal knee-shin system, single axis, manual lock, ultra-light material
Medically necessary when criteria are met
L5812 Addition, endoskeletal knee-shin system, single axis, friction swing and stance phase control (safety knee)
Medically necessary when criteria are met
L5814 Addition, endoskeletal knee-shin system, polycentric, hydraulic swing phase control mechanical stance phase lock
Medically necessary when criteria are met
L5816 Addition, endoskeletal knee-shin system, polycentric, mechanical stance phase lock
May be medically necessary when criteria are met
L5818 Addition, endoskeletal knee-shin system, polycentric, friction swing and stance phase control
May be medically necessary when criteria are met
L5822 Addition, endoskeletal knee-shin system, single axis, pneumatic swing, friction stance phase control
May be medically necessary when criteria are met
L5824 Addition, endoskeletal knee-shin system, single axis, fluid swing phase control
May be medically necessary when criteria are met
L5826 Addition, endoskeletal knee-shin system, single axis, hydraulic swing phase control with miniature high activity frame
May be medically necessary when criteria are met
L5828 Addition, endoskeletal knee-shin system, single axis, fluid swing and stance phase control
May be medically necessary when criteria are met
L5830 Addition, endoskeletal knee-shin system, single axis, pneumatic/swing phase control
May be medically necessary when criteria are met
L5840 Addition, endoskeletal knee-shin system, 4-bar linkage or multiaxial, pneumatic swing phase control
May be medically necessary when criteria are met
L5845 Addition, endoskeletal knee-shin system, stance flexion May be medically necessary when

Prosthetics Created: 09/01/04
Updated: 06/02/15 (mba); 05/10/12; 02/26/08; 03/20/07; 11/21/05 Coded: 08/30/15 (sbm)
Page 19 of 30
Copyright 2012 Healthcare Research & Resolutions. This information is not intended to replace the advice of a healthcare professional or an attorney.
feature, adjustable criteria are met
L5848 Addition to endoskeletal, knee-shin system, hydraulic stance extension, dampening feature, with or without adjustability
May be medically necessary when criteria are met
L5850 Addition, endoskeletal system, above knee or hip disarticulation, knee extension assist
May be medically necessary when criteria are met
L5855 Addition, endoskeletal system, hip disarticulation, mechanical hip extension assist
May be medically necessary when criteria are met
L5856 Addition to lower extremity prosthesis, endoskeletal knee shin system, microprocessor control feature, swing and stance phase, includes electronic sensor(s), any type
May NOT be medically necessary, or may be experimental / investigational
L5857 Addition to lower extremity prosthesis, endoskeletal knee shin system, microprocessor control feature, swing phase only, includes electronic sensor(s), any type
May NOT be medically necessary, or may be experimental / investigational
L5858 Addition to lower extremity prosthesis, endoskeletal knee shin system, microprocessor control feature, stance phase only, includes electronic sensor(s), any type
May NOT be medically necessary, or may be experimental / investigational
L5859 Addition to lower extremity prosthesis, endoskeletal knee-shin system, powered and programmable flexion/extension assist control, includes any type motor(s)
May NOT be medically necessary, or may be experimental / investigational
L5910 Addition, endoskeletal system, below knee, alignable system
May be medically necessary when criteria are met
L5920 Addition, endoskeletal system, above knee or hip disarticulation, alignable system
May be medically necessary when criteria are met
L5925 Addition, endoskeletal system, above knee, knee disarticulation or hip disarticulation, manual lock
May be medically necessary when criteria are met
L5930 Addition, endoskeletal system, high activity knee control frame
May be medically necessary when criteria are met
L5940 Addition, endoskeletal system, below knee, ultra-light material (titanium, carbon fiber or equal)
May be medically necessary when criteria are met
L5950 Addition, endoskeletal system, above knee, ultra-light May be medically
Prosthetics Created: 09/01/04
Updated: 06/02/15 (mba); 05/10/12; 02/26/08; 03/20/07; 11/21/05 Coded: 08/30/15 (sbm)
Page 20 of 30
Copyright 2012 Healthcare Research & Resolutions. This information is not intended to replace the advice of a healthcare professional or an attorney.
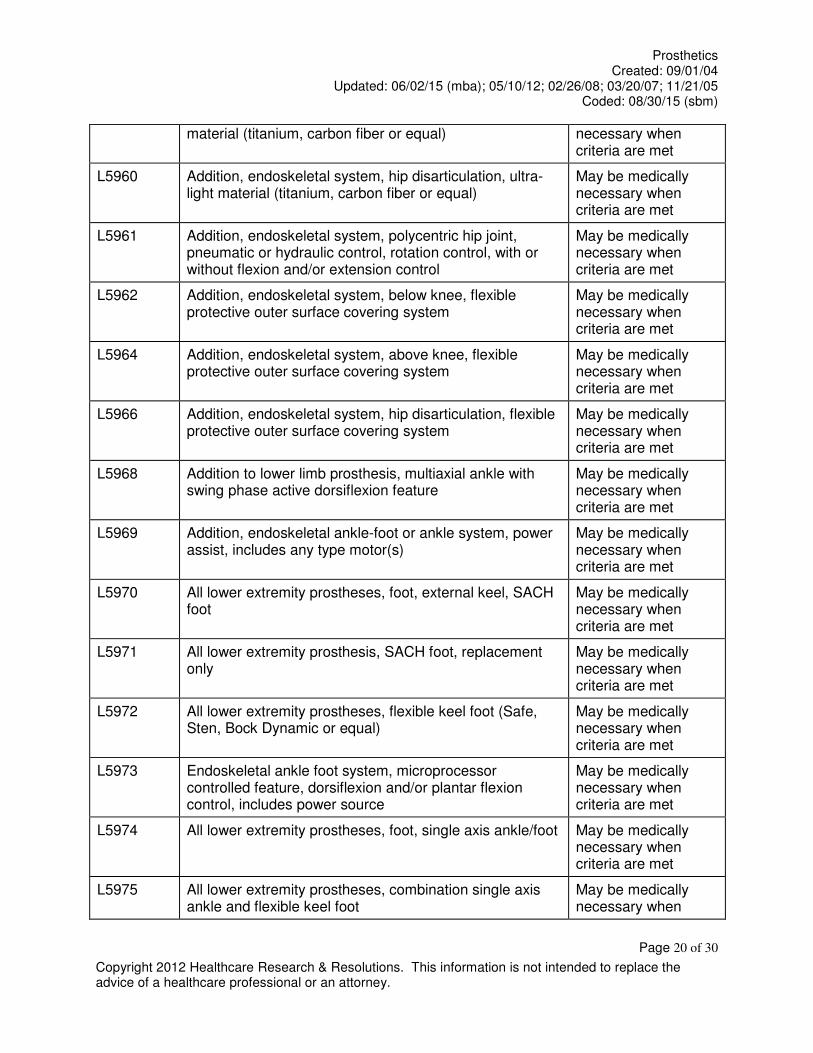
material (titanium, carbon fiber or equal) necessary when criteria are met
L5960 Addition, endoskeletal system, hip disarticulation, ultra-light material (titanium, carbon fiber or equal)
May be medically necessary when criteria are met
L5961 Addition, endoskeletal system, polycentric hip joint, pneumatic or hydraulic control, rotation control, with or without flexion and/or extension control
May be medically necessary when criteria are met
L5962 Addition, endoskeletal system, below knee, flexible protective outer surface covering system
May be medically necessary when criteria are met
L5964 Addition, endoskeletal system, above knee, flexible protective outer surface covering system
May be medically necessary when criteria are met
L5966 Addition, endoskeletal system, hip disarticulation, flexible protective outer surface covering system
May be medically necessary when criteria are met
L5968 Addition to lower limb prosthesis, multiaxial ankle with swing phase active dorsiflexion feature
May be medically necessary when criteria are met
L5969 Addition, endoskeletal ankle-foot or ankle system, power assist, includes any type motor(s)
May be medically necessary when criteria are met
L5970 All lower extremity prostheses, foot, external keel, SACH foot
May be medically necessary when criteria are met
L5971 All lower extremity prosthesis, SACH foot, replacement only
May be medically necessary when criteria are met
L5972 All lower extremity prostheses, flexible keel foot (Safe, Sten, Bock Dynamic or equal)
May be medically necessary when criteria are met
L5973 Endoskeletal ankle foot system, microprocessor controlled feature, dorsiflexion and/or plantar flexion control, includes power source
May be medically necessary when criteria are met
L5974 All lower extremity prostheses, foot, single axis ankle/foot May be medically necessary when criteria are met
L5975 All lower extremity prostheses, combination single axis ankle and flexible keel foot
May be medically necessary when

Prosthetics Created: 09/01/04
Updated: 06/02/15 (mba); 05/10/12; 02/26/08; 03/20/07; 11/21/05 Coded: 08/30/15 (sbm)
Page 21 of 30
Copyright 2012 Healthcare Research & Resolutions. This information is not intended to replace the advice of a healthcare professional or an attorney.
criteria are met
L5976 All lower extremity prostheses, energy storing foot (Seattle Carbon Copy II or equal)
May be medically necessary when criteria are met
L5978 All lower extremity prostheses, foot, multi-axial ankle/foot May be medically necessary when criteria are met
L5979 All lower extremity prostheses, multi-axial ankle, dynamic response foot, one piece system
May be medically necessary when criteria are met
L5980 All lower extremity prostheses, flex-foot system May be medically necessary when criteria are met
L5981 All lower extremity prostheses, flex-walk system or equal May be medically necessary when criteria are met
L5982 All exoskeletal lower extremity prostheses, axial rotation unit
May be medically necessary when criteria are met
L5984 All endoskeletal lower extremity prosthesis, axial rotation unit, with or without adjustability
May be medically necessary when criteria are met
L5985 All endoskeletal lower extremity prostheses, dynamic prosthetic pylon
May be medically necessary when criteria are met
L5986 All lower extremity prostheses, multi-axial rotation unit (MCP or equal)
May be medically necessary when criteria are met
L5987 All lower extremity prosthesis, shank foot system with vertical loading pylon
May be medically necessary when criteria are met
L5988 Addition to lower limb prosthesis, vertical shock reducing pylon feature
May be medically necessary when criteria are met
L5990 Addition to lower extremity prosthesis, user adjustable heel height
May be medically necessary when criteria are met
L5999 Lower extremity prosthesis, not otherwise specified May NOT be medically necessary, or may be experimental / investigational

Prosthetics Created: 09/01/04
Updated: 06/02/15 (mba); 05/10/12; 02/26/08; 03/20/07; 11/21/05 Coded: 08/30/15 (sbm)
Page 22 of 30
Copyright 2012 Healthcare Research & Resolutions. This information is not intended to replace the advice of a healthcare professional or an attorney.
Prosthetics – Upper Limb
Partial Hand
L6000 Partial hand, Robin-Aids, thumb remaining (or equal) May be medically necessary when criteria are met
L6010 Partial hand, Robin-Aids, little and/or ring finger remaining (or equal)
May be medically necessary when criteria are met
L6020 Partial hand, Robin-Aids, no finger remaining (or equal) May be medically necessary when criteria are met
L6026 Transcarpal/metacarpal or partial hand disarticulation prosthesis, external power, self-suspended, inner socket with removable forearm section, electrodes and cables, two batteries, charger, myoelectric control of terminal device, excludes terminal device(s)
May be medically necessary when criteria are met
Wrist Disarticulation
L6050 Wrist disarticulation, molded socket, flexible elbow hinges, triceps pad
May be medically necessary when criteria are met
L6055 Wrist disarticulation, molded socket with expandable interface, flexible elbow hinges, triceps pad
May be medically necessary when criteria are met
Below Elbow
L6100 Below elbow, molded socket, flexible elbow hinge, triceps pad
May be medically necessary when criteria are met
L6110 Below elbow, molded socket (Muenster or Northwestern suspension types)
May be medically necessary when criteria are met
L6120 Below elbow, molded double wall split socket, step-up hinges, half cuff
May be medically necessary when criteria are met
L6130 Below elbow, molded double wall split socket, stump activated locking hinge, half cuff
May be medically necessary when criteria are met
Elbow disarticulation
L6200 Elbow disarticulation, molded socket, outside locking hinge, forearm
May be medically necessary when
Prosthetics Created: 09/01/04
Updated: 06/02/15 (mba); 05/10/12; 02/26/08; 03/20/07; 11/21/05 Coded: 08/30/15 (sbm)
Page 23 of 30
Copyright 2012 Healthcare Research & Resolutions. This information is not intended to replace the advice of a healthcare professional or an attorney.
criteria are met
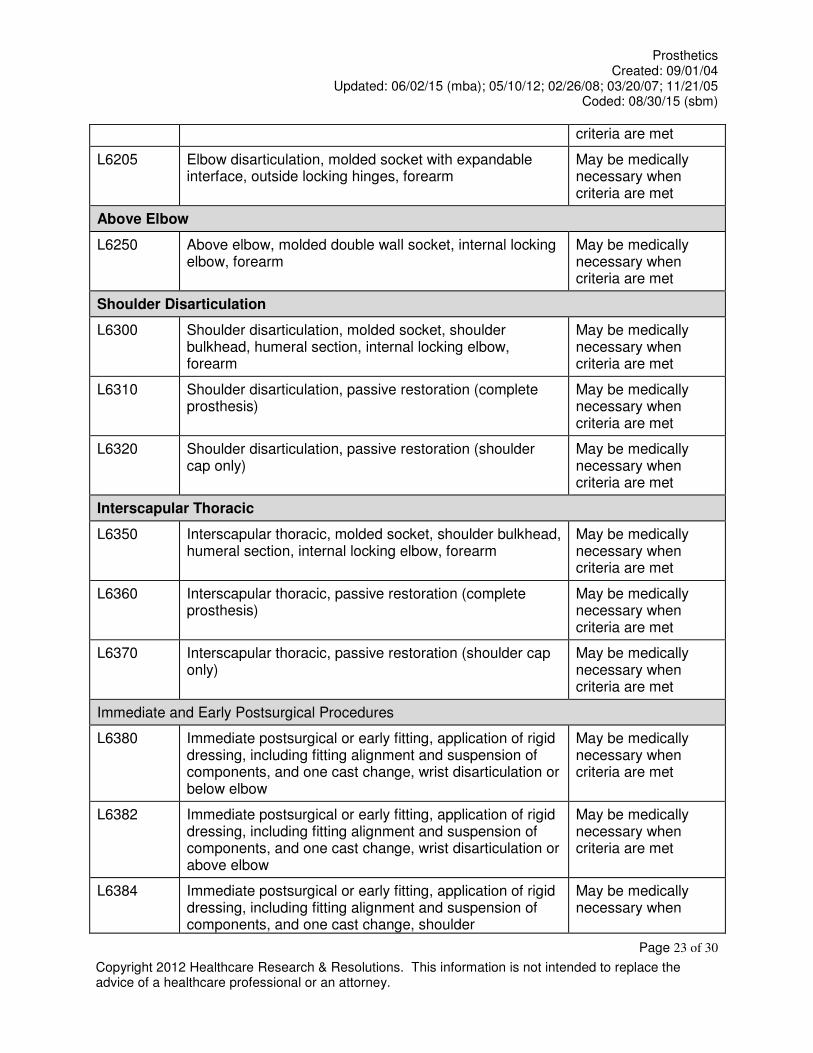
L6205 Elbow disarticulation, molded socket with expandable interface, outside locking hinges, forearm
May be medically necessary when criteria are met
Above Elbow
L6250 Above elbow, molded double wall socket, internal locking elbow, forearm
May be medically necessary when criteria are met
Shoulder Disarticulation
L6300 Shoulder disarticulation, molded socket, shoulder bulkhead, humeral section, internal locking elbow, forearm
May be medically necessary when criteria are met
L6310 Shoulder disarticulation, passive restoration (complete prosthesis)
May be medically necessary when criteria are met
L6320 Shoulder disarticulation, passive restoration (shoulder cap only)
May be medically necessary when criteria are met
Interscapular Thoracic
L6350 Interscapular thoracic, molded socket, shoulder bulkhead, humeral section, internal locking elbow, forearm
May be medically necessary when criteria are met
L6360 Interscapular thoracic, passive restoration (complete prosthesis)
May be medically necessary when criteria are met
L6370 Interscapular thoracic, passive restoration (shoulder cap only)
May be medically necessary when criteria are met
Immediate and Early Postsurgical Procedures
L6380 Immediate postsurgical or early fitting, application of rigid dressing, including fitting alignment and suspension of components, and one cast change, wrist disarticulation or below elbow
May be medically necessary when criteria are met
L6382 Immediate postsurgical or early fitting, application of rigid dressing, including fitting alignment and suspension of components, and one cast change, wrist disarticulation or above elbow
May be medically necessary when criteria are met
L6384 Immediate postsurgical or early fitting, application of rigid dressing, including fitting alignment and suspension of components, and one cast change, shoulder
May be medically necessary when

Prosthetics Created: 09/01/04
Updated: 06/02/15 (mba); 05/10/12; 02/26/08; 03/20/07; 11/21/05 Coded: 08/30/15 (sbm)
Page 24 of 30
Copyright 2012 Healthcare Research & Resolutions. This information is not intended to replace the advice of a healthcare professional or an attorney.
disarticulation or interscapular thoracic criteria are met
L6386 Immediate postsurgical or early fitting, each additional cast change and realignment
May be medically necessary when criteria are met
L6388 Immediate postsurgical or early fitting, application of rigid dressing only
May be medically necessary when criteria are met
Endoskeletal: Below Elbow
L6400 Below elbow, molded socket, endoskeletal system, including soft prosthetic tissue shaping
May be medically necessary when criteria are met
Endoskeletal: Elbow Disarticulation
L6450 Elbow disarticulation, molded socket, endoskeletal system, including soft prosthetic tissue shaping
May be medically necessary when criteria are met
Endoskeletal: Above Elbow
L6500 Above elbow, molded socket, endoskeletal system, including soft prosthetic tissue shaping
May be medically necessary when criteria are met
Endoskeletal: Shoulder Disarticulation
L6550 Shoulder disarticulation, molded socket, endoskeletal system, including soft prosthetic tissue shaping
May be medically necessary when criteria are met
Endoskeletal: Interscapular Thoracic
L6570 Interscapular thoracic, molded socket, endoskeletal system, including soft prosthetic tissue shaping
May be medically necessary when criteria are met
L6580 Preparatory, wrist disarticulation or below elbow, single wall plastic socket, friction wrist, flexible elbow hinges, figure of eight harness, humeral cuff, Bowden cable control, “USMC” or equal pylon, no cover, molded to patient model
May be medically necessary when criteria are met
L6582 Preparatory, wrist disarticulation or below elbow, single wall socket, friction wrist, flexible elbow hinges, figure of eight harness, humeral cuff, Bowden cable control, “USMC” or equal pylon, no cover, direct formed
May be medically necessary when criteria are met
L6584 Preparatory, wrist disarticulation or above elbow, single wall plastic socket, friction wrist, locking elbow, figure of eight harness, fair lead cable control, “USMC” or equal
May be medically necessary when criteria are met

Prosthetics Created: 09/01/04
Updated: 06/02/15 (mba); 05/10/12; 02/26/08; 03/20/07; 11/21/05 Coded: 08/30/15 (sbm)
Page 25 of 30
Copyright 2012 Healthcare Research & Resolutions. This information is not intended to replace the advice of a healthcare professional or an attorney.
pylon, no cover, molded to patient model
L6586 Preparatory, elbow disarticulation or above elbow, single wall socket, friction wrist, locking elbow, figure of eight harness, fair lead cable control, “USMC” or equal pylon, no cover, direct formed
May be medically necessary when criteria are met
L6588 Preparatory, shoulder disarticulation or interscapular thoracic, single wall plastic socket, shoulder joint, locking elbow, friction wrist, chest strap, fair lead cable control, “USMC” or equal pylon, no cover, molded to patient model
May be medically necessary when criteria are met
L6590 Preparatory, shoulder disarticulation or interscapular thoracic, single wall socket, shoulder joint, locking elbow, friction wrist, chest strap, fair lead cable control, “USMC” or equal pylon, no cover direct formed
May be medically necessary when criteria are met
Additions: Upper Limb
L6600 Upper extremity additions, polycentric hinge, pair May be medically necessary when criteria are met
L6605 Upper extremity additions, single pivot hinge, pair May be medically necessary when criteria are met
L6610 Upper extremity additions, flexible metal hinge, pair May be medically necessary when criteria are met
L6611 Addition to upper extremity prosthesis, external powered, additional switch, any type
May be medically necessary when criteria are met
L6615 Upper extremity addition, disconnect locking wrist unit May be medically necessary when criteria are met
L6616 Upper extremity addition, additional disconnect insert for locking wrist unit, each
May be medically necessary when criteria are met
L6620 Upper extremity addition, flexion/extension wrist unit, with or without friction
May be medically necessary when criteria are met
L6621 Upper extremity prosthesis addition, flexion/extension wrist with or without friction, for use with external powered terminal device
May be medically necessary when criteria are met
L6623 Upper extremity addition, spring assisted rotational wrist May be medically necessary when
Prosthetics Created: 09/01/04
Updated: 06/02/15 (mba); 05/10/12; 02/26/08; 03/20/07; 11/21/05 Coded: 08/30/15 (sbm)
Page 26 of 30
Copyright 2012 Healthcare Research & Resolutions. This information is not intended to replace the advice of a healthcare professional or an attorney.
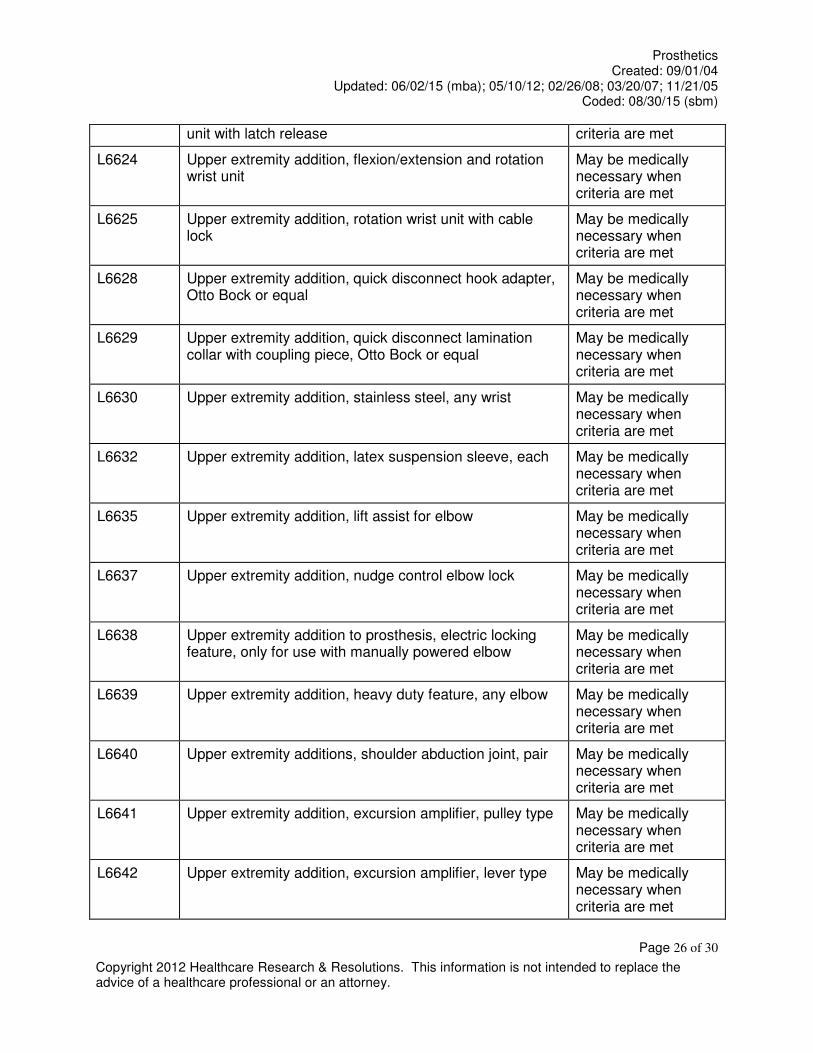
unit with latch release criteria are met
L6624 Upper extremity addition, flexion/extension and rotation wrist unit
May be medically necessary when criteria are met
L6625 Upper extremity addition, rotation wrist unit with cable lock
May be medically necessary when criteria are met
L6628 Upper extremity addition, quick disconnect hook adapter, Otto Bock or equal
May be medically necessary when criteria are met
L6629 Upper extremity addition, quick disconnect lamination collar with coupling piece, Otto Bock or equal
May be medically necessary when criteria are met
L6630 Upper extremity addition, stainless steel, any wrist May be medically necessary when criteria are met
L6632 Upper extremity addition, latex suspension sleeve, each May be medically necessary when criteria are met
L6635 Upper extremity addition, lift assist for elbow May be medically necessary when criteria are met
L6637 Upper extremity addition, nudge control elbow lock May be medically necessary when criteria are met
L6638 Upper extremity addition to prosthesis, electric locking feature, only for use with manually powered elbow
May be medically necessary when criteria are met
L6639 Upper extremity addition, heavy duty feature, any elbow May be medically necessary when criteria are met
L6640 Upper extremity additions, shoulder abduction joint, pair May be medically necessary when criteria are met
L6641 Upper extremity addition, excursion amplifier, pulley type May be medically necessary when criteria are met
L6642 Upper extremity addition, excursion amplifier, lever type May be medically necessary when criteria are met
Prosthetics Created: 09/01/04
Updated: 06/02/15 (mba); 05/10/12; 02/26/08; 03/20/07; 11/21/05 Coded: 08/30/15 (sbm)
Page 27 of 30
Copyright 2012 Healthcare Research & Resolutions. This information is not intended to replace the advice of a healthcare professional or an attorney.
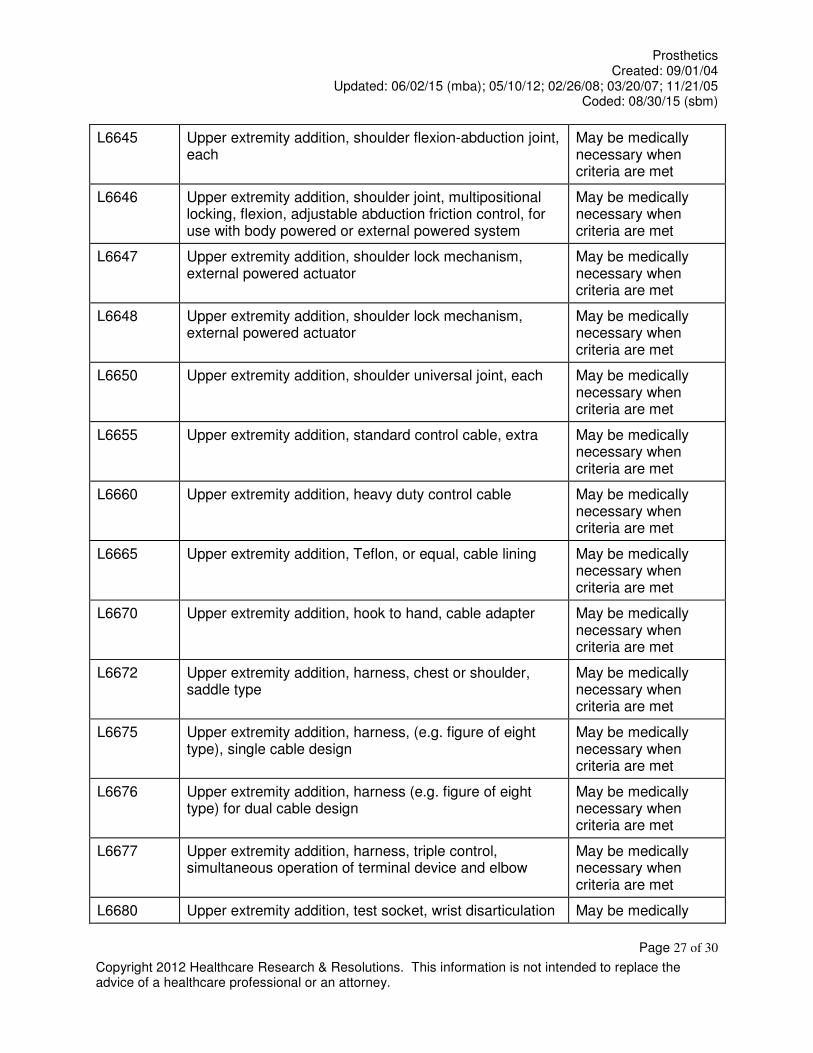
L6645 Upper extremity addition, shoulder flexion-abduction joint, each
May be medically necessary when criteria are met
L6646 Upper extremity addition, shoulder joint, multipositional locking, flexion, adjustable abduction friction control, for use with body powered or external powered system
May be medically necessary when criteria are met
L6647 Upper extremity addition, shoulder lock mechanism, external powered actuator
May be medically necessary when criteria are met
L6648 Upper extremity addition, shoulder lock mechanism, external powered actuator
May be medically necessary when criteria are met
L6650 Upper extremity addition, shoulder universal joint, each May be medically necessary when criteria are met
L6655 Upper extremity addition, standard control cable, extra May be medically necessary when criteria are met
L6660 Upper extremity addition, heavy duty control cable May be medically necessary when criteria are met
L6665 Upper extremity addition, Teflon, or equal, cable lining May be medically necessary when criteria are met
L6670 Upper extremity addition, hook to hand, cable adapter May be medically necessary when criteria are met
L6672 Upper extremity addition, harness, chest or shoulder, saddle type
May be medically necessary when criteria are met
L6675 Upper extremity addition, harness, (e.g. figure of eight type), single cable design
May be medically necessary when criteria are met
L6676 Upper extremity addition, harness (e.g. figure of eight type) for dual cable design
May be medically necessary when criteria are met
L6677 Upper extremity addition, harness, triple control, simultaneous operation of terminal device and elbow
May be medically necessary when criteria are met
L6680 Upper extremity addition, test socket, wrist disarticulation May be medically

Prosthetics Created: 09/01/04
Updated: 06/02/15 (mba); 05/10/12; 02/26/08; 03/20/07; 11/21/05 Coded: 08/30/15 (sbm)
Page 28 of 30
Copyright 2012 Healthcare Research & Resolutions. This information is not intended to replace the advice of a healthcare professional or an attorney.
or below elbow necessary when criteria are met
L6682 Upper extremity addition, test socket, elbow disarticulation or above elbow
May be medically necessary when criteria are met
L6684 Upper extremity addition, test socket, shoulder disarticulation or interscapular thoracic
May be medically necessary when criteria are met
L6686 Upper extremity addition, suction socket May be medically necessary when criteria are met
L6687 Upper extremity addition, frame type socket, below elbow or wrist disarticulation
May be medically necessary when criteria are met
L6688 Upper extremity addition, frame type socket, above elbow or elbow disarticulation
May be medically necessary when criteria are met
L6689 Upper extremity addition, frame type socket, shoulder disarticulation
May be medically necessary when criteria are met
L6690 Upper extremity addition, frame type socket, interscapular-thoracic
May be medically necessary when criteria are met
L6691 Upper extremity addition, removable insert, each May be medically necessary when criteria are met
L6692 Upper extremity addition, silicone gel insert or equal, each
May be medically necessary when criteria are met
L6693 Upper extremity addition, locking elbow, forearm counterbalance
May be medically necessary when criteria are met
L6694 Addition to upper extremity prosthesis, below elbow/ above elbow, custom fabricated from existing mold or prefabricated, socket insert, silicone gel, elastomeric or equal, not for use with locking mechanism
May be medically necessary when criteria are met
L6695 Addition to upper extremity prosthesis, below elbow/ above elbow, custom fabricated from existing mold or prefabricated, socket insert, silicone gel, elastomeric or equal, not for use with locking mechanism
May be medically necessary when criteria are met

Prosthetics Created: 09/01/04
Updated: 06/02/15 (mba); 05/10/12; 02/26/08; 03/20/07; 11/21/05 Coded: 08/30/15 (sbm)
Page 29 of 30
Copyright 2012 Healthcare Research & Resolutions. This information is not intended to replace the advice of a healthcare professional or an attorney.
L6696 Addition to upper extremity prosthesis, below elbow/ above elbow, custom fabricated socket insert for congenital or atypical traumatic amputee, silicone gel, elastomeric or equal, for use with or without locking mechanism, initial only (for other than initial, use code L6694 or L6695
May be medically necessary when criteria are met
L6697 Addition to upper extremity prosthesis, below elbow/ above elbow, custom fabricated socket insert for other than congenital or atypical traumatic amputee, silicone gel, elastomeric or equal, for use with or without locking mechanism, initial only (for other than initial, use code L6694 or L6695
May be medically necessary when criteria are met
L6698 Addition to upper extremity prosthesis, below elbow/ above elbow, lock mechanism, excludes socket insert
May be medically necessary when criteria are met
Terminal Devices
Hooks
L6703 Terminal device, hook, Dorrance or equal, model #3 May be medically necessary when criteria are met
L6704 Terminal device sport/recreational/work attachment, any material, any size
May be medically necessary when criteria are met
L6706 Terminal device, hook, mechanical, voluntary opening, any material, any size, lined or unlined
May be medically necessary when criteria are met
L6707 Terminal device, hook, mechanical, voluntary closing, any material, any size, lined or unlined
May be medically necessary when criteria are met
L6708 Terminal device, hand, mechanical, voluntary opening, any material, any size
May be medically necessary when criteria are met
L6709 Terminal device, hand, mechanical, voluntary closing, any material, any size
May be medically necessary when criteria are met
L6711 Terminal device, hook, mechanical, voluntary opening, any material, any size, lined or unlined, pediatric
May be medically necessary when criteria are met
L6712 Terminal device, hook, mechanical, voluntary closing, any material, any size, lined or unlined, pediatric
May be medically necessary when criteria are met

Prosthetics Created: 09/01/04
Updated: 06/02/15 (mba); 05/10/12; 02/26/08; 03/20/07; 11/21/05 Coded: 08/30/15 (sbm)
Page 30 of 30
Copyright 2012 Healthcare Research & Resolutions. This information is not intended to replace the advice of a healthcare professional or an attorney.
L6713 Terminal device, hand, mechanical, voluntary opening, any material, any size, pediatric
May be medically necessary when criteria are met
L6714 Terminal device, hand, mechanical, voluntary closing, any material, any size, pediatric
May be medically necessary when criteria are met
L6715 Terminal device, multiple articulating digit, includes motor(s), initial issue or replacement
May be medically necessary when criteria are met
L6721 Terminal device, hook or hand, heavy-duty, mechanical, voluntary opening, any material, any size, lined or unlined
May be medically necessary when criteria are met
L6722 Terminal device, hook or hand, heavy-duty, mechanical, voluntary closing, any material, any size, lined or unlined
May be medically necessary when criteria are met
REFERENCES
i The Free Medical Dictionary web site. Prosthetics. Available at: http://www.thefreedictionary.com/prosthetics. Accessed April 10, 2015. ii Turek PJ, Master VA, et al. Safety and efficacy of a new saline filled prosthesis. J Urol. 2004;172(4):1427-1430. iii Hayes, Inc. web site. Search & Summary. Proprio Foot (Össur). July 8, 2013. Available to subscribers at: www.hayesinc.com. Accessed April 23, 2015. iv Traballesi M, Delussu AS, Fusco A, et al. Residual limb wounds or ulcers heal in transtibial amputees using an active suction socket system. A randomized controlled study. Eur J Phys Rehabil Med. 2012;48(4):613-623. v American Academy of Orthotists & Prosthetists web site. Outcome measures in lower limb prosthetics. Available at: www.oandp.org. Accessed April 20, 2015.